papillon-lefèvre syndrome with acroosteolysis
TRANSCRIPT
Volume 24 Number 5, Part 2 May 1991 Tertiary syphilis o f face
18. Kampmeier RH. The late manifestations of syphilis: skel- etal, viscera[ and cardiovascular. Med Clin North Am 1964;48:667-97.
19. Collart P. Etat actuel des recherches sur la persistence des tr6pon6mes au cours de la syphilis tardivement trait6e. Prophyl Saint Morale 1965;37:247-73.
20. Collart P, Borel L, Durel P. Etude de l'action de la p6nicil- line clans la syphilis tardive: persistence du tr6pon6me pale apr6s traitment. Ann Inst Pasteur 1962;102:596-615.
21. Yobs AR, Olansky S, Rockwell DH, et al. Do treponemes survive adequate treatment of late syphilis? Arch Derma- tol 1965;91:379-89.
22. Smith JL, Israel CW. Spirochetes in the aqueous humor in seronegative ocular syphilis: persistence after penicillin therapy. Arch Ophthalmol 1967;77:474-6.
23. Yogeswari L, Chacko CW. Persistence of T. pallidum and its significance in penicillin-treated seropesitive late syphi- lis. Br J Vener Dis 1971;47:339-47.
Papillon-Lef6vre syndrome with acroosteolysis Akiva Trattner, MD, Michael David, MD, and Mir iam Sandbank, MD Petah Tiqva, Israel
The Papillon-Lef~vre syndrome is characterized by palmoplantar hyperkeratosis and juvenUe periodontitis that results in the precocious loss of both the deciduous and permanent teeth. We report a patient with Papillon-Lef6vre syndrome associated with acroesteolysis, an association that has not been previously described. (J AM ACAD DERMATOL 1991;24: 835-8.)
The Papillon-Lef+vre syndrome (PLS) is an au- tosomal recessive trai t characterized by diffuse pal- moplantar hyperkeratosis and premature loss of both the deciduous and permanent teeth. Ectopic intracranial calcification, mental retardation, and increased susceptibility to infections often occur.1
W e describe a patient with PLS and acroosteo- lysis, a previously undescribed association.
C A S E R E P O R T
A 25-year-old Arab woman was admitted for evalua- tion of palmoplantar hyperkeratosis. The patient was one of eight children. One of her brothers had palmoplantar hyperkeratosis and loss of teeth; he died at 9 years of age of rupture of an abdominal mass. Other siblings were un- affected. Her parents are first cousins (Fig. 1).
The patient was the product of a normal pregnancy and delivery. The skin of the palms and soles became red, thick, scaly, and fissured when she was 5 months of age. When she was 5 years old, similar changes appeared on the dorsum of the hands and feet, forearms, and shins. Scaly erythematous and circumscribed patches appeared on both knees and both elbows.
The deciduous teeth were normal, but when the patient
From the Department of Dermatology, Beilinson Medical Center. Reprint requests: A. Trattner, MD, Department of Dermatology, Bei-
linson Medical Center, Petah Tiqva, 49 100 Israel.
16/4/21314
was 4 years old they began to she, d. The permanent teeth erupted normally but started shedding when she was 8 years of age. She had never had any bacterial infections.
On physical examination the patient's height was 154 era. The fingers and toes were comparatively long, and the thenar and hypothenar eminences were almost com- pletely lacking. The skin of the palms, soles, dorsum of the hands and feet, forearms, and distal aspect of the shins were erythematous, markedly hyperkeratotic, and scaly (Fig. 2). On the knees and elbows were circurnscdbed, scaly, erythematous plaques. On the shins were two hy- popigmented patches and on the face a melasma-like hy- perpigmentation.
No abnormalities were detected in the hair. The nails were dubbed and contained transverse ridges (Fig. 3). The patient was completely edentulous but had normal alveolar ridges.
Laboratory studies. Hemogram, automated chemistry panel values (SMA 12), and protein dectrophoresis were within normal limits. The IgA level was mildly elevated at 527 mg/dl (normal 270 _ 80 mg/dl) and IgM at 257 mg/dl (normal 110 + 40 mg/dl).
