indiana program improvement...
TRANSCRIPT

State of Indiana Program Improvement Plan
Department of Child Services
Mitchell E. Daniels, Jr., Governor James W. Payne, Director
July 15, 2008
“Protecting Our Children, Families, and Future”
6/30/2009 Indiana Program Improvement Plan 1

State of Indiana Child and Family Services Reviews
Program Improvement Plan
I. PIP General Information II. PIP Strategy Summary and TA Plan III. PIP Agreement Form IV. PIP Matrix V. List of CFSR Outcomes, Systemic Factors and Associated Items, Data Indicators and Composites VI. QAR Tool Attachments I. PIP General Information ACF Region: I II III IV V X VI VII VIII IX X
State: Telephone Number: 312.353.1786
Lead ACF Regional Office Contact Person: Barbara Putyra, ACF Regional Contact
E-mail Address: [email protected]
Address: 302 W. Washington Street E-306 MS 47 Indianapolis, Indiana 46204
State Agency Name: Indiana Department of Child Services James W. Payne, Director
Telephone Number: 317.234.4705
Telephone Number: 317.234.5005
Lead State Agency CFSR/PIP Contact Person: Regina F. Smith CFSR Program Manager Indiana Department of Child Services
E-mail Address: [email protected]
State PIP Team Members: 1. David Judkins, Deputy Director of Field Operations, Indiana Department of Child Services 2. Allison Chaney, Assistant Deputy Director Field Operations, Indiana Department of Child
Services 3. Reba James, Northern Indiana Executive Manager, Indiana Department of Child Services
6/30/2009 Indiana Program Improvement Plan 2

4. Melissa Norman, Southern Indiana Executive Manager, Indiana Department of Child Services 5. Jane Bisbee, Regional Manager (Region 1), Indiana Department of Child Services 6. Terrence Ciboch, Regional Manger (Region 2), Indiana Department of Child Services 7. Faye Russell, Regional Manager (Region 3), Indiana Department of Child Services 8. Steve E. Scott, Regional Manager (Region 4) , Indiana Department of Child Services 9. Gilbert Smith, Regional Manager (Region 5), Indiana Department of Child Services 10. Glynn Hipp, Regional Manager (Region 6), Indiana Department of Child Services 11. Steven Cox, Regional Manager (Region 7), Indiana Department of Child Services 12. David Uberto, Regional Manager (Region 8), Indiana Department of Child Services 13. Char Burkett-Sims, Regional Manager (Region 9), Indiana Department of Child Services 14. Jennifer Hubbart, Regional Manager (Region 10), Indiana Department of Child Services 15. Michelle Burns, Regional Manager (Region 11), Indiana Department of Child Services 16. Vickie S. Jones, Regional Manager (Region 12) , Indiana Department of Child Services 17. Nicole Henderson, Regional Manager (Region 13), Indiana Department of Child Services 18. Laura Gentry, Regional Manager (Region 14), Indiana Department of Child Services 19. Jennifer Tackitt, Regional Manager (Region 15), Indiana Department of Child Services 20. Virginia Combs, Regional Manager (Region 16), Indiana Department of Child Services 21. Susan Lesko, Regional Manager (Region 17), Indiana Department of Child Services
22. John Kaiser, Regional Manager (Region 18), Indiana Department of Child Services
23. Regina Ashley, Deputy General Counsel, Indiana Department of Child Services
24. Beverly Gatling, Residential Licensing Manager, Indiana Department of Child Services
25. Nikki Dean, FCM Supervisor, Indiana Department of Child Services
26. Sue Romans, Noble County Director, Indiana Department of Child Services
27. Eileen Walters, FCM Supervisor, Indiana Department of Child Services
28. Jan Dotson, FCM Supervisor, Indiana Department of Child Services
29. Monica Lawrence, FCM Supervisor, Indiana Department of Child Services
30. Nancy Wever, Family Case Manager, Indiana Department of Child Services
31. Jodi Stockdale, Family Case Manager, Indiana Department of Child Services
32. Steve Vaughn, Montgomery County Director, Indiana Department of Child Services
33. Krista Hollins, Family Case Manager, Indiana Department of Child Services
34. Yvonne Lee, Family Case Manager, Indiana Department of Child Services
35. Debbie Jackson, Family Case Manager, Indiana Department of Child Services
36. Jillian Hancock, Family Case Manager, Indiana Department of Child Services
37. Barbara South, Putnam County Director, Indiana Department of Child Services
38. Andrea Wilson, Family Case Manager, Indiana Department of Child Services
39. Jennifer Hubbart, Chief Legal Counsel, Indiana Department of Child Services
40. Kris Meltzer, Staff Attorney, Indiana Department of Child Services
6/30/2009 Indiana Program Improvement Plan 3
41. Pete S. Raventos, Staff Attorney, Indiana Department of Child Services
42. Sherry Hartzler, Chief Counsel/Allen County, Indiana Department of Child Services
43. Debbie Burke, Staff Attorney, Indiana Department of Child Services
44. Elizabeth G. Filipow, Staff Attorney, Indiana Department of Child Services
45. Carey H. Wong, Staff Attorney, Indiana Department of Child Services
46. Cassandra Porter, Permanency Manager, Indiana Department of Child Services
47. Phyllis Kidendall, Prevention Manager, Indiana Department of Child Services
48. Rita Sparks, Human Services Consultant, Indiana Department of Child Services
49. Ann Arvidson, SNAP Specialist, Indiana Department of Child Services
50. Charity Colter, SNAP Specialist, Indiana Department of Child Services
51. Janice Ellis, Foster Care Specialist, Indiana Department of Child Services
52. Sandi Sleepy, Preservation Manager, Indiana Department of Child Services
53. M.B. Lippold, Deputy Director of Staff Development, Indiana Department of Child Services
54. Kay Osborne, Training Manager, Indiana Department of Child Services
55. Jerrick Kostelnik, Trainer, Indiana Department of Child Services
56. Mike Fleming, Henry County Director, Indiana Department of Child Services
57. Mindy Berry, Daviess County Director, Indiana Department of Child Services
58. Lou Richey, Porter County Director, Indiana Department of Child Services
59. Charles Barnett, Family Case Manager, Indiana Department of Child Services
60. Julie Deckart, SNAP Specialist, Indiana Department of Child Services
61. Peggy Shively, Kosciusko County Director, Indiana Department of Child Services
62. Jason Bouchard, FCM Supervisor, Indiana Department of Child Services
63. Tammie Washington, Family Case Manager, Indiana Department of Child Services
64. Edna Clancy, FCM Supervisor, Indiana Department of Child Services
65. Vicki Ratcliff, FCM Supervisor, Indiana Department of Child Services
66. Nikki Henderson, Clinical Consultant, Indiana Department of Child Services
67. Rebecca Kirkham, Clinical Consultant, Indiana Department of Child Services
68. Kelly Moore, Human Services Consultant, Indiana Department of Child Services
69. Taren Duncan, Marion County Deputy Director, Indiana Department of Child Services
70. D’Andrea Abdullah, Marion County Division Manager, Indiana Department of Child Services
71. Lindsey Smith, Monroe County Director, Indiana Department of Child Services
72. Mike Carroll, Marshall County Director, Indiana Department of Child Services
73. Jim Gregory, Policy Analyst, Indiana Department of Child Services
74. Ashley Barnett, Policy Analyst, Indiana Department of Child Services
75. Felecia Boyd-Smith, Policy Manager, Indiana Department of Child Services
6/30/2009 Indiana Program Improvement Plan 4

76. Kevin Huston, Data Manager, Indiana Department of Child Services
77. Celia Leaird, Deputy Director Programs and Services, Indiana Department of Child Services
78. John Ryan, Chief Legal Counsel, Indiana Department of Child Services
79. Angela Green, Deputy Director of Practice Support, Indiana Department of Child Services
80. Scott Piller, Human Services Consultant, Indiana Department of Child Services
81. Sarah Sparks, Human Services Consultant, Indiana Department of Child Services
82. Maria Wilson, Practice Reform Program Manager, Indiana Department of Child Services
83. Tiffany Mitchell, Federal Grants Program Manager, Indiana Department of Child Services
84. Tristyn Ryan, Field Initiatives Program Manager, Indiana Department of Child Services
85. Ann Houseworth, Legislative Liaison, Indiana Department of Child Services
86. Deniece Safewright, Deputy General Counsel, Indiana Department of Child Services
87. Sarah Johnson, Foster Care Specialist, Indiana Department of Child Services
88. Lisa Whitaker, Performance and Quality Improvement State Director, Indiana Department of Child Services
89. Valerie Bruce, Quality Assurance Analyst, Indiana Department of Child Services
90. Helen Stevenson, SNAPS Program Director, Indiana Department of Child Services
91. Tschanette Cotton, Policy Analyst, Indiana Department of Child Services
Stakeholders Participating in Program Improvement Plan Development
Name Position Agency
1. Angela Reid-Brown Court Administrator Indiana Court Improvement Project 2. Lisa McGuire Professor IUPUI 3. Sharon Pierce CEO Villages 4. Chris Morrison Executive Director Indiana Foster Care & Adoption
Association 5. Cookie Purvis Foster Parent 6. Bobbie Brooks Foster Parent 7. Kelly Samodral Foster Parent 8. Cheryl Seelig Foster Parent 9. Alfreda Singleton-
Smith Senior Director of Client Services
The Villages
10. Delores Kennedy-Williams
Director of Integration Services
White’s Residential & Family Services
11. Christina Endres Consultant Indiana Department of Education 12. Gina Eckhart Assistant Director Indiana Department of Mental Health 13. Leslie Dunn, Esq. State CASA Director Indiana Supreme Court 14. Janice Klein Executive Vice-President Children’s Bureau 15. John Ireland Community Partner Ireland Home Based Services 16. Judge Marilyn A.
Moores Juvenile Judge Marion Superior Court
6/30/2009 Indiana Program Improvement Plan 5
17. Judge Charles Pratt Juvenile Judge Allen Superior Court 18. Karen Biernacki CASA Director 19. Gregg Ellis Guardian-at-litem (GAL) Child Advocates 20. James Thompson Youth 21. Sasha Dykes-Wilson Youth 22. Yun Qing LU Youth 23. Roger Zimmerman Program Director Indiana Family & Social Services
Administration 24. Betty Walton Consultant Indiana Family & Social Services
Administration 25. Jackie Votapek Training Manager Child Welfare Education and Training
Partnership 26. Lisa Hubbard Training Representative IUPUI 27. Pat Howes IV-E Project Coordinator IUPUI 28. 29. Nathan Samuel
Executive Director Childplace Inc.
30. Miriam Acevedo Davis
Executive Director La Plaza Inc.
31. Nancy Fisher Vice President White’s Residential and Family Services
32. Ruth Ruppert Foster Parent 33. Jan Vogleman Foster Parent 34. Betsy Whaley Shelter Director The Julian Center 35. Michael Singleton Therapist Ireland Home based Services
Persons Responsible for Implementing Action Steps in PIP Matrix
Name Position Contact Information
David Judkins Deputy Director of Field Operations
Indiana Department of Child Services Room E306 - MS 47 302 W. Washington St. Indianapolis, In. 46204-2738 317-234-3999
MB Lippold Deputy Director of Staff Development
Indiana Department of Child Services Room E306 - MS 47 302 W. Washington St. Indianapolis, In. 46204-2738 317-234-3925
Lisa Rich Deputy Director of Programs and Services
Indiana Department of Child Services Room E306 - MS 47 302 W. Washington St. Indianapolis, In. 46204-2738 317-232-4497
6/30/2009 Indiana Program Improvement Plan 6

Angela Green Deputy Director of Practice Support
Indiana Department of Child Services Room E306 - MS 47 302 W. Washington St. Indianapolis, In. 46204-2738 317-232-4631
Jeffrey M. Lozer General Counsel Indiana Department of Child Services Room E306 - MS 47 302 W. Washington St. Indianapolis, In. 46204-2738 317-234-3871
Angela Reid-Brown CIP Grant Administrator
Indiana Judicial Center 30 South Meridian Street, Suite 900 Indianapolis, IN 46204 317-232-1313
Indiana Department of Child Services
1. A Practice Reform Overview:
In 2005, Governor Mitch Daniels changed the course of Indiana’s child welfare system when he established Indiana’s Department of Child Services (DCS) as a separate cabinet-level agency. He charged the new administration with the responsibility of overseeing child welfare services and child support enforcement. DCS engaged national and local organizations for guidance and support to improve the system that cares for its abused and neglected children. This collaboration marked the beginning of Indiana’s practice reform efforts. The centerpiece for Indiana’s Practice Reform include the new Practice Model (TEAPI), infrastructural and systemic changes, staff expansion and training, policy making and revisions, and new legislative amendments. The Practice Model:
With the assistance of the Casey Strategic Consulting Group, the Indiana Department of Child Services researched best child welfare practices in other states. After reviewing several models and traveling to the State of Utah to review the model that state has adopted, Indiana adopted a practice model based on family engagement and involvement, with the cornerstone being the Child and Family Team Meeting. All other initiatives including Staff Development, Performance Quality Improvement, Policy, ICWIS Redesign and Service Standards Development for Programs and Services have been created through the lens of this established Practice Model. The practice model is based on the DCS vision, mission and values. During the implementation phase, DCS staff has been trained to build trust-based relationships with families and partners by exhibiting empathy, professionalism, genuineness and respect. In addition, DCS staff, through training and coaching, has developed the skills of engaging, teaming, assessing, planning and intervening to partner with families and the community to achieve better outcomes for children.
6/30/2009 Indiana Program Improvement Plan 7

The Practice Model (TEAPI) – A Detailed Definition The mainstay of Indiana’s Practice Reform is the new practice model, TEAPI: (Teaming,
Engaging, Assessing, Planning, and Intervening). Engaging is defined as effectively establishing a working relationship with the children, parents, and key participants of the team for the purpose of reaching the identified case plan goals. Teaming is the skill of identifying the family’s informal and formal supports by establishing them as a working group. This group is synonymous to the Child and Family Team formed to assist the family and offer resources necessary to address issues relevant to DCS’ involvement. Assessing is the skill of obtaining information about crucial events that has led the child and the family to DCS and the root causes for their crises. Assessing is a discovery process that searches for both the needs and strengths of the family and in doing so, determines the capacity, willingness, and availability of resources to achieve safety, permanence and well-being of the children. Planning overlaps with Assessing as it depends on the family’s ability to meet the child’s needs long term. This part of the process includes incremental steps that move children and families from where they are to a better and safer level of functioning. Service planning requires the ongoing assessment of circumstances and resources, and often includes the evaluation of the plan’s effectiveness, reworking the plan when necessary, celebrating successes, and searching for contingencies when plans are unsuccessful. Intervening is the ability of field staff to intercede with actions that will decrease risk and increase safety, promote permanency and establish well-being. This skill is practical in nature and ranges from finding housing to enlightening a parent’s thinking about raising children.
The Next Phase of TEAPI The five core skills outlined are the foundation of the practice model process. To further
advance the practice of TEAPI, two ongoing courses have been developed and implemented to include “Supervising the Indiana Practice Change” and “Making Visits Matter”: a three day module for all field workers. The Making Visits Matter module emphasizes the connection between the family case manager and the family with the understanding that the work accomplished is through relationships established between the FCM, the child and family, and increasingly with the family’s informal and formal support systems. In the workshop, the participants explore three layers of knowing the context of their work with children and families. They learn the family based on the principles that guide the work (the practice model skills), and through achievement of the four major outcomes in child welfare (safety, permanency well-being and stability). Using the principles of engagement, teaming and strengths-needs based work; participants also learn new ways to assist families on how to join and connect with their children, and how to utilize their informal and formal supports to achieve their desired outcomes. The curriculum is focused on the critical role of worker’s visits and the relationship visits have in providing safety to children, while supporting effective case plan development, implementation and adaptation. Specific goals identified in the training include:
Identification of purposes and the value of partnership in worker visits with children and families (for children remaining in their homes as well as children placed with substitute caregivers)
Identification of and practice in safety assessment during visits, including observation and interviewing information
6/30/2009 Indiana Program Improvement Plan 8
Individualization of visiting techniques and observations based on developmental considerations, case progress and key decision points in work with children and families
Tracking and adjustment of case plan goals, tasks and accomplishments Development of worker engagement strategies with children, families and caregivers Development of strategies toward team-building during visits to promote progress
and stability for children and families.
DCS Permanency Vision: A DCS core value is to ensure that every child involved in the child welfare system has a right to appropriate care and a permanent home. The interventions that come with DCS’ involvement are not intended to be long-term solutions but the ultimate vision is to be a short-term agency with permanence as the constant goal. With this premise, DCS has launched multiple initiatives to ensure that permanency plans and outcomes are timely, achievable, and establishes long-term stability for each child under DCS’ supervision. Some of the permanency initiatives are internal approaches that include the incorporation of the genogram tool, planning and intervening components of the TEAPI practice model, piloting concurrent planning, the enforcement of diligent searches for non-parent relatives and absent parents, conducting clean up reports of long-standing cases, and the implementation of the regional permanency teams. Other permanency objectives involve the collaboration of external stakeholders, mainly court and legal partners; to assure that permanency planning is effective and remains priority. The Permanency Pilot Project and other CIP and DCS court collaborations (that are included in this report) are examples of DCS’ external initiatives.
Permanency Teams: Permanency Teams are a Field Operations project that originated in 2008 when executive management decided to create an internal way of evaluating long-standing, difficult and stagnant cases that had not yet reached permanency. Permanency teams are regionally-based and members consist of a FCM, FCM supervisor, a Local Office Director, foster care worker, CASA representative and IL worker. The cases are specifically selected based on the length of stay in care, time of involvement and severity of needs identified. The team reviews the case and develops a plan to move the case forward. The recommendations of this team are expected to be shared with the court at the next hearing and implemented by the members of the child’s team. Each region reviews an average of five (5) to six (6) cases monthly. There is a referral process that FCMs complete to have their more difficult cases staffed by the Permanency Team. Infrastructural and Systemic Change:
DCS’ Director, James W. Payne, addressed the infrastructure and systemic needs with immediate changes in operational and organizational development. Six deputy directors were each assigned a division at the executive management level to oversee statewide areas of Field Operations, Staff Development, Practice Support, Legal Operations, Child Support, and Programs and Services. Along with the renovation of the central office structure, the statewide system was reorganized into eighteen (18) regions with local offices serving as divisions within those regions. This allowed each region to focus on, in conjunction with statewide objectives, a regional strategic plan addressing the specific geographical and demographic needs within its
6/30/2009 Indiana Program Improvement Plan 9
counties. Additionally, there was the development of DCS’ mission, vision, values, and practice principles to serve as guideposts for the newly structured organization.
Practice Indicators and Quality Service Reviews:
Along with the newly defined infrastructure and focus on improving case practice, DCS employed several tools such as Practice Indicators, The Performance and Quality Improvement Unit (QSR), and ICWIS redesign to assist in monitoring and supporting systemically the new practice reform efforts. Practice Indicators were created in 2007 within the ICWIS system to manage the data reviews of FCMs, Units, Counties and Regions. The reviews are measured by nine (9) reports and eleven (11) indicators. Many of which were directly connected to the 2001 CFSR report and PIP as well as the outcome measures contained in the current CFSR. The following are the practice indicators:
Initial Assessment – Use of Substitute Care, CHINS Placements by County (reduction of residential placement and the increase
of relative placements), Locally Placed CHINS, Average Number of Placement Moves, Sibling Placement Report, Length of Stay in out-of-home placement, Finalized Adoption Rates and Reunification Rates, Visitations and Contacts Report, (Number of child/parent visits and FCM contacts
with family) Trended Repeat Maltreatment.
The Performance and Quality Improvement (PQI) unit of DCS created in January 2007 developed a new Quality Service Review (QSR) protocol, which measures safety, permanency, well-being, independent living and the practice model skills of engaging, teaming, and assessment, planning and intervening. The Protocol was designed to measure both the elements used by the Federal Government to measure child welfare systems and the specific skills in the practice model needed to achieve better outcomes for children and families. The protocol is a results oriented guide to best social work practice; it takes a holistic view of cases and measure them against established best practice standards to move systems forward towards working with families and children to achieve sustainable changes.
The team piloted the protocol in March 2007 and finalized it by April 2007. Some important factors about QSR: a) there is a roll-out plan in place to review each region in the state every 30 months. The QSR roll-out follows the roll-out of practice reform; b) A QSR review consists of a random selection of cases within in a region which includes CHINS cases, Informal adjustment cases and assessments; c) The review includes a case file review, interviews with key participants, strength-based debriefing, with Family Case Managers and supervisors, and finally scoring the status of the case; d) Mini reviews are conducted in previously reviewed regions to assist the regions in gauging progress towards established regional strategic plans; e) Staff across the agency is currently being trained to become reviewers; f) A case story is written for each case reviewed. The region receives a regional analysis of the data obtained during the review within 60 days of the review; g) Each Regional Manager develops a strategic plan to improve practice based on the results of the QSR data. The Regional Manager reports quarterly accomplishments as part of a continuous quality improvement plan; and h) a bi-annual report
6/30/2009 Indiana Program Improvement Plan 10
will be generated to provide an analysis of statewide data and performance levels in the QSR, the QAR and the Practice Indicators.
The report highlights the strengths and focus on statewide improvements. DCS has completed a comprehensive and disciplined reassessment of ICWIS, as approved by ACF. In general, the reassessment effort was geared towards identifying the critical issues that have prevented ICWIS from becoming fully SACWIS conformant, and determining the best approach to addressing those issues. In addition, through the ICWIS reassessment effort it was clear that the system was not easy to use nor aligned with how the work is done in the field, and that staff were using the system as “an after the fact” tool for data entry and not as an on-going decision support tool. This has led to staff often not entering data into the system in a timely and accurate manner. Future enhancements via the ICWIS Redesign are expected to effectively eliminate or address systemic factors that have notably interfered with accurate and timely data collection. It is Indiana’s assessment that once DCS staff has immediate on-line access to information, to include consideration of wireless capability, the bulk of systemic factors and concerns often discussed will be eliminated. In addition Indiana plans to continuously re-evaluate its equipment, hardware, and software to support these efforts.
Continuous Quality Improvement Process (CQI)
The Department of Child Services’ Continuous Quality Improvement (CQI) process produces a strategic plan that builds on the results of the QSR. The QSR and the QAR results serve as a guide for change, allowing the region to identify strengths as well as opportunities for improvement. The CQI process affords each region the opportunity to develop a plan to continue to enhance identified strengths as well as seize opportunities to improve the outcomes for children and their families. A comprehensive CQI process provides accountability for change at all levels of management and over an extended period of time. The CQI process begins with the completion of the QSR review week. The objective of this process is to provide the regions and the state with opportunities to continue improvement in the areas of practice and performance to ensure better outcomes for children and their families. Following the Grand Round, the Regional Manager utilizes the regional QSR and the QAR results to develop a Regional Strategic Plan. Each plan is unique, as it will encompass the input of community stakeholders and the Regional DCS staff to address areas where concerted action issues are noted and to detail strategies to be implemented for facilitating change for improvement in two indicators. Regional Managers will also outline their plan to improve the regional QAR results by identifying specific strategies for improving any areas affecting safety, permanency and well-being in addition to any areas targeted by the State Program Improvement Plan.
Staff Expansion and Training:
The Field Operations Division is the major catalyst through which practice reform initiatives are tested and implemented. This division of DCS manages clerical staff, family case managers, supervisors, county directors, regional managers, and field operations executive staff. The ultimate goal is to ensure that reform initiatives are translated into the daily work and practice with children and families. Several transformational initiatives have included child and family teams, clinical supervision, maintenance of caseloads, and staff retention. These initiatives were developed to meet the needs of supervisory and field staff. Staff enrichment is a
6/30/2009 Indiana Program Improvement Plan 11

