melanoma
TRANSCRIPT

MELANOMAVAISHNAVI SURESH NAIR

MELANOMA:
These tumours originate in the pigment-producing melanocytes
in the basal layer of the epidermis.
These cancerous growths develop when unrepaired DNA
damage occurs on melanocytes which triggers mutations that
lead the skin cells to multiply rapidly and form malignant tumours.
Melanomas often resemble moles; some develop from moles. The majority of melanomas are black or
brown, but they can also be skin coloured, pink, red, purple, blue or white.
Melanoma is caused mainly by intense, occasional UV exposure(frequently leading to sunburn),
especially in those who are genetically predisposed to the disease.
If melanoma is recognized and treated early, it is almost always curable, but if it is not, the cancer can
advance and spread to other parts of the body, where it becomes hard to treat and can be fatal.
While it is not the most common of the cancers, it causes the most deaths.Male (5%),Female(4%)

Everyone is at some risk for melanoma, but increased risk depends on several factors:
sun exposure, number of moles on the skin, skin type and family history, genetic mutations etc.
CAUSES & RISK FACTORS
SUN EXPOSURE
Both UVA and UVB rays are dangerous to the skin, and can induce skin cancer, including melanoma.
Blistering sunburns in early childhood especially increase risk, but sunburns later in life and cumulative
exposure also may be factors.
People who live in locations that have more sunlight — like Florida, Hawaii, and Australia — develop more
skin cancers, but some more northern locations with light-skinned populations also have a high number
of skin cancers.
Avoid using a tanning booth or tanning bed, since it increases the exposure to UV rays, raising your risk of
developing melanoma and other skin cancers.
MOLES
There are two kinds of moles: normal moles — the small brown blemishes, growths, or "beauty marks" that
appear in the first few decades of life in almost everyone — and atypical moles, also known as dysplastic nevi.
Atypical moles can be precursors to melanoma, and having them puts you at increased risk of melanoma.
But regardless of type, the more moles you have, the greater your risk for melanoma.

SKIN TYPE
As with all skin cancers, people with fairer skin, lighter hair and eye colour are at increased risk.
PERSONAL HISTORY
Once you have had melanoma, you run an increased chance of recurrence.
People who have or have had basal cell carcinoma or squamous cell carcinoma are also at increased risk for
developing melanoma.
WEAKENED IMMUNE SYSTEM
Compromised immune systems as the result of chemotherapy, an organ transplant, excessive sun exposure, and
diseases such as HIV/AIDS or lymphoma can increase your risk of melanoma.
FAMILY HISTORY
Heredity plays a major role in melanoma. About one in every 10 patients diagnosed with the disease has a family
member with a history of melanoma.
If your mother, father, siblings or children have had a melanoma, you are in a melanoma-prone family.
Each person with a first-degree relative diagnosed with melanoma has a 50 percent greater chance of
developing the disease than people who do not have a family history of the disease.

EXAMINE CLOSE RELATIVES
When melanoma is diagnosed, it is standard practice for physicians to recommend that close relatives be
examined immediately for melanoma and for the presence of unusual or atypical moles.These moles are
also called "dysplastic nevi."
FAMILY SYNDROME
When atypical moles are found in an individual belonging to a melanoma family, the condition is
known as FAMMM (Familial Atypical Multiple Mole Melanoma Syndrome).
People with this syndrome are at the greatest risk of developing melanoma.
A research study found that those family members who did not have atypical moles were much less likely
to develop melanoma.

GENETIC RISK FACTORS
BRAF gene mutations:
A mutation BRAF gene, can play a part in causing many melanomas. This mutated gene is found in about half
of all melanomas.
The discovery of BRAF was an exciting research breakthrough, and with the development of vemurafenib
( Zelboraf TM).
Increasing understanding of the BRAF gene could lead to the development of new diagnostic tools and has
already led to the development of several new and improved drug therapies.
p53 gene mutations:
The mutations most commonly seen in familial melanoma occur in gene, p53. When this gene is in its normal
state, it functions as a tumour suppressor, giving damaged cells the chance to repair themselves without
progressing to cancer. But when the gene is altered, it becomes unable to perform this function, and cancer can
result.
New research shows that the same ultraviolet (UV) damage that produces skin damage can damage p53,
causing the alterations that eliminate its ability to suppress tumours.
A number of gene mutations in addition to p53 and BRAF have been associated with familial melanoma, notably
the CDKN2A (cyclin-dependent kinase inhibitor 2A) gene.

