multiple sclerosis, euthyroid restrictive grave's ophthalmopathy, and my asthenia gravis
TRANSCRIPT

Graefe's Arch Clin Exp Ophthalmol (1988)226:168-171 Graefe's Archive tor Clinical and Experimental
Ophthalmology © Springer-Verlag 1988
Multiple sclerosis, euthyroid restrictive Grave's ophthalmopathy, and myasthenia gravis* A case report
Wayne W. Bixenman and Harvey W. Buchsbaum
Abstract. A 53-year-old physician with a 13-year history of multiple sclerosis presented with the subacute onset of an atypical, restrictive, euthyroid Grave's ophthalmopathy. The hypotropia and monocular upgaze restriction re- sponded to a course of systemic and local steroids. Three months later, the patient developed ocular and systemic features of myasthenia gravis. This is the second reported case of coincident multiple sclerosis, myasthenia gravis, and thyroid-related disease complex.
The coexistence of simultaneous diseases with an autoim- mune basis in an infrequent occurrence. Although it has been estimated that 1% of hyperthyroid patients will have myasthenia gravis and conversely, 5% of myasthenic pa- tients will have Grave's disease [9], there have been only ten case reports of coexistent multiple sclerosis and myas- thenia gravis [1, 2, 4, 8, 10, 12]. Only one reference docu- ments the coexistence of hyperthyroidism, multiple sclero- sis, and myasthenia gravis [6].
Case report
This 53-year-old physician originally presented in 1972 with distal paresthesias of the lower extremities. In 1977, he expe- rienced a recurrence of these symptoms. When evaluated in 1979, he had hyperactive deep tendon reflexes in both lower extremities, right Babinski's sign, right leg weakness, diminished vibratory sensation in both feet, abnormal pat- tern reversal visual evoked response (VER) consistent with the right optic nerve dysfunction, and elevated CSF IgG level of 12.5 mg/dl (0-8.4 mg/dl). On the basis of these find- ings, the diagnosis of multiple sclerosis was made.
While driving to work on the morning of 7/27/84, he became aware of intermittent vertical diplopia. Over the next 2 days, his diplopia progressively worsened. An oph- thalmological examination on 7/30/84 demonstrated a 12 prism diopter right hypotropia in primary position with a minimal ( - 1 ) upgaze limitation of the right globe. No other abnormalities were found. While this presumed M.S.-
* Dedicated to Dr. G.K. von Noorden on the occasion of his 60th birthday
Offprint requests to." W.W. Bixenman, E1 Dorado Medical Plaza, Suite 130-a, 1500 N. Wilmot Road, Tucson, Arizona 85712, USA
related phenomenon was being evaluated, an 8 prism diopter base-up Fresnel prism was prescribed for the right spectacle lens which provided relief from the troublesome diplopia. A computerized tomographic (CT) scan with orbi- tal views was normal.
His vertical diplopia continued to progressively worsen and he required a 15 prism diopter base-up prism to main- tain single vision. On follow-up on 8/2/84, he had a 25 prism diopter right hypotropia in primary position which decreased to 15 prism diopters in downgaze and increased to 35 prism diopters in upgaze. A new Fresnel prism correc- tion was prescribed (25 prism diopter base-up right lens) which again provided only temporary relief from his pro- gressive diplopia.
On 8/4/84, which was 7 days after the onset of his diplo- pia, he was referred for a neuroophthalmic evaluation (to WWB). Other than a moderately high myopic refractive error, his background ocular history had been unremark- able. He had not sustained any head trauma prior to the development of his symptoms. On examination, his vision was 20/25 + 1 in both eyes (RE, - 5.50 + 0.50 cx 125/+ 2.00 add; LE, - 6.25 + 0.50 cx 45/+ 2.00 add). On prism-cover testing, he manifested a 35 prism diopter right hypotropia in primary position which was over 50 prism diopters in attempted upgaze and .18 prism diopters in downgaze. In right gaze, he had a 30 prism diopter right hypotropia and 2-3 prism diopter exotropia (XT), while in left gaze, a 25 prism diopter right hypotropia and 8 prism diopter esotro- pia (ET). There was no measurable exophthalmos; no lid retraction or lid lag; no ocular injection; and no chemosis. He had a pronounced ( - 4 ) upgaze limitation of the right eye only (Fig. 1). Forced ductions were positive with a mod- erate restriction of attempted upgaze of the right globe. His intraocular tensions were 24 mmHg in both eyes in primary position while the tension in the right eye increased to 33 mmHg in attempted upgaze, in accordance with a restrictive upgaze limitation. All thyroid function tests were within normal range.
