lab 10: peritoneal cavity and overview of gi
TRANSCRIPT
LAB 10 : PER ITONEAL CAV ITY AND OVERV IEW OF G I10/6/2021
Table of ContentsTable of Contents !
Opening the Peritoneal Cavity
Abdominal Viscera
Liver
Small intestine
Large intestine
Peritoneum and Peritoneal Cavity
Lesser Sac
Greater Omentum
The Other Mesenteries
Inspect the Pelvic Viscera
Imaging
David Conley, PhDOffice: PBS 41A
Shannon Helbling, PhDOffice: PBS 41C
"
+
TO O P E N T H I S PA G E O N T H E L A B M O N I TO R S
1. Turn on the monitor.
2. Choose a browser (Chrome or Firefox—either is Gne!).
3. Tap the URL Geld at the top of the screen to highlight.
4. Tap the keyboard icon in the bottom right-hand corner.
5. Enter this URL: https://tinyurl.com/f8v5wkef
TO D O W N L O A D A P D F O F T H I S L A B G U I D E
GOALS1 Open the anterior abdominal wall and study its internal aspect.
2 Examine the peritoneum, peritoneal cavity, mesenteries, omenta, and peritoneal
ligaments.
3 Locate the subparts of the greater sac.
4 Study the lesser omentum and demonstrate the lesser sac.
5 Study the organs of the abdominal cavity: liver; gallbladder; stomach; small intestines; large
intestines; pancreas; and spleen.
O P E N I N G T H E P E R I TO N E A L C AV I T Y
Open the abdominal wall.
Open the anterior abdominal wall:
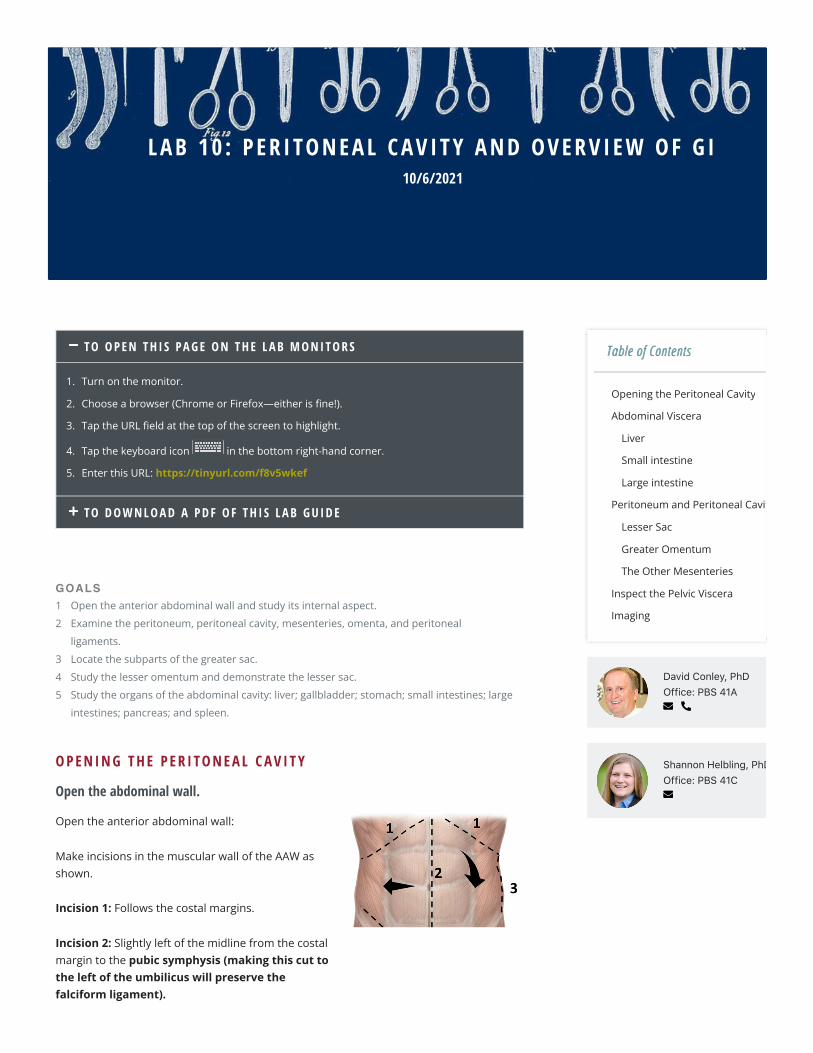
Make incisions in the muscular wall of the AAW asshown.
Incision 1: Follows the costal margins.
Incision 2: Slightly left of the midline from the costalmargin to the pubic symphysis (making this cut tothe left of the umbilicus will preserve thefalciform ligament).
Incision 3: Along the lateral wall from the costalmargin to the iliac crest.
Incision 4: From the pubic symphysis laterally to theanterior superior iliac spine (running above theinguinal canal).
Figure 10.1.
Fold down the left !ap (created by incisions 2 and 3); inspect the internalaspect of the anterior abdominal wall.
Find the lateral umbilical folds: theseare subtle folds created where theperitoneum runs over the inferiorepigastric vessels. Peel the peritoneumaway from the inside of the abdominalwall. Locate the inferior epigastricvessels.
Figure 10.2.
CLINICAL CORRELATIONRecall their role in determining direct vs. indirect inguinal hernias. Identify the bordersof Hesselbach’s triangle from this internal surface.
On each side, the inferior epigastricvessels pass under the arcuate line to enterthe rectus sheath, posterior to the rectusabdominis muscles. Within the rectussheath, the inferior epigastric artery suppliesthe rectus muscle and anastomoses with thesuperior epigastric artery, a terminalbranch of the internal thoracic artery.
This anastomosis could provide an alternateroute for blood to reach the lower limbshould the descending aorta becompromised.
Figure 10.3. Anastomosis between thoracicand abdominal circulations.
CLINICAL CORRELATION Discuss this alternate route with your group. Draw a [owchart.
Fold the right !ap laterally (created by incisions 1 and 4); inspect the internalaspect of the anterior abdominal wall.
Locate the liver, and identify the right and left lobes of the liver—covered in visceralperitoneum.
Examine the sickle-shaped falciform ligament running between the lobes. Thisdouble layer of peritoneum connects the liver to the anterior abdominal wall.
To fully reJect the Jap of the abdominal wall laterally, use scissors or a scalpel totrim the falciform ligament from the surface of the abdominal wall, leaving theligament attached to the liver.
A B D O M I N A L V I S C E R A
COMPLETE ANATOMY: ABDOMINAL V I SCERA
#
Explore and name the organs of the abdominal cavity.
Liver
The sharp inferior border peeks out under the costal margin; reach under thediaphragm to feel the liver’s diaphragmatic surface
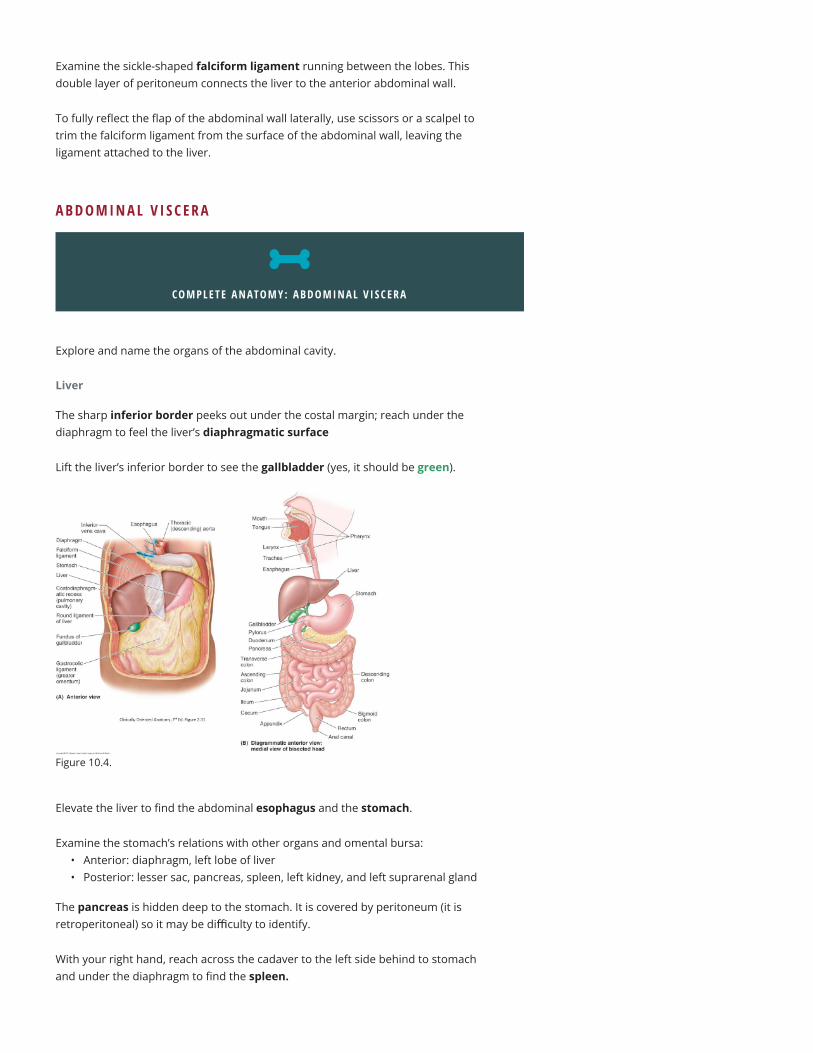
Lift the liver’s inferior border to see the gallbladder (yes, it should be green).
Figure 10.4.
Elevate the liver to Mnd the abdominal esophagus and the stomach.
Examine the stomach’s relations with other organs and omental bursa:• Anterior: diaphragm, left lobe of liver• Posterior: lesser sac, pancreas, spleen, left kidney, and left suprarenal gland
The pancreas is hidden deep to the stomach. It is covered by peritoneum (it isretroperitoneal) so it may be difficulty to identify.
With your right hand, reach across the cadaver to the left side behind to stomachand under the diaphragm to Mnd the spleen.
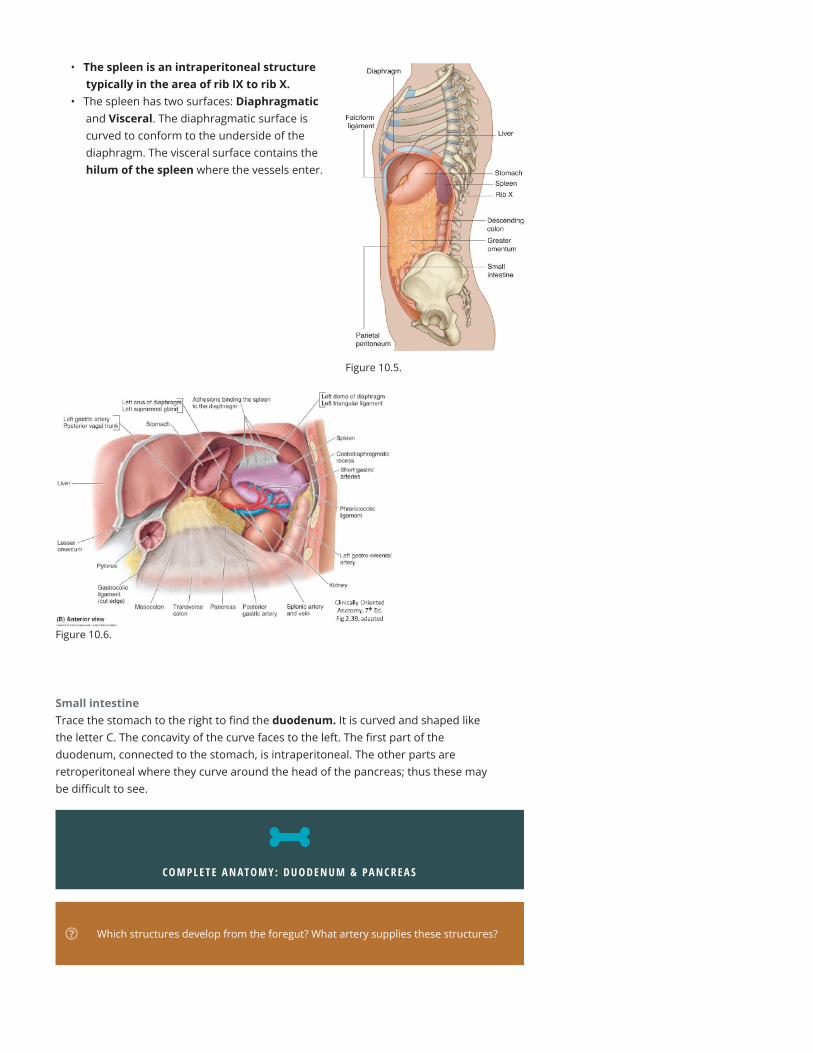
• The spleen is an intraperitoneal structuretypically in the area of rib IX to rib X.
• The spleen has two surfaces: Diaphragmaticand Visceral. The diaphragmatic surface iscurved to conform to the underside of thediaphragm. The visceral surface contains thehilum of the spleen where the vessels enter.
Figure 10.5.
Figure 10.6.
Small intestineTrace the stomach to the right to Mnd the duodenum. It is curved and shaped likethe letter C. The concavity of the curve faces to the left. The Mrst part of theduodenum, connected to the stomach, is intraperitoneal. The other parts areretroperitoneal where they curve around the head of the pancreas; thus these maybe diQcult to see.
COMPLETE ANATOMY: DUODENUM & PANCREAS
#
Which structures develop from the foregut? What artery supplies these structures?
Distal to the duodenum are the otherparts of the small intestine: jejunumand ileum. Push the small intestine tothe right to Mnd the duodenojejunaljunction. Trace the ileum to the rightlower quadrant to Mnd the ileocecaljunction.
Figure 10.7.
Large intestinePush the small intestine to the left to Mnd the ileocecal junction. Now trace in orderfrom proximal to distal: cecum, appendix (if present), ascending colon, transversecolon (lift greater omentum to see it), descending colon, sigmoid colon, andrectum. Notice how the large intestine forms a box around the small intestine.
Which parts of the GI tract are midgut structures? Hindgut? What arteries supply eachof these?
Figure 10.8. Figure 10.9.
P E R I TO N E U M A N D P E R I TO N E A L C AV I T Y
Use your hands to explore the peritoneal cavity, spaces, omenta, mesenteries,and peritoneal ligaments.
Identify:• Parietal peritoneum (on the body wall)• Visceral peritoneum (on the organs)• The peritoneal cavity is the space between the parietal and visceral peritoneum.
REALIZE that the peritoneal cavity is a “potential” space. In a living person, there isvery little space between the parietal and visceral layers of the peritoneum. Thisspace is occupied by a thin layer of serous Juid that lubricates the organs and bodywall and facilitates their friction-less movements.
The two parts of the peritoneal cavity are the greater sac and the lesser sac. Withthe anterior abdominal wall laid open, you are looking into the greater sac.
Identify These Subparts of the Greater Sac:
• Sub-phrenic spaces between the diaphragm and liver• Hepatorenal recess (aka—Morrison’s pouch) between liver and the right kidney• Paracolic gutters (between ascending/descending colon and lateral wall)• Retrocecal recess (behind the cecum—sometimes the appendix hides here!)• Rectovesical pouch in males—in the pelvis, between rectum and bladder• Recto-uterine pouch and vesico-uterine pouch in females (IF there is a uterus
present)—in the pelvis, between rectum and uterus, and uterus and bladder,respectively.
Figure 10.10.
Lesser SacWhere is the lesser sac? To Mnd it, Mrst we need to identify the lesser omentum. Thelesser omentum is a mesentery that attaches the liver above to the stomach and Mrstpart of the duodenum below.
COMPLETE ANATOMY: OMENTA
#
The lesser omentum has two parts:1 Hepatogastric ligament = very thin,
almost transparent. Connects liver tolesser curvature of stomach.
2 Hepatoduodenal ligament = connectsliver to Mrst part of duodenum (theother parts of the duodenum areretroperitoneal). It is thick, because itcontains the portal triad: the hepaticartery proper, the bile duct, and theportal vein. Feel the structures withinthe hepatoduodenal ligament betweenyour thumb and Mnger.
Figure 10.11.
Now, relocate the falciform ligament that attaches the liver to the AAW. Recall fromembryology that the lesser omentum and falciform ligament are derived from theventral mesentery of the stomach.
The lesser sac (omental bursa) is a blind pouch posterior to the lesser omentumand stomach. It gives the stomach space to move freely while churning.
Boundaries: anterior is the liver, stomach, and lesser omentum; posterior isperitoneum on the posterior abdominal wall.
Figure 10.12.
The lesser and greater sacs communicate viathe Omental foramen (Foramen ofWinslow), located posterior to thehepatoduodenal ligament. Place a Mnger inthe omental foramen.
Anterior to your Unger are the structuresof the portal triad. Posterior to yourUnger is the IVC.
Figure 10.13. Clemente’s Atlas of Anatomy.
Greater OmentumExamine the greater omentum, a double-layer of peritoneum hanging down like afatty apron from the greater curvature of the stomach.
NOTEThe greater omentum may adhere to areas that were previously in[amed, resulting ina constricted appearance.
Figure 10.14.
Identify its main subdivisions:• Gastrocolic ligament (stomach to
transverse colon). This is the part thathangs from the greater curvature of thestomach like an apron.
• Gastrosplenic ligament (stomach tospleen)
• Splenorenal ligament (reach way behindthe spleen to feel it with your Mngertips). Itis the part of the greater omentum thatconnects to the posterior body wall.
Figure 10.15.
The Other MesenteriesLift the greater omentum and identify the transverse colon. The double fold ofperitoneum suspending it from the posterior abdominal wall is the transversemesocolon.
Think back to the boundaries of the lesser sac. Examine the Ggure below and discusshow the transverse mesocolon is related to the lesser sac.
Figure 10.16.
Lift the ileum and jejunum and trace their mesentery proper to the posteriorabdominal wall.
Trace the ileum to the cecum and Mnd the appendix, often folded back behind thececum. Feel for its mesoappendix.
Trace the large intestine until you get to the sigmoid colon. It is suspended by asigmoid mesocolon on the left side.
Figure 10.17.
What is the deGnition of a mesentery, and what are the functions?
Mesenteries, peritoneal ligaments, and omenta are all structures composed of twolayers of peritoneum. Mesenteries attach to the posterior abdominal wall, whileomenta attach to the stomach.
List the structures that have mesenteries, and are thus mobile, and called “peritoneal”organs.
Which organs had a mesentery, but then lost it during development? These organs are“secondarily” retroperitoneal.
I N S P E C T T H E P E LV I C V I S C E R A
We will study the pelvic organs in detail in the coming weeks, but now is a good timeto view them superMcially beneath the peritoneum.
NOTE how the peritoneum on the abdominal wall continues into the pelvic cavity and“drapes” itself over the pelvic viscera—much like a “drop cloth” placed over yourfurniture when you paint the walls.
Identify the organs that it drapes over: rectum, uterus, Fallopian (uterine) tubes,and bladder.
IF you have a female cadaver and it has a uterus, the peritoneum that drapes over itand the Fallopian tubes is called the broad ligament.
Demonstrate it to other lab groups if you have it. See if you can spot the ovaries.
IDENTIFY and probe with your hands the pelvic peritoneal pouches: rectovesicalpouch (male), rectouterine pouch and vesicouterine pouch (female).
These pouches are the inferior-most extent of the greater sac. Why would this be ofclinical importance?
Figure 10.18. Figure 10.19.
Figure 10.20.
I M A G I N G
Open the PACS viewer and navigate to your donor CT. Select CT CHAP to openscans of the chest, abdomen and pelvis.
Practice looking at axial, sagittal, and frontal sections of the abdomen. Try to identifysome main organs of the abdominal cavity:
• Liver: Look for the large grey mass just under the right lung• Spleen: Look along the left side tucked under the diaphragm• Stomach: If you Mnd the stomach you may be able to trace it to the duodenum• Loops of bowel (don’t worry about identifying speciMc parts)
C H E C K L I S T, L A B # 1 0R E V I E W A N D M A K E S U R E Y O U H A V E I D E N T I F I E D E A C H O F T H E S T R U C T U R E SB E L O W .
