improving outcome by improving memory for treatment
TRANSCRIPT
Allison G. Harvey, PhD
Professor, Clinical Psychology Director, Golden Bear Sleep and Mood Research Clinic
University of California, Berkeley
Improving Outcome by Improving Memory for Treatment
Recommendations
Memory is poor for CBT – Insomnia patients:
• forgot one third of CBT treatment contents • recall was as low as 13% (Chambers, 1991)
• Bipolar disorder with insomnia:
– recalled 20-37% of CBT treatment contents (Lee & Harvey, 2015, JCCP)
• Major depression:
– 80% thought about and 55% applied CBT session contents, but only 50% were accurate (Gumport et al, 2015)
• Cancer patients: 23% to 33% (Jansen et al., 2008)
• Osteoporosis patients: 31% to 63% (Pickney & Arnason, 2005)
• Chronic pain patients: 30% (Lewkovich & Haneline, 2005)
• High cholesterol patients: 38% (Croyle et al., 2006)
• Particularly poor for health behavior change advice (Flocke & Stange, 2004)
• 60% of the patients did not recall recommendations and 25% recalled recommendations that were not made (Bober, et al., 2007)
Memory is Poor for Medical Advice
Characteristic of: • Alcohol and substance use problems (e.g., Parson &
Prigatono, 2014)
• Bipolar disorder (e.g., Clark et al., 2005; Martino et al., 2011)
• Schizophrenia (e.g., Altshuler et al., 2004; Varga et al., 2007)
• Post-traumatic stress disorder (Bremner et al., 2004; Jelinek et al., 2006)
• Anxiety disorders (Airaksinen et al., 2005)
• Major depression (e.g., Behnken et al., 2010; Campbell & MacQueen, 2004)
• And many others!
Memory Impairment

Fallibility possible at
Initial encoding (formation) Storage (consolidation) Later recollection (retrieval) (Schacter, 2001)
Susceptible to biases (Croyle et al, 2006; Gutchess et al, 2007)
Negative emotion is likely to bias attention (Beck, 1976) and therefore memory (Phelps, 2004)
CBT/DBT/ACT/ITP sessions: are typically 50 mins long & cover complex information
Memory Challenge
Memory impairment is modifiable
• Memory Support (MS) strategies – can improve memory encoding and retention – in patients with dementia and depression (e.g.,
Almkvist et al., 1999; Taconnat et al., 2010)
Harvey et al., 2014, Perspectives in Psychological Science

Is improving memory for the content of
treatment sessions a path to improving outcome and sustaining treatment gains?
Memory Support Intervention (MSI)
Transdiagnostic (other disorders) Pantreatment (other treatments)
Question
NIMH R34MH080958

• CT for depression is well studied (Cuijpers et al., 2013; Cuijpers et
al., 2013).
• As effective as antidepressant medication for moderate to severe depression (e.g., Dimidjian, Hollon, Dobson, Schmaling, Kohlenberg, Addis, Gallop, McGlinchey, Markley, & Gollan, 2006; Dobson et al., 2008) and less likely to relapse (Bockting et al., 2005; Dobson et al., 2008; Hollon et al., 2005; Paykel et al., 2005).
• Room for improvement: One third initially randomized respond and “survive” 1 year without relapse (Dobson, et al.,
2008; Hollon, et al., 2005).
Why CT for depression?
