metastatik kastrasyona dirençli prostat...
TRANSCRIPT

Metastatik Kastrasyona Dirençli Prostat Kanseri
Mustafa ÖZGÜROĞLU İSTANBUL ÜNIVERSİTESİ
CERRAHPAŞA TIP FAKÜLTESİ MEDİKAL ONKOLOJİ
1

Prostat kanseri androjene bağımlıdır
Testosterone
LHRH
Pituitary
Cortisol Adrenal androgens
Prostate
Testes
Prolactin
Adrenal
Hypothalamus

Androjen-reseptör ilişkisi
Feldman BJ. Nature Rev Cancer 2001;1:34-44
AR: androgen receptor; T: testosterone; DHT: dihydrotestosterone
3

Kastrasyona Dirençli Prostat Kanseri
• Tedaviye rağmen, 12-18 ay içinde prostat
kanserli hastaların çoğunluğu androjen
ablasyonuna direnç geliştirmektedir.
4

“Despite regressions of great magnitude, it is obvious that there were many failures of endocrine therapy to control the disease.”
Charles B. Huggins
Nobel Lecture December 13, 1966
KDPK: aslında çok önceden
tanımlanmış bir sorun
Huggins C. Cancer Res. 1967;27:1925-1930.

6

KDPK :
Gerçekten androjenik etkiden bağımsız mı
hareket etmeye başlar???
ASLINDA HAYIR
Kastre düzeydeki testosterona rağmen androjene bağımlı
sinyaller kanser hücrelerini büyütür
KDPK olguları 2. seri hormonal tedavilere de bu nedenle
yanıt verir
Sharifi N, et al. J Investig Med. 2010;58:938-944. Dutt SS, et al. Future Oncol. 2009;5:1403-1413.

8
NOT REALLY TRUE

KDPK – olası mekanizmalar
Liganda bağımlı
• Persiste eden
androjen
• AR mutasyonu
• AR amplifikasyonu
Ligand’dan bağımsız
• AR sinyalizasyonuna
• Doğrudan androjen
reseptör değişiklikleri
• Chaperon üzerine etki
• AR transkripsiyonu üzerine
etki

Persiste eden androjen
10
Primer tümör ve
metastazların
mikroçevresinde
Kaynak
• Adrenal gland
• Prostat kanser hücresi
de novo otokrin sentez
CYP17 enzim sistemi-6 Prostate tumor cells
Adrenal gland
Testis
1. Nishiyama et al. Clin Cancer Res 2004;10:7121-26 2. Titus MA et al. Clin Cancer Res 2005;11:4653-7
3. Montgomery RB et al. Cancer Res 2008;68:4447-54
4. Stanbrough M et al. Cancer Res 2006;66:2815-25 5. Locke JA et al. Cancer Res 2008;68:6407-15 6. Vis AN et al. BJU Int 2009;17:3876-83

AR gen amplifikasyonu
1. Visakorpi T et al. Nature Genet 1995;9:401–406
2. Bubendorf L. Cancer Res 1999;59:803–6 3. Gregory CW et al. Cancer Res 2001;61:2892-8
11
KDPK li olguların %30
unda görülür
Bikalutamid direncinden
sorumludur
Nucleus
4. Kawata H et al. Prostate 2010;70:745-54 T: testosterone; SHBG: sex hormone binding globulin DHT: dihydrotestosterone; HSP: heat shock protein
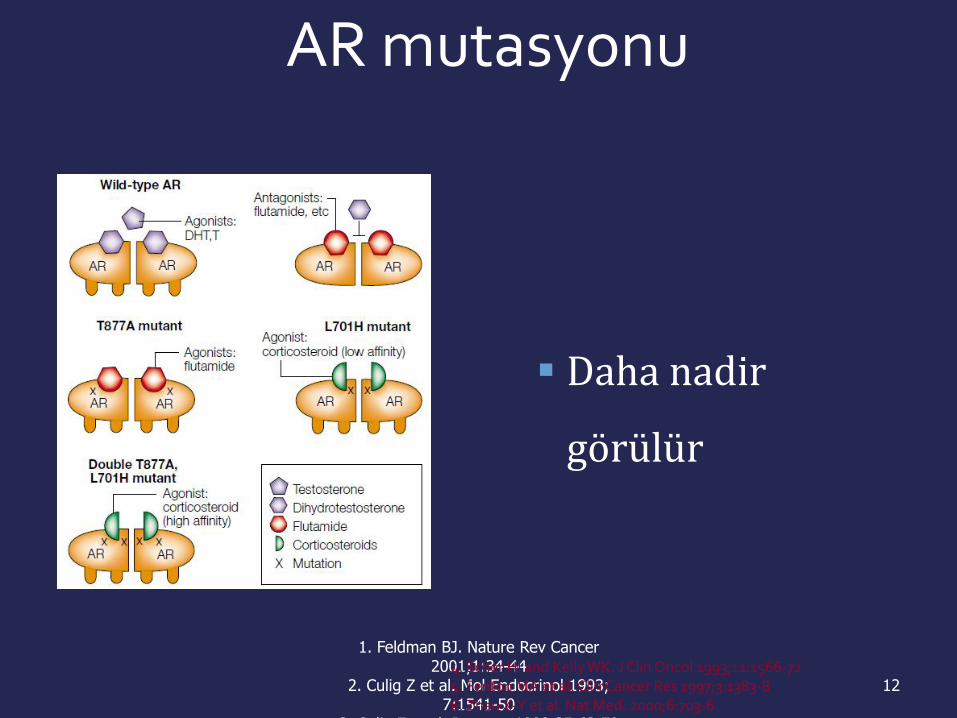
AR mutasyonu
1. Feldman BJ. Nature Rev Cancer 2001;1:34-44
2. Culig Z et al. Mol Endocrinol 1993; 7:1541-50
3. Culig Z et al. Prostate 1998;35:63-70
12
Daha nadir
görülür
4. Scher HI and Kelly WK. J Clin Oncol 1993;11:1566-72 5. Fenton MA et al. Clin Cancer Res 1997;3:1383-8 6. Zhao X-Y et al. Nat Med. 2000;6:703-6

