(ohio state's 2016 ash review) ash 2015 review – lymphoma abstracts
TRANSCRIPT

ASH 2015 REVIEW – LYMPHOMA ABSTRACTS
Kristie A. Blum, MD Professor of Medicine The Ohio State University

• MCL • DLBCL • FL • HL
Key Abstracts for each of these 4 lymphoma subtypes
Overview
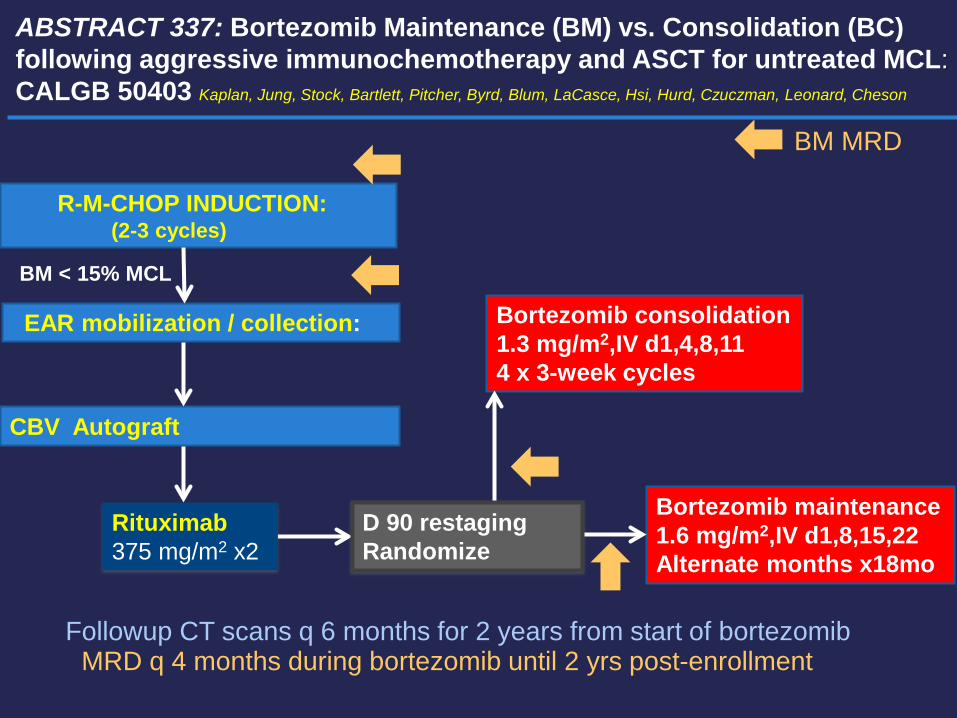
ABSTRACT 337: Bortezomib Maintenance (BM) vs. Consolidation (BC) following aggressive immunochemotherapy and ASCT for untreated MCL: CALGB 50403 Kaplan, Jung, Stock, Bartlett, Pitcher, Byrd, Blum, LaCasce, Hsi, Hurd, Czuczman, Leonard, Cheson
Bortezomib consolidation 1.3 mg/m2,IV d1,4,8,11 4 x 3-week cycles
Bortezomib maintenance 1.6 mg/m2,IV d1,8,15,22 Alternate months x18mo
R-M-CHOP INDUCTION: (2-3 cycles)
EAR mobilization / collection:
CBV Autograft
Rituximab 375 mg/m2 x2
Followup CT scans q 6 months for 2 years from start of bortezomib
BM MRD
BM < 15% MCL
D 90 restaging Randomize
MRD q 4 months during bortezomib until 2 yrs post-enrollment

Enrolled 151 (10/06-6/10)
AE 7 Patient withdrawal 1 Other therapy 1 Progression / NR 6 Other 5
Transplanted 118
Randomized 102
80% AE: 5 Treatment-related death 2 Progression: 2 Ineligible (cytopenia/PFTs) 4 Refused 3
Chemo-immunotherapy 147 Never treated 4
Mobilization 127 AE 3 Progression 2 Death 2 Patient withdrawal 1 Other 1
CALGB 50403: Consort Diagram
69%
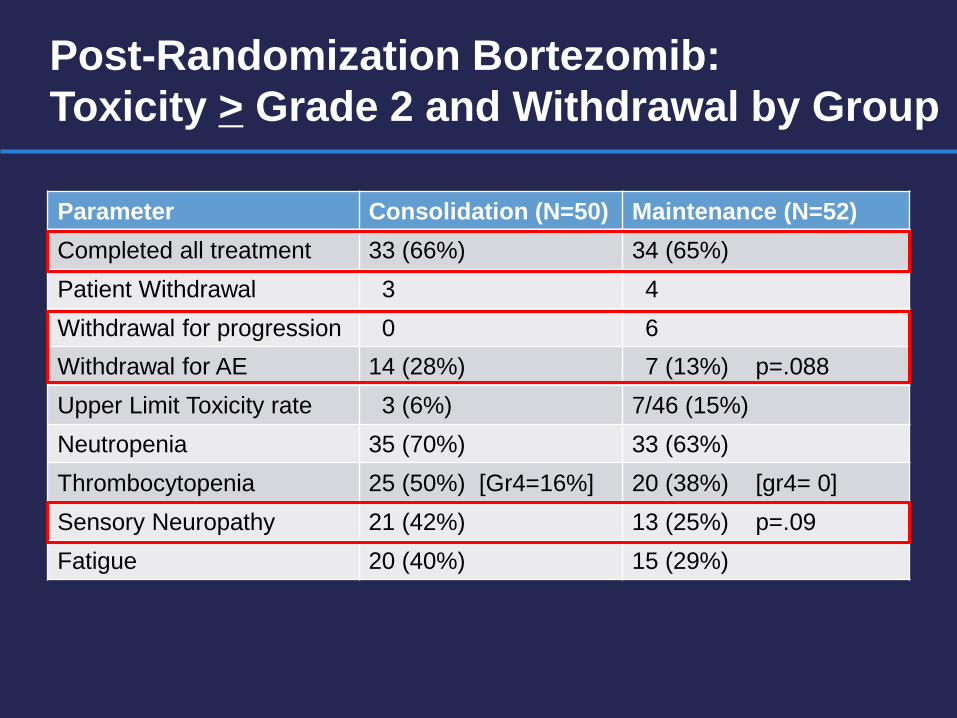
Post-Randomization Bortezomib: Toxicity > Grade 2 and Withdrawal by Group
Parameter Consolidation (N=50) Maintenance (N=52) Completed all treatment 33 (66%) 34 (65%) Patient Withdrawal 3 4 Withdrawal for progression 0 6 Withdrawal for AE 14 (28%) 7 (13%) p=.088 Upper Limit Toxicity rate 3 (6%) 7/46 (15%) Neutropenia 35 (70%) 33 (63%) Thrombocytopenia 25 (50%) [Gr4=16%] 20 (38%) [gr4= 0] Sensory Neuropathy 21 (42%) 13 (25%) p=.09 Fatigue 20 (40%) 15 (29%)

CALGB 50403: PFS Primary Endpoint with CALGB 59909 (no bortezomib)
Comparison p-value Maintenance vs 59909 0.094 (log-rank) Consolidation vs 59909 0.035
• Median PFS >4 years
• Each arm compared w/ 59909 • ITT analysis from entry • Includes 45 non-randomized • Median follow up: 5.5 yr • 6 year PFS: • Maintenance: 58% (44-69) • Consolidation: 64% (50-65)
(1-sample log-rank)

Progression-Free survival from Study Entry: All Patients CALGB 50403 vs 59909
MIPI Score 50403 (n=147) 59909 (n=78) Low 77 (52.4%) 41 (53.2%) Intermediate 45 (30.6%) 24 (31.2%) High 25 (17.1%) 12 (15.6%)
5 yr 72.7%
Years from Study Entry
Prop
ortio
n Pr
ogre
ssio
n-fre
e
0 2 4 6 8
0.0
0.2
0.4
0.6
0.8
CALGB 59909CALGB 50403
N= 78N= 147
Events= 35Events= 52
p-value= 0.0264
• 50403 5 yr : 64% (55-71) • 59909 5 yr : 52% (39-64) • p=0.0026
PFS from study entry, ITT

