nwc england ecosystem event patient centred data … centred data exchange welcome councillor...
TRANSCRIPT

NWC England Ecosystem event
Patient Centred Data Exchange

Welcome
Councillor Alistair Bradley

NWC England Ecosystem
Presented by:
Dr Liz Mear
Chief Executive

House keeping
• In case of emergency
• Mobile phones
• Twitter #NWCEcosystem
• Wifi: Wifi Name: THEvent
Wifi Passcode: 0125751515
Today’s programme
• Working in partnership across the region
• Working with all stakeholders
• Overcoming barriers to integrated care
• Examples of digital products

Aims and objectives of AHSNs Innovation, Health and Wealth • To spread innovation at pace and scale across
regions
• To integrate the strengths of higher education, the NHS, industry, third sector, local authorities
• To improve health of individuals and communities • To focus on the needs of local populations • To speed up adoption of innovation into health
and social care • To build a culture of partnership and collaboration • To create wealth
NWC AHSN Digital Innovation work stream
• Spreading digital innovations at pace and scale across NHS
• Integrating the strengths of higher education, the NHS, industry, third sector
• Empowering health and social care to better track, manage, and improve residents health.
• Reducing inefficiencies in healthcare delivery,
• Making medicine more personalised and precise • Speeding up adoption of innovation into
healthcare • Creating wealth
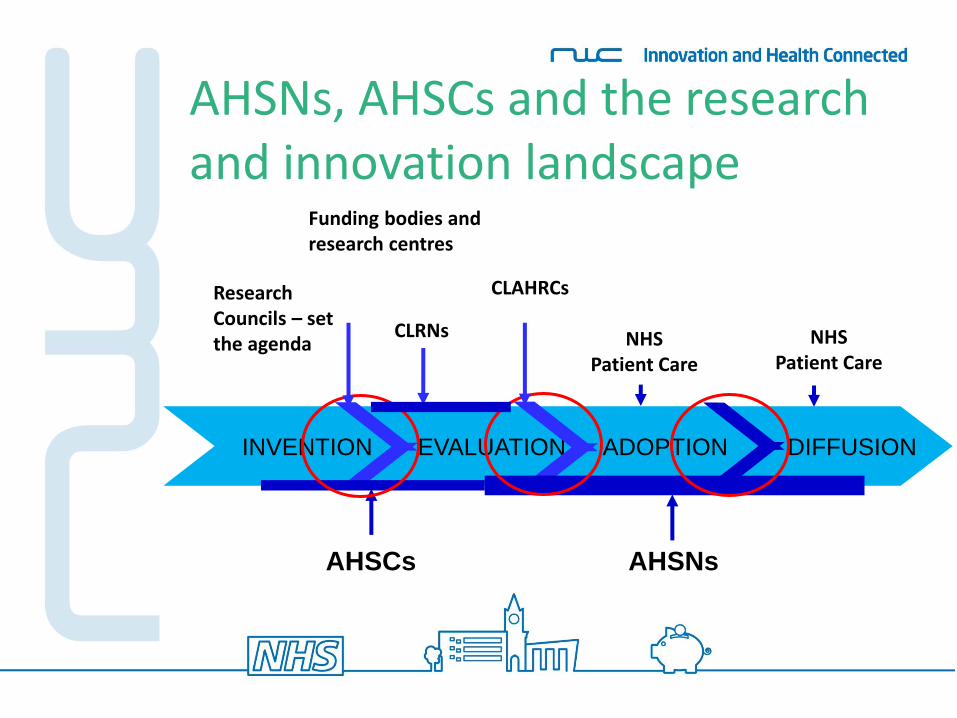
AHSNs, AHSCs and the research and innovation landscape
INVENTION EVALUATION ADOPTION DIFFUSION
Research Councils – set the agenda
CLAHRCs
AHSCs AHSNs
NHS Patient Care
NHS Patient Care
CLRNs
Funding bodies and research centres
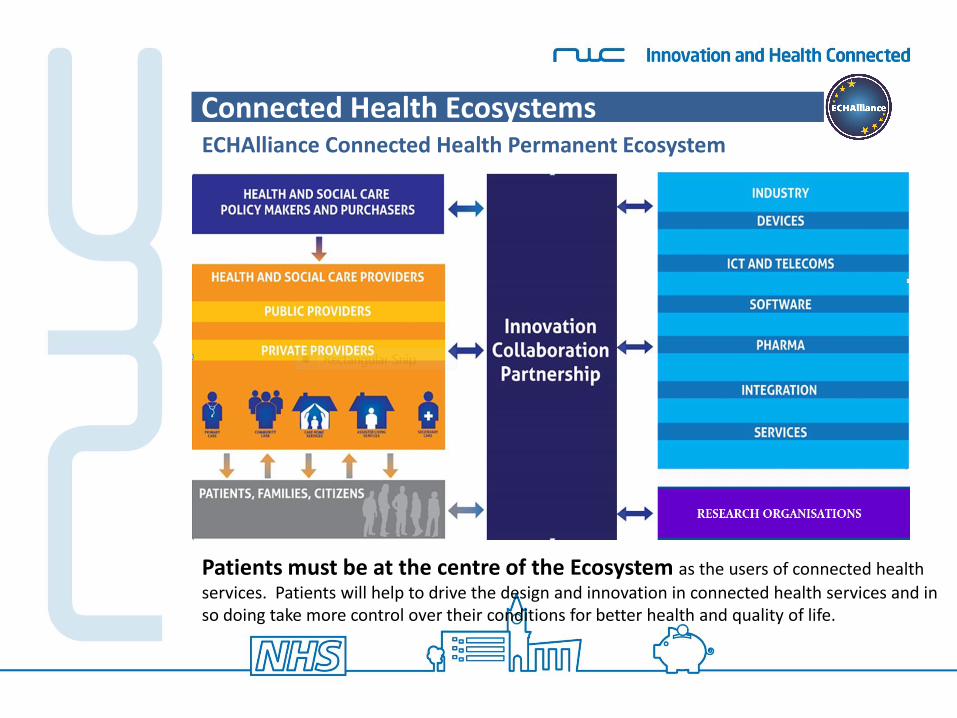
Connected Health Ecosystems ECHAlliance Connected Health Permanent Ecosystem
Patients must be at the centre of the Ecosystem as the users of connected health
services. Patients will help to drive the design and innovation in connected health services and in so doing take more control over their conditions for better health and quality of life.

