pathology in gynecologic cancer – all what you want...
TRANSCRIPT

Pathology in Gynecologic Cancer –all what you want to know as a PhD scientist
Ie-Ming Shih, MD, PhD
http://pathology2.jhu.edu/shihlab/index.cfm

Gross anatomy of female genital organs
Squamous intraepithelial lesion
Squamous carcinoma
Endometrial hyperplasia
Endometrioid carcinoma
LeiomyomaLeiomyosarcoma
“Ovarian” cancer:Primary carcinomaMetastatic carcinomaStromal tumorGerm cell tumor
HPV
estrogen
?
Chorio-carcinoma
mole
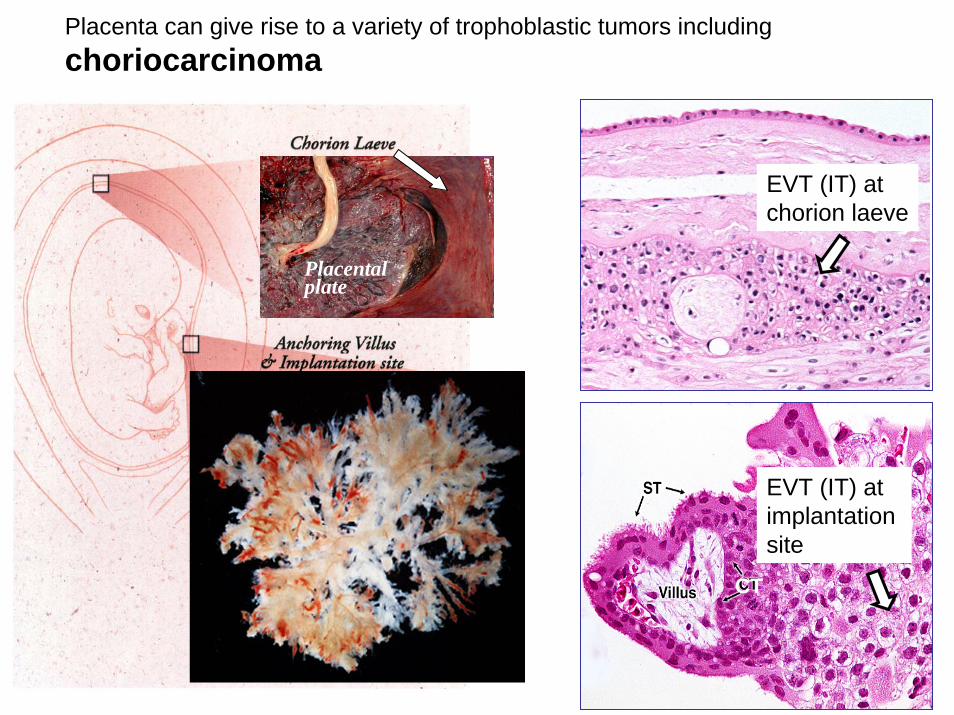
Placenta can give rise to a variety of trophoblastic tumors including choriocarcinoma
EVT (IT) atchorion laeve
EVT (IT) atimplantation site
CT
Placental plate

