motivational orientation of people participating in vocational rehabilitation
TRANSCRIPT
Motivational Orientation of People Participating in VocationalRehabilitation
Kristiina Harkapaa • Aila Jarvikoski •
Raija Gould
� Springer Science+Business Media New York 2014
Abstract Purpose The task of vocational rehabilitation is
to support the employee’s chances of continuing in work-
ing life. The study aimed to examine the motivational
orientation of people participating in vocational rehabili-
tation and to find out what characteristics of the clients,
their life situation, and their beliefs and perceptions were
associated with it. Methods A mail questionnaire was
answered by 839 rehabilitation clients who had received an
affirmative rehabilitation decision under the earnings-
related pension scheme 12 months earlier (response rate
67 %). Two variables depicting motivational orientation
were formed, i.e., motivation for continuing in working life
and motivation for participating in vocational rehabilita-
tion. Logistic regression analyses were applied in exam-
ining the factors associated with each motivation variable.
Results The results indicate that the two motivational ori-
entations can be regarded as partly separate and partly
overlapping constructs. The rehabilitation clients’ motiva-
tional orientations were associated with their experiences
and their perceptions on environmental factors and future
possibilities, both those that precipitated the application for
rehabilitation and those that are important in their current
life situation and their perceived future possibilities. Con-
clusions In the planning of individual rehabilitation pro-
cesses there is a clear need to sort out what factors may
hide behind the client’s weak contextual or situational
motivation. In the course of the rehabilitation process, it is
important to discuss these factors in order to alleviate the
clients’ uncertainty towards change and enhance their
motivation to participate in rehabilitation and re-think their
future prospects of returning to work.
Keywords Vocational rehabilitation � Motivation �Rehabilitation � Questionnaire � Return to work
Introduction
Motivation has been one of the most popular themes in the
rehabilitation practice for decades [1]. The concept of
rehabilitation motivation has been understood in many
different ways, and King and Barrowclough [2] even sug-
gested that the whole concept should be removed from
active use because of its multiple meanings. However,
rehabilitation motivation has a role in determining reha-
bilitation outcomes [3], changes in work ability and quality
of life [4], and future employment [5, 6]. According to
Saeki et al. [7], a lack of motivation is an important pre-
dictor of unsuccessful outcomes. Despite this, motivation
has relatively rarely been the focus of vocational rehabil-
itation studies. Nordt et al. [8] find this scarcity of research
surprising.
Rehabilitation motivation has often been interpreted as
an intrinsic personality trait, and lack of motivation, cor-
respondingly, as a relatively stable individual characteristic
that creates a barrier to successful rehabilitation. However,
the social context also seems to play an important role in
motivation [9]. Motivation can be understood at three
levels of generality, i.e., global motivational orientation,
motivation toward the broad spheres of activities and life
contexts (contextual level, such as education, work or
family relationships), and motivation toward a given
K. Harkapaa (&) � A. Jarvikoski
Faculty of Social Sciences, University of Lapland, P.O. Box 122,
96101 Rovaniemi, Finland
e-mail: [email protected]
R. Gould
Finnish Centre for Pensions, 00065 Elaketurvakeskus, Helsinki,
Finland
123
J Occup Rehabil
DOI 10.1007/s10926-013-9496-z

activity at a specific point in time (situational motivation)
[10, 11]. In rehabilitation, motivation can be directed
towards many kinds of goals that represent different levels
of generality or different life contexts. Nair [12] empha-
sizes that the intensity of motivation depends on, among
other things, the concurrence between a person’s life goals
and the immediate goals set in rehabilitation planning. A
person may thus be interpreted as unmotivated if he or she
cannot find the connection between rehabilitation measures
and life goals. As an example, it is possible to be motivated
for recovery, improved functionality or employment, but
not for rehabilitation, if the person does not see the reha-
bilitation offered as the most appropriate means for
reaching the goals [e.g., 13].
In vocational rehabilitation, people often face motiva-
tional problems because of conflicting motives. Work as
such is an important value and a goal for many and it brings
about, in addition to wages, several other positive things,
referred to by Jahoda [14] as the latent functions of work. At
the same time, work goals may also be connected with
insecurity, uncertainty about the future and problems in
finding suitable work, whereas disability retirement may
seem a more secure and stable choice. The Readiness for
Change Model by Proschaska has often been used in the
context of health promotion [15, 16]. The concepts of deci-
sional balance and readiness for change have also been
applied to return-to-work interventions [17]. Exploring and
resolving ambivalence is an important method in enhancing
change or recovery [18, 19]. In vocational rehabilitation, the
clients’ motivation for change can be enhanced by motiva-
tional conversations focusing on future opportunities and the
changes needed in working and living conditions [20].
Motives and expectations are also influenced by earlier
experiences. If rehabilitation clients feel that their work and
the workplace have had a significant role in the weakening of
their work performance, it may make their future work-
related goals open to doubt.
Using the action-theoretical framework, Berglind and
Gerner [21] emphasized that people’s employment motiva-
tion is clearly connected to their estimated possibilities of
getting work. They showed that clients were inclined to
adjust their preferences because of different factors
obstructing their achieving the goal of staying in working life
or weakening their perceived competence. According to
Bandura [22, 23], people motivate themselves and guide
their action through the exercise of forethought. Self-effi-
cacy, which refers to a person’s confidence in his or her
ability to perform specific tasks, has a central role in moti-
vation and in shaping a person’s life course by influencing
which activities one undertakes. Its significance in rehabili-
tation has been shown in several studies, and helping reha-
bilitation clients strengthen their self-efficacy has been
regarded as an important goal of rehabilitation counseling
[24]. Self-efficacy can enhance a person’s career success,
and career success can correspondingly enhance his or her
self-efficacy in relation to occupational tasks [25]. As for-
mulated by Bandura [22], self-efficacy is typically a task or
domain–specific construct. More generalized constructs of
perceived competence or generalized self-efficacy have been
proposed by other researchers [26–28].
The concept of institutional or vertical trust has not been
used in rehabilitation studies. It is, however, known that all
clients do not believe that they get equal treatment in
rehabilitation [29], and lack of trust can be expected to
influence their motivation to participate in measures
arranged by rehabilitation organizations. Vertical or insti-
tutional trust has been defined as the trust of citizens in the
institutions, particularly the public institutions, of society
[30]. Trust is created by both macro and micro level factors
[31] and it is associated with the perception of getting fair
and equal treatment from public organizations [32, 33].
Distrust in the healthcare system was found to be associ-
ated with risky health behaviors [30]. Perception of orga-
nizational justice is regarded as an important motivational
topic with workers [34, 35] and it also seems to be asso-
ciated with the rate of sickness absence [36]. General
distrust in societal institutions may disrupt one’s motiva-
tion to participate in activities that are arranged by orga-
nizations representing strong institutional power.