MOLES IN ACTIVE STAGE
Moles in people belonging to melanoma-prone families are subject to change at certain times of life. They may
get larger or show alterations in colour or elevation, so for those periods, they are described as being active.
While the reasons for these changes are not fully known, there could be a hormonal component: Moles are
more active at puberty and during pregnancy.
Most physicians advise high-risk individuals not to take hormonal medications, such as oral contraceptives or
hormone replacement therapy.
EXAMINATION SCHEDULING
Individuals with atypical mole syndrome can improve their chances of early detection by increasing the frequency
of skin self-examination and by visiting a physician more often for a full-body skin exam.
The clinician may take photographs to document whether there are new moles or changes in older ones.

IN CHILDREN:
Children in melanoma-prone families need special care, because familial melanoma is likely to make its
appearance early in life.
Even though these cancers usually do not appear until after adolescence, they may arise in much
younger children who have a family history of melanoma.
Most physicians, therefore, advise parents to make a point of studying a child's skin frequently from infancy
on.
Physician examination in these families should start at the age of 10 and continue on a twice-a-year
basis thereafter.
Particular care should be taken at puberty and during adolescence when hormonal changes activate
the moles.
As melanoma families are on the lookout for the disease and seek professional consultation early, the
survival rate for familial melanoma is even higher than that for non-familial melanomas.

SYMPTOMS OF MELANOMA:
In the early stages, melanoma may not cause any symptoms (what you
feel). But sometimes melanoma will:
Itch.
Bleed.
Feel painful.
Many melanomas have these signs and symptoms, but not all. There are
different types of melanoma. One type can first appear as a brown or black
streak underneath a fingernail or toenail. Melanoma also can look like a
bruise that just won’t heal.

Hidden melanomasMelanomas can also develop in areas of your body that have little or no exposure to the sun, such as the spaces
between your toes and on your palms, soles, scalp or genitals. These are sometimes referred to as hidden
melanomas because they occur in places most people wouldn't think to check. When melanoma occurs in people
with darker skin, it's more likely to occur in a hidden area.
Hidden melanomas include:
•Melanoma under a nail:
Acral lentiginous melanoma is a rare form of melanoma that can occur under a fingernail or toenail. It can
also be found on the palms of the hands or the soles of the feet. It's more common in blacks and in other people
with darker skin pigment.
•Melanoma in the mouth, digestive tract, urinary tract or vagina:
Mucosal melanoma develops in the mucous membrane that lines the nose, mouth, oesophagus, anus,
urinary tract and vagina. Mucosal melanomas are especially difficult to detect because they can easily be mistaken
for other far more common conditions.
•Melanoma in the eye:
Eye melanoma, also called ocular melanoma, most often occurs in the uvea — the layer beneath the white
of the eye (sclera). An eye melanoma may cause vision changes and may be diagnosed during an eye exam.

