natural history of lumbar disc hernias: does gadolinium ... · history of lumbar disc hernias: does...
TRANSCRIPT

R
O
Ne
AS
a
b
c
d
e
R
n
2
Document downloa
adiología. 2013;55(5):398---407
www.elsevier.es/rx
RIGINAL ARTICLE
atural history of lumbar disc hernias: Does gadoliniumnhancement have any prognostic value?�
. Ramos Amadora,∗, M. Alcaraz Mexíab, J.L. González Preciadoc,. Fernández Zapardield, R. Salgadoe, A. Páeza,b,c,d,e
Departamento de Radiología, Hospital Universitario de Getafe, Getafe, Madrid, SpainDepartamento de Radiología, Hospital Santa Cristina, Madrid, SpainDepartamento de Radiología, Hospital Virgen de la Salud, Toledo, SpainDepartamento de Radiología, Fundación Hospital Manacor, Manacor, Mallorca, SpainDepartamento de Urología, Hospital de Fuenlabrada, Fuenlabrada, Madrid, Spain
eceived 13 October 2010; accepted 30 October 2011
KEYWORDSHerniated disc;Sciatica;Magnetic resonanceimaging;Contrastenhancement
AbstractObjectives: To evaluate the percentage of disc hernias that have disappeared after one yearof follow-up and the time to disappearance. To determine whether gadolinium enhancementis useful for predicting whether the hernia will disappear. To analyze whether the pattern ofenhancement can help predict whether the fragment will disappear.Materials and methods: This prospective study included 118 patients with acute symptoms oflumbosciatica and a herniated disc diagnosed by CT. In 72 patients, we performed gadolinium-enhanced MRI every 6 months for one year or until the herniation disappeared; we relatedthe findings of protrusion, extrusion, and the enhancement pattern with the disappearance orpersistence of herniated disc material. We analyzed the results with univariate and multivariatestatistics.Results: The 59% of the hernias disappeared within 1 year of follow-up and 66% disappearedwithin the first 8 months of follow-up. The 83% of the extruded hernias disappeared, and this wassignificant in the multivariate analysis (p < .005). The absence of enhancement was significantlyassociated with the persistence of the hernia in the univariate analysis. The enhancement pat-tern was not useful for predicting whether the hernia would disappear. Five hernias disappearedwithin the first two months.
ded from http://zl.elsevier.es, day 28/05/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
Conclusions: A high percentage of disc hernias disappear. We found a significant association
between extrusion and disappearance but no correlation between the pattern of gadoliniumuptake and the disappearance of the hernia.© 2010 SERAM. Published by Elsevier España, S.L. All rights reserved.� Please cite this article as: Ramos Amador A, Alcaraz Mexía M, González Preciado JL, Fernández Zapardiel S, Salgado R, Páez A. Historiaatural de la hernia de disco lumbar. ¿Tiene el realce con gadolinio valor pronóstico? Radiología. 2013;55:398---407.∗ Corresponding author.
E-mail address: [email protected] (A. Ramos Amador).
173-5107/$ – see front matter © 2010 SERAM. Published by Elsevier España, S.L. All rights reserved.

The natural history of disc herniation: Value of gadolinium 399
PALABRAS CLAVEHernia de disco;Ciática;Resonanciamagnética;Realce de contraste
Historia natural de la hernia de disco lumbar. ¿Tiene el realce con gadolinio valorpronóstico?
ResumenObjetivos: Evaluar qué porcentaje de hernias de disco desaparece tras un ano de seguimientoy a qué ritmo; valorar si el uso del realce con gadolinio en RM tiene valor predictivo de ladesaparición de la hernia; y estudiar si el patrón del realce ayuda a predecir la desaparicióndel fragmento.Material y métodos: Se incluyeron en este estudio prospectivo 118 pacientes con clínica delumbociática aguda y que presentaban una hernia de disco diagnosticada mediante TC. A 72pacientes se les realizó una RM con gadolinio cada 6 meses hasta el ano o hasta que la hernia dedisco desaparecía, y se relacionó la presencia de protrusión, extrusión y el patrón de realce conla desaparición o persistencia del material discal. Se realizó un estudio estadístico univariabley multivariable.Resultados: Un 59% de las hernias de disco desaparecieron tras un ano de seguimiento, yde ellas el 66% lo hicieron en los primeros 8 meses. Un 83% de las hernias extruidas desa-parecieron, y este dato tiene significación estadística en el análisis multivariable (p < 0,005).La ausencia de realce tiene asociación con la persistencia de la hernia, con significaciónestadística en el análisis univariable. El patrón de realce no ayuda a predecir la desapari-ción de la hernia. Hubo 5 hernias que desaparecieron muy pronto, dentro de los primeros2 meses.Conclusiones: Un alto porcentaje de hernias de disco desaparecen, se ha encontrado la aso-ciación estadísticamente significativa entre extrusión y desaparición, y falta de correlaciónentre el patrón de captación de gadolinio y la desaparición de la hernia.© 2010 SERAM. Publicado por Elsevier España, S.L. Todos los derechos reservados.