I N T E R N A L A S P E C T O F A N T E R I O R A B D O M I N A L WA L LInferior epigastric vessels
Superior epigastric vessels
Arcuate line
P E R I TO N E U M A N D P E R I TO N E A L C AV I T YParietal and visceral peritoneum
Peritoneal cavity
Greater sac
Subphrenic spaces
Hepatorenal recess
Paracolic gutters
Retrocecal recess
Rectovesical pouch (in pelvis—male)
Recto-uterine and uterovesical pouches (in pelvis—female, when uterus is present)
Lesser sac
Omental foramen
Lesser omentum
Hepatoduodenal ligament
Hepatogastric ligament
Greater omentum
Gastrocolic ligament
Gastrosplenic ligament
Splenorenal ligament
Mesentery of the small intestine
Transverse mesocolon
Sigmoid mesocolon
A B D O M I N A L V I S C E R ALiver
Diaphragmatic surface
Falciform ligament
Gallbladder
Pancreas (retroperitoneal = may be diecult to see)
Spleen
Abdominal esophagus
Stomach
Home Anatomy Review Labs $

LAB 10 : PER ITONEAL CAV ITY AND OVERV IEW OF G I10/6/2021
Table of ContentsTable of Contents !
Opening the Peritoneal Cavity
Abdominal Viscera
Liver
Small intestine
Large intestine
Peritoneum and Peritoneal Cavity
Lesser Sac
Greater Omentum
The Other Mesenteries
Inspect the Pelvic Viscera
Imaging
David Conley, PhDOffice: PBS 41A
Shannon Helbling, PhDOffice: PBS 41C
"
+
TO O P E N T H I S PA G E O N T H E L A B M O N I TO R S
1. Turn on the monitor.
2. Choose a browser (Chrome or Firefox—either is Gne!).
3. Tap the URL Geld at the top of the screen to highlight.
4. Tap the keyboard icon in the bottom right-hand corner.
5. Enter this URL: https://tinyurl.com/f8v5wkef
TO D O W N L O A D A P D F O F T H I S L A B G U I D E
GOALS1 Open the anterior abdominal wall and study its internal aspect.
2 Examine the peritoneum, peritoneal cavity, mesenteries, omenta, and peritoneal
ligaments.
3 Locate the subparts of the greater sac.
4 Study the lesser omentum and demonstrate the lesser sac.
5 Study the organs of the abdominal cavity: liver; gallbladder; stomach; small intestines; large
intestines; pancreas; and spleen.
O P E N I N G T H E P E R I TO N E A L C AV I T Y
Open the abdominal wall.
Open the anterior abdominal wall:
Make incisions in the muscular wall of the AAW asshown.
Incision 1: Follows the costal margins.
Incision 2: Slightly left of the midline from the costalmargin to the pubic symphysis (making this cut tothe left of the umbilicus will preserve thefalciform ligament).
Incision 3: Along the lateral wall from the costalmargin to the iliac crest.
Incision 4: From the pubic symphysis laterally to theanterior superior iliac spine (running above theinguinal canal).
Figure 10.1.
Fold down the left !ap (created by incisions 2 and 3); inspect the internalaspect of the anterior abdominal wall.
Find the lateral umbilical folds: theseare subtle folds created where theperitoneum runs over the inferiorepigastric vessels. Peel the peritoneumaway from the inside of the abdominalwall. Locate the inferior epigastricvessels.
Figure 10.2.
CLINICAL CORRELATIONRecall their role in determining direct vs. indirect inguinal hernias. Identify the bordersof Hesselbach’s triangle from this internal surface.
On each side, the inferior epigastricvessels pass under the arcuate line to enterthe rectus sheath, posterior to the rectusabdominis muscles. Within the rectussheath, the inferior epigastric artery suppliesthe rectus muscle and anastomoses with thesuperior epigastric artery, a terminalbranch of the internal thoracic artery.
This anastomosis could provide an alternateroute for blood to reach the lower limbshould the descending aorta becompromised.
Figure 10.3. Anastomosis between thoracicand abdominal circulations.
CLINICAL CORRELATION Discuss this alternate route with your group. Draw a [owchart.
Fold the right !ap laterally (created by incisions 1 and 4); inspect the internalaspect of the anterior abdominal wall.
Locate the liver, and identify the right and left lobes of the liver—covered in visceralperitoneum.
Examine the sickle-shaped falciform ligament running between the lobes. Thisdouble layer of peritoneum connects the liver to the anterior abdominal wall.
To fully reJect the Jap of the abdominal wall laterally, use scissors or a scalpel totrim the falciform ligament from the surface of the abdominal wall, leaving theligament attached to the liver.
A B D O M I N A L V I S C E R A
COMPLETE ANATOMY: ABDOMINAL V I SCERA
#
Explore and name the organs of the abdominal cavity.
Liver
The sharp inferior border peeks out under the costal margin; reach under thediaphragm to feel the liver’s diaphragmatic surface
Lift the liver’s inferior border to see the gallbladder (yes, it should be green).
Figure 10.4.
Elevate the liver to Mnd the abdominal esophagus and the stomach.
Examine the stomach’s relations with other organs and omental bursa:• Anterior: diaphragm, left lobe of liver• Posterior: lesser sac, pancreas, spleen, left kidney, and left suprarenal gland
The pancreas is hidden deep to the stomach. It is covered by peritoneum (it isretroperitoneal) so it may be difficulty to identify.
With your right hand, reach across the cadaver to the left side behind to stomachand under the diaphragm to Mnd the spleen.
• The spleen is an intraperitoneal structuretypically in the area of rib IX to rib X.
• The spleen has two surfaces: Diaphragmaticand Visceral. The diaphragmatic surface iscurved to conform to the underside of thediaphragm. The visceral surface contains thehilum of the spleen where the vessels enter.
Figure 10.5.
Figure 10.6.
Small intestineTrace the stomach to the right to Mnd the duodenum. It is curved and shaped likethe letter C. The concavity of the curve faces to the left. The Mrst part of theduodenum, connected to the stomach, is intraperitoneal. The other parts areretroperitoneal where they curve around the head of the pancreas; thus these maybe diQcult to see.
COMPLETE ANATOMY: DUODENUM & PANCREAS
#
Which structures develop from the foregut? What artery supplies these structures?
Distal to the duodenum are the otherparts of the small intestine: jejunumand ileum. Push the small intestine tothe right to Mnd the duodenojejunaljunction. Trace the ileum to the rightlower quadrant to Mnd the ileocecaljunction.
Figure 10.7.
Large intestinePush the small intestine to the left to Mnd the ileocecal junction. Now trace in orderfrom proximal to distal: cecum, appendix (if present), ascending colon, transversecolon (lift greater omentum to see it), descending colon, sigmoid colon, andrectum. Notice how the large intestine forms a box around the small intestine.
Which parts of the GI tract are midgut structures? Hindgut? What arteries supply eachof these?
Figure 10.8. Figure 10.9.
P E R I TO N E U M A N D P E R I TO N E A L C AV I T Y
Use your hands to explore the peritoneal cavity, spaces, omenta, mesenteries,and peritoneal ligaments.
Identify:• Parietal peritoneum (on the body wall)• Visceral peritoneum (on the organs)• The peritoneal cavity is the space between the parietal and visceral peritoneum.
REALIZE that the peritoneal cavity is a “potential” space. In a living person, there isvery little space between the parietal and visceral layers of the peritoneum. Thisspace is occupied by a thin layer of serous Juid that lubricates the organs and bodywall and facilitates their friction-less movements.
The two parts of the peritoneal cavity are the greater sac and the lesser sac. Withthe anterior abdominal wall laid open, you are looking into the greater sac.
Identify These Subparts of the Greater Sac:
• Sub-phrenic spaces between the diaphragm and liver• Hepatorenal recess (aka—Morrison’s pouch) between liver and the right kidney• Paracolic gutters (between ascending/descending colon and lateral wall)• Retrocecal recess (behind the cecum—sometimes the appendix hides here!)• Rectovesical pouch in males—in the pelvis, between rectum and bladder• Recto-uterine pouch and vesico-uterine pouch in females (IF there is a uterus
present)—in the pelvis, between rectum and uterus, and uterus and bladder,respectively.
Figure 10.10.
Lesser SacWhere is the lesser sac? To Mnd it, Mrst we need to identify the lesser omentum. Thelesser omentum is a mesentery that attaches the liver above to the stomach and Mrstpart of the duodenum below.
COMPLETE ANATOMY: OMENTA
#
The lesser omentum has two parts:1 Hepatogastric ligament = very thin,
almost transparent. Connects liver tolesser curvature of stomach.
2 Hepatoduodenal ligament = connectsliver to Mrst part of duodenum (theother parts of the duodenum areretroperitoneal). It is thick, because itcontains the portal triad: the hepaticartery proper, the bile duct, and theportal vein. Feel the structures withinthe hepatoduodenal ligament betweenyour thumb and Mnger.
Figure 10.11.
Now, relocate the falciform ligament that attaches the liver to the AAW. Recall fromembryology that the lesser omentum and falciform ligament are derived from theventral mesentery of the stomach.
The lesser sac (omental bursa) is a blind pouch posterior to the lesser omentumand stomach. It gives the stomach space to move freely while churning.
Boundaries: anterior is the liver, stomach, and lesser omentum; posterior isperitoneum on the posterior abdominal wall.
Figure 10.12.
The lesser and greater sacs communicate viathe Omental foramen (Foramen ofWinslow), located posterior to thehepatoduodenal ligament. Place a Mnger inthe omental foramen.
Anterior to your Unger are the structuresof the portal triad. Posterior to yourUnger is the IVC.
Figure 10.13. Clemente’s Atlas of Anatomy.
Greater OmentumExamine the greater omentum, a double-layer of peritoneum hanging down like afatty apron from the greater curvature of the stomach.
NOTEThe greater omentum may adhere to areas that were previously in[amed, resulting ina constricted appearance.
Figure 10.14.
Identify its main subdivisions:• Gastrocolic ligament (stomach to
transverse colon). This is the part thathangs from the greater curvature of thestomach like an apron.
• Gastrosplenic ligament (stomach tospleen)
• Splenorenal ligament (reach way behindthe spleen to feel it with your Mngertips). Itis the part of the greater omentum thatconnects to the posterior body wall.
Figure 10.15.
The Other MesenteriesLift the greater omentum and identify the transverse colon. The double fold ofperitoneum suspending it from the posterior abdominal wall is the transversemesocolon.
Think back to the boundaries of the lesser sac. Examine the Ggure below and discusshow the transverse mesocolon is related to the lesser sac.
Figure 10.16.
Lift the ileum and jejunum and trace their mesentery proper to the posteriorabdominal wall.
Trace the ileum to the cecum and Mnd the appendix, often folded back behind thececum. Feel for its mesoappendix.
Trace the large intestine until you get to the sigmoid colon. It is suspended by asigmoid mesocolon on the left side.
Figure 10.17.
What is the deGnition of a mesentery, and what are the functions?
Mesenteries, peritoneal ligaments, and omenta are all structures composed of twolayers of peritoneum. Mesenteries attach to the posterior abdominal wall, whileomenta attach to the stomach.
List the structures that have mesenteries, and are thus mobile, and called “peritoneal”organs.
Which organs had a mesentery, but then lost it during development? These organs are“secondarily” retroperitoneal.
I N S P E C T T H E P E LV I C V I S C E R A
We will study the pelvic organs in detail in the coming weeks, but now is a good timeto view them superMcially beneath the peritoneum.
NOTE how the peritoneum on the abdominal wall continues into the pelvic cavity and“drapes” itself over the pelvic viscera—much like a “drop cloth” placed over yourfurniture when you paint the walls.
Identify the organs that it drapes over: rectum, uterus, Fallopian (uterine) tubes,and bladder.
IF you have a female cadaver and it has a uterus, the peritoneum that drapes over itand the Fallopian tubes is called the broad ligament.
Demonstrate it to other lab groups if you have it. See if you can spot the ovaries.
IDENTIFY and probe with your hands the pelvic peritoneal pouches: rectovesicalpouch (male), rectouterine pouch and vesicouterine pouch (female).
These pouches are the inferior-most extent of the greater sac. Why would this be ofclinical importance?
Figure 10.18. Figure 10.19.
Figure 10.20.
I M A G I N G
Open the PACS viewer and navigate to your donor CT. Select CT CHAP to openscans of the chest, abdomen and pelvis.
Practice looking at axial, sagittal, and frontal sections of the abdomen. Try to identifysome main organs of the abdominal cavity:
• Liver: Look for the large grey mass just under the right lung• Spleen: Look along the left side tucked under the diaphragm• Stomach: If you Mnd the stomach you may be able to trace it to the duodenum• Loops of bowel (don’t worry about identifying speciMc parts)
C H E C K L I S T, L A B # 1 0R E V I E W A N D M A K E S U R E Y O U H A V E I D E N T I F I E D E A C H O F T H E S T R U C T U R E SB E L O W .
I N T E R N A L A S P E C T O F A N T E R I O R A B D O M I N A L WA L LInferior epigastric vessels
Superior epigastric vessels
Arcuate line
P E R I TO N E U M A N D P E R I TO N E A L C AV I T YParietal and visceral peritoneum
Peritoneal cavity
Greater sac
Subphrenic spaces
Hepatorenal recess
Paracolic gutters
Retrocecal recess
Rectovesical pouch (in pelvis—male)
Recto-uterine and uterovesical pouches (in pelvis—female, when uterus is present)
Lesser sac
Omental foramen
Lesser omentum
Hepatoduodenal ligament
Hepatogastric ligament
Greater omentum
Gastrocolic ligament
Gastrosplenic ligament
Splenorenal ligament
Mesentery of the small intestine
Transverse mesocolon
Sigmoid mesocolon
A B D O M I N A L V I S C E R ALiver
Diaphragmatic surface
Falciform ligament
Gallbladder
Pancreas (retroperitoneal = may be diecult to see)
Spleen
Abdominal esophagus
Stomach
Home Anatomy Review Labs $
LAB 10 : PER ITONEAL CAV ITY AND OVERV IEW OF G I10/6/2021
Table of ContentsTable of Contents !
Opening the Peritoneal Cavity
Abdominal Viscera
Liver
Small intestine
Large intestine
Peritoneum and Peritoneal Cavity
Lesser Sac
Greater Omentum
The Other Mesenteries
Inspect the Pelvic Viscera
Imaging
David Conley, PhDOffice: PBS 41A
Shannon Helbling, PhDOffice: PBS 41C
"
+
TO O P E N T H I S PA G E O N T H E L A B M O N I TO R S
1. Turn on the monitor.
2. Choose a browser (Chrome or Firefox—either is Gne!).
3. Tap the URL Geld at the top of the screen to highlight.
4. Tap the keyboard icon in the bottom right-hand corner.
5. Enter this URL: https://tinyurl.com/f8v5wkef
TO D O W N L O A D A P D F O F T H I S L A B G U I D E
GOALS1 Open the anterior abdominal wall and study its internal aspect.
2 Examine the peritoneum, peritoneal cavity, mesenteries, omenta, and peritoneal
ligaments.
3 Locate the subparts of the greater sac.
4 Study the lesser omentum and demonstrate the lesser sac.
5 Study the organs of the abdominal cavity: liver; gallbladder; stomach; small intestines; large
intestines; pancreas; and spleen.
O P E N I N G T H E P E R I TO N E A L C AV I T Y
Open the abdominal wall.
Open the anterior abdominal wall:
Make incisions in the muscular wall of the AAW asshown.
Incision 1: Follows the costal margins.
Incision 2: Slightly left of the midline from the costalmargin to the pubic symphysis (making this cut tothe left of the umbilicus will preserve thefalciform ligament).
Incision 3: Along the lateral wall from the costalmargin to the iliac crest.
Incision 4: From the pubic symphysis laterally to theanterior superior iliac spine (running above theinguinal canal).
Figure 10.1.
Fold down the left !ap (created by incisions 2 and 3); inspect the internalaspect of the anterior abdominal wall.
Find the lateral umbilical folds: theseare subtle folds created where theperitoneum runs over the inferiorepigastric vessels. Peel the peritoneumaway from the inside of the abdominalwall. Locate the inferior epigastricvessels.
Figure 10.2.
CLINICAL CORRELATIONRecall their role in determining direct vs. indirect inguinal hernias. Identify the bordersof Hesselbach’s triangle from this internal surface.
On each side, the inferior epigastricvessels pass under the arcuate line to enterthe rectus sheath, posterior to the rectusabdominis muscles. Within the rectussheath, the inferior epigastric artery suppliesthe rectus muscle and anastomoses with thesuperior epigastric artery, a terminalbranch of the internal thoracic artery.
This anastomosis could provide an alternateroute for blood to reach the lower limbshould the descending aorta becompromised.
Figure 10.3. Anastomosis between thoracicand abdominal circulations.
CLINICAL CORRELATION Discuss this alternate route with your group. Draw a [owchart.
Fold the right !ap laterally (created by incisions 1 and 4); inspect the internalaspect of the anterior abdominal wall.
Locate the liver, and identify the right and left lobes of the liver—covered in visceralperitoneum.
Examine the sickle-shaped falciform ligament running between the lobes. Thisdouble layer of peritoneum connects the liver to the anterior abdominal wall.
To fully reJect the Jap of the abdominal wall laterally, use scissors or a scalpel totrim the falciform ligament from the surface of the abdominal wall, leaving theligament attached to the liver.
A B D O M I N A L V I S C E R A
COMPLETE ANATOMY: ABDOMINAL V I SCERA
#
Explore and name the organs of the abdominal cavity.
Liver
The sharp inferior border peeks out under the costal margin; reach under thediaphragm to feel the liver’s diaphragmatic surface
Lift the liver’s inferior border to see the gallbladder (yes, it should be green).
Figure 10.4.
Elevate the liver to Mnd the abdominal esophagus and the stomach.
Examine the stomach’s relations with other organs and omental bursa:• Anterior: diaphragm, left lobe of liver• Posterior: lesser sac, pancreas, spleen, left kidney, and left suprarenal gland
The pancreas is hidden deep to the stomach. It is covered by peritoneum (it isretroperitoneal) so it may be difficulty to identify.
With your right hand, reach across the cadaver to the left side behind to stomachand under the diaphragm to Mnd the spleen.
• The spleen is an intraperitoneal structuretypically in the area of rib IX to rib X.
• The spleen has two surfaces: Diaphragmaticand Visceral. The diaphragmatic surface iscurved to conform to the underside of thediaphragm. The visceral surface contains thehilum of the spleen where the vessels enter.
Figure 10.5.
Figure 10.6.
Small intestineTrace the stomach to the right to Mnd the duodenum. It is curved and shaped likethe letter C. The concavity of the curve faces to the left. The Mrst part of theduodenum, connected to the stomach, is intraperitoneal. The other parts areretroperitoneal where they curve around the head of the pancreas; thus these maybe diQcult to see.
COMPLETE ANATOMY: DUODENUM & PANCREAS
#
Which structures develop from the foregut? What artery supplies these structures?
Distal to the duodenum are the otherparts of the small intestine: jejunumand ileum. Push the small intestine tothe right to Mnd the duodenojejunaljunction. Trace the ileum to the rightlower quadrant to Mnd the ileocecaljunction.
Figure 10.7.
Large intestinePush the small intestine to the left to Mnd the ileocecal junction. Now trace in orderfrom proximal to distal: cecum, appendix (if present), ascending colon, transversecolon (lift greater omentum to see it), descending colon, sigmoid colon, andrectum. Notice how the large intestine forms a box around the small intestine.
Which parts of the GI tract are midgut structures? Hindgut? What arteries supply eachof these?
Figure 10.8. Figure 10.9.
P E R I TO N E U M A N D P E R I TO N E A L C AV I T Y
Use your hands to explore the peritoneal cavity, spaces, omenta, mesenteries,and peritoneal ligaments.
Identify:• Parietal peritoneum (on the body wall)• Visceral peritoneum (on the organs)• The peritoneal cavity is the space between the parietal and visceral peritoneum.
REALIZE that the peritoneal cavity is a “potential” space. In a living person, there isvery little space between the parietal and visceral layers of the peritoneum. Thisspace is occupied by a thin layer of serous Juid that lubricates the organs and bodywall and facilitates their friction-less movements.
The two parts of the peritoneal cavity are the greater sac and the lesser sac. Withthe anterior abdominal wall laid open, you are looking into the greater sac.
Identify These Subparts of the Greater Sac:
• Sub-phrenic spaces between the diaphragm and liver• Hepatorenal recess (aka—Morrison’s pouch) between liver and the right kidney• Paracolic gutters (between ascending/descending colon and lateral wall)• Retrocecal recess (behind the cecum—sometimes the appendix hides here!)• Rectovesical pouch in males—in the pelvis, between rectum and bladder• Recto-uterine pouch and vesico-uterine pouch in females (IF there is a uterus
present)—in the pelvis, between rectum and uterus, and uterus and bladder,respectively.
Figure 10.10.
Lesser SacWhere is the lesser sac? To Mnd it, Mrst we need to identify the lesser omentum. Thelesser omentum is a mesentery that attaches the liver above to the stomach and Mrstpart of the duodenum below.