focal point and considerable attention has been placed on staff selection, development, and retention. In 2007, Field Operations and Human Resources partnered together to begin exit interviews. These interviews were with staff who left the agency altogether or transferred from field work to a different department within DCS. The information gathered is used to address staff turnover and offer continual support for case management and supervision. The recurring reason or concern named in exit interviews was poor supervision. Local offices are addressing this by devising plans to focus on retention efforts. In conjunction, Field Operations continues a partnership with Human Resources to create a supervisory workgroup and toolkit. The focus of the workgroup is to develop supervisory-based competencies to improve the screening/interviewing tool used in hiring new supervisors and the toolkit is still under development but will act as a supervision model to train supervisors on how to supervise, manage, and support their staff.
Additionally, clinical consulting became operational in 2007; clinical consultants were assigned to train supervisors statewide on how to engage their staff in decision-making, build trust relationships, recognize and understand personality types, and create productive and safe staffing environments that will enhance the parallel process. These reform efforts created a proactive framework for the influx of new case managers hired to implement the new practice model and to reduce high number of cases assigned to family case managers. On March 31, 2008, DCS and the Governor of Indiana commemorated the graduation of the seventieth (70th) cohort of new case managers and subsequently, two additional cohorts graduated June 30, 2008 making a total of 72. Approximately 1500 case managers have been hired since the reorganization of the Indiana Department of Child Services and seventy-five new supervisors have been hired within the last year.
DCS believes that training and development of staff is paramount to the success of practice reform. Much time, effort, and resources continue to be invested in creating and implementing training curriculum. The goal is to inspire staff to utilize the reform initiatives that will produce positive and long-standing changes in the daily practices and delivery of services. All current staff, which was identified to be trained, has completed the Teaming and Engaging modules of the practice reform skills and have been slated to become Child and Family Team facilitators by July 2008. There is currently a roll-out training plan to ensure that all staff identified will complete training in the final two modules of the TEAPI model: planning, and intervening. This goal allows family case managers to offer Child and Family Team meetings to each family on their case load especially during the assessment (investigation) phase with the goal that comprehensive and timely safety plans are addressed during the initial stage of the case. Providing this support will improve and broaden service delivery and ensure that children and families’ individualized risks and needs are addressed and positive outcomes are achieved. The successful completion of the Teaming and Engaging is credited largely in part to the partnership with the Child Welfare Policy and Practice group that began in 2006. Initially, there was noted resistance to the TEAPI model by field staff. DCS decided to place throughout the state, peer coaches and peer coach trainers, to assist with the training and implementation of teaming and engaging and to oversee the facilitation of Child and Family Teams. The additional support afforded case managers processing time and the opportunity to witness the model in action before trying to implement it.
New workers will learn TEAPI skills during their twelve-week training. Once their training is complete, new workers will be assigned a peer coach to train in facilitation skills needed for Child and Family Team Meetings. Indiana recognizes that the practice model
6/30/2009 Indiana Program Improvement Plan 12

provides staff with a new tool but it does not stop there. Indiana has focused training efforts and supports on addressing best practice principles such as timeliness of service referrals, understanding the importance of locating non-custodial or absent parents, conducting quality visitations, proximal placement, assessing needs of foster parents, and identifying when families have substance abuse and domestic violence issues.
With the new training accomplishments, Indiana is now transitioning from the practice reform stage to practice implementation. Even though Indiana’s robust practice reform training curriculum and initiatives were noted as strengths, assessing on-going training needs for experienced workers is a goal outlined in the PIP. Indiana’s CFSR report indicated that the ongoing training for staff development was an area needing improvement. Coupling this with the non-conformity in the two safety outcomes, protection from abuse/neglect and children safely maintained in their home, Indiana will concentrate its experienced worker training curriculum on improving assessment skills and addressing risk and needs of children and their families. In the PIP matrix, Indiana illustrates the direction DCS wants to take in the next two years to equip field staff not only with the TEAPI skills but to emphasize the importance of locating absent and non-custodial parents, concurrent planning, Child and Family Teaming, setting timelines for permanency, all while engaging children and their families throughout the case planning process.
Clinical Supervision:
When the Clinical Supervision Model was implemented in 2007, the goal was to create a supportive staffing environment and provide supervisors and management with clinical supervision techniques that would enhance and support practice reform. Two clinical consultants were assigned to the state and met monthly or bi-monthly with management staff to provide clinical supervision tools and techniques in a group setting. Open dialogue and modeling occurred in these meetings so that supervisors and/or local office directors would utilize these tools within their supervision. The common themes and topics discussed during these sessions included but were not limited to the empowerment of workers, teambuilding, critical thinking and decision making, process of change, resistance, solution focused techniques, staff motivation, types of power, understanding and identifying biases, dealing with burn-out, and the parallel process. Staff changes have occurred since the inception of the model and both clinical consultant positions are currently vacant. Indiana will address in the PIP a plan to continue clinical supervision beyond its foundational point, as well as collaborating efforts with Staff Development to integrate the clinical supervision tools with staff training to ensure continued support of the practice reform initiatives and the TEAPI model. Policy Making and Revisions: The Practice Support Division of DCS manages policy development and its amendments, quality service reviews/quality assurance reviews, and ICWIS (Indiana Child Welfare Information System). These elements of DCS are crucial as they steer the way ninety-two (92) counties in Indiana implement, monitor, and record their involvement with children and families. In the last two years, Policy developments and revisions have been made to reflect the new practice model and to provide guidance and clarity on best practice standards for the entire state. DCS has undertaken an extensive review and rewrite of its Child Welfare Policy and practice manual. Since the onsite review in July 2007, several policy sections have been revised. Revisions were made that incorporated the preliminary results of the CFSR. The chapters that were revised
6/30/2009 Indiana Program Improvement Plan 13

include: General Case Management, Out of Home Care and Court. Another primary goal was to ensure that policy emphasized the inclusion of the new practice model in all related areas, and that TEAPI is conducted with families at every critical juncture. The new policy revisions have influenced many of the PIP’s action steps/benchmarks.
Diligent Searches for Non-custodial parents: One of the findings of the CFSR reflected in policy change was the engagement of non-
custodial parents in the case planning process. Indiana’s Child Welfare Policy now reflects the expectation that diligent efforts are to be made beginning with the initial involvement with a family to locate and engage the non-custodial parent and the extended family members. FCMs will be expected to present their findings with respect to absent parents at the time of the initial hearing in an Affidavit of Diligent Inquiry Report (ADI). Tools available to assist FCMs in locating absent parent(s) include:
o Indiana Support Enforcement Tracking System (ISETS); o Indiana Child Welfare Information System (ICWIS), o Indiana Client Eligibility System (ICES); o White Pages website at http://www.whitepages.com/; o Bureau of Motor Vehicles (BMV) at http://www.in.gov/bmv/; o County Jail o Department of Corrections (DOC) at http://www.in.gov/idoc/ o US Search at http://www.ussearch.com/
Programs and Services:
The Programs and Services Division is a crucial part of DCS’ structure as it focuses attention on appropriate services for children and families and on the long-term goals of children who have lengthy stays in the child welfare system. Programs and Services manage independent living programs, placement preservation, and adoption services and continue to apply resources toward the permanence and stability of children.
Service Standards:
Service standards are a list of guidelines that the provider has to follow to comply with DCS contractual requirements for each of the contracted services. Service standards were developed by identified needs regionally, agency vision and legislation. DCS’ has thirty-nine (39) service standards that address the following service needs: adoption, independent living, family-centered services, foster parent services and other services that include but are not limited to child advocacy centers, counseling, cross-system coordination and diagnostic/evaluation services. When a potential provider submits a RFP (request for proposal) to provide a service to the agency it must detail the service description, target population, goals and outcome measures, qualifications of all staff, rates/fees, case record documentation, and access to their services. All contracted services are currently monitored by Regional Service Coordinators.
Regional Service Councils:
Regional Service Councils were formed to identify and select services and providers for each region; ensure that needed services are available in the region to meet the needs of families and children; and assist DCS with provider monitoring through the review of outcomes. The final
6/30/2009 Indiana Program Improvement Plan 14
report of Indiana’s 2007 CFSR recognized that the Regional Service Councils contributed to the high level of performance on the CFSR indicators pertaining to several areas: services provided to families to protect children in their homes and prevent removal, permanency goal of another planned permanent living arrangement, placement with siblings, meeting with educational needs and physical health needs.
Independent Living Services:
Indiana current service efforts reflected in the PIP matrix include addressing transitional and independent living needs for children as well as regional training implemented to discuss and identify IL services needed in specific regions. DCS staff along with IL providers are generating more discussion about timeliness of referrals and meeting service needs.
Foster Care System:
Foster care-related needs and services were also addressed in the Final report. The PIP addresses these issues by emphasizing the efforts made by the Placement Unit of Programs and Services that has currently added three new personnel as well as four positions under the foster care title of Foster Care/Recruitment and Retention, Kinship Care, Foster Child and Birth Family. The goal for these different categories is to ensure foster care placement becomes a stronger and more viable process. The Placement Unit is taking a closer look at how both the birth family and resource family can work together in the Child and Family Team Meetings to best foster the child in service. A shortened version of the FAKT training that foster parents attend will be available for family case managers in order to improve their understanding of foster parenting and the licensing process. In addition, the PIP will address how FAKT training responsibility and development will transition to DCS’ department of Staff Development in approximately 2010.
Foster Care Improvement Initiative:
DCS initiated an internal foster care review group in 2008 to conduct a comprehensive evaluation of its foster care system. The current goal is to have executive management staff conduct a close examination of the organizational structure that governs the range of foster care services. Among many of the integral parts reviewed thus far, additional focus has been placed on the appropriateness of placements, foster parent preparedness for placements, placement stability, and the availability of foster family supports. This evaluation has generated additional discussions on how to improve the foster care system. Some preliminary recommendations include the modification of Indiana’s SACWIS system that will aid in matching children with foster families before placements occur, and the adoption of a thorough placement assessment tool that will evaluate the child’s need for placement and corresponding level of care. By utilizing both the SACWIS matching system and the placement assessment tool, DCS will be able to accurately determine the child’s level of care and placement need, i.e. regular, special needs or therapeutic. Additional discussion is centered on the specialization of field units that would take FCMs out of regular case rotation to solely administer foster care specialization and support services.
The ultimate goal of this initiative is to take the final recommendations from this group and implement them into DCS policy and practice with the effort of creating a more effective foster care system. In the PIP matrix, DCS identifies the steps necessary to achieve both foster care
6/30/2009 Indiana Program Improvement Plan 15

specialization units statewide and the adoption of a placement assessment tool within the next two years.
Casey Family Assessment:
DCS is exploring the possibility of using the Casey Family Assessment to assist families in assessing their readiness for foster care or adoption. The tool is designed to create individual family development plans, which can be used throughout the year to aid in foster parent retention. These changes along with DCS’ adoption of the strength-based philosophy and new practice model have paved the way for child welfare to generate more timely and positive outcomes.
Child Support and Fatherhood Initiatives: While efforts continue to improve the service planning and delivery, DCS equally has increased the awareness of how the lack of child support may contribute to the underlying needs of abused and neglected children. A goal has been to bridge the gap between the efficiency of child support payments and providing educational and program-related resources to both single and absent parents. The Child Support Bureau of DCS is currently involved in several grants and initiatives that will improve the way single and absent parents are engaged in the child welfare process. There has been $180,573 of both federal and state monies have been allotted to the Access and Visitation Grant. This grant is being disbursed to four initiatives: Family Services, Inc. (Dads Make a Difference): This program provides services to non-custodial parents who are not playing an active role in the development of their child or who are not paying court ordered child support. The goal is to offer an alternative to incarceration for fathers, provide support and encouragement, foster a relationship with the custodial parent, and allow the father access to parenting information and community resources. Legal Aid-District Eleven, Inc.: The program educates non-custodial parents on their legal rights, responsibilities, and allows them access to the court system for modification or enforcement of their legal rights. The goal is increase paternity establishment, consistency of child support collection, and involvement with children. Brown County Circuit Court (Family Access Program): The Family Access Program is currently in its eighth year providing services to counties in Southern Indiana. The services offered are supervised and therapeutic visitations, jail visitations, and transfer of custody services to non-custodial parents. Additional efforts are underway to increase involvement of fathers with their children, improve parenting skills and provide recent and accurate information for fathers. Fathers and Families Resource/Research Center, Inc is an additional initiative in collaboration with DCS. This program emphasizes the importance of fatherhood in Marion County by providing workshops, small group sessions, and individual counseling. The program offers a wide-range of counseling topics and through these services has increased the father’s involvement, parenting skills and child support collections. These initiatives are outlined in the PIP benchmarks geared toward reaching out to absent fathers and non-custodial parents.
Four-year Pilot Project: Engaging Non-Resident Fathers:
In 2007, DCS Marion County Office was awarded $488, 952 federal dollars to start the four-year pilot project: Engaging Non-Resident Fathers. This initiative is designed to assist fathers in Marion County who have had children removed for safety or neglect reasons. The premise for the project is to locate and then refer the non-resident fathers who are applicable for the program to the Fathers and Families Resource/Research Center, Inc. in Indianapolis, Indiana. This center offers extensive curriculum and support to the fathers. Dr. Gail Folaron from Indiana University
6/30/2009 Indiana Program Improvement Plan 16

School of Social Work is providing oversight for the four year project and will evaluate the effectiveness of the curriculum. Fathers and Families Resource Center has employed a full-time male staff to engage the fathers and incorporate the curriculum. The projected goal is to serve 120 fathers in the next four years. The grant is effective from January 2008 through March 2011. Indiana hopes to take the principles learned from this initiative, and adapt them to the needs of other counties. This goal is included in Strategy 1 in the PIP matrix.
DCS Legal Department and Court Initiatives:
DCS continues to make notable efforts to advance its legal services. The legal division manages various issues that involve contracts, legislation, waivers, licensing statuses, fingerprinting and out of state placements. Initiatives have been implemented within the last year to improve the way legal services are interpreted, accessed and delivered across the state as well as support FCMs as they implemented new practice model and best practice standards. In 2005, DCS began a change from primarily contracted attorneys to staff attorneys. DCS is completing the process of hiring counsel in the dozen or so counties where there are vacancies. These attorneys litigate CHINS and TPR matters. There are more than one hundred (100) such attorneys. There is a goal in the PIP that with the additional staff attorneys, FCMs and Supervisor will get the additional support and training necessary to better advocate for children and families in the court setting.
Court Improvement Project (CIP) Collaboration with DCS:
There are several recent CIP initiatives and training collaborations with DCS that were developed to improve child welfare practices and court responsiveness.
On December 14, 2007, Indiana Department of Child Services, Indiana Judicial Center and several community partners conducted “The Summit on Children – Hard Wired to Connect.” Each county was asked to bring a team to participate in the event, which included break out sessions and presentations geared toward helping the teams develop a county-specific child welfare plan to present to the Indiana Judicial Center. More than thirty-five counties were represented, and presenters included judges, DCS staff, service providers, foster parents, and Court Appointed Special Advocates. Finally, a joint training session with CASA and DCS was planned to address practice reform, the new legislative changes, and improving the working relationship between these parties.
The Court Improvement Program participated in a CHINS Strategic Planning Retreat on February 28-29, 2008 sponsored by the National Council of Juvenile and Family Court Judges Permanency Planning for Children Department and the Indianapolis Model Court. The purpose of the retreat was to identify strengths, areas of concern and recommendations for the dependency practice in Marion County. As a result of the Strategic Planning Retreat, several initiatives were implemented to address the identified concerns. These initiatives include the establishment of a domestic violence unit within the local office of the Indiana Department of Child Services and a mediation and facilitation program for CHINS cases.
The Court Improvement Program assisted with planning and funding the Annual 2-day Juvenile Judges Conference held June 19-20, 2008. The conference consisted of a collaborative meeting on the state of affairs in child welfare and included Juvenile Judges, Indiana Department
6/30/2009 Indiana Program Improvement Plan 17
of Child Service staff and GAL/CASA directors. The conference held a variety of discussions on House Enrolled Act 1001, P.L. 146-2008 and its impact on the judicial branch, Child and Family Service Reviews and Program Improvement Plans, Permanency Planning and Child and Family Team Meetings and a mental health pilot project for dependency cases.
Lastly, the following CIP initiatives outlined are specific to permanency goals and TPR hearings.
CIP provided Johnson County Circuit Court with funds to establish a pre-hearing facilitation program for CHINS and TPR cases. The goal of the program is to reduce the number of contested hearings, encourage the development of customized dispositional goals and service options earlier in the process, and to help move the parties beyond the legal formalities of the case and focus on reconciliation and permanency. It is anticipated that the pre-hearing facilitation will increase the investment and/or “buy-in” of the parties, reducing delay and improving potential for earlier family reunification. In Strategy 4 of the PIP matrix, Indiana addresses this initiative with an action step specific to the DCS Johnson County Local Office regarding mediations.
CIP provided Marion Superior Court, Juvenile Division with funds for a pre-hearing mediation and facilitation program for CHINS cases. The goals of this program are to decrease the number of contested fact-findings in CHINS cases, to achieve compliance with the statutory deadline of sixty (60) days to adjudication; to increase the understanding of families of the CHINS legal process; to achieve more timely permanence for children and to decrease the number of CHINS cases that go on to termination of parental rights. In Strategy 4 of the PIP matrix, Indiana addresses this initiative with an action step specific to the DCS Marion County Local Office.
CIP provided Tippecanoe County Superior Court 3 with funding for the court mediation and facilitation program. The program provides mediation/facilitation services in dependency cases and includes facilitation of case conferences, permanency planning conferences, and extended family conferences for purposes of educating the extended families about their participation in family case conferencing and permanency planning. In Strategy 4 of the PIP matrix, Indiana addresses this initiative with an action step specific to the DCS Tippecanoe County Local Office.
Indiana’s PIP will further address permanency planning with the Collaborative Training- Simulated Termination of Parental Rights trial - an initiative by CIP and DCS. The goal for this initiative is to train internal and external stakeholders on Indiana’s termination of parental rights process. CIP developed a written description of a case and role profiles and DCS employees including the Agency Director, James Payne, were the actors in the mock TPR trial. The facts and profiles were used to present the case as if it were an actual trial. After the direct and cross examination of each witness, participants were given the opportunity to make comments and to ask questions. The training session was professionally videotaped and will be edited into a training video that will be available for distribution to courts and other stakeholders in the child welfare system.
Lastly, DCS and CIP are collaborating on a new initiative: Pilot Permanency Project. Three counties will be identified to participate in this pilot project. Each county will assemble a team consisting of a representative from the court, DCS and GAL/CASA. The team will meet to
6/30/2009 Indiana Program Improvement Plan 18

review cases where parental rights have been terminated, adoption is the permanency plan but the adoption has not yet finalized. The teams will look for delays in permanency, the causes for those delays, and develop a protocol for responding to the reasons for the delays.
House Bill 1001: This bill effective January 1, 2009 has been instrumental in further shaping the funding
streams and practices that support services offered through the Department of Child Services. Following are areas in the PIP in which the bill will or has altered to include the transference of funding, contracts, and state budgetary responsibilities from the county to state level, further defined regional service regions, clarification of the composition of regional plans, and identified requirements for participation and membership of RSCs. In addition, HEA 1001 modified the time standards for IAs, explained DCS’ jurisdiction of wardship cases, services and placements, and illuminated the court process of approval/disapproval of service plans. Lastly, this bill further specified the attorney and court practices related to terminations and CHINS filings, and described the membership and duties of county Child Protection Teams.
Senate Bill No. 365:
This bill is currently in legislative session as of February 2009, and if passed will be instrumental in changing various practices regarding the involvement of family members when a child becomes a ward as well as adoption procedures. Additional possible changes include but are not limited to drug/alcohol screens in fatality cases, cost and reimbursement of Medicaid services, case management and case reporting changes in probation cases, case manager safety, educational updates in a ward’s case plan, requirements for criminal history checks, and redefining or reclassifying various child welfare terminology.
Conclusion Practice Reform Overview:
By providing a historical and thorough account of the initiatives and practice reform efforts, Indiana anticipates that the PIP is not viewed solely as a response to the CFSR findings but more importantly, an extension and implementation of the Practice Reform vision that DCS began over three years ago.
6/30/2009 Indiana Program Improvement Plan 19

Mission:
The Indiana Department of Child Services (DCS) protects children from abuse and neglect. DCS does this by partnering with families and communities to provide safe, nurturing, and stable homes.
Vision: Children thrive in safe, caring, supportive families and communities.
Values: We believe every child has the right to be free from abuse and neglect. We believe every child has the right to appropriate care and a permanent home. We believe parents have the primary responsibility for the care and safety of
their children. We believe the most desirable place for children to grow up is with their own
families, when these families are able to provide safe, nurturing, and stable homes.
We believe in personal accountability for outcomes, including one's growth and development.
We believe every person has value, worth, and dignity.
2. Development of the Program Improvement Plan Indiana’s CFSR onsite review was conducted July 9-13, 2007 in three counties;
Jefferson, Montgomery and Marion. Areas of strength and improvement were noted for each site. The PIP is a detailed instrument guiding how these strengths will be improved and how the deficiencies determined will be addressed. DCS continues efforts to improve the process in which children and families are involved and consequently, modify the same system in which staff and external stakeholders must operate. Indiana’s Department of Child Services (DCS) began developing its Program Improvement Plan (PIP) prior to receiving the CFSR Final report based on the information generated from the statewide assessment and preliminary findings identified through the CFSR exit conference. The PIP is the response to findings presented in the U.S. Department of Health and Human Services Children’s Bureau Report on Indiana’s Child and Family Services Review (CFSR). The CFSR requires any state to implement a PIP if the state is found to be in non-conformity with the requirements of the CFSR.
PIP Kick-off and PIP Workgroups:
DCS sought and received technical assistance from the National Resource Center for Organizational Improvement in order to plan and conduct a statewide PIP Kickoff meeting. This meeting was held on September 14, 2007. From this PIP Kick-off, a Program Improvement Plan (PIP) team was formed to address the issues identified in the CFSR. The focus of the PIP team was to begin work on a comprehensive plan to improve child welfare practice. The PIP team was developed in partnership with several stakeholders who participated in ongoing workgroups.
6/30/2009 Indiana Program Improvement Plan 20