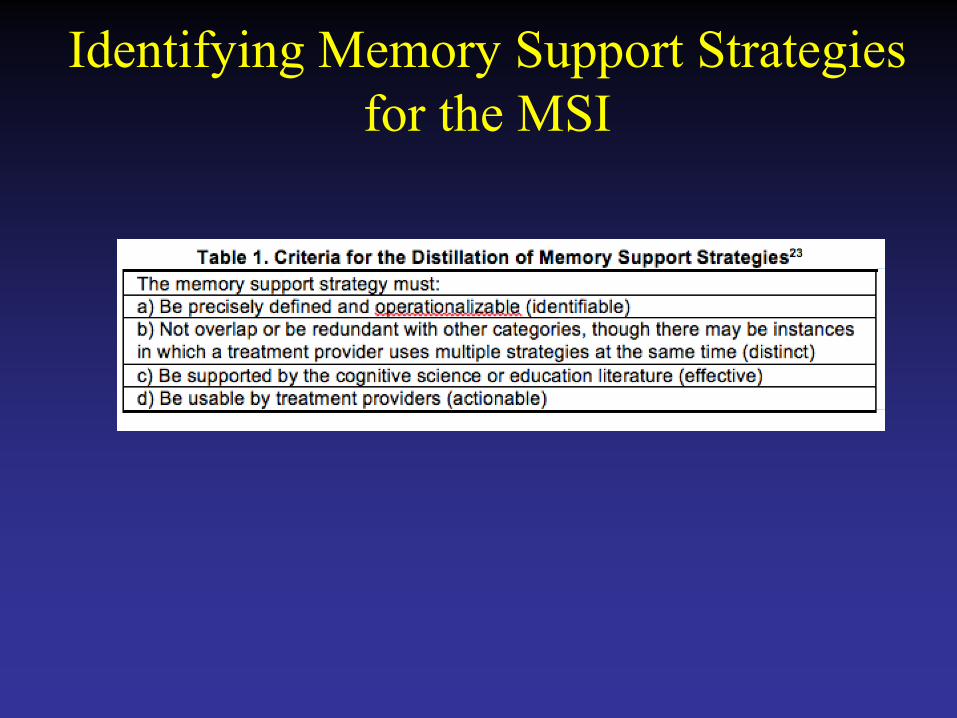
Identifying Memory Support Strategies for the MSI
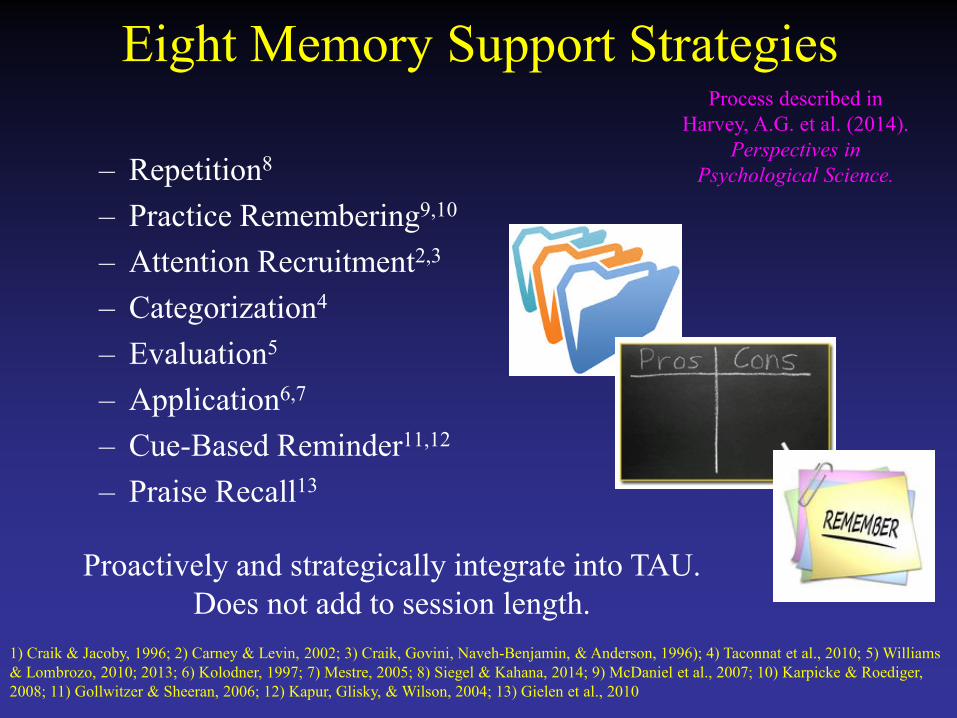
Eight Memory Support Strategies
– Repetition8
– Practice Remembering9,10
– Attention Recruitment2,3
– Categorization4
– Evaluation5
– Application6,7
– Cue-Based Reminder11,12
– Praise Recall13
1) Craik & Jacoby, 1996; 2) Carney & Levin, 2002; 3) Craik, Govini, Naveh-Benjamin, & Anderson, 1996); 4) Taconnat et al., 2010; 5) Williams & Lombrozo, 2010; 2013; 6) Kolodner, 1997; 7) Mestre, 2005; 8) Siegel & Kahana, 2014; 9) McDaniel et al., 2007; 10) Karpicke & Roediger, 2008; 11) Gollwitzer & Sheeran, 2006; 12) Kapur, Glisky, & Wilson, 2004; 13) Gielen et al., 2010
Process described in Harvey, A.G. et al. (2014).
Perspectives in Psychological Science.
Proactively and strategically integrate into TAU. Does not add to session length.