TYPES OF MELANOMA
There are four basic types of melanomas.
3 of them begin in situ (meaning they occupy only the top layers of the skin) and sometimes become
invasive.
The fourth is invasive from the start.
Invasive melanomas are more serious, as they have penetrated deeper into the skin and may have
spread to other areas of the body.
Superficial spreading melanoma
It is the most common type, (about 70 percent of all cases.)
Most often seen in young people.
It grows along the top layer of the skin for a fairly long time before penetrating more deeply.
The first sign is the appearance of a flat or slightly raised discoloured patch that has
irregular borders and is somewhat asymmetrical in form.
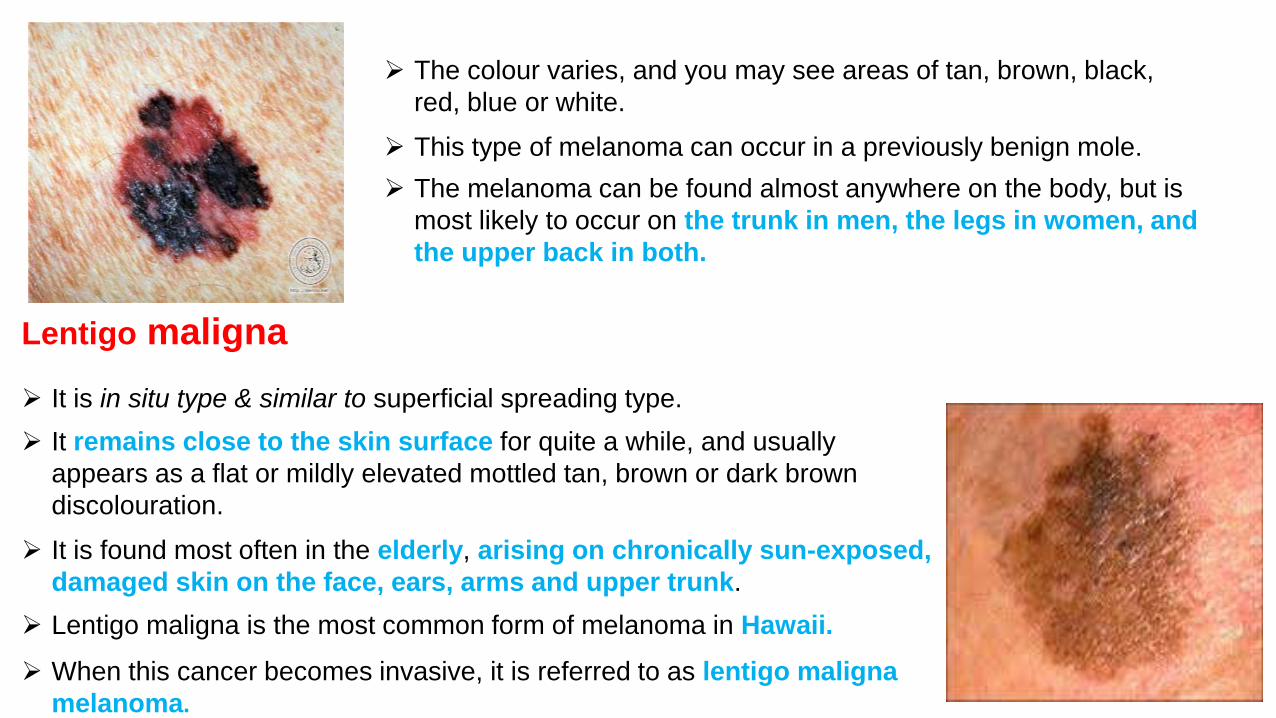
Lentigo maligna
It is in situ type & similar to superficial spreading type.
It remains close to the skin surface for quite a while, and usually
appears as a flat or mildly elevated mottled tan, brown or dark brown
discolouration.
It is found most often in the elderly, arising on chronically sun-exposed,
damaged skin on the face, ears, arms and upper trunk.
Lentigo maligna is the most common form of melanoma in Hawaii.
When this cancer becomes invasive, it is referred to as lentigo maligna
melanoma.
The colour varies, and you may see areas of tan, brown, black,
red, blue or white.
This type of melanoma can occur in a previously benign mole.
The melanoma can be found almost anywhere on the body, but is
most likely to occur on the trunk in men, the legs in women, and
the upper back in both.

Acral lentiginous melanoma
It also spreads superficially before penetrating more deeply.
It usually appears as a black or brown discolouration under the nails or on
the soles of the feet or palms of the hands.
This type of melanoma is sometimes found on dark-skinned people,
and can often advance more quickly than superficial spreading melanoma and
lentigo maligna.
It is the most common melanoma in African-Americans and Asians,
and the least common among Caucasians.
Nodular melanoma
It is usually invasive at the time it is first diagnosed.
The malignancy is recognized when it becomes a bump.
It is usually black, but occasionally is blue, gray, white, brown, tan, red or skin
tone.
The most frequent locations are the trunk, legs, and arms, mainly of elderly
people , as well as the scalp in men.
This is the most aggressive of the melanomas, and is found in 10 to 15 percent
of cases.

New Melanoma Staging System
The classification system recommended by the American Joint Commission on Cancer (AJCC) has
been updated as of 2010 & new findings about melanoma are incorporated to provide the most accurate
diagnosis and prognosis (a forecast of how the disease is likely to progress).
Breslow’s thickness
The most important factors in the new staging system are the thickness of the tumour, known as
Breslow’s thickness (also called Breslow’s depth), the appearance of microscopic ulceration (, and mitotic rate,
the speed of cell division (how fast-growing the cancer cells are).
Breslow's depth
Stage Depth
Stage I less or equal to 0.75mm
Stage II 0.75 mm - 1.5mm
Stage III 1.51 mm - 2.25mm
Stage IV 2.25 mm - 3.0mm
Stage V greater than 3.0 mm
Prognostic importance
tumour Depth
Approximate 5 year survival
<1 mm 95-100%
1 - 2 mm 80-96%
2.1 - 4 mm 60-75%
>4 mm 50%
Level 1 : Melanoma confined to the epidermis (melanoma in situ)
Level 2 : Invasion into the papillary dermis
Level 3 : Invasion to the junction of the papillary and reticular dermis
Level 4 : Invasion into the reticular dermis
Level 5 : Invasion into the subcutaneous fat
Clark’s level of invasion:
Formerly, very thin tumours were classified according to Clark’s level of invasion, the number of layers
of skin penetrated by the tumour. In the newest staging system, Clark’s level has far less importance.
Clark’s level will enter into serious consideration only in the rare instances when mitotic rate cannot
be determined.
To be exact, Breslow’s thickness measures in millimeters (1 mm equals 0.04 inch) the distance
between the upper layer of the epidermis and the deepest point of tumour penetration.
The thinner the melanoma, the better the chance of a cure.
Therefore, Breslow’s thickness is considered one of the most significant factors in predicting the
progression of the disease.

