lower extremity omplications and anagement in …c.ymcdn.com/sites/ · more than 60% of...
TRANSCRIPT

1
LOWER EXTREMITY
COMPLICATIONS AND
MANAGEMENT IN PATIENTS
WITH DIABETES
Don Curtis, DPM, FACFAS
Midwestern University
www.mwuclinic.com
623-572-6160
TOTAL PREVALENCE OF DIABETES
Data from the 2011 National Diabetes Fact Sheet (released Jan. 26, 2011)
TOTAL PREVALENCE OF DIABETES

2
MORBIDITY AND MORTALITY
COMPLICATIONS
� Heart disease and stroke� Heart disease was noted on 68% of diabetes-related death
certificates >65 years.
� Stroke was noted on 16% of diabetes-related death certificates > 65 years.
� Adults with diabetes have heart disease death rates about 2 to 4 times higher than adults without diabetes.
� The risk for stroke is 2 to 4 times higher among people with diabetes.
� High blood pressure� Self reported DM, >20 years:
� 67% had HTN ≥ 140/90 mmHg or used prescription medications HTN.
Data from the 2011 National Diabetes Fact Sheet (released Jan. 26, 2011)
3
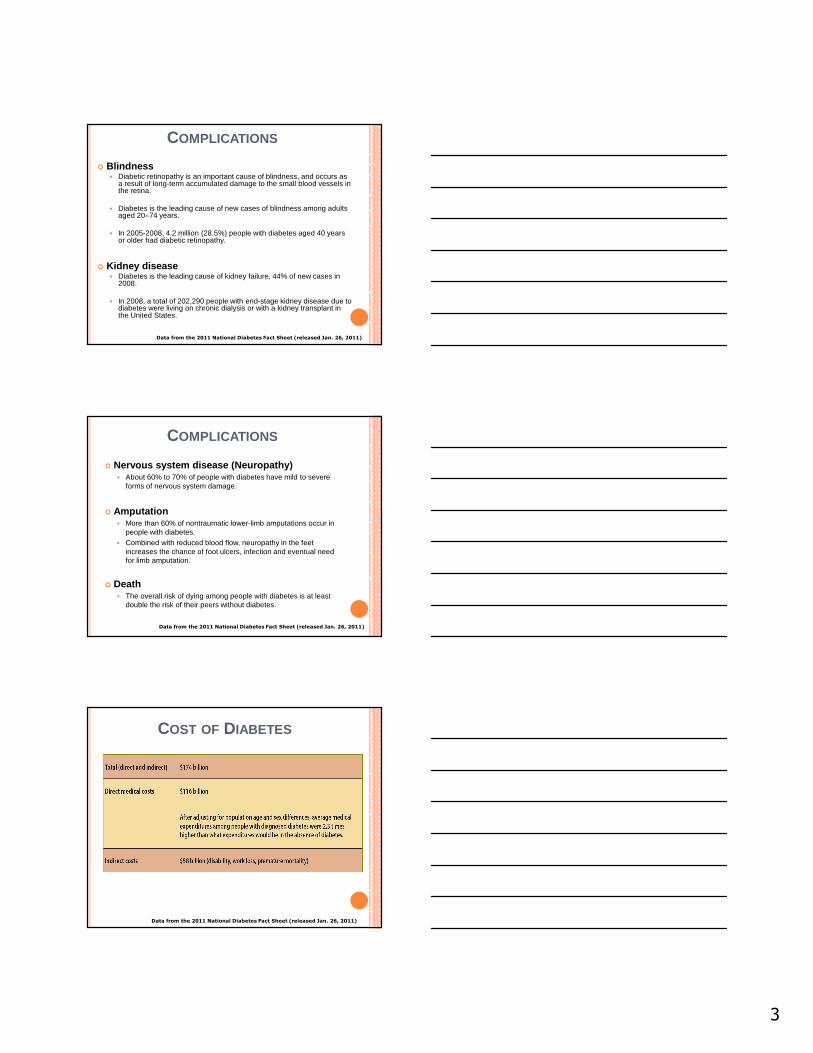
COMPLICATIONS
� Blindness� Diabetic retinopathy is an important cause of blindness, and occurs as
a result of long-term accumulated damage to the small blood vessels in the retina.
� Diabetes is the leading cause of new cases of blindness among adults aged 20–74 years.
� In 2005-2008, 4.2 million (28.5%) people with diabetes aged 40 years or older had diabetic retinopathy.
� Kidney disease� Diabetes is the leading cause of kidney failure, 44% of new cases in
2008.
� In 2008, a total of 202,290 people with end-stage kidney disease due to diabetes were living on chronic dialysis or with a kidney transplant in the United States.
Data from the 2011 National Diabetes Fact Sheet (released Jan. 26, 2011)
COMPLICATIONS
� Nervous system disease (Neuropathy)� About 60% to 70% of people with diabetes have mild to severe
forms of nervous system damage.
� Amputation� More than 60% of nontraumatic lower-limb amputations occur in
people with diabetes.� Combined with reduced blood flow, neuropathy in the feet
increases the chance of foot ulcers, infection and eventual need for limb amputation.
� Death� The overall risk of dying among people with diabetes is at least
double the risk of their peers without diabetes.
Data from the 2011 National Diabetes Fact Sheet (released Jan. 26, 2011)
COST OF DIABETES
Data from the 2011 National Diabetes Fact Sheet (released Jan. 26, 2011)