Antinuclear antibody, rheumatoid factor (Rose- Waaler and latex test), and antibodies against smooth muscle, parietal cells, mitochondria, and thyroid antigens (cytoplasmic and thyroglobulin) were negative.
Peripheral T-lymphocyte subpopulations were normal. Intradermal skin tests to purified protein derivative and
toxoid antigens were negative; Candida antigens elicited a mild response. Lymphocyte transformation tests by the method of C'unnigham-Rundles et a17 were done in
835

836 Trat tner et al.
Journal of the American Academy of
Dermatology
II
, , ,
IV /
0 AFFECTED FEMALE PERSON �9 AFFECTED MALE PERSON C) UNAFFECTED FEMALE PERSON [ ] UNAFFECTED MALE PERSON
~DECEASED f PROBAND
Fig. 1. Pedigree of family.
Fig. 2. Markedly hyperkeratotic erythematous scaly lesions on palms and dorsum of hands bilaterally.
response to phytohemagglutinin and pokeweed mitogen. The maximal response to phytohemagglutinin was 3936 cpm (normal >15,000 cpm), and the maximal response to pokeweed mitogen was 2644 cpm (normal >10,000 cpm).
Histologic findings. A skin biopsy specimen from the dorsum of the hand showed hyperkeratosis with slight in- flammatory perivascular infiltrates in the dermis.