COMPLETE ANATOMY: OMENTA
#
The lesser omentum has two parts:1 Hepatogastric ligament = very thin,
almost transparent. Connects liver tolesser curvature of stomach.
2 Hepatoduodenal ligament = connectsliver to Mrst part of duodenum (theother parts of the duodenum areretroperitoneal). It is thick, because itcontains the portal triad: the hepaticartery proper, the bile duct, and theportal vein. Feel the structures withinthe hepatoduodenal ligament betweenyour thumb and Mnger.
Figure 10.11.
Now, relocate the falciform ligament that attaches the liver to the AAW. Recall fromembryology that the lesser omentum and falciform ligament are derived from theventral mesentery of the stomach.
The lesser sac (omental bursa) is a blind pouch posterior to the lesser omentumand stomach. It gives the stomach space to move freely while churning.
Boundaries: anterior is the liver, stomach, and lesser omentum; posterior isperitoneum on the posterior abdominal wall.
Figure 10.12.
The lesser and greater sacs communicate viathe Omental foramen (Foramen ofWinslow), located posterior to thehepatoduodenal ligament. Place a Mnger inthe omental foramen.
Anterior to your Unger are the structuresof the portal triad. Posterior to yourUnger is the IVC.
Figure 10.13. Clemente’s Atlas of Anatomy.
Greater OmentumExamine the greater omentum, a double-layer of peritoneum hanging down like afatty apron from the greater curvature of the stomach.
NOTEThe greater omentum may adhere to areas that were previously in[amed, resulting ina constricted appearance.
Figure 10.14.
Identify its main subdivisions:• Gastrocolic ligament (stomach to
transverse colon). This is the part thathangs from the greater curvature of thestomach like an apron.
• Gastrosplenic ligament (stomach tospleen)
• Splenorenal ligament (reach way behindthe spleen to feel it with your Mngertips). Itis the part of the greater omentum thatconnects to the posterior body wall.
Figure 10.15.
The Other MesenteriesLift the greater omentum and identify the transverse colon. The double fold ofperitoneum suspending it from the posterior abdominal wall is the transversemesocolon.
Think back to the boundaries of the lesser sac. Examine the Ggure below and discusshow the transverse mesocolon is related to the lesser sac.
Figure 10.16.
Lift the ileum and jejunum and trace their mesentery proper to the posteriorabdominal wall.
Trace the ileum to the cecum and Mnd the appendix, often folded back behind thececum. Feel for its mesoappendix.
Trace the large intestine until you get to the sigmoid colon. It is suspended by asigmoid mesocolon on the left side.
Figure 10.17.
What is the deGnition of a mesentery, and what are the functions?
Mesenteries, peritoneal ligaments, and omenta are all structures composed of twolayers of peritoneum. Mesenteries attach to the posterior abdominal wall, whileomenta attach to the stomach.
List the structures that have mesenteries, and are thus mobile, and called “peritoneal”organs.
Which organs had a mesentery, but then lost it during development? These organs are“secondarily” retroperitoneal.
I N S P E C T T H E P E LV I C V I S C E R A
We will study the pelvic organs in detail in the coming weeks, but now is a good timeto view them superMcially beneath the peritoneum.
NOTE how the peritoneum on the abdominal wall continues into the pelvic cavity and“drapes” itself over the pelvic viscera—much like a “drop cloth” placed over yourfurniture when you paint the walls.
Identify the organs that it drapes over: rectum, uterus, Fallopian (uterine) tubes,and bladder.
IF you have a female cadaver and it has a uterus, the peritoneum that drapes over itand the Fallopian tubes is called the broad ligament.
Demonstrate it to other lab groups if you have it. See if you can spot the ovaries.
IDENTIFY and probe with your hands the pelvic peritoneal pouches: rectovesicalpouch (male), rectouterine pouch and vesicouterine pouch (female).
These pouches are the inferior-most extent of the greater sac. Why would this be ofclinical importance?
Figure 10.18. Figure 10.19.
Figure 10.20.
I M A G I N G
Open the PACS viewer and navigate to your donor CT. Select CT CHAP to openscans of the chest, abdomen and pelvis.
Practice looking at axial, sagittal, and frontal sections of the abdomen. Try to identifysome main organs of the abdominal cavity:
• Liver: Look for the large grey mass just under the right lung• Spleen: Look along the left side tucked under the diaphragm• Stomach: If you Mnd the stomach you may be able to trace it to the duodenum• Loops of bowel (don’t worry about identifying speciMc parts)
C H E C K L I S T, L A B # 1 0R E V I E W A N D M A K E S U R E Y O U H A V E I D E N T I F I E D E A C H O F T H E S T R U C T U R E SB E L O W .
I N T E R N A L A S P E C T O F A N T E R I O R A B D O M I N A L WA L LInferior epigastric vessels
Superior epigastric vessels
Arcuate line
P E R I TO N E U M A N D P E R I TO N E A L C AV I T YParietal and visceral peritoneum
Peritoneal cavity
Greater sac
Subphrenic spaces
Hepatorenal recess
Paracolic gutters
Retrocecal recess
Rectovesical pouch (in pelvis—male)
Recto-uterine and uterovesical pouches (in pelvis—female, when uterus is present)
Lesser sac
Omental foramen
Lesser omentum
Hepatoduodenal ligament
Hepatogastric ligament
Greater omentum
Gastrocolic ligament
Gastrosplenic ligament
Splenorenal ligament
Mesentery of the small intestine
Transverse mesocolon
Sigmoid mesocolon
A B D O M I N A L V I S C E R ALiver
Diaphragmatic surface
Falciform ligament
Gallbladder
Pancreas (retroperitoneal = may be diecult to see)
Spleen
Abdominal esophagus
Stomach
Home Anatomy Review Labs $
LAB 10 : PER ITONEAL CAV ITY AND OVERV IEW OF G I10/6/2021
Table of ContentsTable of Contents !
Opening the Peritoneal Cavity
Abdominal Viscera
Liver
Small intestine
Large intestine
Peritoneum and Peritoneal Cavity
Lesser Sac
Greater Omentum
The Other Mesenteries
Inspect the Pelvic Viscera
Imaging
David Conley, PhDOffice: PBS 41A
Shannon Helbling, PhDOffice: PBS 41C
"
+
TO O P E N T H I S PA G E O N T H E L A B M O N I TO R S
1. Turn on the monitor.
2. Choose a browser (Chrome or Firefox—either is Gne!).
3. Tap the URL Geld at the top of the screen to highlight.
4. Tap the keyboard icon in the bottom right-hand corner.
5. Enter this URL: https://tinyurl.com/f8v5wkef
TO D O W N L O A D A P D F O F T H I S L A B G U I D E
GOALS1 Open the anterior abdominal wall and study its internal aspect.
2 Examine the peritoneum, peritoneal cavity, mesenteries, omenta, and peritoneal
ligaments.
3 Locate the subparts of the greater sac.
4 Study the lesser omentum and demonstrate the lesser sac.
5 Study the organs of the abdominal cavity: liver; gallbladder; stomach; small intestines; large
intestines; pancreas; and spleen.
O P E N I N G T H E P E R I TO N E A L C AV I T Y
Open the abdominal wall.
Open the anterior abdominal wall:
Make incisions in the muscular wall of the AAW asshown.
Incision 1: Follows the costal margins.
Incision 2: Slightly left of the midline from the costalmargin to the pubic symphysis (making this cut tothe left of the umbilicus will preserve thefalciform ligament).
Incision 3: Along the lateral wall from the costalmargin to the iliac crest.
Incision 4: From the pubic symphysis laterally to theanterior superior iliac spine (running above theinguinal canal).
Figure 10.1.
Fold down the left !ap (created by incisions 2 and 3); inspect the internalaspect of the anterior abdominal wall.
Find the lateral umbilical folds: theseare subtle folds created where theperitoneum runs over the inferiorepigastric vessels. Peel the peritoneumaway from the inside of the abdominalwall. Locate the inferior epigastricvessels.
Figure 10.2.
CLINICAL CORRELATIONRecall their role in determining direct vs. indirect inguinal hernias. Identify the bordersof Hesselbach’s triangle from this internal surface.
On each side, the inferior epigastricvessels pass under the arcuate line to enterthe rectus sheath, posterior to the rectusabdominis muscles. Within the rectussheath, the inferior epigastric artery suppliesthe rectus muscle and anastomoses with thesuperior epigastric artery, a terminalbranch of the internal thoracic artery.
This anastomosis could provide an alternateroute for blood to reach the lower limbshould the descending aorta becompromised.
Figure 10.3. Anastomosis between thoracicand abdominal circulations.
CLINICAL CORRELATION Discuss this alternate route with your group. Draw a [owchart.
Fold the right !ap laterally (created by incisions 1 and 4); inspect the internalaspect of the anterior abdominal wall.
Locate the liver, and identify the right and left lobes of the liver—covered in visceralperitoneum.
Examine the sickle-shaped falciform ligament running between the lobes. Thisdouble layer of peritoneum connects the liver to the anterior abdominal wall.
To fully reJect the Jap of the abdominal wall laterally, use scissors or a scalpel totrim the falciform ligament from the surface of the abdominal wall, leaving theligament attached to the liver.
A B D O M I N A L V I S C E R A
COMPLETE ANATOMY: ABDOMINAL V I SCERA
#
Explore and name the organs of the abdominal cavity.
Liver
The sharp inferior border peeks out under the costal margin; reach under thediaphragm to feel the liver’s diaphragmatic surface
Lift the liver’s inferior border to see the gallbladder (yes, it should be green).
Figure 10.4.
Elevate the liver to Mnd the abdominal esophagus and the stomach.
Examine the stomach’s relations with other organs and omental bursa:• Anterior: diaphragm, left lobe of liver• Posterior: lesser sac, pancreas, spleen, left kidney, and left suprarenal gland
The pancreas is hidden deep to the stomach. It is covered by peritoneum (it isretroperitoneal) so it may be difficulty to identify.
With your right hand, reach across the cadaver to the left side behind to stomachand under the diaphragm to Mnd the spleen.
• The spleen is an intraperitoneal structuretypically in the area of rib IX to rib X.
• The spleen has two surfaces: Diaphragmaticand Visceral. The diaphragmatic surface iscurved to conform to the underside of thediaphragm. The visceral surface contains thehilum of the spleen where the vessels enter.
Figure 10.5.
Figure 10.6.
Small intestineTrace the stomach to the right to Mnd the duodenum. It is curved and shaped likethe letter C. The concavity of the curve faces to the left. The Mrst part of theduodenum, connected to the stomach, is intraperitoneal. The other parts areretroperitoneal where they curve around the head of the pancreas; thus these maybe diQcult to see.
COMPLETE ANATOMY: DUODENUM & PANCREAS
#
Which structures develop from the foregut? What artery supplies these structures?
Distal to the duodenum are the otherparts of the small intestine: jejunumand ileum. Push the small intestine tothe right to Mnd the duodenojejunaljunction. Trace the ileum to the rightlower quadrant to Mnd the ileocecaljunction.
Figure 10.7.
Large intestinePush the small intestine to the left to Mnd the ileocecal junction. Now trace in orderfrom proximal to distal: cecum, appendix (if present), ascending colon, transversecolon (lift greater omentum to see it), descending colon, sigmoid colon, andrectum. Notice how the large intestine forms a box around the small intestine.
Which parts of the GI tract are midgut structures? Hindgut? What arteries supply eachof these?
Figure 10.8. Figure 10.9.
P E R I TO N E U M A N D P E R I TO N E A L C AV I T Y
Use your hands to explore the peritoneal cavity, spaces, omenta, mesenteries,and peritoneal ligaments.
Identify:• Parietal peritoneum (on the body wall)• Visceral peritoneum (on the organs)• The peritoneal cavity is the space between the parietal and visceral peritoneum.
REALIZE that the peritoneal cavity is a “potential” space. In a living person, there isvery little space between the parietal and visceral layers of the peritoneum. Thisspace is occupied by a thin layer of serous Juid that lubricates the organs and bodywall and facilitates their friction-less movements.
The two parts of the peritoneal cavity are the greater sac and the lesser sac. Withthe anterior abdominal wall laid open, you are looking into the greater sac.
Identify These Subparts of the Greater Sac:
• Sub-phrenic spaces between the diaphragm and liver• Hepatorenal recess (aka—Morrison’s pouch) between liver and the right kidney• Paracolic gutters (between ascending/descending colon and lateral wall)• Retrocecal recess (behind the cecum—sometimes the appendix hides here!)• Rectovesical pouch in males—in the pelvis, between rectum and bladder• Recto-uterine pouch and vesico-uterine pouch in females (IF there is a uterus
present)—in the pelvis, between rectum and uterus, and uterus and bladder,respectively.
Figure 10.10.
Lesser SacWhere is the lesser sac? To Mnd it, Mrst we need to identify the lesser omentum. Thelesser omentum is a mesentery that attaches the liver above to the stomach and Mrstpart of the duodenum below.
COMPLETE ANATOMY: OMENTA
#
The lesser omentum has two parts:1 Hepatogastric ligament = very thin,
almost transparent. Connects liver tolesser curvature of stomach.
2 Hepatoduodenal ligament = connectsliver to Mrst part of duodenum (theother parts of the duodenum areretroperitoneal). It is thick, because itcontains the portal triad: the hepaticartery proper, the bile duct, and theportal vein. Feel the structures withinthe hepatoduodenal ligament betweenyour thumb and Mnger.
Figure 10.11.
Now, relocate the falciform ligament that attaches the liver to the AAW. Recall fromembryology that the lesser omentum and falciform ligament are derived from theventral mesentery of the stomach.
The lesser sac (omental bursa) is a blind pouch posterior to the lesser omentumand stomach. It gives the stomach space to move freely while churning.
Boundaries: anterior is the liver, stomach, and lesser omentum; posterior isperitoneum on the posterior abdominal wall.
Figure 10.12.
The lesser and greater sacs communicate viathe Omental foramen (Foramen ofWinslow), located posterior to thehepatoduodenal ligament. Place a Mnger inthe omental foramen.
Anterior to your Unger are the structuresof the portal triad. Posterior to yourUnger is the IVC.
Figure 10.13. Clemente’s Atlas of Anatomy.
Greater OmentumExamine the greater omentum, a double-layer of peritoneum hanging down like afatty apron from the greater curvature of the stomach.
NOTEThe greater omentum may adhere to areas that were previously in[amed, resulting ina constricted appearance.
Figure 10.14.
Identify its main subdivisions:• Gastrocolic ligament (stomach to
transverse colon). This is the part thathangs from the greater curvature of thestomach like an apron.
• Gastrosplenic ligament (stomach tospleen)
• Splenorenal ligament (reach way behindthe spleen to feel it with your Mngertips). Itis the part of the greater omentum thatconnects to the posterior body wall.
Figure 10.15.
The Other MesenteriesLift the greater omentum and identify the transverse colon. The double fold ofperitoneum suspending it from the posterior abdominal wall is the transversemesocolon.
Think back to the boundaries of the lesser sac. Examine the Ggure below and discusshow the transverse mesocolon is related to the lesser sac.
Figure 10.16.
Lift the ileum and jejunum and trace their mesentery proper to the posteriorabdominal wall.
Trace the ileum to the cecum and Mnd the appendix, often folded back behind thececum. Feel for its mesoappendix.
Trace the large intestine until you get to the sigmoid colon. It is suspended by asigmoid mesocolon on the left side.
Figure 10.17.
What is the deGnition of a mesentery, and what are the functions?
Mesenteries, peritoneal ligaments, and omenta are all structures composed of twolayers of peritoneum. Mesenteries attach to the posterior abdominal wall, whileomenta attach to the stomach.
List the structures that have mesenteries, and are thus mobile, and called “peritoneal”organs.
Which organs had a mesentery, but then lost it during development? These organs are“secondarily” retroperitoneal.
I N S P E C T T H E P E LV I C V I S C E R A
We will study the pelvic organs in detail in the coming weeks, but now is a good timeto view them superMcially beneath the peritoneum.
NOTE how the peritoneum on the abdominal wall continues into the pelvic cavity and“drapes” itself over the pelvic viscera—much like a “drop cloth” placed over yourfurniture when you paint the walls.
Identify the organs that it drapes over: rectum, uterus, Fallopian (uterine) tubes,and bladder.
IF you have a female cadaver and it has a uterus, the peritoneum that drapes over itand the Fallopian tubes is called the broad ligament.
Demonstrate it to other lab groups if you have it. See if you can spot the ovaries.
IDENTIFY and probe with your hands the pelvic peritoneal pouches: rectovesicalpouch (male), rectouterine pouch and vesicouterine pouch (female).
These pouches are the inferior-most extent of the greater sac. Why would this be ofclinical importance?
Figure 10.18. Figure 10.19.
Figure 10.20.
I M A G I N G
Open the PACS viewer and navigate to your donor CT. Select CT CHAP to openscans of the chest, abdomen and pelvis.
Practice looking at axial, sagittal, and frontal sections of the abdomen. Try to identifysome main organs of the abdominal cavity:
• Liver: Look for the large grey mass just under the right lung• Spleen: Look along the left side tucked under the diaphragm• Stomach: If you Mnd the stomach you may be able to trace it to the duodenum• Loops of bowel (don’t worry about identifying speciMc parts)
C H E C K L I S T, L A B # 1 0R E V I E W A N D M A K E S U R E Y O U H A V E I D E N T I F I E D E A C H O F T H E S T R U C T U R E SB E L O W .
I N T E R N A L A S P E C T O F A N T E R I O R A B D O M I N A L WA L LInferior epigastric vessels
Superior epigastric vessels
Arcuate line
P E R I TO N E U M A N D P E R I TO N E A L C AV I T YParietal and visceral peritoneum
Peritoneal cavity
Greater sac
Subphrenic spaces
Hepatorenal recess
Paracolic gutters
Retrocecal recess
Rectovesical pouch (in pelvis—male)
Recto-uterine and uterovesical pouches (in pelvis—female, when uterus is present)
Lesser sac
Omental foramen
Lesser omentum
Hepatoduodenal ligament
Hepatogastric ligament
Greater omentum
Gastrocolic ligament
Gastrosplenic ligament
Splenorenal ligament
Mesentery of the small intestine
Transverse mesocolon
Sigmoid mesocolon
A B D O M I N A L V I S C E R ALiver
Diaphragmatic surface
Falciform ligament
Gallbladder
Pancreas (retroperitoneal = may be diecult to see)
Spleen
Abdominal esophagus
Stomach
Home Anatomy Review Labs $

LAB 10 : PER ITONEAL CAV ITY AND OVERV IEW OF G I10/6/2021
Table of ContentsTable of Contents !
Opening the Peritoneal Cavity
Abdominal Viscera
Liver
Small intestine
Large intestine
Peritoneum and Peritoneal Cavity
Lesser Sac
Greater Omentum
The Other Mesenteries
Inspect the Pelvic Viscera
Imaging
David Conley, PhDOffice: PBS 41A
Shannon Helbling, PhDOffice: PBS 41C
"
+
TO O P E N T H I S PA G E O N T H E L A B M O N I TO R S
1. Turn on the monitor.
2. Choose a browser (Chrome or Firefox—either is Gne!).
3. Tap the URL Geld at the top of the screen to highlight.
4. Tap the keyboard icon in the bottom right-hand corner.
5. Enter this URL: https://tinyurl.com/f8v5wkef
TO D O W N L O A D A P D F O F T H I S L A B G U I D E
GOALS1 Open the anterior abdominal wall and study its internal aspect.
2 Examine the peritoneum, peritoneal cavity, mesenteries, omenta, and peritoneal
ligaments.
3 Locate the subparts of the greater sac.
4 Study the lesser omentum and demonstrate the lesser sac.
5 Study the organs of the abdominal cavity: liver; gallbladder; stomach; small intestines; large
intestines; pancreas; and spleen.
O P E N I N G T H E P E R I TO N E A L C AV I T Y
Open the abdominal wall.
Open the anterior abdominal wall:
Make incisions in the muscular wall of the AAW asshown.
Incision 1: Follows the costal margins.
Incision 2: Slightly left of the midline from the costalmargin to the pubic symphysis (making this cut tothe left of the umbilicus will preserve thefalciform ligament).
Incision 3: Along the lateral wall from the costalmargin to the iliac crest.
Incision 4: From the pubic symphysis laterally to theanterior superior iliac spine (running above theinguinal canal).
Figure 10.1.
Fold down the left !ap (created by incisions 2 and 3); inspect the internalaspect of the anterior abdominal wall.
Find the lateral umbilical folds: theseare subtle folds created where theperitoneum runs over the inferiorepigastric vessels. Peel the peritoneumaway from the inside of the abdominalwall. Locate the inferior epigastricvessels.
