“lymph node fna: the multiparametric approach” the xxxii...
TRANSCRIPT
“Lymph node FNA: the multiparametric approach”
The XXXII International Academy of Pathology Congress
Dead Sea, Jordan, October 14-18, 2018
Mousa Al-Abbadi, MD, CPE, CPHQ, FCAP, FIACProfessor of Pathology & Cytopathology
University of Jordan
I declare No conflict of interest
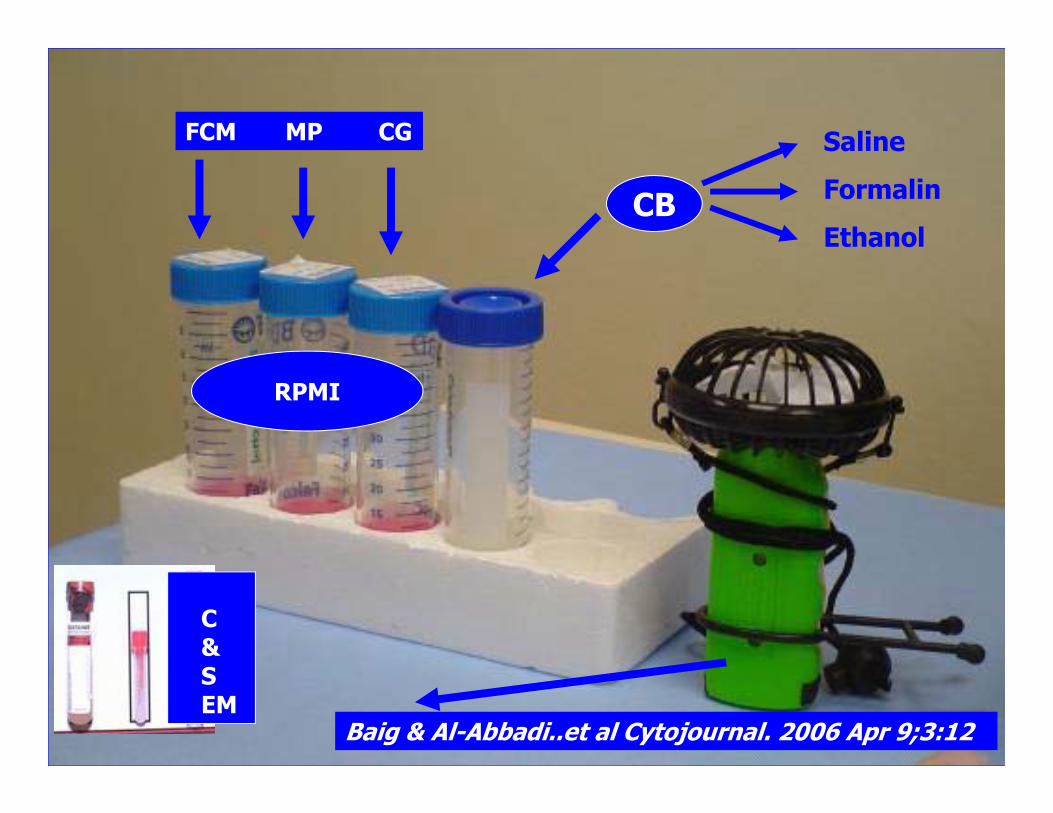
Baig & Al-Abbadi..et al Cytojournal. 2006 Apr 9;3:12
FCM MP CG
CB
RPMI
SalineFormalinEthanol
C&SEM
Sensitivity & specificitySensitivity: 80-90%Specificity: 99-100%Our data:
- FNA performed by non-pathologists: 81% sensitivity and 99% specificity
- FNA by pathologist: 96% sense., 100% spec.
Al-Abbadi & Saleh, CAP annual meeting, Chicago Abstract 2006
Sensitivity & specificitySensitivity: 80-90%Specificity: 99-100%Our data:
- FNA performed by non-pathologists: 81% sensitivity and 99% specificity
- FNA by pathologist: 96% sense., 100% spec.
Al-Abbadi & Saleh, CAP annual meeting, Chicago Abstract 2006
IT IS OPERATOR
