old drugs, new tricks - mayo clinic drugs new...old drugs, new tricks dr. christopher arendt,...
TRANSCRIPT

OLD DRUGS, NEW TRICKSDr. Christopher Arendt, PharmD, RPhSenior Clinical ManagerAssistant ProfessorMayo College of MedicineMayo Clinic
HULTON ARCHIVE with permission

OBJECTIVES
Identify several older medications with new uses.
Recognize the obstacles to re-purposing old pharmaceuticals
Describe several resources available to locate off-label indications
2

WHY AREN’T THERE MORE APPROVED INDICATIONS FOR OLD DRUGS?
PatentsFDA RegulationsTrade Secrecy
3Image By USPTO - United States Patent Office, Public Domain

ERROMS LAW4
J. W. Scannell et al. Nature Rev. Drug Discov. 11, 191–200 (2012)

CURRENT CLINICAL EXAMPLES5

BROMOCRIPTINE
FDA Approved indications Acromegaly
Female infertility of pituitary - hypothalamic origin - HyperprolactinemiaHyperprolactinemiaNon-pregnancy related A-G syndromeParkinson's diseaseProlactinomaType 2 diabetes mellitus ( 2009)
T2DM Cycloset 0.8 mg Twice daily with
Food (Titrate to Max 1.6-4.8 mg/day) Take within 2 hrs of waking in morning.
RESULTS: HbA1c reduction ( 0.6-0.7%)
Reduced plasma TG’s and FFA
Advantages over conventional therapy?
No Hypoglycemia
No edema or CHF
No renal adjusting
Weight Neutrality
Reduced Cardiovascular composite end point by 40% ( 52 wk study)
Diabetes Care 2011 Apr; 34(4): 789-794Diabetes Care 2015 Jan; 38(1): 140-149.
6HGP, hepatic glucose production; TG, triglyceride; FFA, Free Fatty Acid.

7Diabetes Care 2011 Apr; 34(4): 789-794Diabetes Care 2015 Jan; 38(1): 140-149.

SALSALATE
FDA Approved indication:Osteoarthritis
Rheumatoid arthritis
OFF-LABEL USE: T2DM
3.5 grams per day ( in 3 divided doses)
HbA1c decreased by 0.37% ( p<0.001)
Targeting Inflammation Using Salsalate in Type 2 Diabetes (TINSAL-T2D)
Dbl blind, placebo controlled. Age 18-75 yo. 286 patients. HbA1c levels 7-9.5%. 48 weeks.
88.1% on Metformin
52% on Insulin secretagogue
15% on Dipeptidyl pertidate 4 inhibitor
41% on Single agent, 49% on Dual therapy, 5.6% on Triples, and 4.5 % on lifestyle modification aloneAnn Intern Med. 2013;159:1-12
Diabetes Care 2013;36:4132–4139
8

9Ann Intern Med. 2013;159:1-12Diabetes Care 2013;36:4132–4139

IVERMECTIN
FDA Approved indications: Infection by Onchocerca volvulus, non-adult stage
(Adults and Peds) OralIntestinal strongyloidiasis (Adults and Peds)-OralPediculosis capitis (Peds) LotionRosacea, Inflammatory lesions (Adults)-Cream
Off-Label uses Ascariasis
Cutaneous larva migransDermatosis due to mitesEnterobiasisHemopoietic stem cell transplant - Infection by Strongyloides stercoralis; ProphylaxisInfection by Loa loaInfection by Wuchereria bancroftiInfestation by Phthirus pubisMansonelliasisScabies [ See N Engl J Med 2010; 362:717-725February 25, 2010]
Trichuriasis
MalariaJ Eur Acad Dermatol Venereol. 2016 May;30(5):829-36
10

PROPRANOLOL
FDA Approved indications: Angina pectoris, chronic
Capillary hemangiomaCardiac dysrhythmiaEssential tremorHypertensionIdiopathic hypertrophic subaorticstenosisMigraine; ProphylaxisPheochromocytoma; AdjunctPostmyocardial infarction syndrome
Infantile Haemangiomas ( 2015)
OFF-LABEL uses: Aggressive behavior
Cataplexy - NarcolepsyDiabetes mellitus - HypertensionMigraineOphthalmoplegic migrainePostmyocardial infarction syndrome
AnxietyAortic aneurysmBurn, Post-event hypermetabolismCongenital long QT syndromeCongestive heart failureGastrointestinal hemorrhageHeart failurePercutaneous coronary interventionPortal hypertensionSupraventricular tachycardia, Prophylaxis and treatment in infantsTetralogy of FallotThyroid stormThyrotoxicosisVasovagal syncope; Prophylaxis
11

