hospital advisory committee meeting wednesday, 10 december ... 12... · hospital advisory committee...
TRANSCRIPT

Hospital Advisory Committee Meeting
Wednesday, 10 December 2014
9.30am
A+ Trust Room Clinical Education Centre
Level 5 Auckland City Hospital
Grafton
He Oranga Tika Mo Te Iti Te Rahi
Healthy Communities, Quality Healthcare
Published 04 December 2014


Agenda Hospital Advisory Committee
10 December 2014
Venue: A+ Trust Room, Clinical Education Centre Level 5, Auckland City Hospital, Grafton
Time: 9.30am
Committee Members Judith Bassett (Chair) Jo Agnew Peter Aitken Doug Armstrong Dr Chris Chambers Assoc Prof Anne Kolbe Dr Lester Levy Dr Lee Mathias Robyn Northey Morris Pita Gwen Tepania-Palmer Ian Ward
ADHB Executive Leadership Ailsa Claire Chief Executive Officer Simon Bowen Director of Health Outcomes – ADHB/WDHB Margaret Dotchin Chief Nursing Officer Fionnagh Dougan Director Provider Services Naida Glavish Chief Advisor Tikanga and General Manager Māori Health – ADHB/WDHB Dr Debbie Holdsworth Director of Funding – ADHB/WDHB Dr Andrew Old Chief of Strategy, Participation and Improvement Rosalie Percival Chief Financial Officer Linda Wakeling Chief of Intelligence and Informatics Sue Waters Chief Health Professions Officer Dr Margaret Wilsher Chief Medical Officer ADHB Senior Staff Dr Richard Aickin Director Child Health Dr Vanessa Beavis Director Perioperative Services Dr John Beca Director Surgical, Child Health Dr Clive Bensemann Director Mental Health Jo Brown Funding and Development Manager Hospitals Judith Catherwood Director Long Term Conditions Dr Mark Edwards Director Cardiac Services Dr Sue Fleming Director Women’s Health Dr Wayne Jones Director Surgical Services Auxilia Nyangoni Deputy Chief Financial Officer Dr Michael Shepherd Director Medical, Children’s Health Marlene Skelton Corporate Business Manager Dr Barry Snow Director Adult Medical Dr Richard Sullivan Director Cancer and Blood Jesse Taylor Corporate Committee Administrator Clare Thompson General Manager Non Clinical Support Services Frank Tracey General Manager and Acting Director Clinical Support Services Gilbert Wong Director Communications (Other staff members who attend for a particular item are named at the start of the respective minute)
Apologies Members: Nil
Apologies Staff: Richard Aickin, Simon Bowen, Margaret Dotchin
Register of Interests Does any member have an interest they have not previously disclosed? Does any member have an interest that may give rise to a conflict of interest with a matter on the agenda?
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
2

Agenda Please note that agenda times are estimates only
9.30am 1. Attendance and Apologies
9.35am 2. Conflicts of Interest
9.40am 3. Confirmation of Minutes 29 October 2014
9.45am 4. Action Points
9.50am 5. Health and Safety
9.55am 6. Provider Arm Performance Report
6.1 Scorecard
6.2 Overall Provider Performance including Health Target Updates
6.2.1 Four month ESPI – verbal update by Fionnagh Dougan
6.3 Financial and Operational Performance
10.10am 7. Quality Updates
7.1 Compliments Report
7.2 Quality Report
10.20am 8. Directorate Updates
8.1 Mental Health Directorate
8.2 Women’s Health Directorate
8.3 Child Health Directorate
8.4 Surgical Services Directorate
8.5 Perioperative Services Directorate
8.6 Cancer and Blood Directorate
8.7 Community and Long Term Conditions Directorate
8.8 Non-Clinical Support Services
8.9 Clinical Support Services
8.10 Cardiovascular Directorate
8.11 Adult Medical Directorate
11.15am 9. Information Papers
9.1 Management of Slow Moving and Due-to-Expire Inventory and Stock
9.2 National Services Update
9.3 Auckland DHB and Waitemata DHB Contact Centre Collaboration Update
11.30am 10. Resolution to exclude the public Next Meeting: Wednesday, 18 February 2015 at 9.30am A+ Trust Room, Clinical Education Centre Level 5, Auckland City Hospital, Grafton
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
3

Attendance at Hospital Advisory Committee Meetings
Members
11 D
ec. 1
3
19 F
eb. 1
4
02 A
pr. 1
4
14 M
ay. 1
4
25 Ju
n. 1
4
06 A
ug. 1
4
17 S
ep. 1
4
29 O
ct. 1
4
10 D
ec. 1
4
Judith Bassett (Chair) 1 1 1 1 x 1 1 1
Joanne Agnew 1 1 1 1 1 1 1 1
Peter Aitken 1 1 1 1 1 1 1 1
Doug Armstrong 1 1 1 1 1 1 1 1
Chris Chambers 1 1 1 1 1 1 1 1
Anne Kolbe 1 1 1 1 1 x 1 1
Lester Levy 1 1 x 1 1 1 1 1
Lee Mathias 1 1 1 1 1 1 x 1
Robyn Northey 1 1 1 1 1 x 1 1
Morris Pita 1 1 1 1 1 1 x 1
Gwen Tepania-Palmer 1 1 1 1 1 1 1 1
Ian Ward 1 1 1 1 1 1 1 1
Key: x = absent, # = leave of absence
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
1
4


