post-graduate certifcate musculoskeletal ultrasound - the shoulder
TRANSCRIPT

Diagnostic Ultrasound of the Shoulder
Dr. Peter ResteghiniConsultant Physiotherapist Musculoskeletal MedicineMusculoskeletal Sonographer
Course Director Postgraduate Certificate Musculoskeletal Ultrasound
http://www.uel.ac.uk/study/courses/Musculoskeletal.htm
Why Ultrasound? A lack of ionising radiation (Grassi 2004). High spatial resolution, has multiplanar imaging
capability and is considered patient friendly due to its ease of tolerance and non-invasiveness (Wakefield 1999, Backhaus 2001, Tan 2003, Grassi 2004).
Scanning time is short (5-15 minutes for an experienced sonographer compared to approximately 40 minutes for an MRI – Swen 2001)
It provides not only anatomical information, but also informs on the physiological state of the joint, being particularly sensitive to inflammatory changes (Grassi 2003).
Ultrasound is also unique in that scanning occurs in real-time making it possible to discuss reproduction of symptoms with the patient, and to view dynamic images of the structures under examination. ((Tan 2003, Grassi 2000, Ellis 2002, Shirtley 1999).

Guided Injection Ultrasound guided shoulder girdle injections are more accurate and
more effective than landmark guided injections: a systematic review and meta-analysis (Aly, Rajasekaran, Ashworth 2014 )
Lack of aspirate from smaller joints such as the CMCJ of the thumb makes accurate needle placement in these joints also extremely difficult For this reason injections performed under imaging are becoming more popular (Balint 1997, Ghozlan and Vacher 2000, Koski 2000, Weidner et al 2004).
Eustace (1997) demonstrated that even in the hands of musculoskeletal specialists only a minority of injections for shoulder pain are performed accurately (29% of subacromial and 42% of intra-articular injections), not surprisingly outcome significantly correlated with accuracy of injection.
Similar results were found in patients with De Quervains tenosynovitis (Zhingis 1998).
Leopold (2001) assessed the accuracy of needle placement with intra-articular injection using only anatomic landmarks as a guide. Using this ‘blind’ approach the needle pierced or contacted the femoral nerve in 27% of anterior injections and was within 5mm of the femoral nerve in 60% of all anterior attempts. Using a lateral approach the needle was never within 25mm of any neurovascular structure in any injection however only 80% of injections managed to reach the joint cavity.
Ultrasound of the Shoulder Long head of
biceps Rotator cuff Bursa ACJ GHJ Impingement
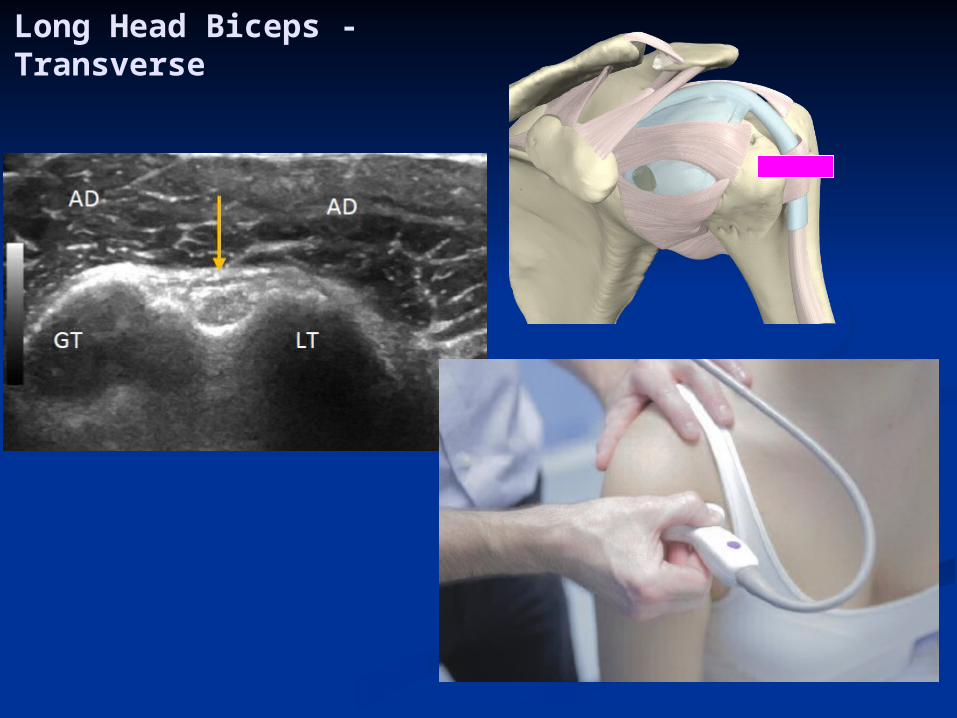
Long Head Biceps - Transverse
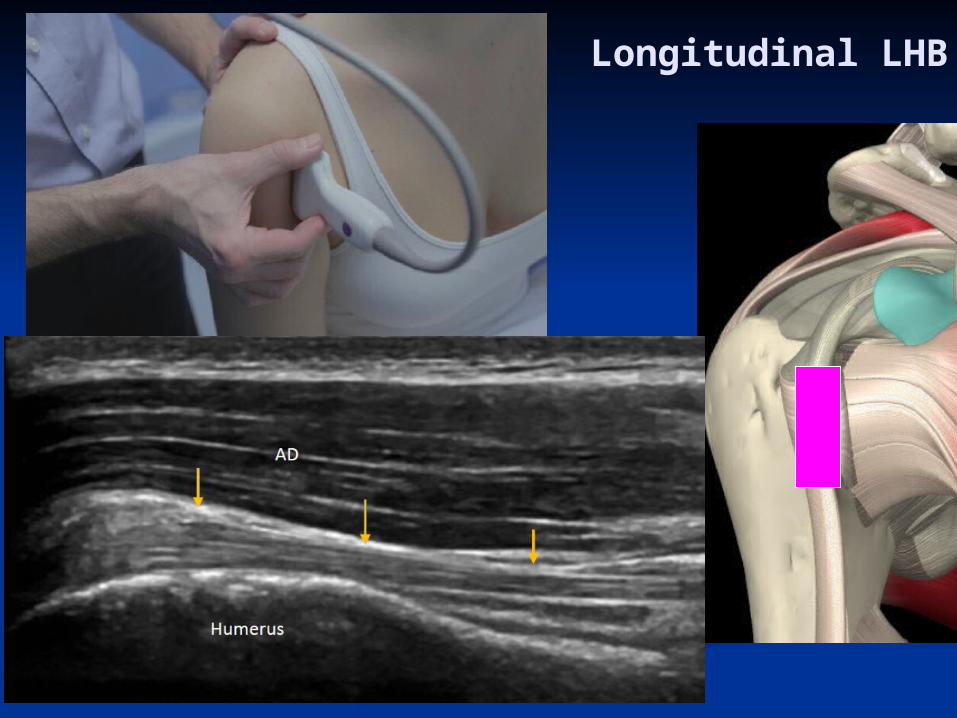
Longitudinal LHB