HEDEFTEKİ ANDROJEN RESEPTÖR
AR: androgen receptor * Src activation, PI3K signaling
13
AR co-activators & co-repressors
AR splice variants
Epigenetic modifications
AR amplification
Persistent androgens
AR mutations
Tyrosine kinase signaling*
mCRPC
Ligand-dependent pathways
Ligand-independent pathways

Prostat kanserinde doğal seyir
Under the care of ONCOLOGIST
Under UROLOGIST care
Nonmetastatic Metastatic
Local therapy
Androgen deprivation
Therapies after LHRH agonists
and antiandrogens
First-line therapy
Salvage therapy
Death
Under ONCOLOGIST care
Higano C, et al. In: Figg WD, et al. Drug management of prostate cancer; 2010.
Burden of disease
Asymptomatic Symptomatic
Castrate sensitive Castrate resistant

Hastalığın progresyon süreleri
dönemlere göre farkldır
•
Castration-Resistant Prostate Cancer
M0 M1 Asymptomatic M1 Symptomatic
M0 M1 M1+
25-30 10-12 10-15
AY

KDPK’de standart tedavi yaklaşımı değişikliğe uğrayacak mı?
Standart yaklaşım
•İkincil hormonal manipulasyonlar
– AA kesilme yanıtına bakılması
– Ketokanazol
KEMOTERAPİ
16

KDPK’ de kemoterapinin tarihçesi ve
sağkalım
Eisenberger MA, et al. J Clin Oncol. 1985;3:827-841.
SA
ĞK
AL
IM
ola
sılığ
ı
HAFTA
0.2
0.4
0.6
0.8
1.0
0 0 20 40 60 80 100
Median SK: ~ 8.5 ay
20 randomize çalışmadaki sağkalım eğrileri

KDPK ilaç gelişimi çok yavaş olmuştur
• Pre- 2004-Mitoksantron katkısı yok
• 2004- Docetaksel – metilprednizolon
• sağkalım avantajı
• 2010 yılına kadar yeni ilaç yok
18

19

Semptomlu HDPK tedavisinde
Mitoksantron/prednizon vs prednizon (n=161)
Sağkalım farkı yok
Ağrı üzerine etkili
Tannock et al. J Clin Oncol 1996;14:1756–1764
Prednizon
% 12 olgu
Mitoksantron/prednizon
% 29 olgu
Palyasyon
Palyasyon yok

2004: İlk defa docetaxel ile sağkalım avantajı
SWOG 9916
• Docetaxel and estramustine compared with mitoxantrone and prednisone for advanced refractory prostate cancer. Petrylak, et al
TAX 327
• Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. Tannock, et al
21
Issue 351, October 2004

TAX 327: genel sağkalım
22
Median
survival Hazard
D q3w: 18.9 0.76 0.009
D weekly 17.3 0.91 0.36
Mitoxantrone: 16.4 — —
Months 0 6 12 18 24 30
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8
0.9 1.0 Docetaxel q3w
Docetaxel weekly
Mitoxantrone
Pro
ba
bili
ty o
f su
rviv
ing
Tannock et al. N Engl J Med 2004;351:1502 1512
2.5 AY

SWOG 9916: genel sağkalım
23
0
20
40
60
80
100
0 12 24 36 48
Time (months)
Docetaxel/estramustine
Mitoxantrone/prednisone
No. at
risk
338
336
No. of
deaths
217
235
Median
(months)
17.5
15.6
HR: 0.80 (95% CI: 0.67–0.97); p=0.02
Surv
ival (%
)
Petrylak et al. N Engl J Med 2004;351:1515 1520
1.9 AY

24

2010 yılına kadar yeni ilaç yok
25

2010 -2013 yılı prostat kanseri için altın yıllar
6 YENİ İLACA ONAY
– Sipuleucel T2
– Cabazitaxel3
– Abiraterone1
– Enzalutamide
– Denosumab
– Radyum 223
26
1. de Bono J et al; ESMO 2010; 2. Kantoff et al, NEJM 2010;
3. de Bono et al, The Lancet 2010.

DOCETAKSEL ÖNCESİ
METASTATİK KDPK 1. BASAMAK TEDAVİ
27

Patient’s white blood cells harvested
Short-term culture with protein “cassette”
Shipping
Cells infused back into patient (IV)
GM-CSF
Prostatic acid phosphatase
Aktif Hücresel
İmmunoterapi(Sipuleucel-T)

29
Sipuleucel-T (Provenge)
1. day
leukopheresis 2.- 3. days
sipuleucel-T
production
3.-4. days
Infused to the pt
Apheresis center Physician office
Treatment period
Weeks 0, 2, 4

30
Faz III IMPACT çalışması
Primary endpoint: SURVIVAL
Asymptomatic
metastatic
CRPC
(N=512)
Pre-
Chemotherapy Placebo
Q 2 weeks
x 3
Sipuleucel-
T
Q 2 w eeks
x 3
P
R
O
G
R
E
S
S
I
V
E
2:1
S
U
R
V
I
V
A
L
Salvage
regimen Placebo
Q 2 weeks
x 3
ANY TX

31
IMPACT: Genel Sağkalım
0 6 1 2 1 8 2 4 3 0 3 6 4 2 4 8 5 4 6 0 6 6 0
2 5
5 0
7 5
1 0 0
Perc
ent S
urv
iva
l
Survival (months)
P = 0.032 (Cox model)
HR = 0.775 [95% CI: 0.614, 0.979]
Sipuleucel-T (n = 341)
Median sağkalım
25.8 ay Placebo (n = 171)
Median survival: 21.7 ay
Kantoff PW, et al. N Engl J Med. 2010;363:411-422. .
4. 1 AY