cpiw
M
WttRtsnmpip
Document downloaded from http://zl.elsevier.es, day 28/05/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
Introduction
Among the different causes of severe lumbosciatica lum-bar disc hernia is one of the most important of all.1 Mostpatients do well with conservative therapy.2---6 However someauthors claim surgery is the best therapy in the short term.7
Some studies8---12 claim that one of the most important causesof improvement is to shrink size of hernia. Other authorsthink that the change of size and shape of hernias do notexplain their clinical evolution.13,14 As a matter of fact thereare several immunological, vascular and biochemical fac-tors that can produce the patients’ painful presentationwith no mass effect or root compression.15,16 This is whyit is not clear if the ideal therapy is conservative or surgi-cal therapy.7,8 Nevertheless conventional wisdom on surgicaltherapy is based on the roots’ mechanical compression bythe disc hernia and this is why if hernia disappears spon-taneously surgical therapy can only be considered in caseswhere there is a serious deterioration of the patients’ qual-ity of life.
One of the important factors speaking against surgeryis risk of back surgery syndrome unforeseen by clinical ormorphological data.
One important aspect of disc hernia evolution is its rela-tion to gadolinium enhancement. Some descriptions say thisenhancement is associated to a good evolution and evendisappearance of hernia.13,17,18 These are retrospective orprospective studies with few patients.13,17,18 In a prospec-
tive study with a great number of patients they only did MRmonitoring at 6 months.19Purpose of this prospective study is analyze the followingissues:
aCti
Assessment after one year of follow-up the percentage ofhernias that finally go away and how fast they do so.Assessment if presence of gadolinium enhancement at thedisc hernia is a factor predisposing to disappearance ofhernia.Assessment if there is some enhancement pattern associ-ated to the disappearance of hernia.
Our work has been planned from an anatomoradiologi-al viewpoint since in the correlation existing between theresentation and the disc hernia there are several factorsnvolved other than mechanistic ones.2---20 Thus correlationith clinical evolution has not occurred.
aterials and methods
e are talking about a prospective study of 118 consecu-ive patients with lumbosciatica and disc hernia diagnosedhrough CT at 26 months. Study was approved by Hospitalesearch Committee (600-bed-2nd degree academic hospi-al) and obtained informed consent from all patients. Ourtudy is basically an anatomoradiological study to analyzeatural history of hernia. Because of the difficult anato-oclinical correlation known to these types of hernia,13,14
resentation was not taken into consideration---just as annitial way of selection. Our series is therefore made up ofatients with lower back pain or lumbosciatalgia 3 weeks
fter medical therapy---when disc hernia was found throughT. In our work we did not assess the type of conservativeherapy and its possible relation to the evolution of anatom-cal or enhancement findings.
4
MC
f
sdi6cns
5G1
Vf(sT25soMsa
ae
ohidb
fawhmw
hccdw
dds
oofidwaio
I
Fep
sits
R
T
Document downloaded from http://zl.elsevier.es, day 28/05/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
00
These were inclusion criteria:
Lower back pain and lumbosciatalgia of over 3 monthsduration.CT showing major disc hernia > 3 mm.Informed consent to do a gadolinium-enhanced MR.
These were the exclusion criteria:
Disc hernia < 3 mm.Moderate or severe stenosis at the lower back rachidealchannel.Spondylolisthesis > stage 2.Cases of a difficult differential diagnosis between herniaand disc bulging.Claustrofobia or other MR complications.
All patients underwent an initial gadolinium-enhancedR after obtaining informed consent. Average time betweenT and MR was just 2 months.
In time 46 patients were excluded from the study for theollowing reasons:
15 underwent surgery.31 were lost to follow-up due to patients’ denial to undergoan MR.
A total of 72 patients with 80 disc hernias entered thetudy. Of these only 5 underwent the initial MR showingisappearance of hernia. Sixty-seven patients were pend-ng study through a gadolinium-enhanced follow-up every
months and for one year or until hernia was gone. In 26ases we only did 2 MR studies due to disappearance of her-ia during first control. In the remaining 45 cases we did 5tudies.
Disposition of patients in the study:
Initial: 118 with TC and presence of disc hernia.Excluded: 46 patients.Initial MR: 72 patients.One MR: 5 patients.Two MR: 26 patients.Three MR: 41 patients.
A conventional L3-S1 transversal slices 5 mm thick every mm-Somatom® HQ (Siemens Medical Solutions, Erlangen,ermany) was used for CT scans; 512 × 512 matrix; 25 cm20---140 kV-vision field.
