immunotherapy
TRANSCRIPT

Immunotherapy
Reviewed by Sirapassorn
Sornphiphatphong, MD.
Immunotherapy
• Definition
• Indication
• Mechanisms of immunotherapy
• Clinical efficacy
• Immunotherapy administration
• Allergen extract selection
• Allergen extract handling
• Special considerations in immunotherapy

Immunotherapy
• In 2011 the allergy community celebrated the
one hundredth anniversary of the initial
description of immunotherapy by Leonard Noon
and John Freeman
• In the 1950s and 1960s, adequately controlled
studies were conducted in England by Frankland
and Augustin and in the United States by Lowell
and Franklin
Middleton 8th

Allergen immunotherapy
• Repeated administration of specific allergens
to patients with IgE mediated conditions
• For protection against the allergic symptoms
and inflammatory reactions associated with
natural exposure to these allergens
• Hyposensitization, allergen-specific
desensitization
Practice parameters 3rd JACI 2011
Indication of Allergen immunotherapy
• Allergic rhinitis
• Allergic conjunctivitis
• Asthma
• Hymenoptera sting hypersensitivity
New indications (2011):
• Atopic dermatitis with aeroallergen sensitization
• VIT: patients who experience recurrent bothersome large local reactions
Practice parameters 3rd JACI 2011
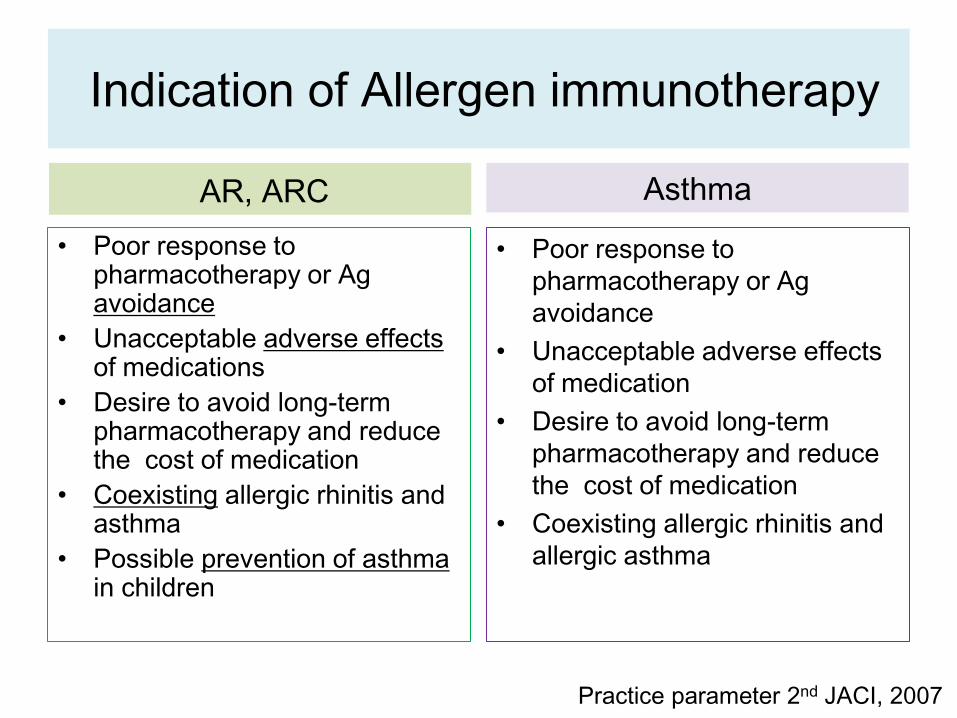
Indication of Allergen immunotherapy
AR, ARC
• Poor response to pharmacotherapy or Ag avoidance
• Unacceptable adverse effects of medications
• Desire to avoid long-term pharmacotherapy and reduce the cost of medication
• Coexisting allergic rhinitis and asthma
• Possible prevention of asthma in children
Asthma
• Poor response to
pharmacotherapy or Ag
avoidance
• Unacceptable adverse effects
of medication
• Desire to avoid long-term
pharmacotherapy and reduce
the cost of medication
• Coexisting allergic rhinitis and
allergic asthma
Practice parameter 2nd JACI, 2007