Years from Study Entry
Pro
babi
lity
Pro
gres
sion
-free
0 2 4 6 8
0.0
0.2
0.4
0.6
0.8
NegativePositive
N= 17N= 25
Events= 3Events= 13
p=0.0169
5 yr PFS 88%
5 yr PFS 51%
p=.017
Progression free and Overall survival by MRD post-induction (Median Follow-up 5.5yr)
MRD-
MRD+
MRD-
MRD+
Progression-free survival Overall Survival
p=.0023
MRD- : n=17 MRD+ : n=25

ABSTRACT 339: Bortezomib maintenance after induction with RCHOP, ARA-C, and ASCT in newly diagnosed MCL, results of a multi-center phase 2 HOVON trials Doorduijn, Minnema, Kersten, Lugtenburg, Schipperus, van Marwijk Kooy, MacKenzie, Zijlstra, Berenschot, Schaafsma, Chitu, Kluin-Nelemans
RCHOP (3 cycles) 140
R-ARAC (2 cycles) 138
BEAM Autograft 115 (85%)
Observation 30 Bortezomib 30 1.3 mg/m2 qow x 2 years
• N= 140 patients (34-66) • MIPI – Low (57%) Intermediate (32%) High (10%) • Only 60 randomized to bortezomib or observation • Median follow-up – 50.9 months • 4-year EFS all patients 61% • 4 year OS all patients is 78% • 4-year EFS with bortezomib 72% • 4-year EFS without bortezomib 71%
• Issues: Low dose of bortezomib
Small numbers

R-HCVAD cycle 1 R-MTX/Ara-C cycle 2
R-Bendamustine x 4 cycles
<PR OFF Study
≥PR
R-Cyclophosphamide
Stem Cell Collection
Restaging Restaging
<PR OFF Study
≥PR
R-HCVAD Cycle 3 Stem cell collection
R-MTX/Ara-C cycle 4
R-bendamustine x 2 cycles
Restaging
<61 yrs: CBV, BEAM or TBI/VP16/Cy 61-65 yrs: CBV or BEAM
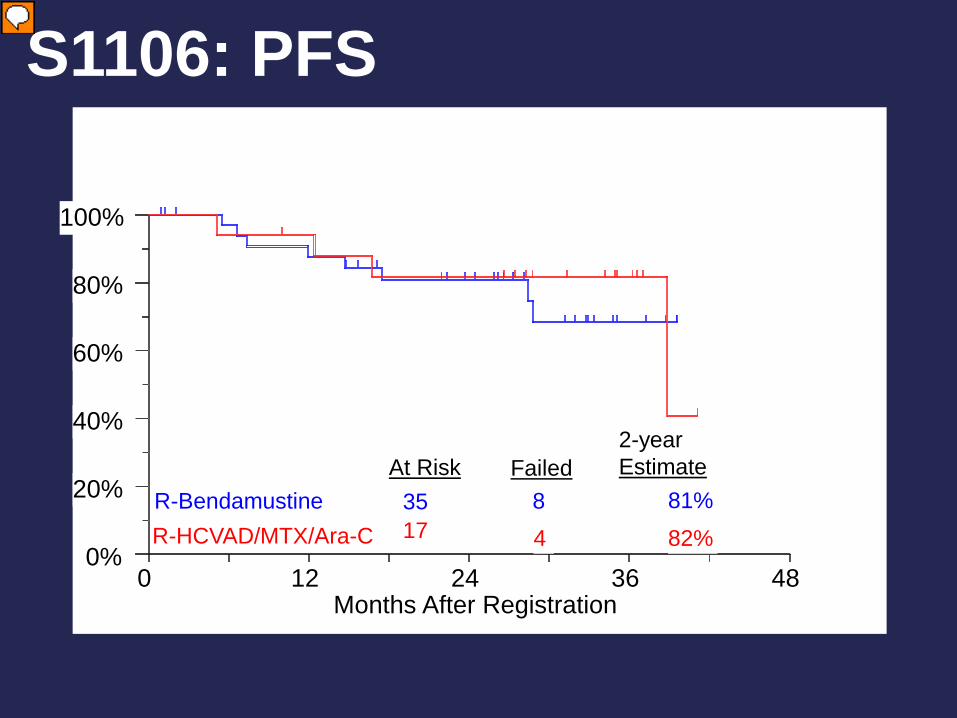
ABSTRACT 518: Pre-Transplant R-Bendamustine Induces High Rates of Minimal Residual Disease in MCL Patients: Updated Results of S1106: US Intergroup Randomized Phase II Trial of R-HCVAD Vs. R-Bendamustine Followed By ASCT for MCL Chen, Li, Bernstein, Rimsza, Forman, Constine, Shea, Cashen, Blum, Fenske, Barr, Leblanc, Fisher, Cheson, Smith, Faham, Wilkins, Leonard, Kahl, Friedberg

S1106 Results N= 51 evaluable
R-HyperCVAD (N=17)
R-Bendamustine (N=35)
Response ORR CR PR Inadequate
94.1%
35% 59%
6%
82.9%
40% 43% 17%
Median F/U (months) 34 (10.0-41.0) 27.3 (1-39.5)
Survival 2-year PFS 2-year OS
82% 88%
81% 87%

Reasons for not going on to ASCT
R-HyperCVAD (17) 12/17
R-Bendamustine (35) 14/35
Failure to collect 5 2 Thrombocytopenia 5 Patient choice 4 Progressive disease 2 Pancytopenia 1 Neutropenia 1 Allergy 1 Seizure 1 Insurance denial 1 Others 1 2
S1106 - Off-Treatment
R-HyperCVAD - 9 (53%) transplanted, 4 off protocol R-Bendamustine - 23 (66%) transplanted, 2 off protocol
0%
20%
40%
60%
80%
100%
0 12 24 36 48 Months After Registration
R-Bendamustine R-HCVAD/MTX/Ara-C
At Risk 35 17
Failed 8 4
2-year Estimate
81%
82%
S1106: PFS

S1106 MRD results • R-HyperCVAD (n = 2):
• 2/2 MRD positive at baseline and achieved MRD negative status
• R-Bendamustine (n = 10): • 8/9 (89%) patients with baseline positive MRD converted to
MRD negative status.
• 3 additional patients were missing MRD status at baseline but were MRD negative status post induction.
• 2 year PFS is 100% for all 11 patients MRD negative at end of induction. (3 did not go to ASCT)
• 1 patient MRD negative at baseline and remained negative at end of induction (PD)

Current Directions R
A N
D O
M I
Z A
T I
O N
BR x 6
BVR x 6
BR x 6
BVR x 6
Rituximab
Rituximab
Lenalidomide + Rituximab
Lenalidomide + Rituximab
E1411: N ~328 (82 eligible per arm)
B = bendamustine, V = bortezomib
1) Should MRD analysis be an primary endpoint in Induction trials in MCL?
2) Do MRD negative patients after induction chemotherapy benefit from ASCT or maintenance therapy?

