osteophytosis of the cervical spine in south african blacks and whites
TRANSCRIPT

Osteophytosis of the Cervical Spine in South AfricanBlacks and Whites
CECIL TAITZ*
Department of Anatomy and Anthropology, Sackler School of Medicine, Ramat Aviv, Israel
Cervical vertebral columns (214) of adult human skeletons belonging to South African blacksand whites were examined for the presence of osteophytes. It was found that the cervicalvertebrae of the black samples were significantly less affected by degenerative changes than inthe whites. This finding has specific clinical implications in that the distribution ofosteophytosis in the blacks also follows a different pattern than in the whites; osteophytesappear to affect either the vertebral body or apophysial joint facets in the cervical vertebrae ofthe blacks. In the whites, in sharp contrast, both sites are often affected on the same vertebra,which in life may result in a pincer-like entrapment of the spinal nerve root and/or vertebralartery. Consideration is given to the possible physiological and/or functional causes of thedifferences in distribution and pattern of development of osteophytes in the cervical spines ofthe two population groups. Clin. Anat. 12:103–109, 1999.r 1999 Wiley-Liss, Inc.
Key words: spondylosis; entrapment; nerve root; vertebral artery
INTRODUCTION
A late consequence of the degenerative changesaffecting the soft tissue support system of the spinalcolumn is the development of bony protrusions orirregular excrescences (osteophytes) at variable pointsof soft tissue vertebral attachments. The soft tissuesupports are the intervertebral discs, the longitudinaland interspinous ligaments, and the facet joint cap-sules, one or more of which may fail in their spinalsupport function as a result of sudden injury or ‘‘wearand tear’’ as a concomitant of the aging process(Resnick and Niwayama, 1981).
The present study is an attempt to determine thefrequency of osteophytosis in the cervical vertebrae inthe two major population groups in South Africa, withdue consideration to age and sex and location of theosteophytes in each group. Consideration is also givento the potential clinical significance of the findings.
MATERIALS AND METHODS
This study is based on observations of 214 vertebralcolumns of adult human skeletons drawn from SouthAfrican black and white cadaver populations. Theskeletal material forms part of the Raymond DartCollection, Department of Anatomy and Human Biol-ogy in the Medical School of the University of the
Witwatersrand, assembled from about 1922 to 1991.All data such as sex, age, and race were taken from theaccession records. Specifically, the material comprised111 skeletons of adult whites (60 males, 51 females)and 103 skeletons of South African blacks (57 males,46 females).
Although there are known ethnic and linguisticdifferences among South African black nations andtribes, genetic and morphological evidence stronglypoints to close biological relationships among them(Tobias, 1972). Hence, in the present study, data forsubjects who belonged to different tribal subgroupshave been pooled into a single South African blackdata-set.
For the purpose of the study, an effort was made tocover the adult life-span of each group. This was doneby a random sample taken within each 10-year inter-val, beginning at age 30, for each sex and for bothblacks and whites, respectively. However, the rela-tively small sample size in the younger age groupnecessitated division of the subjects into two groupsviz a relatively younger age group, 30–59 years, and anolder group 60 years and over.
*Correspondence to: Dr. Cecil Taitz, Department of Anatomy andAnthropology, Sackler School of Medicine, Ramat Aviv 69978,Israel. E-mail: [email protected]
Received 25 February 1998; Revised 18 June 1998
Clinical Anatomy 12:103–109 (1999)
r 1999 Wiley-Liss, Inc.
Grading of Osteophytosis of Cervical VertebralC1-C7
A system of grading of osteophytosis of the cervicalvertebrae was devised to allow for assessment of thelocalization, severity, and extent of encroachment ofthe osteophytes into one or all four of the following:vertebral foramen, intervertebral foramen, foramen ofthe transverse process, and the median atlanto-axialjoint.
The grading of osteophytes follows the classifica-tion of Eisenstein (1980), which in turn was a modifica-tion of the system of the four grades of Nathan (1962).This modified system recognizes three successivesteps in the degeneration of the intervertebral disc andof the zygapophysial joints as indicated below.