The presence of microscopic ulceration upgrades a tumour’s seriousness and can move it into a later stage.
Therefore, the physician may consider using a more aggressive treatment than would otherwise be selected.
Mitotic rate has been introduced into the staging system based on recent evidence that it is also an independent
factor predicting prognosis.
The presence of at least one mitosis (cancer cell division) per millimeter squared (mm2) can upgrade a thin
melanoma to a later stage at higher risk for metastasis.
In situ (non-invasive) melanoma remains confined to the
epidermis.
Thin tumours are less than 1.0 millimeter (mm) in Breslow’s
depth.
Intermediate tumours are 1.0-4.0 mm.
Thick melanomas are greater than 4.0 mm.Two examples of thin melanomas
STAGES OF MELANOMA
The stage refers to the thickness, depth of penetration, and the degree to which the melanoma has spread. The
staging is used to determine treatment.
Stage 0 tumours are in situ, meaning that they are non invasive and have not penetrated below
the surface of the skin
Stage I tumours have invaded the skin but are small, non ulcerated, and are growing at a slow
mitotic rate.
Stage II tumours though localized, are larger (generally over 1 mm. thick) and/or may be ulcerated
or have a mitotic rate of greater than 1/mm2; they are considered intermediate melanomas.
Stages III and IV They have spread (metastasized) to other parts of the body. There are also
subdivisions within stages.
EARLY MELANOMAS (CLINICAL STAGE I & II) - These melanomas (Stages 0 and I) are localized.
LATER STAGES (CLINICAL STAGE III & IV) - They are more advanced melanomas

Stage 0: Melanoma in situ (Clark Level I), 99.9% survival
Stage I / II: Invasive melanoma, 89–95% survival
T1a: Less than 1.0 mm primary tumour thickness, without ulceration, and mitosis < 1/mm2
T1b: Less than 1.0 mm primary tumour thickness, with ulceration or mitoses ≥ 1/mm2
T2a: 1.01–2.0 mm primary tumour thickness, without ulceration
Stage II:
High risk melanoma, 45–79% survival
T2b: 1.01–2.0 mm primary tumour thickness, with ulceration
T3a: 2.01–4.0 mm primary tumour thickness, without ulceration
T3b: 2.01–4.0 mm primary tumour thickness, with ulceration
T4a: Greater than 4.0 mm primary tumour thickness, without ulceration
T4b: Greater than 4.0 mm primary tumour thickness, with ulceration
Stage III:
Regional metastasis, 24–70% survival
N1: Single positive lymph node
N2: Two to three positive lymph nodes or regional skin/in-transit metastasis
N3: Four positive lymph nodes or one lymph node and regional skin/in-transit metastases
Stage IV:
Distant metastasis, 7–19% survival
M1a: Distant skin metastasis, normal LDH
M1b: Lung metastasis, normal LDH
M1c: Other distant metastasis or any distant metastasis with elevated LDH

PHYSICAL EXAMINATION
Total body examination
A total-body skin examination is crucial when evaluating a patient with an atypical nevus or a melanoma. The
skin examination should be performed on initial evaluation of the patient and during all subsequent visits
Crucial to a good skin examination is a well-lit examining room and a completely disrobed patient.
Serial photography and new techniques, such as epiluminescence microscopy and computerized image
analysis, are useful adjuncts.
Epiluminescence microscopy uses a magnifying lens to examine a lesion that has had oil applied.
Computerized image analysis stores images of the lesions and makes them available for comparison over time.
Skin examination
During a skin examination, assess the total number of nevi present on the patient's skin. Attempt to
differentiate between typical and atypical lesions.
Lymph node examination
If a patient is diagnosed with a melanoma, examine all lymph node groups. Melanoma may disseminate through
the lymphatics, leading to the involvement of regional lymph nodes, and hematogenously, leading to the
involvement of any node basin in the body.

WARNING SIGNS:THE ABCDEs OF MELANOMA
Moles, brown spots and growths on the skin are usually harmless — but not always.
Anyone who has more than 100 moles is at greater risk for melanoma.
The first signs can appear in one or more atypical moles.
Look for the ABCDE signs of melanoma, and if you see one or more, consult a physician immediately.
A – ASSYMETRY
If you draw a line through this mole, the two halves will not
match.

B - BORDER
The borders of an early melanoma tend to
be uneven. The edges may be scalloped or
notched.
C- COLOR
Having a variety of colours is another
warning signal. A number of different shades
of brown, tan or black could appear. A
melanoma may also become red, blue or
some other colour
D - DIAMETER
Melanomas usually are larger in diameter than the size of
the eraser on your pencil (1/4 inch or 6 mm), but they may
sometimes be smaller when first detected.
E - EVOLVING
Any change — in size, shape, colour, elevation, or
another trait, or any new symptom such as bleeding,
itching or crusting — points to danger.

