hypertriglyceridemia and acute pancreatitis – how fearful should we
TRANSCRIPT

Hypertriglyceridemia and Acute Pancreatitis – How Fearful Should we be of Pushing the Limits?
Charlie Ramirez, PharmD PGY2 Ambulatory Care Pharmacy Resident South Texas Veterans Health Care System
Pharmacotherapy Grand Rounds
Pharmacotherapy Education and Research Center The University of Texas Health Science Center at San Antonio
The University of Texas at Austin College of Pharmacy September 13, 2013
OBJECTIVES:
1. Describe the pathophysiology and prevalence of hypertriglyceridemia (HTG) 2. Elaborate the potential causes, complications, and management of acute pancreatitis 3. Become familiar with the various classification schemes for HTG 4. Evaluate the management of HTG, including clinical guidelines, pharmacological
therapy, and supportive primary literature 5. Discuss the association between HTG and acute pancreatitis 6. Analyze primary literature surrounding the association between HTG and acute
pancreatitis 7. Determine a safe and effective threshold plasma triglyceride (TG) concentration above
which TG-targeted therapy should be aimed for preventing acute pancreatitis

I. INTRODUCTION Pathophysiology1
A. Lipids i. Lipoproteins
a) Definition: • Macromolecular aggregates (large assemblies) of lipids and
proteins • Soluble form of lipids that circulate in the blood
ii. Lipoprotein Subtypes
Figure 1: Lipoprotein subtypes Source: http://www.scientificpsychic.com/health/lipoproteins.gif
2

Table 1: Lipoprotein characteristics Classification Composition Primary Function Chylomicron TG: 80-95%
Free cholesterol: 1-3% Cholesterol esters: 2-4% Phospholipids: 3-9% Apoproteins: 1-2%
Transport dietary TGs to adipose tissue and muscle for hydrolysis by lipoprotein lipase
Very low-density lipoprotein (VLDL)
TG: 50-65% Free cholesterol: 4-8% Cholesterol esters: 16-22% Phospholipids: 15-20% Apoproteins: 6-10%
Transport endogenous TGs to adipose tissue and muscle for hydrolysis by lipoprotein lipase
Intermediate density lipoprotein (IDL)
Intermediate between VLDL and LDL
Transport endogenous cholesterol for either conversion to LDL or receptor-mediated endocytosis by liver
Low density lipoprotein (LDL)
TG: 4-8% Free cholesterol: 6-8% Cholesterol esters: 45-50% Phospholipids: 18-24% Apoproteins: 18-22%
Transport endogenous cholesterol for receptor-mediated endocytosis by either the liver or extrahepatic tissues
High density lipoprotein (HDL)
TG: 2-7% Free cholesterol: 3-5% Cholesterol esters: 15-20% Phospholipids: 26-32% Apoproteins: 45-55%
Removal of cholesterol from extrahepatic tissues via transfer of cholesterol esters to IDL and LDL
B. Triglyceride (TG) i. Definition:
a) (Triacylglycerol): an ester of glycerol with three fatty acids b) Cellular storage form of fatty acids
ii. Uptake and Transport: a) Plasma TGs are primarily produced by the intestines and liver b) Dietary TGs enter the circulation within chylomicrons c) TGs assembled from de novo synthesized fatty acids and from lipids
returning to the liver are secreted in VLDL Hypertriglyceridemia
A. Prevalence2 i. National Health and Nutrition Examination Survey
a) 1.7% (3.4 million Americans) • 33% of the nearly 6,000 participants (1999 – 2004; 37% men,
30% women) had serum TG ≥ 150 mg/dL o Mild hypertriglyceridemia (150 – 200 mg/dL): 14% o TG 200 – 500 mg/dL: 16% o TG > 500 mg/dL: 2%
ii. Kaiser Permanente b) 1.5%
3
B. Risk factors i. Obesity/overweight
ii. Physical inactivity iii. Cigarette smoking iv. Excess alcohol intake v. High carbohydrate diet (> 60% energy intake)
vi. Several diseases (e.g., type 2 diabetes mellitus, hypothyroidism, chronic renal failure, nephrotic syndrome)
vii. Certain drugs (e.g., corticosteroids, estrogens, retinoids, higher doses of beta-adrenergic blocking agents)
viii. Genetic disorders (e.g., familial combined hyperlipidemia, familial hypertriglyceridemia, familial dysbetalipoproteinemia)
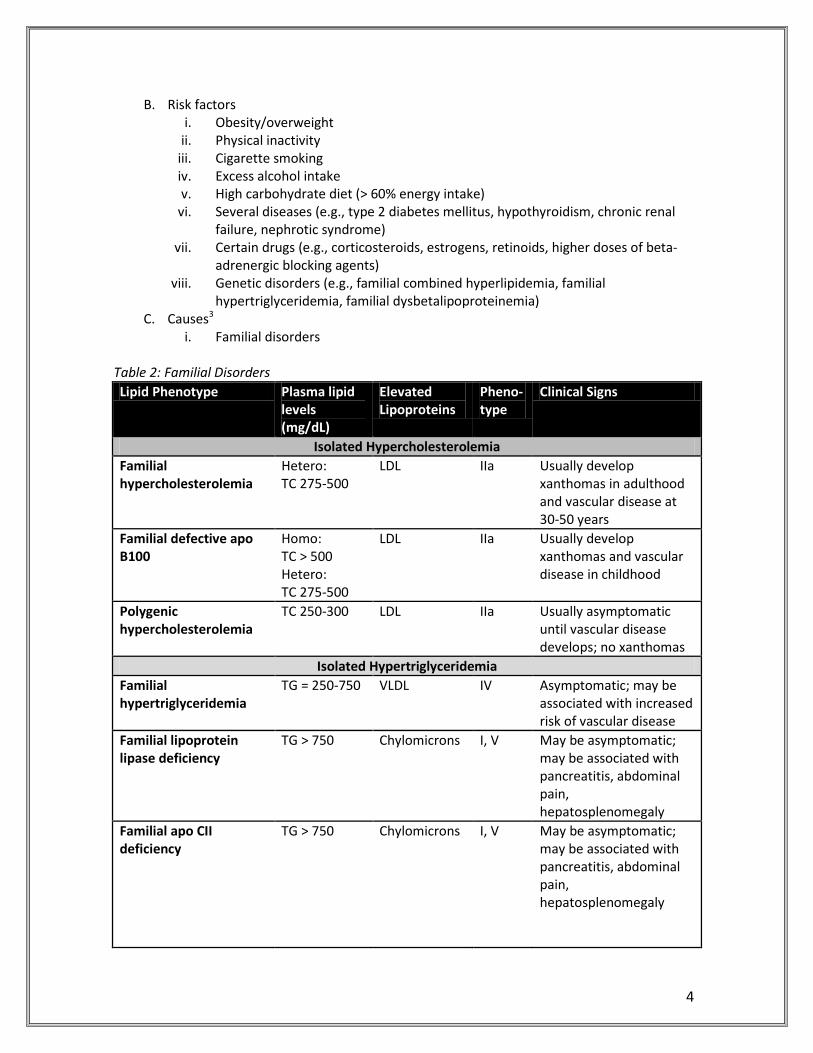
C. Causes3 i. Familial disorders
Table 2: Familial Disorders Lipid Phenotype Plasma lipid
levels (mg/dL)
Elevated Lipoproteins
Pheno- type
Clinical Signs
Isolated Hypercholesterolemia Familial hypercholesterolemia
Hetero: TC 275-500
LDL IIa Usually develop xanthomas in adulthood and vascular disease at 30-50 years
Familial defective apo B100
Homo: TC > 500 Hetero: TC 275-500
LDL IIa Usually develop xanthomas and vascular disease in childhood
Polygenic hypercholesterolemia
TC 250-300 LDL IIa Usually asymptomatic until vascular disease develops; no xanthomas
Isolated Hypertriglyceridemia Familial hypertriglyceridemia
TG = 250-750 VLDL IV Asymptomatic; may be associated with increased risk of vascular disease
Familial lipoprotein lipase deficiency
TG > 750 Chylomicrons I, V May be asymptomatic; may be associated with pancreatitis, abdominal pain, hepatosplenomegaly
Familial apo CII deficiency
TG > 750 Chylomicrons I, V May be asymptomatic; may be associated with pancreatitis, abdominal pain, hepatosplenomegaly
4

