nutrition after operation joint hospital surgical grand round 17 th january 2009 dr. yuhmeei cheng...
TRANSCRIPT
Nutrition after Operation
Joint Hospital Surgical Grand Round
17th January 2009
Dr. YuhMeei ChengDepartment of Surgery
Tseung Kwan O Hospital
Traditionally …..
• NPO
• Decompress stomach

Surgical Insult
Inflammatory Response
Hypermetabolic state
Catabolism
10% metabolic rate 30% energy expenditure 1-2g/kg protein intake
hours
days
fat source energy lean mass metabolism (protein)
Ward N, Nutritional Journal 2003; 2:18
I L-1, I L-6

Surgical Insult
Inflammatory Response
Hypermetabolic state
Catabolism
Protein Energy Malnutrition
10% metabolic rate 30% energy expenditure 1-2g/kg protein intake
Nutrient intake
hours
days
Ward N, Nutritional Journal 2003; 2:18
I L-1, I L-6
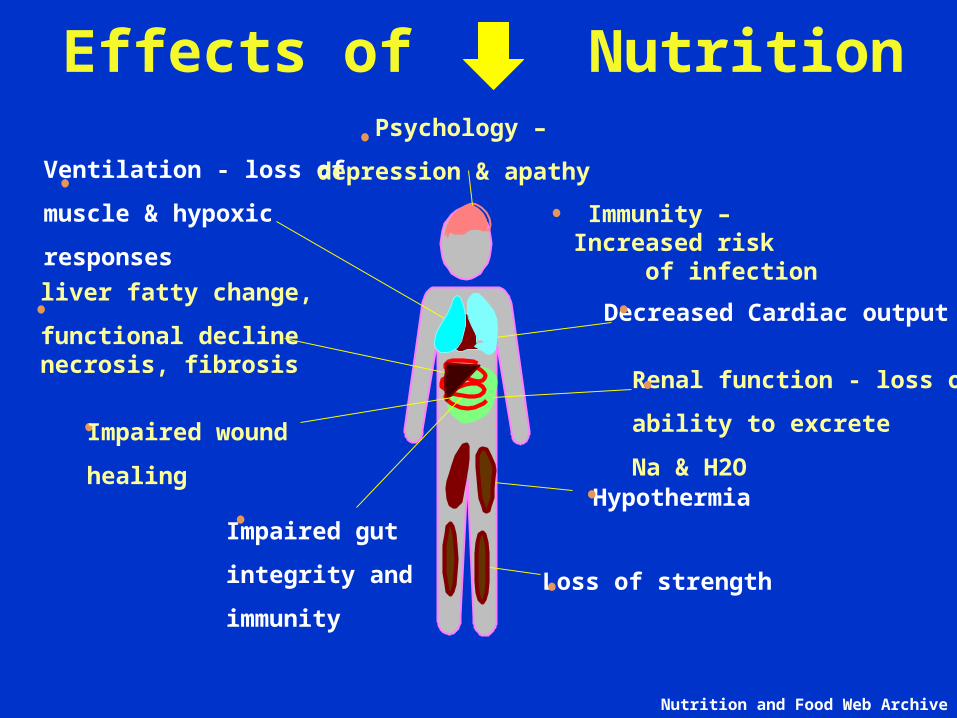
Effects of Nutrition
Immunity – Increased risk of infection
Hypothermia
Impaired gut
integrity and
immunity
Renal function - loss of
ability to excrete
Na & H2O
Decreased Cardiac output
Ventilation - loss of
muscle & hypoxic
responses
Psychology –
depression & apathy
Loss of strength
liver fatty change,
functional declinenecrosis, fibrosis
Impaired wound
healing
Nutrition and Food Web Archive

