lower extremity amputations - mcccbehrensb/documents/213wk2amputations.pdf · lower extremity...
TRANSCRIPT
1
Lower Extremity
AMPUTATIONS
Review of Previous Lecture
You are teaching your patient about their total hip precautions (for a posterior approach) and the patient is sitting in a wheelchair. Is “Don’t turn your foot/toes inward” an appropriate instruction?
Rehab Terminology
STUMP: Residual Limb
Artificial Limb: Prosthesis
Stump sock: Sock
Stump shrinker: Shrinker
2
Cause of LE amputation
The major cause of LE amputation continues to be PVD, especially when associated with smoking and diabetes.
Second leading cause is trauma (MVA or GSW)
Risk Factors
Factors that Influence Vascular Disease
Hypertension
Age
Diabetes mellitus
Infection
Poor nutrition
Cigarette smoking
Risk Factors for Amputation
Vascular disease
Malignancy/tumor
Congenital deformities
Infection
Trauma
Study #1: DM & exercise
DM commonly leads to peripheral neuropathy, which causes motor and sensory deficits, often resulting in mobility-related dysfunction, balance impairments, lower gait velocity, decreased cadence, shorter stride length, increased stance time, decreased ankle strength and mobility, postural instability & increased risk of injurious falls
3
Study #1: DM & exercise
Fall-related injuries are often assumed to trigger vicious cycles b/c of their detrimental influence on physical activity.
Which treatment strategies can improve gait and balance, thereby reducing the risk of falls?