Grade 1 osteophytosis - mild. The term refers tominor bony excrescences projecting from the margins,singly or in combination of (1) the vertebral body, (2)the uncinate processes, and (3) the zygapophysialjoint. This grade of osteophytic projection incorpo-rates the first and second grades of Nathan (1962).Since according to Eisenstein (1980) and Nathan(1962), these osteophytes apparently do not impingeon any vital nervous or vascular structure, they werenot considered in this study to be of clinical signifi-cance.
Grade 2 osteophytosis - moderate. This graderepresents medium to large bony projections into thevertebral foramen, intervertebral foramen, or foramenof the transverse process, singly or in combination.These projections usually extend either from theanterior or posterior margins of the vertebal body,laterally from the uncinate processes and/or anterome-dially, from the facets of the zygapophysial joints.
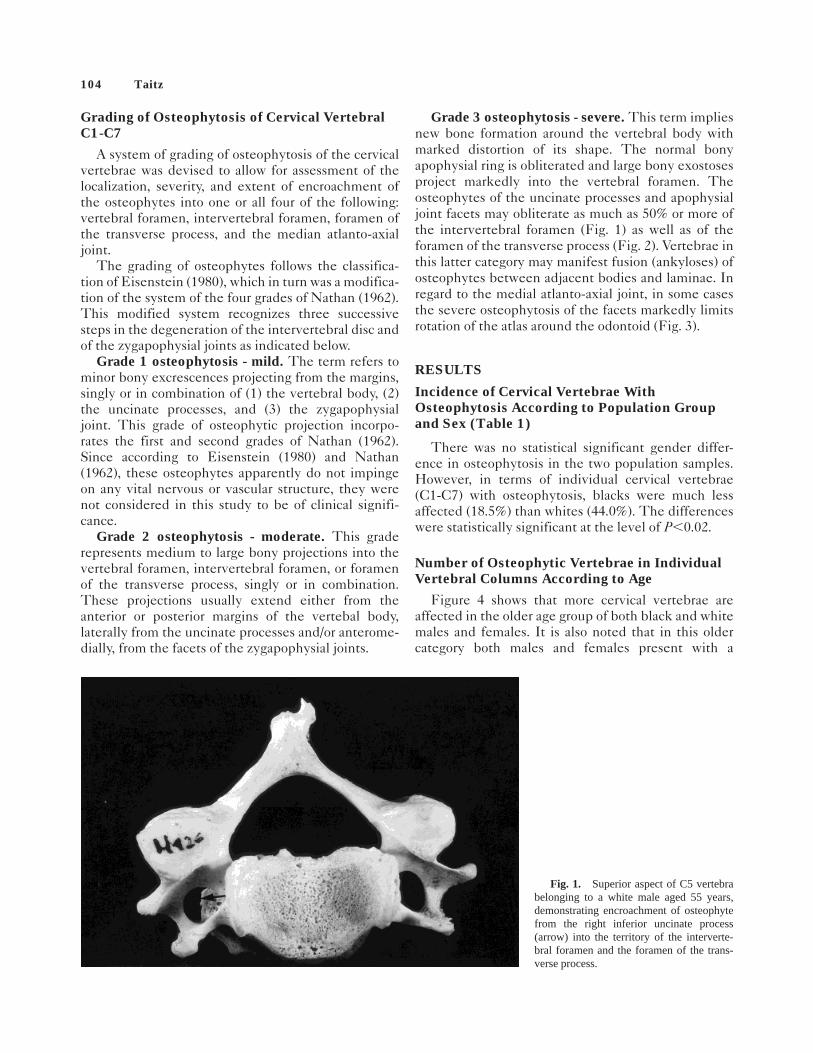
Grade 3 osteophytosis - severe. This term impliesnew bone formation around the vertebral body withmarked distortion of its shape. The normal bonyapophysial ring is obliterated and large bony exostosesproject markedly into the vertebral foramen. Theosteophytes of the uncinate processes and apophysialjoint facets may obliterate as much as 50% or more ofthe intervertebral foramen (Fig. 1) as well as of theforamen of the transverse process (Fig. 2). Vertebrae inthis latter category may manifest fusion (ankyloses) ofosteophytes between adjacent bodies and laminae. Inregard to the medial atlanto-axial joint, in some casesthe severe osteophytosis of the facets markedly limitsrotation of the atlas around the odontoid (Fig. 3).
