physiological detection of emotional states in children
TRANSCRIPT

i
Physiological Detection of Emotional States in Children
with Autism Spectrum Disorder (ASD)
by
Sarah Sarabadani
A thesis submitted in conformity with the requirements
for the degree of Master of Applied Science
Department of Biomaterials and Biomedical Engineering
University of Toronto
© Copyright by Sarah Sarabadani 2016

i
Physiological Detection of Emotional States in Children with
Autism Spectrum Disorder (ASD)
Sarah Sarabadani
Master of Applied Science
Department of Biomaterials and Biomedical Engineering
University of Toronto
2016
Abstract
Autism spectrum disorder (ASD) is associated with difficulties in emotion processing including
attributing emotional states to others and processing of one’s own emotional experiences. These
difficulties are linked to core social impairments and increased severity of psychiatric co-
morbidities such as depression. The nature of these difficulties has remained largely unknown.
This is partially due to limitations in obtaining reliable self report of emotional experiences in
this population.
Emotion detection using physiological signals is a promising direction in addressing this
limitation. Physiological signals can provide a language free method for understanding emotional
states in ASD. The use of this approach has not been studied in ASD.
To this end we develop a physiological approach to detection of emotion in children with ASD.
We showed that emotional states can be classified with accuracies>80% in a sample of children
with ASD which affirms the feasibility of discriminating affective states in this population.
ii
iii
Acknowledgments
Foremost, I would like to express my sincere gratitude to my thesis advisor Dr. Azadeh Kushki
for her patience, motivation, enthusiasm, and immense knowledge. Her guidance helped me in
all the time of research and writing of this thesis. She always steered me in the right direction
whenever she thought I needed it.
Besides my advisor, I would like to thank the rest of my thesis committee: Dr. Jose Zariffa, Dr.
Evdokia Anagnostou, and Dr. Azadeh Yadollahi, for their encouragement and insightful
comments.
My sincere thank also goes to Ali Samadani who always was there to answer my endless
questions. I am gratefully indebted to his very valuable helps with this thesis.
I would like to thank members of Autism Research Centre (ARC), especially Stephanie Chow
who has always supported me and helped me putting pieces together.
Finally, I must express my very profound gratitude to my parents for providing me with unfailing
support and continuous encouragement throughout my years of study and through the process of
researching and writing this thesis. This accomplishment would not have been possible without
them. Thank you.

iv
Table of Contents
Abstract ........................................................................................................................................... ii
Acknowledgments.......................................................................................................................... iii
Table of Contents ........................................................................................................................... iv
List of Tables ................................................................................................................................. vi
List of Figures ............................................................................................................................... vii
Introduction ................................................................................................................................... 1
1.1 Motivation ........................................................................................................................ 1
1.2 Research Question and Objective .................................................................................... 2
Background ................................................................................................................................... 3
2.1 Brain Activity in Emotion Processing .............................................................................. 3
2.2 Emotion Recognition in ASD .......................................................................................... 4
2.3 Automatic Emotion Recognition ...................................................................................... 5
2.4 Emotional model .............................................................................................................. 6
2.4.1 Choice of the emotion model .................................................................................... 7
2.5 Emotion elicitation ........................................................................................................... 8
2.6 Physiological Signals for Emotion Classification ............................................................ 9
2.6.1 Electrocardiogram (ECG) ......................................................................................... 9
2.6.2 Skin Conductance (SC) ........................................................................................... 10
2.6.3 Respiration (RSP) ................................................................................................... 11
2.6.4 Skin temperature (SKT) .......................................................................................... 12
2.7 Existing Systems for Physiological Emotion Recognition ............................................ 12
2.7.1 Typically developing .............................................................................................. 12
2.7.2 ASD......................................................................................................................... 14
Research Methods ....................................................................................................................... 15
3.1 Participants ..................................................................................................................... 15
3.2 Instrumentation............................................................................................................... 16
3.3 Stimuli ............................................................................................................................ 17

v
3.4 Experimental protocol .................................................................................................... 20
Analysis ........................................................................................................................................ 22
4.1 Pre-processing ................................................................................................................ 23
4.2 Feature Extraction .......................................................................................................... 24
4.3 Feature selection ............................................................................................................. 26
4.4 Classification .................................................................................................................. 27
4.5 Performance Evaluation ................................................................................................. 28
Results .......................................................................................................................................... 29
5.1 Participants Demographics ............................................................................................. 29
5.2 SAM Results .................................................................................................................. 30
5.3 Classification Results ..................................................................................................... 35
5.4 Ensemble of Classifiers .................................................................................................. 37
5.5 Classification over arousal axis ...................................................................................... 41
5.6 Modality Specific Results .............................................................................................. 42
5.7 Selected Features ............................................................................................................ 43
5.9 Association of Classification Accuracy and SAM Ratings with Demographics ........... 49
5.10 Effect of Window Size on Accuracy .............................................................................. 52
Discussion and Conclusion ......................................................................................................... 54
6.1 SAM assessment ............................................................................................................ 54
6.2 Feature selection ............................................................................................................. 55
6.3 Classification Results ..................................................................................................... 56
6.4 Effect of demographic variables/behavioural measures on accuracy ............................ 57
Conclusion ................................................................................................................................... 59
References .................................................................................................................................... 61

vi
List of Tables
Table 2.1: Summary of studies on typical individuals .................................................................. 12
Table 3.1: Average rating of final selection of pictures ................................................................ 19
Table 4.1: summary of features, SC: Skin Conductance, ECG: Electrocardiogram .................... 25
Table 5.1: Demographic information ............................................................................................ 29
Table 5.2: Overall SAM results for each participant .................................................................... 30
Table 5.3: Emotion specific SAM results for each participant ..................................................... 30
Table 5.4: Emotion specific SAM results for each parent ............................................................ 31
Table 5.5: Confusion matrix for child SAM ratings ..................................................................... 32
Table 5.6: Confusion matrix for parent SAM ratings ................................................................... 33
Table 5.7: Top ten selected features ............................................................................................. 44
Table 5.8: Accuracy of comparing HP vs. HN for each classifier ................................................ 35
Table 5.9: Accuracy of comparing LP vs. LN .............................................................................. 36
Table 5.10: Classification results of ensemble of methods ........................................................... 37
Table 5.11: Comparing un-weighted and weighted ensemble of classifiers ................................ 38
Table 5.12: Classification results using shuffled labels ................................................................ 39
Table 5.13: Confusion matrices of ensemble of methods ............................................................. 40

vii
List of Figures
Figure 2.1: Discrete and dimensional model [29] ....................................................................... 7
Figure 2.2: SAM [30] .................................................................................................................. 8
Figure 2.3: Example of a QRS waveform in an ECG signal [54] ............................................. 10
Figure 2.4: SC signal [56] ......................................................................................................... 11
Figure 2.5: respiration sensor [61] ............................................................................................ 11
Figure 2.6: Skin temperature sensor [62] .................................................................................. 12
Figure 3.1: Attachment of sensors, Procomp Infiniti hardware manual [65] ............................ 16
Figure 3.2: experimental setup .................................................................................................. 17
Figure 3.3: Procedure of picture selection ................................................................................ 19
Figure 3.4: Experimental protocol ............................................................................................ 21
Figure 4.1: Analysis procedure ................................................................................................. 23
Figure 4.2: Segmentation of each task ...................................................................................... 24
Figure 5.1: Selected features, I will replace figures with larger and clear ones later ............... 44
Figure 5.2: Selected feature for each participant.(a) low arousal, (b) high arousal, (c)
subtracting a from b................................................................................................................... 48
Figure 5.3: Bar plot of results of ensemble of classifiers .......................................................... 41

1
Chapter 1
Introduction
1.1 Motivation
Autism spectrum disorder (ASD) is a neurodevelopmental disorder characterized by social
communication difficulties and the presence of repetitive and restricted behaviors and interests
[1]. ASD is also associated with difficulties in emotion processing, which may underlie some of
the core social impairments in this population [2]. A large body of literature has examined
emotion processing in ASD, suggesting difficulties in attributing mental and emotional states to
others [3, 4, 5]. A few studies have also reported self-awareness and atypical processing of self
emotional experiences in this population [6]. For example, one in two individuals with ASD is
suggested to be affected by alexithymia (difficulties in distinguishing and describing internal
body states) [7]. This is significantly higher than the one in ten prevalence of alexithymia in the
general population [8], [9]. In addition to being closely linked to the core social impairments in
ASD [10], difficulties in interpreting and processing emotions in ASD are known to be
associated with increased severity of psychiatric disorders such as depression [2]. Hence,
assisting individuals with ASD with perceiving and processing their internal body state is
essential.
Emotion detection using physiological signals is a promising direction in addressing this gap. In
this context, a physiological approach to detection of emotions can provide a language-free, non-
invasive, and low-cost way for characterization of emotional states in children with ASD. This
work can ultimately contribute to improving self-awareness of emotions by providing users with
information regarding their actual body state. In addition it will enhance our understanding of
ASD-related emotion processing difficulties.

2
Physiological signals reflect the activity of the Autonomic Nervous System (ANS) [19]. ANS is
responsible for involuntary control of organs and regulating processes such as heart rate and
respiration [20]. Emotional stimuli have been shown to influence the activity of the ANS in a
measureable way [21]. For example, heart rate and blood pressure tend to increase in response to
anger [22].
There is extensive body of literature on characterizing physiological signals to discern emotional
states in typically developed individuals [16, 31, 32, 34, 36]. However, it is unclear that these
methods can be used in this population as ASD is associated with atypical ANS function [45].
1.2 Research Question and Objective
This research aims to answer this question: Is it possible to physiologically differentiate affective
states in children with ASD?
The goal of this study is to develop tools for physiological detection of emotions in children with
ASD. The specific objective is to develop classification techniques to differentiate patterns of
physiological response to four emotional states (high arousal/positive valence, low
arousal/positive valence, high arousal/negative valence, and low arousal/negative valence).

3
Chapter 2
Background
In this chapter we review previous research in the field of emotion recognition. First the
influence of affective state on various physiological signals is discussed. Afterwards, emotion
processing in ASD is investigated from a neurophysiologic perspective. Then, various modalities
in automatic emotion recognition including facial expressions, voice, and physiological signals
are explained and the choice of latter one is justified. Finally, three principal matters in
developing automatic emotion recognition comprising emotional model, emotion elicitation
method, and specific physiological indices of ANS activity are discussed in the following three
sections.
2.1 Brain Activity in Emotion Processing
ANS is one of the divisions of peripheral nervous system (PNS) that controls the involuntary
function of organs. It consists of two branches; the sympathetic nervous system which is known
as “fight or flight” system, activated in fast changes and arousal while inhibits digestion. The
other branch of ANS named parasympathetic nervous system which is known as “rest and
digest” system. It is associated with calming and regular function of the nerves and promoting
digestion. The function of these two parts is opposite and as one of them enhances the
physiological response, the other inhibits it [60].
There are various positions on autonomic response organization in emotion. It has been shown
that valence specific patterns are more consistent with ANS activity than discrete emotion
patterns [61]. James [62] has defined emotion as feeling of the body changes as they occur. He
has argued that emotional states are associated with specific physiological response with

4
variations in symptoms between individuals. Stemmler [65] has stated that autonomic activity
occurs prior to any behavioral changes due to emotional states. This argument is supported by
studies on paralyzed animals where there is lack of external behavior while autonomic activation
has been detected [66]. It contradicts the notion of ANS activity as a result of motoric response
[67]. Stemmler also has suggested that for body protection and behavioral adaptation distinct
autonomic response is required to exist.
A large body of literature has examined the relation between affective states and patterns in
autonomic response. They could successfully show such patterns exist in various emotional
states. As one of the pioneers in this area, Ekman [23] has investigated emotion specific
activities in ANS. He has considered six emotions (surprise, disgust, sadness, anger, fear, and
happiness) and recorded signals of heart activity, skin temperature, skin resistance, and muscle
tension. The changes were observed not only between positive and negative emotions, but also in
various negative affective states. Picard [16] also could differentiate eight discrete emotions
(neutral, anger, hate, grief, platonic love, romantic love, joy, and reverence), looking at ANS
activity through four physiological signals (i.e. muscle tension, heart activity, skin conductance,
and respiration). In another study Kim J [39] has shown there is discernible pattern between
positive/high arousal, negative/high arousal, positive/low arousal, and negative/low arousal. He
has employed four physiological signals to measure heart activity, skin conductance, respiration
rate, and muscle tension. Kim K.H [44] has also indicated pattern between sadness, anger, stress,
and surprise using signals representing heart activity, skin conductance, and temperature. These
major findings along with tons of similar works suggest that detecting pattern in physiological
signals in various emotional states is feasible.
2.2 Emotion Recognition in ASD
ASD is associated with difficulties in identify and describing one's own emotions (alexithymia
[6]). These atypicalities are suggested to be closely linked to the capacity to empathize, a key
area of difficulty in ASD.

