radioprotectors 130719061711-phpapp02
TRANSCRIPT

RADIOPROTECTORS
Dr. KhaleelMODERATOR:-Dr. Arpitha
6/5/14 Time :2 ;30 pm

GOAL OF RADIATION THERAPY

Interventions in the development of
radiation adverse effects are classified as
Prophylaxis/Protection
Mitigation
Treatment

DEFINITIONS
Prophylaxis or protection
Any measure applied before the threshold dose
for the specific side-effect is reached.
Mitigation
Strategies used before the manifestation of clinical
symptoms(latent phase)
Treatment or management
In the symptomatic phase to reduce the side-
effects

WAYS TO IMPROVE THE PROTECTION OF NORMAL TISSUES

RATIONALES FOR USING RADIOPROTECTORS
Therapeutic ratio (TR) =TCP
NTCP
TCP = Tumor control probability
NTCP= Normal tissue complication probability
Efficacy/toxicity profile of radioprotectordepends on therapeutic ratio


IDEAL RADIOPROTECTOR
Preservation of the anti-tumor efficacy of radiation
Wide window of protection against all types of toxicity
High therapeutic ratio
High efficacy/toxicity profile(Low intrinsic toxicity
profile)
Easy and comfortable administration
Reasonable cost-effectiveness

HISTORICALLY KNOWN FACT
NH2
HS-CH2-CH
COOH
Problem was their toxicity
nausea and vomiting
General structure:
i. A free SH group at one end
ii. Strong basic function, i.e. an amine or guanidine at other

HISTORY OF DEVELOPMENT OF RADIOPROTECTERS

After World War II, a development programme was initiated in 1959 by the U.S. Army at the Walter Reed Institute of Research to identify and synthesize drugs capable of conferring protection to individuals in a radiation environment, but without the debilitating toxicity of cysteine or cysteamine.
Over 4,000 compounds were synthesized and tested.

TWO RADIOPROTECTORS IN PRACTICAL USE
CompoundDose
(mg/kg)
Dose reduction factor
Use
7 days (GI)30 days
(Haematopoetic)
WR-638
Cystaphos500 1.6 2.1
Carried in field pack by
Russian army
WR-2721
Amifostine900 1.8 2.7
Protector in radiotherapy
and carried by US
astronauts on lunar trips

First breakthrough to reduce toxicity-
covering the SH group with phosphate
Toxicity of the compound decreased b/c the
phosphate group is stripped inside the
cell, and the SH group begins
scavenging for free radicals.

EFFECT OF ADDING A PHOSPHATE-COVERING
FUNCTION ON THE FREE SH OF CYSTEAMINE
Drug Formula
Mean 50%
lethal dose
(Range) in
mice
Dose
reduction
factor
MEA
mercaptoethyl
amine
NH2-CH2-CH2-SH 343 (323-364)1.6 at
200mg/kg
MEA-PO3NH2-CH2-CH-
SH2PO3
777(700-864)2.1 at
500mg/kg

AMIFOSTINE(WR-2721)

Initially developed at the Walter Reed Army
Research Institute,USA
Under the Antiradiation Drug Development
Program of the US Army Medical Research
and Development Command (Schuchter and
Glick, 1993; Sweeney, 1979).
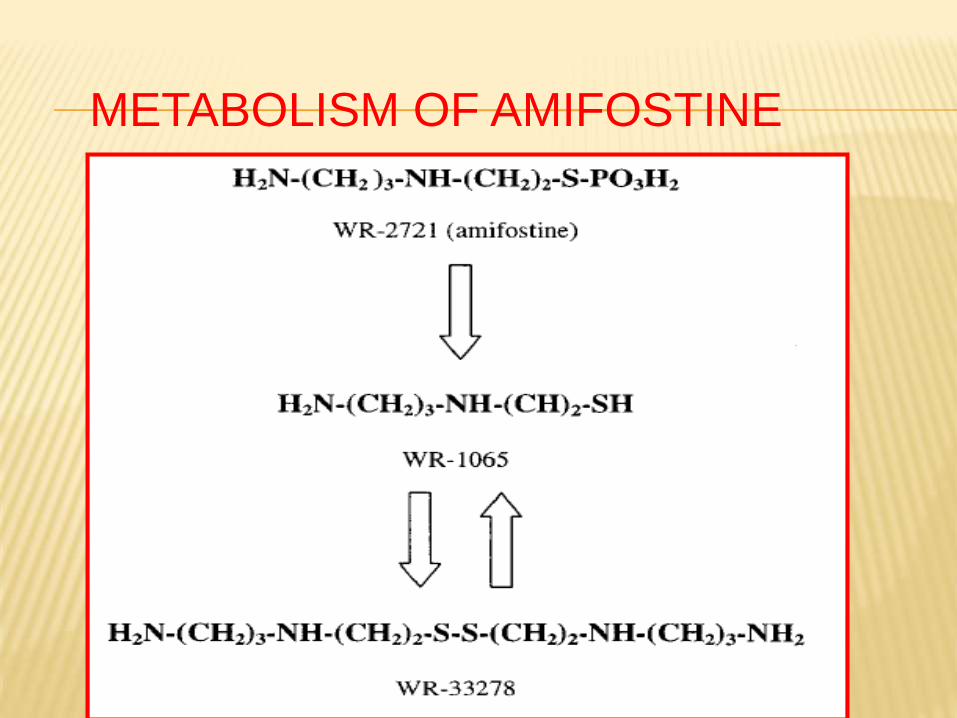
METABOLISM OF AMIFOSTINE