Figure 10.2.
CLINICAL CORRELATIONRecall their role in determining direct vs. indirect inguinal hernias. Identify the bordersof Hesselbach’s triangle from this internal surface.
On each side, the inferior epigastricvessels pass under the arcuate line to enterthe rectus sheath, posterior to the rectusabdominis muscles. Within the rectussheath, the inferior epigastric artery suppliesthe rectus muscle and anastomoses with thesuperior epigastric artery, a terminalbranch of the internal thoracic artery.
This anastomosis could provide an alternateroute for blood to reach the lower limbshould the descending aorta becompromised.
Figure 10.3. Anastomosis between thoracicand abdominal circulations.
CLINICAL CORRELATION Discuss this alternate route with your group. Draw a [owchart.
Fold the right !ap laterally (created by incisions 1 and 4); inspect the internalaspect of the anterior abdominal wall.
Locate the liver, and identify the right and left lobes of the liver—covered in visceralperitoneum.
Examine the sickle-shaped falciform ligament running between the lobes. Thisdouble layer of peritoneum connects the liver to the anterior abdominal wall.
To fully reJect the Jap of the abdominal wall laterally, use scissors or a scalpel totrim the falciform ligament from the surface of the abdominal wall, leaving theligament attached to the liver.
A B D O M I N A L V I S C E R A
COMPLETE ANATOMY: ABDOMINAL V I SCERA
#
Explore and name the organs of the abdominal cavity.
Liver
The sharp inferior border peeks out under the costal margin; reach under thediaphragm to feel the liver’s diaphragmatic surface
Lift the liver’s inferior border to see the gallbladder (yes, it should be green).
Figure 10.4.
Elevate the liver to Mnd the abdominal esophagus and the stomach.
Examine the stomach’s relations with other organs and omental bursa:• Anterior: diaphragm, left lobe of liver• Posterior: lesser sac, pancreas, spleen, left kidney, and left suprarenal gland
The pancreas is hidden deep to the stomach. It is covered by peritoneum (it isretroperitoneal) so it may be difficulty to identify.
With your right hand, reach across the cadaver to the left side behind to stomachand under the diaphragm to Mnd the spleen.
• The spleen is an intraperitoneal structuretypically in the area of rib IX to rib X.
• The spleen has two surfaces: Diaphragmaticand Visceral. The diaphragmatic surface iscurved to conform to the underside of thediaphragm. The visceral surface contains thehilum of the spleen where the vessels enter.
Figure 10.5.
Figure 10.6.
Small intestineTrace the stomach to the right to Mnd the duodenum. It is curved and shaped likethe letter C. The concavity of the curve faces to the left. The Mrst part of theduodenum, connected to the stomach, is intraperitoneal. The other parts areretroperitoneal where they curve around the head of the pancreas; thus these maybe diQcult to see.
COMPLETE ANATOMY: DUODENUM & PANCREAS
#
Which structures develop from the foregut? What artery supplies these structures?
Distal to the duodenum are the otherparts of the small intestine: jejunumand ileum. Push the small intestine tothe right to Mnd the duodenojejunaljunction. Trace the ileum to the rightlower quadrant to Mnd the ileocecaljunction.
Figure 10.7.
Large intestinePush the small intestine to the left to Mnd the ileocecal junction. Now trace in orderfrom proximal to distal: cecum, appendix (if present), ascending colon, transversecolon (lift greater omentum to see it), descending colon, sigmoid colon, andrectum. Notice how the large intestine forms a box around the small intestine.
Which parts of the GI tract are midgut structures? Hindgut? What arteries supply eachof these?
Figure 10.8. Figure 10.9.
P E R I TO N E U M A N D P E R I TO N E A L C AV I T Y
Use your hands to explore the peritoneal cavity, spaces, omenta, mesenteries,and peritoneal ligaments.
Identify:• Parietal peritoneum (on the body wall)• Visceral peritoneum (on the organs)• The peritoneal cavity is the space between the parietal and visceral peritoneum.
REALIZE that the peritoneal cavity is a “potential” space. In a living person, there isvery little space between the parietal and visceral layers of the peritoneum. Thisspace is occupied by a thin layer of serous Juid that lubricates the organs and bodywall and facilitates their friction-less movements.
The two parts of the peritoneal cavity are the greater sac and the lesser sac. Withthe anterior abdominal wall laid open, you are looking into the greater sac.
Identify These Subparts of the Greater Sac:
• Sub-phrenic spaces between the diaphragm and liver• Hepatorenal recess (aka—Morrison’s pouch) between liver and the right kidney• Paracolic gutters (between ascending/descending colon and lateral wall)• Retrocecal recess (behind the cecum—sometimes the appendix hides here!)• Rectovesical pouch in males—in the pelvis, between rectum and bladder• Recto-uterine pouch and vesico-uterine pouch in females (IF there is a uterus
present)—in the pelvis, between rectum and uterus, and uterus and bladder,respectively.
Figure 10.10.
Lesser SacWhere is the lesser sac? To Mnd it, Mrst we need to identify the lesser omentum. Thelesser omentum is a mesentery that attaches the liver above to the stomach and Mrstpart of the duodenum below.
COMPLETE ANATOMY: OMENTA
#
The lesser omentum has two parts:1 Hepatogastric ligament = very thin,
almost transparent. Connects liver tolesser curvature of stomach.
2 Hepatoduodenal ligament = connectsliver to Mrst part of duodenum (theother parts of the duodenum areretroperitoneal). It is thick, because itcontains the portal triad: the hepaticartery proper, the bile duct, and theportal vein. Feel the structures withinthe hepatoduodenal ligament betweenyour thumb and Mnger.
Figure 10.11.
Now, relocate the falciform ligament that attaches the liver to the AAW. Recall fromembryology that the lesser omentum and falciform ligament are derived from theventral mesentery of the stomach.
The lesser sac (omental bursa) is a blind pouch posterior to the lesser omentumand stomach. It gives the stomach space to move freely while churning.
Boundaries: anterior is the liver, stomach, and lesser omentum; posterior isperitoneum on the posterior abdominal wall.
Figure 10.12.
The lesser and greater sacs communicate viathe Omental foramen (Foramen ofWinslow), located posterior to thehepatoduodenal ligament. Place a Mnger inthe omental foramen.
Anterior to your Unger are the structuresof the portal triad. Posterior to yourUnger is the IVC.
Figure 10.13. Clemente’s Atlas of Anatomy.
Greater OmentumExamine the greater omentum, a double-layer of peritoneum hanging down like afatty apron from the greater curvature of the stomach.
NOTEThe greater omentum may adhere to areas that were previously in[amed, resulting ina constricted appearance.
Figure 10.14.
Identify its main subdivisions:• Gastrocolic ligament (stomach to
transverse colon). This is the part thathangs from the greater curvature of thestomach like an apron.
• Gastrosplenic ligament (stomach tospleen)
• Splenorenal ligament (reach way behindthe spleen to feel it with your Mngertips). Itis the part of the greater omentum thatconnects to the posterior body wall.
Figure 10.15.
The Other MesenteriesLift the greater omentum and identify the transverse colon. The double fold ofperitoneum suspending it from the posterior abdominal wall is the transversemesocolon.
Think back to the boundaries of the lesser sac. Examine the Ggure below and discusshow the transverse mesocolon is related to the lesser sac.
Figure 10.16.
Lift the ileum and jejunum and trace their mesentery proper to the posteriorabdominal wall.
Trace the ileum to the cecum and Mnd the appendix, often folded back behind thececum. Feel for its mesoappendix.
Trace the large intestine until you get to the sigmoid colon. It is suspended by asigmoid mesocolon on the left side.
Figure 10.17.
What is the deGnition of a mesentery, and what are the functions?
Mesenteries, peritoneal ligaments, and omenta are all structures composed of twolayers of peritoneum. Mesenteries attach to the posterior abdominal wall, whileomenta attach to the stomach.
List the structures that have mesenteries, and are thus mobile, and called “peritoneal”organs.
Which organs had a mesentery, but then lost it during development? These organs are“secondarily” retroperitoneal.
I N S P E C T T H E P E LV I C V I S C E R A
We will study the pelvic organs in detail in the coming weeks, but now is a good timeto view them superMcially beneath the peritoneum.
NOTE how the peritoneum on the abdominal wall continues into the pelvic cavity and“drapes” itself over the pelvic viscera—much like a “drop cloth” placed over yourfurniture when you paint the walls.
Identify the organs that it drapes over: rectum, uterus, Fallopian (uterine) tubes,and bladder.
IF you have a female cadaver and it has a uterus, the peritoneum that drapes over itand the Fallopian tubes is called the broad ligament.
Demonstrate it to other lab groups if you have it. See if you can spot the ovaries.
IDENTIFY and probe with your hands the pelvic peritoneal pouches: rectovesicalpouch (male), rectouterine pouch and vesicouterine pouch (female).
These pouches are the inferior-most extent of the greater sac. Why would this be ofclinical importance?
Figure 10.18. Figure 10.19.
Figure 10.20.
I M A G I N G
Open the PACS viewer and navigate to your donor CT. Select CT CHAP to openscans of the chest, abdomen and pelvis.
Practice looking at axial, sagittal, and frontal sections of the abdomen. Try to identifysome main organs of the abdominal cavity:
• Liver: Look for the large grey mass just under the right lung• Spleen: Look along the left side tucked under the diaphragm• Stomach: If you Mnd the stomach you may be able to trace it to the duodenum• Loops of bowel (don’t worry about identifying speciMc parts)
C H E C K L I S T, L A B # 1 0R E V I E W A N D M A K E S U R E Y O U H A V E I D E N T I F I E D E A C H O F T H E S T R U C T U R E SB E L O W .
I N T E R N A L A S P E C T O F A N T E R I O R A B D O M I N A L WA L LInferior epigastric vessels
Superior epigastric vessels
Arcuate line
P E R I TO N E U M A N D P E R I TO N E A L C AV I T YParietal and visceral peritoneum
Peritoneal cavity
Greater sac
Subphrenic spaces
Hepatorenal recess
Paracolic gutters
Retrocecal recess
Rectovesical pouch (in pelvis—male)
Recto-uterine and uterovesical pouches (in pelvis—female, when uterus is present)
Lesser sac
Omental foramen
Lesser omentum
Hepatoduodenal ligament
Hepatogastric ligament
Greater omentum
Gastrocolic ligament
Gastrosplenic ligament
Splenorenal ligament
Mesentery of the small intestine
Transverse mesocolon
Sigmoid mesocolon
A B D O M I N A L V I S C E R ALiver
Diaphragmatic surface
Falciform ligament
Gallbladder
Pancreas (retroperitoneal = may be diecult to see)
Spleen
Abdominal esophagus
Stomach
Home Anatomy Review Labs $

LAB 10 : PER ITONEAL CAV ITY AND OVERV IEW OF G I10/6/2021
Table of ContentsTable of Contents !
Opening the Peritoneal Cavity
Abdominal Viscera
Liver
Small intestine
Large intestine
Peritoneum and Peritoneal Cavity
Lesser Sac
Greater Omentum
The Other Mesenteries
Inspect the Pelvic Viscera
Imaging
David Conley, PhDOffice: PBS 41A
Shannon Helbling, PhDOffice: PBS 41C
"
+
TO O P E N T H I S PA G E O N T H E L A B M O N I TO R S
1. Turn on the monitor.
2. Choose a browser (Chrome or Firefox—either is Gne!).
3. Tap the URL Geld at the top of the screen to highlight.
4. Tap the keyboard icon in the bottom right-hand corner.
5. Enter this URL: https://tinyurl.com/f8v5wkef
TO D O W N L O A D A P D F O F T H I S L A B G U I D E
GOALS1 Open the anterior abdominal wall and study its internal aspect.
2 Examine the peritoneum, peritoneal cavity, mesenteries, omenta, and peritoneal
ligaments.
3 Locate the subparts of the greater sac.
4 Study the lesser omentum and demonstrate the lesser sac.
5 Study the organs of the abdominal cavity: liver; gallbladder; stomach; small intestines; large
intestines; pancreas; and spleen.
O P E N I N G T H E P E R I TO N E A L C AV I T Y
Open the abdominal wall.
Open the anterior abdominal wall:
Make incisions in the muscular wall of the AAW asshown.
Incision 1: Follows the costal margins.
Incision 2: Slightly left of the midline from the costalmargin to the pubic symphysis (making this cut tothe left of the umbilicus will preserve thefalciform ligament).
Incision 3: Along the lateral wall from the costalmargin to the iliac crest.
Incision 4: From the pubic symphysis laterally to theanterior superior iliac spine (running above theinguinal canal).
Figure 10.1.
Fold down the left !ap (created by incisions 2 and 3); inspect the internalaspect of the anterior abdominal wall.
Find the lateral umbilical folds: theseare subtle folds created where theperitoneum runs over the inferiorepigastric vessels. Peel the peritoneumaway from the inside of the abdominalwall. Locate the inferior epigastricvessels.
Figure 10.2.
CLINICAL CORRELATIONRecall their role in determining direct vs. indirect inguinal hernias. Identify the bordersof Hesselbach’s triangle from this internal surface.
On each side, the inferior epigastricvessels pass under the arcuate line to enterthe rectus sheath, posterior to the rectusabdominis muscles. Within the rectussheath, the inferior epigastric artery suppliesthe rectus muscle and anastomoses with thesuperior epigastric artery, a terminalbranch of the internal thoracic artery.
This anastomosis could provide an alternateroute for blood to reach the lower limbshould the descending aorta becompromised.
Figure 10.3. Anastomosis between thoracicand abdominal circulations.
CLINICAL CORRELATION Discuss this alternate route with your group. Draw a [owchart.
Fold the right !ap laterally (created by incisions 1 and 4); inspect the internalaspect of the anterior abdominal wall.
Locate the liver, and identify the right and left lobes of the liver—covered in visceralperitoneum.
Examine the sickle-shaped falciform ligament running between the lobes. Thisdouble layer of peritoneum connects the liver to the anterior abdominal wall.
To fully reJect the Jap of the abdominal wall laterally, use scissors or a scalpel totrim the falciform ligament from the surface of the abdominal wall, leaving theligament attached to the liver.
A B D O M I N A L V I S C E R A
COMPLETE ANATOMY: ABDOMINAL V I SCERA
#
Explore and name the organs of the abdominal cavity.
Liver
The sharp inferior border peeks out under the costal margin; reach under thediaphragm to feel the liver’s diaphragmatic surface
Lift the liver’s inferior border to see the gallbladder (yes, it should be green).
Figure 10.4.
Elevate the liver to Mnd the abdominal esophagus and the stomach.
Examine the stomach’s relations with other organs and omental bursa:• Anterior: diaphragm, left lobe of liver• Posterior: lesser sac, pancreas, spleen, left kidney, and left suprarenal gland
The pancreas is hidden deep to the stomach. It is covered by peritoneum (it isretroperitoneal) so it may be difficulty to identify.
With your right hand, reach across the cadaver to the left side behind to stomachand under the diaphragm to Mnd the spleen.
• The spleen is an intraperitoneal structuretypically in the area of rib IX to rib X.
• The spleen has two surfaces: Diaphragmaticand Visceral. The diaphragmatic surface iscurved to conform to the underside of thediaphragm. The visceral surface contains thehilum of the spleen where the vessels enter.
Figure 10.5.
Figure 10.6.
Small intestineTrace the stomach to the right to Mnd the duodenum. It is curved and shaped likethe letter C. The concavity of the curve faces to the left. The Mrst part of theduodenum, connected to the stomach, is intraperitoneal. The other parts areretroperitoneal where they curve around the head of the pancreas; thus these maybe diQcult to see.
COMPLETE ANATOMY: DUODENUM & PANCREAS
#
Which structures develop from the foregut? What artery supplies these structures?
Distal to the duodenum are the otherparts of the small intestine: jejunumand ileum. Push the small intestine tothe right to Mnd the duodenojejunaljunction. Trace the ileum to the rightlower quadrant to Mnd the ileocecaljunction.
Figure 10.7.
Large intestinePush the small intestine to the left to Mnd the ileocecal junction. Now trace in orderfrom proximal to distal: cecum, appendix (if present), ascending colon, transversecolon (lift greater omentum to see it), descending colon, sigmoid colon, andrectum. Notice how the large intestine forms a box around the small intestine.
Which parts of the GI tract are midgut structures? Hindgut? What arteries supply eachof these?
Figure 10.8. Figure 10.9.
P E R I TO N E U M A N D P E R I TO N E A L C AV I T Y
Use your hands to explore the peritoneal cavity, spaces, omenta, mesenteries,and peritoneal ligaments.
Identify:• Parietal peritoneum (on the body wall)• Visceral peritoneum (on the organs)• The peritoneal cavity is the space between the parietal and visceral peritoneum.
REALIZE that the peritoneal cavity is a “potential” space. In a living person, there isvery little space between the parietal and visceral layers of the peritoneum. Thisspace is occupied by a thin layer of serous Juid that lubricates the organs and bodywall and facilitates their friction-less movements.
The two parts of the peritoneal cavity are the greater sac and the lesser sac. Withthe anterior abdominal wall laid open, you are looking into the greater sac.
Identify These Subparts of the Greater Sac:
• Sub-phrenic spaces between the diaphragm and liver• Hepatorenal recess (aka—Morrison’s pouch) between liver and the right kidney• Paracolic gutters (between ascending/descending colon and lateral wall)• Retrocecal recess (behind the cecum—sometimes the appendix hides here!)• Rectovesical pouch in males—in the pelvis, between rectum and bladder• Recto-uterine pouch and vesico-uterine pouch in females (IF there is a uterus
present)—in the pelvis, between rectum and uterus, and uterus and bladder,respectively.
Figure 10.10.
Lesser SacWhere is the lesser sac? To Mnd it, Mrst we need to identify the lesser omentum. Thelesser omentum is a mesentery that attaches the liver above to the stomach and Mrstpart of the duodenum below.
COMPLETE ANATOMY: OMENTA
#
The lesser omentum has two parts:1 Hepatogastric ligament = very thin,
almost transparent. Connects liver tolesser curvature of stomach.
2 Hepatoduodenal ligament = connectsliver to Mrst part of duodenum (theother parts of the duodenum areretroperitoneal). It is thick, because itcontains the portal triad: the hepaticartery proper, the bile duct, and theportal vein. Feel the structures withinthe hepatoduodenal ligament betweenyour thumb and Mnger.
Figure 10.11.
Now, relocate the falciform ligament that attaches the liver to the AAW. Recall fromembryology that the lesser omentum and falciform ligament are derived from theventral mesentery of the stomach.
The lesser sac (omental bursa) is a blind pouch posterior to the lesser omentumand stomach. It gives the stomach space to move freely while churning.
Boundaries: anterior is the liver, stomach, and lesser omentum; posterior isperitoneum on the posterior abdominal wall.
Figure 10.12.
The lesser and greater sacs communicate viathe Omental foramen (Foramen ofWinslow), located posterior to thehepatoduodenal ligament. Place a Mnger inthe omental foramen.
Anterior to your Unger are the structuresof the portal triad. Posterior to yourUnger is the IVC.
Figure 10.13. Clemente’s Atlas of Anatomy.
Greater OmentumExamine the greater omentum, a double-layer of peritoneum hanging down like afatty apron from the greater curvature of the stomach.
NOTEThe greater omentum may adhere to areas that were previously in[amed, resulting ina constricted appearance.
Figure 10.14.
Identify its main subdivisions:• Gastrocolic ligament (stomach to
transverse colon). This is the part thathangs from the greater curvature of thestomach like an apron.
• Gastrosplenic ligament (stomach tospleen)
• Splenorenal ligament (reach way behindthe spleen to feel it with your Mngertips). Itis the part of the greater omentum thatconnects to the posterior body wall.
Figure 10.15.
The Other MesenteriesLift the greater omentum and identify the transverse colon. The double fold ofperitoneum suspending it from the posterior abdominal wall is the transversemesocolon.
Think back to the boundaries of the lesser sac. Examine the Ggure below and discusshow the transverse mesocolon is related to the lesser sac.
Figure 10.16.
Lift the ileum and jejunum and trace their mesentery proper to the posteriorabdominal wall.
Trace the ileum to the cecum and Mnd the appendix, often folded back behind thececum. Feel for its mesoappendix.
Trace the large intestine until you get to the sigmoid colon. It is suspended by asigmoid mesocolon on the left side.
Figure 10.17.
What is the deGnition of a mesentery, and what are the functions?
Mesenteries, peritoneal ligaments, and omenta are all structures composed of twolayers of peritoneum. Mesenteries attach to the posterior abdominal wall, whileomenta attach to the stomach.
List the structures that have mesenteries, and are thus mobile, and called “peritoneal”organs.