5
Lambie and Marcel [11] conceptualized the emotion experience using a two-level model. In this
model, first-order experience of emotion is attributed to neurophysiological arousal associated
with emotional states. Self-awareness of this arousal is second-order experience of emotion
(interoception). In ASD, atypicalies have been reported both levels of emotional experience.
While emotion-related physiological arousal is suggested to be present in ASD [12], its pattern
may be atypical [13]. Interestingly, in a study by Silani et al. [6] reduced emotional awareness
was not found to be associated with reduced response in the brain regions mapped to first order
experience (amygdala and inferior orbitofrontal cortex), suggesting that this circuitry may not
underlie alexithymia symptoms in ASD [6]. Several studies have also reported that the second-
order emotional experience (i.e., aware of bodily states) is atypical in ASD [9, 12, 14, 15]. For
example, in a functional MRI study of individuals with ASD, Silani et al. [6] found a significant
negative correlation between the severity of alexithymia tendencies and activity in brain regions
associated with interoception (e.g., the insula). The authors then concluded that the lack of
awareness of bodily states, or the decoupling between physiological arousal and conscious
representation of emotions, may underlie alexithymia tendencies in ASD.
2.3 Automatic Emotion Recognition
Inferring emotional states automatically by means of computer algorithms has been studied
extensively, mainly in the context of enhancing human-computer interaction [16]. These
algorithms employ changes in internal or external states of users for emotion recognition. The
states commonly considered include facial expressions, voice, and physiological signals.
Emotion detection based on facial expressions has been mainly used for enhancing human-
computer interaction as this approach requires the user to be directly in the field of view of a
camera [17]. ASD has been associated with atypical facial expressions, which may affect the
accuracy of these methods.
Emotion detection based on voice also presents several challenges in the context of this proposal.
First, such a method requires the continuous presence of verbal expression, which may not be
possible for some individuals with ASD. Second, ASD is associated with atypical speech

6
features such as prosody [18], which may affect the recognition accuracy of these methods.
Finally, voice-based emotion detection will not be appropriate for settings, such as classrooms,
where noise is present in the environment or users do not continuously produce speech.
Emotion detection based on physiological signals is especially appropriate for use in this project
for three reasons: 1) this measurement modality can be employed across different environments
and especially in naturalistic settings; 2) physiological signals are relatively independent of
individuals ability profiles and cultural norms; 3) these signals can be measured non-invasively
and with low-cost with relatively low burden on the user. For these reasons, the physiological
approach to emotion detection is chosen for the proposed project. Three key issues need to be
considered in developing automatic emotion recognition namely, choosing the emotional model,
emotion elicitation method, and specific physiological indices of ANS activity. Details are
provided in sections that follow.
2.4 Emotional model
Two approaches are commonly used for quantitative modeling of emotions. The first, proposed
by Ekman [23], assumes the existence of a discrete set of emotions. Building on this assumption,
six classes of emotions (happiness, sadness, surprise, anger, disgust, and fear [24] have been
commonly used in the literature.
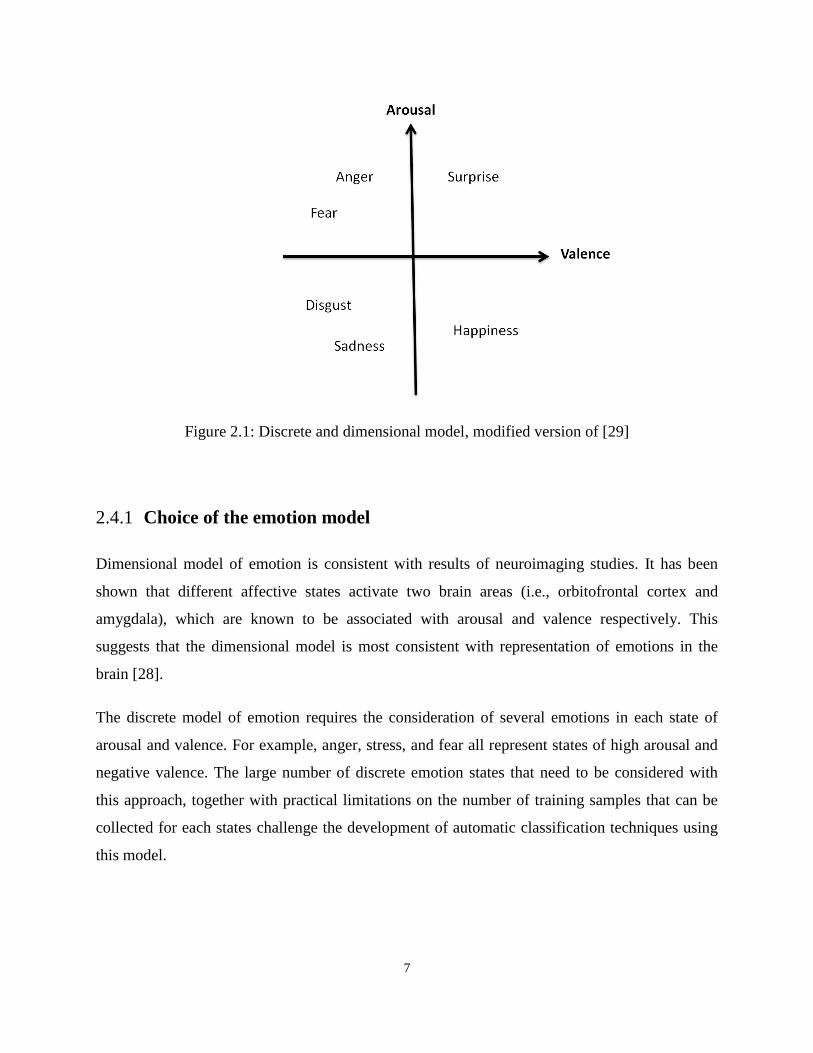
The second model of emotion challenges the discrete nature of emotion and proposes a
continuous space in two dimensions of arousal and valence [25]. Valence represents the
pleasantness of an emotion and ranges from negative to positive. Arousal reflects intensity of an
emotion and ranges from low to high. For example, happiness has positive valence and high
arousal, while sadness has negative valence and low arousal. Six core emotions are shown in the
valence-arousal coordinates in Figure 2.1.
7
Figure 2.1: Discrete and dimensional model, modified version of [29]
2.4.1 Choice of the emotion model
Dimensional model of emotion is consistent with results of neuroimaging studies. It has been
shown that different affective states activate two brain areas (i.e., orbitofrontal cortex and
amygdala), which are known to be associated with arousal and valence respectively. This
suggests that the dimensional model is most consistent with representation of emotions in the
brain [28].
The discrete model of emotion requires the consideration of several emotions in each state of
arousal and valence. For example, anger, stress, and fear all represent states of high arousal and
negative valence. The large number of discrete emotion states that need to be considered with
this approach, together with practical limitations on the number of training samples that can be
collected for each states challenge the development of automatic classification techniques using
this model.

8
2.5 Emotion elicitation
The most commonly stimuli in emotion detection studies in typically developing population is
using International Affective Picture System (IAPS) [31, 32, 33, 34] which is a large set of color
pictures validated to be effective for inducing different levels of arousal and valence [30]. It also
has been used in ASD [12]. For rating the pictures a visual scale, called the self assessment
manikin (SAM), has been suggested by the publishers of IAPS (Figure 2.2). The first and second
rows of SAM correspond to level of valence and arousal which were previously defined. The
third row represents dominance of emotion denoting the level of control vs. the level of being
controlled. For instance, fear and anger both are negative emotions. Regarding dominance
dimension the former is more submissive while the latter is more dominant. Geneva affective
picture database (GAPED) is a relatively new system consisting of 730 pictures similar to IAPS,
in three main categories: positive, neutral, and negative.
Figure 2.2: SAM [30]

9
The majority of the studies in ASD have focused on inducing anxiety. Kushki [45] used the
Stroop color-word interference task and public speaking to elicit anxiety and high arousal. Stroop
is a computer task in which names of colors are printed on the screen in different colors and the
participants are asked to name the color while ignoring the word. Kootz and cohen [46] used
tasks associated with social communication for inducing anxiety. Jansen [47] also used public
speaking for this purpose. Groden and Goodwin [48] chose various tasks from the stress survey
schedule [49].
Liu used computer games to elicit three discrete emotions (i.e. liking, anxiety, and engagement)
[17]. The first task was a computer game named Pong which had been previously utilized to
induce anxiety [50]. In this game the player controls a paddle to strike a free moving ball.
Different affective states were elicited by changing the level of difficulty. The second task was
Anagram. In this task the participant names the correct word that is given with disordered letters.
This game was previously suggested by Pecchinenda and Smith [51] to investigate the relation
between physiology and anxiety.
2.6 Physiological Signals for Emotion Classification
Several channels of physiological signals can be used to quantify the function of the ANS. Four
selected signals in this study are reviewed in the sections that follow. This choice was made in
consideration for participant comfort and ease of sensor attachment.
2.6.1 Electrocardiogram (ECG)
ECG measures the contractile activity of the heart by capturing the action potential related to
heart contraction. Depolarization of the heart ventricles produces the waveform known as QRS
complex [54] (Figure 2.3). Inter beat interval (IBI) is the time interval between two ‘‘R’’ peaks
in the waveform and generally ranges between 300 ms to 1500 ms [17]. Heart rate (HR) is the
number of heart beats per minute (bpm) and is approximately 70-80 bpm at rest. The variation in

10
time interval between two consecutive heart beats is called heart rate variability (HRV) [55].
Mean and standard deviation are two features in time domain that can be extracted from the IBI
series.
Figure 2.3: Example of a QRS waveform in an ECG signal [54]
2.6.2 Skin Conductance (SC)
SC measures the skin's ability to conduct electricity. The change in skin conductivity is
associated with the activity of eccrine sweat glands, which receive input from the sympathetic
nervous system [52]. The SC signal has two components: 1) a slow moving component which
reflects the general activity of sweat glands and shows the ongoing level of skin conductance,
and 2) faster changes influenced by environmental events and appears with an instantaneous
increase in the signal. For instance, anxiogenic stimuli are shown to cause a sudden rise in the
signal [39]. An example of an SC signal is shown in Figure 2.4 [56].

11
Figure 2.4: SC signal [56]
2.6.3 Respiration (RSP)
In general, emotional excitement and physical activity are associated with faster and deeper
breathing, while relaxation and calmness lead to slower and shallower respiration [56].
Respiration sensor is used for measuring depth and rate of breathing (Figure 2.5) [43].
Respiration signal is analyzed in the time domain to extract descriptive statistics or in the
frequency domain by performing power spectral analysis.
Figure 2.5: respiration sensor [61]

12
2.6.4 Skin temperature (SKT)
Variations in skin temperature are mainly associated with changes in cutaneous blood flow.
Blood flow is determined by vascular resistance which is caused by contraction and relaxation of
smooth muscles [57, 58] Mean, slope, and standard deviation of temperature are three key
features of SKT sensor [17] (Figure 2.6).
Figure 2.6: Skin temperature sensor [62]
2.7 Existing Systems for Physiological Emotion Recognition
2.7.1 Typically developing
Based on a review work by Jerritta et al. [29], different physiological based emotion recognition
studies are summarized in Table 2.1.
Table 2.1: Summary of studies on typical individuals, EMG: Electromyogram, ECG:
Electrocardiogram, Temp: Temperature, Resp: Respiration, SC: Skin Conductance, BVP: Blood
Volume Pulse
emotions # of
participants
Induction
method signals
Feature
selection
and
reduction
Classification
method Accuracy (%)
44 Sad, anger, 125 Multimodal ECG used all the Support 78.4 (3 emotions)

