mgr medical university prefinal ent sep 2010 question paper with solution
TRANSCRIPT

8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 1/31
Pre final MBBS Otolaryngology MBBSQuestion Paper of Tamilnadu Dr MGR Medical Univers
September 2010with solution
By
Dr T Balasubramanian

8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 2/31
Third (Final) M.B.B.S. Degree Examination Otolaryngology
September 2010
(2x15=30)
1. What is stridor? Enumerate the causes of stridor. Describe briefly the management modalities
stridor.
Definition:
Stridor is defined as high pitched sound caused due to turbulent airflow in the upper airway due
obstruction. This is actually an emergency and airway should be secured at the earliest in orde
save the patient.
Classification of stridor:
Inspiratory stridor – in case of airway obstruction above the level of vocal cords
Expiratory stridor – in case of obstruction at the level of bronchi (Bronchial asthma)
Biphasic stridor – stridor is present during both during inspiratory and expiratory phases. This
classically caused due to tracheal obstruction. (Tracheomalacia is the classic example).
Causes for stridor in infants and adults are different and variable.
Causes of stridor:
Causes for stridor can be grossly classified into:
Laryngeal causes
Extralaryngeal causes
Laryngeal causes of stridor include varying disorders affecting laryngeal airway leading onto
obstructive airway pathology.
Congenital causes – These conditions cause stridor in infants. They include:
1. Infantile larynx – causing laryngomalacia
2. Laryngeal web / stenosis
3. Laryngomalacia
4. Congenital cysts / hemangioma
Neoplasms:
Includes both benign and malignant lesions.
Papillomas – two types juvenile and adults. Juvenile papilloma are multiple and their adult
counterpart is single. Juvenile papilloma has a high recurrence rate while adult papillomas afte
removal are not known to recur.
Cysts – These are benign and can be surgically removed
Tumors – Benign / malignant. Malignant tumors involving larynx causes stridor due to
1. Obstruction to the airway
2. Paralysis of both vocal cords
3. Fixity of both arytenoids
4. Laryngeal oedema following irradiation

8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 3/31
Figure showing the laryngeal causes of stridor
8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 4/31
Inflammatory causes:
These include
Acute laryngitis – very rarely they cause stridor
Diptheria – Membrane dislodges and obstructs laryngeal inlet
Angioneurotic oedema – Steroids will help in these patients
Acute laryngotracheal bronchitis – common in children
Foreign bodies:
Aspiration of foreign bodies are rare causes of stridor. More common in children.
Neurological:
Vocal cord paralysis – Bilateral abductor paralysis will cause stridor. This can be caused due t
involvement of recurrent laryngeal nerve on both sides due to thyroid malignancy / or due to
injury following total thyroidectomy.
Hypocalcemic tetany can also lead to stridor in rare cases.
Trauma – This includes birth trauma, burns and scalds etc.
8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 5/31
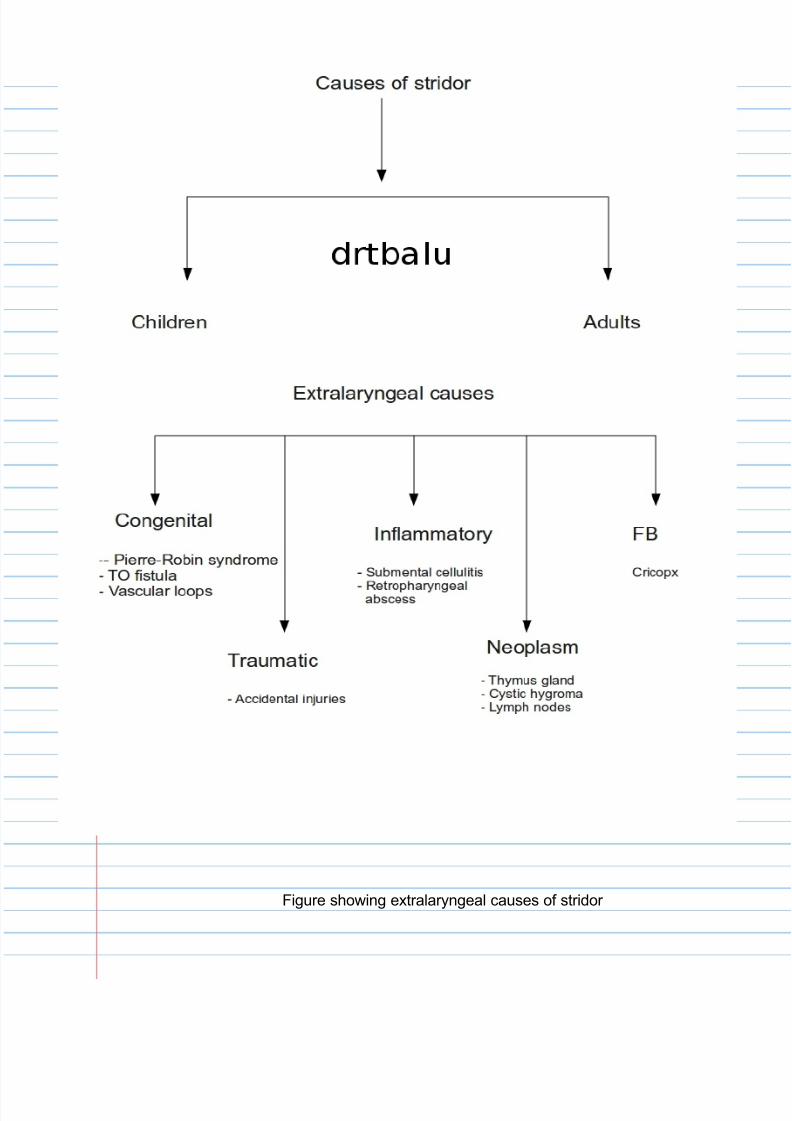
Figure showing extralaryngeal causes of stridor