DEPENDENT
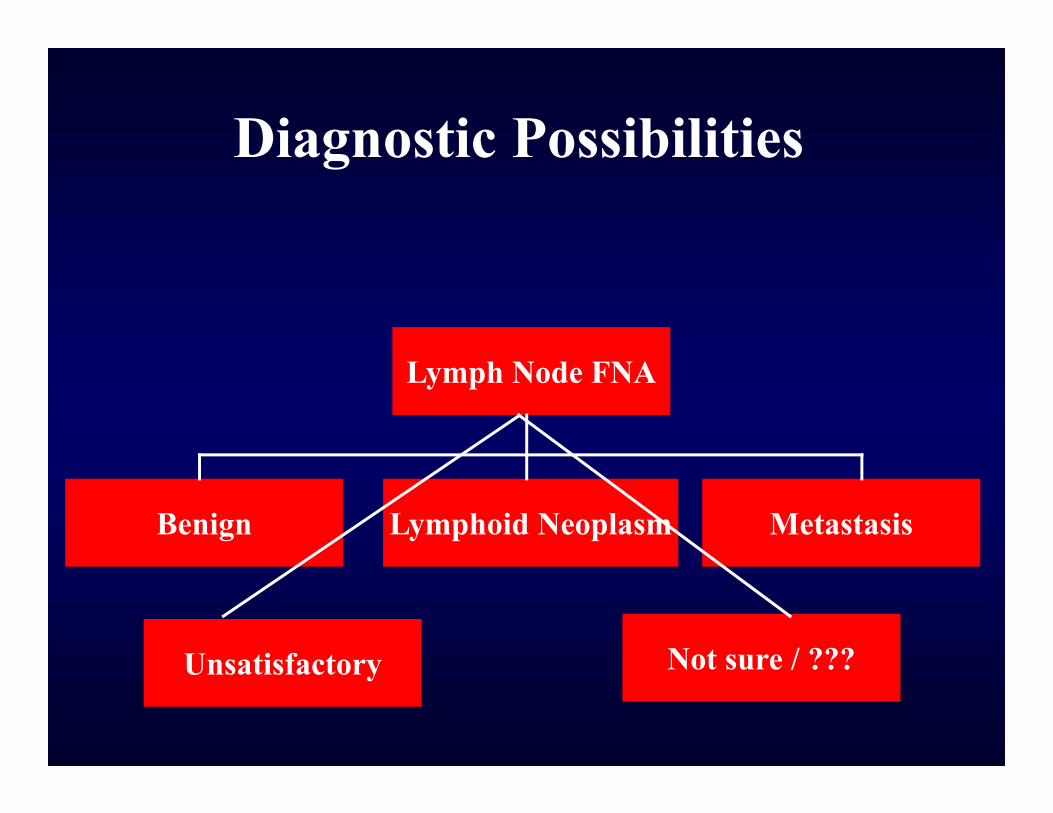
Diagnostic Possibilities
Benign
Lymph Node FNA
Lymphoid Neoplasm Metastasis
Unsatisfactory Not sure / ???
AM I IN A LYMPH NODE?
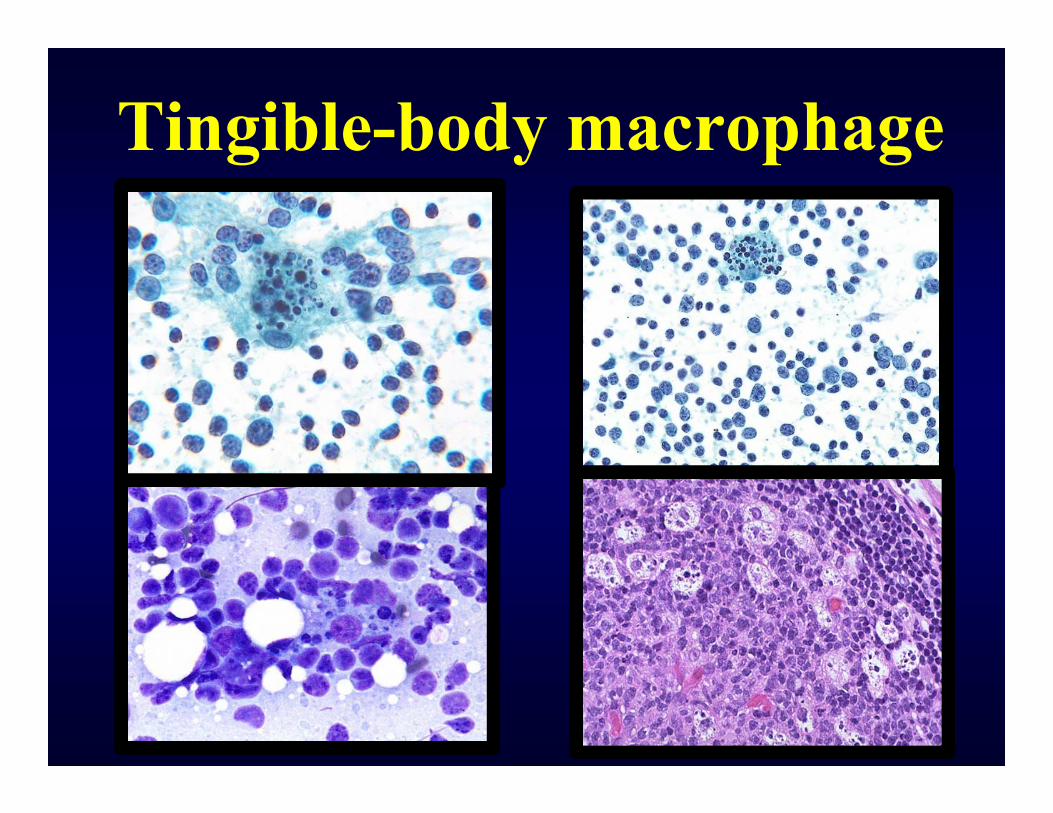
Tingible-body macrophage
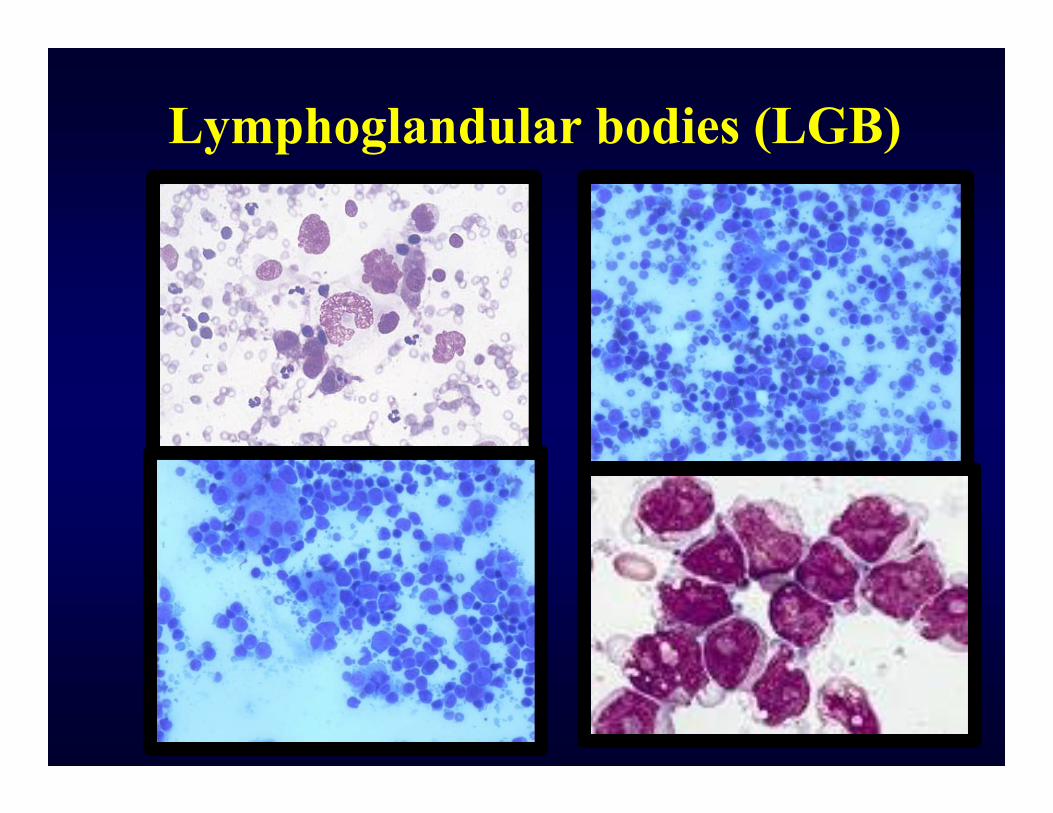
Lymphoglandular bodies (LGB)
Benign Lesions• Reactive hyperplasia• Inflammatory…Infectious• Inflammatory…Non
Infectious• Benign lymphoid disorders
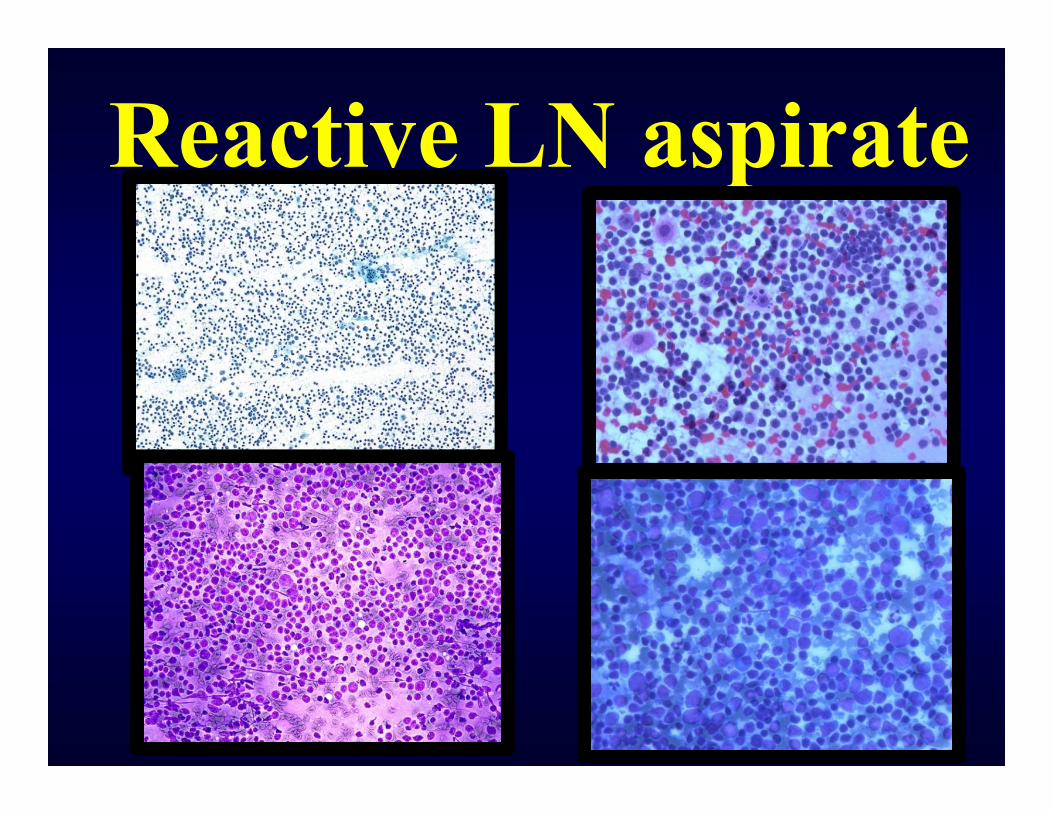
Reactive LN aspirate
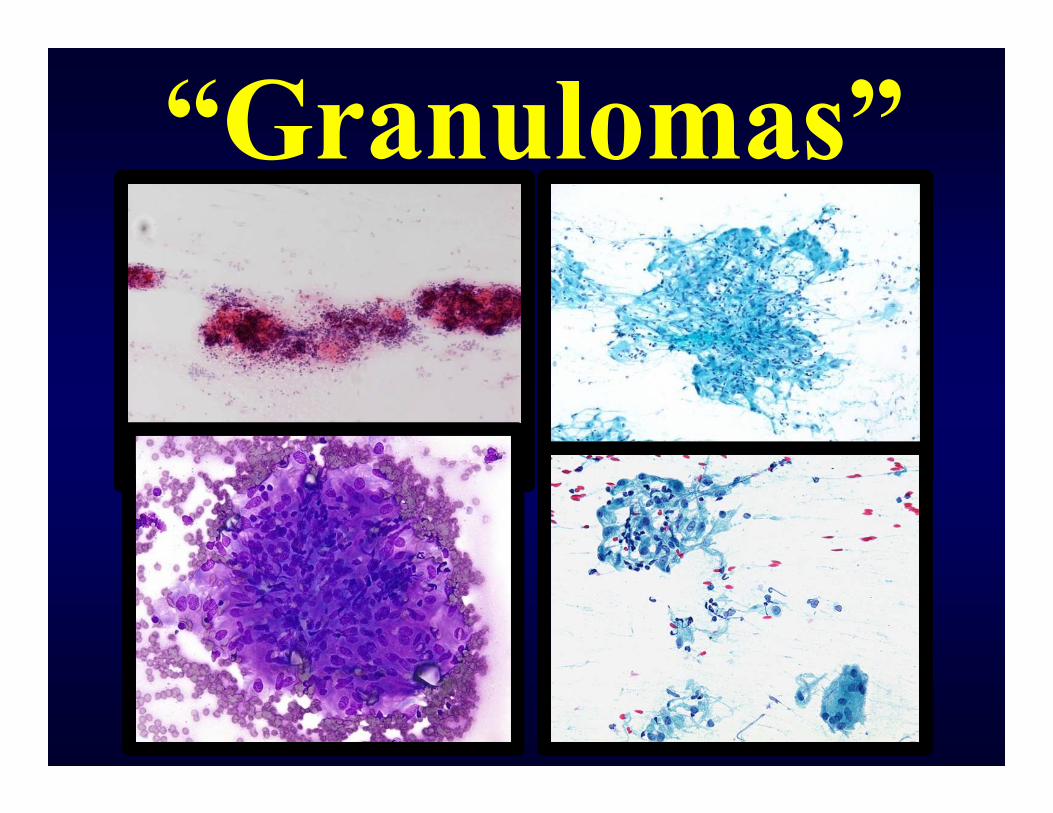
“Granulomas”
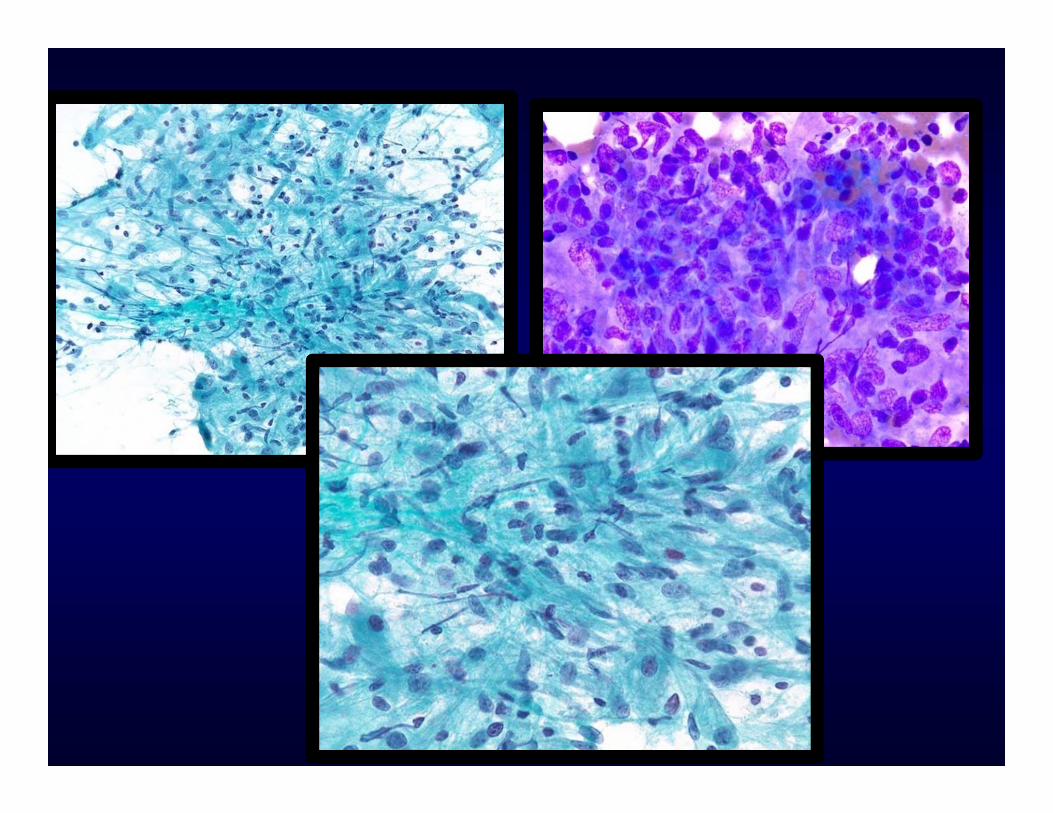
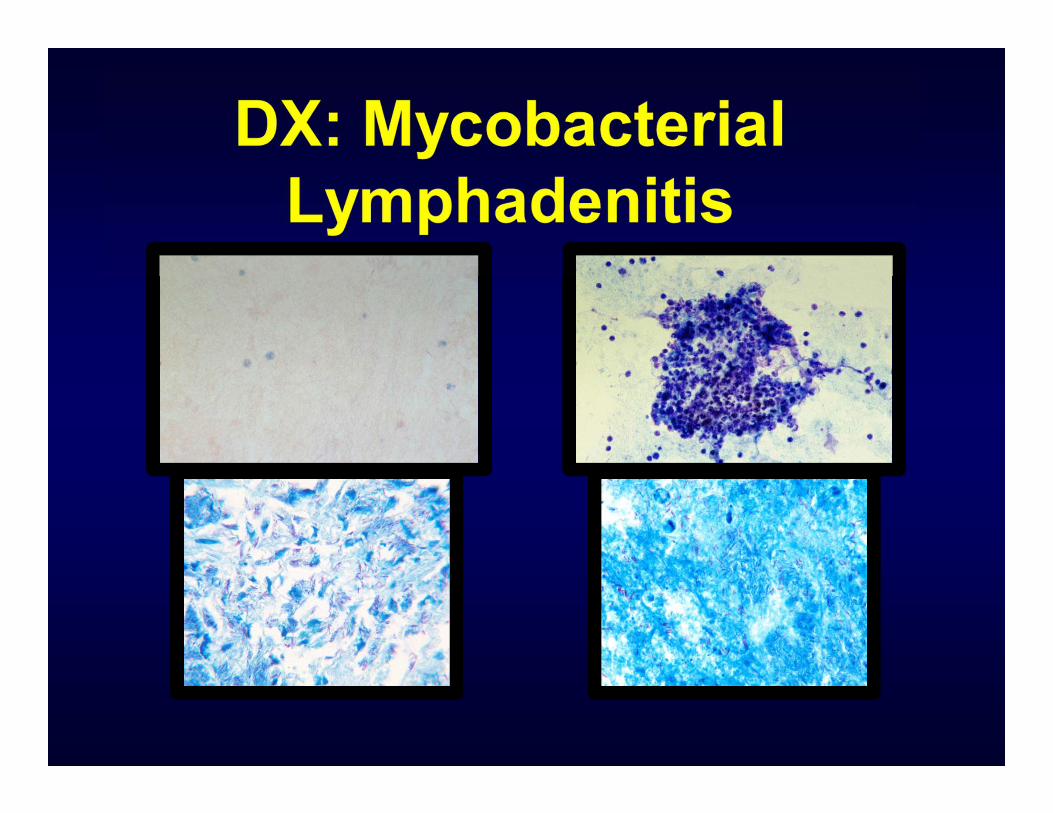
Approach to Granulomatous lymphadenitis :
• Triage on site• Immediate smears evaluation• Smears for AFB and other stains• Material sent for culture and PCR• If AFB + ve…cancel PCR and keep
culture• If AFB –ve …proceed with PCR and
culture
Non Hodgkin lymphomaMONOTONY
MONOTONOUS
Ancillary studies help to:• Lymphoid vs non-lymphoid• Clonality (FCM)• Sub classification• Grading (s-phase, DNA, cell size)• Reed-Sternberg cells (IHC)• PCR, Southern Blot A, FISH,