Table 2: Familial Disorders (Cont’d) Hypertriglyceridemia and Hypercholesterolemia
Combined hyperlipidemia
TG = 250-750 Total cholesterol = 250 -500
VLDL, LDL IIb Usually asymptomatic until vascular disease develops; familiar form may also present as isolated high TG or an isolated high LDL cholesterol
Dysbetalipoproteinemia TG = 250-500 Total cholesterol = 250 -500
VLDL, IDL LDL normal
III Usually asymptomatic until vascular disease develops; may have palmar or tuboeruptive xanthomas
a) Patients with types I, IV, and V hyperlipidemia (in which HTG is an
association) are predisposed to developing pancreatitis • Majority of adults with familial hyperlipidemia and pancreatitis
would have a type V or IV defect • Types I and V can present with spontaneous pancreatitis in the
absence of a secondary factor • Type IV almost always requires a secondary factor to increase
TG levels substantially b) Type I hyperlipidemia: fasting chylomicronemia4
• Almost always presents in infancy and early childhood • Characteristics:
o Eruptive xanthomas, lipemia retinalis, hepatosplenomegaly, and, although not invariably, acute pancreatitis
• Factors that reduce VLDL clearance can raise TG concentrations because of the competition with chylomicrons for a common saturable removal mechanism
o Genetic hypertriglyceridemia: Rare genetic syndromes:
• LPL deficiency (familial type I), apo CII deficiency, apo AV homozygosity, GPIHBP1
Other genetic syndromes: • Heterozygous apo AV, heterozygous LPL
deficiency, familial hypertriglyceridemia, FCHL, dysbetalipoproteinemia (familial type III)
Typically younger patients presenting with the chylomicronemia syndrome and an increased risk for pancreatitis
5

• Type V phenotype o Complex interaction between genetic (less severe
disorders of TG metabolism) and environmental factors o Fasting chylomicronemia and increased VLDL o TG concentrations exceed 1000 mg/dL and, when
exacerbated by weight gain, certain medications, or metabolic perturbations, can lead to the chylomicronemia syndrome and increased risk of pancreatitis
• Though no single threshold of TG concentration above which pancreatitis may occur, increased risk is defined arbitrarily by levels exceeding 1000 mg/dL
• Chait and Brunzell studied 123 patients referred to their lipid clinic for elevated TG (> 2,000 mg/dL)5
o All patients had a genetic basis for their HTG o 110 out of 123 had an associated secondary factor
contributing to their elevated TG levels o Identifying presence of secondary factors is important
when managing a patient with severe HTG
ii. Obesity4 a) Evidence from epidemiological and controlled clinical trials suggests a
marked relationship between TG levels and body weight status and body fat distribution
Table 3: Association between BMI and Hypertriglyceridemic State
6

D. Complications i. Vascular disease4, 6
Figure 2: Atherogenicity of TG-Rich Lipoproteins
a) Remnant hypothesis: • Conversion of TGs to remnants produces particles that enter the
arterial wall and deposit cholesterol b) Lipolytic toxin hypothesis:
• During lipolysis of TGs, inflammatory lipids are released that alter the endothelial biology
• Such inflammatory lipids increase expression of adhesion molecules and cytokines that promote coagulation
ii. Acute pancreatitis3
a) Etiology • Prevalence: < 1% in the United States • Approximately six per 100,000 populations will develop chronic
pancreatitis
Table 4: Causes of Acute Pancreatitis Common Causes
Gallstones (including microlithiasis)* Alcohol (acute and chronic alcoholism)* Hypertriglyceridemia Endoscopic retrograde cholangiopancreatography (ERCP), especially after biliary manometry Trauma (especially blunt abdominal trauma) Postoperative (abdominal and non-abdominal operations) Drugs (azathioprine, 6-mercaptopurine, sulfonamides, estrogens, tetracycline, valproic acid, anti-HIV medications) Sphincter of Oddi dysfunction
7