All MR scans were done with a 1.5 Tesla (Magneton-ision, Siemens Medical Systems, Erlangen, Germany) withollowing sequences, all of them obtained with 3 mm thick10% separation) and 3 acquisitions: sagittal T1-weightedpin-echo (TR/TE: 800 ms/12 ms; matrix: 512 × 256), axial1-weighted spin-echo (TR/TE: 894 ms/12 ms; matrix:56 × 256), and sagittal T2-weighted fast spin-echo (TR/TE:500/128 ms; matrix: 322 × 512). Both sagittal and axialequences on T1 were obtained after IV administration
f 0.1 mmol per kg of Gadoteridol (ProHance®, Bracco,ilan, Italy) with the same parameters that non contrastequences. Interval between the administration of contrastnd the beginning of the first sequence was 30 s.
hllv
A. Ramos Amador et al.
Systematically all patients were assessed according toge, gender, level of hernia and presence and type of hernianhancement.
Following criteria by the American Society of Spin Radi-logy and the American Society of Neuroradiology,22 discernia was defined as a disc material spreading beyond thenterverbral disc it comes from in a focal way---different fromisc buldging where the disc margin spreads not in a focalut in a diffuse way.
Protrusion was seen as the asymmetrical expansion ofocal disc spreading beyond the disc it comes from with anxis in any inferior level to the disc seat. Finally extrusionas achieved when the asymmetrical expansion of focal discad a base at the disc it comes from, inferior to the maxi-um extension diameter of such border. One loose fragmentas considered extrusion.
Gadolinium enhancement was classified as peripheral,omogeneous or heterogeneous. In the peripheral one theontrast had the shape of a ring surrounding a non-enhancedenter. Homogeneous enhancement enhanced most of theisc, and heterogeneous enhancement existed when thereas a hernia enhancement associated to unenhanced areas.
Degree of hernia shrinkage was classified as:
Disappearance: when over 90% of disc material was gone.Shrinkage of over 50%.Shrinkage of less than 50%.Unchanged.
Hernia was gone in 5 patients when the first MR scan wasone. Absolute size of hernia was not taken into accounturing the follow-up of our patients considering that mosttudies do not give meaning to these data.13,17---20
Assessment of MR scans in relation to location, evolutionf size, type of hernia or contrast enhancement was carriedut independently in a delayed way by 2 readers---the tworst authors with huge experience in spine MR. When theyisagreed a consensus reading was carried out. Size of herniaas measured at the axial image in a perpendicular pointpart from the disc. Situation of hernia at the axial image orts signal features on T1 or T2 sequences were not assessedn the axial level---central, lateral, foraminal.
Statistical study was done with software SPSS 11.0 (SPSSnc., Chicago, IL, USA).
Univariate analysis was done through Chi-Squared test orisher’s Exact Test. Demographic values, gender, age andnhancement patterns correlated to persistence or disap-earance of hernia.
Multivariate logistic regression analysis assessing per-istence or disappearance of hernia was carried out withndependent variables associated with age, gender, loca-ion, and enhancement pattern. p < 0.05 was statisticallyignificant.
esults
able 1 shows univariate analysis of 75 MR-scanned disc
ernias associated with hernia disappearance, age, gender,evel and type of hernia and contrast enhancement. If weook at this table we can see that contrast enhancement wasery common (93.3%). Lack of enhancement only happened
The natural history of disc herniation: Value of gadolinium 401
Table 1 Univariate analysis of 75 disc hernias. Association between disappearance of hernia and age, gender, level of hernia,type of hernia and contrast enhancement.
# hernias (%) # hernias gone (%) p value*
Age <35 years 18 (24) 12 (66.7)35 ---44 13 (17.3) 6 (46.2) 0.71045---54 33 (44) 18 (54.5)>54 11 (14.7) 6 (54.5)
Gender Males 44 (58.7) 26 (59) 0.521Females 31 (41.3) 16 (48.4)
Level of hernia L3-L4 6 (8) 3 (50) 0.562L4-L5 23 (30.7) 15 (65)L5-S1 46 (61.3) 24 (52.2)
Type of hernia Extruded 24 (32) 20 (80.31) <0.001Protruded 51 (68) 22 (43.1)
Gadolinium-enhancement Present 70 (93.3) 42 (60) 0.562Absent 5 (6.7) 0 <0.01
Type of gadolinium-enhancement Homogeneous 19 (27) 14 (63) 0.576Heterogeneous 15 (21.2) 9 (60)Peripheral 36 (51.5) 19 (65.5)
Document downloaded from http://zl.elsevier.es, day 28/05/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
* Chi-Squared test or Fisher’ Exact Test for small values.
in 6.7% of patients and held a significant statistical corre-lation to persistence of hernia. The most common contrastenhancement was peripheral enhancement (50.6%), yet noone enhancement had any significant statistical relations tohernia disappearance. Figs. 1---3 show some good examplesof types of enhancement. There were no changes in the typeof enhancement during follow-up (not shown in the table).
