long term care trends in the united states choices for independence summit lisa alecxih vice...
TRANSCRIPT

Long Term Care Trendsin the United States
Choices for Independence SummitLisa Alecxih
Vice President
December 5, 2006
Posted 12/8/06
2
Overview
Review of the Basics
Major Trends Demographics Delivery Financing
Implications for the Future

3
What is Long Term Care?
Services and supports needed when one’s ability to care for self has been reduced by a chronic illness, disability, or frailty.
Services usually provided: by family and friends at home through home and community-based services, such
as home health care, personal care, and adult day services
in institutional settings, such as nursing homes or residential care facilities

4
Who Might Need Long Term Services and Supports?
1.1% 1.6% 2.2% 3.7% 4.8% 6.5% 9.7%15.0%
27.1%
43.2%
66.7%
80.5%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
18-2
9
30-3
9
40-4
9
50-5
9
60-6
4
65-6
9
70-7
4
75-7
9
80-8
4
85-8
9
90-9
4
95+
Age
% o
f In
div
idu
als
wit
h a
Dis
abil
ity
Source: 1999 National Long Term Care Survey and the 1994 National Health Interview Survey Disability Supplement.

5
Most Seniors with Disabilities Supported by Unpaid Care in the Community
Source: 1999 National Long Term Care Survey, 2002 Medicare Current Beneficiary Survey, and 2005 CMS Minimum Data Set.
Alternative Residential
NursingFacility
Community
Community Paid Only
Community Unpaid Only
Community Paid and Unpaid
8%
21% 71%
25%
42%
4%

6
Who Uses Any Paid Services?
14.2%
7.5%
17.4%
31.3%
Source: 2003 Medical Expenditure Panel Survey, 2002 Medicare Current Beneficiary Survey, and 2005 CMS Minimum Data Set.
3.3% 3.5%
11.5%
5.9%
9.6%
6.2%
12.7%
14.0%
1.0%
1.3%1.3%
0.3%0%
5%
10%
15%
20%
25%
30%
35%
Age 65+ 65-74 75-84 85+
Per
cen
t U
sin
g P
aid
LT
C
Nursing Facilities Alternative Residential Paid HCBS
7
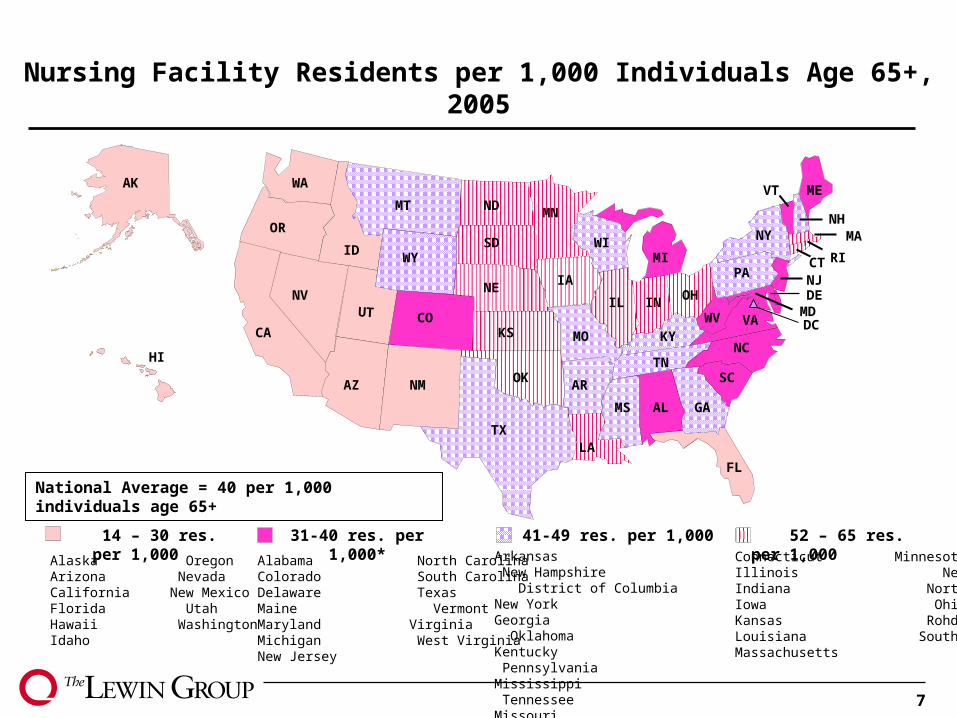
31-40 res. per 1,000* 14 – 30 res. per 1,000 41-49 res. per 1,000Connecticut MinnesotaIllinois NebraskaIndiana North DakotaIowa Ohio Kansas Rohde IslandLouisiana South Dakota Massachusetts
Alabama North CarolinaColorado South CarolinaDelaware TexasMaine Vermont Maryland VirginiaMichigan West VirginiaNew Jersey
Alaska OregonArizona Nevada California New MexicoFlorida UtahHawaii WashingtonIdaho
Nursing Facility Residents per 1,000 Individuals Age 65+, 2005
Arkansas New Hampshire District of Columbia New York Georgia Oklahoma Kentucky PennsylvaniaMississippi Tennessee Missouri WisconsinMontana Wyoming
52 – 65 res. per 1,000
HI
AK
MT
ID
WA
CO
WY
NV
CA
NMAZ
MN
KS
TX
IA
WI
IL
KY
TN
INOH
MI
ALMS
AR
LA
GA
FL
SC
WV VA
NC
MDDE
PANJ
VT
RI
ME
NHOR
UT
SD
ND
MO
OK
NE
NY
CT
DC
MA
National Average = 40 per 1,000 individuals age 65+