Which organs had a mesentery, but then lost it during development? These organs are“secondarily” retroperitoneal.
I N S P E C T T H E P E LV I C V I S C E R A
We will study the pelvic organs in detail in the coming weeks, but now is a good timeto view them superMcially beneath the peritoneum.
NOTE how the peritoneum on the abdominal wall continues into the pelvic cavity and“drapes” itself over the pelvic viscera—much like a “drop cloth” placed over yourfurniture when you paint the walls.
Identify the organs that it drapes over: rectum, uterus, Fallopian (uterine) tubes,and bladder.
IF you have a female cadaver and it has a uterus, the peritoneum that drapes over itand the Fallopian tubes is called the broad ligament.
Demonstrate it to other lab groups if you have it. See if you can spot the ovaries.
IDENTIFY and probe with your hands the pelvic peritoneal pouches: rectovesicalpouch (male), rectouterine pouch and vesicouterine pouch (female).
These pouches are the inferior-most extent of the greater sac. Why would this be ofclinical importance?
Figure 10.18. Figure 10.19.
Figure 10.20.
I M A G I N G
Open the PACS viewer and navigate to your donor CT. Select CT CHAP to openscans of the chest, abdomen and pelvis.
Practice looking at axial, sagittal, and frontal sections of the abdomen. Try to identifysome main organs of the abdominal cavity:
• Liver: Look for the large grey mass just under the right lung• Spleen: Look along the left side tucked under the diaphragm• Stomach: If you Mnd the stomach you may be able to trace it to the duodenum• Loops of bowel (don’t worry about identifying speciMc parts)
C H E C K L I S T, L A B # 1 0R E V I E W A N D M A K E S U R E Y O U H A V E I D E N T I F I E D E A C H O F T H E S T R U C T U R E SB E L O W .
I N T E R N A L A S P E C T O F A N T E R I O R A B D O M I N A L WA L LInferior epigastric vessels
Superior epigastric vessels
Arcuate line
P E R I TO N E U M A N D P E R I TO N E A L C AV I T YParietal and visceral peritoneum
Peritoneal cavity
Greater sac
Subphrenic spaces
Hepatorenal recess
Paracolic gutters
Retrocecal recess
Rectovesical pouch (in pelvis—male)
Recto-uterine and uterovesical pouches (in pelvis—female, when uterus is present)
Lesser sac
Omental foramen
Lesser omentum
Hepatoduodenal ligament
Hepatogastric ligament
Greater omentum
Gastrocolic ligament
Gastrosplenic ligament
Splenorenal ligament
Mesentery of the small intestine
Transverse mesocolon
Sigmoid mesocolon
A B D O M I N A L V I S C E R ALiver
Diaphragmatic surface
Falciform ligament
Gallbladder
Pancreas (retroperitoneal = may be diecult to see)
Spleen
Abdominal esophagus
Stomach
Home Anatomy Review Labs $

LAB 10 : PER ITONEAL CAV ITY AND OVERV IEW OF G I10/6/2021
Table of ContentsTable of Contents !
Opening the Peritoneal Cavity
Abdominal Viscera
Liver
Small intestine
Large intestine
Peritoneum and Peritoneal Cavity
Lesser Sac
Greater Omentum
The Other Mesenteries
Inspect the Pelvic Viscera
Imaging
David Conley, PhDOffice: PBS 41A
Shannon Helbling, PhDOffice: PBS 41C
"
+
TO O P E N T H I S PA G E O N T H E L A B M O N I TO R S
1. Turn on the monitor.
2. Choose a browser (Chrome or Firefox—either is Gne!).
3. Tap the URL Geld at the top of the screen to highlight.
4. Tap the keyboard icon in the bottom right-hand corner.
5. Enter this URL: https://tinyurl.com/f8v5wkef
TO D O W N L O A D A P D F O F T H I S L A B G U I D E
GOALS1 Open the anterior abdominal wall and study its internal aspect.
2 Examine the peritoneum, peritoneal cavity, mesenteries, omenta, and peritoneal
ligaments.
3 Locate the subparts of the greater sac.
4 Study the lesser omentum and demonstrate the lesser sac.
5 Study the organs of the abdominal cavity: liver; gallbladder; stomach; small intestines; large
intestines; pancreas; and spleen.
O P E N I N G T H E P E R I TO N E A L C AV I T Y
Open the abdominal wall.
Open the anterior abdominal wall:
Make incisions in the muscular wall of the AAW asshown.
Incision 1: Follows the costal margins.
Incision 2: Slightly left of the midline from the costalmargin to the pubic symphysis (making this cut tothe left of the umbilicus will preserve thefalciform ligament).
Incision 3: Along the lateral wall from the costalmargin to the iliac crest.
Incision 4: From the pubic symphysis laterally to theanterior superior iliac spine (running above theinguinal canal).
Figure 10.1.
Fold down the left !ap (created by incisions 2 and 3); inspect the internalaspect of the anterior abdominal wall.
Find the lateral umbilical folds: theseare subtle folds created where theperitoneum runs over the inferiorepigastric vessels. Peel the peritoneumaway from the inside of the abdominalwall. Locate the inferior epigastricvessels.
Figure 10.2.
CLINICAL CORRELATIONRecall their role in determining direct vs. indirect inguinal hernias. Identify the bordersof Hesselbach’s triangle from this internal surface.
On each side, the inferior epigastricvessels pass under the arcuate line to enterthe rectus sheath, posterior to the rectusabdominis muscles. Within the rectussheath, the inferior epigastric artery suppliesthe rectus muscle and anastomoses with thesuperior epigastric artery, a terminalbranch of the internal thoracic artery.
This anastomosis could provide an alternateroute for blood to reach the lower limbshould the descending aorta becompromised.
Figure 10.3. Anastomosis between thoracicand abdominal circulations.
CLINICAL CORRELATION Discuss this alternate route with your group. Draw a [owchart.
Fold the right !ap laterally (created by incisions 1 and 4); inspect the internalaspect of the anterior abdominal wall.
Locate the liver, and identify the right and left lobes of the liver—covered in visceralperitoneum.
Examine the sickle-shaped falciform ligament running between the lobes. Thisdouble layer of peritoneum connects the liver to the anterior abdominal wall.
To fully reJect the Jap of the abdominal wall laterally, use scissors or a scalpel totrim the falciform ligament from the surface of the abdominal wall, leaving theligament attached to the liver.
A B D O M I N A L V I S C E R A
COMPLETE ANATOMY: ABDOMINAL V I SCERA
#
Explore and name the organs of the abdominal cavity.
Liver
The sharp inferior border peeks out under the costal margin; reach under thediaphragm to feel the liver’s diaphragmatic surface
Lift the liver’s inferior border to see the gallbladder (yes, it should be green).
Figure 10.4.
Elevate the liver to Mnd the abdominal esophagus and the stomach.
Examine the stomach’s relations with other organs and omental bursa:• Anterior: diaphragm, left lobe of liver• Posterior: lesser sac, pancreas, spleen, left kidney, and left suprarenal gland
The pancreas is hidden deep to the stomach. It is covered by peritoneum (it isretroperitoneal) so it may be difficulty to identify.
With your right hand, reach across the cadaver to the left side behind to stomachand under the diaphragm to Mnd the spleen.
• The spleen is an intraperitoneal structuretypically in the area of rib IX to rib X.
• The spleen has two surfaces: Diaphragmaticand Visceral. The diaphragmatic surface iscurved to conform to the underside of thediaphragm. The visceral surface contains thehilum of the spleen where the vessels enter.
Figure 10.5.
Figure 10.6.
Small intestineTrace the stomach to the right to Mnd the duodenum. It is curved and shaped likethe letter C. The concavity of the curve faces to the left. The Mrst part of theduodenum, connected to the stomach, is intraperitoneal. The other parts areretroperitoneal where they curve around the head of the pancreas; thus these maybe diQcult to see.
COMPLETE ANATOMY: DUODENUM & PANCREAS
#
Which structures develop from the foregut? What artery supplies these structures?
Distal to the duodenum are the otherparts of the small intestine: jejunumand ileum. Push the small intestine tothe right to Mnd the duodenojejunaljunction. Trace the ileum to the rightlower quadrant to Mnd the ileocecaljunction.
Figure 10.7.
Large intestinePush the small intestine to the left to Mnd the ileocecal junction. Now trace in orderfrom proximal to distal: cecum, appendix (if present), ascending colon, transversecolon (lift greater omentum to see it), descending colon, sigmoid colon, andrectum. Notice how the large intestine forms a box around the small intestine.
Which parts of the GI tract are midgut structures? Hindgut? What arteries supply eachof these?
Figure 10.8. Figure 10.9.
P E R I TO N E U M A N D P E R I TO N E A L C AV I T Y
Use your hands to explore the peritoneal cavity, spaces, omenta, mesenteries,and peritoneal ligaments.
Identify:• Parietal peritoneum (on the body wall)• Visceral peritoneum (on the organs)• The peritoneal cavity is the space between the parietal and visceral peritoneum.
REALIZE that the peritoneal cavity is a “potential” space. In a living person, there isvery little space between the parietal and visceral layers of the peritoneum. Thisspace is occupied by a thin layer of serous Juid that lubricates the organs and bodywall and facilitates their friction-less movements.
The two parts of the peritoneal cavity are the greater sac and the lesser sac. Withthe anterior abdominal wall laid open, you are looking into the greater sac.
Identify These Subparts of the Greater Sac:
• Sub-phrenic spaces between the diaphragm and liver• Hepatorenal recess (aka—Morrison’s pouch) between liver and the right kidney• Paracolic gutters (between ascending/descending colon and lateral wall)• Retrocecal recess (behind the cecum—sometimes the appendix hides here!)• Rectovesical pouch in males—in the pelvis, between rectum and bladder• Recto-uterine pouch and vesico-uterine pouch in females (IF there is a uterus
present)—in the pelvis, between rectum and uterus, and uterus and bladder,respectively.
Figure 10.10.
Lesser SacWhere is the lesser sac? To Mnd it, Mrst we need to identify the lesser omentum. Thelesser omentum is a mesentery that attaches the liver above to the stomach and Mrstpart of the duodenum below.
COMPLETE ANATOMY: OMENTA
#
The lesser omentum has two parts:1 Hepatogastric ligament = very thin,
almost transparent. Connects liver tolesser curvature of stomach.
2 Hepatoduodenal ligament = connectsliver to Mrst part of duodenum (theother parts of the duodenum areretroperitoneal). It is thick, because itcontains the portal triad: the hepaticartery proper, the bile duct, and theportal vein. Feel the structures withinthe hepatoduodenal ligament betweenyour thumb and Mnger.
Figure 10.11.
Now, relocate the falciform ligament that attaches the liver to the AAW. Recall fromembryology that the lesser omentum and falciform ligament are derived from theventral mesentery of the stomach.
The lesser sac (omental bursa) is a blind pouch posterior to the lesser omentumand stomach. It gives the stomach space to move freely while churning.
Boundaries: anterior is the liver, stomach, and lesser omentum; posterior isperitoneum on the posterior abdominal wall.
Figure 10.12.
The lesser and greater sacs communicate viathe Omental foramen (Foramen ofWinslow), located posterior to thehepatoduodenal ligament. Place a Mnger inthe omental foramen.
Anterior to your Unger are the structuresof the portal triad. Posterior to yourUnger is the IVC.
Figure 10.13. Clemente’s Atlas of Anatomy.
Greater OmentumExamine the greater omentum, a double-layer of peritoneum hanging down like afatty apron from the greater curvature of the stomach.
NOTEThe greater omentum may adhere to areas that were previously in[amed, resulting ina constricted appearance.
Figure 10.14.
Identify its main subdivisions:• Gastrocolic ligament (stomach to
transverse colon). This is the part thathangs from the greater curvature of thestomach like an apron.
• Gastrosplenic ligament (stomach tospleen)
• Splenorenal ligament (reach way behindthe spleen to feel it with your Mngertips). Itis the part of the greater omentum thatconnects to the posterior body wall.
Figure 10.15.
The Other MesenteriesLift the greater omentum and identify the transverse colon. The double fold ofperitoneum suspending it from the posterior abdominal wall is the transversemesocolon.
Think back to the boundaries of the lesser sac. Examine the Ggure below and discusshow the transverse mesocolon is related to the lesser sac.
Figure 10.16.
Lift the ileum and jejunum and trace their mesentery proper to the posteriorabdominal wall.
Trace the ileum to the cecum and Mnd the appendix, often folded back behind thececum. Feel for its mesoappendix.
Trace the large intestine until you get to the sigmoid colon. It is suspended by asigmoid mesocolon on the left side.
Figure 10.17.
What is the deGnition of a mesentery, and what are the functions?
Mesenteries, peritoneal ligaments, and omenta are all structures composed of twolayers of peritoneum. Mesenteries attach to the posterior abdominal wall, whileomenta attach to the stomach.
List the structures that have mesenteries, and are thus mobile, and called “peritoneal”organs.
Which organs had a mesentery, but then lost it during development? These organs are“secondarily” retroperitoneal.
I N S P E C T T H E P E LV I C V I S C E R A
We will study the pelvic organs in detail in the coming weeks, but now is a good timeto view them superMcially beneath the peritoneum.
NOTE how the peritoneum on the abdominal wall continues into the pelvic cavity and“drapes” itself over the pelvic viscera—much like a “drop cloth” placed over yourfurniture when you paint the walls.
Identify the organs that it drapes over: rectum, uterus, Fallopian (uterine) tubes,and bladder.
IF you have a female cadaver and it has a uterus, the peritoneum that drapes over itand the Fallopian tubes is called the broad ligament.
Demonstrate it to other lab groups if you have it. See if you can spot the ovaries.
IDENTIFY and probe with your hands the pelvic peritoneal pouches: rectovesicalpouch (male), rectouterine pouch and vesicouterine pouch (female).
These pouches are the inferior-most extent of the greater sac. Why would this be ofclinical importance?
Figure 10.18. Figure 10.19.
Figure 10.20.
I M A G I N G
Open the PACS viewer and navigate to your donor CT. Select CT CHAP to openscans of the chest, abdomen and pelvis.
Practice looking at axial, sagittal, and frontal sections of the abdomen. Try to identifysome main organs of the abdominal cavity:
• Liver: Look for the large grey mass just under the right lung• Spleen: Look along the left side tucked under the diaphragm• Stomach: If you Mnd the stomach you may be able to trace it to the duodenum• Loops of bowel (don’t worry about identifying speciMc parts)
C H E C K L I S T, L A B # 1 0R E V I E W A N D M A K E S U R E Y O U H A V E I D E N T I F I E D E A C H O F T H E S T R U C T U R E SB E L O W .
I N T E R N A L A S P E C T O F A N T E R I O R A B D O M I N A L WA L LInferior epigastric vessels
Superior epigastric vessels
Arcuate line
P E R I TO N E U M A N D P E R I TO N E A L C AV I T YParietal and visceral peritoneum
Peritoneal cavity
Greater sac
Subphrenic spaces
Hepatorenal recess
Paracolic gutters
Retrocecal recess
Rectovesical pouch (in pelvis—male)
Recto-uterine and uterovesical pouches (in pelvis—female, when uterus is present)
Lesser sac
Omental foramen
Lesser omentum
Hepatoduodenal ligament
Hepatogastric ligament
Greater omentum
Gastrocolic ligament
Gastrosplenic ligament
Splenorenal ligament
Mesentery of the small intestine
Transverse mesocolon
Sigmoid mesocolon
A B D O M I N A L V I S C E R ALiver
Diaphragmatic surface
Falciform ligament
Gallbladder
Pancreas (retroperitoneal = may be diecult to see)
Spleen
Abdominal esophagus
Stomach
Home Anatomy Review Labs $
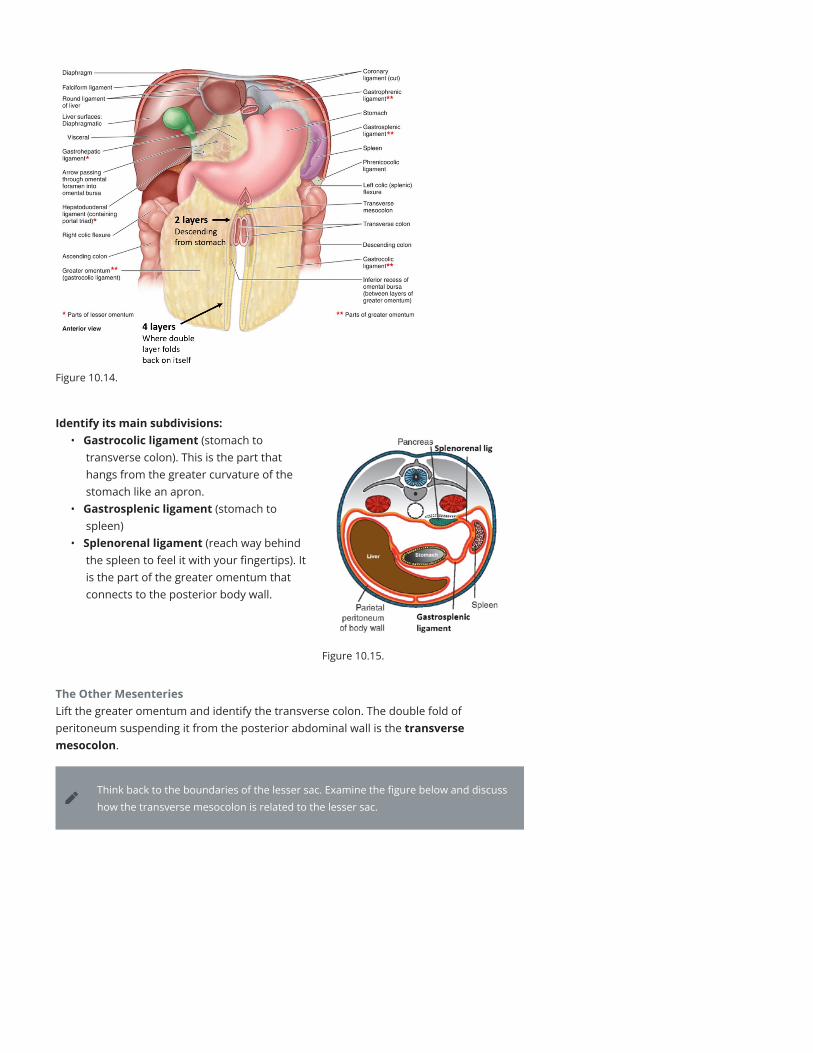
LAB 10 : PER ITONEAL CAV ITY AND OVERV IEW OF G I10/6/2021
Table of ContentsTable of Contents !
Opening the Peritoneal Cavity
Abdominal Viscera
Liver
Small intestine
Large intestine
Peritoneum and Peritoneal Cavity
Lesser Sac
Greater Omentum
The Other Mesenteries
Inspect the Pelvic Viscera
Imaging
David Conley, PhDOffice: PBS 41A
Shannon Helbling, PhDOffice: PBS 41C
"
+
TO O P E N T H I S PA G E O N T H E L A B M O N I TO R S
1. Turn on the monitor.
2. Choose a browser (Chrome or Firefox—either is Gne!).
3. Tap the URL Geld at the top of the screen to highlight.
4. Tap the keyboard icon in the bottom right-hand corner.
5. Enter this URL: https://tinyurl.com/f8v5wkef
TO D O W N L O A D A P D F O F T H I S L A B G U I D E
GOALS1 Open the anterior abdominal wall and study its internal aspect.
2 Examine the peritoneum, peritoneal cavity, mesenteries, omenta, and peritoneal
ligaments.
3 Locate the subparts of the greater sac.
4 Study the lesser omentum and demonstrate the lesser sac.
5 Study the organs of the abdominal cavity: liver; gallbladder; stomach; small intestines; large
intestines; pancreas; and spleen.
O P E N I N G T H E P E R I TO N E A L C AV I T Y
Open the abdominal wall.
Open the anterior abdominal wall:
Make incisions in the muscular wall of the AAW asshown.
Incision 1: Follows the costal margins.
Incision 2: Slightly left of the midline from the costalmargin to the pubic symphysis (making this cut tothe left of the umbilicus will preserve thefalciform ligament).
Incision 3: Along the lateral wall from the costalmargin to the iliac crest.
Incision 4: From the pubic symphysis laterally to theanterior superior iliac spine (running above theinguinal canal).
Figure 10.1.
Fold down the left !ap (created by incisions 2 and 3); inspect the internalaspect of the anterior abdominal wall.
Find the lateral umbilical folds: theseare subtle folds created where theperitoneum runs over the inferiorepigastric vessels. Peel the peritoneumaway from the inside of the abdominalwall. Locate the inferior epigastricvessels.