Since our last event…
• Engaging with key networks - Europe-wide • Raising awareness and developing new
partnerships • Established connected health working party • Readiness tool for tele-health • Working with national leads to share leads
to share learning and best practice. • Events on specific areas of work: healthy
apps

Digital Technology innovation Healthy App work
Engagement events with key stakeholders to
– review needs, wants and expectations
– support new partnerships and working arrangements across health and industry
– showcase best in class examples
– discuss barriers and solutions to achieve improved care.
VIDEO LINK…….
https://www.youtube.com/watch?v=r2c9-DMMtxY
Interoperability: The opportunity
Bleddyn Rees
Partner and Head of Healthcare here at Wragge Lawrence Graham & Co and is a Non-Executive Director at the European Connected Health Alliance (ECHA).
North West Coast Academic Health Science Network
NWC England Ecosystem Meeting Wednesday, 8th October 2014
Interoperability: the Opportunity?
Bleddyn Rees NED ECHAlliance
European Connected Health Alliance Bringing Together the future of Health, social care & Wellness
@bleddyn_rees
Overview
1. Refresh about the European Connected Health Alliance.
2. A vision for digital health and social services for me, you and everyone.
3. What is interoperability?
4. The use & challenge of standards
5. Interoperability Projects in the EU
6. Update of ECHAlliance Events & News

16
About us…
Community Interest Company
Not for profit, Connected Health Alliance CIC (registered in Northern Ireland)
Our Mission
“Bringing Together the future of Health, social care & Wellness”
Our Mantra
“Health & Social care is an investment for people wellbeing and for growth & jobs creation”
Membership Organisation
220+ members in over 20 countries
Connected Health Ecosystems
International network of Ecosystems
Promote Connected Health and our members
Connect & support the innovators
Implement & scale-up solutions
through Ecosystems
Business models &
Entrepreneurship
Act on Public policies
(Health/social and Economy)
Educate, Communicate &
Disseminate
Primary functions
Montpelier
France
Scotland (UK)
Manchester (UK)
Athens (Greece)
New York (USA)
NWC England (UK)
Oulu
(Finland)
Barcelona
(Spain)
Northern
Ireland (UK)
Yorkshire
& Humber UK
Wales
UK Latvia
International network of Permanent Connected Health Ecosystems
Skane
Sweden
Nice
France
Toulouse France
Estonia Galicia Spain
Limousin
France Netherlands
Republic of Ireland
Turku
Finland
Basque
Spain
Italy
Canada

2. A vision for digital health and social services for me, you and everyone.
(1) Online access/Patient Portal where I can
• Book GP, Optician (?) and Dentist (?) appointments
• Book Hospital appointments
• See my test results from my GP or Hospital
• See my Medical Records
• Store my wellness data?
• See my Optician’s Results/Prescription?
• See my Dental Records?
• All ePublic Services (e.g. the XRoad Estonia)?
2. A vision for digital health and social services for me, you and everyone.
(2) System Integration
• GP & Hospital access “my” record in real time
• Health & Social Care records can be accessed
• In EU & US my summary care record can be accessed if I am unwell

2.3 The NHS & ICT
• “Our vision is of an information revolution which people have the information they need to stay healthy, to take decisions about and exercise more control of their care, and to make the right choices for themselves and their families. This includes an accurate record of their care, available to them electronically *
• “Health and adult social care information will be liberated from a closed, bureaucratic system in order to serve patients and the public, and to help drive better care, improve outcomes, innovation and the better use of resources” *
Liberating the NHS July 2010
• “I believe that the NHS must develop a more open, innovative and integrated culture – one that improves the health of the public and the quality of care by putting patient voices and patients needs at the heart of a new clinically-led system”
• “The world is shrinking: in an age of connectivity where people access information at the click of a button, the NHS cannot remain in the information dark ages”
Professor Steve Field, NHS Future Forum, 10 January 2012

2.4 A vision for digital health and social services for me, you and everyone.
Source: Dr Oliver Harrison,
Healthways

2.5 A vision for digital health and social services for me, you and everyone.
Source: Dr Oliver Harrison,
Healthways

2.6 A vision for digital health and social services for me, you and everyone.
Source: Dr Oliver Harrison,
Healthways

2.7 Which countries are leading the way?
Source: Dr Oliver Harrison,
Healthways

3.1 What is interoperability in a healthcare context?
• Technical ICT equipment/systems are compatible & able to work
together
• Semantic Information is compatible/the same
• Allowing different IT systems and software to:
o Communicate
o Exchange data
o Use the information that has been exchanged.
3.2 Why is it important?
• an interoperable environment improves healthcare delivery and ultimately healthcare outcomes by making the right data available at the right time to the right people
• Enables the development of a Global healthcare industry & sustainable health systems
Implementing the HHS-EC MoU on Cooperation Surrounding
Health IT
Transatlantic Cooperation Assembly
October 23, 2013
Doug Fridsma, MD, PhD, FACP, FACMI
Chief Science Officer & Director, Office of Science & Technology
ONC
US Department of Health & Human Services
Introduction
• December 17, 2010: Secretary Kathleen Sebelius signed non-binding MoU with European Commission – Facilitate availability and routine use of
international standards
– Strengthen relationships and cooperation on mutual health ICT goals
• MoU outlines approach to foster mutual understanding of challenges faced by both sides in advancing the use of health IT

Issues of Immediate Focus
• Development of internationally recognized standards & specifications for interoperability
• Strategies to promote and develop a highly skilled health IT technical/support workforce