8
How Much Does Long Term Care Cost?
Nursing Home Care Average annual cost -- $74,095 $41,975 in Shreveport, Louisiana to $193,815 in Alaska
Assisted Living Average annual cost -- $34,860 $19,740 in Jackson, MS to $55,548 in Boston, MA
Home Care Average rate for home health aide -- $19/hour $12/hr in Shreveport, LA to $26/hr in Colorado Springs,
Co Average rate for homemaker/companion -- $17/hour $12/hr in Shreveport, LA to $23/hr in Minneapolis/St.
Paul, MNSource: The MetLife Market Survey of Nursing Home & Home Care Costs in 2005 and Assisted Living in 2005 which
includes private pay rates and services provided by home health agencies.

9
Medicare Covers Limited LTC Benefits Primarily post-acute care Home health services
Beneficiaries who are homebound Need part-time skilled nursing or therapy services,
and Under the care of a physician 27 visits per user on average in 2005
Skilled nursing facility care Up to 100 days for those recently discharged from a
hospital 35 days covered on average in 2005

10
Eligibility Criteria Among LTC Users Makes Medicaid the Payer of Last Resort
Pathway Income EligibilityAsset Limit
Individual/Couple
Mandatory Population
SSI Cash Assistance < 74% of poverty(SSI income eligibility)
$2,000$3,000
Optional Populations
Medically Needy* Spend income down to a specified level ($100-$825; $416 on average)
$2,000$3,000
Poverty Level < 100% of poverty $2,000$3,000
Special Income Rule for Nursing Home Residents
Income < 300% of the SSI level (1,809/month)
$2,000Spousal Impoverishment
HCBS Waivers Income up to 300% SSI level (37 states);
8 states at poverty level; some states allow spousal impoverishment
$2,000$3,000 or Spousal Impoverishment
*Medicaid benefits may be more limited than for SSI.

11
HCBS 20-32%* HCBS 35-54% HCBS 10-19% Alabama ConnecticutDelaware DCFlorida Georgia Indiana KentuckyMaryland Mississippi New Hampshire North DakotaPennsylvania South Dakota Tennessee Utah
Arkansas KansasMaine MassachusettsMissouri MontanaNevada New Jersey New York Oklahoma Vermont Virginia
Alaska CaliforniaIdaho MinnesotaNew Mexico North CarolinaOregon TexasWashington Wisconsin
Percent HCBS of Medicaid LTC Among Aged/Disabled, 2005
Colorado HawaiiIllinois IowaLouisiana MichiganNebraska OhioRhode Island South CarolinaWest Virginia Wyoming
HCBS <10%
National Average = 22.9%
HI
AK
MT
ID
WA
CO
WY
NV
CA
NMAZ
MN
KS
TX
IA
WI
IL
KY
TN
INOH
MI
ALMS
AR
LA
GA
FL
SC
WV VA
NC
MDDE
PANJ
VT
RI
ME
NHOR
UT
SD
ND
MO
OK
NE
NY
CT
DC
MA