Protein Energy Malnutrition
30-50% hospitalized patients
Definition
> 10% loss of lean body mass < 2 weeks
Serum albumin < 35g/L
Ward N, Nutritional Journal 2003; 2:18
Protein Energy Malnutrition
Indices– Clinical: body weight/ BMI– Anthropometric measurements– Nutritional assessments– Biochemical markers
• serum albumin predict clinical outcome
Ward N, Nutritional Journal 2003; 2:18
Ann Nutr Metab 2006;50:394-398

serum albumin related to post-op. morbidity
Gibbs J. et. al, Arch Surg 1999; 134: 36-42
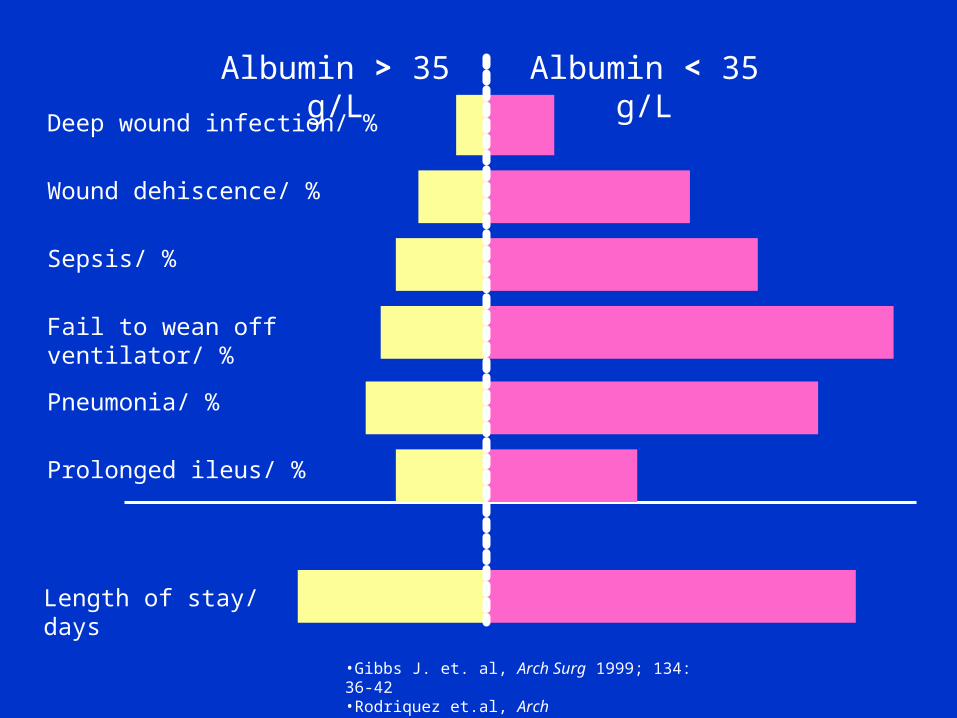
•Gibbs J. et. al, Arch Surg 1999; 134: 36-42•Rodriquez et.al, Arch Surg. 2002;137:805-812
Deep wound infection/ %
Wound dehiscence/ %
Sepsis/ %
Fail to wean off ventilator/ %
Pneumonia/ %
Prolonged ileus/ %
Length of stay/ days
Albumin > 35 g/L Albumin < 35 g/L