Hymenoptera sting hypersensitivity
• Hx of a systemic reaction and evidence of
clinically relevant specific IgE Ab
• Patients >16 yrs with a Hx of a systemic reaction
limited to the skin and evidence of clinically
relevant specific IgE Ab
• Adults and children with a Hx of a systemic
reaction to fire ant and evidence of clinically
relevant specific IgE Ab
Practice parameter 2nd JACI, 2007
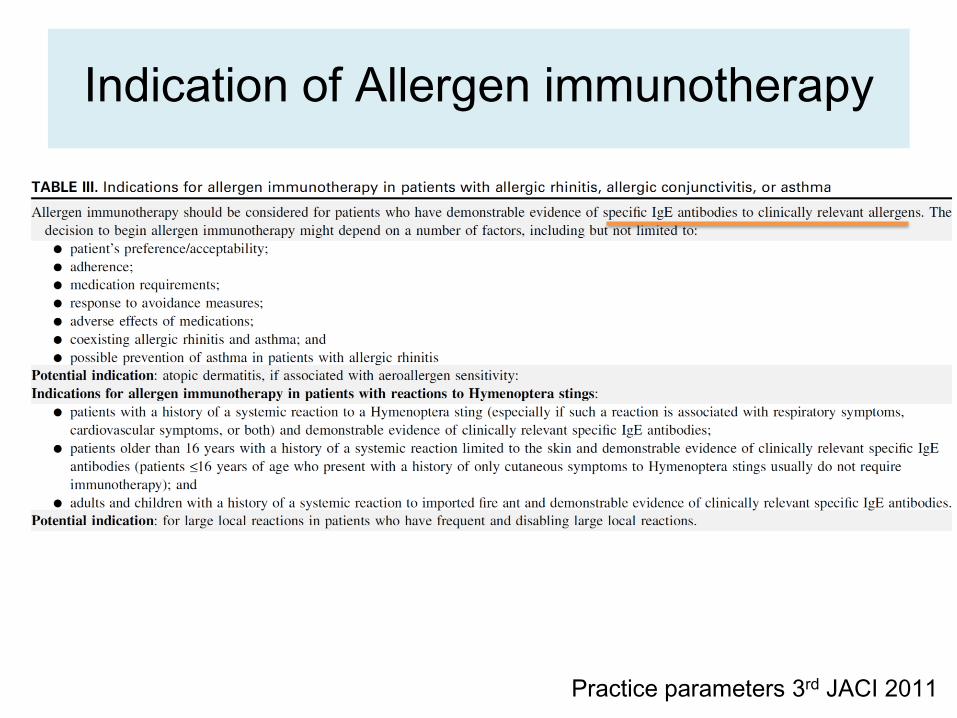
Indication of Allergen immunotherapy
Practice parameters 3rd JACI 2011
Mechanisms of immunotherapy