12
Out-of-Pocket Covers A Significant Portion Some individuals pay for LTC on their own
Those who qualify for Medicaid also pay out-of-pocket Nursing facility residents with Medicaid financing contribute
all of their income with the exception of a personal needs allowance ($30-$100/month)
– On average, Medicaid nursing facility residents contribute 20% of their cost
Many states also require cost-sharing for their HCBS waiver
Medicaid rules protect the primary residence while the individual or their spouse is alive
– OBRA ’93 mandated estate recovery
– In 2003, states recovered a total of $347.4 million – on average 0.5% of Medicaid LTC costs, however, Oregon recovered 2.2% (AARP, 2005)

13
Long Term Care Insurance (LTCI) Plays a Limited Role LTCI market emerged during the 1980s 9.2 million total policies sold through 2002 However, only approximately 10 percent of those
age 65+ own LTCI policies because of: Complicated and expensive policies -- $1,337 to $2,862 at age
65 Consumer lack of awareness and denial of need Most policies must be “sold” by agents
Limited benefit payouts Early policies offered limited benefits – nursing home only and
often no inflation protection Benefits based on daily amount purchased and may not cover
full cost of care Many people lapse their policy prior to benefits
Source: American Health Insurance Plans (AHIP) (2004) Long Term Care Insurance in 2002 for number of policies sold and average premium.

14
LTC Sources of Financing Among Seniors
Medcaid38%
Medicare20%
Other Public3%
LTCI3%
Family Resources
36%
Source: The Lewin Group based on the Long Term Care Financing Model.
Total in 2005 =$140.8B

15
Major U.S. Long Term Care System Trends
Demographics
Delivery
Financing
Demographic Trends

17
Disability Rates Declined Between 3.0 and 6.5 percentage points or 10.5 to 25 percent
12.2%
29.1%
62.0%
9.2%
23.4%
55.5%
0%
10%
20%
30%
40%
50%
60%
70%
65-74 75-85 85+Pe
rce
nt
of
Ag
e G
rou
p w
ith
Dis
ab
ilit
y
1984
1989
1994
1999
Disability Rates Among Individuals Age 65 and Over by Age
Source: Brenda C. Spillman (2003) Changes in Elderly Disability Rates and the Implications for Health Care Utilization and Cost for the Office of the Assistant Secretary for Planning and Evaluation at http://aspe.hhs.gov/daltcp/reports/hcutlcst.htm.

18
Poverty Rates Among Oldest Old Declined by More Than 1/3rd
8.9
13.4
21.2
10.9
17.4
12.4
10.1
14.6
7
9
11
13
15
17
19
21
23
Perc
en
t o
f In
div
idu
als
with
Inco
me
Belo
w P
overt
y T
hre
sh
old
85+ 75-84 65-74 65 or Older
Elderly Poverty Rates Over Time
Source: Current Population Survey, Annual Supplement, 1983-2006.

19
Dip in Childless Women & Spike in Average Number of Children Among Mothers
Source: Bureau of the Census data..
Status at Age 40-44 and Year When Age 85-89
0%
5%
10%
15%
20%
25%
1975
1980
1985
1990
1995
2000
2005
2010
2015
2020
2025
2030
2035
2040
2045
2050
0.00.51.01.52.02.53.03.54.04.5
Percent Childless
Women
Average # of Children
Among those with
Children