13
stress,
surprise
Temp
SC
features Vector
Machine
61.8 (4 emotions)
39 Joy, Anger,
Sad, Pleasure 3 Music
EMG
ECG
SC
Resp
sequential
forward
selection
(SFS)
sequential
backward
selection
(SBS)
Linear
Discriminant
Analysis
95 (personal)
70 (group)
71 Valance,
Arousal 36
Robot
Actions
SC
ECG
used all the
features
Hidden
Markov
Model
83 Arousal ,80
Valance (personal )
66 Arousal , 66
Valance (group)
16
Neutral,
Anger, Hate,
Grief,
Platonic love
Romantic
love, Joy,
Reverence
1 Personalized
Imagery
EMG
BVP
SC
Resp
Fisher
projection
Hybrid Linear
Discriminant
Analysis
81(personal)
31 Happiness,
Disgust, Fear 9
IAPS
pictures
EMG
ECG
SC
Resp
Simba
algorithm
Principal
Component
Analysis
K Nearest
Neighbor
Random
Forest
62.70 (group)
62.41(group)
32 Valance,
Arousal
IAPS
pictures
EMG
ECG
SC
Temp
BVP
Resp
used all the
features
Neural
Network
Classifier
Valance 89.7
(personal)
Arousal 63.76
(personal)
36
Sad, Anger,
Surprise,
Fear,
Frustration,
Amusement
14 Movies SC
ECG
used all the
features
K NN
DFA
Marquardt
Back
Propagation
71(personal):KNN
74(personal):DFA
83(personal):MBP
72 Joy, Anger,
Sad, Pleasure 1 Music
ECG
EMG
SC
Resp
used all the
features
Support
Vector
Machine
76 (Fission
,personal)
and 62 (Fusion,
personal)

14
41 Joy, Anger,
Sad, Pleasure 1 Music EMG
used all the
features
Neural
Network 82.29 (personal)
73 Joy, Anger,
Sad, Pleasure 1 Music
ECG
EMG
SC
Resp
used all the
features
Linear
Discriminant
Analysis
83.4 (personal)
33
Amusement,
Contentment,
Disgust,
Fear, Sad,
Neutral
10 IAPS
pictures
BVP
EMG
Temp
SC
Resp
used all the
features
Support
Vector
Machine,
Fisher Linear
Discriminant
Analysis
90(personal) and
92(personal)
34
Anger,
Interest,
Contempt,
Disgust,
Distress,
Fear, Joy,
Shame,
Surprise
28 IAPS
pictures
ECG
BVP
SC
EMG
Resp
Sequential
Floating
Forward
Selection
(SFFS),
Fischer
Projection
K Nearest
Neighbour ,
50(group)
90.7(personal)
2.7.2 ASD
Only a few studies have examined physiological emotion detection in ASD. The works of
Groden [48] and Ben Shalom [12] investigated trends in physiological signals in response to
emotional stimuli, but no automatic classification techniques were proposed. In particular,
Groden considered stress and used ECG to examine the trend of heart rate in four different
situations that were designed to elicit stress [49]. Shalom investigated physiological responses to
pleasant, unpleasant, and neutral stimuli in children with ASD using the IAPS pictures. He used
skin conductance and performed analysis of variance (ANOVA) to analyze the signals.
Liu [17] showed that three emotional states (anxiety, engagement, and liking) can be classified in
children with ASD using a wide range of physiological signals (i.e. ECG, EDA, EMG, BVP,
temperature, bioimpedance, and heart sound). He obtained accuracies 85.0% for liking, 79.5%
for anxiety, and 84.3%. Kushki [13] used heart rate to detect arousal related to anxiety in ASD,

15
obtaining an accuracy of 95%. To our knowledge none of the studies considered both arousal and
valence axes. They considered emotions either discretely or only in arousal axis.
Chapter 3
Research Methods
In this chapter we discuss the experimental setup for collecting the data used to develop and test
the algorithms in this thesis. Specifically, recruitment criteria, stimuli selection, instrumentation,
and the experimental protocol are discussed.
3.1 Participants
Fifteen participants with ASD were recruited for this study. Participants had a clinical diagnosis
of ASD using DSM-IV criteria supported by the Autism Diagnostic Observation Schedule [64],
and the Autism Diagnostic Interview - revised (ADI-R). Also they completed the Weschler
Abbreviated Scale of Intelligence, the Social Communication Questionnaire, and the Child
Behaviour Checklist (CBCL) to characterize intelligence, ASD symptomatology, and related
comorbidities. All these measures were provided by Province of Ontario Neurodevelopmental
Disorders (POND). The inclusion criteria for participants were age between 12 and 18 years,
full-scale IQ scores above 70, and no sensory impairments such as deafness or blindness.
Participants’ parents/caregivers also participated in the study. The inclusion criterion for parents
was being able to understand instructions and respond to questions in English.
The Bloorview Research Institute and University of Toronto research ethics boards approved the
study.

16
3.2 Instrumentation
Physiological signals were measured using Procomp Infiniti (Thought Technology Ltd). The
specific sensors used included ECG, SC, respiration, and skin temperature. Heart activity was
measured by a three lead ECG attached to the body using pre-gelled electrodes. Respiration
signal was recorded by a belt sensor using a latex rubber band which wrapped around abdomen.
SC was measured using a pair of 10 mm diameter dry Ag-AgCl electrodes secured to the palmar
surface of the proximal phalanges of the second and third digits of the non-dominant hand. Skin
temperature was measured using a thermistor fastened to the palmar surface of the distal phalanx
of the fourth digit of the hand. ECG sensor captured signals at the rate of 2048 Hz and all the
other sensors at the rate of 256 Hz. The attachment of the sensors to the body is shown in Figure
3.1.
Figure 3.1: Attachment of sensors, Procomp Infiniti hardware manual [65]
Three connected computers were used in the experiment room; one in front of participant for
viewing and rating the stimuli, the other for the parent for rating the child’s emotional reactions
to the stimuli, and the third one to control the data collection procedures. The position of

17
computers was such that the parent could see the child thoroughly. The signals were recorded on
the experimenter computer. The experimental setup is shown in Figure 3.2.
Figure 3.2: experimental setup
3.3 Stimuli
We selected visual stimuli to elicit four combinations of arousal and valence: high
arousal/positive valence, low arousal/positive valence, high arousal/negative valence, and low
arousal/negative valence. The stimuli were selected from IAPS and GAPED picture systems
which include 956 and 730 pictures respectively.
The pictures are from a variety of topics and not culturally specific. The database provided
ratings for each picture in three dimensions of arousal, valence, and dominance. For IAPS, a
number in 9-point scale was attributed to each picture (1: lowest arousal/pleasure/dominance, 9
the highest arousal/pleasure/dominance). These are normative ratings obtain from a sample of
approximately 100 adults. For GAPED a group of 60 adults participated in a study to evaluate
pictures in terms of arousal and valence. Each picture is rated in arousal and valence scales with
a number between 0 and 100; (100 is the highest arousal, most positive) [66].

18
IAPS has been used in several studies on ASD. Shalom used IAPS to elicit different levels of
valence in high functioning children with ASD [12]. Silani [6] used IAPS to study neural
correlates of emotion recognition in ASD. Bolte [52] also employed IAPS and the adapted SAM
to investigate physiological responses to emotional stimuli in ASD. GAPED has also been used
in studies on typical individuals [84, 85]; however, it has not been employed in studies on ASD
yet.
Collectively, the two databases contain over 1386 pictures. A subset of 214 pictures from these
databases was selected excluding pictures of faces, erotic photos, and those depicting brutality
and mutilation themes, which were considered inappropriate for the age range of the study. This
selection was then refined by consulting with clinicians. During the clinician refinement process,
60 pictures (15 in each theme) were not rated with confidence. To assess the suitability of this
subset, an online survey was designed and completed by 13 parents of children with ASD.
Parents provided their rating as well as comments for every picture determining whether the
picture elicits positive or negative emotion and whether it is weak or strong. Parents choices
combined with preliminary selection altogether constituted the final set of 24 pictures in each
class (96 pictures in total).The stimuli selection procedure is represented in Figure 3.3.

19
Figure 3.3: Procedure of picture selection
Table 3.1: Average rating of final selection of pictures
Valence Arousal
HP 6.91±0.44 5.38±0.98
HN 3.67±0.53 5.98±0.67
LP 8.1±0.45 2.16±1.38
LN 3.41±1.2 5.11±0.98
Figure 3.4 shows the average ratings of pictures selected for each class on valence axis. The right
and left ends correspond to most positive and most negative valence. The negative intended
stimuli are closer to the center which denotes neutral valence compared to positive pictures.
Figure 3.4: Location of average ratings of the stimuli for each class on valence axis
Final set of 96 pictures (24 in each class)
Parents of children with ASD provided rating for 60 pictures with concern of appropriateness through online
survey
Refining selection after consulting with clinicians
preliminary selection of 214 pictures
1386 pictures from IAPS and GAPED

20
3.4 Experimental protocol
For all participants written consent was obtained from parents and children who had the capacity
for consent. In cases the child did not have the capacity to consent, he/she signed the assent and
the parent consented on behalf of child.
At the beginning of the experimental session, sensors were attached to the participant and the
task was explained to both the parent and child. Participants were asked to practice the task to
ensure understanding of the protocol. Participants were told to request breaks as needed.
The protocol began and ended with a 15-minute baseline involving movie watching to allow for
acclimation to the lab environment. Participants then viewed two blocks emotional pictures, each
separated by a five minute baseline. Each block consisted of eight, 2-minute stimuli presentation
blocks, which were presented in random sequence. Pictures in each block elicited one of the four
affective states considered herein (2 blocks/emotion type). This resulted in four minutes of
physiological data per affective state. After completing each block, both child and parent
completed the SAM to assess the child’s affective state during stimulus viewing. The overview
of experimental protocol is shown in Figure 3.5.

21
Figure 3.5: Experimental protocol

22
Chapter 4
Analysis
In this chapter, we describe the methods and algorithms used for data analysis. The analysis
pipeline is shown in Figure 4.1. First, raw data from each sensor was preprocessed to remove
noise and extract baseline and stimuli segments. Next, data segments were used to extract
features for classification. Given the short duration of data for each stimulus block, we focused
on extracting temporal features and did not use frequency-based features. Best features for each
classification problem and participant were selected using an automatic feature selection
algorithm. Classification was performed per participant using two linear and five nonlinear
classifiers. To improve accuracy, classification results from multiple classifiers were combined
to provide final classification decisions.

23
Figure 4.1: Analysis procedure
4.1 Pre-processing
ECG: the signal was captured at the rate of 2048 Hz. All the other signals were recorded with
the sampling frequency of 256 Hz. The algorithm described in Pan and Tompkins [69] and
implemented in Matlab by BioSig software [86] was used to extract the inter-beat-interval series
from the ECG signal. In order to attenuate noise due to physical movement, power line noise,
and baseline wander band pass filter was applied with low and high cut off frequencies of 5 Hz
and 15 Hz. The identified peaks were visually reviewed for one task randomly for each
participant to examine the authenticity of detection algorithm. After performing QRS peak
detection algorithm, a median filter with order 9 (considering 9 points at a time) was applied on
the recognized QRS complexes. Heart rate was obtained as the inverse of RR intervals.
• Pre-processing
• Segmentation and baseline subtraction
• Feature extraction
• Feature selection
• Classification
Physiologica
l measures
Predicted
Labels

24
Respiration: The signal was band passed filtered with low and high cut off frequencies of 0.1
Hz and 0.5 Hz as the shortest average breathing interval in adults is 3 seconds [81]. Peaks of
signal were identified semi automatically by the criterion of being located at least 1 second apart
to accommodate fast breathing due to arousal. The validity of detected intervals less than 3
seconds was visually confirmed.
Skin conductance: The signal was detrended over the entire session to minimize the effects of
thermoregulation and changes in sensor adhesion resulting from perspiration. The signal was
then low-pass filtered using a 10th order Butterworth filter with cut-off frequency of 1 Hz. The
criteria for considering a peak as SC response were rise time of 1-3 seconds, amplitude between
0.1 and 1 µs, and minimum height of 0.05 µs. To analyze SC signal the Matlab implementation
of Ledalab software [87] was used.
Temperature: The signal was detrended and low pass filtered with cut off frequency of 0.1 Hz.
4.2 Feature Extraction
Analyses were performed offline using Matlab version 2016a. Since in classification the test data
should be completely unseen by the training data, before extracting features the entire data is
segmented into two parts regarded as train and test. Then, inside each set, various sub-windows
are defined (Figure 4.2). Each window was used to generate one training point.
Figure 4.2: Segmentation of each task
To mitigate carry-over effect, the average of last two minutes of signal in previous baseline is
subtracted from each task.