Cytogenetic studies (T-cell)
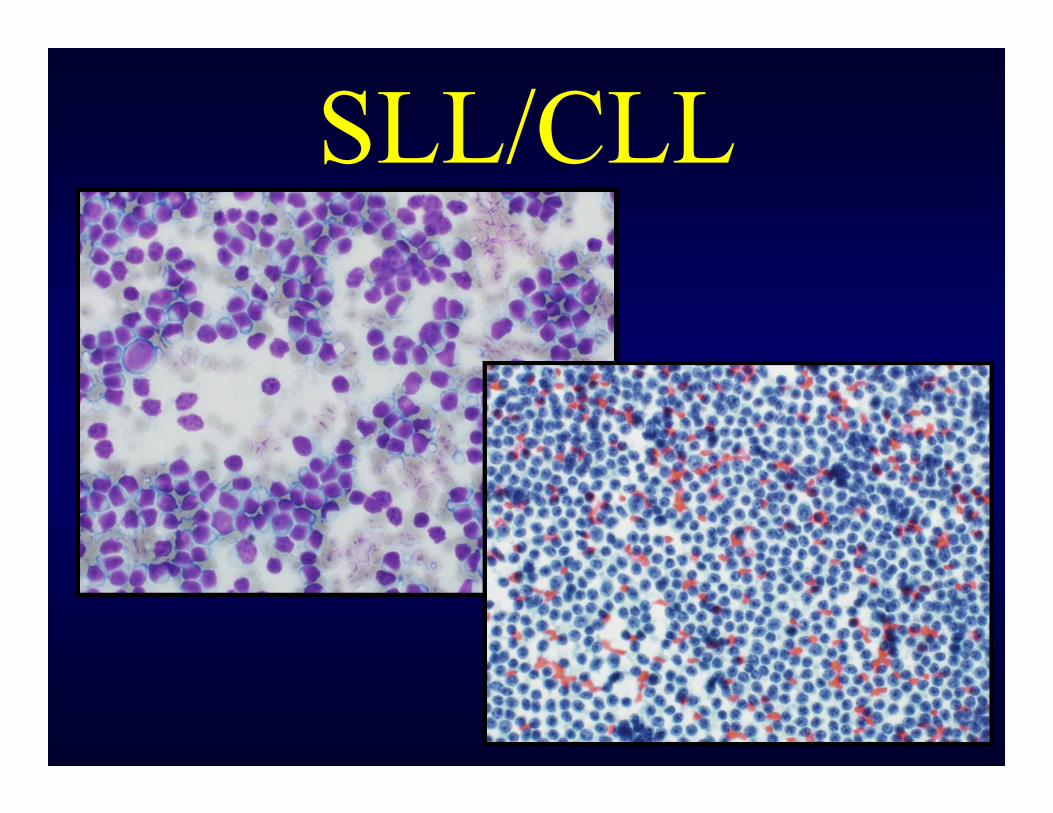
SLL/CLL
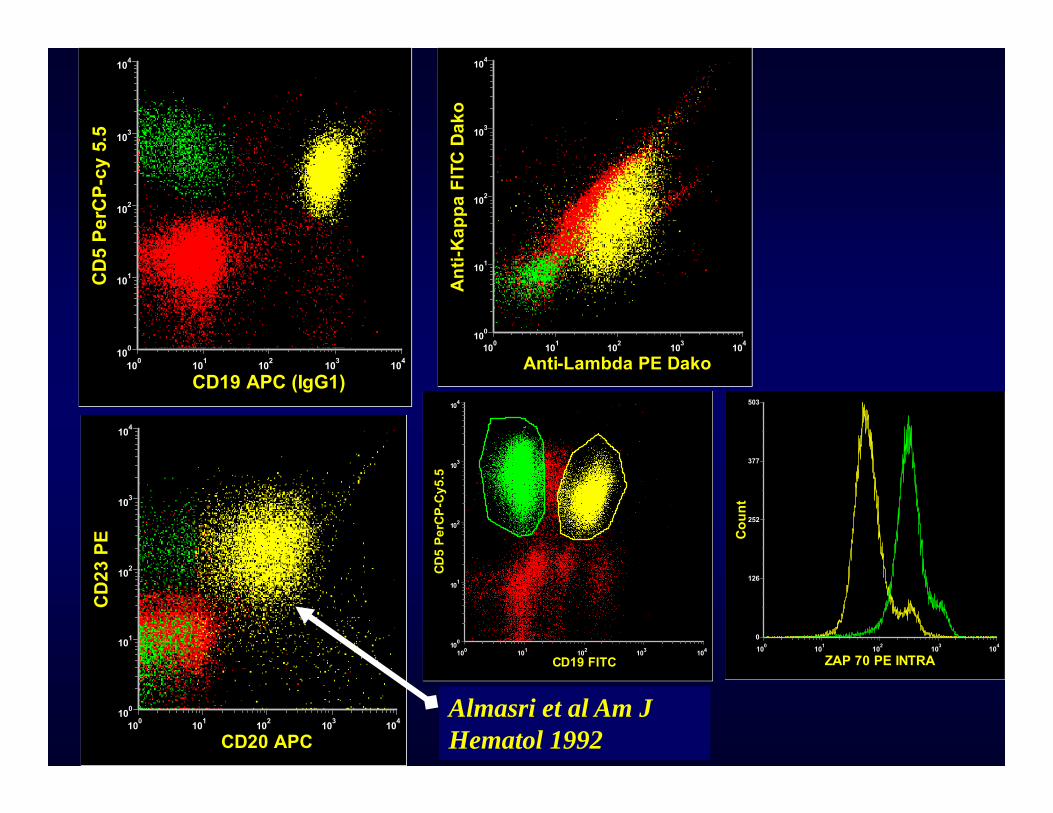
CD19 APC (IgG1)
CD5
PerC
P-cy
5.5
100 101 102 103 104100
101
102
103
104
Anti-Lambda PE Dako
Anti-
Kap
pa F
ITC
Dako
100 101 102 103 104100
101
102
103
104
CD20 APC
CD23
PE
100 101 102 103 104100
101
102
103
104
CD19 FITC
CD5
PerC
P-C
y5.5
100 101 102 103 104100
101
102
103
104
ZAP 70 PE INTRA
Coun
t
100 101 102 103 1040
126
252
377
503
Almasri et al Am J Hematol 1992
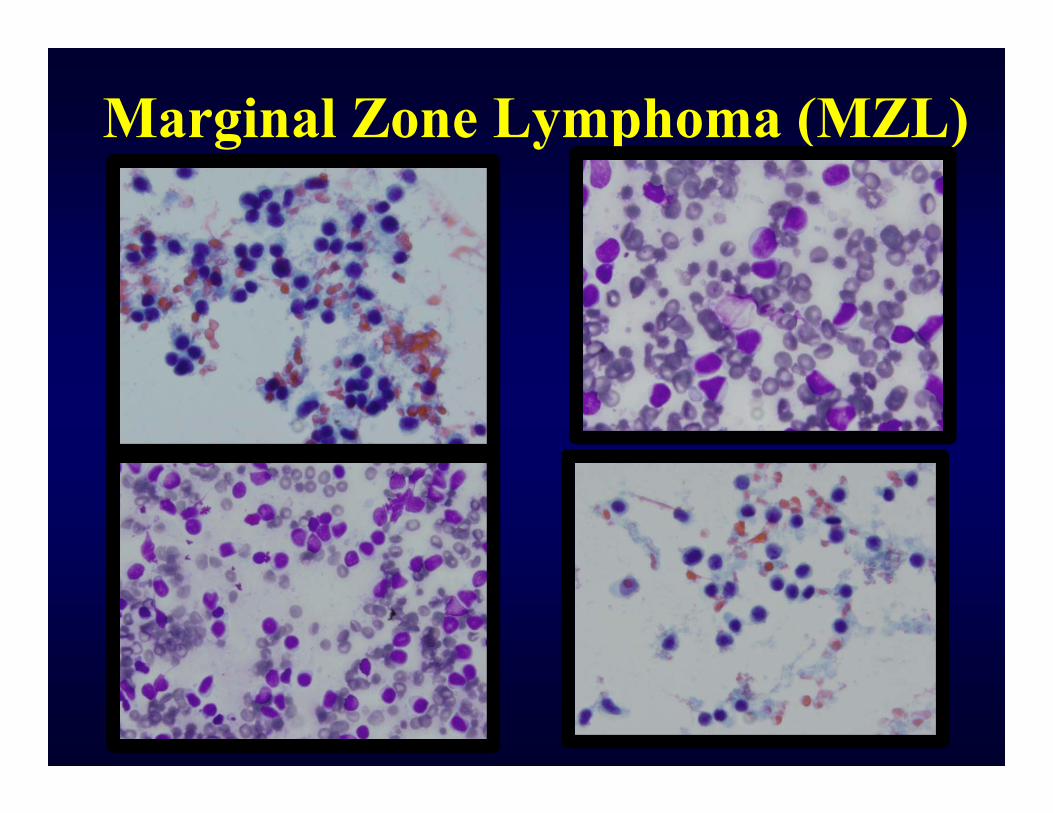
Marginal Zone Lymphoma (MZL)
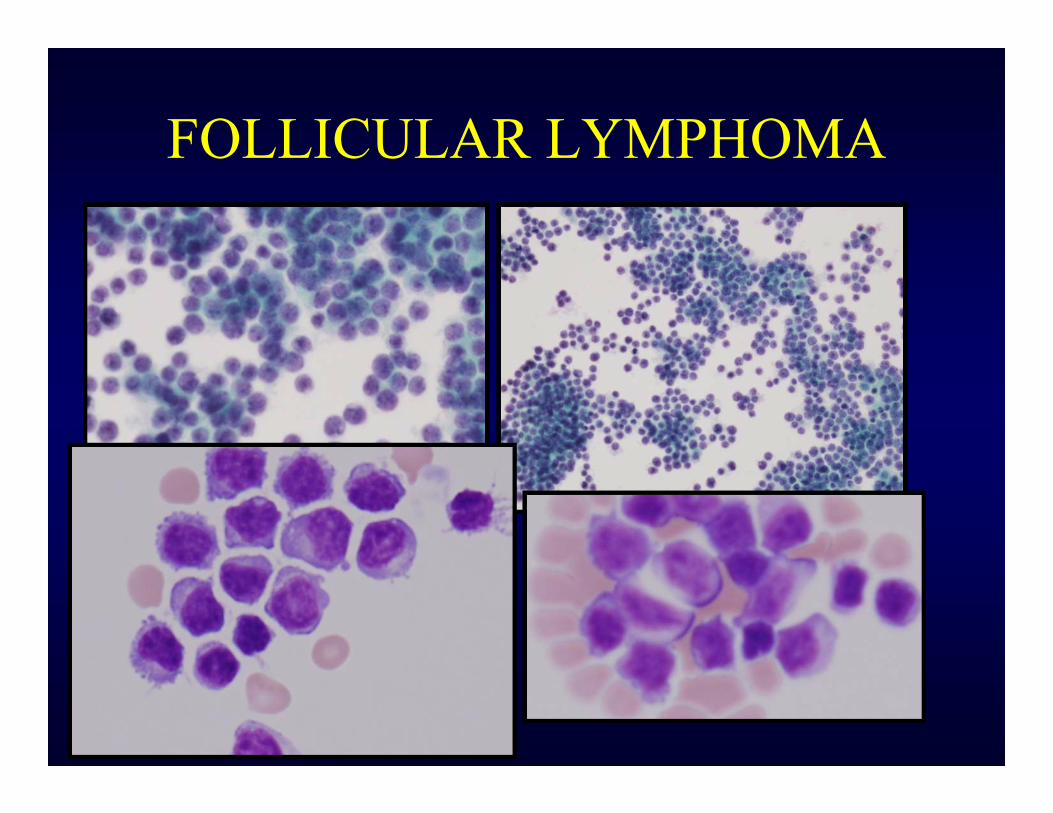
FOLLICULAR LYMPHOMA
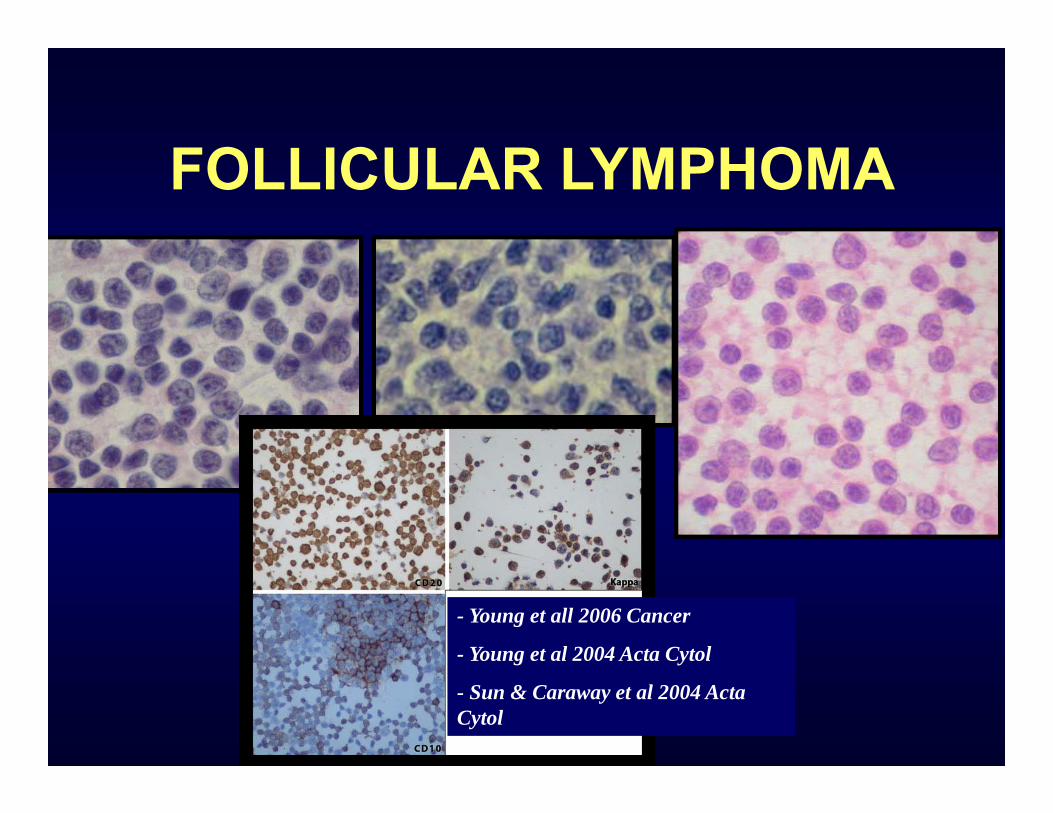
FOLLICULAR LYMPHOMA
- Young et all 2006 Cancer
- Young et al 2004 Acta Cytol
- Sun & Caraway et al 2004 Acta Cytol

Mantle Cell Lymphoma
CD20 +
CD5 +
Cyclin D1
T(11;14)
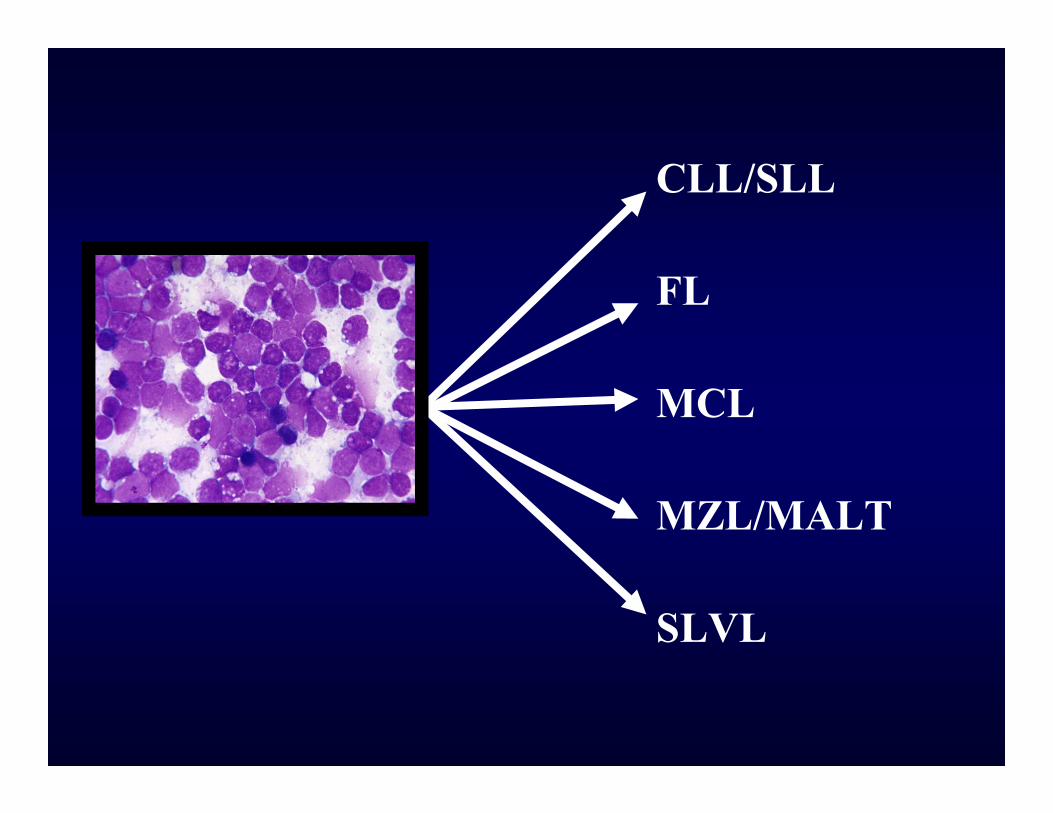
CLL/SLL
FL
MCL
MZL/MALT
SLVL