Dx OF MELANOMA
Sometimes cancer can be detected simply by looking at your skin, but the only way to accurately diagnose
melanoma is with a biopsy. In this procedure, all or part of the suspicious mole or growth is removed, and a
pathologist analyses the sample. Biopsy procedures used to diagnose melanoma include:
Punch biopsy. During a punch biopsy, your doctor uses a tool with a circular blade. The blade is pressed into
the skin around a suspicious mole, and a round piece of skin is removed.
Excisional biopsy. In this procedure, the entire mole or growth is removed along with a small border of
normal-appearing skin.
Incisional biopsy. With an incisional biopsy, only the most irregular part of a mole or growth is taken for
laboratory analysis.
The type of skin biopsy procedure you undergo will depend on your situation. Doctors prefer to use punch biopsy
or excisional biopsy to remove the entire growth whenever possible. Incisional biopsy may be used when other
techniques can't easily be completed.

Diagnostic Considerations
Differentials to consider in the diagnosis of malignant melanoma include the following conditions:
Benign melanocytic lesions
Dysplastic nevus
Squamous cell carcinoma
Metastatic tumours to the skin
Blue nevus
Epithelioid (Spitz) tumour
Pigmented spindle cell tumour
Halo nevus
Atypical fibroxanthoma
Pigmented actinic keratosis
Sebaceous carcinoma
Histiocytoid hemangioma
Differential Diagnoses
Basal Cell Carcinoma
Lentigo Maligna Melanoma
Mycosis Fungoides

PREVENTION
Since its inception in 1979, The Skin Cancer Foundation has always recommended using a sunscreen with an SPF 15
or higher as one important part of a complete sun protection regimen. But sunscreen alone is not enough.
Seek the shade, especially between 10 AM and 4 PM.
Do not burn.
Avoid tanning and never use UV tanning beds.
Cover up with clothing, including a broad-brimmed hat and UV-blocking sunglasses.
Use a broad spectrum (UVA/UVB) sunscreen with an SPF of 15 or higher every day. For extended outdoor
activity, use a water-resistant, broad spectrum (UVA/UVB)sunscreen with an SPF of 30 or higher.
Apply 1 ounce (2 tablespoons) of sunscreen to your entire body 30 minutes before going outside. Reapply every
two hours or immediately after swimming or excessive sweating.
Keep new-borns out of the sun. Sunscreens should be used on babies over the age of six months.
Examine your skin head-to-toe every month.
See your physician every year for a professional skin exam.

SURGICAL TECHNIQUES
The first step in treatment is the removal of the melanoma, and the standard method of doing this is by surgical
excision (cutting it out).
Patients do just as well after the laser surgery, which is easier to tolerate and produces a smaller scar.
Surgical excision is also called resection, and the borders of the entire area excised are known as the margins.
TREATMENT
OP/OFFICE SURGERY
In most cases, the surgery for thin melanomas can be done in the doctor’s office or as an outpatient procedure
under local anaesthesia. Stitches (sutures) remain in place for one to two weeks, and most patients are advised to
avoid heavy exercise during this time. Scars are usually small and improve over time.
Dis colourations and areas that are depressed or raised following the surgery can be concealed with cosmetics
specially formulated to provide camouflage. If the melanoma is larger and requires more extensive surgery, a better
cosmetic appearance can be obtained with flaps made from skin near the tumour, or with grafts of skin taken from
another part of the body. For grafting, the skin is removed from areas that are normally or easily covered with
clothing.
There is now a trend towards performing sentinel node biopsy and tumour removal surgery at the same time,
provided the tumour is 1 mm or more thick. When the procedures are combined in this way, the patient is spared an
extra visit.

SURGICAL EXCISION
It is also called resection, and the borders of the entire area excised are known as the margins. Surgical excision
is used to treat all types of skin cancer.
The physician begins by outlining the tumour with a marking pen. A "safety margin" of healthy-looking tissue will
be included, because it is not possible to determine with the naked eye how far microscopic strands of tumour
may have extended. The extended line of excision is drawn, so the skin may be sewn back together.
The physician will administer a local anaesthetic, and then cut along the lines that were drawn. The entire
procedure takes about thirty minutes for smaller lesions.
Wounds heal rapidly, usually in a week or two. Scarring depends on many factors, including the placement of
the tumour and the patient's care of the wound after the procedure.
The tissue sample will be sent to a lab, to see if any of the "safety margin" has been invaded by skin cancer. If
this is the case, it is assumed that the cancer is still present, and additional surgery is required.
Sometimes, Mohs micrographic surgery is a good option at this point.