On the basis of this acquired, monocular, upgaze restric- tion, the diagnosis of euthyroid, restrictive Grave's ophthal- mopathy was made. As his presentation was relatively sub- acute, with worsening hypotropia and serial forced ductions demonstrating greater restriction, it was elected to place him on a course of systemic steroids. This 3-week course of prednisone (80 mg per day) was supplemented with a single subTenon's injection of deposteroid (30 mg Depo- medrol) into the inferior oblique-inferior rectus complex.
{? : , , * , •
169
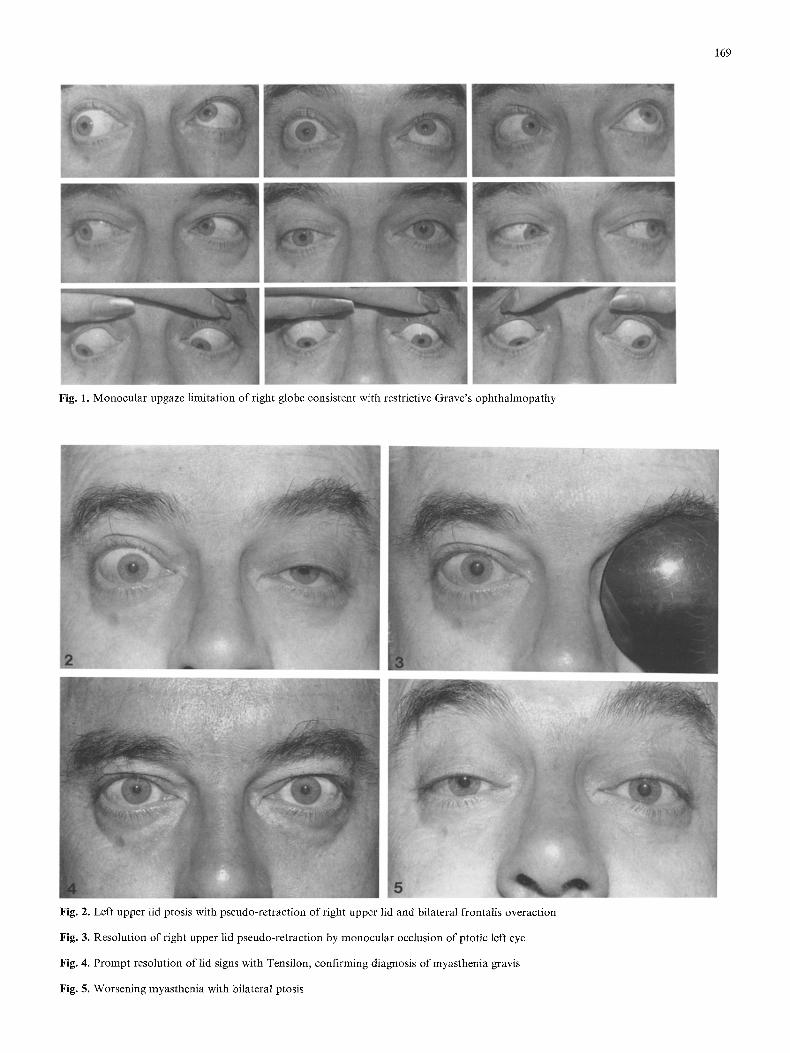
Fig. 1. Monocular upgaze limitation of right globe consistent with restrictive Grave's ophthalmopathy
Fig. 2. Left upper lid ptosis with pseudo-retraction of right upper lid and bilateral frontalis overaction
Fig. 3. Resolution of right upper lid pseudo-retraction by monocular occlusion of ptotic left eye