RCT = 71 subjects put into control and intervention groups. Control group received nothing
Study #1: DM & exercise
Intervention group received 60 minutes, 2X/week X 12 weeks of: stance on heels/toes, tandem stance, SLS, different kinds of walking, sit to stand, walk up/down slope, stair climbing, mini-hops, interactive game such as badminton.
Gait, balance, fear of falls, muscle strength and joint mobility were measured at baseline, after 12 weeks and 6 month f/u
Study #1: DM & exercise
Results: Significant improvements for intervention group for increased habitual walking speed, balance, performance-oriented mobility, degree of concern re: falling, hip and ankle plantarflexor strength, and hip flexion mobility.
After 6 months, all remained significant except Biodex sway index and ankle PF strength
4
Study #1: DM & exercise
Specific training can improve gait speed, balance, muscle strength and joint mobility in patients with diabetes.
Allet et al (2009)
LEVELS OF AMPUTATION
Usually identified by anatomical considerations/body region
What are the gait implications?
Toe Disarticulation
Gait Implication:
The hallux affects propulsion during fast ambulation
Can use toe fillers in the shoe
5
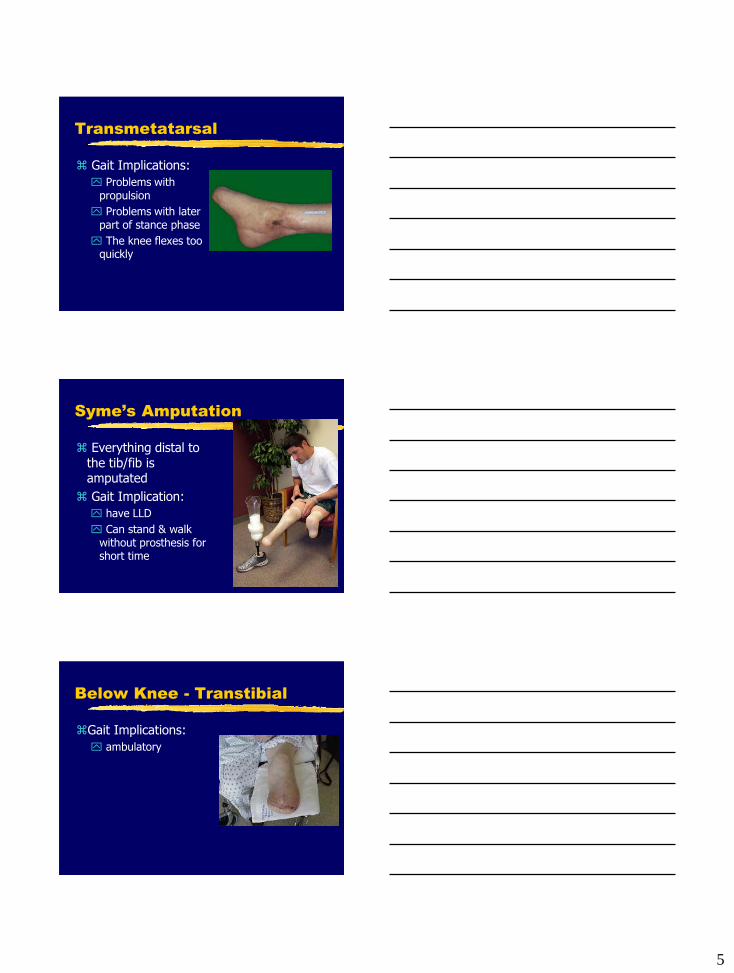
Transmetatarsal
Gait Implications:
Problems with propulsion
Problems with later part of stance phase
The knee flexes too quickly
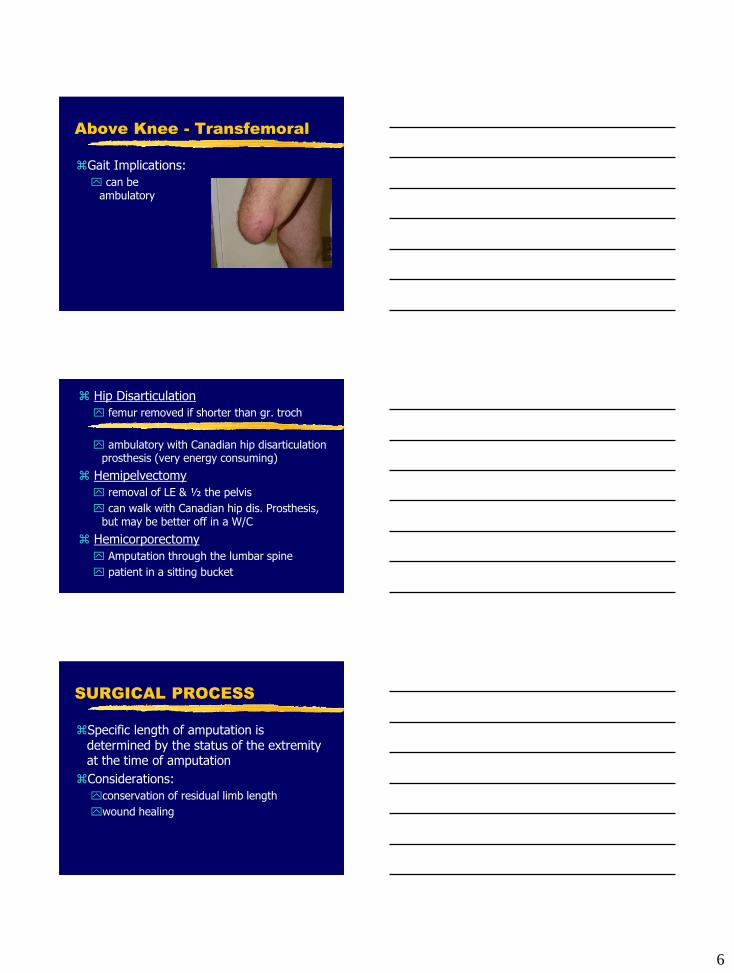
Syme’s Amputation
