prp therapy for tendonitis fasciitis acute sprains and muscular lesions by ultrasonographic...
TRANSCRIPT

Ph ADAM, MDSports Clinic
Medipole Garonne Toulouse France
11ème congrès de la Société Marocaine
d’Arthroscopie03-04 Février 2017 à
Marrakech
PRP Therapy for Tendonitis Fasciitis Acute Sprains and Muscular Lesions
By UltraSonographic Guidance

Tobermory (Scotland, Mull Island)
A/Diagnosis with UltraSonic (US) Imaging is easy, rapid and inexpensive
1/ Accurate localization and palpation of lesions with Ultrasonic Probe : pain ? +++
2/ Morphological study (static and dynamic) is better, simpler and faster with US than with MRI
Hypoechogenic tendon+++ with loss of fibrillar structure Thickening Nodule Tendinous slot
Bursitis Enthesitis Muscular cavity Gap
3/Vascularization and Tissue Elasticity can be estimated

B/Treatment by US Guiding of needle and injection is efficient
1/ mechanical way : needling, tenotomy, evacuation of collection
2/ biochemical way : direct injection of PRP (growth factors)into a cavity and around tendon or fascia
(collagen synthesis and stimulation of cells)
C/US evaluation of anatomical improvement after PRP and correlation with clinical improvement
Pain Echogenicity Size of lesions
Vascularization Elasticity

Tendonitis and Fasciitis are Mechanical and Degenerative diseases
(collagen tears+++ neovessels)
Non-Inflammatory disease

« There is increasing evidence that EUS can be used to measure the mechanical properties of musculoskeletal tissue in clinical practice, with the future potential for early diagnosis to both guide and monitor therapy »
The British Journal of Radiology, 85 (2012), 1435–1445
REVIEW ARTICLE Ultrasound elastography for musculoskeletal
applications 1E E DRAKONAKI, MD, PhD, 2G M ALLEN, FRCR, MRCP and 2D J WILSON, FRCP,
FRCR

Efficacy of intra-tendinous injection of platelet-rich plasma in treating tendinosis : Comprehensive assessment of a rat model
Benjamin Dallaudière et al, Eur Radiol (2013) 23:2830–2837, DOI 10.1007/s00330-013-2926-7
PRP treatment for tendons is not a placebo !!!

Achille tendonitis : Double Needle Approach (premedication, meopa)

Achille tendonitis : Double Needle Approach (big slit)

Achille’s tendonitis : cavity in the body of tendon and nodule
Filling of cavity by PRP
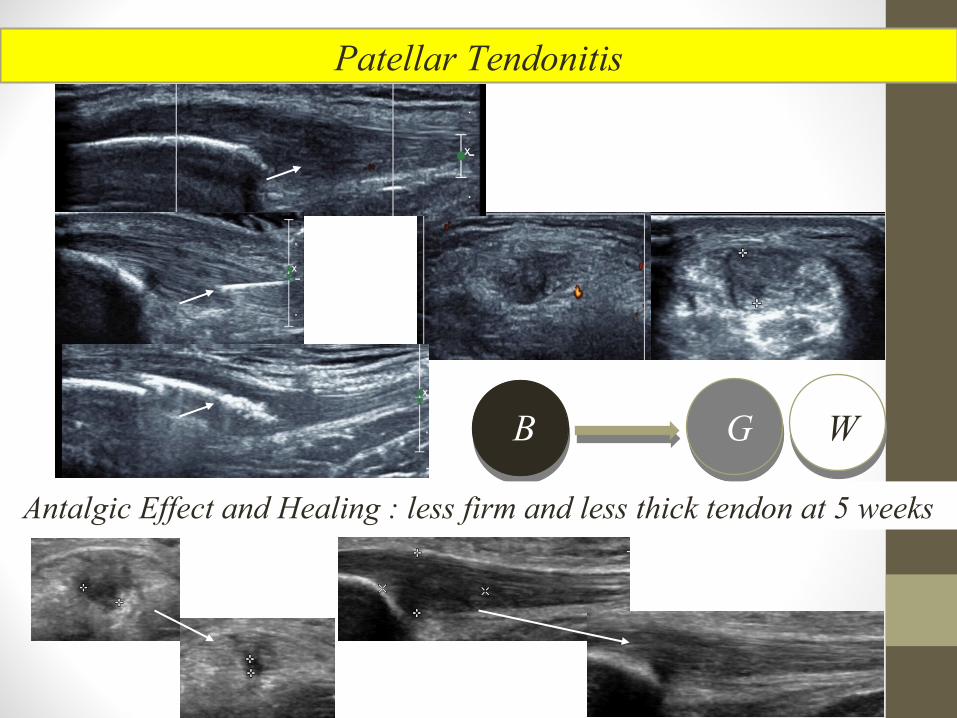
Antalgic Effect and Healing : less firm and less thick tendon at 5 weeks
Patellar Tendonitis
B G W