The most important findings associated with change ofsize in disc hernia during time are shown in Tables 2 and 3.Table 2 shows in time the number of disc hernias gone sinceCT was done. Total number of disc hernias gone was 47% outof a total of 80 (Fig. 4), of these 66% in less than 8 months
and the rest in the remaining 6 months.Table 3 shows relation between changes of size in 80disc hernias during follow-up year. Among those that did not
Table 2 Natural history of disc hernia gone: evolution intime.
Time Number %
<2 months 5 112---8 months 26 558---14 months 16 34
Total 47 100
Table 3 Disc hernias: evolution of size.
Number %
Gone 47 59Unchanged 17 21Increase in size 3 4Shrinking < 50% 9 11Shrinking > 50% 4 5
Total 80 100
Figure 1 Homogeneous enhancement. T1-weighted sequen-ces, axial level. (A) No contrast image. Extruded disc hernia(arrow) on L5-S1 with partial occupation of left lateral recessand slightly compression of root S1. (B) Image after contrast.Homogeneous enhancement (arrow) of disc hernia.

402 A. Ramos Amador et al.
Figure 2 Heterogeneous enhancement. T1-weighted sequen-ces, axial level. (A) No contrast image. Large hernia (arrow) onLg
gis
7id
1
23
4
Figure 3 Peripheral enhancement (in ring). T1-weighted se-quences, axial level. (A) No contrast image. Extruded dischc
5
ghd
D
Ftc
sdhard to quantify. Busch et al. did a prospective CT-study with
Document downloaded from http://zl.elsevier.es, day 28/05/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
5-S1 compressing thecal sac. (B) Image after contrast. Hetero-eneous enhancement of disc hernia.
o away 17 did not show any changes (21%). There was anncrease in size in 3 hernias (3.7%); in 9 hernias there wasize shrinkage <50% (11%) and in 4 size shrinkage >50% (5%).
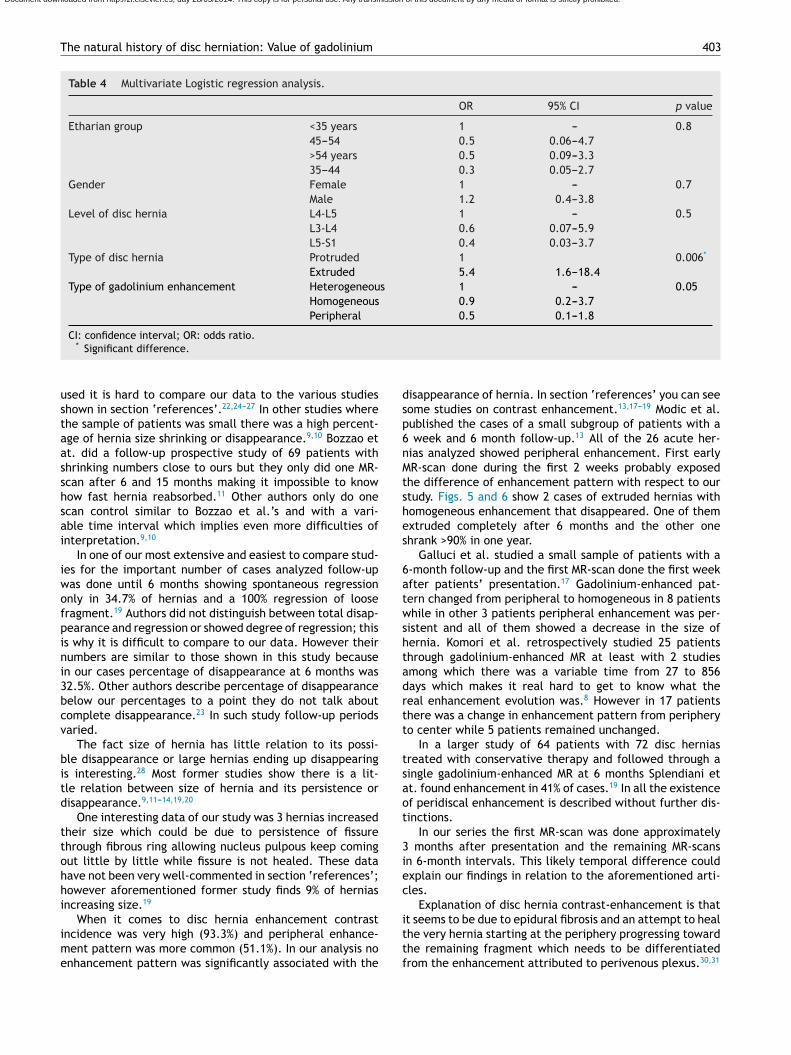
Table 4 shows multivariate analysis of 67 patients with5 disc hernias (8 of them had level two-disc hernias) stud-ed with the help of gadolinium and associated with theisappearance of hernia.
In all tables these were the most revealing findings:
. Fifty-nine per cent of hernias disappeared---among these66% in less than 8 months. Also 5% of hernias shrank >50%.Adding all up we have some 64%.
