management of acute ischemic stroke -...
TRANSCRIPT

Management of acute ischemic
stroke
To feed the flame!
László Csiba

MI and stroke
cases 1st year
(M Ft)
2nd year
(M Ft)
MI 16 000 5 052 444
Stroke 42 000 15 360 1 416

In acute stroke :CT or MRI Ischemia 80% Bleeding 10-15%
3
Subarachnoidal Bleeding
2-4%

After MI 70-80%
Normal lifestyle
After Stroke 10%
4

Diagnosis in stroke
From blood
•BSR, counts
•glucose, ions
•hemostasis
•lipids, homocsyt.
•Immunological
(in youngs)
Blood gases
Heart
Functional •BP monitoring
•ECG
•Holter ECG
Morphological •TTE
•TEE
TEE
Carotid, vertebral •ultrasound
•CT AG
•MRA
•DSA
Brain imaging •CT •MRI
•Diff. WI •Perf. WI
•TCD •Angiogr.(DSA, MRA) •SPECT, PET

EBM in stroke
• Stroke unit
• Iv. thrombolysis
• aspirin
• Hemicraniectomy in malignant MCA infarct
On site activity in acute stroke 1




Airway
Breathing
Circulation
Disability
Exposure
-nvironment
-vents
-valuation
On site activity in acute stroke
2: ABCDE

Diagnosis
Lab+Imaging etc.
Gen.+Neurol. exam
Observation
Autoanamnesis
Heteroanamnesis

1.Hetereoanamnesis
Hőmérséklet?
4.1.Consciousness? (alert-somnolent-stupor-coma?)
4.2.Aphasia?
4.3. Eye, mouth, nose ear
Coniugated eyes?
• Anisocoria?
• Tongue biting?
• Rest of medicaments?
• Lip-cyanosis?
4.7.position?
Babinski?
Severity of paresis?:
• Upper extr.?
• Lower extr?
• total-medium-mild?
ANY CHANGE DURING THE OBSERVATION PERIOD?
TIME OF ONSET OF PARESIS??
4. Examination
4.4.Bruit?
On site activity in acute stroke 3
3.Observation 2. Autoanamn.
4.5.RR
Pulse
Fever
auscult
4.6.Defense
Bladder?
Peristalt?
Sore?

Suspect for…..
• ischemia: – vascular risk factors,
– carotid bruit,
– onset in the morning, disturbance of consciousness is rare,
– RR slightly elevated breath normal
• bleeding – hypertension
– onset at dailly activity
– severe symptoms, plethora
– somnolent, forced breathing
• embolic origin • sudden onset, maximal quickly improving symtoms
• arhythmia, cardiac problems (eg. AF)
• previous stroke in the other hemipsh.
• vitium (heart)
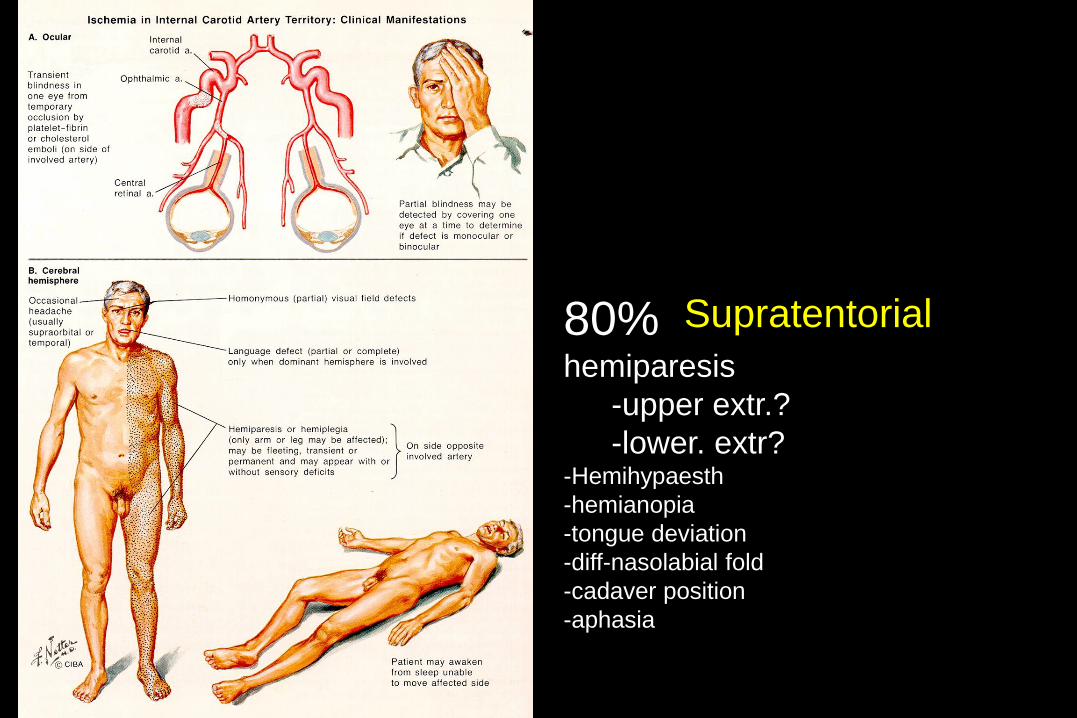
80% hemiparesis
-upper extr.?
-lower. extr? -Hemihypaesth
-hemianopia
-tongue deviation
-diff-nasolabial fold
-cadaver position
-aphasia
Supratentorial

