november 17, 2015 bojana babic md frcpc faap · · 2017-06-14mothers, families and society ......
TRANSCRIPT

Defining and Managing Medical Supplementation –
When is formula truly needed?
November 17, 2015
Bojana Babic MD FRCPC FAAP
1. Financial Disclosure
Nil
2. Unlabelled / Unapproved Use Disclosure Nil
Objectives:
• Review strategies to avoid early medical supplementation in the newborn
• Provide clarity on what are the medical indications for supplementation
• Review the strategies and importance of providing positive support to families when there are feeding challenges

Position Statement
• The Baby-Friendly initiative:
Protecting, promoting and supporting breastfeeding.
CM Pound, SL Unger Paediatr Child Health 2012;
17(6):317-21. Updated May 2015.

Position Statement
Breast milk:
– Provides many health benefits for infants, mothers, families and society
– Is species-specific
– Offers unique bioactive matrix
• Live cellular components
• Immunoglobulins
• Hormones
– Is the physiologic norm – we are mammals

Position Statement
Breastfeeding:
– Decreases incidence of many infectious diseases
– Reduces SIDS
– Enhances performance on neurocognitive testing
– Decreases the breast and ovarian cancer rate in mothers
– Delays ovulation
Position Statement
Breastfeeding:
– Leads to greater post-partum weight loss for the mother
– Is economical for families and society
– Benefits are manifold and cited by CPS, Health Canada, the WHO, UNICEF and many others


The Baby Friendly Initiative
• 1989 – the WHO and UNICEF developed “Ten Steps to Successful Breastfeeding”
• 1990 – Innocenti Declaration
• Critical Public Health Initiative

The Baby Friendly Initiative


Breastfeeding Policy 2015 10 Steps
Every facility providing maternity services and care for newborn infants should:
• Have a written breastfeeding policy that is routinely communicated to all health care providers and volunteers.
• Ensure health care staff have the knowledge skills necessary to implement this policy.
• Inform all pregnant women about the importance and process of breastfeeding. • Place babies skin-to-skin with their mother immediately following birth for at least
1 hour or completion of the first feed or as long as a mother wishes. • Assist mothers to breastfeed, and maintain lactation should they face challenges
including separation from their infants. • Support mothers to exclusively breastfeed for the first six months, unless
supplements are medically indicated. • Facilitate 24 hour rooming-in for all mother–infant dyads: Zero separation. • Encourage baby-led or cue-based breastfeeding. • Support mothers to feed and care for their breastfeeding babies without the use
of artificial teats or pacifiers (also called dummies or soothers) . • Provide a seamless transition of services between the hospital, community health
services and peer support programs.
Breastfeeding Policy 2015
Summary of the International Code of Marketing of Breast Milk Substitutes
• No advertising of these products to the public. • No free samples to mothers. • No promotion of products in healthcare facilities. • No company mothercraft nurses to advise mothers. • No gifts or personal samples to health workers. • No words or pictures idealizing artificial feeding, including pictures of infants on
the labels of the products. • Information to health workers should be scientific and factual. • All information on artificial infant feeding, including the labels, should explain the
benefits of breastfeeding and the costs and hazards associated with artificial feeding.
• Unsuitable products such as sweetened condensed milk should not be promoted for babies.
• All products should be of a high quality and take account of the climatic and storage conditions of the country where they are used.
What is normal (expected) volume intake and weight loss?
‘Normal’ Weight Loss Academy of Breastfeeding Medicine Protocol Committee, 2009
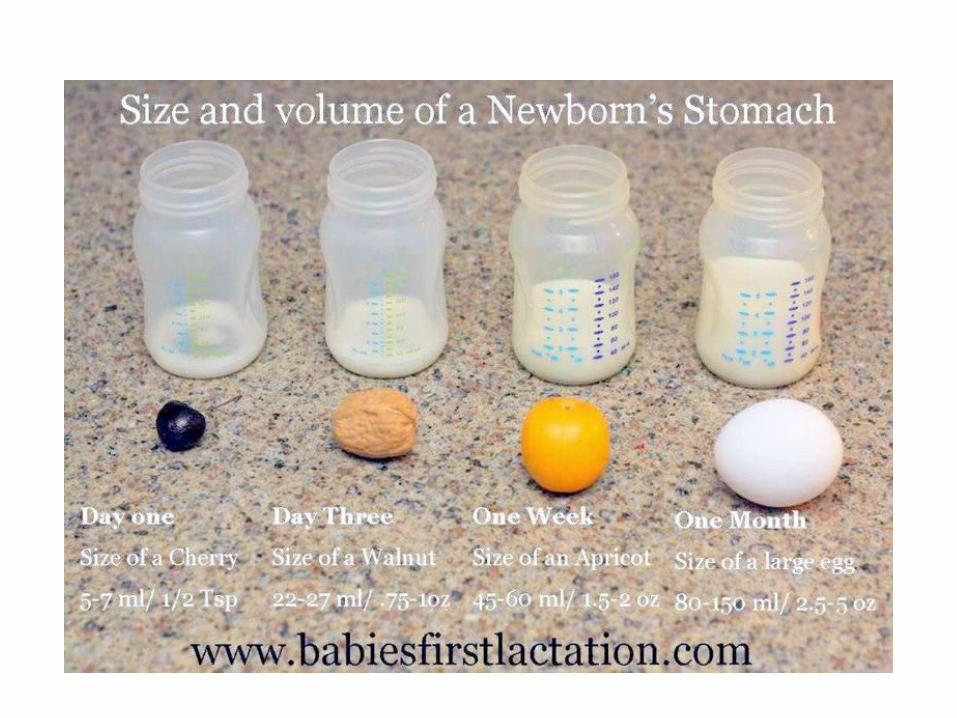
• Small colostrum feedings are appropriate for the size of newborn stomach
• Colostrum is sufficient to prevent hypoglycemia in the healthy, term, AGA infant
• It is easy to manage as the infant learns to coordinate sucking, swallowing and breathing
• Newborns lose weight because of the physiologic diuresis of ECF
• The ‘normal’ wt loss is 5-6 % in optimally breastfed infants and occurs at day 2-3, can range to 11.8%
• Optimally breast fed infants regain Bwt at an average of 8.3 days, with 97.5 % of them regaining it by day 21