LHB - Proximal
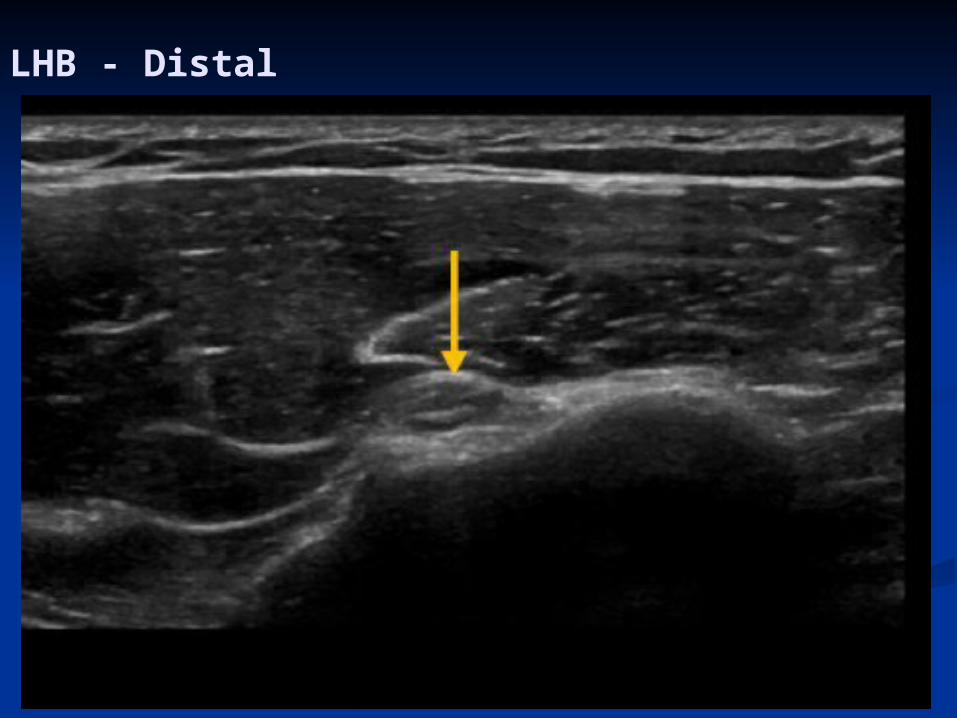
LHB - Distal

LHB – Tenosynovitis

Subluxed LHB
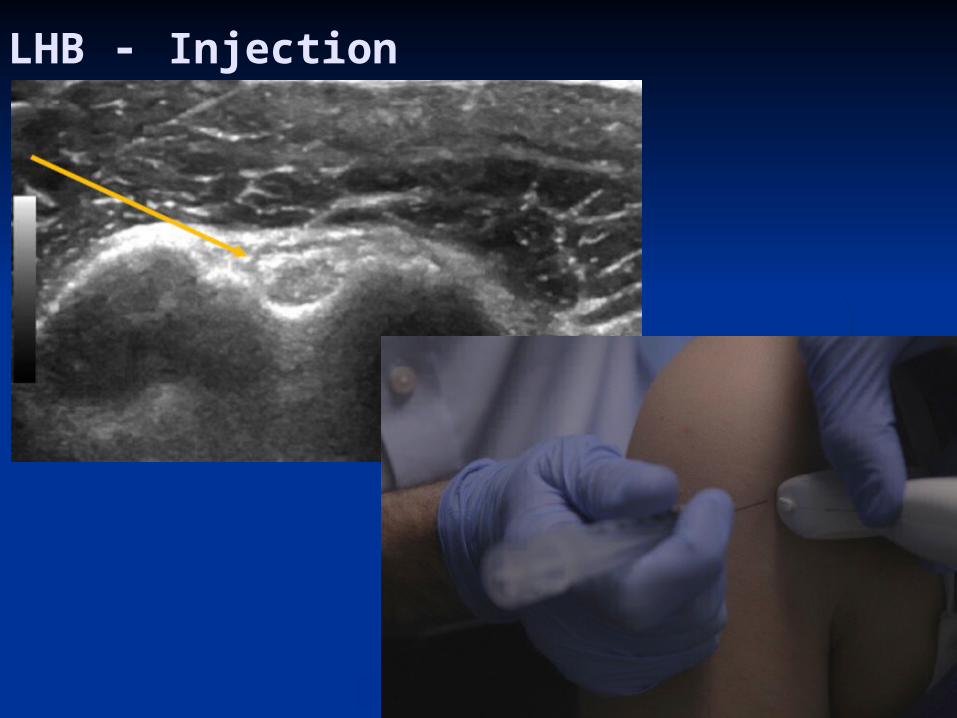
LHB - Injection