. Twenty-one per cent of hernias remained unchanged.
. Percentage of extruded disc hernias gone was veryhigh (83.3%). Univariate analysis showed some signifi-cant association between disappearance of hernia and
extruded hernias (p < 0.05).. Lack of hernia enhancement was associated with its per-sistence (p < 0.001).
aoo
ernia with loose fragment on L5-S1 (arrow). (B) Image afterontrast. Intense annular enhancement of disc hernia.
. The only statistically significant data on multivariateanalysis was extruded disc hernia (p < 0.006). This anal-ysis strengthens univariate analysis as it was doneregardless of other analyzed factors like age, gender,or level of hernia. Extruded hernias are 5.4 times morelikely to disappear than protruded hernias.
Analyzing data from the aforementioned tables, age,ender, location, and contrast enhancement pattern do notave statistical significance as prognostic factors of herniaisappearance.
iscussion
ormer studies on the natural history of disc hernias showrend toward reducing size and disappearance in a high per-entage of untreated hernias.
Cervical spine seems to have a similar natural history in atudy of few patients.21 In lumbar spine hernia shrinkage orisappearance seems hard to evaluate in time and frequency
large group of patients.4 CT and MR offer a similar degreef information in the evaluation of disc hernia but becausef the lack of consent and normalization in the terminology
The natural history of disc herniation: Value of gadolinium 403
Table 4 Multivariate Logistic regression analysis.
OR 95% CI p value
Etharian group <35 years 1 --- 0.845---54 0.5 0.06---4.7>54 years 0.5 0.09---3.335---44 0.3 0.05---2.7
Gender Female 1 --- 0.7Male 1.2 0.4---3.8
Level of disc hernia L4-L5 1 --- 0.5L3-L4 0.6 0.07---5.9L5-S1 0.4 0.03---3.7
Type of disc hernia Protruded 1 0.006*
Extruded 5.4 1.6---18.4Type of gadolinium enhancement Heterogeneous 1 --- 0.05
Homogeneous 0.9 0.2---3.7Peripheral 0.5 0.1---1.8
dsp6nMtshes
6atwshtadrtt
tsaot
3iec
Document downloaded from http://zl.elsevier.es, day 28/05/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
CI: confidence interval; OR: odds ratio.* Significant difference.
used it is hard to compare our data to the various studiesshown in section ‘references’.22,24---27 In other studies wherethe sample of patients was small there was a high percent-age of hernia size shrinking or disappearance.9,10 Bozzao etat. did a follow-up prospective study of 69 patients withshrinking numbers close to ours but they only did one MR-scan after 6 and 15 months making it impossible to knowhow fast hernia reabsorbed.11 Other authors only do onescan control similar to Bozzao et al.’s and with a vari-able time interval which implies even more difficulties ofinterpretation.9,10
In one of our most extensive and easiest to compare stud-ies for the important number of cases analyzed follow-upwas done until 6 months showing spontaneous regressiononly in 34.7% of hernias and a 100% regression of loosefragment.19 Authors did not distinguish between total disap-pearance and regression or showed degree of regression; thisis why it is difficult to compare to our data. However theirnumbers are similar to those shown in this study becausein our cases percentage of disappearance at 6 months was32.5%. Other authors describe percentage of disappearancebelow our percentages to a point they do not talk aboutcomplete disappearance.23 In such study follow-up periodsvaried.
The fact size of hernia has little relation to its possi-ble disappearance or large hernias ending up disappearingis interesting.28 Most former studies show there is a lit-tle relation between size of hernia and its persistence ordisappearance.9,11---14,19,20
One interesting data of our study was 3 hernias increasedtheir size which could be due to persistence of fissurethrough fibrous ring allowing nucleus pulpous keep comingout little by little while fissure is not healed. These datahave not been very well-commented in section ‘references’;however aforementioned former study finds 9% of herniasincreasing size.19
When it comes to disc hernia enhancement contrastincidence was very high (93.3%) and peripheral enhance-ment pattern was more common (51.1%). In our analysis noenhancement pattern was significantly associated with the
ittf
isappearance of hernia. In section ‘references’ you can seeome studies on contrast enhancement.13,17---19 Modic et al.ublished the cases of a small subgroup of patients with a
week and 6 month follow-up.13 All of the 26 acute her-ias analyzed showed peripheral enhancement. First earlyR-scan done during the first 2 weeks probably exposed
he difference of enhancement pattern with respect to ourtudy. Figs. 5 and 6 show 2 cases of extruded hernias withomogeneous enhancement that disappeared. One of themxtruded completely after 6 months and the other onehrank >90% in one year.