8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 6/31
Extralaryngeal causes of stridor:
Congenital:
PIERRE ROBIN SYNDROME: This congenital condition is associated with facial anomalies wh
include an unusually small mandible (Micrognathia), posterior displacement of tongue (glossop
causing an upper airway obstruction.
Tracheo oesophageal fistula – Can be congenital / acquired. This is a surgical emergency.
Inflammatory causes:
Ludwig's angina – Submental oedema causing tongue to fall back obstructing the airway.
Retropharyngeal abscess – Surgical emergency
Foreign body cricopharynx – A big foreign body at the level of cricopharynx can cause upper
airway obstruction due to attendant airway oedema.
Neoplasm:
Enlarged thymus causing compression over upper trachea.
Cystic hygroma causing airway obstruction due to involvement of tongue (or fall back of it).
Enlarged prelaryngeal / cervical lymphnodes causing airway compression.
Management:
Priority should be given to securing the airway as early as possible.
Depending on the probable cause of stridor the management modality can be decided.
Attempting to oxygenate the patient: This is done on an immediate basis as a first aid procedu
Oxygen can be administered either by nasal prongs / face mask. Nasal prongs are better toler
by patients.
Intubation- This is the easiest way to secure the airway on an immediate basis. This may not w
stridor is caused due to tumors / oedema of larynx. Attempting to intubate these patients would
more harm than good in these patients.
Contraindications for intubation:
1. Presence of hoarseness of voice in addition to stridor – This indicates coexistant malignancy
Larynx of these patients should be examined before attempting intubation. This can be perform
by indirect laryngeal examination / video laryngoscopic examination.
2. Absence of laryngeal crepitus – This again indicates either the presence of foreign body at th
level of cricopharynx or growth at the level of cricopharynx. Intubation should not be attempted
in these patients.
3. Extralaryngeal causes of stridor is a contraindication for intubation.

8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 7/31

8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 8/31
Tracheostomy should be performed as a life saving procedure in these patients if intubation fail
or if it is contraindicated.
Before taking up the patient for tracheostomy the following investigations are a must:
Xray soft tissue neck lateral view to assess the adequacy of subglottic air column. For a
a successful tracheostomy a patient must have an adequate subglottic air column. This x ray
will also show any foreign body at the level of cricopharynx, retropharyngeal abscess etc.
Surgically securing the airway can be performed by any of these following methods:
Percutaneous tracheostomy
Criothyroidotomy
Tracheostomy
The aim of all these procedures is to secure the airway by surgically bypassing the obstructing
airway lesion.
2. Mention the differential diagnosis of white patch in tonsil
Causes of white patch seen over the tonsil can be classified according to their etiology.
Infections: Could be viral, bacterial and fungal.
Viral infections: Viral infections causing a white patch in the tonsil include:
Infectious mononucleosis – This infection is caused by EB virus. This infection commonly caus
unilateral enlargement of tonsil. The involved tonsil is covered with membrane (pseudomembr
These patients also have cervical adenitis and hepatosplenomegaly. Paul Bunnel test is positiv
Herpes simplex infections involving the tonsil will be seen as ulcerative lesions which are cover
with membranous slough. Initially these lesions appear as multiple shallow small ulcers. Thes
ulcers coalesce to form a large ulcer covered with membranous slough.
HIV infection – Membranous tonsillitis in these patients occur due to secondary infections.
Bacterial infections:
Can be further subclassified into:
Acute non specific type
Acute specific type
Chronic non specific type
Chronic specific type
Acute non specific type – This type is caused by a variety of bacteria. Acute follicular tonsillitis
belong to this category. Organism involved include streptococci, H influenza, pneumococci etc
dirty white membrane which is formed over the crypts of the tonsil can easily be peeled off the
tonsil without any bleeding. In this condition membrane is seen only over the tonsil and not ove
any other portion of the oral cavity.
Staphylococcal pseudomembranous tonsillitis is another condition in which a membrane is see
over the tonsil. Membrane formed is pseudomembrane type and can easily be peeled off witho
bleeding. These patients commonly manifest with cutaneous lesions characteristic of staphylo

8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 9/31
infection.
Acute specific type:
Faucial diphtheria – Caused by corynebacterium diphtheria. Membrane could be seen extensi
covering the tonsil, uvula and soft palate. The membrane formed is true membrane. It doesn't
strip easily. Even when attempted to be removed it leaves behind raw area which bleeds.
Significantly pain is absent in faucial diphtheria. Swab taken from the membrane demonstrates
corynebacterium diphtheria. Schick test is positive in these patients.
Vincent's angina – This infection is caused by two organisms namely Fuciform bacillus and
spirocheta denticulata. These patients have foul smelling breath, high grade fever and cervica
adenitis in addition to membranous tonsillitis. Smear from the membrane is diagnostic. Memb
when peeled causes considerable loss of tissue.
Chronic non specific type:
Keratosis of tonsil – In this condition keratin could be seen coming out of the crypts of tonsil. T
appear as whitish plaques. There are also associated keratosis seen over the posterior 1/3 of
and posterior pharyngeal wall. These patients are asymptomatic and the whole condition is an
incidental finding.
Chronic specific type – This type include tuberculous and syphilitic tonsillar infections. In tuber
the whole tonsil along with their pillars show ulceration. Smaller ulcers coalesce to form large
ones covered by dirty colored slough which appears like a membrane. Swab taken from
membrane shows mycobacterium.
Secondary syphilis involving the tonsil appear as white colored painless mucosal patch. Ulcers
seen over the tonsil appear like snail tracks and hence they are known as snail tract ulcers.
These ulcers are the characteristic feature of syphilitic tonsillitis.
Fungal infections: involving the tonsil appear as whitish patches if the infecting fungus happens
to be candida. This condition is also known as the oral thrush. Fungal infections involving the
tonsil are seen in immunocompromised individuals.
Autoimmune conditions causing whitish patch over the tonsil – Include Lichen planus and wege
granulomatosis. These conditions are caused by autoimmunity for mucous membrane coverin
the tonsil.
Traumatic causes of membrane formation over tonsil – These include surgical trauma, thermal
injuries, foreign body, corrosive poisoning and post irradiation.
Premalignant conditions presenting as a patch over the tonsil – include Leukoplakia and
submucosal fibrosis. These conditions are painless and non inflammatory in nature.
Tumor and tumor like conditions causing whitish patch over tonsil include:
Tonsillar cyst – Painless and incidental finding
Tonsillolith – Painless commonly and incidental
Papilloma – Painless and incidental
Fibroma of tonsil – Painless and incidental
Malignancy of tonsil – Pain may be present. Associated JD node enlargement can be seen.
8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 10/31
Systemic conditions causing membrane over tonsil include:
Leukemia
Agranulocytosis
Aplastic anaemia
Blood dyscrasias
These conditions can be ruled out by performing routine blood smear examination.
infection causes membranous tonsillitis.
3. Write short notes on:
10x5=50
a. FESS
Introduction:
FESS is an acronym for Functional Endoscopic Sinus Surgery. This surgery aims at restoring
the normal function of paranasal sinuses.
Indications for FESS:
1. Chronic sinusitis resistant to medical management
2. Repeated acute exacerbations of chronic sinusitis
3. In order to remove resistant focal infections from the paranasal sinuses
4. In the management of fungal sinusitis in an effort aimed at ventilation of paranasal sinuses
Aim of FESS -
Aim of FESS is to remove paranasal sinus drainage block there by facilitating faster recovery of
the mucociliary mechanism of nose and paranasal sinuses. Experiments have shown that
drainage of sinuses always occur through their natural ostium because cilia always beat toward
their natural ostium.
Procedure:
This surgery is usually performed under local / general anesthesia.
The nasal cavity is packed with 4% xylocaine mixed with 1 in 100,000 units of adrenaline. Xylo
anesthetizes the nasal mucosa while adrenaline decongests the nasal mucosa thereby increas
dimensions of nasal cavity and reduces bleeding during surgery. 0 degree nasal endoscope is
to perform the surgery.
Steps of surgery:
1. Medialization of the middle turbinate. This is done gently using a freer's elevator. Infiltrating
the root of middle turbinate with ¼ cc of 2% xylocaine mixed with 1 in 100,000 units adrenaline
will ensure anesthesia of the middle meatus which is the area of surgery.
Uncinectomy:
Uncinate process is identified and medialized using a probe. It is completely removed using a
sickle knife / back biting forceps. It is important that the uncinate process is removed complete
including its inferior horizontal portion. Natural ostium of maxillary sinus can be seen when the
horizontal portion of inferior part of uncinate is removed. The natural ostium can be widened
using a back biting forceps.