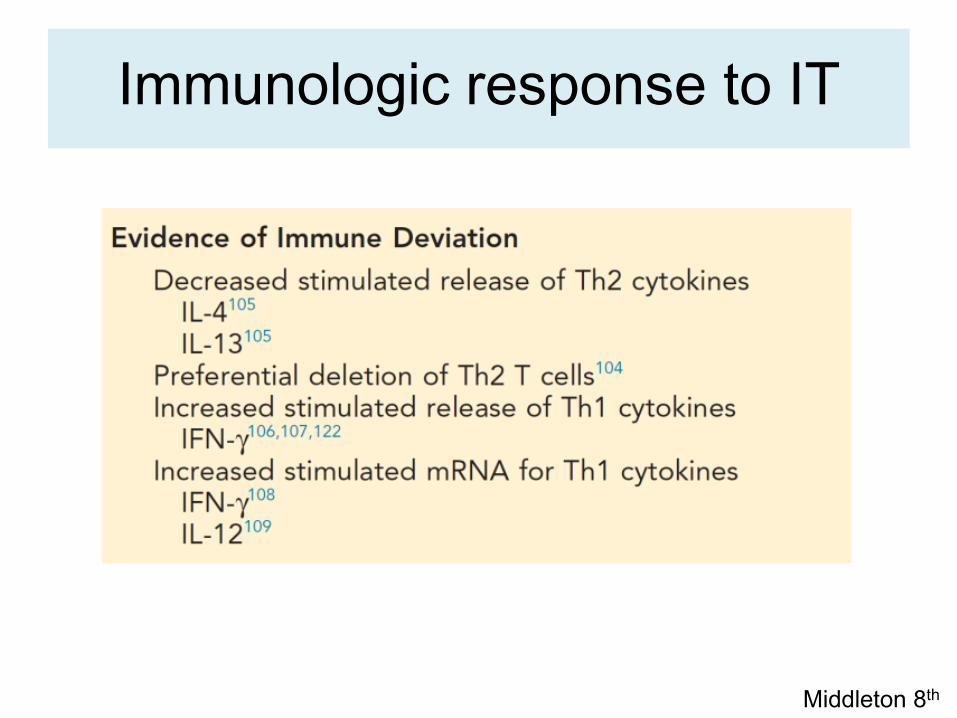
Immunologic response to IT
• Immunologic changes complex
• Block both the immediate and late-phase allergic
response
• Decrease the recruitment of mast cells,
basophils, and eosinophils in the skin, nose,
eye, and bronchial mucosa after provocation or
natural exposure to allergens
• Successful immunotherapy associated with a
change toward a TH1 CD4+ cytokine profile

Immunologic response to IT
Middleton 8th

Humeral response
Immunoglobulin E
• Initially increase in specific IgE antibody levels
• Followed by a gradual decrease to a level that is
still higher than that present before treatment
• Clinical improvement develops before decreases
in their IgE antibody
• Whose IgE antibody levels never decrease,
thereby demonstrating that efficacy
Efficacy from immunotherapy is not dependent
on reduction in specific IgE levels
Middleton 8th
Practice parameter

Immunoglobulin G
• Increase serum allergen-specific IgG1 and IgG4
• Competition between IgG4 and IgE antibodies
for binding to the specific allergen
• Block IgE-dependent histamine release
• After stop IT, ↓IgG1 and ↓ IgG4 but clinical
improvement persisted
Not predictive of the duration and degree of
efficacy of immunotherapy

Immunologic response to IT
Middleton 8th

Immunologic response to IT
Middleton 8th
Immunologic tolerance
• Relative decrease in antigen specific
responsiveness, immune deviation, or anergy
• Relative decrease in allergen-specific
responsiveness and by the generation of
CD4+CD25+ regulatory T lymphocytes
• Producing IL-10, TGF-β
Immunologic response to IT
Middleton 8th

Immunologic response to IT
Middleton 8th
Specific allergen
• Effective for pollen, animal allergens, dust mite,
fungi, hymenoptera venom (honeybee, yellow
jacket, hornet, fire ants, wasp)
• Extract selection should be based on
- Hx in correlation with positive allergy skin test
or serum specific IgE Ab
- Clinically relevant allergen with exposure
Practice parameters 3rd JACI 2011

Allergen extracts
Nonstandardized extracts • Vary widely in biologic activity
• Labeled as wt/vol (grams/ml), PNU
– a potency of 1:100 indicates that 1 g of dry allergen (eg, ragweed) was added to 100 ml of a buffer for extraction
– 1 PNU equals 0.01 g of protein nitrogen
• Neither method confers any direct or comparative information about an extract’s biologic potency
• not be considered equipotent
Allergen extracts
Standardized extracts
• Selection of a reference extract
• Selection of an assay or procedure to compare
the manufactured extract with the reference
extract
• More consistent biologic activity
• Less risk of an adverse reaction caused by
extract potency variability
Practice parameters 3rd JACI 2011

Standardized extracts
•Potency of allergen extract by
• US: ID50EAL system Units
– BAU (bioequivalent allergy unit)
– AU (arbitrary units)
• Europe: Nordic system
ID50EAL; intradermal dilution for 50 mm
sum of erythema determines the
bioequivalent allergy units