Indiana Department of Child Services established these workgroups consisting of internal and external stakeholders. Many of the same state and local stakeholders were instrumental in developing the Statewide Assessment. The external stakeholders included judges, GAL/CASA, university partners, service providers, faith community, educational partners, tribal entities, youth, parents and foster parents. The stakeholders were assigned to workgroups based on their subject matter expertise and experience. Ten (10) workgroups were formed and assigned a specific outcome to identify goals, formulate strategies to meet these goals, and develop action steps needed to achieve and accomplish the necessary work. The workgroups were:
1. Safety Outcome 1: Children are first and foremost, protected from abuse and neglect. 2. Safety Outcome 2: Children are safely maintained in their homes whenever possible and
appropriate. 3. Permanency Outcome 1: Children have permanency and stability in their living
situations. 4. Permanency Outcome 2: The continuity of family relationships and connections is
preserved for children. 5. Well-Being 1: Families have enhanced capacity to provide for their needs. 6. Well-Being 2: Children receive appropriate services to meet their educational needs. 7. Well-Being 3: Children receive adequate services to meet their physical and mental
health needs. Additional workgroups:
8. Independent living 9. Engaging absent Parents (non-custodial, absent fathers) 10. Foster Parent Recruitment, retention and Support.
The workgroups held a series of meetings beginning 9-14-07 to share the feedback from the
Exit conference and solicit input regarding strategies to address areas not found to be in substantial conformity. Plans to implement systemic change and make improvements for areas found not to be in substantial conformity were generated from this input.
The success of this PIP lies in its holistic approach with each program area supporting the other and forming the foundation which to build sustainable reform. Since, the CFSRs measures for safety, permanency, and well-being can not be focused on separately, change should occur in all areas simultaneously. PIP Conference:
After the receipt of the final report, Indiana reconvened the PIP workgroups and held a PIP conference May 14, 2008. Nearly eighty (80) DCS staff and external stakeholders attended the event. The ten PIP outcome workgroups met to discuss the findings of the final report and later conducted break-out sessions to review the rough draft of the PIP matrix and devise additional action steps and benchmarks as needed. Four additional workgroups were created to address the non-conformance in the following systemic factors: Case Review System, Training, Service Array, and Quality Assurance System.
Indiana PIP Format:
6/30/2009 Indiana Program Improvement Plan 21
Indiana patterned its PIP based on the standard format suggested by Administration for Children & Families (ACF). It is a combination of narrative and matrix formats. The narrative describes the various divisions within the Department of Child Services and gives brief descriptions of current initiatives in each area. The matrix details four primary strategies, action steps, and benchmarks that the state will pursue to achieve its goals for improving safety, permanency, and well-being outcomes for children and families of Indiana. The matrix is formatted in such a manner that Indiana will be able to utilize it to report on PIP progress. Summary of CFSR Findings:
ACF determined that based on the data profiles gathered from FY 2004, 2005, and the end of the 12-month CFSR data reporting period of March 31st 2006, Indiana’s Department of Child Services was not in substantial conformity with the safety and permanency outcomes. The on-site case reviews consisted of reviewing the case files, interviewing community partners, stakeholders, foster parents and youth involved with the child welfare system. Although the results of the on-site case reviews indicated that DCS was not in substantial conformity with any of the seven outcomes and systemic factors, strengths were found in key areas. Strengths were found in the following items measured: foster care re-entry, proximity of placement, statewide information system, periodic reviews in a judicial setting, notification of foster parents and pre-adoptive parents of judicial hearings for such a child, staff ensures that programming in place that protects the safety and health of children, staff training and development program that support goals and objectives of titles IV-B and IV-E funding, individualized services to meet unique needs, state engagement with community-based and professional stakeholders to ensure the goals and objectives of Child and Family Services Plan (CFSP) are achieved, the services under the CFSP are coordinated with services or benefits of other federally assisted programs serving the same populations, state’s standards for foster family homes and child care institutions are in accord with national standard, standards are applied to all licensed or approved foster family homes are child care institutions receiving title IV-B and IV-E funds, state compliance to criminal background clearances as related to licensing or approving foster care and adoptive placements, and lastly, Indiana is noted to have an effective process in place for timeliness of adoptions.
DCS feels confident that while the agency conducts an overhaul in practice changes, philosophy, and organizational structure, the current reform initiatives will permeate throughout all levels of Indiana’s child welfare system. By concerted hard work, DCS will ensure the practice model and other initiatives translate to all aspects of service delivery with children and families. Although it has been three years since the establishment of DCS and its new practice reform, Indiana realizes that successes are incremental and efforts will continue forward with the parallel and transparent process. This progress will then manifest in the data profiles, interactions between case managers and children and families, and become overwhelmingly reflective in future federal reviews. PIP Primary Strategies:
Indiana’s Practice reform is the mainstay for the development of the primary strategies and action steps to follow. DCS selected its four primary strategies (themes) to serve as guideposts in the development of the PIP matrix. After careful discussion and collaboration among the DCS
6/30/2009 Indiana Program Improvement Plan 22
Director, Deputy Director of Field Operations, and the eighteen (18) regional managers throughout the state, it was concluded that Indiana’s child welfare system must identify and focus on the strategies (themes) that would address staff development, community partnership, individualized services, and systemic change. The strategies are the overarching goals for Indiana and have been developed to maximize the practice reform efforts currently in progress, and catapult effective and long-term changes both systemically and with the abused and neglected children and their families in which this system serves. The action steps and benchmarks for the permanency, well-being, and safety outcomes were organized under each related strategy. Thus, each primary strategy will have a combination of action steps that will address safety, permanency, and well-being needs and concerns. The Primary Strategies are:
1. Development of staff to have assessment skills and competencies that determine the risks and needs of children and their families.
a. (Goal) Maintain the ability of staff to appropriately assess and address the risk and needs of children and families.
The Practice Reform Principles in which this strategy supports:
If a child is determined to be unsafe, DCS and the family will develop a timely plan to keep the child safe, with all efforts toward services to protect the child in his/her own home.
When children require out-of-home placements, careful assessment and evaluation shall
be utilized when making placement decisions in an effort to promote a single placement for children.
All efforts should be made for children to remain in their own neighborhoods and
maintain existing connections with families, schools, and friends.
Reunification and permanency is accelerated when visitation between parents and children is frequent and in the most normalized environment possible.
Parents should be empowered and given the opportunity to take responsibility for their
children and resolve issues of abuse and neglect.
When children require out-of-home placements, they should maintain essential connections through frequent and meaningful contact with significant persons in their lives.
Children and families will receive prompt and individualized service planning
Every person has value and worth and will be treated with honesty and dignity. Every
family has strengths that can be developed.
6/30/2009 Indiana Program Improvement Plan 23
Family members are experts of their own families. Service planning will consider the family rules, traditions, history, and culture.
Concurrent planning shall begin at the commencement of CHINS proceedings.
One of the core values for Indiana’s Department of Child Services is that every person
has value, worth, and dignity. This value is honored when each child and family’s individualized needs are assessed and addressed. When this occurs, families are allowed to assume the primary responsibility for the care and safety of their children. Indiana’s CFSR report acknowledged the praiseworthy efforts available in Indiana regarding service array. However, there were concerns noted with service gaps in areas of behavioral health, substance abuse services, foster homes, lack of services and training opportunities for Spanish speaking children and families, and delayed implementation of independent living services. 2. Ensure that individualized programs and services are delivered to families and
children in order to achieve safety, permanency, and well-being outcomes. a. (Goal) Properly credentialed and culturally competent staff with specific areas of
expertise delivers services. The Practice Reform Principles in which this strategy supports:
Services to children and families shall be planned and delivered through a
straightforward, flexible individualized service plan developed by the child, family, and service team.
To facilitate reunification, parents must be involved in treatment planning and service
plan delivery, because when the strengths and voices children and families are recognized, respected and affirmed, they are more likely to use them for change.
Developing effective services is a shared responsibility best achieved by families,
community partners, and public agencies working collaboratively.
The Department of Child Services will assist families in this community / family collaboration to find resources that make children and families safe.
Strengths-based service plans are developed using a family team and a comprehensive
assessment of the child and family’s needs. Plans should be needs-based and should specify steps to be taken by each member of the team, time frames for accomplishment of goals, and concrete measurements to monitor the progress of the child and family.
An additional systemic factor included within this section is Foster Parent Licensing
Recruitment and Support. The 2007 CFRS Final Report noted that Indiana in regards to Item 6: Placement stability, Item 34: foster parent, adoptive parents and licensed facilities and training needs, and Item 44: diversity of foster care recruitment, did not meet standard and were all areas
6/30/2009 Indiana Program Improvement Plan 24
needing improvement. The action steps and benchmarks listed in this section address these concerns by focusing on respite care services as a preventative measure, development of strategic plans to increase the quantity of diverse foster homes, and increase the accessibility of foster parent training.
3. Ensure that services are developed and planned in partnership with families and communities to protect children in their community through cooperation and communication.
a. (Goal) Increase the inclusion of community partners in the assessment and delivery of services for the protection of children.
The Practice Reform Principles in which this strategy supports:
Families and communities are responsible for ensuring that children thrive.
DCS will work jointly with service providers who adhere to effective social work practices in the delivery of services and providers will be held responsible for demonstrating expected outcomes.
DCS staff relationships and communications with community partners will be conducted
with empathy, honesty, and openness.
Services should be planned and developed in partnership with families and communities and provided in the least restrictive and most home-like settings.
One of the key established values within DCS is that “developing effective services is a
shared responsibility best achieved by families, community partners and public agencies working collaboratively”. DCS recognizes that it takes the collective efforts and commitment from public and private social service systems to ensure positive outcomes with children and their families. DCS enforces this belief by partnering with families and communities to provide safe, nurturing, and stable homes. Although Indiana scored well with Agency Responsiveness to the Community, the systemic factors of Service Array and Case Review System were areas needing improvement. Therefore, collaborations with multiple partners will be the focus of the action steps within this primary strategy. The efforts include collaborations with CASA to promote absent parent involvement, introducing legislation to ensure DOE continues to educate wards by providing the advocacy necessary to meet their educational needs, continued support of foster parents, expanding databases to locate absent parents, ensuring FCMs are empowered advocates in the court settings, and education of staff on domestic violence issues.
4. Create an infrastructure that will support and sustain all components of delivery within the child welfare system.
a. (Goal) Staff is better equipped to meet safety, permanency, and well-being outcomes for children and their families.
The practice reform principles in which this strategy supports:
6/30/2009 Indiana Program Improvement Plan 25
A timely, thorough, and thoughtful response to child safety concerns is critical in effectively protecting children.
Since the establishment of DCS as a separate entity, many synchronized attempts have
been made to ensure practice consistency and efficiency, organizational development, practice supports, and staff development.
Families are core members of the decision making team, therefore decisions about child
and family team interventions shall be relevant, comprehensive, and effective.
Coordination of the family team and accomplishment of its goal is essential and works most effectively when it occurs via regular face-to-face meetings that ensure more successful and positive outcomes.
Plans that are needs based, rather than service driven, are more likely to facilitate safety,
well-being, and permanency.
Historically, the dysfunctions of the child welfare system prohibited the achievement of outcomes and allowed varied practices throughout the ninety-two (92) counties. Indiana’s practice reform efforts included uniformity of practice with all levels of child welfare and the provision of tools and supports necessary to serve abused and neglected children and their families.
One of the missions in creating effective staff infrastructure is collaborative assistance and guidance in the recruiting, selection, and management of staff throughout the state. High rates of staff turnover had a direct negative impact on the agency’s ability to achieve successful outcomes for families and children. One critical objective was to increase total staffing over the last three years to meet the agency’s statutory mandate to reduce caseloads to 12/17 throughout the state. DCS began a three-year initiative and increased FCM staffing from 708 in July 2005 to 1582 by July 2008.
Recognizing that the case management system suffered and needed adjustment due to the high influx of new FCMs and supervisors, Indiana squarely focused its PIP action steps around case review concerns noted in the CFSR final report. Within this section Indiana addresses parental involvement in case planning; clarifying the TPR process with stakeholders, court advocacy, and permanency hearing related issues. Several action steps in this section address the court initiatives regarding permanency, TPR hearings and the timeliness of these processes. Indiana has two technical assistance tools, ICWIS and QAR, which support child welfare data collection and integrity. The CFSR final report acknowledged that ICWIS was in substantial conformity for its ability to capture critical and federally required information throughout the life of a child welfare case. Even though the quality assurance process in Indiana was under major expansion and revision during the CFSR review period, Indiana did not meet conformity standards in the Quality Assurance systemic factor. Indiana will utilize the PIP process to thoroughly address this area of need. Action steps under this strategy focuses on continuous quality improvement and how to measure overall practice efforts and progress.
6/30/2009 Indiana Program Improvement Plan 26
3. Quality Assurance Review (QAR Tool) One of the purposes of a Child Welfare Quality Assurance Review (QAR-Compliance)
review is to strengthen the operation of the Department of Child Services, improving services to families in Indiana. The second purpose of a QAR review is to provide the Department Director with an objective analysis of the child welfare system managed across the state by the Local Department of Child Services. The analysis identifies strengths of the system as well as areas that need specific attention in order to further strengthen the system and remain in compliance with federal and state laws, regulations and policies.
The tools are designed to assess the level of compliance with federal and state statutes, regulations, and policies, and adherence to best social work practice. (See Attachment: Indiana QAR Tools Part 1, Part 2 and Part 3) The Quality Assurance Review Tool assists DCS in ensuring safety, permanency, child and family well-being, as well as evaluating systemic factors in the local departments and statewide, such as case review system, service array, and agency responsiveness to the community. The results will be utilized by DCS to achieve positive outcomes for children.
Method of Review for Second Party Reviews: The second party (self) review process consists of a random sample of two cases per worker
per Supervisor per quarter in each county data pool which results in approximately 12,000 cases reviewed annually. Marion County’s pull is approximately 20% of all the cases reviewed. Currently there are 240 Supervisors and 1589 Family Case Managers statewide. The pull consists of the following case types: Child Protection Intake and Investigative Reports Informal Adjustments (IA) Children in Need of Services (CHINS/Wardship) cases
The pull consists of any case with an open case type within the previous 6 months from the pull date. The period under review is the previous year dating from the date of the review back one year. The review is aimed at measuring compliance, consistency and good practice. The Quality Assurance Tools are standardized instruments of policy questions, which are then applied to the cases reviewed. The supervisor reviews both hard copy files and the Indiana Child Welfare Information System (ICWIS). All case types were reviewed until December 2007. Service Referral Agreements are no longer reviewed due to a change in legislation restricting the creation of SRA cases beyond 7-1-2007.
Method of Review for Third Party Reviews: The third party (peer) review process consists of a random regional sample of second party
cases that were reviewed during the previous quarter. The number of cases pulled is determined by the number of administrative staff assigned to each region divided in half to conduct a one day peer review of cases from the regional pull: Child Protection Intake and Investigative Reports
6/30/2009 Indiana Program Improvement Plan 27

Informal Adjustments Children in Need of Services (CHINS/Wardship) cases 50 Screen Outs per region (900 total per quarter)
The pull consists of any case with an open case type within the previous 6 months for the pull date and 50 screen outs per the entire region. As with the second party reviews, the period under review is the previous year dating from the date of the review back to one year and the cases are reviewed for compliance, consistency and good practice. The Quality Assurance Tools are standardized instruments of policy questions was applied to the cases reviewed. The supervisor reviews both hard copy files and the Indiana Child Welfare Information System (ICWIS).
DCS began a comprehensive redesign of its Quality Assurance Review (QAR-compliance) process in October 2005. As part of this effort, DCS staff began researching QAR practice used in other state agencies and those of other Child Welfare organizations. The QAR process began the automation processes in December 2006. Multiple redesign meetings occurred between Performance and Quality Improvement management staff, the Indiana Office of Technology and the Office of Data Management to research an appropriate data base to house the QAR review information. As a result, the QAR reviews are now done quarterly by each supervisor by accessing the data base. Third party peer reviews will be conducted following each quarterly review completed by supervisors. In addition, plans to partially automate the Share Point data base by drawing data from the ICIWIS in conjunction with results submitted through quarterly supervisory reviews are in process. The new QAR process was piloted in February 2007 on a Share Point data base.
In March 2007, corrections were made to the data base and the random pull process. In April 2007, QAR training was conducted for all regional DCS administrative staff that will participate in the QAR processes. In May 2007, supervisors began using the QAR process. The first regularly scheduled QAR began July 1, 2007 and continued through to December 31, 2007. As mentioned earlier, the QAR paused from January 1, 2008 through June 30, 2008 to allow the Department to focus on compliance with caseload sizes legislated to begin July 1, 2008. Quarterly reviews resumed July 1, 2008. Due to logistical reasons and the pause, the first third party review began October 1, 2008.
4. Technical Assistance (TA) Workplan There has been discussion between Indiana and National Resource Center for Organizational Improvement, NRCOI, to determine specific Technical Assistance (TA) needs. Attached below is the TA Matrix identifying the TA needs and the TA services either in place or underway to meet those needs. Additionally, TA support with Casey Family Programs for leadership consultation began in Fall 2008 and will through Summer 2009.
6/30/2009 Indiana Program Improvement Plan 28

TECHNICAL ASSISTANCE MATRIX INDIANA DEPARTMENT OF CHILD SERVICES
ISSUE ACTIVITY (TA) TA LEADS INDIANA LEAD STATUS
TECHNICAL ASSISTANCE – Concurrent Planning
Formally integrate concurrent planning within all aspects of the child welfare system
NRC for Family-Centered Practice and Permanency Planning (Stephanie Boyd Serafin)
Regina Smith/Steven Cox
Discussion and consultation between NRCOI and Indiana will continue
Training System Assist in the further development of IN Training System, assessment of staff training needs and expansion of training linked to the Practice Reform initiatives.
NRC for Organizational Improvement (Susan Kanak)
MB Lippold NRCOI has been consulting with IN on various IN Training System issues and will continue to do so.
Independent Living
Education of DCS staff and providers regarding IL requirements and services; training on use of Ansell Casey instrument
NRC for Youth Development (Dottie Ansell)
Cassandra Porter NRCYD has been working with IN on IL issues.
PIP Measurement Develop a PIP measurement strategy for IN PIP
NRC for Organizational Improvement (Peter Watson)
Angela Green and Regina Smith
Discussion and consultation between NRCOI and Indiana will continue
6/30/2009 Indiana Program Improvement Plan 29

II. PIP Strategy Summary and TA Plan
State: Indiana Date Submitted: July 15, 2008
PRIMARY STRATEGIES KEY CONCERNS TA RESOURCES NEEDED
1. Development of staff to have assessment skills and competencies that determine the risks and needs of children and their families.
Timely initiation of assessments (investigations).
Inadequate or lack of safety
plans and/or incomplete risk assessments.
Formalized concurrent planning
is either not practiced or varies in practice from county to county.
Infrequency and inconsistency
with visitation between case worker and child and with child and his/her family members.
Preservation of the family and
community connections of children placed in care to include family-friendly visitations, frequent siblings contacts, and when possible remains in their community school.
Child and Family Team
meetings are not utilized properly to identify and address the needs of children.
Continuity of care on caseloads
Many children aging out of care
are not prepared for independent living.
6/30/2009 Indiana Program Improvement Plan 30
PRIMARY STRATEGIES KEY CONCERNS TA RESOURCES NEEDED
Inconsistency in establishing permanency goals and achieving permanency goals of reunification, permanent placement with relatives, guardianships or adoptions in a timely manner.
6/30/2009 Indiana Program Improvement Plan 31
PRIMARY STRATEGIES KEY CONCERNS TA RESOURCES NEEDED
2. Ensure individualized programs and services are delivered to families and children in order to achieve safety, permanency, and well-being outcomes.
Individualized programs and services need to reflect the following: practice reform initiatives, best practices related to emergency and safety responses, client services and implementation, information sharing across counties, and staff work expectations.
Insufficient assessment of
domestic violence issues when intervening with children and their families.
Foster parents are inadequately
prepared to care for behavioral, emotional and special needs of children.
Funding for programs and
services to support the least restrictive environments is made available.
Children have multiple
placements or unstable placements and efforts to place siblings together are not consistent throughout a child’s time in care.
6/30/2009 Indiana Program Improvement Plan 32
PRIMARY STRATEGIES KEY CONCERNS TA RESOURCES NEEDED
3. Engage multiple partners to protect children in their communities through cooperation and communication.
All systemic partners involved with child and/or family speak the common language and share collaborative goals.
6/30/2009 Indiana Program Improvement Plan 33

PRIMARY STRATEGIES KEY CONCERNS TA RESOURCES NEEDED
4. Continue infrastructure within DCS that will support and sustain all components of program delivery.
Staff professional growth and staff sustainability is addressed.
Quality Assurance review in
placed to ensure quality and improvement of services.
Permanency and TPR hearings
are inconsistent as it relates to planning, court proceedings and inclusion of all parties involved with case.
Clinical supervision of staff
needs to reflect the new practice model.
6/30/2009 Indiana Program Improvement Plan 34
III. PIP Agreement Form
Agreements The following Federal and State officials agree to the content and terms of the attached Program Improvement Plan:
7/15/08
Name of State Executive Officer for Child Welfare Services Date
Children’s Bureau Date
6/30/2009 Indiana Program Improvement Plan 35

6/30/2009 Indiana Program Improvement Plan 36
Amendments
Approval of State Executive Officer for Child Welfare Services
Renegotiated Action Steps, Benchmarks, or Improvement Goals
Date Renegotiated
Approval Children’s Bureau
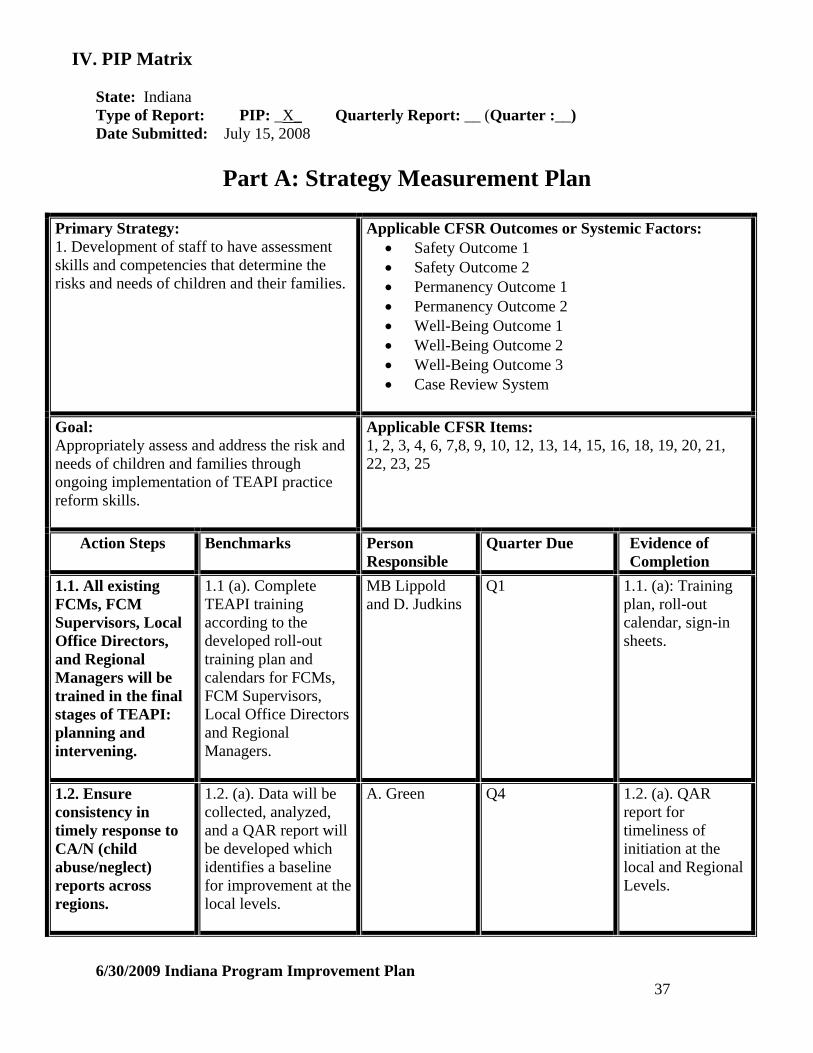
IV. PIP Matrix State: Indiana Type of Report: PIP: _X_ Quarterly Report: __ (Quarter :__)
Date Submitted: July 15, 2008
6/30/2009 Indiana Program Improvement Plan 37
Part A: Strategy Measurement Plan
Primary Strategy: 1. Development of staff to have assessment skills and competencies that determine the risks and needs of children and their families.
Applicable CFSR Outcomes or Systemic Factors: Safety Outcome 1 Safety Outcome 2 Permanency Outcome 1 Permanency Outcome 2 Well-Being Outcome 1 Well-Being Outcome 2 Well-Being Outcome 3 Case Review System
Goal: Appropriately assess and address the risk and needs of children and families through ongoing implementation of TEAPI practice reform skills.
Applicable CFSR Items: 1, 2, 3, 4, 6, 7,8, 9, 10, 12, 13, 14, 15, 16, 18, 19, 20, 21, 22, 23, 25
Action Steps
Benchmarks
Person Responsible
Quarter Due Evidence of Completion
1.1. All existing FCMs, FCM Supervisors, Local Office Directors, and Regional Managers will be trained in the final stages of TEAPI: planning and intervening.
1.1 (a). Complete TEAPI training according to the developed roll-out training plan and calendars for FCMs, FCM Supervisors, Local Office Directors and Regional Managers.
MB Lippold and D. Judkins
Q1
1.1. (a): Training plan, roll-out calendar, sign-in sheets.
1.2. Ensure consistency in timely response to CA/N (child abuse/neglect) reports across regions.
1.2. (a). Data will be collected, analyzed, and a QAR report will be developed which identifies a baseline for improvement at the local levels.
A. Green Q4 1.2. (a). QAR report for timeliness of initiation at the local and Regional Levels.