8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 11/31
Clearance of frontal recess area comes next. The frontal recess area can be widened after bu
ethmoidalis is deroofed.
The horizontal portion of middle turbinate separates the anterior ethmoidal cells from the poste
group. If the posterior group of ethmoidal cells are found to be involved then they can be acce
after breaching the basal lamella. The idea is to remove the diseased mucosa, widening the
drainage channels of paranasal sinuses thereby allowing them to be ventilated normally. This
ensures faster regeneration of the ciliated columnar epithelium and restoration of normal ciliary
motility.
Complications of FESS:
1. Bleeding
2. CSF leak
3. Injury to orbit and its contents
4. Synechiae formation

8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 12/31
b. Stapedial reflex:
Introduction:
Contraction of stapedial muscle occurs under normal conditions when a loud acoustic stimulus
is presented to the auditory system. This muscle contraction causes a stiffening of the
ossicular chain and decreases the compliance of the middle ear system. This change in the
middle ear compliance an be recorded by tympanometry. This reflex is binaural and simultaneo
occurs in both the ears. This reflex is activated in normal adults when the sound pressure leve
range between 70-105 dBHL.
Stapedial muscle contraction in response to intense sound signal occurs bilaterally because the
reflex pathway has both ipsilateral and contralateral projections. Acoustic reflex thresholds are
usually estimated in response to stimuli of 500, 1000, 2000, and 4000 Hz. For screening
purposes it is sufficient if recording is made at 1000 Hz.
Reflex pathway:
Any reflex pathway by definition should include:
1. Sensory limb - Input
2. Central integration
3. Motor limb – Output
This stapedial reflex is designed to be protective in nature that limits the damage caused by hig
intensity sound. The sensory signals travel to the cochlear nuclei via the auditory component
of the 8th cranial nerve. From the cochlear nucleus signals travel to the superior olivary comple
bilaterally, and from there to the lower motor neurons in the facial nucleus which innervates
the stapedius muscle.
Indications:
1. Objective assessment of hearing – Range of acoustic reflex in persons with normal hearing
averages between 70-100dB sound pressure level. In conductive hearing losses, greater the lo
greater becomes the acoustic threshold reflex. Where as in sensorineural hearing loss the
acoustic reflex threshold may be within normal range, this is true in patients with mild to
moderate levels of sensorineural hearing losses with recruitment.
2. Can be used as a topognostic test in patients with facial nerve paralysis
3. Can be used in identifying deafness in infants
4. Acoustic neuroma dianosis
Contraindications:
1. In infants under the age of 7 months due to extreme pliability of external canal
2. In the presence of wax as the results may not be reliable
c. Scarlet fever:
Introduction:
Also known as scarlatina. It is an exotoxin mediated disease arising from group A Beta hemoly
streptococcal infection. This condition usually evolves from tonsillar / pharyngeal focal infection
8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 13/31
Bacteriology:
Group A Betahemolytic streptococci are known to secrete a number of enzymes of toxins. One
such toxin is known as the erythrogenic toxin which is responsible for the pathognomonic rash
of scarlet fever. These organisms are known to survive extremes of temperature and are sprea
via fomites.
During the 18th century scarlet fever was one of the most dreaded epidemics. With the advent
excellent antibiotics this condition is not threatening anymore.
Incidence:
This condition frequently affects children between 4-8 years. This infection is rare in children u
the age of 2 because of the presence of maternal antibodies.
Clinical features:
Scarlet fever has an incubation period ranging from 1-4days. Evolution and presentation of thi
disease is usually dramatic. These patients complain of:
Sudden onset fever
Throat pain
Malaise
Myalgia
Characteristic skin rash appears within 12 – 48 hours after the onset of fever.
If these patients are untreated the fever peaks by 48 hours.
Condition abates within a couple of days after starting treatment with appropriate antibiotics.
On examination:
Exudative tonsillitis usually precede this condition.
Tonsillar infections are usually accompanied by erythematous oral mucous membrane along w
petechiae / punctate red macules over hard palate/soft palate/uvula. These spots are known a
Forchheimer's spots. The tongue appears coated and reddish “raspberry tongue”.
Features of skin rash:
1. Rash generally appears within 12 – 48 hours after the onset of fever. In the beginning it app
as erythematous patches below the pinna, chest and axilla. Dissemination to the trunk and
extremities occur within the first day.
2. The rashes typically consist of scarlet macules over generalized erythema (Boiled lobster
appearance).
3. The skin lesion later evolves to become more diffuse, and later turn punctate resembling
sunburn / goose pimples.
4. Fragile capillaries under the skin ruptures displaying arrays of petechiae known as (Pastia
lines).
5. Circumoral pallor is another distinguishing feature seen in these patients.
6. Peeling of skin occurs in the skin of axilla, groin, and toes.
Blood count – shows predominant leucocytosis. Eosinophilia develops during the first week of
infection.
Throat culture is diagnostic. It also helps in deciding the sensitivity of the organism to the spec
8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 14/31
antibiotic.
Management:
The goals in managing this disease are
1. Prevention of acute rheumatic fever
2. Reducing the spread of infections
3. Prevention of suppurative complications
4. Shortening the course of ailment
Antibiotics:
Penicillin is the drug of choice. Could be administered either orally / parenterally. Amoxycillin
has gradually replaced penicillin as the first choice antibiotic in these patients.
d. Septal hematoma
Introduction:
Septal hematoma is defined as collection of blood between the perichondrium of nasal septum
the septal cartilage. Since nose is the most prominent part of the face it is more prone to injuri
which could lead to septal hematoma formation.
Pathophysiology:
The submucosal blood vessels present under the mucosal lining of nasal septum may be dama
due to sharp buckling forces to which nasal septum could be subjected to in case of trauma. If
mucosa is intact then blood will collect under the perichondrium leading on to hematoma forma
This will strip the muco perichondrial layer away from the septal cartilage causing a bulge which
could be seen in the nasal septal area. If the trauma is severe enough to cause fracture of nas
septal cartilage then blood may seep to the opposite side also stripping the muco perichondrial
layer on the opposite side also. This condition can be identified by the presence of bilateral
septal swelling. This bilateral septal hematoma is really critical because it can compromise the
nourishment of the septal cartilage which occurs only when the perichondrium is in contact with
This nutritional compromise can lead to liquifaction necrosis of the septal cartilage leading on to
pig snout deformity. Cartilage resorption starts to occur from the third day of vascular comprom
If the septal hematoma is unilateral and small it may cause localized necrosis of cartilage leadin
on to fibrosis and thickening of cartilage in that area.
Signs & symptoms:
The predominant symptom is nasal obstruction. If the hematoma is unilateral then nasal obstru
too is unilateral, if the same is bilateral then nasal block is also bilateral.
Examination:
Should be carried out without the introduction of nasal speculum. The nasal septum can be cle
viewed by just lifting up the tip of the nose. Examination will reveal a smooth rounded unilatera
bilateral rounded swelling extending up to the lateral nasal wall. The swelling will be fluctuant
and may blanch on application of gentle pressure. Long standing septal hematoma can lead to
formation of septal absess. Presence of pain and tenderness indicate abscess formation.