Everything distal to the tib/fib is amputated
Gait Implication:
have LLD
Can stand & walk without prosthesis for short time
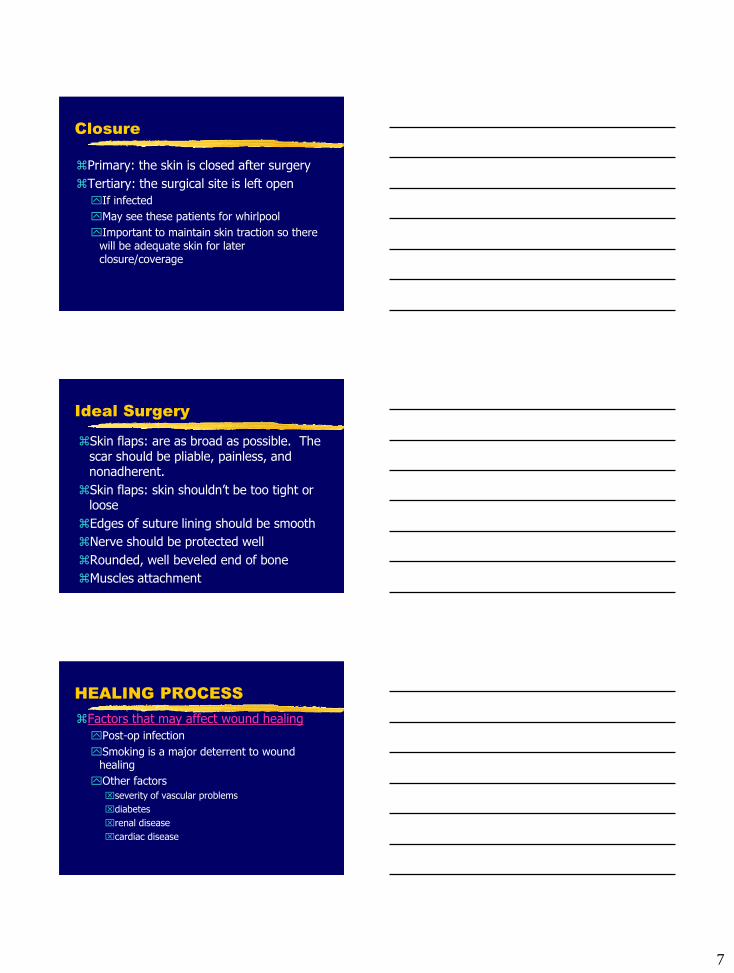
Below Knee - Transtibial
Gait Implications:
ambulatory
6
Above Knee - Transfemoral
Gait Implications:
can be ambulatory
Hip Disarticulation
femur removed if shorter than gr. troch
ambulatory with Canadian hip disarticulation prosthesis (very energy consuming)
Hemipelvectomy
removal of LE & ½ the pelvis
can walk with Canadian hip dis. Prosthesis, but may be better off in a W/C
Hemicorporectomy
Amputation through the lumbar spine
patient in a sitting bucket
SURGICAL PROCESS
Specific length of amputation is determined by the status of the extremity at the time of amputation
Considerations:
conservation of residual limb length
wound healing
7
Closure
Primary: the skin is closed after surgery
Tertiary: the surgical site is left open
If infected
May see these patients for whirlpool
Important to maintain skin traction so there will be adequate skin for later closure/coverage
Ideal Surgery
Skin flaps: are as broad as possible. The scar should be pliable, painless, and nonadherent.
Skin flaps: skin shouldn’t be too tight or loose
Edges of suture lining should be smooth
Nerve should be protected well
Rounded, well beveled end of bone
Muscles attachment
HEALING PROCESS
Factors that may affect wound healing
Post-op infection
Smoking is a major deterrent to wound healing
Other factors
severity of vascular problems