IV. PIP Matrix State: Indiana Type of Report: PIP: _X_ Quarterly Report: __ (Quarter :__)
Date Submitted: July 15, 2008
6/30/2009 Indiana Program Improvement Plan 38
Primary Strategy 1 (con’t)
1.2(b). The Regional Manager will review QAR results for each county that is found to be in non-compliance of timely initiation response for one (1) QAR review.
D. Judkins
Q4, Q6, Q8
1.2. (b). Review schedule and review plan at Q4, Q6 and Q8.
1.2. (c). Each Region will submit a quarterly Strategic Action Plan (SAP) that will address response timeliness in compliance with statutory requirements
D. Judkins Q4, Q6, Q8 1.2 (c). SAP report
1.2. (d). The SAPs will be based on the practice indicators, and QAR results and reviewed by executive management quarterly for discussion and further planning.
D. Judkins
Q4, Q6, Q8
1.2. (d). SAP reports and outcomes of further planning determined.
1.3. CFTMs/case conferences will be used to develop effective and achievable safety plans to ensure children are safe at the time of DCS’ initial involvement and thereafter until case closure.
1.3 (a). Assessors (investigators) will conduct a CFTM/case conference during the initial stage of the case and develop a safety plan when a report is substantiated and further action is determined (IA, In-home CHINS, and Out of Home CHINS).
D. Judkins
Q2
1.3. (a). QAR Report will indicate the percentage of initial CFTMs completed with a safety plan developed.
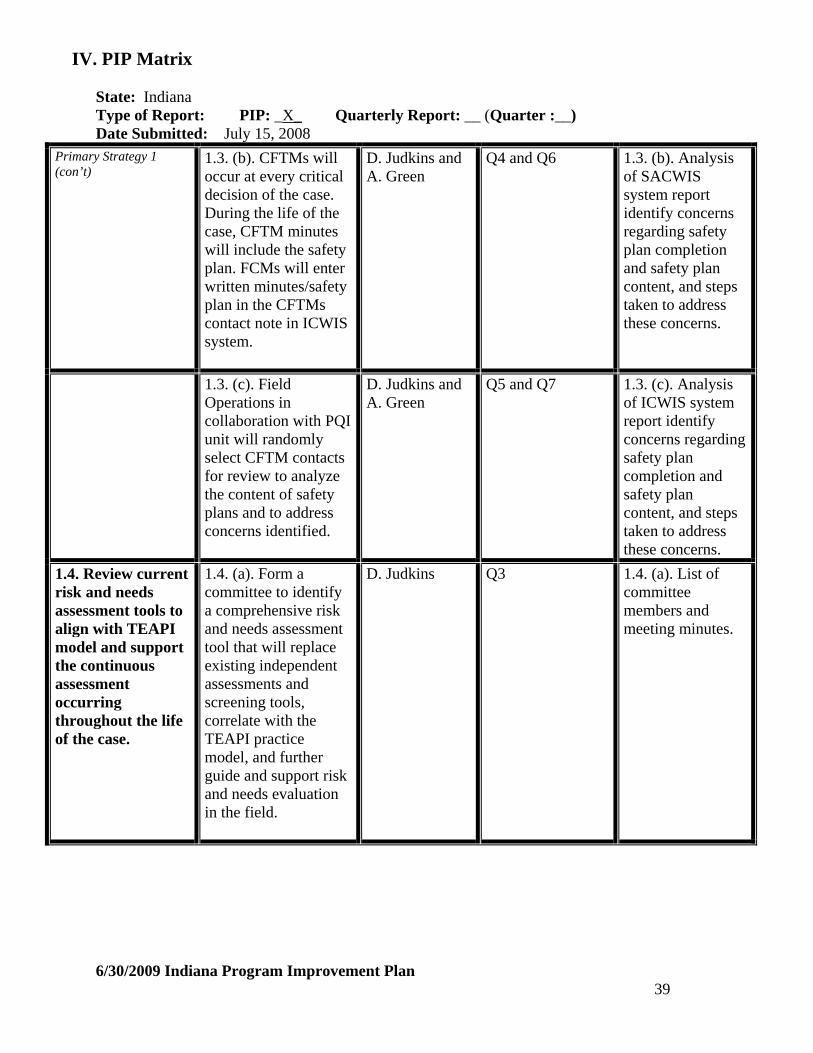
IV. PIP Matrix State: Indiana Type of Report: PIP: _X_ Quarterly Report: __ (Quarter :__)
Date Submitted: July 15, 2008
6/30/2009 Indiana Program Improvement Plan 39
Primary Strategy 1 (con’t)
1.3. (b). CFTMs will occur at every critical decision of the case. During the life of the case, CFTM minutes will include the safety plan. FCMs will enter written minutes/safety plan in the CFTMs contact note in ICWIS system.
D. Judkins and A. Green
Q4 and Q6 1.3. (b). Analysis of SACWIS system report identify concerns regarding safety plan completion and safety plan content, and steps taken to address these concerns.
1.3. (c). Field Operations in collaboration with PQI unit will randomly select CFTM contacts for review to analyze the content of safety plans and to address concerns identified.
D. Judkins and A. Green
Q5 and Q7 1.3. (c). Analysis of ICWIS system report identify concerns regarding safety plan completion and safety plan content, and steps taken to address these concerns.
1.4. Review current risk and needs assessment tools to align with TEAPI model and support the continuous assessment occurring throughout the life of the case.
1.4. (a). Form a committee to identify a comprehensive risk and needs assessment tool that will replace existing independent assessments and screening tools, correlate with the TEAPI practice model, and further guide and support risk and needs evaluation in the field.
D. Judkins
Q3
1.4. (a). List of committee members and meeting minutes.
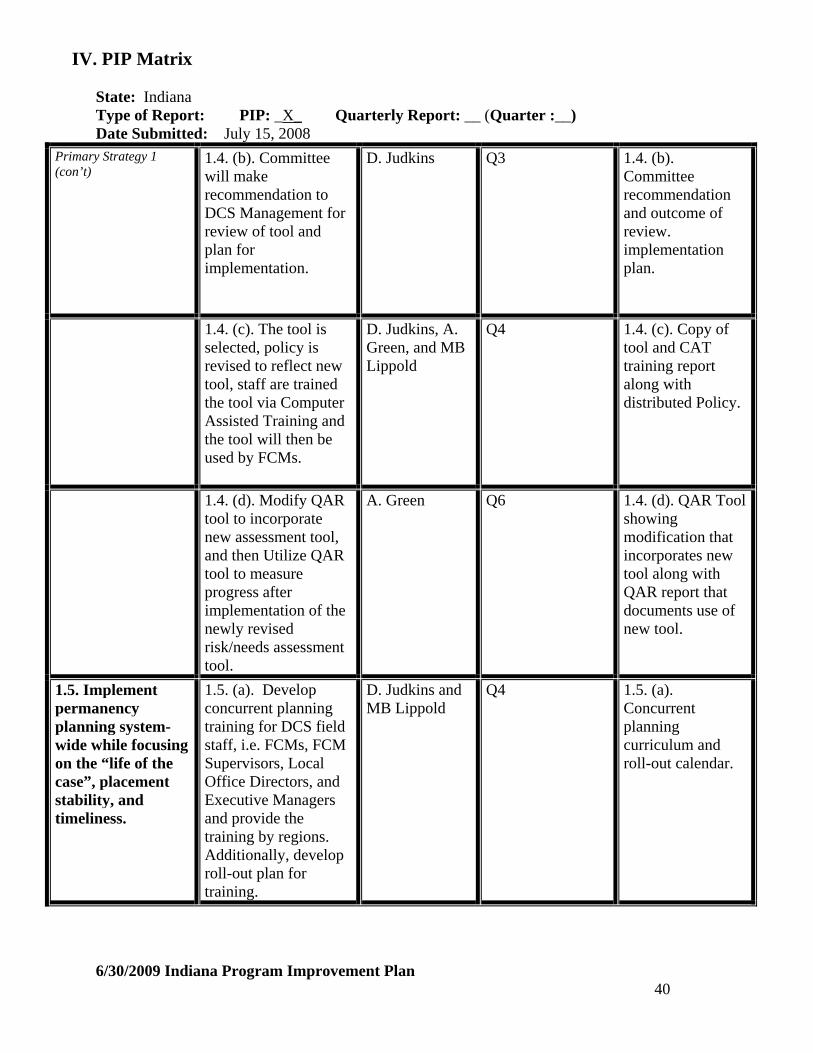
IV. PIP Matrix State: Indiana Type of Report: PIP: _X_ Quarterly Report: __ (Quarter :__)
Date Submitted: July 15, 2008
6/30/2009 Indiana Program Improvement Plan 40
Primary Strategy 1 (con’t)
1.4. (b). Committee will make recommendation to DCS Management for review of tool and plan for implementation.
D. Judkins
Q3
1.4. (b). Committee recommendation and outcome of review. implementation plan.
1.4. (c). The tool is selected, policy is revised to reflect new tool, staff are trained the tool via Computer Assisted Training and the tool will then be used by FCMs.
D. Judkins, A. Green, and MB Lippold
Q4
1.4. (c). Copy of tool and CAT training report along with distributed Policy.
1.4. (d). Modify QAR tool to incorporate new assessment tool, and then Utilize QAR tool to measure progress after implementation of the newly revised risk/needs assessment tool.
A. Green
Q6 1.4. (d). QAR Tool showing modification that incorporates new tool along with QAR report that documents use of new tool.
1.5. Implement permanency planning system-wide while focusing on the “life of the case”, placement stability, and timeliness.
1.5. (a). Develop concurrent planning training for DCS field staff, i.e. FCMs, FCM Supervisors, Local Office Directors, and Executive Managers and provide the training by regions. Additionally, develop roll-out plan for training.
D. Judkins and MB Lippold
Q4 1.5. (a). Concurrent planning curriculum and roll-out calendar.
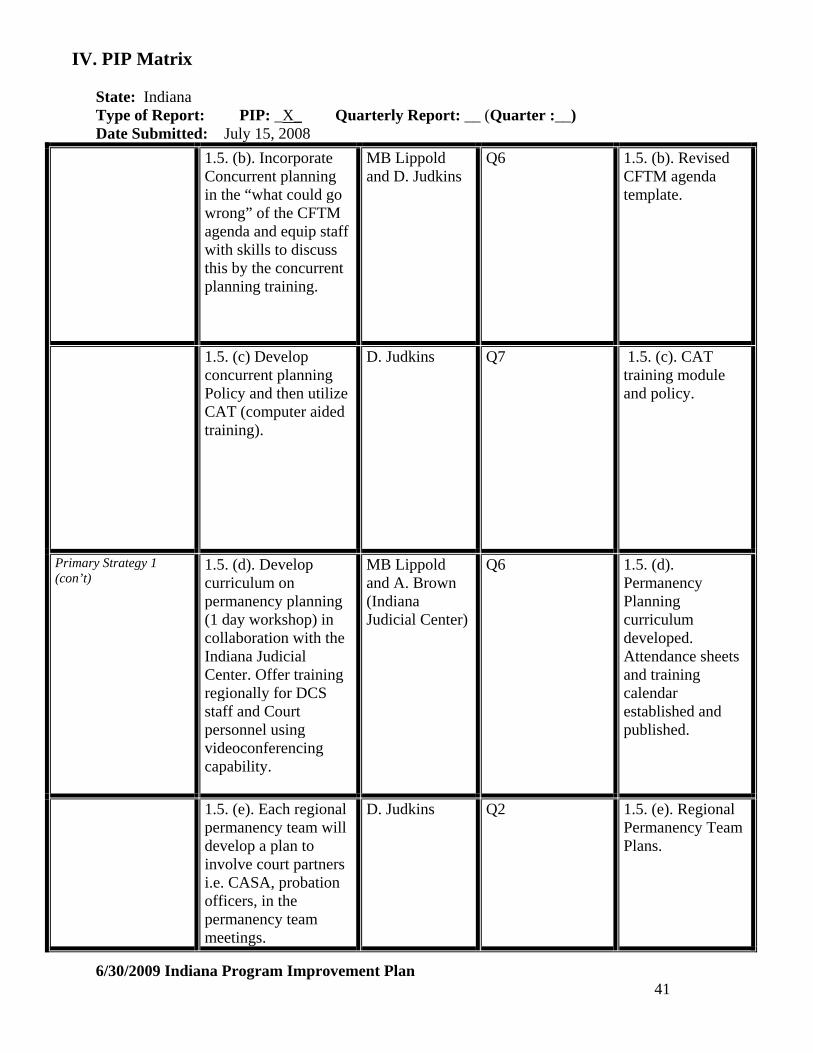
IV. PIP Matrix State: Indiana Type of Report: PIP: _X_ Quarterly Report: __ (Quarter :__)
Date Submitted: July 15, 2008
6/30/2009 Indiana Program Improvement Plan 41
1.5. (b). Incorporate Concurrent planning in the “what could go wrong” of the CFTM agenda and equip staff with skills to discuss this by the concurrent planning training.
MB Lippold and D. Judkins
Q6 1.5. (b). Revised CFTM agenda template.
1.5. (c) Develop concurrent planning Policy and then utilize CAT (computer aided training).
D. Judkins
Q7
1.5. (c). CAT training module and policy.
Primary Strategy 1 (con’t)
1.5. (d). Develop curriculum on permanency planning (1 day workshop) in collaboration with the Indiana Judicial Center. Offer training regionally for DCS staff and Court personnel using videoconferencing capability.
MB Lippold and A. Brown (Indiana Judicial Center)
Q6 1.5. (d). Permanency Planning curriculum developed. Attendance sheets and training calendar established and published.
1.5. (e). Each regional permanency team will develop a plan to involve court partners i.e. CASA, probation officers, in the permanency team meetings.
D. Judkins Q2 1.5. (e). Regional Permanency Team Plans.
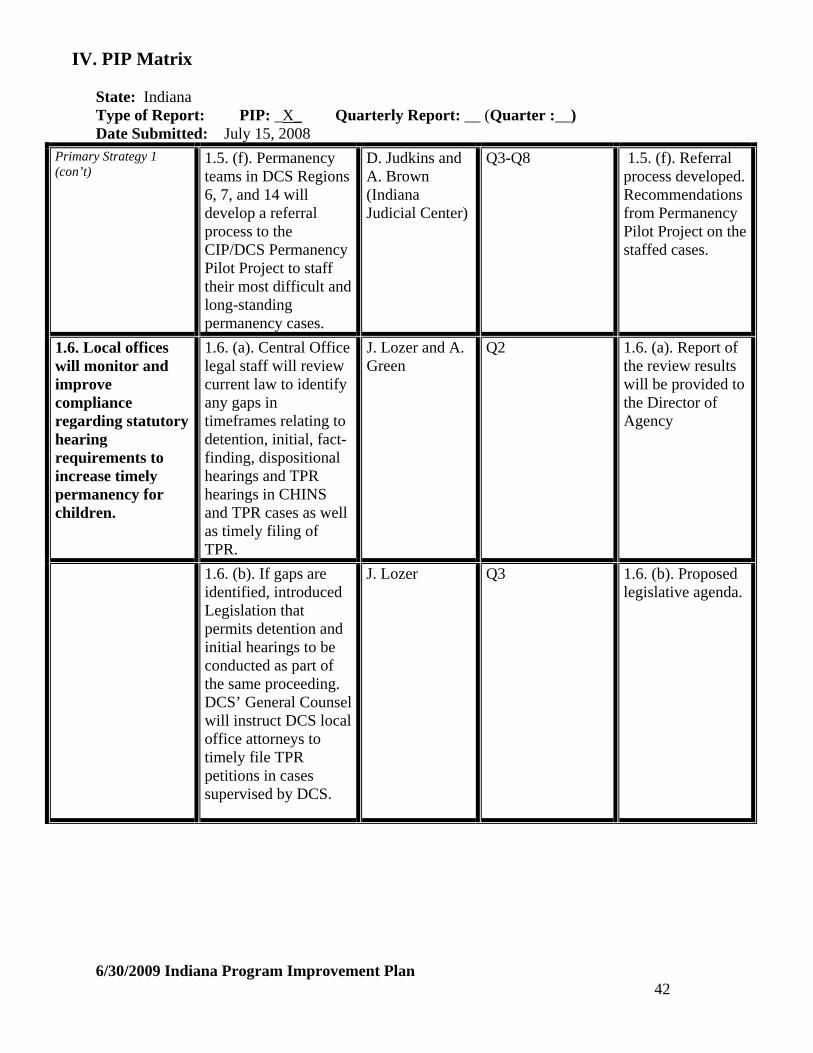
IV. PIP Matrix State: Indiana Type of Report: PIP: _X_ Quarterly Report: __ (Quarter :__)
Date Submitted: July 15, 2008
6/30/2009 Indiana Program Improvement Plan 42
Primary Strategy 1 (con’t)
1.5. (f). Permanency teams in DCS Regions 6, 7, and 14 will develop a referral process to the CIP/DCS Permanency Pilot Project to staff their most difficult and long-standing permanency cases.
D. Judkins and A. Brown (Indiana Judicial Center)
Q3-Q8 1.5. (f). Referral process developed. Recommendations from Permanency Pilot Project on the staffed cases.
1.6. Local offices will monitor and improve compliance regarding statutory hearing requirements to increase timely permanency for children.
1.6. (a). Central Office legal staff will review current law to identify any gaps in timeframes relating to detention, initial, fact-finding, dispositional hearings and TPR hearings in CHINS and TPR cases as well as timely filing of TPR.
J. Lozer and A. Green
Q2
1.6. (a). Report of the review results will be provided to the Director of Agency
1.6. (b). If gaps are identified, introduced Legislation that permits detention and initial hearings to be conducted as part of the same proceeding. DCS’ General Counsel will instruct DCS local office attorneys to timely file TPR petitions in cases supervised by DCS.
J. Lozer
Q3
1.6. (b). Proposed legislative agenda.
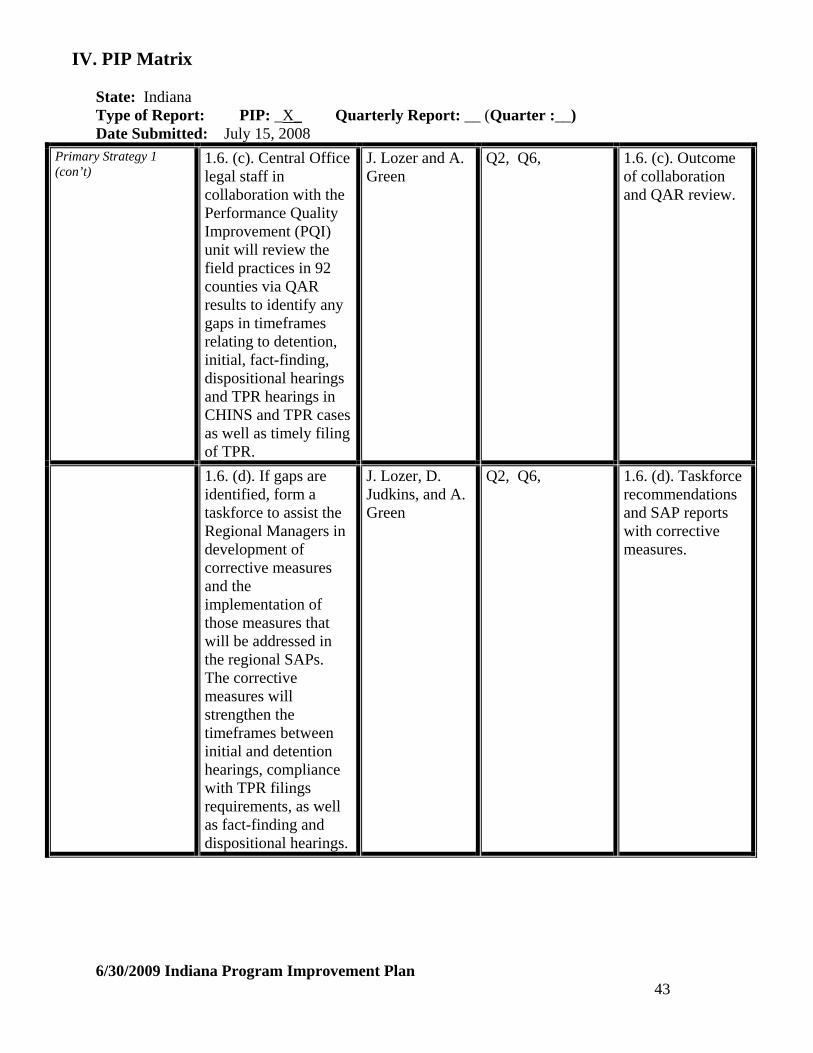
IV. PIP Matrix State: Indiana Type of Report: PIP: _X_ Quarterly Report: __ (Quarter :__)
Date Submitted: July 15, 2008
6/30/2009 Indiana Program Improvement Plan 43
Primary Strategy 1 (con’t)
1.6. (c). Central Office legal staff in collaboration with the Performance Quality Improvement (PQI) unit will review the field practices in 92 counties via QAR results to identify any gaps in timeframes relating to detention, initial, fact-finding, dispositional hearings and TPR hearings in CHINS and TPR cases as well as timely filing of TPR.
J. Lozer and A. Green
Q2, Q6, 1.6. (c). Outcome of collaboration and QAR review.
1.6. (d). If gaps are identified, form a taskforce to assist the Regional Managers in development of corrective measures and the implementation of those measures that will be addressed in the regional SAPs. The corrective measures will strengthen the timeframes between initial and detention hearings, compliance with TPR filings requirements, as well as fact-finding and dispositional hearings.
J. Lozer, D. Judkins, and A. Green
Q2, Q6, 1.6. (d). Taskforce recommendations and SAP reports with corrective measures.
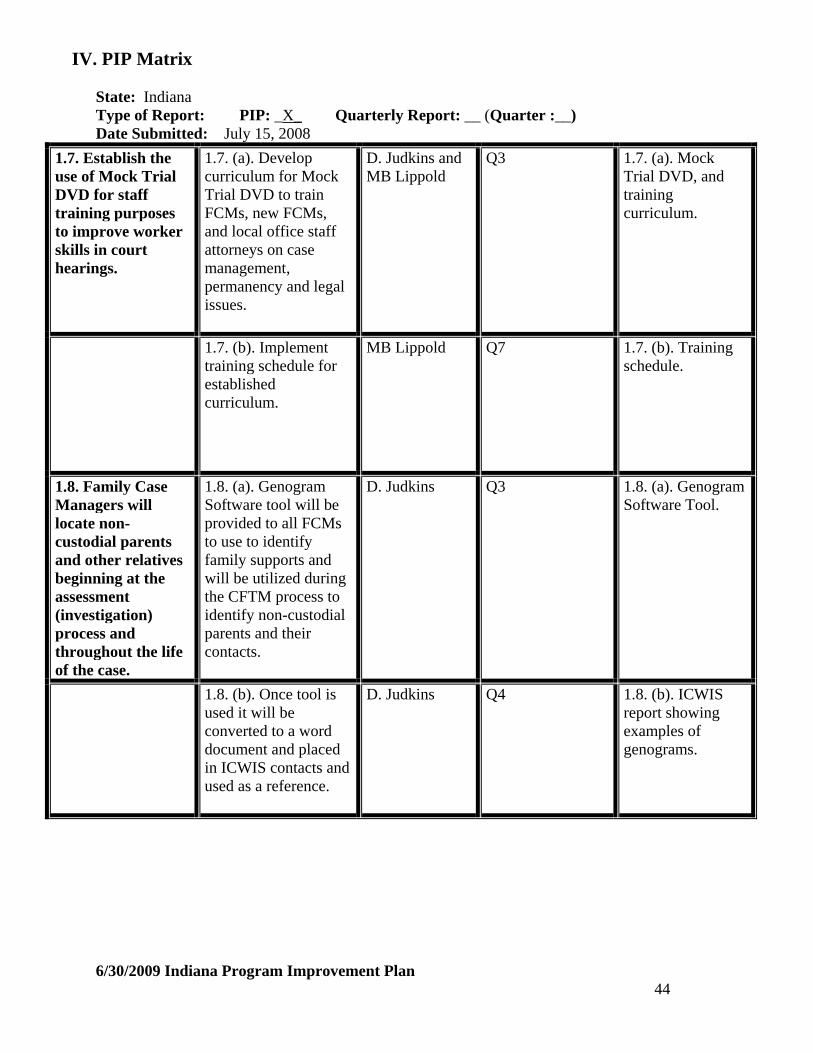
IV. PIP Matrix State: Indiana Type of Report: PIP: _X_ Quarterly Report: __ (Quarter :__)
Date Submitted: July 15, 2008
6/30/2009 Indiana Program Improvement Plan 44
1.7. Establish the use of Mock Trial DVD for staff training purposes to improve worker skills in court hearings.
1.7. (a). Develop curriculum for Mock Trial DVD to train FCMs, new FCMs, and local office staff attorneys on case management, permanency and legal issues.
D. Judkins and MB Lippold
Q3 1.7. (a). Mock Trial DVD, and training curriculum.
1.7. (b). Implement training schedule for established curriculum.
MB Lippold Q7 1.7. (b). Training schedule.
1.8. Family Case Managers will locate non-custodial parents and other relatives beginning at the assessment (investigation) process and throughout the life of the case.
1.8. (a). Genogram Software tool will be provided to all FCMs to use to identify family supports and will be utilized during the CFTM process to identify non-custodial parents and their contacts.
D. Judkins Q3 1.8. (a). Genogram Software Tool.
1.8. (b). Once tool is used it will be converted to a word document and placed in ICWIS contacts and used as a reference.
D. Judkins Q4 1.8. (b). ICWIS report showing examples of genograms.