Table 4: Causes of Acute Pancreatitis (Cont’d) Uncommon Causes
Vascular causes and vasculitis (ischemic-hypoperfusion states after cardiac surgery) Connective tissue disorders and thrombotic thrombocytopenic purpura (TTP) Cancer of the pancreas/hereditary pancreatitis Hypercalcemia Periampullary diverticulum Pancreas divisum Cystic fibrosis Renal failure
Rare Causes Infections (mumps, coxsackievirus, cytomegalovirus, echovirus, parasites) Autoimmune (e.g., Sjorgen’s syndrome)
Causes to Consider in Patients with Recurrent Bouts of Acute Pancreatitis without an Obvious Etiology
Occult disease of the biliary tree or pancreatic ducts, especially microlithiasis, sludge drugs Hypertriglyceridemia Pancreas divisum Pancreatic cancer Sphincter of Oddi dysfunction Cystic fibrosis *Most common causes in the United States
b) Pathophysiology • Premature activation of trypsinogen to trypsin within the
pancreas, leading to activation of other digestive enzymes and autodigestion of the gland
• Activated enzymes released into the pancreas and surrounding tissues produce damage and necrosis of the pancreatic tissue, surrounding fat, vascular endothelium, and adjacent structures
• Release of cytokines by acinar cells injures those cells and enhances the inflammatory response
8
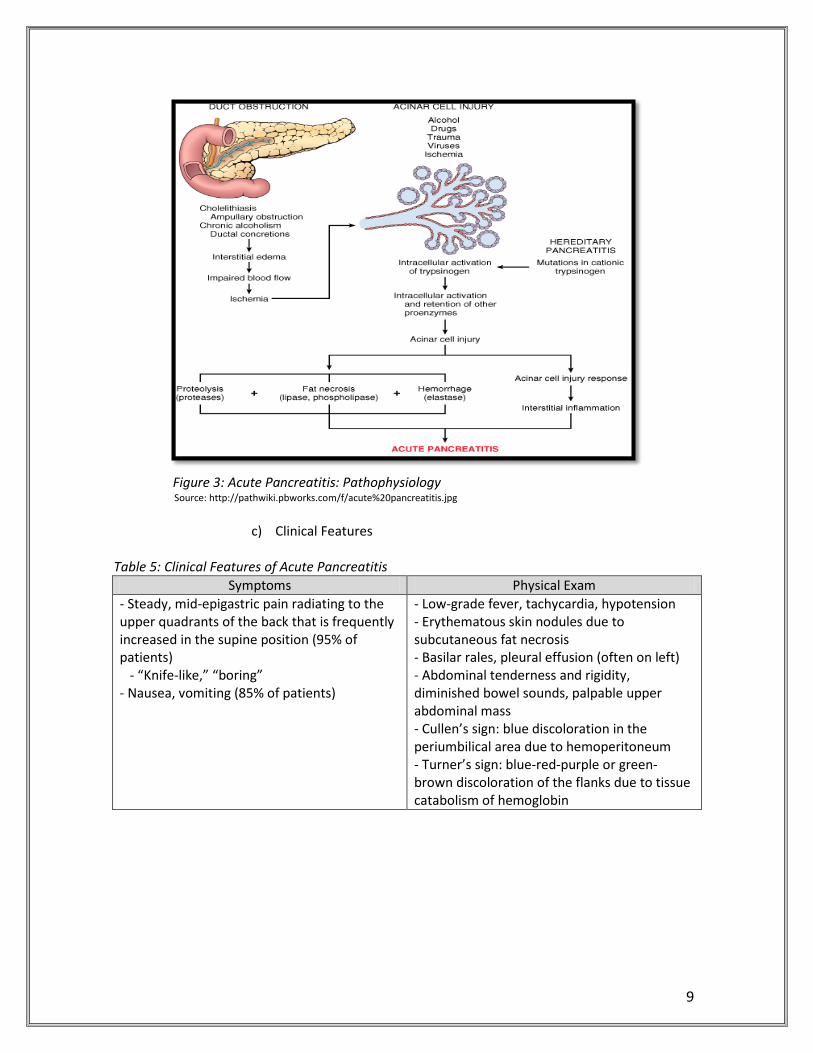
Figure 3: Acute Pancreatitis: Pathophysiology Source: http://pathwiki.pbworks.com/f/acute%20pancreatitis.jpg
c) Clinical Features
Table 5: Clinical Features of Acute Pancreatitis Symptoms Physical Exam
- Steady, mid-epigastric pain radiating to the upper quadrants of the back that is frequently increased in the supine position (95% of patients) - “Knife-like,” “boring” - Nausea, vomiting (85% of patients)
- Low-grade fever, tachycardia, hypotension - Erythematous skin nodules due to subcutaneous fat necrosis - Basilar rales, pleural effusion (often on left) - Abdominal tenderness and rigidity, diminished bowel sounds, palpable upper abdominal mass - Cullen’s sign: blue discoloration in the periumbilical area due to hemoperitoneum - Turner’s sign: blue-red-purple or green-brown discoloration of the flanks due to tissue catabolism of hemoglobin
9

d) Laboratory findings • Serum amylase:
o > 3 x ULN o Typically return to normal in 48-72 hours
• Serum lipase: o > 3 x ULN o Increases in parallel with serum amylase level
• Hypocalcemia (25% of patients) • Hyperglycemia • Hypoalbuminemia • Leukocytosis: 15,000-20,000/µL • Hypertriglyceridemia (15-20% of patients) • Transient elevations: serum bilirubin, alkaline phosphatase,
aspartame aminotransferase • Hypoxemia (25% of patients)
e) Imaging
• Abdominal radiographs: abnormal in 30-50% of patients (not specific for pancreatitis)
• Abdominal computerized tomography (CT) scan
f) Diagnosis • Should be made within 48 hours • Characteristics of abdominal pain + elevations of amylase,
lipase, or both to at least 3 X ULN
g) Treatment
Figure 4: Treatment Algorithm: Acute Pancreatitis
10