In this study, our interest was in two constructs: motiva-
tional orientation towards working life on the one hand, and
motivation for vocational rehabilitation on the other. To our
knowledge, there are no studies where both of them have
been used together or compared with each other. They can,
however, represent different levels of the motivational
hierarchy, and factors associated with them can differ from
each other. Motivational orientation towards working life
probably addresses the relatively general aspects of moti-
vation in the context of work. Motivation for vocational
rehabilitation, in turn, represents a more situational moti-
vation, connected with specific rehabilitation services and a
specific time and place. There can be several, even con-
flicting factors behind the pursuit of vocational rehabilita-
tion. For some clients, the motives for participation in
rehabilitation are based on their strong motivation to remain
in working life. With others, a need for security may be a
background factor, which means that they aim to change
their unstable position between work and sickness absence to
a more secure one, either in working life or retirement.
The study thus has two main aims. Firstly, we aim to
examine (a) rehabilitation clients’ motivational orientation
towards working life and their motivation to participate in
vocational rehabilitation, and (b) the relationship between
these two orientations. The second aim is to find out what
kind of health-related, psychological, social and work-
related factors are associated with the motivational
J Occup Rehabil
123

orientation towards working life in general and a person’s
motivation for vocational rehabilitation. The underlying
assumption in the study was that the two motivational
orientations represent separate constructs, and there are
differences between their predictors. However, as the study
was mainly explorative, no hypotheses on the directions or
differences between the predictors were formulated.
Method
The data of this study were gathered during the project
‘‘The functioning of vocational rehabilitation within the
earnings-related pension scheme’’, the main results of
which were reported in Finnish in 2012 [37]. The context
of this study is vocational rehabilitation under the earnings-
related pension scheme in Finland. The task of rehabilita-
tion within this scheme is to support the employee’s
chances of continuing to work. A person is entitled to
vocational rehabilitation within this scheme if his/her work
ability is limited due to an illness in such a way that it
poses a threat of the person having to retire on a disability
pension within approximately 5 years. Rehabilitation
within this scheme is considered relevant if it serves to
postpone disability retirement. When evaluating relevance,
the employee’s age, profession, previous jobs, education
and participation in the labor market are all taken into
account. Rehabilitation under this scheme consists of sev-
eral kinds of vocational or work-related measures, e.g.,
counseling, work try-outs, vocational training, work and
study aids, and subsidies for starting up entrepreneurial
activities. If medical rehabilitation is needed, it must be
supplied under other rehabilitation schemes.
Study Group
Between the start of October 2004 and the end of June
2005, 4,453 persons received a rehabilitation decision
under the earnings-related pension scheme. A stratified
random sampling, based on the employer sector (private,
state and municipal-sector employees), resulted in 1,680
persons of which 1,260 had received an affirmative reha-
bilitation decision. The present study group consisted of
839 persons in the latter group, who responded to a mail
questionnaire sent to them approximately 12 months after
the rehabilitation decision (response rate 67 %).
The main characteristics of the rehabilitation partici-
pants are presented in Table 1.
Methods
The following variables or variable groups were used in the
study:
1. Sociodemographic variables were (a) age, (b) gender
(1 = male, 2 = female), c) basic education
(1 = less than 9 years; 2 = 9 to 11 years;
3 = 12 years or more); (d) vocational education
(1 = no/a vocational course; 2 = vocational school;
3 = vocational college, polytechnic or university);
(e) occupation, first classified using the Classification
of Occupations 2010 by Statistics Finland, and then
further classified into three larger groups: 1 = work-
ers in manual occupations (groups 6–9); 2 = clerical
support workers, and service & sales workers (groups
4–5); 3 = managers, professionals, and technicians
(groups 1-3); (f) labor market situation at the time of
the rehabilitation decision made by the pension
provider (0 = on temporary disability pension,
1 = in labor force); (g) household financial situation
(1 = good to 5 = income does not meet consump-
tion needs, financial support needed; 6 = difficult to
say).
2. Factors that contributed to the need and application
for rehabilitation were based on a 14-item scale,
using a question: ‘‘Did some of the following factors
contribute to your subjective need for rehabilitation
and application for rehabilitation’’ (1 = had no
effect, to 4 = had much effect). The scale was a
brief version of a 24-item scale used in an early
rehabilitation study of state employees [38]. A factor
analysis was applied to secure the structure of the
brief scale in this sample, with the primary purpose
of computing composite scores for the factors
underlying the brief scale. The Kaiser-Meyer-Olking
measure of sampling adequacy was acceptable
(0.84), and Bartlett’s test of sphericity significant
(p = 0.000). Principal component analysis was used
as the extraction method. Three components had
eigenvalues higher than 1.0 and they explained 31.5,
13.5 and 9.4 % of the total variance (in total 54 %).
A Varimax rotation was applied. One item was
eliminated because it failed to meet a minimum
criterion of a factor loading of 0.45. On the basis of
the rotated matrix, three composite variables were
formed: (a) physical factors (four items: the physical
strenuousness of work; the hazards of the work
environment; increasing difficulty in coping at work;
disadvantages related to physical disabilities); Coef-
ficient Alpha = 0.57; (b) psychosocial factors (six
items: mental stress at work; problems with the
supervisor and the work community; mental health
problems; problems caused by work arrangements
and responsibilities; stressful life situation; a
decrease in devotion to work), Coefficient Alpha =
0.84; (c) work uncertainty factors (three items: the
J Occup Rehabil
123

uncertainty of the employment contract; changes in
ownership or other significant changes in the work-
place; feelings of not being needed), Coefficient
Alpha = 0.74. The theoretical range of all three
variables was 1–4.
3. Generalized self-efficacy was measured using the
Self-Performance Survey [26, 27]. The original
version includes 8 items (e.g., ‘‘I usually succeed in
tasks that I get up to’’), each assessed using scale 1–6.
The Coefficient Alpha of the 8-item scale was in
Wallston et al. [27] 0.83. A short four-item version,
with a reliability of 0.72, was also recommended by
Wallston. The Coefficient Alpha of the 8-item
Finnish version was, in a sample of rehabilitees,
0.78 [39]. In this study, the four-item version was
used. The theoretical range of this measure varied
between 1 and 6 (stronger self-efficacy) and the
Coefficient Alpha was 0.77.