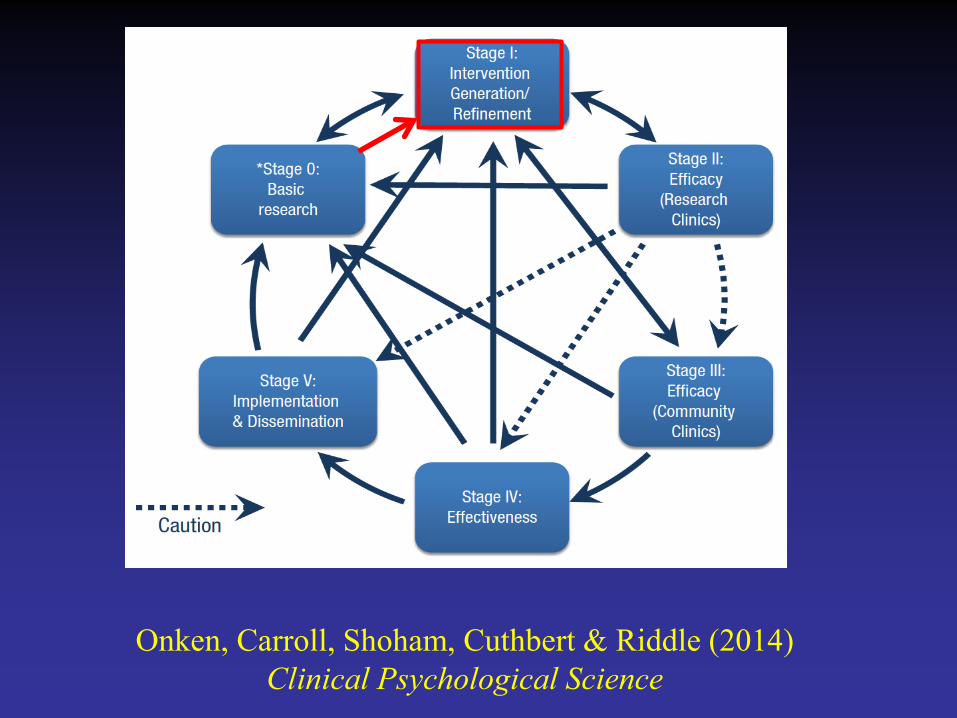
Onken, Carroll, Shoham, Cuthbert & Riddle (2014) Clinical Psychological Science
CBT already includes Memory Support
• For example:
– Capsule summaries
– Note taking of major points – Writing down the homework list
– Recall of prior session at the beginning of each session
– Recap of the session at the end of each session
But do all therapists use these memory supports?
Would outcome improve if more memory supports were used?

Next Steps
Two New Measures
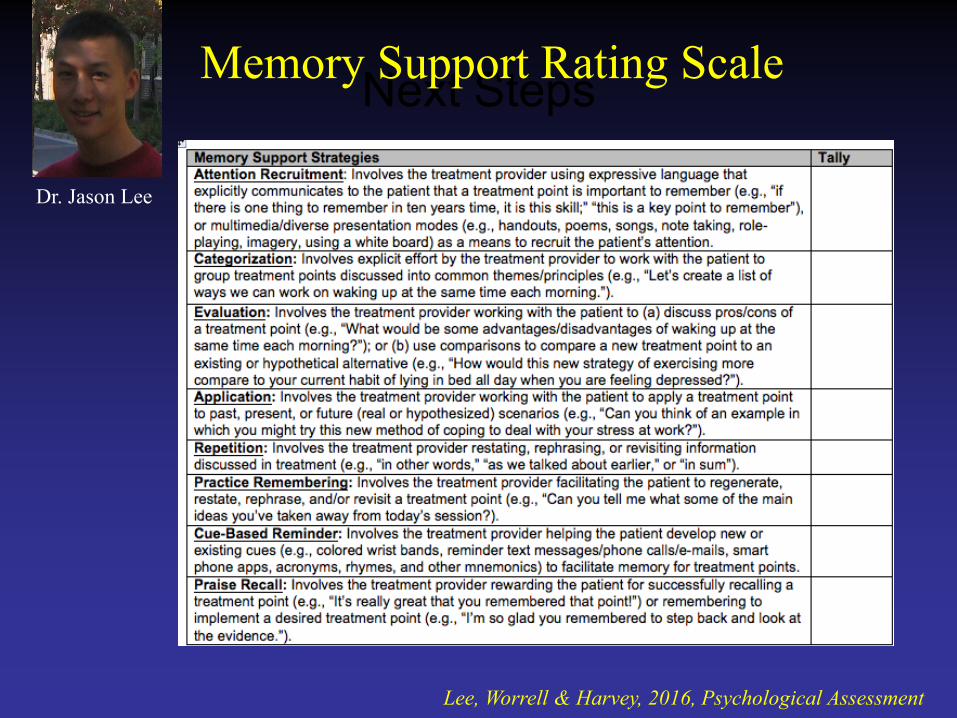
Next Steps Memory Support Rating Scale
Lee, Worrell & Harvey, 2016, Psychological Assessment
Dr. Jason Lee
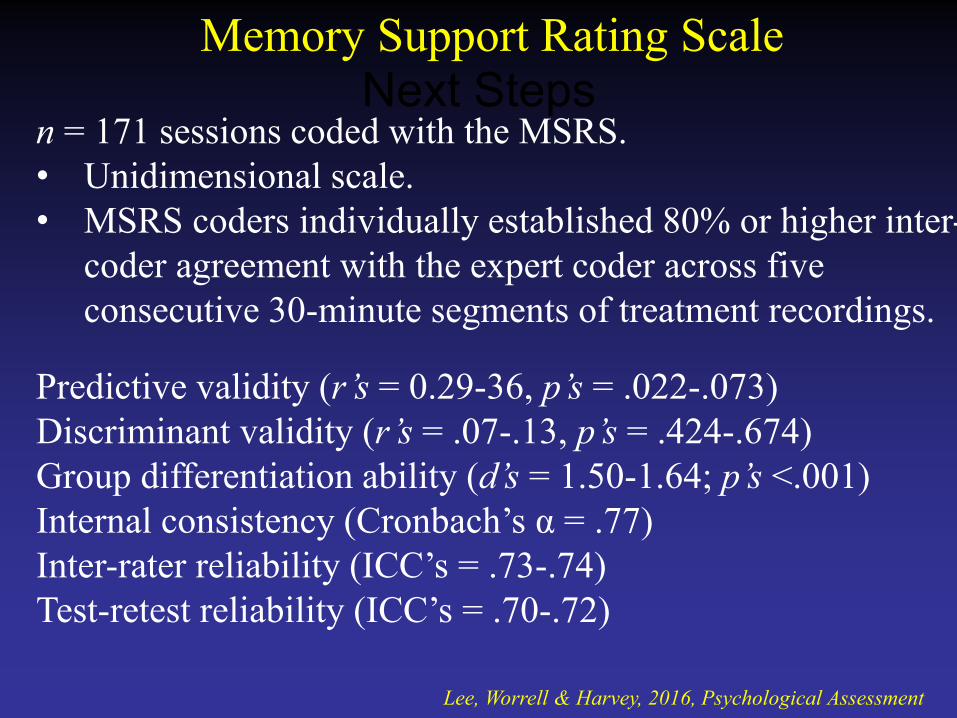
Next Steps Memory Support Rating Scale
n = 171 sessions coded with the MSRS. • Unidimensional scale. • MSRS coders individually established 80% or higher inter-