Conflicts of Interest Quick Reference Guide Under the NZ Public Health and Disability Act Board members must disclose all interests, and the full nature of the interest, as soon as practicable after the relevant facts come to his or her knowledge.
An “interest” can include, but is not limited to:
• Being a party to, or deriving a financial benefit from, a transaction • Having a financial interest in another party to a transaction • Being a director, member, official, partner or trustee of another party to a transaction or a
person who will or may derive a financial benefit from it • Being the parent, child, spouse or partner of another person or party who will or may derive a
financial benefit from the transaction • Being otherwise directly or indirectly interested in the transaction
If the interest is so remote or insignificant that it cannot reasonably be regarded as likely to influence the Board member in carrying out duties under the Act then he or she may not be “interested in the transaction”. The Board should generally make this decision, not the individual concerned.
Gifts and offers of hospitality or sponsorship could be perceived as influencing your activities as a Board member and are unlikely to be appropriate in any circumstances.
• When a disclosure is made the Board member concerned must not take part in any deliberation or decision of the Board relating to the transaction, or be included in any quorum or decision, or sign any documents related to the transaction.
• The disclosure must be recorded in the minutes of the next meeting and entered into the interests register.
• The member can take part in deliberations (but not any decision) of the Board in relation to the transaction if the majority of other members of the Board permit the member to do so.
• If this occurs, the minutes of the meeting must record the permission given and the majority’s reasons for doing so, along with what the member said during any deliberation of the Board relating to the transaction concerned.
IMPORTANT
If in doubt – declare.
Ensure the full nature of the interest is disclosed, not just the existence of the interest.
This sheet provides summary information only - refer to clause 36, schedule 3 of the New Zealand Public Health and Disability Act 2000 and the Crown Entities Act 2004 for further information (available at www.legisaltion.govt.nz) and “Managing Conflicts of Interest – Guidance for Public Entities” (www.oag.govt.nz ).
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
2
5

Register of Interests – Hospital Advisory Committee
Member Interest Latest Disclosure
Judith BASSETT (Chair)
Fisher and Paykel Healthcare Westpac Banking Corporation
14.05.2014
Jo AGNEW Professional Teaching Fellow - School of Nursing, Auckland University Appointed trustee Starship Foundation Casual Staff Nurse - ADHB
01.03.2014
Peter AITKEN Pharmacy Locum - Pharmacist Shareholder/ Director, Consultant - Pharmacy Care Systems Ltd Shareholder/ Director - Pharmacy New Lynn Medical Centre
17.01.2014
Doug ARMSTRONG Fisher and Paykel Healthcare Ryman Healthcare Daughter is a partner – Russell McVeagh Lawyers
12.03.2014
Chris CHAMBERS Employee - ADHB Wife is an employee - Starship Trauma Service Clinical Senior Lecturer in Anaesthesia - Auckland Clinical School Member – Association of Salaried Medical Specialists Associate - Epsom Anaesthetic Group Shareholder - Ormiston Surgical
26.01.2014
Anne KOLBE Joint owner - Kolbe Medical Services Ltd Senior Consultant - Communio NZ Senior Consultant - Siggins Miller, Australia Member - Risk and Audit Committee, Whanganui District Health Board Chair - National Health Committee Member - Australian Institute of Directors Husband:
Professor of Medicine, University of Auckland Chair - Health Research Council of NZ, Clinical Trials Advisory Committee Member - Australian Medical Council, Medical School Advisory Committee Lead - Medical Specialties Advisory Committee Accreditation Team, Royal Australian College of General Practitioners Member - Executive Committee, International Society for Internal Medicine Chair - RACP Re-validation Working Party Member - RACP Governance Working Party
Son: Employee - Hawkins Construction
01.02.2014
Lester LEVY Chairman - Waitemata District Health Board Chairman - Auckland Transport Independent Chairman - Tonkin & Taylor Deputy Chairman – Health Benefits Ltd Chief Executive - New Zealand Leadership Institute Professor (Adjunct) of Leadership - University of Auckland Business School Trustee of the Well Foundation (ex-officio member as Waitemata DHB Chairman) Director - Orion Health Board Director and sole shareholder – Brilliant Solutions Ltd
17.09.2014
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
6