Histology

Leiomyoma, the most common benign uterine tumor in women
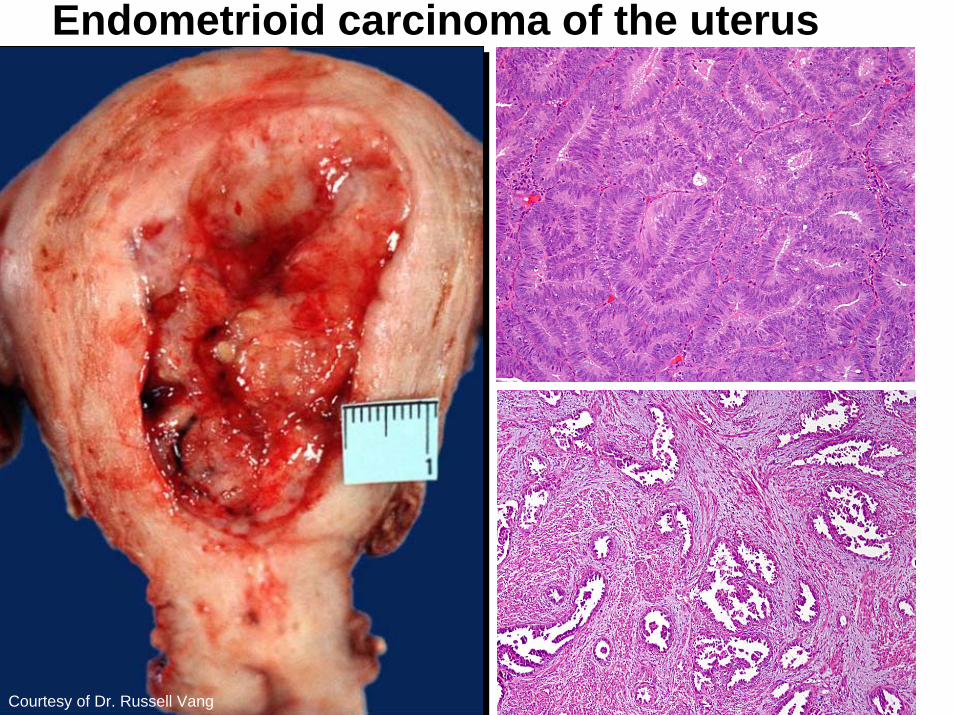
Endometrioid carcinoma of the uterus
Courtesy of Dr. Russell Vang

Gestational Trophoblastic Diseases
Lesions of fetal origin
Maternal Fetus Paternal

Homozygous complete mole- 80-90%
Empty Egg
23X
46XX
46XX
46XX
PaternalChromosomes
Only

23X
23Y
23X
23Y46XY
46XY
46XY
Dispermy
Diploid androgeniccells
Heterozygous complete mole-< 20%
PaternalChromosomes
Only

23Y
69XXY
69XXY
69XXY
23X 23X
23Y Triploid 69XXY Cells
Maternal Chromosomeswith Paternal Extra Set
23X
23X
Dispermy Diandry



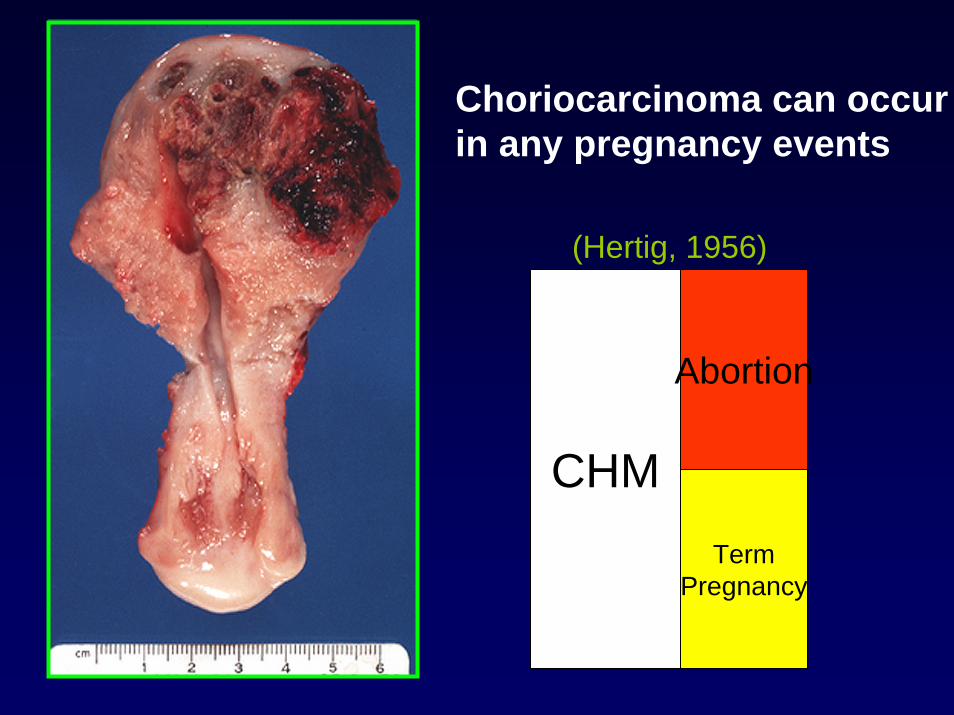
Choriocarcinoma can occur in any pregnancy events
(Hertig, 1956)
CHM
Abortion
TermPregnancy