Figure 10.2.
CLINICAL CORRELATIONRecall their role in determining direct vs. indirect inguinal hernias. Identify the bordersof Hesselbach’s triangle from this internal surface.
On each side, the inferior epigastricvessels pass under the arcuate line to enterthe rectus sheath, posterior to the rectusabdominis muscles. Within the rectussheath, the inferior epigastric artery suppliesthe rectus muscle and anastomoses with thesuperior epigastric artery, a terminalbranch of the internal thoracic artery.
This anastomosis could provide an alternateroute for blood to reach the lower limbshould the descending aorta becompromised.
Figure 10.3. Anastomosis between thoracicand abdominal circulations.
CLINICAL CORRELATION Discuss this alternate route with your group. Draw a [owchart.
Fold the right !ap laterally (created by incisions 1 and 4); inspect the internalaspect of the anterior abdominal wall.
Locate the liver, and identify the right and left lobes of the liver—covered in visceralperitoneum.
Examine the sickle-shaped falciform ligament running between the lobes. Thisdouble layer of peritoneum connects the liver to the anterior abdominal wall.
To fully reJect the Jap of the abdominal wall laterally, use scissors or a scalpel totrim the falciform ligament from the surface of the abdominal wall, leaving theligament attached to the liver.
A B D O M I N A L V I S C E R A
COMPLETE ANATOMY: ABDOMINAL V I SCERA
#
Explore and name the organs of the abdominal cavity.
Liver
The sharp inferior border peeks out under the costal margin; reach under thediaphragm to feel the liver’s diaphragmatic surface
Lift the liver’s inferior border to see the gallbladder (yes, it should be green).
Figure 10.4.
Elevate the liver to Mnd the abdominal esophagus and the stomach.
Examine the stomach’s relations with other organs and omental bursa:• Anterior: diaphragm, left lobe of liver• Posterior: lesser sac, pancreas, spleen, left kidney, and left suprarenal gland
The pancreas is hidden deep to the stomach. It is covered by peritoneum (it isretroperitoneal) so it may be difficulty to identify.
With your right hand, reach across the cadaver to the left side behind to stomachand under the diaphragm to Mnd the spleen.
• The spleen is an intraperitoneal structuretypically in the area of rib IX to rib X.
• The spleen has two surfaces: Diaphragmaticand Visceral. The diaphragmatic surface iscurved to conform to the underside of thediaphragm. The visceral surface contains thehilum of the spleen where the vessels enter.
Figure 10.5.
Figure 10.6.
Small intestineTrace the stomach to the right to Mnd the duodenum. It is curved and shaped likethe letter C. The concavity of the curve faces to the left. The Mrst part of theduodenum, connected to the stomach, is intraperitoneal. The other parts areretroperitoneal where they curve around the head of the pancreas; thus these maybe diQcult to see.
COMPLETE ANATOMY: DUODENUM & PANCREAS
#
Which structures develop from the foregut? What artery supplies these structures?
Distal to the duodenum are the otherparts of the small intestine: jejunumand ileum. Push the small intestine tothe right to Mnd the duodenojejunaljunction. Trace the ileum to the rightlower quadrant to Mnd the ileocecaljunction.
Figure 10.7.
Large intestinePush the small intestine to the left to Mnd the ileocecal junction. Now trace in orderfrom proximal to distal: cecum, appendix (if present), ascending colon, transversecolon (lift greater omentum to see it), descending colon, sigmoid colon, andrectum. Notice how the large intestine forms a box around the small intestine.
Which parts of the GI tract are midgut structures? Hindgut? What arteries supply eachof these?
Figure 10.8. Figure 10.9.
P E R I TO N E U M A N D P E R I TO N E A L C AV I T Y
Use your hands to explore the peritoneal cavity, spaces, omenta, mesenteries,and peritoneal ligaments.
Identify:• Parietal peritoneum (on the body wall)• Visceral peritoneum (on the organs)• The peritoneal cavity is the space between the parietal and visceral peritoneum.
REALIZE that the peritoneal cavity is a “potential” space. In a living person, there isvery little space between the parietal and visceral layers of the peritoneum. Thisspace is occupied by a thin layer of serous Juid that lubricates the organs and bodywall and facilitates their friction-less movements.
The two parts of the peritoneal cavity are the greater sac and the lesser sac. Withthe anterior abdominal wall laid open, you are looking into the greater sac.
Identify These Subparts of the Greater Sac:
• Sub-phrenic spaces between the diaphragm and liver• Hepatorenal recess (aka—Morrison’s pouch) between liver and the right kidney• Paracolic gutters (between ascending/descending colon and lateral wall)• Retrocecal recess (behind the cecum—sometimes the appendix hides here!)• Rectovesical pouch in males—in the pelvis, between rectum and bladder• Recto-uterine pouch and vesico-uterine pouch in females (IF there is a uterus
present)—in the pelvis, between rectum and uterus, and uterus and bladder,respectively.
Figure 10.10.
Lesser SacWhere is the lesser sac? To Mnd it, Mrst we need to identify the lesser omentum. Thelesser omentum is a mesentery that attaches the liver above to the stomach and Mrstpart of the duodenum below.
COMPLETE ANATOMY: OMENTA
#
The lesser omentum has two parts:1 Hepatogastric ligament = very thin,
almost transparent. Connects liver tolesser curvature of stomach.
2 Hepatoduodenal ligament = connectsliver to Mrst part of duodenum (theother parts of the duodenum areretroperitoneal). It is thick, because itcontains the portal triad: the hepaticartery proper, the bile duct, and theportal vein. Feel the structures withinthe hepatoduodenal ligament betweenyour thumb and Mnger.
Figure 10.11.
Now, relocate the falciform ligament that attaches the liver to the AAW. Recall fromembryology that the lesser omentum and falciform ligament are derived from theventral mesentery of the stomach.
The lesser sac (omental bursa) is a blind pouch posterior to the lesser omentumand stomach. It gives the stomach space to move freely while churning.
Boundaries: anterior is the liver, stomach, and lesser omentum; posterior isperitoneum on the posterior abdominal wall.
Figure 10.12.
The lesser and greater sacs communicate viathe Omental foramen (Foramen ofWinslow), located posterior to thehepatoduodenal ligament. Place a Mnger inthe omental foramen.
Anterior to your Unger are the structuresof the portal triad. Posterior to yourUnger is the IVC.
Figure 10.13. Clemente’s Atlas of Anatomy.
Greater OmentumExamine the greater omentum, a double-layer of peritoneum hanging down like afatty apron from the greater curvature of the stomach.
NOTEThe greater omentum may adhere to areas that were previously in[amed, resulting ina constricted appearance.
Figure 10.14.
Identify its main subdivisions:• Gastrocolic ligament (stomach to
transverse colon). This is the part thathangs from the greater curvature of thestomach like an apron.
• Gastrosplenic ligament (stomach tospleen)
• Splenorenal ligament (reach way behindthe spleen to feel it with your Mngertips). Itis the part of the greater omentum thatconnects to the posterior body wall.
Figure 10.15.
The Other MesenteriesLift the greater omentum and identify the transverse colon. The double fold ofperitoneum suspending it from the posterior abdominal wall is the transversemesocolon.
Think back to the boundaries of the lesser sac. Examine the Ggure below and discusshow the transverse mesocolon is related to the lesser sac.
Figure 10.16.
Lift the ileum and jejunum and trace their mesentery proper to the posteriorabdominal wall.
Trace the ileum to the cecum and Mnd the appendix, often folded back behind thececum. Feel for its mesoappendix.
Trace the large intestine until you get to the sigmoid colon. It is suspended by asigmoid mesocolon on the left side.
Figure 10.17.
What is the deGnition of a mesentery, and what are the functions?
Mesenteries, peritoneal ligaments, and omenta are all structures composed of twolayers of peritoneum. Mesenteries attach to the posterior abdominal wall, whileomenta attach to the stomach.
List the structures that have mesenteries, and are thus mobile, and called “peritoneal”organs.
Which organs had a mesentery, but then lost it during development? These organs are“secondarily” retroperitoneal.
I N S P E C T T H E P E LV I C V I S C E R A
We will study the pelvic organs in detail in the coming weeks, but now is a good timeto view them superMcially beneath the peritoneum.
NOTE how the peritoneum on the abdominal wall continues into the pelvic cavity and“drapes” itself over the pelvic viscera—much like a “drop cloth” placed over yourfurniture when you paint the walls.
Identify the organs that it drapes over: rectum, uterus, Fallopian (uterine) tubes,and bladder.
IF you have a female cadaver and it has a uterus, the peritoneum that drapes over itand the Fallopian tubes is called the broad ligament.
Demonstrate it to other lab groups if you have it. See if you can spot the ovaries.
IDENTIFY and probe with your hands the pelvic peritoneal pouches: rectovesicalpouch (male), rectouterine pouch and vesicouterine pouch (female).
These pouches are the inferior-most extent of the greater sac. Why would this be ofclinical importance?
Figure 10.18. Figure 10.19.
Figure 10.20.
I M A G I N G
Open the PACS viewer and navigate to your donor CT. Select CT CHAP to openscans of the chest, abdomen and pelvis.
Practice looking at axial, sagittal, and frontal sections of the abdomen. Try to identifysome main organs of the abdominal cavity:
• Liver: Look for the large grey mass just under the right lung• Spleen: Look along the left side tucked under the diaphragm• Stomach: If you Mnd the stomach you may be able to trace it to the duodenum• Loops of bowel (don’t worry about identifying speciMc parts)
C H E C K L I S T, L A B # 1 0R E V I E W A N D M A K E S U R E Y O U H A V E I D E N T I F I E D E A C H O F T H E S T R U C T U R E SB E L O W .
I N T E R N A L A S P E C T O F A N T E R I O R A B D O M I N A L WA L LInferior epigastric vessels
Superior epigastric vessels
Arcuate line
P E R I TO N E U M A N D P E R I TO N E A L C AV I T YParietal and visceral peritoneum
Peritoneal cavity
Greater sac
Subphrenic spaces
Hepatorenal recess
Paracolic gutters
Retrocecal recess
Rectovesical pouch (in pelvis—male)
Recto-uterine and uterovesical pouches (in pelvis—female, when uterus is present)
Lesser sac
Omental foramen
Lesser omentum
Hepatoduodenal ligament
Hepatogastric ligament
Greater omentum
Gastrocolic ligament
Gastrosplenic ligament
Splenorenal ligament
Mesentery of the small intestine
Transverse mesocolon
Sigmoid mesocolon
A B D O M I N A L V I S C E R ALiver
Diaphragmatic surface
Falciform ligament
Gallbladder
Pancreas (retroperitoneal = may be diecult to see)
Spleen
Abdominal esophagus
Stomach
Home Anatomy Review Labs $

LAB 10 : PER ITONEAL CAV ITY AND OVERV IEW OF G I10/6/2021
Table of ContentsTable of Contents !
Opening the Peritoneal Cavity
Abdominal Viscera
Liver
Small intestine
Large intestine
Peritoneum and Peritoneal Cavity
Lesser Sac
Greater Omentum
The Other Mesenteries
Inspect the Pelvic Viscera
Imaging
David Conley, PhDOffice: PBS 41A
Shannon Helbling, PhDOffice: PBS 41C
"
+
TO O P E N T H I S PA G E O N T H E L A B M O N I TO R S
1. Turn on the monitor.
2. Choose a browser (Chrome or Firefox—either is Gne!).
3. Tap the URL Geld at the top of the screen to highlight.
4. Tap the keyboard icon in the bottom right-hand corner.
5. Enter this URL: https://tinyurl.com/f8v5wkef
TO D O W N L O A D A P D F O F T H I S L A B G U I D E
GOALS1 Open the anterior abdominal wall and study its internal aspect.
2 Examine the peritoneum, peritoneal cavity, mesenteries, omenta, and peritoneal
ligaments.
3 Locate the subparts of the greater sac.
4 Study the lesser omentum and demonstrate the lesser sac.
5 Study the organs of the abdominal cavity: liver; gallbladder; stomach; small intestines; large
intestines; pancreas; and spleen.
O P E N I N G T H E P E R I TO N E A L C AV I T Y
Open the abdominal wall.
Open the anterior abdominal wall:
Make incisions in the muscular wall of the AAW asshown.
Incision 1: Follows the costal margins.
Incision 2: Slightly left of the midline from the costalmargin to the pubic symphysis (making this cut tothe left of the umbilicus will preserve thefalciform ligament).
Incision 3: Along the lateral wall from the costalmargin to the iliac crest.
Incision 4: From the pubic symphysis laterally to theanterior superior iliac spine (running above theinguinal canal).
Figure 10.1.
Fold down the left !ap (created by incisions 2 and 3); inspect the internalaspect of the anterior abdominal wall.
Find the lateral umbilical folds: theseare subtle folds created where theperitoneum runs over the inferiorepigastric vessels. Peel the peritoneumaway from the inside of the abdominalwall. Locate the inferior epigastricvessels.
Figure 10.2.
CLINICAL CORRELATIONRecall their role in determining direct vs. indirect inguinal hernias. Identify the bordersof Hesselbach’s triangle from this internal surface.
On each side, the inferior epigastricvessels pass under the arcuate line to enterthe rectus sheath, posterior to the rectusabdominis muscles. Within the rectussheath, the inferior epigastric artery suppliesthe rectus muscle and anastomoses with thesuperior epigastric artery, a terminalbranch of the internal thoracic artery.
This anastomosis could provide an alternateroute for blood to reach the lower limbshould the descending aorta becompromised.
Figure 10.3. Anastomosis between thoracicand abdominal circulations.
CLINICAL CORRELATION Discuss this alternate route with your group. Draw a [owchart.
Fold the right !ap laterally (created by incisions 1 and 4); inspect the internalaspect of the anterior abdominal wall.
Locate the liver, and identify the right and left lobes of the liver—covered in visceralperitoneum.
Examine the sickle-shaped falciform ligament running between the lobes. Thisdouble layer of peritoneum connects the liver to the anterior abdominal wall.
To fully reJect the Jap of the abdominal wall laterally, use scissors or a scalpel totrim the falciform ligament from the surface of the abdominal wall, leaving theligament attached to the liver.
A B D O M I N A L V I S C E R A
COMPLETE ANATOMY: ABDOMINAL V I SCERA
#
Explore and name the organs of the abdominal cavity.
Liver
The sharp inferior border peeks out under the costal margin; reach under thediaphragm to feel the liver’s diaphragmatic surface
Lift the liver’s inferior border to see the gallbladder (yes, it should be green).
Figure 10.4.
Elevate the liver to Mnd the abdominal esophagus and the stomach.
Examine the stomach’s relations with other organs and omental bursa:• Anterior: diaphragm, left lobe of liver• Posterior: lesser sac, pancreas, spleen, left kidney, and left suprarenal gland
The pancreas is hidden deep to the stomach. It is covered by peritoneum (it isretroperitoneal) so it may be difficulty to identify.
With your right hand, reach across the cadaver to the left side behind to stomachand under the diaphragm to Mnd the spleen.
• The spleen is an intraperitoneal structuretypically in the area of rib IX to rib X.
• The spleen has two surfaces: Diaphragmaticand Visceral. The diaphragmatic surface iscurved to conform to the underside of thediaphragm. The visceral surface contains thehilum of the spleen where the vessels enter.
Figure 10.5.
Figure 10.6.
Small intestineTrace the stomach to the right to Mnd the duodenum. It is curved and shaped likethe letter C. The concavity of the curve faces to the left. The Mrst part of theduodenum, connected to the stomach, is intraperitoneal. The other parts areretroperitoneal where they curve around the head of the pancreas; thus these maybe diQcult to see.
COMPLETE ANATOMY: DUODENUM & PANCREAS
#
Which structures develop from the foregut? What artery supplies these structures?
Distal to the duodenum are the otherparts of the small intestine: jejunumand ileum. Push the small intestine tothe right to Mnd the duodenojejunaljunction. Trace the ileum to the rightlower quadrant to Mnd the ileocecaljunction.
Figure 10.7.
Large intestinePush the small intestine to the left to Mnd the ileocecal junction. Now trace in orderfrom proximal to distal: cecum, appendix (if present), ascending colon, transversecolon (lift greater omentum to see it), descending colon, sigmoid colon, andrectum. Notice how the large intestine forms a box around the small intestine.
Which parts of the GI tract are midgut structures? Hindgut? What arteries supply eachof these?
Figure 10.8. Figure 10.9.
P E R I TO N E U M A N D P E R I TO N E A L C AV I T Y
Use your hands to explore the peritoneal cavity, spaces, omenta, mesenteries,and peritoneal ligaments.
Identify:• Parietal peritoneum (on the body wall)• Visceral peritoneum (on the organs)• The peritoneal cavity is the space between the parietal and visceral peritoneum.
REALIZE that the peritoneal cavity is a “potential” space. In a living person, there isvery little space between the parietal and visceral layers of the peritoneum. Thisspace is occupied by a thin layer of serous Juid that lubricates the organs and bodywall and facilitates their friction-less movements.
The two parts of the peritoneal cavity are the greater sac and the lesser sac. Withthe anterior abdominal wall laid open, you are looking into the greater sac.
Identify These Subparts of the Greater Sac:
• Sub-phrenic spaces between the diaphragm and liver• Hepatorenal recess (aka—Morrison’s pouch) between liver and the right kidney• Paracolic gutters (between ascending/descending colon and lateral wall)• Retrocecal recess (behind the cecum—sometimes the appendix hides here!)• Rectovesical pouch in males—in the pelvis, between rectum and bladder• Recto-uterine pouch and vesico-uterine pouch in females (IF there is a uterus
present)—in the pelvis, between rectum and uterus, and uterus and bladder,respectively.
Figure 10.10.
Lesser SacWhere is the lesser sac? To Mnd it, Mrst we need to identify the lesser omentum. Thelesser omentum is a mesentery that attaches the liver above to the stomach and Mrstpart of the duodenum below.
COMPLETE ANATOMY: OMENTA
#
The lesser omentum has two parts:1 Hepatogastric ligament = very thin,
almost transparent. Connects liver tolesser curvature of stomach.
2 Hepatoduodenal ligament = connectsliver to Mrst part of duodenum (theother parts of the duodenum areretroperitoneal). It is thick, because itcontains the portal triad: the hepaticartery proper, the bile duct, and theportal vein. Feel the structures withinthe hepatoduodenal ligament betweenyour thumb and Mnger.
Figure 10.11.
Now, relocate the falciform ligament that attaches the liver to the AAW. Recall fromembryology that the lesser omentum and falciform ligament are derived from theventral mesentery of the stomach.
The lesser sac (omental bursa) is a blind pouch posterior to the lesser omentumand stomach. It gives the stomach space to move freely while churning.
Boundaries: anterior is the liver, stomach, and lesser omentum; posterior isperitoneum on the posterior abdominal wall.
Figure 10.12.
The lesser and greater sacs communicate viathe Omental foramen (Foramen ofWinslow), located posterior to thehepatoduodenal ligament. Place a Mnger inthe omental foramen.
Anterior to your Unger are the structuresof the portal triad. Posterior to yourUnger is the IVC.
Figure 10.13. Clemente’s Atlas of Anatomy.
Greater OmentumExamine the greater omentum, a double-layer of peritoneum hanging down like afatty apron from the greater curvature of the stomach.
NOTEThe greater omentum may adhere to areas that were previously in[amed, resulting ina constricted appearance.
Figure 10.14.
Identify its main subdivisions:• Gastrocolic ligament (stomach to
transverse colon). This is the part thathangs from the greater curvature of thestomach like an apron.
• Gastrosplenic ligament (stomach tospleen)
• Splenorenal ligament (reach way behindthe spleen to feel it with your Mngertips). Itis the part of the greater omentum thatconnects to the posterior body wall.
Figure 10.15.
The Other MesenteriesLift the greater omentum and identify the transverse colon. The double fold ofperitoneum suspending it from the posterior abdominal wall is the transversemesocolon.
Think back to the boundaries of the lesser sac. Examine the Ggure below and discusshow the transverse mesocolon is related to the lesser sac.
Figure 10.16.
Lift the ileum and jejunum and trace their mesentery proper to the posteriorabdominal wall.
Trace the ileum to the cecum and Mnd the appendix, often folded back behind thececum. Feel for its mesoappendix.
Trace the large intestine until you get to the sigmoid colon. It is suspended by asigmoid mesocolon on the left side.
Figure 10.17.
What is the deGnition of a mesentery, and what are the functions?
Mesenteries, peritoneal ligaments, and omenta are all structures composed of twolayers of peritoneum. Mesenteries attach to the posterior abdominal wall, whileomenta attach to the stomach.
List the structures that have mesenteries, and are thus mobile, and called “peritoneal”organs.