Lee MATHIAS Chair - Counties Manukau Health Deputy Chair - Auckland District Health Board Chair - Health Promotion Agency Chair - Unitec. Director - Health Innovation Hub Director - Health Alliance Limited Director - Health Alliance (FPSC) Limited Chair - IAC IP Limited Director/shareholder - Pictor Limited Director - Lee Mathias Limited Director - John Seabrook Holdings Limited Advisory Chair - Company of Women Limited Trustee - Lee Mathias Family Trust Trustee - Awamoana Family Trust Trustee - Mathias Martin Family Trust
23.10.2014
Robyn NORTHEY Self-employed Contractor - Project management, service review, planning etc. Board Member - Hope Foundation Trustee - A+ Charitable Trust
20.06.2012
Morris PITA Member – Waitemata District Health Board Shareholder – Turuki Pharmacy, South Auckland Owner and operator with wife - Shea Pita & Associates Ltd Wife is member of Northland District Health Board Wife provides advice to Maori health organisations
13.12.2013
Gwen TEPANIA-PALMER
Board Member - Waitemata District Health Board Board Member - Manaia PHO Chair - Ngati Hine Health Trust Committee Member - Te Taitokerau Whanau Ora Committee Member - Lottery Northland Community Committee Member - Health Quality and Safety commission
02.04.2013
Ian WARD Board Member - NZ Blood Service Director and Shareholder – C4 Consulting Ltd CEO – Auckland Energy Consumer Trust Shareholder – Vector Group
09.07.2014
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
2
7


Minutes
Hospital Advisory Committee Meeting 29 October 2014
Minutes of the Auckland District Health Board meeting held on Wednesday, 29 October 2014 in the A+ Trust Room, Clinical Education Centre, Level 5, Auckland City Hospital, Grafton commencing at 9.45am
Committee Members Present Dr Lester Levy Jo Agnew Peter Aitken Doug Armstrong Judith Bassett (Chair) Dr Chris Chambers Assoc Prof Anne Kolbe Dr Lee Mathias Robyn Northey Morris Pita Gwen Tepania-Palmer Ian Ward
ADHB Executive Leadership Team Present Ailsa Claire Chief Executive Officer Margaret Dotchin Chief Nursing Officer Fionnagh Dougan Director Provider Services Rosalie Percival Chief Financial Officer Sue Waters Chief Health Professions Officer Dr Margaret Wilsher Chief Medical Officer ADHB Senior Staff Present Dr Vanessa Beavis Director Perioperative Services Dr Clive Bensemann Director Mental Health Services Joanne Brown Funding and Development Manager Hospitals Judith Catherwood Director Adult Community & Long Term Conditions Dr Mark Edwards Director Cardiovascular Services Dr Wayne Jones Director Surgical Services Dr Michael Shepherd Director Medical, Children’s Health Marlene Skelton Corporate Business Manager Dr Barry Snow Director Adult Medical Services Dr Richard Sullivan Director Cancer and Blood Services Jesse Taylor Corporate Committee Administrator Frank Tracey General Manager and Acting Director Clinical
Support Services
(Other staff members who attend for a particular item are named at the start of the minute for that item)
1. APOLOGIES
Apologies were received from staff members Clare Thompson, Anna Schofield, Gilbert Wong, Dr Andrew Old, and Dr Sue Fleming.
2. CONFLICTS OF INTEREST
There were no declarations of conflicts of interest for any items on the open agenda.
Lee Mathias drew attention to the fact that her registered interests had been updated between meetings with the revised interests appearing in this agenda.
3. CONFIRMATION OF MINUTES 17 September 2014 (Pages 8 - 19)
Resolution: Moved Gwen Tepania-Palmer / Seconded Jo Agnew
That the minutes of the Hospital Advisory Committee meeting held on 17 September 2014 be confirmed as a true and accurate record.
Carried
Auckland District Health Board Hospital Advisory Committee Meeting 29 October 2014 Page 1 of 13
3
8

4. ACTION POINTS (Pages 20 - 21)
There was no comment with regard to action points from previous meetings.
5. HEALTH AND SAFETY
There was no comment with regard to matters of health and safety.
6. PROVIDER ARM PERFORMANCE REPORT (Pages 22 - 31)
6.1 Scorecard
Fionnagh Dougan, Director Provider Services, advised that the scorecard results would be covered through the Directorate reports. Maori and Pacific Did Not Attend (DNA) rates continue to be a major concern and are a key focus for all Directorates.
6.2 Overall Provider Performance including Health Target Updates
There was no discussion under this item.
6.3 Financial and Operational Performance
Rosalie Percival, Chief Financial Officer, asked that the report be taken as read. The following points were highlighted:
An unfavourable variance for cleaning services exists due to incorrect information provided by the previous contractor and relates primarily to amounts of leave being brought over with staff cross-cover. The situation is being managed and mitigation strategies have been put in place going forward.
Year to date performance is slightly unfavourable due to staffing and outsourced personnel pressures in September. Despite heavy utilisation and activity good overall trends are being demonstrated and the targeted savings for clinical supplies are tracking well.
Work with healthAlliance on reporting to RC codes is underway to enable services to see where price savings have been achieved. Should the targeted initiative perform well it could potentially be rolled out regionally.
The issue of increased FTE costs due to MECA conditions is currently being addressed as the increases are higher than what has been funded for inflation.
7. DIRECTORATE UPDATES (Pages 52 - 122)
7.1 Mental Health Directorate
Dr Clive Bensemann, Director Mental Health, asked that the report be taken as read. The following points were highlighted:
Nine of the 14 medication errors reported were near misses for the Buchanan Rehabilitation Centre and relate to prescription changes not being reflected in blister packaging. The
Auckland District Health Board Hospital Advisory Committee Meeting 29 October 2014 Page 2 of 13
9