ChoriocarcinomaInvasive pushing borderCentral massive necrosis/hemorrhageLack of angiogenesisDimorphic appearance- syncytiotrophoblast
alternating with mononucleate trophoblastNo chorionic villi or fetal partsOccasional mixed with PSTT or ETT
β-hCG stain
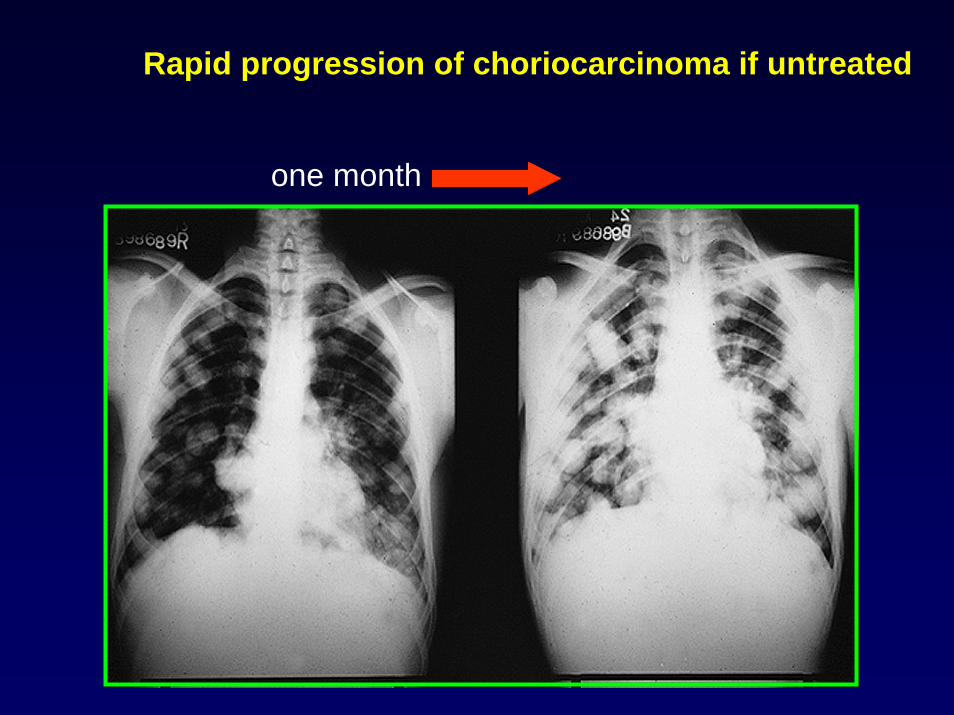
Rapid progression of choriocarcinoma if untreated
one month

Gestational trophoblastic disease
GTD is a semi-allogenic tissue to the patient: abnormally formed placenta (molar pregnancy) neoplasms (choriocaricnoma, PSTT and others)
Reproductive ages- symptoms or signs related to an (antecedent) pregnancy
CHM is a risk factor for choriocarcinoma which is highly aggressive and fatal if untreated
With chemotherapy (MTX), all choriocarcinomas are curable
β-hCG is the gold standard surrogate serum marker for follow-up BUT NOT FOR DIAGNOSIS