h) Complications
Table 6: Complications of Acute Pancreatitis Systemic
Shock, GI bleeding, common duct obstruction, ileus, splenic infarction or rupture, DIC, subcutaneous fat necrosis, ARDS, pleural effusion, acute renal failure, sudden blindness
Local - Pancreatic necrosis:
• Necrosis may become secondarily infected in 40-60% of patients • Typically 1-2 weeks after the onset of pancreatitis • Most frequent organisms: gram-negative bacteria of alimentary origin
- Pancreatic pseudocysts: • Occurs in 15% of patients • Typically develops over 1-4 weeks • Abdominal pain is the usual complaint +/- upper abdominal mass • Can be detected by abdominal ultrasound or CT scan
- Pancreatic abscess: • Ill-defined liquid collection of pus that evolves over 4-6 weeks
- Pancreatic ascites and pleural effusions: • Disruption of the main pancreatic duct
i) Risk factors that adversely affect survival
• Associated with organ failure and/or local complications such as necrosis
• Clinical manifestations o Obesity (BMI > 30) o Hemoconcentration (hematocrit > 44%) o Age > 70
• Organ failure o Shock o Pulmonary insufficiency (oxygen partial pressure [PO2] <
60) o Renal failure (CR > 2.0 mg/dL) o GI bleeding
• ≥ 3 Ransom criteria (not fully utilizable until 48h) • Apache II score > 8
11

II. CLASSIFICATION OF HYPERTRIGLYCERIDEMIA7
National Cholesterol Education Program Adult Treatment Panel III (ATP III) Normal TGs < 150 mg/dL Borderline-high TGs 150 – 199 mg/dL High TGs 200 – 499 mg/dL Very high TGs ≥ 500 mg/dL
The Endocrine Society Clinical Practice Guideline Normal < 150 mg/dL Mild hypertriglyceridemia 150 – 199 mg/dL Moderate hypertriglyceridemia 200 – 999 mg/dL Severe hypertriglyceridemia* 1000 – 1999 mg/dL Very severe hypertriglyceridemia ≥ 2000 mg/dL
*Severe hypertriglyceridemia, although not causative of pancreatitis, indicates risk for development of severe hypertriglyceridemia
III. MANAGEMENT OF HYPERTRIGLYCERIDEMIA General principle: accurate measurement of TG requires fasting for 9-12 hours prior to the test
A. VA/DoD Lipid Guidelines8
TG >200-499 mg/dL TG ≥500 mg/dL TG > 1000 mg/dL • Lifestyle management • Weight loss • Alcohol cessation • Secondary causes
• Very low fat diet • Low concentrated
carbohydrate diet • Alcohol cessation • Secondary causes • Consider drugs, if no
response to above • Consider referral
• Strict MNT (avoidance of alcohol, fat, and restrict calories)
• Secondary causes • Drug therapy, if no
response to above • Consider referral
*MNT (Medical nutrition therapy)
B. ATPIII Guidelines9 TG 150-199 mg/dL TG 200-499 mg/dL TG ≥ 500 mg/dL
• Life habit changes: o Body weight
control o Regular physical
activity o Smoking cessation
• Restriction of alcohol use (when consumed in excess)
• Avoid high carbohydrate intakes (> 60% of calories)
First-line therapy: • Weight reduction • Increased physical activity Second-line therapy (drugs to achieve non-HDL goal): • Statins (LDL, VLDL) • Fibrates (VLDL-TG, VLDL) • Nicotinic acid (LDL, VLDL)
TG lowering to prevent pancreatitis: • Very low-fat diet when TG
> 1000 mg/dL (< 15% of total calories as fat)
• Institute weight reduction/physical activity
• Fish oils (replace some long-change TGs in diet)
• TG-lowering drugs (fibrate or nicotinic acid)
12

C. The Endocrine Society Clinical Practice Guideline7 TG 150-999 mg/dL TG ≥ 1000 mg/dL
Lifestyle therapy:
• Dietary counseling • Decreased carbohydrate intake, increased
fat (monounsaturated/poly-unsaturated) intake
• Increased physical activity • 30 – 60 minutes of intermittent aerobic
exercise or mild resistance exercise • Weight reduction
Combination of reduction of dietary fat/simple carbohydrate intake with drug treatment • Recommend fibrate be used as first-line
agent for reduction of TG in patients at risk for TG-induced pancreatitis
• Recommend three drug classes (fibrates, niacin, n-3 fatty acids) alone or in combination with statins be considered as treatment options in patients with moderate to severe TG levels
Evidence8
Table 7: Summary of Evidence for TG-Lowering Modalities Recommendation Source of Evidence QE Overall Quality R
Elevated TG should receive intensive MNT, exercise, and screening for underlying causes
NCEP ATP-III, 2002 Stone & Blum, 2002
II-3 Fair B
Consider drug therapy to prevent pancreatitis
Cleeman, 1998 NCEP ATP-III, 2002 Stone & Blum, 2002
III Poor I
Use of fibrates, niacin, and fish oil to lower hypertriglyceridemia
Farmer et al., 2001 Harris, 1997
I Fair B
QE = quality of evidence R = Recommendation Pharmacologic Therapy8
A. Fibrates i. MOA:
- Bind to PPARs (peroxisome proliferator-activated receptors), which help regulate lipid metabolism - Increase expression of lipoprotein lipase decreased triacylglycerides
13