Fig. 3. Clubbing of finger with transverse grooves of fingernail.
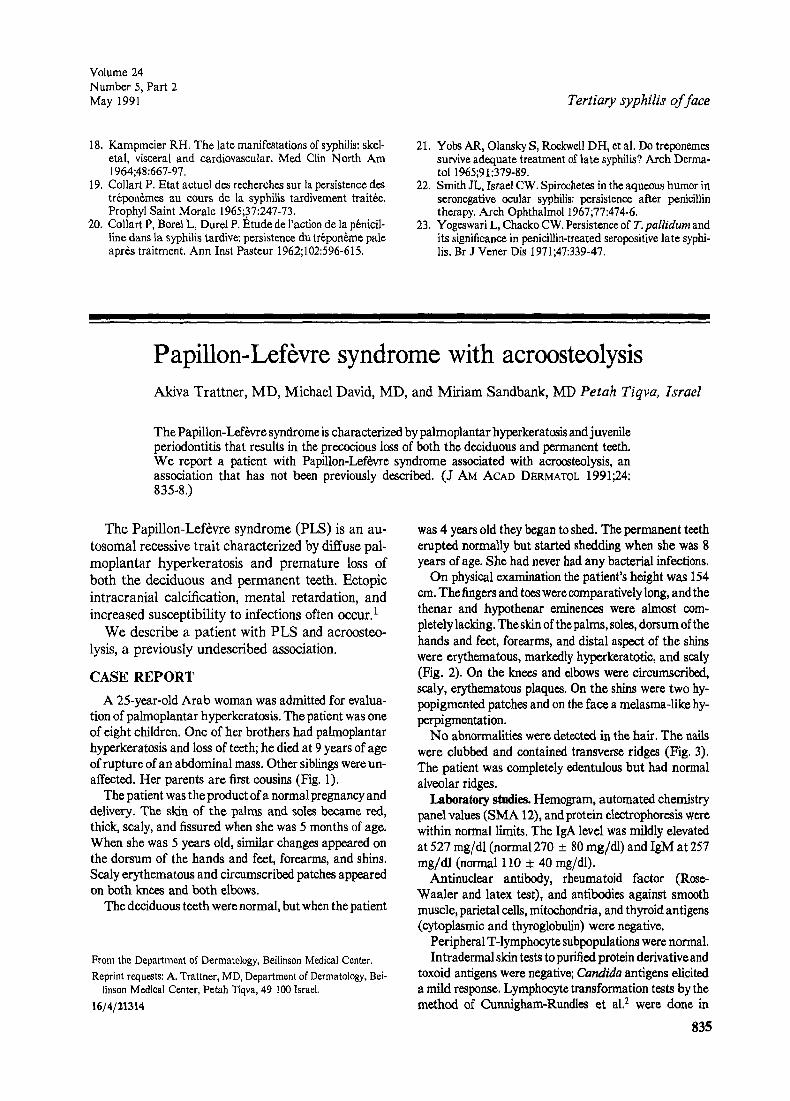
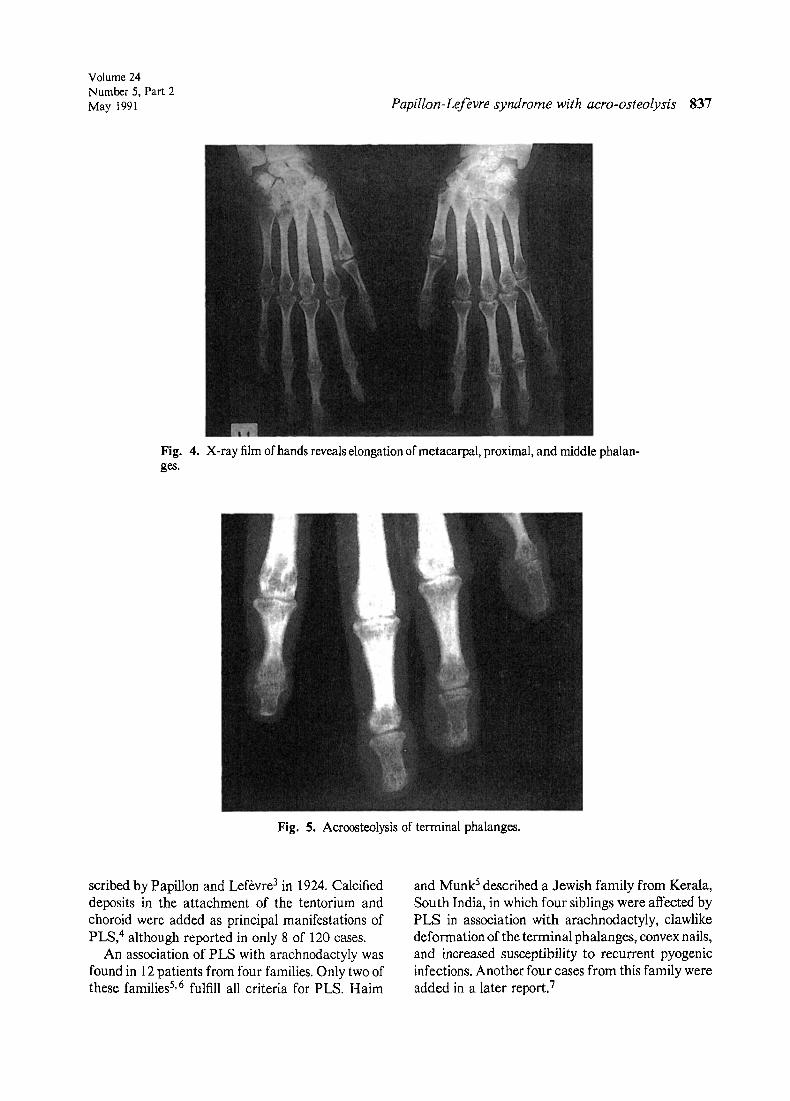
Radiographic study. Roentgenogram of the hands re- vealed marked elongation of the metacarpal, the proxi- mal, and the middle phalanges (Fig. 4). Osteoarthro- pathic changes were present. In the terminal phalanges was a disappearance of the distal parts (Fig. 5).
An x-ray film of the feet showed marked elongation of the metatarsal, the proximal, and middle phalanges. The mandible showed absence of teeth and mild alveolar bone destruction. Mild scoliosis was found in the spine. Cervi- cal spine and skull x-ray films were normal. Computer- ized tomography of skull and brain was normal, as was an electroencephalogram.
DISCUSSION
The association of a transient palmoplantar kera- toderma with juvenile periodontitis was first de-
Volume 24 Number 5, Part 2 May 1991 Papillon-Lefbvre syndrome with acro-osteolysis 837
Fig. 4. X-ray film of hands reveals elongation of metacarpal, proximal, and middle phalan- ges.