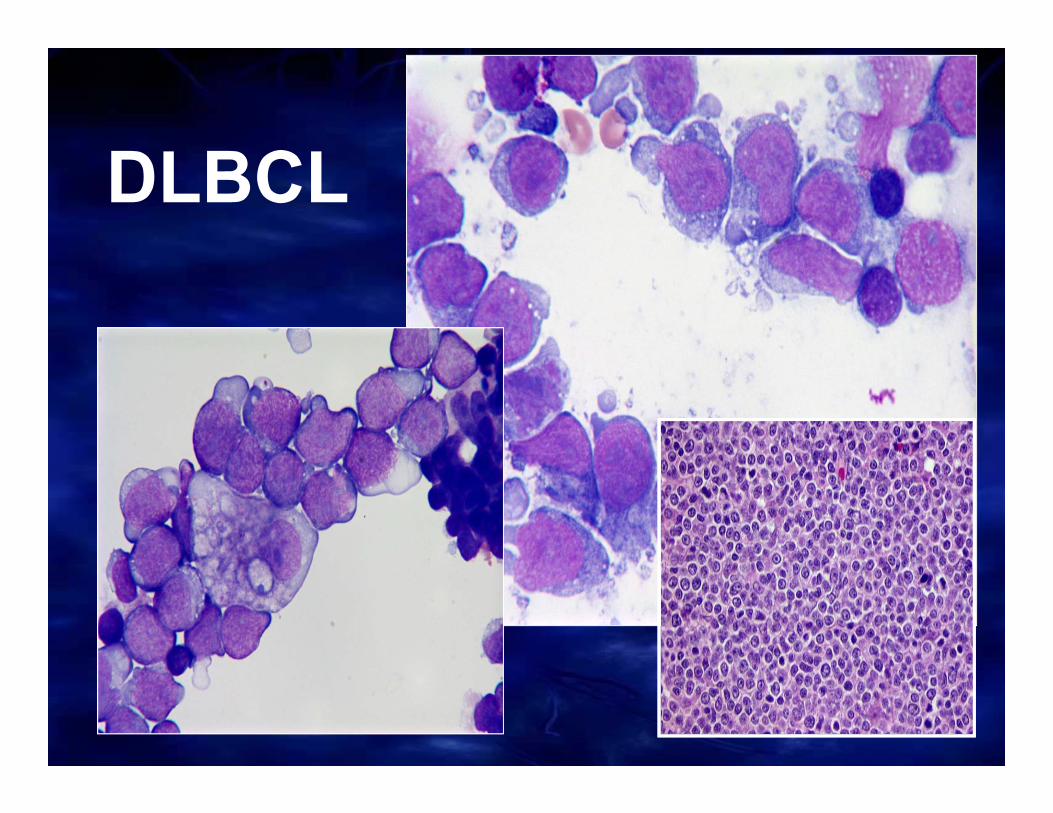
DLBCL
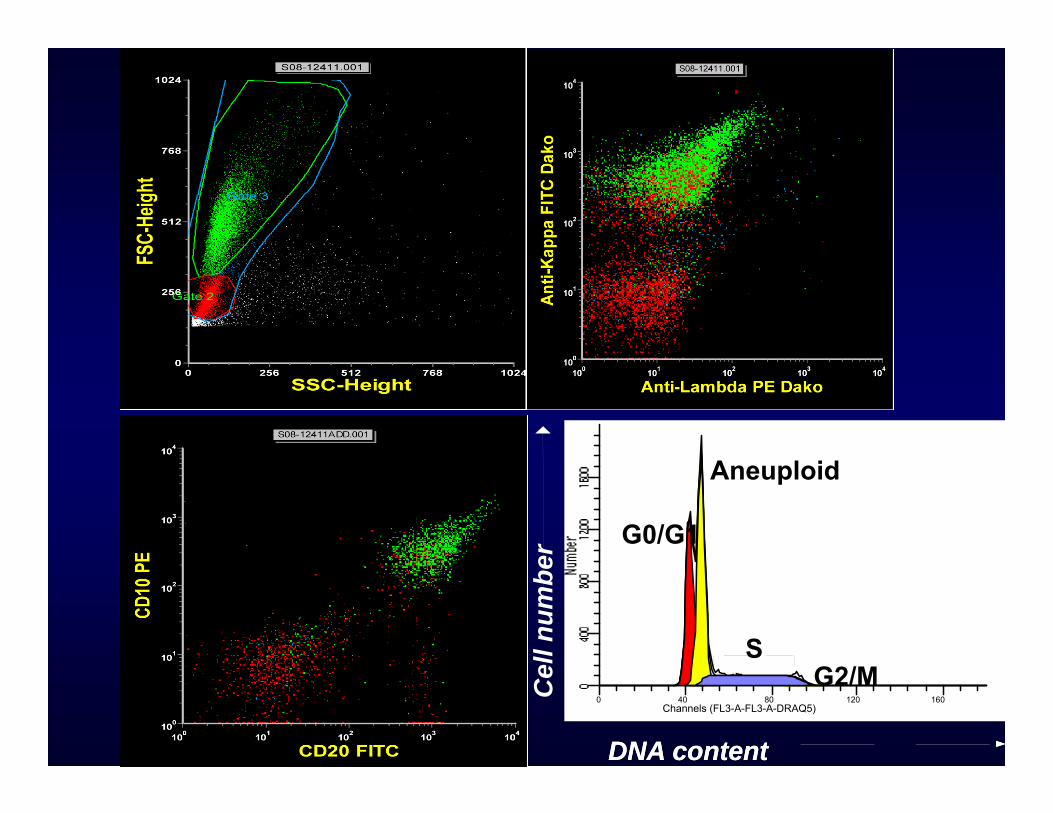
Channels (FL3-A-FL3-A-DRAQ5)0 40 80 120 160C
ell n
umbe
r
DNA contentDNA content
G0/G1
G2/MS
Aneuploid
Tumor specific S-phase=20%
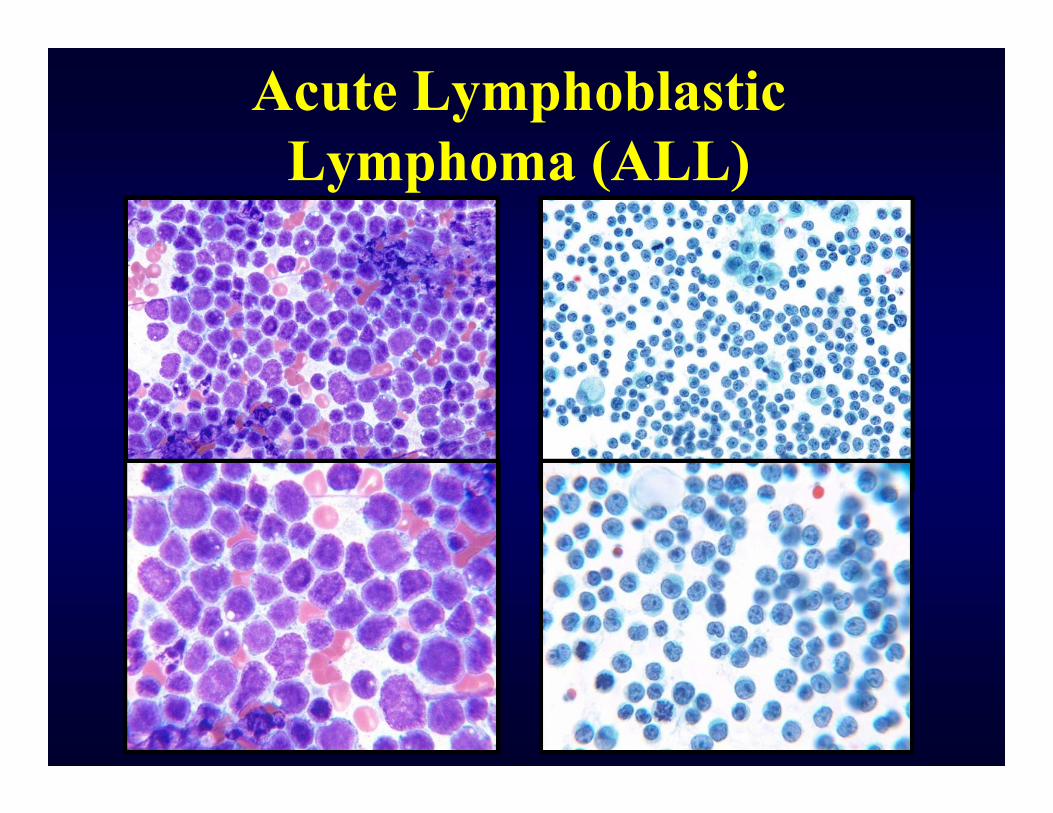
Acute Lymphoblastic Lymphoma (ALL)
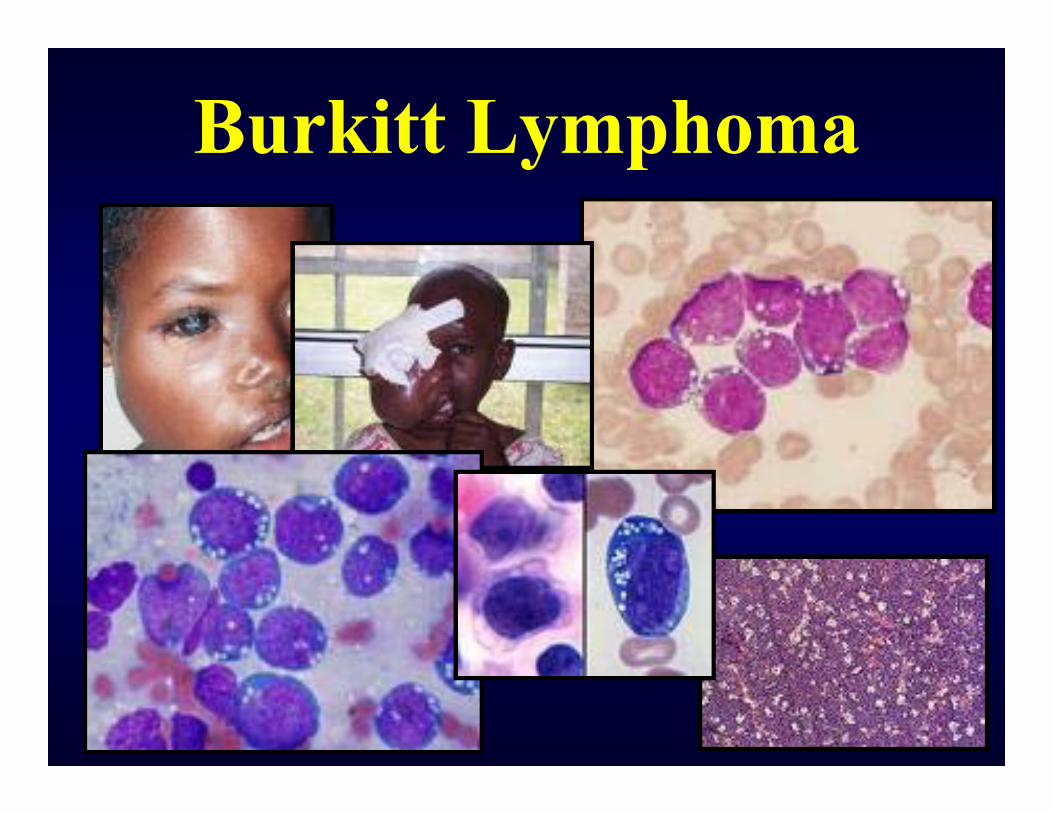
Burkitt Lymphoma

KI-67
Burkitt Lymphoma
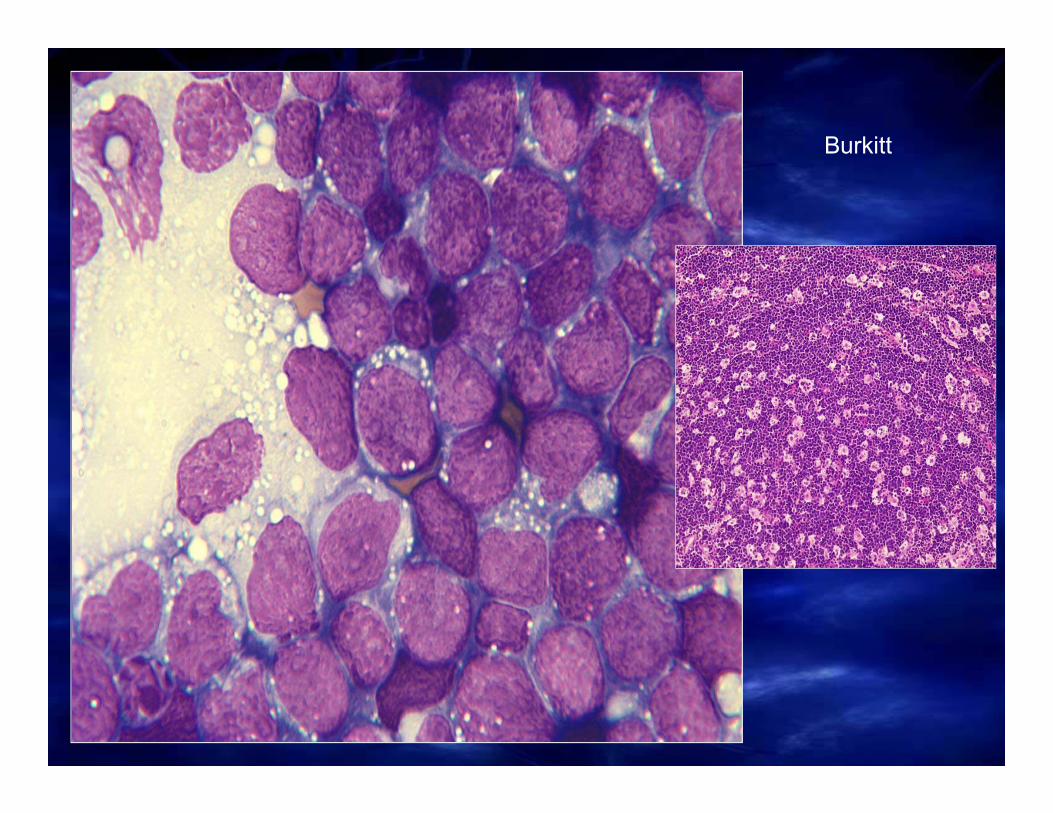
Burkitt
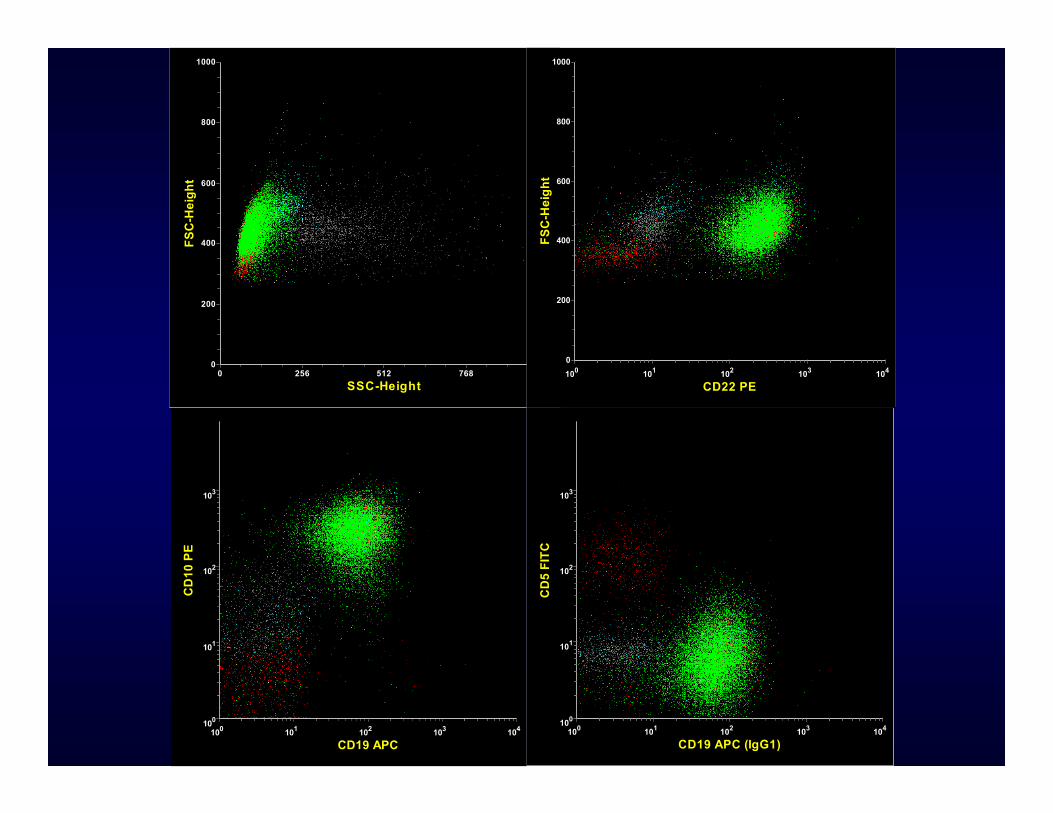
SSC-Height0 256 512 768 1024
FSC
-Hei
ght
0
200
400
600
800
1000
CD19 APC010 110 210 310 410
CD
10 P
E
010
110
210
310
CD19 APC (IgG1)010 110 210 310 410
CD
5 FI
TC
010
110
210
310
CD22 PE010 110 210 310 410
FSC
-Hei
ght
0
200
400
600
800
1000
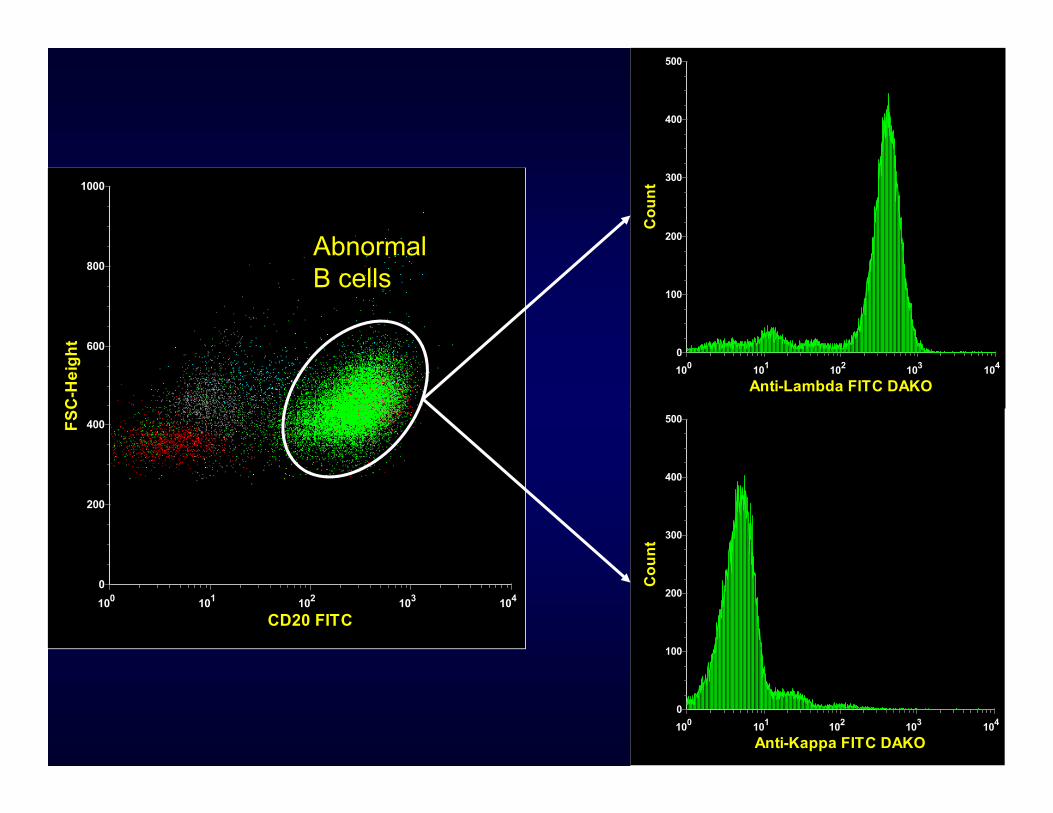
CD20 FITC010 110 210 310 410
FSC
-Hei
ght
0
200
400
600
800
1000
Anti-Kappa FITC DAKO010 110 210 310 410
Cou
nt
500
400
300
200
100
0
Anti-Lambda FITC DAKO010 110 210 310 410
Cou
nt
500
400
300
200
100
0
Abnormal B cells
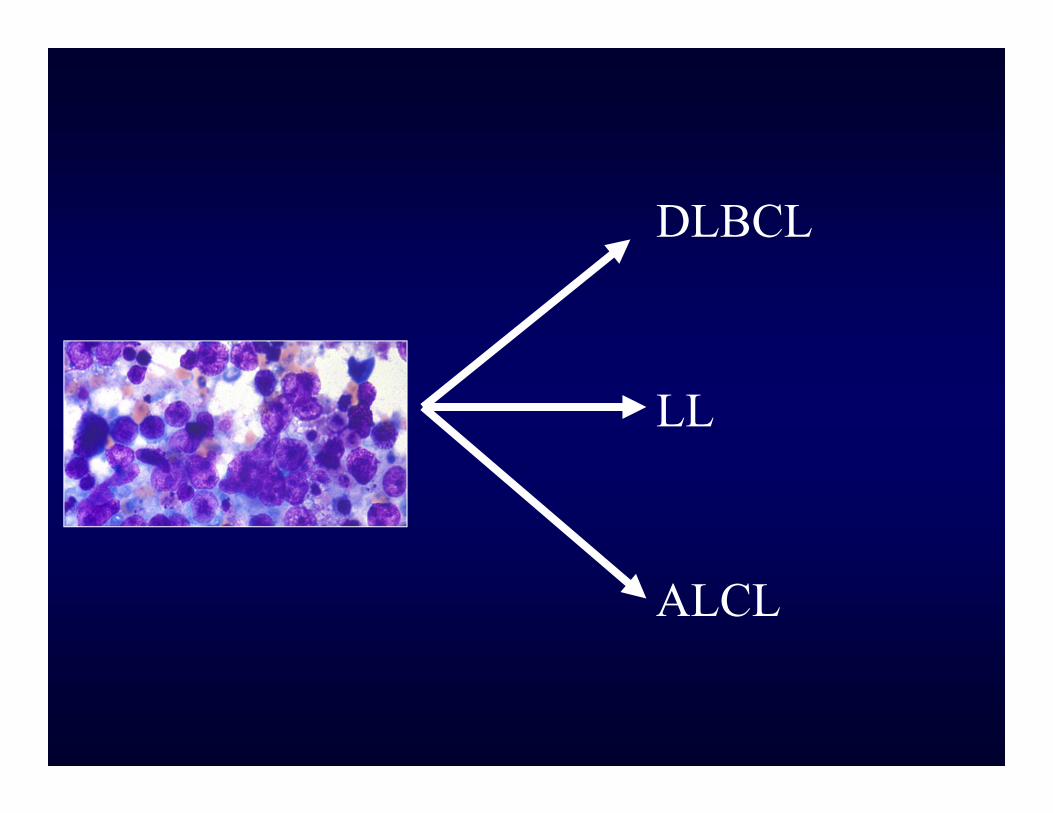
DLBCL