coder agreement with the expert coder across five consecutive 30-minute segments of treatment recordings.
Predictive validity (r’s = 0.29-36, p’s = .022-.073) Discriminant validity (r’s = .07-.13, p’s = .424-.674) Group differentiation ability (d’s = 1.50-1.64; p’s <.001) Internal consistency (Cronbach’s α = .77) Inter-rater reliability (ICC’s = .73-.74) Test-retest reliability (ICC’s = .70-.72)
Lee, Worrell & Harvey, 2016, Psychological Assessment
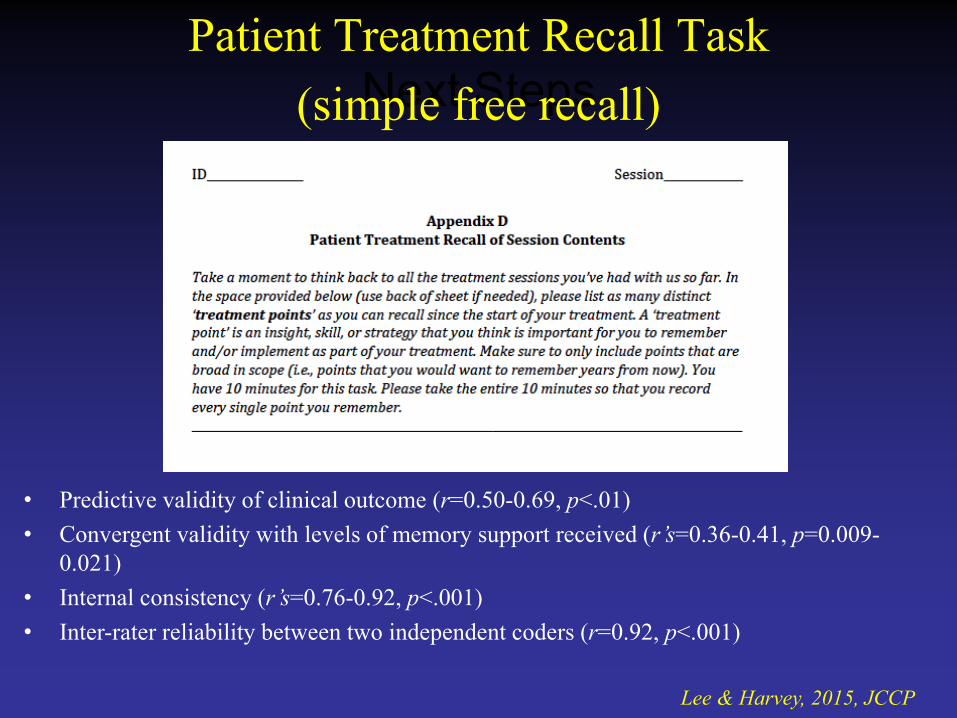
Next Steps Patient Treatment Recall Task
(simple free recall)
Lee & Harvey, 2015, JCCP
• Predictive validity of clinical outcome (r=0.50-0.69, p<.01) • Convergent validity with levels of memory support received (r’s=0.36-0.41, p=0.009-
0.021) • Internal consistency (r’s=0.76-0.92, p<.001) • Inter-rater reliability between two independent coders (r=0.92, p<.001)