ID50EAL system
• The quantitative skin test method for BAU
• The dilution that results in erythema size after
serial ID injecting 0.05 mL to 3 fold dilution of the
reference that end point 50 mm of erythema
• Mean D50 is calculated the potency of the
extract
Practice parameters 3rd JACI 2011

Standardized extracts; US-licensed
• Aeroallergen: cat hair, cat pelt, dust mites
(D. pteronyssinus, D. farina), short ragweed,
Bermuda grass, Kentucky bluegrass, perennial
rye grass, orchard grass, timothy grass, meadow
fescue, red top, sweet vernal grass
• Hymenoptera venoms: yellow jacket, wasp
honey bee, yellow hornet, white-faced hornet
Practice parameters 3rd JACI 2011

Principle of mixing allergen
immunotherapy
Consideration of the following:
(1) Cross-reactivity of allergens
(2) The optimal dose of each constituent
(3) Potential interaction between different
types of allergens; proteolytic enzymes
Practice parameters 3rd JACI 2011

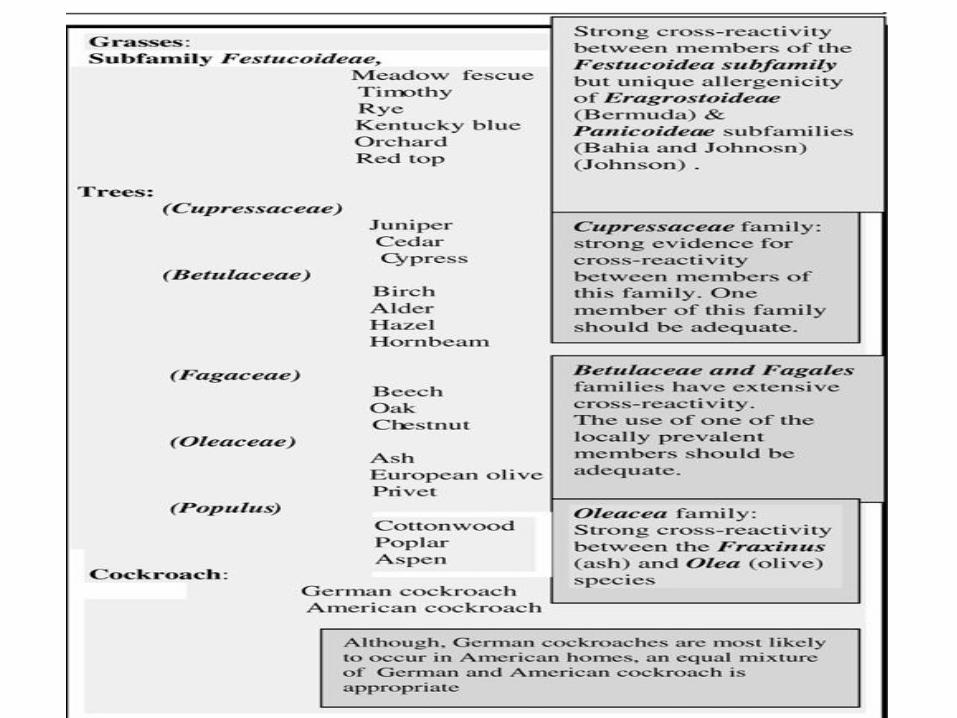
Cross-reactivity of allergen extract
• Limit the number of allergens in a vial to attain
optimal therapeutic doses of each components
• Cross-reactivity is variable for many grass and
weed pollens, their intrinsic allergenicity,
prevalence, and aerobiologic characteristics
within a specific region should be considered
• Single pollen within the cross-reactive genus or
subfamily that are maximally effective
Practice parameters 3rd JACI 2011

Principle of mixing allergen
immunotherapy
Consideration of the following:
(1) Cross-reactivity of allergens
(2) The optimal dose of each constituent
(3) Potential interaction between different
types of allergens; proteolytic enzymes
Practice parameters 3rd JACI 2011