Fig. 5. Acroosteolysis of terminal phalanges.
scribed by Papillon and Lef+vre 3 in 1924. Calcified deposits in the attachment of the tentorium and choroid were added as principal manifestations of PLS, 4 although reported in only 8 of 120 cases.
An association of PLS with arachnodactyly was found in 12 patients from four families. Only two of these families 5,6 fulfill all criteria for PLS. Haim
and Munk ~ described a Jewish family from Kerala, South India, in which four siblings were affected by PLS in association with arachnodactyly, clawlike deformation of the terminal phalanges, convex nails, and increased susceptibility to recurrent pyogenic infections. Another four cases from this family were added in a later report. 7

838 Trattner et al.
Journal of the American Academy of
Dermatology
Macard et al.6 described a case of PLS associated with Marfan's syndrome. Our patient had short stature and lacked other manifestations of Marian's syndrome.
Most patients with PLS associated with arach- nodactyly had convex nails, 5, 7 whereas our patient had clubbing and transverse ridges. Clubbing of the fingers has been reported in association with palmo- plantar keratoderma s, 9 but not with PLS.
The most unique association in this case was the loss of the edges of the distal phalanges, as seen in acroosteolysis. 1~ Acroosteolysis can be primary as seen in diverse group of inherited disorders or secondary as induced by polyvinylchloride or as it occurs in pyknodysostosis, Rothmund's syndrome, and collagen vascular disorders. None of the mani- festations of the acquired forms were present in this case. One of the inherited disorders of acroosteo- lysis, acroosteolysis syndrome of Hajdu and Cheney, l 0 has some features, such as acroosteolysis, short stature, pseudo-clubbing of the dints, and early loss of teeth, that were seen in our patient. However, none of the other features of this syn- drome, namely, joint laxity, conductive hearing loss, speech impairment, recessed mandible, and other radiographic features, were present. In addition, palmoplantar keratoderma is not a feature of the Hajdu-Cheney syndrome.
The patient had distinctly reduced lymphocyte transformation and a hypoergia. These are compat-
ible with a defect in cell-mediated immunity. How- ever, she had no history of infections.
REFERENCES
1. Haneke E. The Papillon-Lef6vre syndrome: keratosis pal- moplantaris with periodontopathy--report of a case and review of the cases in the literature. Hum Genet 1979;51:1- 35.
2. Cunnigham-Rundles S, Harsen JA, Dupont BO. Lympho- cyte transformation in vitro in response to mitogens and antigens. Clin Immunol 1976;3:151-93.
3. Papillon MM, Lef6vre P. Deux cas de keratodermie palmaire et plantaire symetrique familiale (maladie de Meleda) chez le fr~re et la soeur: coexistence darts les deux cas d'alterations dentaires graves. Bull Soc Dermatol Syph 1924;31:82-7.
4. Gorlin R J, Sedano H, Anderson VE. The syndrome of pal- mar-plantar hyperkerat~is and premature periodontal de- struction of the teeth. J Pediatr 1964;65:895-908.
5. Halm S, Munk J. Keratosks palmo-plantaris congenita with periodontosis, arachnodactyly and a peculiar deformity of the terminal phalanges. Br J Dermatol 1965;77:42-54.
6. Marcard P, Casteigt, Prabes. Syndrome de Papillon- Lef6vre et syndrome de Marfan. Bull Soc Fr Dermatol Syph 1971;78:56-7.
7. Smith P, Rosenzweig KA. Seven cases of Papillon-Lef~vre syndrome. Periodontics 1967;9:42-6.
8. Bureau Y, Barriere H, Thomas M. Hippocratisme digital congenital avee hyperkeratose palmo-plantaire et troubles osseux. Ann Dermatol Syph 1959;86:611-22.
9. Herdstrand H, Berglund G, Werner I. Keratodermia pal- marks et plantaris with clubbing and skeletal deformity of the terminal phalanges of the hands and feet. Acta Derm Venereol (Stockh) 1972;52:278-80.
10. Resnick D, Niwayama G. Osteolysis and chondrolysis. In: Diagnosis of bone and joint disorders. Philadelphia: WB Saunders, 1981:3017-36.