Delivery Trends

21
Significant Declines in the Use of Nursing Facilities Among Oldest Old
Source: 1973-4, 1997, 1985, 1995, 1997, 1999 and 2004 National Nursing Home Survey.
3.8%
1.1%
5.0%
21.1%
3.6%
0.9%
3.6%
13.9%
0%
5%
10%
15%
20%
25%
65+ 65-74 75-84 85+
Pe
rce
nt
of
Po
pu
lati
on
Wh
o A
reR
es
ide
nts
of
Nu
rsin
g F
ac
ilit
ies
1973-74
1977
1985
1995
1997
1999
2004

22
Much of Decline From Growth in Alternative Residential Settings
Source: 1985 and 2004 National Nursing Home Survey and 2002 Medicare Current Beneficiary Survey.
13.9%
4.1%
0.9%
4.9%
0.3%0.2%
0%
5%
10%
15%
20%
25%
65-74
Alt. Residential - Community
Alt. Residential - Facility
Certified Nursing Home
2004
18.8%
22.9%
1.4%
5.9%
3.6%
1.2%1.1%
75-84 85+
4.7%
1.0%
5.2%
21.1%
1.8%
0.6%
0.2%0%
5%
10%
15%
20%
25%
65-74 75-84 85+
Non-Certified Nursing Home
Certified Nursing Home
1985
1.2%
5.8%
22.9%
Financing Trends

24
Medicaid LTC Devoted to HCBS for Aged and Disabled Grew Significantly Since 2000
11.1%11.9%
13.0%
14.6%
19.0%18.0%
17.0%
14.3%13.7%
11.8%11.1%
20.6%
12.3%
22.6%
10%
12%
14%
16%
18%
20%
22%
24%
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005P
rop
ort
ion
of
Med
icai
d L
TC
Sp
end
ing
for
HC
BS
Am
on
g A
ged
an
d D
isab
led
Source: 2005 MedStat LTC Data, Lewin Analysis. Long term care includes nursing facility, state plan personal care and home and community-based waivers for the aged and disabled.
25
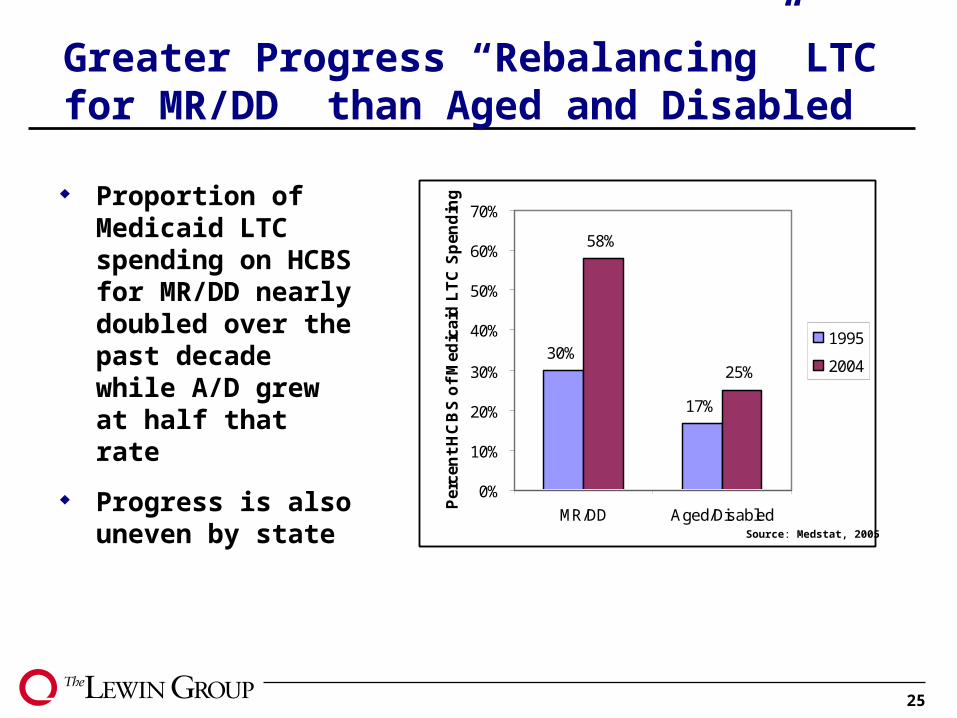
Greater Progress “Rebalancing” LTC for MR/DD than Aged and Disabled
30%
17%
58%
25%
0%
10%
20%
30%
40%
50%
60%
70%
MR/DD Aged/DisabledPer
cen
t H
CB
S o
f M
edic
aid
LT
C S
pen
din
g
1995
2004
Proportion of Medicaid LTC spending on HCBS for MR/DD nearly doubled over the past decade while A/D grew at half that rate
Progress is also uneven by state Source: Medstat, 2005

