neoplasms of the meninges james g. smirniotopoulos, m.d. professor of radiology and neurology...
TRANSCRIPT

NEOPLASMS OF THE MENINGES
James G. Smirniotopoulos, M.D. Professor of Radiology and Neurology
Chairman, Department of Radiology Uniformed Services University of the Health Sciences
4301 Jones Bridge RoadBethesda, MD 20814 USA
Voice: 301-295-3145FAX: 301-295-3893
Email: [email protected] us on the WEB at: http://rad.usuhs.mil

DISCLAIMER
The opinions expressed herein are those of the author(s), and are not necessarily representative of the Uniformed Services University of the Health Sciences (USUHS), the Department of Defense (DOD); or the World Health Organization (WHO). Medicine is a constantly changing field, and medical information is subject to frequent correction and revision. Therefore the reader is entirely responsible for verifying the accuracy and relevance of the information contained herein. Portions copyright 1997-2000 James G. Smirniotopoulos, M.D.

Meningioma
• 4 H or 5H Tumor• Most (75%) have Typical Imaging• Atypical Imaging =/= Atypical
Histology• Most (50-75%) Have Edema• Edema ~ Resection ~ Prognosis• Hemangiopericytoma is NOT a
meningioma
Meningioma - 4H/5H
• Hormonally Modulated F >> M• Hemispheric shape• Homogeneous
– hyperdense (CT)– enhancing
• Hyperostosis

PRIMARY MENINGEAL NEOPLASMS
1. MENINGIOMA:
a. Meningioma (typical and metaplastic) b. Atypical Meningioma c. Anaplastic (Malignant) Meningioma2. MESENCHYMAL (non‑meningothelial)3. Primary MELANOCYTIC Lesions4. UNCERTAIN Origin a. Hemangiopericytoma (pericyte) b. Hemangioblastoma (mesenchyme)

MENINGEAL TUMORS: WHO Grades
• MENINGIOMA I• (including most subtypes)• ATYPICAL MENINGIOMA II• PAPILLARY MENINGIOMA III• HEMANGIOPERICYTOMA II III
• ANAPLASTIC MENINGIOMA III

MENINGIOMASCell of Origin
• Dural Fibroblast ?• Arachnoid Cap Cell
– "meningothelial cell"– arachnoid granulations– dural sinuses esp. Sup.
Sag./Sphenoparietal

MENINGIOMABenign Subtypes - WHO I• SYNCYTIAL (Meningothelial)• FIBROBLASTIC (Fibrous)• TRANSITIONAL (Features of Both)• PSAMMOMATOUS• Microcystic (Humid), Secretory• METAPLASTIC FEATURES
– Lipoblastic, Osteoblastic, Chondroblastic
– Myxoid, Xanthomatous, Melanotic

MENINGIOMA:Etiologic Factors
• TRAUMA• RADIATION• VIRUSES• FAMILIAL NON-NF2• NEUROFIBROMATOSIS ‑ Type 2

MENINGIOMARadiation
• Immigrants to Israel (1940's)– Tinea Capitis– Superficial Low Dose (<800
cGray)– High Incidence of Meningioma
• High Dose (> 2000 cGray)

MENINGIOMAMolecular Biology
• Postulate Tumor suppressor Gene• Chromosome 22 ‑ deletion in tumor cells
– both sporadic and inherited– w/ or w/o NF‑2
• Homozygous for TWO wild-type copies is normal
• Heterozygous for 22 develops neoplasm– Because there is a subsequent loss of the
OTHER wild-type gene• Inherited (germline) deletion of 22
– w/Schwannoma = NF2

MENINGIOMAS• 1/7 to 1/4 of all Intracranial Primary
~ 6/ 100k / yearsmall ones in ~ 1.4% of autopsies
• 1/4 ‑ 1/3 of all Intraspinal Tumors• Middle age (40‑60)• Female > Male
cranial 2‑4:1spinal 4‑8:1– Progesterone receptors in 2/3– Estrogen receptors less common

MENINGIOMAS ‑ CT Findings
J. Neurosurg 71:665-672, 1989
• Retrospective, 1980‑1987• 193 Meningiomas, incidence
2.3/100K• Incidence increased to 8.4/100K in
8th decade• 2F:1M Benign, 1:1 for Malignant

Morphology
• Globose (spherical, hemispherical)• en plaque (pancake, crepe, wonton
wrapper, tortilla, pita ...)