The optimal dose
• The maintenance concentrate vial is the highest
concentration allergy IT vial (1:1 vol/vol)
• The projected effective dose; maintenance goal
• The maintenance dose is the dose that provides
therapeutic efficacy without significant adverse
local or systemic reactions and might not
always reach the initially calculated projected
effective dose
Practice parameters 3rd JACI 2011

The optimal dose
Middleton 8th edition
Optimal maintenance dose:
5-20 mcg of major allergen for
inhalant allergens

Practice parameters 3rd JACI 2011

Potential interaction between different types of allergens
• Many fungal extracts, cockroach extracts
contain proteases that are capable of
degrading the proteins in other extracts
with pollen, house dust mite, and dander
extracts
• not recommended to mix venoms together

Immunotherapy schedules
The build-up phase
• Starting doses: 1000- or 10,000-fold dilution of the maintenance concentrate
• Increasing amounts of the allergen
• 1-3 times a week
• Duration ranges from 3-6 months
The maintenance phase
• Begins when the effective therapeutic dose is reached
• The intervals between the injections are increased
• Every 4-8 weeks for venom
• Every 2-4 weeks for inhalant allergens
Practice parameters 3rd JACI 2011
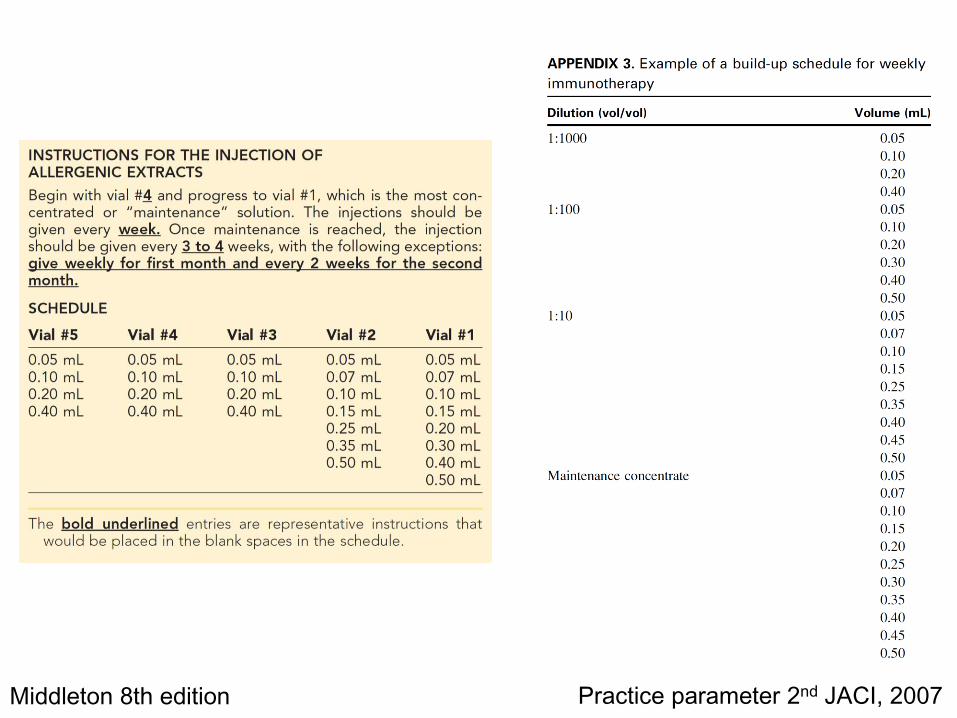
Middleton 8th edition Practice parameter 2nd JACI, 2007