process for reconciling prescriptions with blister packaging is being reviewed.
Successful delivery on the wait time targets for 0-19 years is now being reflected in the rolling 12 month figure presented in the scorecard. Access rates also continue to improve monthly.
Other highlights included the Health of Older Persons Executive Group being a useful forum to better align services, opening of the Regional Mother and Baby Acute Unit, and funding approval for the Huntington's Disease Regional Service clinical pathway.
A favourable financial result can primarily be attributed to vacancies, including positions for new service components that have not yet been filled. All vacancies are actively being recruited to.
Matters covered in discussion of the report included:
• In response to concern with the way medication errors are reported it was advised that staff are encouraged to report near misses so that they can be used as learning tools. Consequently the number of reported medication errors will continue to rise as occurrences of errors causing harm reduces. It was agreed that the way this is reported is unclear and that future reporting should differentiate between near misses and errors causing harm. A report on the investigation into medication errors and the key lessons learned be provided to the Committee in February 2015.
• It was confirmed that a mental health service is available for the refugee community.
Actions: 1. Future reporting of medication errors to differentiate between near misses and errors causing
harm.
2. A report on the investigation into medication errors be provided in February 2015.
[Secretarial Note: This report was considered after item 6.4 Surgical Services]
7.2 Women’s Health Directorate
Karin Drummond, General Manager Women’s Health, asked that the report be taken as read. The following points were highlighted:
Five new Clinical Directors have been appointed across the service. Aligning the Level 4 staff structure with the new service structure is now a focus with consultation to begin in November.
Auckland DHB is the first DHB to achieve Baby Friendly Hospital accreditation without conditions.
Matters covered in discussion of the report included:
• Advice that Auckland DHB and Waitemata DHB are collaborating to develop a clinical pathway for tongue tie, and to address wider issues related to inconsistent availability of of community-based lactation support services.
Auckland District Health Board Hospital Advisory Committee Meeting 29 October 2014 Page 3 of 13
3
10
7.3 Child Health Directorate
Dr Michael Shepherd, Director Child Health, asked that the report be taken as read. The following points were highlighted:
Feedback received on the organisational structure consultation document is currently being considered.
Delivery to the Emergency Department target is slightly off track following a difficult period of high volumes, acuity, and staff sickness. The Directorate is working to ensure patient experience and metrics are improved.
The Starship theatre redevelopment project is on track with only a minor number of cancellations during the decant process.
Matters covered in discussion of the report included:
• Morale amongst staff remains high despite on-going pressures. Allocation of FTE in focused roles such as acute flow coordinators is proving effective although improvements can be made to discharge patients earlier and better utilise short stay facilities.
• It was noted that there is no requirement to restrain recruitment and that vacancies held are to accommodate new graduates which is an agreed strategy.
• Assoc Prof Anne Kolbe commented that addressing Did Not Attend (DNA) rates has been an on-going issue with a lot of resource invested to deliver improvements. She suggested it could be worthwhile taking a step back to determine what a good level of service looks like and how the resource implications of delivering it can be minimised. Dr Shepherd advised that there are a range of interventions planned within the directorate including a project to look at DNA rates within specific areas noting that DNA’s are often patients from outside Auckland DHB. DNA’s are followed up to understand the reasons behind non-attendance however the staff doing this work require more training to build their cultural competence and customer service skills. The Committee discussed examples of successful campaigns using public figures to reach audiences and agreed that it may be a worthwhile approach for Auckland DHB.
• Planning is underway with the Directorate’s small, vulnerable services to enable staff to take leave however it will be a slow process due to the difficulties in organising appropriate cover.
7.4 Surgical Services Directorate
Dr Wayne Jones, Director Surgical Services, asked that the report be taken as read. The following points were highlighted:
Elective discharges have delivered only 88% of the target due to an over delivery of Inter-District Flow (IDF) procedures and 95% WIES delivery. The metrics reported don't yet take
Auckland District Health Board Hospital Advisory Committee Meeting 29 October 2014 Page 4 of 13
11

into account additional cases that have not yet been coded.
Moderate non-compliance with the ESPI-2 and ESPI-5 targets is due to the Starship theatre decant and lack of Department of Critical Care Medicine beds. Theatre usage is good with 98% of allocated sessions utilised, and Ward 31 has been opened to support the flow of acute patients and reduce cancellation of electives.
Falls, pressure injuries, and medication errors were noted, as was the on-going issue of patients who Did Not Attend (DNA).
An unfavourable financial result was recorded for September however the Directorate remains favourable for the year to date.
7.4.1 Electives – Delivering in 90 days
Dr Wayne Jones, Director Surgical Services, and Tara Argent, General Manager Surgical Services, tabled a presentation on ensuring people receive treatment within 90 days (included as attachment 7.4.1). The Ministry of Health has decreed that ESPI-2 and ESPI-5 measures must be compliant with a four month target by the end of the calendar year. In response the Directorate has pledged that all patients will be treated within 90 days for ESPI-2 and ESPI-5 with key initiatives to deliver on this outlined as follows:
• The Directorate is working closely with other general managers and staff members to ensure all patients have been dated within the four month target. Provisional booking for elective surgery has also been introduced.
• A weekly review is undertaken to monitor patients to be booked within the month, suspensions due for review and insourcing and outsourcing requirements. The team then identifies capacity requirements to determine where staff resource is best allocated.
• An awareness campaign involving a countdown clock on the intranet, visual images, and tag lines is being developed with the Communications team. Improving customer service and validation of the wait list are other key priorities.
Matters covered in discussion of the presentation included:
• The option of allowing patients to choose their own time was recognised as a useful tool for outpatient clinics. However, this is currently impractical for inpatient procedures due to the scheduling of all resources involved.
7.5 Perioperative Services Directorate
Dr Vanessa Beavis, Director Perioperative Services, asked that the report be taken as read. The following points were highlighted:
All staff involved in the Starship theatre decant were commended for their efforts as 98% of allocated lists were utilised during the period.
The new Post Anaesthesia Care Unit on level four is now operational, and development of a hybrid theatre is on track to be completed by March 2015.
Auckland District Health Board Hospital Advisory Committee Meeting 29 October 2014 Page 5 of 13
3
12