Gibbs J. et. al, Arch Surg 1999; 134: 36-42
serum albumin related to post-op. mortality
Nutritional Support
Aim
• Provide substrate for energy production• Promote anabolism• Promote post-operative recovery• Prevent morbidity/ complications
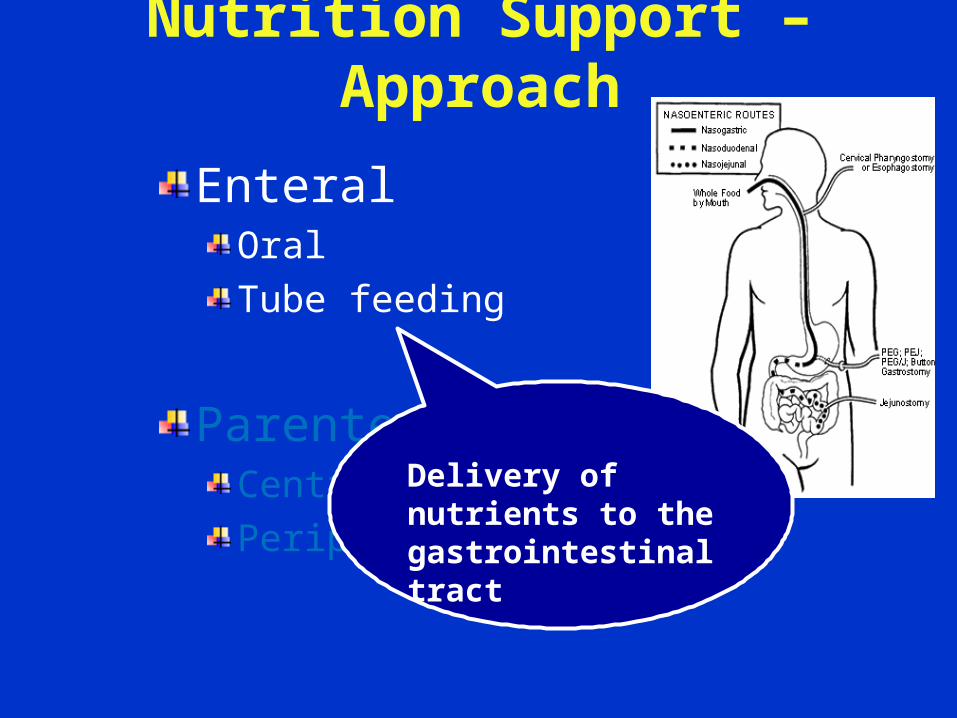
Nutrition Support – Approach
EnteralOral
Tube feeding
Parenteral Central
Peripheral
Delivery of nutrients to the gastrointestinal tract

Nutrition Support -- Approach
EnteralOral
Tube feeding
Parenteral Central
Peripheral
Delivery of nutrients directly into a vein

