musculoskeletal trauma - american academy of … · 2016-11-14 · 2012 musculoskeletal trauma...
TRANSCRIPT

MusculoskeletalTrauma
2012Self-Assessment Examinati
onAnswer Book
P

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 9
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figure 1
Question 1Figure 1 is the radiograph of a 62-year-old woman who fell and sustained a left hip fracture. A radiograph is shown in Figure 1. Which of the following preoperative risk factors is associated with the highest postoperative mortality rate?
1. Fracture pattern 2. Chronic renal failure 3. Female gender 4. Coronary artery disease 5. Diabetes mellitus
PREFERRED RESPONSE: 2
DISCUSSION: In the study by Bhattacharyya and associates in 2002, they retrospectively reviewed over 43,000 in-patient orthopaedic procedures to identify preoperative risk factors associated with postoperative mortality. Their study identified five “critical” risk factors placing patients at increased risk for death. These included chronic renal failure, congestive heart failure, chronic obstructive pulmonary disease, hip fracture, and age of older than 70 years. Their study also demonstrated a linear increase in mortality observed with the increased number of risk factors. The risk factors of diabetes, gender, fracture pattern, coronary artery disease, peripheral vascular disease, septic arthritis, and rheumatoid arthritis did not achieve significance. Identification of patients with risk factors for mortality is important for individualizing treatment plans, accurate prognosis, and informed consent.
RECOMMENDED READING(S): Bhattacharyya T, Iorio R, Healy WL. Rate of and risk factors for acute inpatient mortality after orthopaedic surgery. J Bone Joint Surg Am. 2002 Apr;84-A(4):562-72. PubMed PMID: 11940616.Karaeminogullari O, Demirors H, Sahin O, Ozalay M, Ozdemir N, Tandogan RN. Analysis of outcomes for surgically treated hip fractures in patients undergoing chronic hemodialysis. J Bone Joint Surg Am. 2007 Feb;89(2):324-31. PubMed PMID: 17272447.

10 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 2A 37-year-old man fell from 24 feet and sustained a subarachnoid hemorrhage and closed femoral shaft fracture. What is most likely to lead to an adverse outcome?
1. Intraoperative hypotension 2. Temporizing external fixation 3. Elevated cerebral perfusion pressure 4. Immediate reamed intramedullary nailing 5. Skeletal traction with intramedullary nailing in 72 hours
PREFERRED RESPONSE: 1
DISCUSSION: In patients with femoral fractures and associated closed head injuries, there have been conflicting studies regarding timing of fracture care and eventual neurologic outcome. It is known that an episode of hypotension and elevated intracranial pressure will lower the cerebral perfusion pressure, which is known to be detrimental to the neurologic outcome. Intraoperative hypoxia may also worsen the neurologic outcome and increased fluid administration may elevate the intracranial pressure. If early fracture fixation is necessary, the intracranial pressure should be monitored and the cerebral perfusion pressure maintained during the procedure. Immediate reamed intramedullary nailing is appropriate if the patient is hemodynamically stable and the cerebral perfusion pressure is maintained. If not, external fixation would be appropriate treatment. Temporary skeletal traction may be appropriate if the intracranial pressure is labile and precludes the patient from going to the operating room.
RECOMMENDED READING(S): Anglen JO, Luber K, Park T. The effect of femoral nailing on cerebral perfusion pressure in head-injured patients. J Trauma. 2003 Jun;54(6):1166-70. PubMed PMID: 12813339.Pietropaoli JA, Rogers FB, Shackford SR, Wald SL, Schmoker JD, Zhuang J. The deleterious effects of intraoperative hypotension on outcome in patients with severe head injuries. J Trauma. 1992 Sep;33(3):403-7. PubMed PMID: 1404509.McKee MD, Schemitsch EH, Vincent LO, Sullivan I, Yoo D. The effect of a femoral fracture on concomitant closed head injury in patients with multiple injuries. J Trauma. 1997 Jun;42(6):1041-5. PubMed PMID: 9210538.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 11
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 3
Figure 3cFigure 3a Figure 3b
Figure 3a is the initial radiograph of a 19-year-old man who sustained a closed clavicle fracture. Figures 3b and 3c show postoperative radiographs. If the patient had been treated nonsurgically, which of the following would most likely occur?
1. Normal shoulder strength and function 2. Local sensory deficits 3. Fracture union 4. Infection 5. Malunion
PREFERRED RESPONSE: 5
DISCUSSION: Recent studies comparing surgical treatment with nonsurgical management in displaced clavicle fractures have revealed a decreased rate of malunion and nonunion with surgery. In addition, significant malunions can lead to functional deficits at the shoulder. Thus, with open reduction and internal fixation and anatomic or near-anatomic reduction, there should be a higher likelihood of normal shoulder strength and function. Infection and local sensory deficits would not be expected with nonsurgical management, whereas surgical treatment has a small risk of infection and a high likelihood of sensory deficits from iatrogenic damage to the supraclavicular nerves.
RECOMMENDED READING(S): Kim W, McKee MD. Management of acute clavicle fractures. Orthop Clin North Am. 2008 Oct;39(4):491-505, vii. Review. PubMed PMID: 18803979.Canadian Orthopaedic Trauma Society. Nonoperative treatment compared with plate fixation of displaced midshaft clavicular fractures. A multicenter, randomized clinical trial. J Bone Joint Surg Am. 2007 Jan;89(1):1-10. PubMed PMID: 17200303.McKee MD, Pedersen EM, Jones C, Stephen DJ, Kreder HJ, Schemitsch EH, Wild LM, Potter J. Deficits following nonoperative treatment of displaced midshaft clavicular fractures. J Bone Joint Surg Am. 2006 Jan;88(1):35-40. PubMed PMID: 16391247.

12 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 4What is the most common anatomic location of the lateral femoral cutaneous nerve?
1. Deep to the psoas muscle 2. Medial to the femoral vein 3. Under the inguinal ligament 4. Adjacent to the femoral nerve 5. Deep to the iliopectineal fascia
PREFERRED RESPONSE: 3
DISCUSSION: The lateral femoral cutaneous nerve most commonly originates from the lumbar plexus and runs on the surface of the iliacus muscle and enters the thigh by passing under the inguinal ligament before piercing the fascia lata. Its path can be variable.
RECOMMENDED READING(S): Hoppenfeld S, deBoer P, Buckley R, eds. Surgical Exposures in Orthopaedics: The Anatomic Approach. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:440-441.Anderson JE, ed. Grant’s Atlas of Anatomy. 8th ed. Baltimore/London: Williams and Wilkins; 1983:fig 4-7, 4-18, 4-20.Masquelet AC, McCullough CJ, Tubiana R: An Atlas of Surgical Exposures of the Lower Extremity. Philadelphia, PA: JB Lippincott; 1993:7,10.
2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 13
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
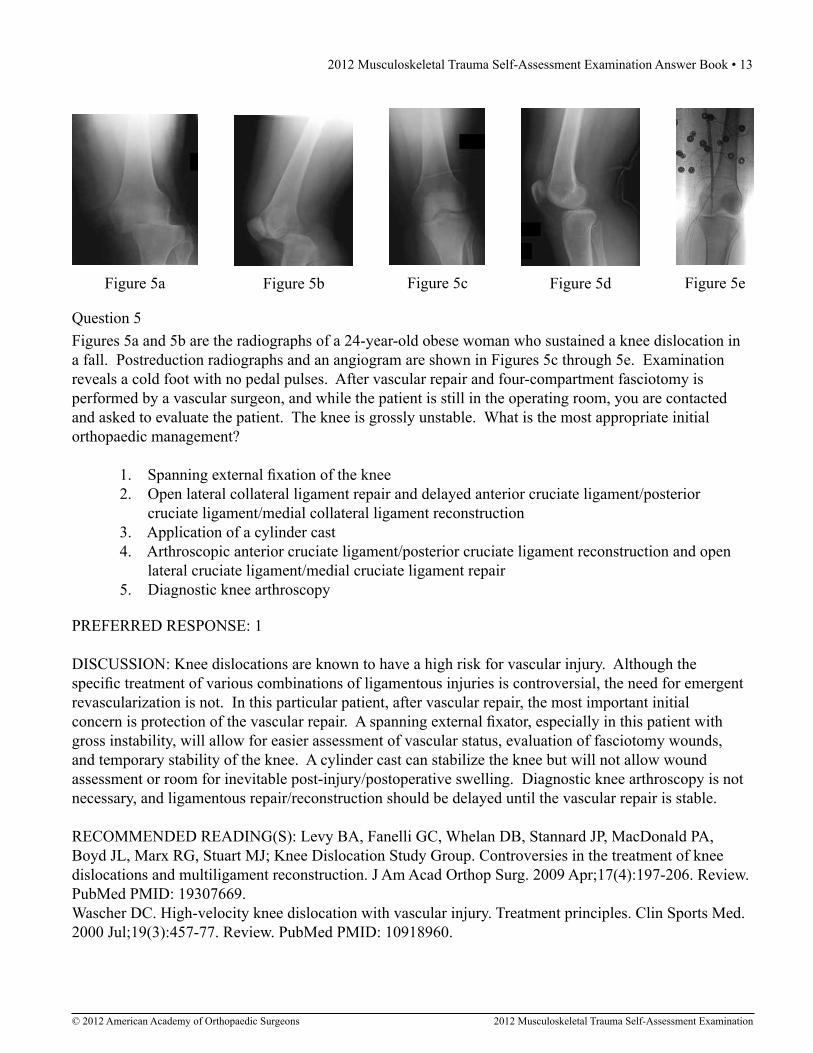
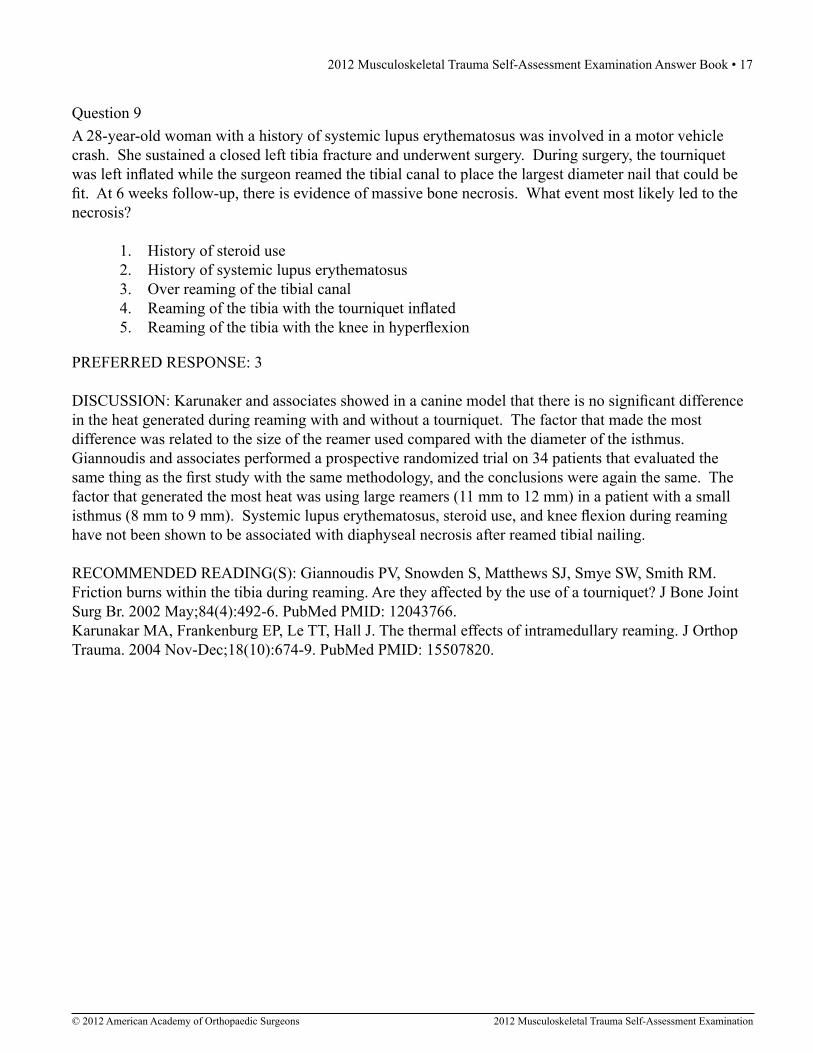
Figures 5a and 5b are the radiographs of a 24-year-old obese woman who sustained a knee dislocation in a fall. Postreduction radiographs and an angiogram are shown in Figures 5c through 5e. Examination reveals a cold foot with no pedal pulses. After vascular repair and four-compartment fasciotomy is performed by a vascular surgeon, and while the patient is still in the operating room, you are contacted and asked to evaluate the patient. The knee is grossly unstable. What is the most appropriate initial orthopaedic management?
1. Spanning external fixation of the knee 2. Open lateral collateral ligament repair and delayed anterior cruciate ligament/posterior cruciate ligament/medial collateral ligament reconstruction 3. Application of a cylinder cast 4. Arthroscopic anterior cruciate ligament/posterior cruciate ligament reconstruction and open lateral cruciate ligament/medial cruciate ligament repair 5. Diagnostic knee arthroscopy
Question 5
Figure 5dFigure 5c Figure 5eFigure 5a Figure 5b
PREFERRED RESPONSE: 1
DISCUSSION: Knee dislocations are known to have a high risk for vascular injury. Although the specific treatment of various combinations of ligamentous injuries is controversial, the need for emergent revascularization is not. In this particular patient, after vascular repair, the most important initial concern is protection of the vascular repair. A spanning external fixator, especially in this patient with gross instability, will allow for easier assessment of vascular status, evaluation of fasciotomy wounds, and temporary stability of the knee. A cylinder cast can stabilize the knee but will not allow wound assessment or room for inevitable post-injury/postoperative swelling. Diagnostic knee arthroscopy is not necessary, and ligamentous repair/reconstruction should be delayed until the vascular repair is stable.
RECOMMENDED READING(S): Levy BA, Fanelli GC, Whelan DB, Stannard JP, MacDonald PA, Boyd JL, Marx RG, Stuart MJ; Knee Dislocation Study Group. Controversies in the treatment of knee dislocations and multiligament reconstruction. J Am Acad Orthop Surg. 2009 Apr;17(4):197-206. Review. PubMed PMID: 19307669.Wascher DC. High-velocity knee dislocation with vascular injury. Treatment principles. Clin Sports Med. 2000 Jul;19(3):457-77. Review. PubMed PMID: 10918960.

14 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figure 6a Figure 6b
Question 6Figures 6a and 6b are the radiographs of a thin 23-year-old man who sustained a closed injury to his left arm in a fall. He has no other injuries and his neurologic examination is normal. What is the most appropriate treatment?
1. Intramedullary nailing 2. Hanging arm cast for 6 weeks 3. Shoulder immobilizer for 4 to 6 weeks 4. Open reduction and internal fixation 5. Coaptation splinting with conversion to a fracture brace
PREFERRED RESPONSE: 5
DISCUSSION: The patient is a thin man with an isolated left humerus fracture. The fracture has bony apposition and should be amenable to closed treatment; therefore the most appropriate treatment is coaptation splinting with conversion to a fracture brace. A hanging arm cast is not recommended for a transverse fracture because of the propensity to distract the fragments, especially if left in place for a long period of time. A shoulder immobilizer is not an appropriate treatment for a humeral shaft fracture. A transverse fracture line is sometimes considered a relative indication for surgical treatment if the fragments are distracted, but in this patient, immediate surgical fixation is not warranted in the absence of other indications for surgical treatment.
RECOMMENDED READING(S): Sarmiento A, Zagorski JB, Zych GA, Latta LL, Capps CA. Functional bracing for the treatment of fractures of the humeral diaphysis. J Bone Joint Surg Am. 2000 Apr;82(4):478-86. PubMed PMID: 10761938.Koch PP, Gross DF, Gerber C. The results of functional (Sarmiento) bracing of humeral shaft fractures. J Shoulder Elbow Surg. 2002 Mar-Apr;11(2):143-50. PubMed PMID: 11988725.Lin KC, Krishnan SG. Shoulder trauma: Bone. In: Fischgrund JS, ed. Orthopaedic Knowledge Update 9. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:287-299.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 15
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 7
Figure 7
Figure 7 is the pelvic radiograph of a 33-year-old man involved in a high-speed automobile crash. Examination reveals a blood pressure of 90/50 mm Hg and a pulse rate of 120/min. Radiographs of the chest and lateral cervical spine are normal. A CT scan of the abdomen does not reveal any intra-abdominal bleeding. What is the most appropriate management for the pelvic fracture?
1. Angiography 2. Application of a pelvic binder 3. Anterior external fixation 4. Anterior external fixation with pelvic packing 5. Open reduction and internal fixation of the pubic symphysis
PREFERRED RESPONSE: 2
DISCUSSION: Since the patient has not had any mechanical stabilization to the pelvic ring, the first step in management should be application of a sheet or binder along with resuscitation. Pelvic binders have been shown to be effective in decreasing transfusion needs and are quick and simple to apply. Emergent external fixation, pelvic packing, or angiography is not indicated unless the patient is unresponsive to these initial measures. The order in which these measures are used is controversial and somewhat institution dependent. Repair of the pubic symphysis is indicated as part of the definitive treatment but should not be done prior to resuscitation with pelvic binder placement.
RECOMMENDED READING(S): Krieg JC, Mohr M, Ellis TJ, Simpson TS, Madey SM, Bottlang M. Emergent stabilization of pelvic ring injuries by controlled circumferential compression: a clinical trial. J Trauma. 2005 Sep;59(3):659-64. PubMed PMID: 16361909.Croce MA, Magnotti LJ, Savage SA, Wood GW 2nd, Fabian TC. Emergent pelvic fixation in patients with exsanguinating pelvic fractures. J Am Coll Surg. 2007 May;204(5):935-9; discussion 940-2. PubMed PMID: 17481514.Routt ML Jr, Falicov A, Woodhouse E, Schildhauer TA. Circumferential pelvic antishock sheeting: a temporary resuscitation aid. J Orthop Trauma. 2002 Jan;16(1):45-8. PubMed PMID: 11782633.

16 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 8
Figure 8
What is the most common cause of death in a patient with the injury shown in Figure 8?
1. Visceral injury 2. Exsanguination 3. Closed head injury 4. Under-resuscitation 5. Disseminated intravascular coagulation
PREFERRED RESPONSE: 3
DISCUSSION: The most common identifiable cause of death in patients with lateral compression fractures is closed head injury. In contrast, the identifiable cause of death in patients with anteroposterior compression injuries is combined pelvic and visceral injury. Lateral compression injury results from a lateral impact to the pelvis that rotates the pelvis on the side of the impact toward the midline. The sacrotuberous and sacrospinous ligaments, as well as the internal iliac vessels, are shortened and are not subjected to tensile forces. Disruption of large named vessels (eg, internal iliac artery, superior gluteal artery) is relatively uncommon with lateral compression injuries.
RECOMMENDED READING(S): Burgess AR, Eastridge BJ, Young JW, Ellison TS, Ellison PS Jr, Poka A, Bathon GH, Brumback RJ. Pelvic ring disruptions: effective classification system and treatment protocols. J Trauma. 1990 Jul;30(7):848-56. PubMed PMID: 2381002.Weiner G, Styf J, Nakhostine M, Gershuni DH. Effect of ankle position and a plaster cast on intramuscular pressure in the human leg. J Bone Joint Surg Am. 1994 Oct;76(10):1476-81. PubMed PMID: 7929495.
2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 17
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 9A 28-year-old woman with a history of systemic lupus erythematosus was involved in a motor vehicle crash. She sustained a closed left tibia fracture and underwent surgery. During surgery, the tourniquet was left inflated while the surgeon reamed the tibial canal to place the largest diameter nail that could be fit. At 6 weeks follow-up, there is evidence of massive bone necrosis. What event most likely led to the necrosis?
1. History of steroid use 2. History of systemic lupus erythematosus 3. Over reaming of the tibial canal 4. Reaming of the tibia with the tourniquet inflated 5. Reaming of the tibia with the knee in hyperflexion
PREFERRED RESPONSE: 3
DISCUSSION: Karunaker and associates showed in a canine model that there is no significant difference in the heat generated during reaming with and without a tourniquet. The factor that made the most difference was related to the size of the reamer used compared with the diameter of the isthmus. Giannoudis and associates performed a prospective randomized trial on 34 patients that evaluated the same thing as the first study with the same methodology, and the conclusions were again the same. The factor that generated the most heat was using large reamers (11 mm to 12 mm) in a patient with a small isthmus (8 mm to 9 mm). Systemic lupus erythematosus, steroid use, and knee flexion during reaming have not been shown to be associated with diaphyseal necrosis after reamed tibial nailing.
RECOMMENDED READING(S): Giannoudis PV, Snowden S, Matthews SJ, Smye SW, Smith RM. Friction burns within the tibia during reaming. Are they affected by the use of a tourniquet? J Bone Joint Surg Br. 2002 May;84(4):492-6. PubMed PMID: 12043766.Karunakar MA, Frankenburg EP, Le TT, Hall J. The thermal effects of intramedullary reaming. J Orthop Trauma. 2004 Nov-Dec;18(10):674-9. PubMed PMID: 15507820.

18 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figures 10a and 10b are the radiographs of a 33-year-old man who was involved in a high-speed motorcycle crash. He sustained an isolated injury to the right lower extremity. On the day of injury, he was treated with open reduction and internal fixation of the femoral neck and retrograde nailing of the femur. Radiographs are shown in Figures 10c through 10f. Alternative treatment with a cephalomedullary device alone would be more likely to lead to which of the following outcomes?
1. More postoperative pain 2. More rapid healing of the femoral neck fracture 3. Higher union rate of the femoral neck fracture 4. Higher union rate of the femoral shaft fracture 5. Higher rate of malreduction of one of the fractures
Question 10
Figure 10d
Figure 10bFigure 10a Figure 10c
Figure 10e Figure 10f
PREFERRED RESPONSE: 5
DISCUSSION: The patient has ipsilateral fractures of the femoral neck and femoral shaft. This is not an uncommon scenario, often found in high-energy injuries in younger patients. There is some controversy as to the best method of fixation with some authors recommending separate implants for the two fractures, and some recommending a single antegrade cephalomedullary nail for treatment of both fractures. The use of a single implant does not increase healing time of the femoral neck fracture or limit postoperative pain. However, the use of a single implant is associated with higher malreduction rates of either the shaft or neck component which could lead to increased rates of nonunion or malunion.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 19
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
RECOMMENDED READING(S): Bedi A, Karunakar MA, Caron T, Sanders RW, Haidukewych GJ. Accuracy of reduction of ipsilateral femoral neck and shaft fractures--an analysis of various internal fixation strategies. J Orthop Trauma. 2009 Apr;23(4):249-53. PubMed PMID: 19318867.Smith RM, Giannoudis PV. Femoral shaft fractures. In: Browner BD, Jupiter JB, Levine AM, Trafton PG, Krettek C, eds. Skeletal Trauma: Basic Science, Management, and Reconstruction. Vol 2. 4th ed. Philadelphia, PA: WB Saunders; 2008:2073-2130.Peljovich AE, Patterson BM. Ipsilateral femoral neck and shaft fractures. J Am Acad Orthop Surg. 1998 Mar-Apr;6(2):106-13. PubMed PMID: 9682073.
Figures 11a and 11b show the radiographs of the open fracture of a 46-year-old man who injured his elbow on his nondominant arm in a motorcycle crash. On the day of injury, he underwent irrigation and débridement of the fracture. He was also treated with antibiotics. Which of the following definitive treatment methods will most likely lead to the best functional outcome?
1. Cast immobilization 2. Intramedullary screw fixation 3. Open reduction and plate fixation 4. Open reduction and internal fixation with tension band wiring 5. Fragment excision and triceps advancement
Question 11
Figure 11a Figure 11b
PREFERRED RESPONSE: 3
DISCUSSION: The patient has an open comminuted transolecranon fracture-dislocation. This occurs when the distal humerus is driven through the proximal ulna, and it is often associated with comminution of the olecranon and proximal ulna. The distal fragment translates anteriorly. Results of surgical treatment of transolecranon fracture-dislocations are best and most reliable when the fracture is reduced anatomically and plate fixation is used. Nonsurgical management is not indicated in this injury pattern. Excision of the comminuted fragments and advancement of the triceps will likely lead to persistent anterior instability of the elbow. Tension band wiring relies on cortical contact which will not be possible in this fracture. Intramedullary screw fixation is also not possible because of the significant comminution.