LL
ALCL
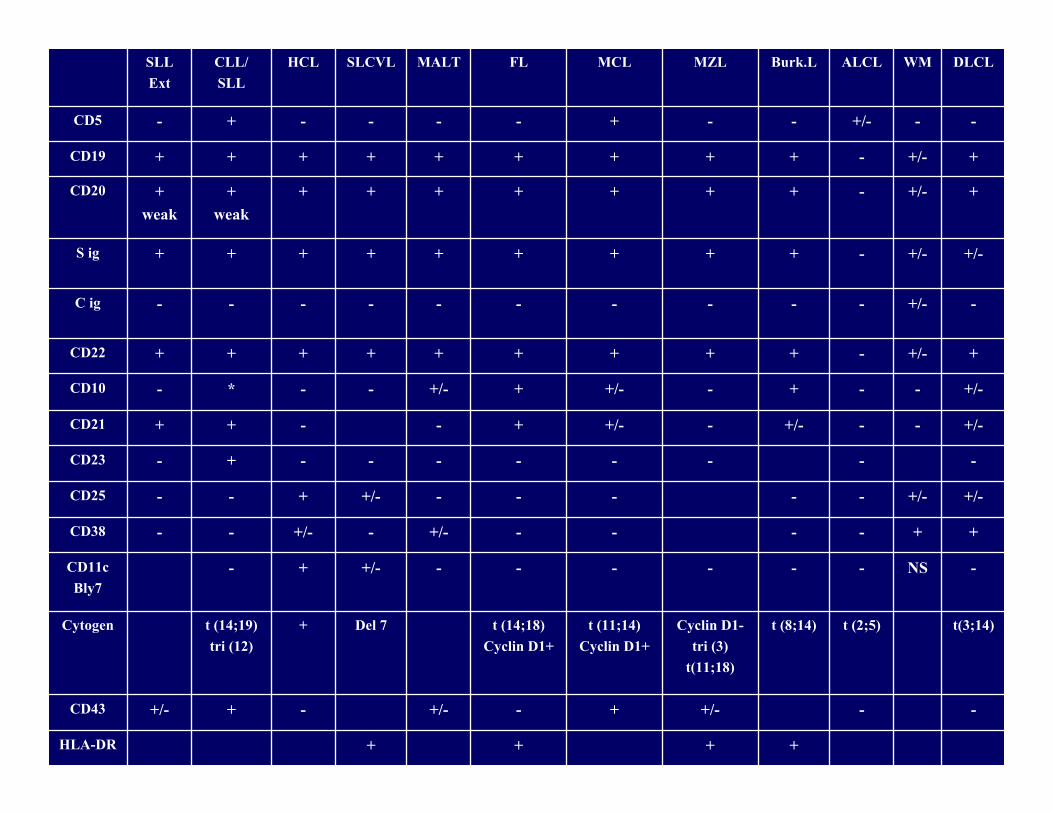
SLLExt
CLL/SLL
HCL SLCVL MALT FL MCL MZL Burk.L ALCL WM DLCL
CD5 - + - - - - + - - +/- - -
CD19 + + + + + + + + + - +/- +
CD20 +weak
+weak
+ + + + + + + - +/- +
S ig + + + + + + + + + - +/- +/-
C ig - - - - - - - - - - +/- -
CD22 + + + + + + + + + - +/- +
CD10 - * - - +/- + +/- - + - - +/-
CD21 + + - - + +/- - +/- - - +/-
CD23 - + - - - - - - - -
CD25 - - + +/- - - - - - +/- +/-
CD38 - - +/- - +/- - - - - + +
CD11cBly7
- + +/- - - - - - - NS -
Cytogen t (14;19)tri (12)
+ Del 7 t (14;18)Cyclin D1+
t (11;14)Cyclin D1+
Cyclin D1-tri (3)
t(11;18)
t (8;14) t (2;5) t(3;14)
CD43 +/- + - +/- - + +/- - -
HLA-DR + + + +
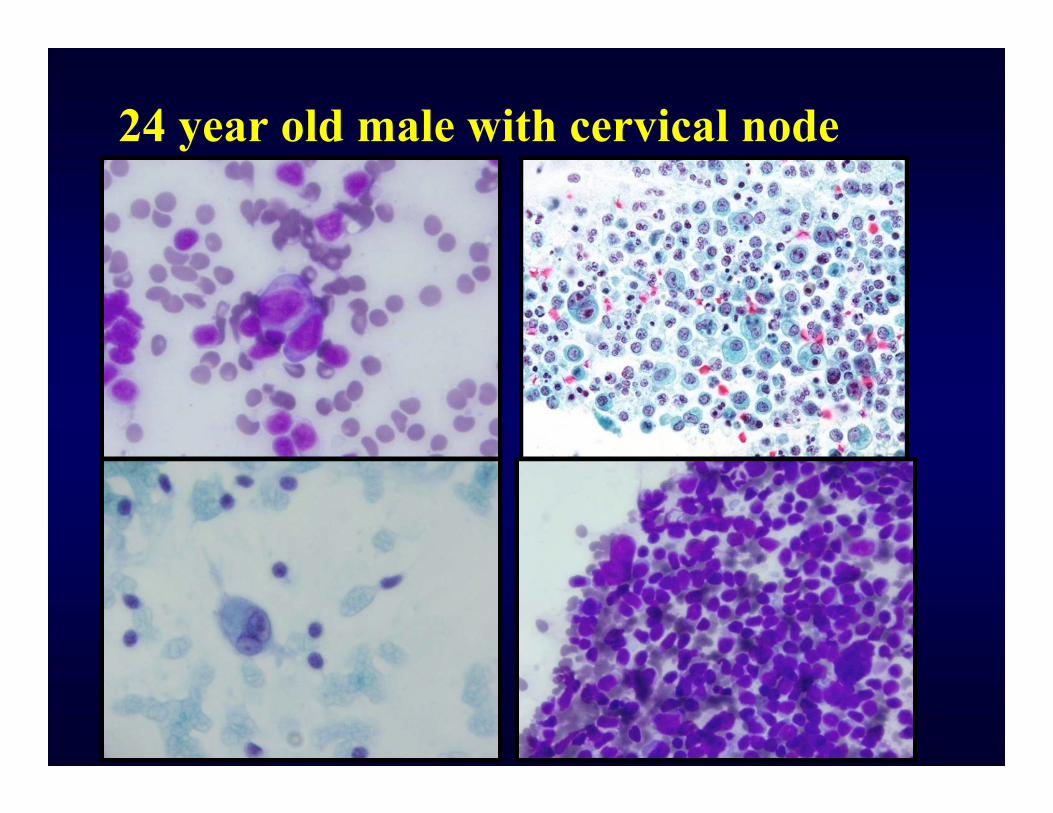
24 year old male with cervical node
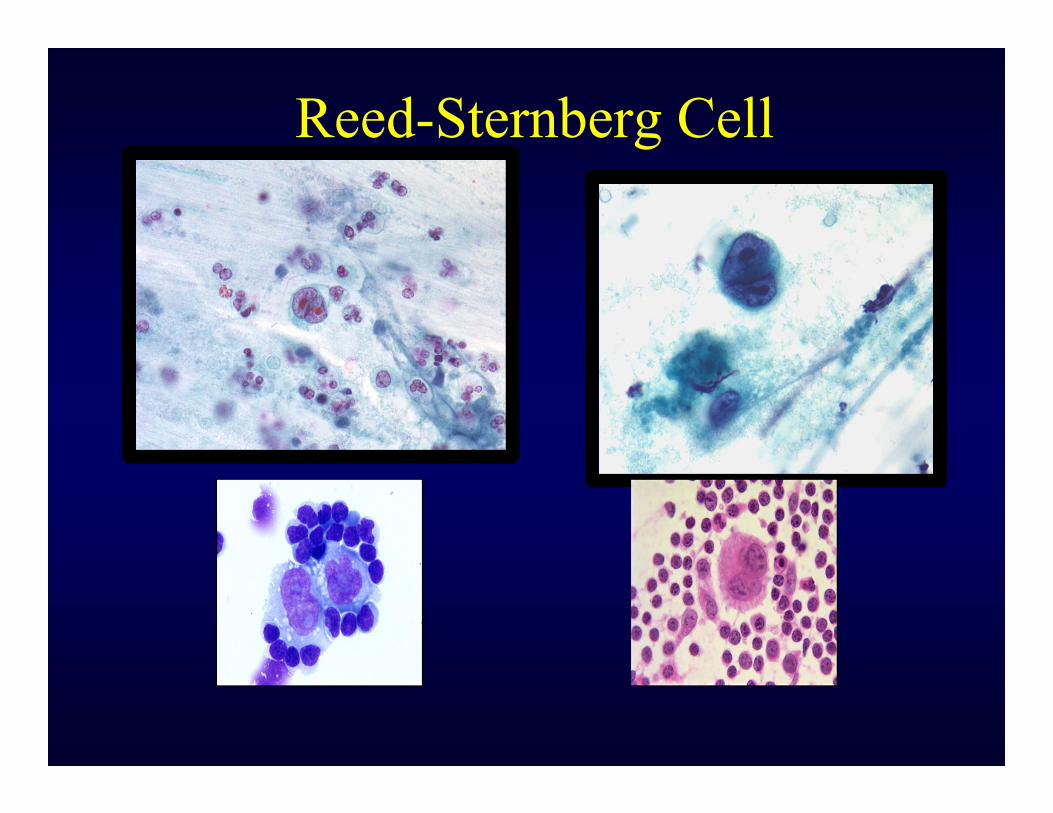
Reed-Sternberg Cell
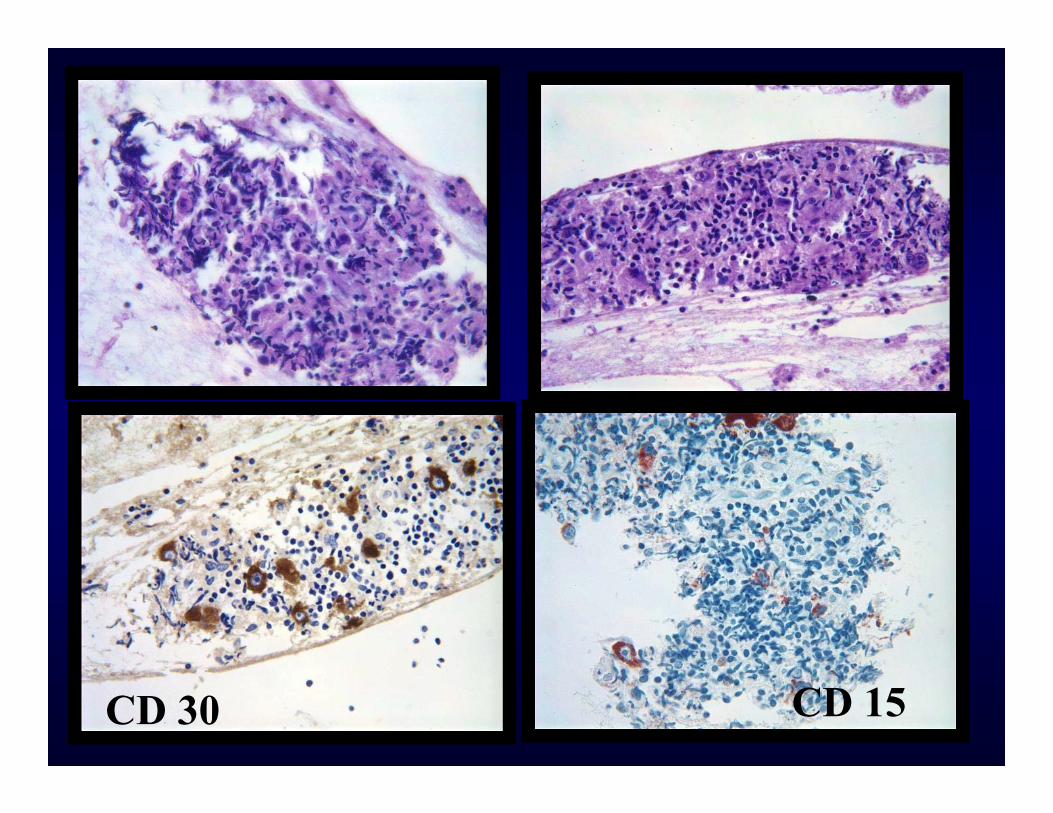
CD 30 CD 15

LCA
CD 20 CD 3
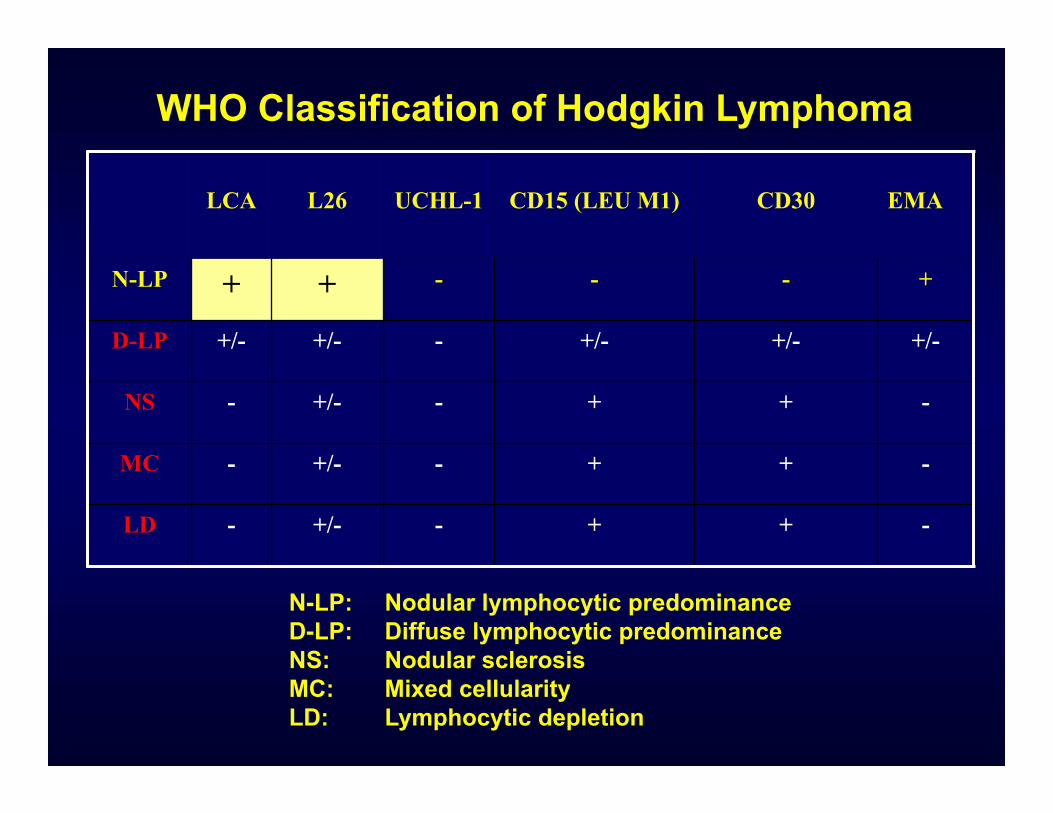
LCA L26 UCHL-1 CD15 (LEU M1) CD30 EMA
N-LP + + - - - +
D-LP +/- +/- - +/- +/- +/-