diabetes
renal disease
cardiac disease
8
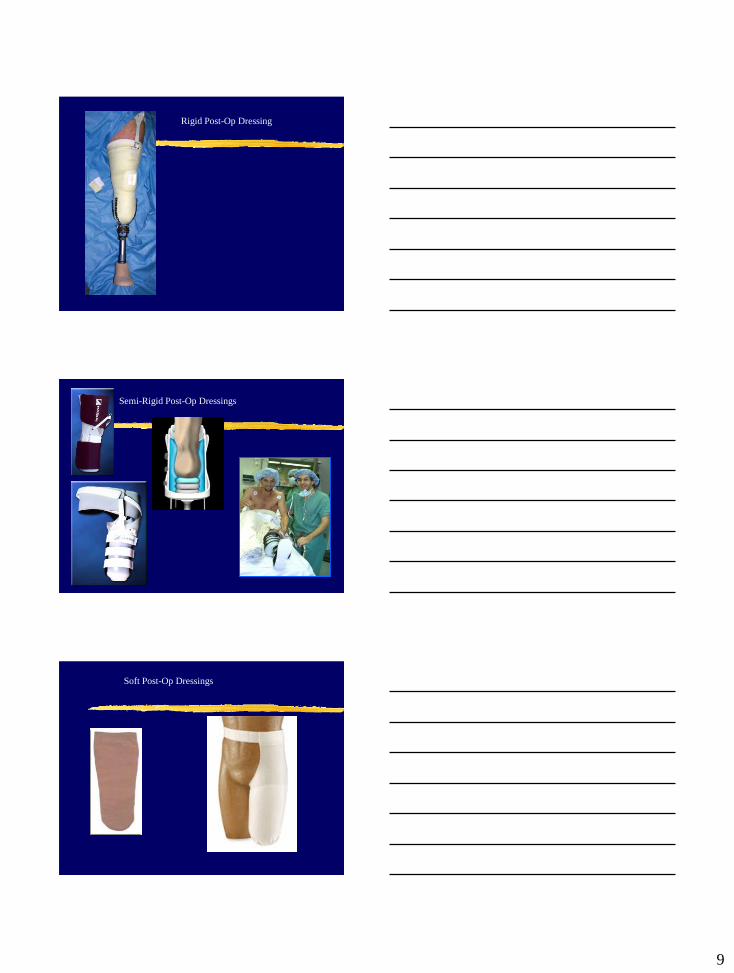
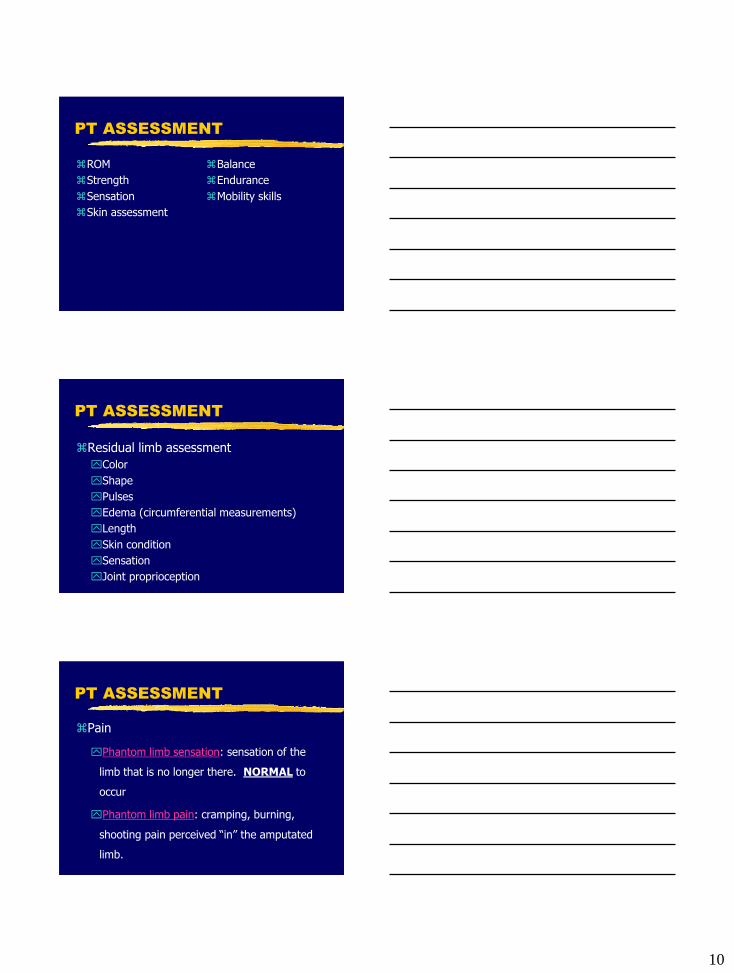
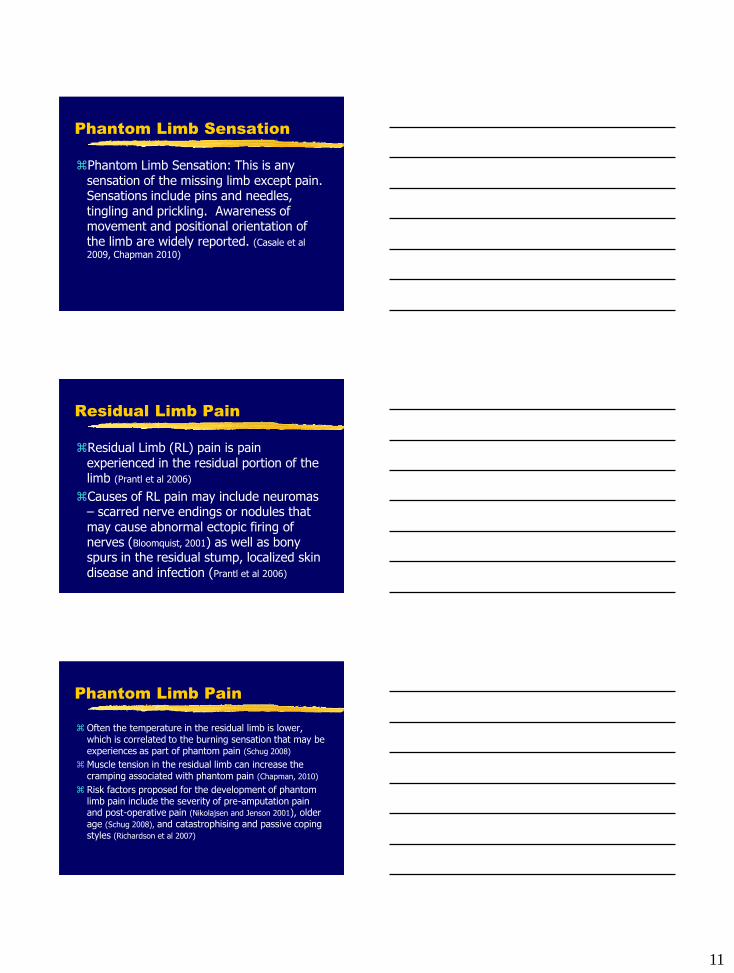
Post-operative Dressings
It is important for some sort of edema control to be used post operatively because excessive edema in the residual limb can compromise healing and cause pain
Post-Op Dressings
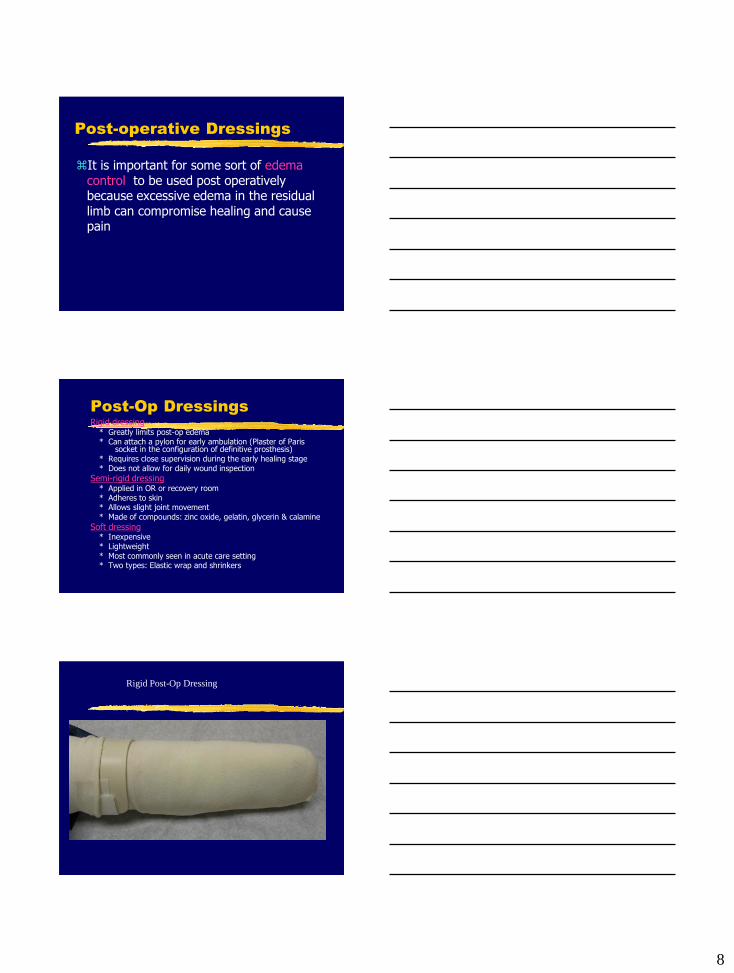
Rigid dressing * Greatly limits post-op edema * Can attach a pylon for early ambulation (Plaster of Paris
socket in the configuration of definitive prosthesis) * Requires close supervision during the early healing stage * Does not allow for daily wound inspection
Semi-rigid dressing * Applied in OR or recovery room * Adheres to skin * Allows slight joint movement * Made of compounds: zinc oxide, gelatin, glycerin & calamine
Soft dressing * Inexpensive * Lightweight * Most commonly seen in acute care setting * Two types: Elastic wrap and shrinkers
Rigid Post-Op Dressing
9
Rigid Post-Op Dressing
Semi-Rigid Post-Op Dressings
Soft Post-Op Dressings
10
PT ASSESSMENT
ROM
Strength
Sensation
Skin assessment
Balance
Endurance
Mobility skills
PT ASSESSMENT
Residual limb assessment
Color
Shape
Pulses
Edema (circumferential measurements)
Length
Skin condition
Sensation
Joint proprioception
PT ASSESSMENT
Pain
Phantom limb sensation: sensation of the
limb that is no longer there. NORMAL to
occur
Phantom limb pain: cramping, burning,
shooting pain perceived “in” the amputated