Galluci et al. studied a small sample of patients with a-month follow-up and the first MR-scan done the first weekfter patients’ presentation.17 Gadolinium-enhanced pat-ern changed from peripheral to homogeneous in 8 patientshile in other 3 patients peripheral enhancement was per-
istent and all of them showed a decrease in the size ofernia. Komori et al. retrospectively studied 25 patientshrough gadolinium-enhanced MR at least with 2 studiesmong which there was a variable time from 27 to 856ays which makes it real hard to get to know what theeal enhancement evolution was.8 However in 17 patientshere was a change in enhancement pattern from peripheryo center while 5 patients remained unchanged.
In a larger study of 64 patients with 72 disc herniasreated with conservative therapy and followed through aingle gadolinium-enhanced MR at 6 months Splendiani ett. found enhancement in 41% of cases.19 In all the existencef peridiscal enhancement is described without further dis-inctions.
In our series the first MR-scan was done approximately months after presentation and the remaining MR-scansn 6-month intervals. This likely temporal difference couldxplain our findings in relation to the aforementioned arti-les.
Explanation of disc hernia contrast-enhancement is that
t seems to be due to epidural fibrosis and an attempt to healhe very hernia starting at the periphery progressing towardhe remaining fragment which needs to be differentiatedrom the enhancement attributed to perivenous plexus.30,31
404 A. Ramos Amador et al.
Figure 4 Disappearance of disc hernias. (A) Early CT, axiallevel. Disc hernia (arrow) L5-S1 extruded and lateralized tothe left. (B) Follow-up MR, axial level at CT same level. Dis-apperance of hernia. (C) Early TC. Extruded disc hernia (arrow)on S1. (D) Follow-up MR, axial level at the same level of CT.Disappearance of hernia.
Figure 5 Extruded hernia disc occupying the lateral recess onL4. T1-weighted sequences, axial level. (A) No contrast image.Disc hernia (arrow) occupying the lateral recess of L4. (B) Imageafter contrast. Homogeneous enhancement of disc hernia. (C)Control MR (no contrast) after 6 months. Complete disappear-ance of hernia.
Document downloaded from http://zl.elsevier.es, day 28/05/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.

The natural history of disc herniation: Value of gadolinium
Figure 6 Big extruded hernia disc on L5-S1. T1-weightedsequences, axial level. (A) No contrast image. Big disc herniacompressing the thecal sac (arrow). (B) Image after contrast.Homogeneous enhancement of disc hernia. Annular enhance-ment of disc hernia. (C) Control MR (no contrast) after 6 months.Disappearance of 90% of hernia.
OofitoawdotTpnahphwstmpTitaabotbeScigtoatfsr
wlus
bfvtsitvctgla
Document downloaded from http://zl.elsevier.es, day 28/05/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
405
n the histological level epidural scar was identical to thene seen on surgical patients and contains a mixture ofbrocites, collagen and small vessels.31 To many pathologistshe margins of neovascularization of disc material are thenly valuable data that disc hernia really occurred and theyllow the pathologist to see the disc of hernia.32 Togetherith granulation tissue the scar is likely to reabsorb theisc material.33 Thus we could expect during the processf scarring the disc fragment to be invaded by granula-ion tissue that would break, fragment and reabsorb hernia.he total homogeneous enhancement we found in someatients supports the purpose of this mechanism despiteot all homogeneous enhancements meant disappearancet one year. Unfortunately we do not know what would haveappened during longer follow-up. According to this theoryeripheral enhancement should evolve toward some otheromogeneous central enhancement as long as disc materialas absorbed. But this did not happen in several circum-
tances and peripheral enhancement persisted throughouthe study. But because in the 6-month interval of subsequentonitoring many fragments were gone it is possible thateripheral evolution toward the center really happened.o support this hypothesis we would have needed shorternterval-monitoring and longer follow-up periods. Whateverhe radiological---pathological correlation might be with dis-ppearance of disc fragments and existing interrelation withcute inflammatory episodes based on our data it is impossi-le to predict persistence or disappearance of hernia basedn the presence and type of enhancement contrast. In sec-ion ‘references’ there are disagreeing data on the relationetween enhancement and disappearance of hernias. Modict al. find a shrinkage percentage of 60% similar to ours whilependiani et al. talk about 83% shrinkage.13,19 Disagreementan be partly due to enhancement percentages close to 41%n Splendiani et al.’ study, while our study and Modic et al.’soes beyond 90%,13,19 or due to the fact that they do not dis-inguish between disappearance and degree of shrinkage. Inur series the addition of disappearance and partial shrink-ge was 75%. Other authors relate hernia disappearance tohickness of enhancement wall as an important predictingactor.18,35 However our homogeneous-enhancement caseshowing maximum wall thickness we could not confirm thoseesults.