NS - +/- - + + -
MC - +/- - + + -
LD - +/- - + + -
WHO Classification of Hodgkin Lymphoma
N-LP: Nodular lymphocytic predominanceD-LP: Diffuse lymphocytic predominanceNS: Nodular sclerosisMC: Mixed cellularityLD: Lymphocytic depletion
Cytologic Mimickers of Reed-Sternberg Cells
• Immunoblasts• Megakaryocytes• Dendritic cells• Reactive mesothelial cells• Large cell lymphoma & ALCL cells• Melanoma• Plasmablast (myeloma cells)• Pleomorphic sarcoma & large cell
carcinoma
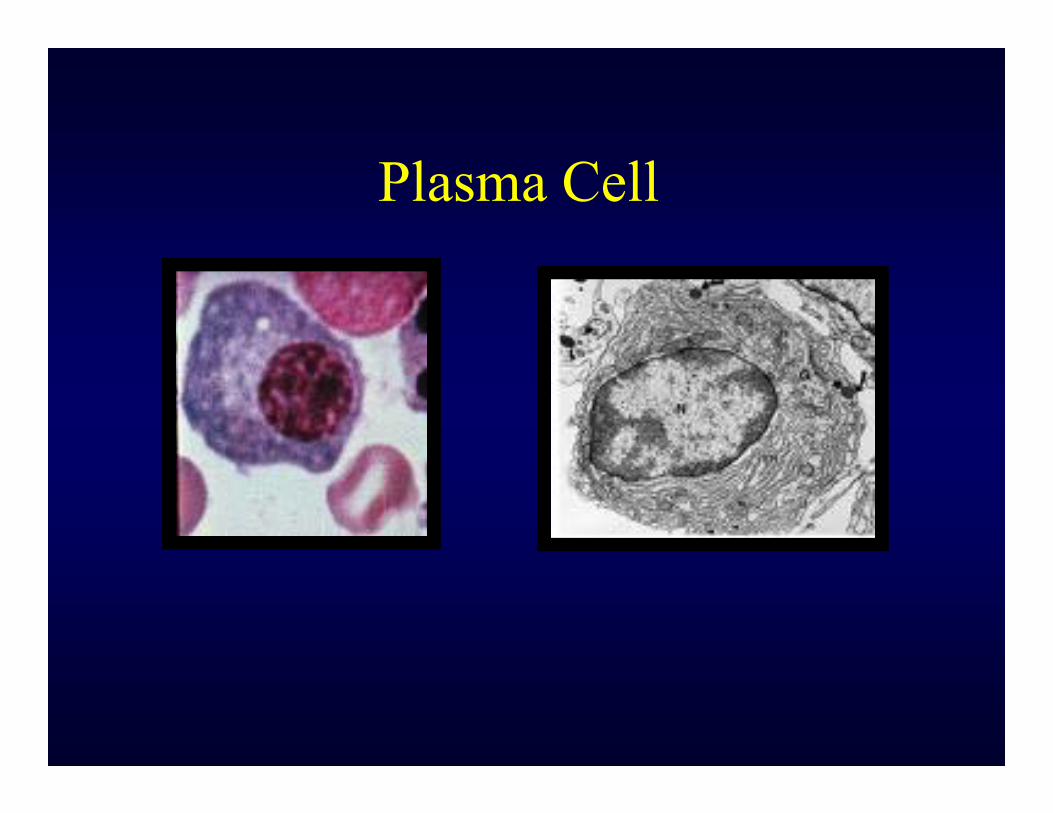
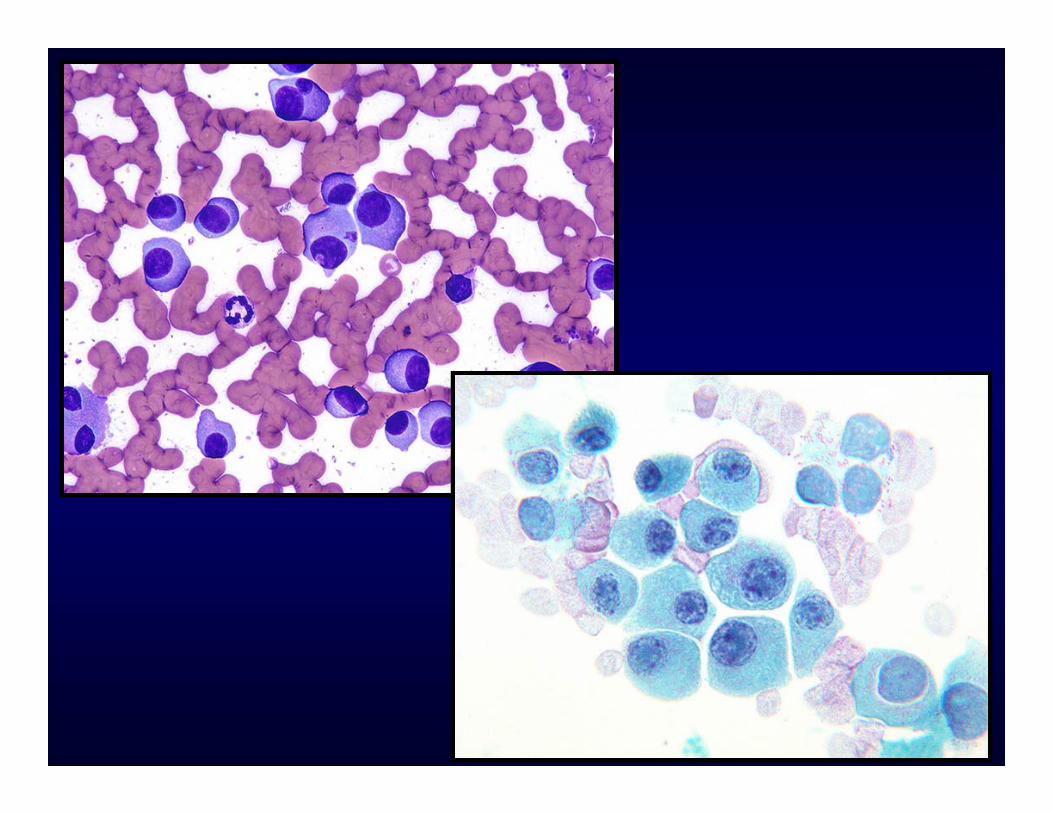
Plasma Cell
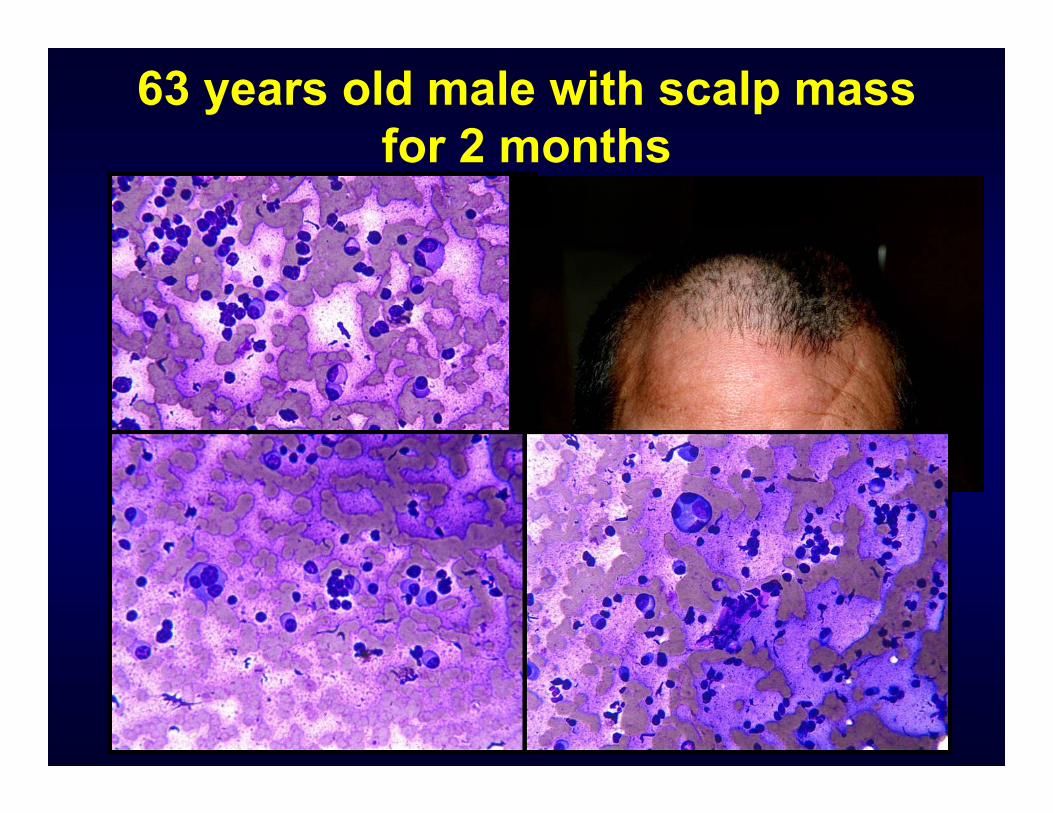
63 years old male with scalp mass for 2 months
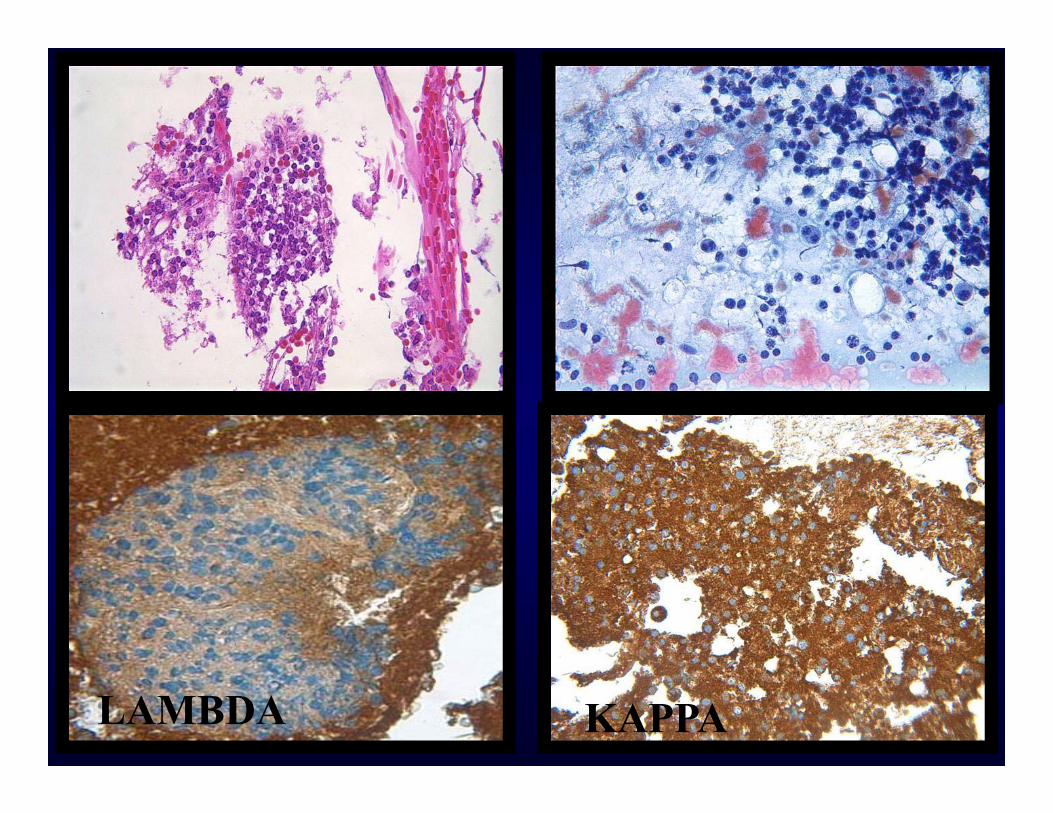
LAMBDA KAPPA
DX: Plasma Cell Neoplasm
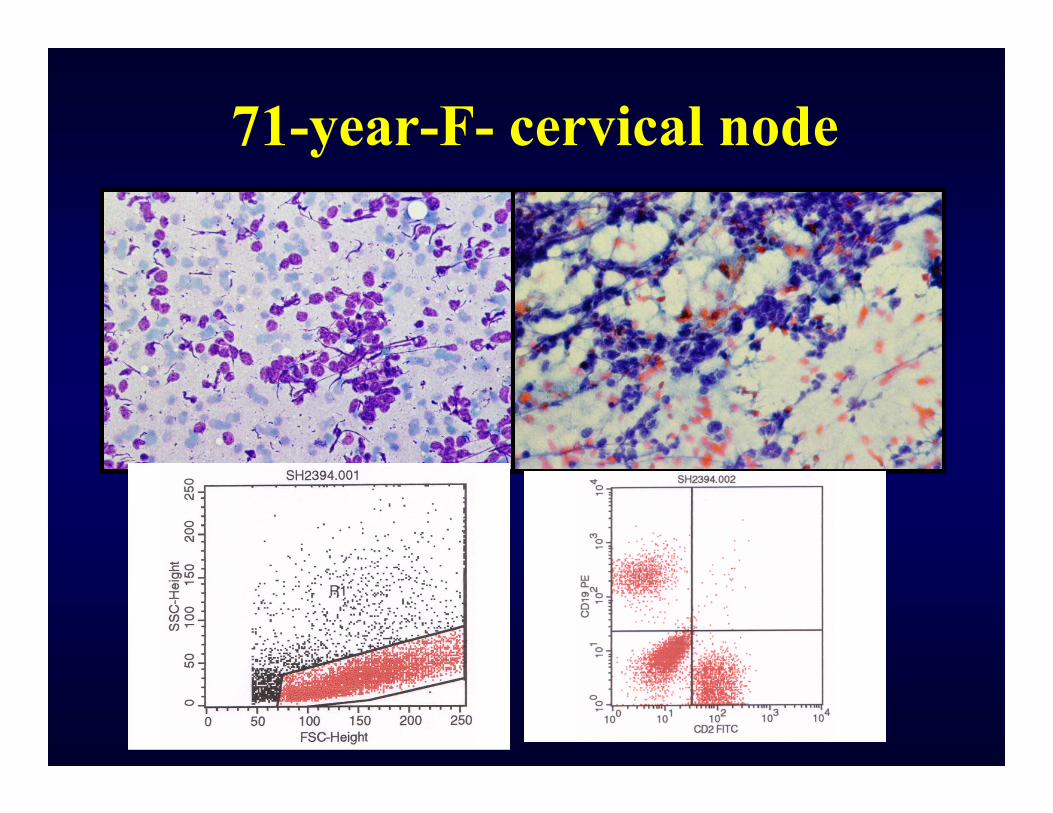
71-year-F- cervical node
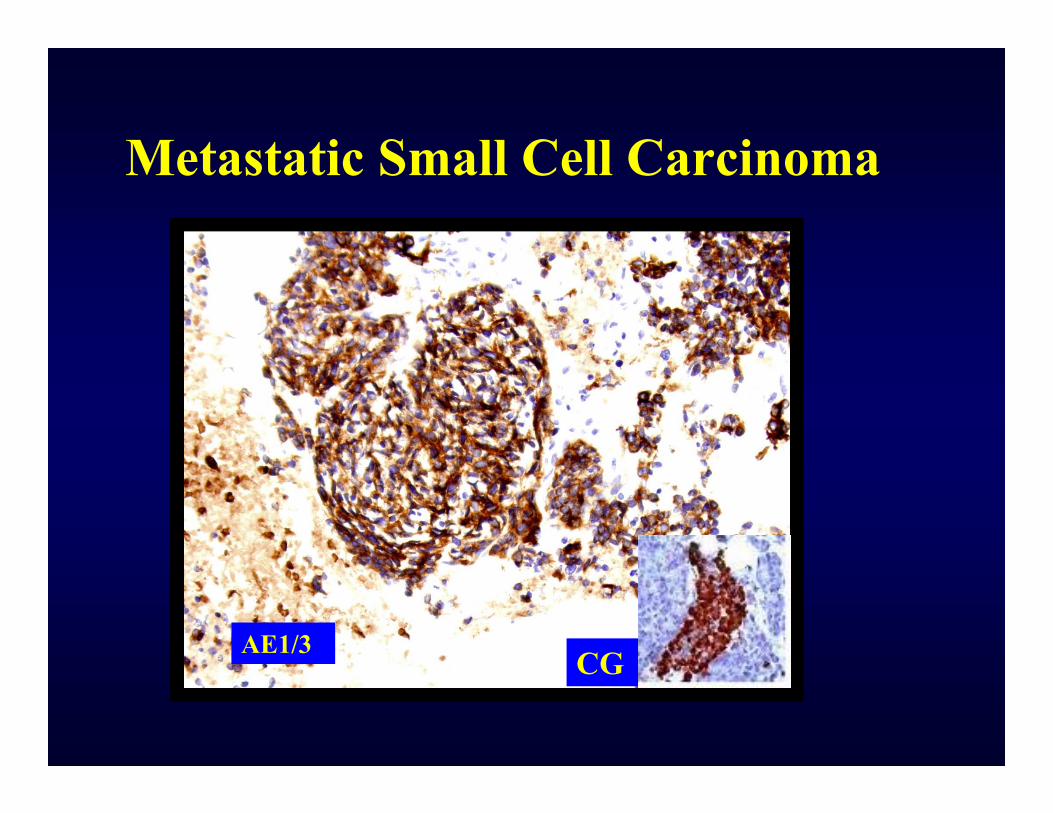
Metastatic Small Cell Carcinoma
Chromogranin CK+
AE1/3CG
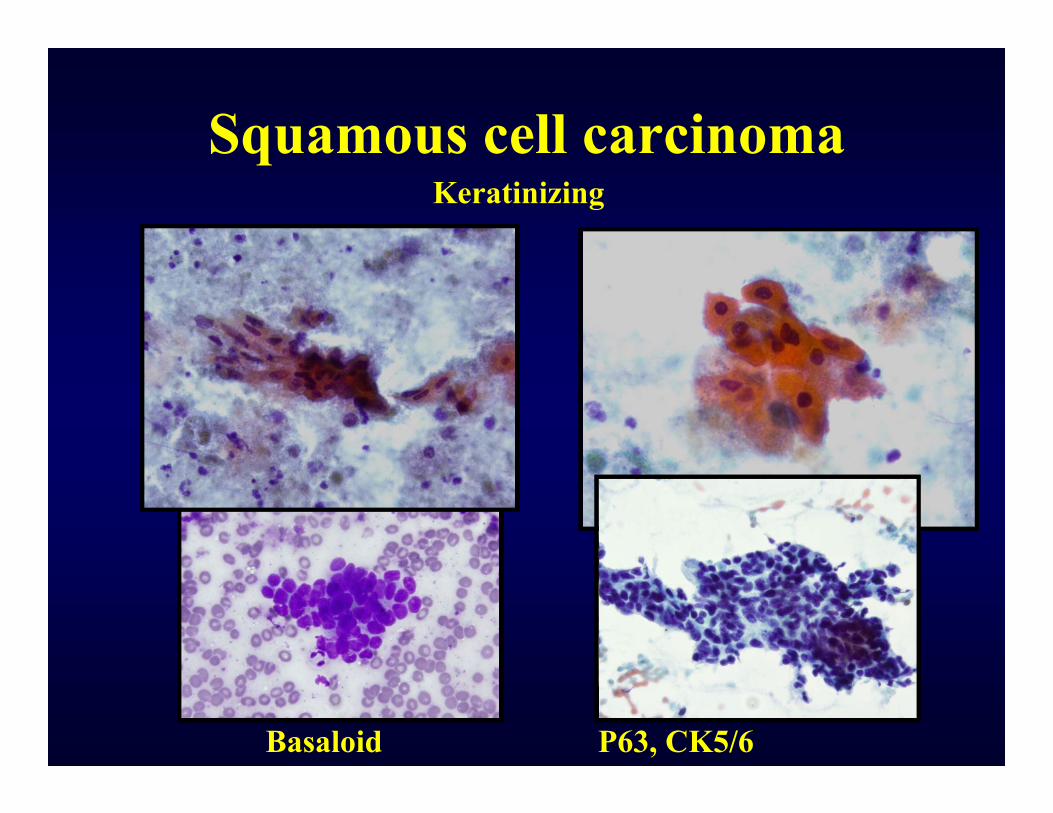
Squamous cell carcinomaKeratinizing
Basaloid P63, CK5/6