20 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
RECOMMENDED READING(S): Veillette CJ, Steinmann SP. Olecranon fractures. Orthop Clin North Am. 2008 Apr;39(2):229-36, vii. Review. PubMed PMID: 18374813.Mortazavi SM, Asadollahi S, Tahririan MA. Functional outcome following treatment of transolecranon fracture-dislocation of the elbow. Injury. 2006 Mar;37(3):284-8. Epub 2006 Jan 25. PubMed PMID: 16442109.Ring D, Jupiter JB, Sanders RW, Mast J, Simpson NS. Transolecranon fracture-dislocation of the elbow. J Orthop Trauma. 1997 Nov;11(8):545-50. PubMed PMID: 9415859.
Figures 12a through 12c show the radiographs of the closed fracture of a 24-year-old man who sustained an isolated injury to his left foot in a motorcycle crash. He was splinted and, on the following day, he underwent open reduction and internal fixation. Postoperative radiographs are shown in Figures 12d through 12f. What is the most likely complication of this injury?
1. Malunion 2. Nonunion 3. Osteomyelitis 4. Osteonecrosis 5. Posttraumatic arthritis
Question 12
Figure 12d Figure 12e Figure 12f
Figure 12a Figure 12b Figure 12c
PREFERRED RESPONSE: 5

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 21
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
DISCUSSION: The patient has a talar neck fracture that is associated with several well-known complications. Posttraumatic arthritis is the most common complication and osteonecrosis is slightly less common. These two complications are often out of the control of the orthopaedic surgeon and do not seem to be influenced by the timing of fixation. Malunion and nonunion are relatively uncommon when an anatomic reduction and stable fixation can be obtained. Open reduction can help ensure the best possible reduction, and plate fixation may be a more stable method of fixation, especially useful in preventing collapse through areas of comminution. Osteomyelitis is rare in closed fractures.
RECOMMENDED READING(S): Herscovici D Jr, Anglen JO, Archdeacon M, Cannada L, Scaduto JM. Avoiding complications in the treatment of pronation-external rotation ankle fractures, syndesmotic injuries, and talar neck fractures. J Bone Joint Surg Am. 2008 Apr;90(4):898-908. PubMed PMID: 18381329.Lindvall E, Haidukewych G, DiPasquale T, Herscovici D Jr, Sanders R. Open reduction and stable fixation of isolated, displaced talar neck and body fractures. J Bone Joint Surg Am. 2004 Oct;86-A(10):2229-34. PubMed PMID: 15466732.Vallier HA, Nork SE, Barei DP, Benirschke SK, Sangeorzan BJ. Talar neck fractures: results and outcomes. J Bone Joint Surg Am. 2004 Aug;86-A(8):1616-24. PubMed PMID: 15292407.Fleuriau Chateau PB, Brokaw DS, Jelen BA, Scheid DK, Weber TG. Plate fixation of talar neck fractures: preliminary review of a new technique in twenty-three patients. J Orthop Trauma. 2002 Apr;16(4):213-9. PubMed PMID: 11927801.
Question 13When comparing the results of open reduction and internal fixation (ORIF) versus antegrade intramedullary nailing (IMN) fixation of the humeral diaphysis in prospective randomized trials, which of the following statements is most accurate?
1. Union rates are higher with IMN. 2. Reoperation rates are higher with IMN. 3. Shoulder outcomes are similar for ORIF and IMN. 4. Infection rates are higher with ORIF. 5. Radial nerve complications are higher with ORIF.
PREFERRED RESPONSE: 2
DISCUSSION: There are relatively few comparative studies of the treatment of diaphyseal fractures of the humerus in the literature. In a meta-analysis of three prospective randomized trials comparing ORIF with IMN, open reduction and internal fixation showed a 90% risk reduction of shoulder impingement symptoms and a 75% risk reduction of reoperation. There is no difference in infection rate, nonunion rate, and radial nerve issues.
22 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
RECOMMENDED READING(S): Bhandari M, Devereaux PJ, McKee MD, Schemitsch EH. Compression plating versus intramedullary nailing of humeral shaft fractures--a meta-analysis. Acta Orthop. 2006 Apr;77(2):279-84. Review. PubMed PMID: 16752291.Green A, Reid JS, Carlson DA. Fractures of the humerus. In: Baumgaertner MR, Tornetta P III, eds. Orthopaedic Knowledge Update: Trauma 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2005:163-180.
Question 14Which inflammatory marker is most closely tied to a systemic inflammatory response following orthopaedic injury and treatment?
1. Interleukin 1 (IL-1) 2. Interleukin 6 (IL-6) 3. Interleukin 10 (IL-10) 4. Tumor necrosis factor, alpha 5. D-dimer
PREFERRED RESPONSE: 2
DISCUSSION: Significant basic science research has been done on identifying inflammatory markers associated with systemic inflammatory response following trauma and musculoskeletal injury. Although not yet clinically applicable, IL-6 has been identified as a marker that correlates well with musculoskeletal injury (ie, femur fracture) and treatment of these injuries (ie, intramedullary nailing). IL-1 and IL-10 do not correlate with treatment of musculoskeletal injury. Tumor necrosis factor, alpha and D-dimer, although often elevated following trauma, do not correlate with musculoskeletal treatment.
RECOMMENDED READING(S): Sears BW, Stover MD, Callaci J. Pathoanatomy and clinical correlates of the immunoinflammatory response following orthopaedic trauma. J Am Acad Orthop Surg. 2009 Apr;17(4):255-65. Review. PubMed PMID: 19307674.Pape HC, Griensven MV, Hildebrand FF, Tzioupis CT, Sommer KL, Krettek CC, Giannoudis PV; Epoff Study group. Systemic inflammatory response after extremity or truncal fracture operations. J Trauma. 2008 Dec;65(6):1379-84. PubMed PMID: 19077630.Pape HC, Schmidt RE, Rice J, van Griensven M, das Gupta R, Krettek C, Tscherne H. Biochemical changes after trauma and skeletal surgery of the lower extremity: quantification of the operative burden. Crit Care Med. 2000 Oct;28(10):3441-8. PubMed PMID: 11057799.
2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 23
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
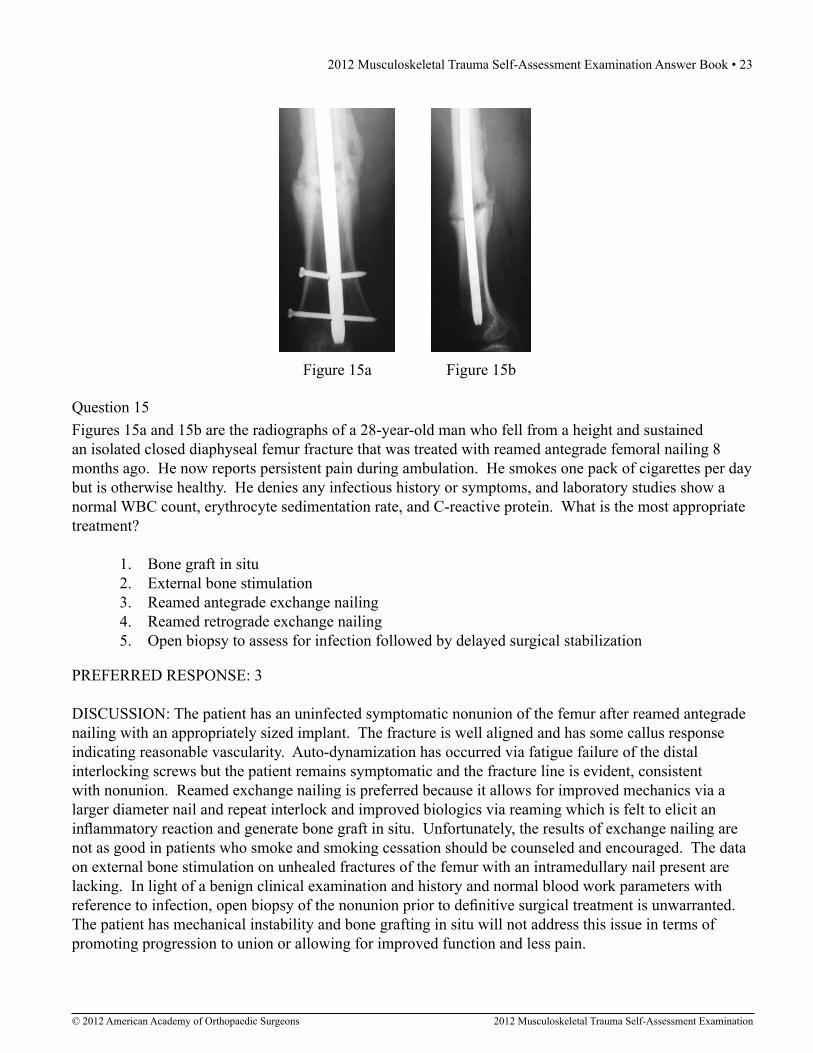
Question 15
Figure 15a Figure 15b
Figures 15a and 15b are the radiographs of a 28-year-old man who fell from a height and sustained an isolated closed diaphyseal femur fracture that was treated with reamed antegrade femoral nailing 8 months ago. He now reports persistent pain during ambulation. He smokes one pack of cigarettes per day but is otherwise healthy. He denies any infectious history or symptoms, and laboratory studies show a normal WBC count, erythrocyte sedimentation rate, and C-reactive protein. What is the most appropriate treatment?
1. Bone graft in situ 2. External bone stimulation 3. Reamed antegrade exchange nailing 4. Reamed retrograde exchange nailing 5. Open biopsy to assess for infection followed by delayed surgical stabilization
PREFERRED RESPONSE: 3
DISCUSSION: The patient has an uninfected symptomatic nonunion of the femur after reamed antegrade nailing with an appropriately sized implant. The fracture is well aligned and has some callus response indicating reasonable vascularity. Auto-dynamization has occurred via fatigue failure of the distal interlocking screws but the patient remains symptomatic and the fracture line is evident, consistent with nonunion. Reamed exchange nailing is preferred because it allows for improved mechanics via a larger diameter nail and repeat interlock and improved biologics via reaming which is felt to elicit an inflammatory reaction and generate bone graft in situ. Unfortunately, the results of exchange nailing are not as good in patients who smoke and smoking cessation should be counseled and encouraged. The data on external bone stimulation on unhealed fractures of the femur with an intramedullary nail present are lacking. In light of a benign clinical examination and history and normal blood work parameters with reference to infection, open biopsy of the nonunion prior to definitive surgical treatment is unwarranted. The patient has mechanical instability and bone grafting in situ will not address this issue in terms of promoting progression to union or allowing for improved function and less pain.

24 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
RECOMMENDED READING(S): Ostrum RF, Gruen GS, Zelle BA. Fractures of the femoral diaphysis. In: Baumgaertner MR, Tornetta P III, eds. Orthopaedic Knowledge Update: Trauma 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2005:387-395.Hak DJ, Lee SS, Goulet JA. Success of exchange reamed intramedullary nailing for femoral shaft nonunion or delayed union. J Orthop Trauma. 2000 Mar-Apr;14(3):178-82. PubMed PMID: 10791668.
Question 16
Figure 16b Figure 16a
Figures 16a and 16b show the initial radiograph and CT scan after the application of a pelvic binder in a 24-year-old woman who sustained a pelvic ring injury in a motor vehicle accident. What does the fracture of the sacrum best indicate?
1. Pelvic instability 2. Indication to repair the sacrum 3. Higher likelihood of bowel injury 4. Lower likelihood of neurologic injury 5. Lower likelihood of internal bleeding
PREFERRED RESPONSE: 1
DISCUSSION: The radiograph and CT scan reveal a fracture of the lateral sacrum due to avulsion of the sacrospinous and sacrotuberous ligaments. These ligaments are disrupted in an unstable anteroposterior compression-type pelvic ring injury. Higher grade injuries have a higher risk of vascular and/or neurologic injuries.
RECOMMENDED READING(S): Tile M. Acute Pelvic Fractures: I. Causation and Classification. J Am Acad Orthop Surg. 1996 May;4(3):143-151. PubMed PMID: 10795049.Tile M. Describing the injury: Classification of pelvic ring injuries. In: Tile M, Helfet D, Kellam J, eds. Fractures of the Pelvis and Acetabulum. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003:130-167.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 25
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 17When attempting to treat a proximal tibial metadiaphyseal fracture with an intramedullary nail, what is the most common angular malalignment?
1. Varus alone 2. Valgus alone 3. Varus and procurvatum 4. Valgus and procurvatum 5. Valgus and recurvatum
PREFERRED RESPONSE: 4
DISCUSSION: Fractures of the proximal metadiaphysis of the tibia can be treated successfully with intramedullary nails but historic rates of malalignment are up to 84%. The typical deformity is valgus and procurvatum due to the metaphyseal bony anatomy, eccentric start point, deforming force of the patellar tendon, and implant factors such as the Herzog curve of the nail. An ideal starting point is mandatory and should be at the medial border of the lateral tibial eminence on a true AP view and very proximal and anterior on a true lateral view with appropriate coronal and sagittal trajectory of the entry reamer. A reduction should be obtained and maintained during reaming, implant insertion, and interlocking. This can be facilitated via a variety of techniques including intraoperative external fixation, percutaneous reduction clamps or joysticks, semi-extended positioning, blocking screws, and ancillary plate fixation.
RECOMMENDED READING(S): Higgins T, Templeman D. Fractures of the tibial diaphysis. In: Baumgaertner MR, Tornetta P III, eds. Orthopaedic Knowledge Update: Trauma 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2005:431-439.Lang GJ, Cohen BE, Bosse MJ, Kellam JF. Proximal third tibial shaft fractures. Should they be nailed? Clin Orthop Relat Res. 1995 Jun;(315):64-74. PubMed PMID: 7634688.

26 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figures 18a through 18c show injuries sustained by a 22-year-old woman after falling 45 feet while mountain climbing. After being airlifted to the nearest trauma center, her arterial blood gas was 7.21, pO2 84, pCO2 48, and base arterial blood gas was 7.21, pO2 84, pCO2 48, and delta base -11 mmol/L. Her Hg is 8.7 and her resuscitation is ongoing. Based on this data, what would be the best management of her orthopaedic injuries?
1. External fixation of the pelvis, external fixation of the distal femur, and splinting of the humerus 2. External fixation of the pelvis, external fixation of the distal femur, and intramedullary nailing of the humerus 3. External fixation of the pelvis, open reduction and internal fixation of the distal femur, and splinting of the humerus 4. Open reduction and internal fixation of the pelvis, open reduction and internal fixation of the distal femur, and intramedullary nailing of the humerus 5. Open reduction and internal fixation of the pelvis, open reduction and internal fixation of the distal femur, and open reduction and internal fixation of the humerus
Question 18
Figure 18cFigure 18a Figure 18b
PREFERRED RESPONSE: 1
DISCUSSION: The patient is under-resuscitated and would benefit from minimally invasive stabilization of the pelvic ring and long bone fractures in a “damage-control” approach. External fixation of the pelvis and femur can be performed quickly and with minimal blood loss which should limit the “second hit” associated with more prolonged, invasive surgery. Upper extremity fractures are best managed acutely with splints in this clinical setting. Definitive fracture fixation should be delayed until the patient is adequately resuscitated.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 27
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
RECOMMENDED READING(S): Pape HC, Hildebrand F, Pertschy S, Zelle B, Garapati R, Grimme K, Krettek C, Reed RL 2nd. Changes in the management of femoral shaft fractures in polytrauma patients: from early total care to damage control orthopedic surgery. J Trauma. 2002 Sep;53(3):452-61; discussion 461-2. PubMed PMID: 12352480.Pape HC, Grimme K, Van Griensven M, Sott AH, Giannoudis P, Morley J, Roise O, Ellingsen E, Hildebrand F, Wiese B, Krettek C; EPOFF Study Group. Impact of intramedullary instrumentation versus damage control for femoral fractures on immunoinflammatory parameters: prospective randomized analysis by the EPOFF Study Group. J Trauma. 2003 Jul;55(1):7-13. PubMed PMID: 12855874.Pape HC, Rixen D, Morley J, Husebye EE, Mueller M, Dumont C, Gruner A, Oestern HJ, Bayeff-Filoff M, Garving C, Pardini D, van Griensven M, Krettek C, Giannoudis P; EPOFF Study Group. Impact of the method of initial stabilization for femoral shaft fractures in patients with multiple injuries at risk for complications (borderline patients). Ann Surg. 2007 Sep;246(3):491-9; discussion 499-501. PubMed PMID: 17717453.
Question 19
Figure 19b
Figures 19a and 19b are the radiographs of a 32-year-old woman who has sustained multiple injuries after being struck by a motor vehicle while riding a bicycle. She is intubated on arrival and remains tachycardic and hypotensive. Pulses are hard to palpate but the right hand is somewhat cooler to touch than the left hand. She has a large open wound over the upper arm. What is the most important predictor of outcome with these injuries?
1. Open wound size 2. Open wound contamination 3. Time to débridement 4. Adequacy of débridement 5. Neurovascular status
Figure 19a
PREFERRED RESPONSE: 5

28 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
DISCUSSION: The patient has lateral translation of the shoulder girdle on the chest radiograph as measured from the spinous process to the medial border of the scapula with resultant acromioclavicular widening consistent with the diagnosis of scapulothoracic dissociation. She also has an ipsilateral open fracture of the proximal humeral diaphysis. This represents an extremely high-energy injury to the upper extremity with a dismal prognosis. The overall mortality in the presence of scapulothoracic dissociation is 10%. Over 90% of patients will have neurologic injury which is often a complete and permanent brachial plexopathy, and a significant percentage will have associated limb-threatening vascular injuries. In the presence of a complete vascular and neurologic injury, amputation must be considered. While important, wound size and contamination, and time or adequacy of débridement will not likely drive the clinical outcomes in the presence of such a significant concomitant injury.
RECOMMENDED READING(S): Schmidt AH. Shoulder trauma. In: Baumgaertner MR, Tornetta P III, eds. Orthopaedic Knowledge Update: Trauma 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2005:151-161.Clements RH, Reisser JR. Scapulothoracic dissociation: a devastating injury. J Trauma. 1996 Jan;40(1):146-9. PubMed PMID: 8576982.
Figures 20a and 20b are the radiographs of a 19-year-old woman who was involved in a motor vehicle accident. What mechanism of injury is most consistent with the injury?
1. Vertical shear 2. External rotation 3. Sagittal translation 4. Lateral compression 5. Anterior posterior compression
Question 20
Figure 20bFigure 20a
PREFERRED RESPONSE: 4

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 29
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
DISCUSSION: The radiographs show a lateral compression pelvic ring injury with a displaced superior ramus fracture, or tilt fracture. Tilt fractures are most commonly caused by a lateral compression mechanism. These injuries are often seen in female patients and careful examination, including vaginal examination, is required to rule out open fractures. Lateral compression results in internal rotation, not external rotation, of the pelvic ring. Tilt fractures are not commonly seen with anterior-posterior compression injuries or vertical shear injuries. Sagittal translation is not a term used to describe pelvic ring injuries.
RECOMMENDED READING(S): Tile M. Acute pelvic fractures: I. causation and classification. J Am Acad Orthop Surg. 1996 May;4(3):143-151. PubMed PMID: 10795049.Lefaivre KA, Padalecki JR, Starr AJ. What constitutes a Young and Burgess lateral compression-I (OTA 61-B2) pelvic ring disruption? A description of computed tomography-based fracture anatomy and associated injuries. J Orthop Trauma. 2009 Jan;23(1):16-21. PubMed PMID: 19104299.Koo H, Leveridge M, Thompson C, Zdero R, Bhandari M, Kreder HJ, Stephen D, McKee MD, Schemitsch EH. Interobserver reliability of the young-burgess and tile classification systems for fractures of the pelvic ring. J Orthop Trauma. 2008 Jul;22(6):379-84. PubMed PMID: 18594301.
Question 21
Figure 21
Figure 21 is the radiograph of a 45-year-old woman who was severely injured in a motorcycle crash. Her injuries include a traumatic subarachnoid hemorrhage, bilateral pneumothoraces with pulmonary contusions and flail chest, fracture-dislocation of the left hip, and open fractures of the right distal femur and proximal tibia. Antibiotics and tetanus are administered in the emergency department. The patient is intubated and bilateral chest tubes are placed. A closed reduction is performed on the left hip. After appropriate resuscitation, what is the most appropriate initial management of the right knee injury?
1. Skeletal traction 2. Irrigation and débridement of the open fractures 3. Irrigation and débridement and spanning external fixation of the knee 4. Open reduction and internal fixation of the proximal tibia and distal femur 5. Percutaneous screw fixation of the articular fragments with retrograde femoral nailing and antegrade tibial nailing
PREFERRED RESPONSE: 3

30 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
DISCUSSION: Although the radiographic evaluation is incomplete, the single lateral view shows a comminuted fracture of the distal femur with suspicion of intra-articular injury and an ipsilateral proximal tibia fracture. This is an open fracture that requires antibiotics, débridement, and skeletal stabilization. The fractures are complicated and the patient is polytraumatized; therefore, rapid but complete surgical débridement and simple stabilization of the knee with a spanning external fixator would be the most appropriate management. Definitive surgical stabilization will likely be complicated and is less desirable during the early post-injury period.
RECOMMENDED READING(S): Parekh AA, Smith WR, Silva S, Agudelo JF, Williams AE, Hak D, Morgan SJ. Treatment of distal femur and proximal tibia fractures with external fixation followed by planned conversion to internal fixation. J Trauma. 2008 Mar;64(3):736-9. PubMed PMID: 18332816.Berkson EM, Virkus WW. High-energy tibial plateau fractures. J Am Acad Orthop Surg. 2006 Jan;14(1):20-31. Review. PubMed PMID: 16394164.Haidukewych GJ. Temporary external fixation for the management of complex intra- and periarticular fractures of the lower extremity. J Orthop Trauma. 2002 Oct;16(9):678-85. Review. PubMed PMID: 12368651.
Question 22
Figure 22
Which of the following strategies is helpful to avoid the complication seen in Figure 22?
1. Fibular plating 2. Blocking screws 3. Medial starting point 4. Nailing in the flexed position 5. Cross Kirschner wire fixation prior to nail insertion
PREFERRED RESPONSE: 2

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 31
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
DISCUSSION: This is the classic deformity encountered during intramedullary nailing of a proximal one third tibia fracture: apex anterior angulation and anterior translation of the proximal segment. Blocking screws, nailing in the semi-extended position and a lateral starting point all may help avoid the malalignment seen with proximal tibial metaphyseal fractures. Fibular plating may help with distal tibial metaphyseal fracture alignment. Cross Kirschner wire stabilization is not used in adult fracture patterns. A temporary unicortical plate, external fixator, or distractor may be used instead to hold provisional reduction while the nail is inserted.
RECOMMENDED READING(S): Ricci WM, O’Boyle M, Borrelli J, Bellabarba C, Sanders R. Fractures of the proximal third of the tibial shaft treated with intramedullary nails and blocking screws. J Orthop Trauma. 2001 May;15(4):264-70. PubMed PMID: 11371791.Krettek C, Miclau T, Schandelmaier P, Stephan C, Mohlmann U, Tscherne H. The mechanical effect of blocking screws (“Poller screws”) in stabilizing tibia fractures with short proximal or distal fragments after insertion of small-diameter intramedullary nails. J Orthop Trauma. 1999 Nov;13(8):550-3. PubMed PMID: 10714781.
Question 23
Figure 23
Figure 23 is the radiograph of a 22-year-old woman who was involved in a motor vehicle collision. She reports isolated pain in her left shoulder. She is hemodynamically stable, respiring comfortably, and neurovascularly intact. Based on these findings, which of the following statements regarding treatment is most appropriate?
1. Union rates are in excess of 95% if treated nonsurgically. 2. A figure-of-8 brace is superior to a sling for nonsurgical management. 3. Open reduction and internal fixation increases the likelihood of a nonunion. 4. Open reduction and internal fixation results in improved functional outcomes. 5. Open reduction and internal fixation and nonsurgical management have equivalent outcomes at 1 year.
PREFERRED RESPONSE: 4

32 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
DISCUSSION: The patient has sustained an isolated, closed, transverse fracture of the middle third of the clavicle with greater than 100% displacement and greater than 2 cm of shortening. Whereas the traditional treatment of clavicle fractures has been overwhelmingly conservative, recent reports suggest that surgical fixation should be considered for certain injury patterns. The union rates of displaced clavicle fractures are more recently noted to be approximately 85%, which is lower than the traditional literature. In a prospective randomized trial of clavicle fractures with greater than 100% displacement, union rates were higher and functional outcomes were better at all time points up to 1 year after injury in the surgical group when compared with nonsurgical management.
RECOMMENDED READING(S): Zlowodzki M, Zelle BA, Cole PA, Jeray K, McKee MD; Evidence-Based Orthopaedic Trauma Working Group. Treatment of acute midshaft clavicle fractures: systematic review of 2144 fractures: on behalf of the Evidence-Based Orthopaedic Trauma Working Group. J Orthop Trauma. 2005 Aug;19(7):504-7. Review. PubMed PMID: 16056089.Canadian Orthopaedic Trauma Society. Nonoperative treatment compared with plate fixation of displaced midshaft clavicular fractures. A multicenter, randomized clinical trial. J Bone Joint Surg Am. 2007 Jan;89(1):1-10. PubMed PMID: 17200303.
A 19-year-old man underwent intramedullary nailing of a closed tibia fracture 1 year ago and has never been pain free. While playing football, he was tackled and sustained the injury shown in Figure 24a. What is the best treatment option based on the radiographs seen in Figures 24b and 24c?
1. Circular fixator 2. Exchange nailing 3. Iliac crest bone graft 4. Straightening of the leg and casting 5. Removal of the nail and functional bracing
Figure 24a Figure 24b Figure 24c
Question 24
PREFERRED RESPONSE: 2

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 33
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
DISCUSSION: This is a young, healthy man with a tibial nonunion and a failed implant. He requires treatment for the nonunion. In the absence of bone loss and/or infection, the injury is best treated with removal of the bent nail and a reamed exchange nailing. Casting alone or functional bracing is not the best option in a patient with an atrophic nonunion. Use of circular fixators is an option; however, in a young, healthy patient with a fracture that has bony contact, the first line of treatment is exchange nailing.
RECOMMENDED READING(S): Brinker MR, O’Connor DP. Nonunions: Evaluation and treatment. In: Browner BD, Jupiter JB, Levine AM, Trafton PG, Krettek C, eds. Skeletal Trauma: Basic Science, Management, and Reconstruction. Vol 1. 4th ed. Philadelphia, PA: WB Saunders; 2008:615-707.Brinker MR, O’Connor DP. Exchange nailing of ununited fractures. J Bone Joint Surg Am. 2007 Jan;89(1):177-88. Review. PubMed PMID: 17200326.
Question 25
Figure 25c
Figures 25a through 25c show the radiographs, including a stress radiograph, of a 58-year-old woman who twisted her ankle on a step. She has no history of diabetes or vascular disease. Examination reveals a closed injury with moderate swelling about the ankle. Her neurologic examination is normal. She has a strong dorsalis pedis pulse and tenderness over the lateral malleolus and the medial side of her ankle. What is the most appropriate management?
1. MRI scan of the ankle 2. Non-weight-bearing cast for 6 weeks 3. Removable walking boot and progressive weight bearing 4. Open reduction and internal fixation of the fibula 5. Open reduction and internal fixation of the fibula with medial ligament repair
Figure 25a Figure 25b
PREFERRED RESPONSE: 3

34 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
DISCUSSION: The patient has a lateral malleolus fracture with an ankle mortise that is stable to a stress examination; therefore, surgical treatment is not indicated. In a stable lateral malleolus fracture, strict non-weight-bearing is not necessary, and a removable walking boot or walking cast can be used along with progressive weight bearing. The presence of tenderness or swelling medially at the ankle has been shown to be a poor indicator of medial-sided injury. The clinical utility of MRI scans in ankle fractures is controversial. Studies have used MRI scans to evaluate the competence of the deltoid ligament and have shown that the ligament may remain intact even with an increased medial clear space on a stress examination. In the patient, the stress examination does not show talar subluxation so the deltoid ligament is not incompetent.
RECOMMENDED READING(S): McConnell T, Creevy W, Tornetta P 3rd. Stress examination of supination external rotation-type fibular fractures. J Bone Joint Surg Am. 2004 Oct;86-A(10):2171-8. PubMed PMID: 15466725.Egol KA, Amirtharajah M, Tejwani NC, Capla EL, Koval KJ. Ankle stress test for predicting the need for surgical fixation of isolated fibular fractures. J Bone Joint Surg Am. 2004 Nov;86-A(11):2393-8. Erratum in: J Bone Joint Surg Am. 2005 Jan;87-A(1):161. Amirtharage, Mohana [corrected to Amirtharajah, Mohana]. J Bone Joint Surg Am. 2005 Apr;87(4):857. PubMed PMID: 15523008.Koval KJ, Egol KA, Cheung Y, Goodwin DW, Spratt KF. Does a positive ankle stress test indicate the need for operative treatment after lateral malleolus fracture? A preliminary report. J Orthop Trauma. 2007 Aug;21(7):449-55. PubMed PMID: 17762475.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 35
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 26
Figure 26
Figure 26 is the radiograph of a 33-year-old woman who was involved in a high-speed motor vehicle crash. Her initial blood pressure is 80/50 mm Hg and she has a pulse rate of 120 bpm. After hemodynamic stabilization and temporizing measures have been performed, the patient is cleared for surgery. What is the most appropriate method of definitive fixation?
1. External fixation 2. Open reduction and internal fixation of the pubic symphysis with a two-hole plate 3. Open reduction and internal fixation of the pubic symphysis with a two-hole plate and posterior triangular osteosynthesis 4. Open reduction and internal fixation of the pubic symphysis with a multi-hole plate 5. Open reduction and internal fixation of the pubic symphysis with a multi-hole plate and posterior plate osteosynthesis
PREFERRED RESPONSE: 4
DISCUSSION: The patient has sustained an anterior posterior compression (APC) grade II pelvic ring injury. Initial management should consist of pelvic volume reduction with pelvic binding or sheeting. Once the patient is hemodynamically stable, the decision for definitive management should be made. In a retrospective review of more than 200 patients, Sagi and Papp investigated plate osteosynthesis of the pubic symphysis. They found significantly fewer malunions in the multi-hole plate group and a trend toward fewer surgeries in the same group. Typically external fixation should be reserved for temporary fixation and not a definitive management in stable patients. Posterior fixation is reserved for injuries with disruption of the posterior ligamentous constraints, typically APC grade III injuries. Triangular osteosynthesis is a strategy for fixation of unstable vertical shear fractures that require fixation of the pelvis to the lumbar spine.
RECOMMENDED READING(S): Sagi HC, Papp S. Comparative radiographic and clinical outcome of two-hole and multi-hole symphyseal plating. J Orthop Trauma. 2008 Jul;22(6):373-8. PubMed PMID: 18594300.Stover MD, Mayo KA, Kellam JF. Pelvic ring disruptions. In: Browner BD, Jupiter JB, Levine AM, Trafton PG, Krettek C, eds. Skeletal Trauma: Basic Science, Management, and Reconstruction. Vol 1. 4th ed. Philadelphia, PA: WB Saunders; 2008:1107-1170.