Vertebrobasilar
20% -vertigo? -ataxia? -dysarthria? -double vision? -swallowing? -paresis?

The differential diagnosis
– seizure with postictal paralysis
– Hypoglycemia
– brain tumor
– Migraine
– head trauma
– brain abscess
– Encephalitis

Blood sugar
• No routinous iv. or per os glucose!
• First measure!
• Hypo- or hyperglycemia? (< 2,7 mmol/l or >11
mmol/l), please correct!
• Avoid hyperglycemia!!
Most important question?
Is he/she a candidate for
thrombolysis or not?

ESO 2008
•
• ..Priority transport with
advance notification ...
• .. personnel be trained
to recognise stroke
using simple
instruments such as the
Face-Arm–Speech-
Test …

Modified Cincinnati Prehospital Stroke Scale
(CPSS)
Evaluation
Facial paresis
X
Upper extr. paresis
X
Lower extr. paresis
Speech

ESO 2008
• • ..helicopter transfer..
• ….telemedicine ….
• …suspected TIA be
referred without delay..

Activity during transport?
• Pulsoximetry
• ECG
• Blood sugar? Strip
• (if possible blood sampling)
• BP at 5-10 min
• Change of consciousness, paresis?
• If stable condition→directly to CT!!!

In the hospital
Immediate CT!!!!!
Quick labs!
Rapid onset of therapy

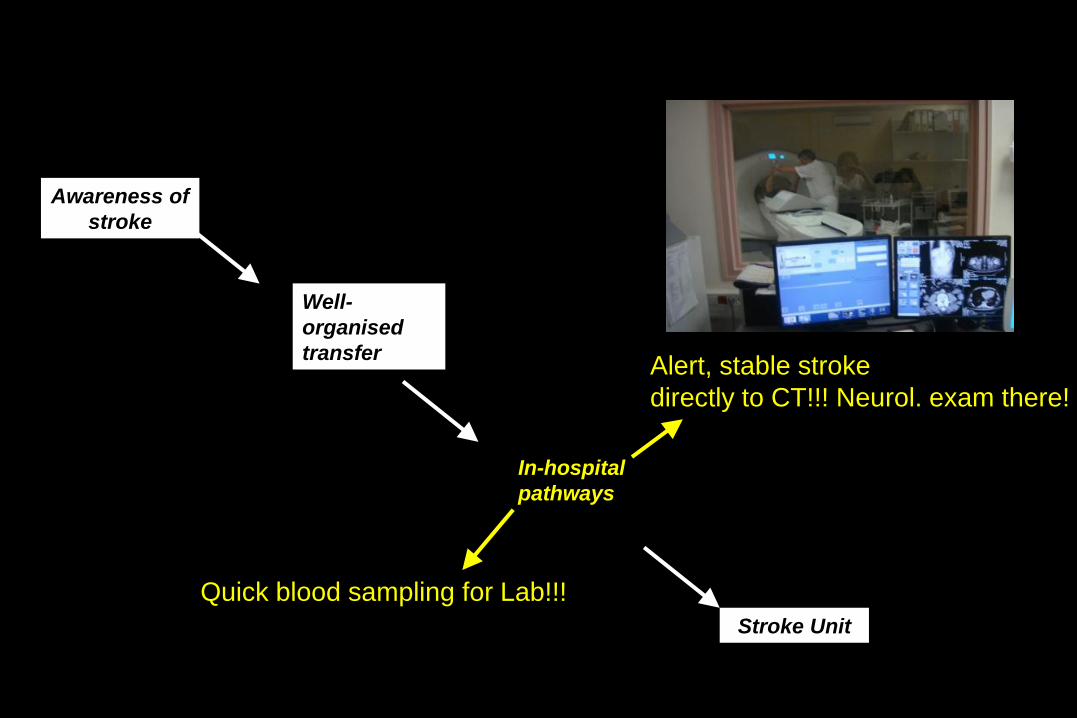
Awareness of
stroke
In-hospital
pathways
Stroke Unit
Well-
organised
transfer
The success of stroke care depends on the
stroke chain