International Interoperability Standards
• Achieving interoperability across international borders is a key goal of immediate importance and immense potential.
• 3 distinct work streams: – Standardized terminology (clinical, laboratory, RX
& administrative data)
– Standard message structure
– Standardized patient-controlled electronic exchange
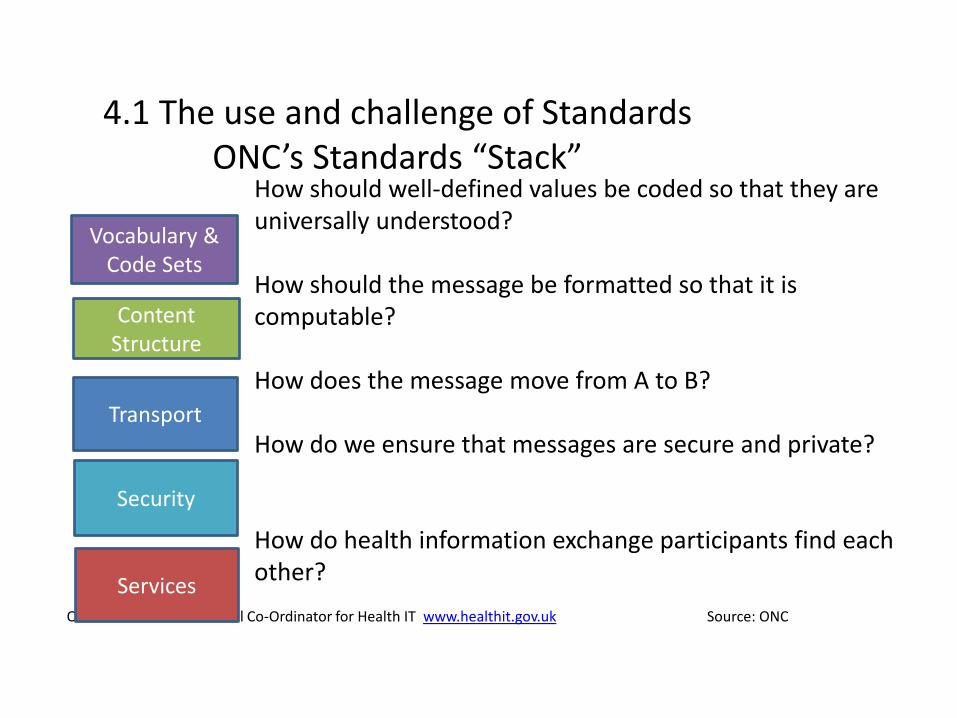
4.1 The use and challenge of Standards ONC’s Standards “Stack”
How should well-defined values be coded so that they are universally understood? How should the message be formatted so that it is computable? How does the message move from A to B? How do we ensure that messages are secure and private? How do health information exchange participants find each other?
ONC: Office of the National Co-Ordinator for Health IT www.healthit.gov.uk Source: ONC
Vocabulary & Code Sets
Content Structure
Transport
Security
Services
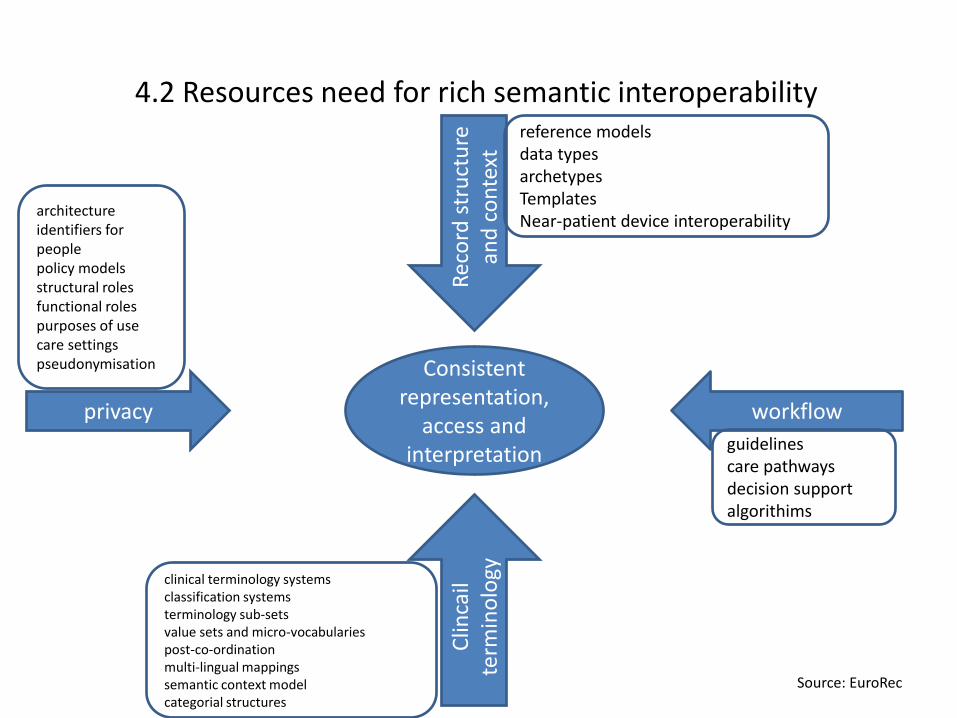
4.2 Resources need for rich semantic interoperability
Rec
ord
str
uct
ure
an
d c
on
text
privacy workflow
Clin
cail
term
ino
logy
Consistent representation,
access and interpretation
reference models data types archetypes Templates Near-patient device interoperability
guidelines care pathways decision support algorithims
architecture identifiers for people policy models structural roles functional roles purposes of use care settings pseudonymisation
clinical terminology systems classification systems terminology sub-sets value sets and micro-vocabularies post-co-ordination multi-lingual mappings semantic context model categorial structures
Source: EuroRec
5.1 Examples from across the ECHAlliance International Network
• There are local, national, European and international examples of interoperability initiatives
– Locally – Manchester AHSN Datawell project, focus of June Ecosystem meeting in Manchester
– Nationally – Northern Ireland’s Electronic Care Record –integrated health and social care record rolled out in 2013/14
5.2 Examples from across the ECHAlliance International Network
• Europe – epSOS project
– 6 year EC funded pilot project completed in June 2014;
– Aim to design, build and evaluate a service infrastructure that demonstrates cross-border interoperability between electronic health record systems in Europe
– 25 different European countries
– www.epsos.eu