Which organs had a mesentery, but then lost it during development? These organs are“secondarily” retroperitoneal.
I N S P E C T T H E P E LV I C V I S C E R A
We will study the pelvic organs in detail in the coming weeks, but now is a good timeto view them superMcially beneath the peritoneum.
NOTE how the peritoneum on the abdominal wall continues into the pelvic cavity and“drapes” itself over the pelvic viscera—much like a “drop cloth” placed over yourfurniture when you paint the walls.
Identify the organs that it drapes over: rectum, uterus, Fallopian (uterine) tubes,and bladder.
IF you have a female cadaver and it has a uterus, the peritoneum that drapes over itand the Fallopian tubes is called the broad ligament.
Demonstrate it to other lab groups if you have it. See if you can spot the ovaries.
IDENTIFY and probe with your hands the pelvic peritoneal pouches: rectovesicalpouch (male), rectouterine pouch and vesicouterine pouch (female).
These pouches are the inferior-most extent of the greater sac. Why would this be ofclinical importance?
Figure 10.18. Figure 10.19.
Figure 10.20.
I M A G I N G
Open the PACS viewer and navigate to your donor CT. Select CT CHAP to openscans of the chest, abdomen and pelvis.
Practice looking at axial, sagittal, and frontal sections of the abdomen. Try to identifysome main organs of the abdominal cavity:
• Liver: Look for the large grey mass just under the right lung• Spleen: Look along the left side tucked under the diaphragm• Stomach: If you Mnd the stomach you may be able to trace it to the duodenum• Loops of bowel (don’t worry about identifying speciMc parts)
C H E C K L I S T, L A B # 1 0R E V I E W A N D M A K E S U R E Y O U H A V E I D E N T I F I E D E A C H O F T H E S T R U C T U R E SB E L O W .
I N T E R N A L A S P E C T O F A N T E R I O R A B D O M I N A L WA L LInferior epigastric vessels
Superior epigastric vessels
Arcuate line
P E R I TO N E U M A N D P E R I TO N E A L C AV I T YParietal and visceral peritoneum
Peritoneal cavity
Greater sac
Subphrenic spaces
Hepatorenal recess
Paracolic gutters
Retrocecal recess
Rectovesical pouch (in pelvis—male)
Recto-uterine and uterovesical pouches (in pelvis—female, when uterus is present)
Lesser sac
Omental foramen
Lesser omentum
Hepatoduodenal ligament
Hepatogastric ligament
Greater omentum
Gastrocolic ligament
Gastrosplenic ligament
Splenorenal ligament
Mesentery of the small intestine
Transverse mesocolon
Sigmoid mesocolon
A B D O M I N A L V I S C E R ALiver
Diaphragmatic surface
Falciform ligament
Gallbladder
Pancreas (retroperitoneal = may be diecult to see)
Spleen
Abdominal esophagus
Stomach
Home Anatomy Review Labs $

LAB 10 : PER ITONEAL CAV ITY AND OVERV IEW OF G I10/6/2021
Table of ContentsTable of Contents !
Opening the Peritoneal Cavity
Abdominal Viscera
Liver
Small intestine
Large intestine
Peritoneum and Peritoneal Cavity
Lesser Sac
Greater Omentum
The Other Mesenteries
Inspect the Pelvic Viscera
Imaging
David Conley, PhDOffice: PBS 41A
Shannon Helbling, PhDOffice: PBS 41C
"
+
TO O P E N T H I S PA G E O N T H E L A B M O N I TO R S
1. Turn on the monitor.
2. Choose a browser (Chrome or Firefox—either is Gne!).
3. Tap the URL Geld at the top of the screen to highlight.
4. Tap the keyboard icon in the bottom right-hand corner.
5. Enter this URL: https://tinyurl.com/f8v5wkef
TO D O W N L O A D A P D F O F T H I S L A B G U I D E
GOALS1 Open the anterior abdominal wall and study its internal aspect.
2 Examine the peritoneum, peritoneal cavity, mesenteries, omenta, and peritoneal
ligaments.
3 Locate the subparts of the greater sac.
4 Study the lesser omentum and demonstrate the lesser sac.
5 Study the organs of the abdominal cavity: liver; gallbladder; stomach; small intestines; large
intestines; pancreas; and spleen.
O P E N I N G T H E P E R I TO N E A L C AV I T Y
Open the abdominal wall.
Open the anterior abdominal wall:
Make incisions in the muscular wall of the AAW asshown.
Incision 1: Follows the costal margins.
Incision 2: Slightly left of the midline from the costalmargin to the pubic symphysis (making this cut tothe left of the umbilicus will preserve thefalciform ligament).
Incision 3: Along the lateral wall from the costalmargin to the iliac crest.
Incision 4: From the pubic symphysis laterally to theanterior superior iliac spine (running above theinguinal canal).
Figure 10.1.
Fold down the left !ap (created by incisions 2 and 3); inspect the internalaspect of the anterior abdominal wall.
Find the lateral umbilical folds: theseare subtle folds created where theperitoneum runs over the inferiorepigastric vessels. Peel the peritoneumaway from the inside of the abdominalwall. Locate the inferior epigastricvessels.
Figure 10.2.
CLINICAL CORRELATIONRecall their role in determining direct vs. indirect inguinal hernias. Identify the bordersof Hesselbach’s triangle from this internal surface.
On each side, the inferior epigastricvessels pass under the arcuate line to enterthe rectus sheath, posterior to the rectusabdominis muscles. Within the rectussheath, the inferior epigastric artery suppliesthe rectus muscle and anastomoses with thesuperior epigastric artery, a terminalbranch of the internal thoracic artery.
This anastomosis could provide an alternateroute for blood to reach the lower limbshould the descending aorta becompromised.
Figure 10.3. Anastomosis between thoracicand abdominal circulations.
CLINICAL CORRELATION Discuss this alternate route with your group. Draw a [owchart.
Fold the right !ap laterally (created by incisions 1 and 4); inspect the internalaspect of the anterior abdominal wall.
Locate the liver, and identify the right and left lobes of the liver—covered in visceralperitoneum.
Examine the sickle-shaped falciform ligament running between the lobes. Thisdouble layer of peritoneum connects the liver to the anterior abdominal wall.
To fully reJect the Jap of the abdominal wall laterally, use scissors or a scalpel totrim the falciform ligament from the surface of the abdominal wall, leaving theligament attached to the liver.
A B D O M I N A L V I S C E R A
COMPLETE ANATOMY: ABDOMINAL V I SCERA
#
Explore and name the organs of the abdominal cavity.
Liver
The sharp inferior border peeks out under the costal margin; reach under thediaphragm to feel the liver’s diaphragmatic surface
Lift the liver’s inferior border to see the gallbladder (yes, it should be green).
Figure 10.4.
Elevate the liver to Mnd the abdominal esophagus and the stomach.
Examine the stomach’s relations with other organs and omental bursa:• Anterior: diaphragm, left lobe of liver• Posterior: lesser sac, pancreas, spleen, left kidney, and left suprarenal gland
The pancreas is hidden deep to the stomach. It is covered by peritoneum (it isretroperitoneal) so it may be difficulty to identify.
With your right hand, reach across the cadaver to the left side behind to stomachand under the diaphragm to Mnd the spleen.
• The spleen is an intraperitoneal structuretypically in the area of rib IX to rib X.
• The spleen has two surfaces: Diaphragmaticand Visceral. The diaphragmatic surface iscurved to conform to the underside of thediaphragm. The visceral surface contains thehilum of the spleen where the vessels enter.
Figure 10.5.
Figure 10.6.
Small intestineTrace the stomach to the right to Mnd the duodenum. It is curved and shaped likethe letter C. The concavity of the curve faces to the left. The Mrst part of theduodenum, connected to the stomach, is intraperitoneal. The other parts areretroperitoneal where they curve around the head of the pancreas; thus these maybe diQcult to see.
COMPLETE ANATOMY: DUODENUM & PANCREAS
#
Which structures develop from the foregut? What artery supplies these structures?
Distal to the duodenum are the otherparts of the small intestine: jejunumand ileum. Push the small intestine tothe right to Mnd the duodenojejunaljunction. Trace the ileum to the rightlower quadrant to Mnd the ileocecaljunction.
Figure 10.7.
Large intestinePush the small intestine to the left to Mnd the ileocecal junction. Now trace in orderfrom proximal to distal: cecum, appendix (if present), ascending colon, transversecolon (lift greater omentum to see it), descending colon, sigmoid colon, andrectum. Notice how the large intestine forms a box around the small intestine.
Which parts of the GI tract are midgut structures? Hindgut? What arteries supply eachof these?
Figure 10.8. Figure 10.9.
P E R I TO N E U M A N D P E R I TO N E A L C AV I T Y
Use your hands to explore the peritoneal cavity, spaces, omenta, mesenteries,and peritoneal ligaments.
Identify:• Parietal peritoneum (on the body wall)• Visceral peritoneum (on the organs)• The peritoneal cavity is the space between the parietal and visceral peritoneum.
REALIZE that the peritoneal cavity is a “potential” space. In a living person, there isvery little space between the parietal and visceral layers of the peritoneum. Thisspace is occupied by a thin layer of serous Juid that lubricates the organs and bodywall and facilitates their friction-less movements.
The two parts of the peritoneal cavity are the greater sac and the lesser sac. Withthe anterior abdominal wall laid open, you are looking into the greater sac.
Identify These Subparts of the Greater Sac:
• Sub-phrenic spaces between the diaphragm and liver• Hepatorenal recess (aka—Morrison’s pouch) between liver and the right kidney• Paracolic gutters (between ascending/descending colon and lateral wall)• Retrocecal recess (behind the cecum—sometimes the appendix hides here!)• Rectovesical pouch in males—in the pelvis, between rectum and bladder• Recto-uterine pouch and vesico-uterine pouch in females (IF there is a uterus
present)—in the pelvis, between rectum and uterus, and uterus and bladder,respectively.
Figure 10.10.
Lesser SacWhere is the lesser sac? To Mnd it, Mrst we need to identify the lesser omentum. Thelesser omentum is a mesentery that attaches the liver above to the stomach and Mrstpart of the duodenum below.
COMPLETE ANATOMY: OMENTA
#
The lesser omentum has two parts:1 Hepatogastric ligament = very thin,
almost transparent. Connects liver tolesser curvature of stomach.
2 Hepatoduodenal ligament = connectsliver to Mrst part of duodenum (theother parts of the duodenum areretroperitoneal). It is thick, because itcontains the portal triad: the hepaticartery proper, the bile duct, and theportal vein. Feel the structures withinthe hepatoduodenal ligament betweenyour thumb and Mnger.
Figure 10.11.
Now, relocate the falciform ligament that attaches the liver to the AAW. Recall fromembryology that the lesser omentum and falciform ligament are derived from theventral mesentery of the stomach.
The lesser sac (omental bursa) is a blind pouch posterior to the lesser omentumand stomach. It gives the stomach space to move freely while churning.
Boundaries: anterior is the liver, stomach, and lesser omentum; posterior isperitoneum on the posterior abdominal wall.
Figure 10.12.
The lesser and greater sacs communicate viathe Omental foramen (Foramen ofWinslow), located posterior to thehepatoduodenal ligament. Place a Mnger inthe omental foramen.
Anterior to your Unger are the structuresof the portal triad. Posterior to yourUnger is the IVC.
Figure 10.13. Clemente’s Atlas of Anatomy.
Greater OmentumExamine the greater omentum, a double-layer of peritoneum hanging down like afatty apron from the greater curvature of the stomach.
NOTEThe greater omentum may adhere to areas that were previously in[amed, resulting ina constricted appearance.
Figure 10.14.
Identify its main subdivisions:• Gastrocolic ligament (stomach to
transverse colon). This is the part thathangs from the greater curvature of thestomach like an apron.
• Gastrosplenic ligament (stomach tospleen)
• Splenorenal ligament (reach way behindthe spleen to feel it with your Mngertips). Itis the part of the greater omentum thatconnects to the posterior body wall.
Figure 10.15.
The Other MesenteriesLift the greater omentum and identify the transverse colon. The double fold ofperitoneum suspending it from the posterior abdominal wall is the transversemesocolon.
Think back to the boundaries of the lesser sac. Examine the Ggure below and discusshow the transverse mesocolon is related to the lesser sac.
Figure 10.16.
Lift the ileum and jejunum and trace their mesentery proper to the posteriorabdominal wall.
Trace the ileum to the cecum and Mnd the appendix, often folded back behind thececum. Feel for its mesoappendix.
Trace the large intestine until you get to the sigmoid colon. It is suspended by asigmoid mesocolon on the left side.
Figure 10.17.
What is the deGnition of a mesentery, and what are the functions?
Mesenteries, peritoneal ligaments, and omenta are all structures composed of twolayers of peritoneum. Mesenteries attach to the posterior abdominal wall, whileomenta attach to the stomach.
List the structures that have mesenteries, and are thus mobile, and called “peritoneal”organs.
Which organs had a mesentery, but then lost it during development? These organs are“secondarily” retroperitoneal.
I N S P E C T T H E P E LV I C V I S C E R A
We will study the pelvic organs in detail in the coming weeks, but now is a good timeto view them superMcially beneath the peritoneum.
NOTE how the peritoneum on the abdominal wall continues into the pelvic cavity and“drapes” itself over the pelvic viscera—much like a “drop cloth” placed over yourfurniture when you paint the walls.
Identify the organs that it drapes over: rectum, uterus, Fallopian (uterine) tubes,and bladder.
IF you have a female cadaver and it has a uterus, the peritoneum that drapes over itand the Fallopian tubes is called the broad ligament.
Demonstrate it to other lab groups if you have it. See if you can spot the ovaries.
IDENTIFY and probe with your hands the pelvic peritoneal pouches: rectovesicalpouch (male), rectouterine pouch and vesicouterine pouch (female).
These pouches are the inferior-most extent of the greater sac. Why would this be ofclinical importance?
Figure 10.18. Figure 10.19.
Figure 10.20.
I M A G I N G
Open the PACS viewer and navigate to your donor CT. Select CT CHAP to openscans of the chest, abdomen and pelvis.
Practice looking at axial, sagittal, and frontal sections of the abdomen. Try to identifysome main organs of the abdominal cavity:
• Liver: Look for the large grey mass just under the right lung• Spleen: Look along the left side tucked under the diaphragm• Stomach: If you Mnd the stomach you may be able to trace it to the duodenum• Loops of bowel (don’t worry about identifying speciMc parts)
C H E C K L I S T, L A B # 1 0R E V I E W A N D M A K E S U R E Y O U H A V E I D E N T I F I E D E A C H O F T H E S T R U C T U R E SB E L O W .
I N T E R N A L A S P E C T O F A N T E R I O R A B D O M I N A L WA L LInferior epigastric vessels
Superior epigastric vessels
Arcuate line
P E R I TO N E U M A N D P E R I TO N E A L C AV I T YParietal and visceral peritoneum
Peritoneal cavity
Greater sac
Subphrenic spaces
Hepatorenal recess
Paracolic gutters
Retrocecal recess
Rectovesical pouch (in pelvis—male)
Recto-uterine and uterovesical pouches (in pelvis—female, when uterus is present)
Lesser sac
Omental foramen
Lesser omentum
Hepatoduodenal ligament
Hepatogastric ligament
Greater omentum
Gastrocolic ligament
Gastrosplenic ligament
Splenorenal ligament
Mesentery of the small intestine
Transverse mesocolon
Sigmoid mesocolon
A B D O M I N A L V I S C E R ALiver
Diaphragmatic surface
Falciform ligament
Gallbladder
Pancreas (retroperitoneal = may be diecult to see)
Spleen
Abdominal esophagus
Stomach
Home Anatomy Review Labs $

LAB 10 : PER ITONEAL CAV ITY AND OVERV IEW OF G I10/6/2021
Table of ContentsTable of Contents !
Opening the Peritoneal Cavity
Abdominal Viscera
Liver
Small intestine
Large intestine
Peritoneum and Peritoneal Cavity
Lesser Sac
Greater Omentum
The Other Mesenteries
Inspect the Pelvic Viscera
Imaging
David Conley, PhDOffice: PBS 41A
Shannon Helbling, PhDOffice: PBS 41C
"
+
TO O P E N T H I S PA G E O N T H E L A B M O N I TO R S
1. Turn on the monitor.
2. Choose a browser (Chrome or Firefox—either is Gne!).
3. Tap the URL Geld at the top of the screen to highlight.
4. Tap the keyboard icon in the bottom right-hand corner.
5. Enter this URL: https://tinyurl.com/f8v5wkef
TO D O W N L O A D A P D F O F T H I S L A B G U I D E
GOALS1 Open the anterior abdominal wall and study its internal aspect.
2 Examine the peritoneum, peritoneal cavity, mesenteries, omenta, and peritoneal
ligaments.
3 Locate the subparts of the greater sac.
4 Study the lesser omentum and demonstrate the lesser sac.
5 Study the organs of the abdominal cavity: liver; gallbladder; stomach; small intestines; large
intestines; pancreas; and spleen.
O P E N I N G T H E P E R I TO N E A L C AV I T Y
Open the abdominal wall.
Open the anterior abdominal wall:
Make incisions in the muscular wall of the AAW asshown.
Incision 1: Follows the costal margins.
Incision 2: Slightly left of the midline from the costalmargin to the pubic symphysis (making this cut tothe left of the umbilicus will preserve thefalciform ligament).
Incision 3: Along the lateral wall from the costalmargin to the iliac crest.
Incision 4: From the pubic symphysis laterally to theanterior superior iliac spine (running above theinguinal canal).
Figure 10.1.
Fold down the left !ap (created by incisions 2 and 3); inspect the internalaspect of the anterior abdominal wall.
Find the lateral umbilical folds: theseare subtle folds created where theperitoneum runs over the inferiorepigastric vessels. Peel the peritoneumaway from the inside of the abdominalwall. Locate the inferior epigastricvessels.
Figure 10.2.
CLINICAL CORRELATIONRecall their role in determining direct vs. indirect inguinal hernias. Identify the bordersof Hesselbach’s triangle from this internal surface.
On each side, the inferior epigastricvessels pass under the arcuate line to enterthe rectus sheath, posterior to the rectusabdominis muscles. Within the rectussheath, the inferior epigastric artery suppliesthe rectus muscle and anastomoses with thesuperior epigastric artery, a terminalbranch of the internal thoracic artery.
This anastomosis could provide an alternateroute for blood to reach the lower limbshould the descending aorta becompromised.
Figure 10.3. Anastomosis between thoracicand abdominal circulations.
CLINICAL CORRELATION Discuss this alternate route with your group. Draw a [owchart.
Fold the right !ap laterally (created by incisions 1 and 4); inspect the internalaspect of the anterior abdominal wall.
Locate the liver, and identify the right and left lobes of the liver—covered in visceralperitoneum.
Examine the sickle-shaped falciform ligament running between the lobes. Thisdouble layer of peritoneum connects the liver to the anterior abdominal wall.
To fully reJect the Jap of the abdominal wall laterally, use scissors or a scalpel totrim the falciform ligament from the surface of the abdominal wall, leaving theligament attached to the liver.
A B D O M I N A L V I S C E R A
COMPLETE ANATOMY: ABDOMINAL V I SCERA
#
Explore and name the organs of the abdominal cavity.
Liver
The sharp inferior border peeks out under the costal margin; reach under thediaphragm to feel the liver’s diaphragmatic surface
Lift the liver’s inferior border to see the gallbladder (yes, it should be green).
Figure 10.4.
Elevate the liver to Mnd the abdominal esophagus and the stomach.
Examine the stomach’s relations with other organs and omental bursa:• Anterior: diaphragm, left lobe of liver• Posterior: lesser sac, pancreas, spleen, left kidney, and left suprarenal gland
The pancreas is hidden deep to the stomach. It is covered by peritoneum (it isretroperitoneal) so it may be difficulty to identify.
With your right hand, reach across the cadaver to the left side behind to stomachand under the diaphragm to Mnd the spleen.
• The spleen is an intraperitoneal structuretypically in the area of rib IX to rib X.
• The spleen has two surfaces: Diaphragmaticand Visceral. The diaphragmatic surface iscurved to conform to the underside of thediaphragm. The visceral surface contains thehilum of the spleen where the vessels enter.
Figure 10.5.
Figure 10.6.
Small intestineTrace the stomach to the right to Mnd the duodenum. It is curved and shaped likethe letter C. The concavity of the curve faces to the left. The Mrst part of theduodenum, connected to the stomach, is intraperitoneal. The other parts areretroperitoneal where they curve around the head of the pancreas; thus these maybe diQcult to see.
COMPLETE ANATOMY: DUODENUM & PANCREAS
#
Which structures develop from the foregut? What artery supplies these structures?