ABİRATERON 1. BASAMAK
DOCETAXEL ÖNCESİ FDA ONAYI ALMIŞTIR-
ARALIK 2012
32

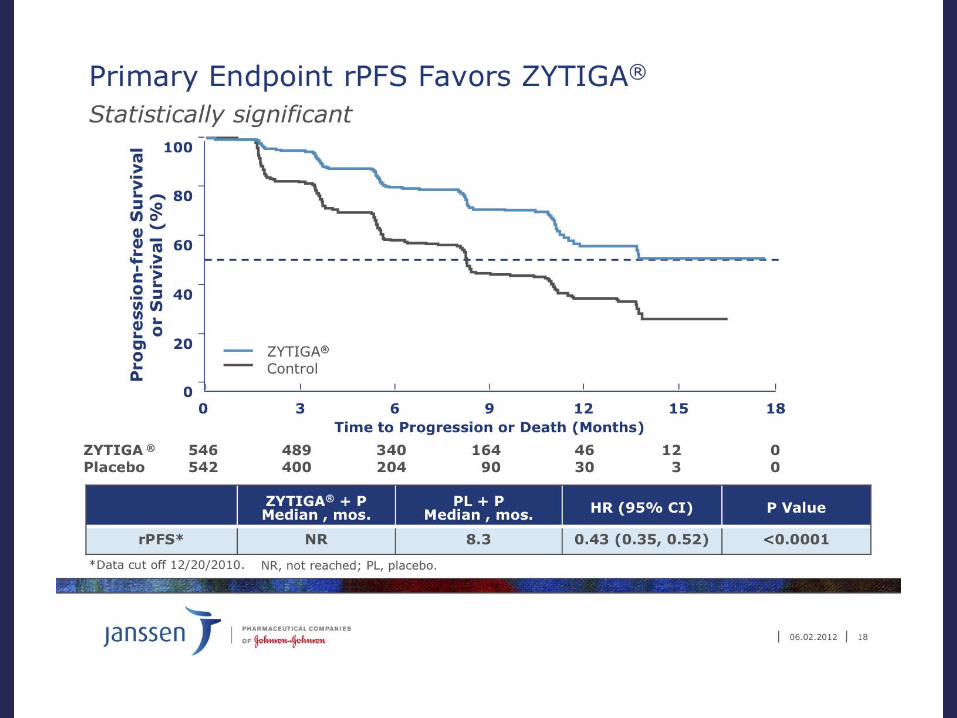
COU-AA-302
• Stratification by ECOG performance status 0 vs 1
Ryan CJ et al. Proc ASCO 2012;Abstract LBA4518.
R
Patients
•Progressive chemo-
naïve mCRPC patients
(Planned N = 1,088)
•Asymptomatic or mildly
symptomatic
1:1
Co-Primary:
• rPFS by central review
• OS
Secondary:
• Time to opiate use (cancer-related pain)
• Time to initiation of chemotherapy
• Time to ECOG-PS deterioration
• TTPP
Efficacy endpoints
AA 1,000 mg daily
Prednisone 5 mg BID
(Actual n = 546)
Placebo daily
Prednisone 5 mg BID
(Actual n = 542)

Interim Analysis (IA) Results of COU-AA-302, a Randomized, Phase 3 Study of Abiraterone Acetate (AA) in Chemotherapy-naïve Patients (pts) with Metastatic Castration-resistant Prostate Cancer (mCRPC)
CJ Ryan,1 MR Smith,2 JS de Bono,3 A Molina,4 C Logothetis,5 P De Souza,6 K Fizazi,7 P Mainwaring,8 JR Piulats,9 S Ng,10 J Carles,11
PFA Mulders,12 T Kheoh4, T Griffin4, EJ Small,1 HI Scher,13 D Rathkopf,13 on behalf of the COU-AA-302 investigators
34
/tmp/PreviewPasteboardItems/FINAL_ZYTIGA_Webcast_Update_6-4-
2012 (dragged) 1.pdf
35

36

KDPK ‘de dosetaksel sonrası tedavi seçenekleri
• CABAZİTAKSEL
• ABİRATERON
• ENZALUTAMİDE
• ALFARADİN
37

TROPIC Çalışması
CABAZITAKSEL:
38
Ref: ClinicalTrials.gov Identifier: NCT00417079

Metastatik KDPK XRP6258
TROPIC TRAİL
39
PRİMER SONLANIM: SAĞKALIM
Cabazitaxel 25 mg/m² IV q3w 1 Prednisone 10 mg/day
oral 10 cycles
360 pts
360 pts
Docetaxel
failure
CRPC
Mitoxantrone 12 mg/m² IV q3w
Prednisone 10 mg/day oral
10 cycles
R
A
N
D
O
M
I
Z
E Stratification factors: Measurable vs non-measurable ECOG 0-1 vs. 2
progression ex
O OO
O
OCOCH3
OCOC6H
5
HOH
O
O
OH
NH
O
O
CH3
CH3
XRP6258

De BONO J , OUDARD S, OZGUROGLU M et al. Lancet, 2010, 376:1147-54

genel sağkalım avantajı
41
MP 377 300 188 67 11 1
CBZP
378 321 231 90 28 4
Number at risk
Proportion of OS (%)
80
60
40
20
0
100
0 months 6 months 12 months 18 months 24 months 30 months
15.1 12.7 Median OS (AY)
0.59–0.83 95% CI <.0001 P-value
0.70 Hazard Ratio
CBZP MP
2.4 AY

Progresyonsuz sağkalım(PFS)
42
Number at risk
Proportion of PFS (%)
80
60
40
20
0
100
0 months 3 months 9 months 15 months 18 months 21 months 6 months 12 months
PFS composite endpoint: PSA progression, pain progression, tumor progression, symptom deterioration, or death.
2.8 1.4 Median PFS (months)
0.64–0.86 95% CI <.0001 P-value
0.74 Hazard Ratio
CBZP MP
MP 377 115 52 27 9 6 4 2
CBZP
378 168 90 52 15 4 0 0

Tüm alt gruplarda sağkalı m avantajı
43
Factors Hazard ratio
(95% CI)
f a v o r s C B Z P | f
a v o r s M P
Tüm hastalar 0.70 (0.59–0.83)
ECOG status: 0,1 0.68 (0.57–0.82)
ECOG status: 2 0.81 (0.48–1.38)
Measurable disease: No 0.72 (0.55–0.93)
Measurable disease: Yes 0.68 (0.54–0.85)
No. of prior chemo: 1 0.67 (0.55–0.83)
No. of prior chemo: ≥2 0.75 (0.55–1.02)
Age: <65 0.81 (0.61–1.08)
Age: ≥65 0.62 (0.50–0.78)
Rising PSA: No 0.88 (0.61–1.26)
Rising PSA: Yes 0.65 (0.53–0.80)
Total docetaxel dose: <225 mg/m² 0.96 (0.49–1.86)
Total docetaxel dose: ≥225 to 450 mg/m²
0.60 (0.43–0.84)
Total docetaxel dose: ≥450 to 675 mg/m²
0.83 (0.60–1.16)
Total docetaxel dose: ≥675 to 900 mg/m²
0.73 (0.48–1.10)
Total docetaxel dose: ≥900 mg/m² 0.51 (0.33–0.79)
Progression: During last docetaxel treatment
0.65 (0.47–0.90)
Progression: <3 months since last docetaxel dose
0.70 (0.55–0.91)
Progression: ≥3 months since last docetaxel dose
0.75 (0.51–1.11)
0 1 2 0.5 1.5
0 1 2 0.5 1.5