Cluster immunotherapy
• Accelerated build-up schedule
• Several injections at increasing doses (generally 2-3
per visit), 30-min intervals
• Achieved more rapidly within 4 to 8 weeks
• Antihistamine 2 hours before dosing reduced local
and systemic reactions
Middleton 8th edition
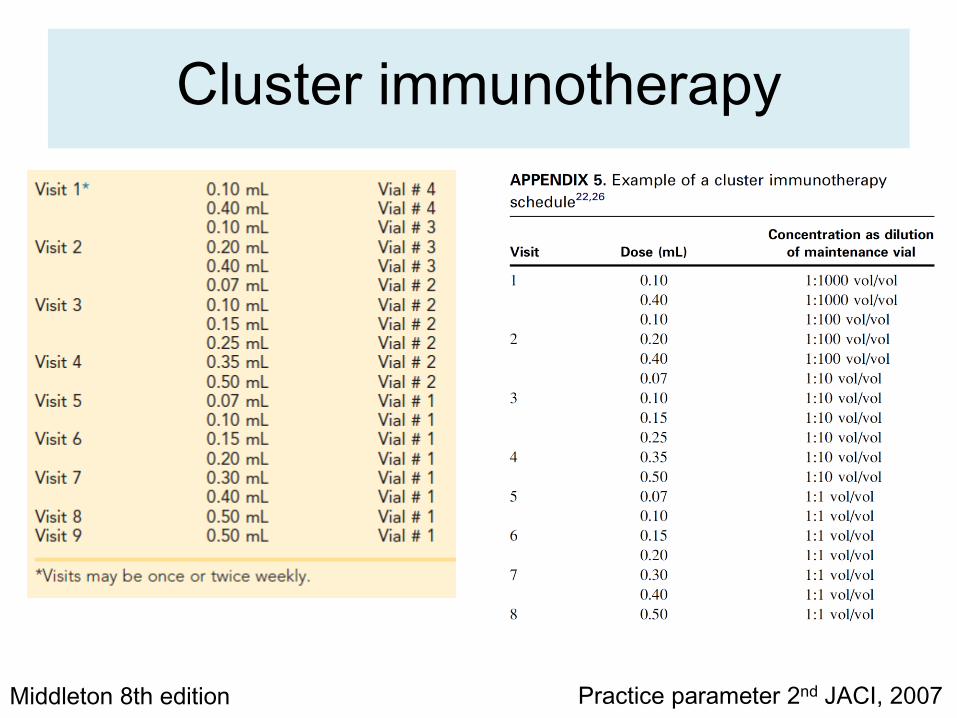
Cluster immunotherapy
Middleton 8th edition Practice parameter 2nd JACI, 2007

Rush immunotherapy
• Increase doses of allergen at intervals 15-60
minutes over 1-3 days until the target
therapeutic dose is achieved
• Inhalant allergens associated with a greater risk
of systemic reactions
• Hymenoptera VIT have not been associated with
a similar high incidence of systemic reactions
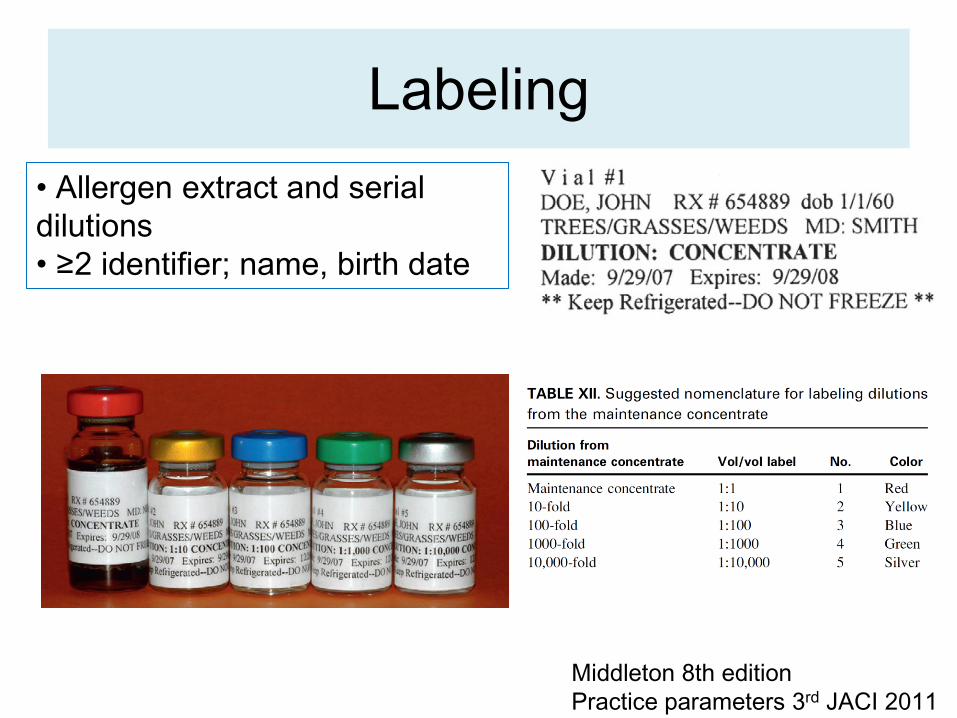
Labeling
Middleton 8th edition
Practice parameters 3rd JACI 2011
• Allergen extract and serial
dilutions
• ≥2 identifier; name, birth date
Duration of treatment
• Clinical improvement shortly after the patient
reaches a maintenance dose
• Evaluated at least every 6 -12 months
• No specific tests or clinical markers to the
relapse and remission after discontinuing IT
• Duration determined by the physician and
patient after considering the risks and benefits
associated with discontinuing or continuing IT
Safety
Local reactions
• Poor predictors of subsequent systemic
reactions at the next injection
• Dose reductions are unnecessary
• Not predict local reactions next injection
Large local reactions
• Defined ≥25 mm
• LLRs not predictive of future systemic reactions,
but 1/3 preceded systemic reactions
• LLRs 25-30 mm: repeat the dose
• LLRs 30-50 mm: reduce the dose for LLRs
Practice parameters 3rd JACI 2011