Distal to the duodenum are the otherparts of the small intestine: jejunumand ileum. Push the small intestine tothe right to Mnd the duodenojejunaljunction. Trace the ileum to the rightlower quadrant to Mnd the ileocecaljunction.
Figure 10.7.
Large intestinePush the small intestine to the left to Mnd the ileocecal junction. Now trace in orderfrom proximal to distal: cecum, appendix (if present), ascending colon, transversecolon (lift greater omentum to see it), descending colon, sigmoid colon, andrectum. Notice how the large intestine forms a box around the small intestine.
Which parts of the GI tract are midgut structures? Hindgut? What arteries supply eachof these?
Figure 10.8. Figure 10.9.
P E R I TO N E U M A N D P E R I TO N E A L C AV I T Y
Use your hands to explore the peritoneal cavity, spaces, omenta, mesenteries,and peritoneal ligaments.
Identify:• Parietal peritoneum (on the body wall)• Visceral peritoneum (on the organs)• The peritoneal cavity is the space between the parietal and visceral peritoneum.
REALIZE that the peritoneal cavity is a “potential” space. In a living person, there isvery little space between the parietal and visceral layers of the peritoneum. Thisspace is occupied by a thin layer of serous Juid that lubricates the organs and bodywall and facilitates their friction-less movements.
The two parts of the peritoneal cavity are the greater sac and the lesser sac. Withthe anterior abdominal wall laid open, you are looking into the greater sac.
Identify These Subparts of the Greater Sac:
• Sub-phrenic spaces between the diaphragm and liver• Hepatorenal recess (aka—Morrison’s pouch) between liver and the right kidney• Paracolic gutters (between ascending/descending colon and lateral wall)• Retrocecal recess (behind the cecum—sometimes the appendix hides here!)• Rectovesical pouch in males—in the pelvis, between rectum and bladder• Recto-uterine pouch and vesico-uterine pouch in females (IF there is a uterus
present)—in the pelvis, between rectum and uterus, and uterus and bladder,respectively.
Figure 10.10.
Lesser SacWhere is the lesser sac? To Mnd it, Mrst we need to identify the lesser omentum. Thelesser omentum is a mesentery that attaches the liver above to the stomach and Mrstpart of the duodenum below.
COMPLETE ANATOMY: OMENTA
#
The lesser omentum has two parts:1 Hepatogastric ligament = very thin,
almost transparent. Connects liver tolesser curvature of stomach.
2 Hepatoduodenal ligament = connectsliver to Mrst part of duodenum (theother parts of the duodenum areretroperitoneal). It is thick, because itcontains the portal triad: the hepaticartery proper, the bile duct, and theportal vein. Feel the structures withinthe hepatoduodenal ligament betweenyour thumb and Mnger.
Figure 10.11.
Now, relocate the falciform ligament that attaches the liver to the AAW. Recall fromembryology that the lesser omentum and falciform ligament are derived from theventral mesentery of the stomach.
The lesser sac (omental bursa) is a blind pouch posterior to the lesser omentumand stomach. It gives the stomach space to move freely while churning.
Boundaries: anterior is the liver, stomach, and lesser omentum; posterior isperitoneum on the posterior abdominal wall.
Figure 10.12.
The lesser and greater sacs communicate viathe Omental foramen (Foramen ofWinslow), located posterior to thehepatoduodenal ligament. Place a Mnger inthe omental foramen.
Anterior to your Unger are the structuresof the portal triad. Posterior to yourUnger is the IVC.
Figure 10.13. Clemente’s Atlas of Anatomy.
Greater OmentumExamine the greater omentum, a double-layer of peritoneum hanging down like afatty apron from the greater curvature of the stomach.
NOTEThe greater omentum may adhere to areas that were previously in[amed, resulting ina constricted appearance.
Figure 10.14.
Identify its main subdivisions:• Gastrocolic ligament (stomach to
transverse colon). This is the part thathangs from the greater curvature of thestomach like an apron.
• Gastrosplenic ligament (stomach tospleen)
• Splenorenal ligament (reach way behindthe spleen to feel it with your Mngertips). Itis the part of the greater omentum thatconnects to the posterior body wall.
Figure 10.15.
The Other MesenteriesLift the greater omentum and identify the transverse colon. The double fold ofperitoneum suspending it from the posterior abdominal wall is the transversemesocolon.
Think back to the boundaries of the lesser sac. Examine the Ggure below and discusshow the transverse mesocolon is related to the lesser sac.
Figure 10.16.
Lift the ileum and jejunum and trace their mesentery proper to the posteriorabdominal wall.
Trace the ileum to the cecum and Mnd the appendix, often folded back behind thececum. Feel for its mesoappendix.
Trace the large intestine until you get to the sigmoid colon. It is suspended by asigmoid mesocolon on the left side.
Figure 10.17.
What is the deGnition of a mesentery, and what are the functions?
Mesenteries, peritoneal ligaments, and omenta are all structures composed of twolayers of peritoneum. Mesenteries attach to the posterior abdominal wall, whileomenta attach to the stomach.
List the structures that have mesenteries, and are thus mobile, and called “peritoneal”organs.
Which organs had a mesentery, but then lost it during development? These organs are“secondarily” retroperitoneal.
I N S P E C T T H E P E LV I C V I S C E R A
We will study the pelvic organs in detail in the coming weeks, but now is a good timeto view them superMcially beneath the peritoneum.
NOTE how the peritoneum on the abdominal wall continues into the pelvic cavity and“drapes” itself over the pelvic viscera—much like a “drop cloth” placed over yourfurniture when you paint the walls.
Identify the organs that it drapes over: rectum, uterus, Fallopian (uterine) tubes,and bladder.
IF you have a female cadaver and it has a uterus, the peritoneum that drapes over itand the Fallopian tubes is called the broad ligament.
Demonstrate it to other lab groups if you have it. See if you can spot the ovaries.
IDENTIFY and probe with your hands the pelvic peritoneal pouches: rectovesicalpouch (male), rectouterine pouch and vesicouterine pouch (female).
These pouches are the inferior-most extent of the greater sac. Why would this be ofclinical importance?
Figure 10.18. Figure 10.19.
Figure 10.20.
I M A G I N G
Open the PACS viewer and navigate to your donor CT. Select CT CHAP to openscans of the chest, abdomen and pelvis.
Practice looking at axial, sagittal, and frontal sections of the abdomen. Try to identifysome main organs of the abdominal cavity:
• Liver: Look for the large grey mass just under the right lung• Spleen: Look along the left side tucked under the diaphragm• Stomach: If you Mnd the stomach you may be able to trace it to the duodenum• Loops of bowel (don’t worry about identifying speciMc parts)
C H E C K L I S T, L A B # 1 0R E V I E W A N D M A K E S U R E Y O U H A V E I D E N T I F I E D E A C H O F T H E S T R U C T U R E SB E L O W .
I N T E R N A L A S P E C T O F A N T E R I O R A B D O M I N A L WA L LInferior epigastric vessels
Superior epigastric vessels
Arcuate line
P E R I TO N E U M A N D P E R I TO N E A L C AV I T YParietal and visceral peritoneum
Peritoneal cavity
Greater sac
Subphrenic spaces
Hepatorenal recess
Paracolic gutters
Retrocecal recess
Rectovesical pouch (in pelvis—male)
Recto-uterine and uterovesical pouches (in pelvis—female, when uterus is present)
Lesser sac
Omental foramen
Lesser omentum
Hepatoduodenal ligament
Hepatogastric ligament
Greater omentum
Gastrocolic ligament
Gastrosplenic ligament
Splenorenal ligament
Mesentery of the small intestine
Transverse mesocolon
Sigmoid mesocolon
A B D O M I N A L V I S C E R ALiver
Diaphragmatic surface
Falciform ligament
Gallbladder
Pancreas (retroperitoneal = may be diecult to see)
Spleen
Abdominal esophagus
Stomach
Home Anatomy Review Labs $

LAB 10 : PER ITONEAL CAV ITY AND OVERV IEW OF G I10/6/2021
Table of ContentsTable of Contents !
Opening the Peritoneal Cavity
Abdominal Viscera
Liver
Small intestine
Large intestine
Peritoneum and Peritoneal Cavity
Lesser Sac
Greater Omentum
The Other Mesenteries
Inspect the Pelvic Viscera
Imaging
David Conley, PhDOffice: PBS 41A
Shannon Helbling, PhDOffice: PBS 41C
"
+
TO O P E N T H I S PA G E O N T H E L A B M O N I TO R S
1. Turn on the monitor.
2. Choose a browser (Chrome or Firefox—either is Gne!).
3. Tap the URL Geld at the top of the screen to highlight.
4. Tap the keyboard icon in the bottom right-hand corner.
5. Enter this URL: https://tinyurl.com/f8v5wkef
TO D O W N L O A D A P D F O F T H I S L A B G U I D E
GOALS1 Open the anterior abdominal wall and study its internal aspect.
2 Examine the peritoneum, peritoneal cavity, mesenteries, omenta, and peritoneal
ligaments.
3 Locate the subparts of the greater sac.
4 Study the lesser omentum and demonstrate the lesser sac.
5 Study the organs of the abdominal cavity: liver; gallbladder; stomach; small intestines; large
intestines; pancreas; and spleen.
O P E N I N G T H E P E R I TO N E A L C AV I T Y
Open the abdominal wall.
Open the anterior abdominal wall:
Make incisions in the muscular wall of the AAW asshown.
Incision 1: Follows the costal margins.
Incision 2: Slightly left of the midline from the costalmargin to the pubic symphysis (making this cut tothe left of the umbilicus will preserve thefalciform ligament).
Incision 3: Along the lateral wall from the costalmargin to the iliac crest.
Incision 4: From the pubic symphysis laterally to theanterior superior iliac spine (running above theinguinal canal).
Figure 10.1.
Fold down the left !ap (created by incisions 2 and 3); inspect the internalaspect of the anterior abdominal wall.
Find the lateral umbilical folds: theseare subtle folds created where theperitoneum runs over the inferiorepigastric vessels. Peel the peritoneumaway from the inside of the abdominalwall. Locate the inferior epigastricvessels.
Figure 10.2.
CLINICAL CORRELATIONRecall their role in determining direct vs. indirect inguinal hernias. Identify the bordersof Hesselbach’s triangle from this internal surface.
On each side, the inferior epigastricvessels pass under the arcuate line to enterthe rectus sheath, posterior to the rectusabdominis muscles. Within the rectussheath, the inferior epigastric artery suppliesthe rectus muscle and anastomoses with thesuperior epigastric artery, a terminalbranch of the internal thoracic artery.
This anastomosis could provide an alternateroute for blood to reach the lower limbshould the descending aorta becompromised.
Figure 10.3. Anastomosis between thoracicand abdominal circulations.
CLINICAL CORRELATION Discuss this alternate route with your group. Draw a [owchart.
Fold the right !ap laterally (created by incisions 1 and 4); inspect the internalaspect of the anterior abdominal wall.
Locate the liver, and identify the right and left lobes of the liver—covered in visceralperitoneum.
Examine the sickle-shaped falciform ligament running between the lobes. Thisdouble layer of peritoneum connects the liver to the anterior abdominal wall.
To fully reJect the Jap of the abdominal wall laterally, use scissors or a scalpel totrim the falciform ligament from the surface of the abdominal wall, leaving theligament attached to the liver.
A B D O M I N A L V I S C E R A
COMPLETE ANATOMY: ABDOMINAL V I SCERA
#
Explore and name the organs of the abdominal cavity.
Liver
The sharp inferior border peeks out under the costal margin; reach under thediaphragm to feel the liver’s diaphragmatic surface
Lift the liver’s inferior border to see the gallbladder (yes, it should be green).
Figure 10.4.
Elevate the liver to Mnd the abdominal esophagus and the stomach.
Examine the stomach’s relations with other organs and omental bursa:• Anterior: diaphragm, left lobe of liver• Posterior: lesser sac, pancreas, spleen, left kidney, and left suprarenal gland
The pancreas is hidden deep to the stomach. It is covered by peritoneum (it isretroperitoneal) so it may be difficulty to identify.
With your right hand, reach across the cadaver to the left side behind to stomachand under the diaphragm to Mnd the spleen.
• The spleen is an intraperitoneal structuretypically in the area of rib IX to rib X.
• The spleen has two surfaces: Diaphragmaticand Visceral. The diaphragmatic surface iscurved to conform to the underside of thediaphragm. The visceral surface contains thehilum of the spleen where the vessels enter.
Figure 10.5.
Figure 10.6.
Small intestineTrace the stomach to the right to Mnd the duodenum. It is curved and shaped likethe letter C. The concavity of the curve faces to the left. The Mrst part of theduodenum, connected to the stomach, is intraperitoneal. The other parts areretroperitoneal where they curve around the head of the pancreas; thus these maybe diQcult to see.
COMPLETE ANATOMY: DUODENUM & PANCREAS
#
Which structures develop from the foregut? What artery supplies these structures?
Distal to the duodenum are the otherparts of the small intestine: jejunumand ileum. Push the small intestine tothe right to Mnd the duodenojejunaljunction. Trace the ileum to the rightlower quadrant to Mnd the ileocecaljunction.
Figure 10.7.
Large intestinePush the small intestine to the left to Mnd the ileocecal junction. Now trace in orderfrom proximal to distal: cecum, appendix (if present), ascending colon, transversecolon (lift greater omentum to see it), descending colon, sigmoid colon, andrectum. Notice how the large intestine forms a box around the small intestine.
Which parts of the GI tract are midgut structures? Hindgut? What arteries supply eachof these?
Figure 10.8. Figure 10.9.
P E R I TO N E U M A N D P E R I TO N E A L C AV I T Y
Use your hands to explore the peritoneal cavity, spaces, omenta, mesenteries,and peritoneal ligaments.
Identify:• Parietal peritoneum (on the body wall)• Visceral peritoneum (on the organs)• The peritoneal cavity is the space between the parietal and visceral peritoneum.
REALIZE that the peritoneal cavity is a “potential” space. In a living person, there isvery little space between the parietal and visceral layers of the peritoneum. Thisspace is occupied by a thin layer of serous Juid that lubricates the organs and bodywall and facilitates their friction-less movements.
The two parts of the peritoneal cavity are the greater sac and the lesser sac. Withthe anterior abdominal wall laid open, you are looking into the greater sac.
Identify These Subparts of the Greater Sac:
• Sub-phrenic spaces between the diaphragm and liver• Hepatorenal recess (aka—Morrison’s pouch) between liver and the right kidney• Paracolic gutters (between ascending/descending colon and lateral wall)• Retrocecal recess (behind the cecum—sometimes the appendix hides here!)• Rectovesical pouch in males—in the pelvis, between rectum and bladder• Recto-uterine pouch and vesico-uterine pouch in females (IF there is a uterus
present)—in the pelvis, between rectum and uterus, and uterus and bladder,respectively.
Figure 10.10.
Lesser SacWhere is the lesser sac? To Mnd it, Mrst we need to identify the lesser omentum. Thelesser omentum is a mesentery that attaches the liver above to the stomach and Mrstpart of the duodenum below.
COMPLETE ANATOMY: OMENTA
#
The lesser omentum has two parts:1 Hepatogastric ligament = very thin,
almost transparent. Connects liver tolesser curvature of stomach.
2 Hepatoduodenal ligament = connectsliver to Mrst part of duodenum (theother parts of the duodenum areretroperitoneal). It is thick, because itcontains the portal triad: the hepaticartery proper, the bile duct, and theportal vein. Feel the structures withinthe hepatoduodenal ligament betweenyour thumb and Mnger.
Figure 10.11.
Now, relocate the falciform ligament that attaches the liver to the AAW. Recall fromembryology that the lesser omentum and falciform ligament are derived from theventral mesentery of the stomach.
The lesser sac (omental bursa) is a blind pouch posterior to the lesser omentumand stomach. It gives the stomach space to move freely while churning.
Boundaries: anterior is the liver, stomach, and lesser omentum; posterior isperitoneum on the posterior abdominal wall.
Figure 10.12.
The lesser and greater sacs communicate viathe Omental foramen (Foramen ofWinslow), located posterior to thehepatoduodenal ligament. Place a Mnger inthe omental foramen.
Anterior to your Unger are the structuresof the portal triad. Posterior to yourUnger is the IVC.
Figure 10.13. Clemente’s Atlas of Anatomy.
Greater OmentumExamine the greater omentum, a double-layer of peritoneum hanging down like afatty apron from the greater curvature of the stomach.
NOTEThe greater omentum may adhere to areas that were previously in[amed, resulting ina constricted appearance.
Figure 10.14.
Identify its main subdivisions:• Gastrocolic ligament (stomach to
transverse colon). This is the part thathangs from the greater curvature of thestomach like an apron.
• Gastrosplenic ligament (stomach tospleen)
• Splenorenal ligament (reach way behindthe spleen to feel it with your Mngertips). Itis the part of the greater omentum thatconnects to the posterior body wall.
Figure 10.15.
The Other MesenteriesLift the greater omentum and identify the transverse colon. The double fold ofperitoneum suspending it from the posterior abdominal wall is the transversemesocolon.
Think back to the boundaries of the lesser sac. Examine the Ggure below and discusshow the transverse mesocolon is related to the lesser sac.
Figure 10.16.
Lift the ileum and jejunum and trace their mesentery proper to the posteriorabdominal wall.
Trace the ileum to the cecum and Mnd the appendix, often folded back behind thececum. Feel for its mesoappendix.
Trace the large intestine until you get to the sigmoid colon. It is suspended by asigmoid mesocolon on the left side.
Figure 10.17.
What is the deGnition of a mesentery, and what are the functions?
Mesenteries, peritoneal ligaments, and omenta are all structures composed of twolayers of peritoneum. Mesenteries attach to the posterior abdominal wall, whileomenta attach to the stomach.
List the structures that have mesenteries, and are thus mobile, and called “peritoneal”organs.
Which organs had a mesentery, but then lost it during development? These organs are“secondarily” retroperitoneal.
I N S P E C T T H E P E LV I C V I S C E R A
We will study the pelvic organs in detail in the coming weeks, but now is a good timeto view them superMcially beneath the peritoneum.
NOTE how the peritoneum on the abdominal wall continues into the pelvic cavity and“drapes” itself over the pelvic viscera—much like a “drop cloth” placed over yourfurniture when you paint the walls.
Identify the organs that it drapes over: rectum, uterus, Fallopian (uterine) tubes,and bladder.
IF you have a female cadaver and it has a uterus, the peritoneum that drapes over itand the Fallopian tubes is called the broad ligament.
Demonstrate it to other lab groups if you have it. See if you can spot the ovaries.
IDENTIFY and probe with your hands the pelvic peritoneal pouches: rectovesicalpouch (male), rectouterine pouch and vesicouterine pouch (female).
These pouches are the inferior-most extent of the greater sac. Why would this be ofclinical importance?
Figure 10.18. Figure 10.19.
Figure 10.20.
I M A G I N G
Open the PACS viewer and navigate to your donor CT. Select CT CHAP to openscans of the chest, abdomen and pelvis.
Practice looking at axial, sagittal, and frontal sections of the abdomen. Try to identifysome main organs of the abdominal cavity:
• Liver: Look for the large grey mass just under the right lung• Spleen: Look along the left side tucked under the diaphragm• Stomach: If you Mnd the stomach you may be able to trace it to the duodenum• Loops of bowel (don’t worry about identifying speciMc parts)
C H E C K L I S T, L A B # 1 0R E V I E W A N D M A K E S U R E Y O U H A V E I D E N T I F I E D E A C H O F T H E S T R U C T U R E SB E L O W .
I N T E R N A L A S P E C T O F A N T E R I O R A B D O M I N A L WA L LInferior epigastric vessels
Superior epigastric vessels
Arcuate line
P E R I TO N E U M A N D P E R I TO N E A L C AV I T YParietal and visceral peritoneum
Peritoneal cavity
Greater sac
Subphrenic spaces
Hepatorenal recess
Paracolic gutters
Retrocecal recess
Rectovesical pouch (in pelvis—male)
Recto-uterine and uterovesical pouches (in pelvis—female, when uterus is present)
Lesser sac
Omental foramen
Lesser omentum
Hepatoduodenal ligament
Hepatogastric ligament
Greater omentum
Gastrocolic ligament
Gastrosplenic ligament
Splenorenal ligament
Mesentery of the small intestine
Transverse mesocolon
Sigmoid mesocolon
A B D O M I N A L V I S C E R ALiver
Diaphragmatic surface
Falciform ligament
Gallbladder
Pancreas (retroperitoneal = may be diecult to see)
Spleen
Abdominal esophagus
Stomach
Home Anatomy Review Labs $