IV. PIP Matrix State: Indiana Type of Report: PIP: _X_ Quarterly Report: __ (Quarter :__)
Date Submitted: July 15, 2008
6/30/2009 Indiana Program Improvement Plan 45
Primary Strategy 1 (con’t)
1.8. (c). FCMs will complete an ADI (Diligent Search) on every non-custodial parent during the assessment (investigation) phase, before a change to the permanency plan or when additional information about an absent parent is provided.
D. Judkins and A. Green
Q2 1.8. (c). ADI: Diligent Search Policy
1.8. (d). Include Diligent Search question in the QAR tool for continuous review of practice.
A. Green Q2 1.8. (d). Revised QAR Tool that includes Diligent Search question.
1.8. (e). Policy regarding placing children with non-custodial parent and other relatives when it is in child’s best interest will be reinforced via Director’s Note.
D. Judkins
Q3 1.8. (e). Director’s Note addressing practice expectation.
1.8. (f). DCS will track the diligent search efforts quarterly through QAR report.
D. Judkins Q4, Q6 1.8. (f). QAR results

IV. PIP Matrix State: Indiana Type of Report: PIP: _X_ Quarterly Report: __ (Quarter :__)
Date Submitted: July 15, 2008
6/30/2009 Indiana Program Improvement Plan 46
Primary Strategy 1 (con’t)
1.8. (g). DCS will identify additional counties to model the key principles of the Marion County’s federal grant initiative: Engaging Non-Resident Fathers and adapt it to the counties’ needs.
D. Judkins Q7 1.8. (g). Counties identified and implementation plan developed.
1.9. DCS will expand placement options to consider non-related adults when it is in the best interest of the child.
1.9. (a). Policy staff will research non-relative kin definitions from other states.
A. Green and D. Judkins
Q5 1.9. (a). Policy brief on kin definition
1.9. (b). Policy will collaboratively draft with Court Improvement Project (CIP) a new definition of non-relative kin.
A. Green and D. Judkins
Q5 1.9. (b). Approved definition of kin.
1.9. (c). Policy statement and computer assisted training (CAT) will be provided to field staff, i.e. FCMs, FCM Supervisors, Local Office Directors, and Executive Managers.
MB Lippold and A. Green
Q5 1.9. (c). Policy statement and CAT module and/or Admin letter.
1.9. (d). DCS will provide presentations to court staff on the new definition and expectations on non-relative kin.
D. Judkins and MB Lippold
Q5 1.9. (d). Presentation materials and sign-in sheets.

IV. PIP Matrix State: Indiana Type of Report: PIP: _X_ Quarterly Report: __ (Quarter :__)
Date Submitted: July 15, 2008
6/30/2009 Indiana Program Improvement Plan 47
Primary Strategy 1 (con’t)
1.9. (e). Add the newly defined kinship placement to ICWIS and the Practice Indicator under CHINS placements.
D. Judkins and A. Green
Q5 1.9. (e). Revised ICWIS and practice indicator for Increased Relative Care.
1.10. DCS will emphasize to all field staff the value of proximity and preserving essential connections to the child’s family, culture, religion and community.
1.10. (a). Quarterly Mandatory management meetings (QUAD) will have proximity and preserving connections as a recurring agenda item.
D. Judkins Q2
1.10. (a). Quad meeting notes.
1.10. (b). Information, decisions and/or suggestions generated about proximity and essential connections from the QUAD Meetings will be dispersed to staff through unit meetings.
D. Judkins Q2 1.10. (b). Distributed information
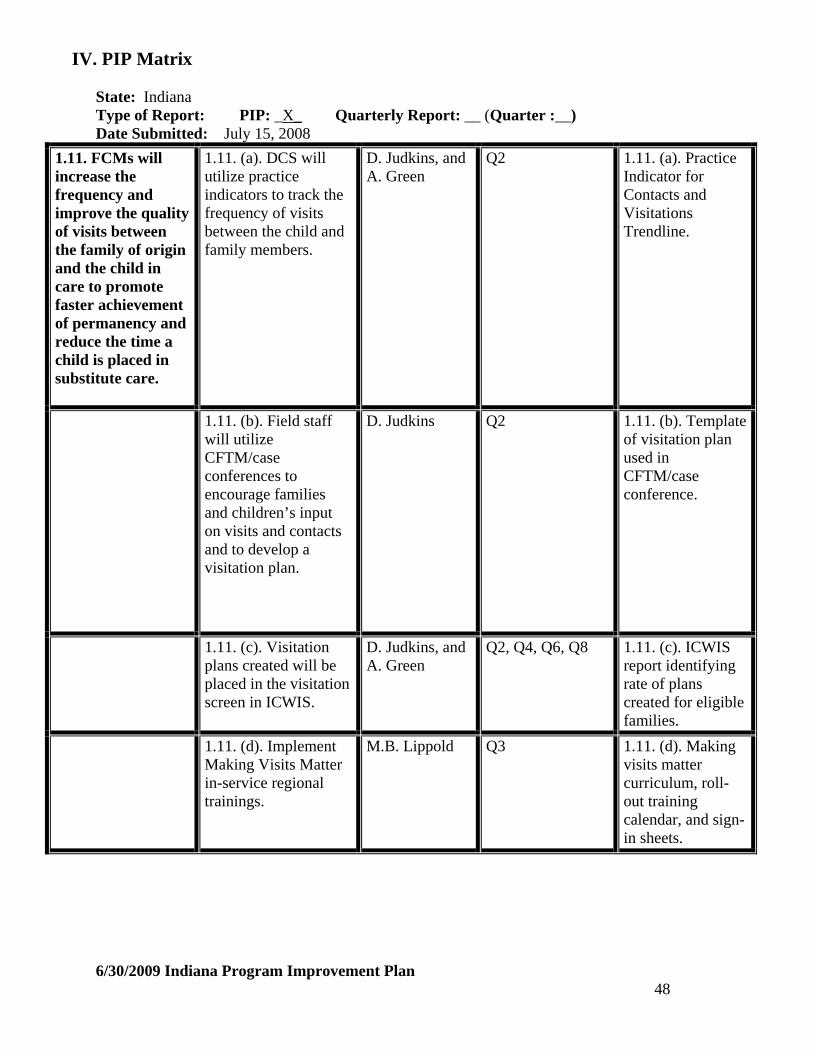
IV. PIP Matrix State: Indiana Type of Report: PIP: _X_ Quarterly Report: __ (Quarter :__)
Date Submitted: July 15, 2008
6/30/2009 Indiana Program Improvement Plan 48
1.11. FCMs will increase the frequency and improve the quality of visits between the family of origin and the child in care to promote faster achievement of permanency and reduce the time a child is placed in substitute care.
1.11. (a). DCS will utilize practice indicators to track the frequency of visits between the child and family members.
D. Judkins, and A. Green
Q2 1.11. (a). Practice Indicator for Contacts and Visitations Trendline.
1.11. (b). Field staff will utilize CFTM/case conferences to encourage families and children’s input on visits and contacts and to develop a visitation plan.
D. Judkins Q2 1.11. (b). Template of visitation plan used in CFTM/case conference.
1.11. (c). Visitation plans created will be placed in the visitation screen in ICWIS.
D. Judkins, and A. Green
Q2, Q4, Q6, Q8 1.11. (c). ICWIS report identifying rate of plans created for eligible families.
1.11. (d). Implement Making Visits Matter in-service regional trainings.
M.B. Lippold
Q3 1.11. (d). Making visits matter curriculum, roll-out training calendar, and sign-in sheets.

IV. PIP Matrix State: Indiana Type of Report: PIP: _X_ Quarterly Report: __ (Quarter :__)
Date Submitted: July 15, 2008
6/30/2009 Indiana Program Improvement Plan 49
Primary Strategy 1 (con’t)
1.11. (e). DCS will form a workgroup that will discuss the development of FCMs’ facilitation skills necessary to ensure visitations between the child and the parent as well as visitations between the child with participating relatives are progressive and productive.
D. Judkins Q5 1.11. (e). Outcome of workgroup and plan developed.
1.11. (f). The recommendations from this workgroup will be reviewed to determine policy development and practice guidance on case worker involvement in visitations.
A. Green Q6 1.11. (f). Policy developed.
1.12. DCS will ensure FCMs’ compliance with the case worker contacts policy regarding frequency and quality of visitation with parents and children.
1.12. (a). DCS’ office of data management will develop a monthly tracking report that will measure the frequency of case worker contacts with parents in regard to child out-of-home placements, IAs, and in-home CHINs.
D. Judkins and A. Green
Q1 1.12. (a). Current Case worker contacts policy and Monthly tracking report.

IV. PIP Matrix State: Indiana Type of Report: PIP: _X_ Quarterly Report: __ (Quarter :__)
Date Submitted: July 15, 2008
6/30/2009 Indiana Program Improvement Plan 50
1.12. (b). Regional Managers will monitor the monthly tracking report and address non-compliance issues in Strategic Action Plans.
D. Judkins Q1 1.12. (b). Regional Strategic action plans.
Primary Strategy 1 (con’t)
1.12. (c). The Family Functional Assessment (FFA) will be used as a tool guide for FCMs in preparation for quality visits in all case types (in-home CHINS, IAs, and out home placements.)
D. Judkins Q2 1.12. (c). Copy of Family Functioning Assessment
1.12. (d). Provide Director’s note that will require FCMs to use the FFA in preparation for quality visits.
D. Judkins Q2 1.12. (d). Director’s Note
1.12. (e). FFA will be an agenda item for discussion at Regional Managers’ Meeting.
D. Judkins Q2 1.12. (e). Regional Managers Meeting Agenda and notes.
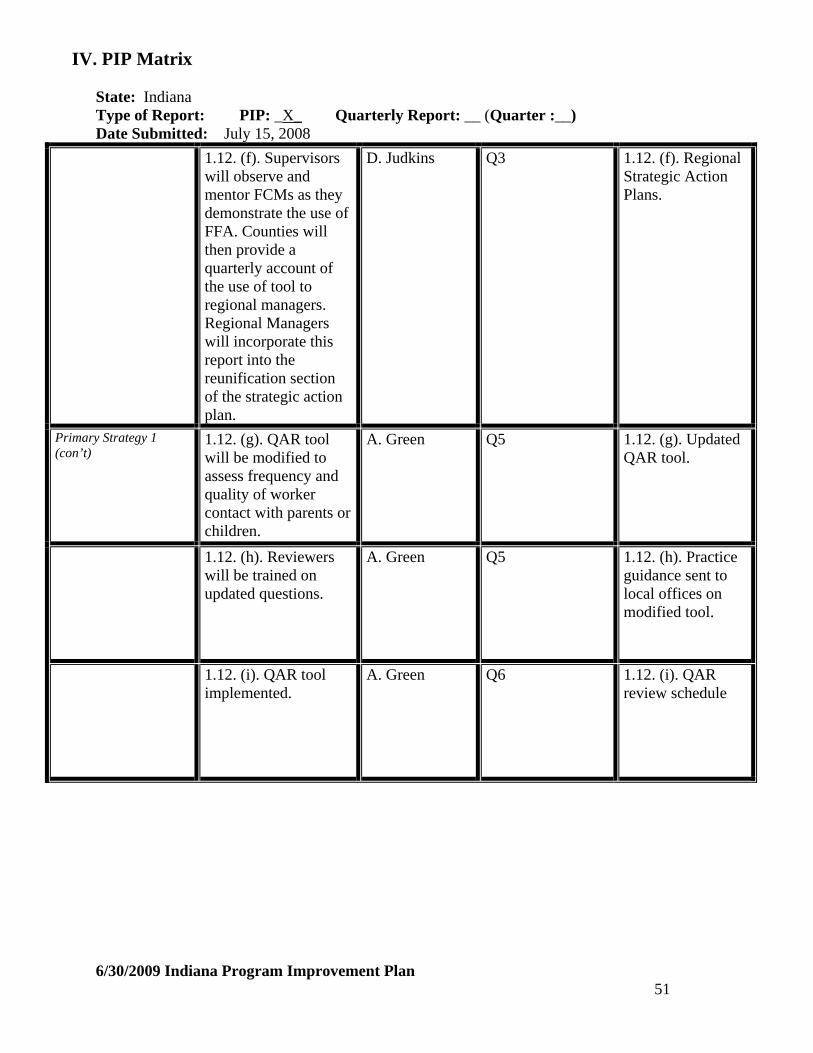
IV. PIP Matrix State: Indiana Type of Report: PIP: _X_ Quarterly Report: __ (Quarter :__)
Date Submitted: July 15, 2008
6/30/2009 Indiana Program Improvement Plan 51
1.12. (f). Supervisors will observe and mentor FCMs as they demonstrate the use of FFA. Counties will then provide a quarterly account of the use of tool to regional managers. Regional Managers will incorporate this report into the reunification section of the strategic action plan.
D. Judkins Q3 1.12. (f). Regional Strategic Action Plans.
Primary Strategy 1 (con’t)
1.12. (g). QAR tool will be modified to assess frequency and quality of worker contact with parents or children.
A. Green Q5 1.12. (g). Updated QAR tool.
1.12. (h). Reviewers will be trained on updated questions.
A. Green Q5 1.12. (h). Practice guidance sent to local offices on modified tool.
1.12. (i). QAR tool implemented.
A. Green Q6 1.12. (i). QAR review schedule

IV. PIP Matrix State: Indiana Type of Report: PIP: _X_ Quarterly Report: __ (Quarter :__)
Date Submitted: July 15, 2008
6/30/2009 Indiana Program Improvement Plan 52
1.13. All CHINS Cases will be monitored to ensure that IL services are appropriately provided to eligible youth at the earliest possible age, and that all children are involved in the development of their IL plan.
1.13. (a). FCMs will facilitate child-centered (or child-specific) CFTM to assess IL needs and is to be held at least 6 months prior to the child’s 16th birthday. During which, the IL plan will be developed with the child and updated for every permanency hearing thereafter. This process will be reflected in policy.
D. Judkins and L. Rich and A. Green
Q4 1.13. (a). Template of IL Plan to be utilized. Policy and procedural guidance.
Primary Strategy 1 (con’t)
1.13. (b). IL consultants will develop a protocol and monitoring tool to assess the performance of service providers, their activities and services requirements.
L. Rich
Q4 1.13. (b). Protocol and Monitoring tool
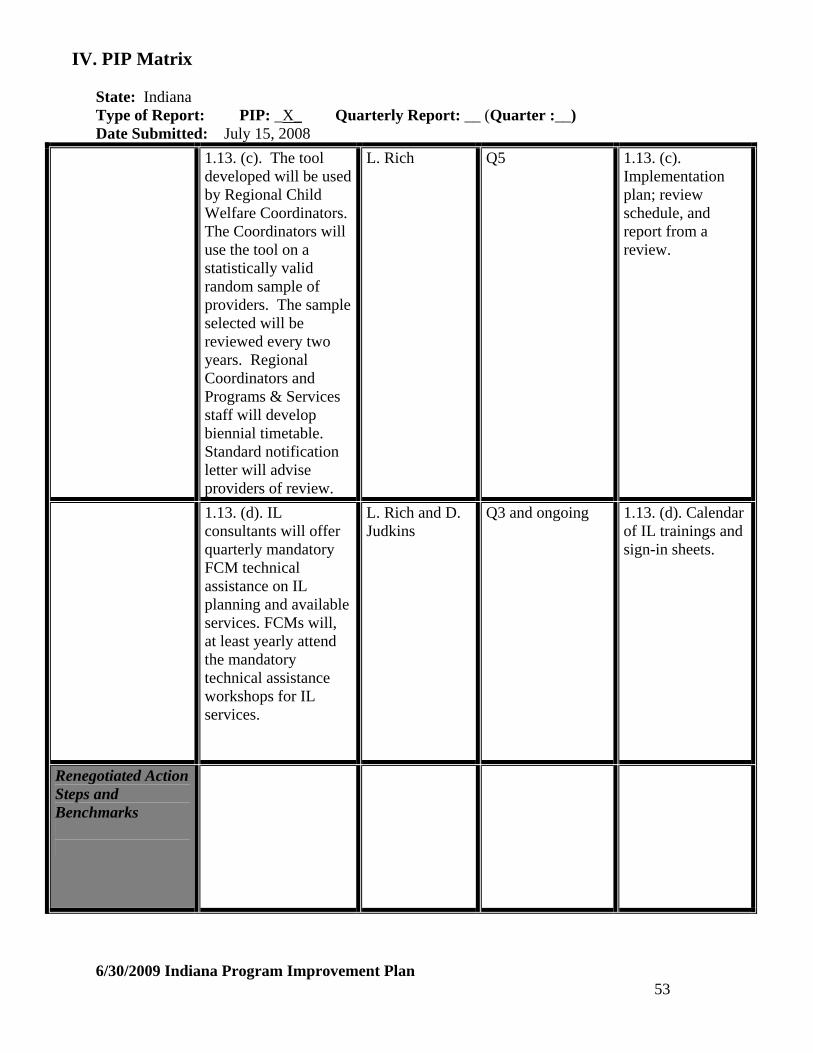
IV. PIP Matrix State: Indiana Type of Report: PIP: _X_ Quarterly Report: __ (Quarter :__)
Date Submitted: July 15, 2008
6/30/2009 Indiana Program Improvement Plan 53
1.13. (c). The tool developed will be used by Regional Child Welfare Coordinators. The Coordinators will use the tool on a statistically valid random sample of providers. The sample selected will be reviewed every two years. Regional Coordinators and Programs & Services staff will develop biennial timetable. Standard notification letter will advise providers of review.
L. Rich Q5 1.13. (c). Implementation plan; review schedule, and report from a review.
1.13. (d). IL consultants will offer quarterly mandatory FCM technical assistance on IL planning and available services. FCMs will, at least yearly attend the mandatory technical assistance workshops for IL services.
L. Rich and D. Judkins
Q3 and ongoing 1.13. (d). Calendar of IL trainings and sign-in sheets.
Renegotiated Action Steps and Benchmarks
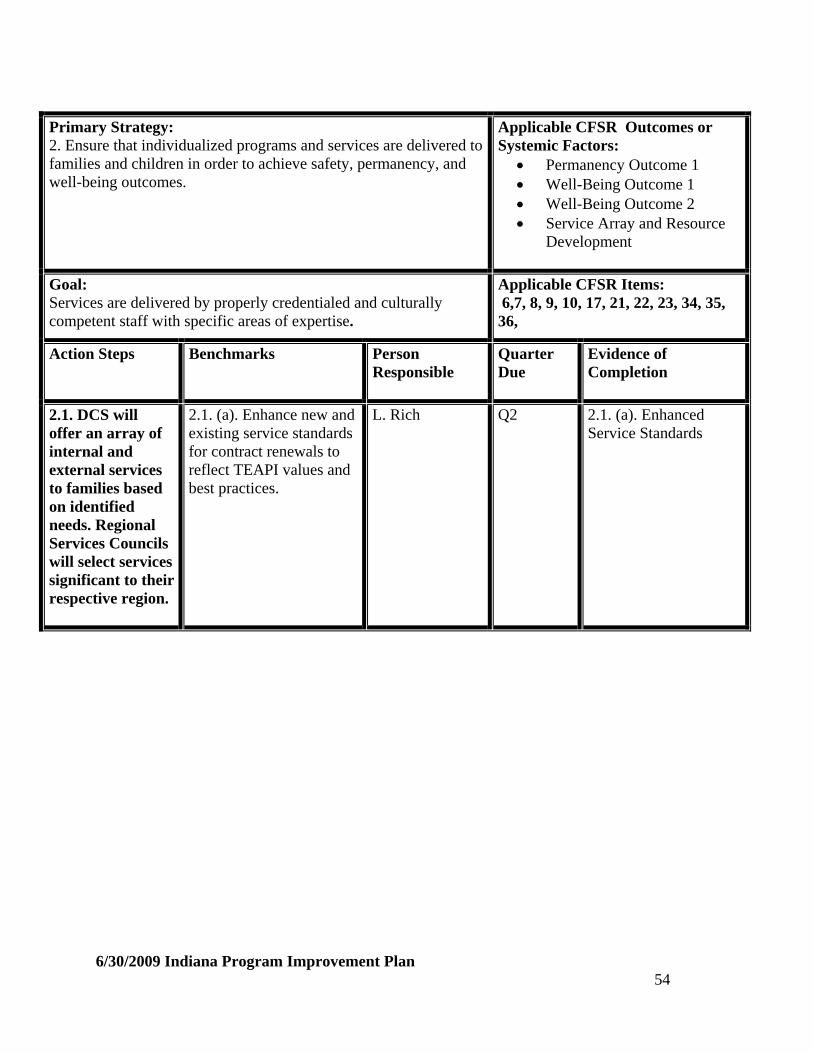
Primary Strategy: 2. Ensure that individualized programs and services are delivered to families and children in order to achieve safety, permanency, and well-being outcomes.
Applicable CFSR Outcomes or Systemic Factors:
Permanency Outcome 1 Well-Being Outcome 1 Well-Being Outcome 2 Service Array and Resource
Development
Goal: Services are delivered by properly credentialed and culturally competent staff with specific areas of expertise.
Applicable CFSR Items: 6,7, 8, 9, 10, 17, 21, 22, 23, 34, 35, 36,
Action Steps
Benchmarks
Person Responsible
Quarter Due
Evidence of Completion
2.1. DCS will offer an array of internal and external services to families based on identified needs. Regional Services Councils will select services significant to their respective region.
2.1. (a). Enhance new and existing service standards for contract renewals to reflect TEAPI values and best practices.
L. Rich
Q2
2.1. (a). Enhanced Service Standards
6/30/2009 Indiana Program Improvement Plan 54