Enteral NutritionSmall bowel motility returns normal 6-8 hrs after operation
Absorption exits even in absence of normal peristalsis
Nutrition to alimentary tract prevents gut mucosal atrophy
Improves blood flow Increases collagen deposition over anastomosis
Enhances IgA expressionIncreases villi height Decreases permeability
Decreases bacterial translocation
•Ward N, Nutritional Journal 2003; 2:18
Enteral Nutrition
Advantages Disadvantages infection risks/ complications
Need functional GI tract
Improves wound healing Risks of bowel necrosis < 3%
Better glycaemic control reduce metabolic stress
Vomiting + aspiration risk(gastroparesis ~ 60%)
More physiological GIT intolerance (15-30%)
length of hospital stay/ costsAccess complications (tube feeding/ PEG/ jejunostomy)
Hcukleberry Y. Am J Health-Syst Pharm 61(7):671-82Lewis et.al, BMJ 2001; 323:1-5
Parenteral Nutrition
Advantages DisadvantagesNot depend on normal GIT function
Mucosal atrophy risk of bacteria translocation
Better tolerated Access complications
More septic complications
$$$$
Evidence – early enteral feeding
Meta-analysis of controlled trials 11 studies 837 patients for elective GI surgery
Early enteral feeding vs. NPO + IVF
Clinical outcome measured• Anastomostic dehiscence• Infection
• Wound infection/ pneumonia/ intra-abd. abscess• Vomiting• Mortality
Lewis et.al, BMJ 2001; 323:1-5
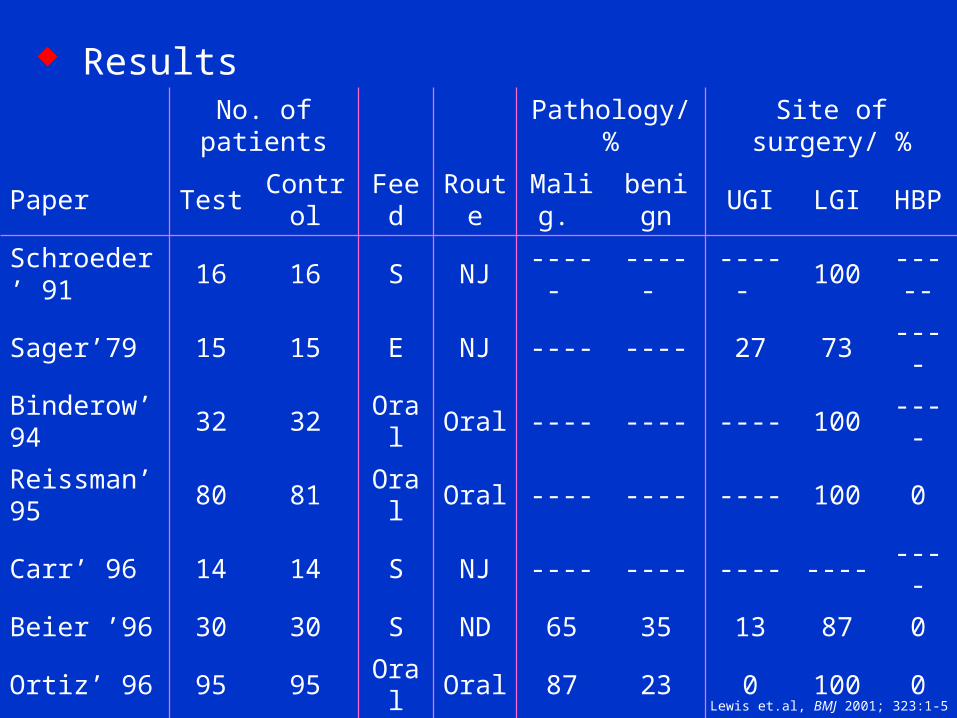
ResultsNo. of patients Pathology/ % Site of surgery/ %
Paper Test Control Feed Route Malig. benign UGI LGI HBP
Schroeder’ 91
16 16 S NJ ----- ----- ----- 100 -----
Sager’79 15 15 E NJ ---- ---- 27 73 ----
Binderow’94 32 32 Oral Oral ---- ---- ---- 100 ----
Reissman’ 95 80 81 Oral Oral ---- ---- ---- 100 0
Carr’ 96 14 14 S NJ ---- ---- ---- ---- ----
Beier ’96 30 30 S ND 65 35 13 87 0
Ortiz’ 96 95 95 Oral Oral 87 23 0 100 0
Heslin’ 97 97 98 IE J 93 7 51 0 49
Hastsell’ 97 29 29 S oral 64 28 0 100 0
Watters’ 97 15 16 S J 93 7 96 0 4
Stewart’ 98 40 40 Oral Oral ---- ---- 0 100 0
Lewis et.al, BMJ 2001; 323:1-5

Early Enteral Feeding
Lewis et.al, 2001
Comments ~
There seems to be no clear advantage to keeping patients nil by mouth after elective gastrointestinal resection.
Early enteral feeding may be of benefit.
Comparison – enteral vs. parenteral
Multi-centre RCT 10 centers 317 patients x elective surgery
“curative-intent” for GI malignancies
Enteral nutrition vs. parenteral nutrition to malnourished patients with GI cancers
Same calories and protein content
Clinical outcome measured• Primary end-point: complications• Secondary end-point: length of stay/
adverse effects (intolerance)
Bozzetti et.al, Lancet 2001, 358:1487-92