The fact of ovarian cancer• Ovarian carcinoma is the major disease of
cancer mortality in women (20,180 new cases 15,310 new deaths in 2006)
• Molecular etiology is poorly understood • Patients are usually on death roll if tumors recur• A peritoneal disease, ideal for i.p. therapy
Issues of borderline tumors
Prediction of outcome in SBT, invasive vs non-invasive implants
Pathogenesis of high-grade serous carcinomaTarget-based therapy in recurrent tumors
Several others…

Ovarian cancers include:

“Aggressive scale” of ovarian epithelial tumors
Serous Endometrioid Clear cell Mucinous Transitional
Carcinoma
Borderline tumor(LMP)
Adenoma
H L

Ovarian Epithelial Tumors- Type I and Type II (the dualistic pathway)Ovarian Epithelial Tumors- Type I and Type II (the dualistic pathway)
Serous Endometrioid Clear cell Mucinous Transitional
Carcinoma
Borderline tumor(LMP)
Adenoma
H L
Type I Low-grade serous CA + endometrioid CA + clear cell CA
Type II High-grade serous CA + some other types

Serous borderline tumor

Morphological continuum of low-grade serous carcinoma:
cystadenoma- SBT- intraepithelial LG CA- invasive LG CA
Genes involved:KRASBRAFERBB2 (Her2/neu)
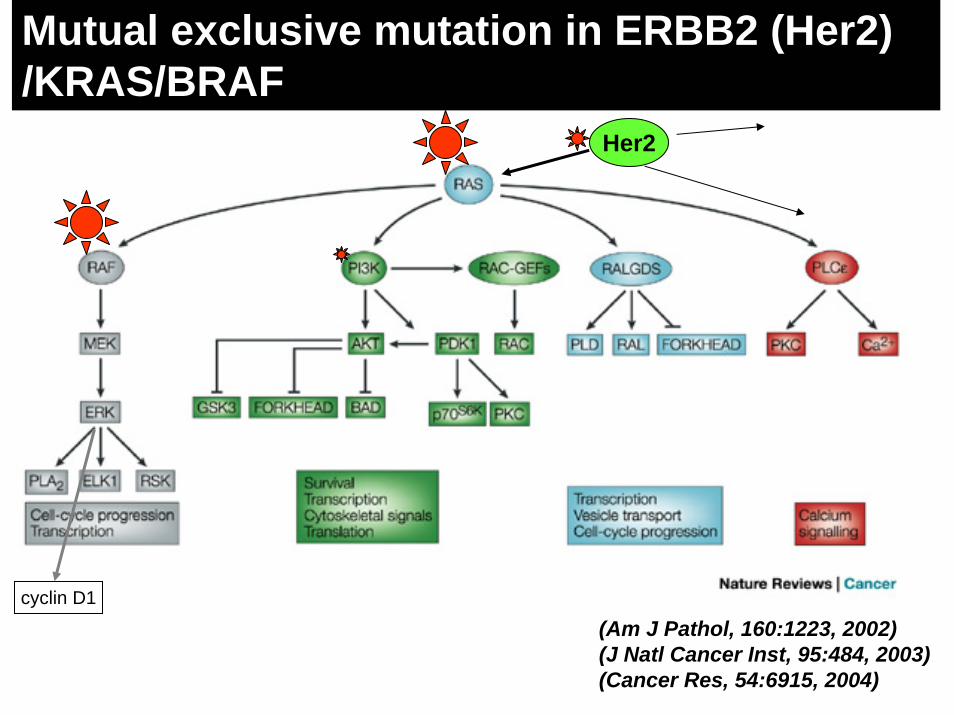
Her2
Mutual exclusive mutation in ERBB2 (Her2)/KRAS/BRAF
cyclin D1
(Am J Pathol, 160:1223, 2002)(J Natl Cancer Inst, 95:484, 2003)(Cancer Res, 54:6915, 2004)