Primary Strategy 2 (con’t)
2.1. (b). Service specific review tools will be developed and implemented by Regional Coordinators and Programs and Services staff to ensure services provided are in accordance with contract requirements and reflective of TEAPI values. The tool developed will be used by Regional Child Welfare Coordinators. The Coordinators will use the tool on a statistically valid random sample of providers. Sample selected will be reviewed every two years. Regional Coordinators and Programs & Services staff will develop biennial timetable. Standard notification letter will advise providers of reviews.
L. Rich
Q3, Q5
2.1. (b). Service specific review tools, review timetable, review notification letter, Quarter 3. Reviews implemented Quarter 5
2.1. (c). DCS service standards will require that providers train their staff on substance abuse and domestic violence as part of the contract requirements.
L. Rich Q3 2.1. (c). Contract Development and Management Standards
6/30/2009 Indiana Program Improvement Plan 55
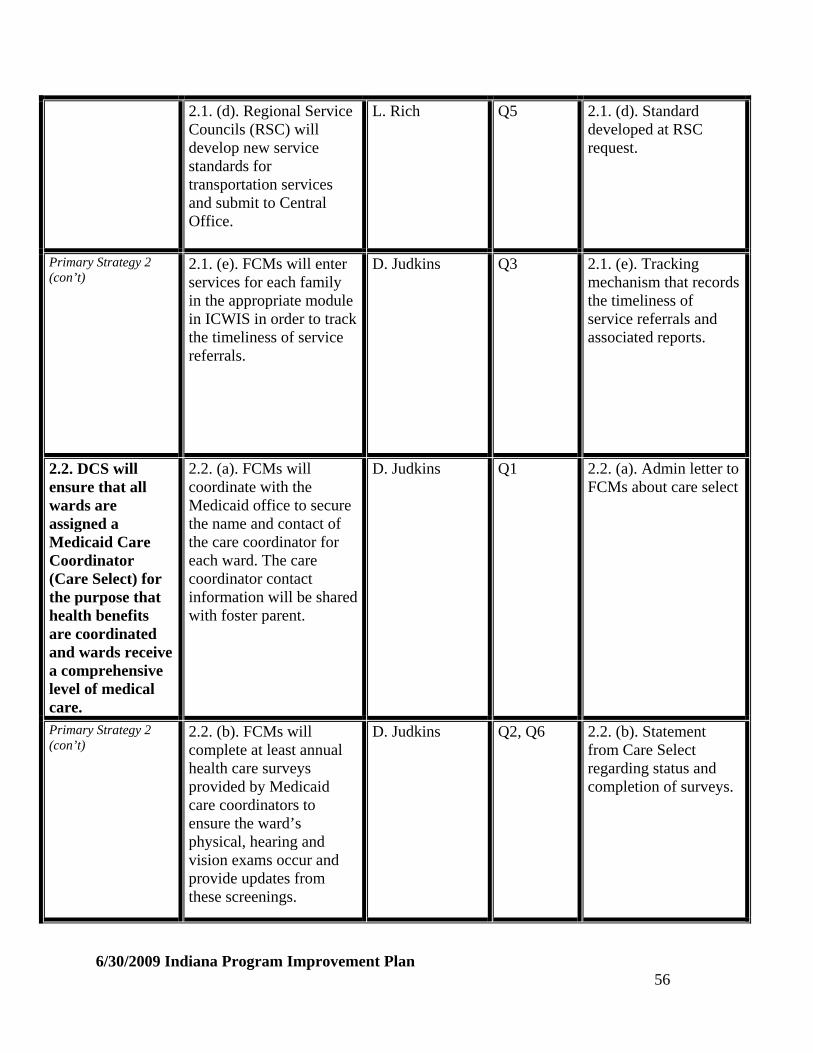
2.1. (d). Regional Service Councils (RSC) will develop new service standards for transportation services and submit to Central Office.
L. Rich
Q5
2.1. (d). Standard developed at RSC request.
Primary Strategy 2 (con’t)
2.1. (e). FCMs will enter services for each family in the appropriate module in ICWIS in order to track the timeliness of service referrals.
D. Judkins
Q3
2.1. (e). Tracking mechanism that records the timeliness of service referrals and associated reports.
2.2. DCS will ensure that all wards are assigned a Medicaid Care Coordinator (Care Select) for the purpose that health benefits are coordinated and wards receive a comprehensive level of medical care.
2.2. (a). FCMs will coordinate with the Medicaid office to secure the name and contact of the care coordinator for each ward. The care coordinator contact information will be shared with foster parent.
D. Judkins Q1 2.2. (a). Admin letter to FCMs about care select
Primary Strategy 2 (con’t)
2.2. (b). FCMs will complete at least annual health care surveys provided by Medicaid care coordinators to ensure the ward’s physical, hearing and vision exams occur and provide updates from these screenings.
D. Judkins Q2, Q6 2.2. (b). Statement from Care Select regarding status and completion of surveys.
6/30/2009 Indiana Program Improvement Plan 56
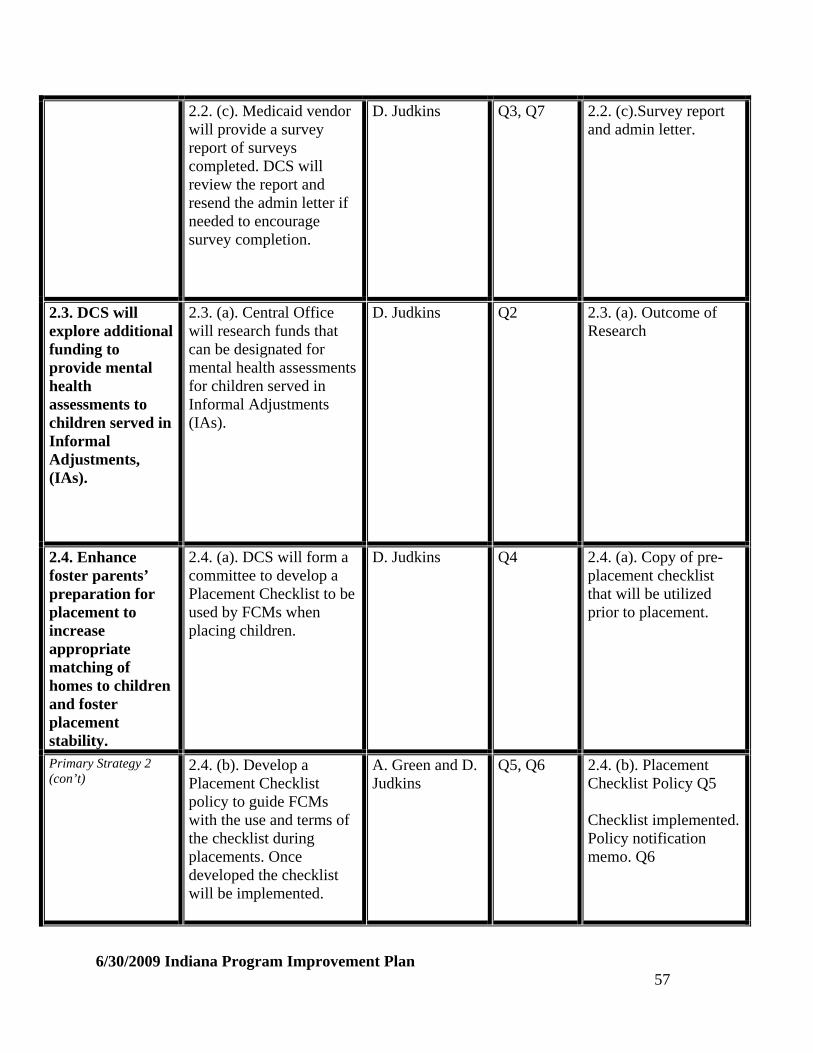
2.2. (c). Medicaid vendor will provide a survey report of surveys completed. DCS will review the report and resend the admin letter if needed to encourage survey completion.
D. Judkins Q3, Q7 2.2. (c).Survey report and admin letter.
2.3. DCS will explore additional funding to provide mental health assessments to children served in Informal Adjustments, (IAs).
2.3. (a). Central Office will research funds that can be designated for mental health assessments for children served in Informal Adjustments (IAs).
D. Judkins
Q2
2.3. (a). Outcome of Research
2.4. Enhance foster parents’ preparation for placement to increase appropriate matching of homes to children and foster placement stability.
2.4. (a). DCS will form a committee to develop a Placement Checklist to be used by FCMs when placing children.
D. Judkins
Q4
2.4. (a). Copy of pre-placement checklist that will be utilized prior to placement.
Primary Strategy 2 (con’t)
2.4. (b). Develop a Placement Checklist policy to guide FCMs with the use and terms of the checklist during placements. Once developed the checklist will be implemented.
A. Green and D. Judkins
Q5, Q6 2.4. (b). Placement Checklist Policy Q5 Checklist implemented. Policy notification memo. Q6
6/30/2009 Indiana Program Improvement Plan 57

2.4. (c). DCS Programs and Services Department will have an orientation with Regional Managers, Local Office Directors, FCM Supervisors, FCMs and foster care licensing staff, on the use of the CASEY Family Assessment tool.
L. Rich
Q2
2.4. (c). Outcome of the 2-day training. Sign in sheets. Training materials.
2.4. (d). Develop a plan to pilot the use of the Casey family assessment to determine realistic expectations about foster parenting, and appropriate matching between child and family. Identify pilot counties that already have foster care specialists to use the assessment tool.
L. Rich
Q3
2.4. (d). Formalized plan for pilot with counties identified to implement the CASEY family assessment tool.
2.4. (e). Develop a plan to train and then implement the use of the CASEY Family Assessment tool statewide by identifying and selecting foster care specialists for each county/region.
L. Rich Q4 2.4. (e). Statewide roll-out training and implementation plan. List of foster care specialists for each county/region.
6/30/2009 Indiana Program Improvement Plan 58

Primary Strategy 2 (con’t)
2.4. (f). DCS will update placement matching functionality in ICWIS system to aid staff during placement decisions.
A. Green Q3, Q6 2.4. (f). ICWIS Placement matching updates.
2.4. (g). ICWIS Coordinators will conduct task training to all field staff (FCMs, FCM supervisors, Local office Directors, and Regional Managers) on how to use the new tool during regional in-service trainings.
A. Green Q4 2.4. (g). Training schedule/roll-out calendar. Sign-in sheets
2.5. Reduce factors that contribute to foster parent attrition during the licensing process.
2.5. (a). Develop a committee to review licensing issues to include evaluating the paperwork associated with the licensing process as well as timeliness standards for home studies and licensure activities.
L. Rich
Q3
2.5. (a). Committee member list and meeting dates. Outcome documentation from committee.
2.5. (b). Develop a position and then appoint regional licensing specialists to enhance agency responsiveness and timeliness to the needs of prospective foster parents during the licensure process.
L. Rich and J. Lozer
Q5
2.5. (b). List of Regional Licensing Specialists and their job duties.
6/30/2009 Indiana Program Improvement Plan 59
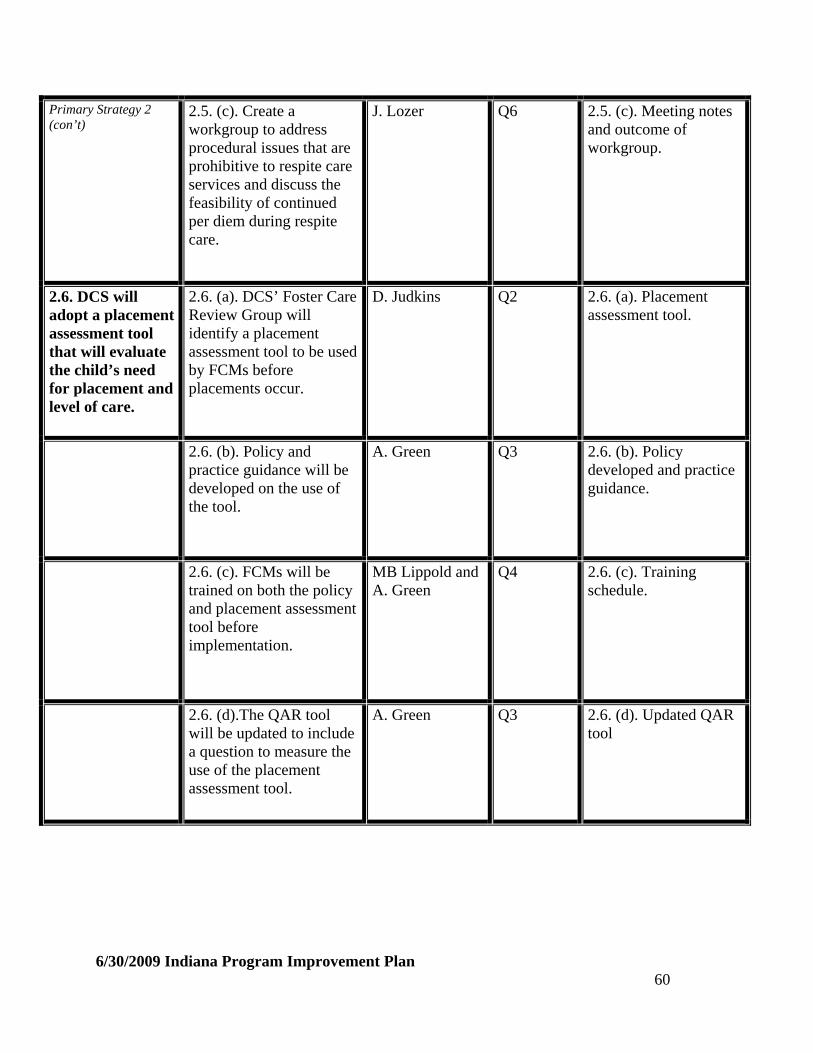
Primary Strategy 2 (con’t)
2.5. (c). Create a workgroup to address procedural issues that are prohibitive to respite care services and discuss the feasibility of continued per diem during respite care.
J. Lozer Q6 2.5. (c). Meeting notes and outcome of workgroup.
2.6. DCS will adopt a placement assessment tool that will evaluate the child’s need for placement and level of care.
2.6. (a). DCS’ Foster Care Review Group will identify a placement assessment tool to be used by FCMs before placements occur.
D. Judkins Q2 2.6. (a). Placement assessment tool.
2.6. (b). Policy and practice guidance will be developed on the use of the tool.
A. Green Q3 2.6. (b). Policy developed and practice guidance.
2.6. (c). FCMs will be trained on both the policy and placement assessment tool before implementation.
MB Lippold and A. Green
Q4 2.6. (c). Training schedule.
2.6. (d).The QAR tool will be updated to include a question to measure the use of the placement assessment tool.
A. Green Q3 2.6. (d). Updated QAR tool
6/30/2009 Indiana Program Improvement Plan 60

Primary Strategy 2 (con’t)
2.6. (e). Regional Managers will utilize data from the QAR report to address concerns or progress related to the new tool in the Region’s Strategic Action Plans.
D. Judkins Q8 2.6. (e). QAR report and SAPs
2.7. DCS will create foster care specialization units statewide to focus efforts on recruitment, placement stability, foster care in-service trainings, respite care coordination, and after hour supports.
2.7. (a). DCS’ foster care review group will develop a statewide strategy on how to implement specialization units throughout the state. The strategy will include the job description of the foster care specialist, service and support expectations to be rendered to foster families, and plan to develop the specialization units.
D. Judkins Q4 2.7. (a). Strategy Developed and Implementation plan
2.7. (b). Develop job description for foster care specialist.
D. Judkins Q4 2.7. (b). Foster Care specialist job
2.8. DCS will develop a list of mental health providers and dentists who accept Medicaid and provide information to FCMs and foster parents.
2.8. (a). Programs and Services will disseminate the list of providers and dentists who accept Medicaid to FCMs via email. The list will be updated and sent out annually. FCMs will be encouraged to share updated list with foster parents during visits.
L. Rich Q3 and Q7 2.8. (a). List of providers and distribution list.
6/30/2009 Indiana Program Improvement Plan 61

Primary Strategy 2 (con’t)
2.8. (b). Programs and Services will provide a current providers list to new foster parents during FAKT training.
L. Rich Q3 2.8. (b). Provider list
6/30/2009 Indiana Program Improvement Plan 62

Primary Strategy: 3. Engage multiple partners to protect children in their community through cooperation and communication.
Applicable CFSR Outcomes or Systemic Factors:
Well-Being Outcome 1 Well-Being Outcome 2 Well-Being Outcome 3 Case Review System Permanency 1 Outcome Service Array
Goal: Increase the inclusion of community partners in the assessment and delivery of services for the protection of children.
Applicable CFSR Items: 17, 21, 22, 23, 27, 28, 35, 36
Action Steps
Benchmarks
Person Responsible
Quarter Due
Evidence of Completion
3.1. DCS will collaborate with community partners to develop domestic violence guidelines.
3.1. (a). DCS Domestic Violence workgroup will identify the community providers, who offer domestic violence services, to develop a partnership.
D. Judkins
Q1
3.1. (a). Workgroup membership. Partnership membership.
3.1. (b). The DCS DV workgroup will develop recommendations from the collaboration to develop policy for field staff to assess domestic violence more effectively.
D. Judkins and A. Green
Q2
3.1 (b). Recommendation from workgroup and written approved policy.
6/30/2009 Indiana Program Improvement Plan 63
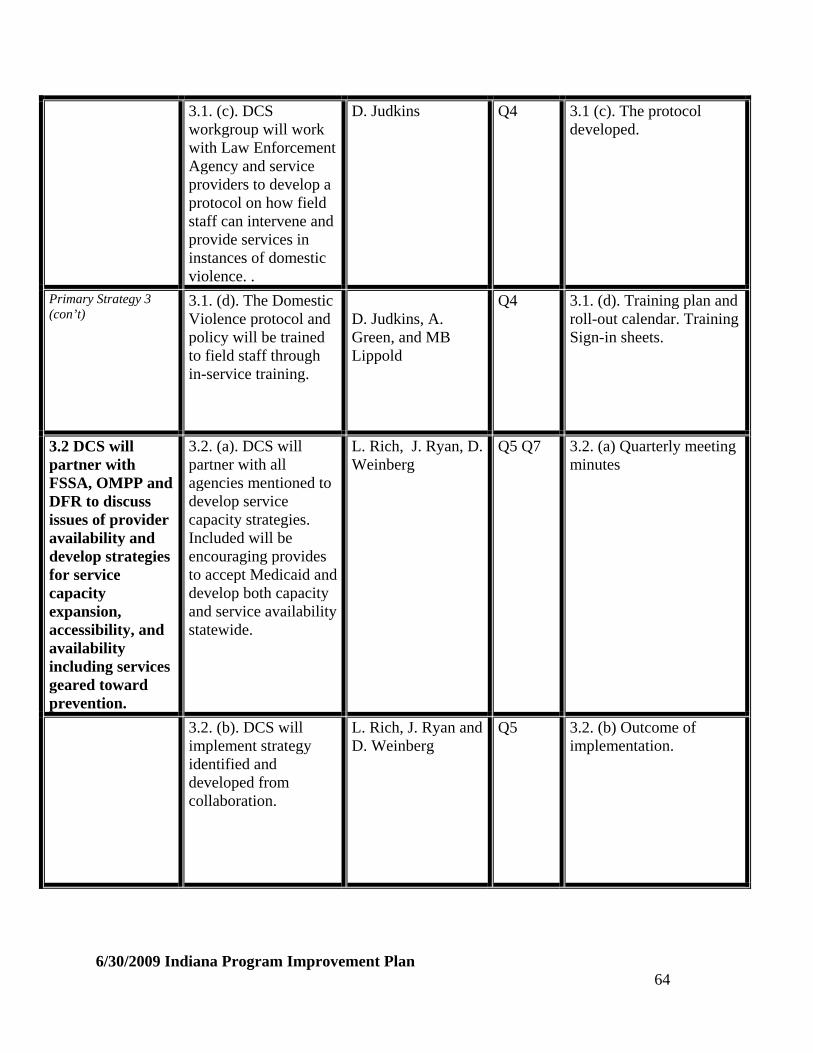
3.1. (c). DCS workgroup will work with Law Enforcement Agency and service providers to develop a protocol on how field staff can intervene and provide services in instances of domestic violence. .
D. Judkins
Q4
3.1 (c). The protocol developed.
Primary Strategy 3 (con’t)
3.1. (d). The Domestic Violence protocol and policy will be trained to field staff through in-service training.
D. Judkins, A. Green, and MB Lippold
Q4 3.1. (d). Training plan and roll-out calendar. Training Sign-in sheets.
3.2 DCS will partner with FSSA, OMPP and DFR to discuss issues of provider availability and develop strategies for service capacity expansion, accessibility, and availability including services geared toward prevention.
3.2. (a). DCS will partner with all agencies mentioned to develop service capacity strategies. Included will be encouraging provides to accept Medicaid and develop both capacity and service availability statewide.
L. Rich, J. Ryan, D. Weinberg
Q5 Q7
3.2. (a) Quarterly meeting minutes
3.2. (b). DCS will implement strategy identified and developed from collaboration.
L. Rich, J. Ryan and D. Weinberg
Q5 3.2. (b) Outcome of implementation.
6/30/2009 Indiana Program Improvement Plan 64