Appropriate normal volumes
Newborn age Colostrum OR commercial formula
First 24 hrs 2-10 ml /feed for a range of 10-120/24 hrs (average is 37ml /24hrs)
30 ml/kg/24 hrs
24-48 hrs 5-15 ml/feed for an average total of 60-120ml/ 24 hrs
60 ml/kg/24 hrs
48-72 hrs: 90 ml/kg total in 24 hrs. 72-96 hrs: 120 ml/kg total in 24 hrs 96-120 hrs: 150-180 ml/kg/24 hrs

Expected Urinary and Stool Output of the Newborns
DAY URINE (per day) STOOL (per day)
1 1-2 voids At least 1 meconium
2 1-2 voids (may contain urate) At least 1 meconium or greenish transitional
3 3 or more (may contain urate) At least 3 brown, green or yellow
4 4 or more voids 3-4 soft seedy yellow stools
5 6 or more voids (no uric acid crystals) 3-4 soft seedy yellow
6-30 6-8 voids At least 3 soft yellow stools

When is it ok to supplement?
How should we do it?
Supplementary Feeding Policy
Acceptable Medical Reasons for Supplementation
• Babies with hypoglycaemia that does not improve with increased effective breastfeeding.
• Babies with dehydration that does not improve with increased
effective breastfeeding. - Serum sodium level of greater than or equal to 150mmol/L. - Baby has lost greater than 7% of birth weight in 24-48 hours
or greater than 10 % after 48 hours and: increased effective feeding has not helped, voiding and stooling patterns/appearance indicate dehydration

Supplementary Feeding Policy
Acceptable Medical Reasons for Supplementation
• Hyperbilirubinemia associated with ineffective breastfeeding or if accompanied by a significant weight loss/inadequate output. These babies are not meeting their minimal metabolic requirements – usually a milk transfer problem that may be resolved quickly with breastfeeding intervention.
• Babies with inborn errors of metabolism (I.e. Galactosemia or PKU) • Babies who are unable to feed at the breast due to congenital
malformations • Maternal medications that are contraindicated with breastfeeding Refer to mother risk at 416 813 6780 or academy of breastfeeding
medicine at www.bfmed.org or http://neonatal.ttuhsc/lact/

Supplementary Feeding Policy
Acceptable Medical Reasons for Supplementation
• Babies and mothers who are separated due to severe illness
• Delayed lactogenesis II (day 3-5 or later)
– Retained placenta
– Sheehan’s syndrome
– Primary glandular insufficiency
• Breast pathology or prior surgery
• Intolerable pain despite appropriate interventions

Supplementation is NOT indicated:
• Sleepy infant with fewer than 8-12 feeds in the first 24-48 hrs, otherwise well
• Fussy infant at night, constantly feeding for several hours
• Sleeping mother (exceptions?)

Supplement volumes combined with regular feeds: with the
exception of dehydration or hypoglycemia
Day Volume of supplement
1 5 ml to 15 ml per feed
2 15ml to 30 ml per feed
3 5-10 ml/kg per feed based on 8-12 feeds per day
4-ongoing Increasing amounts needed thereafter
160 ml/kg/day

Supplement volumes: For dehydration or hypoglycemia
• 5-10 ml/kg/feed (based on 8-12 feeds per day)
• Are we offering too much?
• It is not uncommon for a breastfeeding baby to be mildly
hypernatremic (serum Na+ 146-149 mmol/L) within the first 3-4 days of life and have normal outcomes,
• Hypernatremia is not related to breastfeeding; it is related to breastfeeding that is not going well.
• Actions to correct hypernatremia should not jeopardize the breastfeeding relationship between mother and baby
• Mothers should be assisted with breastfeeding techniques and assisted with establishing and maintaining their milk supply.

Options for Supplementation
• Expressed breast milk is the first choice for supplement
• Donor milk – LBW and critically ill
• Formula

Ways to Supplement
• Cup/spoon feeding (found to be safe in Prems)
• Finger feeding
• Lactation aid
• Syringe feeding
• Bottle feeding

How to Optimize Breastfeeding

How to Optimize Breastfeeding
• Skin to skin
• Initiate hand expression
• Antenatal education, in-hospital support, post discharge support (village of women)
• Room-in 24 hrs
• Anticipate who may need extra help, start hand-expression early, and bring in your LC support early:
– Late prem, LGA, SGA, bruised baby
– Primigravida, prolonged labour, C/S
• Educate parents regarding feeding choices – should be an informed decision


Effective Communication is a powerful tool
Is associated with:
Higher patient satisfaction
Better adherence to medication direction
Lower likelihood of mistakes
Fewer malpractice cases
Even affects patient health outcomes:
A review of research concluded that effective physician-patient communication improves patients’ emotional health, symptoms, physiologic responses, and pain levels

Challenges…