• Trillium Bridge Project
– Feasibility study on Bridging Patient Summaries across the Atlantic
• How:
– MU2 and epSOS patient health summaries
• When:
– From: July 2013 to February 2015
• Who:
– Consortium comprising EU member state ministries, provider networks, industry, SDOs
5.3 Examples from across the ECHAlliance International Network
5.4 Objectives of Trillium Bridge
• Building the Transatlantic bridge for patient summaries – Use cases gap analysis identify barriers and easy wins – Interoperability assets Implementations Validation – Policy alignment, future standardization, and sustainability – Feasibility study to guide future developments
• Why? – Reduce barriers for transatlantic coordination, health care, and
trade – Decrease standards development and implementation costs – Accelerate convergence towards global standards – Support rights of citizens to their health information
• Realize the vision of EU-US eHealth cooperation • http://www.trilliumbridge.eu/

5.5 Samsung’s vision
Combine diverse technologies and disciplines to enable preventive health
Algorithms
Preventive Health
Semiconductor and Hardware
Cloud & Big Data
Mobile
Behavioural Science
Healthcare

Conclusion: US “Meaningful Use” & 5 overarching goals for Health IT
1. Improve quality, safety and efficiency
2. Engage patients and their families
3. Improve care co-ordination
4. Improve population and public health and reduce disparities in care
5. Ensure privacy and security protections

eHealth week
ECHAlliance was the strategic partner of the
Greek Presidency of EU for the eHealth Forum
2014, in Athens. It was a huge success for
ECHAlliance and all of our members and
partners. We really succeeded in driving forward
the conversation about eHealth at an international
level.
The busy forum included:
• 4th EU-US eHealth Marketplace & Cooperation Assembly - organised by ECHAlliance in partnership with US Trade &
Commerce, Office of National Coordinator, Washington USA & the European Commission. It addressed the commercial
opportunities for companies on both sides of the Atlantic and provided an update on progress on interoperability and
workforce skills.
• B2B Matchmaking session - with hundreds of pre-arranged or informal networking.
• Speakers’ Corner - 3 days, 35 speakers, 14 countries, countless new connections.
• European Innovation Partnership (EIP) meets Connected Health Ecosystems - ECHAlliance was delighted to partner with
the EIP programme session at the eHealth Forum.
• Boosting SME growth & competitiveness –'GET Funded & International' @ eHealth Forum provided a unique opportunity
for SMEs to present their investment and internationalisation plans to an international panel of investors, purchasers and
industry leaders.
Listen to Brian’s interview with TechTalks @ eHealth Forum:
‘Can connected health reform healthcare?’ here
ECHAlliance collaborates with the European
Commission for the eHealth Week 2015, in Riga
(Latvia), 11-13 May 2015. Especially on B2B
matchmaking sessions, EIP AHA reference
sites/Ecosystems cooperation, Speakers’ Corner, EU-US
marketplace… See next news on www.echalliance.com or write us on

EU Marketplace for eHealth and the EIP on AHA, Brussels 2014
ECHAlliance has organised the “EU Market place for eHealth and EIP on AHA”, in cooperation
with the European Commission, GET Project, AAL Programme and AGE Platform Europe.
The EU Marketplace event was focused on bringing together large industry, SMEs, policy makers, researchers, care
professionals, service providers, buyers and consumers through formal and informal meetings.
The objective was to provide a platform for all stakeholders in connected health and AHA actors’ to meet, share best
practices and develop effective collaborations leading to new projects and business opportunities. The event also provided
a platform for the exchange of information between procurers and potential suppliers.
Key figures
180+ attendees registered
40% of companies, 17% of Governments and private insurances Supporting Partners
200+ B2B matchmaking
16 topics through the “Meet & Debate” tables
20 short presentations through the Speakers’ Corner
European Commission offices
All Action Groups and several Reference sites of EIP on AHA represented

EU-US Marketplace & Conference, Boston 2014
ECHAlliance organises the 5th EU-US eHealth Business Marketplace & Conference “Transforming Care
& Accelerating Economies”, 21-22 October in Boston, as part of the Massachusetts Connected Health week 2014.
Join global connected health innovators, public officials, patient groups, academics and entrepreneurs this fall at the 5th
EU-US eHealth Marketplace and Conference. The action packed EU-US eHealth Marketplace will take place in the
prestigious surroundings of the Massachusetts State House in Boston.
ECHAlliance is actively engaging with NIMAC, colleagues in Massachusetts, the US Department of Health and Human
Services (DHHS), the European Commission DG Connect (EC) and the wide network of ECHAlliance members across the
USA and Europe to organise this exciting event.
All information and registration on: https://www.b2match.eu/eu-us-ehealth-marketplace-2014
The programme includes:
• EU/US workshops to foster continued work on the Memorandum of Understanding between the federal Department of
Health and Human Services and the European Commission on work force development and interoperability.
• B2B Matchmaking opportunities for businesses to find other industry partners.
• Informative sessions featuring prominent speakers on Big Data Analytics, Patient Engagement and Global
Partnerships.
• Two networking receptions including: Opening reception at the Massachusetts State House Library and closing
reception at the Partners Connected Health Symposium.
• Shark Tank: SMEs and start-ups will have the opportunity to present their business to experts and investors.

SAVE THE DATE 2nd Health & Wellness @ Mobile World Congress 2015 Barcelona | 3 – 4 March 2015 The European Connected Health Alliance (ECHAlliance) is delighted to announce the 2nd Health & Wellness vertical programme of the Mobile World Congress 2015, Barcelona 3 - 4 March 2015.
After the success of the Health & Wellness @ Mobile World Congress 2014 we know 2015 is going to be even bigger and better. The agenda so far:
Tuesday 3 March supported by Mobile World Capital Barcelona will be dedicated to interactive sessions and workshops. It will be held in the Mobile World Centre, at the centre of Barcelona. Wednesday 4 March will include a high level programme including international leaders in the health and wellness sector. It will be held in the heart of the Mobile World Congress at Fira Gran Via, Hall 8.0 Theatre District.
Register your interest in learning more and keeping up to date as planning develops – email [email protected]


Website: www.echalliance.com
Email: [email protected]
European Connected Health Alliance Bringing Together the future of Health, social care & Wellness
Thank you & Questions

The Challenge

47
What has been happening across the International
Network

Brian O’Connor, Chair
European Connected Health Alliance
[email protected] www.echcalliance.com
48
www.echalliance.com
@ECHAlliance
-
ECHAlliance