4
LOWER EXTREMITY DIABETIC
FOOT EXAM�Dermatologic Exam:
� Skin Appearance� Color, texture, turgor, quality, dry skin
and fissures
� Calluses � Nails
� Onychomycosis� Paronychia
� Ulcerations� Markers for Diabetes
� Shin Spots – diabetic dermopathy
� Necrobiosis Lipoidica � Bullosum diabeticorum
� Granuloma annulare
� Anthosis nigricans

5
WAGNER WOUND CLASSIFICATION
� Wagner Grading System� Grade 0: No open lesions� Grade 1: Superficial Ulcer � Grade 2: Deep Ulcer
� Involves ligament, tendon, joint capsule or fascia � No abscess or osteomyelitis
� Grade 3: Deep ulcer with abscess, osteomyelitis, or joint sepsis
� Grade 4: Local Gangrene of forefoot or heel � Grade 5: Extensive gangrene of entire foot
� Reference � Wagner (1987) Orthopedics 10:163-72
LOWER EXTREMITY
DIABETIC FOOT EXAM�Vascular Examination
� Palpation of Pulses� Handheld Doppler Examination� Skin/Limb color changes
� Cyanosis, erythema,
� Elevation pallor – dependent rubor
� Edema� Temperature gradient� Integumentary Changes
� Skin atrophy
� Thin, smooth, parchment-like � hair growth absent.

6
VASCULOPATHY
� Signs and symptoms of poor circulation of the lower extremities include:� Cool or cold feet
� Pale or blue color of toes
� Slow return of color after squeezing toes
� Decreased leg hair in men
� Calf pain with walking
� Slow healing
ACCELERATED ATHEROSCLEROSIS
LOWER EXTREMITY
DIABETIC FOOT EXAM
�Neurological Exam� Vibration perception:
� Tuning fork 128cps
� Light Pressure:� Semmes-Weinstein 10 g
monofilament
� Light Touch� Two Point Discrimination� Pain: pinprick (sterile)� Temperature perception� Deep Tendon Reflexes� Clonus, Babinski and Romberg

7
SENSORY NEUROPATHY
� ‘Pain arising as a direct consequence of abnormalities in the somatosensory system in people with diabetes.’� International Association for
the Study of Pain
� A diagnosis of exclusion and is a clinical diagnosis� Relying on the patient’s
description� A careful clinical history� A thorough neurological and
vascular exam is essential
SUBJECTIVE COMPLAINTS
� Burning� Cramping
� Aching� Tingling
� Stinging� Walking on marbles� Knife-like
� Warm/Cold� Numbness
� Hypersensitivity� Cramping
� Walking on hot sand