Systemic reactions
• Less than 1% in conventional IT
• ~34% in some studies of rush IT
• AAAAI fatality rate 1:2.5 million injections
• Most serious systemic reactions occur within 30
minutes after an injection, patients should
remain in the medical clinic for at least 30
minutes after the IT injection
• The dose should be reduced after a systemic
reaction
Dose reductions
• After a systemic reaction
• During periods of exacerbation of symptoms
• When the interval between injections is
prolonged
• New vial
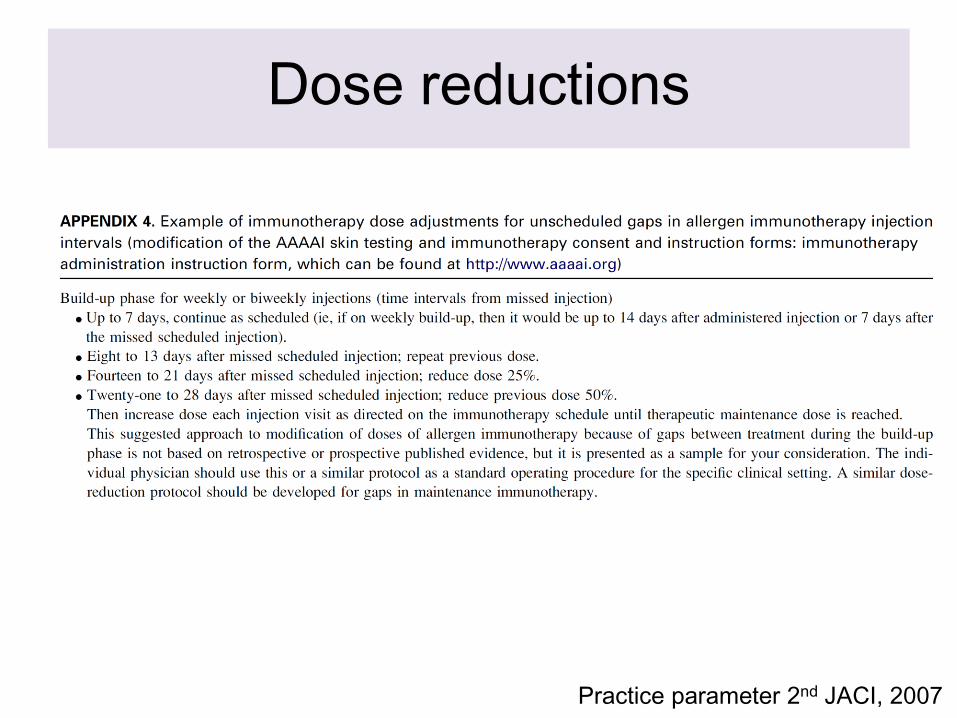
Dose reductions
Practice parameter 2nd JACI, 2007