36 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 27
Figure 27
Figure 27 is the radiograph of a 75-year-old woman with a 1-year history of left arm pain following a fall. What is the most appropriate management?
1. Thermal imaging 2. Metabolic/endocrine work-up 3. MRI of the arm 4. PET scan 5. Infection work-up
PREFERRED RESPONSE: 2
DISCUSSION: The patient should be evaluated for any correctable metabolic or endocrine abnormality that may exist prior to any surgical intervention. Infection in the absence of previous surgery is very unlikely. There are no radiographic findings suggestive of a malignancy; therefore, MRI and PET scans are not indicated. Thermal imaging is not in use in orthopaedics.
RECOMMENDED READING(S): Brinker MR, O’Connor DP, Monla YT, Earthman TP. Metabolic and endocrine abnormalities in patients with nonunions. J Orthop Trauma. 2007 Sep;21(8):557-70. PubMed PMID: 17805023.Kuo I, Ong C, Simmons L, Bliuc D, Eisman J, Center J. Successful direct intervention for osteoporosis in patients with minimal trauma fractures. Osteoporos Int. 2007 Dec;18(12):1633-9. Epub 2007 Jun 30. PubMed PMID: 17603741.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 37
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Of the following variables, which has the strongest influence on external fixator stiffness?
1. Pin diameter 2. Pin spread 3. Bone quality 4. Stacking a second fixator bar 5. Distance from bone to fixator bar
Question 28
PREFERRED RESPONSE: 1
DISCUSSION: Whereas all of the factors will have an impact on frame rigidity and stability, the single biggest factor is the pin diameter because it has an exponential effect.
RECOMMENDED READING(S): Ruedi TR, Buckley RE, Moran CG, eds. AO Principles of Fracture Management. 2nd ed. New York, NY: Thieme; 2007.Hipp JA, Hayes WC. Biomechanics of fractures. In: Browner BD, Jupiter JB, Levine AM, Trafton P, Krettek C, eds. Skeletal Trauma: Basic Science, Management, and Reconstruction. 3rd ed. Philadelphia, PA: Saunders Elsevier; 2003:51-82.
Question 29
Figure 29
Figure 29 is the radiograph of a 30-year-old man who sustained an isolated tibial shaft fracture. What is the most common deformity with nonsurgical management?
1. Varus 2. Malrotation 3. Valgus 5. Valgus and recurvatum 4. Valgus and procurvatum
PREFERRED RESPONSE: 1
38 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
DISCUSSION: Studies have shown that approximately 25% of diaphyseal fractures of the tibia with intact fibulae will go onto varus malunion if treated nonsurgically. Limb-length discrepancies are also common. Here the fibula acts as a strut, preventing valgus collapse but predisposing to varus collapse. Valgus and procurvatum is the typical deformity in proximal tibial fractures.
RECOMMENDED READING(S): Teitz CC, Carter DR, Frankel VH. Problems associated with tibial fractures with intact fibulae. J Bone Joint Surg Am. 1980 Jul;62(5):770-6. PubMed PMID: 7391100.Gicquel P, Giacomelli MC, Basic B, Karger C, Clavert JM. Problems of operative and non-operative treatment and healing in tibial fractures. Injury. 2005 Feb;36 Suppl 1:A44-50. PubMed PMID: 15652936.
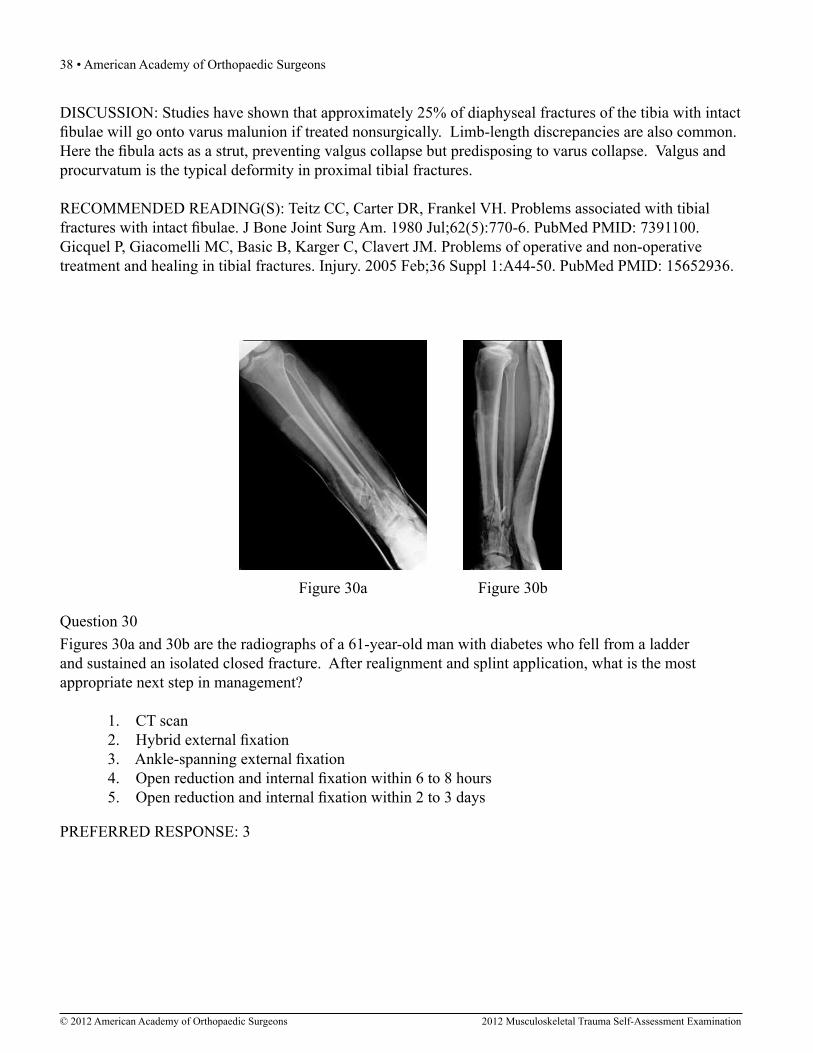
Figures 30a and 30b are the radiographs of a 61-year-old man with diabetes who fell from a ladder and sustained an isolated closed fracture. After realignment and splint application, what is the most appropriate next step in management?
1. CT scan 2. Hybrid external fixation 3. Ankle-spanning external fixation 4. Open reduction and internal fixation within 6 to 8 hours 5. Open reduction and internal fixation within 2 to 3 days
Question 30
Figure 30a Figure 30b
PREFERRED RESPONSE: 3

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 39
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
DISCUSSION: The patient has sustained a high-energy severely comminuted AO/OTA C2 fracture of the distal tibia. This injury is notably fraught with soft-tissue complications that can lead to disastrous clinical results. In general, a staged protocol is now preferred in an effort to avoid these complications and has shown substantial decreases in infection rates and wound healing problems. A CT scan is certainly appropriate for preoperative planning but should be obtained after frame application because the indirect reduction that is achieved improves one’s ability to understand the fracture characteristics and morphology. Hybrid external fixation has fallen out of favor because of its limited biomechanic rigidity and clinical results. Open reduction and internal fixation in the acute phase (6 to 8 hours) or sub-acute phase (2 to 3 days) is difficult.
RECOMMENDED READING(S): Patterson MJ, Cole JD. Two-staged delayed open reduction and internal fixation of severe pilon fractures. J Orthop Trauma. 1999 Feb;13(2):85-91. PubMed PMID: 10052781.Sirkin M, Sanders R, DiPasquale T, Herscovici D Jr. A staged protocol for soft tissue management in the treatment of complex pilon fractures. J Orthop Trauma. 1999 Feb;13(2):78-84. PubMed PMID: 10052780.
Question 31A starting point entry portal that is too lateral on a trochanteric femoral nail will result in what deforming force?
1. Varus 2. Valgus 3. Flexion 4. Extension 5. Excessive hoop stress
PREFERRED RESPONSE: 1
DISCUSSION: The trochanteric entry portal for femoral nail insertion is increasingly being used by orthopaedic surgeons both for cephalomedullary implants and standard femoral nailing. In contradistinction to the piriformis fossa, the tip of the trochanter is not co-linear to the diaphyseal isthmus and an errant start can lead to the introduction of malalignment and/or iatrogenic comminution at the fracture site. The desired starting point should be at the tip or slightly medial to the tip of the greater trochanter to avoid varus malalignment and blow out of the lateral wall.
RECOMMENDED READING(S): Ruedi TR, Buckley RE, Moran CG, eds. AO Principles of Fracture Management. 2nd ed. New York, NY: Thieme; 2007.Ostrum RF, Marcantonio A, Marburger R. A critical analysis of the eccentric starting point for trochanteric intramedullary femoral nailing. J Orthop Trauma. 2005 Nov-Dec;19(10):681-6. PubMed PMID: 16314714.
40 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 32A 26-year-old man is involved in a high-speed motorcycle accident. He sustains a grade IIIB open tibia fracture. Examination reveals a large soft-tissue defect and an insensate foot. What is the expected outcome in this scenario?
1. Equal functional outcome when limb salvage is compared with amputation 2. Worse functional outcome with limb salvage than with primary amputation 3. Better functional outcome when amputation is compared with limb salvage 4. Amputation within 6 months of injury 5. Permanent loss of plantar sensation
PREFERRED RESPONSE: 1
DISCUSSION: The Lower Extremity Assessment Project data have shown that absent plantar sensation is not an indication for primary amputation. When looking at a comparison between an insensate salvage group and a sensate salvage group at 2 years follow-up, both groups had an equal proportion (55%) of normal plantar sensation and functionally both groups were equivalent. Absent plantar sensation at initial evaluation is not prognostic for long-term plantar sensory status or functional outcome.
RECOMMENDED READING(S): Bosse MJ, McCarthy ML, Jones AL, Webb LX, Sims SH, Sanders RW, MacKenzie EJ; Lower Extremity Assessment Project (LEAP) Study Group. The insensate foot following severe lower extremity trauma: an indication for amputation? J Bone Joint Surg Am. 2005 Dec;87(12):2601-8. PubMed PMID: 16322607.MacKenzie EJ, Bosse MJ. Factors influencing outcome following limb-threatening lower limb trauma: lessons learned from the Lower Extremity Assessment Project (LEAP). J Am Acad Orthop Surg. 2006;14(10 Spec No.):S205-10. Review. PubMed PMID: 17003200.
Question 33Which of the following clinical scenarios represents the strongest indication for locked plating technique in a 70-year-old woman?
1. Segmentally comminuted ulnar fracture 2. Simple diaphyseal fracture of the humerus 3. Transverse midshaft displaced clavicle fracture 4. Periprosthetic femur fracture distal to a well-fixed total hip arthroplasty 5. Schatzker 2 fracture of the tibia with severe joint depression and comminution
PREFERRED RESPONSE: 4

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 41
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
DISCUSSION: Locking screw fixation is a relatively new option in the armamentarium of orthopaedic surgeons treating fractures. The understanding of the biomechanics, implications to healing, and optimal indications and surgical techniques is still in evolution. A periprosthetic proximal femur fracture with a stable prosthesis is best treated with open reduction and internal fixation with locking proximal fixation with or without cerclage cables. Diaphyseal fractures treated with compression plating or bridge plating can be treated well with conventional implants unless osteoporosis is severe. An AO/OTA B-type partial articular fracture is also better suited to standard buttress plating with periarticular rafting lag screws. Locking fixation is not always required for a transverse displaced midshaft clavicle fracture.
RECOMMENDED READING(S): Anglen J, Kyle RF, Marsh JL, Virkus WW, Watters WC 3rd, Keith MW, Turkelson CM, Wies JL, Boyer KM. Locking plates for extremity fractures. J Am Acad Orthop Surg. 2009 Jul;17(7):465-72. Review. PubMed PMID: 19571302.Cantu RV, Koval KJ. The use of locking plates in fracture care. J Am Acad Orthop Surg. 2006 Mar;14(3):183-90. PubMed PMID: 16520369.
A 65-year-old woman with rheumatoid arthritis is involved in a motor vehicle accident. Her injuries include a right displaced femoral neck fracture, a left open tibial pilon fracture, a left open tibial plateau fracture, multiple rib fractures, and bilateral pulmonary contusions. Her vitals signs on admission are a heart rate of 115 bpm and a systolic blood pressure of 90 mm Hg. Laboratory studies show a hemoglobin of 10.0 g/dL and a delta base of -6.0 mmol/L. What finding in this patient is most significantly associated with increased mortality?
1. Heart rate 2. Base deficit 3. Hemoglobin 4. Urine output 5. Systolic blood pressure
Question 34
PREFERRED RESPONSE: 2
DISCUSSION: The severity of injuries and the lack of physiologic reserve in this and other elderly patients often result in mortality. Base deficit has shown to be a reliable predictor of mortality even in normotensive elderly blunt trauma patients. Although tachycardia, low systolic blood pressure, and low hemoglobin may all contribute to these patients’ mortality, base deficit may be used as a predictor of mortality and a measure of resuscitation.

42 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
RECOMMENDED READING(S): Callaway DW, Shapiro NI, Donnino MW, Baker C, Rosen CL. Serum lactate and base deficit as predictors of mortality in normotensive elderly blunt trauma patients. J Trauma. 2009 Apr;66(4):1040-4. PubMed PMID: 19359912.Paladino L, Sinert R, Wallace D, Anderson T, Yadav K, Zehtabchi S. The utility of base deficit and arterial lactate in differentiating major from minor injury in trauma patients with normal vital signs. Resuscitation. 2008 Jun;77(3):363-8. Epub 2008 Mar 25. PubMed PMID: 18367305.Martin M, Murray J, Berne T, Demetriades D, Belzberg H. Diagnosis of acid-base derangements and mortality prediction in the trauma intensive care unit: the physiochemical approach. J Trauma. 2005 Feb;58(2):238-43. Erratum in: J Trauma. 2005 Oct;59(4):1035. PubMed PMID: 15706182.
Question 35A fracture of what portion of the coronoid is most often associated with a terrible triad injury?
1. Tip 2. Rim 3. Base 4. Anterolateral facet 5. Anteromedial facet
PREFERRED RESPONSE: 1
DISCUSSION: The most common pattern of cornoid fracture with a terrible triad injury is a transverse fracture of 2 mm to 3 mm of the tip. The mechanism of injury of a terrible triad injury is typically valgus and supination. These forces force the radial head against and then under the capitellum, resulting in a fracture of the radial head. The coronoid is then driven under the trochlea and sheared off as the valgus force continues. The lateral collateral ligament typically tears next.
RECOMMENDED READING(S): Steinmann SP. Coronoid process fracture. J Am Acad Orthop Surg. 2008 Sep;16(9):519-29. Review. PubMed PMID: 18768709.Doornberg JN, Ring D. Coronoid fracture patterns. J Hand Surg Am. 2006 Jan;31(1):45-52. PubMed PMID: 16443103.Doornberg JN, Ring DC. Fracture of the anteromedial facet of the coronoid process. J Bone Joint Surg Am. 2006 Oct;88(10):2216-24. PubMed PMID: 17015599.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 43
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
A 45-year-old man sustained the injury shown in Figures 36a and 36b. The involved side is his dominant side. What is the most appropriate management?
1. Closed reduction 2. Arthroscopic labral repair 3. MRI to evaluate the rotator cuff 4. Stress radiographs to evaluate instability 5. Early motion in a structured physical therapy program
Question 36
Figure 36a Figure 36b
PREFERRED RESPONSE: 5
DISCUSSION: This minimally displaced (one-part) proximal humerus fracture is best treated with nonsurgical management. Early motion and physical therapy should be instituted to optimize functional results. No reduction is required. There is no indication for an acute MRI scan. If symptoms exist after healing, one may be obtained. Labral injuries are not typically associated with this type of injury. Instability is not associated with a one-part fracture and stress radiographs are not described.
RECOMMENDED READING(S): Tejwani NC, Liporace F, Walsh M, France MA, Zuckerman JD, Egol KA. Functional outcome following one-part proximal humeral fractures: a prospective study. J Shoulder Elbow Surg. 2008 Mar-Apr;17(2):216-9. Epub 2008 Jan 22. PubMed PMID: 18207430.Hanson B, Neidenbach P, de Boer P, Stengel D. Functional outcomes after nonoperative management of fractures of the proximal humerus. J Shoulder Elbow Surg. 2009 Jul-Aug;18(4):612-21. PubMed PMID: 19559373.

44 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 37Which set of patient characteristics has the highest risk of developing osteonecrosis after an intracapsular femoral neck fracture?
1. 45-year-old woman with a displaced fracture 2. 55-year-old man with a nondisplaced fracture 3. 70-year-old woman with a nondisplaced fracture 4. 70-year-old man with a displaced fracture 5. 85-year-old woman with a displaced fracture
PREFERRED RESPONSE: 1
DISCUSSION: Loizou and associates prospectively studied 1,023 patients who sustained an intracapsular hip fracture that was treated with internal fixation using contemporary methods. The overall incidence of osteonecrosis was 6.6%. Osteonecrosis was less common for undisplaced (4.0%) than for displaced fractures (9.5%) and in men (4.9%) than women (11.4%) who had a displaced fracture. The incidence of osteonecrosis for those patients younger than 60 years and who sustained a displaced fracture was 20.6%, compared with 12.5% for those aged 60 to 80 years and 2.5% for those older than age 80 years. Barnes and associates reported that late segmental collapse was more common in displaced fractures in women younger than age 75 years than in those older than age 75 years.
RECOMMENDED READING(S): Loizou CL, Parker MJ. Avascular necrosis after internal fixation of intracapsular hip fractures; a study of the outcome for 1023 patients. Injury. 2009 Nov;40(11):1143-6. Epub 2009 Apr 1. PubMed PMID: 19342046.Barnes R, Brown JT, Garden RS, Nicoll EA. Subcapital fractures of the femur. A prospective review. J Bone Joint Surg Br. 1976 Feb;58(1):2-24. PubMed PMID: 1270491.
When compared with reamed intramedullary nailing for an unstable diaphyseal tibia fracture, unreamed nailing is associated with which of the following?
1. Longer surgical times 2. Higher infection rates 3. Lower functional outcome scores 4. Similar union rates in open fractures 5. Higher incidence of pulmonary complications
Question 38
PREFERRED RESPONSE: 4

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 45
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
DISCUSSION: The Investigators Randomized Trial of Reamed versus Non-Reamed Intramedullary Nailing of Tibial Shaft Fractures (SPRINT) study, a large, randomized, controlled trial, has shown a benefit of reamed intramedullary (IM) nailing versus unreamed IM nailing for closed tibial shaft fractures with regard to reoperation rates. No such association exists for open tibial fractures; ie, union rates are the same for open fractures. The infection rates are the same, as is functional outcome, and surgical time is potentially shorter for unreamed nails. The potential pulmonary benefits from unreamed nailing have never been clinically proven.
RECOMMENDED READING(S): Study to Prospectively Evaluate Reamed Intramedullary Nails in Patients with Tibial Fractures Investigators, Bhandari M, Guyatt G, Tornetta P 3rd, Schemitsch EH, Swiontkowski M, Sanders D, Walter SD. Randomized trial of reamed and unreamed intramedullary nailing of tibial shaft fractures. J Bone Joint Surg Am. 2008 Dec;90(12):2567-78. PubMed PMID: 19047701.Finkemeier CG, Schmidt AH, Kyle RF, Templeman DC, Varecka TF. A prospective, randomized study of intramedullary nails inserted with and without reaming for the treatment of open and closed fractures of the tibial shaft. J Orthop Trauma. 2000 Mar-Apr;14(3):187-93. PubMed PMID: 10791670.