MENINGIOMA - Location• Parasagittal 25%• Convexity 20%
• Ant. Basal 40%• Sphenoid 20%• Olfactory 10%• Suprasellar 10%
• Tentorial10%• Ventricular 5%

MENINGIOMAS ‑ CT FindingsJ. Neurosurg 71:665-672, 1989
• LOCATION INCIDENCE• Convexity 34%• Parasagittal 22%• Sphenoid Ridge 17%• Lateral Vent. 5%• Tentorium 4%• CRBLL Convex. 5%• Tuberculum 4%• Olfactory 3%• CPA 2%

MENINGIOMACT Imaging
• Non‑Contrast– Sharply Circumscribed– Homogeneous– Hyperdense (+/‑ Ca++)– NOT from psammoma bodies !– Broad Dural Surface– Bone Changes (Hyperostosis)
• Enhanced CT– Homogeneous Enhancement

MENINGIOMAS: CT Findings (193)
J. Neurosurg 71:665-672, 1989• BENIGN MENINGIOMAS:• Homogeneous Enhancement 72%• Heterogeneous Enhancement 23%• Calcification 27%• Hyperostosis 18%• Midline Shift (large) 72%• "Mushrooming" 0%

MENINGIOMAVasogenic Edema
• VASCULAR– parasitization of MCA, etc.– compression of cortical aa./vv.
• COMPRESSIVE TRAUMA• SECRETORY EFFECT• "TRANSCORTICAL FLOW"
– thinned cortex– gradient from meningioma into
brain
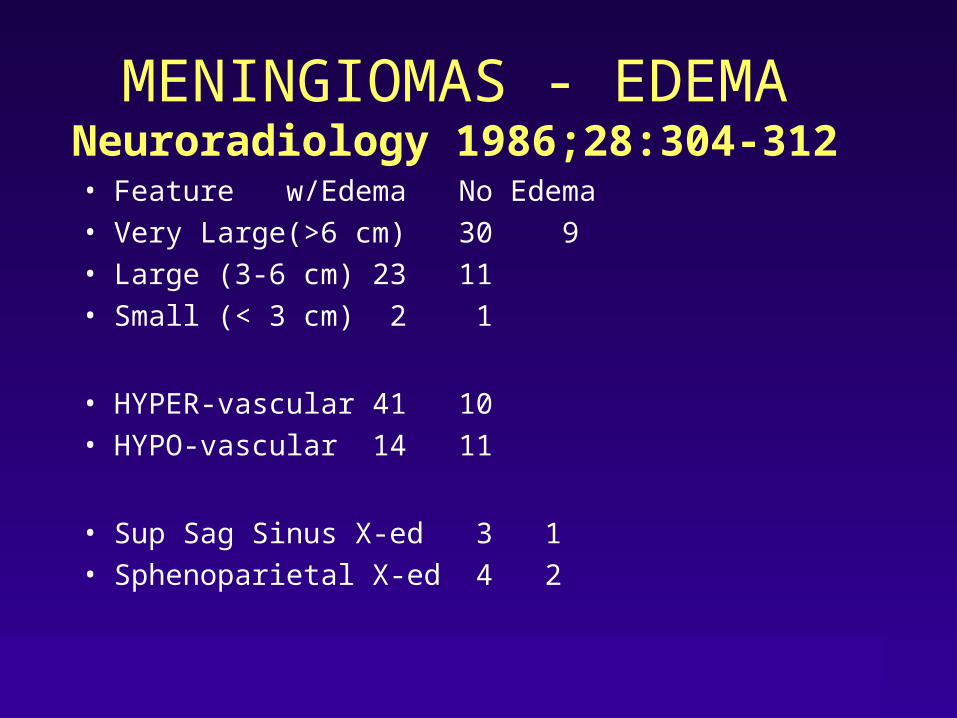
MENINGIOMAS ‑ EDEMANeuroradiology 1986;28:304-312
• Feature w/Edema No Edema• Very Large(>6 cm) 30 9• Large (3-6 cm) 23 11• Small (< 3 cm) 2 1
• HYPER-vascular 41 10• HYPO-vascular 14 11
• Sup Sag Sinus X-ed 3 1• Sphenoparietal X-ed 4 2

MENINGIOMASMR Imaging
• "Meningiomas are ISO‑intense."– usually on T1W– vary pulse sequence to see
• EXTRA‑axial Features– Gray‑matter buckling– Pseudo‑capsule of vessels– Meningeal/dural "TAIL"
• GADOLINIUM ENHANCEMENT

MENINGIOMA*Imaging Features: CT vs. MR
• Mass effect 88% 90%• Extraaxial Location 42% 70%• Broad Dural Attach. 74% 98%• Typical. Dense./Intensity 92% 74%• Hyperostosis 10% 14%• Homogeneous 76% 76%• Enhancement 96%(78%) 96%(80%)
(Homogeneous) • Meningeal. Enhance 2% 50%• “Capsule” 14% 68%
• *Neuroradiology 1990;32: 467-473

MENINGIOMAAngiography - Supply
• External Carotid 85%• Internal Carotid 63%• Tumor Blush 95%

MENINGIOMAAngiography - Transit
Time• Blush or Stain
– early arterial– prominent in VENOUS phase– capillaries/sm. arterioles– (too small to see individually)
• Venous Filling– characteristic if delayed– may fill with/ before Nl. vv.