3.2. (c). DCS will partner with FSSA, OMPP and DFR to ensure that dental health providers who accept Medicaid have both the capacity and availability to serve wards throughout the state.
L. Rich and J. Ryan. Q5, Q7 3.2. (c). List of dental health providers. Q5 for baseline Q7 Increase of providers over baseline
3.3 DCS will work with community partners to emphasis the importance of the involvement of non-custodial parents, absent parents, and other significant relatives.
3.3. (a). Develop a taskforce of those involved with Fatherhood initiatives, LEA, CASA, Juvenile Judges and CIP to formulate strategies to increase non-custodial and absent parent involvement.
D. Judkins Q4 3.3. (a). Recommendations developed from the taskforce.
3.3 (b). Recommendations from the taskforce will be considered for policy and procedural development.
D. Judkins and A. Green
Q4
3.3. (b). Policy and procedural guidance.
6/30/2009 Indiana Program Improvement Plan 65

3.3. (c). DCS will offer Computer Assisted Training to DCS staff on new policy. The training will be placed on DCS Intranet and coordinated with the Judicial Center to offer the training to external legal partners.
MB Lippold, A. Green, and A. Brown (Indiana Judicial Center)
Q4, Q6, Q8
3.3. (c). Roll-out training calendar and sign-in sheets. Q4 Percentage of DCS and Courts staff/external partners trained. Q6 and Q8
3.4 DCS will collaborate with CIP to improve the process of reaching permanency outcomes.
3.4. (a). Develop a plan to implement the Permanency Project Pilot Court/DCS initiative to improve the permanency outcome.
D. Judkins and J. Lozer
Q1
3.4. (a). Implementation plan
3.4. (b). Ensure the three counties selected will continue collaboration between the Local office directors and Juvenile Judges.
D. Judkins and J. Lozer
Q2
3.4. (b). Meeting minutes
3.4. (c). Develop review process for cases selected.
D. Judkins and J. Lozer
Q3
3.4. (c). Formalized process in which the cases were selected.
3.4 (d). Generate checklist for cases reviewed in order to move cases to permanency.
D. Judkins and J. Lozer
Q3
3.4 (d). Checklist
6/30/2009 Indiana Program Improvement Plan 66
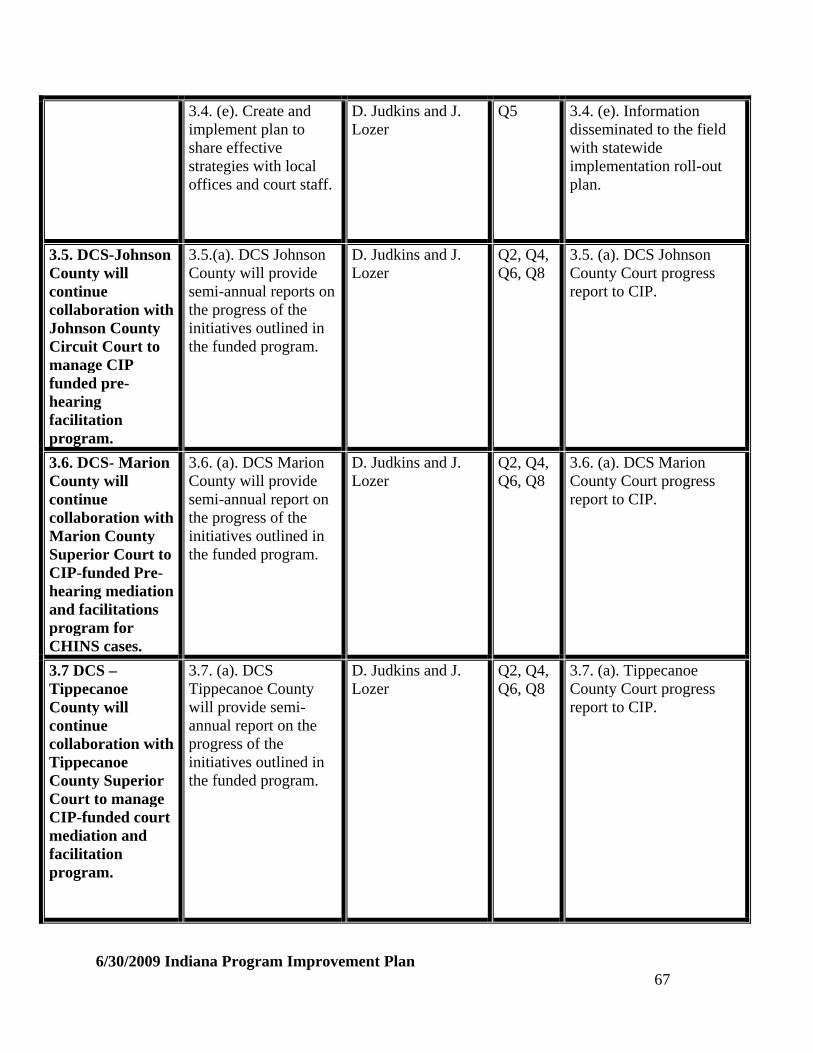
3.4. (e). Create and implement plan to share effective strategies with local offices and court staff.
D. Judkins and J. Lozer
Q5 3.4. (e). Information disseminated to the field with statewide implementation roll-out plan.
3.5. DCS-Johnson County will continue collaboration with Johnson County Circuit Court to manage CIP funded pre-hearing facilitation program.
3.5.(a). DCS Johnson County will provide semi-annual reports on the progress of the initiatives outlined in the funded program.
D. Judkins and J. Lozer
Q2, Q4, Q6, Q8
3.5. (a). DCS Johnson County Court progress report to CIP.
3.6. DCS- Marion County will continue collaboration with Marion County Superior Court to CIP-funded Pre-hearing mediation and facilitations program for CHINS cases.
3.6. (a). DCS Marion County will provide semi-annual report on the progress of the initiatives outlined in the funded program.
D. Judkins and J. Lozer
Q2, Q4, Q6, Q8
3.6. (a). DCS Marion County Court progress report to CIP.
3.7 DCS – Tippecanoe County will continue collaboration with Tippecanoe County Superior Court to manage CIP-funded court mediation and facilitation program.
3.7. (a). DCS Tippecanoe County will provide semi-annual report on the progress of the initiatives outlined in the funded program.
D. Judkins and J. Lozer
Q2, Q4, Q6, Q8
3.7. (a). Tippecanoe County Court progress report to CIP.
6/30/2009 Indiana Program Improvement Plan 67
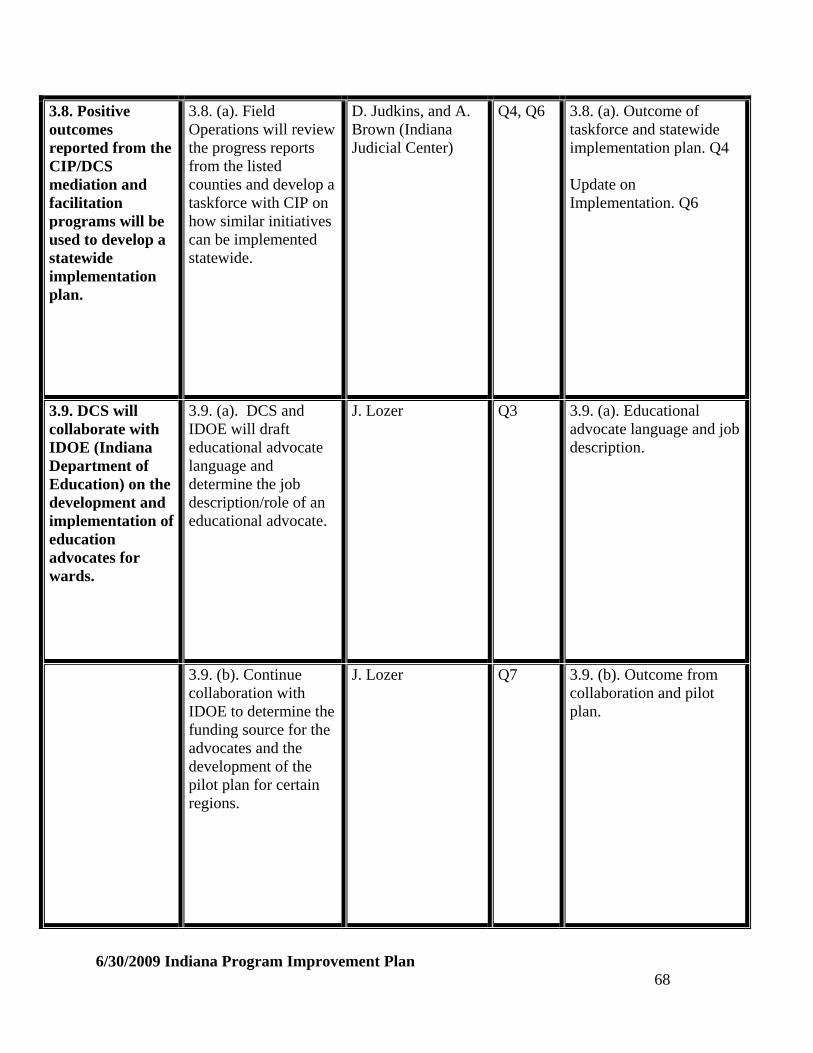
3.8. Positive outcomes reported from the CIP/DCS mediation and facilitation programs will be used to develop a statewide implementation plan.
3.8. (a). Field Operations will review the progress reports from the listed counties and develop a taskforce with CIP on how similar initiatives can be implemented statewide.
D. Judkins, and A. Brown (Indiana Judicial Center)
Q4, Q6 3.8. (a). Outcome of taskforce and statewide implementation plan. Q4 Update on Implementation. Q6
3.9. DCS will collaborate with IDOE (Indiana Department of Education) on the development and implementation of education advocates for wards.
3.9. (a). DCS and IDOE will draft educational advocate language and determine the job description/role of an educational advocate.
J. Lozer Q3 3.9. (a). Educational advocate language and job description.
3.9. (b). Continue collaboration with IDOE to determine the funding source for the advocates and the development of the pilot plan for certain regions.
J. Lozer Q7 3.9. (b). Outcome from collaboration and pilot plan.
6/30/2009 Indiana Program Improvement Plan 68
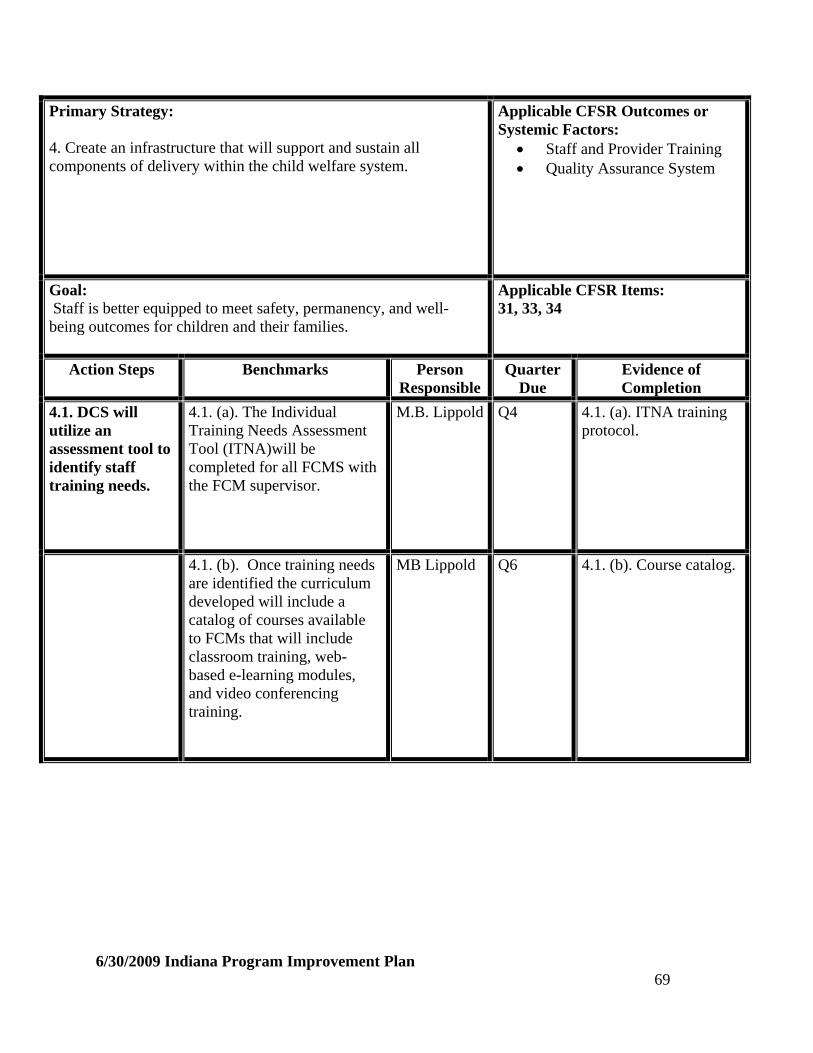
Primary Strategy: 4. Create an infrastructure that will support and sustain all components of delivery within the child welfare system.
Applicable CFSR Outcomes or Systemic Factors:
Staff and Provider Training Quality Assurance System
Goal: Staff is better equipped to meet safety, permanency, and well-being outcomes for children and their families.
Applicable CFSR Items: 31, 33, 34
Action Steps
Benchmarks
Person Responsible
Quarter Due
Evidence of Completion
4.1. DCS will utilize an assessment tool to identify staff training needs.
4.1. (a). The Individual Training Needs Assessment Tool (ITNA)will be completed for all FCMS with the FCM supervisor.
M.B. Lippold
Q4
4.1. (a). ITNA training protocol.
4.1. (b). Once training needs are identified the curriculum developed will include a catalog of courses available to FCMs that will include classroom training, web-based e-learning modules, and video conferencing training.
MB Lippold
Q6
4.1. (b). Course catalog.
6/30/2009 Indiana Program Improvement Plan 69

Primary Strategy 4 (con’t)
4.1. (c). A schedule for needs-based training courses will be published and distributed to FCMs to review.
MB Lippold Q6 4.1. (c). Training schedule.
4.1. (d). FCMs will attend classes and complete all requirements including evaluation summary.
MB Lippold Q8 4.1. (d). Published evaluation data based on satisfaction surveys completed and reviewed for training effectiveness.
4.1. (e). Form a committee to identify and secure additional funding for cost-effective trainings held outside the partnership for Child Welfare Training and Education, and establish a protocol on how FCMs can access these funds.
M.B. Lippold
Q2
4.1. (e). Protocol developed and approved by the Director.
4.1 (f). Develop a policy to determine the required in-service training hours for FCMs each year.
MB Lippold and A. Green
Q3
4.1 (f). Policy
4.1. (g). Development of a comprehensive training record information system to track all trainings attended and completed by FCMs.
M.B. Lippold Q3 4.1. (g). Tracking reports generated to show number of hours completed.
6/30/2009 Indiana Program Improvement Plan 70

4.2. DCS will provide consistent quality foster parent training to new and ongoing foster parents.
4.2. (a). Develop Director’s Note to inform all DCS staff of the plan to transition FAKT training from Programs and Services Department to the Staff Development Department.
L. Rich and MB Lippold
Q6
4.2. (a). Director’s Note
4.2. (b). During transition, Training Staff will review Current FAKT curriculum and identify areas to improve based on TEAPI model as well as update pre and post foster parent training materials to include more reality-based and situational learning.
MB Lippold
Q6
4.2. (b). Documentation of FAKT curriculum review and Revised FAKT training curriculum.
4.2. (c). DCS Hispanic Initiative Program Manager will review current FAKT forms and training materials to ensure the use and correctness of the Spanish language.
D. Judkins Q2 4.2. (c). Updated bilingual materials/curriculum
4.2. (d). Staff development will develop a plan to have training available for Spanish Speaking foster parents.
MB Lippold Q5 4.2. (d). Plan completed with an implementation timeline.
6/30/2009 Indiana Program Improvement Plan 71

4.3. DCS will train foster parents, FCMs and FCMs supervisors on how to become educational surrogates.
4.3 (a). DCS will incorporate the educational surrogate training into FAKT training.
MB Lippold Q7 4.3(a). FAKT training curriculum.
4.3. (b). Provide practice guidance or policy tips to FCMs on how to secure an educational surrogate for children in placement, primarily special education students, as well as practice tips on how to advocate on behalf of the child to ensure educational needs and/or educational plans are met.
A. Green Q3 4.3. (b). Policy tips and practice guidance.
4.3. (c). DCS will provide a Computer Assisted Training on how to become educational surrogates available to FCMs and FCM Supervisors. Training will be tracked through Enterprise Learning Management System (ELMS) for all who completed the training.
M.B. Lippold Q7 4.3. (c). CAT training completed and ELMS report of staff trained.
4.3. (d). The Foster care specialization units will generate a report of foster parents who become educational surrogates.
D. Judkins Q8 4.3. (b). List of foster parents/educational surrogates.
4.4. Enhance Practice Indicator review process to measure safety more effectively.
4.4. (a). Expand definition of safety in practice indicator to measure safety more effectively.
D. Judkins Q1 4.4. (a). Revised practice indicator
6/30/2009 Indiana Program Improvement Plan 72
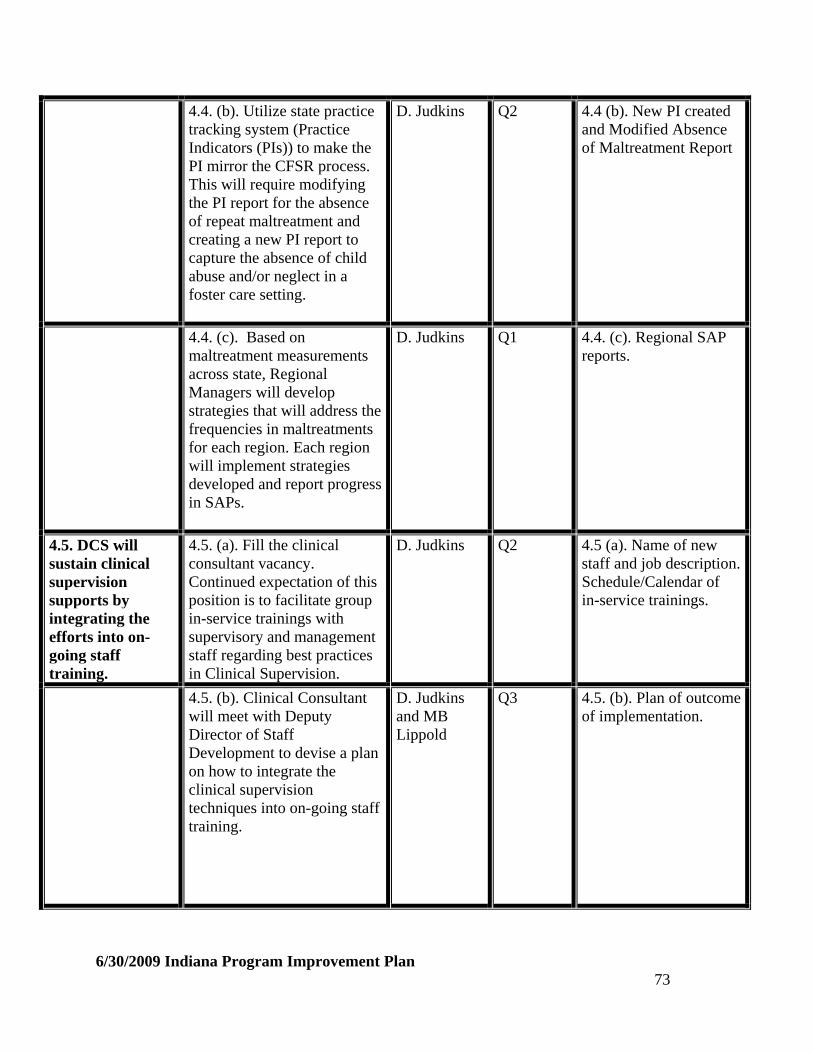
4.4. (b). Utilize state practice tracking system (Practice Indicators (PIs)) to make the PI mirror the CFSR process. This will require modifying the PI report for the absence of repeat maltreatment and creating a new PI report to capture the absence of child abuse and/or neglect in a foster care setting.
D. Judkins Q2
4.4 (b). New PI created and Modified Absence of Maltreatment Report
4.4. (c). Based on maltreatment measurements across state, Regional Managers will develop strategies that will address the frequencies in maltreatments for each region. Each region will implement strategies developed and report progress in SAPs.
D. Judkins Q1 4.4. (c). Regional SAP reports.
4.5. DCS will sustain clinical supervision supports by integrating the efforts into on-going staff training.
4.5. (a). Fill the clinical consultant vacancy. Continued expectation of this position is to facilitate group in-service trainings with supervisory and management staff regarding best practices in Clinical Supervision.
D. Judkins Q2 4.5 (a). Name of new staff and job description. Schedule/Calendar of in-service trainings.
4.5. (b). Clinical Consultant will meet with Deputy Director of Staff Development to devise a plan on how to integrate the clinical supervision techniques into on-going staff training.
D. Judkins and MB Lippold
Q3 4.5. (b). Plan of outcome of implementation.
6/30/2009 Indiana Program Improvement Plan 73
Primary Strategy 4 (con’t)
4.5. (c). Clinical supervision techniques will be incorporated into New Supervisor training, Practice Model Supervision Training and Leadership Training. Trainers will incorporate new material into appropriate modules.
M.B. Lippold Q4 4.5. (c). Curriculum developed and updated modules.
4.5. (d). The Clinical Consultant in collaboration with Peer Coach Consultants (Regionally-based staff) will develop a plan to mentor/coach staff on the fidelity of clinical supervision techniques as it relates to the implementation of the TEAPI model.
D. Judkins and MB Lippold
Q6 4.5. (d). Outcome of plan developed.
6/30/2009 Indiana Program Improvement Plan 74