limb.
11
Phantom Limb Sensation
Phantom Limb Sensation: This is any sensation of the missing limb except pain. Sensations include pins and needles, tingling and prickling. Awareness of movement and positional orientation of the limb are widely reported. (Casale et al
2009, Chapman 2010)
Residual Limb Pain
Residual Limb (RL) pain is pain experienced in the residual portion of the limb (Prantl et al 2006)
Causes of RL pain may include neuromas – scarred nerve endings or nodules that may cause abnormal ectopic firing of nerves (Bloomquist, 2001) as well as bony spurs in the residual stump, localized skin disease and infection (Prantl et al 2006)
Phantom Limb Pain
Often the temperature in the residual limb is lower, which is correlated to the burning sensation that may be experiences as part of phantom pain (Schug 2008)
Muscle tension in the residual limb can increase the cramping associated with phantom pain (Chapman, 2010)
Risk factors proposed for the development of phantom limb pain include the severity of pre-amputation pain and post-operative pain (Nikolajsen and Jenson 2001), older age (Schug 2008), and catastrophising and passive coping styles (Richardson et al 2007)
12
Phantom Limb Pain continued
Catastrophising refers to a coping style characterized by excessively negative thoughts and emotions in relation to pain (Vase et al 2010)
REHABILITATION GOALS
Short Term Goals Edema reduction
Prevent contractures
Regain strength in both LE