8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 15/31
Management:
Early evacuation of hematoma will definitely reduce the risk of cartilage necrosis, hence it is alw
worthwhile trying it out. Evacuation can be performed under local anesthesia via a hemitransfix
incision. This incision is sited at the lower border of the septal cartilage. The septal hematoma
would have already elevated the mucoperichondrial flap away from the septal cartilage, hence
evacuation of hematoma would be pretty straight forward. If the cartilage show evidence of ne
it should be immediately removed and homograft cartilage should be used to cover the defect.
The homograft cartilage are sourced from patients who have undergone submucosal resection
nasal septum. This cartilage can be stored in 0.1% sodium mercurothiosalicylate solution.
Nowadays cartilage banks are commonly available.
Antibiotics and anti inflammatory drugs should be prescribed for these patients as a routine ino
to prevent development of septal abscess.

8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 16/31
Complications:
1. External deformity of nose – The dorsum of the nose derives its support from the septal carti
If this support is lost then it would lead on to the formation of saddle nose deformity. If this
injury occurs during early childhood then it would cause under development of the whole of
middle third of face causing maxillary hypoplasia.
2. Septal abscess – Blood is an excellent culture medium and hence could get infected leading
on to abscess formation. The presence of septal abscess will lead on to constitutional
symptoms like fever, toxemia etc.
3. Septal deviation – Unilateral septal hematoma can cause local thickening of nasal septum th
causing deviation of nasal septum.
e. CROUP:
Synonyms: Acute laryngotracheal bronchitis, Viral laryngotracheal bronchitis
Introduction:
This clinical syndrome is characterized by:
a. Hoarseness of voice
b. Stridor which could be inspiratory or biphasic
c. Barking cough
d. Fever
e. Malaise
Pathophysiology:
This condition is usually caused by mucosal oedema of larynx and trachea. The lining mucosa
larynx and trachea is pretty lax in infants, and hence can swell up rapidly causing airway
compromise. Inflammation and oedema occurs in the subglottic area and trachea commonly.
Children of age between 6 months and 3 years are affected commonly. Peak age of occurren
happens to be 2 years.
Causative organism:
Viruses have been implicated as the common cause. They include:
Parainfluenza type I virus, Parainfluenza type II virus, Respiratory syncitial virus and Influenza
type A and type B viruses.
Management:
Since it is a self limiting disease reassurance and supportive therapy may be all that is needed
Child usually improves dramatically within the first 24 hours and complete recovery occurs wit
4 days even without treatment.