Yan etki profili: >grade 3
44
MP (n=371) CBZP (n=371)
ALL GRADES(%)
GRADE ≥3 (%)
ALL GRADES(%)
GRADES ≥3 (%)
ANY SIDE EFFECT 88.4 39.4 95.7 57.4
Febrile
neutropenia
1.3 1.3 7.5 7.5
Diarrhea 10.5 0.3 46.6 6.2
Fatigue 27.5 3 36.7 4.9
Asthenia 12.4 2.4 20.5 4.6
Back pain 12.1 3 16.2 3.8
Nausea 22.9 0.3 34.2 1.9
Vomiting 10.2 0 22.6 1.9
Hematüria 3.8 0.5 16.7 1.9
Abdominal pain 3.5 0 11.6 1.9

TROPIC ÖZETİ
• CABAZITAKSEL:
• Mitoksantrona sağkalım avantajı
– 30% risk azalması (HR = 0.70, P <.0001)
– Median sağkalım CBZP vs mitok: 15.1 ay vs 12.7
ay
– en sık gözlenen yan etki
• Nötropeni, ishal, yorgunluk ve asteni,
45

46
Cabazitaxel : diğer sorular
•
•Hangi doz 25 vs 20 ?
– PROSELICA
•1. BASAMAKTA ETKİLİ Mİ ?
–FIRSTANA çalışması
•
ENZALUTAMİDE RADIUM 223
ABİRATERONE
47

Androjenik sinyal aksını inhibe ederler
Androgen
Biosynthesis
Inhibitors (ABI):
Ketoconazole
Abiraterone
TAK700 Second generation
AR inhibitors (ARI):
Enzalutamide
(MDV3100)
ARN509
ABI
ARI
Reprinted from Chen Y, et al. Lancet Oncology. 2009;10:981-991; with permission from Elsevier.

49
Abiraterone: lyase inhibitor The Institute of Cancer Research, Sutton
Barrie et al, 1994; Potter et al 1995; Rowlands et al, 1995

Abiraterone Acetate:
ANDROJEN BİYOSENTEZ
İNHİBİTÖRÜ
– Testis
– Adrenal
– Prostat kanser hücreleri
50 50
1. Attard G et al, J Clin Oncol, 2008; 2. Attard G et al. J Clin Oncol. 2009; 3. Reid AH et al. J
Clin Oncol. 2010;
4. Ryan C et al, J Clin Oncol, 2009; 5. Danila D et al, J Clin Oncol, 2010.

Abiraterone: Etki mekanizması
ACTH
Pregnenolone Deoxycorticosterone Corticosterone Aldosterone
Cortisol 11-deoxycortisol 17OH-Progesterone 17OH-Pregnenolone
CYP17: 17α-hydroxylase
CYP17: C17,20-lyase
DHEA Androstenedione
Testosterone
Estradiol
Negative feedback
Hypokalemia
Hypertension
Fluid overload
Positive drive
x 5
x 10 x 40 x 1.5
x 3
x 3
x 4 x 2
< 2 ng/dL
< 1 ng/dL
< 80 ng/dL
Attard G, et al. J Clin Oncol. 2008;26:4563-4571.
Suppression of renin

52
COU-AA-301 Trial
52
Abiraterone 1000 mg daily
Prednisone 5 mg BID
N=797
Primary end point:
•OS (25% improvement; HR
0.8)
Secondary end points (ITT):
•TTPP
• rPFS
•PSA response
Efficacy endpoints (ITT)
Placebo daily
Prednisone 5 mg BID
n=398
R A N D O M I Z E D
2:1
•1195 patients with
progressive, mCRPC
•Failed 1 or
2 chemotherapy
regimens, one of
which contained
docetaxel
Patients
Clinicaltrials.gov identifier: NCT00638690. Chief Investigators: de Bono & Scher.


54
COU-AA-301: GENEL SAĞKALIM AVANTAJI
54
0 100 200 300 400 500 600 700
0
20
40
60
80
100
Surv
ival
(%)
Days from Randomization
3.9 ay
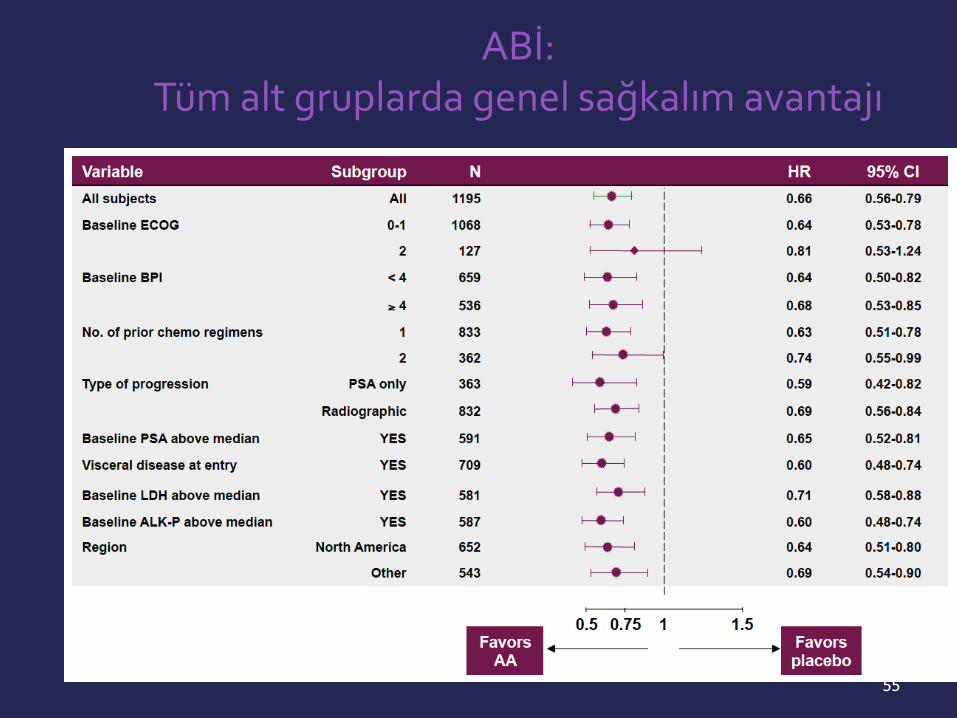
55
ABİ: Tüm alt gruplarda genel sağkalım avantajı