RAN
DO
MIZ
ATIO
N
MRD assessment
MRD- CR
PR or MRD+ CR
ASCT + R maintenance
ASCT + R maintenance
RAN
DO
MIZ
ATIO
N
Backbone
Backbone + Drug X
Backbone + Drug Y
Backbone could be: • Intensive Ara-c-containing regimen • R-bendamustine Drug X, Y, etc. could be: BTK inhibitor, Bcl-2 inhibitor, PI3Ki, CDKi, etc.
Phase II Goal: increase MRD-negative rate from 70% to 90%
R maintenance
Phase III Superiority Design: 5 year OS of 85% vs 76% among patients who were MRD-negative after induction
Could do sequential 2-arm trials Or a single multi-arm trial
FUTURE DIRECTIONS: US INTERGROUP AND NCIC TRIALS
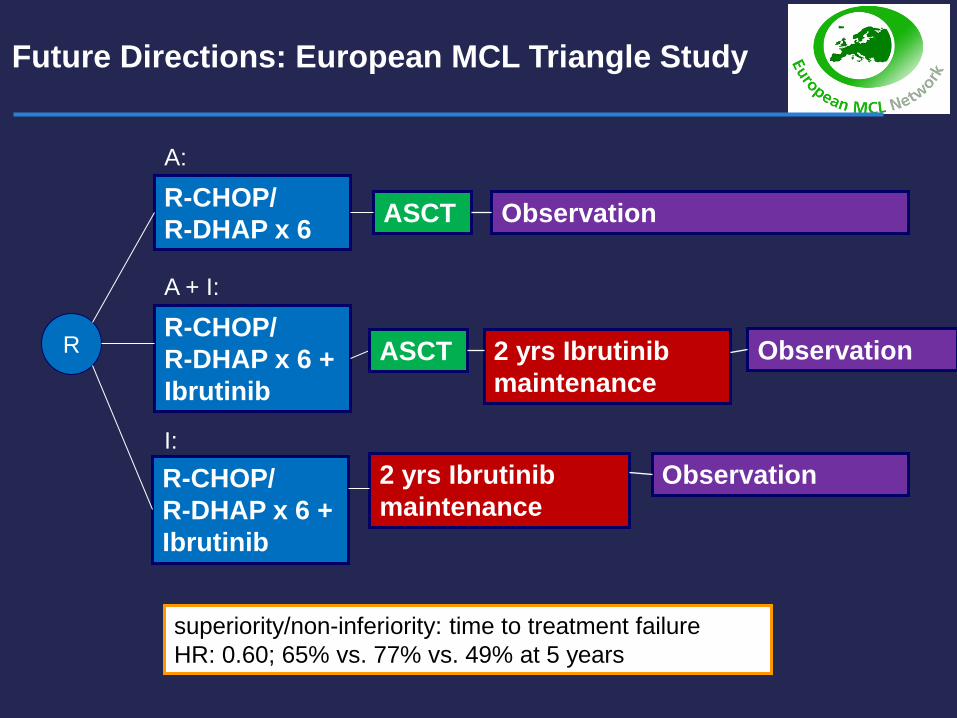
Future Directions: European MCL Triangle Study
Observation R-CHOP/ R-DHAP x 6 ASCT
2 yrs Ibrutinib maintenance
2 yrs Ibrutinib maintenance
R R-CHOP/ R-DHAP x 6 + Ibrutinib
R-CHOP/ R-DHAP x 6 + Ibrutinib
ASCT Observation
Observation
A:
A + I:
I:
superiority/non-inferiority: time to treatment failure HR: 0.60; 65% vs. 77% vs. 49% at 5 years

Outcomes for patients relapsing/progressing on ibrutinib
Cheah, Ann Onc, 26, 2015 ● 42 discontinued ibrutinib (or R-ibrutinib) 19% primary progression 47% relapsed 14% AE 10% transplant 10% patient choice ● Median 6.5 cycles (1-43) ● 31 patients salvage with ORR 32% regardless of regimen – HyperCVAD,bendamustine lenalidomide, bortezomib ● MEDIAN OS 8.4 months
• Martin, Hematol Onc, abstr. 207, 2015
● 114 discontinued ibrutinib 32% primary progression 54% relapsed 2% AE 1% patient choice ● Median 4.7 cycles (0.7-43.6) ● 73 patients salvage with ORR 36% no differences in median
OS with any specific regimen – cytarabine, bendamustine, lenalidomide ● MEDIAN OS 2.9 months
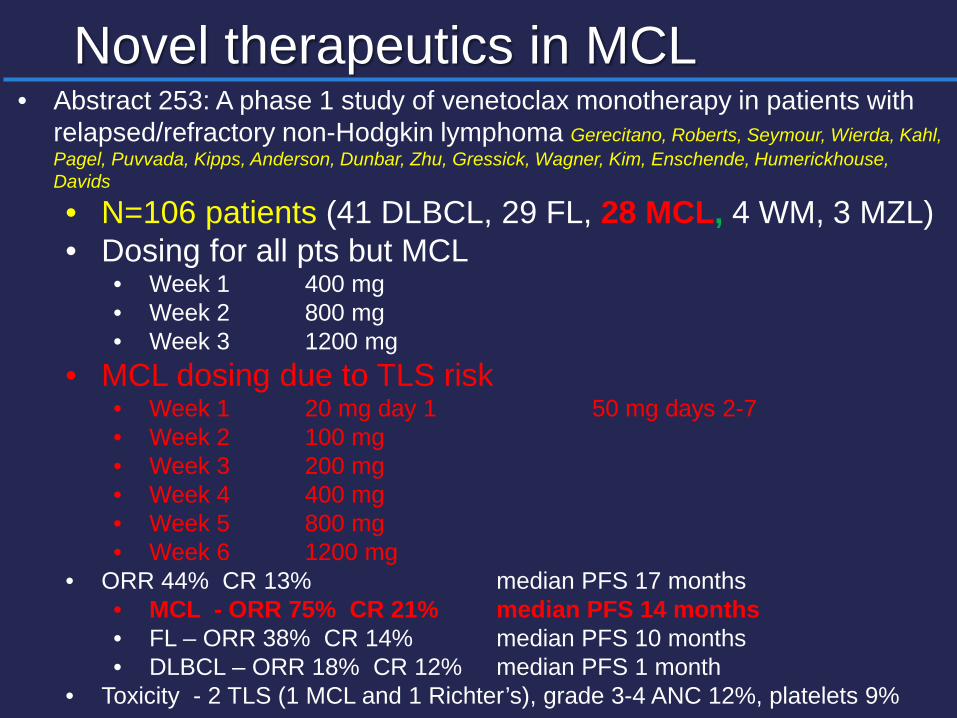
Novel therapeutics in MCL • Abstract 253: A phase 1 study of venetoclax monotherapy in patients with
relapsed/refractory non-Hodgkin lymphoma Gerecitano, Roberts, Seymour, Wierda, Kahl, Pagel, Puvvada, Kipps, Anderson, Dunbar, Zhu, Gressick, Wagner, Kim, Enschende, Humerickhouse, Davids
• N=106 patients (41 DLBCL, 29 FL, 28 MCL, 4 WM, 3 MZL) • Dosing for all pts but MCL
• Week 1 400 mg • Week 2 800 mg • Week 3 1200 mg
• MCL dosing due to TLS risk • Week 1 20 mg day 1 50 mg days 2-7 • Week 2 100 mg • Week 3 200 mg • Week 4 400 mg • Week 5 800 mg • Week 6 1200 mg
• ORR 44% CR 13% median PFS 17 months • MCL - ORR 75% CR 21% median PFS 14 months • FL – ORR 38% CR 14% median PFS 10 months • DLBCL – ORR 18% CR 12% median PFS 1 month
• Toxicity - 2 TLS (1 MCL and 1 Richter’s), grade 3-4 ANC 12%, platelets 9%

DLBCL - ABSTRACT 811: Randomized phase 2 study of RCHOP + Bortezomib in Untreated Non-Germinal Center type DLBCL: PYRAMID TRIAL Leonard, Kolibaba, Reeves, Tulpule, Flinn, Lolevska, Robles, Flower, Collins, DiBella, Papish, Venugopal, Horodner, Tabatabai, Hajdenberg, Mulligan, Neuwirth, Suryanaranyan, Esseltine, de Vos
Arm A (n=95) R-CHOP 21 X 6 cycles Bortezomib 1.3 mg/m2
IV, Days 1 and 4
Arm B (n=95) R-CHOP 21 X 6 cycles
Non-GCB Selection
Previously untreated
DLBCL • Measurable
disease • ECOG PS 0–2
IHC algorithm Assay/scoring in real
time at central US lab* Hans method1
(CD10, bcl-6, MUM-1) 48–72 hour turnaround Retrospective
molecular analyses of RNA patterns, DNA mutations
R A N D O M I Z E
*Local IHC testing by certified local pathologits was also employed, confirmed by central review;