Immunosorting
Minced to small fragments and collagenase digestion
Trypsin digestion
SBT HG tumor
37oC
Primary culturePrimary culture
ImmunosortingImmunosorting
Minced to small fragments and collagenase digestion
Trypsin digestion
SBT HG tumor
37oC37oC
Primary culturePrimary culture
10 20 30 40 50 60
0
2
4
6
8
10
12
Ch 19
10 20 30 40 50 60
0
2
4
6
8
10
12
Ch 19
**
(Cancer Biol Ther, 5:779, 2006)

0 10 20 30 40 50 60 70 80 90 100 110
OVCAR3SKOV3CAOV3
OVPC-8OVPC-7OVPC-6OVPC-5OVPC-4OVPC-3OVPC-2OVPC-1MPSC1Stroma
OSEwt wtwt wtwt mutmut wtwt mutmut wtwt mutwt wtwt wtwt wtwt wtwt wtwt wtwt wt
KRAS BRAF
Cell number (% of DMSO controls)
Mutation status
SBT/LG
HG
SBTs with KRAS/BRAF mutations are more sensitive to theMEK inhibitor in vitro than the conventional HG carcinomas
(Cancer Res, 65:1994, 2005)

Tumor progression model in ovarian endometrioid carcinoma
Endometriosis Endometrioid borderline tumor Endometrioid carcinoma
Genes involved:
PTENCTNNB1 (β-catenin)PIK3CAp53 (in high-grade CA)
Transgenic mice with PTEN and β-cateninmutations give ovarian endometrioid carcinoma. (Cho et al, Cancer Cell, in press)

Transvaginal ultrasound studies
Konishi et al. Gyn Oncol, 88:309, 2003
cystno cyst
Borderline tumorsClear cell carcinomaEndometrioid carcinom
High-grade serous carcinoma

A 38-year-old, infertile woman October 1989, a 5-cm endometriotic cyst. In 1995, she was given hormonal treatment.In December 1998, the cyst re-increased in size, and the solid portion appeared.Laparotomy revealed stage-Ia clear cell carcinoma.
(Gyn Oncol, 88:309, 2003)
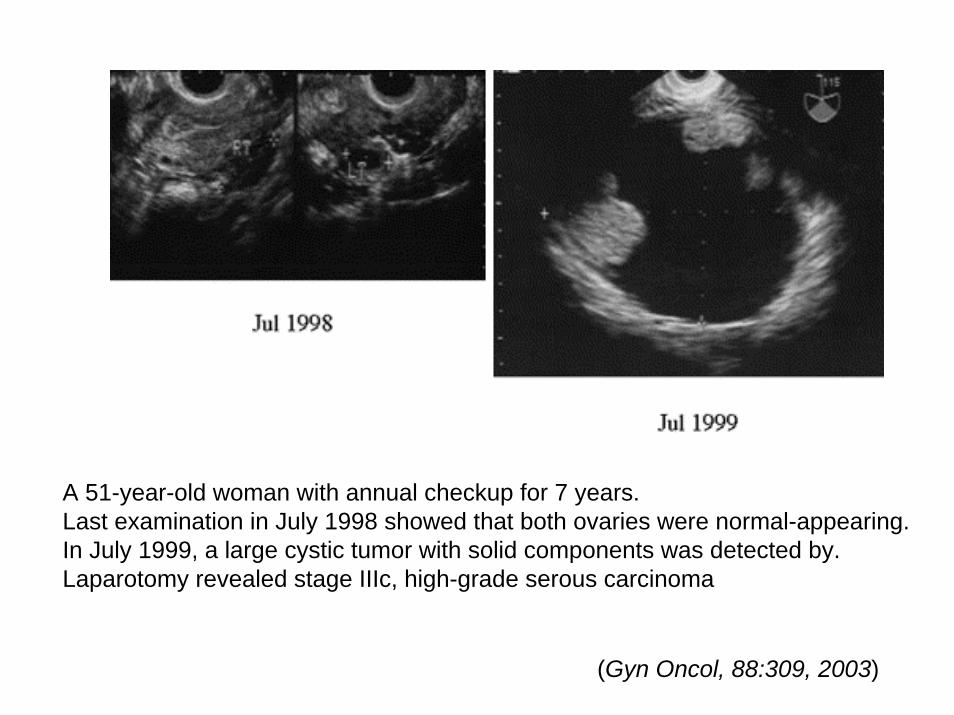
A 51-year-old woman with annual checkup for 7 years.Last examination in July 1998 showed that both ovaries were normal-appearing. In July 1999, a large cystic tumor with solid components was detected by. Laparotomy revealed stage IIIc, high-grade serous carcinoma
(Gyn Oncol, 88:309, 2003)