MENINGIOMAAngiography - Transit
Time• Venous Filling (Stattin,1966)
– 170 Meningiomas– delayed in 136 (80%)– with Nl. vv. in 10 (6%)– earlier in 24 (14%) – ( 8 in early arterial phase)
• Leeds & Taveras (1969)– EDV in 6/36 (16%)

MENINGIOMAAngiography - Tumor
Blush• May come early• Usually very DENSE• Stays way too long• (Persistent!)
• The “In-Law Effect”

MENINGIOMAEffect on Skull
• Hyperostosis– w or w/o micro invasion
• Pressure Erosion– periosteal remodeling
• Bone Destruction– (micro invasion)

HYPEROSTOSIS IN MENINGIOMAS

MENINGIOMAHyperostosis
• 15 - 90% of Meningioma– more common with subfrontal and
en plaque• Does NOT prove invasion of bone
– “sympathetic change” (Alk. Phos.?)• Implies CHRONICITY and benign
behavior• Skull Base
– Invasion via Haversian Canals

Hyperostosis - DDX
• Increased Density– Paget Disease– Fibrous Dysplasia– Metastasis
• Breast• Prostate• Lymphoma
– Ca++ Hematoma• SDH• Cephalohematom
a
• Widened Diploe– Paget disease– Fibrous Dysplasia– Dilantin Tx– Tx Hydrocephalus– Ca++ Hematoma
• SDH• Cephalohematoma

Atypical “Meningioma”
• Atypical Imaging– 25% of meningioma
• Atypical Pathology– Atypical meningioma ( 5- 7%)– Malignant meningioma ( 1-3%)
• Hemangiopericytoma ( 1.5 - 2.5 %)

MENINGIOMAAtypical Imaging
• Focal Lucency Outside (arachnoid cyst)
• Focal Lucency Inside (necrosis, cyst)• Hypodensity ("humid", lipoblastic)• Focal Hyperdensity (metaplasia,
hemorrhage)• Heterogeneous• Hyperintensity on T1W• Hyperintensity on T2W

MENINGIOMACysts
• Inside of neoplasm– (rim enhancement)
• Between tumor and brain– ("arachnoid cysts")
• Inside Brain– PIA separates tumor from brain– ?? Result of Chronic Edema– Vacuolization of White Matter

MENINGIOMAAtypical Histology
• Atypical Meningioma ~ 5-7 % • Anaplastic Meningioma ~ 1-3%
~ 0.2 / 100k per year• Higher incidence of Recurrence• Shorter time to Recurrence• "Atypical Histology"
necrosisexcessive mitoses* invasion into brain

Meningioma:Brain Invasion
• Independent Variable for Prognosis– Decreases Resectability– Increases Recurrence
• Seen more often with Atypical/Anaplastic– Can occur with “benign”
meningioma• Associated with EDEMA
– but not necessary for Edema
MENINGIOMA“Malignant
Meningioma”• Anaplastic (Malignant) Meningioma• Papillary Meningioma• "Benign" Metastasizing
Meningioma• Hemangio‑Peri‑Cytoma (HPC)• Malignant Fibrous Histiocytoma
(MFH)

Hemangiopericytoma
• Syn: “angioblastic meningioma”• Cell of Origin - perivascular
pericyte of Zahn• <1% of primary CNS• M 1.4:1 F• Age - 40’s• Dural based, bone destruction,
lobulated

HEMANGIOPERICYTOMA(HPC)
• Narrow dural base ("Mushrooming")• No Hyperostosis• Lobulated (not hemispheric)• Internal Signal Voids (on MRI)
– irregular and multiple• Hypervascular on Angio
– irregular patterns

MENINGIOMARadiologic Features -
CT• Feature Benign/Malignant• Homogeneous Enhancement 72% /36%
• Heterogeneous Enhancement 23% /64%
• Hyperostosis 18% / 7%• Calcification 27% / 0%• “Mushrooming” 0% /57%
– narrow attachment and larger “cap” invaginating into brain