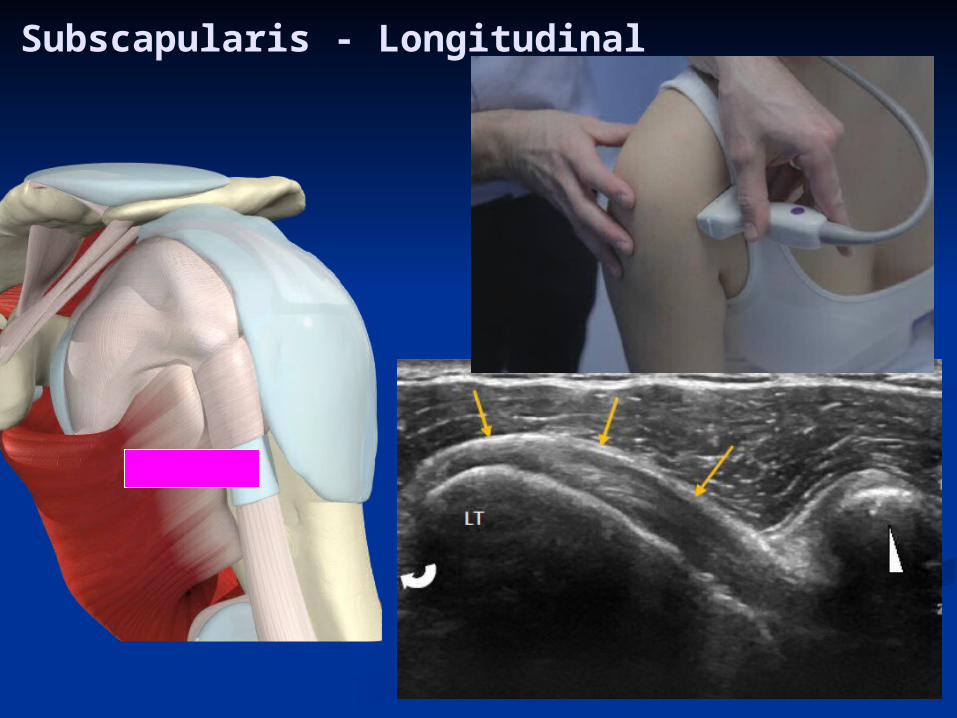
Subscapularis - Longitudinal

Medial
COR
SHB
SUBSCAP
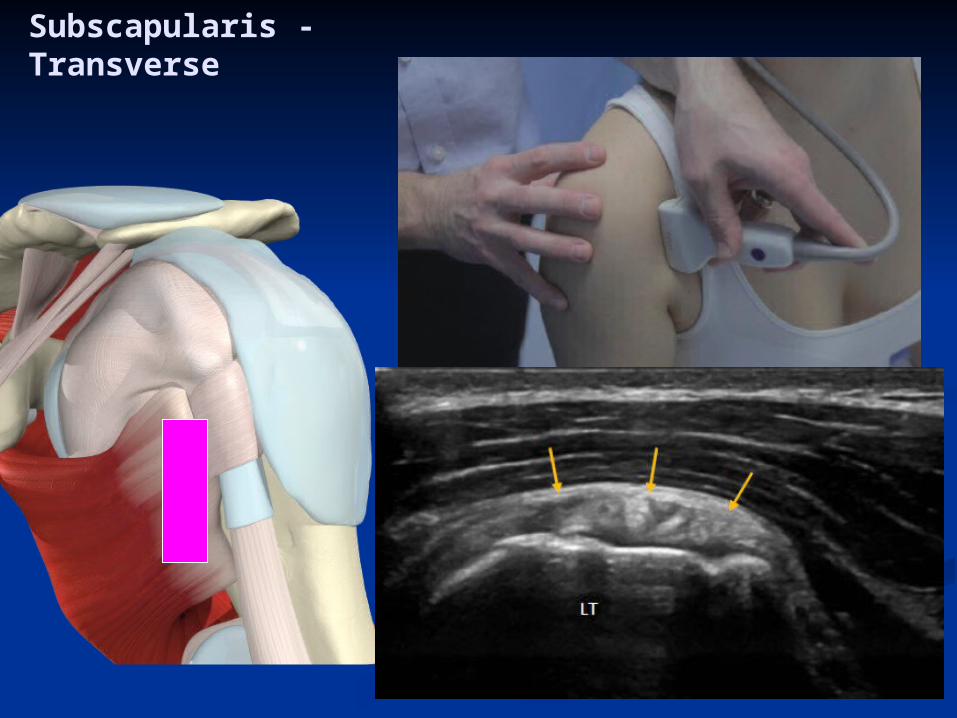
Subscapularis - Transverse