Best Overall response rate*
53% (R-CHOP) and 59% (VR-CHOP) of patients had a negative FDG-PET result† at the end-of-treatment visit
R-CHOP (n=86) VR-CHOP (n=90)
Perc
ent o
f pat
ient
s
49
98
56
96
CR CR/PR
1. Cheson BD, et al. J Clin Oncol. 2007;25:579–86
*Response-evaluable population (confirmed non-GCB DLBCL, measureable disease and at least one post-baseline response assessment); response assessments based on the 2007 Revised Response Criteria for Malignant Lymphoma1; †Investigator-assessed
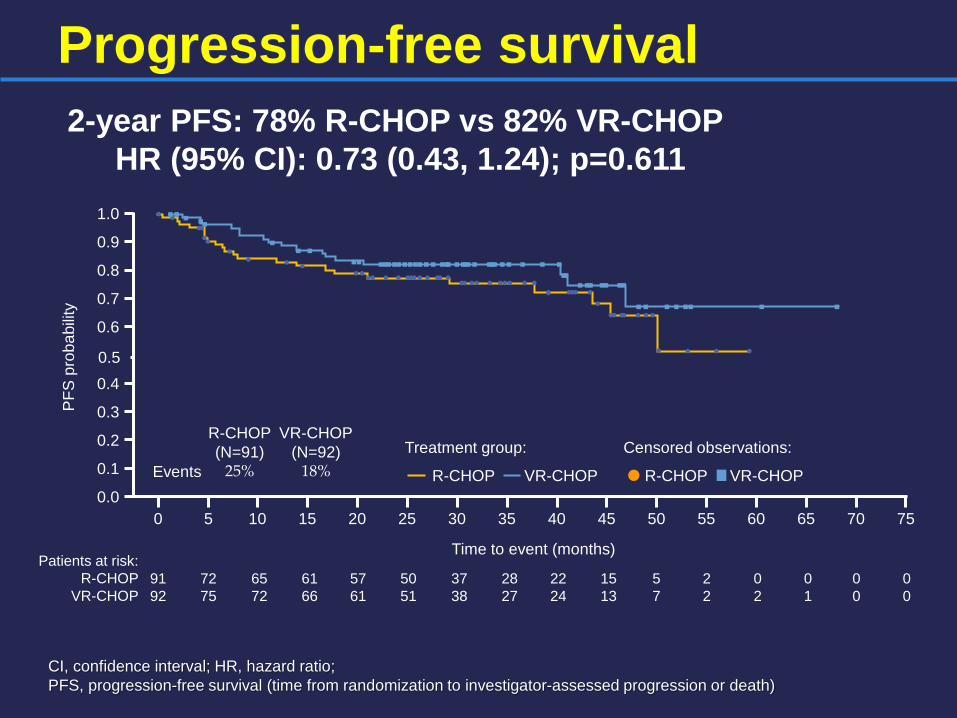
Progression-free survival
CI, confidence interval; HR, hazard ratio; PFS, progression-free survival (time from randomization to investigator-assessed progression or death)
Patients at risk: R-CHOP
VR-CHOP
PFS
pro
babi
lity
Time to event (months)
0.0
0.1
0.2
0.3
0.4
0.6
0.7
0.8
0.9
1.0
0 5 10 15 20 25 30 35 50 55 60 65 70 75 40 45
91 92
72 75
65 72
61 66
57 61
50 51
37 38
28 27
5 7
2 2
0 2
0 1
0 0
0 0
22 24
15 13
Treatment group: Censored observations:
R-CHOP VR-CHOP R-CHOP VR-CHOP
R-CHOP (N=91)
25% Events
VR-CHOP (N=92)
18%
0.5
2-year PFS: 78% R-CHOP vs 82% VR-CHOP HR (95% CI): 0.73 (0.43, 1.24); p=0.611
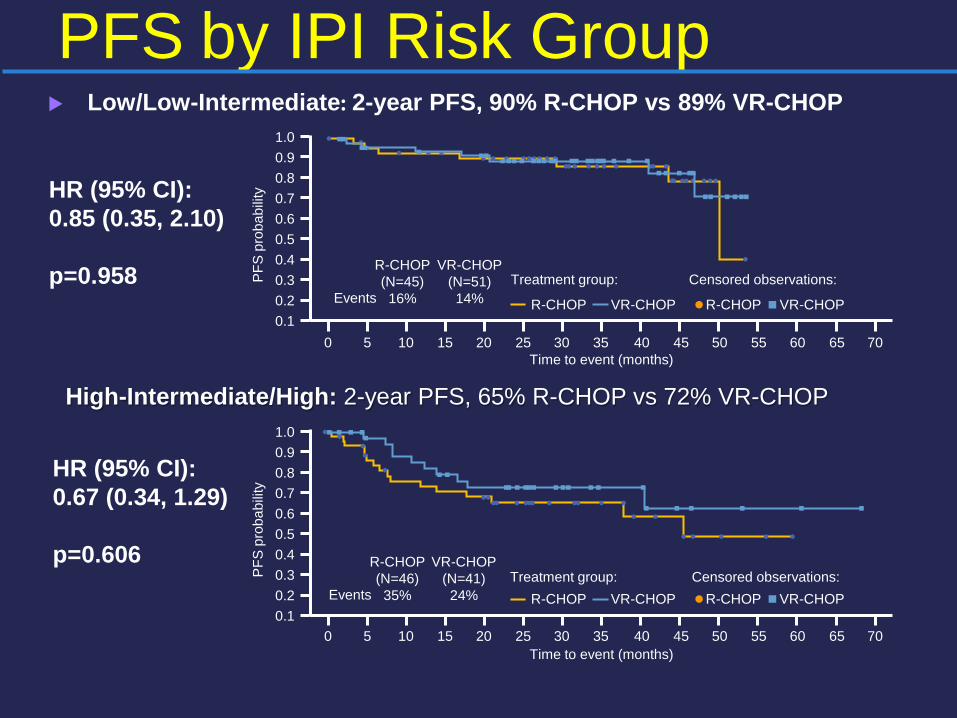
Low/Low-Intermediate: 2-year PFS, 90% R-CHOP vs 89% VR-CHOP
PFS by IPI Risk Group
HR (95% CI): 0.85 (0.35, 2.10) p=0.958
HR (95% CI): 0.67 (0.34, 1.29) p=0.606
PFS
pro
babi
lity
1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 Time to event (months)
PFS
pro
babi
lity
1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70
Treatment group: Censored observations: R-CHOP VR-CHOP R-CHOP VR-CHOP
Treatment group: Censored observations:
R-CHOP (N=46) 35% Events
VR-CHOP (N=41) 24%
R-CHOP (N=45) 16% Events
VR-CHOP (N=51) 14%
Time to event (months)
R-CHOP VR-CHOP R-CHOP VR-CHOP
High-Intermediate/High: 2-year PFS, 65% R-CHOP vs 72% VR-CHOP

Overall survival 2-year OS: 88% R-CHOP vs 93% VR-CHOP
- HR (95% CI), 0.75 (0.38, 1.45); p=0.763
OS, overall survival (time from randomization to death)
Patients at risk: R-CHOP
VR-CHOP
Time to event (months)
91 92
82 88
80 85
75 83
73 80
64 68
47 49
35 38
6 13
3 4
0 3
0 1
0 0
0 0
28 33
20 23
OS
pro
babi
lity
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Treatment group: Censored observations:
R-CHOP VR-CHOP R-CHOP VR-CHOP
R-CHOP (N=91)
15% Events
VR-CHOP (N=92)
12%
0 5 10 15 20 25 30 35 50 55 60 65 70 75 40 45

R-CHOP in ABC/Non-GCB (Other trials) • Retrospective (Lenz, NEJM 359: 2313-2323, 2008)
• 2-year PFS 40% ABC by GEP with R-CHOP • Higher PFS rates for GCB vs ABC subtype (P<0.001)
• Prospective (Offner, Blood 126: 1893-1901, 2015)
• 2-year PFS 77.1% non-GCB by IHC with R-CHOP • 2-year PFS 76% non-GCB by IHC with VR-CAP (Bortezomib + RCHOP
without vincristine) • 2-year OS were 80.1 and 79% with VR-CAP and RCHOP