25
ECG: Since the duration of data recording was short, extraction of frequency-domain features
was deemed unfeasible and only features in time domain were acquired. These included
statistical temporal features, namely, mean, maximum, minimum, standard deviation, slope, and
median of top and bottom quartiles of signal were derived from heart rate and RR intervals.
Respiration: Analogous to ECG, the same statistical features from respiration rate and
respiration interval were obtained.
Skin Conductance: Number of SC responses, mean, and slope were extracted from SC signal.
Temperature: Statistical features including mean, standard deviation, minimum, maximum, and
slope of the signal were obtained.
Table 4.1 summarizes features of each sensor.
Table 4.1: summary of features, SC: Skin Conductance, ECG: Electrocardiogram
Number Feature Number Feature
1 Mean RR interval 17 Median of top quartiles of respiration
intervals
2 Minimum RR interval 18 Median of bottom quartiles of respiration
intervals
3 Maximum RR interval 19 Mean respiration rate
4 Standard deviation of RR intervals 20 Minimum respiration rate
5 Median of top quartiles of RR
intervals 21 Maximum respiration rate
6 Median of bottom quartiles of RR
intervals 22 Median of top quartiles of respiration rate
7 Mean heart rate 23 Median of bottom quartiles of respiration
rate
8 Minimum heart rate 24 Slope of respiration signal
9 Maximum heart rate 25 Mean temperature
10 Standard deviation of heart rates 26 Standard deviation of temperatures
11 Median of top quartiles of heart rates 27 Minimum temperature

26
12 Median of bottom quartiles of heart
rates 28 Maximum temperature
13 Slope of ECG signal 29 Slope of temperature signal
14 Mean respiration interval 30 Mean SC
15 Minimum respiration interval 31 Slope of SC signal
16 Maximum respiration interval 32 Number of SC responses
4.3 Feature selection
Given that the number of features is larger than training sample size, using all features in
classification may lead to overfitting and curse of dimensionality which will give rise to
reduction in prediction power of the classifier. Therefore, the most useful features should be
determined. To this end, sequential forward selection and backward elimination, a methods
commonly used in previous works was used. Forward selection algorithm starts with an empty
set and in each run adds subsets of features not yet selected that best predict the labels until there
is no improvement in prediction. Backward elimination, on the other hand, starts with a full set
of features (here with the features already selected by forward algorithm) and sequentially
removes features until eliminating more features does not boost the prediction.
At each run of cross-validation the subset of features is divided to test and train sections. The
latter one is used to train a model (here linear discriminant), and then label values for test data
are calculated using that model. In the cross-validation calculation for a given candidate feature
set, the number of misclassified observations was considered as loss measure to evaluate each
subset.
The output of this stage which was the input for classification problem was a matrix whose rows
corresponded to data points obtained in each subwindow, and the columns corresponded to
selected features.

27
4.4 Classification
In this thesis, we addressed two classification problems: 1) differentiating between high
arousal/negative valence and high arousal/positive valence, and 2) differentiating between low
arousal/negative valence and low arousal/positive valence.
We tested three classes of classification techniques, namely, K-Nearest Neighbour (KNN), linear
discriminant analysis (LDA), and support vector machines (linear and kernel). These classifiers
were chosen as representatives of linear and nonlinear algorithms which have been previously
used in automatic classification of emotions. To further improve classification accuracy, we
combined the output of the individual classifiers. This model allows for a consensus-based
decision making process and has been shown to improve accuracy in various classification
problems [78, 79, 80]. While different methods are available for classifier combination, we have
selected the weighted majority vote scheme for this application. In this case, the final
classification decision for nth
data point xn, with yi as predicted label for i
th classifier is defined
as:
Where the weight of each classifier decision wi is derived based on its training error e
i [78]:
denotes training error of the i
th classifier defined as:
Where Nincorrect and Ntest show the number of misclassified test points and the total number of test
points respectively.

28
4.5 Performance Evaluation
Our primary outcome measure was classification accuracy defined as:
Where Ncorrect indicates the number of correctly classified test points.
Classification performance was evaluated through cross-validation by randomly segmenting the
data into train and test sets for 100 times, training the classifier on the training set and averaging
over acquired accuracies on the test set.
Accuracy of different classifiers was compared using the rank-sum test, with the null hypothesis
that the classifiers perform similarly.
29
Chapter 5
Results
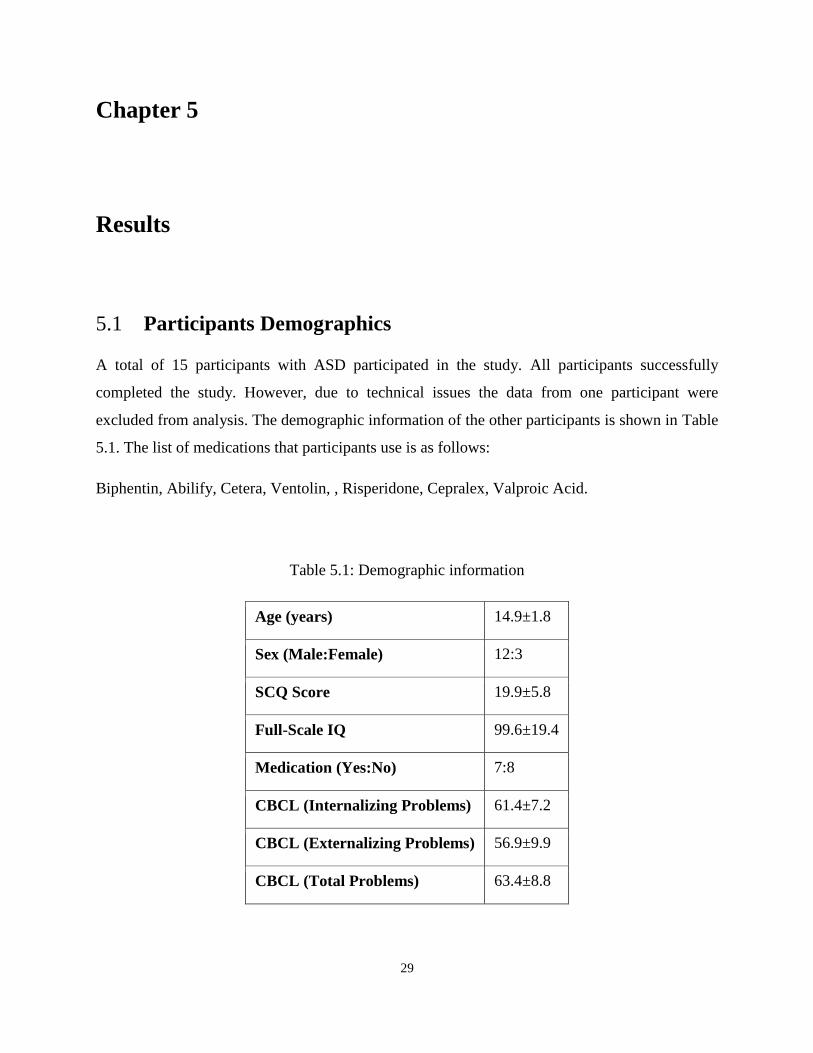
5.1 Participants Demographics
A total of 15 participants with ASD participated in the study. All participants successfully
completed the study. However, due to technical issues the data from one participant were
excluded from analysis. The demographic information of the other participants is shown in Table
5.1. The list of medications that participants use is as follows:
Biphentin, Abilify, Cetera, Ventolin, , Risperidone, Cepralex, Valproic Acid.
Table 5.1: Demographic information
Age (years) 14.9±1.8
Sex (Male:Female) 12:3
SCQ Score 19.9±5.8
Full-Scale IQ 99.6±19.4
Medication (Yes:No) 7:8
CBCL (Internalizing Problems) 61.4±7.2
CBCL (Externalizing Problems) 56.9±9.9
CBCL (Total Problems) 63.4±8.8

30
5.2 SAM Results
The results of child and parent assessments are summarized in Tables 5.2, 5.3, and 5.4. These
results were obtained after dichotomizing the valence into positive and negative as well as the
arousal into high and low. As seen in general there is poor agreement between ratings. The only
exception is agreement between child’s ratings and actual label for positive stimuli.
Table 5.2: Overall SAM results for each participant
Agreement (%)
Participant Child & Actual Parent & Actual Child & Parent
1 25 25 0
2 37.5 0 37.5
3 25 37.5 25
4 37.5 12.5 37.5
5 25 37.5 12.5
6 50 25 12.5
7 37.5 0 0
8 0 25 0
9 0 12.5 25
10 25 25 12.5
11 25 25 0
12 25 25 37.5
13 12.5 12.5 12.5
14 25 25 0
Mean 25±13.9 20.5±11.6 15.2±14.9
Table 5.3: Emotion specific SAM results for each participant

31
Agreement between child & actual labels (%)
participant Low High Positive Negative
1 100 0 100 0
2 0 100 100 75
3 50 25 75 75
4 25 50 75 100
5 0 75 100 25
6 75 100 75 50
7 25 100 100 25
8 25 0 50 25
9 25 0 100 0
10 50 25 75 100
11 25 75 100 25
12 75 0 75 50
13 100 0 0 50
14 75 0 100 25
Mean 46.4±33.8 39.3±42.4 80.4±28.0 44.6±32.8
Table 5.4: Emotion specific SAM results for each parent
Agreement between parent and actual labels (%)
Participant Low High Positive Negative
1 25 75 50 25
2 0 25 75 50
3 25 100 50 75
4 25 0 50 50
5 100 50 100 0
6 50 25 100 50

32
7 0 25 0 0
8 75 0 25 50
9 25 25 50 75
10 25 75 50 75
11 50 25 25 25
12 75 75 25 50
13 100 0 50 25
14 75 50 25 50
Mean 46.4±33.8 39.3±32.1 48.2±28.5 42.9±24.9
Tables 5.5 and 5.6 demonstrate confusion matrix for children and parents assessing high and low
arousal as well as positive and negative valence. Errors were due to negative stimuli being rated
as positive and positive ones being assessed as negative. As it can be seen, for both parent and
child the number of mislabeled pictures for high stimuli is slightly more than low stimuli.
Regarding valence, for parent the error is comparable between two cases; however, children
assessed positive pictures more correctly than negative ones.
Table 5.5: Confusion matrix for child SAM ratings
Child choice
n=112 High Low Neutral
Actual
labels
High 22 25 9
Low 18 26 12
Child choice
n=112 Positive Negative Neutral
Actual
labels
Positive 45 2 9
Negative 18 25 13

33
Table 5.6: Confusion matrix for parent SAM ratings
Parent choice
n=112 High Low Neutral
Actual
labels
High 22 25 9
Low 15 27 14
Parent choice
n=112 Positive Negative Neutral
Actual
labels
Positive 27 17 12
Negative 19 24 13
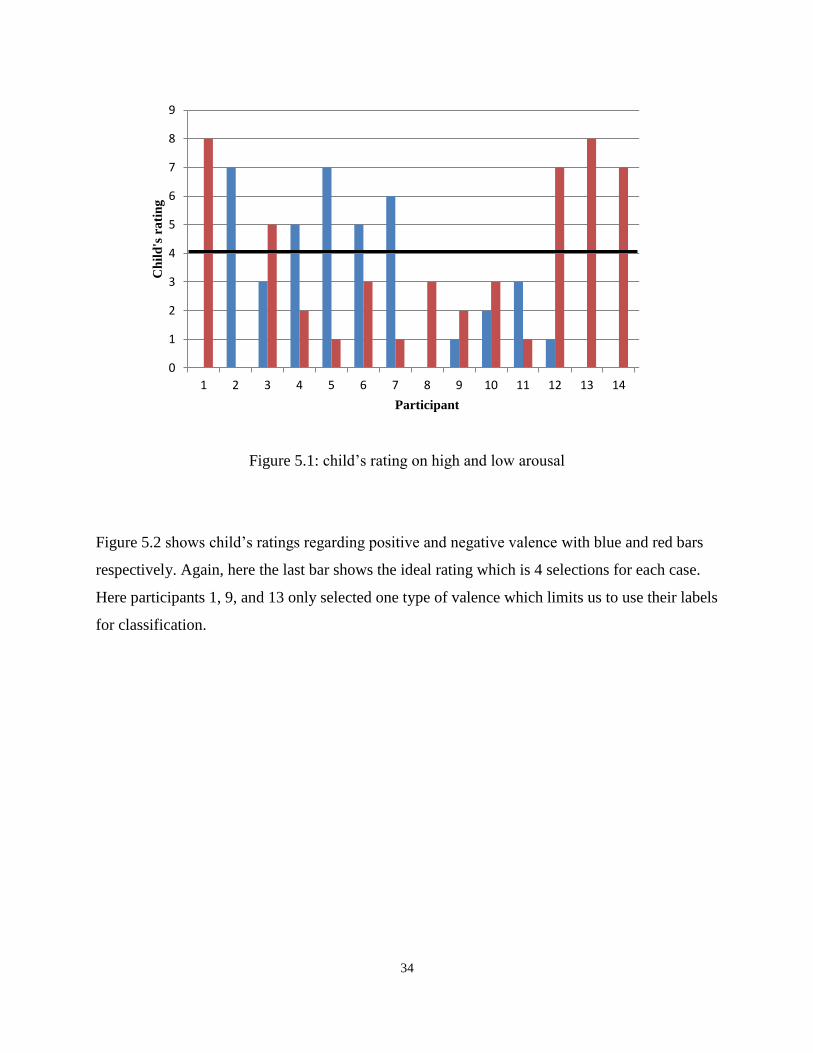
Figure 5.1 shows child’s ratings on high and low arousal. The blue and red bars denote high and
low arousal respectively. The horizontal black bar indicates the desirable case in which both
arousal and valence are selected equally 4 times as it was intended. It can be found that for none
of the participants ratings are balanced. In 5 cases (participants 1, 2, 8, 13, and 14) we only have
one bar instead of two which means that the child only has selected one type of arousal (i.e.
either high or low). This restricts us from using their labels for classification as two different
labels are required for two classes.
34
Figure 5.1: child’s rating on high and low arousal
Figure 5.2 shows child’s ratings regarding positive and negative valence with blue and red bars
respectively. Again, here the last bar shows the ideal rating which is 4 selections for each case.
Here participants 1, 9, and 13 only selected one type of valence which limits us to use their labels
for classification.
0
1
2
3
4
5
6
7
8
9
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Ch
ild
's r
ati
ng
Participant