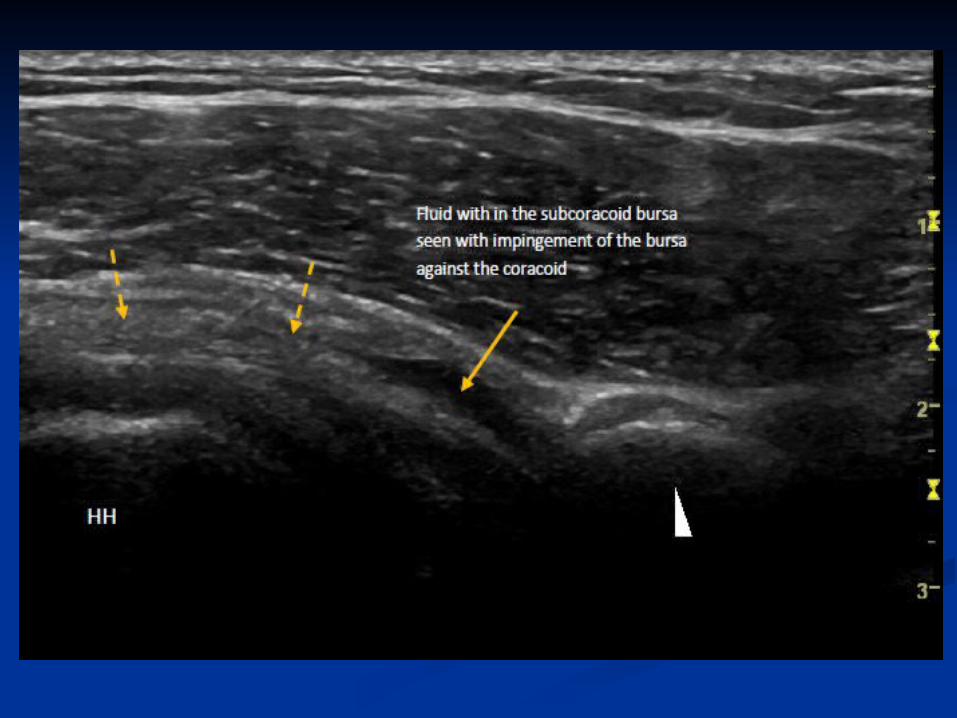

Sh thickened subcoracoid bursa with fluid and impingement.wmv
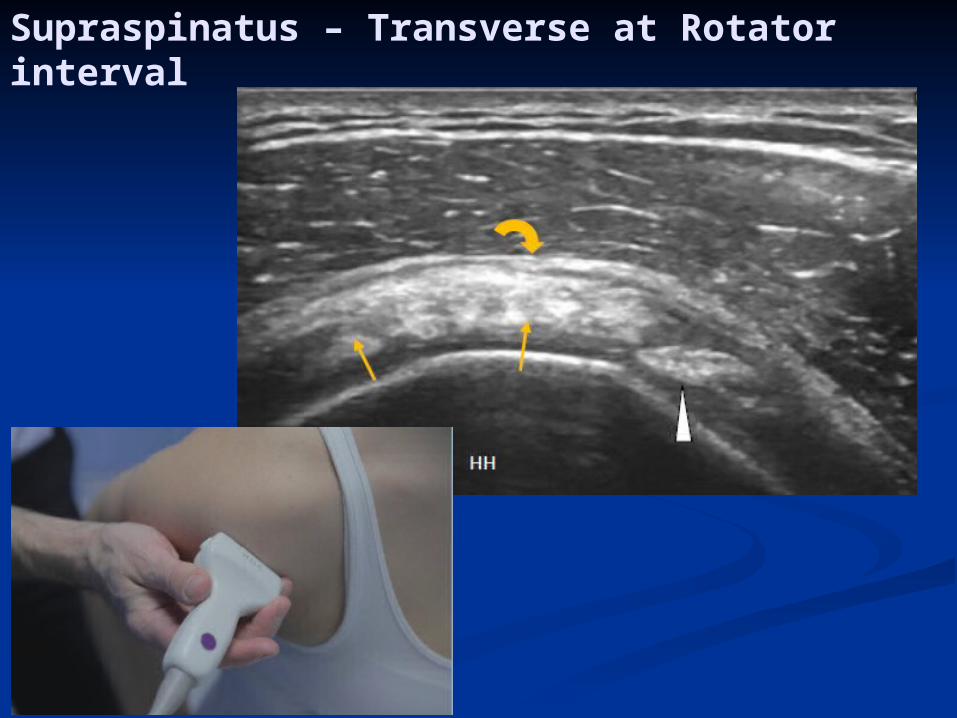
Supraspinatus – Transverse at Rotator interval
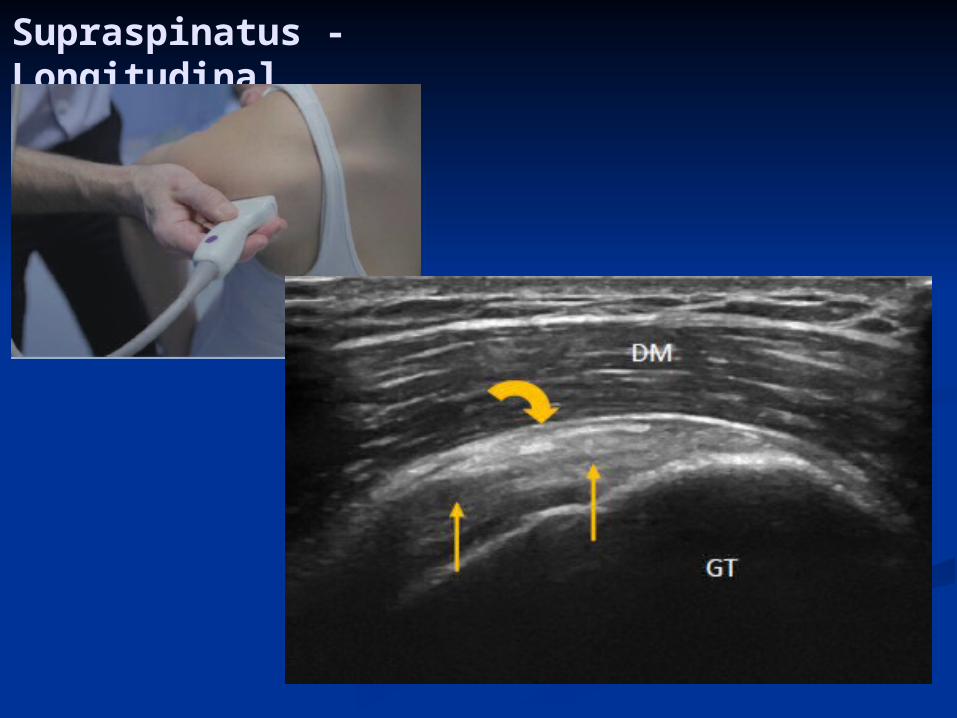
Supraspinatus - Longitudinal
Ultrasound – SST tears
Full thickness tears: sensitivity 96-100% specificity 85%Partial thickness tears: sensitivity 93% specificity 94%

Ultrasound and MRI are comparable in both sensitivity and specificity (Joseph 2009)
98.6% sensitivity & 99.3% specificity full thickness tears 97.9% sensitivity & 94.4% specificity partial thickness tears (Al Shawi, Bunker 2005)