SETTING THE MARGINS
In the new approach to surgery, much less of the normal skin around the tumour is removed and the margins,
therefore, are much narrower than they ever were before. This spares significant amounts of tissue and reduces
the need for postoperative cosmetic reconstructive surgery.
Most US surgeons today follow the guidelines recommended by the National Institutes of Health and the American
Academy of Dermatology Task Force on Cutaneous Melanoma.
When there is an in situ melanoma, the surgeon excises 0.5-1 centimetre of the normal skin surrounding the
tumour and takes off the skin layers down to the fat.
In removing an invasive melanoma that is 1 mm or less in Breslow’s thickness, the margins of surrounding skin
are extended to 1 cm and the excision goes through all skin layers and down to the fascia (the layer of tissue
covering the muscles).
If the melanoma is 1.01 to 2 mm thick, a margin of 1-2 cm is taken.
If the melanoma is 2.01 mm thick or greater, a margin of 2 cm is taken.
These margins all fall within the range of what is called “narrow” excision. When you consider that until recently,
margins of 3 to 5 cm (wide excision) were standard, even for comparatively thin tumours, you can see how
dramatically surgery has changed for the better. When melanomas have reached a thickness of 4 mm or more,
increasing the margins beyond 2 cm does not increase survival.

MOHS MICROGRAPHIC SURGERY
Mohs Micrographic Surgery is the most effective technique for removing basal cell and squamous cell
carcinomas (the two most common skin cancers), is being increasingly used as an alternative to standard
excision for certain melanomas.
In this technique, one thin layer of tissue is removed at a time, and as each layer is removed, its margins are
studied under the microscope for the presence of cancer cells. If the margins are cancer-free, the surgery is
ended.
If not, more tissue is removed, and this procedure is repeated until the margins of the final tissue examined are
clear of cancer. Mohs surgery can eliminate the guesswork in the removal of skin cancers and pinpoint the
cancer’s location when it is invisible to the naked eye.
Mohs surgery differs from other techniques since the microscopic examination of all excised tissues during the
surgery eliminates the need to “estimate” how far out or deep the roots of the skin cancer go. This allows the
Mohs surgeon to remove all of the cancer cells while sparing as much normal tissue as possible.
In recent years, however, efforts to improve and refine the Mohs surgeon’s ability to identify melanoma cells
have resulted in the development of special stains that highlight these cells. These special stains are known as
immunocytochemistry or immunohistochemistry (IHC) stains and use substances that preferentially stick to
pigment cells (melanocytes), where melanoma occurs, making them much easier to see with the microscope.

ADJUVANT THERAPY
For patients with Stages III and IV disease, surgery is usually followed with an additional adjuvant therapy.
CHEMOTHERAPY
Used as Mono/poly chemotherapy.
Dacarbazine (DTIC), given by injection.
DTIC may be combined with carmustin (BCNU) and tamoxifen, or with cisplatin and vinblastine.
Temozolomide, an oral drug closely resembling DTIC, is FDA-approved for brain cancers but also used off-label for
melanomas that have spread to the brain or nervous system.
Another class of drugs, based on a different principle, has come into use more recently. They are anti- angiogenic,
which means that they prevent new blood vessels from forming. It cut off the blood supply that would nourish the
cancer cells and enable them to grow. Studies are under way with the anti- angiogenic drug thalidomide, combined
with the chemotherapeutic agent, temozolomide.
Angiostatin and endostatin are two other drugs in this class that have shown some degree of activity against
melanoma in preliminary studies.
Isolated Limb Perfusion Method This palliative treatment, which relieves symptoms, is sometimes used when melanoma metastases have reached
an arm or leg.
“Isolated” means that the chemotherapy is “perfused” (shunted directly) to the blood flowing through the affected
limb, but to no other part of the body, to limit toxic effects. The drug melphalan is the chemotherapy most frequently
used, often combined with other agents.