Independence in basic residual limb exercises, positioning, bandaging, & care
Learn proper care of remaining extremity
Promote as high a level of independent function as possible (bed mobility, transfers, self care, supervised or independent mobility with walker or crutches)
Decrease hypersensitivity
REHABILITATION GOALS
Long Term Goal
To help the patient regain the pre-surgical level of function
13
Rehab Interventions
Residual Limb Care
Residual Limb Wrapping
Pain Management
Positioning
Exercise
Mobility
Temporary Prostheses
Patient Education
Nonprosthetic Management
Residual Limb Care
Edema Control
limb wrapping
shrinkers
Proper hygiene and skin care
Clean & dry
Scar massage (TFM)
Visual inspection
Early handling by the patient
RESIDUAL LIMB WRAPPING
Never wrap in a circular, tourniquet fashion which creates a bulbous end and compromises healing
Effective wrapping should: be smooth and wrinkle free
emphasize angular turns
provide pressure distally
encourage proximal joint extension
14
Residual Limb Wrapping
Residual Limb WRAPPING
1. Apply firm, even pressure to decrease post-
op edema
2. Residual limb should be completely covered
3. Semicircular turns are made posteriorly to
align the wrap to cross anteriorly in an
angular line
4. Cross wraps by 1/2”
5. Use tape/Velcro to secure. NEVER clips
Pain Management
Chan et al (2007) demonstrated that mirror therapy reduced phantom limb pain in patients who had undergone lower limb amputation.