HEMANGIOPERICYTOMAParkway Deli Sign
• Parkway Delight Reuben• PastramiCorned Beef• Cole Slaw Sauerkraut• Muenster Swiss Cheese• Thousand Island Russian Dressing
• PumpernickelRye Bread
Parkway Delight Vs. Rueben
Pastrami Corned BeefColeslaw Sauerkraut
Thousand lsand Russian
Muenster SwissPumpernikel Rye Bread

Just Like a Rueben!Except ...
Parkway Delight Vs. Rueben
Pastrami Corned BeefColeslaw Sauerkraut
Thousand lsand Russian
Muenster SwissPumpernikel Rye Bread

HEMANGIOPERICYTOMAParkway Deli Sign
• Hemangiopericytoma <> Meningioma
• Narrow Base Broad-based• Bone Destruction Hyperostosis• Heterogeneous Homogeneous• Large Irregular Vessels Spoke-
wheel• Lobulated Hemispheric
Hemangiopericytoma Vs. Meningioma
Narrow Base Broad BaseLobulated Hemisphere
Heterogeneous Homogeneous
Bone Destruction HyperostosisLarge I rregular
VesselsSpoke Wheel
Vessels

MENINGIOMA Summary: The 4H - 5H
Tumor• Benign, slowly growing• Arachnoid Cap Cell, meningothelial• Sharply Circumscribed EXTRA‑axial• Hemispheric / en plaque• Broad‑based on DURA• HPC is NOT a meningioma

Meningioma:Suggestive Features
• Homogeneous Hemispheric Mass• Broad Dural Base• Hyperostosis• Transdural Mass (falx, tentorium)• Hyperdense on Plain CT• Dural Tail • ~ GM Signal on MR