Enteral Parenteral
Patient no. 159 158
Mean pre-op serum albumin/ g/L 34 35
Premorbid state/ %
DM/ HT 11/ 13 11/ 16
cardiac/ respiratory disease 6/ 9 6/ 9
Types of operation done/ %
Subtotal gastrectomy 21 20
Total gastrectomy 26 24
Oesophagectomy 5 4
Whipple’s operation 16 16
Hepatectomy 5 4
APR 11 12
LAR 9 11
Bozzetti et.al, Lancet 2001, 358:1487-92
Patient Characteristics
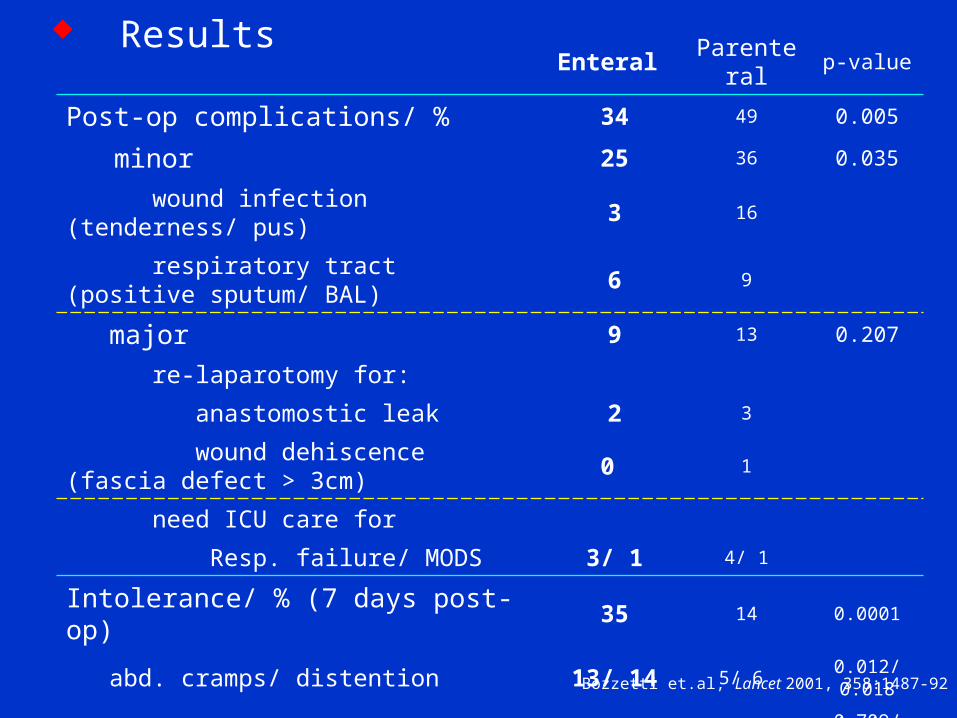
Results Enteral Parenteral p-value
Post-op complications/ % 34 49 0.005
minor 25 36 0.035
wound infection (tenderness/ pus) 3 16
respiratory tract (positive sputum/ BAL) 6 9
major 9 13 0.207
re-laparotomy for:
anastomostic leak 2 3
wound dehiscence (fascia defect > 3cm) 0 1
need ICU care for
Resp. failure/ MODS 3/ 1 4/ 1
Intolerance/ % (7 days post-op) 35 14 0.0001
abd. cramps/ distention 13/ 14 5/ 6 0.012/ 0.018
vomiting/ diarrhoea 3/ 8 2/ 6 0.709/ 0.385
Length of stay/ days 13.4 15.0 0.009
Mortality/ % 1.3 3.2Bozzetti et.al, Lancet 2001, 358:1487-92

Comment ~
Early enteral nutrition significantly reduces the complication rate and duration of postoperative stay compared with parenteral nutrition.
Although parenteral nutrition is better tolerated than enteral nutrition.