ii. Drugs: Agent Dose Gemfibrozil 1200 mg/day (divided BID before meals) Fenofibrate 160-200 mg/day
iii. Potential Adverse Effects:
a) GI symptoms (nausea [2.3%], abdominal pain [4.6%], vomiting, diarrhea [2.3%]), rash, hepatitis, gallstones, myopathy [3.4%], and rhabdomyolysis [3%])
iv. Precautions/Contraindications/Comments: a) Gallbladder disease b) Monitor LFTs throughout therapy; contraindicated in hepatic disease c) Reduce dose in modest renal insufficiency; contraindicated in severe
renal dysfunction d) Risk of myopathy/rhabdomyolysis increases when combined with
statins e) Monitor INR; may need to adjust warfarin dosage to prevent bleeding
complications
B. Nicotinic acid i. MOA:
ii. Drugs:
Agent Dose Niacin ER 500 mg – 2 g daily at bedtime Niacin IR 1.5 – 3 g/day (divided TID)
Start IR 50-100 mg BID – TID Increase dose by 300 mg/day per week
iii. Potential Adverse Effects:
a) Flushing [88%], blurred vision, GI distress [2-9%], itching, headache, hepatotoxicity, hyperglycemia, hyperuricemia
- Inhibit lipolysis in adipose tissue, the primary producer of circulating free fatty acids (precursor to triacylglycerol synthesis) - Lowering of VLDL synthesis
14

iv. Precautions/Contraindications/Comments: a) Hepatic disease; persistent elevation of LFTs b) Monitor LFTs at baseline; 6-12 weeks after start or dosage change; monitor
every 6-12 months thereafter c) Active peptic ulcer disease (PUD); avoid in patients with a documented
history of PUD d) Arterial bleeding e) May cause glucose intolerance; caution in DM f) Decreases urinary secretion of uric acid, caution with gout g) Take with food to avoid flushing or GI upset h) ASA 30 minutes prior to dose may minimize flushing
C. Fish oil
i. MOA: Lower fasting and postprandial TG levels in a dose-dependent fashion ii. Drugs:
Agent Dose Omega-3 fatty acid 2-4 g daily or in divided doses Lovaza (omega-3 ethyl ester) 4 g daily or in divided doses
iii. Potential Adverse Effects
a) GI (nausea [3%], eructation [4%], and taste perversion or fishy taste [4%]) b) LDL-C elevation (especially in those with very high TG and no concomitant
statin) c) ALT elevation
iv. Precautions/Contraindications/Comments: a) Drug to drug interaction with anticoagulants b) ALT should be checked at baseline and 6-12 weeks after initiation of fish oils
and periodically thereafter c) Lipid panel, including TG and LDL-C should be checked within 6-12 weeks of
initiation of treatment Efficacy8
A. As monotherapy, fibrates offer the most TG reduction, followed by immediate-release niacin, omega-3 methyl esters, extended-release niacin, statins, and ezetimibe4
i. Non-Statins
Drug Expected % Reduction in TG Fibrates -20 to -50 Niacin -20 to -35 Fish oil -20 to -30
15

ii. Statins10
Statin Rosuvastatin Atorvastatin Simvastatin Pravastatin
10mg 19.8% 20% 11.9% 8.2% 20mg 23.7% 22.6% 17.6% 7.7% 40mg 26.1% 26.8% 14.8% 13.2% 80mg - 28.2% 18.2% -
B. Fibrates have more commonly been shown to provide greater benefit in subgroups with
increased TG levels4
Table 8: Summary of Evidence for Fibrate Therapy Trial Name Population Duration
(years) Intervention
(n) Baseline
TG Follow-Up TG
Primary Endpoint
Helsinki Heart Study
Primary 5 Placebo (2030) Gemfibrozil (2051)
176.7 175.3
177.7 114.8
Fatal/non-fatal MI and cardiac death: Yes NNT 71
Benzafibrate Infarction Prevention Study
Stable CHD 6.2 Placebo (1542) Benzafibrate (1548)
145 145
149.6 124.4
Fatal/non-fatal MI or sudden death: No
Fenofibrate Intervention and Event Lowering in Diabetes Study
High Risk 5 Placebo (4900) Fenofibrate (4895)
153.3 154.2
165.7 130.2
First occurrence of either non-fatal MI or death from coronary heart disease: No
Veterans Affairs HDL Intervention Trial
Stable CHD 5.1 Placebo (1267) Gemfibrozil (1264)
160 161
166 115
Non-fatal MI and death from coronary heart disease: Yes NNT 23
Diabetes Atherosclerosis Intervention Study
Stable CHD 3 Placebo (211) Fenofibrate (207)
214.4 229.5
Not reported
Change in mean lumen diameter: No
Action to Control Cardiovascular Risk in Diabetes
Primary Prevention
4.7 Placebo + simva (2753) Fenofibrate + simva (2765)
162 164
152 120
Composite of the first event of death from CHD, non-fatal MI, ischemic stroke, hospitalization, ACS, or symptom-driven coronary or cerebral revascularization: No
Note: Benefit was shown in the subgroup with elevated TG levels (> 204 mg/dL) and low HDL (<34 mg/dL)
16