Premedication
• Reduce the frequency of systemic reactions
caused by conventional IT, cluster IT, rush IT
• Increased the proportion of patients who
achieved the target maintenance dose
Premedication
• Oral nonsedating antihistamine 2 hr before
injection
– reduced the frequency of severe systemic
reactions caused by conventional IT and
increased who achieved the target maintenance
dose
– Reduced severe systemic reactions in cluster,
rush IT
– Decreased large local reactions
Nielsen L, et al. J Allergy Clin Immunol 1996;97:1207-13
Berchtold E, et al. Clin Exp Allergy 1992;22:59-65
Reimers A, et al. Allergy 2000;55:484-8

Premedication
LTRA
• Delays the onset and decreases the size of local reactions during rush VIT
• No controlled studies on the incidence of systemic reactions
Combination pretreatment
• Prednisone, an H1 and H2 histamine receptor antagonist before rush immunotherapy with inhalant allergens reduced a systemic reaction from 73% to 27% of patients
Wohrl S, et al Int Immunol 2007;144:137-42
Portnoy J, et al. Ann Allergy 1994;73:409-18
Shelly M, et al.AAAI 2004;92:414-419

Omalizumab pretreatment
• Fivefold decrease in the risk of anaphylaxis by
the rush immunotherapy
• Reduction in the rate of systemic reactions
during the weekly buildup phase, from 9.7% to
zero
Casale TB, et al. J Allergy Clin Immunol 2006;117:134-40

Omalizumab in combination
• Improve the safety and tolerability of
cluster and rush immunotherapy in
moderate persistent asthma and allergic
rhinitis
• Effective in improving symptom scores
compared with immunotherapy alone
Kopp MV, et al. J Allergy Clin Immuno 2002;110:728-35
Kuehr J, et al. J Allergy Clin Immunol 2002;109:274-80

Allergen selection and
handling

Allergen immunotherapy extract handling
(1) Storage temperature: 4-8oC
(2) Presence of stabilizers and bactericidal agents
(3) Concentration:
– more dilute concentrations, shorter shelf life
(4) Presence of proteolytic enzymes
(5) Volume of the storage vial
(1:1 vol/vol up to 1:10 vol/vol) when kept at 4oC
relatively constant and to be used until the
expiration date on the label
Allergen immunotherapy extract handling
• 0.03% HSA, 50% glycerin to maintain potency
• HSA prevent the loss of potency within storage vials by preventing absorption of allergen on the inner surface of the glass vial
• Glycerin
– preservative
– prevent loss of allergenic potency
– Inhibit the activity of proteolytic and glycosidic enzymes in certain extracts
– Pain when injected if >0.2 ml
• Phenol, preservative to prevent growth of microorganisms
Practice parameters 3rd JACI 2011
Injection techniques
• Wiped with an alcohol to remove gross
contamination from the skin surface
• Calibrated small-volume syringe with a 26- to
27-gauge 1/2 or 3/8-inch nonremovable needle
• Subcutaneously in the posterior portion of the
middle third of the upper arm
Practice parameters 3rd JACI 2011

Special considerations in immunotherapy
Immunotherapy in children
• Effective and well tolerated
• Prevent the new onset of allergen sensitivities or progression to asthma
• Can be initiated in young children
• Indications are similar to those of other age groups
• Difficulty cooperating with an IT program
• Consider the benefits and risks of immunotherapy
• Not considered in infants and toddlers because
– difficulty in communicating with the child regarding systemic reactions
– traumatic injection to very young children

Immunotherapy in Pregnancy
• Can be continued but is usually not initiated in
the pregnant patient
• Discontinuation IT if the pregnancy occurs
during the build-up phase and the pt is receiving
a dose unlikely to be therapeutic