4. Institutional or vertical trust has previously been
measured by asking the respondent to rate the degree of
their trust in societal institutions (e.g. ‘‘What trust do
you have in the following institutions in society?’’),
such as police, government, and politicians [40], or by
asking the respondents to indicate their degree of
agreement with brief statements (e.g., ‘‘There is one
law for the rich and one law for the poor’’; ‘‘No
political party would benefit me’’) [41]. In some
studies, more specific measures have been used, e.g.
targeting the respondent’s perceptions of two institu-
tions, healthcare and media [30]. In addition, confi-
dence in getting fair and equal treatment has been
shown to be a core element in the forming of trust in
public institutions and organizations. According to a
Swedish study [33], a very strong correlation was
found between the respondents’ experience of how
Table 1 Study participants
Men (n = 416) Women (n = 423) All (n = 839) p
Age: mean (SD) 44.4 (8.05) 46.0 (7.60) 45.2 (7.86) 0.005
Basic education (%)
Less than 9 years 34.9 29.5 32.2 0.000
9–11 years 53.0 42.8 47.8
12 years or more 12.1 27.8 20.0
Vocational education (%)
No/vocational course 25.4 24.9 25.2 0.000
Vocational school 59.4 46.0 52.6
Vocational college/polytechnic or university 15.2 29.1 22.3
Occupational group (%)
Managers, professionals etc. 17.1 25.2 21.2 0.000
Clerical support &, service and sales workers 8.9 39.6 24.3
Workers in manual occupations 74.0 35.3 54.6
Household financial situation (%)
Good 17.5 18.2 17.9 n.s.
Compromising sometimes needed 27.3 22.4 24.8
Compromising often needed/Financial support needed 55.1 59.4 57.3
Health disorders (%)
Back disorders 41.1 26.2 33.6 0.000
Other musculoskeletal disorders 19.7 24.3 22.1 n.s.
Mental disorders 13.0 22.0 17.5 0.001
Work ability: mean (SD) 3.21 (2.46) 3.16 (2.43) 3.18 (2.44) n.s.
Labour market situation (%)
On temporary disability pension 28.4 26.8 27.6 n.s.
In labour force 71.6 73.2 72.4
Perceived possibility to get a suitable job
Does not believe in getting a suitable job 14.9 16.1 15.5 n.s.
Believes to be able to continue at work 70.9 71.1 71.0
No answer 14.2 12.8 13.5
J Occup Rehabil
123

they were treated by the important societal organiza-
tions at their disposal and their simple ratings of trust in
the same. In the present study, four statements were
used, depicting one’s trust in public authorities and
officials in general (‘‘Citizens cannot nowadays trust in
the actions of public authorities’’; ‘‘Public officials and
experts are usually trustworthy and just’’), one’s
conception of the trustworthiness of the service system
(‘‘In the Finnish service system all clients are equal’’)
and one’s experience of being treated fairly or unfairly
in society (‘‘Society has treated me unjustly’’). Items 1
and 4 were reversed before summing. The Coefficient
Alpha was 0.77 and the theoretical range was 1–6
(stronger trust).
5. State of health: (a) Self-assessed state of health
(1 = very good to 5 = very poor); (b) reported main
health disorders (back disorders; other musculoskel-
etal disorders; mental health disorders);
6. Self-rated work ability compared with life time best
(0 = poor, 10 = excellent) is the first item of the
Work Ability Index [42, 43]. This item has been used
as a general measure of work ability in several
studies. It has been regarded as a good alternative for
the whole index [44]. In this study, participants
assessed their work ability at the time of applying for
rehabilitation.
7. Perceived possibility to get a suitable job was
measured with an affirmative answer to the item ‘‘I
believe that I am not able to get a job that is suitable
for me’’.
8. Self-rated motivation for vocational rehabilitation was
operationalized using a simple question ‘‘How moti-
vated or eager were you to take part in earnings-related
vocational rehabilitation?’’ with a 5-point scale
(1 = very motivated to 5 = not at all motivated).
This type of question represents a client’s conscious
motivation for participating in the measures included
in the rehabilitation plan, aiming towards securing
employment. This question was used in a Finnish study
[45] with persons who had got a preliminary affirma-
tive rehabilitation decision but whose rehabilitation
had failed to start. It correlated negatively with the time
out of work and positively with one’s wish to continue
in working life.
9. The items used in assessing the importance of
personal goals were based on a nine-item measure
developed in a study of work evaluation clients [5].
In the present study, four goal variables were used:
(1) staying in or returning to working life (working
life as a goal); (2) getting a disability pension
(disability retirement as a goal); (3) improvement in
the physical condition and decrease of pain and
discomfort (better physical condition as a goal); (4)
improvement in mental health and coping (better
mental health as a goal). The clients were instructed
to assess how important each goal was for them,
using the rating scale from 1 = very important to
4 = not important.
10. Motivational orientation towards working life: The
self-assessed importance of staying at or returning to
working life was used in this study in operationaliz-
ing the clients’ motivation towards working life [cf.
also 8, 46]. However, on the basis of an earlier study
[5] it was anticipated that some clients would be
ambivalent in their goals, i.e., they would rate both
employment and retirement as important goals. After
the cross-tabulation of the rated importance of staying
in or returning to working life with the rated
importance of retiring to disability pension, a three-
level categorical variable of motivation towards
working life was formed: (1) Stable motivation to
working life (staying in working life an important or
very important goal and retirement not an important
goal); (2) motivational ambivalence (both staying in
working life and retirement are important goals); and
(3) no motivation to working life (retirement an
important goal and staying in working life not
important; or neither working life nor retirement
important goals).
Data Analysis
In order to take into account the stratification and to
decrease the non-response bias, weight coefficients and
imputation of missing data were used in all data analyses
[47, 48]. The statistical analysis was based on frequency
distributions, cross-tabulations, correlations, analyses of
variance, and logistic regression analyses. All analyses
were computed using SPSS version 17.0 for Windows
(SPSS Inc., Chicago, Illinois, 2008).
Logistic regression analyses were used to identify the
variables associated with both motivation variables.
Logistic regression was chosen because one of the depen-
dent variables, motivation for working life, was categori-
cal, and the other, motivation for vocational rehabilitation,
was strongly skewed. For the analyses, motivation for
working life was dichotomized as follows: 1 = stable
orientation (61 % of the participants), 0 = others. Moti-
vation for vocational rehabilitation was dichotomized as
follows: 1 = very motivated clients (56 %), 0 = others. In
logistic regression analyses, the predictor variables were
seven variables presented in Sects. 1–7 above, the variables
(c) and (d) in Sect. 8, and the three variables depicting the
J Occup Rehabil
123

most common disease groups (back disorders; other mus-
culoskeletal diseases; mental disorders).
In each analysis, the age-adjusted association of each
predictor variable with the dependent variable was first
analyzed separately (Models A). In the second phase, those
predictors which had a statistically significant independent
association with the dependent variable were entered into
the regression model simultaneously (Model B). Age-
adjustment was used in all models. The Wald test was used
in assessing the contribution of the independent variables
to the overall model.