Part B: National Standards Measurement Plan
Safety Outcome 1: Absence of Recurrence of Maltreatment
National Standard 94.6%
Performance as Measured in Final Report/Source Data Period
92.7% (4-1-05b to 3-31-06a)
Performance as Measured at Baseline/Source Data Period
93.2% (07ab)
Negotiated Improvement Goal 93.8%
Renegotiated Improvement Goal
Q1 Q2 Q3 Q4 Q5 Q6 Q7 Q8 Q9 Q10 Q11 Q12Status (Enter the current quarter measurement for the reported quarter.)
Safety Outcome 1: Absence of Maltreatment of Children in Foster Care
National Standard 99.68%
Performance as Measured in Final Report/Source Data Period
99.3%
Performance as Measured at Baseline/Source Data Period
99.69% (FY 07ab)
Negotiated Improvement Goal N/A. Met National Standard: (Indiana Data Profile, July 9,2008)
Renegotiated Improvement Goal
Q1 Q2 Q3 Q4 Q5 Q6 Q7 Q8 Q9 Q10 Q11 Q12Status (Enter the current quarter measurement for the reported quarter.)
6/30/2009 Indiana Program Improvement Plan 75
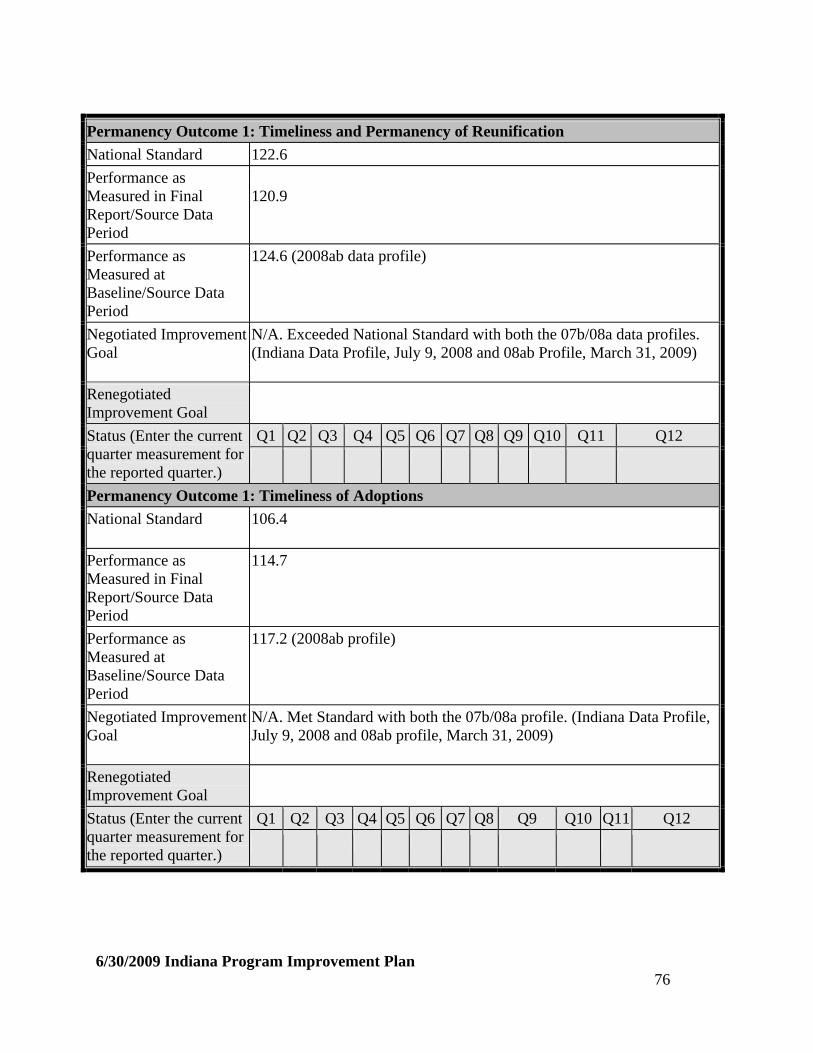
Permanency Outcome 1: Timeliness and Permanency of Reunification
National Standard 122.6
Performance as Measured in Final Report/Source Data Period
120.9
Performance as Measured at Baseline/Source Data Period
124.6 (2008ab data profile)
Negotiated Improvement Goal
N/A. Exceeded National Standard with both the 07b/08a data profiles. (Indiana Data Profile, July 9, 2008 and 08ab Profile, March 31, 2009)
Renegotiated Improvement Goal
Q1 Q2 Q3 Q4 Q5 Q6 Q7 Q8 Q9 Q10 Q11 Q12 Status (Enter the current quarter measurement for the reported quarter.)
Permanency Outcome 1: Timeliness of Adoptions
National Standard 106.4
Performance as Measured in Final Report/Source Data Period
114.7
Performance as Measured at Baseline/Source Data Period
117.2 (2008ab profile)
Negotiated Improvement Goal
N/A. Met Standard with both the 07b/08a profile. (Indiana Data Profile, July 9, 2008 and 08ab profile, March 31, 2009)
Renegotiated Improvement Goal
Q1 Q2 Q3 Q4 Q5 Q6 Q7 Q8 Q9 Q10 Q11 Q12 Status (Enter the current quarter measurement for the reported quarter.)
6/30/2009 Indiana Program Improvement Plan 76
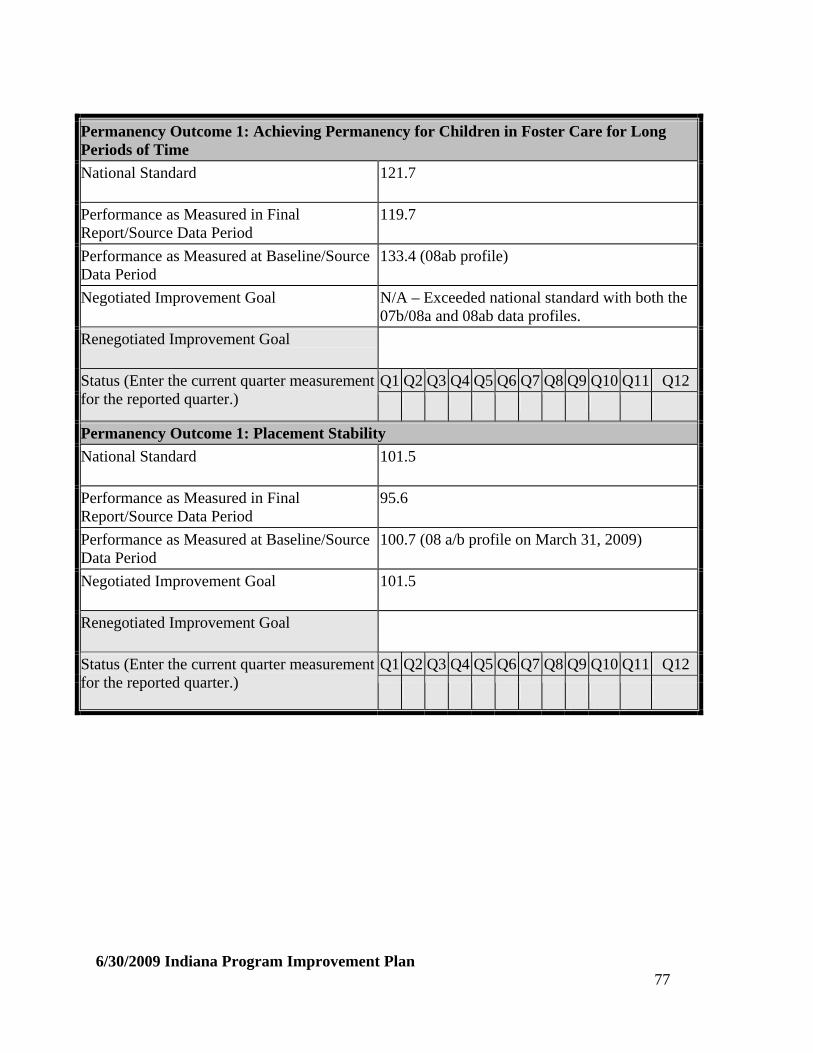
Permanency Outcome 1: Achieving Permanency for Children in Foster Care for Long Periods of Time
National Standard 121.7
Performance as Measured in Final Report/Source Data Period
119.7
Performance as Measured at Baseline/Source Data Period
133.4 (08ab profile)
Negotiated Improvement Goal N/A – Exceeded national standard with both the 07b/08a and 08ab data profiles.
Renegotiated Improvement Goal
Q1 Q2 Q3 Q4 Q5 Q6 Q7 Q8 Q9 Q10 Q11 Q12Status (Enter the current quarter measurement for the reported quarter.)
Permanency Outcome 1: Placement Stability
National Standard 101.5
Performance as Measured in Final Report/Source Data Period
95.6
Performance as Measured at Baseline/Source Data Period
100.7 (08 a/b profile on March 31, 2009)
Negotiated Improvement Goal 101.5
Renegotiated Improvement Goal
Q1 Q2 Q3 Q4 Q5 Q6 Q7 Q8 Q9 Q10 Q11 Q12Status (Enter the current quarter measurement for the reported quarter.)
6/30/2009 Indiana Program Improvement Plan 77
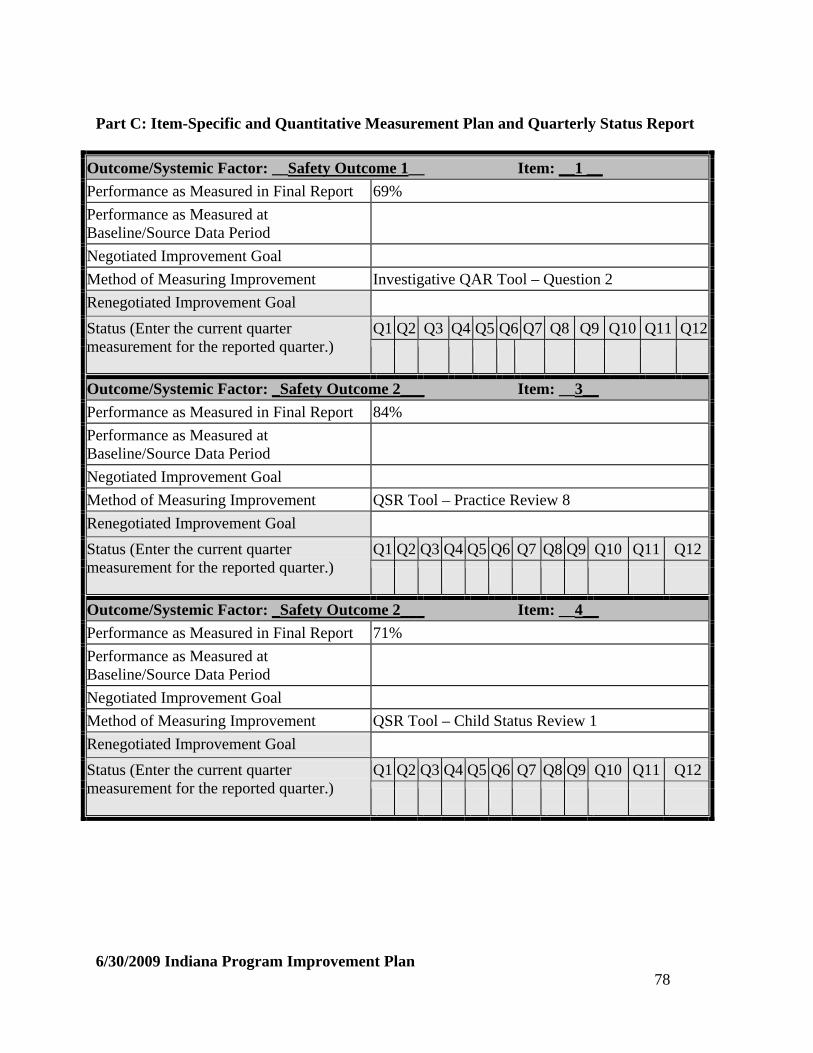
Part C: Item-Specific and Quantitative Measurement Plan and Quarterly Status Report
Outcome/Systemic Factor: __Safety Outcome 1__ Item: __1 __
Performance as Measured in Final Report 69%
Performance as Measured at Baseline/Source Data Period
Negotiated Improvement Goal
Method of Measuring Improvement Investigative QAR Tool – Question 2
Renegotiated Improvement Goal
Q1 Q2 Q3 Q4 Q5 Q6 Q7 Q8 Q9 Q10 Q11 Q12Status (Enter the current quarter measurement for the reported quarter.)
Outcome/Systemic Factor: _Safety Outcome 2___ Item: __3__
Performance as Measured in Final Report 84%
Performance as Measured at Baseline/Source Data Period
Negotiated Improvement Goal
Method of Measuring Improvement QSR Tool – Practice Review 8
Renegotiated Improvement Goal
Q1 Q2 Q3 Q4 Q5 Q6 Q7 Q8 Q9 Q10 Q11 Q12Status (Enter the current quarter measurement for the reported quarter.)
Outcome/Systemic Factor: _Safety Outcome 2___ Item: __4__
Performance as Measured in Final Report 71%
Performance as Measured at Baseline/Source Data Period
Negotiated Improvement Goal
Method of Measuring Improvement QSR Tool – Child Status Review 1
Renegotiated Improvement Goal
Q1 Q2 Q3 Q4 Q5 Q6 Q7 Q8 Q9 Q10 Q11 Q12Status (Enter the current quarter measurement for the reported quarter.)
6/30/2009 Indiana Program Improvement Plan 78

6/30/2009 Indiana Program Improvement Plan 79
Outcome/Systemic Factor: _Permanency Outcome 1___ Item: _7___
Performance as Measured in Final Report 53%
Performance as Measured at Baseline/Source Data Period
Negotiated Improvement Goal
Method of Measuring Improvement QAR Tool – new question
Renegotiated Improvement Goal
Q1 Q2 Q3 Q4 Q5 Q6 Q7 Q8 Q9 Q10 Q11 Q12Status (Enter the current quarter measurement for the reported quarter.)
Outcome/Systemic Factor: __Permanency Outcome 1__ Item: __10__
Performance as Measured in Final Report 88%
Performance as Measured at Baseline/Source Data Period
Negotiated Improvement Goal
Method of Measuring Improvement QSR Tool – Child Status Review 9: Pathways to Independence.
Renegotiated Improvement Goal
Q1 Q2 Q3 Q4 Q5 Q6 Q7 Q8 Q9 Q10 Q11 Q12Status (Enter the current quarter measurement for the reported quarter.)
Outcome/Systemic Factor: _Well-being Outcome 1___ Item: _17___
Performance as Measured in Final Report 45%
Performance as Measured at Baseline/Source Data Period
Negotiated Improvement Goal
Method of Measuring Improvement QSR Tool – Practice Review 4: Assessing and Understanding

Renegotiated Improvement Goal
Q1 Q2 Q3 Q4 Q5 Q6 Q7 Q8 Q9 Q10 Q11 Q12Status (Enter the current quarter measurement for the reported quarter.)
Outcome/Systemic Factor: _Well-Being Outcome 1___ Item: _18___
Performance as Measured in Final Report 51%
Performance as Measured at Baseline/Source Data Period
Negotiated Improvement Goal
Method of Measuring Improvement QSR Tool – Practice Review 1: Engaging-Role and Voice of Family Members
Renegotiated Improvement Goal
Q1 Q2 Q3 Q4 Q5 Q6 Q7 Q8 Q9 Q10 Q11 Q12Status (Enter the current quarter measurement for the reported quarter.)
Outcome/Systemic Factor: _Well-Being Outcome 1 Item: _19___
Performance as Measured in Final Report 77%
Performance as Measured at Baseline/Source Data Period
Negotiated Improvement Goal
Method of Measuring Improvement QAR Tools – (wardship and IA) new questions
Renegotiated Improvement Goal
Q1 Q2 Q3 Q4 Q5 Q6 Q7 Q8 Q9 Q10 Q11 Q12Status (Enter the current quarter measurement for the reported quarter.)
Outcome/Systemic Factor: _Well-Being Outcome 1___ Item: _20___
Performance as Measured in Final Report 37%
Performance as Measured at Baseline/Source Data Period
Negotiated Improvement Goal
6/30/2009 Indiana Program Improvement Plan 80
Method of Measuring Improvement QAR Tool – new language to address mothers and fathers
Renegotiated Improvement Goal
Q1 Q2 Q3 Q4 Q5 Q6 Q7 Q8 Q9 Q10 Q11 Q12Status (Enter the current quarter measurement for the reported quarter.)
6/30/2009 Indiana Program Improvement Plan 81
V. List of CFSR Outcomes and Systemic Factors, and
Associated Items, Data Indicators, and Data Composites
Safety Outcome 1: Children are, first and foremost, protected from abuse and neglect.
Item 1. Timeliness of initiating investigations of reports of child maltreatment. Item 2. Repeat maltreatment. Data Indicator: Absence of Recurrence of Maltreatment Data Indicator: Absence of Maltreatment of Children in Foster Care
Safety Outcome 2: Children are safely maintained in their homes whenever possible and appropriate.
Item 3. Services to family to protect child (ren) in home and prevent removal or re-entry into foster care.
Item 4. Risk assessment and safety management.
Permanency Outcome 1: Children have permanency and stability in their living situations.
Item 5. Foster care re-entries. Item 6. Stability of foster care placement. Item 7. Permanency goal for child. Item 8. Reunification, guardianship, or permanent placement with relatives.
Item 9. Adoption. Item 10. Other planned permanent living arrangement. Permanency Composite 1: Timeliness and Permanency of Reunification Permanency Composite 2: Timeliness of Adoptions Permanency Composite 3: Achieving Permanency for Children in Foster Care for Long
Periods of Time Permanency Composite 4: Placement Stability
6/30/2009 Indiana Program Improvement Plan 82

Permanency Outcome 2: The continuity of family relationships and connections is preserved for children.
Item 11. Proximity of foster care placement. Item 12. Placement with siblings. Item 13. Visiting with parents and siblings in foster care. Item 14. Preserving connections. Item 15. Relative placement. Item 16. Relationship of child in care with parents.
Child and Family Well-Being Outcome 1: Families have enhanced capacity to provide for their children’s needs.
Item 17. Needs and services of child, parents, foster parents. Item 18. Child and family involvement in case planning. Item 19. Caseworker visits with child. Item 20. Caseworker visits with parents.
Child and Family Well-Being Outcome 2: Children receive appropriate services to meet their educational needs.
Item 21. Educational needs of the child. Child and Family Well-Being Outcome 3: Children receive adequate services to meet their physical and mental health needs.
Item 22. Physical health of the child. Item 23. Mental/behavioral health of the child.
Systemic Factor: Statewide Information System
Item 24. The State is operating a statewide information system that, at a minimum, can readily identify the legal status, demographic characteristics, location, and goals for the placement of every child who is (or within the immediately preceding 12 months, has been) in foster care.
6/30/2009 Indiana Program Improvement Plan 83
Systemic Factor: Case Review System
Item 25. The State provides a process that ensures that each child has a written case plan to be developed jointly with the child’s parent(s) that includes the required provisions.
Item 26. The State provides a process for the periodic review of the status of each child, no
less frequently than once every 6 months, either by a court or by administrative review.
Item 27. The State provides a process that ensures that each child in foster care under the
supervision of the State has a permanency hearing in a qualified court or administrative body no later than 12 months from the date the child entered foster care and no less frequently than every 12 months thereafter.
Item 28. The State provides a process for termination of parental rights proceedings in
accordance with the provisions of the Adoption and Safe Families Act. Item 29. The State provides a process for foster parents, pre-adoptive parents, and relative
caregivers of children in foster care to be notified of, and have an opportunity to be heard in, any review or hearing held with respect to the child.
Systemic Factor: Quality Assurance System
Item 30. The State has developed and implemented standards to ensure that children in foster care are provided quality services that protect the safety and health of the children.
Item 31. The State is operating an identifiable quality assurance system that is in place in
the jurisdictions where the services included in the Child and Family Services Plan are provided, evaluates the quality of services, identifies strengths and needs of the service delivery system, provides relevant reports, and evaluates implemented program improvement measures.
Systemic Factor: Staff and Provider Training
Item 32. The State is operating a staff development and training program that supports the goals and objectives in the Child and Family Services Plan, addresses services provided under titles IV-B and IV-E, and provides initial training for all staff that delivers these services.
Item 33. The State provides for ongoing training for staff that addresses the skills and
knowledge base needed to carry out their duties with regard to the services included in the Child and Family Services Plan.
6/30/2009 Indiana Program Improvement Plan 84
Item 34. The State provides training for current or prospective foster parents, adoptive parents, and staff of State licensed or approved facilities that care for children receiving foster care or adoption assistance under title IV-E that addresses the skills and knowledge base needed to carry out their duties with regard to foster and adopted children.
Systemic Factor: Service Array and Resource Development
Item 35. The State has in place an array of services that assess the strengths and needs of children and families and determine other service needs, address the needs of families in addition to individual children in order to create a safe home environment, enable children to remain safely with their parents when reasonable, and help children in foster and adoptive placements achieve permanency.
Item 36. The services in item 35 are accessible to families and children in all political
jurisdictions covered in the State’s Child and Family Services Plan. Item 37. The services in item 35 can be individualized to meet the unique needs of children
and families served by the agency. Systemic Factor: Agency Responsiveness to the Community
Item 38. In implementing the provisions of the Child and Family Services Plan, the State engages in ongoing consultation with tribal representatives, consumers, service providers, foster care providers, the juvenile court, and other public and private child- and family-serving agencies and includes the major concerns of these representatives in the goals and objectives of the Child and Family Services Plan.
Item 39. The agency develops, in consultation with these representatives, Annual Progress
and Services Reports pursuant to the Child and Family Services Plan. Item 40. The State’s services under the Child and Family Services Plan are coordinated
with services or benefits of other Federal or federally assisted programs serving the same population.
Systemic Factor: Foster and Adoptive Parent Licensing, Recruitment, and Retention
Item 41. The State has implemented standards for foster family homes and child care institutions that are reasonably in accord with recommended national standards.
Item 42. The standards are applied to all licensed or approved foster family homes or child
care institutions receiving title IV-E or IV-B funds. Item 43. The State complies with Federal requirements for criminal background clearances
as related to licensing or approving foster care and adoptive placements and has in
6/30/2009 Indiana Program Improvement Plan 85
6/30/2009 Indiana Program Improvement Plan 86
place a case planning process that includes provisions for addressing the safety of foster care and adoptive placements for children.
Item 44. The State has in place a process for ensuring the diligent recruitment of potential
foster and adoptive families who reflect the ethnic and racial diversity of children in the State for whom foster and adoptive homes are needed.
Item 45. The State has in place a process for the effective use of cross-jurisdictional
resources to facilitate timely adoptive or permanent placements for waiting children.
Attachments: QAR Tools