COU-AA-301: Yan etki profili
Overall incidence of AEs similar between arms
– Slight increase in fluid retention, hypokalemia, and cardiac disorders
observed with abiraterone acetate, but events primarily
mild/moderate in severity
Treatment-Related AEs, % Abiraterone Acetate
(n = 791)
Placebo
(n = 394)
All Grades Grade 3/4 All Grades Grade 3/4
All treatment-related AEs 99 55 99 58
Fluid retention 31 2 22 1
Hypokalemia 17 3 8 1
Cardiac disorders* 13 3 11 2
Hypertension 10 1 8 < 1
LFT abnormalities 10 3 8 3
de Bono JS, et al. N Eng J Med. 2011;364:1995-2005. Scher HI, et al. ASCO GU 2011. Abstract 4.
*Most frequent cardiac disorders were tachycardia and atrial fibrillation.

AR
T
Metastatik prostat kanserinde
ENZALUTAMIDE
MDV3100: novel, oral AR
antagonist
Testesteronun AR üne
bağlanmasını önler
Nükleer translokasyonu önler
DNAya bağlanmasını önler
1. Higano CS, et al. ASCO GU 2011. Abstract 134. 2. Scher HI, et al. Lancet. 2010;375:1437-1446.
Testosterone synthesis
Tumor death Testosterone
MDV3100
No prednisone
required
AR binding blocked
Nuclear translocation impaired
Cell nucleus
DNA binding and activation blocked
T
X X
X 3
2
1

ENZALUTAMİD –AR sinyalizasyon kaskadında birden fazla basamakta inhibisyona neden olur
Mukherji D et al. Expert Opin Investig Drugs 2012;21:227-33. Carson C et al. Urology 2003;61:2-7.
Testosterone/DHT Enzalutamide

Enzalutamid
Enzalutamid bir AR sinyalizasyon inhibitörüdür ve AR sinyalizasyonunu
üç farklı yoldan inhibe eder:
DHT
1. AR bağlanmasını bloke eder
3. DNA bağlanmayı aktibloke eder
Enzalutamid Enzalutamid AR
Sitoplazma Nükleus
2. Nükleer translokasyonu bozar
Enzalutamid
Tran et al. Science 2009;324:787–90; Watson et al. Proc Natl Acad Sci USA 2010;107:16759–65.
AR, androjen reseptörü; DHT, dihidrotestosteron
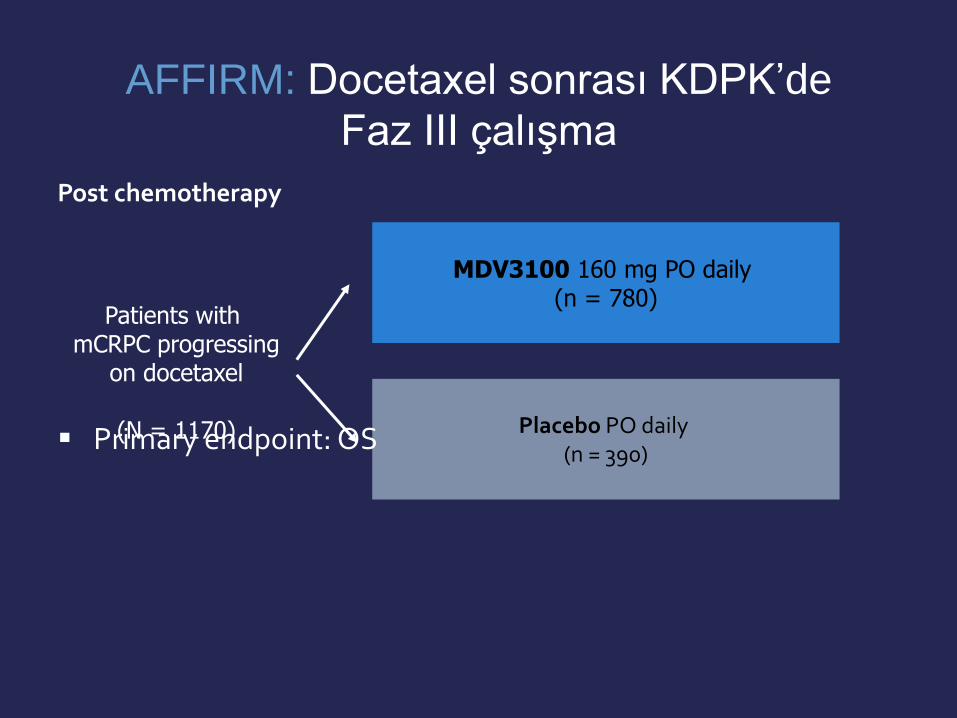
Placebo PO daily (n = 390)
MDV3100 160 mg PO daily (n = 780)
Patients with mCRPC progressing
on docetaxel
(N = 1170)
AFFIRM: Docetaxel sonrası KDPK’de
Faz III çalışma
Post chemotherapy
Primary endpoint: OS

AFFIRM çalışma dizaynı
• Primer sonlanım noktası: Genel sağkalım
• Tabakalama değişkenleri: – ECOG performans skoru (0–1’e karşı 2)
– Ortalama Kısa Ağrı Envanteri Soru#3 skoru(<4, ≥ 4)
Scher et al, Increased Survival with Enzalutamide in Prostate Cancer after Chemotherapy, N Engl J Med. 2012 Sep 27; 367(13): 1187-97. Epub 2012 Aug 15.
ECOG, Eastern Cooperative Oncology Group; HR, hazard ratio