Ethical Considerations
Ethical approval for the study was granted by the Finnish
Centre of Pensions and the ethical committee of the
Rehabilitation Foundation. Information on the study was
given to the participants in the cover letter for the ques-
tionnaire. It emphasized that answering the questionnaire
was voluntary. It also provided the contact details of the
principal investigator of the Finnish Centre for Pensions.
Results
There were several statistically significant differences
between men and women (Table 1). The average age and
the educational level were higher among women than
among men, and men worked more often in manual
occupations. Back disorders were more common among
men and mental health disorders among women.
Almost 90 % of the rehabilitation participants regarded
staying in working life as an important or very important
goal. At the same time, a third of all participants regarded
disability retirement as an important goal. Better physical
condition was an important goal for two thirds, and better
mental health for half of the participants. Among women,
the goals of staying in working life and better mental health
were important more often than among men (Table 2).
Sixty-one percent of the respondents had a stable
motivational orientation for working life. Motivational
ambivalence (both work and disability pension as impor-
tant goals) was found in 28 %, and 11 % reported no
motivation for staying in working life. The share of those
having a stable motivation was greater in the younger age
group. Among those over 45 years, a third showed moti-
vational ambivalence. Motivation ambivalence was also
more common for women than for men, while the share of
those not motivated was greater among men. Motivation
for rehabilitation was strong or fairly strong in 88 % of the
participants. Women felt very motivated more often than
men did, and the younger age group more often than the
older one (Table 2).
The association between the two motivation variables
was statistically significant (Kendall’s tau b = 0.374;
Pearson correlation = 0.420). The cross-tabulation of the
variables showed that a fifth of those not motivated for
participation in working life felt very motivated for reha-
bilitation, and 29 % of those not motivated for rehabilita-
tion perceived staying in working life to be an important
goal for them.
Logistic regression analyses, using motivation towards
working life as the dependent variable, are presented in
Table 3. First, the independent association of each pre-
dictor with the dependent variable was analyzed separately
(adjusted for age; Models A). In the second phase, all
variables with statistically significant independent associ-
ations with the dependent variable were entered in the
regression model simultaneously (Model B).
According to Models A, better education, better work
ability, stronger generalized self-efficacy, and stronger
institutional trust increased the chances of stable orienta-
tion towards working life statistically significantly. Factors
decreasing the chances of stable motivation towards
working life, on the other hand, were older age, being on
disability pension, weak financial status, a greater number
of physical, psychosocial and uncertainty factors at work
contributing to the need for rehabilitation, poor health, lack
of belief in getting a suitable job, and regarding the
improvement of physical condition as an important goal.
Gender, occupational group, regarding better mental health
as an important goal, and reported health disorders (back
disorders, other musculoskeletal disease and mental dis-
orders) did not have statistically significant associations
with the dependent variable.
In the simultaneous Model B, statistically significant
contributions to the final model were provided by age,
labor market situation, psychosocial factors, self-assessed
health, generalized self-efficacy, institutional trust, and
lack of belief in getting a suitable job. The chances of
having stable motivation for working life were statistically
significantly increased by stronger institutional trust
(p = 0.000) and stronger self-efficacy (0.002). On the other
hand, the chances of stable motivation were decreased by a
lack of belief in getting a job (p = 0.000), poor self-
assessed health (0.002), older age (0.003), being on dis-
ability pension (0.018), and a greater number of psycho-
social factors contributing to the need for rehabilitation
(0.038) (Table 3).
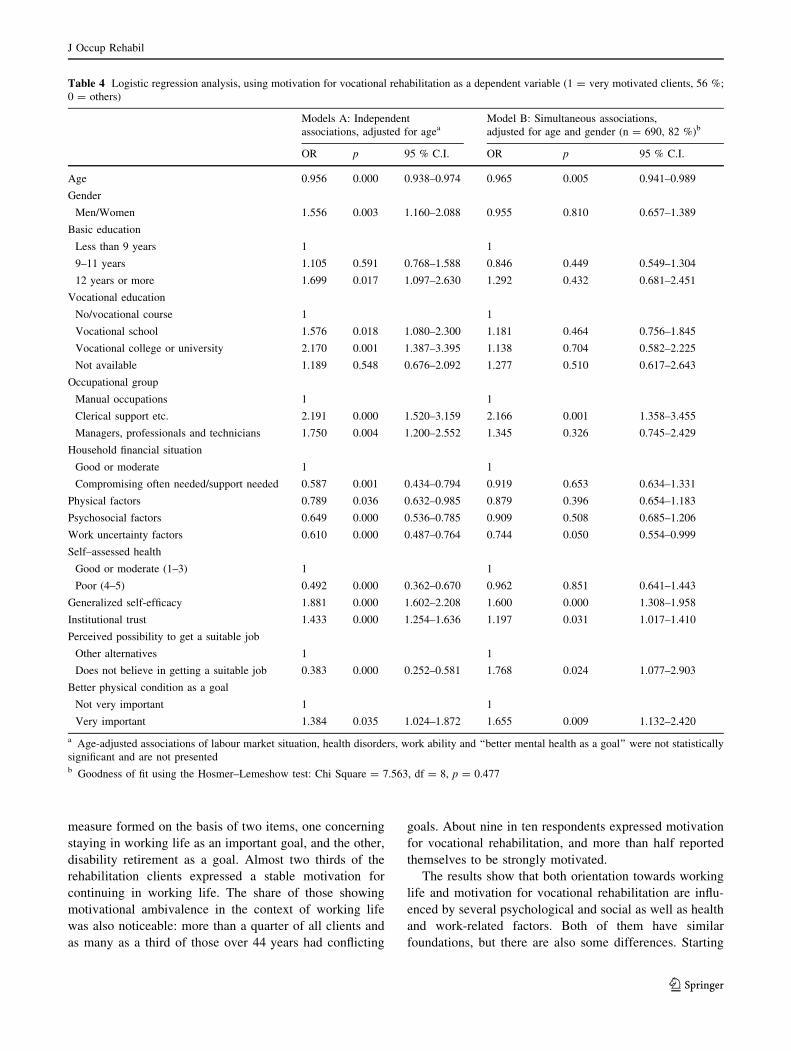
Variables associated with motivation for vocational
rehabilitation are presented in Table 4. In Models A, good
basic education (12 years or more) and vocational educa-
tion (vocational college/university), occupational group
other than manual work, stronger generalized self-efficacy,
stronger institutional trust, and better physical condition as
an important goal increased the chances of having strong
J Occup Rehabil
123

motivation for vocational rehabilitation statistically sig-
nificantly. On the other hand, older age, male gender,
weaker than moderate financial situation, a greater number
of factors contributing to the need for rehabilitation, poor
health, and lack of belief in one’s possibilities to get a job
decreased the chances of strong motivation. Labor market
situation, the occurrence of back disorders, other muscu-
loskeletal disorders and mental disorders, self-rated work
ability, and regarding better mental health as an important
goal did not have statistically significant associations with
the motivation for rehabilitation and are not presented in
the table.