RESULTS
Incidence of Cervical Vertebrae WithOsteophytosis According to Population Groupand Sex (Table 1)
There was no statistical significant gender differ-ence in osteophytosis in the two population samples.However, in terms of individual cervical vertebrae(C1-C7) with osteophytosis, blacks were much lessaffected (18.5%) than whites (44.0%). The differenceswere statistically significant at the level of P,0.02.
Number of Osteophytic Vertebrae in IndividualVertebral Columns According to Age
Figure 4 shows that more cervical vertebrae areaffected in the older age group of both black and whitemales and females. It is also noted that in this oldercategory both males and females present with a
Fig. 1. Superior aspect of C5 vertebrabelonging to a white male aged 55 years,demonstrating encroachment of osteophytefrom the right inferior uncinate process(arrow) into the territory of the interverte-bral foramen and the foramen of the trans-verse process.
104 Taitz

relatively similar incidence of affected vertebrae,namely, 3–5. The breakdown was as follows: blackmales 34.4%; black females 36.4%; white males 56.7%;white females, 54.1%. Spinal columns with 6–7 verte-brae affected are only present in the older category andpredominated in the males and females of the whiteseries.
Incidence by Site of Osteophytosis on CervicalVertebrae C3-C7
The site of osteophytes in the cervical vertebrae,especially in relationship to the bodies and/or articularfacets, is noted in Figure 5.
It should also be noted that only ‘‘typical’’ cervicalvertebrae (C3–C7) present with uncovertebral joints;thus the atlas (C1) and the axis (C2) have beenomitted from Figure 5.
In the total sample of osteophytic vertebrae, about athird involved the vertebral margins only, a little over athird the apophysial facet joint margins, and a quarterevidently affected both sites.
Ethnicity substantially affected the site of osteophy-tosis. Thus there was a greater tendency for osteo-phytes to occur only on the vertebral bodies in blackmales (54.5%), as compared to white males (32.1%);these differences were significantly different at the
Fig. 2. Superior aspect of C4 vertebraof a black male aged 60 years, showing alarge facet osteophyte encroaching into theintervertebral foramen and foramen of thetransverse process.
Fig. 3. Posterosuperior view of C1and C2 vertebrae of a white male aged 70years, demonstrating severe degenerativechanges of median atlanto-axial joint. Notethe marked bony outgrowths on the dens(arrows).
Osteophytosis of the Cervical Spine in South African Blacks and Whites 105

level of P,0.02. Facets only were affected in 40.0% ofblack males and 34.6% in white males; these differ-ences were not statistically significant.
The incidence of osteophytosis on both body andfacets showed a striking contrast between black and
white males, the percentage values being only 5.5% inthe former and 33.3% in the latter; in both black andwhite females the facets only category, is modal with41.7% and 52.2%, respectively. Here again, a relativelysmall number of blacks showed lesions of both bodyand facets of the same vertebra.
Incidence of Osteophytosis of the MedianAtlanto-axial Joint (Table 2)
The median atlanto-axial joint showed a statisticallysignificantly higher frequency of osteophytosis inwhites than in blacks (43.2% vs. 8.7%) (P,0.01).Strong sexual dimorphism was also evident; blackmales 12.3%; black females 4.1%; white males 48.3%;white females 37.3%.
Incidence of Osteophytosis of InferiorApophysial Facets of Axis (Table 3)
Relatively few of the inferior facets of the axis in theblacks of both sexes are affected by osteophytosis ascompared to the whites, namely, 6.6% vs. 24.8%. Thedifferences are statistically significant at a level ofP,0.01.
In regard to sexual differences, Table 3 shows thatmales in both blacks and whites show a higher
TABLE 1. Number and Relative Frequencies of CervicalVertebrae C1–C7 With Osteophytosis According to Sexand Ethnic Group
Group and sexVertebral
columns N
Vertebrae
Total NAffected
N %
BlacksMales 57 399 73 18.0Females 46 322 60 18.6
Total 103 721 133 18.5
WhitesMales 60 420 184 43.8Females 51 357 158 44.3
Both sexes 111 777 342 44.0
Fig. 4. Incidence of vertebrae with osteophytosis in individualvertebral columns according to age.A, males;B, females.
Fig. 5. Relative frequency of cervical body and/or facet osteophy-toses in cervical vertebrae C3-C7.