Patients attempt to perform movements of the phantom limb while viewing the reflected image of the movement of the intact limb.
http://www.youtube.com/watch?v=YL_6OMPywnQ
15
Pain Management continued
MacIver et al (2008) used a mental imagery technique with a group of 13 people with upper limb amputation. The participants had 6 weeks of intensive training in mental imagery, which included a “body scan” exercise and imagined movement and sensation in the phantom limb. They showed changes in cortical reorganization using functional MRI with a corresponding reduction in some aspects of phantom limb pain.
Pain Management continued
Transcutaneous electrical nerve stimulation may also be considered to relieve pain.
However, current evidence in conflicting and a recent Cochrane review found no studies met the eligibility criteria for inclusion in the review and recommended that a large multicenter RCT is needed (Mulvey et al 2010)
POSITIONING
Major goal is to prevent post-op contractures
BKA: must prevent hip & knee flexion contractures; full extension necessary for proper prosthetic use
AKA: must prevent hip flexion, abd, & ER contractures; full hip extension crucial for prosthetic function (prone lying)
16
EXERCISE
The exercise program needs to be individualized & should include strengthening, balance (in sit & stand), coordination, & function
Depends on the patient’s pre-op status
Need to focus on trunk and upper body for ambulation
Early mobility is essential
resumption of independent activities (self-care, bed mobility, transfers)
Strengthening
BKA:
Strengthen the Quads!!
Active patients – strengthen Hamstring too
Strengthen proximal muscles around the pelvis (glut med)
AKA:
Strengthen the hip extensors!!
Strengthen glut med
Exercise
Specific exercises for both BKA & AKA will be reviewed and practiced in Lab
17
Decreasing Hypersensitivity
Don’t confuse it with a neuroma or phantom limb pain
How to decrease hypersensitivity?
TENS
Massage
Slapping the residual limb
Using various materials
MOBILITY
Gait training can begin early on in rehab using a swing through 3 point gait pattern and crutches.
Will improve general fitness (CV & muscular endurance)
All individuals with an amputation need to learn some form of mobility without a prosthesis for use at night or when the prosthesis is not worn for some other reason.
TEMPORARY PROSTHESIS
A temporary prosthesis can be fitted as soon as the wound has healed
Advantages to using a temp prosthesis: Allows for early bipedal ambulation
May allow patients to return to full active
daily life
Some patients can return to work
Positive motivating factor
Shrinks the residual limb more effectively
than wrapping
18
PATIENT EDUCATION
As with all pts, education is crucial. With these patients, it is essential that they are instructed in:
care of the residual limb
proper care of the uninvolved extremity
positioning
exercises
diet
Patient Education cont…
Skin Inspection:
Foot Care:
Foot Wear:
May, 2002
Bilateral Amputation
The post surgical program is similar to the one for unilateral amputation, except ambulation
These patients will need a wheelchair on a permanent basis
Mat activities to regain a sense of body position & balance
Functional mobility stresses independence in bed mobility, transfers & W/C use
19
Bilateral Amputation
These patients spend a considerable amount of time sitting
Stubbies: shortened prosthesis (no knee joint, modified rocker bottoms to prevent falling backwards)
http://www.youtube.c
om/watch?v=sW9-
akxea_U&feature=rel
ated
NONPROSTHETIC
MANAGEMENT
There are some patients who, for any number of reasons, are not fitted with a prosthesis (and will not be fitted in the future)
20
Study #1
21 participants with lower limb amputations who were ambulatory with prostheses and 20 age-matched healthy individuals as the control group.