Table 2 Goals and motivational orientations by gender and age (%)
Very important Important Not important Together % (n) p
Working life as a goal
Gender
Male 63.5 21.9 14.6 100 (416) 0.000
Female 74.3 18.2 7.5 100 (423)
All 68.9 20.0 11.1 100 (839)
Disability retirement as a goal
Gender
Male 18.3 16.4 65.3 100 (415) n.s.
Female 17.8 17.5 64.7 100 (422)
All 18.0 17.0 65.0 100 (839)
Better physical condition as a goal
Gender
Male 61.5 22.4 16.0 100 (416) n.s.
Female 67.5 16.8 15.6 100 (422)
All 64.6 19.6 15.8 100 (839)
Better mental health as a goal
Gender
Male 42.8 36.1 21.2 100 (416) 0.000
Female 57.0 27.0 16.1 100 (423)
All 49.9 31.5 18.6 100 (839)
Strong and stable Motivational ambivalence No motivation
Motivational orientation towards working life
Gender
Male 61.3 24.0 14.7 100 (416) 0.001
Female 62.0 30.7 7.3 100 (423)
Age
18–44 72.8 18.3 8.9 100 (360) 0.000
45–64 52.9 34.4 12.7 100 (480)
All 61.4 27.5 11.1 100 (839)
Very motivated Motivated Not motivated
Motivation for vocational rehabilitation
Gender
Male 51.6 32.4 16.0 100 (376) 0.004
Female 60.2 31.2 8.6 100 (394)
Age
18–44 64.4 26.8 8.8 100 (340) 0.000
45–64 49.4 35.7 14.9 100 (429)
All 56.1 31.9 12.0 100 (770)
J Occup Rehabil
123

In Model B, age, occupational group, the number of work
uncertainty factors, generalized self-efficacy, institutional
trust, lack of belief in getting a job, and better physical con-
dition as an important goal made statistically significant
contributions to the final model. The chances of strong moti-
vation for vocational rehabilitation were increased by stronger
generalized self-efficacy (p = 0.000), belonging to the
occupational group of clerical, service and sales workers
(0.001), having better physical condition as an important goal
(0.009) and having stronger institutional trust (0.031). On the
other hand, the chances of strong motivation were decreased
by older age (p = 0.005), lack of belief in getting a job (0.024)
and a greater number of work uncertainty factors (0.050)
(Table 4).
Discussion
In this study, two simple indicators of motivation were
used. Motivation for participation in working life was a
Table 3 Logistic regression analysis, using motivational orientation towards working life as a dependent variable (1 = clients with stable
motivation, 61 %; 0 = other clients, 47 %)
Models A: Independent
associations, adjusted for ageaModel B: Simultaneous associations,
adjusted for age and gender (n = 738)b
OR p 95 % C.I. OR p 95 % C.I.
Age 0.940 0.000 0.922–0.958 0.961 0.003 0.937–0.987
Basic education
Less than 9 years 1 1
9–11 years 1.415 0.051 0.998–2.007 0.976 0.910 0.635–1.499
12 years or more 1.831 0.006 1.189–2.819 1.278 0.399 0.722–2.263
Vocational education
No or vocational course 1
Vocational school 1.979 0.000 1.373–2.851
Vocational college or university 2.157 0.001 1.391–3.345
Not available 0.927 0.782 0.544–1.582
Labour market situation
In labour force 1
On disability pension 0.535 0.000 0.391–0.733 0.622 0.018 0.420–0.922
Household financial situation
Good or moderate (1–3) 1 1
Compromising often needed/support needed (4–5) 0.440 0.000 0.323–0.599 1.007 0.971 0.687–1.477
Physical factors 0.585 0.000 0.464–0.739 0.771 0.091 0.570–1.042
Psychosocial factors 0.641 0.000 0.532–0.773 0.738 0.038 0.554–0.983
Work uncertainty factors 0.740 0.005 0.600–0.913 1.039 0.802 0.773–1.396
Work ability (0–10) 1.222 0.000 1.147–1.303
Self–assessed health (1–5)
Good or moderate (1–3) 1 1
Poor (4–5) 0.242 0.000 0.177–0.330 0.532 0.002 0.358–0.791
Generalized self-efficacy 2.006 0.000 1.711–2.353 1.359 0.002 1.114–1.657
Institutional trust 1.600 0.000 1.397–1.833 1.376 0.000 1.159–1.634
Perceived possibility to get a suitable job
Other alternatives 1 1
Does not believe in getting a suitable job 0.145 0.000 0.092–0.227 0.249 0.000 0.148–0.419
Better physical condition as a goal
Not very important 1 1
Very important 0.719 0.033 0.531–0.973 0.844 0.406 0.566–1.258
a Age-adjusted associations of gender, occupational group, health disorders and ‘‘better mental health as a goal’’ were not statistically significant
and are not presented (Model A)b Goodness of fit of Model B, using the Hosmer & Lemeshow Test: Chi Square = 8.49, df = 8, p = 0.387. To improve the test value vocational
education and work ability were not included in Model B
J Occup Rehabil
123
measure formed on the basis of two items, one concerning
staying in working life as an important goal, and the other,
disability retirement as a goal. Almost two thirds of the
rehabilitation clients expressed a stable motivation for
continuing in working life. The share of those showing
motivational ambivalence in the context of working life
was also noticeable: more than a quarter of all clients and
as many as a third of those over 44 years had conflicting
goals. About nine in ten respondents expressed motivation
for vocational rehabilitation, and more than half reported
themselves to be strongly motivated.
The results show that both orientation towards working
life and motivation for vocational rehabilitation are influ-
enced by several psychological and social as well as health
and work-related factors. Both of them have similar
foundations, but there are also some differences. Starting
Table 4 Logistic regression analysis, using motivation for vocational rehabilitation as a dependent variable (1 = very motivated clients, 56 %;
0 = others)
Models A: Independent
associations, adjusted for ageaModel B: Simultaneous associations,
adjusted for age and gender (n = 690, 82 %)b
OR p 95 % C.I. OR p 95 % C.I.