8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 17/31
If the affected child has acute airway obstruction then hospitalization is a must. Coexistent
measles infections and bronchopneumonia may complicate the issue.
Croup scores:
Grading croup will help us in deciding the optimal management modality of these patients:
Commonly used grading system is the Westley scale.
Westley scale:
This scoring system helps the examiner in assessing the degree of respiratory compromise.
Usually the following five factors are taken in to consideration in this scoring system:
Inspiratory stridor:
None – 0 points
Upon agitation – 1 point
At rest – 2 points
Chest retractions:
Mild – 1 point
Moderate – 2 points
Severe – 3 points
Air entry:
Normal – 0 points
Mild decrease – 1 point
Marked decrease – 2 points
Cyanosis:
None – 0 points
Upon agitation – 4 points
At rest – 5 points
Level of consiousness:
Normal – 0 point
Depressed – 5 points
Over all score:
Less than 3 – mild
3-6 moderate
6 and above is severe
DD:
Ideally croup should be differentiated from conditions causing stridor. They include:
Allergic reaction, angioneurotic oedema, subglottic tumors, neck space infections etc.
8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 18/31
Plain x-ray chest – Shows classic steeple sign in the laryngotracheal air column. The shadow
resembles steeple of a church. This is due to significant subglottic narrowing seen in these
patients.
Arterial blood gas estimations are not routinely done. They are indicated only in patients with
significant amount of cyanosis.
The child should be made as comfortable as possible. Moist air will help these children to reco
faster. Injection dexamethazone in doses of 0.15mg/kg if administered within 2-4 hours of attac
can alleviate symptoms because of its antiinflammatory effects.
In patients with severe distress administration of nebulized L epinephrine will help. This acts b
constriction of precapillary arterioles causing a reduction in the capillary hydrostatic pressure.
Heliox an inert gas inhaled in combination with oxygen causes greater laminar flow in the
respiratory tract ensuring better gas exchange.
Antibiotics are not indicated in these patients.
f. Lateral wall of Nasal cavity
Introduction:
With the advent of nasal endoscopes and use of endoscopes in nasal surgeries the anatomy of
the lateral nasal wall has been rewritten. The current description of anatomy of lateral nasal w
is infact the endoscopic anatomy of lateral nasal wall only.
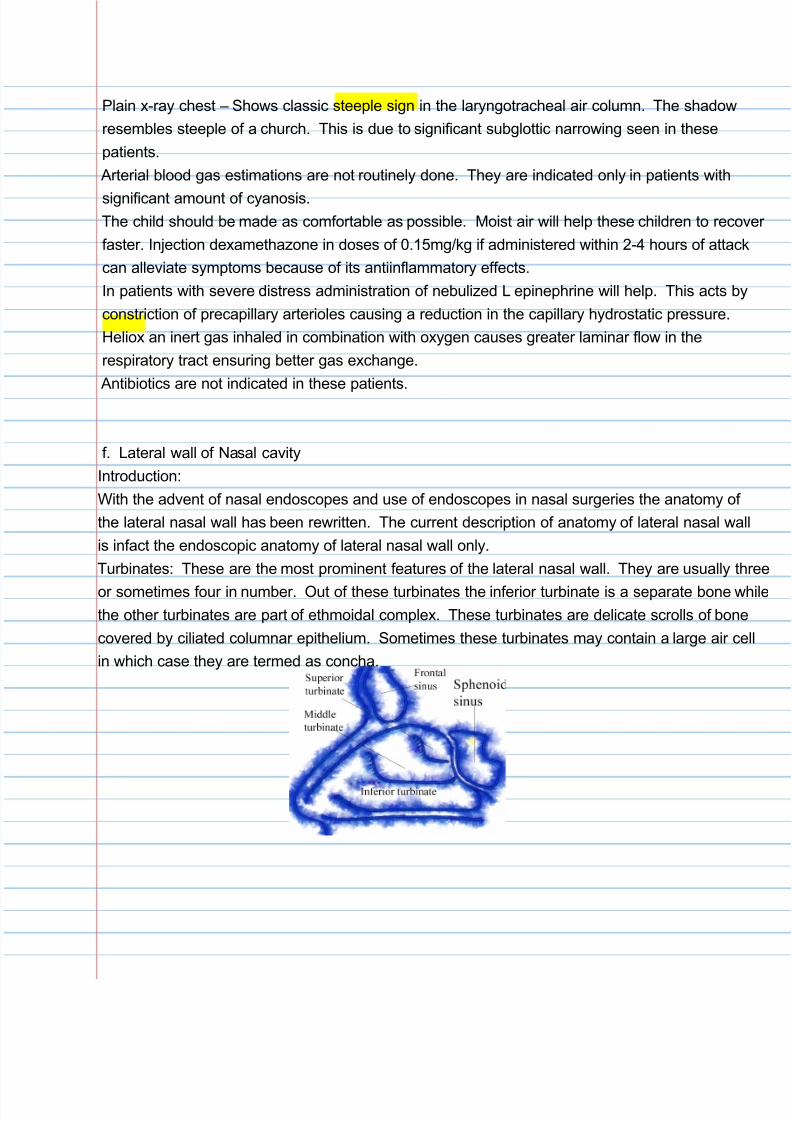
Turbinates: These are the most prominent features of the lateral nasal wall. They are usually t
or sometimes four in number. Out of these turbinates the inferior turbinate is a separate bone w
the other turbinates are part of ethmoidal complex. These turbinates are delicate scrolls of bon
covered by ciliated columnar epithelium. Sometimes these turbinates may contain a large air c
in which case they are termed as concha.

8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 19/31
These turbinates are named according to their positions:
Superior turbinate
Middle turbinate
Inferior turbinate
Supreme turbinate rarely
A prominence can be seen commonly anterior to the attachment of middle turbinate. This is kn
as aggernasi. This projection usually overlie the lacrimal sac. This prominence may be of
varying shapes in different individuals. This prominence is considered to be remnants of
nasoturbinal bones seen in animals.
Under each of these turbinates and lateral nasal wall a space is enclosed. The space between
inferior turbinate and lateral nasal wall is known as the inferior meatus. The nasolacrimal duct
into the inferior meatus in its anterior third. This opening is covered by mucosal valve known a
Hassner's valve. The course of the nasolacrimal duct lie under the agger nasi cell.
Middle meatus:
This critical space lies between the middle turbinate and the lateral nasal wall. In this space op
the drainage channels of the anterior group of paranasal sinuses. These include:
1. Frontal sinus
2. Maxillary sinus
3. Anterior ethmoidal sinus
4. Middle group ethmoidal sinus
It is this space which is critical in the pathophysiology of sinusitis. It is this space that is relevan
in functional endoscopic sinus surgery.
Figure showing the lateral nasal wall after removal of turbinates
8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 20/31
Uncinate process: This boomerang shaped (L) shaped bone forms the first layer (lamella) of
middle meatus. This bone should be removed in its entirety in order to visualize the natural
ostium of maxillary sinus and frontal sinus drainage channel.
Ethmoidal infundibulum: This is a cleft like three dimensional space in the lateral wall of the nos
This space is bounded medially by the uncinate process and the mucosa covering it. Major po
of its lateral wall is bounded by lamina papyracea, and the frontal process of maxilla to a lesser
extent. Defects in the medial wall of infundibulum is covered with dense connective tissue and
periosteum. These defects are known as anterior and posterior fontanelles.
Hiatus semilunaris: This lies between the anterior wall of bulla and the free posterior margin of
uncinate process. This hiatus semilunaris leads to the ethmoidal infundibulum.
Osteomeatal complex:
This term is used by the surgeon to indicate to indicate the area bound by middle turbinate med
lamina papyracea laterally and the basal lamella superiorly and posteriorly. It is through this ar
the anterior group of sinuses drain. This area happens to be a cesspool of secretions from all
the anterior group of sinuses.
g. Atrophic rhinitis
Definition:
Atrophic rhinitis is defined as a chronic nasal disease characterized by progressive atrophy of n
mucosa along with the underlying bones of turbinates. There is also presence of viscid secreti
which gets dried up leading on to the formation of foul smelling crusts. The characteristic foetid
odour emanating from these crusts is known as ozaena. The nasal cavity in these patients app
to be abnormally patent. The patients with this condition are fortunately unaware of this condit
because of the coexisting presence of anosmia (Merciful anosmia).
Etiology:
Still remains obscure. Numerous pathogens have been implicated. The most important of them
a. Coccobacillus
b. Bacillus mucosus
c. Coccobacillus foetidis ozenae
d. Diptheroid bacilli
e. Klebsiella ozenae
Even though these organisms have been repeatedly isolated from the nasal cavity of these pat
they have not been categorically proved to be the cause.
Other predisposing causative factors include:
a. Chronic sinusitis
b. Excessive destruction of nasal mucosa and turbinates (overzealous nasal surgeries)