Liz Page ‘Joining the dots for patients and Families’

Liz Page Patient Voice
Joining the dots for patients and families
“Interoperability means the ability of health information systems
to work together within and across organizational boundaries in
order to advance the effective delivery of healthcare for
individuals and communities.”
Wikipedia
Interoperability 101…


What patients and families have to navigate…
Patient Pathway



YP
Endocrinology
Paediatric Neuropsycholog
y
Genetics
Paediatric Neurology
Adult specialist Neurology
Centre - London
Haematology
Children’s Dental Hospital
GP
Pharmacy
Community Physio
School
Youth Service
Children’s Services
Young carers
Local Authority
3rd
sector
Adult
endocrine
Adult
Haematology
College
Health &
Social Care
plan
Adult
Psychology
Adult
Dental
Hospital

Who is talking to whom? P
aed
ia
tric
En
do
crin
olo
gy
Pa
ed
ia
tric
Ne
uro
lo
gy
Pa
ed
ia
tric
Ne
uro
ps
yc
ho
lo
g
y
Ad
ult S
pe
cia
lis
t
Ne
uro
lo
gy
Ce
ntre
Pa
ed
ia
tric
Ha
em
ato
lo
gy
De
nta
l H
os
pita
l
GP
Co
mm
un
ity
Ph
ysio
Sc
ho
ol
Lo
cal A
uth
ority
Ch
ild
ren
's
Se
rv
ice
s
Yo
uth
S
erv
ice
3rd
S
ecto
r
Yo
un
g C
are
rs
Pa
re
nt
Neuropsych Neuropsych Neuropsych Neuropsych Neuropsych Neuropsych Neuropsych Neuropsych Endocrine
Neurology Endocrine Endocrine Endocrine Endocrine Endocrine Endocrine Endocrine Endocrine Endocrine Endocrine Neuropsych
Specialist
neuro
Specialist
Neurology Neurology Neurology Neurology Neurology Neurology Neurology Neurology Neurology Neurology Neurology
Haematology Haematology
Specialist
Neurology
Specialist
Neurology
Specialist
Neurology
Specialist
Neurology
Specialist
Neurology
Specialist
Neurology
Specialist
Neurology
Specialist
Neurology
Dental Dental Haematology Haematology Haematology Haematology Haematology Haematology Haematology Haematology Haematology Haematology
GP GP GP Dental Dental Dental Dental Dental
Community
Physio
Community
Physio
Community
Physio
Community
Physio
Community
Physio
Community
Physio
Community
Physio
Community
Physio
School School School GP GP GP GP GP GP GP GP
Local
Authority
Local
Authority Local Authority School School School School School School School School School School School
Children's
Services
Children's
Services
Children's
Services
Children's
Services
Children's
Services
Children's
Services
Children's
Services
Parent Parent Parent
Local
Authority Local Authority
Local
Authority
Local
Authority
Local
Authority
Local
Authority
Local
Authority Local Authority Local Authority Local Authority
3rd Sector Youth Service Parent Parent Parent Parent Parent Parent Parent Parent Parent Parent Parent Youth Service
Youth Service Youth Service Young Carers Youth Service Youth Service Young Carers
3rd Sector 3rd Sector 3rd Sector 3rd Sector 3rd SectorYoung Carers Young Carers
Pathway of a single letter
• PATIENT • dictated • prioritised • typed • sent • prioritised by receiving secretary • placed for attention to recipient • read • response • dictated • prioritised • typed • sent
• received back by originating secretary • read • prioritised • placed before consultant. • read • decision • outcome given at next appointment. • PATIENT
So why is data share needed ?
“Shifting work to other departments is a phony efficiency…”
Fred Lee – (If Disney ran your hospital, p39)
Could data share have prevented this?
I go to Hospital X.
“We can’t deal with your case, we are sending you to Hospital Y.”
I go to Hospital Y, which is in another region: sadly, after a few
months, and a couple of visits, the consultant dies.
Hospital Y no longer has a specialist and tell me:
“We are sending you back to referring Hospital X.”
I hear nothing for a YEAR, so contact original referring Hospital X.
“Oh, we thought you were being treated by Hospital Y.”
Continued……. “Well they thought that I was still being seen by you.” “But we have discharged you because we sent you to Hospital Y.” “Well they have discharged me back to you because they think I am still under
you. And they have no consultant now.” “Well you’ll have to be re-referred to us, as too much time has passed. And
you’ll have to wait to be seen as a new referral.” It transpires letters crossed but were ignored as both places deemed I wasn’t
their patient any more. The fact that the person they suggested refer me had died was not their
problem. It was mine. As was the delay in treatment. I had to go to Hospital Z.

Timely care…?
• Endocrine and Haematology Departments in same space
• A letter from one to the other takes 8 weeks
• Treatment withheld in this time
• Inpatient procedures needed, and done by non specialist staff
• No understanding of the tests or necessity for strict timing
• Would not call consultant to verify parent’s information as it was late at night
Saving time or lives? Let’s do both!
• Notes in two folders both over a foot thick
• Letters from different places filed in there since last visit
• Consultant does not/will not attempt to find them
• Patient carries hand held copies of all letters received to show in order for treatment to be informed.
Person centred care? You decide…
• Visits to London Hospital
• 3 family members seen
• Different appointments through year for clinic
• Repeated story telling
• Travel and cost to escort family members
• Forgetting one of the reasons we need them is difficulties with mobility!
• Tooth extraction required
• Need information from different departments/hospitals
• Many visits – nothing ready
• Finally after 2 YEARS all information available.
• Tooth took 5 minutes to extract!