Fig. 4. Prompt resolution of lid signs with Tensilon, confirming diagnosis of myasthenia gravis
Fig. 5. Worsening myasthenia with bilateral ptosis
170
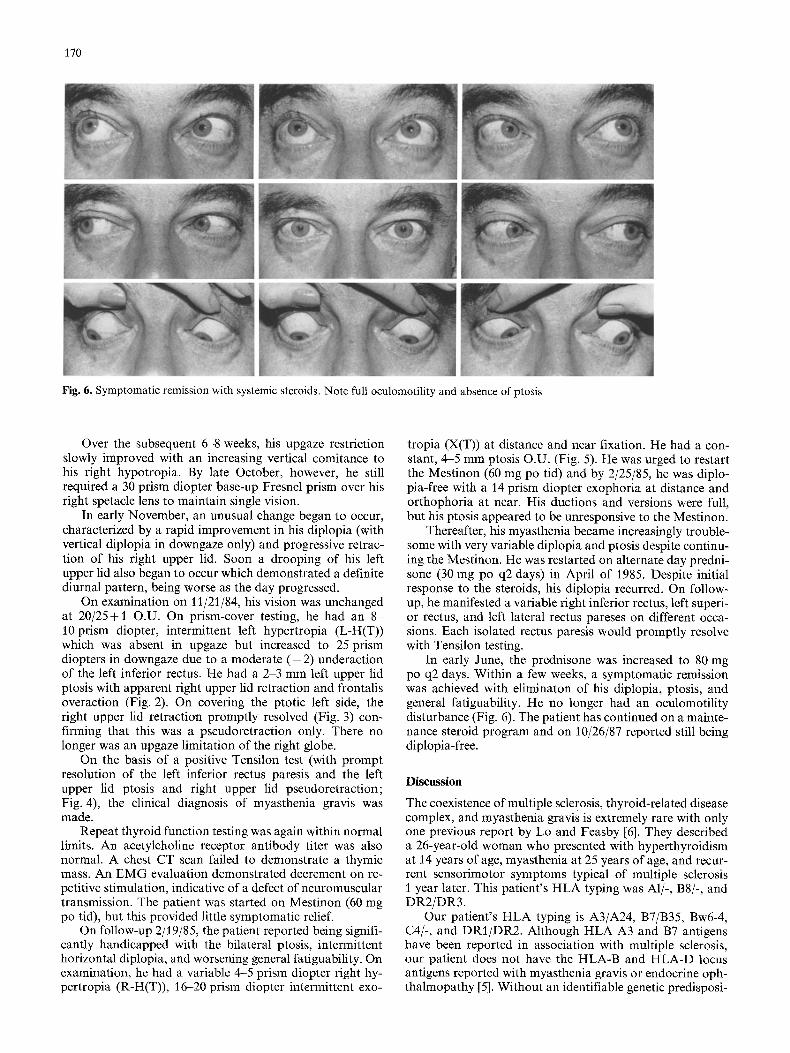
Fig. 6. Symptomatic remission with systemic steroids. Note full oculomotility and absence of ptosis
Over the subsequent 6-8 weeks, his upgaze restriction slowly improved with an increasing vertical comitance to his fight hypotropia. By late October, however, he still required a 30 prism diopter base-up Fresnel prism over his right spetacle lens to maintain single vision.
In early November, an unusual change began to occur, characterized by a rapid improvement in his diplopia (with vertical diplopia in downgaze only) and progressive retrac- tion of his right upper lid. Soon a drooping of his left upper lid also began to occur which demonstrated a definite diurnal pattern, being worse as the day progressed.