8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 21/31
c. Nutritional deficiencies
d. Syphilis
e. Endocrine imbalances (This disease is known to worsen with pregnancy)
f. Hereditary
g. Autoimmune mechanisms – According to Faud these patients have altered cellular immunity
leading on to intolerance to nasal tissues. This immune intolerance can be caused by viral
infections.
Fraenkel triad:
Dr Bernhard Fraenkel described a classic triad of symptoms seen in these patients. According
Fraenkel the presence of this triad is a must for the diagnosis of atrophic rhinitis. This triad inc
1. Fetor
2. Crusting
3. Atrophy
Age of onset – This disorder commonly occurs at puberty.
Females are more commonly affected than males
Bernat postulated that iron deficiency could probably cause this condition.
Histopathology:
1. Metaplasia of ciliated columnar epithelium into squamous epithelium
2. There is a decrease in the number and size of nasal compound alveolar glands
3. Dilated capillaries can be seen
Pathologically atrophic rhinitis has been divided into two types:
Type I – This is characterized by the presence of endarteritis and periarteritis of terminal arterio
Usually this type could be caused by chronic infections. These patients benefit from the
vasodilator effects of oestrogen. Majority of these patients belong to this categoty.
Type II – This type is characterised by vasodilatation of capillaries and these patients are likely
worsen with oestrogen therapy. The endothelial cells of these capillaries contain more cytoplas
than those of normal capillaries. These cells also show active reaction for alkaline phosphatas
indicating rapid bone destruction.
Clinical classification of atrophic rhinitis:
Clinically atrophic rhinitis can be classified into primary and secondary types.
Primary atrophic rhinitis:
This is the classic form of atrophic rhinitis and is supposed to arise denovo. Diagnosis of this ty
of atrophic rhinitis is by the process of exclusion. All the known causes of atrophic rhinitis shou
be ruled out before branding the patient to be suffering from primary atrophic rhinitis. The
causative organisms in these patients are usually klebsiella ozenae.
Secondary atrophic rhinitis:
This is the most common form of atrophic rhinitis seen in developed countries. The most comm
8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 22/31
causes of this form of atrophic rhinitis include:
1. Extensive destruction of nasal mucosa and turbinates during nasal surgery
2. Following irradiation
3. Following granulomatous infections like syphilis, leprosy and tuberculosis
Clinical features:
1. Nasal obstruction
2. Epistaxis
3. Anosmia (Merciful)
4. Foul smelling greenish yellow crust can be seen inside the nasal cavity
5. Roomy nasal cavity due to atrophy of nasal mucosa and turbinate bones
6. These patients are psychologically depressed because of the foul smelling crusts in the nose
Reason for nasal obstruction despite the presence of roomy nasal cavity:
The nasal cavity is filled with sensory nerve endings close to the nasal valve area.
These receptors sense the flow of air through this area thus giving a sense of freeness in
the nasal cavity. These nerve endings are destroyed in patients with atrophic rhinitis
thus depriving the patient of this sensation. In the absence of these sensation the nose
feels blocked.
Radiographic findings:
This is more or less the same for both type I and type II atrophic rhinitis. Plain x-rays paranasa
sinuses show:
1. Lateral bowing of nasal walls
2. Thin / absent turbinates
3. Hypoplastic maxillary sinuses
CT scan findings:
1. Mucoperiosteal thickening of paranasal sinuses
2. Loss of definition of osteomeatal complex due to destruction of bulla
3. Hypoplastic maxillary sinuses
4. Enlargement of nasal cavity with erosion of lateral nasal wall
5. Atrophy of inferior and middle turbinates
Management:
Conservative:
Nasal douching – Patient is encouraged to douch the nasal cavity at least twice a day with solu
prepared with:

8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 23/31
1. Sodabicarb – 28.4 g
2. Sodium diborate – 28.4 g
3. Sodium chloride – 56.7 g
mixed in 280 ml of luke warm water.
The greenish yellow crusts can be removed by suction or by teasing with forceps.
Glucose glycerine drops:
25% glucose dissolved in glycerine can be administered into the nasal cavity. Glycerine is an
hygroscopic agent hence moistens the nasal cavity thereby softening the crusts. 25% glucose
inhibits proteolytic organisms which are commonly present in the nasal cavity of these patients
Patients with histological type I atrophic rhinitis could benefit from nasal topical administration o
oestradiol in arachis oil in concentrations of 10,000 units / ml.
Another topical medication that could benefit these patients is Kemecitine antiozena solution.
Kemecitine antiozena solution contains:
1. Chloramphenicol – 90 mg
2. Oestradiol dipropionate – 0.64 mg
3. Vitamin D2 – 900 IU
4. Propylene glycol
5. Isotonic saline 1 ml
Oral administration of potassium iodide has been tried in an effort to increase nasal secretions
with varying degrees of success.
Systemic administration of placental extracts have also been attempted in these patients.
Surgical management:
Submucous injection of paraffin - This happens to be one of the procedures that displaces the
lateral nasal wall medially. Various materials are being used for this procedure. This medializa
procedure is also known as “Lautenslauger's operation”. Recently teflon strips / autogenous
cartilages are being inserted after elevating the flaps in the lateral wall and floor of the nasal ca
Wilson's operation: Submucosal injection of 50% teflon in glycerine paste. This not only narro
the nasal cavity but also helps in dislodging the crusts.
Stellate ganglion blocks: This helps to some extent in increasing the glandular secretions of th
nasal cavity. Sometimes this process may need to be repeated more than once for optimal
benefit.
Young's operation:
This procedure aims at closing the nasal cavity by raising mucocutaneous flaps. In this method
mucocutaneous flaps are raised all around inside the nasal cavity. This flap is then sutured in
such a way that the whole nasal cavity is obliterated. The nasal cavity is kept blocked for a per