Checks and Balances…??
• Unplanned admission to hospital for unrelated cause
• Specialist knowledge required before standard drug regime to be followed
• No-one willing to make the call – patient had to refuse treatment due to risk
• Patient called specialist nurse on mobile from bed whilst doctor looked on, and handed phone to them.
• “Well you learn something new every day..!”
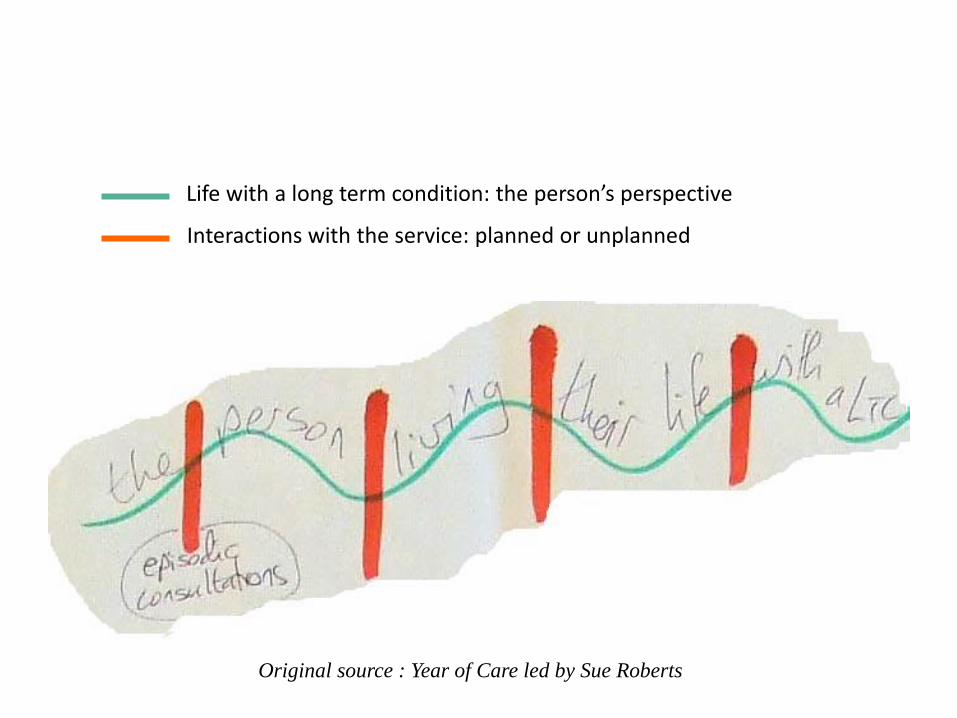
Original source : Year of Care led by Sue Roberts
Life with a long term condition: the person’s perspective
Interactions with the service: planned or unplanned

Data Share Devices
www.theidbandco.com


Thank you!
Colin Brown Consultant Physician and Gastroenterologist, University Hospitals of Morecambe Bay.
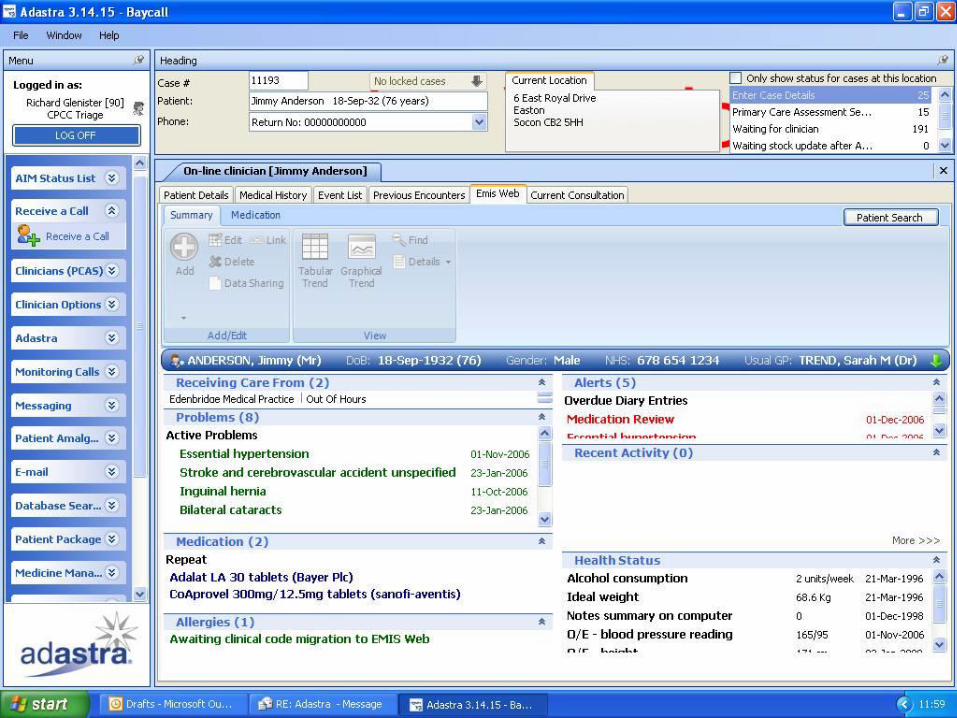
Connecting Patient Records and
Patient Care in the 21st Century Dr Colin Brown Chief Clinical Information Officer Chorley Town Hall – October 2014