Amifostin (WR-2721)
Phosphorothioate prodrug-inactive, does not readily permeate cells.
Active thiol (WR 1065)
WR – 33278(polyamine like disulphide metabolite)
Radioprotection

WR-1065
i. Free radical scavenging-
Protects cellular membranes
and DNA from damage
ii. H2 atom donation
To facilitate direct chemical
repair at sites of DNA damage
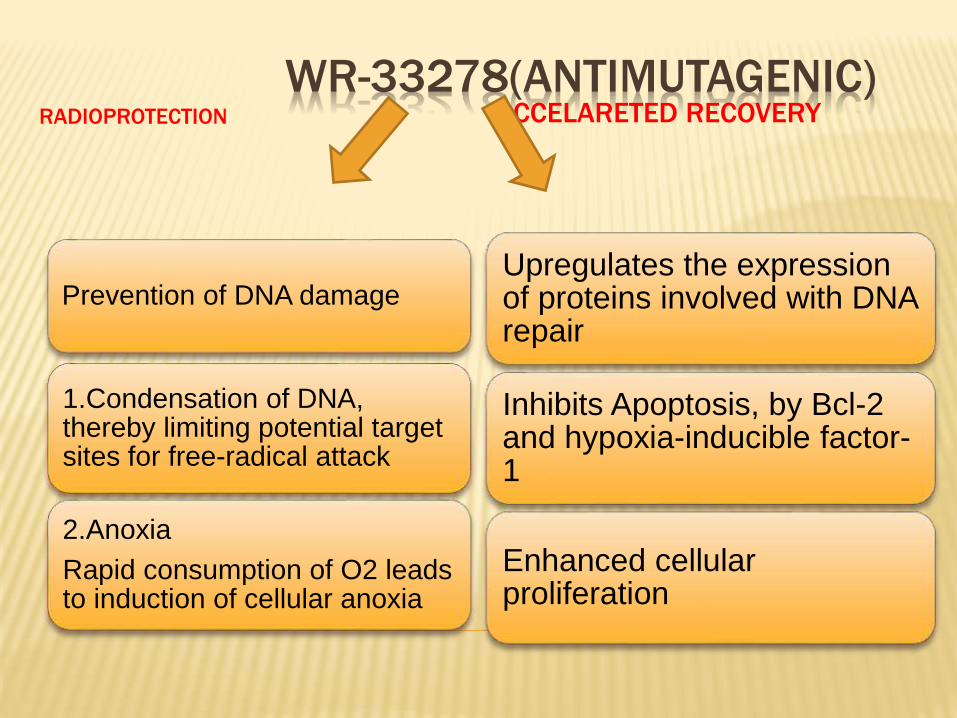
WR-33278(ANTIMUTAGENIC)RADIOPROTECTION ACCELARETED RECOVERY
Prevention of DNA damage
1.Condensation of DNA, thereby limiting potential target sites for free-radical attack
2.Anoxia
Rapid consumption of O2 leads to induction of cellular anoxia
Upregulates the expression of proteins involved with DNA repair
Inhibits Apoptosis, by Bcl-2 and hypoxia-inducible factor-1
Enhanced cellular proliferation
WHY SELECTIVE CYTOPROTECTION?
Differential expression of alkaline phosphatase
in tumor tissue
Hypovascularity & hypoxia
Acidic environment of the tumor
100 folds decreased concentration in tumor tissue

Absorption- Not orally bioavailable.
Distribution- Confined primarily to intravascular
compartment.
Once amifostine enters the plasma, it is rapidly
metabolized and the active metabolites are
distributed in the tissues.
Half life <1 min and >90% drug cleared from
plasma in 6 min after admin.
Amifostine is rapidly cleared from plasma ,
whereas the excretion of the metabolic products
is very slow.