Patellar Tendonitis : 2 targets (upper, lower) , 2 needles
Lower part
Upper part
Vascularization is increased under patella

Patellar Tendonitis

US guided injection of PRP for elbow (lateral epicondylitis)

Lateral epicondylitis : PRP « filling » of intra-tendinous tear
Calcifying epicondylitis : PRP « crushing »

Edematous lateral epicondylitis (before and after)
After PRP tendon is thin and homogeneous
Vascularization is increased into the tendon

Posterior tibial tendonitis (ankle, table tennis)Injection of PRP around the tendon (synovial sheath)

Plantar Fasciitis : spreading of PRP under US control

Partial disruption of plantar fascia (rugby, before and after PRP, no pain 4 weeks)
Total disruption

Biceps Femoris tendonitis at the knee (fibular insertion)

US guided filling by PRP Pain and cleft decreased at one month
Rotator cuff tendonitis with tear (shoulder)
Brèche Supra-Epineux

Acute recent Lateral ankle Sprain and Chronic pain after Sprain
Needle under the anterior fascicle of collateral lateral ligament
Hypervascularization of the scar in front of synovial wall3 weeks after

Acute knee Sprain (Medial Collateral
Ligament)
Axial US plane
Coronal US plane
Separation between capsulo-meniscal plane and medial collateral ligament
PRP spreading

Bigard : J Traum Sport (2012) 29, 164-170
For muscular lesions we are also using biochemical way (growth factors : stimulation of promyoblastic cells
« stem cells like » for scaffolding)
And mechanical way (draining of haematoma and occupation of the empty space by muscular fascicles)
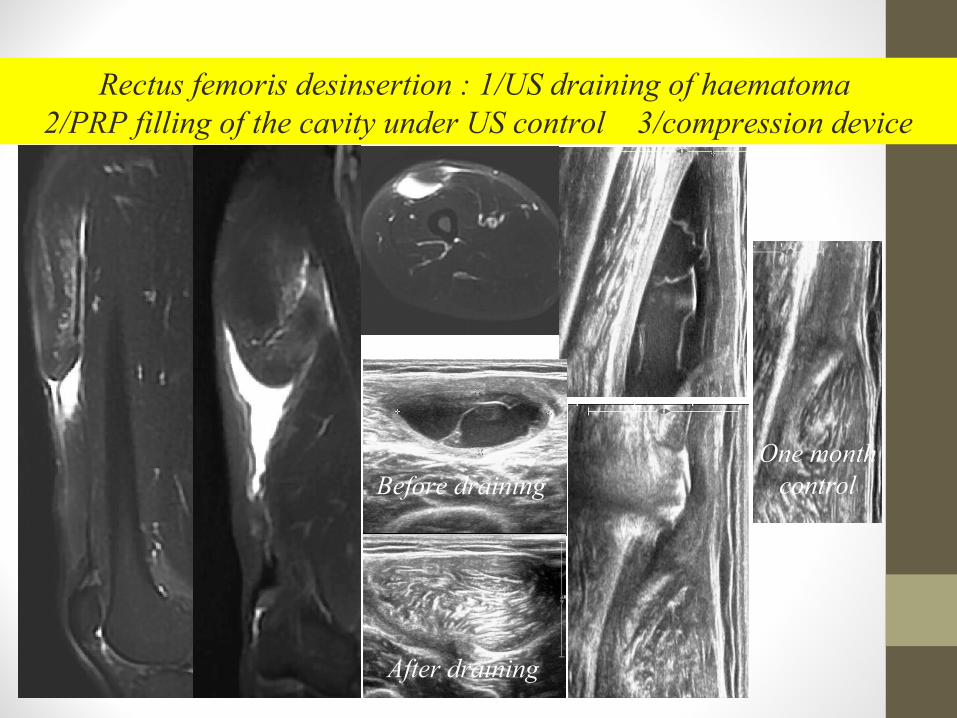
Rectus femoris desinsertion : 1/US draining of haematoma 2/PRP filling of the cavity under US control 3/compression device
After draining
Before drainingOne month
control

Adductor long muscle desinsersion : 1/US draining of haematoma 2/PRP filling of the cavity under US control 3/Compression device

Hamstring muscle is brocken at the ischiatic enthesis PRP therapy is a very good alternative to surgery

Groin Strain (soccer)

Myo-aponeurotic desinsertion : Medial Gastrocnemius
Slowly emptying then filling (US guiding)

Key Points (tendonitis, fasciitis, sprain, muscle)
*PRP treatment with US guidance is easy and accurate with poor risks and adverse effects very limited
*PRP treatment is usually performed with only one injection
*Healing speed is highly increased with PRP (in vitro and in vivo proved)
*PRP treatment is a team working (look after the cause of the
conflict and not only the consequence, sport overtraining)
*Early treatment = Early recovery for Sportmen
(very fast for muscle injuries)