46 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figures 39a and 39b are the radiographs of a 45-year-old man with diabetes who fell 12 feet from a ladder and sustained an isolated closed injury to his left leg. Examination revealed that he was neurovascularly intact and compartments were soft. A damage control knee spanning external fixator was applied and after 2 weeks in the frame, his blisters have resolved and his skin now wrinkles. What is the most appropriate treatment?
1. Conversion to a periarticular ”hybrid” frame 2. Open reduction and internal fixation with a lateral nonlocking plate 3. Open reduction and internal fixation with a lateral locking plate 4. Open reduction and internal fixation with medial and lateral plates 5. Open reduction and internal fixation with posteromedial and lateral plates
Question 39
Figure 39a Figure 39b
PREFERRED RESPONSE: 5
DISCUSSION: The patient has sustained a severely comminuted bicondylar fracture of the tibial plateau. The mechanism and radiographs highlight the high-energy mechanism of the injury and should warrant aggressive monitoring for compartment syndrome which is relatively common in this scenario. A staged surgical approach is warranted with application of a spanning damage control external fixator to maintain length and alignment while the soft-tissue injury recovers and to allow for surveillance and examination of the limb. The radiographs reveal a comminuted bicondylar pattern with significant depression of the lateral articular surface and a split fracture with condylar widening. This element of the fracture will require direct elevation of the joint surface and reduction/buttress of the lateral condyle. This is best achieved with a lateral plate with subchondral rafting screws. The medial articular surface is coronally split and the posteromedial fragment is displaced. This fragment requires direct reduction and buttress via a separate posteromedial approach which is frequently performed prior to the lateral approach and fixation. A lateral buttress plate or a lateral locking plate alone does not reliably capture or adequately support the displaced posteromedial fragment. A medial and lateral plate construct is less soft-tissue friendly, particularly if inserted through a single incision. A medial plate would also fail to give direct buttress to the posteromedial fragment.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 47
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
RECOMMENDED READING(S): Marsh JL, Templeman D. Fractures of the tibial plateau. In: Baumgaertner MR, Tornetta P III, eds. Orthopaedic Knowledge Update: Trauma 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2005:419-429.Higgins TF, Kemper D, Klatt J. Incidence and morphology of the posteromedial fragment in bicondylar tibial plateau fractures. J Orthop Trauma. 2009 Jan;23(1):45-51. PubMed PMID: 19104303.
Question 40A patient with an unstable pelvic ring injury has just undergone an emergent laparotomy and currently has a packed abdomen. Stabilization of the pelvic ring is performed with an anterior external fixator. What is an advantage of using an external fixator with pins in the iliac crest rather than pins in the anterior inferior iliac spine?
1. Greater pelvic ring stability 2. Lower risk of pin tract infection 3. Less reliance on fluoroscopy for pin placement 4. Better ability to control a posterior pelvic injury 5. Less likely to interfere with future incisions for definitive pelvic internal fixation
PREFERRED RESPONSE: 3
DISCUSSION: There are relative advantages to both types of these external fixators. A frame based on the iliac crest is oftentimes easier to place rapidly because it is less dependent on fluoroscopy. This is also advantageous in this clinical scenario because the patient may not be on a radiolucent table. A frame with pins in the anterior inferior iliac spines may be advantageous in that the pin sites will be away from any future needed incisions if an ilioinguinal approach is needed. There is, however, a higher risk of lateral femoral cutaneous nerve injury or intra-articular pin placement at the hip joint with this frame configuration. This technique is generally more dependent on fluoroscopy for pin placement. Some biomechanic studies have shown advantages to AIIS-based frames but this does not give a definite clinical advantage because neither frame alone is adequate to definitively treat an unstable associated posterior pelvic ring injury. There is no known difference in pin site infection rates between these frame types.
RECOMMENDED READING(S): Rommens P, Hessmann M. External fixation for the injured pelvic ring. In: Tile M, Helfet D, Kellam J, eds. Fractures of the Pelvis and Acetabulum. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003:203-216.Haidukewych GJ, Kumar S, Prpa B. Placement of half-pins for supra-acetabular external fixation: an anatomic study. Clin Orthop Relat Res. 2003 Jun;(411):269-73. PubMed PMID: 12782884.
48 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 41What finding would most likely be present on an AP radiograph of a nondislocated elbow with an anteromedial coronoid fracture?
1. A “fleck” sign 2. The AP radiograph would appear normal 3. Equal joint spaces between the medial trochlea and the coronoid 4. Progressive narrowing of the joint space from lateral to medial between the medial trochlea and the coronoid 5. Progressive narrowing of the joint space from medial to lateral between the medial trochlea and the coronoid
PREFERRED RESPONSE: 4
DISCUSSION: Because of the fracture of the anteromedial portion of the coronoid, the medial side of the elbow is unsupported to varus stresses. As a result, the joint line will narrow from lateral to medial secondary to medial collapse of the joint. There is no “fleck” sign for this injury.
RECOMMENDED READING(S): Steinmann SP. Coronoid process fracture. J Am Acad Orthop Surg. 2008 Sep;16(9):519-29. Review. PubMed PMID: 18768709.Steinmann SP. Coronoid process fracture. J Am Acad Orthop Surg. 2008 Sep;16(9):519-29. Review. PubMed PMID: 18768709.Doornberg JN, Ring D. Coronoid fracture patterns. J Hand Surg Am. 2006 Jan;31(1):45-52. PubMed PMID: 16443103.Doornberg JN, Ring DC. Fracture of the anteromedial facet of the coronoid process. J Bone Joint Surg Am. 2006 Oct;88(10):2216-24. PubMed PMID: 17015599.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 49
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 42
Figure 42a Figure 42b
Figures 42a and 42b are the AP pelvis and normal chest radiographs of a 40-year-old man who was a restrained driver in a high-speed motor vehicle crash. He reports right hip pain in the emergency department. He was awake and alert, normotensive, and tachycardic. Hemoglobin was 14 gm/dL. Thoracolumbar radiographs are normal. A closed reduction of the right hip was performed and the patient was monitored in the emergency department. One hour later, he was transported to the intensive care unit and, en route, he started to report chest pain and new onset of lower extremity weakness. He was noted to be tachycardic and hypotensive. Which of the following studies should be obtained?
1. CT scan of the head 2. CT scan of the pelvis 3. CT scan of the lumbar spine 4. CT angiography of the chest 5. Angiography of the right lower extremity
PREFERRED RESPONSE: 4
DISCUSSION: Posterior hip dislocation associated with a deceleration injury is associated with traumatic rupture of the thoracic aorta. Usually the chest radiograph reveals some abnormality such as mediastinal widening but this sign may be absent. This patient’s mental status is normal so an intracranial process is not a likely cause of the change in status. The patient is not reporting back pain. Posterior dislocation is not commonly associated with intrapelvic bleeding or lower extremity vascular injury. A high index of suspicion is necessary; however, in light of the patient’s chest pain and hypotension as well as lower extremity weakness (likely from spinal cord ischemia); therefore, the most appropriate study is CT angiography of the chest followed by prompt cardiothoracic surgical intervention.
RECOMMENDED READING(S): Routt ML Jr. Surgical treatment of acetabular fractures. In: Browner BD, Jupiter JB, Levine AM, Trafton PG, Krettek C, eds. Skeletal Trauma: Basic Science, Management, and Reconstruction. Vol 1. 4th ed. Philadelphia, PA: WB Saunders; 2008:2073-2130.Marymont JV, Cotler HB, Harris JH Jr, Miller-Crotchett P, Browner BD. Posterior hip dislocation associated with acute traumatic injury of the thoracic aorta: a previously unrecognized injury complex. J Orthop Trauma. 1990;4(4):383-7. PubMed PMID: 2266442.

50 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figure 43 is the radiograph of a 22-year-old right-hand dominant man who sustained the injury shown 1 year ago. He now reports persistent pain with activity. Which of the following interventions would most reliably relieve the patient’s symptoms?
1. Functional bracing 2. Compression plating 3. Iliac crest bone grafting 4. Reamed intramedullary nailing 5. Internal electrical bone stimulation
Question 43
Figure 43
PREFERRED RESPONSE: 2
DISCUSSION: This is a hypertrophic nonunion of the forearm. Vascularity to the fracture site has been preserved; however, there is too much mechanical instability leading to failure of healing. Compression plating alone is all that is necessary to achieve fracture site stability and union. Iliac crest bone grafting is needed in atrophic-type nonunions. Internal electrical bone stimulation is used as an adjunct occasionally, but again is usually reserved for atrophic nonunion types. This patient has failed to respond to nonsurgical management, and functional bracing will not provide enough mechanical stability to the nonunion site to promote union. A plate and screw device provides greater mechanical stability than a reamed intramedullary nail. Furthermore, use of a reamed intramedullary nail has never been described for the treatment of a nonunion of the forearm.
RECOMMENDED READING(S): Brinker MR, O’Connor DP. Nonunions: Evaluation and treatment. In: Browner BD, Jupiter JB, Levine AM, Trafton PG, Krettek C, eds. Skeletal Trauma: Basic Science, Management, and Reconstruction. Vol 1. 4th ed. Philadelphia, PA: WB Saunders; 2008:615-707.Nadkarni B, Srivastav S, Mittal V, Agarwal S. Use of locking compression plates for long bone nonunions without removing existing intramedullary nail: review of literature and our experience. J Trauma. 2008 Aug;65(2):482-6. PubMed PMID: 18695487.
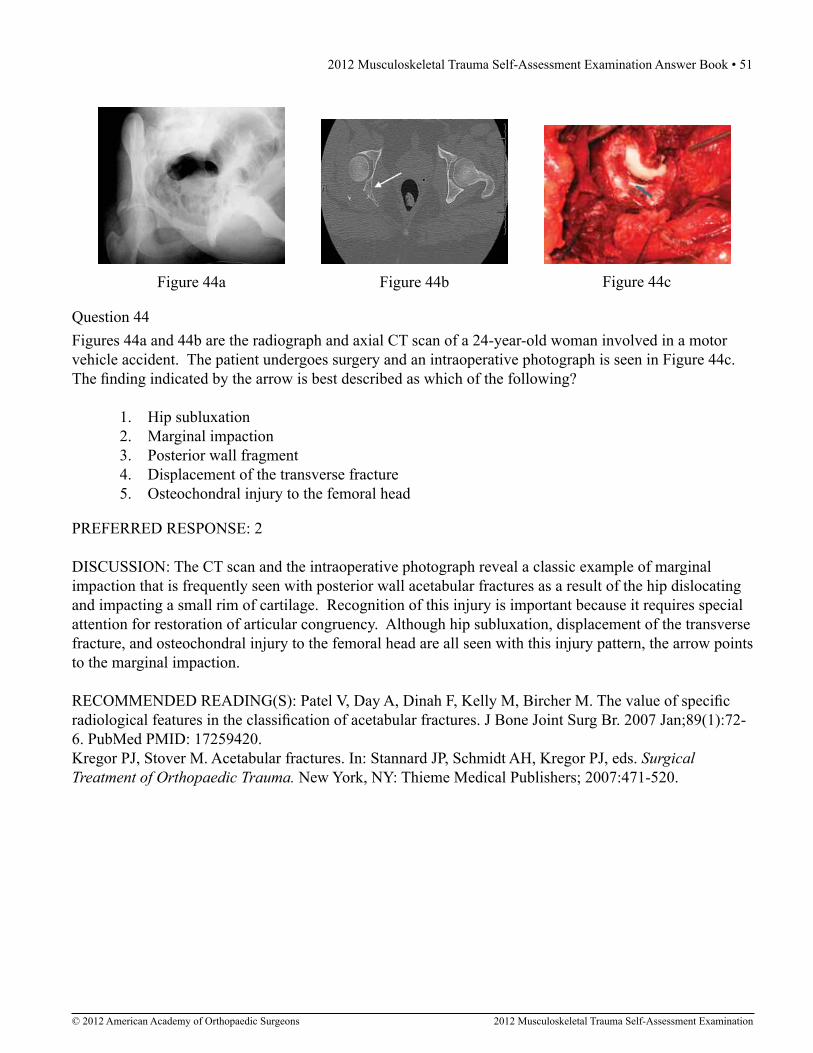
2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 51
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 44
Figure 44c
Figures 44a and 44b are the radiograph and axial CT scan of a 24-year-old woman involved in a motor vehicle accident. The patient undergoes surgery and an intraoperative photograph is seen in Figure 44c. The finding indicated by the arrow is best described as which of the following?
1. Hip subluxation 2. Marginal impaction 3. Posterior wall fragment 4. Displacement of the transverse fracture 5. Osteochondral injury to the femoral head
Figure 44a Figure 44b
PREFERRED RESPONSE: 2
DISCUSSION: The CT scan and the intraoperative photograph reveal a classic example of marginal impaction that is frequently seen with posterior wall acetabular fractures as a result of the hip dislocating and impacting a small rim of cartilage. Recognition of this injury is important because it requires special attention for restoration of articular congruency. Although hip subluxation, displacement of the transverse fracture, and osteochondral injury to the femoral head are all seen with this injury pattern, the arrow points to the marginal impaction.
RECOMMENDED READING(S): Patel V, Day A, Dinah F, Kelly M, Bircher M. The value of specific radiological features in the classification of acetabular fractures. J Bone Joint Surg Br. 2007 Jan;89(1):72-6. PubMed PMID: 17259420.Kregor PJ, Stover M. Acetabular fractures. In: Stannard JP, Schmidt AH, Kregor PJ, eds. Surgical Treatment of Orthopaedic Trauma. New York, NY: Thieme Medical Publishers; 2007:471-520.

52 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 45Which of the following is associated with increased fetal morbidity and mortality in acetabular fractures during pregnancy?
1. Fetal position 2. Surgical approach 3. Mechanism of injury 4. Fracture classification 5. Trimester of pregnancy
PREFERRED RESPONSE: 3
DISCUSSION: Fixation of pelvic and acetabular fractures in pregnancy is not contraindicated. However, both maternal and fetal morbidity and mortality is increased in this patient subset. Factors shown to be associated with increased fetal mortality include: injury severity, mechanism of injury, and maternal hemorrhage. Surgical approach, fracture classification, fetal position, and the trimester of pregnancy have not been shown to affect fetal morbidity or mortality.
RECOMMENDED READING(S): Leggon RE, Wood GC, Indeck MC. Pelvic fractures in pregnancy: factors influencing maternal and fetal outcomes. J Trauma. 2002 Oct;53(4):796-804. Review. PubMed PMID: 12394889.Flik K, Kloen P, Toro JB, Urmey W, Nijhuis JG, Helfet DL. Orthopaedic trauma in the pregnant patient. J Am Acad Orthop Surg. 2006 Mar;14(3):175-82. PubMed PMID: 16520368.Desai P, Suk M. Orthopedic trauma in pregnancy. Am J Orthop (Belle Mead NJ). 2007 Nov;36(11):E160-6. Review. PubMed PMID: 18075614.
Which of the following is the major blood supply to the heel pad?
1. Lateral calcaneal artery 2. Lateral malleolar artery 3. Artery of the sinus tarsi 4. Artery of the tarsal canal 5. Medial calcaneal branch of the posterior tibial artery
Question 46
PREFERRED RESPONSE: 5
DISCUSSION: The medial calcaneal branch of the posterior tibial artery is the major vascular supply to the heel pad. Heel pad avulsions are severe injuries associated with high-energy trauma and often carry a poor prognosis because of the potential for heel pad necrosis. The lateral calcaneal artery and the lateral malleolar artery, along with the lateral tarsal artery, provide perfusion to the lateral flap associated with a standard extensile approach to the calcaneus. The artery of the tarsal canal is a branch of the posterior tibial artery, and the artery of the sinus tarsi is a branch of the perforating peroneal artery. Both provide perfusion to the talus.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 53
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
RECOMMENDED READING(S): Banerjee R, Nickisch F, Easley ME, DiGiovanni CW. Foot injuries. In: Browner BD, Jupiter JB, Levine AM, Trafton PG, Krettek C, eds. Skeletal Trauma: Basic Science, Management, and Reconstruction. Vol 2. 4th ed. Philadelphia, PA: WB Saunders; 2008:2585-2748.Libermanis O. Replantation of the heel pad. Plast Reconstr Surg. 1993 Sep;92(3):537-9. PubMed PMID: 8341757.
Question 47
Figure 47a Figure 47b
Figures 47a and 47b are the radiograph and CT scan of a 45-year-old man who was involved in a high-speed motor vehicle accident. What is the most appropriate treatment?
1. Subtalar arthrodesis 2. Percutaneous screw fixation 3. Closed reduction and cast application 4. Open reduction and internal fixation 5. Non-weight-bearing and early range of motion
PREFERRED RESPONSE: 4
DISCUSSION: The radiograph and CT scan show a displaced talar neck fracture that is best treated with anatomic reduction and stable internal fixation. Neither non-weight-bearing and early range of motion nor closed reduction and cast application address the unstable fracture or restore articular congruity. The fracture is displaced with an interposed fragment in the fracture line and therefore requires open reduction prior to screw placement. Subtalar arthrodesis should be reserved for talar fractures with severe injury to the subtalar joint.
RECOMMENDED READING(S): Sanders DW, Busam M, Hattwick E, Edwards JR, McAndrew MP, Johnson KD. Functional outcomes following displaced talar neck fractures. J Orthop Trauma. 2004 May-Jun;18(5):265-70. PubMed PMID: 15105747.Vallier HA, Nork SE, Benirschke SK, Sangeorzan BJ. Surgical treatment of talar body fractures. J Bone Joint Surg Am. 2004 Sep;86-A Suppl 1(Pt 2):180-92. PubMed PMID: 15466758.

54 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figure 48a Figure 48cFigure 48b
Question 48Figures 48a and 48b are the initial radiograph and clinical photograph of a 21-year-old woman who sustained a severe mangling injury to her left foot in a rollover ATV crash. After multiple débridements, she underwent definitive transmetatarsal amputation with split-thickness skin graft. She did have intact plantar sensation. Figure 48c shows the clinical photograph 10 days after amputation. Her wounds healed without infection and she did not require further surgery. At 2 years after injury, which of these factors is most likely to be associated with improved level of satisfaction?
1. Female gender 2. Use of skin graft 3. Ability to return to work 4. Retained plantar sensation 5. Initial treatment by amputation
PREFERRED RESPONSE: 3
DISCUSSION: The LEAP study is a multicenter prospective study evaluating multiple aspects of reconstruction versus amputation in the treatment of mangled extremity injuries. With regard to patient satisfaction, treatment variables such as decision for reconstruction versus amputation, or initial presence or absence of plantar sensation have little impact. In addition, demographic factors such as age, gender, socioeconomic status, and education level do not predict patient satisfaction. Instead, the most important predictors of patient satisfaction at 2 years after injury include the ability to return to work, absence of depression, faster walking speed, and decreased pain.
RECOMMENDED READING(S): O’Toole RV, Castillo RC, Pollak AN, MacKenzie EJ, Bosse MJ; LEAP Study Group. Determinants of patient satisfaction after severe lower-extremity injuries. J Bone Joint Surg Am. 2008 Jun;90(6):1206-11. PubMed PMID: 18519312.Bosse MJ, MacKenzie EJ, Kellam JF, Burgess AR, Webb LX, Swiontkowski MF, Sanders RW, Jones AL, McAndrew MP, Patterson BM, McCarthy ML, Travison TG, Castillo RC. An analysis of outcomes of reconstruction or amputation after leg-threatening injuries. N Engl J Med. 2002 Dec 12;347(24):1924-31. PubMed PMID: 12477942.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 55
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 49
Figure 49
Which of the following is expected as a sequela with the use of a knee-spanning external fixator as a temporary method of stabilization for the injury shown in Figure 49?
1. Diminished distal pulses 2. An increased rate of pulmonary injury 3. Inability to access soft-tissue envelope 4. Transient compartmental pressure changes 5. Longer time to soft-tissue resolution for definitive surgery
PREFERRED RESPONSE: 4
DISCUSSION: The use of bridging external fixation about the knee for severe tibial plateau fractures is associated with all of the following: swelling reduction, improved blood flow, access to the soft-tissue envelope, with only transient increases in intracompartmental pressure during application. It has no effect on pulmonary injuries.
RECOMMENDED READING(S): Egol KA, Bazzi J, McLaurin TM, Tejwani NC. The effect of knee-spanning external fixation on compartment pressures in the leg. J Orthop Trauma. 2008 Nov-Dec;22(10):680-5. PubMed PMID: 18978542.Egol KA, Tejwani NC, Capla EL, Wolinsky PL, Koval KJ. Staged management of high-energy proximal tibia fractures (OTA types 41): the results of a prospective, standardized protocol. J Orthop Trauma. 2005 Aug;19(7):448-55; discussion 456. PubMed PMID: 16056075.

56 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 50
Figure 50c
Figure 50a is the radiograph of a 25-year-old man who fell off his bike, landed on his outstretched elbow, and sustained a closed fracture-dislocation of the elbow. After urgent closed reduction, he has no neurovascular compromise. Postreduction radiographs are shown in Figures 50b and 50c. What is the most appropriate management?
1. Transarticular screw fixation 2. Hinged external fixation and medial collateral ligament repair 3. Radial head excision, coronoid open reduction and internal fixation, and lateral collateral ligament repair 4. Open reduction and internal fixation of the coronoid, radial head arthroplasty, and lateral ulnar collateral ligament repair 5. Open reduction and internal fixation of the radial head, repair of the lateral collateral ligament, and excision of the coronoid fragment
Figure 50a Figure 50b
PREFERRED RESPONSE: 4
DISCUSSION: The radiographs reveal a terrible triad injury of the elbow. This is a constellation of injuries involving an elbow dislocation, radial head fracture, and coronoid fracture and it is notorious for persistent instability and redislocation if treatment is inadequate. After initial closed reduction, surgical management is indicated to prevent or limit long-term complications. This involves repair or replacement of the injured radial head, reduction and fixation of the coronoid/anterior capsule complex, and lateral ligamentous repair. If there is persistent instability, then additional medial ligamentous repair should be undertaken. Nonsurgical management with bracing or cast immobilization is inadequate for this injury. Isolated treatment of either the coronoid or radial head, without addressing the other injury components is inadequate. Hinged external fixation is associated with a high complication rate and is generally reserved for salvage cases. The radial head should not be excised in an unstable elbow injury. Transarticular screw fixation is reserved for salvage situations.
RECOMMENDED READING(S): Mathew PK, Athwal GS, King GJ. Terrible triad injury of the elbow: current concepts. J Am Acad Orthop Surg. 2009 Mar;17(3):137-51. Review. PubMed PMID: 19264707.Pugh DM, Wild LM, Schemitsch EH, King GJ, McKee MD. Standard surgical protocol to treat elbow dislocations with radial head and coronoid fractures. J Bone Joint Surg Am. 2004 Jun;86-A(6):1122-30. PubMed PMID: 15173283.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 57
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figure 51b Figure 51c
Question 51A 31-year-old man sustained an unstable closed left posterior hip dislocation in a motorcycle accident. A postreduction radiograph is shown in Figure 51a. 3-D CT scans are shown in Figures 51b and 51c. What is the optimal surgical approach that will allow for the most appropriate treatment?
1. Surgical dislocation 2. Watson-Jones approach 3. Smith-Peterson approach 4. Kocher-Langenbach approach 5. Extensile iliofemoral approach
Figure 51a
PREFERRED RESPONSE: 1
DISCUSSION: The radiograph and CT scans show a posterior wall acetabular fracture with an associated femoral head fracture. As is the case in most of these injuries, the femoral head fracture is located on the anterior aspect of the femoral head. Surgical dislocation with a trochanteric flip osteotomy as described by Solberg and associates and Henle and associates allows for exposure and treatment of the posterior wall fracture as well as surgical dislocation for treatment of the femoral head fracture. A Smith-Peterson approach or Watson-Jones approach would allow for anterior exposure and may help to address the femoral head fracture, but not the posterior wall fracture. A Kocher-Langenbach approach would allow exposure of the posterior wall fracture, but not the femoral head fracture. An extensile iliofemoral approach is unnecessary for this injury pattern.
RECOMMENDED READING(S): Solberg BD, Moon CN, Franco DP. Use of a trochanteric flip osteotomy improves outcomes in Pipkin IV fractures. Clin Orthop Relat Res. 2009 Apr;467(4):929-33. Epub 2008 Sep 18. PubMed PMID: 18800211.Giannoudis PV, Kontakis G, Christoforakis Z, Akula M, Tosounidis T, Koutras C. Management, complications and clinical results of femoral head fractures. Injury. 2009 Dec;40(12):1245-51. Epub 2009 Nov 7. PubMed PMID: 19897188.Henle P, Kloen P, Siebenrock KA. Femoral head injuries: Which treatment strategy can be recommended? Injury. 2007 Apr;38(4):478-88. Epub 2007 Apr 2. PubMed PMID: 17400227.

58 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 52What is the most common complication following surgery for a “terrible triad” elbow fracture-dislocation?
1. Arthritis 2. Infection 3. Re-dislocation 4. Restricted range of elbow motion 5. Posterior interosseous nerve (PIN) palsy
PREFERRED RESPONSE: 4
DISCUSSION: Recurrent instability, PIN palsy, infection, and posttraumatic arthritis have all been reported following these injuries; however, elbow contracture or loss of motion is nearly universal following these injuries.
RECOMMENDED READING(S): Egol KA, Immerman I, Paksima N, Tejwani N, Koval KJ. Fracture-dislocation of the elbow functional outcome following treatment with a standardized protocol. Bull NYU Hosp Jt Dis. 2007;65(4):263-70. PubMed PMID: 18081545.McKee MD, Wilson TL, Winston L, Schemitsch EH, Richards RR. Functional outcome following surgical treatment of intra-articular distal humeral fractures through a posterior approach. J Bone Joint Surg Am. 2000 Dec;82-A(12):1701-7. PubMed PMID: 11130643.
Figure 53 is the radiograph obtained at the time of transfer to the trauma center of a 41-year-old man who was involved in a motor vehicle accident. What is the most appropriate initial management?
1. MRI scan 2. CT scan of the pelvis 3. Application of skeletal traction 4. Closed reduction of the right hip 5. Open reduction and internal fixation
Figure 53
Question 53
PREFERRED RESPONSE: 4

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 59
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
DISCUSSION: The radiograph reveals a displaced transverse posterior wall acetabular fracture, and the hip is dislocated. On recognition of a hip dislocation, the hip should be promptly reduced. A time to reduction of greater than 12 hours has been associated with adverse outcomes. Although skeletal traction and a CT scan are essential elements in this patient’s care, the hip should be reduced prior to these actions. An MRI scan is not indicated in this patient, particularly with the hip dislocated. The ultimate surgical treatment for this injury will be open reduction and internal fixation, but the patient should be stabilized, the hip reduced, and appropriate imaging obtained before taking the patient to surgery.
RECOMMENDED READING(S): Moed BR, Willson Carr SE, Watson JT. Results of operative treatment of fractures of the posterior wall of the acetabulum. J Bone Joint Surg Am. 2002 May;84-A(5):752-8. PubMed PMID: 12004016.Reilly MC, Olson SA. Treatment considerations for surgical and nonsurgical management of acetabular fractures. In: Olson SA, Reilly MC, eds. Acetabular and Pelvic Fractures. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2007:43-65.
Figure 54a Figure 54b
Question 54Figures 54a and 54b are the radiographs of a 23-year-old man who fell from a height and sustained an isolated injury to his right leg. Which of the following is a useful surgical technique to optimize alignment during intramedullary nailing?
1. Move the starting point slightly medial 2. Move the starting point slightly lateral 3. Hyperflexion of the knee 4. Anterior blocking screw 5. Medial blocking screw
PREFERRED RESPONSE: 2
60 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
DISCUSSION: Fractures of the proximal metadiaphysis of the tibia can be treated successfully with intramedullary nails, but previous studies showed rates of malalignment of up to 84%. The typical deformity is valgus and procurvatum. An ideal starting point is mandatory and should be slightly lateral to the medial border of the lateral tibial eminence on a true AP view and very proximal and anterior on a true lateral view with appropriate coronal and sagittal trajectory of the entry reamer. A medial start point will exacerbate valgus deformity and should be avoided. A reduction should be obtained and maintained during reaming, implant insertion, and interlocking. This can be facilitated via a variety of techniques including intraoperative external fixation, percutaneous reduction clamps or joysticks, semi-extended positioning, blocking screws that are typically inserted posterior and lateral to the nail, and ancillary plate fixation. With careful attention to these techniques, more recent studies report low rates of malalignment.
RECOMMENDED READING(S): Higgins T, Templeman D. Fractures of the tibial diaphysis. In: Baumgaertner MR, Tornetta P III, eds. Orthopaedic Knowledge Update: Trauma 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2005:431-439.Nork SE, Barei DP, Schildhauer TA, Agel J, Holt SK, Schrick JL, Sangeorzan BJ. Intramedullary nailing of proximal quarter tibial fractures. J Orthop Trauma. 2006 Sep;20(8):523-8. PubMed PMID: 16990722.
Question 55A 27-year-old man who was involved in a high-speed motor vehicle crash arrives at the trauma center with loss of consciousness, multiple posterior rib fractures, a left scapula body fracture, a left humerus fracture, bilateral femoral shaft fractures, and an open right ankle fracture-dislocation. Initial vital signs are a blood pressure of 88/50 mm Hg, a pulse of 120 bpm, and respirations of 22/min. His injury severity score is 28 and lactate levels are 2.7. CT scans of the head and abdomen are negative for hemorrhage, and after initial resuscitation the patient is cleared for surgery. Initial orthopaedic management should consist of débridement and irrigation of the right ankle with
1. external fixation, intramedullary nailing of bilateral femurs, and intramedullary nailing of the left humerus. 2. external fixation, external fixation of bilateral femurs, and splinting of the left humerus. 3. external fixation, external fixation of bilateral femurs, and open reduction and internal fixation of the left humerus. 4. open reduction and internal fixation, intramedullary nailing of bilateral femurs, and open reduction and internal fixation of the left humerus. 5. open reduction and internal fixation, external fixation of bilateral femurs, and intramedullary nailing of the left humerus.
PREFERRED RESPONSE: 2