Awareness
of stroke
In-hospital
pathways
Stroke Unit
Well-
organised
transfer
•Stroke day
•press, local TV
•Family physician
Awareness of
stroke
In-hospital
pathways
Stroke Unit
Well-
organised
transfer
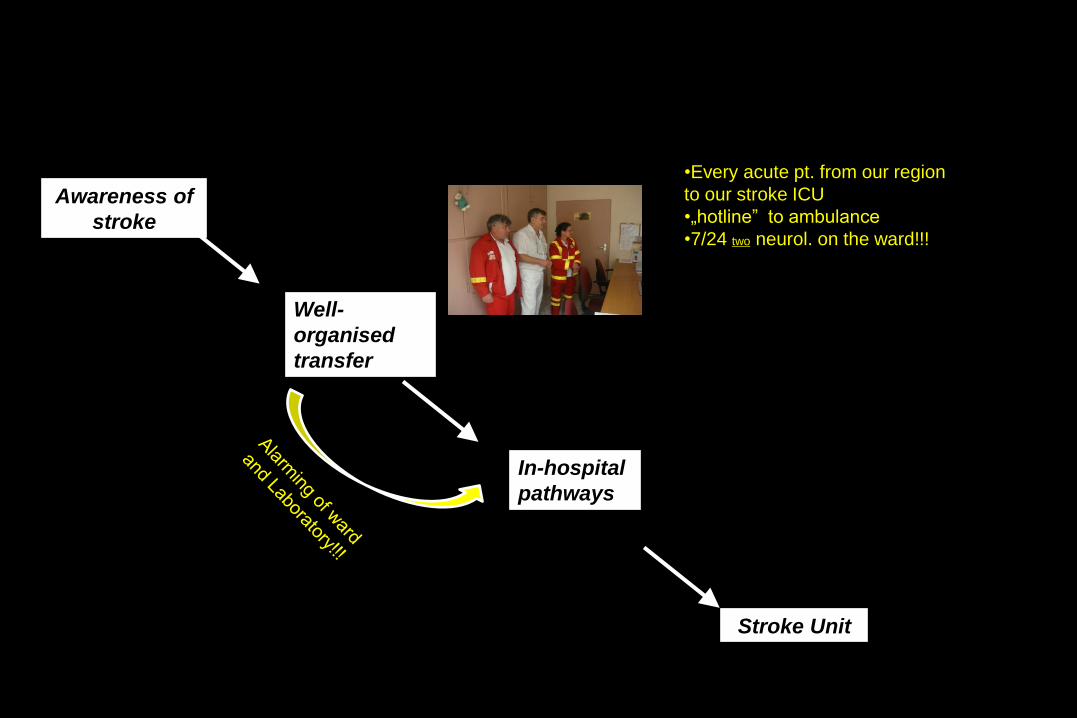
•Every acute pt. from our region
to our stroke ICU
•„hotline” to ambulance
•7/24 two neurol. on the ward!!!