Supraspinatus – complete rupture
Ruptures IST with associated posterior GHJ Effusion.wmv
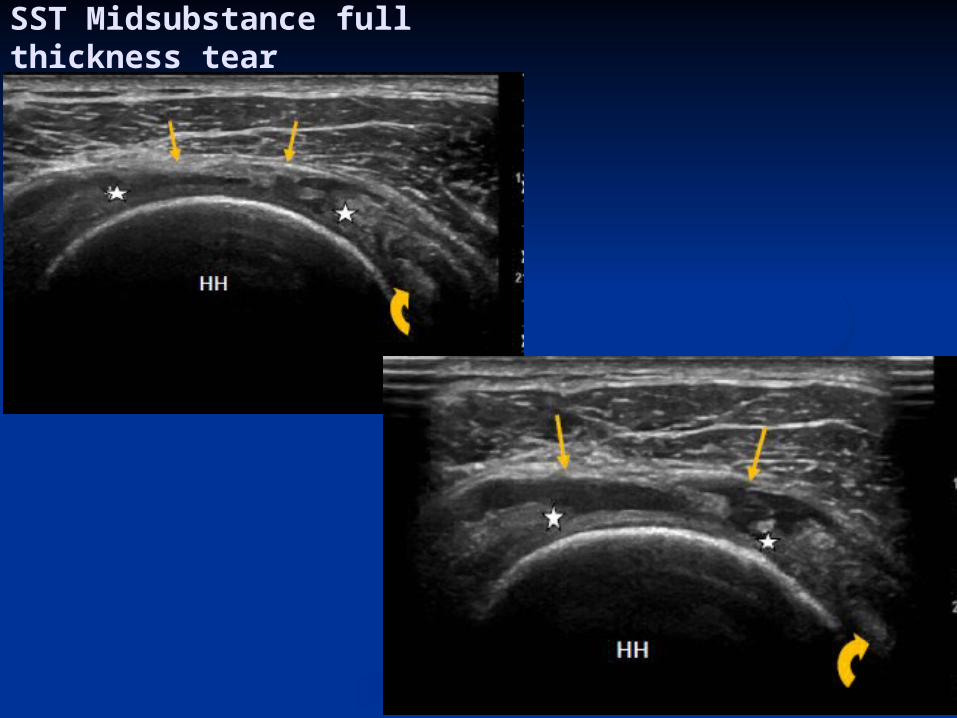
SST Midsubstance full thickness tear
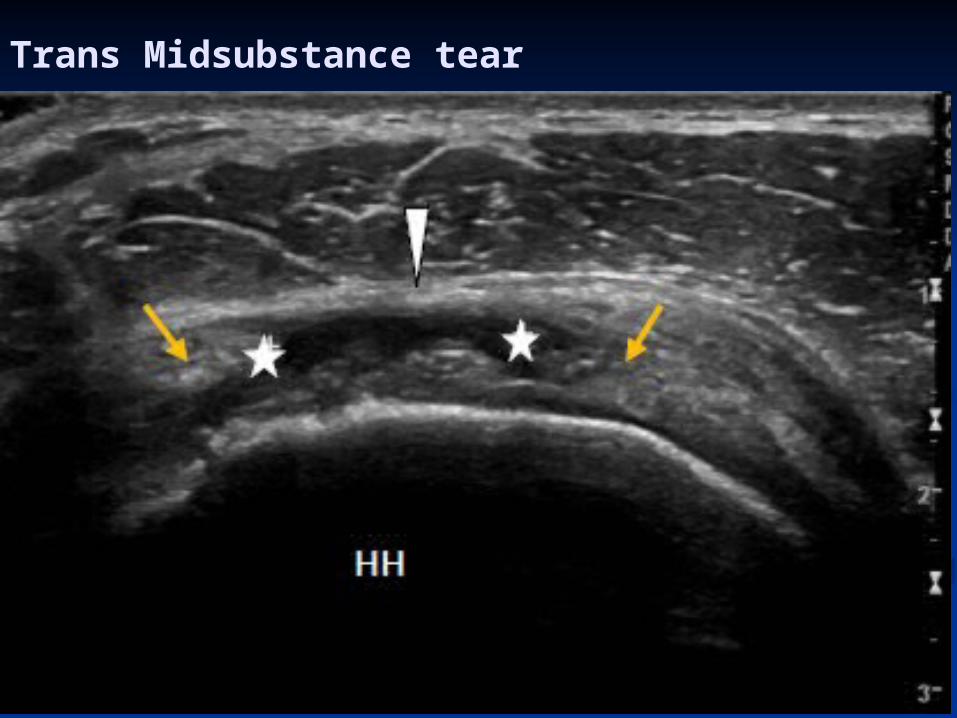
Trans Midsubstance tear