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 61
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
DISCUSSION: The transition from early total care (ETC) to damage control orthopaedics has developed over the past 20 years in orthopaedic polytrauma situations. A vast number of studies over the past several years have investigated the timing and technique of orthopaedic intervention in the care of these patients and effects on outcomes. The goal is to avoid an iatrogenic second hit that can push a patient into adult respiratory distress syndrome (ARDS) or multiple organ failure (MOF). In a patient who is unstable, the algorithm shifts to damage control orthopaedics (DCO). In this patient, the minimum intervention to achieve orthopaedic stability is indicated; therefore, débridement and irrigation of open fractures, external fixation of lower extremity long bones, and splinting of upper extremity fractures is appropriate. There are several parameters that can help classify a patient’s condition and therefore guide the surgeon’s initial management (see Figure 55). Grade I is stable and the patient can be cleared for surgery for early total care. Grade II is borderline and these patients are found along a continuum. In general, the priority of each injury should be determined and the most important fixed first. The surgeon should continually check the patient’s status and proceed as long as the patient is stable. Once the patient shows signs of deteriorating status, DCO should be implemented for the remaining injuries. Grade III is unstable and DCO should be the initial course of action. Grade IV is in extremis with life-threatening injuries and DCO should be implemented if possible. In this scenario, answer choices 1 and 2 involve an ETC philosophy and would be inappropriate for this patient who is unstable with significant chest trauma. In answer choice 3, the humerus is not a higher priority than the femur fractures and should be one of the last fractures addressed surgically. Open reduction and internal fixation of the ankle fracture would not be indicated in an unstable patient.
RECOMMENDED READING(S): Pape HC, Tornetta P 3rd, Tarkin I, Tzioupis C, Sabeson V, Olson SA. Timing of fracture fixation in multitrauma patients: the role of early total care and damage control surgery. J Am Acad Orthop Surg. 2009 Sep;17(9):541-9. Review. PubMed PMID: 19726738.Pape HC. Effects of changing strategies of fracture fixation on immunologic changes and systemic complications after multiple trauma: damage control orthopedic surgery. J Orthop Res. 2008 Nov;26(11):1478-84. PubMed PMID: 18524013.
Stable (grade I)
Borderline (grade II)
Unstable (grade III)
In extremis (grade IV)
Blood pressure ≥ 100 80-100 60-90 >50-60 Lactate levels Normal ~2.5 >2.5 acidotic ATLS Class I II-III III-IV IV
Strategy ETC ETC/DCO DCO DCO Figure 55

62 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figures 56a and 56b are the radiographs of an 88-year-old woman who had a ground level fall. Examination reveals no neurovascular compromise, and the skin condition is good. The patient is otherwise in good health, does not take medication, and lives by herself. What is the most appropriate treatment?
1. Sling 2. Total elbow arthroplasty 3. Long-arm cast immobilization 4. Closed reduction, Kirschner wire fixation, and cast immobilization 5. Open reduction and internal fixation with medial and lateral column plates
Figure 56a Figure 56b
Question 56
PREFERRED RESPONSE: 2
DISCUSSION: Most distal humerus fractures are treated with open reduction and plate fixation. There is increasing evidence that in an elderly, osteoporotic patient with a comminuted or very distal fracture, total elbow arthroplasty is associated with better outcomes than open reduction and internal fixation. Nonsurgical management, ie, a sling or cast immobilization, is generally reserved for patients with significant medical conditions that preclude surgery. Kirschner wires and casting is the treatment of choice in children. In adults, however, the periosteum is not as robust and does not help in maintaining reduction. Stiffness is inevitable with cast immobilization.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 63
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
RECOMMENDED READING(S): McKee MD, Veillette CJ, Hall JA, Schemitsch EH, Wild LM, McCormack R, Perey B, Goetz T, Zomar M, Moon K, Mandel S, Petit S, Guy P, Leung I. A multicenter, prospective, randomized, controlled trial of open reduction--internal fixation versus total elbow arthroplasty for displaced intra-articular distal humeral fractures in elderly patients. J Shoulder Elbow Surg. 2009 Jan-Feb;18(1):3-12. Epub 2008 Sep 26. PubMed PMID: 18823799.Athwal GS, Goetz TJ, Pollock JW, Faber KJ. Prosthetic replacement for distal humerus fractures. Orthop Clin North Am. 2008 Apr;39(2):201-12, vi. Review. PubMed PMID: 18374810.Frankle MA, Herscovici D Jr, DiPasquale TG, Vasey MB, Sanders RW. A comparison of open reduction and internal fixation and primary total elbow arthroplasty in the treatment of intraarticular distal humerus fractures in women older than age 65. J Orthop Trauma. 2003 Aug;17(7):473-80. PubMed PMID: 12902784.
Figure 57 is the radiograph of a 58-year-old woman who is right-hand dominant and has fallen on her flexed right elbow and is seen in the emergency department reporting isolated episodes of right elbow pain. Examination reveals that the skin is contused but intact, and her distal neurovascular examination is normal. What is the most appropriate treatment?
1. Percutaneous pinning 2. Closed reduction and extension casting 3. Fragment excision and triceps advancement 4. Open reduction and internal fixation with plate fixation 5. Open reduction and internal fixation with tension band wire construct
Figure 57
Question 57
PREFERRED RESPONSE: 4

64 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
DISCUSSION: The patient has sustained an isolated, closed fracture of the olecranon without associated instability. The bone is radiographically osteopenic and the fracture is displaced, comminuted, and includes articular marginal impaction. Plate fixation is preferred in the presence of comminution or associated transolecranon or radiocapitellar instability. Displaced fractures are generally treated surgically in an effort to restore articular congruity, restore extensor function, and to allow for early mobilization in an effort to maximize functional outcomes. A tension band wire construct is a commonly used technique but is reserved for simple fracture patterns without comminution. Excision and triceps advancement can be considered in elderly, low-demand patients that have small unreconstructable fracture patterns without associated elbow instability.
RECOMMENDED READING(S): McKee MD, Ricci WM. Fractures of the elbow. In: Baumgaertner MR, Tornetta P III, eds. Orthopaedic Knowledge Update: Trauma 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2005:181-197.Bailey CS, MacDermid J, Patterson SD, King GJ. Outcome of plate fixation of olecranon fractures. J Orthop Trauma. 2001 Nov;15(8):542-8. PubMed PMID: 11733669.
Question 58A 41-year-old man is involved in a high-speed motor vehicle crash and sustains a closed femoral midshaft fracture and a unilateral pulmonary contusion with a hemothorax, requiring placement of a chest tube. He has an initial blood pressure of 90/50 mm Hg. After receiving two liters of crystalloid, he has a blood pressure of 115/70 mm Hg and a heart rate of 90 bpm. He has normal mentation and does not require ventilator support. An arterial blood gas reveals that his delta base is -2 mmol/L. What is the most appropriate treatment for his femoral fracture?
1. Skeletal traction 2. Temporizing external fixation 3. Reamed intramedullary nailing 4. Unreamed intramedullary nailing 5. Open reduction and internal fixation
PREFERRED RESPONSE: 3
DISCUSSION: The patient responded to crystalloid resuscitation and hemodynamic parameters and the base deficit indicate that he is adequately resuscitated for definitive fracture care. In a resuscitated patient, a reamed nail is not detrimental in the setting of a pulmonary injury and is favorable for fracture union. An unreamed nail has a higher nonunion rate than a reamed nail for femoral fractures. In a skeletally mature patient with a midshaft fracture, an intramedullary nail is preferred to open reduction and internal fixation. In an adult patient, skeletal traction should be considered only as a temporary treatment prior to surgical fixation of the femoral fracture.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 65
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
RECOMMENDED READING(S): Pallister I, Empson K. The effects of surgical fracture fixation on the systemic inflammatory response to major trauma. J Am Acad Orthop Surg. 2005 Mar-Apr;13(2):93-100. Review. PubMed PMID: 15850366.Tisherman SA, Barie P, Bokhari F, Bonadies J, Daley B, Diebel L, Eachempati SR, Kurek S, Luchette F, Carlos Puyana J, Schreiber M, Simon R. Clinical practice guideline: endpoints of resuscitation. J Trauma. 2004 Oct;57(4):898-912. Review. PubMed PMID: 15514553.Pape HC, Hildebrand F, Pertschy S, Zelle B, Garapati R, Grimme K, Krettek C, Reed RL 2nd. Changes in the management of femoral shaft fractures in polytrauma patients: from early total care to damage control orthopedic surgery. J Trauma. 2002 Sep;53(3):452-61; discussion 461-2. PubMed PMID: 12352480.
Question 59A 20-year-old concert pianist sustained a diaphyseal radius fracture and underwent open reduction and internal fixation 3 years ago. She is thin and reports that the plate is irritating her after playing the piano for an hour or more. She undergoes elective plate removal of the 3.5 mm plate and 2 weeks later she refractures the radius. Which of the following statements is most accurate?
1. Diaphyseal plate removals are at higher risk of refracture. 2. Postoperative splinting increases the chance of refracture. 3. The patient would not have sustained a refracture if the plate was 4.5 mm. 4. The risk of fracture increased because the plate was removed within 5 years. 5. Waiting 5 years to remove the hardware would have decreased the risk of refracture.
PREFERRED RESPONSE: 1
DISCUSSION: The risk of refracture after hardware removal is multifactorial. Multiple variables have been looked at, such as protective splinting for 6 weeks after hardware removal, waiting 12 months or more prior to hardware removal, and the location of the fracture. The one variable that seems to correlate the most with the risk of refracture is a diaphyseal location of the initial fracture. Large fragment plates (4.5 mm), when removed, are at higher risk for refracture in the forearm.
RECOMMENDED READING(S): Deluca PA, Lindsey RW, Ruwe PA. Refracture of bones of the forearm after the removal of compression plates. J Bone Joint Surg Am. 1988 Oct;70(9):1372-6. PubMed PMID: 3182889.Rumball K, Finnegan M. Refractures after forearm plate removal. J Orthop Trauma. 1990;4(2):124-9. PubMed PMID: 2358925.
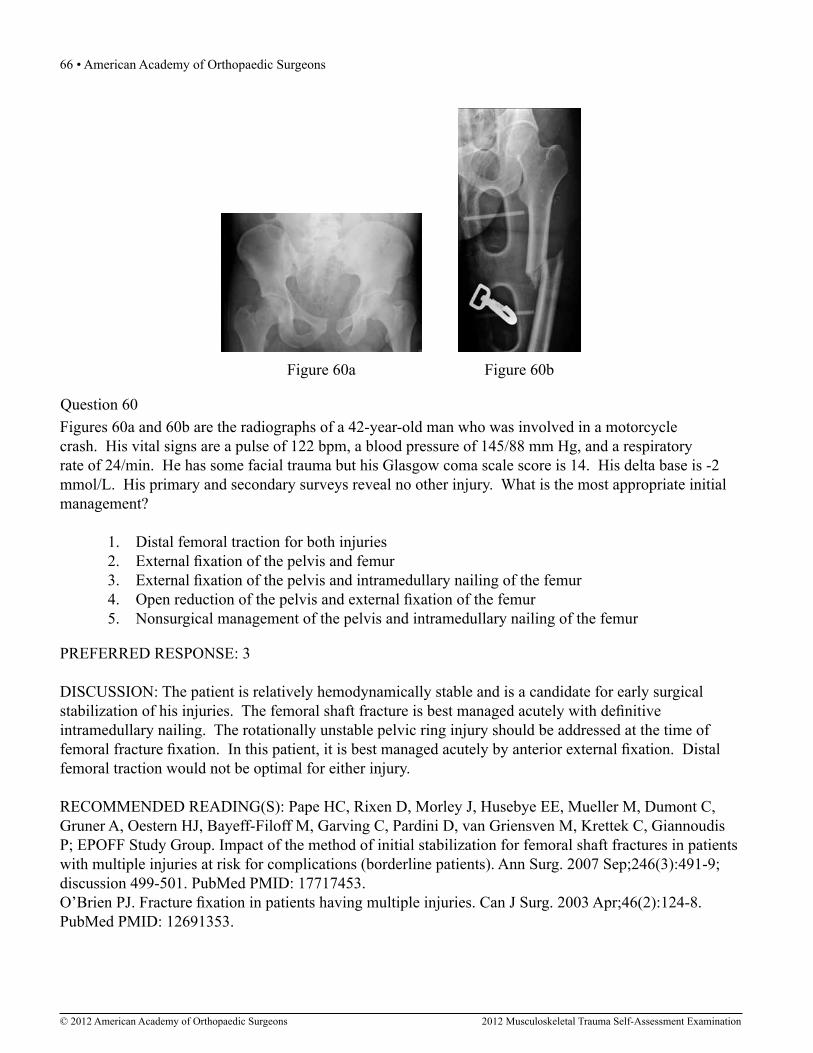
66 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figures 60a and 60b are the radiographs of a 42-year-old man who was involved in a motorcycle crash. His vital signs are a pulse of 122 bpm, a blood pressure of 145/88 mm Hg, and a respiratory rate of 24/min. He has some facial trauma but his Glasgow coma scale score is 14. His delta base is -2 mmol/L. His primary and secondary surveys reveal no other injury. What is the most appropriate initial management?
1. Distal femoral traction for both injuries 2. External fixation of the pelvis and femur 3. External fixation of the pelvis and intramedullary nailing of the femur 4. Open reduction of the pelvis and external fixation of the femur 5. Nonsurgical management of the pelvis and intramedullary nailing of the femur
Figure 60a Figure 60b
Question 60
PREFERRED RESPONSE: 3
DISCUSSION: The patient is relatively hemodynamically stable and is a candidate for early surgical stabilization of his injuries. The femoral shaft fracture is best managed acutely with definitive intramedullary nailing. The rotationally unstable pelvic ring injury should be addressed at the time of femoral fracture fixation. In this patient, it is best managed acutely by anterior external fixation. Distal femoral traction would not be optimal for either injury.
RECOMMENDED READING(S): Pape HC, Rixen D, Morley J, Husebye EE, Mueller M, Dumont C, Gruner A, Oestern HJ, Bayeff-Filoff M, Garving C, Pardini D, van Griensven M, Krettek C, Giannoudis P; EPOFF Study Group. Impact of the method of initial stabilization for femoral shaft fractures in patients with multiple injuries at risk for complications (borderline patients). Ann Surg. 2007 Sep;246(3):491-9; discussion 499-501. PubMed PMID: 17717453.O’Brien PJ. Fracture fixation in patients having multiple injuries. Can J Surg. 2003 Apr;46(2):124-8. PubMed PMID: 12691353.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 67
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figure 61
Question 61Figure 61 is the radiograph of a 34-year-old woman who was involved in a rollover motor vehicle accident. On arrival at the trauma center she is hypotensive and tachycardic. An abdominal CT scan reveals a spleen laceration. The patient remains hypotensive despite resuscitation and is taken to surgery for an emergent laparotomy and splenectomy. After surgery her delta base is -9 mmol/L. What is the most appropriate management of her pelvic ring injury?
1. Application of a pelvic binder 2. Application of skeletal traction 3. Open reduction and internal fixation 4. Placement of percutaneous iliosacral screws 5. Placement of an anterior pelvic external fixator
PREFERRED RESPONSE: 2
DISCUSSION: The patient has a displaced iliac wing and bilateral rami fractures with superior migration of the right hip. To prevent further deformity, the patient’s right hip should be placed into skeletal traction. A pelvic binder may worsen the deformity because of the iliac wing fracture. Anterior external fixation is problematic with an iliac wing fracture. Although the patient will eventually require open reduction and internal fixation and/or placement of iliosacral screws, she must be stabilized and resuscitated prior to this treatment.
RECOMMENDED READING(S): Olson SA, Reilly MC, Zura R. Treatment considerations for surgical and nonsurgical management of pelvic ring injuries. In: Olson SA, Reilly MC, eds. Acetabular and Pelvic Fractures. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2007:15-41.Smith WR, Suzuki T, Tornetta P III. Pelvic fractures: Evaluation and acute management. In: Schmidt AH, Teague DC, eds. Orthopaedic Knowledge Update: Trauma 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2010:279-292.

68 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 62When planning pin placement for external fixation of the tibia, what is the maximum extent of the knee capsular reflection from the subchondral joint line?
1. 4 mm 2. 6 mm 3. 10 mm 4. 14 mm 5. 20 mm
PREFERRED RESPONSE: 4
DISCUSSION: Intracapsular pin placement is a concern for septic arthritis. Reid and associates and DeCoster and associates have demonstrated that the maximum distal extent of the knee capsule is 14 mm from the subchondral line and occurs in the posterolateral region. The recommended placement of external fixation pins is greater than 14 mm from the subchondral line of the proximal tibia.
RECOMMENDED READING(S): DeCoster TA, Crawford MK, Kraut MA. Safe extracapsular placement of proximal tibia transfixation pins. J Orthop Trauma. 2004 Sep;18(8 Suppl):S43-7. PubMed PMID: 15472565.Reid JS, Van Slyke MA, Moulton MJ, Mann TA. Safe placement of proximal tibial transfixation wires with respect to intracapsular penetration. J Orthop Trauma. 2001 Jan;15(1):10-7. PubMed PMID: 11147682.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 69
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figure 63a Figure 63b
Question 63Figures 63a and 63b are the radiographs of a 24-year-old left-hand dominant man who felt a “snap” in the left mid-arm while arm wrestling. Examination reveals an isolated closed injury. He has significant pain and gross instability about the upper arm. His compartments are soft and he has good pulses with a well-perfused hand. He is unable to actively extend his wrist and fingers. Following splinting of the arm, his examination findings remain unchanged. What is the next most appropriate step in management?
1. Splintage followed by functional bracing 2. Intramedullary nailing with radial nerve exploration 3. Intramedullary nailing without radial nerve exploration 4. Open reduction and internal fixation with radial nerve exploration 5. Open reduction and internal fixation without radial nerve exploration
PREFERRED RESPONSE: 1
DISCUSSION: The patient has sustained an isolated, closed, comminuted fracture of the humeral diaphysis with an associated radial nerve palsy. In a report of 922 patients, Sarmiento and associates noted a nonunion rate of less than 2% with overall acceptable alignment and satisfactory functional results. Even in the presence of a radial nerve palsy, most humeral shaft fractures should be treated with functional bracing. Whereas open reduction and internal fixation and intramedullary nailing are viable treatment options, this fracture is acceptably aligned and is amenable to closed treatment. The absolute indications for surgical management include vascular injury, severe soft-tissue injury precluding closed treatment, compartment syndrome, open fracture, and associated ipsilateral forearm fracture, ie, floating elbow. Relative indications for surgical management include: segmental fracture, intra-articular extension, transverse fracture pattern with significant distraction, bilateral fracture, patient factors that preclude closed treatment such as head injury or morbid obesity, inability to maintain acceptable alignment via closed means, and polytrauma.

70 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
RECOMMENDED READING(S): Sarmiento A, Zagorski JB, Zych GA, Latta LL, Capps CA. Functional bracing for the treatment of fractures of the humeral diaphysis. J Bone Joint Surg Am. 2000 Apr;82(4):478-86. PubMed PMID: 10761938.Green A, Reid JS, Carlson DA. Fractures of the humerus. In: Baumgaertner MR, Tornetta P III, eds. Orthopaedic Knowledge Update: Trauma 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2005:163-180.
Figure 64a Figure 64b
Question 64Figures 64a and 64b are the radiographs of a 62-year-old woman who is seen in the emergency department after a fall to a flexed knee. She underwent posterior-stabilized total knee arthroplasty 6 years ago. She has no other injuries and was previously a community ambulatory without assistance. What is the most appropriate treatment?
1. Closed reduction and casting 2. Closed reduction and fracture bracing 3. Retrograde intramedullary nailing 4. Minimally invasive plate osteosynthesis 5. Revision total knee arthroplasty with distal femoral replacement
PREFERRED RESPONSE: 4

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 71
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
DISCUSSION: The patient has a displaced periprosthetic fracture just proximal to a posterior-stabilized total knee arthroplasty. Whereas distal bone stock is limited and there is evidence of radiographic osteopenia, there does not appear to be disruption of the bone-prosthetic interface and the prosthesis appears to be well fixed. Surgical fixation is indicated to restore alignment and allow for early range of motion and mobilization in an effort to optimize functional outcomes. Unless the patient is unable to tolerate surgical management, closed reduction and casting or functional bracing should be reserved for stable, minimally displaced or impacted fracture patterns. Whereas retrograde nailing is a viable treatment option, it can be difficult in the presence of a posterior-stabilized prosthetic design and distal fixation can be problematic in the setting of poor bone stock or quality. Minimally invasive plate osteosynthesis using modern-locking periarticular plates allows for indirect reduction techniques in an effort to optimize the biologic milieu and offers optimal biomechanical stability. Revisional total knee arthroplasty with a distal femoral replacement is not a good option for a young patient.
RECOMMENDED READING(S): Leighton RK. Periprosthetic fractures. In: Baumgaertner MR, Tornetta P III, eds. Orthopaedic Knowledge Update: Trauma 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2005:507-517.Schutz M, Muller M, Krettek C, Hontzsch D, Regazzoni P, Ganz R, Haas N. Minimally invasive fracture stabilization of distal femoral fractures with the LISS: a prospective multicenter study. Results of a clinical study with special emphasis on difficult cases. Injury. 2001 Dec;32 Suppl 3:SC48-54. PubMed PMID: 11888194.
Question 65A patient undergoes open reduction and internal fixation of a displaced radial neck fracture. What position should the forearm be in during the approach and during fixation?
1. Supinated during the approach and neutral for plate application 2. Neutral during the approach and pronated for plate application 3. Pronated during the approach and neutral for plate application 4. Pronated during the approach and pronated for plate application 5. Pronated during the approach and supinated for plate application
PREFERRED RESPONSE: 3
DISCUSSION: Pronating the forearm during the surgical approach decreases the danger to the posterior interosseous nerve by moving it away from the surgical field. Placing the plate straight lateral with the forearm in neutral rotation puts the plate in the safe zone that does not articulate with the proximal radioulnar joint to prevent impingement of the plate during forearm rotation.
RECOMMENDED READING(S): Mathew PK, Athwal GS, King GJ. Terrible triad injury of the elbow: current concepts. J Am Acad Orthop Surg. 2009 Mar;17(3):137-51. Review. PubMed PMID: 19264707.Cheung EV, Steinmann SP. Surgical approaches to the elbow. J Am Acad Orthop Surg. 2009 May;17(5):325-33. Review. PubMed PMID: 19411644.
72 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 66A 45-year-old man sustained bilateral femur fractures in a motorcycle accident. On admission to the emergency department, the patient is unconscious with a heart rate of 120 bpm and a systolic blood pressure of 80 mm Hg. A chest radiograph reveals bilateral pulmonary contusions. After resuscitation with 2 L of crystalloid, the patient’s heart rate is 115 bpm, the systolic blood pressure is 90 mm Hg, and the patient’s delta base is -10 mmol/L. What is the most appropriate treatment for the femoral fractures at this point?
1. External fixation 2. Percutaneous plating 3. Reamed antegrade intramedullary nailing 4. Reamed retrograde intramedullary nailing 5. Unreamed antegrade intramedullary nailing
PREFERRED RESPONSE: 1
DISCUSSION: The patient is in shock, has pulmonary contusions, and needs further resuscitation. Damage control orthopaedics (ie, external fixation of the femoral fractures) is rapid, safe, and assists in patient resuscitation. Although the patient may ultimately undergo definitive treatment with reamed intramedullary nailing or percutaneous plating, to do so at this time would not further assist resuscitation and may increase pulmonary dysfunction. Unreamed intramedullary nailing is not indicated in this patient.
RECOMMENDED READING(S): Pape HC, Rixen D, Morley J, Husebye EE, Mueller M, Dumont C, Gruner A, Oestern HJ, Bayeff-Filoff M, Garving C, Pardini D, van Griensven M, Krettek C, Giannoudis P; EPOFF Study Group. Impact of the method of initial stabilization for femoral shaft fractures in patients with multiple injuries at risk for complications (borderline patients). Ann Surg. 2007 Sep;246(3):491-9; discussion 499-501. PubMed PMID: 17717453.Canadian Orthopaedic Trauma Society. Reamed versus unreamed intramedullary nailing of the femur: comparison of the rate of ARDS in multiple injured patients. J Orthop Trauma. 2006 Jul;20(6):384-7. PubMed PMID: 16825962.Pape HC, Giannoudis PV, Krettek C, Trentz O. Timing of fixation of major fractures in blunt polytrauma: role of conventional indicators in clinical decision making. J Orthop Trauma. 2005 Sep;19(8):551-62. Review. PubMed PMID: 16118563.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 73
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figure 67
Question 67What approach should be chosen for the injury seen in Figure 67?
1. Stoppa 2. Hardinge 3. Ilioinguinal 4. Watson Jones 5. Kocher-Langenbeck
PREFERRED RESPONSE: 5
DISCUSSION: The injury shown is a transverse plus posterior wall fracture of the acetabulum. The anterior and posterior columns are fractured as one piece, the ischiopubic segment, and need to be reduced along with the posterior wall. The Kocher-Langenbeck approach will allow visualization of the transverse component through the joint and also direct exposure of the posterior wall. The ilioinguinal approach would not allow visualization or access to the posterior wall. The Stoppa, Watson Jones, and the Hardinge approaches do not allow adequate visualization of the posterior column which is needed to reduce the posterior wall. The other option is the extended iliofemoral approach which would allow excellent visualization and ability to reduce this fracture.
RECOMMENDED READING(S): de Peretti F, Schlatterer B, Cambas PM, Argenson C. [Letournel’s ilio-femoral way in acetabular fractures of the two columns. A prospective study]. Rev Chir Orthop Reparatrice Appar Mot. 1994;80(6):476-84. French. PubMed PMID: 7784643.Alonso JE, Davila R, Bradley E. Extended iliofemoral versus triradiate approaches in management of associated acetabular fractures. Clin Orthop Relat Res. 1994 Aug;(305):81-7. PubMed PMID: 8050250.