R-CHOP in ABC/Non-GCB (Other trials) Abstract 812: Prospective randomized trial of targeted therapy for DLBCL based on real-time GEP: Remodl-B trial of UK and SAKK lymphoma groups Davies, et al. • RCHOP x 1 central GEP on FFPE LN randomization to
RCHOP + bortezomib 1.6 mg/m2 days 1 & 8 or RCHOP x 5 • N= 1132 patients (246 ABC (27%), 476 GCB (52%), 199
unclassifiable)
• No difference in ORR in ABC patients with RCHOP or BR-CHOP • No difference in ORR in GCB patients with RCHOP or BR-CHOP • No differences in PFS of ABC and GCB patients, 2-year PFS 71% • Still awaiting 30 months of f/up which was primary endpoint
Subtype ORR CR ABC 90% 66% GCB 87% 63%
Follicular lymphoma: Ibrutinib
Bartlett, ASH annual meeting abstracts no. 800, 2014 • Phase 2 multi-center ibrutinib trial, 40 patients with FL, 38 evaluable
• ORR 28% (2 CR and 9 PR) • 65% had reduction in tumor size at median f/up of 10.2 months • Median time to response 2.8 months • Median PFS 9.9 months
Maddocks, Blood 125:242-248, 2015 • Phase 1 of R-bendamustine + ibrutinib • 12 FL; ORR 90% (5 CR and 4 PR) • Median PFS not yet reached • 7 of 12 FL patients had grade 3 rash on this trial, & 2 couldn’t tolerate re-challenge
Fowler, ASH annual meeting abstracts no. 623, 2012 • Phase 1 ibrutinib trial, 16 patients with FL, 11 eligible for efficacy
• ORR 54.5% (3 CR and 3 PR) at doses > 2.5 mg/kg/day • Median DOR 12.3 months • Median PFS 13.4 months
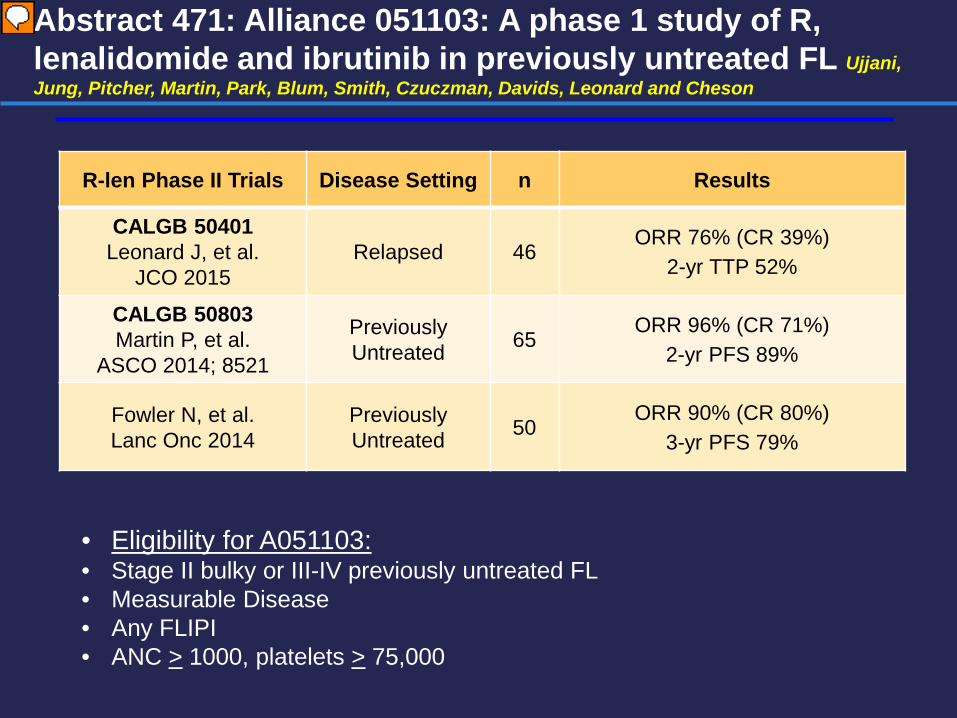
Abstract 471: Alliance 051103: A phase 1 study of R, lenalidomide and ibrutinib in previously untreated FL Ujjani, Jung, Pitcher, Martin, Park, Blum, Smith, Czuczman, Davids, Leonard and Cheson
R-len Phase II Trials Disease Setting n Results
CALGB 50401 Leonard J, et al.
JCO 2015 Relapsed 46
ORR 76% (CR 39%) 2-yr TTP 52%
CALGB 50803 Martin P, et al.
ASCO 2014; 8521
Previously Untreated 65
ORR 96% (CR 71%) 2-yr PFS 89%
Fowler N, et al. Lanc Onc 2014
Previously Untreated 50
ORR 90% (CR 80%) 3-yr PFS 79%
• Eligibility for A051103: • Stage II bulky or III-IV previously untreated FL • Measurable Disease • Any FLIPI • ANC > 1000, platelets > 75,000

Dosing Schema
Dose Level Cohorts Dose Level Lenalidomide Ibrutinib
Level -2 5 mg 280 mg Level -1 10 mg 420 mg
Level 0 (n=3) 15 mg 420 mg Level 1 (n=3) 15 mg 560 mg Level 2 (n=16) 20 mg 560 mg
Lenalidomide Days 1-21 for 18 cycles
1 2 3 4 5 6 7 8 9 10 11 18 19 PD
Rituximab 375 mg/m2 x 8 doses
Cycle
Ibrutinib daily until progression (PD)
*Allopurinol for TLS prophylaxis, Aspirin for DVT prophylaxis with lenalidomide
(28 days)
RP2D/NO DLT
Compared to R-Len in front-line, there was increased: • Rash (36% gr. 3) • Diarrhea • Arthralgia • Neoplasm
• Cutaneous (2) • Carcinomas (3)