Other positive events included all anaesthetic trainees passing their final exam, the Minister of Health's visit coinciding with National Anaesthesia Day, and the public response to the 'stop before the op' campaign.
7.6 Cardiovascular Directorate
Dr Mark Edwards, Director Cardiovascular, asked that the report be taken as read. The following point was highlighted:
Delivering on the Cardiac Surgery Bypass wait list continues to be a challenge however it is pleasing to note the list has reduced to an acceptable level. Improvements can be attributed to a number of interventions, team effort, and positive engagement from management and clinicians.
There were no questions.
7.7 Adult Medical Directorate
Dr Barry Snow, Director Adult Medical, asked that the report be taken as read. The following points were highlighted:
Pressures over Winter have had knock-on effects resulting in failure to meet targets, a rise in complaints, excess annual leave and increased staff sickness. Those deliverables better able to be controlled, such as colonoscopy procedures, have been brought back in line however there are still training issues that need addressing.
Work undertaken to improve follow-up attendance is delivering positive results and a new booking system which provides patients with more appointment options may also help to address the issue of Did Not Attend (DNA). .
Financial results for the Directorate remain unfavourable however the savings plan is on target and tracking well.
Matters covered in discussion of the report included:
• The five year strategic planning process involves looking at the difference between ‘doing things right’ and ‘doing the right thing’. The future focus will be on what is right for the patient. The model used for advanced care planning has proven successful and will be rolled-out across the Directorate.
7.8 Cancer and Blood Directorate
Dr Richard Sullivan, Director Cancer and Blood, asked that the report be taken as read. The following points were highlighted:
Maori and Pacific Did Not Attend (DNA) rates have been a focus of the Directorate in recent years with Ministry of Health funding utilised for a Maori and Pacific Navigation pilot to develop an early engagement process for these patients and to sustain their engagement right through the process. The pilot has been running between Auckland and Northland and evaluation tools have been developed.
Auckland District Health Board Hospital Advisory Committee Meeting 29 October 2014 Page 6 of 13
13

There is a continued focus on achieving the 31/62 day target. The aim is to ensure all First Specialist Appointments are delivered within seven days of receipt of referral.
Financial results for the Directorate are favourable and savings targets have been achieved.
There were no questions.
7.9 Clinical Support Services
Frank Tracey, General Manager and Acting Director Clinical Support Services, asked that the report be taken as read. The following points were highlighted:
Delivery of MRI and CT targets remains stable and acceptable. Achieving the ultrasound target continues to be an issue however it is expected that there will be an improvement to the wait list going forward.
Work to configure resource in a way that meets patient demand continues as diagnostic testing becomes increasingly popular. The Directorate is engaging with General Practitioners to better understand the increase in referrals and determine how volumes can best be managed. Consideration is being given to outsourcing some ultrasound procedures which should result in rapid improvement to delivery.
Favourable financial results continue to be achieved, as do savings targets.
Responsibility for the Contact Centre Collaboration project was recently shifted to the Clinical Support Services Directorate and is progressing well. Consultation with staff suggests the initiative is being well received and that there is an appreciation of the change required.
Reconfiguration of the Clinical Engineering Department is complete with the right leadership structure now in place and continued involvement of staff throughout the change process. Relationships with Counties Manukau and Waitemata DHBs have also been strengthened.
Clinical Support staff were acknowledged for their efforts during what has been an exceptionally busy Winter period.
There were no questions
7.10 Non-Clinical Support Services
Frank Tracey, General Manager and Acting Director Clinical Support Services, asked that the report be taken as read. The following points were highlighted on behalf of Clare Thompson, General Manager Non-Clinical Support Services:
The Health Benefits Limited (HBL) food services proposal has been a complex piece of work however it is progressing well with good engagement from unions and stakeholders.
The Contact Centre Collaboration project has involved engagement with staff to determine how performance can be improved. Staff have embraced the need to improve how they work as individuals as well as initiatives that can be implemented across the system to alleviate pressure.
Matters covered in discussion of the report included:
Auckland District Health Board Hospital Advisory Committee Meeting 29 October 2014 Page 7 of 13
3
14