AFFIRM: Başlangıç hasta özellikleri
Scher et al, Increased Survival with Enzalutamide in Prostate Cancer after Chemotherapy, N Engl J Med. 2012 Sep 27; 367(13): 1187-97. Epub 2012 Aug 15.
Enzalutamid (n = 800)
Plasebo (n = 399)
Yaş, medyan yaş (aralık) 69
(41−92) 69
(49−89)
ECOG performans skoru 2, n (%) 70 (8.8) 32 (8.0)
Ortalama Kısa Ağrı Envanteri skoru ≥4 soru 3 için, n (%)
226 (28.3) 115 (28.8)
Kemik hastalığı, n (%) 735 (92.2) 364 (91.5)
Yumuşak doku hastalığı, n (%) 567 (70.9) 275 (68.9)
Visseral karaciğer hastalığı, n (%) 92 (11.6) 34 (8.5)
Visseral akciğer hastalığı, n (%) 122 (15.4) 59 (14.8)
ECOG, Eastern Cooperative Oncology Group

AFFIRM: Önceki hormonal ve kemoterapi tedavileri
Enzalutamid (n = 800)
Plasebo (n = 399)
Önceki hormonal tedavi serilerinin sayısı, % 1 2 ≥ 3
8.2
42.3 49.1
8.8
37.9 53.1
Önceki KT serilerinin sayısı, % 1 2 ≥ 3
72.4 24.5 3.1
74.2 23.8 2.0
Önceki medyan dosetaksel siklus sayısı, n 8.5 8.0
Scher et al, Increased Survival with Enzalutamide in Prostate Cancer after Chemotherapy, N Engl J Med. 2012 Sep 27; 367(13): 1187-97. Epub 2012 Aug 15.
De Bono et al. Oral presentation at ASCO 48th Annual Meeting; Chicago, IL, 1–5 June, 2012.

AFFIRM: genel sağkalım avantajı
0
10
20
30
40
50
60
70
80
90
100 S
urv
ival
(%
)
Enzalutamide: 18.4 mos (95% CI: 17.3-NYR)
Placebo: 13.6 mos (95% CI: 11.3-15.8)
HR: 0.631 (95% CI: 0.529-0.752; P < .001) 37% reduction in risk of death
Scher HI, et al. ASCO GU 2012. Abstract LBA1.
0 3 6 9 12 Duration of OS (Mos)
15 18 21 24
800 399
775 376
701 317
627 263
400 167
211 81
72 33
7 3
0 0
Enzalutamide Placebo

Scher et al,, N Engl J Med. 2012 Sep 27; 367(13): 1187-97. Epub 2012 Aug 15.
Radyografik progresyonsuz sağkalım
Enzalutamid, n = 800 583 447 287 140 58 13 1 0
Plasebo, n = 399 176 86 46 20 7 3 0 0
rPFS yumuşak doku için RECIST 1.1 ve kemik hastalığı için Prostat Kanseri Çalışma Grubu (PCWG2) göre tanımlanmıştır.
0 0
10
20
30
40
50
60
70
80
90
100
3 6 9 12 15 18 21 24
Sağk
alım
(%
)
Genel sağkalım süresi (ay)
plasebo: 2.9 ay (%95 GA: 2.8−3.4)
Enzalutamid: 8.3 ay (%95 GA: 8.2−9.1)
HR = 0.40 (%95 GA: 0.35−0.47) p<0.0001
GA, güven aralığı HR, hazard ratio
Risk altındaki hasta sayısı:

Enzalutamid : tüm alt gruplarda sağkalım avantajı
Altgrup Ölüm için Hazard ratio (%95 GA)
Medyan OS (ay) Enzalutamid/plasebo
Tüm hastalar 0.63 (0.53–0.75) 18.4/13.6
Yaş < 65 ≥ 65
0.63 (0.46–0.87) 0.63 (0.51–0.78)
–/12.4
18.4/13.9
Başlangıç ECOG performans skoru 0–1 2
0.62 (0.52–0.75) 0.65 (0.39–1.07)
–/14.2
10.5/7.2
Başlangıç ortalama ağrı skoru (BPI-SF soru 3) < 4 ≥ 4
0.59 (0.47–0.74) 0.71 (0.54–0.94)
–/16.2
12.4/9.1
Coğrafi bölge Kuzey Amerika Diğer
0.63 (0.47–0.83) 0.64 (0.51–0.80)
17.4/12.3
–/14.4
Önceki KT serilerinin sayısı 1 ≥ 2
0.59 (0.48–0.73) 0.74 (0.54–1.03)
–/14.2
15.9/12.3
Çalışmaya girişte progresyonun tipi Tek başına PSA progresyonu Radyografik progresyon PSA progresynu
0.62 (0.46–0.83) 0.64 (0.52–0.80)
–/19.5
17.3/13.0
Başlangıç değeri > medyan PSA LDH
0.62 (0.50–0.78) 0.61 (0.50–0.76)
15.3/10.3 12.4/8.5
Scher et al,, N Engl J Med. 2012 Sep 27; 367(13): 1187-97. Epub 2012 Aug 15.
0 0.5 1.0 1.5 2.0
Enzalutamid lehine Plasebo lehine
Dairelerin büyüklüğü altgrupların büyüklüğü ile orantılıdır.
BPI-SF, Kısa Ağrı Envanteri – Kısa Form; GA, güven aralığı; ECOG, Eastern Cooperative Oncology Group; LDH, laktat dehidrojenaz; PSA, Prostat-spesifik antijen

Advers olaylar, n (%)
Toplam olaylar (tüm gradeler) Grade ≥ 3 olay
Enzalutamid (n = 800)
Plasebo (n = 399)
Enzalutamid (n = 800)
Plasebo (n = 399)
yorgunluk 269 (34) 116 (29) 50 (6) 29 (7)
Diyare 171 (21) 70 (18) 9 (1) 1 (<1)
Sıcak basması 162 (20) 41 (10) 0 0
Kas-iskelet ağrıları 109 (14) 40 (10) 8 (1) 1 (<1)
Baş ağrısı 93 (12) 22 (6) 6 (<1) 0
Scher et al,, N Engl J Med. 2012 Sep 27; 367(13): 1187-97. Epub 2012 Aug 15.
*Bu kategoriye Enzalutamid grubunda hastaların >%10’undan oluşan ve plasebo grubuna göre en az %2 daha yüksek olan advers olaylar dahil edilmiştir .
AFFIRM: enzalutamid ile en yaygın olarak görülen advers olaylar*