C. In patients with HTG, statin therapy may be beneficial in the setting of an LDL-C level that merits treatment4,8
i. If further TG lowering is required, addition of niacin or fish oils may be considered for additional lowering (although there are no clinical endpoint trials examining the combination of statins plus fish oils)
D. Discourage the use of statin-fibrate combination for synergistic TG lowering10 i. Health outcomes
a) The Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial lacked evidence to support a greater benefit in health outcomes with combination therapy versus a statin alone11
ii. Pharmacokinetics a) Gemfibrozil has been found to significantly increase the AUC and Cmax of
lovastatin, simvastatin, pravastatin and rosuvastatin b) Fenofibrate has been noted to cause a “small increase” in AUC and Cmax
when combined with pravastatin and rosuvastatin, though data is only available for these two statins
iii. Adverse Effects a) Risk for muscle toxicity with combination therapy is greater than that for
either statins or fibrates alone b) One systematic review reported (out of 1,674 patients) two patients (0.12%)
experiencing myopathy (myalgia with creatinine kinase > 10 time the upper limit of normal) and 33 patients (1.9%) developing other muscle-related symptoms, including myalgias, myositis, muscle weakness, or musculoskeletal pain
E. Discourage the use of ezetimibe-fibrate combination for synergistic TG lowering8 i. Aside from LDL lowering, there is no evidence to support a reduction in
cardiovascular events with ezetimibe when used alone for primary or secondary prevention of coronary heart disease
ii. Ezetimibe should not be used in combination with statins or fenofibrates due to increases in transaminases
IV. ASSOCIATION BETWEEN HYPERTRIGLYCERIDEMIA AND ACUTE PANCREATITIS
A. The association of hypertriglyceridemia with cardiovascular events and pancreatitis: a
systematic review and meta-analysis12 i. Eligibility criteria:
a) Randomized and observational studies b) Patients enrolled with untreated hypertriglyceridemia and a reported
relative association measure between fasting serum TG levels and the outcomes of interest
ii. Exclusion criteria: a) Uncontrolled studies b) Studies of non-fasting hypertriglyceridemia
iii. Outcomes of interest: a) All-cause mortality b) Cardiovascular death and events c) Pancreatitis
17
iv. Results: a) Total number of included studies: 35 b) Hypertriglyceridemia was significantly associated with cardiovascular death,
cardiovascular events, myocardial infarction, and pancreatitis; with odds ratios (95% confidence interval) of 1.8 (1.31 – 2.49), 1.37 (1.23 – 1.53), 1.31 (1.15 – 1.49), and 3.96 (1.27 – 12.34), respectively
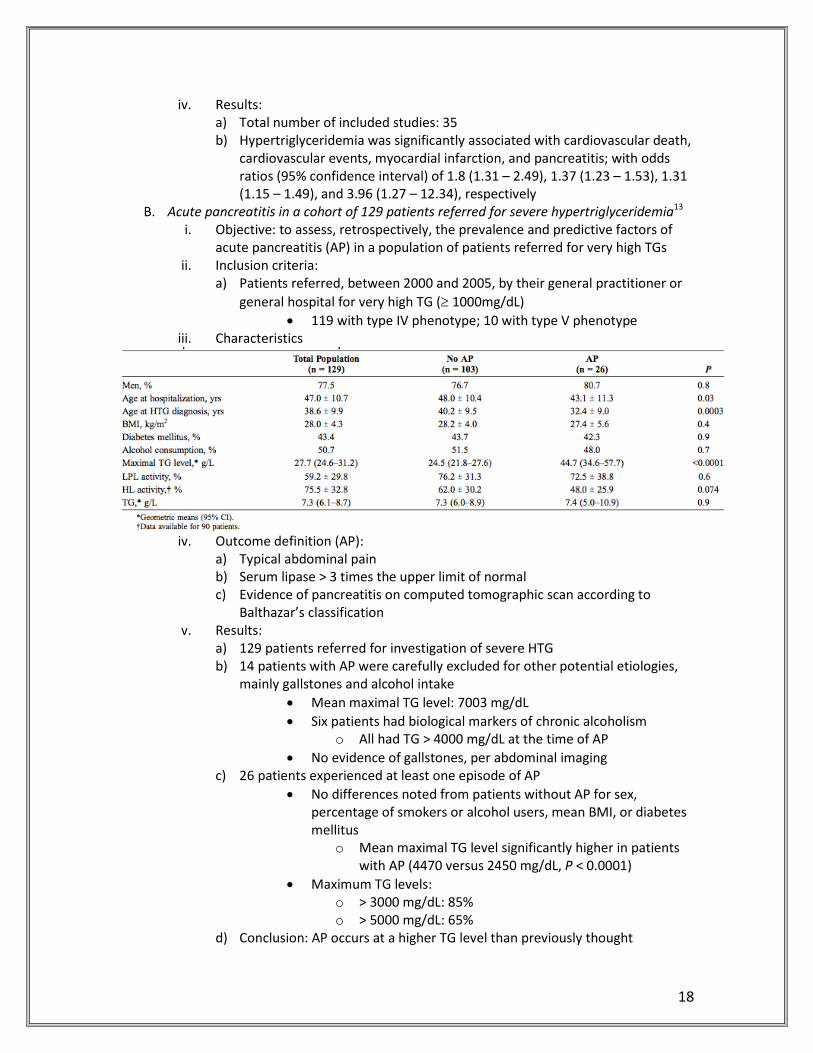
B. Acute pancreatitis in a cohort of 129 patients referred for severe hypertriglyceridemia13 i. Objective: to assess, retrospectively, the prevalence and predictive factors of
acute pancreatitis (AP) in a population of patients referred for very high TGs ii. Inclusion criteria:
a) Patients referred, between 2000 and 2005, by their general practitioner or general hospital for very high TG (≥ 1000mg/dL)
• 119 with type IV phenotype; 10 with type V phenotype iii. Characteristics
iv. Outcome definition (AP):
a) Typical abdominal pain b) Serum lipase > 3 times the upper limit of normal c) Evidence of pancreatitis on computed tomographic scan according to
Balthazar’s classification v. Results:
a) 129 patients referred for investigation of severe HTG b) 14 patients with AP were carefully excluded for other potential etiologies,
mainly gallstones and alcohol intake • Mean maximal TG level: 7003 mg/dL • Six patients had biological markers of chronic alcoholism
o All had TG > 4000 mg/dL at the time of AP • No evidence of gallstones, per abdominal imaging
c) 26 patients experienced at least one episode of AP • No differences noted from patients without AP for sex,
percentage of smokers or alcohol users, mean BMI, or diabetes mellitus
o Mean maximal TG level significantly higher in patients with AP (4470 versus 2450 mg/dL, P < 0.0001)
• Maximum TG levels: o > 3000 mg/dL: 85% o > 5000 mg/dL: 65%
d) Conclusion: AP occurs at a higher TG level than previously thought
18