DIFFERENTIAL UPTAKE
Extensive uptake is seen in:-
Salivary glands
Kidneys
Intestinal mucosa
Markedly lower uptake is seen in:-
Tumour tissues
Amifostine and metabolites do not cross the blood-brain barrier

TIMING OF ADMINISTRATION
Timely administration of amifostine is necessary.
Amifostine before 30 min. of RT provide optimal benefit for cytoprotection of normal tissues.
Single morning dose of amifostineprovides superior radioprotection than with a single afternoon dose

>30 min---NO difference

<30 min--- Difference present
ROUTES OF ADMINISTRATION
i.v. Amifostine
At a dose of 200 mg/m2 daily, given as a slow i.v. push over 3 minutes,15–30 minutes before each fraction of radiation therapy
Well hydrated and in supine position
Antiemetics.
B.P. should be measured before and immediately after the 3-minute amifostineinfusion.

s.c. Amifostine
s.c. injection of 500 mg of amifostine
Nausea
Fever/rash reaction
Hypotension
Endorectal
1,500 mg intra rectally 20 –30 minutes before each radiotherapy session
Useful for pelvic irradiation
Benefit demonstrated in a phase I study
SIDE EFFECTS
1. Nausea, vomiting & other GI effects
2. Transient hypotension- in 60%. Mean time of onset is 14 mins into infusion. BP reverts in 5-15 min.
3. Infusion related :- flushing and feeling of warmth, Chills, Dizziness, somnolence, hiccups & sneezing
4. Hypocalcemia in <1%- clinically asymptomatic by inhibition of PTH secretion
5. Metallic taste during infusion
6. Allergic reactions include rash, fever, and anaphylactic shock.

AMIFOSTINE
USE
IN RADIATION THERAPY

HEAD & NECK CANCERS
SCC of H&N
75% parotid gland was present in the fields
Dose was 200 mg/m2 daily,15–30 minutes before each fraction of radiation therapy
(1.8 –2.0 Gy/day, 5 days per week for 5–7 weeks, to a total dose of 50–70 Gy).


Amifostine significantly reduced acute and
late xerostomia and associated symptoms.
Saliva production after 1 year was
significantly higher with amifostine (72%
versus 49%; p .003).
At 1 year, with a median follow-up of 20
months, the LR tumor control rates did not
differ, and DFS & OS were comparable.

LUNG CANCER
Factor
studied
Amifostine+
RT
RT alone P value
Pneumonitis 9% 43% <0.001
Fibrosis 53% 28% <0.05
Esophagitis 4% 42% <0.001
CR or PR 75% 76%
•Antonadou et al.
•Dose:-340 mg/m2 15 minutes before
irradiation.
•No evidence of tumor protection

MDACC trial (Komaki et al. ):evaluated the
cytoprotective role of amifostine for
esophagitis . hematologic and pulmonary
toxicities in a randomized study of patients
with stage II or III non-small cell lung
cancer receiving concurrent
chemoradiotherapy.
Did reduce incidence and severity of
esophageal, pulmonary and hematologic
toxicity. Did not affect survival.

PELVIC MALIGNANCIES
Gasrointestinal mucositis
Various routes of administration of amifostine(i.v., s.c. and intrarectal) are effective.
Intrarectal administration was more effective at reducing radiotherapy-induced rectal toxicities.
s.c. administration was more effective at reducing radiotherapy-induced urinary toxicities.
Combined route for optimal cytoprotection.

STATUS
The U.S. FDA has approved the i.v. use of amifostinein:-
Patients with advanced ovarian cancer to
reduce the cumulative renal toxicity associated with repeated administration of cisplatin. (1996)
Patients undergoing postoperative radiation treatment for head and neck cancer, where the radiation port includes a substantial portion of the parotid glands to reduce the incidence of moderate to severe xerostomia.(1999)

ISSUE OF TUMOR PROTECTION
A meta-analysis (Sasse et al.,2006) concluded that
Amifostine does not affect the efficacy of radiotherapy
To the contrary, patients receiving amifostinewith RT achieved higher rates of complete response presumably the result of fewer treatment interruptions because of reduced acute toxicity of the treatment.

HERBAL RADIOPROTECTORS
WHY NOT USEDProtection of salivary glands could also be achieved by using IMRT.
Uncertain to what extent amifostine protects against fibrosis and other dose-limiting late reactions.
The optimal dosage and schedule of amifostine has not been established.
Major concern related to radioprotectors remains the potential hazard of tumor protection. Even the trial conducted by Brizel et al,73 which recruited over 300 patients, has had sufficient statistical power to detect and quantify a possible tumor protective effect of amifostine. the lack of statistical power in these studies hinders any firm conclusions being drawn regarding tumor protection.
T/t & toxicites cumbursome repeted puncture & hypotension.