74 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figure 68a Figure 68b
Question 68Figures 68a and 68b are the radiographs of a 58-year-old right-hand dominant woman who fell from a standing height directly onto her left shoulder and now reports left shoulder pain and is unable to elevate her arm. She has a normal sensory examination. The patient refuses any type of surgical intervention. What factor will have the greatest impact on her outcome at 1 year?
1. Age 2. Bone quality 3. Hand dominance 4. Initial angulation of fracture 5. Use of a physical therapy program
PREFERRED RESPONSE: 1
DISCUSSION: In a review of over 1,000 proximal humerus fractures, Court-Brown and McQueen looked at outcomes of impacted varus fractures. These accounted for 13% of the fractures in their review. All impacted varus fractures, with the exception of two, were treated nonsurgically and were followed for 1 year. They determined that the age of the patient was the major factor in overall outcome. Good results can be expected with younger patients, but results deteriorate with advancing age. In regards to angulation of the fracture, they found no correlation between increased varus angulation and shoulder function. Most patients had good or excellent results no matter how much final varus was achieved. They also noted that physical therapy did not have a significant impact on outcome. In their study, poor results in patients who lacked therapy were more related to the advanced age of the patients. Hanson and associates prospectively evaluated nonsurgical management of 124 proximal humerus fractures for 1 year. They found that displacement of the fracture only gradually influenced the constant scores and that the DASH revealed the patients on average had not fully recovered at 1 year. They also noted that 97.6% of employed patients were able to return to work and that employed patients on average had significantly lower differences in side-to-side constant and DASH scores. Solid bony union was seen in 93% at 1 year and fracture consolidation was seen in 98%. The predicted risk of delayed and nonunion was 7% with smoking increasing the nonunion risk by 5.5 times.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 75
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
RECOMMENDED READING(S): Court-Brown CM, McQueen MM. The impacted varus (A2.2) proximal humeral fracture: prediction of outcome and results of nonoperative treatment in 99 patients. Acta Orthop Scand. 2004 Dec;75(6):736-40. PubMed PMID: 15762264Hanson B, Neidenbach P, de Boer P, Stengel D, Functional outcomes after nonoperative management of fractures of the proximal humerus, J Shoulder Elbow Surg, 2009 Jul-Aug, 18(4):612-21. PubMED PMID 19559373.
Figure 69
Question 69Figure 69 is the radiograph of a 52-year-old right-hand dominant man who fell while skiing. He was initially treated at a mountainside clinic where he was placed in a sling. He now reports moderate shoulder pain but has no other complaints. What is the most appropriate management?
1. Hemiarthroplasty 2. Total shoulder arthroplasty 3. Open reduction and internal fixation 4. Sling for 6 to 8 weeks followed by mobilization 5. Sling followed by early mobilization within 2 to 3 weeks
PREFERRED RESPONSE: 3
DISCUSSION: The patient sustained a four-part valgus impacted fracture of the proximal humerus with a significantly increased head-shaft angle and resultant displacement of the greater and lesser tuberosities. In an effort to restore anatomic alignment and optimize functional outcomes, open reduction and internal fixation is indicated. A valgus impacted pattern has been noted to have improved outcomes and lower rates of osteonecrosis. In addition, this patient has adequate bone stock and all efforts should be made to salvage his shoulder. A sling will not change the overall alignment and is therefore not the most appropriate treatment option. Hemiarthroplasty is reserved for unreconstructable patterns, and total shoulder arthroplasty would only be considered in the acute scenario if there was significant preexisting glenoid wear or inflammatory arthropathy.

76 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
RECOMMENDED READING(S): Green A, Reid JS, Carlson DA. Fractures of the humerus. In: Baumgaertner MR, Tornetta P III, eds. Orthopaedic Knowledge Update: Trauma 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2005:163-180.Robinson CM, Page RS. Severely impacted valgus proximal humeral fractures. Results of operative treatment. J Bone Joint Surg Am. 2003 Sep;85-A(9):1647-55. PubMed PMID: 12954821.
Question 70Pelvic packing for a hemodynamically unstable patient with a pelvic ring fracture is best described by which of the following techniques?
1. Placing a pelvic external fixator followed by packing the pelvis with lap pads via a subumbilical incision 2. Placing lap pads for packing via a subumbilical incision in the angiography suite 3. Placing lap pads for packing using the lateral window of the ilioinguinal approach (anterior approach to the internal iliac fossa) 4. Packing the retroperitoneum with lap pads after exploration of the abdomen by the general surgeons 5. Direct exploration of the pelvic vasculature via a midline incision followed by packing with lap pads
PREFERRED RESPONSE: 1
DISCUSSION: For the technique of pelvic packing patients are placed supine on an operating room table. For rotationally and/or vertically unstable fracture patterns, an external fixator is then placed to stabilize the pelvis so that the volume of the pelvis is decreased and the packing has counterforce acting against it. An approximately 6 cm to 8 cm midline incision is made extending upwards from the pubic symphysis and heading toward the umbilicus. The rectus fascia is then divided in the midline. The bladder is retracted to one side and three lap pads are packed deep to the pelvic brim. The bladder is retracted to the other side and three more lap pads are placed on that side as well. The first sponge is placed at the level of the sacroiliac joint, the second anterior to the first sponge, and the third in the retropubic space lateral and just deep to the bladder. All should be placed below the level of the pelvic brim. The fascia is then closed. If the patient is hemodynamically unstable after stabilization, then packing of the pelvis angiography should be considered.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 77
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
RECOMMENDED READING(S): Hak DJ, Smith WR, Suzuki T. Management of hemorrhage in life-threatening pelvic fracture. J Am Acad Orthop Surg. 2009 Jul;17(7):447-57. Review. PubMed PMID: 19571300.Osborn PM, Smith WR, Moore EE, Cothren CC, Morgan SJ, Williams AE, Stahel PF. Direct retroperitoneal pelvic packing versus pelvic angiography: A comparison of two management protocols for haemodynamically unstable pelvic fractures. Injury. 2009 Jan;40(1):54-60. Epub 2008 Nov 30. PubMed PMID: 19041967.Cothren CC, Osborn PM, Moore EE, Morgan SJ, Johnson JL, Smith WR. Preperitonal pelvic packing for hemodynamically unstable pelvic fractures: a paradigm shift. J Trauma. 2007 Apr;62(4):834-9; discussion 839-42. PubMed PMID: 17426537.Smith WR, Moore EE, Osborn P, Agudelo JF, Morgan SJ, Parekh AA, Cothren C. Retroperitoneal packing as a resuscitation technique for hemodynamically unstable patients with pelvic fractures: report of two representative cases and a description of technique. J Trauma. 2005 Dec;59(6):1510-4. PubMed PMID: 16394933.
Question 71A previously healthy man who weighs 70 kg (154 lb) sustains an acute blood loss of 2 liters after a motorcycle crash. Which of the following statements about physiologic parameters is unique to this amount of blood loss?
1. Pulse pressure will be widened. 2. Urine output will be at the lower limits of normal. 3. Tachycardia will be present, but with no change in systolic blood pressure. 4. Systolic blood pressure will be decreased with a narrowed pulse pressure. 5. Systolic blood pressure will be maintained with an elevated diastolic blood pressure.
PREFERRED RESPONSE: 4
DISCUSSION: The normal adult blood volume is approximately 7% of body weight. For example, a man weighing 70 kg has a circulating blood volume of approximately 5 liters. A blood loss of 2 liters places the patient in a class IV hemorrhage of more than 40% blood volume loss. Signs and symptoms of class IV hemorrhage include marked tachycardia of greater than 140 bpm, a significant decrease in blood pressure, and a very narrow pulse pressure. Urinary output is negligible, and mental status is markedly depressed. The skin is cold and pale. Physiologic parameters associated with a class II hemorrhage include: urine output that is at the lower limits of normal; the presence of tachycardia but with no change in the systolic blood pressure; and maintenance of the systolic blood pressure with an elevated diastolic blood pressure. A widened pulse pressure correlates with a class I hemorrhage.
RECOMMENDED READING(S): American College of Surgeons Committee on Trauma, eds. ATLS: Advanced Trauma Life Support for Doctors. 8th ed. Chicago, IL: American College of Surgeons;2008:69-85.Hak DJ, Stahel PF, Giannoudis P. Pathophysiology of the polytrauma patient. In: Schmidt AH, Teague DC, eds. Orthopaedic Knowledge Update: Trauma 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2010:117-131.

78 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figures 72a through 72d are the radiographs and CT scans of a 45-year-old man who fell 10 feet from a ladder and sustained an injury to the right knee. Examination reveals no open wounds and the skin was in good condition with moderate swelling and no fracture blisters. The patient is neurovascularly intact. What is the most appropriate treatment?
1. Hinged knee brace and non-weight-bearing for 6 weeks 2. Percutaneous screw fixation 3. Open reduction and internal fixation with a laterally applied nonlocking plate 4. Open reduction and internal fixation with posteromedial and lateral plates via one anterior approach 5. Open reduction and internal fixation with posteromedial and lateral plates via dual incisions
Figure 72c Figure 72d
Question 72
Figure 72a Figure 72b
PREFERRED RESPONSE: 5
DISCUSSION: The patient has a bicondylar tibial plateau fracture with metadiaphyseal separation, depressed lateral articular surface, and a medial articular coronal split. This fracture is ideally treated with open reduction and internal fixation. A nonlocking lateral plate may not be able to protect against varus collapse through the metaphysis as well as a locking plate. However, neither plate can reliably deal with reduction and reliable fixation of the medial articular fracture. Recent studies have shown the relative frequency of the so-called “posteromedial fragment,” and have recommended supplemental fixation of the medial articular surface because standard lateral implants may not be able to gain screw purchase in the posteromedial bone. Other studies have shown good fracture reduction and maintenance of reduction with low complication rates using the two-incision technique with double plating. Placing dual plates via one anterior incision is associated with soft-tissue complications.
RECOMMENDED READING(S): Higgins TF, Kemper D, Klatt J. Incidence and morphology of the posteromedial fragment in bicondylar tibial plateau fractures. J Orthop Trauma. 2009 Jan;23(1):45-51. PubMed PMID: 19104303.Barei DP, O’Mara TJ, Taitsman LA, Dunbar RP, Nork SE. Frequency and fracture morphology of the posteromedial fragment in bicondylar tibial plateau fracture patterns. J Orthop Trauma. 2008 Mar;22(3):176-82. PubMed PMID: 18317051.Barei DP, Nork SE, Mills WJ, Henley MB, Benirschke SK. Complications associated with internal fixation of high-energy bicondylar tibial plateau fractures utilizing a two-incision technique. J Orthop Trauma. 2004 Nov-Dec;18(10):649-57. PubMed PMID: 15507817.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 79
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figure 73c
Question 73Figures 73a through 73c are the radiographs of a 57-year-old woman who twisted her ankle stepping off a curb and now has lateral foot pain. Examination reveals intact skin and point tenderness over the base of the fifth metatarsal. What is the most appropriate treatment?
1. Fragment excision 2. Intramedullary screw fixation 3. Non-weight-bearing cast for 6 weeks 4. Percutaneous Kirschner wire fixation 5. Immediate weight bearing with a postoperative shoe
Figure 73a Figure 73b
PREFERRED RESPONSE: 5
DISCUSSION: The patient has an avulsion fracture of the fifth metatarsal base. Unlike a true Jones-type fracture, this is amenable to immediate weight bearing. Intramedullary screw fixation may be indicated in select patients with a Jones fracture but not with this fracture type. Fragment excision can be considered in the presence of a symptomatic nonunion of this fracture, but is not indicated acutely. Percutaneous pinning is not indicated.
RECOMMENDED READING(S): Dameron TB Jr. Fractures of the Proximal Fifth Metatarsal: Selecting the Best Treatment Option. J Am Acad Orthop Surg. 1995 Mar;3(2):110-114. PubMed PMID: 10790659.Schwartz AK, Brage ME, Laughlin RT, Stephen D. Foot injuries. In: Baumgaertner MR, Tornetta P III, eds. Orthopaedic Knowledge Update: Trauma 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2005:453-468.

80 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 74Which of the following factors is associated with improved outcomes following surgery for hip fractures?
1. Immediate surgical intervention 2. Early discharge to a skilled nursing facility 3. Choosing spinal versus general anesthesia for surgery 4. Choosing total hip arthroplasty instead of hemiarthroplasty for a displaced femoral neck fracture 5. Correction of metabolic abnormalities prior to surgical intervention
PREFERRED RESPONSE: 5
DISCUSSION: Many studies have looked at patient outcomes following hip fracture surgery. While early surgery in these patients is recommended, medical optimization prior to surgical intervention is warranted in all cases. Anesthetic type and discharge status have not been proven to alter patient outcomes. Total hip arthroplasty has improved function at 1 year compared with hemiarthroplasty; no changes in mortality have been reported.
RECOMMENDED READING(S): Egol KA, Strauss EJ. Perioperative considerations in geriatric patients with hip fracture: what is the evidence? J Orthop Trauma. 2009 Jul;23(6):386-94. Review. PubMed PMID: 19550223.Parvizi J, Ereth MH, Lewallen DG. Thirty-day mortality following hip arthroplasty for acute fracture. J Bone Joint Surg Am. 2004 Sep;86-A(9):1983-8. PubMed PMID: 15342761.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 81
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figure 75e
Figure 75a Figure 75b Figure 75c
Figure 75d
Figures 75a through 75e are the CT scans and radiographs of a 56-year-old man who is a restrained driver involved in a motor vehicle accident in which his car is struck at 35 mph. He has pain to the right buttock and groin regions. Examination reveals that he is neurologically intact and has no evidence of other injuries. What is the most appropriate management at this time?
1. Anterior pelvic external fixation 2. Iliosacral screw fixation on the right side 3. Open reduction and internal fixation of the sacrum 4. Bed rest for 1 to 2 weeks, followed by non-weight-bearing on the right side for 4 weeks 5. Immediate mobilization and weight bearing as tolerated on the right lower extremity
Question 75
PREFERRED RESPONSE: 5
DISCUSSION: The patient has a lateral compression-type pelvic fracture with an incomplete fracture of the sacrum. This is a stable pattern that will tolerate immediate weight bearing with little risk of displacement. Anterior pelvic external fixation is occasionally indicated for a lateral compression-type pelvic fracture to reduce a severe internal rotation deformity, but that is not present in this patient. Iliosacral screw fixation may be indicated if the patient has pain that prevents mobilization with this injury or in the case of a sacral fracture that is complete or comminuted, which can indicate a higher risk of displacement.

82 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
RECOMMENDED READING(S): Tile M. Acute Pelvic Fractures: II. Principles of Management. J Am Acad Orthop Surg. 1996 May;4(3):152-161. PubMed PMID: 10795050.Sembler G, Lien J, Tornetta P: Nonoperative Immediate Weightbearing of Minimally Displaced Lateral Compression Sacral Fractures Does Not Result in Displacement. Proceedings of the Orthopaedic Trauma Association 25th Annual Meeting, San Diego, CA 2009. Rosemont, IL, Orthopaedic Trauma Association 2009.Bruce B, Reilly M, Sims S: Predicting future displacement of non-operatively managed sacral fractures: Can it be done? Proceedings of the Orthopaedic Trauma Association 25th Annual Meeting, San Diego, CA 2009. Rosemont, IL, Orthopaedic Trauma Association 2009.
How is the fracture pattern shown in Figures 76a through 76c best classified?
1. Moore 1 2. Moore 3 3. Schatzker 3 4. Schatzker 6 5. OTA type 41C
Figure 76a
Question 76
Figure 76b Figure 76c
PREFERRED RESPONSE: 2
DISCUSSION: This fracture is best classified as a “rim avulsion pattern”: Moore type 3. A Moore 1 is a posteromedial shear fracture associated with subluxation of the tibiofemoral joint. This classifiaction is useful for fractures associated with knee instability and patterns that do not fit into the Shatzker classification. A Shatzker 3 is a pure depression type, and a type 6 has metaphyseal-diahyseal dissociation. OTA type C are complete articular fractures.
RECOMMENDED READING(S): Egol KA, Koval KJ. Fractures of the proximal tibia. In: Bucholz RW, Heckman JD, Court-Brown C, eds. Rockwood and Green’s Fractures in Adults. 6th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2006:1999-2029.Moore TM. Fracture--dislocation of the knee. Clin Orthop Relat Res. 1981 May;(156):128-40. PubMed PMID: 7226641.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 83
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figures 77a and 77b are the radiographs of a 45-year-old man who fell into a ditch and sustained a twisting injury to the left lower extremity. Examination in the emergency department reveals normal neurologic function, no skin compromise, and palpable pedal pulses. The patient has no other complaints and has an otherwise normal examination. What additional imaging study is recommended?
1. MRI of the left knee 2. Arterial duplex of the left leg 3. CT scan of the left ankle 4. CT scan of the chest, abdomen, and pelvis 5. CT scan of the cervical, thoracic, and lumbar spine
Figure 77a Figure 77b
Question 77
PREFERRED RESPONSE: 3
DISCUSSION: Spiral distal tibia fractures are frequently associated with intra-articular fracture extension, usually involving the posterior malleolus. This may or may not be visible on the radiographs. A CT scan of the ankle is recommended to identify this associated injury. This is especially important when considering intramedullary nail fixation of the distal tibia fracture because a previously nondisplaced intra-articular fracture may become displaced as the nail is inserted to its final depth. Anteroposterior screw fixation prior to nailing may be useful in these cases. With the patient’s history, there is no indication of thoracic, abdominal, pelvic, or spinal trauma. There are no signs of vascular injury and preoperative MRI is not indicated.
RECOMMENDED READING(S): Hou Z, Zhang Q, Zhang Y, Li S, Pan J, Wu H. A occult and regular combination injury: the posterior malleolar fracture associated with spiral tibial shaft fracture. J Trauma. 2009 May;66(5):1385-90. PubMed PMID: 19430243.Boraiah S, Gardner MJ, Helfet DL, Lorich DG. High association of posterior malleolus fractures with spiral distal tibial fractures. Clin Orthop Relat Res. 2008 Jul;466(7):1692-8. Epub 2008 Mar 18. PubMed PMID: 18347885.

84 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 78Long-term alendronate (Fosamax) use for osteoporosis has been associated with which of the following?
1. Scurvy 2. Detached retina 3. Uterine carcinoma 4. Osteonecrosis of the femoral head 5. Diaphyseal femoral insufficiency fractures
PREFERRED RESPONSE: 5
DISCUSSION: Alendronate is a bisphosphonate that inhibits the ruffled border of the osteoclast. When used long term, this class of medication prevents the normal bone remodeling process. Long-term use has recently been shown to be associated with insufficiency fractures of the femur. Osteonecrosis of the jaw has been described but not in other anatomic locations. Scurvy occurs because of a lack of vitamin C and use of bisphosphonates is not associated with uterine cancer or a detached retina.
RECOMMENDED READING(S): Lenart BA, Lorich DG, Lane JM. Atypical fractures of the femoral diaphysis in postmenopausal women taking alendronate. N Engl J Med. 2008 Mar 20;358(12):1304-6. PubMed PMID: 18354114.Goh SK, Yang KY, Koh JS, Wong MK, Chua SY, Chua DT, Howe TS. Subtrochanteric insufficiency fractures in patients on alendronate therapy: a caution. J Bone Joint Surg Br. 2007 Mar;89(3):349-53. PubMed PMID: 17356148.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 85
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figures 79a and 79b are the radiographs of a 78-year-old right-hand dominant man who fell at home and sustained an isolated injury to his right shoulder. He lives alone and is independent with his activities of daily living. Examination reveals a closed injury and a normal neurologic examination. What is the most appropriate management?
1. Shoulder hemiarthroplasty 2. Hanging arm cast for 6 to 8 weeks 3. Shoulder immobilizer for 6 weeks, followed by range-of-motion exercises 4. Open reduction and internal fixation of the proximal humerus with a locking plate 5. Sling, followed by pendulum exercises with elbow range of motion within 1 to 2 weeks
Figure 79a Figure 79b
Question 79
PREFERRED RESPONSE: 5
DISCUSSION: The patient has an isolated proximal humerus fracture in acceptable alignment, thus surgical treatment is not indicated. Multiple studies have shown the benefits of earlier mobilization and therapy in patients who are treated nonsurgically for proximal humerus fractures. A hanging arm cast can be used in proximal humerus fractures, but typically would not be recommended for a length of 6 to 8 weeks because a prolonged time in a hanging arm cast has the disadvantage of immobilizing the elbow during that time as well.
RECOMMENDED READING(S): Lin KC, Krishnan SG. Shoulder trauma: Bone. In: Fischgrund JS, ed. Orthopaedic Knowledge Update 9. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:287-299.Koval KJ, Gallagher MA, Marsicano JG, Cuomo F, McShinawy A, Zuckerman JD. Functional outcome after minimally displaced fractures of the proximal part of the humerus. J Bone Joint Surg Am. 1997 Feb;79(2):203-7. PubMed PMID: 9052540.Lefevre-Colau MM, Babinet A, Fayad F, Fermanian J, Anract P, Roren A, Kansao J, Revel M, Poiraudeau S. Immediate mobilization compared with conventional immobilization for the impacted nonoperatively treated proximal humeral fracture. A randomized controlled trial. J Bone Joint Surg Am. 2007 Dec;89(12):2582-90. PubMed PMID: 18056488.

86 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 80A 38-year-old woman is polytraumatized in a motor vehicle crash. She has multiple injuries including a unilateral femur fracture. The patient is felt to be borderline and, although she is currently stable, she could potentially deteriorate quickly. Which of the following parameters has been suggested as an indicator of which patients would benefit from damage control?
1. Normothermia 2. Hemoglobin of less than 9 g/dL 3. Unilateral lung contusion evident on CT only 4. Injury severity score of greater than 40 without thoracic injury 5. Injury Severity Score of less than 18 with a pulmonary contusion
PREFERRED RESPONSE: 4
DISCUSSION: Polytraumatized patients can be classified as stable, unstable, borderline, or in extremis. Management of the borderline patient is controversial because it is unclear which patients can safely undergo early definitive surgical stabilization of fractures, and which patients would benefit from temporizing “damage control” stabilization to allow adequate resuscitation and physiologic stabilization prior to definitive treatment. Although the question of damage control versus early total care is unresolved, there are several clinical parameters that have been suggested for use in deciding who should be treated with early damage control. These include Injury Severity Score of greater than 40, Injury Severity Score of greater than 20 with thoracic trauma, multiple injuries with severe pelvic/abdominal trauma and hemorrhagic shock, bilateral femoral fractures, pulmonary contusion noted on radiographs, hypothermia of less than 35 degrees C), and a head injury with an Abbreviated Injury Score of 3 or greater. A hemoglobin of 9 g/dL is not included in these suggested parameters.
RECOMMENDED READING(S): Bosse MJ, Kellam JR. Damage control orthopaedic surgery. In: Browner BD, Jupiter JB, Levine AM, Trafton PG, Krettek C, eds. Skeletal Trauma: Basic Science, Management, and Reconstruction. Vol 1. 4th ed. Philadelphia, PA: WB Saunders; 2008:197-218.Pape HC, Tornetta P 3rd, Tarkin I, Tzioupis C, Sabeson V, Olson SA. Timing of fracture fixation in multitrauma patients: the role of early total care and damage control surgery. J Am Acad Orthop Surg. 2009 Sep;17(9):541-9. Review. PubMed PMID: 19726738.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 87
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figure 81c Figure 81d
Question 81A 37-year-old man is evaluated in the emergency department after a motor vehicle accident at 40 mph. He reports low back and buttock pain and numbness in his perineum. After initial radiographic evaluation of his pelvis, he is advised to attempt weight bearing but is unable to because of severe pain. A CT scan of the pelvis is ordered. The radiographs and CT scan are shown in Figures 81a through 81d. What study should be obtained next?
1. CT scan of the abdomen 2. Judet views of the pelvis 3. MRI scan of the lumbar spine 4. Lateral radiograph of the sacrum 5. Electromyography of the lumbosacral plexus
Figure 81a Figure 81b
PREFERRED RESPONSE: 4
DISCUSSION: The patient has a U-type fracture of the sacrum. The best way to visualize this fracture is with a lateral view of the sacrum or sagittal reformatted images of the CT scan. Standard pelvic radiographs often miss this injury. A high index of suspicion must be maintained for a transverse fracture component (H- or U-type fracture) in a patient with bilateral sacral injuries, especially without any anterior pelvic ring fractures. This injury occurs by a different mechanism than pelvic ring disruptions, thus the sacrum will fracture oftentimes without associated anterior pelvic injuries. These injuries have a high rate of associated neurologic injury. Treatment of these injuries varies based on neurologic compromise and displacement.