26
Change in Per Capita Medicaid Nursing Facility Residents, 1995-2005
HI
AK
MT
ID
WA
CO
WY
NV
CA
NMAZ
MN
KS
TX
IA
WI
IL
KY
TN
INOH
MI
ALMS
AR
LA
GA
FL
SC
WV VA
NC
MDDE
PANJ
VT
RI
ME
NHOR
UT
SD
ND
MO
OK
NE
NY
CT
DC
MA
National Average = 15.2% Decline
20% to 30% Decline 30% or More Decline 10% to 20% Decline
Alabama Mississippi District of Columbia New JerseyFlorida New YorkHawaii OhioIowa PennsylvaniaKentucky South CarolinaMichigan West Virginia
Alaska Washington Maine UtahOregon
Arizona Massachusetts California Missouri Connecticut NebraskaDelaware New Hampshire Idaho North CarolinaIllinois North DakotaKansas Rhode IslandMaryland South Dakota
Less than 10% Decline
Arkansas New MexicoColorado OklahomaGeorgia TennesseeIndiana TexasLouisiana VermontMinnesota VirginiaMontana WisconsinNevada Wyoming

27
A few well established programs and numerous start-ups.
Top Managed Care Programs:
Arizona – 42,125 lives (8/2006)New York – 16,224 lives (4/2006)Florida – 13,600 lives (8/2006)Wisconsin – 12,545 lives (8/2006)
Remaining Programs:
Massachusetts – 3,700 lives (2/2006)Texas – 3,300 lives (4/2006)Minnesota – 2,100 lives (1/2006)California -- unknown
New Programs:
Kentucky HawaiiIdaho MarylandNew Mexico North CarolinaSouth Carolina WashingtonVermont
Active & Pending Programs
Potential Expansions/Pilots
LTC Programs
Many States Looking to Managed Long Term Care to Rebalance Medicaid

28
Implications of Financing System
Financing silos and institutional bias of Medicaid eligibility make rebalancing difficult
Olmstead Decision and President’s New Freedom Initiative focus on individual choice and shifting the balance
Lack of insurance to spread risk means individuals responsible for paying for much of their care
Medicaid managed care re-emerging as states seek to eliminate institutional bias, improve service provision, and control costs May stand in contrast to consumer direction movement