• Efforts are being made to rebase values and increase engagement of Contact Centre staff as over time they have lost some degree of their sense of engagement as part of the DHB team. Staff working in the Contact Centre are a good reflection of the Auckland DHB population and their up-skilling will provide an opportunity to improve health literacy within the community.
7.11 Community and Long Term Conditions Directorate
Judith Catherwood, Director Community and Long Term Conditions, asked that the report be taken as read. The following points were highlighted:
Plans to address issues with Did Not Attend (DNA) rates and excess annual leave have been put in place. It is hoped that improvements in both areas will be experienced before the end of the calendar year.
No SAC 1 or 2 incidents or falls with major harm occurred during September. Initiatives trialled in the Falls Prevention concept ward have proven successful and will be rolled out across other inpatient wards. Examples of initiatives trialled include the use of sticky socks and wrist bands to assist staff in identifying high-risk patients as well as improved signage to help re-orientate and direct patients.
The Wander Search electronic tracking system is to be trialled amongst patients with cognitive impairment. The system enables staff to locate and retrieve these patients quickly, however is reliant on the tracking device remaining in place on the patient.
The Regional Sexual Health Services Model of Care is being reviewed with Funding and Planning. Consultation will include the Community and Public Health Advisory Committee and the Board.
Financial results for the month and year to date are favourable. It is expected that the FTE expenditure will increase to budget in coming months.
There were no questions.
That the Directorate updates be received
8. QUALITY UPDATES (Pages 123 - 140)
8.1 Compliments Report
Sue Waters, Chief Health Professions Officer, asked that the report be taken as read.
The top three themes amongst the 73 compliments received in September were care and treatment, staff attitude, and food.
That the Compliments Report be received.
8.2 Quality Report
Sue Waters, Chief Health Professions Officer, asked that the report be taken as read. The reports suggest that patients are primarily concerned with the provision of good information
Auckland District Health Board Hospital Advisory Committee Meeting 29 October 2014 Page 8 of 13
15

and coordination of care.
The patient experience report focus was on food and dietary need and identified opportunities for improvement with special dietary requirements and assistance. The feedback highlighted the importance of the service associated with the provision of food in hospitals which should be addressed through the Auckland Metro consultation for food services.
Patient experience information is made available to all services and reviewed by the Clinical Board before being reported to the Committee. The information is also publicly available on the website.
There were no questions.
That the Quality Report be received.
8.3 National Inpatient Experience Survey Update
Sue Waters, Chief Health Professions Officer, presented the report noting that the information available from the survey is not yet weighted however Auckland DHB appears to be in a positive position compared to other similar DHBs.
There were no questions.
That the National Inpatient Survey Update report be received.
8.4 2013/14 Privacy Commissioner Annual Report
There was no discussion with the report being taken as read.
Resolution: Moved Robyn Northey / Seconded Gwen Tepania-Palmer
That the Committee receives the letter from the Privacy Commissioner.
That the Committee notes the progress and status of the 2013/14 Privacy Commissioner Annual Report.
Carried
9. INFORMATION PAPERS (Pages 141 - 155)
9.1 Improving Cancer Outcomes – A Strategic View
Dr Richard Sullivan, Director Cancer and Blood, asked that the report be taken as read noting that the report is intended to clarify the proposed structure for cancer services and provide an overview of the direction of cancer diagnosis and treatment going forward.
• The new tumour stream approach is about anticipated on-going requirements for patients based on the primary site of diagnosis as the pathway of care varies for each. A faster cancer treatment pathway is imminent however comes with challenges due to the cancer activity that spans the directorates. The concept of a Cancer Outcomes Director is
Auckland District Health Board Hospital Advisory Committee Meeting 29 October 2014 Page 9 of 13
3
16
being considered to monitor and measure the entire pathway of cancer patients.
• The Northern Region Cancer Governance Board is developing a strategic plan for the Northern Cancer Network and will look at how to operationalise the plan within the involved DHBs to ensure the right services are provided in the right location and remain consistent across the spectrum.
Matters covered in discussion of the report included:
• Consideration will be given to adopting a care pathway approach for other conditions should the cancer care pathway approach prove successful.
• A 31/62 day target governance group comprised of directors and staff from service areas where there is a need to deliver change has been established. The primary focus of the group is ensuring delivery against the target and is part of a wider proposal for change which will be released in coming weeks.
• Dr Lee Mathias commented on the ICT system used by the Victorian Cancer Consortium advising that it has the capability to follow patients through various services and could be leveraged for use here.
• Assoc Prof Anne Kolbe referenced the work of Dame Carol Black, suggesting that measures for success should consider how a patient integrates and contributes to society following conclusion of their treatment.
Resolution: Moved Anne Kolbe / Seconded Gwen Tepania-Palmer
That the Committee receives the Improving Cancer Outcomes – A Strategic View report.
That the Committee notes the aspirations and proposed direction for the governance of cancer outcomes within the Auckland District Health Board.
Carried
9.2 Preparations for Emerging Infectious Diseases
Fionnagh Dougan, Director Provider Services, advised that the purpose of the paper was to provide an update on preparedness in the event a patient with an emerging infectious disease presented at Auckland City Hospital.
There are four centres in New Zealand that will take the lead on any emerging viral diseases. Counties Manukau DHB is primarily responsible for patients that arrive through the airport however it is appropriate for Auckland DHB to be equally prepared. All treatment providers within the region are adopting the same protocols.
Changes to existing facilities have been proposed and a clear care pathway has been developed. Staff training for the use of Personal Protective Equipment is underway however needs to be delivered faster given the care burden associated with these patients.
Matters covered in discussion of the report included:
• Doug Armstrong queried why an urgent request for funding in these circumstances was
Auckland District Health Board Hospital Advisory Committee Meeting 29 October 2014 Page 10 of 13
17