88 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
RECOMMENDED READING(S): Mehta S, Auerbach JD, Born CT, Chin KR. Sacral fractures. J Am Acad Orthop Surg. 2006 Nov;14(12):656-65. Review. PubMed PMID: 17077338.Schildhauer TA, Bellabarba C, Nork SE, Barei DP, Routt ML Jr, Chapman JR. Decompression and lumbopelvic fixation for sacral fracture-dislocations with spino-pelvic dissociation. J Orthop Trauma. 2006 Jul;20(7):447-57. PubMed PMID: 16891935.Templeman D, Tornetta P III. Pelvic and acetabular fractures. In: Fischgrund JS, ed. Orthopaedic Knowledge Update 9. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:389-397.
Figures 82a and 82b are the radiographs of a 52-year-old woman who fell down the stairs and sustained an acute hemarthrosis of the elbow. What is the most common complication following surgical treatment of this injury?
1. Elbow contracture 2. Complex regional pain syndrome 3. Posterior interosseous nerve palsy 4. Bridging heterotopic ossification of the elbow 5. Elbow instability requiring ligamentous reconstruction
Figure 82a Figure 82b
Question 82
PREFERRED RESPONSE: 1
DISCUSSION: The patient has a displaced capitellum fracture that requires surgical intervention. Wheras complex regional pain syndrome, posterior interosseous nerve palsy, bridging heterotopic ossification of the elbow, and elbow instability requiring ligamentous reconstruction are seen as sequelae of various traumatic elbow injuries, elbow contracture is frequently seen following this specific injury.
RECOMMENDED READING(S): Ruchelsman DE, Tejwani NC, Kwon YW, Egol KA. Open reduction and internal fixation of capitellar fractures with headless screws. Surgical technique. J Bone Joint Surg Am. 2009 Mar 1;91 Suppl 2 Pt 1:38-49. PubMed PMID: 19255199.Ring D, Jupiter JB, Gulotta L. Articular fractures of the distal part of the humerus. J Bone Joint Surg Am. 2003 Feb;85-A(2):232-8. PubMed PMID: 12571299.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 89
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
The vessel that is exposed crossing the interval used for an anterior approach to the hip between the tensor fascia lata and the sartorius muscle is a branch of what artery?
1. Deep femoral artery (profunda) 2. Superficial femoral artery 3. Superior gluteal artery 4. Descending recurrent femoral artery 5. External iliac
Question 83
PREFERRED RESPONSE: 1
DISCUSSION: The ascending branch of the lateral femoral circumflex artery crosses the surgical field between the tensor fascia lata and the sartorius muscles and has to be ligated during this approach. It is a branch of the profunda femoris artery.
RECOMMENDED READING(S): Hoppenfeld S, deBoer P, Buckley R, eds. Surgical Exposures in Orthopaedics: The Anatomic Approach. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:409-419.Anderson JE, ed. Grant’s Atlas of Anatomy. 8th ed. Baltimore/London, Williams and Wilkins; 1983:fig 4-11, 4-25.Masquelet AC, McCullough CJ, Tubiana R. An Atlas of Surgical Exposures of the Lower Extremity. Philadelphia, PA: JB Lippincott; 1993:76, 81.

90 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figure 84b Figure 84c
Question 84
Three years following repair of a subtrochanteric femur fracture, a 26-year-old man has a draining sinus shown in Figure 84a. Radiographs are shown in Figures 84b and 84c. Management should consist of which of the following?
1. Hip disarticulation 2. Infectious diseases consultation and long-term suppressive antibiotics 3. Incision and drainage, removal of hardware, excision of heterotopic bone, and culture-directed antibiotics 4. Excision of heterotopic bone and radiation therapy to prevent recurrence 5. Excision of heterotopic bone and administration of nonsteroidal anti-inflammatory drugs to prevent recurrence
Figure 84a
PREFERRED RESPONSE: 3
DISCUSSION: This is a case of chronic osteomyelitis with infected hardware and a healed fracture. Limb salvage should be attempted in the patient. The presence of a chronic draining sinus requires surgical débridement . Removal of the implant and as much of the infected heterotopic bone will reduce the bacterial load. Culture-directed antibiotics are started after deep cultures are obtained. Infectious diseases consultation is obtained following surgical intervention. Long-term suppressive antibiotics are not the treament of choice in healthy patients who can tolerate a surgical procedure.
RECOMMENDED READING(S): Cierny G III, DiPasquale D. Adult osteomyelitis. In: Cierny G III, McLaren AC, Wongworawat MD, eds. Orthopaedic Knowledge Update: Musculoskeletal Infection. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2009:135-153.Egol KA, Singh JR, Nwosu U. Functional outcome in patients treated for chronic posttraumatic osteomyelitis. Bull NYU Hosp Jt Dis. 2009;67(4):313-7. PubMed PMID: 20001930.Motsitsi NS. Management of infected nonunion of long bones: the last decade (1996-2006). Injury. 2008 Feb;39(2):155-60. Epub 2008 Jan 29. Review. PubMed PMID: 18234202.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 91
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 85Which of the following is the best predictor of mortality after a patient has sustained a pelvic ring injury?
1. Gender 2. Comorbidities 3. Fracture pattern 4. Use of angiography 5. Shock on presentation
PREFERRED RESPONSE: 5
DISCUSSION: Starr and associates demonstrated that age and shock on presentation were predictors of mortality after pelvic ring injury. Smith and associates showed that the amount of blood transfusions in the first 24 hours was also predictive of mortality. Gender, fracture pattern, use of angiography, and comorbidities do not correlate directly with mortality.
RECOMMENDED READING(S): Smith W, Williams A, Agudelo J, Shannon M, Morgan S, Stahel P, Moore E. Early predictors of mortality in hemodynamically unstable pelvis fractures. J Orthop Trauma. 2007 Jan;21(1):31-7. PubMed PMID: 17211266.Starr AJ, Griffin DR, Reinert CM, Frawley WH, Walker J, Whitlock SN, Borer DS, Rao AV, Jones AL. Pelvic ring disruptions: prediction of associated injuries, transfusion requirement, pelvic arteriography, complications, and mortality. J Orthop Trauma. 2002 Sep;16(8):553-61. PubMed PMID: 12352563.
Question 86What is the best way to determine whether a radial head implant is too thick intraoperatively?
1. Visually assess the radiocapitellar joint. 2. Visually assess widening of the lateral ulnohumeral joint. 3. Assess widening of the radiocapitellar joint on an AP radiograph. 4. Assess the elbow for concentric reduction on a lateral radiograph. 5. Assess widening of the medial ulnohumeral joint on an AP radiograph.
PREFERRED RESPONSE: 2
DISCUSSION: Widening of the medial ulnohumeral joint on an AP radiograph is only visible after overlengthening of the radial head by 6 mm or more. At least in this cadaver study, the most sensitive method was to visually assess the lateral aspect of the ulnohumeral joint with the radial head resected and then with the trial radial head in place. This method allows detection of any overlengthening.
RECOMMENDED READING(S): Frank SG, Grewal R, Johnson J, Faber KJ, King GJ, Athwal GS. Determination of correct implant size in radial head arthroplasty to avoid overlengthening. J Bone Joint Surg Am. 2009 Jul;91(7):1738-46. PubMed PMID: 19571097.Doornberg JN, Linzel DS, Zurakowski D, Ring D. Reference points for radial head prosthesis size. J Hand Surg Am. 2006 Jan;31(1):53-7. PubMed PMID: 16443104.

92 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figure 87a Figure 87b
Question 87Figures 87a and 87b are the radiographs of an 18-year-old pedestrian who was struck by a car. During intramedullary nailing, it is difficult to maintain proper alignment. Poller blocking screws placed in the proximal fragment at which position(s) relative to the nail can help prevent the typical deformity?
1. Anterior only 2. Anterior and medial 3. Anterior and lateral 4. Posterior and medial 5. Posterior and lateral
PREFERRED RESPONSE: 5
DISCUSSION: This is a proximal one third tibial shaft fracture. Typically nailing of this fracture creates a valgus and procurvatum malalignment that must be addressed. This can be difficult when using an intramedullary nail in the wide metaphyseal bone of the proximal tibia. To help direct and center the nail in the metaphysis, blocking screws can be used. Blocking screws should be placed where the nail should not travel. If the nail was passed with the proximal fragment in this position, it would occupy the lateral and posterior aspects of the metaphyseal fragment. To prevent this, blocking screws should be placed in the lateral and posterior aspects of the proximal fragment.
RECOMMENDED READING(S): Stedtfeld HW, Mittlmeier T, Landgraf P, Ewert A. The logic and clinical applications of blocking screws. J Bone Joint Surg Am. 2004;86-A Suppl 2:17-25. PubMed PMID: 15691104.Lindvall E, Sanders R, Dipasquale T, Herscovici D, Haidukewych G, Sagi C. Intramedullary nailing versus percutaneous locked plating of extra-articular proximal tibial fractures: comparison of 56 cases. J Orthop Trauma. 2009 Aug;23(7):485-92. PubMed PMID: 19633457.Lang GJ, Cohen BE, Bosse MJ, Kellam JF. Proximal third tibial shaft fractures. Should they be nailed? Clin Orthop Relat Res. 1995 Jun;(315):64-74. PubMed PMID: 7634688.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 93
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 88What mechanism of injury is most likely to cause a fracture of the anteromedial facet of the coronoid?
1. Extension and axial load 2. Varus and posteromedial rotation 3. Valgus and posteromedial rotation 4. Varus and posterolateral rotation 5. Valgus and posterolateral rotation
PREFERRED RESPONSE: 2
DISCUSSION: The mechanism of injury in a fracture of the anteromedial facet of the coronoid is typically a varus and posteromedial rotation force on the forearm which is the opposite of a terrible triad injury. First, the lateral collateral ligament is injured and then the medial coronoid is compressed against and then under the medial trochlea.
RECOMMENDED READING(S): Steinmann SP. Coronoid process fracture. J Am Acad Orthop Surg. 2008 Sep;16(9):519-29. Review. PubMed PMID: 18768709.Doornberg JN, Ring D. Coronoid fracture patterns. J Hand Surg Am. 2006 Jan;31(1):45-52. PubMed PMID: 16443103.Doornberg JN, Ring DC. Fracture of the anteromedial facet of the coronoid process. J Bone Joint Surg Am. 2006 Oct;88(10):2216-24. PubMed PMID: 17015599.
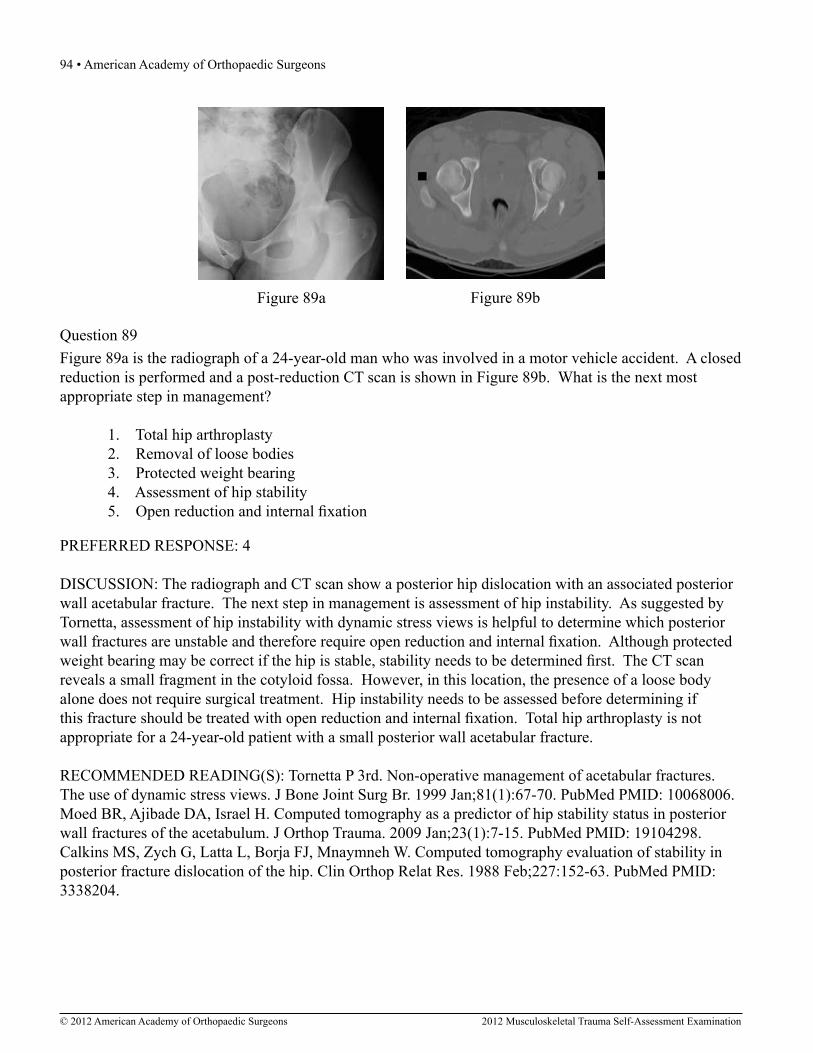
94 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figure 89a Figure 89b
Question 89Figure 89a is the radiograph of a 24-year-old man who was involved in a motor vehicle accident. A closed reduction is performed and a post-reduction CT scan is shown in Figure 89b. What is the next most appropriate step in management?
1. Total hip arthroplasty 2. Removal of loose bodies 3. Protected weight bearing 4. Assessment of hip stability 5. Open reduction and internal fixation
PREFERRED RESPONSE: 4
DISCUSSION: The radiograph and CT scan show a posterior hip dislocation with an associated posterior wall acetabular fracture. The next step in management is assessment of hip instability. As suggested by Tornetta, assessment of hip instability with dynamic stress views is helpful to determine which posterior wall fractures are unstable and therefore require open reduction and internal fixation. Although protected weight bearing may be correct if the hip is stable, stability needs to be determined first. The CT scan reveals a small fragment in the cotyloid fossa. However, in this location, the presence of a loose body alone does not require surgical treatment. Hip instability needs to be assessed before determining if this fracture should be treated with open reduction and internal fixation. Total hip arthroplasty is not appropriate for a 24-year-old patient with a small posterior wall acetabular fracture.
RECOMMENDED READING(S): Tornetta P 3rd. Non-operative management of acetabular fractures. The use of dynamic stress views. J Bone Joint Surg Br. 1999 Jan;81(1):67-70. PubMed PMID: 10068006.Moed BR, Ajibade DA, Israel H. Computed tomography as a predictor of hip stability status in posterior wall fractures of the acetabulum. J Orthop Trauma. 2009 Jan;23(1):7-15. PubMed PMID: 19104298.Calkins MS, Zych G, Latta L, Borja FJ, Mnaymneh W. Computed tomography evaluation of stability in posterior fracture dislocation of the hip. Clin Orthop Relat Res. 1988 Feb;227:152-63. PubMed PMID: 3338204.
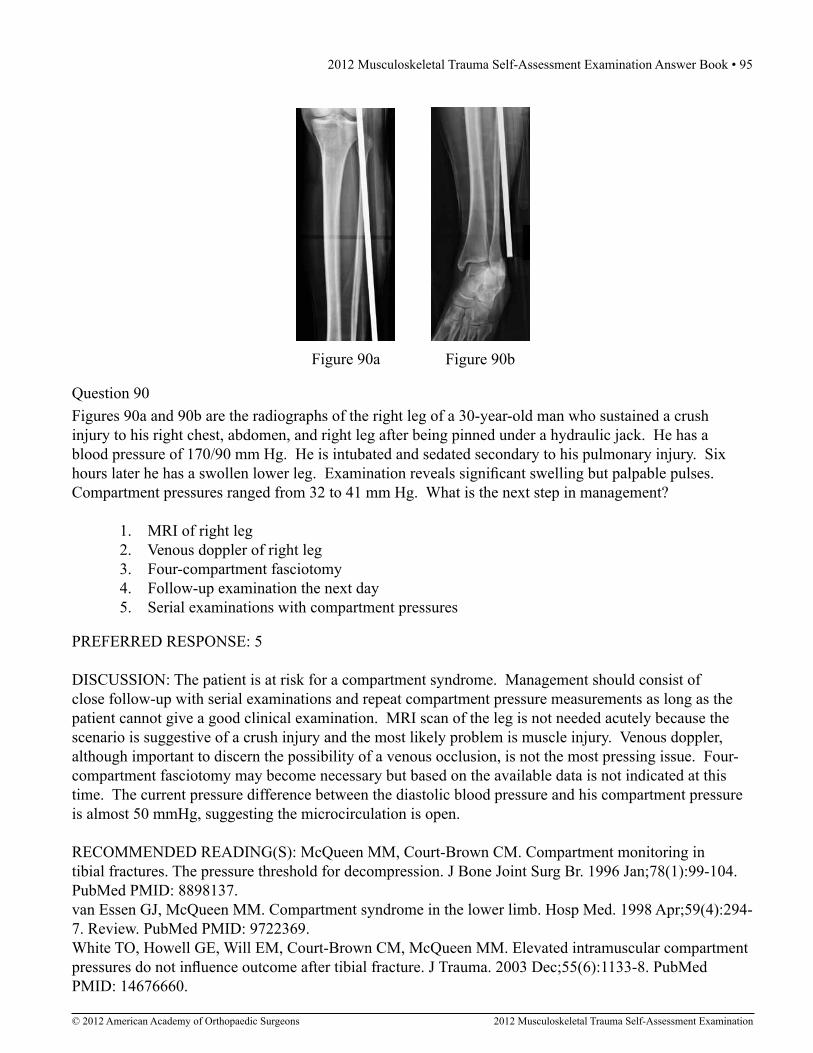
2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 95
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figure 90a Figure 90b
Question 90Figures 90a and 90b are the radiographs of the right leg of a 30-year-old man who sustained a crush injury to his right chest, abdomen, and right leg after being pinned under a hydraulic jack. He has a blood pressure of 170/90 mm Hg. He is intubated and sedated secondary to his pulmonary injury. Six hours later he has a swollen lower leg. Examination reveals significant swelling but palpable pulses. Compartment pressures ranged from 32 to 41 mm Hg. What is the next step in management?
1. MRI of right leg 2. Venous doppler of right leg 3. Four-compartment fasciotomy 4. Follow-up examination the next day 5. Serial examinations with compartment pressures
PREFERRED RESPONSE: 5
DISCUSSION: The patient is at risk for a compartment syndrome. Management should consist of close follow-up with serial examinations and repeat compartment pressure measurements as long as the patient cannot give a good clinical examination. MRI scan of the leg is not needed acutely because the scenario is suggestive of a crush injury and the most likely problem is muscle injury. Venous doppler, although important to discern the possibility of a venous occlusion, is not the most pressing issue. Four-compartment fasciotomy may become necessary but based on the available data is not indicated at this time. The current pressure difference between the diastolic blood pressure and his compartment pressure is almost 50 mmHg, suggesting the microcirculation is open.
RECOMMENDED READING(S): McQueen MM, Court-Brown CM. Compartment monitoring in tibial fractures. The pressure threshold for decompression. J Bone Joint Surg Br. 1996 Jan;78(1):99-104. PubMed PMID: 8898137.van Essen GJ, McQueen MM. Compartment syndrome in the lower limb. Hosp Med. 1998 Apr;59(4):294-7. Review. PubMed PMID: 9722369.White TO, Howell GE, Will EM, Court-Brown CM, McQueen MM. Elevated intramuscular compartment pressures do not influence outcome after tibial fracture. J Trauma. 2003 Dec;55(6):1133-8. PubMed PMID: 14676660.

96 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figure 91
Question 91Figure 91 is the radiograph of a 20-year-old man who kicked a door while intoxicated. At the emergency department, his leg is placed into a long-leg cast. After 2 hours, he reports increasing pain, numbness, and tingling in his toes. What is the most appropriate initial treatment?
1. Elevate leg on pillows 2. Administer IV morphine 3. Observation of the patient 4. Bivalve and spread the cast 5. Apply ice to the lower extremity
PREFERRED RESPONSE: 4
DISCUSSION: The patient appears to have some indications of a compartment syndrome: increasing pain and signs of nerve compression. Tibia fractures also should heighten the suspicion for a compartment syndrome. Two basic mechanisms of compartment syndrome are that an increase in volume occurs in an enclosed space or there is a decrease in size of the space. In this situation, both are likely occurring; post-fracture swelling is occurring within a closed space and if a cast is in place that may constrict the space even more. One way to increase the available space for swelling would be to bivalve and spread the cast. If the extremity has been casted, then it is vitally important that the cast is bivalved and the surrounding soft dressings under the cast be removed so that all external compression of the compartment has been eliminated. In the face of compartment syndrome, elevation of the limb, masking the pain with morphine, application of ice, or observation alone are all inappropriate.
RECOMMENDED READING(S): Browner BD, Jupiter JB, Levine AM, Trafton P, Krettek C, eds. Skeletal Trauma: Basic Science, Management, and Reconstruction. 3rd ed. Philadelphia, PA: Saunders Elsevier; 2003:268-292.Weiner G, Styf J, Nakhostine M, Gershuni DH. Effect of ankle position and a plaster cast on intramuscular pressure in the human leg. J Bone Joint Surg Am. 1994 Oct;76(10):1476-81. PubMed PMID: 7929495.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 97
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figure 92
Question 92Figure 92 is the radiograph of a 45-year-old man who was thrown from his horse and now reports groin pain. Which of the following is the most common long-term sequelae of this injury?
1. Gait abnormality 2. Sexual dysfunction 3. Chronic low back pain 4. Quadriceps weakness 5. Posttraumatic osteoarthritis
PREFERRED RESPONSE: 2
DISCUSSION: The radiograph reveals an anterior posterior compression injury to the pelvic ring which is commonly seen after horseback riding injuries. In a large series of patients with this type of injury, 18 of 20 patients had sexual dysfunction after sustaining this injury. Posttraumatic osteoarthritis of the sacroiliac joints may occur, but is less common in this type of injury. Chronic low back pain, gait abnormalities, and quadriceps weakness are not typically seen with this type of injury.
RECOMMENDED READING(S): Collinge CA, Archdeacon MT, LeBus G. Saddle-horn injury of the pelvis. The injury, its outcomes, and associated male sexual dysfunction. J Bone Joint Surg Am. 2009 Jul;91(7):1630-6. PubMed PMID: 19571085.Smith I, Jamieson EW, Davey KJ, McDonald IJ. Pelvic diastasis from the saddle: not to be forgotten. J Trauma. 2002 Dec;53(6):1179-82. PubMed PMID: 12478049.van Nieuwenhoven AL, van Laarhoven CJ, Van der Werken C. Pelvic injuries in equestrians on buck-jumping horses. J Trauma. 1997 Nov;43(5):867-8. PubMed PMID: 9390505.

98 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 93A 23-year-old woman is involved in a motorcycle accident. She sustains bilateral femur fractures (Abbreviated Injury Score [AIS]=3), an intra-abdominal injury (AIS=3), facial fractures (AIS=2), and a pulmonary injury (AIS=2). What is her Injury Severity Score (ISS)?
1. 13 2. 18 3. 22 4. 27 5. 35
PREFERRED RESPONSE: 3
DISCUSSION: The ISS is calculated as the sum of the squares of three highest AIS scores from the six body regions, thus this patient’s ISS score is 22. The ISS does correlate with mortality, but the ISS does not score multiple injuries to the same body region, hence the bilateral femur fractures score the same as a unilateral fracture. The New Injury Severity Score (NISS) was developed because of this shortcoming of the ISS. The ISS is used in studies to characterize patient injury severity, with a value of 18 or above indicating polytrauma in many studies.
RECOMMENDED READING(S): Poole GV, Tinsley M, Tsao AK, Thomae KR, Martin RW, Hauser CJ. Abbreviated Injury Scale does not reflect the added morbidity of multiple lower extremity fractures. J Trauma. 1996 Jun;40(6):951-4; discussion 954-5. PubMed PMID: 8656482.Balogh ZJ, Varga E, Tomka J, Süveges G, Tóth L, Simonka JA. The new injury severity score is a better predictor of extended hospitalization and intensive care unit admission than the injury severity score in patients with multiple orthopaedic injuries. J Orthop Trauma. 2003 Aug;17(7):508-12. PubMed PMID: 12902789.
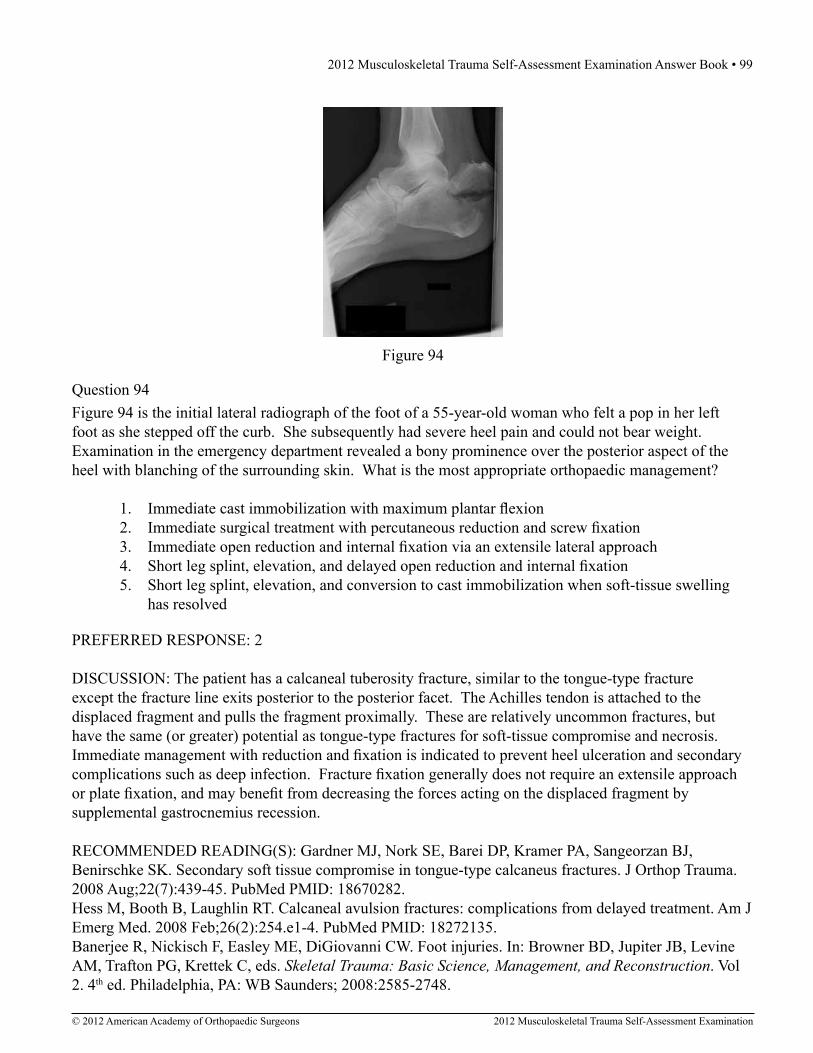
2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 99
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figure 94
Question 94Figure 94 is the initial lateral radiograph of the foot of a 55-year-old woman who felt a pop in her left foot as she stepped off the curb. She subsequently had severe heel pain and could not bear weight. Examination in the emergency department revealed a bony prominence over the posterior aspect of the heel with blanching of the surrounding skin. What is the most appropriate orthopaedic management?
1. Immediate cast immobilization with maximum plantar flexion 2. Immediate surgical treatment with percutaneous reduction and screw fixation 3. Immediate open reduction and internal fixation via an extensile lateral approach 4. Short leg splint, elevation, and delayed open reduction and internal fixation 5. Short leg splint, elevation, and conversion to cast immobilization when soft-tissue swelling has resolved
PREFERRED RESPONSE: 2
DISCUSSION: The patient has a calcaneal tuberosity fracture, similar to the tongue-type fracture except the fracture line exits posterior to the posterior facet. The Achilles tendon is attached to the displaced fragment and pulls the fragment proximally. These are relatively uncommon fractures, but have the same (or greater) potential as tongue-type fractures for soft-tissue compromise and necrosis. Immediate management with reduction and fixation is indicated to prevent heel ulceration and secondary complications such as deep infection. Fracture fixation generally does not require an extensile approach or plate fixation, and may benefit from decreasing the forces acting on the displaced fragment by supplemental gastrocnemius recession.
RECOMMENDED READING(S): Gardner MJ, Nork SE, Barei DP, Kramer PA, Sangeorzan BJ, Benirschke SK. Secondary soft tissue compromise in tongue-type calcaneus fractures. J Orthop Trauma. 2008 Aug;22(7):439-45. PubMed PMID: 18670282.Hess M, Booth B, Laughlin RT. Calcaneal avulsion fractures: complications from delayed treatment. Am J Emerg Med. 2008 Feb;26(2):254.e1-4. PubMed PMID: 18272135.Banerjee R, Nickisch F, Easley ME, DiGiovanni CW. Foot injuries. In: Browner BD, Jupiter JB, Levine AM, Trafton PG, Krettek C, eds. Skeletal Trauma: Basic Science, Management, and Reconstruction. Vol 2. 4th ed. Philadelphia, PA: WB Saunders; 2008:2585-2748.