Age 0.956 0.000 0.938–0.974 0.965 0.005 0.941–0.989
Gender
Men/Women 1.556 0.003 1.160–2.088 0.955 0.810 0.657–1.389
Basic education
Less than 9 years 1 1
9–11 years 1.105 0.591 0.768–1.588 0.846 0.449 0.549–1.304
12 years or more 1.699 0.017 1.097–2.630 1.292 0.432 0.681–2.451
Vocational education
No/vocational course 1 1
Vocational school 1.576 0.018 1.080–2.300 1.181 0.464 0.756–1.845
Vocational college or university 2.170 0.001 1.387–3.395 1.138 0.704 0.582–2.225
Not available 1.189 0.548 0.676–2.092 1.277 0.510 0.617–2.643
Occupational group
Manual occupations 1 1
Clerical support etc. 2.191 0.000 1.520–3.159 2.166 0.001 1.358–3.455
Managers, professionals and technicians 1.750 0.004 1.200–2.552 1.345 0.326 0.745–2.429
Household financial situation
Good or moderate 1 1
Compromising often needed/support needed 0.587 0.001 0.434–0.794 0.919 0.653 0.634–1.331
Physical factors 0.789 0.036 0.632–0.985 0.879 0.396 0.654–1.183
Psychosocial factors 0.649 0.000 0.536–0.785 0.909 0.508 0.685–1.206
Work uncertainty factors 0.610 0.000 0.487–0.764 0.744 0.050 0.554–0.999
Self–assessed health
Good or moderate (1–3) 1 1
Poor (4–5) 0.492 0.000 0.362–0.670 0.962 0.851 0.641–1.443
Generalized self-efficacy 1.881 0.000 1.602–2.208 1.600 0.000 1.308–1.958
Institutional trust 1.433 0.000 1.254–1.636 1.197 0.031 1.017–1.410
Perceived possibility to get a suitable job
Other alternatives 1 1
Does not believe in getting a suitable job 0.383 0.000 0.252–0.581 1.768 0.024 1.077–2.903
Better physical condition as a goal
Not very important 1 1
Very important 1.384 0.035 1.024–1.872 1.655 0.009 1.132–2.420
a Age-adjusted associations of labour market situation, health disorders, work ability and ‘‘better mental health as a goal’’ were not statistically
significant and are not presentedb Goodness of fit using the Hosmer–Lemeshow test: Chi Square = 7.563, df = 8, p = 0.477
J Occup Rehabil
123

with the differences, four factors call for attention. They
are gender, occupational status, labor market status, and
regarding better physical condition as a goal in
rehabilitation.
Gender was not associated with motivation towards
working life, whereas strong motivation for rehabilitation
was more frequent among women than men. Respectively,
occupational status was not associated with a stable moti-
vation towards working life, but it was strongly associated
with motivation for vocational rehabilitation. Motivation
for rehabilitation was the strongest among the predomi-
nantly female group of clerical, service and sales workers
and weakest among the predominantly male group working
in manual occupations. One possible interpretation of this
result lies in the difference of the meaning and anticipated
consequences of vocational rehabilitation in these groups.
For persons in physically or mentally strenuous occupa-
tions, vocational rehabilitation often means a change of
occupation or workplace. For many manual workers, it
may mean lower salaries because of decreased working
hours or fewer responsibilities. Strong occupational com-
mitments in certain occupations may also form a barrier to
accepting possible changes and may lower the inclination
to participate in rehabilitation. Otto et al. [49] emphasize
that if people are worried about meeting the demands of
work, it may be especially difficult for them to meet
additional challenges connected with a change of
occupation.
The respondent’s labor market status was, in turn,
associated with motivation for working life but not with
motivation for vocational rehabilitation. Stable motivation
for working life was much more probable with those still in
the labor force than among those on a temporary or per-
manent pension, who were more often ambivalent in their
motives. However, those on pension expressed strong
motivation for rehabilitation as often as the employed
group. A possible interpretation for this is that their will-
ingness to participate in vocational rehabilitation may also
arise from values and needs different from, or even oppo-
site to, the work-related ones. They may be security and
safety needs, or needs connected to physical and mental
health. In this study, this kind of relationship was shown by
the result that the goal of achieving better physical con-
dition correlated positively with motivation for vocational
rehabilitation, but negatively with motivational orientation
towards working life.
On a more general level, however, both motivational
orientations seem to have similar psychological and social
foundations. In addition to a person’s socioeconomic sta-
tus, they are based on his or her meta-cognitions and atti-
tudes, addressing both personal competences and
perceptions of the possibilities opened up by society—or
the lack of them.
Education and household financial situation are common
indicators of socioeconomic status. Clients with better
education and a good or sufficient self-rated household
income were more motivated to stay in working life and to
participate in rehabilitation than the average client. In a
Finnish study [50], socioeconomic status was negatively
associated with early retirement intentions among middle-
aged employees. According to Gould [51], better socio-
economic status and other life chances may enable
employees to prefer employment to early retirement [see
also 52, 53], and Kim and Feldman [54] found that lower
salary and expectations of higher pension benefits together
led to early retirement decisions among employees.
The strongest associations of the person’s motivational
orientations were with the person’s meta-cognitions,
beliefs and attitudes, that is, the perceived competence, the
assessment of one’s possibilities at the labor market, and
institutional trust. Considering the first of these, the results
confirmed the importance of perceived competence or
generalized self-efficacy as the basis of both motivational
orientations. Belief in one’s possibilities to accomplish
what one has aimed for strongly enhances both the moti-
vation to stay in working life and the motivation for
vocational rehabilitation. Locus of control beliefs have
been shown to be associated positively with rehabilitation
results [4, 55, 56] and negatively with disability retirement
in back pain patients [57]. A person’s confidence in his or
her capabilities to overcome obstacles is a characteristic
that develops in the course of the life span [22]. It can also
be strengthened by paying attention to successful events
during the rehabilitation process.
Another factor addressing future expectations was one’s
belief in getting work suitable for one’s abilities, which
was also strongly associated with both motivational ori-
entations. Insecurity of employment is the major source of
work-related risks in present societies which influences, in
addition to work motivation [see 34, 58], a person’s general
inclination to continue in working life and the willingness
to participate in rehabilitation interventions. The best way
to strengthen the rehabilitation clients’ motivation towards
working life is probably to show them that a job suitable to
their abilities is available; unfortunately this is not always
possible. The assessment of one’s future possibilities is
always based, in part, on the work history. In this study, a
great number of physical, psychosocial and uncertainty
factors at work were regarded as having contributed to the
problems experienced, and also seemed to decrease moti-
vation for continuing in working life and participating in
rehabilitation [see also 49, 59].
The concept of institutional or vertical trust has not, as
far as we know, been addressed in rehabilitation studies
before. In this study, institutional trust was understood as a
general trust in societal institutions, including perceptions
J Occup Rehabil
123

of receiving just and equal treatment by society, social
institutions and officials. This simple index was associated
with both the motivation for rehabilitation and, especially,
with motivation for working life. Its associations with both
motivation variables were strong and consistent. The con-
struct of institutional trust, as applied in this study, seems
to address the general perception of getting fair treatment
from society when one is in special need for help. As such,
a lack of it also weakens the individual’s inclination to
participate in the labor market when faced with chronic
illness.
There are limitations in this study that warrant attention.