On examination on 11/21/84, his vision was unchanged at 20/25 + 1 0 . U . On prism-cover testing, he had an 8- 10 prism diopter, intermittent left hypertropia (L-H(T)) which was absent in upgaze but increased to 25 prism diopters in downgaze due to a moderate ( - 2 ) underaction of the left inferior rectus. He had a 2-3 mm left upper lid ptosis with apparent fight upper lid retraction and frontalis overaction (Fig. 2). On covering the ptotic left side, the fight upper lid retraction promptly resolved (Fig. 3) con- firming that this was a pseudoretraction only. There no longer was an upgaze limitation of the right globe.
On the basis of a positive Tensilon test (with prompt resolution of the left inferior rectus paresis and the left upper lid ptosis and right upper lid pseudoretraction; Fig. 4), the clinical diagnosis of myasthenia gravis was made.
Repeat thyroid function testing was again within normal limits. An acetylcholine receptor antibody titer was also normal. A chest CT scan failed to demonstrate a thymic mass. An EMG evaluation demonstrated decrement on re- petitive stimulation, indicative of a defect of neuromuscular transmission. The patient was started on Mestinon (60 mg po tid), but this provided little symptomatic relief.
On follow-up 2/19/85, the patient reported being signifi- cantly handicapped with the bilateral ptosis, intermittent horizontal diplopia, and worsening general fatiguability. On examination, he had a variable 4-5 prism diopter right hy- pertropia (R-H(T)), 16-20 prism diopter intermittent exo-
tropia (X(T)) at distance and near fixation. He had a con- stant, 4-5 mm ptosis O.U. (Fig. 5). He was urged to restart the Mestinon (60 mg po tid) and by 2/25/85, he was diplo- pia-free with a 14 prism diopter exophoria at distance and orthophoria at near. His ductions and versions were full, but his ptosis appeared to be unresponsive to the Mestinon.
Thereafter, his myasthenia became increasingly trouble- some with very variable diplopia and ptosis despite continu- ing the Mestinon. He was restarted on alternate day predni- sone (30 mg po q2 days) in April of 1985. Despite initial response to the steroids, his diplopia recurred. On follow- up, he manifested a variable right inferior rectus, left superi- or rectus, and left lateral rectus pareses on different occa- sions. Each isolated rectus paresis would promptly resolve with Tensilon testing.
In early June, the prednisone was increased to 80 mg po q2 days. Within a few weeks, a symptomatic remission was achieved with eliminaton of his diplopia, ptosis, and general fatiguability. He no longer had an oculomotility disturbance (Fig. 6). The patient has continued on a mainte- nance steroid program and on 10/26/87 reported still being diplopia-free.
Discussion
The coexistence of multiple sclerosis, thyroid-related disease complex, and myasthenia gravis is extremely rare with only one previous report by Lo and Feasby [6]. They described a 26-year-old woman who presented with hyperthyroidism at 14 years of age, myasthenia at 25 years of age, and recur- rent sensorimotor symptoms typical of multiple sclerosis 1 year later. This patient's HLA typing was A1/-, B8/-, and DR2/DR3.
Our patient's HLA typing is A3/A24, B7/B35, Bw6-4, C4/-, and DRI/DR2. Although HLA A3 and B7 antigens have been reported in association with multiple sclerosis, our patient does not have the HLA-B and HLA-D locus antigens reported with myasthenia gravis or endocrine oph- thalmopathy [5]. Without an identifiable genetic predisposi-

171
tion, it is conjectural as to whether or not his presentation was simply the coincidental occurrence of three disease enti- ties with known autoimmune basis. The apparent rarity of this presentation would certainly suggest that such is the case.
Eyelid retraction secondary to a contralateral ptosis is a fascinating clinical sign which is usually seen in myasthe- nia gravis [11], but may occur in cases of ptosis of varying etiologies. The mechanism proposed is based on Hering's law of motor correspondence. Although exceptions fre- quently occur, fixation is presumably preferred with the ptotic eye and the excessive levator innervation so required to maintain an adequate lid position results in concurrent retraction of the contralateral " n o r m a l " upper lid. Cover- ing or occluding the ptotic eye results in normalization of the eyelid retraction in the contralateral eye with varying degrees of promptness (Figs. 2 and 3), confirming that this is a "pseudoret ract ion." As the eyelid retraction in the nor- mal eye may be cosmetically more noticeable than the ptosis in the involved eye, the patient may be misdiagnosed as having a thyroid eyelid retraction (i.e., Dalrymple's sign). This may be especially confusing where a dysthyroid oph- thalmopathy does indeed exist [7]. Thus, it is important to remember this occlusion test in cases of monocular eyelid retraction as a subtle ptosis may be the first sign o f a con- current myasthenic condition.