100 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
A 24-year-old man is involved in a motor vehicle accident at 60 mph. He sustains multiple injuries including an intra-abdominal injury requiring a splenectomy and a closed right femoral shaft fracture. Which variable will best indicate the patient’s resuscitation status when deciding whether to proceed with definitive care of the fracture at the conclusion of the laparotomy?
1. Heart rate 2. Hematocrit 3. Base deficit 4. Urine output 5. Systolic blood pressure
Question 95
PREFERRED RESPONSE: 3
DISCUSSION: A metabolic parameter such as the base deficit or lactate level has been shown to better reflect the resuscitation status and survival after trauma. Normalization of hemodynamic parameters does not accurately reflect the resuscitation status and a patient can be in compensated shock (occult tissue hypoperfusion) despite normalization of the heart rate and blood pressure. The use of temporizing measures with delayed definitive fracture treatment has been shown to decrease systemic complications in these patients with occult hypoperfusion.
RECOMMENDED READING(S): Tisherman SA, Barie P, Bokhari F, Bonadies J, Daley B, Diebel L, Eachempati SR, Kurek S, Luchette F, Carlos Puyana J, Schreiber M, Simon R. Clinical practice guideline: endpoints of resuscitation. J Trauma. 2004 Oct;57(4):898-912. Review. PubMed PMID: 15514553.Crowl AC, Young JS, Kahler DM, Claridge JA, Chrzanowski DS, Pomphrey M. Occult hypoperfusion is associated with increased morbidity in patients undergoing early femur fracture fixation. J Trauma. 2000 Feb;48(2):260-7. PubMed PMID: 10697084.Pallister I, Empson K. The effects of surgical fracture fixation on the systemic inflammatory response to major trauma. J Am Acad Orthop Surg. 2005 Mar-Apr;13(2):93-100. Review. PubMed PMID: 15850366.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 101
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 96A 27-year-old woman who was an unrestrained driver in a head-on collision sustained the following injuries: bilateral supracondylar femur fractures, a left talus fracture, multiple left metatarsal fractures, a right distal radius fracture, and a left open elbow fracture-dislocation. Which of the following serologic inflammatory markers drawn in this patient has been shown to be a reliable measure of systemic inflammatory response, correlating with injury severity and outcome?
1. IL-6 2. IL-8 3. IL-10 4. C-reactive protein 5. Tumor necrosis factor-alpha
PREFERRED RESPONSE: 1
DISCUSSION: In response to trauma, the body demonstrates a systemic inflammatory response that varies in intensity according to the severity of the injuries sustained. Increased production of proinflammatory cytokines serves to activate the host immune system. The activation of systemic inflammatory response may lead to remote end organ damage with neutrophil demargination and disruption of the vascular endothelium. Disturbances in microcirculation exacerbate local tissue hypoxia, and parenchymal necrosis may ensue. Furthermore, the systemic inflammatory response serves as the basis for the development of adult respiratory response distress syndrome (ARDS) and multiple organ failure following trauma. Several serologic inflammatory markers have been investigated for their potential usefulness in measuring and monitoring the inflammatory response to a major trauma. These markers include IL-1, IL-6, IL-8,-IL-10, and C-reactive protein and tumor necrosis factor-alpha. For many of these markers, serum concentration is noted to increase following severe trauma, but the extent and duration of elevation have been too variable to allow for clinical application. IL-6 has been shown to be a reliable measure of systemic inflammatory response, correlating with injury severity and outcome. It has been recommended that measurement of IL-6 concentration be traced to evaluate the severity of the inflammatory response. In this way, it may be possible to clarify the risks associated with secondary procedures such as fracture fixation and to determine when these procedures should be performed.
RECOMMENDED READING(S): Keel M, Trentz O. Pathophysiology of polytrauma. Injury. 2005 Jun;36(6):691-709. Review. PubMed PMID: 15910820.Pape HC, van Griensven M, Rice J, Gansslen A, Hildebrand F, Zech S, Winny M, Lichtinghagen R, Krettek C. Major secondary surgery in blunt trauma patients and perioperative cytokine liberation: determination of the clinical relevance of biochemical markers. J Trauma. 2001 Jun;50(6):989-1000. PubMed PMID: 11426112.Sears BW, Stover MD, Callaci J. Pathoanatomy and clinical correlates of the immunoinflammatory response following orthopaedic trauma. J Am Acad Orthop Surg. 2009 Apr;17(4):255-65. Review. PubMed PMID: 19307674.

102 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figure 97b
Question 97Figures 97a and 97b are the radiographs of a 27-year-old man involved in a motorcycle crash who sustained a right proximal humerus fracture. Which of the following is most associated with osteonecrosis?
1. Intact medial hinge 2. Metaphyseal head extension of fracture of less than 8 mm 3. Tobacco use 4. Age 5. Angular displacement of the head of 30 degrees
Figure 97a
PREFERRED RESPONSE: 2
DISCUSSION: Hertel and associates demonstrated factors that are predictive of osteonecrosis of the humeral head after fracture. Factors shown to be predictive of osteonecrosis include: fractures consisting of four fragments, angular displacement of the head (greater than 45 degrees), the amount of displacement of the tuberosities (displacement of greater than 10 mm), glenohumeral dislocation, and head-split components. Factors associated with good prognosis include: length of the metaphyseal head extension (calcar segments of greater than 8 mm), the integrity of the medial hinge, and the basic fracture pattern. When the above criteria (anatomic neck, short calcar, disrupted hinge) were combined, positive predictive values of up to 97% could be obtained for osteonecrosis. However, the degree to which this osteonecrosis impacts long-term outcome is unclear and should not be the only indication for proximal humeral arthroplasty.
RECOMMENDED READING(S): Hertel R, Hempfing A, Stiehler M, Leunig M. Predictors of humeral head ischemia after intracapsular fracture of the proximal humerus. J Shoulder Elbow Surg. 2004 Jul-Aug;13(4):427-33. PubMed PMID: 15220884.Nho S, Brophy RH, Barker JU, Cornell CN, MacGillivray JD, Innovations in management of displaced proximal humerus fractures, J Am Acad Orthop Surg, 2007 Jan;15(1):12-26. Review. PMID: 17213379.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 103
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 98Clinical staging of osteomyelitis using the Cierney-Mader classification system takes into account which of the following factors?
1. Age and gender of patient 2. Fracture type and type of bacteria 3. Host status and extent of infected bone 4. Immune status and chronicity of infection 5. Bacterial resistance and source of infection
PREFERRED RESPONSE: 3
DISCUSSION: The Cierney-Mader classification system takes into account three types of patients with osteomyelitis: (A) healthy, (B) those with comorbidities, and (C) a host in whom treatment will lead to greater morbidity than the infection. Furthermore, the disease is addressed based on its complexity: type I-medullary, type II-superficial, type III-localized, and type IV-diffuse.
RECOMMENDED READING(S): Cierny G III, DiPasquale D. Adult osteomyelitis. In: Cierny G III, McLaren AC, Wongworawat MD, eds. Orthopaedic Knowledge Update: Musculoskeletal Infection. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2009:135-153.Mader JT, Shirtliff M, Calhoun JH. Staging and staging application in osteomyelitis. Clin Infect Dis. 1997 Dec;25(6):1303-9. Review. PubMed PMID: 9431368.

104 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Figure 99b
Question 99Figures 99a and 99b are the radiographs of a 76-year-old woman who sustained an injury to her dominant arm in a fall. Which of the following is the most common complication seen following treatment with a locked plate and screw construct?
1. Osteomyelitis 2. Osteonecrosis 3. Posttraumatic osteoarthritis 4. Deltoid heterotopic ossification 5. Screw penetration of the articular surface
Figure 99a
PREFERRED RESPONSE: 5
DISCUSSION: The most common complication reported following use of a locked plate construct for a displaced proximal humerus fracture is screw penetration of the humeral head (16% to 30%). Heterotopic ossification can be seen following proximal humerus fracture and repair and is associated with a deltoid split approach. The rate of osteonecrosis following a valgus impacted three-part fracture is 5% to 10%. Posttraumatic osteoarthritis is not seen frequently following surgical repair of these fractures. Infection is uncommon after this surgery, and chronic osteomyelitis is rare.
RECOMMENDED READING(S): Egol KA, Ong CC, Walsh M, Jazrawi LM, Tejwani NC, Zuckerman JD. Early complications in proximal humerus fractures (OTA Types 11) treated with locked plates. J Orthop Trauma. 2008 Mar;22(3):159-64. PubMed PMID: 18317048.Brunner F, Sommer C, Bahrs C, Heuwinkel R, Hafner C, Rillmann P, Kohut G, Ekelund A, Muller M, Audigé L, Babst R. Open reduction and internal fixation of proximal humerus fractures using a proximal humeral locked plate: a prospective multicenter analysis. J Orthop Trauma. 2009 Mar;23(3):163-72. PubMed PMID: 19516088.

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 105
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 100A 63-year-old woman with osteopenia is struck by a motor vehicle and sustains a Schatzker 2 (AO/OTA Type B) fracture of the lateral tibial plateau. She has 1.5 cm of joint depression and 7 mm of condylar widening. What is the most appropriate surgical fixation for this injury?
1. Lateral nonlocking plate 2. Percutaneous screws 3. External fixation 4. Lateral locking plate 5. Medial and lateral plating
PREFERRED RESPONSE: 1
DISCUSSION: The patient has a significantly displaced partial articular fracture of the tibial plateau. Surgical treatment is preferred in an effort to restore the axis of the knee, achieve an articular reduction, and allow for repair of commonly associated soft-tissue injuries such as meniscal tears. This requires direct reduction, and fixation should provide subarticular support, interfragmentary compression, and buttress. This is best achieved with an undercontoured lateral nonlocking plate. Screws alone are unlikely to be adequately stable in this patient. Locking plates do not provide buttress effect when used in pure locking mode. In addition, locking plates add significant incremental cost to the procedure.
RECOMMENDED READING(S): Marsh JL, Templeman D. Fractures of the tibial plateau. In: Baumgaertner MR, Tornetta P III, eds. Orthopaedic Knowledge Update: Trauma 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2005:419-429.Karunakar MA, Egol KA, Peindl R, Harrow ME, Bosse MJ, Kellam JF. Split depression tibial plateau fractures: a biomechanical study. J Orthop Trauma. 2002 Mar;16(3):172-7. PubMed PMID: 11880780.

106 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
RESPONSES FOR QUESTIONS 101 THROUGH 104 1. Open reduction and internal fixation with absolute stability 2. Open reduction and internal fixation with relative stability 3. Closed reduction with casting 4. Reamed locked intramedullary nailing 5. External fixation
For each of the following fractures choose the best method for definitive fixation.
A 25-year-old man fell off a golf cart and injured his right forearm. The radiographs show both a radial shaft and an ulna fracture. The fractures are highly comminuted, and there is a small laceration of about 1 cm over the fracture site.
Question 101
Question 102A 45-year-old man was skiing when he sustained a direct blow to the lateral side of his left knee. Radiographs reveal a left split depression tibial plateau fracture.
Question 103A 19-year-old woman was involved in a high-speed motor vehicle accident. She has an obvious deformity of her right thigh. Radiographs reveal a transverse mid-shaft femur fracture.
Question 104A 22-year-old woman injured her ankle when she fell off a ladder. Radiographs reveal a displaced large posterior malleolus fracture of about 45% of the joint.
PREFERRED RESPONSE: 2
PREFERRED RESPONSE: 1
PREFERRED RESPONSE: 4
PREFERRED RESPONSE: 1

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 107
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
DISCUSSION FOR QUESTIONS 101 THROUGH 104: Basic understanding of fracture care requires a fundamental knowledge of the principles regarding absolute and relative stability. Compression plating and anatomic reduction of articular fractures are examples of absolute stability. Bridge plating, external fixation, casting, and intramedullary nailing are all examples of relative stability. Both bone forearm fractures have long been treated with open reduction and internal fixation even in the light of open wounds. Results have been excellent with plate fixation. Recently, intramedullary nails that are contoured and locked have been used in the treatment of both bone forearm fractures, but they are not reamed. It is well established that with restoring the proper radial bow, length, and alignment, optimal function can be achieved. Open reduction and internal fixation allows this achievement. In cases where comminution exists, absolute stability may have to be sacrificed so as to not strip small comminuted bone fragments. Therefore, a bridging technique is worthwhile. External fixation can be used as a temporary technique until the soft tissues are more amenable to definitive fixation. Cast treatment is not indicated in adult forearm fractures. Locking nails for forearm use are not reamed. With regards to articular fractures, anatomic reduction and rigid stabilization are required to achieve the best results and allow for fracture healing. This environment also allows for the best chance of the cartilage repair process to form “hyaline-like” cartilage. Open reduction and internal fixation with absolute stability is the mainstay of treatment for partial articular fractures such as split depression tibial plateau fractures and posterior malleolus fractures involving greater than about 25% to 30% of the joint. The gold standard for the treatment of a closed femur fracture is a reamed intramedullary locked nail. Results are uniformly excellent. This can be done without stripping of the soft tissues such as in open reduction and internal fixation. External fixation can be used as a temporary device in patients in extremis for damage control reasons.
RECOMMENDED READING(S) FOR QUESTIONS 101 THROUGH 104: Moed BR, Kellam JF, Foster RJ, Tile M, Hansen ST Jr. Immediate internal fixation of open fractures of the diaphysis of the forearm. J Bone Joint Surg Am. 1986 Sep;68(7):1008-17. PubMed PMID: 3745238.Jones DB Jr, Kakar S. Adult diaphyseal forearm fractures: intramedullary nail versus plate fixation. J Hand Surg Am. 2011 Jul;36(7):1216-9. Epub 2011 May 14. PubMed PMID: 21571446.Gardner MJ, Streubel PN, McCormick JJ, Klein SE, Johnson JE, Ricci WM. Surgeon practices regarding operative treatment of posterior malleolus fractures. Foot Ankle Int. 2011 Apr;32(4):385-93. PubMed PMID: 21733441.Ricci WM, Gruen GS, Summers H, Siska PA. Fractures of the femoral diaphysis. In: Schmidt AH, Teague DC, eds. Orthopaedic Knowledge Update: Trauma 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2010:431-444.Forberger J, Sabandal PV, Dietrich M, Gralla J, Lattmann T, Platz A. Posterolateral approach to the displaced posterior malleolus: functional outcome and local morbidity. Foot Ankle Int. 2009 Apr;30(4):309-14. PubMed PMID: 19356354.De Vries JS, Wijgman AJ, Sierevelt IN, Schaap GR. Long-term results of ankle fractures with a posterior malleolar fragment. J Foot Ankle Surg. 2005 May-Jun;44(3):211-7. PubMed PMID: 15940600.Bai B, Kummer FJ, Sala DA, Koval KJ, Wolinsky PR. Effect of articular step-off and meniscectomy on joint alignment and contact pressures for fractures of the lateral tibial plateau. J Orthop Trauma. 2001 Feb;15(2):101-6. PubMed PMID: 11232647.Rüedi TP, Murphy M, eds. AO Principles of Fracture Management. Thieme, Stuttgart, 2000.
END OF SERIES

108 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
CLINICAL SITUATION FOR QUESTIONS 105 THROUGH 107Figure 105 is the radiograph of a 72-year-old woman who fell down the steps and injured her left leg. Because she was unable to get up on her own or reach a telephone, she was not discovered until 24 hours after the incident and was then brought to the emergency department by ambulance. The patient is a community ambulator, who drives and lives alone. Her medical history includes hypertension, type 2 diabetes mellitus, and hypothyroidism. She takes enalapril, levothyroxine, and rosiglitazone. She is obese (BMI>30). Examination reveals that the left lower extremity is shortened and externally rotated. She has pain with movement of the extremity. There is no other bony tenderness in either the upper or contralateral lower extremity.
Figure 105
Question 105Which of the following imaging studies must be obtained for this patient?
1. Duplex scan of both lower extremities 2. MRI scan of the hip 3. Traction internal rotation radiograph of the hip 4. Frog lateral of the hip 5. CT scan of the abdomen and pelvis
PREFERRED RESPONSE: 1
2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 109
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 106What is the most appropriate protocol for surgical management of this patient?
1. Must be performed within the first 24 hours 2. Should be delayed until a stress test is performed 3. May occur only following optimization of medical conditions 4. Must be postponed until normalization of the BMI 5. A delay of several days after admission results in greater technical ease
PREFERRED RESPONSE: 3
Question 107Treatment of the patient’s injury is best accomplished by which of the following?
1. Cephalomedullary nail 2. Closed reduction and percutaneous pinning 3. Open reduction and internal fixation 4. Total hip arthroplasty 5. Hemiarthroplasty
PREFERRED RESPONSE: 4
DISCUSSION FOR QUESTIONS 105 THROUGH 107:This scenario is a common one for the presentation of a displaced intracapsular hip fracture. Injured elderly patients not found for an extended period of time prior to hospital admission are at greater risk for the development of a venous thromboembolism and should have a screening Doppler. Whereas a traction-internal rotation radiograph is valuable in further delineating the fracture pattern, it is not necessary in making the diagnosis. The frog lateral radiograph should be avoided in hip fracture management because it causes unneeded pain and risks displacement if none exists. An MRI scan is not indicated in a displaced fracture, but may be useful in diagnosing nondisplaced fractures. A CT scan is not warranted in the absence of clinical signs of intra-abdominal trauma or a high-energy mechanism. Surgical treatment is warranted in this ambulatory, independent patient. Whereas many studies have looked at optimal timing of surgery, no definitive time frame has been elucidated. Most authors agree that surgery is urgent and should follow optimization of all comorbid medical conditions. Technical aspects of the surgery are not dependent on time from injury. Given that this is a displaced femoral neck fracture in an elderly patient, the options of fracture repair, which include intramedullary nailing, closed reduction and pinning, and open reduction and internal fixation, are associated with high rates of complications and revision surgery. Of the two arthroplasty choices, total hip arthroplasty has been shown to yield the best clinical and functional results with a lower rate of reoperation. Hemiarthroplasty is reserved for low functioning or minimally ambulatory patients.

110 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
RECOMMENDED READINGS FOR QUESTIONS 105 THROUGH 107:Hefley FG Jr, Nelson CL, Puskarich-May CL. Effect of delayed admission to the hospital on the preoperative prevalence of deep-vein thrombosis associated with fractures about the hip. J Bone Joint Surg Am. 1996 Apr;78(4):581-3. PubMed PMID: 8609137.van den Bekerom MP, Hilverdink EF, Sierevelt IN, Reuling EM, Schnater JM, Bonke H, Goslings JC, van Dijk CN, Raaymakers EL. A comparison of hemiarthroplasty with total hip replacement for displaced intracapsular fracture of the femoral neck: a randomised controlled multicentre trial in patients aged 70 years and over. J Bone Joint Surg Br. 2010 Oct;92(10):1422-8. Erratum in: J Bone Joint Surg Br. 2011 Jan;93(1):140. PubMed PMID: 20884982.
END OF SERIES
CLINICAL SITUATION FOR QUESTIONS 108 THROUGH 110A 23-year-old man was injured in a high-speed motorcycle accident. He sustained bilateral pulmonary contusions, a closed left femoral fracture, an open, comminuted, contaminated, diaphyseal left tibia fracture without bone loss, and a small subdural bleed. His blood pressure in the trauma bay was 85/50 mm Hg and did not respond to initial volume resuscitation. He has a heart rate of 122/min and a core temperature of 34.7°C.
Question 108What is the optimal initial treatment for his orthopaedic injuries?
1. Irrigation and débridement of the open fracture and reamed intramedullary nailing of the femoral and tibial fractures 2. Irrigation and débridement of the open fracture, reamed intramedullary nailing of the femur, and external fixation of the tibia 3. Irrigation and débridement of the open fracture and external fixation of both fractures 4. Irrigation and débridement of the open fracture, a reamed femoral nail, and an unreamed tibial nail 5. Irrigation and débridement of the open fracture in the ICU and a calcaneal traction pin
PREFERRED RESPONSE: 3

2012 Musculoskeletal Trauma Self-Assessment Examination Answer Book • 111
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
Question 109Definitive fixation of the tibia is ideally
1. uniplanar external fixation. 2. a reamed intramedullary nail. 3. an unreamed intramedullary nail. 4. either a reamed or an unreamed intramedullary nail. 5. bridge plating.
PREFERRED RESPONSE: 4
Question 110Four months after injury, the tibia is showing evidence of slow healing on radiographs. What is the optimal treatment for this potential nonunion?
1. Convert to circular external fixation 2. Exchange nailing and autograft 3. Exchange nailing and bone morphogenetic protein 4. Tibial plate 5. Observation until 6 months after injury
PREFERRED RESPONSE: 5
DISCUSSION FOR QUESTIONS 108 THROUGH 110:This patient is unstable and is not a good candidate for Early Total Care (ETC) and therefore should be managed by the tenets of Damage Control Orthopaedics (DCO). Débridement and external fixation is preferable for this patient. Intramedullary nails would be a component of ETC. Calcaneal traction is not considered ideal because it does not allow the patient to travel as easily. The S.P.R.I.N.T. study concluded that while reamed nails may offer benefit in closed fractures, there was no difference between reamed or unreamed nails in the treatment of open fractures of the tibia. Uniplanar external fixation and tibial plating are not considered the best options for open tibia fractures. Additional findings of the S.P.R.I.N.T. study conclude that delaying surgical intervention for at least 6 months after injury may reduce the need for reoperation.

112 • American Academy of Orthopaedic Surgeons
© 2012 American Academy of Orthopaedic Surgeons 2012 Musculoskeletal Trauma Self-Assessment Examination
RECOMMENDED READINGS FOR QUESTIONS 108 THROUGH 110:Pape HC, Tornetta P 3rd, Tarkin I, Tzioupis C, Sabeson V, Olson SA. Timing of fracture fixation in multitrauma patients: the role of early total care and damage control surgery. J Am Acad Orthop Surg. 2009 Sep;17(9):541-9. Review. PubMed PMID: 19726738.Renaldo N, Egol K. Damage-control orthopedics: evolution and practical applications. Am J Orthop (Belle Mead NJ). 2006 Jun;35(6):285-91; discussion 291. Review. PubMed PMID: 16841792.Study to Prospectively Evaluate Reamed Intramedullary Nails in Patients with Tibial Fractures Investigators, Bhandari M, Guyatt G, Tornetta P 3rd, Schemitsch EH, Swiontkowski M, Sanders D, Walter SD. Randomized trial of reamed and undreamed intramedullary nailing of tibial shaft fractures. J Bone Joint Surg Am. 2008 Dec;90(12):2567-78. PubMed PMID: 19047701.Finkemeier CG, Schmidt AH, Kyle RF, Templeman DC, Varecka TF. A prospective, randomized study of intramedullary nails inserted with and without reaming for the treatment of open and closed fractures of the tibial shaft. J Orthop Trauma. 2000 Mar-Apr;14(3):187-93. PubMed PMID: 10791670.
END OF SERIES