Lack of contrast enhancement is statistically associatedith persistence of hernia even though these data are of a
ittle practical importance due to the small percentage ofn-enhanced hernias both in our series and other series soystematic use of gadolinium would not be justified.13,17,19
Enhancement difference happening at hernia level cane justified by the different histological composition of discragment.34 Experimental studies have proven that bloodessels from the neighboring fibrovascular tissue infiltratehe hernia’ tissue---not the cartilage and blood vessels andecondary inflammation produce shrinkage of the size ofnfiltrated ring material. Cartilaginous tissue from small ver-ebral plateaus causes inhibition due to inflammation andascular episodes.34---36 Thus lack of enhancement can indi-ate there is a high percentage of cartilaginous material in
he disc fragment. On the other hand there seems to be aood correlation between changes of signal intensity and theower bone marrow and terminal plateaus (Modic’ criteria)nd cartilaginous material at hernia level.34 We have not
4
aco
tathbtp
hiSr
hebd‘
A
1
C
A
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
Document downloaded from http://zl.elsevier.es, day 28/05/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
06
ssessed Modic’ criteria so it would be interesting to do aorrelation study of those criteria, presence of bone defectsf vertebral angles and disappearance of disc hernia.
There are several limitations in our study. Most impor-ant ones are patient selection bias, limited size of samplend lack of correlation to surgical findings. Another limita-ion is the fact that normal asymptomatic populations canave a 24---33% frequency of protruded hernias.29 Data cane important since within percentage of persistent herniashere can be a proportion of hernias found in asymptomaticopulations.
In sum, in our study and in literature extruded discernias usually disappear and shrink; and extrusion is anmportant predictive factor for shrinking of hernia size.peed of reabsorption is variable and many hernias reabsorbapidly.
Contrast enhancement is a very common data in discernias and probably plays a role in hernia reabsorptionven though in our series; we could not confirm a relationetween type of enhancement and disappearance. Theseata partially disagree with the aforementioned sectionreferences’.
uthors
1. Manager of the study: ARA.2. Study concept: ARA.3. Study design: ARA, MAM.4. Data gathering: JLGP, SFZ, RS.5. Data analysis and interpretation: ARA, MAM.6. Statistical treatment: AP.7. Bibliographic search: RS, ARA.8. Writing: ARA.9. Critical review and intellectually relevant notes: ARA,
MAM, RS.0. Final version approval: ARA.
onflicts of interest
uthors report no relevant conflicts of interest.
eferences
1. Porter R, Hibbert C, Evans C. The natural history or root entrap-ment syndrome. Spine. 1984;9:418---21.
2. Bell GR, Rothman RH. The conservative treatment of sciatica.Spine. 1984;9:54---6.
3. Weber H, Holme I, Ameliee E. The natural course of acute sci-atica with nerve root symptoms. Spine. 1993;18:1433---8.
4. Busch K, Couwan N, Katc DE, Fisher PH. The naturalhistory of sciatica associated with disc pathology. Spine.1992;17:1205---11.
5. Andersson GB, Brown MD, Dvorak J, Herzog RJ, Kambin P, MalterA, et al. Consensus summary on the diagnosis and treatment oflumbar disc herniation. Spine. 1996;21 24 Suppl:75S---8S.
6. Saal JA, Saal JS. Nonoperative treatment of herniated lumbarintervertebral disc with radiculopathy. Spine. 1989;14:431---6.
7. Weber H. Lumbar disc herniation a controlled prospective studywith ten years of observation. Spine. 1983;8:131---40.
8. Teplick JG, Haskin ME. Spontaneuos regression of herniatednucleous pulposus. Am J Roentgenol. 1985;145:371---5.
2
2
A. Ramos Amador et al.
9. Saal JA, Saal JS, Herzog RJ. The natural history of lumbarintervertebral disc extrusion treated nonoperatively. Spine.1990;15:683---6.
0. Delauche-Cavallier M, Budet CH, Laredo JD, Debie B, WybierM, Dorfmann H, et al. Lumbar disc herniation. Computedtomography scan changes after conservative treatment ofnerve root compression. Spine (Phila Pa 1976). 1992;17:927---33.
1. Bozzao A, Galluci M, Masciocochi C, Aprile I, Barile A, Pas-sariello R. Lumbar disc herniation: MR imaging assessment ofnatural history in patient treated without surgery. Radiology.1992;185:135---45.
2. Komori H, Shinomiya K, Nakai D, Yamura I, Takeda S, Furuya K.The natural history of herniated nucleus pulposus with radicu-lopathy. Spine. 1996;21:225---9.
3. Modic MT, Ross JS, Obuchowski NA, Browning KH, Cianflocco AJ,Mazanec DJ. Contrast enhanced MR imaging in acute lumbarradiculopathy: a pilot study of the natural history. Radiology.1995;195:429---35.
4. Baldwin NG. Lumbar disc disease: the natural history. NeurosurgFocus. 2002;13:E2.
5. Cooper RG, Freemont RS, Hoyland JA, Cooper RG, FreemontAJ, Hoyland JA, et al. Herniated intervertebral disc associatedperiradicular fibrosis and vascular abnormalities occur withoutinflammatory cell infiltration. Spine. 1995;20:591---8.