What do we need for healthcare ?
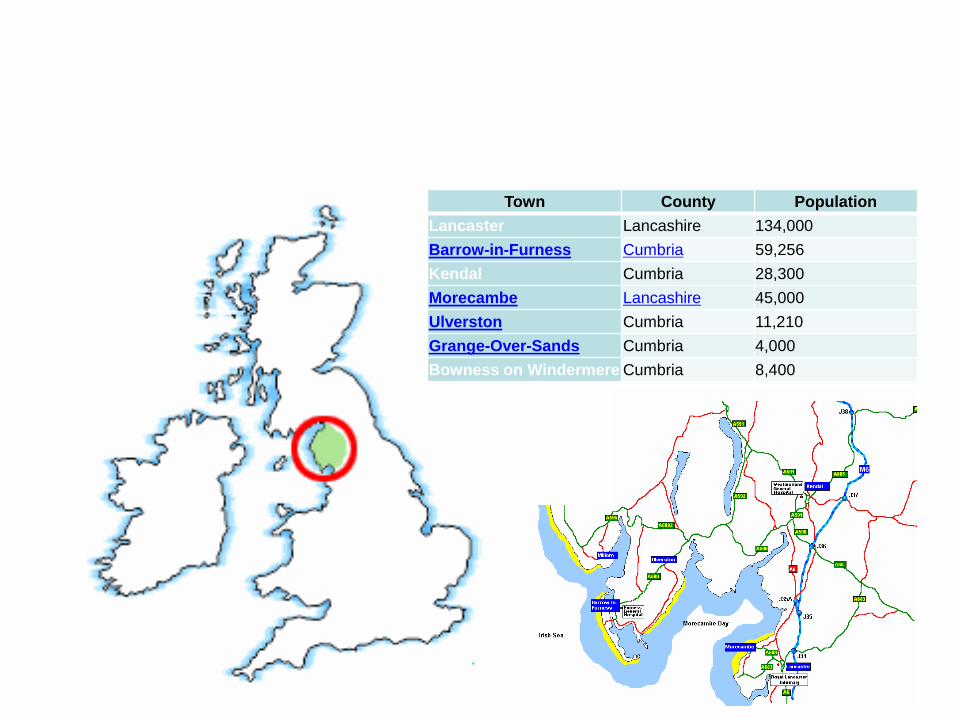
Town County Population
Lancaster Lancashire 134,000
Barrow-in-Furness Cumbria 59,256
Kendal Cumbria 28,300
Morecambe Lancashire 45,000
Ulverston Cumbria 11,210
Grange-Over-Sands Cumbria 4,000
Bowness on Windermere Cumbria 8,400
Connecting Patient Records and Patient Care in the 21st Century
• Ageing Population
• Increasing Fragility
• Dementia
• Cancer Survivorship
• Chronic Disease
• Complex MDT clinical care and pathways of care
• Poverty / access to Healthcare / Digital awareness
Healthcare Challenges in the 21st Century
Connecting Patient Care in the 21st Century
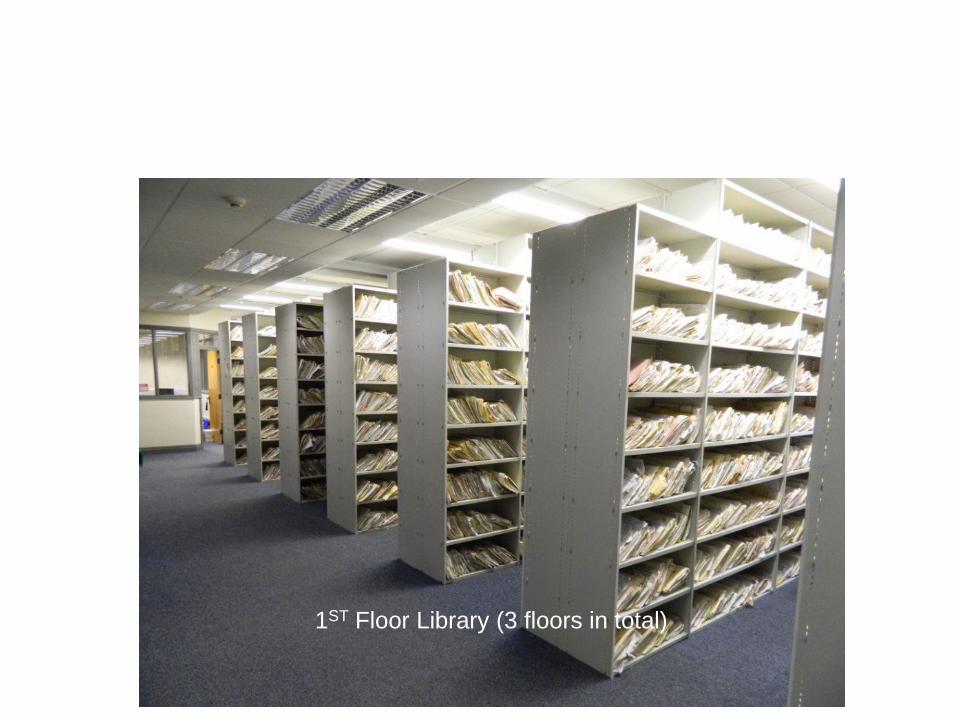
1ST Floor Library (3 floors in total)
Patient Records in the 21st Century
0
500
1000
1500
2000
2500
3000
3500
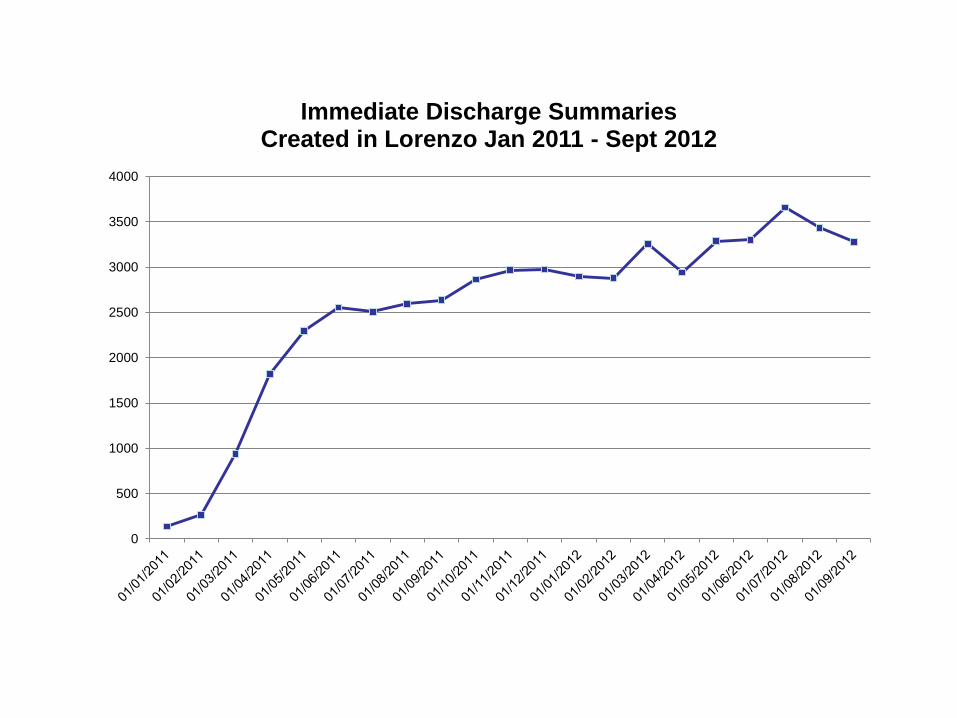
4000
Immediate Discharge Summaries Created in Lorenzo Jan 2011 - Sept 2012