withheld until a scheduled Board meeting for approval. The Committee was advised that any urgent and essential expenditure was covered by the Incident Management Team. The finalised figures were only recently confirmed, and the request had been brought directly to the Board without first going through the Audit and Finance Committee. The proposed expenditure is to create improvements and sustainability for the model that is already in place.
Resolution: Moved Doug Armstrong / Seconded Ian Ward
That the Committee receives the report.
Carried
9.3 National Services Update
Fionnagh Dougan, Director Provider Services, asked that the report be taken as read noting that it was timely for the Committee to have visibility of the work that has been done to address wider issues that are emerging for nationally provided services.
There has been a need for national funders to understand that providing payment per procedure is not sufficient to ensure the sustainability of these services.
There were no questions.
Resolution: Moved Lee Mathias / Seconded Peter Aitken
That the Committee receives the National Services Update report.
That the Committee notes the current progress and status of the work programme for National Services provided by Auckland District Health Board with the National Health Board.
Carried
10. Resolution to Exclude the Public (Pages 156 - 157)
Resolution: Moved Lee Mathias / Seconded Peter Aitken
That in accordance with the provisions of Clauses 32 and 33, Schedule 3, of the New Zealand Public Health and Disability Act 2000 (“Act”), the Auckland District Health Board Hospital Advisory Committee resolve that the public now be excluded from the meeting for consideration of the following items, for the reasons and grounds set out below:
General subject of each item to be considered:
Reasons for passing this resolution in relation to each item:
Ground(s) under Clause 32 for the passing of this resolution
1 Confirmation of the Public Excluded Minutes of the Hospital Advisory Committee Meeting 17 September 2014
Confirmation of Minutes As per resolution(s) from the open section of the minutes of the above meeting, in terms of the NZPH&D Act 2000.
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except
Auckland District Health Board Hospital Advisory Committee Meeting 29 October 2014 Page 11 of 13
3
18

section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
2 Confirmation of the Public Excluded Action Points of the Hospital Advisory Committee Meeting 17 October 2014
Confirmation of Action Points As per resolution(s) from the open section of the minutes of the above meeting, in terms of the NZPH&D Act 2000.
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
3 Risk Report Negotiations To enable the Board to carry on, without prejudice or disadvantage, negotiations (including commercial and industrial negotiations) [Official Information Act 1982 S.9 (2) (j)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
4 Complaints Report Negotiations To enable the Board to carry on, without prejudice or disadvantage, negotiations (including commercial and industrial negotiations) [Official Information Act 1982 S.9 (2) (j)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
5 Health and Safety Commercial Activities To enable the Board to carry out, without prejudice of disadvantage, commercial activities [Official Information Act 1982 s9(2)(i)] Obligation of Confidence The disclosure of information would not be in the public interest because of the greater need to protect information which is subject to an obligation of confidence [Official Information Act 1982 s9(2)(ba)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
6 Information Papers
Commercial Activities To enable the Board to carry out, without prejudice of disadvantage, commercial activities [Official Information Act 1982 s9(2)(i)] Obligation of Confidence The disclosure of information would not be in the public interest because of the greater need to protect information
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
Auckland District Health Board Hospital Advisory Committee Meeting 29 October 2014 Page 12 of 13
19

which is subject to an obligation of confidence [Official Information Act 1982 s9(2)(ba)]
7 Discussion Papers Commercial Activities To enable the Board to carry out, without prejudice of disadvantage, commercial activities [Official Information Act 1982 s9(2)(i)] Obligation of Confidence The disclosure of information would not be in the public interest because of the greater need to protect information which is subject to an obligation of confidence [Official Information Act 1982 s9(2)(ba)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
8 Service Review Updates Commercial Activities To enable the Board to carry out, without prejudice of disadvantage, commercial activities [Official Information Act 1982 s9(2)(i)] Obligation of Confidence The disclosure of information would not be in the public interest because of the greater need to protect information which is subject to an obligation of confidence [Official Information Act 1982 s9(2)(ba)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
Carried
The meeting closed at 12.40pm.
Signed as a true and correct record of the Hospital Advisory Committee meeting held on Wednesday, 29 October 2014
Chair: Date: Judith Bassett
Auckland District Health Board Hospital Advisory Committee Meeting 29 October 2014 Page 13 of 13
3
20