Atypical, restrictive, euthyroid Grave's ophthalmopathy has been previously reported [3]. It is an uncommon presen- tation seldom appreciated by both ophthalmologists and neurologists alike. These patients present with acquired, monocular, typically upgaze limitations with abrupt onset of vertical diplopia. As in the reported case, there initially may be diagnostic confusion with an upgaze limitation on a neurogenic basis due to a localized brainstem ischemic or demyelinating episode. The positive forced duction test- ing, however, affirms that this is a restrictive ductional limi- tation and points to myogenic factors of orbital origin. As there is no antecedent congestive " t hy ro id" orbitopathy and as the restrictive ductional limitation appears to arise de novo, the condition has been labeled "atypical ." Abnor- mal thyroid function testing may or may not develop and may present at any time during the clinical course [3]. These cases are in fact examples of euthyroid orbital myositis.
Our special interest in this patient is that this restrictive form of Grave's ophthalmopathy was documented from
onset. Although the subjective onset of the diplopia may be abrupt, the upgaze limitation may progress over a number of days in a subacute fashion with worsening hypo- tropia and greater restriction on serial forced duction test- ing. If seen early on in their presentation, the initial upgaze restriction, due to presumed inflammatory myositis, may respond to a short course of high-dose steroid supplemented by a local sub Tenon's injection of deposteroid into the region of the inferior rectus-inferior oblique complex. With time, fibrosis ensues leaving surgery the only option to han- dle monocular hypotropia and consequent diplopia [3].
References
1. Achari AN, Trontelj JV, Campos R (1976) Multiple sclerosis and myasthenia gravis. A case report with single fiber electro- myography. Neurology (Minneap) 26:544-546
2. Aita JF, Snyder DH, Riechl W (1974) Myasthenia gravis and multiple sclerosis : an unusual combination of diseases. Neurol- ogy (Minneap) 24 : 72-75
3. Bixenman WW, Noorden GK yon (1981) Atypical presentation of restrictive orbital myositis. J Pediatr Ophthalmol Strabismus 18:6-10
4. Keane JR, Hoyt WF (1970) Myasthenic (vertical) nystagmus. Verification by edrophonium tomography. JAMA 212:1209- 1210
5. Ladas ID (1983) Histocompatibility (HLA) antigens and eye diseases other than uveitis. Surv Ophthalmol 27 : 233-244
6. Lo R, Feasby TE (1983) Multiple sclerosis and autoimmune diseases. Neurology (NY) 33:97-98
7. Lohman L, Burns JA, Penland WR, Cahill KV (1984) Unilater- al eyelid retraction secondary to contralateral ptosis in dysthyr- old ophthalmopathy. J Clin Neuro Ophthalmol 4:163-166
8. Margolis LH, Graves RW (1945) Occurrence of myasthenia gravis in a patient with multiple sclerosis. NC Med J 6:243- 244
9. Millikan CH, Haines SF (1953) The thyroid gland in relation to neuromuscular diseases. Arch Intern Med 92 : 540
10. Patten BM, Hart A, Lovelace R (1972) Multiple sclerosis asso- ciated with defects in neuromuscular transmission. J Neurol Neurosurg Psychiatry 35:385-394
11. Schechter RD (1978) Ptosis with contralateral lid retraction due to excessive innervation of the levator palpebrea superioris. Ann Ophthalmol 10:1324-1328
12. Simpson JA (1966) The biochemistry of myasthenia gravis. In: Kuhn (ed) Progressive Muskeldystrophie, Myotonie, Myasthe- nia. Springer, Berlin Heidelberg New York, pp 339-349