6. Grönblad M, Virri J, Tolonen J, Seitsalo S, Kääpä E, KankareJ, et al. A controlled immunohistochemical study of inflam-matory cell in disc herniation tissue. Spine (Phila Pa 1976).1994;19:2744---51.
7. Gallucci M, Bozzao A, Orlandi B, Manetta R, Brughitta G,Lupattelli L. Does postcontrast MR enhancement in lumbardisk herniation have prognostic value. J Comput Assist Tomogr.1995;19:34---8.
8. Komori H, Okawa A, Haro H, Maneta T, Yamamoto H, Shi-noimiya K. Contrast enhanced magnetic resonance imaging inconservative management of lumbar disc herniation. Spine.1998;23:67---73.
9. Splendiani A, Puglielli E, De Amicis R, Barile A, MasciocchiC, Gallucci M. Spontaneous resolution of lumbar disck hernia-tion: predictive signs for prognostic evaluation. Neuroradiology.2004;46:919---22.
0. Modic MT, Obuchowki NA, Ross JS, Brant-Zawardzki MN, GrooffPN, Mazanec DJ, et al. Acute low back pain and radioculopa-thy: MR imaging findings and their prognostic role and effect onoutcome. Radiology. 2005;237:597---604.
1. Maigne JY, Deligne L. Computed tomography follow-up study of21 cervical cases of nonoperatively treated cervical interverte-bral soft disc herniation. Spine. 1994;19:189---91.
2. Fardon DF, Micette PC, Combined Task Forces of the North Amer-ican Spine Society, American Society of Spine Radiology, andAmerican Society of Neuroradiology. Nomenclature and clas-sification of lumbar disc pathology. Recommendations of theCombined task Forces of the North American Spine Society,American Society of Spine Radiology, and American Society ofNeuroradiology. Spine. 2001;26:E93---100.
3. Matsubara Y, Kato F, Mimatsu K, Kajino G, Nakamura S, NittaH. Serial changes on MRI in lumbar disc herniations treatedconservatively. Neuroradiology. 1995;37:378---83.
4. Thornbury JR, Fryback DG, Turski PA, Javid MJ, McDonald JV,Beinlich BR, et al. Disk-caused nerve compression in patientwith acute low-back pain: diagnosis with MR, CT mielographyand plain CT. Radiology. 1993;186:731---8.
5. Jarvik JG, Deyo RA. Diagnostic evaluation of low back pain withemphasis on imaging. Ann Intern Med. 2002;137:586---97.
6. Milette P. The proper terminology of reporting intervertebral
disc disorders. Am J Neuroradiol. 1997;18:1859---64.7. Brandt-Zawadzki M, Jensen M. Spinal nomenclature. Spine.1995;20:388---90.

3
3
3
3
Document downloaded from http://zl.elsevier.es, day 28/05/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
The natural history of disc herniation: Value of gadolinium
28. Cribb GL, Jaffray DC, Cassar-Pullicino VN. Observations on thenatural history of massive lumbar disc herniation. J Bone JointSurg Br. 2007;89:782---4.
29. Stadnik TW, Lee RR, Coen HL, Neirynck EC, Buisseret TS,Osteaux MJ. Annular tears and disk herniation: prevalence andcontrast enhancement on MR images in the absence of low backpain or sciatica. Radiology. 1998;206:49---55.
30. Ross JS, Modic MT, Masaryk T, Carter J, Marcus RE,Bohlman H. Assessment of extradural degenerative diseasewith GD-DTPA-enhanced MR imaging: correlation with sur-gical and pathologic findings. Am J Neuroradiol. 1989;10:
1243---9.31. Hueftle MG, Modic MT, Ross JS, Masanyk TJ, Carter JR, WilberRG, et al. Lumbar spine postoperative MR imaging with GD-DTPA. Radiology. 1988;167:817---24.
3
407
2. Weidner N, Rice DT. Intervertebral disk material crite-ria for determining probable prolapse. Human Pathol.1988;19:406---10.
3. Lindblom K, Hultqvist G. Absorption of protruded disc tissue.J Bone Joint Surg Am. 1950;32[A]:557---60.
4. Schmid G, Witteler A, Willburger R, Kuhnen C, Jergas M, KoesterO. Lumbar disk herniation correlation of histologic findings withmarrow signal intensity changes in vertebral endplates at MRchanges. Radiology. 2004;231:352---8.
5. Autio RA, Karppinen J, Niinimäki J, Ojala R, Kurunlahti M,Haapea M, et al. Determinants of spontaneous resorption of
intervertebral disc herniations. Spine. 2006;31:1247---52.6. Carreon LY, Ito T, Yamada M, Uchiyama S, Takahashi HE. Neo-vascularization induced by anulus and its inhibition by cartilageendplates: its role in disc absorption. Spine. 1997;22:1429---34.