Next Steps
Pilot RCT
Caveats • CT is an already efficacious treatment (Hollon et al.,
2014; Ann Rev of Clin Psych)
• Pilot RCT: – not powered to obtain significant effects – ‘more about learning than confirming’ (Lee, Whitehead et
al., 2014, BMC Medical Research Methodology)
• We have used this pilot to empirically derive the optimal dose of memory support – Current study: optimal dose will be delivered in every
treatment session
Young & Beck, 1980; Vallis, Shaw & Dobson, 1986
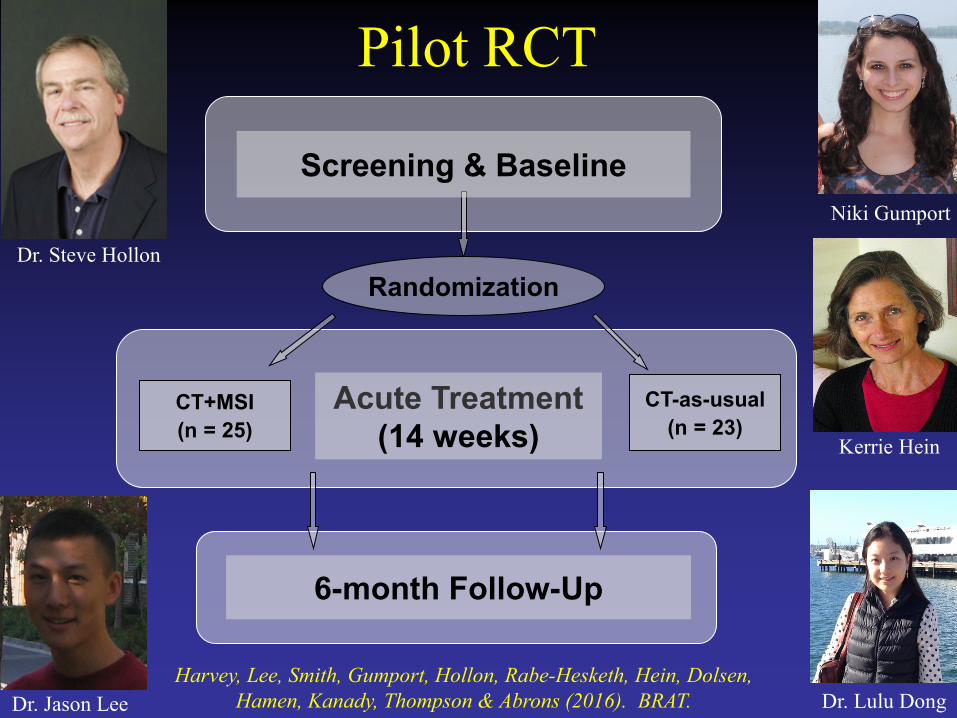
CT-as-usual (n = 23)
CT+MSI (n = 25)
Acute Treatment (14 weeks)
6-month Follow-Up
Randomization
Screening & Baseline
Pilot RCT
Dr. Steve Hollon
Harvey, Lee, Smith, Gumport, Hollon, Rabe-Hesketh, Hein, Dolsen, Hamen, Kanady, Thompson & Abrons (2016). BRAT. Dr. Jason Lee Dr. Lulu Dong