Propranolol dosing in Infantile Hemangioma Age 5 weeks-5 months 3.4 mg/kg in 2 divided doses daily for 6
months Week 1 – starting dose is (0.6 mg/kg/dose)
twice daily Week 2 – increase dose to (1.1 mg/kg/dose)
twice daily Week 3 – increase to a maintenance dose to
(1.7 mg/kg/dose) twice daily Administer twice daily doses at least 9 hours
apart during or after feeding Readjust dose for changes in the child’s
weight Monitor heart rate and blood pressure for 2
hours after the first dose or increasing dose Duration of treatment: 6 months
Give with Feedings ( To reduce risk of Hypoglycemia)
ADR: Sleep Disorders ( insomnia) Diarrhea Vomiting Aggravated respiratory tract
infections
Use of the 20 mg/5 mL solution or 40 mg/5 mL solution vs 4.28 mg/mL solution.
12

OXYBUTYNIN
FDA Approved indications: Bladder muscle dysfunction
- overactiveNeurogenic bladder
Off-Label Bladder pain, Catheter-related
Hot sweats, RefractoryNocturnal Enuresis 5 to 10 mg at bedtime
Hyperhidrosis 2.5 mg daily x 1 week
2.5 mg Twice daily x 2 weeks
5 mg Twice daily thereafter
ADR: Dry mouth, Constipation and drowsiness
Skin Appendage Disord 2015;1:6-13J Vasc Surg 2012;55:1696-1700Ann Vasc Surg 2014;28:1106-1112. Pediatr Dermatol 2014;31:48-53
Pediatr Nephrol. 2001 Aug; 16(8):662-4.J Urol. 2005 Sep; 174(3):1084-7.J Urol. 2001;166(6):2459–62.Urol Clin North Am. 2004 Aug; 31(3):491-8, ix.
13

RITUXIMAB
FDA Approved indications: Chronic lymphoid leukemia, In combination with
fludarabine and cyclophosphamide Microscopic polyarteritis nodosa, In combination with glucocorticoidsNon-Hodgkin's lymphoma, Diffuse, large B-cell, CD20-positive, in combination for first-line treatmentNon-Hodgkin's lymphoma, Follicular, CD20-positive, B-cell, in combination with first-line chemotherapy & as single-agent maintenanceNon-Hodgkin's lymphoma, Low-grade, CD20-positive, B-cell, stable or responsive to prior CVP (cyclophosphamide, vincristine, and prednisone) chemotherapyNon-Hodgkin's lymphoma, Relapsed or refractory, low-grade or follicular, CD20-positive, B-cellRheumatoid arthritis (Moderate to Severe), In combination with methotrexate, in patients who had an inadequate response to one or more tumor-necrosis-factor antagonist therapiesWegener's granulomatosis, In combination with glucocorticoids
OFF-Label Uses: Acquired factor VIII deficiency disease
Autoimmune hemolytic anemiaB-cell lymphomaChronic lymphoid leukemia, In combination for first-line treatmentChronic lymphoid leukemia, Relapsed or refractoryEpstein-Barr virus disease; Prophylaxis - Hemopoietic stem cell transplantEvans syndrome, Refractory to immunosuppressive therapyGraft-versus-host disease, chronic, Steroid-refractoryHairy cell leukemiaHodgkin's disease, CD20-positive, as monotherapyIdiopathic thrombocytopenic purpuraImmune thrombocytopenia, Previously treatedMalignant ascites - Non-Hodgkin's lymphomaMantle cell lymphoma, Untreated, induction therapy, in combination with anthracycline-based regimensMinimal change disease, Refractory, steroid-dependent or steroid-resistantMyasthenia gravis, RefractoryPemphigus vulgarisPost-transplant lymphoproliferative disorderPrimary cutaneous B-cell lymphomaPrimary Sjögren's syndromeRelapsing remitting multiple sclerosisRheumatoid arthritis, In combination with methotrexate, in patients with an inadequate response to methotrexateSystemic lupus erythematosus, Refractory to immunosuppressive therapy; AdjunctThrombotic thrombocytopenic purpura, In combination with steroids and plasma exchangeWaldenström macroglobulinemia
Myalgic encephalomyelitis/Chronic fatigue syndrome.
14

BACLOFEN
FDA Approved Indication: Spasticity
Off-Label Uses: Alcohol withdrawal syndrome
DystoniaHiccoughs, IntractablePeripheral neuropathy, Chemotherapy-inducedStiff-man syndromeTrigeminal neuralgia
Refractory GERD 10 mg daily, increased to 20 mg Three times
daily as tolerated.
ADR: Drowsiness, Dizziness
Aliment Pharmacol Ther 2012; 35: 1036–1044Aliment Pharmacol Ther 2003; 17:243.J Pediatr 2006; 149:468.Gut 2003; 52:1397.
15