• Median time to first response: 2.3 months (1.9-11.1) • Median time to best response: 5.5 months (1.9-20.2) * 8 patients who achieved a negative PET/CT did not
undergo confirmatory bone marrow biopsy
Response
Overall (n = 22)
DL 0 (n = 3)
DL 1 (n = 3)
DL 2 (n = 16)
ORR 95% 100% 100% 94%
CR* 63% 67% 33% 69%
PR 32% 33% 67% 25%
SD 5% 0 0 6%
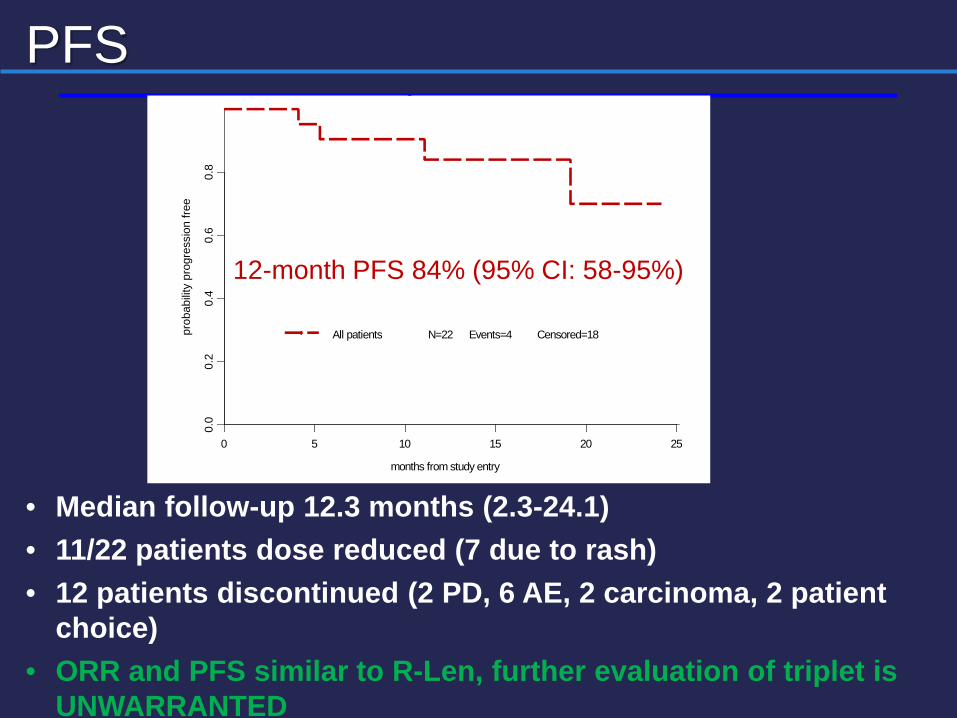
• Median follow-up 12.3 months (2.3-24.1) • 11/22 patients dose reduced (7 due to rash) • 12 patients discontinued (2 PD, 6 AE, 2 carcinoma, 2 patient
choice) • ORR and PFS similar to R-Len, further evaluation of triplet is
UNWARRANTED
PFS
months from study entry
prob
abilit
y pr
ogre
ssio
n fre
e
0 5 10 15 20 25
0.0
0.2
0.4
0.6
0.8
g
All patients N=22 Events=4 Censored=18
12-month PFS 84% (95% CI: 58-95%)
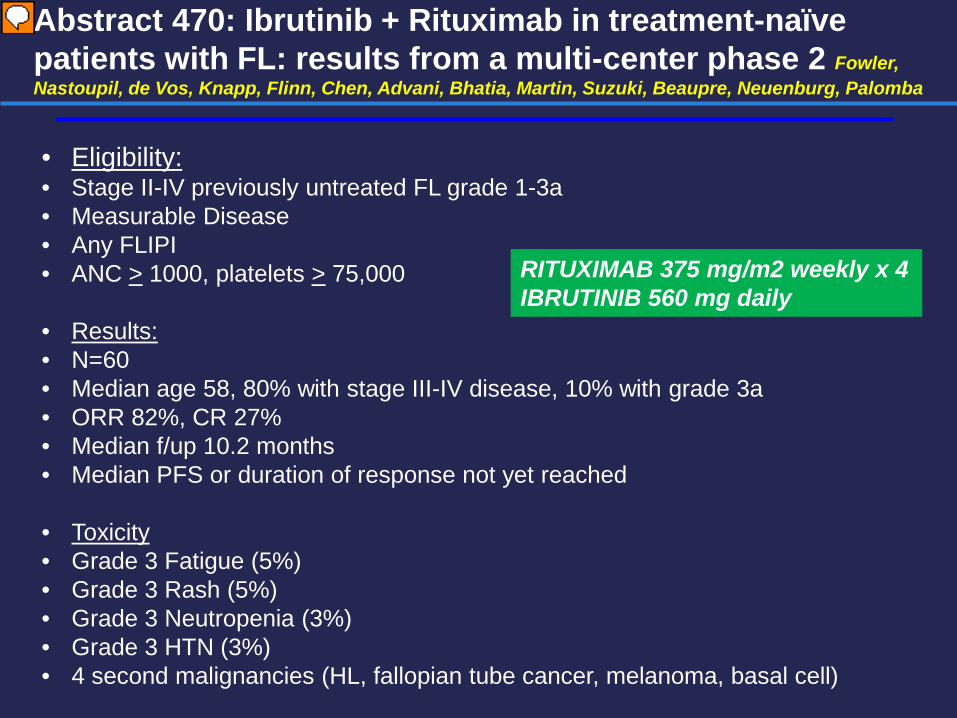
Abstract 470: Ibrutinib + Rituximab in treatment-naïve patients with FL: results from a multi-center phase 2 Fowler, Nastoupil, de Vos, Knapp, Flinn, Chen, Advani, Bhatia, Martin, Suzuki, Beaupre, Neuenburg, Palomba
• Eligibility: • Stage II-IV previously untreated FL grade 1-3a • Measurable Disease • Any FLIPI • ANC > 1000, platelets > 75,000
• Results: • N=60 • Median age 58, 80% with stage III-IV disease, 10% with grade 3a • ORR 82%, CR 27% • Median f/up 10.2 months • Median PFS or duration of response not yet reached
• Toxicity • Grade 3 Fatigue (5%) • Grade 3 Rash (5%) • Grade 3 Neutropenia (3%) • Grade 3 HTN (3%) • 4 second malignancies (HL, fallopian tube cancer, melanoma, basal cell)
RITUXIMAB 375 mg/m2 weekly x 4 IBRUTINIB 560 mg daily

Hodgkin’s Abstract 578 – US Intergroup trial of response adapted chemotherapy or Chemo/Radiation based on PET for non-bulky stage I and II HL (CALGB 50604) – Straus, Pitcher, Kostakoglu, Grecula, Hsi, Schoder, Jung, Popplewell, Chang, Moskowitz, Wagner-Johnson, Leonard, Friedberg, Kahl, Cheson, Bartlett
Regi
stra
tion
ABVD
x 2
cyc
les
Post
cycl
e 2
PET/
CT*
PET— ABVD x 2 cycles
PET+ Escalated BEACOPP x 2 cycles
+ 3060 cGy IF RT
Follo
w-u
p
*PET/CT reviewed centrally (2 reviewers, 1 adjudicator) assessed according to 5-point
scale (Deauville criteria), PET 1-3 negative
Primary Endpoint: 3 year PFS in PET- group, Target > 85%
ELIGIBILITY: Untreated stage 1 or 2 non-bulky HL
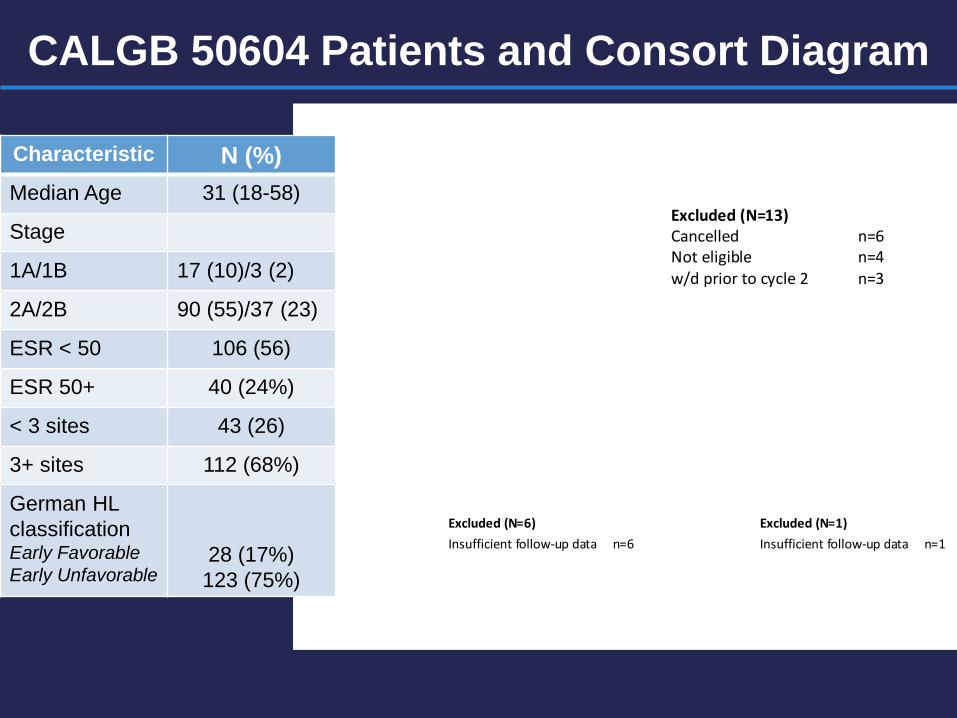
CALGB 50604 Patients and Consort Diagram Registered to CALGB 50604
N = 164
Excluded (N=13) Cancelled n=6 Not eligible n=4 w/d prior to cycle 2 n=3
PET assessment N = 151
PET-negative N = 137
PET-positive N = 14
Excluded (N=1) Insufficient follow-up data n=1
Analyzed N = 13
Analyzed N = 131
Excluded (N=6) Insufficient follow-up data n=6
Characteristic N (%) Median Age 31 (18-58)
Stage
1A/1B 17 (10)/3 (2)
2A/2B 90 (55)/37 (23)
ESR < 50 106 (56)
ESR 50+ 40 (24%)
< 3 sites 43 (26)
3+ sites 112 (68%)
German HL classification Early Favorable Early Unfavorable
28 (17%) 123 (75%)