Postural stability and balance were studied using computerized dynamic posturography
Study #1
Results:
1. equilibrium scores were significantly reduced in persons with amputations as compared to those without
2. equilibrium scores were significantly reduced in persons with amputations due to vascular problems as compared to persons with amputations due to trauma
3. no significant differences were found in equilibrium scores between BKA & AKA
Study #1
Mohieldin A, Chidambaram A, Sabapathivinayagam, R, et al. Quantitative Assessment of Postural Stability and Balance Between Persons with Lower Limb Amputation and Normal Subjects by using Dynamic Posturography. Macedonian Journal of Medical Sciences. 2010; Jun 15; 3(2): 138-143.
21
Review of Today’s Lecture
Amputee-coalition.org
Looking Ahead
Prosthetics
Review
You are instructing a patient in w/c mobility. To have them turn to their right, which wheel of the w/c should be held still and stabilized?
A. Right
B. Left
C. Both
D. Neither
22
References
Allet L, Armand, S, et al (2009) The Gait and Balance of Patients with Diabetes can be Improved: A Randomized Controlled Trial. Diabetologia 53: 458-466.
Bloomquist T (2001) Amputation and phantom limb pain: a pain-prevention model. Journal of the American Association of Nurse Anesthetists. 69, 3, 211-217.
Casale R, Alaa L, Mallick M, Ring H (2009) Phantom limb related phenomena and their rehabilitation after lower limb amputation. European Journal of Physical Rehabilitation Medicine. 45, 4, 559-566.
Chan BL, Witt R, Charrow AP et al (2007) Mirror therapy for phantom limb pain. New England Journal of Medicine. 357, 21, 2206-2207.
Chapman S. Pain Management in Patients Following Limb Amputation. Nursing Standard. 2010; 25(19):35-40.
References Continued
MacIver K, Lloyd DM, Kelly S, Roberts N, Nurmikko T (2008) Phantom limb pain, cortical reorganization and the therapeutic effect of mental imagery. Brain. 131, Pt 8, 2181-2191.
May, B.M., (2002), Amputations & Prosthetics: A Case Study Approach, 2nd Ed., F.A. Davis Company: Philadelphia.
References Continued
Mohieldin A, Chidambaram A, Sabapathivinayagam, R, et al. Quantitative Assessment of Postural Stability and Balance Between Persons with Lower Limb Amputation and Normal Subjects by using Dynamic Posturography. Macedonian Journal of Medical Sciences. 2010; Jun 15; 3(2): 138-143.
Mulvey MR, Bagnall AM, Johnson MI, Marchant PR (2010) Transcutaneous electrical nerve stimulation (TENS) for phantom pain and stump pain following amputation in adults. Cochrane Database of Systematic Reviews. Issue 5.
Nikolajsen L, Ilkjaer S, Christensen JH, Krøner K, Jensen TS (1997) Randomised trial of epidural bupivicaine and morphine in prevention of stump and phantom pain in lower-limb amputation.
The Lancet. 350, 9088, 1353-1357.
23
References continued
O’Sullivan, S.B. & Schmitz, T.J., (2000), Physical Rehabilitation, 4th Ed., F.A. Davis Company: Philadelphia.
Prantl L, Schreml S, Heine N, Eisenmann-Klein M, Angele P (2006) Surgical treatment of chronic phantom limb sensation and limb pain after lower limb amputation. A randomized clinical trial. Plastic and Reconstructive Surgery. 118, 7, 1562-1572.
Richardson C, Glenn S, Horgan M, Nurmikko T (2007) A prospective study of factors associated with the presence of phantom limb pain six months after major lower limb amputation in patients with peripheral vascular disease. Journal of Pain. 8, 10, 793-801.
References continued
Schug S (2008) Acute neuropathic pain:
amputations. Acute Pain. 10, 3-4, 189-190.
Vase L, Nikolajsen L, Christensen B et al (2010) Cognitiveemotional sensitization contributes to wind-up like pain in phantom limb pain patients. Pain. doi: 10.1016/j.pain.2010.10.013.