V. PRIMARY LITERATURE: ACUTE PANCREATITIS Sandhu S, Al-Sarraf A, Taraboanta C, Frohlich J, Francis GA. Incidence of pancreatitis, secondary causes, and treatment of patients referred to a specialty lipid clinic with severe hypertriglyceridemia: a retrospective cohort study. Lipids Health Dis. 2011;10:157.14 Objective Determine the frequency of physical signs and symptoms of high TGs, including
pancreatitis, among patients with severe hypertriglyceridemia Inclusion Criteria
Patients with severe hypertriglyceridemia (TG > 1772 mg/dL) referred to a specialty lipid disorders clinic between 1986 to 2007 (n = 95)
Methods Retrospective chart review Statistical Analysis
- Cohort’s characteristics: mean and standard deviation for continuous variables - Means compared using paired Student t tests
Outcomes 1. Frequency of classical signs and symptoms associated with severe hypertriglyceridemia
2. Most common secondary factors contributing to TG > 1772 mg/dL 3. Differences in treatment for severe hypertriglyceridemia between referring
physicians and lipid clinic specialists 4. Changes in the lipid profile of patients with severe hypertriglyceridemia
followed at a specialty clinic Results
History of Pancreatitis (n = 15) TG Levels - Time of non-acute presentation (mean): 3377 mg/dL
- Lowest level associated with prior pancreatitis: 1815 mg/dL Cohort of 91 patients with TG levels between 886-1771 mg/dL: - 3 patients with a history of pancreatitis - All levels at the time of acute pancreatitis > 1771 mg/dL
Risk Factors - 75 patients (78.9%) had high fat (>35%) and carbohydrate intake (>55% total calories) - 42 patients (49.4%) had no regular exercise - 11 patients (11.6%) consumed > 14 alcoholic drinks/week - 8 patients (8.4%) consumed 7-14 drinks/week - Of the 15 (17.1%) of patients with hypothyroidism, 5 were inadequately controlled - 24 patients (25.3%) had smoked cigarettes within the past year - 16 patients (16.9%) were on beta-blockers, 6 (6.4%) were on estrogen therapy, 4 (4.3%) were on anti-retroviral therapy, and 3 (3.2%) were on a thiazide diuretic - BMI (kg/m2): - > 30: 45 (47.4%) - 25-30: additional 29.5% - Dysglycemia: - 30 patients (31.6%) had a prior diagnosis of diabetes mellitus (DM) - 23 had poor control (FBS 179 ± 79 mg/dL)
19

Medication Use Upon Arrival Clinic
Treatment Latest Visit
n (%) n (%) n (%) Monotherapy
Fibrate 17 (17.9) 54 (56.8) 31 (36.9) Statin 16 (16.8) 1 (1.1) 6 (7.1) Fish oil 1 (1.1) 8 (8.4) 3 (3.6) Niacin 1 (1.1) 0 2 (2.4) Resin 1 (1.1) 0 1 (1.2)
Combination
Fibrate/statin 4 (4.2) 9 (9.5) 11 (13.1) Fibrate/ niacin/ fish oil
1 (1.1) 1 (1.1) 1 (1.20
Fibrate/ fish oil
1 (1.1) 16 (16.8) 4 (4.8)
Other 0 2 (2.2) 17 (20.02) Frequency of Clinical Findings
n/N % Body Mass Index
> 30 kg/m2 45/95 47.4 25 – 30 kg/m2 28/95 29.5 < 25 kg/m2 22/95 23.2
Dermatological
Eruptive xanthomas 8/95 8.5 Palmar xanthomas 3/95 3.2
Ophthamalogical Corneal arcus 24/95 25.3 Lipemia retinalis 2/95 2.1
Gastrointestinal Abdominal tenderness
3/95 3.2
Hepatomegaly 6/95 6.3 Discussion - Acute pancreatitis, as a consequence of HTG, occurs rarely unless TG > 1772
mg/dL - Most common risk factors predisposing to HTG: high fat and carbohydrate diet, physical inactivity, and obesity - Most common co-morbidities: uncontrolled DM and hypothyroidism
Miller A, Lees RS, McCluskey MA, Warshaw AL. The natural history and surgical significance of hyperlipemic abdominal crisis. Ann Surg. 1979;190: 401-8.15 Methods - 35 patients with proven Type V hyperlipoproteinemia investigated and treated
at the Arteriosclerosis Center, Massachusetts Institute of Technology, between the years 1969-1978 - Diagnosis of acute pancreatitis: - Clinical characteristics ± - Laboratory features (elevation of serum amylase or depression of calcium)
20

Results - 19 patients: multiple episodes of abdominal pain ± attacks of pancreatitis A) Pancreatitis as the initial manifestation B) Multiple episodes of abdominal pain of varying severity preceding one or more attacks of acute pancreatitis C) Multiple episodes of abdominal pain (similar to those in group B), without progression to acute pancreatitis Highest mean pre-treatment TG plasma TGs (mg/dL): A) 2030 B) 6127 C) 6017
Patient Cholesterol (mg/dL) Triglycerides (mg/dL) 19 1071 8400 23 1420 7100 25 486 6790 29 548 10800 35 764 11371
Milder episodes of abdominal discomfort (not requiring urgent medical attention) were associated with TGs in the range of 2000-5000 mg/dL - 16 patients: no history of abdominal pain or pancreatitis
Discussion - Clinical manifestations of Type V hyperlipoproteinemia are directly related to the patients’ plasma lipid concentrations - Patients presenting with severe abdominal pain or pancreatitis all had TGs > 6000 mg/dL - Lesser attacks were associated with plasma TGs between 2000-5000 mg/dL - Although it was not possible to identify a threshold plasma TG concentration above which pain inevitably occurred, it was possible to specify a concentration below which pain did not occur, approximately 2000 mg/dL
Fortson MR, Freedman SN, Webster PD 3rd. Clinical assessment of hyper-lipidemic pancreatitis. Am J Gastroenterol.16 Objectives Three questions:
1. What is the clinical syndrome of pancreatitis secondary to hyperlipidemia? 2. What is the role of alcohol, diabetes, or other known causes of HTG in such
patients? 3. Does the course of pancreatitis secondary to HTG differ from that of other
etiologies?
21