35
Figure 5.2: child’s rating on positive and negative valence
5.3 Classification Results
Tables 5.7 and 5.8 represent classification accuracy for each classifier in comparison of high
arousal/positive valence vs. high arousal/negative valence, and low arousal/positive valence vs.
low arousal/negative valence respectively. The results are not significantly different for various
classifiers as examined by rank sum test.
Table 5.7: Accuracy of comparing HP vs. HN for each classifier
High/positive vs. high/negative (%)
Participant KNN3 KNN5 KNN7 LDA SVML SVM poly SVM rbf
1 74.2 74.2 73.3 77.3 74.4 75 74.4
2 55.8 54.4 55.6 58.8 54.8 60.4 59.2
3 59.4 53.1 55 62.3 61.5 63.1 53.3
4 90.6 91 90.6 88.3 89.6 91.7 91
0
1
2
3
4
5
6
7
8
9
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Ch
ild
's r
ati
ng
Participants

36
5 71 69.2 66.7 61.7 63.1 64 69
6 49 47.7 47.9 49.4 45.6 48.1 50.2
7 76.7 75.2 74 80 68.1 77.7 77.7
8 85.4 87.5 86.9 89.2 84 87.3 87.7
9 71.3 70.4 70.6 66.3 57.5 66.5 69.8
10 63.3 63.3 62.3 69.6 53.5 63.8 62.3
11 75.2 75 74.4 78.1 76.3 80.6 80.8
12 74.8 73.5 73.1 71.9 72.1 73.5 71.9
13 68.3 69.4 68.8 71.7 68.3 71.7 70.2
14 73.5 74.8 75.4 71.5 70.8 74 72.5
Mean 70.6±11.0 69.9±12.2 69.6±11.7 71.1±11.1 67.1±12.1 71.2±11.4 70.7±11.8
Table 5.8: Accuracy of comparing LP vs. LN
Low/positive vs. low/negative (%)
Participant KNN3 KNN5 KNN7 LDA SVML SVM poly SVM rbf
1 75.8 74.6 74.0 87.5 66.7 74.8 76.3
2 84.8 85.2 84.4 85.4 86.0 85.4 85.4
3 90.4 89.8 88.3 90.8 90.8 92.5 90.6
4 74.0 73.8 72.9 77.5 74.2 81.0 76.7
5 80.2 80.0 80.4 76.9 77.5 81.3 80.8
6 49.6 55.2 52.9 61.5 61.7 63.1 43.8
7 90.8 89.8 88.8 83.3 81.3 82.9 92.3
8 85.4 85.2 86.9 88.5 86.7 86.5 85.6
9 74.4 74.6 76.9 78.3 77.5 76.9 74.0
10 68.5 69.2 65.4 70.6 67.1 70.4 72.5
11 58.5 59.2 57.9 60.8 57.3 57.7 56.5
12 95.6 95.2 97.5 96.5 95.8 96.3 97.3
13 89.0 89.0 87.3 93.1 89.4 94.4 88.8
14 65.0 64.0 62.3 67.1 66.5 67.5 67.3

37
Mean 77.3±13.4 77.5±12.4 76.8±13.2 79.9±11.5 77.0±11.9 79.3±11.7 77.7±14.6
5.4 Ensemble of Classifiers
To improve outcome the classification outputs were combined using weighted majority vote as
described earlier. Table 5.9 summarizes the classification results of ensemble of methods for two
classification problems as well as maximum accuracy obtained from individual classifiers.
Although the average result is improved by combining classifiers, rank sum test showed that it is
not significantly different from the maximum distinct result.
Table 5.9: Classification results of ensemble of methods
Participant
Accuracy
(%) HP vs.
HN
Max accuracy of HP
vs. HN for individual
classifiers(%)
Accuracy
(%) LP vs.
LN
Max accuracy of LP
vs. LN for individual
classifiers(%)
1 81.2 77.3 86.1 87.5
2 75.8 60.4 85.1 86.0
3 73.8 63.1 95.0 92.5
4 93.8 91.7 82.5 81.0
5 79.6 71.0 87.9 81.3
6 70.5 50.2 73.9 63.1
7 87.4 80.0 92.2 92.3
8 91.0 89.2 90.7 88.5
9 83.5 71.3 79.8 78.3
10 84.8 69.6 78.3 72.5
11 83.4 80.8 71.8 60.8
12 77.8 74.8 97.9 97.5
13 80.4 71.7 90.3 94.4
38
14 78.1 75.4 79.4 67.5
Mean 81.5±6.4 73.3±10.9 85.1±7.8 81.7±11.8
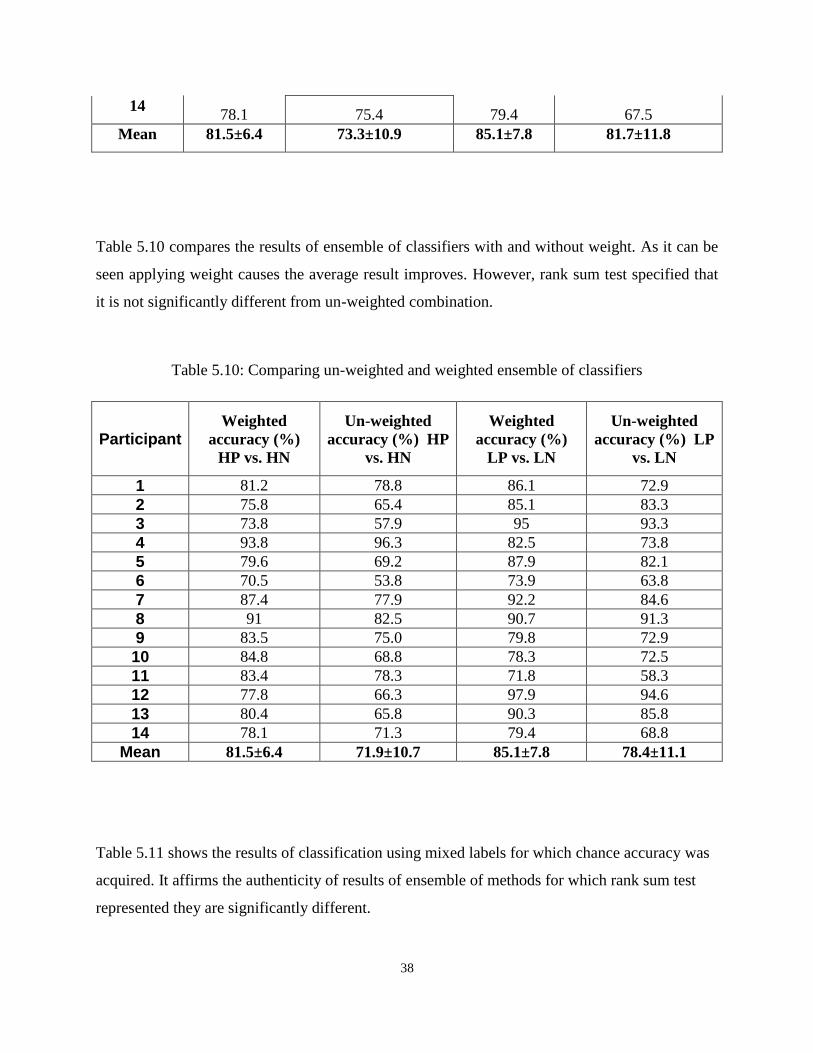
Table 5.10 compares the results of ensemble of classifiers with and without weight. As it can be
seen applying weight causes the average result improves. However, rank sum test specified that
it is not significantly different from un-weighted combination.
Table 5.10: Comparing un-weighted and weighted ensemble of classifiers
Participant Weighted
accuracy (%)
HP vs. HN
Un-weighted
accuracy (%) HP
vs. HN
Weighted
accuracy (%)
LP vs. LN
Un-weighted
accuracy (%) LP
vs. LN
1 81.2 78.8 86.1 72.9
2 75.8 65.4 85.1 83.3
3 73.8 57.9 95 93.3
4 93.8 96.3 82.5 73.8
5 79.6 69.2 87.9 82.1
6 70.5 53.8 73.9 63.8
7 87.4 77.9 92.2 84.6
8 91 82.5 90.7 91.3
9 83.5 75.0 79.8 72.9
10 84.8 68.8 78.3 72.5
11 83.4 78.3 71.8 58.3
12 77.8 66.3 97.9 94.6
13 80.4 65.8 90.3 85.8
14 78.1 71.3 79.4 68.8
Mean 81.5±6.4 71.9±10.7 85.1±7.8 78.4±11.1
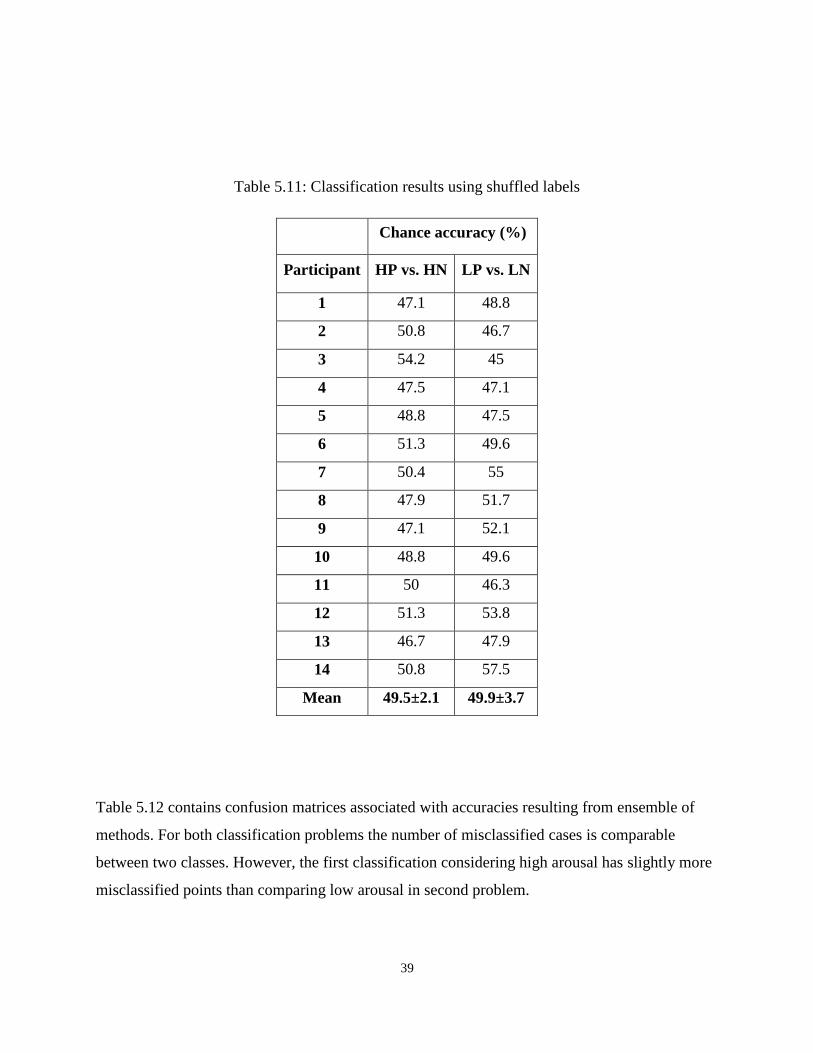
Table 5.11 shows the results of classification using mixed labels for which chance accuracy was
acquired. It affirms the authenticity of results of ensemble of methods for which rank sum test
represented they are significantly different.
39
Table 5.11: Classification results using shuffled labels
Chance accuracy (%)
Participant HP vs. HN LP vs. LN
1 47.1 48.8
2 50.8 46.7
3 54.2 45
4 47.5 47.1
5 48.8 47.5
6 51.3 49.6
7 50.4 55
8 47.9 51.7
9 47.1 52.1
10 48.8 49.6
11 50 46.3
12 51.3 53.8
13 46.7 47.9
14 50.8 57.5
Mean 49.5±2.1 49.9±3.7
Table 5.12 contains confusion matrices associated with accuracies resulting from ensemble of
methods. For both classification problems the number of misclassified cases is comparable
between two classes. However, the first classification considering high arousal has slightly more
misclassified points than comparing low arousal in second problem.