Preparing for the Future

30
Aging of Baby Boomers Will More than Double the Number of Older Adults Age 65+ with Disabilities
0
2
4
6
8
10
12
14
16
1996
-00
2000
-04
2005
-09
2010
-14
2015
-19
2020
-24
2025
-29
2030
-34
2035
-39
2040
-44
2045
-49
Nu
mb
er o
f E
lder
ly w
ith
Dis
abili
ties
(i
n m
illio
ns)
2+ ADLs
1 ADL
IADL Only
Source: The Lewin Group based on the Long Term Care Financing Model.
31
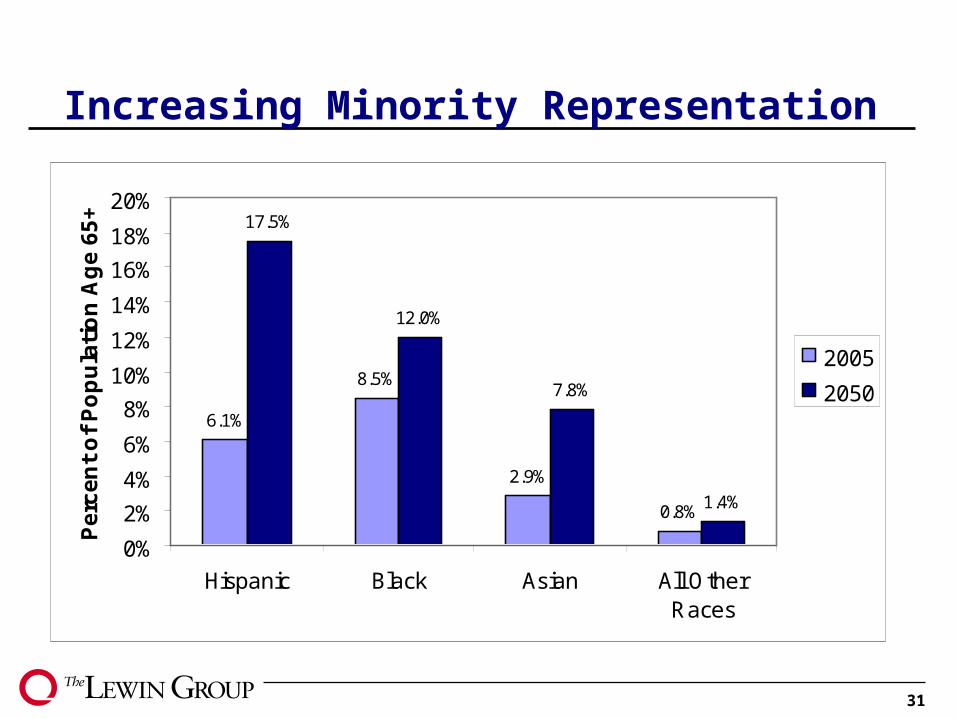
Increasing Minority Representation
6.1%
8.5%
2.9%
0.8%
17.5%
12.0%
7.8%
1.4%
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
Hispanic Black Asian All OtherRaces
Pe
rce
nt
of
Po
pu
lati
on
Ag
e 6
5+
2005
2050

32
Remaining Lifetime Use of LTC by People Turning 65 in 2005
Type of CareAverage Years of
Care% of People Using
Type of Care
All LTC need 3.0 69
At home
Informal care only 1.4 59
Formal care 0.5 42
Any care at home 1.9 65
In facilities
Nursing facilities 0.8 35
Assisted living 0.3 13
Any care in facilities 1.1 37Source: Kemper, Komisar & Alecxih; Inquiry; Vol. 42, Winter 2005/2006.

33
While Most Could Save Enough, Over 25% Face Expenses Over $100,000 2000 median net worth among elderly was
$110,000, but only $25,000 excluding home equity
Average lifetime per capita at age 65 =
$47,000
Distribution of Lifetime Expenditures After Age 65
No expenditures
(family and friendssupport)
42%
$1-$9,999
19%
$10,000-$24,999
8%
$25,000- $99,999
5%
$100,000+
Source: Kemper, Komisar & Alecxih; Inquiry; Vol. 42, Winter 2005/2006.
26%
34
Few Americans Plan Ahead for LTC Needs
Less than 10% of those age 65+ own a long term care insurance policy
Long term care insurance policies can be expensive and may be unaffordable for many middle-income Americans.
Baby boomers had children later than any previous generation and worry more about college tuition than financing future LTC needs
Older adults own nearly $3 trillion in home equity, yet few take advantage of methods to tap this resource.

35
Lifestyle Choices Affect Nursing Home Use
Source: Valiyeva E, et al. Lifestyle-Related Risk Factors and Risk of Future Nursing Home Admission. Archives of Internal Medicine. 2006; 166:985-90. May 8, 2006.
Relative Risk for Nursing Home Admission Over the Next 20 Years at Age 45-64
1.001.35
1.89
3.25
4.55
0.0
1.0
2.0
3.0
4.0
5.0
Normal BloodPressure
High BP High BP +inactivity
Diabetic Diabetic +inactive
36
Conclusions Consumers need trusted and reliable information
about their options to make informed decision Expect support options to continue to evolve:
Respond to market demand Role of technology States interests in lower cost alternatives
Encouraging purchase at younger ages would be the most effective policy for increasing the role of LTC insurance.
Standardizing the reverse mortgage process could promote the use and/or access to assistance for care planning when using personal assets.