TABLE 2. Numbers and Relative Frequencies of Axesof Cervical Spines With Osteophytosis of MedianAtlanto-axial Joints
Group
Median atlanto-axial joint inMales Females Both sexes
Totaljoints
Affected Totaljoints
Affected Totaljoints
AffectedN % N % N %
Blacks 57 7 12.3 46 2 4.3 103 9 8.7Whites 60 29 48.3 51 19 37.3 111 48 43.7
106 Taitz

incidence of affected facets than females, however, thedifferences are not significant.
DISCUSSION
A literature search reveals four other comparativestudies of osteophytosis of the cervical spine in blacksand whites. Cave et al. (1955) compared the incidenceof osteophytosis of the cervical spine in skeletons ofEuropeans and Nigerians; Davis (1960) carried out asimilar study of the latter two population groups, andRoche (1957) and Nathan (1962) studied the cervicaland lumbar spine of American blacks and whites. Allfour authors found a significantly higher incidence ofosteophytosis of the cervical vertebrae in the whitegroups.
The only other comparative study of osteophytosisof the vertebrae of South African blacks and whites is
that of Eisenstein (1980), who focused his attention onthe lumbar spine. In that study, the black samplemanifested less osteophytosis than in the whites.
Perhaps the most significant findings of the presentstudy are not only that there is a much lower incidenceof cervical osteophytosis in the black population groupof both sexes as compared to the white group, butthere also appears to be a characteristic pattern ofdistribution of each ethnic group. This pattern isclearly discerned in the graphs in Figure 5, where it isseen that in the white group a significant number ofpathological vertebrae have both cervical body andapophysial facet osteophytosis on the same vertebrae.In contrast, the black group mostly manifests osteophy-tosis either on the vertebral body, or on the apophysialfacet only. In the white sample, the degree of facetosteophytosis is also more marked. The above findingshave obviously important implications for both thephysical anthropologist and the clinician. In the latterregard, it is relevant to note that osteophytes of theuncinate process have a tendency to grow in a postero-lateral direction toward the intervertebral foramen, orin a lateral direction toward the foramen of thetransverse process (Fig. 1). Osteophytes from theapophysial facet margin may similarly encroach onthe territory of the spinal nerve in the intervertebralforamen (Fig. 2), or that of the vertebral artery in theforamen of the transverse process (Fig. 6). It issuggested that when osteophytes impinge on thenerve root or vertebral artery from one or the other site(as is the situation in the black sample), the neurovas-cular structures may escape severe entrapment due totheir surrounding ‘‘safety cushion’’ of fat (Holt and
TABLE 3. Relative Frequency of Axes ofCervical Spines of Blacks and Whites WithOsteophytosis of One or Both InferiorApophysial Articulating Facets by Sex
Group/sex N
Osteophyticaxes
N %
BlacksMales 57 5 8.8Females 49 2 4.0
Total 106 7 6.6
WhitesMales 60 15 25.0Females 54 13 24.0
Total 114 28 24.8
Fig. 6. Anterior view of dissectionof vertebral arteries. Note the entrapmentof the right vertebral artery by the pincer-like effect of osteophytes of the apophy-sial facet (small arrow) and correspondinguncinate process (large arrow).