40
Table 5.12: Confusion matrices of ensemble of methods
Predicted labels
n=8400 High/Negative High/Positive
Actual
labels
High/Negative 3453 747
High/Positive 853 3347
Predicted labels
n=8400 Low/Negative Low/Positive
Actual
labels
Low/Negative 3598 602
Low/Positive 613 3587
The results of two classification approaches are shown in Figure 5.3 to easier interpret. For all
participants the accuracies are above 70%. As it can be understood from the bars, there are
variations between individual results.

41
Figure 5.3: Bar plot of results of ensemble of classifiers
5.5 Classification over arousal axis
The goal of this thesis was to find patterns along valence axis as it has already been shown that
the difference between high and low arousal is detectable [13]. To examine the veracity of this
supposition we also have discriminated data in high/positive vs. low/positive as well as
high/negative vs. low/negative classes. The results are demonstrated in Table 5.13. It can be
inferred that the accuracies are considerably better than chance which confirms the possibility of
distinguishing pattern in arousal level.
Table 5.13: Discriminating high vs. low arousal
Participant HP vs. LP (%) HN vs. LN (%)
1 85.9 85.8

42
2 92.3 75.2
3 85.8 98.4
4 86.5 98.1
5 85.1 89.7
6 83.8 77.5
7 91.7 97.3
8 91.3 91.3
9 71.4 81.2
10 74.3 86.3
11 84.8 72.5
12 95.2 84.5
13 75.6 91.8
14 85.8 79.1
Mean 85.0±6.7 86.3±8.2
5.6 Modality Specific Results
To investigate the effect of physiological modality on the final results classification was
performed using features of each signal separately. Table 5.14 sums up the sensor specific results
of ensemble of classifiers. Rank sum test has indicated that there is no significant difference
between the results of each sensor.
Table 5.14: Signal specific results, SC: Skin Conductance, Resp: Respiration, Temp:
Temperature
High/positive vs. high/negative Low/positive vs. low/negative
Par ECG SC Resp Temp All
sensors ECG SC Resp Temp
All
sensors
1 72.3 87.1 71.7 77.7 81.2 92.1 76 73.5 72.9 86.1
2 74.8 71 81.5 76.7 75.8 70.8 85.2 83.5 76.3 85.1
3 76.5 75 73.5 75.8 73.8 89.8 77.3 95.6 79.6 95
4 70 88.8 84.6 71.9 93.8 75.8 81.5 97.7 70 82.5
5 72.3 83.3 76.3 78.8 79.6 67.9 82.1 70.6 78.5 87.9
6 74.6 70.8 73.3 73.3 70.5 74.6 69.6 70.8 74.2 73.9
7 71.5 98.1 82.1 73.3 87.4 75.2 80 79.4 96.7 92.2
8 72.7 78.3 73.1 77.3 91 74.2 92.3 76.7 73.3 90.7
9 74.6 76.9 74.4 88.1 83.5 82.5 77.9 76.3 74.6 79.8

43
10 76.3 74 83.3 80 84.8 72.5 71.3 74.2 71.9 78.3
11 74.4 85.4 73.8 75.4 83.4 80.4 72.7 70 73.3 71.8
12 69.8 73.5 73.1 85.8 77.8 75.2 99.4 75.2 73.3 97.9
13 75.6 70.8 83.5 76.3 80.4 99.2 75.8 96.7 69.4 90.3
14 71.9 75.4 80.2 72.9 78.1 74 70.4 76 78.5 79.4
Mean 73.4±2.2 79.2±8.2 77.5±4.8 77.4±4.7 81.5±6.4 78.9±9.0 79.4±8.5 79.7±9.8 75.9±6.7 85.1±7.8
We ran the classification for each modality without feature selection. As can be seen in Figure
5.4 the accuracies for all the participants, except one result for participant 4, are above 70%.
Figure 5.4: Accuracy results with full feature set for each signal
5.7 Selected Features
A histogram of selected features for two classification methods is demonstrated in Figure 5.5. As
the figure shows, average SC signal is the most frequent selected signal followed by average
temperature in both cases. There is no feature that is not selected at any time.

44
Figure 5.5: Selected features, RR-int: RR intervals of ECG, HR: heart rate, RI: respiration
intervals, RR: respiration rate, Resp: respiration, Temp: temperature, SCR: skin conductance
response
Top ten features for each classification problem are listed in Table 5.15. Features from all four
sensors are among the most selected features.
Table 5.15: Top ten selected features
Feature ranking HP vs. HN LP vs. LN

45
1 Mean SC Mean SC
2 Mean temperature Mean temperature
3 Minimum temperature Minimum respiration rate
4 Minimum respiration rate Mean RR interval
5 Standard deviation of temperature Mean temperature
6 Slope of SC signal Standard deviation respiration interval
7 Mean respiration interval Minimum respiration interval
8 Slope of temperature signal Mean respiration rate
9 Mean respiration rate Maximum RR interval
10 Minimum respiration interval Slope of temperature
Figure 5.6 includes heat maps indicating selected features for each participant in low arousal,
high arousal, and subtraction of low from high arousal respectively. The numbers on each plot
signify the number of times the feature was selected in 100 runs of classification.

46
(a) Frequency of selecting each feature in classifying low/positive vs. low/negative

47
(b) Frequency of selecting each feature in classifying high/positive vs. high/negative

48
(c) Difference of frequency of feature selection in two classification problems
Figure 5.6: Frequency of feature selection for each participant for: (a) low arousal, (b) high
arousal, (c) subtracting a from b. The numbers on the plot show the number of times each feature
is selected out of 100 runs of classification

49
5.9 Association of Classification Accuracy and SAM Ratings with
Demographics
We conducted linear regression analysis to examine the effect of demographic information on
classification accuracy. The results are summarized in Tables 5.16 (a) and (b). As it is indicated
age, gender, IQ, and CBCL scores do not have significant effect on classification accuracy.
However, SCQ score has significant effect on accuracy in comparison high/positive vs.
high/negative states. We may not detect effects for other demographics due to inadequate power
caused by limited sample size. Figure 5.7 demonstrates the scatter plot of accuracy results of
classifying high/positive vs. high/negative against SCQ score. It indicates that the higher SCQ
score, the lower accuracy.
Table 5.16: Effect of demographic information on classification accuracy
Regression slope Standard Error t-stat P-value
Age 1.116 0.998 1.119 0.285
Gender -3.720 4.231 -0.879 0.397
IQ 0.116 0.086 1.353 0.201
SCQ -0.889 0.216 -4.118 0.001*
CBCL-Internalizing problems -0.236 0.249 -0.949 0.361
CBCL-Externalizing problems 0.175 0.182 0.963 0.354
(a) Effect of demographic information on classification results of high/positive vs. high/negative
Regression slope Standard Error t-stat P-value
Age 0.717 1.257 0.570 0.579
Gender 3.750 5.192 0.722 0.484
IQ 0.003 0.112 0.027 0.979
SCQ 0.519 0.379 1.370 0.196
CBCL-Internalizing problems -0.236 0.249 -0.949 0.361
CBCL-Externalizing problems 0.175 0.182 0.963 0.354

50
(b) Effect of demographic information on classification results of low/positive vs. low/negative
Figure 5.7: Accuracy of classifying HP vs. HN against SCQ scores
Tables 5.17 (a) to (d) show the effect of demographics on the results of consistency of children’s
rating with actual labels. As can be seen, none of the parameters has significant effect on the
results. Agaian, we may not be able to detect the effects due to small power because of limited
sample size.
Table 5.17: Effect of demographic information on SAM results
Regression slope Standard Error t-stat P-value
Age -5.245 5.286 -0.992 0.341

51
Gender 15.152 22.469 0.674 0.513
IQ -0.343 0.474 -0.722 0.484
SCQ 0.663 1.749 0.379 0.711
CBCL-Internalizing problems -0.344 1.349 -0.255 0.803
CBCL-Externalizing problems -1.841 0.833 -2.210 0.047
(a) Effect of demographic information on results of consistency of child’s ratings and actual labels for
stimuli with low arousal
Regression slope Standard Error t-stat P-value
Age 3.234 6.844 0.473 0.645
Gender 34.848 26.941 1.294 0.220
IQ -0.914 0.548 -1.666 0.122
SCQ 1.298 2.179 0.596 0.562
CBCL-Internalizing problems 1.190 1.664 0.715 0.488
CBCL-Externalizing problems -0.641 1.228 -0.522 0.611
(b) Effect of demographic information on results of consistency of child’s ratings and actual labels for
stimuli with high arousal
Regression slope Standard Error t-stat P-value
Age -7.430 4.031 -1.843 0.090
Gender 3.788 18.980 0.200 0.845
IQ -0.267 0.395 -0.677 0.511
SCQ 1.137 1.424 0.799 0.440
CBCL-Internalizing problems 1.330 1.056 1.260 0.232
CBCL-Externalizing problems 0.854 0.783 1.091 0.297
(c) Effect of demographic information on results of consistency of child’s ratings and actual labels for
stimuli with positive valence
Regression slope Standard Error t-stat P-value
Age 4.983 5.141 0.969 0.352
Gender -3.788 22.199 -0.171 0.867
IQ 0.381 0.457 0.834 0.421

52
SCQ -1.012 1.683 -0.601 0.559
CBCL-Internalizing problems 1.521 1.238 1.229 0.243
CBCL-Externalizing problems 0.292 0.956 0.306 0.765
(d) Effect of demographic information on results of consistency of child’s ratings and actual labels for
stimuli with negative valence
5.10 Effect of Window Size on Accuracy
Figures 5.8 and 5.9 indicate the effect of window size in which features are extracted to be used
in classification as data points on the performance of classifiers. Each bar denotes accuracy of
ensemble of methods for one specific segmentation. Different window lengths are listed in Table
5.18. As examined by rank sum test there is no significant difference between various cases.
Figure 5.8: Results of various segmentations in classifying LP vs. LN

53
Figure 5.9: Results of various segmentations in classifying HP vs. HN
Table 5.18: Data partitioning
Segmentation Length of train:test (sec) Sub-window size (sec) Shift (sec)
1 320:160 30 15
2 320:160 20 15
3 360:120 20 15
4 320:160 30 10
5 320:160 20 10
6 360:120 20 10
7 320:160 30 5
8 320:160 20 5
9 360:120 20 5

54
Chapter 6
Discussion and Conclusion
6.1 SAM assessment
Overall, the results of our study revealed poor agreement between child/parent assessments of
emotional stimuli and the true labels as well as between child and parent assessments. The results
of child assessments are not supervising given the known difficulties with emotion processing
and recognition in ASD [6]. We did not find a significant effect of age or IQ on assessment
agreement, indicating that the discrepancy is not likely due to misunderstanding the task. There
was also no effect of symptom severity, measured by the SCQ, on assessment agreement.
Interestingly, when looking at the results per emotion type, we found that there was a high
agreement between child SAM reports and actual labels for the positive stimuli. These results
suggest a bias toward interpretation of negative stimuli in ASD [75], a finding consistent with
existing reports in the literature.
The differences in recognition accuracy between positive and negative emotions may also be
related to an imbalance in the stimuli potency between negative and positive stimuli. In
particular, we excluded highly negative stimuli from our picture selection as these were
inappropriate for child viewing. There was such restriction for erotic pictures in positive stimuli
while there were suitable alternatives in other themes for them.
Our results also show poor agreement between parent assessments and actual labels as well as
child labels. Anecdotally, several parents reported that they were unable to discern their
children’s reactions during the study as overt expressions were minimal.