8
AUTONOMIC NEUROPATHY
� Cardiovascular� sudden death, silent MI, decreased
exercise tolerance, CHARCOT?
� Genitourinary � erectile dysfunction, urinary retention
� Gastrointestinal� gastroparesis, anorexia, nausea,
vomiting, diarrhea, constipation
� Cutaneous� sweat disturbances, reduced nutrient
delivery, reduced blood flow
MOTOR NEUROPATHY
� Muscle weakness/wasting
� Limitation of joint motion� Glycosylation of collagen limits
flexibility� Range of motion is diminished� Ankles, subtalar joints, 1st mtpj’s
commonly affected
� Common symptoms:� Foot drop / loss in function� Tripping / gait disturbances� Deformities (hammertoes)� Equinus
LOWER EXTREMITY
DIABETIC FOOT EXAM
�Musculoskeletal Exam� Biomechanical Abnormalities� Structural Deformities
� Bunion, Hammertoes, Tailor’s Bunion
� Flat feet/High arches� Charcot Deformity
� Prior Amputations� Limited Joint Mobility� Achilles Contracture� Gait Exam� Muscle Strength Testing� Plantar Pressure Assessment

9
LOWER EXTREMITY
DIABETIC FOOT EXAM
�Footwear Examination� Type of Shoe
� Athletic, dress, sandal
� Fit� Too loose can cause friction blisters
� Too tight can cause pressure ulcers
� Depth of toe box� Wear pattern
� Shows high pressure points
� Lining� Foreign body� Supports/orthotics
RISK STRATIFICATION
� Category Risk Profile Eval Frequency� 0 Normal q 12 months� 1 Periph Neurop q 6 months� 2 LOPS, deformity,
+/- PAD q 3 months� 3 Previous ulcer or amp q 1-3 months

10
American Diabetes Association. Diabetes 1996 Vital Statistics.
SURVIVAL RATES AFTER AMPUTATION
�After 1 major lower-extremity amputation� 3-year survival rate is 50%� 5-year survival rate is 40%
�Contralateral amputation� 42% of patients within 1 to 3 years after
first amputation� 56% of patients within 3 to 5 years after
first amputation
5-YEAR SURVIVAL RATES AFTER AMPUTATION
�Add Some Perspective
2007: Armstrong et al; Are diabetes related wounds and amputations worse than cancer?
RATES OF LOWER EXTREMITY
AMPUTATIONS

11
RATES OF LOWER EXTREMITY
AMPUTATIONS
3RD DIGIT OSTEOMYELITIS

12
TEAM APPROACH TO DIABETIC
FOOT CARE
PATIENT CARE INSTRUCTIONS
� 1. Inspect feet daily-watch for�Color changes (redness, streaking, blue, pale)�Swelling�Temperature changes (increased or decreased)�Sensation changes�“Hot Spots” - red areas due to friction�Cracks, sores, blisters, ulcers�Toenail problems�Drainage and Odor

13
PATIENT CARE INSTRUCTIONS
� 2. Never walk barefoot� Even indoors
� Always wear socks and shoes together� Make sure shoes fit properly
� Inspect shoes for foreign objects
� 3. Check water temperature with elbows prior to entering� Dry well between toes
� 4. Use lotions or creams daily� Do not apply between toes
PATIENT CARE INSTRUCTIONS
� 5. Don’t treat wounds, corns, or calluses yourself.� Unless directed by your Podiatrist
� 6. Don’t smoke or quit smoking.� Smoking causes decreased blood flow and reduced healing potential
�CONTROL YOUR DIABETES!!
REFERENCES
� Diabetic Foot Disorders: A Clinical Practice Guideline. Frykberg et al. Journal of Foot & Ankle Surgery Vol 45, Number 5, September/Ocober 2006 Supplement.
� 2012 Infectious Disease Society of America; Clinical Practice Guideline for the Diagnosis & Treatment of Diabetic Foot Infections (IDSA Guidelines). Lipsky et al. Clinical Infectious Diseases 2012:54 (12):132-173.
� The Diagnosis of Charcot Foot. Rogers & Bevilacqua. Clinics in Podiatric Medicine & Surgery 25(2008) 43-51.
� Medical Imaging of the Diabetic Foot. Loredo et al. Clinics in Podiatric Medicine & Surgery 24(2007) 397-424.
� Painful Diabetic Peripheral Neuropathy: Consensus Recommendations on Diagnosis, Assessment & Management. Tesfaya et al. Diabetes/Metabolism Research & Reviews 2011; 27:629-638
� Are Diabetes-Related Wounds & Amputations Worse Than Cancer? Armstrong et al. International Wound Journal 2007 Vol.4 No.4
� Shoes, Orthoses & Prostheses for Partial Foot Amputations & Diabetic Foot Infections. Janisse et al. Foot & Ankle Clinics of North America 15(2010) 509-523