Niki Gumport
Kerrie Hein
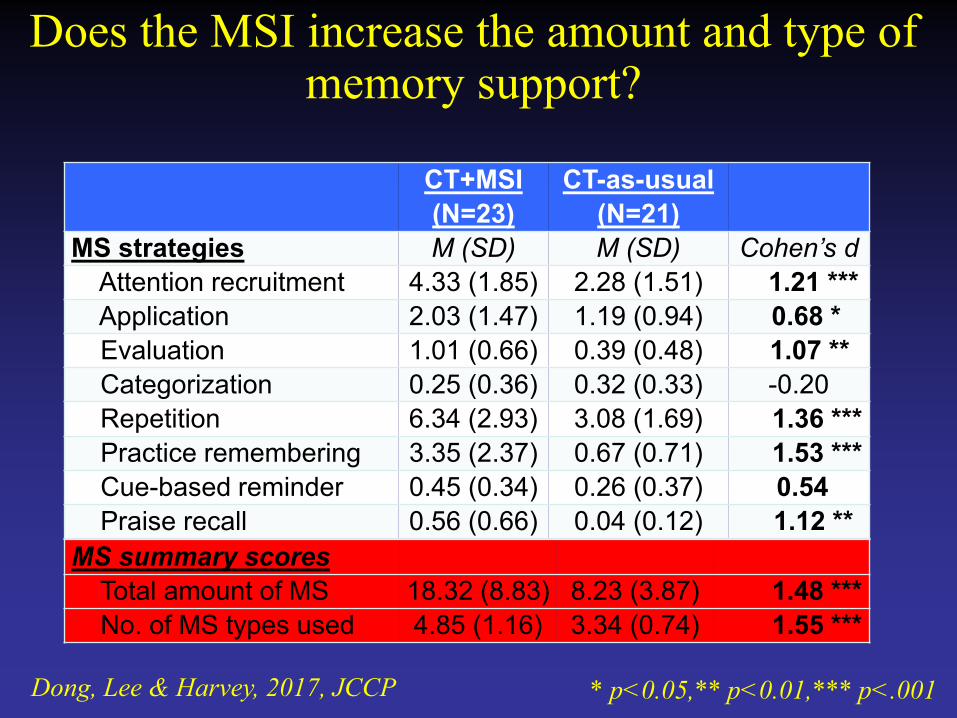
Does the MSI increase the amount and type of memory support?
CT+MSI (N=23)
CT-as-usual (N=21)
MS strategies M (SD) M (SD) Cohen’s d Attention recruitment 4.33 (1.85) 2.28 (1.51) 1.21 *** Application 2.03 (1.47) 1.19 (0.94) 0.68 * Evaluation 1.01 (0.66) 0.39 (0.48) 1.07 ** Categorization 0.25 (0.36) 0.32 (0.33) -0.20 Repetition 6.34 (2.93) 3.08 (1.69) 1.36 *** Practice remembering 3.35 (2.37) 0.67 (0.71) 1.53 *** Cue-based reminder 0.45 (0.34) 0.26 (0.37) 0.54 Praise recall 0.56 (0.66) 0.04 (0.12) 1.12 ** MS summary scores Total amount of MS 18.32 (8.83) 8.23 (3.87) 1.48 *** No. of MS types used 4.85 (1.16) 3.34 (0.74) 1.55 ***
* p<0.05,** p<0.01,*** p<.001
Dong, Lee & Harvey, 2017, JCCP
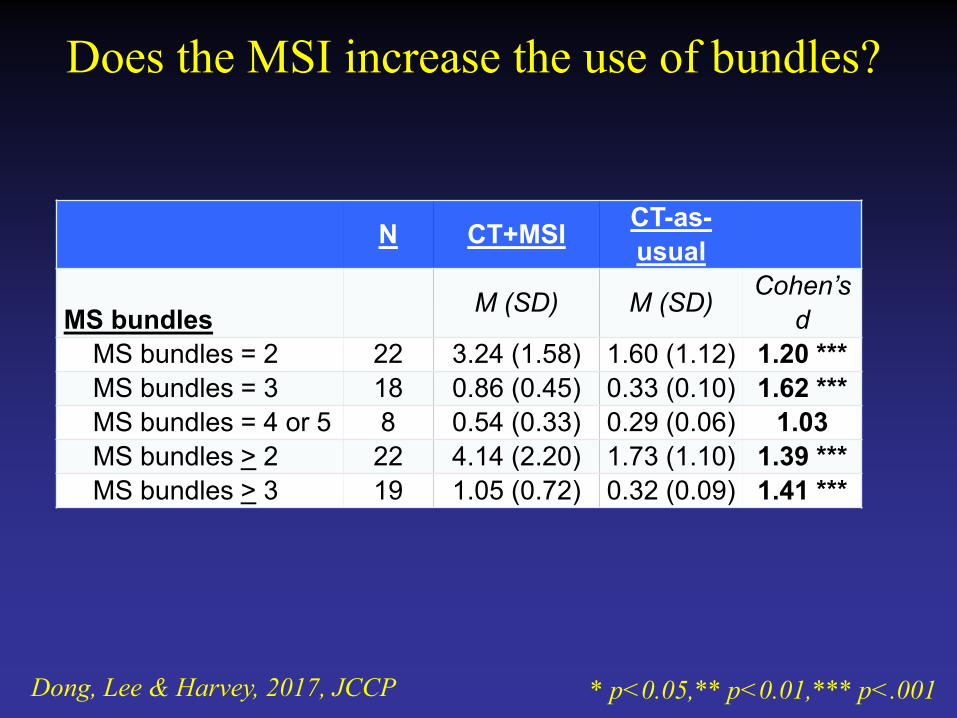
Does the MSI increase the use of bundles?