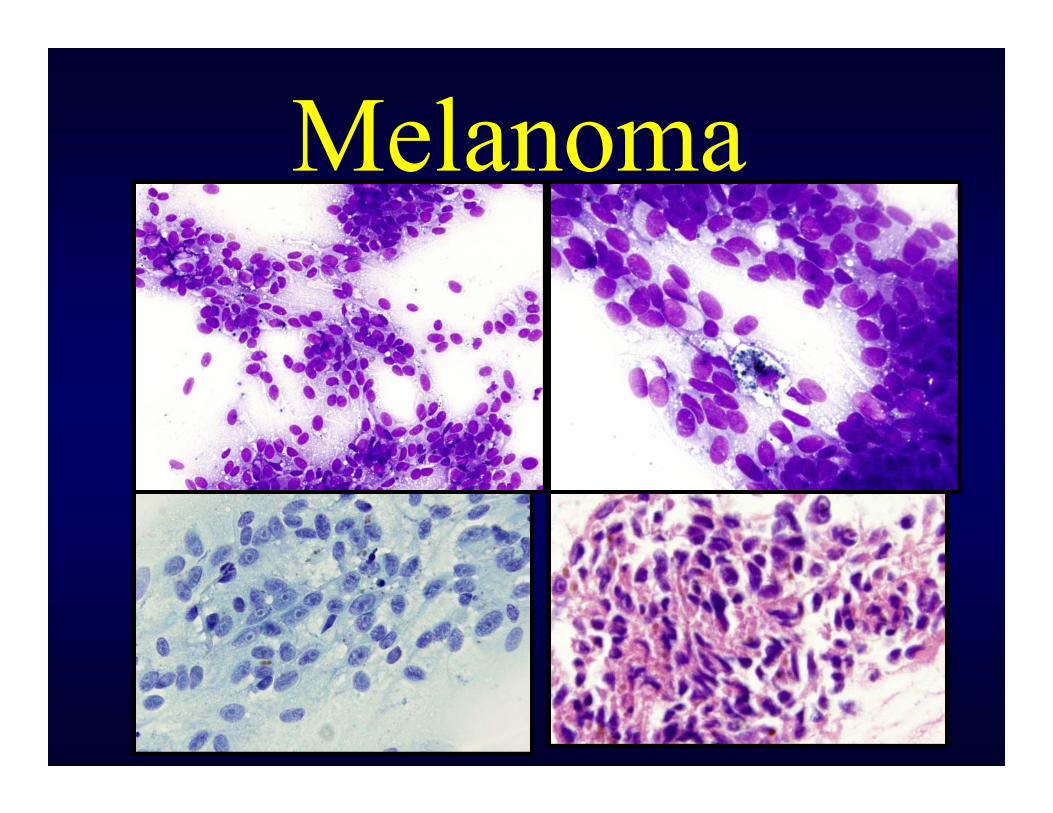
Melanoma
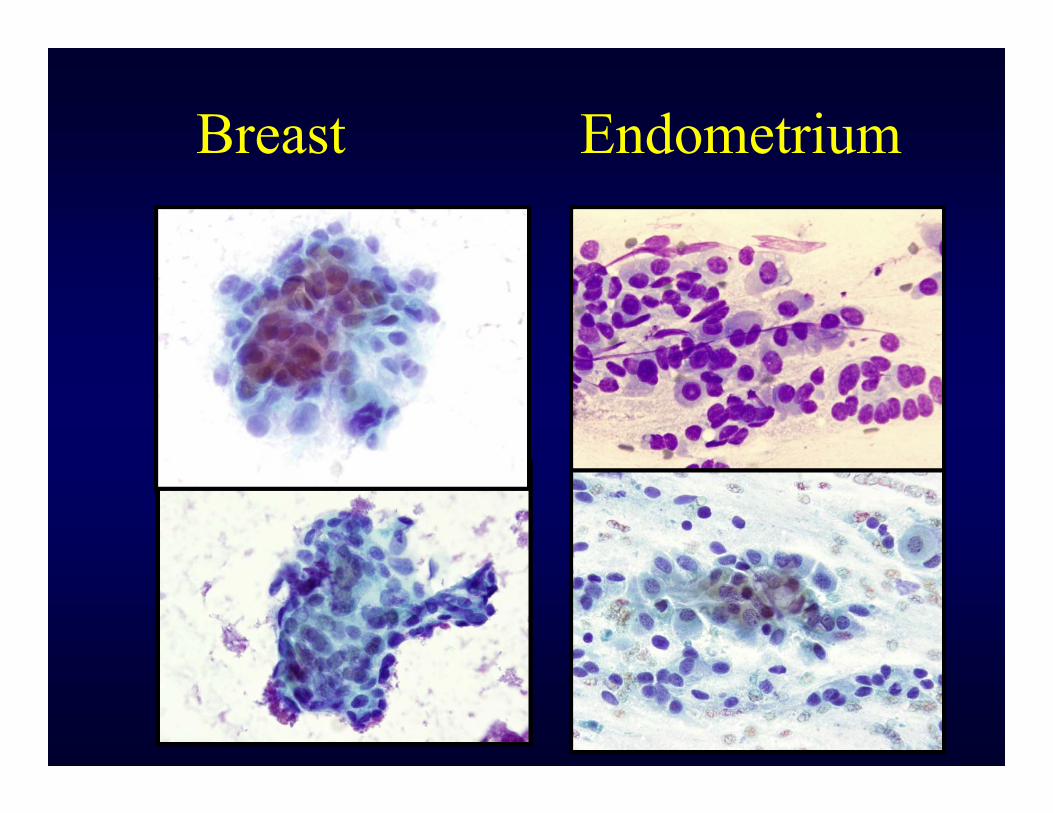
Breast Endometrium
Final message:• Lymph node FNA is the preferred
initial diagnostic procedure; though controversial
• In experienced hands; diagnostic accuracy, sensitivity and specificity are high (operator dependent)
• Proper sampling is key for better sampling and enough material for immunophenotyping and other needed studies
• Benign lesions and non Hodgkin’s lymphomas can be accurately diagnosed by FNA in most cases…whether newly diagnosed or as a follow up
• Cl. Hodgkin’s lymphoma diagnosis can be made provided a negative FCM and available CB with confirmatory IHC.
• FNA as a follow up for a previously diagnosed case of Hodgkin’s lymphoma can be done…if negative, excisional biopsy is recommended
• Metastatic tumors should not pose any diagnostic challenges provided cell block material is obtained for IHC
Problems of the FNA approach:
• Benign lymphoid lesions…no specific diagnosis