• PREVAIL bir faz III randomize, çift kör, plasebo kontrollü çalışmadır.
• İki primer sonlanım noktası: OS ve PFS
mKDPK hastalarında kemoterapi öncesi enzalutamidin devam eden çalışmaları
n = 1680 ADT sonrası mKDPK asemptomatik veya hafif semptomatik
progresyon
• TERRAIN bir faz II randomize, çift kör etkililik ve güvenlilik çalışmasıdır. Bikalutamide karşı Enzalutamid
• Primer sonlanım noktası : PFS
n = 370 Başarısız LHRH sonrası mKDPK veya bilateral
orşiektomi
R
Enzalutamid 160 mg qd
Bikalutamid 50 mg qd
TERRAIN2 PREVAIL1 (AB’de çalışmaya hasta alımı tamalanmıştır)
R
Enzalutamid 160 mg qd
Plasebo qd
ADT, androjen deprivasyon tedavisi; LHRH, luteinizan hormon releasing hormon; mKDPK, metastatik kastrasyona dirençli prostat kanseri; OS, genel sağkalım; PFS, progresyonsuz sağkalım R, randomizasyon; qd, günde bir kez
1. http://clinicaltrials.gov/ct2/show/NCT01212991 2. https://webcasts.trentt.com/emuc2011/poster/3
7194/MDV10034_3004_EMUC.pdf

ENZALUTAMİD Özeti
•KDPK’de androjen reseptörü önemli bir hedeftir
•Enzalutamid faz III çalışmasında (AFFIRM) plaseboya
göre:
– Genel sağkalımı anlamlı derecede uzatmıştır
• Medyan artış 4.8 ay (HR = 0.63; p<0.0001)
KDPK, Kastrasyona dirençli prostat kanseri

Range of alpha-particle
Radium-223
Bone surface
Parker C, et al. ECCO/ESMO/ESTRO 2011. Abstract 1LBA
ALFARADİN: YENİ BİR RADYOİZOTOP
• alfa- partiküller:
– ÇİFT SARMAL DNA kırıklarına neden olur

70
80
90
27
100
60
50
40
30
20
10
0
Months
0 3 6 9 12 15 18 21 24
Ove
rall
Su
rviv
al (
%)
ALSYMPCA: SAĞKALIMI plaseboya kıyasla uzatmaktadır
Radium-223 PBO
Median OS (months) 14.0 11.2
Hazard ratio 0.695
95% CI 0.552–0.874
P value = 0.00185
placebo (PBO, n=268)
radium-223 (n=541)

DENOSUMAB ÇALIŞMALARI
KEMİK ÜZERİNE ETKİLİ AJAN
72

OPG / RANKL / RANK Reseptörü
• RANKL osteoblast ve kemik illiği stromal hücreleri tarafından salınır
• RANKL osteoklastı aktive ederek apoptozu engeller
OPG
Osteoclast Precursor
Bone
Osteoblasts
Osteoclast
RANK Ligand
RANK
Hormones Cytokines
RANK
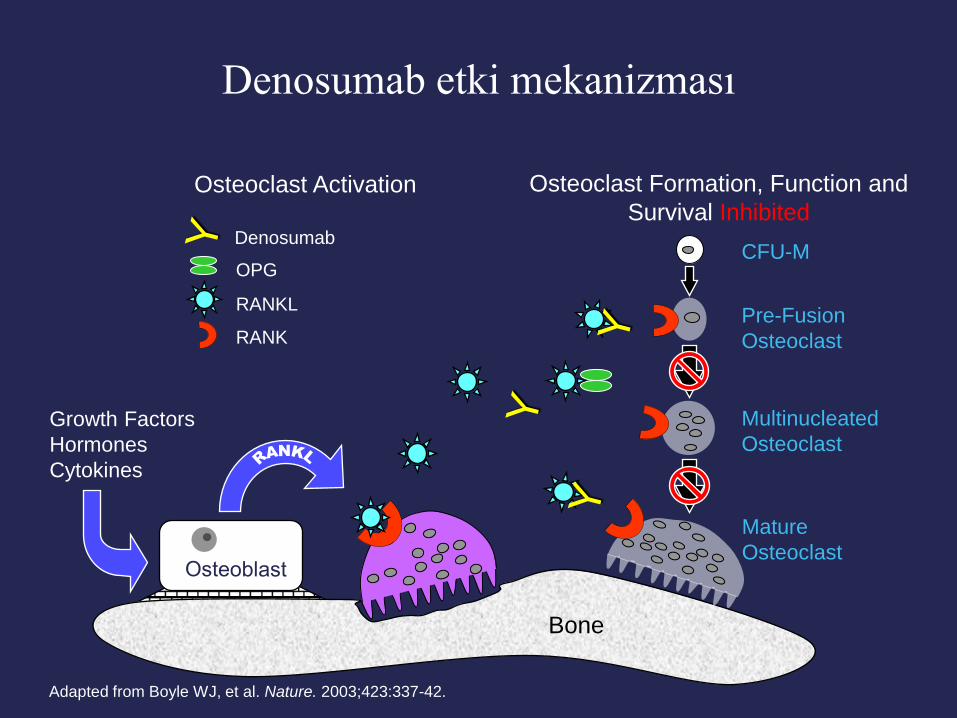
Denosumab etki mekanizması
Osteoclast Formation, Function and
Survival Inhibited Osteoclast Activation
Adapted from Boyle WJ, et al. Nature. 2003;423:337-42.
Mature
Osteoclast
CFU-M
Pre-Fusion
Osteoclast
Multinucleated
Osteoclast
Growth Factors
Hormones
Cytokines
RANK
RANKL
OPG
Bone
Denosumab

Denosumab 120 mg SC + Placebo IV q4w
(n = 950)
Zoledronic Acid 4 mg IV + Placebo SC q4w
(n = 951)
Patients with CRPC and bone metastases, no current or previous
IV treatment with bisphosphonate
(N = 1901)
Denosumab vs Zoledronic Acid
SRE önlenmesinde
Fizazi K, et al. Lancet. 2011;377:813-822.
Primary endpoint SREs: fracture, radiation or surgery to bone,
spinal cord compression