Osteophytosis of the Cervical Spine in South African Blacks and Whites 107
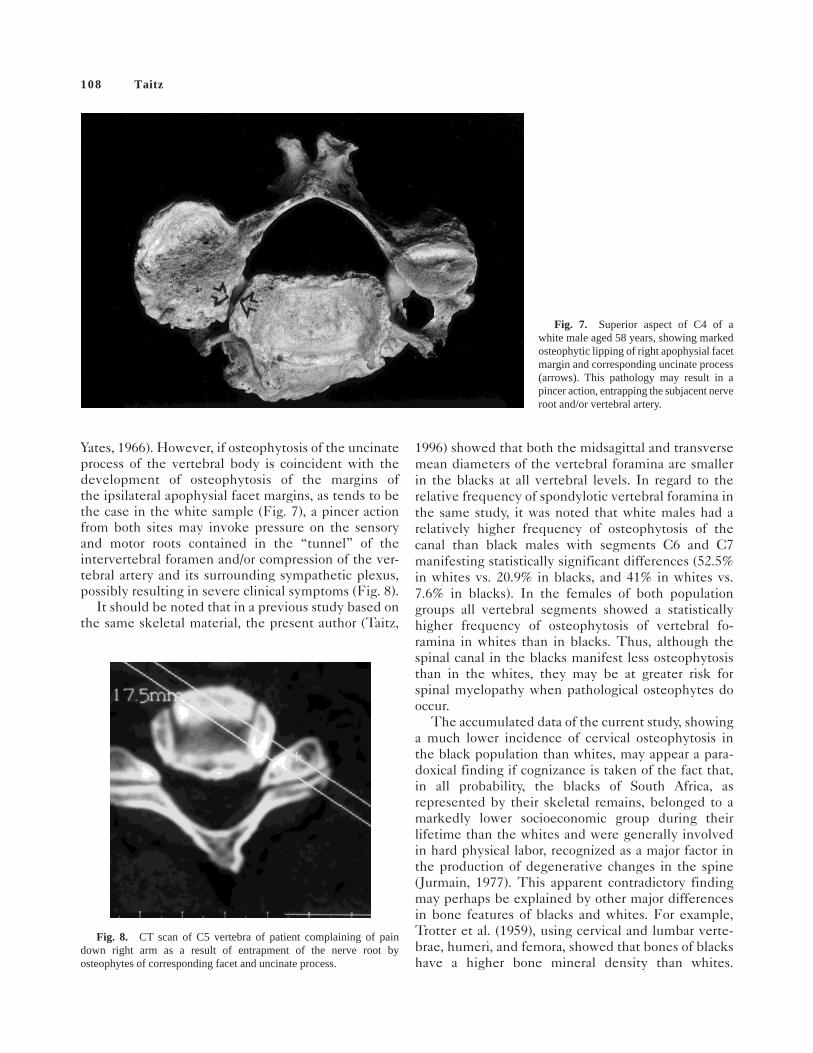
Yates, 1966). However, if osteophytosis of the uncinateprocess of the vertebral body is coincident with thedevelopment of osteophytosis of the margins ofthe ipsilateral apophysial facet margins, as tends to bethe case in the white sample (Fig. 7), a pincer actionfrom both sites may invoke pressure on the sensoryand motor roots contained in the ‘‘tunnel’’ of theintervertebral foramen and/or compression of the ver-tebral artery and its surrounding sympathetic plexus,possibly resulting in severe clinical symptoms (Fig. 8).
It should be noted that in a previous study based onthe same skeletal material, the present author (Taitz,
1996) showed that both the midsagittal and transversemean diameters of the vertebral foramina are smallerin the blacks at all vertebral levels. In regard to therelative frequency of spondylotic vertebral foramina inthe same study, it was noted that white males had arelatively higher frequency of osteophytosis of thecanal than black males with segments C6 and C7manifesting statistically significant differences (52.5%in whites vs. 20.9% in blacks, and 41% in whites vs.7.6% in blacks). In the females of both populationgroups all vertebral segments showed a statisticallyhigher frequency of osteophytosis of vertebral fo-ramina in whites than in blacks. Thus, although thespinal canal in the blacks manifest less osteophytosisthan in the whites, they may be at greater risk forspinal myelopathy when pathological osteophytes dooccur.
The accumulated data of the current study, showinga much lower incidence of cervical osteophytosis inthe black population than whites, may appear a para-doxical finding if cognizance is taken of the fact that,in all probability, the blacks of South Africa, asrepresented by their skeletal remains, belonged to amarkedly lower socioeconomic group during theirlifetime than the whites and were generally involvedin hard physical labor, recognized as a major factor inthe production of degenerative changes in the spine(Jurmain, 1977). This apparent contradictory findingmay perhaps be explained by other major differencesin bone features of blacks and whites. For example,Trotter et al. (1959), using cervical and lumbar verte-brae, humeri, and femora, showed that bones of blackshave a higher bone mineral density than whites.
Fig. 7. Superior aspect of C4 of awhite male aged 58 years, showing markedosteophytic lipping of right apophysial facetmargin and corresponding uncinate process(arrows). This pathology may result in apincer action, entrapping the subjacent nerveroot and/or vertebral artery.
Fig. 8. CT scan of C5 vertebra of patient complaining of paindown right arm as a result of entrapment of the nerve root byosteophytes of corresponding facet and uncinate process.