55
6.2 Feature selection
We employed an automatic feature selection algorithm to reduce the number of features for
classification. This algorithm chooses a subset of features that maximize classification accuracy.
As such, the results of feature selection can provide insight into the usefulness of each feature to
differentiating between the emotional responses. Our results show that features from each
individual sensor (ECG, SC, respiration, and temperature) provide viable features for
classification with over 70% accuracy for the two classification problems considered herein. In
addition, mean SC was the most frequently selected feature for classification across all
participants.
SC signal receives inputs only from sympathetic branch of ANS while other signals have input
of both sympathetic and parasympathetic nervous system [76]. It may be related to the fact SC
reflects emotional states better than other signals as it is stimulated more specifically. Our results
also show that combining features across sensors improves average classification accuracies. It
can be due to existence of complimentary information in the separated signals.
Comparing the selected features for each participants, it is evidence that although some features
are more frequently selected across participants overall, the subset of optimal features is person-
dependent. This is consistent with reports of person stereotypy – that is, for each individual, the
autonomic response to stimuli may exhibit different, but reproducible, levels of activity in each
physiological measure [77].
Differences in selected features may also be related to varying quality of data recorded from each
sensor for different participants. Differences in data quality may have results from differences in
sensor positioning and adhesion, or varying degrees of noise (e.g., participant) affecting each
sensor. An important implication of our findings is that classification algorithms should focus on
individual participants instead of considering groups.
Usability purposes make it essential to reach an integrated set of features for each participant as
in the real world it is not efficient to select the optimum set of features in each circumstance. In
this regard classification was performed using the data of each signal at a time without feature
selection. The accuracy results are above 70% in all the cases except in one participant for one of

56
the signals. This finding suggests that even if we consider one signal and use the genuine
features we still obtain an acceptable result better than chance.
6.3 Classification Results
Overall, our results indicate that positive and negative affective states can be automatically
differentiated with accuracies greater than 80%. In this study, the average of accuracy in
differentiating of differently valenced states was higher under low arousal conditions as
compared to high arousal. This may be related to the potency of the stimuli as was shown in the
ratings of selected stimuli. For instance, for low positive emotion elicitation the average of
valence is 8.1 while for high positive it is 6.91 (the closer to 9, the more positive). The level of
arousal is 2.16 and 5.38 for the first and second stimuli respectively which implies the former
one is close enough to low arousal as it supposed to be while the later one is close to neutral
whereas it is intended to be high arousal.
To investigate whether the difference in the classification results is due to masking the valence
patterns by arousal, the pattern recognition was also performed to distinguish variations in
arousal level (comparing high/positive vs. low/positive and high/negative vs. low/negative). The
average of the results is also higher than 80% in these two cases. It can be inferred that the data
shows pattern in both arousal and valence dimensions.
As specified in table 5.10 classification results of ensemble of methods in general is higher than
individual classifiers. Using ensemble of classifiers boosted the average classification accuracy.
The best obtained accuracy for single classifiers was 79.9% and 71.2% respectively for
comparing low/positive vs. low/negative and high/positive vs. high negative. The accuracy
increased to 85.1% and 81.5% respectively by combining classifiers which is 5.2% improvement
for the first and 10.3% for the second case.
For all participants in comparison of high/positive vs. high/negative states and for 12 cases out of
14 participants in discriminating low/positive vs. low/negative the combination of classifiers
outperformed the maximum result achieved by a single method. In those two cases that it did not

57
enhance the accuracy, the results were comparable (the accuracies were 86.3% and 85.8% for
combined model, and 87.5% and 86.0% for maximum result of separate methods respectively. It
was also shown that weighted majority vote has performed better than simple majority vote. It is
attributable to the fact that in weighted model methods with higher performance receive greater
weight than the ones acted poorly while in simple majority vote all the methods have equal effect
on the final result.
Confusion matrices in table 5.13 shows the number of correctly classified points between
high/positive and high/negative emotions as well as low/positive and low/negative ones are
relatively similar, indicating that the classifier is not biased towards any of the classes.
According to bar plot of various methods of segmentation, partitioning order number 9 for which
the number of obtained data points is slightly higher than the other cases acquired better results.
As it was aforementioned the intended labels were decided to be used in the analyses. Three
possible scenarios can be considered: 1- The child’s labels are similar to intended labels. As it
was shown it is not the case in this study. 2- The child’s labels are different from actual labels
and the latter one is correct. It was what we assumed here and obtained acceptable accuracy for
classification. 3- The child’s labels and intended labels are different and the former is the right
label. To test this hypothesis we tried to use child’s ratings for classification. As it was shown in
Figures 5.1 and 5.2 the labels prevented us from performing classification as for several
participants we only had one type of label, while two distinct labels are required for pattern
analysis. Therefore, testing this case was impossible in this study.
6.4 Effect of demographic variables/behavioural measures on
accuracy
According to Figure 5.5 (e), SCQ score has significant effect on the result of discriminating
high/positive vs. high/negative emotions and the higher SCQ score, the lower accuracy of
classification. This effect can stem from different reasons. SCQ score is a representation of
severity of autism. Higher SCQ implies less ability in perceiving stimuli intended influence, and
therefore not discriminating between various emotional states effectively. It also can cause

58
variations in physiological signals so that the changes may not be clearly distinguishable for each
affective state.
Age, IQ, gender, and CBCL score do not have any significant effect on the results. This implies
that possibility of finding patterns in physiological data in various affective states is similar for
all participants regardless of these three specifications. It is also possible that we have not
detected effects for other demographics due to inadequate power caused by limited sample size.

59
Chapter 7
Conclusion
In this study the feasibility of differentiating physiological signals of children with ASD in four
emotional classes namely, high/positive, high/negative, low/positive, and low/negative was
investigated. 15 participants with ASD completed the task of watching pictures as stimuli to
elicit targeted emotions. The pictures were selected from gold standard collections which were
used in several related studies before. After collecting physiological signals using four sensors
including ECG, EDA, temperature, and respiration, pre-processing was done to remove artifacts
from the data. Then various statistical features in the time domain were extracted from each
signal. As the number of features was high compared to number of data points, feature selection
was performed using sequential forward selection, backward elimination. Then, Seven
classification methods comprise of KNN with K equal to 3, 5, and 7; LDA; SVM Linear, SVM
with polynomial kernel (order 3), and SVM with Radial Basis Function were combined using
weighted majority vote. The intended labels were considered for classification due to severe
mismatch between ratings of participants and parents with actual labels. The results suggest that
there is distinguishable pattern in the signals between aforementioned classes as supported by
average classification accuracies of 81.0% for comparing high/positive vs. high/negative and
84.9% for discriminating low/positive vs. low/negative. It was also indicated that the result of
ensemble of methods had higher performance than individual classifiers. It acted significantly
better chance which supports its validity.
The outcome of this research was a physiological approach to detection of emotions which can
provide a language-free, non-invasive, and low-cost way for characterization of emotional states
in children with ASD. This work can ultimately contribute to improving self-awareness of
emotions by providing users with information regarding their actual body state. In addition it will
enhance our understanding of ASD-related emotion processing difficulties.

60
The limitations on the way of this study included: 1- being ethically restricted in choosing
powerful stimuli. 2- Short length of measured signals which impacted the quality and amount of
extractable information; for instance, frequency features were not suitable to be obtained for this
signal size. 3- Sample size was small implying that applying some algorithms is unfavorable. As
an example, finding subgroups of individuals in different measures can be done on a larger
sample sizes.
In future, the sample size can be increased to enable performing clustering to find subgroups of
similar individuals. Also, a group of typical participants can be added for comparison purposes
and investigating whether or not detecting patterns in the physiological signals is better
achievable in one group than the other. Lastly, the design of study can be changed to multiple
visits of each participant to have longer duration of data recording which increases the amount of
information.

61
References
[1] American Psychiatric Association. Diagnostic and statistical manual of mental disorders,
text revision (DSM-IV-TR). American Psychiatric Association, 2000.
[2] Honkalampi, K., Hintikka, J., Tanskanen, A., Lehtonen, J., & Viinamäki, H. (2000).
Depression is strongly associated with alexithymia in the general population. Journal of
psychosomatic research, 48(1), 99-104.
[3] Baron-Cohen, S. E., Tager-Flusberg, H. E., & Cohen, D. J. (1994). Understanding other
minds: Perspectives from autism. In Most of the chapters in this book were presented in draft
form at a workshop in Seattle, Apr 1991. Oxford University Press.
[4] Frith, U. (2004). Emanuel Miller lecture: Confusions and controversies about Asperger
syndrome. Journal of child psychology and psychiatry, 45(4), 672-686.
[5] Baron-Cohen, S., Lombardo, M., Tager-Flusberg, H., & Cohen, D. (Eds.). (2013).
Understanding Other Minds: Perspectives from developmental social neuroscience. OUP
Oxford.
[6] Silani, G., Bird, G., Brindley, R., Singer, T., Frith, C., & Frith, U. (2008). Levels of
emotional awareness and autism: an fMRI study. Social neuroscience, 3(2), 97-112.
[7] Sifneos, Peter E. "The prevalence of'alexithymic'characteristics in psychosomatic patients."
Psychotherapy and psychosomatics 22 (1973): 255-62.
[8] Linden, W., Wen, F., & Paulhus, D. L. (1995). Measuring alexithymia: reliability, validity,
and prevalence. Advances in personality assessment, 10, 51-95.
[9] Hill, Elisabeth, Sylvie Berthoz, and Uta Frith. "Brief report: Cognitive processing of own
emotions in individuals with autistic spectrum disorder and in their relatives." Journal of autism
and developmental disorders 34, no. 2 (2004): 229-235.
62
[10] Bachevalier, J., & Loveland, K. A. (2006). The orbitofrontal–amygdala circuit and self-
regulation of social–emotional behavior in autism. Neuroscience & Biobehavioral Reviews,
30(1), 97-117.
[11] Lambie, J. A., & Marcel, A. J. (2002). Consciousness and the varieties of emotion
experience: a theoretical framework. Psychological review, 109(2), 219.
[12] Shalom, D. Ben, S. H. Mostofsky, R. L. Hazlett, M. C. Goldberg, R. J. Landa, Y. Faran, D.
R. McLeod, and R. Hoehn-Saric. "Normal physiological emotions but differences in expression
of conscious feelings in children with high-functioning autism." Journal of autism and
developmental disorders 36, no. 3 (2006): 395-400.
[13] Kushki, Azadeh, Ajmal Khan, Jessica Brian, and Evdokia Anagnostou. "A Kalman
Filtering Framework for Physiological Detection of Anxiety-Related Arousal in Children with
Autism Spectrum Disorder." (2014).
[14] Kennedy, Daniel P., Elizabeth Redcay, and Eric Courchesne. "Failing to deactivate: resting
functional abnormalities in autism." Proceedings of the National Academy of Sciences 103, no.
21 (2006): 8275-8280.
[15] Rieffe, C., Terwogt, M. M., & Kotronopoulou, K. (2007). Awareness of single and multiple
emotions in high-functioning children with autism. Journal of autism and developmental
disorders, 37(3), 455-465.
[16] Picard, R. W., Vyzas, E., & Healey, J. (2001). Toward machine emotional intelligence:
Analysis of affective physiological state. Pattern Analysis and Machine Intelligence, IEEE
Transactions on, 23(10), 1175-1191.
[17] Liu, Changchun, Karla Conn, Nilanjan Sarkar, and Wendy Stone. "Physiology-based affect
recognition for computer-assisted intervention of children with Autism Spectrum Disorder."
International journal of human-computer studies 66, no. 9 (2008): 662-677.
[18] Baltaxe, Christiane AM, and James Q. Simmons III. "Prosodic development in normal and
autistic children." In Communication problems in autism, pp. 95-125. Springer US, 1985.

63
[19] Luu, Sheena, and Tom Chau. "Decoding subjective preference from single-trial near-
infrared spectroscopy signals." Journal of neural engineering 6, no. 1 (2009): 016003.
[20] Kandel, Eric R., James H. Schwartz, and Thomas M. Jessell, eds. Principles of neural
science. Vol. 4. New York: McGraw-Hill, 2000.
[21] Andreassi, John L. Psychophysiology: Human behavior & physiological response.
Psychology Press, 2000.
[22] Nasoz, Fatma, Christine L. Lisetti, Kaye Alvarez, and Neal Finkelstein. "Emotion
recognition from physiological signals for user modeling of affect." In Proceedings of the 3rd
Workshop on Affective and Attitude User Modelling (Pittsburgh, PA, USA. 2003.
[23] Ekman, Paul, Wallace V. Friesen, Maureen O'Sullivan, Anthony Chan, Irene Diacoyanni-
Tarlatzis, Karl Heider, Rainer Krause et al. "Universals and cultural differences in the judgments
of facial expressions of emotion." Journal of personality and social psychology 53, no. 4 (1987):
712.
[24] Peter, Christian, and Antje Herbon. "Emotion representation and physiology assignments in
digital systems." Interacting with Computers 18, no. 2 (2006): 139-170.
[25] Lang, Peter J. "The emotion probe: studies of motivation and attention." American
psychologist 50, no. 5 (1995): 372.
[26] Hamann, Stephan. "Mapping discrete and dimensional emotions onto the brain:
controversies and consensus." Trends in cognitive sciences 16, no. 9 (2012): 458-466.
[27] Wilson-Mendenhall, Christine D., Lisa Feldman Barrett, and Lawrence W. Barsalou.
"Neural evidence that human emotions share core affective properties." Psychological science
24, no. 6 (2013): 947-956.
[28] Barrett, Lisa Feldman, and Eliza Bliss‐Moreau. "Affect as a psychological primitive."
Advances in experimental social psychology 41 (2009): 167-218.