IMMUNOTHERAPY
Clinical trials of various types of vaccine are under way with patients whose disease is in Stages III and IV. The
vaccines are intended to stimulate the immune system so that it reacts more strongly against a patient's melanoma
cells, destroying the cancer or slowing the progression. These vaccines are not a part of routine treatment at this
time.
Another type of immunotherapy (also known as biologic therapy) makes use of chemicals that occur naturally in
the body. Also there is injectable interferon (IFN) alpha-2b, the only drug with FDA approval to treat “high-risk”
Stage II and Stage III melanomas.
High-risk melanomas are tumours that have a high chance of recurring (such as those that are ulcerated or over 4
mm thick) or have spread to the nearby lymph nodes. At first, IFN alpha-2b appeared to increase overall 5-year
survival. After further study, it proved to give patients a longer period without relapse, extending their disease-free
interval to an average of 9 months, but did not lengthen overall survival. It has significant flu-like side effects.
In 2011, the FDA approved a new drug, peginterferon alfa-2b (also known as Sylatron), to treat Stage III melanoma
patients – those found to have microscopic or palpable metastatic disease that has reached the lymph nodes. The
drug, injected subcutaneously, was the first adjuvant, or additional, therapy for Stage III patients approved since
high-dose IFN alfa-2b in 1995.
This approval followed on the heels of a trial in which melanoma patients taking Sylatron remained relapse-free an
average of nine months longer than patients not taking the drug (34.8 months vs. 25.5 months). There was no
difference in overall survival.
tumour necrosis factor (tumor-killing) factor is another of these naturally occurring substances. Both of these —
especially interferon alpha-2b — are produced by white cells (lymphocytes) when they come in contact with
tumour cells, viruses or other harmful substances, and have been shown to kill a number of tumours, including
melanomas. They have some anti-angiogenic properties as well. Interferon alpha-2b is FDA-approved, tumour
necrosis factor is not.
Lymphokines, immune chemicals naturally produced by the white blood cells in small quantities, are being used
for Stage IV patients. They may also be produced by white blood cells that have been specially stimulated by
antigens, a basic part of the immune system, to make them better “killers” of malignant cells.
The best known of these therapies uses the injectable lymphokine interleukin-2 (IL-2), with or without the addition
of interferon alpha or other biotherapies and chemotherapies. It enters melanoma cells and attacks them. High-
dose IL-2 (“Proleukin”) was the first FDA-approved immunotherapy used to treat Stage IV metastatic melanoma.
It is associated with very significant side effects when given in high doses, but has been found to increase
disease-free and overall survival in some patients. About 10-16 percent of carefully selected patients on IL-2
regimens respond to the drug, with 6 percent having complete responses (remissions), and about 60 percent of
the complete responders have significantly extended lives.
Tumor-infiltrating lymphocytes (TILs) also play a part in some new therapies for advanced melanoma. Of
special note is a technique from the National Cancer Institute called adoptive cell transfer (ACT), which involves
harvesting TILs from the patient’s blood, then isolating from them the cells expressing T cell receptors that can
recognize melanoma-specific antigens; in other words, the most aggressive melanoma-killing lymphocytes are
identified and isolated. These are then grown in large numbers in the lab and reinjected into the patient in the
hope that they will massively attack the patient’s melanoma cells.
High doses of IL-2 may be added to make these tumor-fighting cells mature and multiply, and certain drugs are
used to eliminate immune factors that might inhibit the tumor-fighting cells; this is called lymphodepletion. In
clinical trials with metastatic melanoma patients who had not responded to previous treatment, the patients’
response rates have been far higher than those seen with chemotherapy.
In the latest trials, total-body irradiation was added to enhance lymphodepletion, and response rates up to 72
percent were observed in 93 patients, with 11 achieving complete remissions lasting 18 to 75 months or more.
CHECKPOINT BLOCKADE THERAPY
Anti-CTLA-4 therapy is another important new direction for melanoma immunotherapy. CTLA-4 is a kind of natural
“brake” in the immune system that can inhibit activation of healing T-cells to keep them from overproducing. Anti-
CTLA-4 therapies are designed to block CTLA-4 so that more T-cells can be produced when needed to fight a
cancer. The therapy is also referred to as “checkpoint blockade” immunotherapy.
The first successful checkpoint blockade therapy was ipilimumab (YervoyTM), approved by the FDA in 2011 for
patients with advanced melanoma. A monoclonal antibody (a purified class of antibodies cloned and mass-
produced in the lab from one specific type of cell or cell line) that blocks CTLA-4, ipilimumab has yielded dramatic,
sustained responses akin to “cures” in certain patients, with some surviving more than 5 years.
Two additional immune-checkpoint-blockading drugs, nivolumab and MK-3475 (pembrolizumab), are in late-stage
clinical trials and are likely to be FDA-approved in 2014 or 2015. Both inhibit another molecule (programmed
death-1, or PD-1) that suppresses T-cells.
PD-1 can directly interact with tumour cells by binding to a molecule called programmed death ligand-1 (PD-L1),
and cancer cells may use PD-L1 to hide from attack by T-cells, but these drugs can release the T-cells to fight the
cancer.
A third drug, MPDL3280A, is designed to inhibit PD-L1, and appears to hold promise in early clinical studies.
Initial results indicate that PD-1/PD-L1 blockade results in higher response rates and a more favorable side effect
profile than that seen with ipilmumab. Several randomized trials comparing ipilimumab with anti-PD-1 therapy are
ongoing.
TARGETED THERAPY
Targeted therapies are types of treatment that use drugs or other substances to identify and attack specific types of
cancer cells, or to block the action of certain enzymes, proteins or other molecules that promote the growth and
spread of cancer cells.
vemurafenib (Zelboraf TM), FDA-approved in 2011, which inhibits the gene called BRAF.
BRAF produces a protein that normally regulates skin cells, causing them to multiply only when growth is needed.
However, a specific mutated version of BRAF called v600E (found in about half of all melanoma patients) produces
an abnormal version of the protein that stays switched on. This leads to out-of-control growth, i.e., cancer.
Vemurafenib can bind to the defective protein and deactivate it. Phase I and II studies showed striking and rapid
antitumor activity in patients with BRAF v600E-mutated melanoma.
Then, a randomized Phase III trial comparing vemurafenib to standard chemotherapy showed both a progression-
free and overall survival (OS) advantage in vemurafenib patients (median OS of 13.6 months for vemurafenib
patients vs. 9.7 months for chemotherapy patients). As with imatinib, the hope is that altering the dosing regimen
and combining vemurafenib v with other therapies will significantly lengthen survival.