Bibliography
Amundsen P, Dugstad G, Syvertsen A. The reliability of computer tomography for the diagnosis and differential diagnosis of meningioma, gliomas, and brain metastasis. Acta Neurochirurgica 1978;41:177-90.
Aoki S, Sasaki T, Machida T, Tonioka H. Contrast-enhanced MR Images in Patients with meningioma: Importance of enchancement of the dura adjacent to the tumor. AJNR Am J Neuroradiol 1990;11:935-8.
Aoki S, Sasaki Y, Machida T, and Tanioka H. Contrast-Enhanced MR Images in Patients with Meningioma: Importance of Enhancement of the Dura Adjacent to the Tumor. AJNR 1990;11935-8.
Ayton Hope JK, Armstrong DA, Babyn PS, Humphreys RR, Harwood-Nash DC, Chuang SH, and Marks PV. Primary Meningeal Tumors in Children: Correlation of Clinical and CT Findings with Histologic Type and Progress. AJNR 1992;131353-64.
Becker D, Norman D, Wilson C. Computerized tomography and pathological correlation in cystic meningiomas: Report of two cases. J Neurosurg 1979;50:103-5.
Bradac G, Ferszt R, Bender A, Schorner W. Peritumoral edema in meningiomas; a radiological and histological study. Neuroradiology 1986;28:304-12.
Bradac GB, Ferszt R, Bender A, Schorner. "Peritumoral edema in meningiomas. A Radiological and Histological Study. Neuroradiology 28 (1986): 304-312 1994;304-312.
Buetow MP, Buetow PC, Smirniotopoulos JG. Typical, atypical, and misleading features in meningioma. Radiographics 1991;11:1087-106.
Bydder G, Kingsley P, Brown W, Neindorf P, Young I. MR. imaging of meningiomas including studies with and without gadolinium-DTPA. J Comp Assist Tomogr 1985;9(6):690-7.
Chiechi M, Smirniotopoulos JG, Mena H. Intracranial hemangiopericytomas: MR and CT features. AJNR 1996;17:1365-71.
Demaerel P, Wilms G, Lammens M, and et al. Intracranial meningiomas: Correlation between MRI and histology in fifty patients. J Comp Assist Tomogr 1991;15(1):45-51.
Domenicucci M, Santoro A, D'Osvaldo DH, Delfini R, Cantore GP, Guidetti B. Multiple Intracranial Meningiomas. J Neurosurg 1989;70:41-44. 1989.
Eljamel MSM, Foy PM. Multiple Meningiomas and Their Relation to Neurofibromatosis. Review of the Literature and Report of Seven Cases. Surg Neurol 1989;32:131-136.
Elster A, Challa V, Gilbert T, Richardson D, Contento J. Meningiomas: MR and histopathologic features. Radiology 1989;170:857-62.
Goldsher D, Litt AW, Pinto RS, Bannon KR, and Kricheff II. Dural "Tail" Associated with Meningiomas on Gd-DTPA-enhanced MR Images: Characteristics, Differential Diagnosis Value, and Possible Implications for Treatment. Radiology 1990;176447-50.
Gupta S, Gupta RK, Banerjee D, Gujral RB. Problems with the dural tail sign. Neuroradiology 1993;35:541-2.
Hilal S, Chang C. Specificity of computed tomography in the diagnosis of supratentorial neoplasms: Consideration of metastasis and meningiomas. Neuoradiology 1978;16:537-9.
Jelinek J, Smirniotopoulos JG, Parisi JE, Kanzer M. Lateral ventricular neoplasms of the brain: differential diagnosis based on clinical, CT, and MR findings. AJR 1990;155:365-72.
Kaneko T, Harada A, Isshiki K, Murakami H, Nakao A, Nonami T, Yano M, Kakumu S, Takagi H. Hemangiopericytomatous meningioma metastasized to the liver: report of a case and review of the literature. Surg Today 1993;23:644-8.
Kaplan RD, Coons S, Drayer BP, Bird CR, and Johnson PC. MR Characteristics of Meningioma Subtypes at 1.5 Tesla. J Comput Assist Tomogr 1992;16(3):366-71.
Kendall B, Pullicino P. Comparison of consistency of meningiomas and CT appearance. Neuroradiology 1979;18:173-6.
Kepes JJ. Meningiomas. biology, pathology and differential diagnosis. New York: Masson; 1982;
Kim KS, Rogers LF, and Lee C. The dural lucent line: Characteristic sign of hyperostosing meningioma en plaque. AJR 1983;1411217-21.
Kleihues P, Burger PC, and Scheithauer BW. The New WHO Classification of Brain Tumours. Brain Pathology 1993;3(3):255-68.
Kutcher TJ, Brown DC, Maurer PK, Ghaed VN. Dural tail adjacent to acoustic neuroma: MR features. J Comput Assist Tomogr 1991;15:669-70.
Leroux P, Hope A, Lofton S, Harris A. Lipomatous meningioma: A uncommon tumor with distinct radiographic findings. Surg Neurol 1989;32:360-5.
Nagele T, Petersen D, Klose U, Grodd W, Opitz H, Voigt K. The dural tail adjacent to meningiomas studied by dynamic contrast-enhanced MRI: a comparison with histopathology. Neuroradiology 1994;36:303-7.
Ortiz O, Schochet SS, Kotzan JM, Kostick D. Meningioma of the optic nerve sheath. AJNR Am J Neuroradiol 1996;17:901-6.
Pasquier B, Gasnier F, Pasquier D, Keddari E, Morens A, and Couderc P. Papillary meningioma. Clinicopathologic study of seven cases and review of the literature. Cancer 1986;58(2):299-305.
Perrott-Applanat M, Groyer-Picard M, and Kujas M. Immunohistochemical Study of Progersterone Receptors in Human Meningioma. Acta Neurochir 1992;(115):20-30.
Pullicino P, Wilbur D, Levy R, Eskin T, Kido D. Infarction in a meningioma after cardiac arrest. Arch Neurol 1983;40:456-7.
Pulst S, Rouleau G, Marineau C, Fain P, Sieb J. Familial meningioma is not allelic to neurofibromatosis 2. Neurology 1993;43:2096-8.
Rengachary Se. Cystic lesions associated with intracranial meningiomas. Neurosurg 1979;4:107-14.
Rohringer M, Sutherland G, Louw D, Sima A. Incidence and clinicopathological features of meningioma. J Neurosurg 1989;71:665-72.
Sheporaitis LA, Osborn AG, Smirniotopoulos JG, Clunie DA, Howieson J, D'Agostino AN. Radiologic-Pathologic Correlation: Intracranial meningioma. AJNR 1992;13:29-37.
Smirniotopoulos JG, Yue NC, Rushing EJ. Cerebellopontine angle masses: radiologic-pathologic correlation. Radiographics 1993;13:1131-47.
Tien RD, Yang PJ, Chu PK. Dural tail sign: a specific MR sign for meningioma? J Comput Assist Tomogr 1991;15:64-6.
Tokumaru A, O'uchi T, Eguchi T, Kawmoto S, Kokubo T, Suzuki M, Kameda T. Prominent meningeal enhancement adjacent to meningioma on go-DTPA-enhanced MR Images. Histopathologic Correlation. Radiology 1990;175:431-3.
Wilms G, Lammens M, Marchal G, and et al. Thickening of dura surrounding meningiomas: MR features. J Comput Assist Tomogr 1989;13763-8.