New hypothesis- fallopian tube origin of “ovarian” (pelvic) serous carcinoma
Fallopian tube
Tumor celldissemination
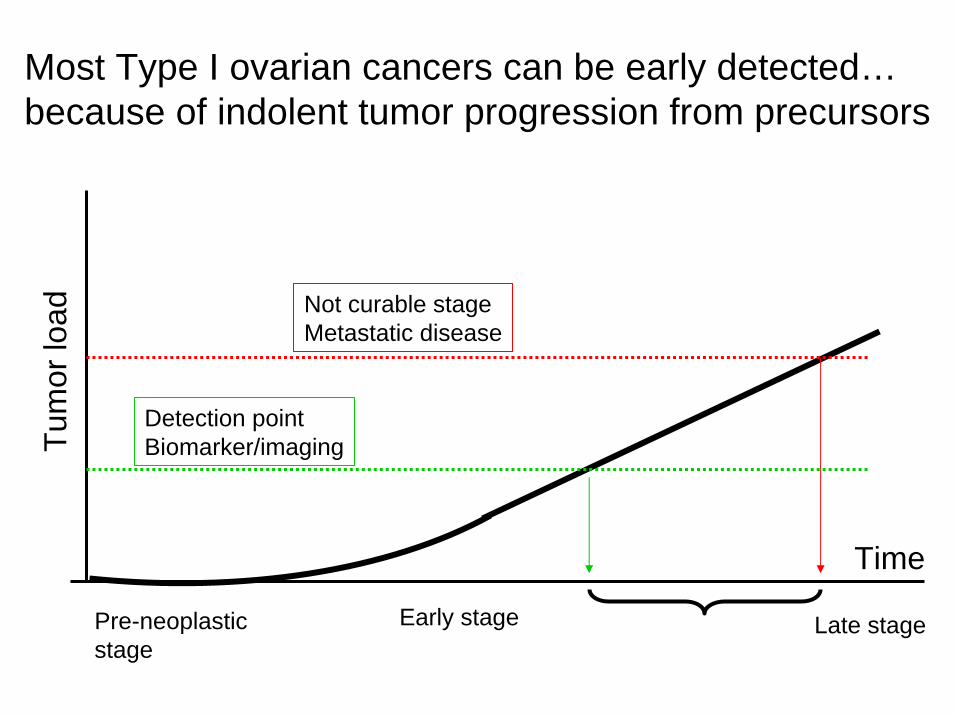
Most Type I ovarian cancers can be early detected… because of indolent tumor progression from precursors
Time
Not curable stageMetastatic disease
Detection pointBiomarker/imagingTu
mor
load
Early stagePre-neoplasticstage
Late stage