Another targeted therapy, imatinib (Gleevec), has produced encouraging but mixed early results in metastatic
melanoma, and greater numbers of patients must be tested. Imatinib inhibits c-KIT, the receptor for an enzyme
called tyrosine kinase, which has been associated with some cancers, including melanoma.
Genetic aberrations or mutations in KIT have been frequently found in certain gastrointestinal tumours and
leukemias, which have responded well to treatment with imatinib.
Some types of melanoma also frequently have KIT mutations, so it has been hypothesized that these melanomas
will similarly respond to imatinib treatment. Indeed, lab experiments have been promising, and some patients,
especially those with acral lentiginous melanoma and mucosal melanoma, have initially responded well, but thus
far, significant clinical improvements from the drug as a single therapy have been minimal. Imatinib is continuing to
be tested in different dosage regimens and combined with other therapies.
In 2013, two other treatments directed toward BRAF and a related molecule called MEK were also approved:
the BRAF inhibitor dabrafenib (Taflinar®) and the MEK inhibitor trametinib (Mekinist®).
Recently, the FDA also approved the use of these two drugs in combination for patients with inoperable or
metastatic melanoma with a BRAF V600E or V600K mutation. The hope is that these different drugs and drug
combinations will increase tumour shrinkage and extend the length of time before the melanoma starts growing
again.

GENE THERAPY
This treatment is in the very early stages of research, and its effectiveness is yet to be proven conclusively.
One form of gene therapy is based on creating alterations in the white blood cells or in the tumor-infiltrating
lymphocytes (TILS) so that they will attack the melanoma. This is achieved by removing these cells from the
patient, growing them outside the body and treating them so as to increase their number.
The next step is the addition of genetic material that produces one of the many growth factors which make the
lymphocytes more aggressive as cancer-fighters. These more aggressive lymphocytes are returned to the
patient's body in an effort to stimulate the immune system to kill the melanoma and its metastases.
The focus of current research is the identification of genes for specific melanoma antigens. These are molecules
found on the cell wall that stimulate the production of antibodies, which are a part of the body's immune defence
system. An antibody attaches itself to only one type of antigen.
By injecting the gene for the melanoma antigens, the hope is to increase their number and produce a broad
attack by the patient's immune system.

IMPROVING LONG TERM SURVIVAL
The advances in understanding melanoma and the immune system have set the stage for continual
improvements in the treatment of advanced disease. Some patients have already derived significant long-term
benefits.
One recent report suggested that 20 percent of patients who received ipilimumab are alive after 10 years. (In
contrast, only about 4-6 percent of patients were ever found to achieve long-term survival with Interleukin-2, and
no overall survival advantage was ever demonstrated with chemotherapy.)
Similarly, early clinical trials have described an improved likelihood of significant tumour shrinkage using
combinations of these new drugs, specifically dabrafenib combined with trametinib or ipilimumab with
nivolumab.
The next goal will be to determine which combinations and methods are most suitable to shrink melanoma most
effectively, maintain the best possible quality of life for patients and extend patients’ lives as long as possible.
Many other novel approaches are also on the horizon, currently either in active laboratory study or clinical trials;
the hope is to turn metastatic melanoma from a deadly disease into a manageable chronic condition.

CLINICAL TRIALS
Many patients, especially those with advanced disease, are participating in clinical
trials to obtain new treatments that are still experimental and not generally available.
Patients who have Stage III and IV melanoma might consider enrolling in a clinical
trial of a new or experimental treatment.
There are risks involved in enrolling in a clinical trial, but there can be benefits as
well. More treatment possibilities exist than ever before, giving new hope to people with
melanoma.