N CT+MSI CT-as-usual
MS bundles M (SD) M (SD) Cohen’s d
MS bundles = 2 22 3.24 (1.58) 1.60 (1.12) 1.20 *** MS bundles = 3 18 0.86 (0.45) 0.33 (0.10) 1.62 *** MS bundles = 4 or 5 8 0.54 (0.33) 0.29 (0.06) 1.03 MS bundles > 2 22 4.14 (2.20) 1.73 (1.10) 1.39 *** MS bundles > 3 19 1.05 (0.72) 0.32 (0.09) 1.41 ***
* p<0.05,** p<0.01,*** p<.001
Dong, Lee & Harvey, 2017, JCCP
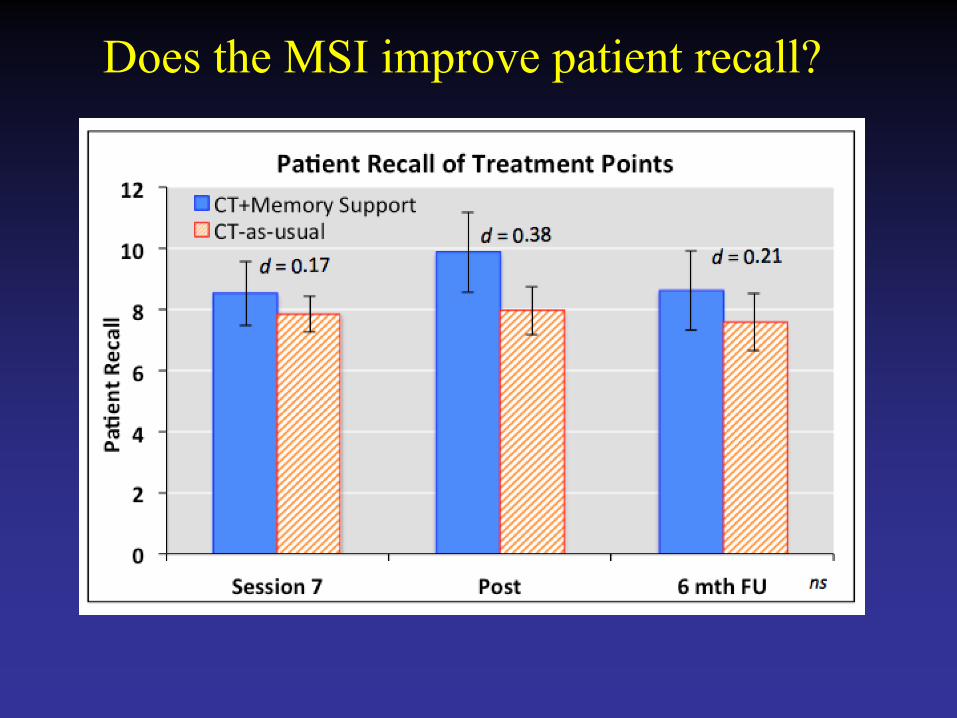
Does the MSI improve patient recall?
Does the MSI improve treatment outcome?
• ACNP criteria (Rush et al., 2006) • ‘Response’
• 54.50% in CT+Memory Support Intervention • 30.00% in CT-as-usual • Odds ratio of 2.80 (95% CI [0.72-14.57])
• ‘Remission’
• 36.40% in CT+Memory Support Intervention • 15.00% in CT-as-usual • Odds ratio of 3.24 (95% CI [0.72-14.57])
Harvey et al. 2016, BRAT
Do poor treatment response characteristics moderate effectiveness of the MSI?
• Older age • Lower intelligence • More chronic depression • Impairment in declarative memory • Fewer years of education
Bearden et al., 2006; Bremner, Vythilingam, Vermetten, Vaccarino, & Charney, 2004; Deuschle et al., 2004; Fournier et al., 2009; Majer et al., 2004

Less education (<16yrs) was associated with better response to CT+Memory Support
Depression Severity General Functioning
What is the Optimal Dose of Memory
Support?