Impingement - Calcific SST & Subacromial bursa


Impingement SAB
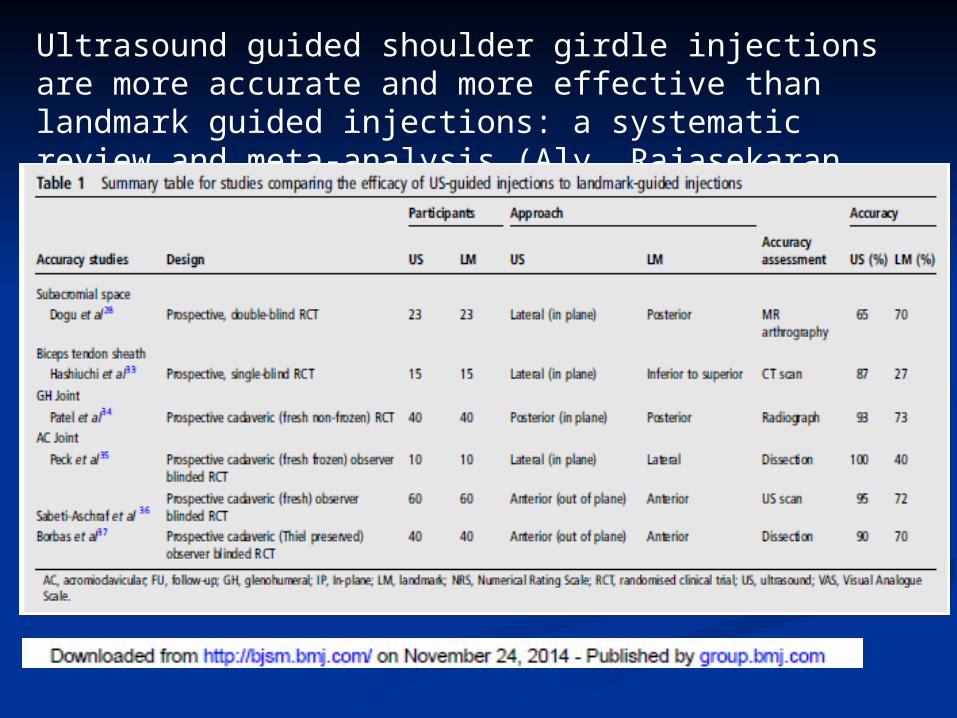
Ultrasound guided shoulder girdle injections are more accurate and more effective than landmark guided injections: a systematic review and meta-analysis (Aly, Rajasekaran, Ashworth 2014 BJSM)
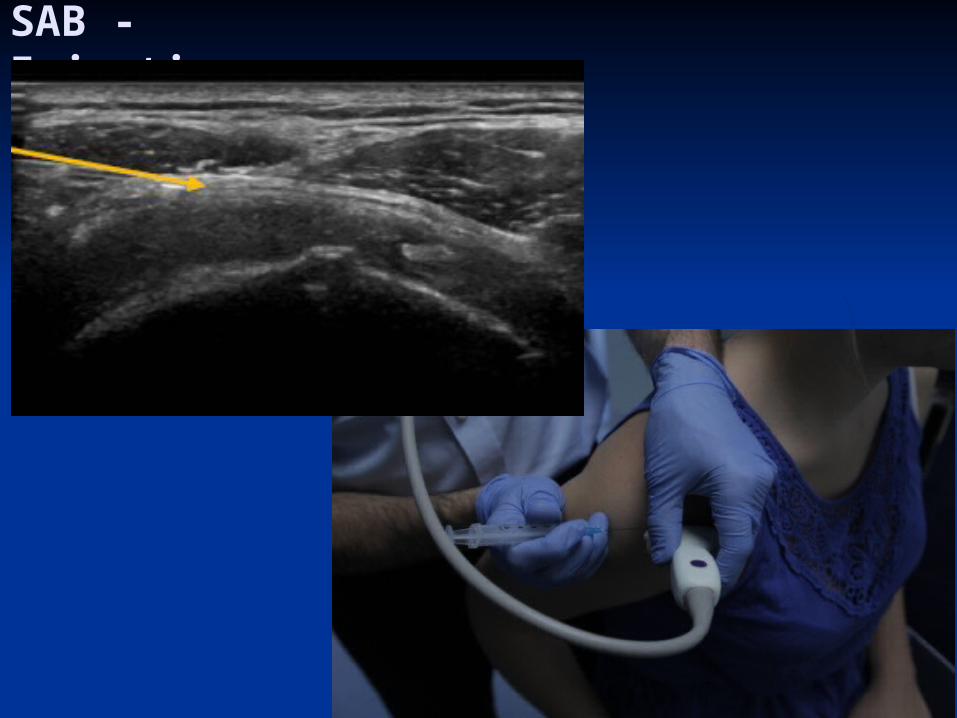
SAB - Injection