108 Taitz

Pollitzer and Anderson (1989) confirmed these find-ings and suggested that ethnic-genetic, diet, physicalactivity, and hormones play a causal role in thedifferences of bone density in the two populationgroups. Wright et al. (1995) showed that the secretionof growth hormone is higher in black men than inwhite men and may indeed contribute to a higher bonemineral density in blacks and lower incidence ofosteoporosis and fractures than whites. More recently,Parfitt (1997) showed that the differences in bonedensity are already evident in the fetus and thus have agenetic basis.
Based on the above studies, it could be postulatedthat the higher mineral bone density in skeletons ofthe black sample may, perhaps, indirectly facilitatehigher joint stability, thus reducing the potential forthe development of osteophytes (Professor Zvi Nevo,personal communication).
The differences in site of osteophyte development(i.e., either on the vertebral body, facet or both) in thetwo population groups may be more difficult to ex-plain. In normal circumstances, the apophyseal facets,as opposed to the vertebral bodies, are considered toplay a minimal role in weight-bearing, ,18% accord-ing to White and Panjabi (1978). However, any in-crease in the normal cervical lordosis as a result offunctional stress in the region may cause the facets toplay a more weight-bearing role, thus facilitating thedevelopment of facet osteophytosis. In this regard it isof interest to note that the pathological and radiologi-cal characteristics of osteophytosis of the facet jointsare recorded as similar to those accompanying degen-erative diseases of other weight-bearing synovial articu-lations such as the hip and knee (Sokoloff, 1969).
ACKNOWLEDGMENTS
The author gratefully acknowledges the kindnessand support of Professor P.V. Tobias and staff of theDept. of Anatomy at Wits whilst carrying out the study.
REFERENCESCave AJE, Griffiths JD, Whiteley MM. 1955. Osteo-arthritis
deformans of the Luschka’s joints. Lancet 1:176–185.Davis PR. 1960. Observations on vertebrae in different races.
Anthrop et ethnol Paris 1:443–450.Eisenstein SMF. 1980. The human lumbar vertebral canal: A
study of skeletal material of South African Negroes andCaucasoids with special reference to spinal stenosis, Ph.Dthesis, University of the Witwatersrand, Johannesburg.
Holt S, Yates PO. 1966. Cervical spondylosis and nerve rootlesions. Bone Jt Surg 48B: 407–412.
Jurmain RD. 1977. Stress and the etiology of osteoarthritis. AmJ Phys Anthrop 46:353–366.
Nathan H. 1962. Osteophytes of the vertebral column. J Bone JSurg 44:243–268.
Parfitt AM. 1997. Genetic effects on bone mass and turnover-relevance to black/white differences. J Am Coll Nutr 16:325–333.
Pollitzer WS, Anderson JJB. 1989. Ethnic and genetic differ-ences in bone mass: A review with a hereditary vs environ-mental perspective. Am J Clin Nutr 50:1244–1259.
Resnick D, Niwayama G. 1981. Degenerative disease of thespine. Diagnosis of bone and joint disorders, Vol. 2. Toronto:W.B. Saunders.
Roche MB. 1957. Incidence of osteophytosis and osteoarthritisin 419 skeletonized vertebral columns. Am J Phys Anthrop15:433–434.
Sokoloff L. 1969. The biology of degenerative joint disease.Chicago: University of Chicago Press. 162 p.
Taitz C. 1996. Anatomical observations of the developmentaland spondylotic cervical spinal canal in South African blacksand whites. Clin Anat 9:395–400.
Tobias PV. 1972. Recent human biological studies in SouthernAfrica, with special reference to Negroes and Khoisans.Trans Roy Soc S Afric 40:109–133.
Trotter M, Broman GE, Peterson RR. 1959. Density of cervicalvertebrae and comparison with densities of other bones. AmJ Phys Anthrop 17:19–25.
White AA, Panjabi MM. 1978. Clinical biomechanics of thespine. Philadelphia: Lippincott. 534 p.
Wright NM, Renault J, Willi S, Veldhuis JD, Pandey JP, GordonL, Key LL, Bell NH. 1995. Greater secretion of growthhormone in black than in white men: Possible factor ingreater bone mineral density - A clinical research centerstudy. J Clin Endoc Metabol 80:2291–2297.
Osteophytosis of the Cervical Spine in South African Blacks and Whites 109