Immunonutrition
Nutrients that can influence
metabolic response to disease
Ward N, Nutritional Journal 2003; 2:18
Hcukleberry Y. Am J Health-Syst Pharm 61(7):671-82
1. Amino acids
glutamine
L-arginine
2. Fatty acids
Omega -3
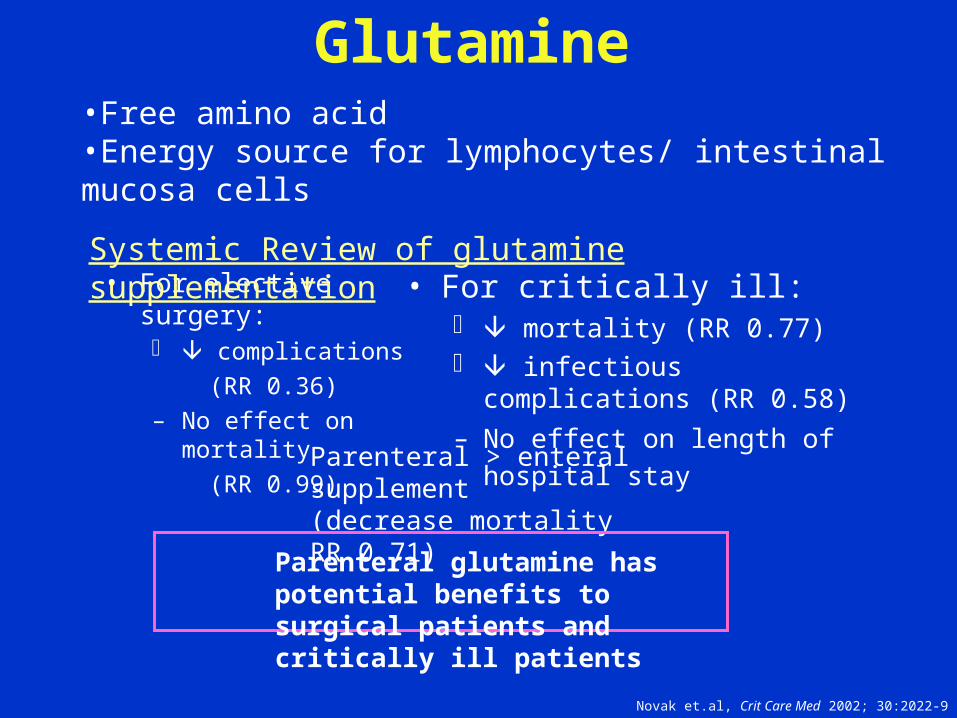
Glutamine
• For elective surgery: complications
(RR 0.36)
– No effect on mortality
(RR 0.99)
• For critically ill: mortality (RR 0.77) infectious complications (RR 0.58)
– No effect on length of hospital stay
•Free amino acid•Energy source for lymphocytes/ intestinal mucosa cells
Novak et.al, Crit Care Med 2002; 30:2022-9
Parenteral > enteral supplement (decrease mortality RR 0.71)
Systemic Review of glutamine supplementation
Parenteral glutamine has potential benefits to surgical patients and critically ill patients
Fatty acids• Omega – 3 fatty acids • Essential fatty acids
– Maintain cell membrane structure and function
Its metabolites I L/ PG regulate metabolic
process
L – Arginine• Highest nitrogen content• Semi – essential amino acid
Promote macrophage/ T-cell activity
Precursor for nitric oxide/ protein synthesis
Regulation of immune function
Under Research for
Hcukleberry Y. Am J Health-Syst Pharm 61(7):671-82
Conclusions
Early enteral nutrition intake
~ 24 – 48 hrs
If haemodynamically stableIntact GI tractOral diet >>> tube feeding
American Society of Parenteral & Enteral Nutrition Guideline 2004
European Society of Parenteral & Enteral Nutrition Guideline 2005

Conclusions
Exceptions
Intestinal obstruction or ileusIntestinal ischaemia
American Society of Parenteral & Enteral Nutrition Guideline 2004
European Society of Parenteral & Enteral Nutrition Guideline 2005

Conclusions
Exceptions
Intestinal obstruction or ileusIntestinal ischaemia
American Society of Parenteral & Enteral Nutrition Guideline 2004
European Society of Parenteral & Enteral Nutrition Guideline 2005
Parenteral Nutrition

www. Cartoonstock.com
Thank you