POPULATION WITH THE MOST “OFF LABEL USE”
Pediatrics
16

Benefit
No Benefit
Adverse Effects
Photo Warner –Dirty Harry 1971
17

J Pediatr Pharmacol Ther. 2016 Jan-Feb;): 36–53.
Strong Evidence
18

J Pediatr Pharmacol Ther. 2016 Jan-Feb;): 36–53.
Strong Evidence
19

J Pediatr Pharmacol Ther. 2016 Jan-Feb;): 36–53.
Intermediate Evidence
20
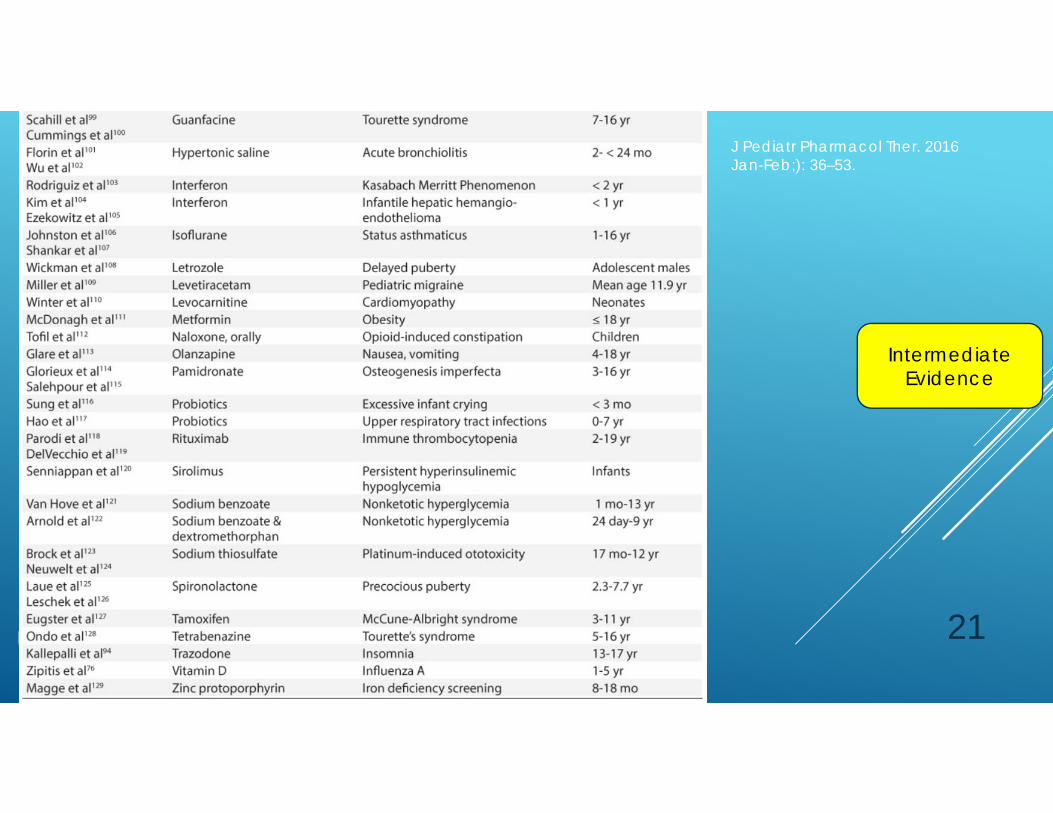
J Pediatr Pharmacol Ther. 2016 Jan-Feb;): 36–53.
Intermediate Evidence
21

Weak Evidence
J Pediatr Pharmacol Ther. 2016 Jan-Feb;): 36–53.
22

Pediatric AND Adult Drug Information
All provide OFF-LABEL indications, as well as
FDA approved
• Micromedex• Epocrates
23

PHARMACOGENOMICS
24

CLINICAL CASES- AUDIENCE RESPONSE
25

JT a 58 yo Farmer from central Iowa has Pustular Rosacea.
He has been on Metronidazole Cream for 6 months, and has not seen much improvement.
Should he…A. Start Ivermectin 1% Cream once
dailyB. Start Doxycycline 100 mg twice dailyC. Invest in a ski mast company.
26
ML is a 45 yo Accountant who likes her sweets. Her glucose intolerance has been growing steadily.
She is on Metformin and Glimepiride. She was started on Bromocriptine by a specialist looking for alternative approaches.
Which of the following is true:A. You can expect to see more
Hypoglycemia compared to other agents.
B. It is contraindicated in CHFC. It can reduce A1c 0.6-0.7%
27

SUMMARY
New analytics are helping us discover new indications for older medications in a shorter time frame at lesser research expense.
While the pipeline is growing, we still have many needs for off-label uses of medications, and many products may never have FDA reviewed approval.
There are many drug information resources available with OFF-label medication use references. Practitioners should cautiouslyevaluate the evidence surrounding any medication and its use in their patient.
Future use of pharmacogenomicbased clinical decision support tools may improve or enhance our use of older and newer medications.
28

OLD DRUGS, NEW TRICKSDr. Christopher Arendt, PharmD, RPhSenior Clinical ManagerAssistant ProfessorMayo College of MedicineMayo Clinic
Photo: Archives of Bayer AG