Most of the variables of the study were based on cross-
sectional data collected by means of a questionnaire. It
does not allow for making inferences on causal connections
between different factors. Both of the motivation variables
used were simple, one based on a person’s goals of
continuing in working life and retirement, and the other
based on a single question of a person’s willingness and
eagerness to participate in rehabilitation. On the other
hand, the study has clear advantages. It is based on a rel-
atively large and representative sample of vocational
rehabilitation clients, representing all age, educational and
occupational groups and having a range of physical or
mental disabilities.
To sum up, the results indicate that the two motivational
orientations can be regarded as partly separate and partly
overlapping constructs. It seems necessary to make a dis-
tinction between these constructs especially when it is
apparent that the motivational orientations of quite a few
rehabilitation clients may be ambivalent. The results
clearly show that the rehabilitation clients’ motivational
orientations are associated with their experiences and their
perceptions on environmental factors and future possibili-
ties, both those that precipitated the application for reha-
bilitation and those that are important in their current life
situation and their perceived future possibilities. In the
planning of individual rehabilitation processes, there is a
clear need to sort out what factors may hide behind the
client’s weak contextual or situational motivation. In the
course of the rehabilitation process, it is important to dis-
cuss these factors in order to alleviate the clients’ uncer-
tainty towards change and enhance their motivation to
participate in rehabilitation and re-think their future pros-
pects of returning to work.
Acknowledgements: The data of this study was gathered in the
project ‘‘The functioning of vocational rehabilitation within the
earnings-related pension scheme’’, supported financially by the
Finnish Centre for Pensions. The manuscript of this study was pre-
pared as part of the project ‘‘Shared Agency and Empowerment in
Rehabilitation’’ financed by the Academy of Finland.
References
1. Fink SL. Crisis and motivation: a theoretical model. Arch Phys
Med Rehab. 1965;48:592–7.
2. King P, Barrowclough C. Rating the motivation of elderly
patients on a rehabilitation ward. Clin Rehabil. 1989;3:289–91.
3. Maclean N, Pound P, Wolfe C, Rudd A. Qualitative analysis of
stroke patients’ motivation for rehabilitation. Brit Med J.
2000;321:1051–4.
4. Grahn B, Ekdahl C, Borgquist L. Motivation as a predictor of
changes in quality of life and working ability in multidisciplinary
rehabilitation. Disabil Rehabil. 2000;22:639–54.
5. Jarvikoski A, Ojala S, Ravaja N. Mita kuntoutustutkimuksen
jalkeen? (What after the rehabilitation assessment?) Working
reports 7/1992. Helsinki: Rehabilitation Foundation; 1992 (In
Finnish.).
6. Tan V, Cheatle MD, Mackin S, Moberg PJ, Esterhai JL. Goal
setting as a predictor of return to work in a population of chronic
musculoskeletal pain patients. Int J Neurosci. 1997;92:1–8.
7. Saeki D, Ogata H, Okubo T, Takahashi K, Hoshuyama T. Impact
of factors indicating a poor prognosis on stroke rehabilitation
effectiveness. Clin Rehabil. 1993;7:99–104.
8. Nordt C, Brantschen E, Kawohl W, Bartsch B, Haker H, Rusch
N, Rossler W. ’Placement budgets’ for supported employment—
improving competitive employment for people with mental ill-
ness: study protocol of a multicentre randomized controlled trial.
BMC Psychiatry. 2012;12:165–70.
9. Senecal C, Vallerand RJ, Guay F. Antecedents and outcomes of
work-family conflict: toward a motivational model. Pers Soc
Psychol B. 2001;27:176–86.
10. Vallerand RJ. Deci and Ryan’s self-determination theory: a view
from the hierarchical model of intrinsic and extrinsic motivation.
Psychol Inq. 2000;11:312–8.
11. Guay E, Mageau G, Vallerand RJ. On the hierarchial structure of
self-determined motivation: a test of top-down and bottom-up
effects. Pers Soc Psychol B. 2003;29:992–1004.
12. Nair KPS. Life goals: the concept and its relevance to rehabili-
tation. Clin Rehabil. 2003;7:192–202.
13. Maclean N, Pound P, Wolfe C, Rudd A. The concept of patient
motivation. a qualitative analysis of stroke professionals’ atti-
tudes. Stroke. 2002;33:444–8.
14. Jahoda M. Employment and unemployment: a social-psycho-
logical analysis. Cambridge: Cambridge University Press; 1982.
15. Proschaska J, DiClemente CC. Stages and processes of self-
change of smoking: toward an integrative model of change.
J Consult Clin Psych. 1983;51:390–5.
16. Cole G, Leonard B, Hammond S, Fridinger F. Using 0stages of
behavioral change0 constructs to measure the short-term effects of
a worksite-based intervention to increase moderate physical
activity. Psychol Rep. 1998;82:615–8.
17. Franche R-L, Krause N. Readiness for return to work following
injury or illness: conceptualizing the interpersonal impact of
health care, workplace, and insurance factors. J Occup Rehabil.
2002;12:233–56.
18. Miller RW, Rollnick S. Motivational interviewing: preparing
people for change. New York: Guilford Press; 2002.
19. Manthey T, Jackson C, Evans-Brown P. Motivational inter-
viewing and vocational rehabilitation: a review with suggestions
for administrators and counselors. J Appl Rehabil Couns.
2001;42:3–14.
20. Gard G, Larsson A. Focus on motivation in the work rehabilita-
tion planning process: a qualitative study from the employer’s
perspective. J Occup Rehabil. 2003;13:159–67.
J Occup Rehabil
123
21. Berglind H, Gerner U. Motivation and return to work among the
long-term sick-listed: an action theory perspective. Disabil
Rehabil. 2002;24:719–26.
22. Bandura A. Social foundations of thought and action. Englewood
Cliffs: Prentice-Hall; 1986.
23. Bandura A. Social cognitive theory: an agentic perspective. Ann
Rev Psychol. 2001;52:1–26.
24. O’Sullivan D, Strauser DR. Operationalizing self-efficacy, related
social cognitive variables, and moderating effects. Implications
for rehabilitation research and practice. Rehabil Couns Bull.
2009;52:251–8.
25. Abele AE, Spurk D. The longitudinal impact of self-efficacy and
career goals on objective and subjective career success. J Vocat
Behav. 2009;74:53–62.
26. Wallston KA. Hocus-pocus, the focus isn’t strictly on locus:
Rotter’s social learning theory modified for health. Cogn Ther
Res. 1992;16:183–99.
27. Wallston KA, Osborn CY, Wagner LJ, Hilker KA. The perceived
medical condition self-management scale applied to persons with
HIV/AIDS. J Health Psychol. 2011;16:109–15.