Methods - Retrospective chart review (n = 70) - Inclusion criteria: Patients discharged between 1982 and 1994 with a diagnosis of pancreatitis and HTG with: - Clinical presentation consistent with acute pancreatitis - Elevated amylase and lipase or evidence of pancreatitis by ultrasound, CT imaging, or surgery - Serum TG levels or lipemic serum documented shortly after admission Participating hospitals: Medical College of Georgia Hospital (MCGH), the Veterans Affairs Medical Center (VAMC), The University Hospital (UV), and St. Joseph’s Hospital (SJH), Augusta, Georgia
Group A Group B - All 70 patients - Data only from the first hospital admission
- 18 patients who received their entire treatment at the MCGH
Results Frequency of HLP as an Etiology of Pancreatitis Cases HLP/100 Patients with
Pancreatitis (%) MCGH 33 3.8 VAMC 14 1.4 University Hospital 18 1.3 St. Joseph Hospital 5 3.5 Total Cases 70
Admission Findings (%) Abdominal pain Nausea/vomiting Lipemic serum Shock/critical MICU admission Overweight Obese
100 91 45 21 32 80 68
Laboratory Data Mean ± SD Median Range TGs (mg/dL) 4587 ± 3616 3300 600 – 17,770 Serum amylase* 600 ± 698 309 17 – 3,250 Serum lipase** 386 ± 1113 100 12 – 4,980 * > 2 x ULN: 54% > 5 x ULN: 31% ** > 2 x ULN: 67% > 5 x ULN: 27%
Discussion - The frequency of hyperlipidemia as an etiological factor in patients with pancreatitis ranged from 1.3 to 3.5% - No patients with hyperlipidemic pancreatitis had admission TG levels lower than 1000 mg/dL
22

VI. CONCLUSIONS
A. Hypertriglyceridemia poses a potential, yet controversial, risk for contributing to the development of acute pancreatitis
B. Supportive primary literature consists primarily of retrospective analyses i. Majority of subjects evaluated possessed genetic pre-dispositions for HTG
C. Acute pancreatitis, as a consequence of HTG, occurs rarely unless TG > 1772 mg/dL i. When retrospectively evaluating patients discharged with a diagnosis of
pancreatitis and HTG, the frequency of hyperlipidemia as an etiological factor ranged from 1.3 to 3.5%
ii. Most common risk factors predisposing to HTG: high fat and carbohydrate diet, physical inactivity, and obesity
D. Most common co-morbidities associated with acute pancreatitis: uncontrolled DM and hypothyroidism
VII. RECOMMENDATIONS
A. Given supportive literature, recommend TG-targeted therapy when TGs ≥ 1000mg/dL
for prevention of acute pancreatitis B. Given lack of head-to-head evidence, recommend fibrates as first-line therapy for
reduction of TG, when no indication for statin therapy is present i. Recommend statin monotherapy in the setting of an LDL-C level that merits
treatment or when statin indication is present a) If additional TG lowering is required, recommend addition of niacin or fish
oils
23

References:
1. Talbert RL. Chapter 28. Dyslipidemia. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM, eds. Pharmacotherapy: A Pathophysiologic Approach. 8th ed. New York: McGraw-Hill; 2011. http://www.accesspharmacy.com/content.aspx?aID=7974214. Accessed September 4, 2013
2. Lederle F, Bloomfield H. Drug treatment of asymptomatic hypertriglyceridemia to prevent pancreatitis: where is the evidence? Annals of Internal Medicine. 2012; 157(9); 662-665.
3. Fauci A, Braunwald E, Kasper D, et al. Harrison’s Manual of Medicine. 17th ed. New York: McGraw-Hill; 2009.
4. Miller M, Stone N, Ballantyne C, et al. Triglycerides and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2011; 123: 2292-2333.
5. Yadav D, Pitchumoni C. Issues in hyperlipidemic pancreatitis. J Clin Gastroenterol. 2003; 26(1): 54-62.
6. Goldberg I, Eckel R, McPherson R. Triglycerides and heart disease: still a hypothesis? Arterioscler Thromb Vasc Biol. 2011; 31:1716-1725
7. Berglund M, Brunzell J, Goldberg A, et al. Evaluation and treatment of hypertriglyceridemia: an endocrine society clinical practice guidelines. J Clin Endocrinol Metab. September 2012, 97: 2969–2989.
8. The Management of Dyslipidemia- Working Group. VA/DoD Clinical Practice Guideline for the Management of Dyslipidemia.
9. National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Pro- gram (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002; 106:3143-421.
10. Jones P, Davidson M, Stein E, et al. Comparison of the efficacy and safety of rosuvastatin versus atorvastatin, simvastatin, and pravastatin across doses. Am J Cardiol. 2003; 92(2):152-60.
11. Statin-Fibrate Report: Focus on Safety. VHA Pharmacy Benefits Management-Strategic Healthcare Group and The Medical Advisory Panel.
12. The ACCORD Study Group. Effects of combination lipid therapy in type 2 diabetes mellitus. N Engl J Med. 2010; 362:1563-1574.
13. Murad M, Hazem A, Coto-Yglesias F, et al. The association of hypertriglyceridemia with cardiovascular events and pancreatitis: a systematic review and meta-analysis. BMC Endocrine Disorders 2012, 12:2.
14. Linares C, Pelletier A, Czernichow S, et al. Pancreatitis in a cohort of 129 patients referred for severe hypertriglyceridemia. Pancreas 2008; 37:13Y18
15. Sandhu S, Al-Sarraf A, Taraboanta C, Frohlich J, Francis GA. Incidence of pancreatitis, secondary causes, and treatment of patients referred to a specialty lipid clinic with severe hypertriglyceridemia: a retrospective cohort study. Lipids Health Dis. 2011; 10:157.
16. Miller A, Lees RS, McCluskey MA, Warshaw AL. The natural history and surgical significance of hyperlipemic abdominal crisis. Ann Surg. 1979; 190: 401-8.
17. Fortson MR, Freedman SN, Webster PD 3rd. Clinical assessment of hyper- lipidemic pancreatitis. Am J Gastroenterol. 1995; 90:2134-9.
24