8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 24/31
of 9 months during which time the nasal mucosa would have regenerated. After 9 months the
nasal mucosa can be assessed by performing a post nasal examination. If it had regenerated
then the sutured flaps can be released and the nasal cavity reopened. This procedure should
be performed on one side first, then after opening up the nasal cavity after 9 months the other s
should be attempted.
Modified young's operation:
In this procedure a small hole measuring 3 mm is left while the flaps are being sutured. This ho
helps the patient to breath normally through the nasal cavity. The healing process can also be
monitored by performing periodical nasal endoscopic examination via the opening.
h. Physiology of hearing
In the study of physiology of hearing the role played by external ear, middle ear and internal ea
should be discussed separately.
Role played by external ear:
Because of its funnel shape the external ear helps in capturing sound waves and focuses it
on the ear drum. The portions of external ear which play an important role in sound conduction
are: Pinna, concha and external auditory meatus.
Functions of external ear:
1. By acting as an resonator it increases the pressure of sound at the level of ear drum in a freq
specific manner. It is known to resonate better in the frequency range of 2-5 Khz.
2. It helps in sound localization
3. The pinna conchal system acts like a trumpet focussing the sound to the ear drum for transm
Role of ear drum in sound conduction:
The ear drum conducts sound from external ear to middle ear. According to Bekesey the ear d
moves like a stiff plate up to the frequency levels of 2 KHz. Above this frequency the vibrating
pattern gets broken up and becomes more complex. The ear drum serves to conduct sound
preferentially in the frequency ranges between 2-5 Khz. The handle of the malleus is attached
to the centre of the ear drum. This relationship helps in conduction of sound from the external
to the middle ear.
Role of middle ear in sound conduction:
The middle ear serves to couple sound energy to the fluids of cochlea. It should be borne in m
that sound gets reflected from the interface separating two media with different impedances. T
is true of the middle and inner ear interface because the cochlear fluids have higher impedance
to sound when compared to that of air in the middle ear cavity. In order to conduct sound
efficiently without loss the middle ear should function as an impedance matcher. The middle ea
serves to convert low pressure high displacement vibrations to high pressure low displacement
ones which is favorable for sound conduction via cochlear fluids. The middle ear apparatus

8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 25/31
couples sound preferentially to one window of the cochlea thereby creating differential pressure
between the oval and round windows which pushes the cochlear fluid in a forward direction.
Components of middle ear transformer mechanism:
1. The surface area of ear drum is 55 mm2, while the surface area of foot plate of stapes is
3.2 mm2. The difference between these surface areas happens to be roughly 17 times. Thu
the forces collected by the ear drum are concentrated over a small area causing movement
of cochlear fluids towards round window.
2. Ossicular lever ratio. This roughly works out to 2.1 times. The incus is shorter than the mall
and this is very important for lever action of ossicles. This lever action increases the force
and decreases the velocity at the level of stapes.
3. Buckling effect of ear drum: The ear drum curves from its rim to its attachment to the manub
This buckling effect causes greater displacement of the ear drum and lesser displacement of
the manubrium.
This middle ear transformer mechanism ensures that atleast 50% of the incident sound energy
gets transmitted to the cochlea.
Role played by cochlea:
Sound traveling through cochlea causes a mechanical traveling wave which forms the basis
of frequency selectivity. Features of cochlear traveling wave:
1. As the wave travels along the cochlea it reaches a peak and dies down rapidly
2. The basilar membrane vibrates at a constant frequency for all low frequency sounds and dro
abruptly above certain frequency levels.
It has been shown that basal turn of cochlea responds best to high frequency sounds and the a
cochlea responds better to low frequency sounds.
Role of auditory fibers:
In response to stimulus, neurotransmitter is released in the synapses at the base of inner hair c
This gives rise to action potentials in the auditory nerve fibers. Single auditory nerve stimuli is
always excitatory and never inhibitory. This action potential is conveyed to the auditory centers
of brain by the auditory division of the 8 th nerve.
The following are the proposed theories of hearing:
Place theory of Helmontz - This theory proposes that frequency resolution occurs at the level
of basilar membrane. The various zones of basilar membrane are sensitive to different frequen
and this spatial relationship play a role in frequency resolution.
Telephone theory of Rutherford – This theory assumes that the whole cochlea responds as a w
to all the frequencies. This theory assumes that cochlea reacts to various frequencies like a
telephone cable.
Volley theory of weaver – This theory proposed by Wever assumes that several neurons acting
as a group can fire in response to the frequency to which they are sensitive to.
Place theory of Lawrence – Lawrence combined both volley and place theories to explain how
sounds are perceived.
Traveling wave theory of Bekesy – This theory assumes that frequency coding took place at the

8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 26/31
of cochlea.
Auditory center of brain is located at the superior gyrus of temporal lobe.
Functions of auditory center:
Sound localization and lateralization
Speech discrimination
Auditory performance with competing acoustic signals
Auditory performance with degraded signals.
I. Pure tone audiometry
Introduction:
This procedure is performed to measure the auditory threshold of an individual. The instrumen
used for this purpose is known as the audiometer.
Components of a pure tone audiometer:
Oscillator:
The function of an oscillator is to generate electronically standardized sound whose frequencie
within + / - 3% of their supposed value. The frequencies generated include: 125, 250,500, 750
1500, 2000, 3000, 4000, 6000 and 8000 Hz.
Interrupter switch:
This switch helps in turning on and off the sounds which are presented to the patient from the
oscillator. This is important because presenting a continuous tone to a patient may cause audi
decay causing problems with interpretation of results. This switch provides the option of prese
the sound in a continuous / interrupted manner.
Equalization circuit:
This circuit contains resistors which helps in equalization of the sound generated. This process
important because the threshold of human hearing is not uniform and it is very good for
frequencies around 2 kHz. Above and below this level the sensitivity of human hearing varies.
Output power amplifier:
The signals generated by the oscillator needs to be amplified. The vital feature of any power
amplifier is that it should have a good signal to noise ratio and should produce very little distorti
In most audiometers the power amplifier is run at constant high signal output levels.
Hearing level attenuator:
This controls the level of signal from the audiometer within a range of 110-120 dB. This attenua
can be varied in steps of 5 dB. The basic reference point is marked as “0”. This point technica
indicates -5 to -10 dB hearing threshold levels. The attenuator steps should be accurate.