CALGB 50604 Progression Free Survival Post cycle 2 ABVD PET- and PET+ Patients
Years from Study Entry
Prob
abilit
y pr
ogre
ssio
n fre
e
0 1 2 3 4
0.0
0.2
0.4
0.6
0.8
PET-negativePET-positive
N= 131N= 13
Events= 8Events= 4
p-value= 0.0008
Est. 3-yr PFS Hazard Ratio PET - 92% (84%-96%) 6.04 (1.82-20.08) PET + 66% (32%-86%)
Follow-up time Median: 2.1 years Range: < 1month – 4.3 years 1 Death (Suicide – PET +)
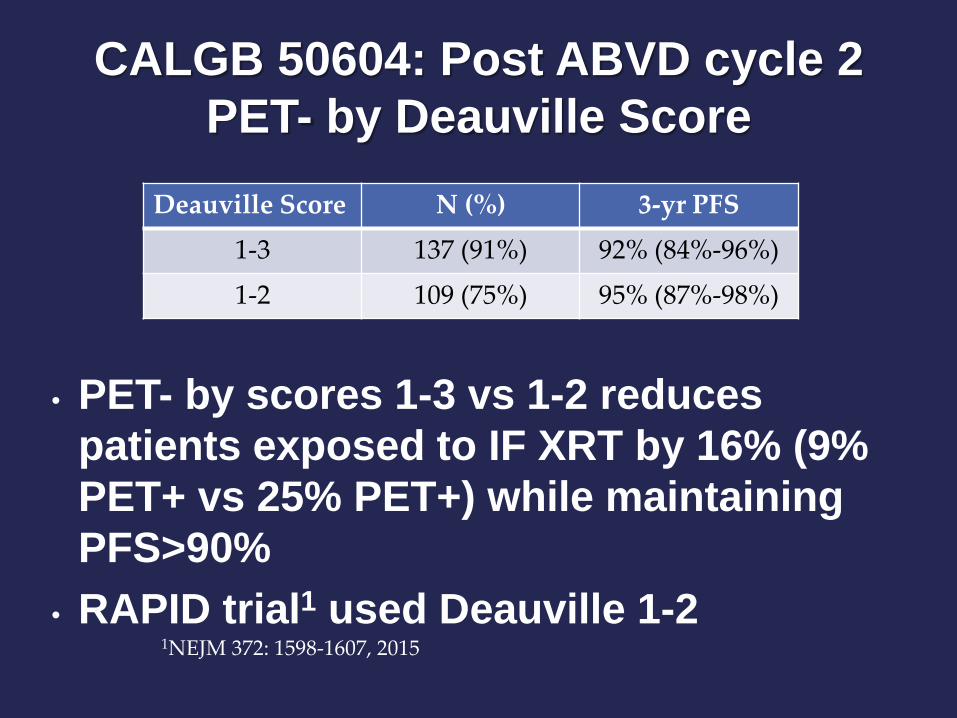
CALGB 50604: Post ABVD cycle 2 PET- by Deauville Score
• PET- by scores 1-3 vs 1-2 reduces patients exposed to IF XRT by 16% (9% PET+ vs 25% PET+) while maintaining PFS>90%
• RAPID trial1 used Deauville 1-2 1NEJM 372: 1598-1607, 2015
Deauville Score N (%) 3-yr PFS 1-3 137 (91%) 92% (84%-96%)
1-2 109 (75%) 95% (87%-98%)
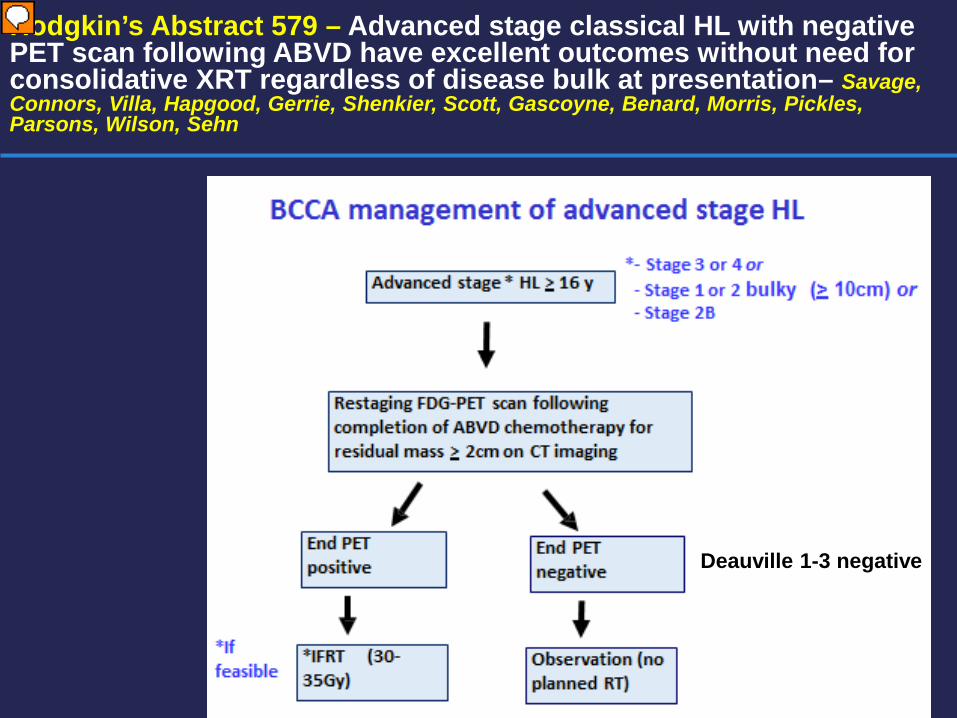
Hodgkin’s Abstract 579 – Advanced stage classical HL with negative PET scan following ABVD have excellent outcomes without need for consolidative XRT regardless of disease bulk at presentation– Savage, Connors, Villa, Hapgood, Gerrie, Shenkier, Scott, Gascoyne, Benard, Morris, Pickles, Parsons, Wilson, Sehn
Deauville 1-3 negative

Advanced stage HL > 16 y with End-PET scan post ABVD chemotherapy
End PET positive N=49 (15.5%)
End PET negative N=261 (82.6%) *Including DX N=6
Consolidative RT YES 75.5%% (N=37) NO 24.5% (N=12)
N=261 No RT 99% (N=259) RT 1% (N=2)
Exclusions N=61 •Progressive disease N=26 •Received brentuximab vedotin with primary treatment(study) N=13 •Not ABVD N=12 •Tx outside of BC N=3 •Mid-tx PET N=2 •Toxicity during ABVD N=1 •Lost to follow-up N= 1 •Hx low grade lymphoma N=1 •Refused treatment N=1 •Concurrent other cancer N=1
Results
PET Indeterminate N=6 (1.9%)
Total N=316 End PET scan

FFTF advanced stage cHL: End PET-neg vs End PET-pos
Median follow-up 4.6 years
P<0.0001
PET-pos 5 y FFTF 53%
PET-neg 5 y FFTF 89%