• Ideal dose of memory support per session • ROC to establish the minimum dose of MS needed
to result in patients freely recalling the highest number of treatment points
• CT+MS = 19 units per 50 min session
Lee et al., in prep
• Average amount of memory support per session in CT-as-usual • 8-9 units per 50 min session
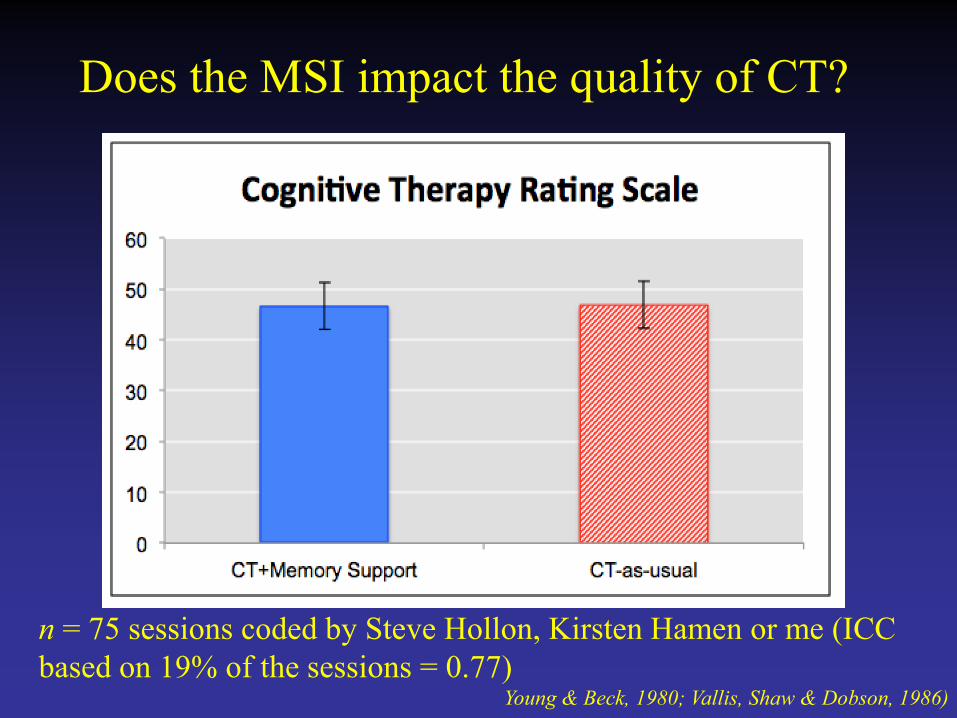
Does the MSI impact the quality of CT?
n = 75 sessions coded by Steve Hollon, Kirsten Hamen or me (ICC based on 19% of the sessions = 0.77)
Young & Beck, 1980; Vallis, Shaw & Dobson, 1986)

How do patients evaluate the MSI?
Credibility and Expectancy Questionnaire; Devilly & Borkovec, (2000)
• CT+MSI and CT-as-usual did not differ • treatment expectations • credibility
• Relative to CT-as-usual, the CT+MSI group were: • more confident in recommending this
treatment to a friend (p=0.06)
• more satisfied (p=0.07)
• reported stronger relationships with their treatment provider (p=0.09)
Summary
• Signal that the MSI may exert an influence on patient recall • Concern that free recall is not the appropriate memory test • Alternatives? • We are working on a vignette task (Garret Zieve)
• Signal that the MSI improves the outcome
(depression)
• Derived the optimal dose
Future Directions
• R01MH108657; N = 178
• Precisely mapping the role of memory for treatment in the behavior change process
• This is a within session approach (audio tapes / text messaging = between session approach)
• Focus on making sure it is scalable to: • Transdiagnostic (other disorders) • Pantreatment (other treatments)
R34, Memory in MDD Dr. Steve Hollon Dr. Lulu Dong Dr. Jason Lee Kerrie Hein Niki Gumport
R01, Memory in MDD Dr. Steve Hollon Dr. Lulu Dong Dr. Jason Lee Kerrie Hein Niki Gumport Molly McNamara Claire Weaver Armando Martinez Haruka Notsu Alison Tuck Melanie Tran Garret Zieve Cece Armstrong
Vignette Task
• Nathan: problems in his marriage, a critical boss, believes
he is a failure. (1 page description) • Why do you think Nathan is experiencing symptoms of
depression? • What do you think Nathan could do to start feeling better? • How do you think your recommendations will help
Nathan?
Garret Zieve