Zoledronic acid 951 733 544 407 299 207 140 93 64 47
Denosumab 950 758 582 472 361 259 168 115 70 39
Pts at Risk, N
0
1.00
Pro
po
rtio
n o
f Su
bje
cts
Wit
ho
ut
SR
E
0 3 6 9 12 15 18 21 24 27
0.25
0.50
0.75
KM Estimate of Median Mos
Denosumab
Zoledronic acid
20.7
17.1
HR: 0.82 (95% CI: 0.71-0.95; P = .0002 noninferiority; P = .008 superiority)
Study Mo
18% Risk
reduction
Time to First On-Study Skeletal-Related Event
Fizazi K, et al. Lancet. 2011;377:813-822.
Reprinted from The Lancet with permission from Elsevier. www.sciencedirect.com/science/journal/01406736
Denosumab vs Zoledronic Acid:
İlk SRE gelişene kadar

Metastazın geciktirilmesinde
Denosumab
Denosumab 60 mg monthly Patients with castrate-resistant prostate cancer and no bone
metastases; PSA > 8 or PSADT < 10 mos
(N = 1435)
Placebo monthly
ClinicalTrials.gov. NCT00286091. Smith MR, et al. 2011 AUA Annual Meeting. Plenary.

Smith MR, et al. 2011. AUA Annual Meeting. Plenary.
Primer sonlanım:
Kemikte metastazsız sağkalım
Placebo 716 691 569 500 421 375 345 300 259 215 168 137 99 60 36
Denosumab 716 695 605 521 456 400 368 324 279 228 185 153 111 59 35
Pro
port
ion o
f Patients
With
Bone M
eta
stasi
s–Fre
e S
urv
ival
HR: 0.85 (95% CI: 0.73-0.98; P = .028)
Median Mos
25.2
29.5 Placebo Denosumab
Study Mo
0
0.2
0.4
0.6
0.8
1.0
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42
Patients at Risk, n

KDPK : KEMOTERAPİ ÖNCESİ
FDA onayı alanlar
– Leuprolide
– Goserelin
– Bicalutamide
– Flutamide
– Ketoconazole
– Alpharadin
– Sipuleucel-T (2010)
– Abirateron 2012
Çalışmaları devam eden
– Enzalutamide
– Ipilimumab
– Orteronel (TAK700)
– Cabozantinib

KDPK: 1. basamak kemoterapi
Onay almış
– Docetaxel
– Mitoxantrone*
– Bisphosphonates*
– RT*
Devam eden çalışmalar
(docetaxel) ile kombine
– Aflibercept (VEGF-Trap)
– Dasatinib
– Ipilimumab
– Lenalidomide
– CABAZİTAXEL

KDPK: 2. basamak tedavi
Onay almış
– Docetaxel
– Mitoxantrone*
– Cabazitaxel (2010)
– Abiraterone (2011)
– enzalutamid
– alfaradin
Devam eden
– Orteronel (TAK-700)
– Ipilimumab
– Cabozantinib
– Ixabepilone

1984-1989
KDPK TEDAVİ ÖZETİ
1. The Leuprolide Study Group. N Engl J Med. 1984;311:1281-1286. 2. Crawford ED, et al. N Engl J Med. 1989;321:419-424. 3. Tannock IF, et al. J Clin Oncol. 1996;14:1756-1764. 4. Saad F, et al. J Natl Cancer Inst. 2002;94:1458-1468. 5. Petrylak DP, et al. N Engl J Med. 2004;351:1513-1520. 6. Tannock IF, et al. N Engl J Med. 2004;351:1502-1512. 7. de Bono JS, et al. Lancet. 2010;376:1147-1154. 8. Kantoff PW, et al. N Engl J Med. 2010;363:411-422. 9. Fizazi K, et al. Lancet. 2011;377:813-822. 10. de Bono JS, et al. N Engl J Med. 2011;364:1995-2005. 11. Scher HI, et al. ASCO GU 2012. Abstract LBA1. 12. Parker C, et al. ASCO GU 2012. Abstract 8.
1996 2002 2004 .... 2010 2011
Mitoxantrone[3] Docetaxel*[5,6]
Sipuleucel-T*[8]
LHRH agonists*[1,2]
Abiraterone*[10]
Reversible AR blockers[1,2]
Cabazitaxel*[7] Denosumab[9] Zoledronic Acid[4]
MDV3100[11]
Radium-223[12]
* Approved agent for PCa

YENİ AJANLARIN ÖZETİ
Trial Regimen Pts HR N Survival
(months) Delta
(months)
IMPACT1 Sipuleucel-T CRPC 0.78 512 25.8 vs 21.7 4.1
TAX 3272 Docetaxel+Prednisone vs Mitoxantrone+Prednisone
CRPC Chemonaive
0.76 1006 18.9 vs 16.5 2.4
TROPIC3 Cabazitaxel+Prednisone vs Mitoxantrone+Prednisone
CRPC Post-docetaxel
0.70 755 15.1 vs 12.7 2.4
COU-AA-3014 Abiraterone +Prednisone vs Prednisone
CRPC Post-docetaxel
0.74 1195 15.8 vs 11.2 4.6
ALSYMCA5 Alpharadin vs Placebo
CRPC 0.695 809 14.0 vs 11.2 3.6
AFFIRM6 MDV3100 vs Placebo
CRPC Post-docetaxel
0.63 1199 18.4 vs 13.6 4.8
83
1. Kantoff PW et al. N Engl J Med 2010;363:411-22. 2. Tannock IF et al. N Engl J Med 2004;351:1502-12. 3. de Bono JS et al. Lancet 2010;376:1147-54.
4. Fizazi K et al. Lancet Oncol 2012. 5. Parker C et al. ASCO 2012 (LBA 4512). 6. Scher H et al. N Engl J Med 2012;367:1187-97.
ANCAK, SAĞKALIMA KATKI ORTALAMA 3.5 AY

84
MKDPK ‘de 2013 yılında güncel durum Yeni ilaçlar=Artmış maaliyet
?

SONUÇ: Çok geniş bir portfolyo
85
AKILCI KULLANIM
Kaotik bir şekilde kullanılırsa
Cabazitaxel
Denosumab
Sipuleucel-T
Zoledronic
acid
Docetaxel
ADT
Abiraterone
Radium-223 Enzalutamide
BÜYÜK ŞANS
potansiyel tehlike