Awareness of
stroke
In-hospital
pathways
Stroke Unit
Well-
organised
transfer
The success of stroke care depends on the
stroke chain
16% of delay
Awareness of
stroke
In-hospital
pathways
Stroke Unit
Well-
organised
transfer Alert, stable stroke
directly to CT!!! Neurol. exam there!
Quick blood sampling for Lab!!!
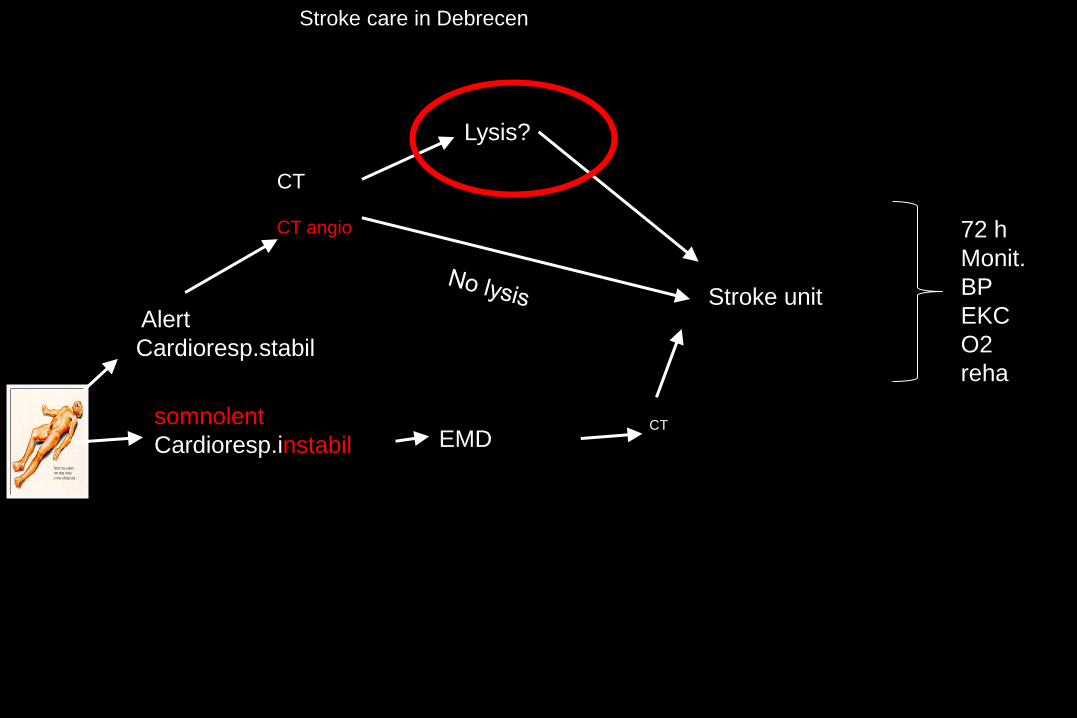
Stroke care in Debrecen
Alert
Cardioresp.stabil
CT
CT angio
somnolent
Cardioresp.instabil EMD CT
Stroke unit
Lysis?
72 h
Monit.
BP
EKC
O2
reha

Thrombus location and likelihood of its
recanalization with systemic tPA.
Alexandrov , J Int. Medicine 267; 209–219 2010.

Stroke-care:Team-work
Neuropsychol Social worker
Cardiologist
Radiologist Logopedist
Stroke nurse Strokologist Physiotherapeuta
Prof. Kaste 32

Time is brain!
• 700 km axon/hour
• 2 mi neuron/min
• Every hour of stroke →3.6 yrs↓

Infarct
infarktus infarktus
Survival or death? hours

Lysis as soon as possible….
(Lancet 2004; 363: 768-74)
min
Ra
tio
of
su
cc
es
s
2,0
2,5
3,0
3,5
4,0
1,5
1,0
0,5
0 60 90 120 150 180 210 240 270 300 330 360
4 9 21 45
NNT for 1 symptom-free?
60’ 2!!