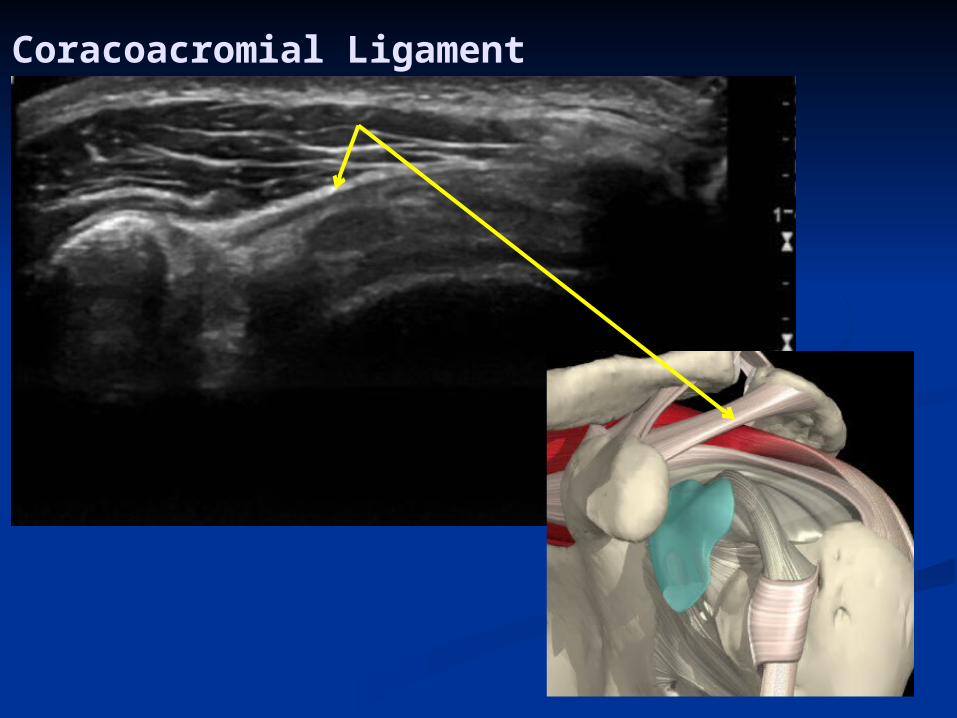
Coracoacromial Ligament

Infraspinatus
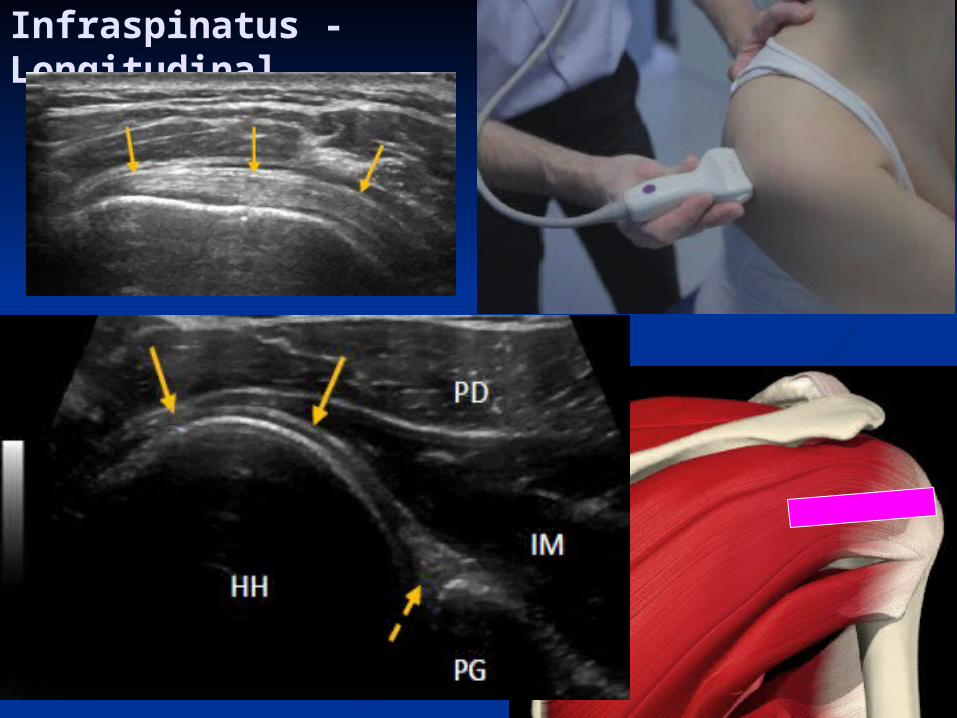
Infraspinatus - Longitudinal

Infraspinatus – complete rupture

SCJ - Injection

Acromioclavicular joint
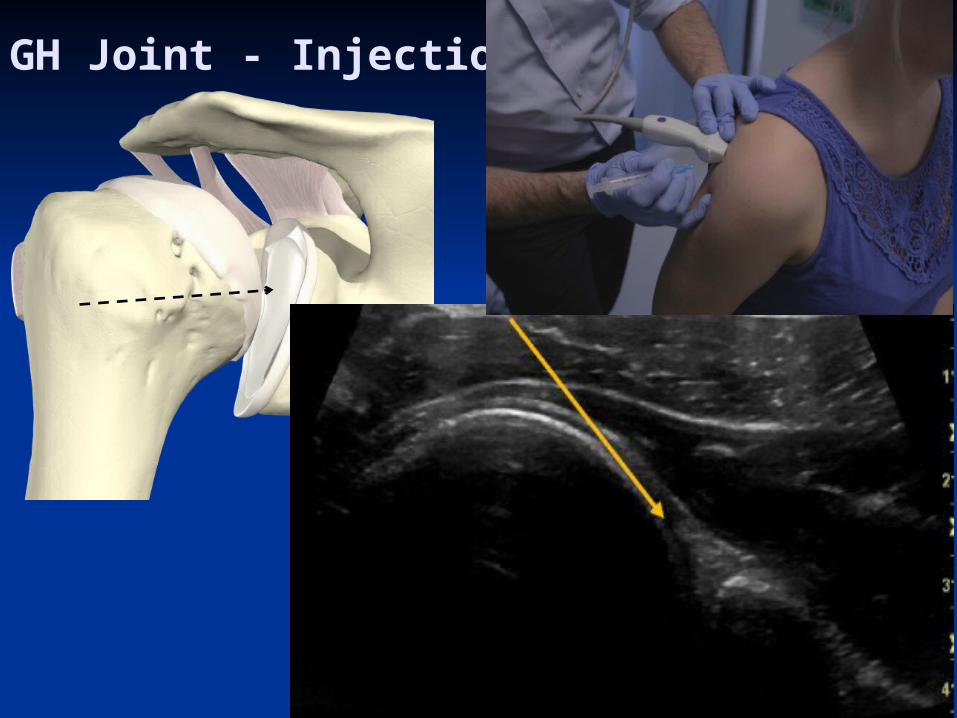
GH Joint - Injection

SN - Injection

Homerton University Hospital Department of Physiotherapy & Sports Medicine
Dr. Peter ResteghiniConsultant Physiotherapist Musculoskeletal MedicineMusculoskeletal Sonographer
Course Director Postgraduate Certificate Musculoskeletal Ultrasound
http://www.uel.ac.uk/study/courses/Musculoskeletal.htm