64
[29] Jerritta, S., Murugappan, M., Nagarajan, R., & Wan, K. (2011, March). Physiological
signals based human emotion recognition: a review. In Signal Processing and its Applications
(CSPA), 2011 IEEE 7th International Colloquium on (pp. 410-415). IEEE.
[30] Lang, Peter J., Margaret M. Bradley, and Bruce N. Cuthbert. "International affective picture
system (IAPS): Affective ratings of pictures and instruction manual." Technical report A-8
(2008).
[31] Rigas, G., Katsis, C. D., Ganiatsas, G., & Fotiadis, D. I. (2007). A user independent,
biosignal based, emotion recognition method. In User Modeling 2007 (pp. 314-318). Springer
Berlin Heidelberg.
[32] Haag, A., Goronzy, S., Schaich, P., & Williams, J. (2004, June). Emotion recognition using
bio-sensors: First steps towards an automatic system. In ADS (pp. 36-48).
[33] Maaoui, C., Pruski, A., & Abdat, F. (2010). Emotion recognition through physiological
signals for human-machine communication. INTECH Open Access Publisher.
[34] Gu, Y., Tan, S. L., Wong, K. J., Ho, M. H. R., & Qu, L. (2010, July). A biometric signature
based system for improved emotion recognition using physiological responses from multiple
subjects. In Industrial Informatics (INDIN), 2010 8th IEEE International Conference on (pp. 61-
66). IEEE.
[35] Gross, James J., and Robert W. Levenson. "Emotion elicitation using films." Cognition &
Emotion 9, no. 1 (1995): 87-108.
[36] Nasoz, F., Alvarez, K., Lisetti, C. L., & Finkelstein, N. (2004). Emotion recognition from
physiological signals using wireless sensors for presence technologies. Cognition, Technology &
Work, 6(1), 4-14.
[37] Li, L., & Chen, J. H. (2006, December). Emotion recognition using physiological signals
from multiple subjects. In Intelligent Information Hiding and Multimedia Signal Processing,
2006. IIH-MSP'06. International Conference on (pp. 355-358). IEEE.

65
[38] Wan-Hui, W., Yu-Hui, Q., & Guang-Yuan, L. (2009, March). Electrocardiography
recording, feature extraction and classification for emotion recognition. In Computer Science and
Information Engineering, 2009 WRI World Congress on (Vol. 4, pp. 168-172). IEEE.
[39] Kim, Jonghwa, and Elisabeth André. "Emotion recognition based on physiological changes
in music listening." Pattern Analysis and Machine Intelligence, IEEE Transactions on 30, no. 12
(2008): 2067-2083.
[40] Wagner, J., Kim, J., & André, E. (2005, July). From physiological signals to emotions:
Implementing and comparing selected methods for feature extraction and classification. In
Multimedia and Expo, 2005. ICME 2005. IEEE International Conference on (pp. 940-943).
IEEE.
[41] Cheng, B., & Liu, G. Y. (2008, May). Emotion recognition from surface EMG signal using
wavelet transform and neural network. In Proceedings of The 2nd International Conference on
Bioinformatics and Biomedical Engineering (ICBBE) (pp. 1363-1366).
[42] Zhu, X. (2010, April). Emotion recognition of EMG based on BP neural network. In Proc
Int Symposium Network. Network Security (pp. 227-229).
[43] Kim, Jonghwa. Bimodal emotion recognition using speech and physiological changes.
INTECH Open Access Publisher, 2007.
[44] Kim, Kyung Hwan, S. W. Bang, and S. R. Kim. "Emotion recognition system using short-
term monitoring of physiological signals." Medical and biological engineering and computing
42, no. 3 (2004): 419-427.
[45] Kushki, Azadeh, Ellen Drumm, Michele Pla Mobarak, Nadia Tanel, Annie Dupuis, Tom
Chau, and Evdokia Anagnostou. "Investigating the autonomic nervous system response to
anxiety in children with autism spectrum disorders." PLoS one 8, no. 4 (2013): e59730.
[46] Kootz, John P., and Donald J. Cohen. "Modulation of sensory intake in autistic children:
Cardiovascular and behavioral indices." Journal of the American Academy of Child Psychiatry
20, no. 4 (1981): 692-701.

66
[47] Jansen, Lucres Mc, Christine C. Gispen-de Wied, Rutger-Jan van der Gaag, and Herman
van Engeland. "Differentiation between autism and multiple complex developmental disorder in
response to psychosocial stress." Neuropsychopharmacology: official publication of the
American College of Neuropsychopharmacology 28, no. 3 (2003): 582-590.
[48] Groden, June, Matthew S. Goodwin, M. Grace Baron, Gerald Groden, Wayne F. Velicer,
Lewis P. Lipsitt, Stefan G. Hofmann, and Brett Plummer. "Assessing cardiovascular responses to
stressors in individuals with autism spectrum disorders." Focus on Autism and Other
Developmental Disabilities 20, no. 4 (2005): 244-252.
[49] Groden, June, Amy Diller, Margaret Bausman, Wayne Velicer, Gregory Norman, and
Joseph Cautela. "The development of a stress survey schedule for persons with autism and other
developmental disabilities." Journal of Autism and Developmental Disorders 31, no. 2 (2001):
207-217.
[50] Brown, R. Michael, Lisa R. Hall, Roee Holtzer, Stephanie L. Brown, and Norma L. Brown.
"Gender and video game performance." Sex Roles 36, no. 11-12 (1997): 793-812.
[51] Pecchinenda, Anna. "The affective significance of skin conductance activity during a
difficult problem-solving task." Cognition & Emotion 10, no. 5 (1996): 481-504.
[52] Bölte, S., Feineis-Matthews, S., & Poustka, F. (2008). Brief report: Emotional processing in
high-functioning autism—physiological reactivity and affective report. Journal of Autism and
Developmental Disorders, 38(4), 776-781.
[53] Kim, Kyung Hwan, S. W. Bang, and S. R. Kim. "Emotion recognition system using short-
term monitoring of physiological signals." Medical and biological engineering and computing
42, no. 3 (2004): 419-427.
[54] Brown, R. Michael, Lisa R. Hall, Roee Holtzer, Stephanie L. Brown, and Norma L. Brown.
"Gender and video game performance." Sex Roles 36, no. 11-12 (1997): 793-812.
[55] Bradley, Margaret M., and Peter J. Lang. "Emotion and motivation." Handbook of
psychophysiology 2 (2000): 602-642.

67
[56] Katsis, Christos D., Nikolaos Katertsidis, George Ganiatsas, and Dimitrios I. Fotiadis.
"Toward emotion recognition in car-racing drivers: A biosignal processing approach." Systems,
Man and Cybernetics, Part A: Systems and Humans, IEEE Transactions on 38, no. 3 (2008):
502-512.
[57] SHUSTERMAN, V, and BARNEA, O. (1995): 'Analysis of skin-temperature variability
compared to variability of blood pressure and heart rate', IEEE Ann. Conf Engineering Medicine
Biology Society, pp. 1027-1028
[58] KATAOKA, H., KANO, H., YOSHIDA, H., SAIJO, A., YASUDA, M., and OSUMI, M.
(1998): 'Development of a skin temperature measuring system for non-contact stress evaluation'.
IEEE Ann. Conf. Engineering Medicine Biology Society, pp. 940-943
[59] Peper, E., Harvey, R., Lin, I. M., Tylova, H., & Moss, D. (2007). Is there more to blood
volume pulse than heart rate variability, respiratory sinus arrhythmia, and cardiorespiratory
synchrony?. Biofeedback, 35(2).
[64] Lord, C., Risi, S., Lambrecht, L., Cook Jr, E. H., Leventhal, B. L., DiLavore, P. C., ... &
Rutter, M. (2000). The Autism Diagnostic Observation Schedule—Generic: A standard measure
of social and communication deficits associated with the spectrum of autism. Journal of autism
and developmental disorders, 30(3), 205-223.
[66] Dan-Glauser, E. S., & Scherer, K. R. (2011). The Geneva affective picture database
(GAPED): a new 730-picture database focusing on valence and normative significance. Behavior
research methods, 43(2), 468-477.
[68] Bradley, M., & Lang, P. J. (1999). The International affective digitized sounds (IADS)[:
stimuli, instruction manual and affective ratings. NIMH Center for the Study of Emotion and
Attention.
[69] Pan, J., & Tompkins, W. J. (1985). A real-time QRS detection algorithm. Biomedical
Engineering, IEEE Transactions on, (3), 230-236.
[70] Lacey, John I., and Beatrice C. Lacey. "Verification and extension of the principle of
autonomic response-stereotypy." The American journal of psychology (1958): 50-73.

68
[71] Kulic, D., & Croft, E. (2007). Affective state estimation for human–robot interaction.
Robotics, IEEE Transactions on, 23(5), 991-1000.
[72] Zong, C., & Chetouani, M. (2009, December). Hilbert-Huang transform based
physiological signals analysis for emotion recognition. In Signal Processing and Information
Technology (ISSPIT), 2009 IEEE International Symposium on (pp. 334-339). IEEE.
[73] Hönig, F., Wagner, J., Batliner, A., & Nöth, E. (2009). Classification of user states with
physiological signals: On-line generic features vs. specialized feature sets. In Proc. of the 17th
European Signal Processing Conference (EUSIPCO-2009).
[74] Faul, F., Erdfelder, E., Lang, A. G., & Buchner, A. (2007). G* Power 3: A flexible
statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior
research methods, 39(2), 175-191.
[75] Ashwin, C., Chapman, E., Colle, L., & Baron-Cohen, S. (2006). Impaired recognition of
negative basic emotions in autism: A test of the amygdala theory. Social neuroscience, 1(3-4),
349-363.
[76] Boucsein, W. (2012). Electrodermal activity. Springer Science & Business Media.
[77] Lacey, J. I., & Lacey, B. C. (1958). Verification and extension of the principle of autonomic
response-stereotypy. The American journal of psychology, 71(1), 50-73.
[78] Schapire, R. E., Freund, Y., Bartlett, P., & Lee, W. S. (1998). Boosting the margin: A new
explanation for the effectiveness of voting methods. Annals of statistics, 1651-1686.
[79] Dietterich, T. G. (2000). An experimental comparison of three methods for constructing
ensembles of decision trees: Bagging, boosting, and randomization. Machine learning, 40(2),
139-157.
[80] Kuncheva, L. I., & Whitaker, C. J. (2003). Measures of diversity in classifier ensembles
and their relationship with the ensemble accuracy. Machine learning, 51(2), 181-207.
[81] Ganong, W. F., & Barrett, K. E. (1995). Review of medical physiology (pp. 474-478).
Norwalk, CT: Appleton & Lange.

69
[82] Cuthbert, B. N., Schupp, H. T., Bradley, M. M., Birbaumer, N., & Lang, P. J. (2000). Brain
potentials in affective picture processing: covariation with autonomic arousal and affective
report. Biological psychology, 52(2), 95-111.
[83] Thayer, J. F., & Lane, R. D. (2000). A model of neurovisceral integration in emotion
regulation and dysregulation. Journal of affective disorders, 61(3), 201-216.
[84] Jatupaiboon, N., Pan-ngum, S., & Israsena, P. (2013). Real-time EEG-based happiness
detection system. The Scientific World Journal, 2013.
[85] Jatupaiboon, N., Pan-ngum, S., & Israsena, P. (2013). Real-time EEG-based happiness
detection system. The Scientific World Journal, 2013.
[86] http://biosig.sourceforge.net/download.html
[87] Benedek, M., & Kaernbach, C. (2010). A continuous measure of phasic electrodermal
activity. Journal of neuroscience methods, 190(1), 80-91.