Does early cancer detection work at all for Type II CA?Does stage I high-grade serous CA exist?
Pre-neoplasticstage
Tum
or lo
ad
Time
Not curable stageMetastatic disease
Detection pointBiomarker/imaging
Early stage Late stage
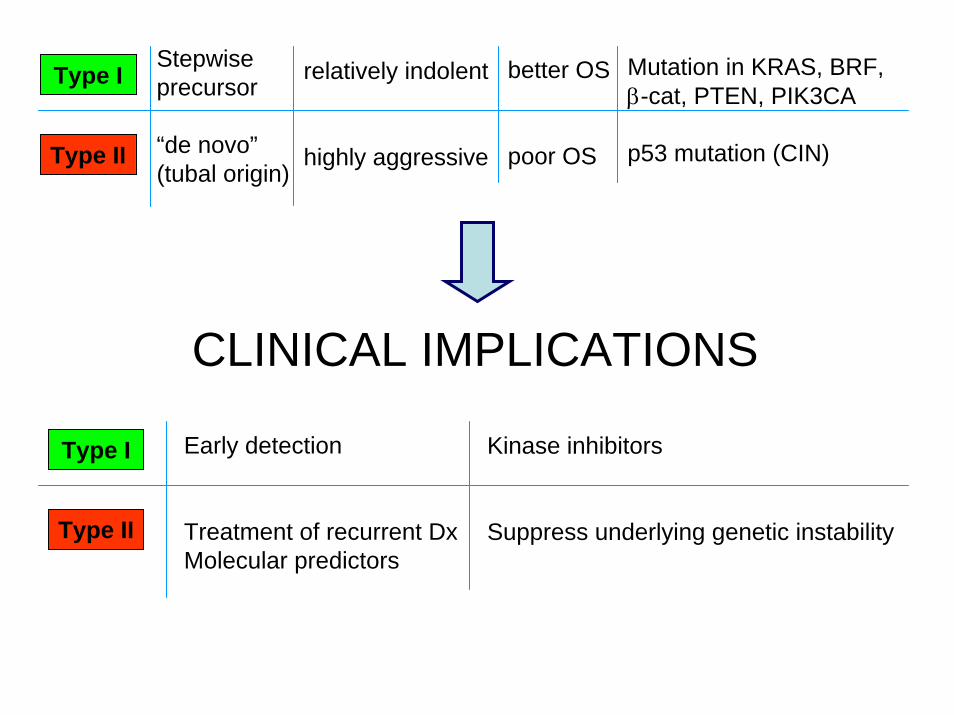
Type I
Type II
Stepwiseprecursor
“de novo”(tubal origin)
relatively indolent
highly aggressive
better OS
poor OS
Mutation in KRAS, BRF, β-cat, PTEN, PIK3CA
p53 mutation (CIN)
CLINICAL IMPLICATIONS
Type I
Type II
Early detection
Treatment of recurrent DxMolecular predictors
Kinase inhibitors
Suppress underlying genetic instability

Aggressive CAVery CINfulp53 mutationsUnique gene
expression
Indolent tumorLess CINfulKRAS/BRAF
mutationsLOH Ch1p+Ch19qUnique gene
expression
(Am J Pathol; 164:1511, 2004)(Clin Cancer Res; 11:7274, 2005)

Predicting Suboptimal SurgeryCase Study
Now what?Now what?

Advanced Ovarian Cancer• United States: 14,000 new cases annually• Long-term survival 25% to 50%• Important Prognostic Factors: - Age
- Performance status- FIGO stage- Ascites volume- Tumor grade/subtype- Chemosensitivity- Residual disease

Advanced Ovarian Cancer:WHY does the surgeon make a difference?WHY does molecular genetics make a difference?

Radical Oophorectomy
Sigmoid Sigmoid TumorTumor
Left OvaryLeft Ovary
Right OvaryRight OvaryUterusUterus
Bladder TumorBladder Tumor
Bristow et al. J Am Coll Surg 2003; 197: 565.

Radical Oophorectomy
Culdesac TumorCuldesac Tumor
Distal SigmoidDistal Sigmoid CervixCervix
UterusUterus
Bladder TumorBladder Tumor
Bristow et al. J Am Coll Surg 2003; 197: 565.