2003 februárban az agyi érbetegek kórházi felvételének száma
188161
529
436
383356
330
181176
515
435408403
366
204
148
515
456430
383365
173176
502
405440
364388
0
100
200
300
400
500
600
20
03
.02
.01
20
03
.02
.03
20
03
.02
.05
20
03
.02
.07
20
03
.02
.09
20
03
.02
.11
20
03
.02
.13
20
03
.02
.15
20
03
.02
.17
20
03
.02
.19
20
03
.02
.21
20
03
.02
.23
20
03
.02
.25
20
03
.02
.27
Week-end Week-end
Stroke during the week end week-end
36
Week-end Week-end
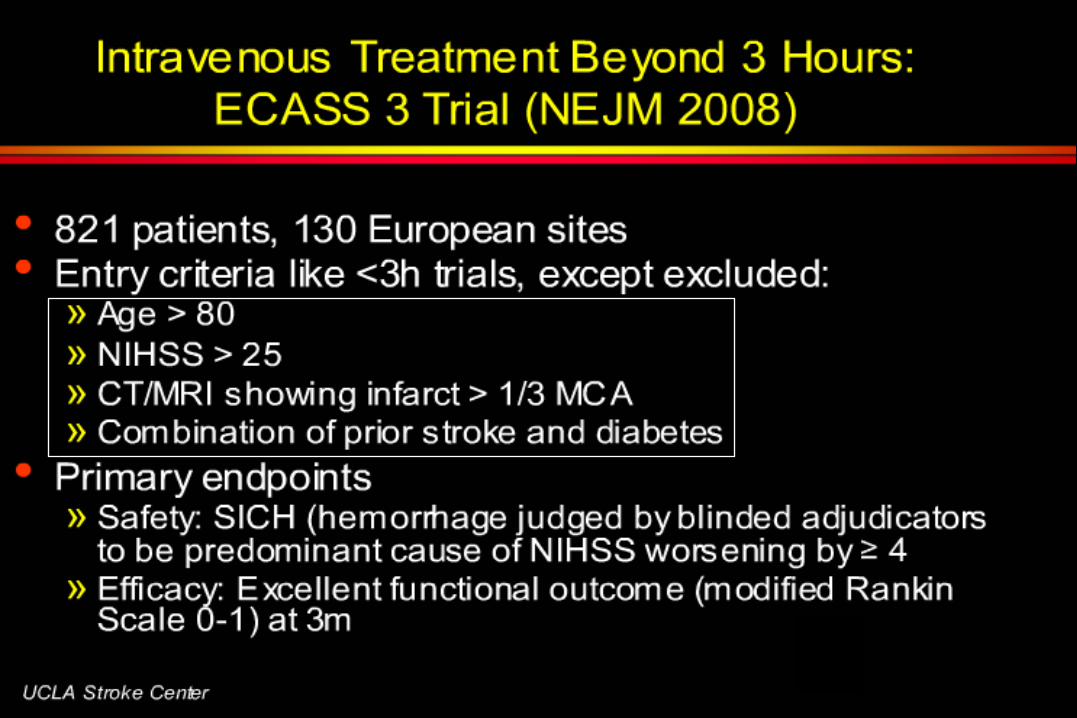
„Táguló” időablak: 4,5 h

Intravenous Alteplase Absolute contraindications
Evidence of intracranial hemorrhage on pretreatment evaluation
• Suspicion of SAH
• Recent (within 3 mo) intracranial or intraspinal surgery,
• serious head trauma, or previous stroke
• History of intracranial hemorrhage
• Uncontrolled hypertension at time of treatment (> 185 mm Hg systolic or >
110 mm Hg diastolic blood pressure)
• Active internal bleeding
• Intracranial neoplasm, AVM or aneurysm
• oral anticoagulants (e.g., warfarin sodium) if INR 1.7 or a prothrombin time
15 seconds
• heparin within 48 hours before the onset of stroke and an elevated activated
partial thromboplastin time at presentation
•

t-PA (alteplase)
• alteplase dose 0.9 mg/kg (maximum 90 mg), with a bolus of 10% of the dose administered over 1 minute, and the remainder infused over 60 minutes
• Significant drug interactions – OAC and AP increase the bleeding risk.
– The greatest risk sympt intracranial bleeding
– therapeutic heparin, antithrombotics, and OAC are contraindicated within 24 hours after administration of alteplase.
• Sc. heparin at a daily dose of 10,000 units or less without increased bleeding
• laryngeal and orolingual angioedema <1%, but urgent airway stabilization.
• orolingual angioedema was 1.7% (95% confidence interval [CI] 0.2–5.9%) with angiotensin-converting enzyme (ACE) inhibitor