8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 27/31
Output transducers:
These are of three types:
a. Ear phones
b. Bone vibrator
c. Loud speaker
The ear phones of an audiometer are real special. They cannot be changed / replaced without
recalibrating the whole equipment. A good ear phone should have long term stability, should h
flat frequency response, and should have the ability to deliver high output sounds.
Bone vibrators unlike ear phones has a limited frequency range. It cannot be used to reliably
record frequencies above 4 kHz because it wont vibrate beyond this range. At low frequencies
shows distortions and is incapable of transmitting high frequencies.
Loud speakers are used in free field audiometry.
Technique of measurement of hearing acuity:
Air conduction threshold of a patient is measured using ear phones. It can be measured from g
from an inaudible to an audible stimulus intensity. This is known as the ascending method of
evaluation of air conduction threshold. There is one other method that uses the descending m
of threshold estimation. In this method the air conduction threshold is assessed by going from
audible to inaudible signal intensity. The patient should be instructed to raise his / her index
finger even if the sound is mildly audible.
Care should be taken to ensure that the headphones are properly seated over the external
auditory canal, because patient's pinna may be in different shapes and sizes. Improper placem
of headphones will lead to threshold variations of 15 – 20 dB. Before placing the ear phones o
patient, wax free ear canal should be ensured because the presence of wax could cause a
discrepancy of about 30 dB. While plotting the values red color ink is used to plot results of
right ear and blue color is used to plot the results of left ear.

8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 28/31
Figure showing air conduction audiometry
Bone conduction audiometry: is usually performed by using a bone vibrator which is placed ove
the mastoid process. The opposite ear should be masked by using appropriate masking
stimulus. Auditory thresholds are estimated as done for air conduction audiometry. Usually
air conduction values should be better than bone conduction ones. If bone conduction value
is better than air conduction then the patient should be suffering from conductive deafness. In
sensorineural hearing losses both air and bone conduction curves will take a dip. This dip
will be pronounced for high frequencies.

8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 29/31
j. Leukoplakia
Introduction:
This is a clinical term used to indicate patches of keratosis seen over the mucous membrane
of oral cavity, palate, tongue etc. On gross appearance it is seen as adherent white patches
over the mucous membrane. It is considered to be a premalignant condition. Common in ciga
smokers.
Causative factors:
1. Tobacco chewing
2. Smoking
3. Ill fitting dentures
4. UV radiation
5. Presence of torus palatinus
6. Alcoholism
Gross appearance:
Leukoplakia begin as gray or grayish white plaques. They may appear somewhat translucent,
wrinkled, typically flat. Usually they are soft on palpation. Their borders are usually sharply
demarcated, sometimes gradually blending with the surrounding mucosa. When a leukoplakic
patch becomes red it is known as “erythroplakia” which is definitely a premalignant lesion.
Histology:
Histologically it is a thickened surface layer of parakeratin and sometimes orthokeratin. Basilar
and keratinocytes show no evidence of dysplasia. There may be mild basilar hyperplasia. If th
basilar cells and keratinocytes show evidence of dysplasia then it should be considered to be a
premalignant lesion.
Staging of leukoplakia:
Phase I leukoplakia – In this phase the leukoplakic patch appears rather thin. It is so thin that
the underlying mucosa can be clearly seen through it. This stage leukoplakia can undergo
spontaneous regression if the offending cause is removed.
Phase II leukoplakia – These patches are homogeneous, thick and sometimes fissured. A
leukoplakia can remain in this stage for ever or may progress to phase III.
Phase III leukoplakia – These patches are thick and have surface irregularities which could
be nodular. Hence it is also known as Nodular leukoplakia. Leukoplakia belonging to this phas
may turn dysplastic and become invasive.
Phase IV leukoplakia – This type is rather inhomogeneous. When it is reddish in color it is kno
erythroplakia. It also goes by the name speckled leukoplakia. This lesion may undergo malign
transformation.

8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 30/31
Short answer questions: 10x2=20
1. Mention two premalignant lesions of oral cavity
a. Leukoplakia
b. Erythroplakia
2. Mention any two tuning fork tests
a. Rinne test
b. Weber test
3. Mention any two clinical findings in nasal cavity of a patient suffering from allergic rhinitis
a. Pale boggy nasal mucosa
b. Mulberry shaped hypertrophy of inferior turbinate
4. Mention two important causes of sinusitis
5. Tracheostomy
This is an emergency procedure performed in order to secure the airway when the obstruction
is above the level of vocal folds and subglottic area. An opening is created in the anterior wall
of trachea ideally between the second and third tracheal rings. A tracheostomy tube is introduc
into the trachea through the opening.
6. Two absolute indications for tonsillectomy
a. Obstructive sleep apnoea syndrome
b. Failure to thrive due to excessive enlargement of adenoid and tonsils

8/8/2019 MGR Medical university prefinal ENT sep 2010 question paper with solution
http://slidepdf.com/reader/full/mgr-medical-university-prefinal-ent-sep-2010-question-paper-with-solution 31/31
7. Two causes of perichondritis pinna
a. Trauma
b. Frost bite
8. Four modalities of tonsillectomy
a. Dissection & snare method
b. Guillotine method
c. Laser tonsillectomy
d. Cryotonsillectomy
9. Two surgical approaches to maxillary sinus
a. Caldwel Luc procedure
b. Endoscopy guided middle meatal antrostomy
10. Tympanoplasty:
This is a surgical procedure that is preformed to remove disease from the middle ear cavity
and reconstruct the sound conducting mechanism. There are 5 types of tympanoplasty
procedures devised to reconstruct middle ear conduction system.
Type I tympanoplasty – Is myringoplasty which is performed if all the three ossicles are intact
Type II tympanoplasty – Is indicated when malleus is absent and the neotympanum is grafted
to the intact incus and stapes.
Type III tympanoplasty – Is indicated when the suprastructure of stapes alone is present and th
neotympanum is draped over the suprastructure
Type IV tympanoplasty – is indicated when the suprastructure also is eroded and the neotympa
is draped over the foot plate (columella effect)
Type V tympanoplasty – is fenestration of lateral canal