Immediate Discharge Summary Letters

Cumbria - Whole system approach
• Connectivity COIN-Fibre to all, NHS wireless for all
• Hardware- Full virtualisation inc BYOD/any device
• Software – Interoperable ePR
– Electronic postal service (views and documents) • STATIC
– Air Traffic Control for patients/clients • DYNAMIC


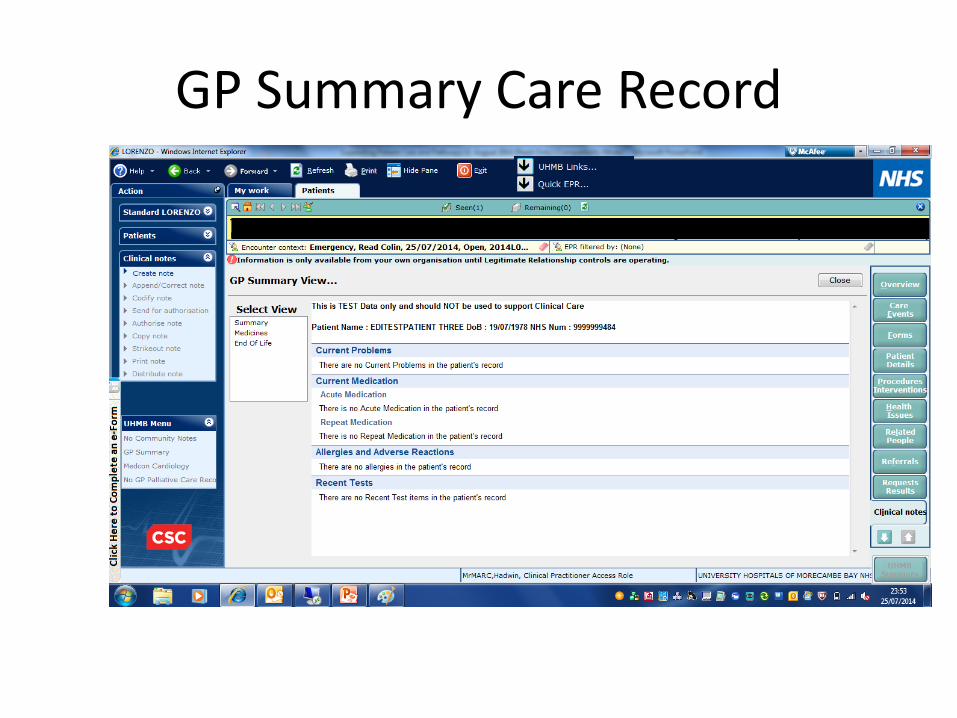
GP Summary Care Record

Palliative Care - Epaccs

Better information…….
Better decisions…….
Better outcomes
Patient Records in the 21st Century
Don’t be scared of disrupting the Status Quo

Questions to the Panel
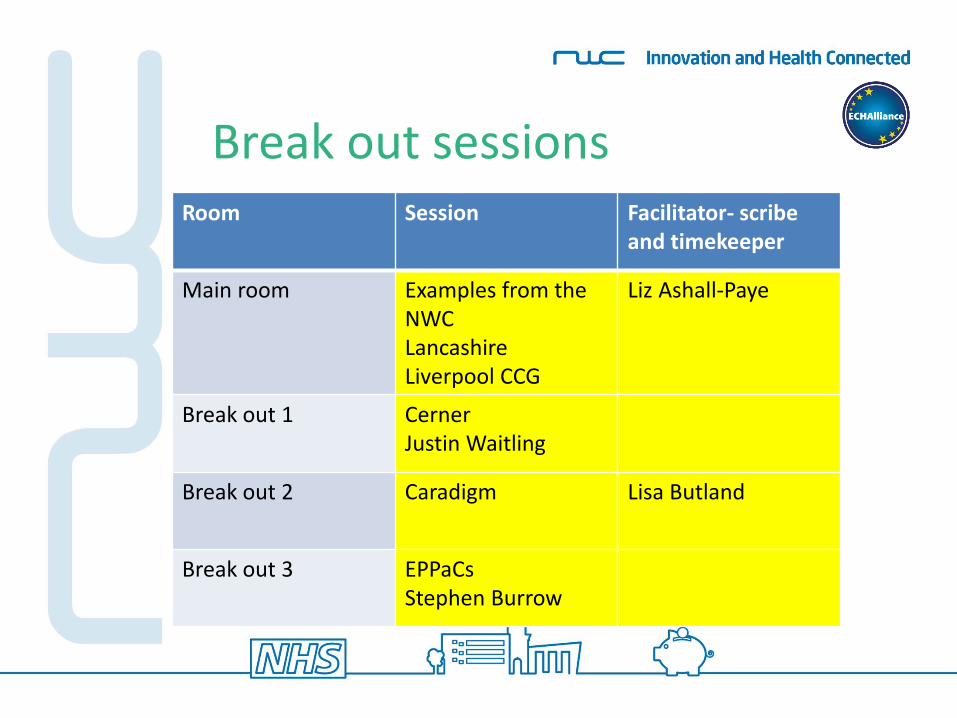
Break out sessions Room Session Facilitator- scribe
and timekeeper
Main room Examples from the NWC Lancashire Liverpool CCG
Liz Ashall-Paye
Break out 1 Cerner Justin Waitling
Break out 2 Caradigm Lisa Butland
Break out 3 EPPaCs Stephen Burrow

Refreshment Break

Healthier Lancashire Digital Health Work Stream
Declan Hadley
Digital Health Lead
NHS England (Lancashire) Local Area Team

Lunch Break (1 hour)

Break out sessions Room Session
Main room Information Governance Janet King NHS England
Break out 1 AIMES Dennis Kehoe
Break out 2 E-Redbook
Break out 3 Structured Networking Belddyn Rees

Group discussions Reflections
1. where are we now? 2. where do we want to be?
3. How can you help us to get there?

Lorraine Acheson Liz Ashall-Payne
Philip Dylak Lorna Green Lisa Butland
Liz Mear
Facilitators

Next Steps
Dr Liz Mear
Chief Executive
North West Coast Academic Health Science Network