FFTF Advanced stage cHL End PET-neg: Bulky vs non-bulky
Median follow-up 4.6 years
Bulky (N=113) 5 y FFTF 89%
Non-bulky (N=148) 5 y FFTF 88% P=.458
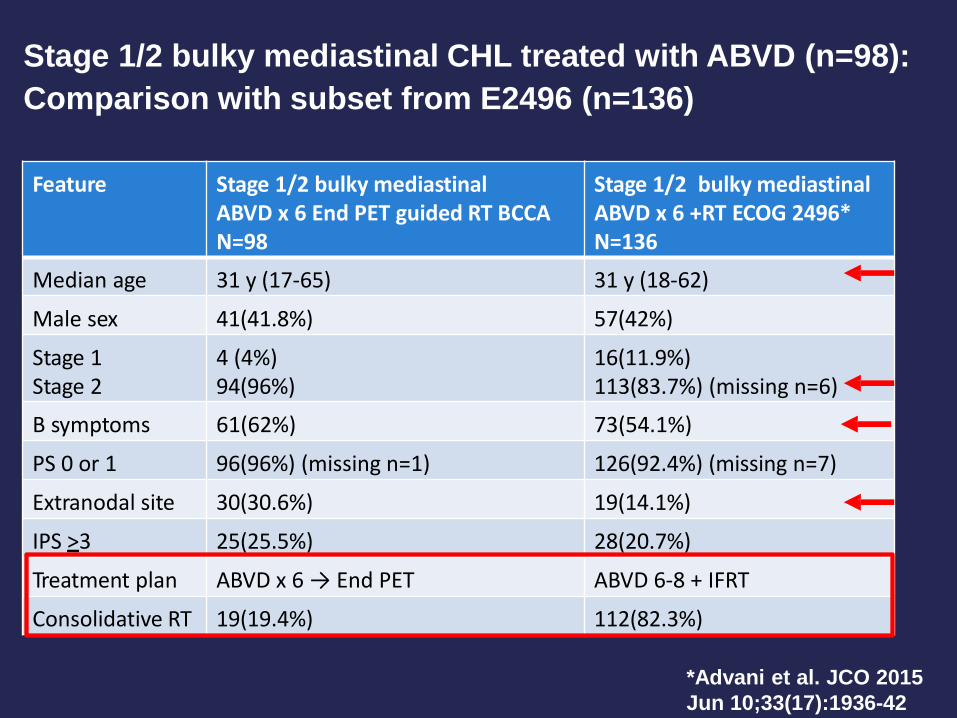
Feature Stage 1/2 bulky mediastinal ABVD x 6 End PET guided RT BCCA N=98
Stage 1/2 bulky mediastinal ABVD x 6 +RT ECOG 2496* N=136
Median age 31 y (17-65) 31 y (18-62)
Male sex 41(41.8%) 57(42%)
Stage 1 Stage 2
4 (4%) 94(96%)
16(11.9%) 113(83.7%) (missing n=6)
B symptoms 61(62%) 73(54.1%)
PS 0 or 1 96(96%) (missing n=1) 126(92.4%) (missing n=7)
Extranodal site 30(30.6%) 19(14.1%)
IPS >3 25(25.5%) 28(20.7%)
Treatment plan ABVD x 6 → End PET ABVD 6-8 + IFRT
Consolidative RT 19(19.4%) 112(82.3%)
*Advani et al. JCO 2015 Jun 10;33(17):1936-42
Stage 1/2 bulky mediastinal CHL treated with ABVD (n=98): Comparison with subset from E2496 (n=136)

ABVD 5 y OS 96% ABVD 5 y FFS 85%
Advani et al. JCO 2015
Outcome of stage 1/2 bulky mediastinal cHL following ABVD
82.6% received RT
5 y FFTF 86%
19.4% received RT
5 y OS 96%
BCCA
PET-neg N=79 (80.6%) 5 y FFTF 90%
PET-pos N=19 (19.4%) 5 y FFTF 68%
P= 0.013

Nivolumab/Pembrolizumab in Relapsed/Refractory HL (Abstracts 583 and 584 ) Ansell, Armand, Timmerman, Shipp, Garelick, Zhu, Lesokhin and Armand, Shipp, Ribrag, Michot, Zinzani, Gutierriez, Snyder, Ricart, Moskowitz
• HL frequently harbors amplification at 9p24.1 leading to overexpression of PD-L1 and PD-L2
• In addition EBV infection and JAK2 amplification further increase PD-L1
• HL may have a genetically driven vulnerability to PD-1 blockade
• Nivolumab phase 1 trial (N=23 HL)
• ORR 87% CR 22%, Duration of response NR (18-82 weeks) • 3mg/kg every 2 weeks until CR or maximum 2 years for PR/SD
• Pembrolizumab phase 1 study (N= 31 HL) • ORR 65% CR 16%, Duration of response NR (0.14-74 weeks), • PFS at 24 weeks 67% • 10 mg/kg every 2 weeks for at least 24 weeks (CR) or max 2 years

Nivolumab Responses
44
0 8 16 24 32 40 48 56 64 72 80 88 96 104 112
17
15
20 19 18
16
14 13 12 11
9
7 6 5 4 3 2 1
10
8
Patie
nts
First CR First PR Death Ongoing response
• On treatment, ongoing responses
• 13 patients off treatment
without disease progression
• 6 with maximum clinical benefit
• 5 proceeded to transplant
• 2 discontinued for toxicity Disease progression following initial response
PFS Responders Time, Weeks

Conclusions • MCL
1. MRD negativity post-induction improves outcomes in patients with MCL undergoing ASCT
• Unclear what induction regimen provides highest MRD negativity rate • Favor RCHOP/RDHAP, RDHAP x 4 (Lyma trial), or Nordic-2 regimens
2. Rituximab maintenance improves outcomes in younger patients after ASCT (LYMA trial, ASH 2014) as well as older patients not receiving ASCT
• Duration ? 3. For MCL patients failing ibrutinib, outcomes are extremely poor
• Consider allogeneic transplant for these patients in good CR/PR • Need novel therapeutics in this setting
• DLBCL
1. Currently NO ROLE for cell-of-origin directed therapy with RCHOP + bortezomib in ABC/non-GCB type DLBCL • Outcomes in this subgroup with RCHOP may be better than observed in
retrospective studies • Front-line study of RCHOP +/- ibrutinib (NCT01855750) just completed in this
group

Conclusions • FL
1. Single agent activity of ibrutinib is low 2. Numerous novel front-line therapies available in this disease
• Chemotherapy (R-bendamustine, RCVP, RCHOP, etc) • Non-chemotherapy (Rituximab, R-lenalidomide, idelalisib, R-ibrutinib)
3. Rituximab maintenance probably not necessary in all FL patients • Re-treatment strategy is equally effective and more COST effective in low
risk patients • HL
1. Abbreviated chemotherapy (3-4 ABVD) without XRT is highly effective in early stage HL with interim PET negativity
2. Consolidative XRT may be eliminated in PET negative advanced stage and bulky HL
3. PD1 inhibitors: very active in HL relapsed after transplant and Brentuximab • Genetically driven mechanism of action (9p amplification driving PDL1
expression in nearly all HL cases) • Supports phase 2 evaluation of these agents and evaluation of these
agents in other 9p amplified diseases (i.e. PMBCL) • Duration of f/up short and long term toxicity is not known (Caution if going to
allogeneic transplant) • Single agent activity of these agents in NHL is lower

ADDITIONAL SLIDES

Additional abstracts of interest: DA-REPOCH for BL Dunleavy, Noy, Abramson, LaCasce, Link, Parekh, Jagadeesh, Bierman, Mitsuyasu, Watson, Peace, Averbrook, Naina, Leach, Hanna, Powell, Nagpal, Roschewski, Lucas, Steinberg, Kahl, Friedberg, Likle, Bartlett, Fanale, and Wilson
• Multi-center prospective phase 2 of DA-REPOCH for BL


Additional abstracts of interest: TEDDI-R for CNS lymphoma Dunleavy, Lai, Roschewski, Brudno, Widemann, Pittaluga, Jaffe, Lucas, Stevenson, Yuan, Harris, Cole, Butman, Little, Staudt, and Wilson

RESULTS: DA-REPOCH for BL and TEDDI-R for CNS lymphoma Dunleavy et al
• N=14
• Median age 65 (50-87)
• 9 Relapsed or refractory (median 3 prior tx), 5 previously untx
• ORR • Ibrutinib alone (14 day lead in for cycle 1 only)
• 10 PR of 11 evaluable patients


RESULTS: Case Example Patient 4 (52 yo) – DA-TEDDI-R