For Type II OVCA- focus on recurrent tumors?
Eventually, all chemotherapyfails in recurrent tumors…
Recurrent tumors are always inevitable…

Gene discovery
High-throughput nucleotide sequencing
Digital Karyotyping
SNP array
LongSAGE (Serial Analysis of Gene Expression)
http://www.digitalkaryotyping.org/
Proteomics

CIN at molecular genetic levelsDigitalkaryotyping
SNP array 1
2
3
4
5
6
7
89
1011
13141516171819
x
202122
12
chro
mos
ome
LG HG
(Nakayama et al, Int J Cancer, in press)(Shih et al. PNAS, 102: 14004, 2005)

Amplicons in ovarian serous carcinomas
AKT2 Cyclin E1 Notch3
Cyclin E1 Notch3 AKT2 Rsf-1 PIK3CA
NormalGain Amp
Total
NormalGainAmp
Total
47(56.6)* 47(58.1) 70(79.5) 73(82.1) 56(75.7) 6(7.2) 16(19.8) 6(6.8) 2(2.2) 10 (13.5)
30(36.1) 18(22.1) 12(13.6) 14(15.7) 8(10.8)
83 81 88 89 74
26(100) 22(91.7) 24(100) 25(100) 20(100)0 2(8.3) 0 0 0 0 0 0 0 0
26 24 24 25 20
* Percentage of cases in parenthesis. Amp: amplification
Notch3 Rsf-1
FISH validation
HG CA
LG CA
Digital karyotypingSNP arrays
Prioritize amplicons
FISH on TMA

p = 0.03
0 40 80 120 160 2000
20
40
60
80
100
Not amplifiedAmplified
Overall survival (months)
Perc
ent S
urvi
val
Johns Hopkins Hospital(primary solid tumors, FISH)
0 20 40 60 80 100 120
OP bis Todeszeitpunkt
0,0
0,2
0,4
0,6
0,8
1,0
Kum
. Übe
rlebe
n
Univ. Muenster Hospital(primary solid tumors, FISH)
Amp
Amp
p = 0.012
p = 0.015
p = 0.03
0 20 40 60 80 1000
20
40
60
80
100
Low expressionHigh expression
Overall survival (months)
Perc
ent S
urvi
val
Norwegian Radium Hospital(primary effusion samples, real-time PCR)
p = 0.037
Vancouver General Hospital(primary solid tumors, FISH)
p = 0.026
Amp
High

Things to remember…
1. All the female reproductive tract and organs including placenta can give rise to neoplastic diseases. Some are common and some are rare!
2. The most common neoplasm among gynecologic tumors is leiomyoma (smooth muscle tumors from myometrium in the uterus) which causes pain, bleeding and infertility in women. Not much research is going on.
3. Endometrioid carcinoma is the most common malignant tumors in the uterus. Most of cases are at early stages and prognosis is excellent. This type of cancer arises from precursors, endometrial hyperplasia and is characterized by defined mutations in PTEN and beta-catenin genes.

Things to remember…
4. Ovarian “cancer” is a heterogeneous group of tumors and can be broadly classified into primary epithelial, stromal, germ cell and metastatic tumors.
5. Within the primary epithelial tumors, they can be classified into different histologic subtypes and each subtype can have benign, borderline or malignant categories.
6. Different histologic subtypes have unique molecular pathways for their development and progression. So, study of ovarian cancer should separate different histological types.

Things to remember…7. Based on clinical and molecular studies, ovarian epithelial
neoplasms can be viewed as two groups- type I and type II for research purposes.
8. The high-grade serous carcinoma is what has been referred as “ovarian cancer”. It is the most common and lethal type of all ovarian neoplasms.
9. The origin of “ovarian” cancer is still not known. Increased ovulation (causes surface inclusion bodies) is a risk factor…A new hypothesis of tubal origin has been recently proposed.
10. Early detection of type II tumor may not work… Focus on the studies of recurrent tumors may likely have a translational impact.