• Hodgkin’s lymphoma• T-cell rich B-cell Lymphoma• T-cell lymphomas• Necrotic/cystic tumors• Grading of some lymphomas• Some rare and mixed lymphomas
Young N 2006 Cancer Feb.
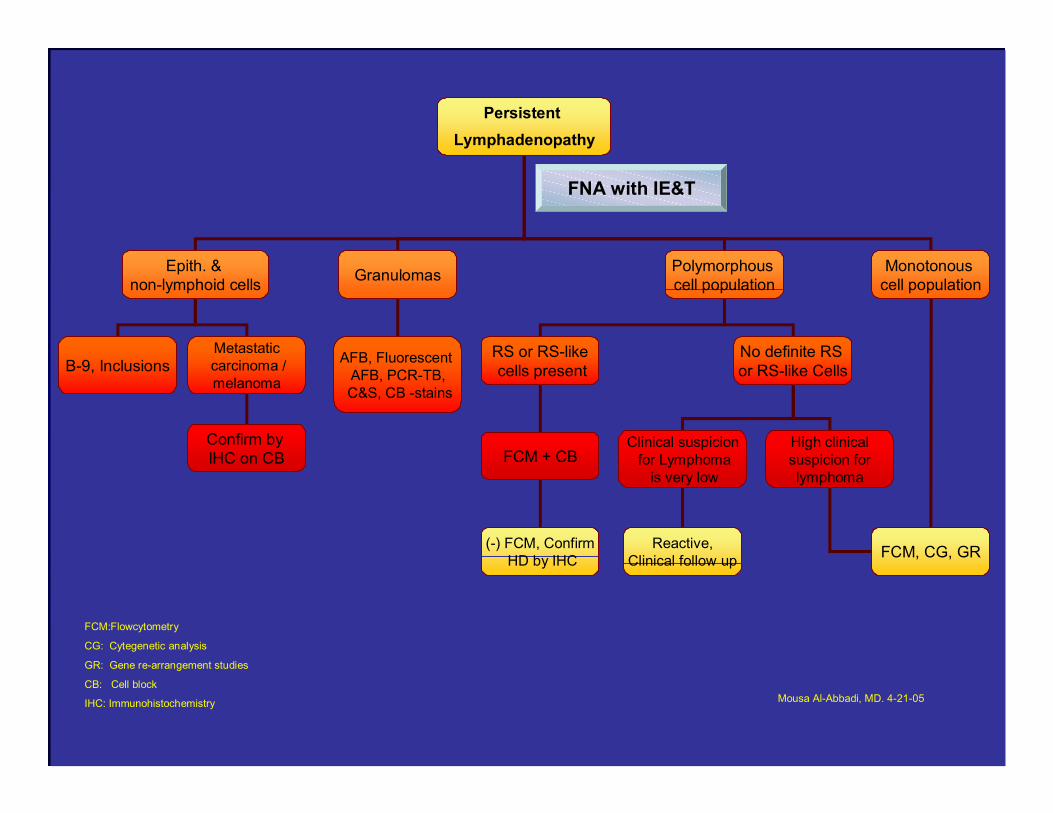
Persistent Lymphadenopathy
Epith. & non-lymphoid cells Granulomas Polymorphous
cell populationMonotonous
cell population
RS or RS-likecells present
No definite RS or RS-like Cells
Clinical suspicionfor Lymphoma
is very low
High clinicalsuspicion for lymphoma
Reactive,Clinical follow up FCM, CG, GR
FCM + CB
(-) FCM, ConfirmHD by IHC
AFB, Fluorescent AFB, PCR-TB,C&S, CB -stains
B-9, InclusionsMetastaticcarcinoma /melanoma
Confirm by IHC on CB
FNA with IE&T
FCM:Flowcytometry
CG: Cytegenetic analysis
GR: Gene re-arrangement studies
CB: Cell block
IHC: Immunohistochemistry Mousa Al-Abbadi, MD. 4-21-05
+/- =DX
Multiple Approach
Alquran, Al-Abbadi, Braylan: Arch Pathol Lab Med. 2004 Nov;128(11):1309
In hematopathology, love is every where
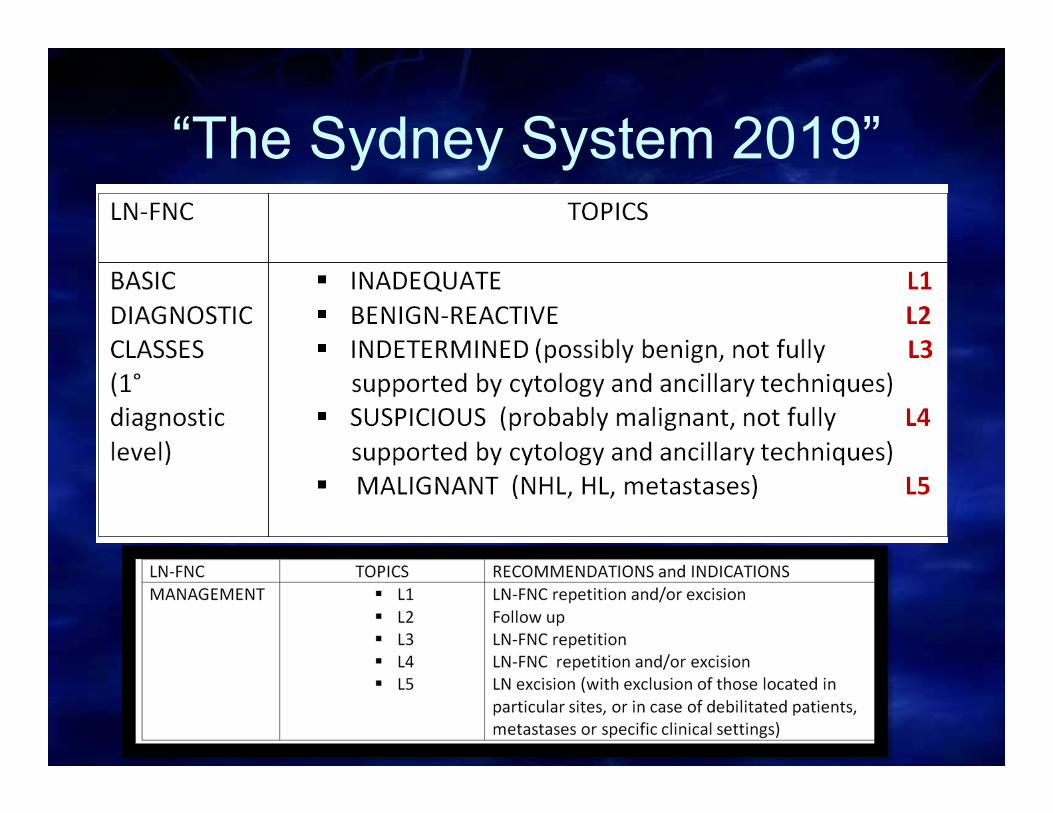
“The Sydney System 2019”

THANK YOU