Patient Evaluation and Management
in the Emergency Department • blood glucose level,
• serum electrolyte level,
• complete blood cell count,
• platelet count,
• renal function studies,
• prothrombin time,
• activated partial thromboplastin time,
• continuous oxygen therapy with oxygen saturation
• cardiac monitoring.
• with a cardiac history electrocardiography

Misbelieves in in acute stroke
• Early signs of ischaemia on CT excludes lysis
within the first 3 h NOT TRUE!
• Hyperdense MCA sign excludes thrombolysis.
NOT TRUE!
• Present anticoagulation excludes lysis . NOT
TRUE! except INR≥1.7
• Epileptic seizure excludes thrombolysis
NOT TRUE!
Control of intracranial bleeding from
fibrinolytic
– infusion of platelets 6–8 units and cryoprecipitate that contains factor VIII to rapidly correct the fibrinolytic state
– 10 units of cryoprecipitate be administered rapidly because cryoprecipitate contains fibrinogen, the most specific reversal agent for fibrinolytics
– To obtain cryoprecipitate, a type and screen is necessary.
– Neurosurgical evacuation may be warranted.
lysis ESO 2008
• New!
…Intra-arterial treatment
of acute MCA occlusion
within a 6-hour time
window is
recommended as an
option..
• Mechanical
Embolus
Removal in
Cerebral
Ischemia
MERCI

ESO 2008 MERCI
• Mechanical Embolus Removal in Cerebral
Embolism (MERCI)
• Recanalisation in 48% (68/141) within 8
hours

http://www.eso-
stroke.org/ppt/ESO08_Slides_25thApril.
PPT#444,11,Classification of Evidence

Therapy if NO lysis…..

Stroke unit
Neurosurgery
lysis
Op.
Isch/ICH
CT!!!
CT+AG!!
Neu. Status
labs
5-10%
80%

If BP >220mmHg use…
• α- and/or β-receptor-blocking (eg. urapidil,
metoprolol), careful monitoring of BP (measuring at
5-10 min)
• Stabilize at 160 Hgmm

If NO lysis… ESO 2008
• aspirin (160–325 mg loading dose) be given within 48 hours after ischemic stroke

If NO thrombolysis… in acute stroke
• NOT(!) recommended in acute phase:
– Early UFH,
– low molecular weight heparin or heparinoids
• meta-analysis of 22 trials,
– 9 ↓ recurr isch strokes per 1000 treated pts
– BUT 9/1000 in sympt intracranial
hemorrhages (Cochrane 2006].

Incr ICP ESO 2008
• New!
Surgical decompressive therapy within 48 hours up to 60 y with evolving malignant MCA infarcts
• New!
No recommendation can be given regarding hypothermic therapy in patients with space-occupying infarctions

Dept. of Neurology
Debrecen, Hungary
Basilar artery occlusio:. Intraarterial or iv. thrombolysis till 12 hours, if the
patient worsens
Intraarterial lysis is an option in MCA till 6 hours, but start with
iv.
iv.. thrombolysis 3 h –new time 4.5 hours with iv. t-PA
3-4,5 hour interval is NOT valid: 80y 1/3 MCA infarct, 25 NIHS, combin.
Of prior stroke+diabetes
Acute ischemic stroke therapy
Ih NO lysis :
100 mg aspirin, if NO lysis
2-4 lit/min oxygen
if BP 220 Hgmm decrease!!!
idő
Mechanical thrombus removal (eg.. MERCI, Penumbra etc) MCA occlusion 8
hours