28. Jerusalem M, Schwarzer R. Self-efficacy as a resource factor in
stress appraisal processes. In: Schwarzer R, editor. Self-efficacy:
thought control of action. Washington, DC: Hemisphere; 1992.
p. 195–213.
29. Nikkanen P, Puumalainen J, Hokkanen L, Jarvoski A. Kela va-
ikeavammaisten kuntoutuksen jarjestajana [Medical rehabilita-
tion for severely disabled persons organsed by the Social
Insurance Institution]. In: Jarvikoski A, Hokkanen L, Harkapaa
K, editors. Asiakkaan aanella [Voice of the customer]. Research
Reports 80/2009. Helsinki: Rehabilitation Foundation; 2009.
p. 146–69.
30. Lindstrom M, Janzon E. Social capital, institutional (vertical) trust
and smoking: a study of daily smoking and smoking cessation
among ever smokers. Scand J Public Health. 2007;35:460–7.
31. Fuglsang L, Jagd S. Making sense of institutional trust in orga-
nizations: bridging institutional context and trust. Organization.
2013. doi:10:1177/1350508413496577.
32. Gronlund K, Setala M. In honest officials we trust: institutional
confidence in Europe. Am Rev Public Adm. 2012;42:523–42.
33. Irestig R, Burstrom K, Wessel M, Lynoe N. How are homeless
people treated in the healthcare system and other societal insti-
tutions? Study of their experiences and trust. Scand J Public
Health. 2010;38:225–31.
34. Latham GP, Ernst CT. Keys to motivating tomorrow’s workforce.
Human Resource Manage Rev. 2006;16:181–98.
35. Cropanzano R, Rupp DE. An overview of organizational justice:
implications for work motivation. In: Porter LW, Bigley G, Steers
RM, editors. Motivation and work behavior. 7th ed. New York:
McGraw-Hill Irwin; 2003.
36. Elovainio M, Kivimaki M, Vahtera J. Organizational justice:
evidence of a new psychosocial predictor of health. Am J Public
Health. 2002;92:105–8.
37. Gould R, Harkapaa K, Jarvikoski A., editors. Toimiiko ty-
oelakekuntoutus? [Functioning of vocational rehabilitation within
the earnings-related pension scheme]. Research Reports 01/2012.
Helsinki: Finnish Centre for Pensions. 2012.
38. Jarvikoski A, Jyrkama O, Tossavainen A, Nurminen U-M. Var-
haiskuntoutukseen ja tyokykya yllapitavaan toimintaan kohdi-
stuvat odotukset ja valmiudet [Expectations from and readiness to
participate in early rehabilitation]. Kuntoutus [Rehabilitation].
1993;16:16–24.
39. Harkapaa K. Optimismi, kompetenssi ja selviytymiskeinot.
Kasitteiden ja empirian tarkastelua kuntoutuksen nakokulmasta
[Optimism, competence and coping strategies. Analysis of con-
cepts and empirical results in the context of rehabilitation].
Helsinki: Rehabilitation Foundation; 1995. Working papers 11.
40. Kouvo A. The sources of generalized trust and institutional
confidence in Europe. Res Finnish Soc. 2011;4:29–40.
41. Schoon L, Cheng H. Determinants of political trust: a lifetime
learning model. Dev Psychol. 2011;47:619–31.
42. Tuomi K, Ilmarinen J, Jahkola A, Katajarinne L, Tulkki A. Work
Ability Index. 2nd revised edition. Helsinki: Finnish Institute of
Occupational Health. 1998.
43. Ilmarinen J. The Work Ability Index (WAI). Occup Med.
2007;57:160.
44. Ahlstrom L, Grimby-Ekman A, Hagberg M, Dellve L. The work
ability index and single-item question: associations with sick leave,
symptoms, and health – a prospective study of women on long-term
sick leave. Scand J Work Environ Health. 2010;36:404–12.
45. Estama J, Arola A-M. Kuntoutus ei aina kaynnisty [Rehabilita-
tion does not always start up]. In: Jarvikoski A, Lindh J, Sui-
kkanen A, editors. Kuntoutus muutoksessa [Rehabilitation in
transition]. Rovaniemi: Lapland University Press; 2011. p. 63–72.
46. Mehnert A, Koch U. Predictors of employment among cancer
survivors after medical rehabilitation—a prospective study.
Scand J Work Environ Health. 2013;39:76–87.
47. Kim JK, Kim JJ. Nonresponse weighting adjustment using esti-
mated response probability. Can J Stat. 2007;35:401–54.
48. Lehikoinen T, Gould R, Jarvikoski A. Tutkimuksen toteutus
[Execution of the study]. In: Gould R, Harkapaa K, Jarvikoski A,
editors. Toimiiko tyoelakekuntoutus? [Functioning of vocational
rehabilitation within the earnings-related pension scheme].
Research Reports 01/2012. Helsinki: Finnish Centre for Pensions;
2012. pp. 25–36.
49. Otto K, Dette-Hagenmeyer DE, Dalbert C. Occupational mobility
in members of the labor force: explaining the willingness to
change occupations. J Career Dev. 2010;36:262–88.
50. Huhtaniemi P. The sense of life control and thoughts of early
retirement. Annales Universitatis Turkuensis B:210. Turku:
University of Turku; 1995.
51. Gould R. Choice or chance—late retirement in Finland. Soc Pol
Soc. 2010;5:519–31.
52. Von Bonsdorff ME, Huuhtanen P, Tuomi K, Seitsamo J. Pre-
dictors of employees’ early retirement intentions: an 11-year
longitudinal study. Occup Med. 2010;60:94–100.
53. Wang M, Shultz KS. Employee retirement: a review and recom-
mendations for future investigation. J Manage. 2010;36:172–206.
54. Kim S, Feldman DC. Healthy, wealthy, or wise: predicting actual
acceptances of early retirement incentives at three points in time.
Pers Psychol. 1998;51:623–42.
55. Selander J, Marnetoft SU, Asell M, Selander U. Internal locus of
control and vocational rehabilitation. Work. 2008;30:149–55.
56. Harkapaa K, Jarvikoski A, Mellin G, Hurri H, Luoma K. Health
locus of control beliefs and psychological distress as predictors
for treatment outcome in low back pain patients: results of a
3-month follow up of a controlled intervention study. Pain.
1991;46:35–41.
57. Harkapaa K. Psychosocial factors as predictors for early retire-
ment in patients with chronic low back pain. J Psychosom Res.
1992;36:553–9.
58. Matheson C. The motivation of public sector employees: an
outline of six orientations to work. Adm Soc. 2012;44:207–37.
59. Elovainio M, Forma P, Kivimaki M, Sinervo T, Sutinen R, Laine
M. Job demands and job control as correlates of early retirement
thoughts in Finnish social and health care employees. Work
Stress. 2005;19:84–92.
J Occup Rehabil
123