Action Points from Previous Hospital Advisory Committee Meetings
As at Wednesday, 03 December 2014
Meeting and Item
Detail of Action Designated to Action by
6 Aug 2013 Item 6
Ethnicity Data Ethnicity Data/benchmarking data to be provided when the new national Cardio surgical Database is implemented
F Dougan Date to be advised when determined by MoH
6 Aug 2014 Item 5.1
Management of Obsolete and Due-to-Expire Inventory That a further update on progress on obsolete and due-to-expire inventory, including pandemic stock, both regionally and nationally be provided in three months.
R Percival Complete – on the agenda for this meeting
6 Aug 2014 Item 7.3
Starship Hospital That an update be provided to the Board in February 2015 on the current situation and future planning for Starship.
F Dougan 18 Feb 2015
6 Aug 2014 Item 7.7
Colonoscopy Update That a report detailing the progress of planning to deliver colonoscopy volumes within Auckland DHB and the work being undertaken on the regional strategy working in collaboration with other District Health Boards be provided in four months-time.
F Dougan and B Snow
18 Feb 2015
17 Sep 2014 Item 6.1
Eating Disorders Service model redesign That a brief presentation on the outcome of the model redesign be provided in the new year.
C Bensemann 18 Feb 2014
17 Sep 2014 Item 6.2
Women’s Health That a paper outlining options for change in service provision as part of the Auckland/Waitemata DHB Women’s Health collaboration be provided in December.
S Fleming Complete – provided to 10 Dec 2014 Board meeting
29 Oct 2014 Item 7.1
Medication Errors – Mental Health Directorate Future reporting of medication errors to differentiate between near misses and errors causing harm. A report on the investigation into medication errors be provided in February 2015.
C Bensemann 18 Feb 2015
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
4
21


Actual Target Prev Period
% AED patients seen within triage time - triage category 2 (10 minutes) PR006 82.5% >= 80% 80.5%Green Green
% CED patients seen within triage time - triage category 2 (10 minutes) PR008 81.7% >= 80% 88.4%Green Green
Number of reported adverse events causing harm (SAC 1&2) PR084 6 <= 12 7Green Green
Central line associated bacteraemia rate per 1,000 central line days PR087 0 <= 1 0Green Green
Healthcare-associated Staphylococcus aureus bacteraemia per 1,000 bed days PR088 N/A <= 0.2 0.16Grey Green
Healthcare-associated bloodstream infections per 1,000 bed days - Adult PR089 N/A <= 1.6 0.74Grey Green
Healthcare-associated bloodstream infections per 1,000 bed days - Child PR090 N/A <= 2.4 1.62Grey Green
Falls with major harm per 1,000 bed days PR095 0.12 <= 0.09 0.03Red Green
Nosocomial pressure injury point prevalence (% of in-patients) PR097 5.2% <= 6% 5.6%Green Green
Healthcare-associated Clostridium difficile infection rate per 10,000 bed days (Quarterly) PR143 3.06 <= 4 3.33Green Green
% Hand Hygiene Compliance (4-Monthly) PR144 76.3% >= 70% 76.3%Green Green
(MOH-01) % AED patients with ED stay < 6 hours PR013 92.3% >= 95% 91.8%Red Red
(MOH-01) % CED patients with ED stay < 6 hours PR016 94% >= 95% 94.6%Amber Amber
% Inpatients on Older Peoples Health waiting list for 4 days or less PR023 91.2% >= 80% 88.9%Green Green
HT2 Elective discharges cumulative variance from target PR035 0.99 >= 1 0.93Amber Red
(ESPI-2) Patients waiting longer that 5 months for their FSA PR038 0.2% 0% 0.2%Amber Amber
(ESPI-5) Patients given a commitment to treatment but not treated within 5 months PR039 0.3% 0% 0.5%Amber Amber
Cardiac Bypass Surgery Waiting List PR042 71 <= 104 96Green Green
% Accepted referrals for elective coronary angiography treated within 3 months PR043 99.3% >= 90% 99.3%Green Green
% Urgent Diagnostic colonoscopy procedures treated < 14 days PR044 100% >= 75% 77.3%Green Green
% Non urgent colonoscopy procedures treated < 42 days PR045 98.8% >= 60% 76.9%Green Green
% Outpatients & community referred MRI completed < 6 weeks PR046 75.2% >= 80% 74.8%Red Red
% Outpatients & community referred CT completed < 6 weeks PR047 65.7% >= 90% 78.1%Red Red
Elective day of surgery admission (DOSA) rate PR048 69.4% >= 68% 68.1%Green Green
% Day Surgery Rate PR052 100% >= 70% 100%Green Green
Inhouse Elective WIES through theatre - per day PR053 127.07 >= 99 121.92Green Green
% DNA rate for outpatient appointments - All Ethnicities PR056 9.3% <= 9% 9.5%Amber Amber
% DNA rate for outpatient appointments - Maori PR057 18% <= 9% 17.8%Red Red
Bet
ter Q
ualit
y C
are
Maori Health is working with cancer and blood to progress the faster cancer treatment and support the DNA strategies across the provider arm. Our team have includedcardiac patients in their reminder call, in line with pacific services.
Out-patient bookings have been down for CT due to the installation of the two new CT scanners on the GCC and ACH site.
MRI compliance remains steady with the Paediatric GA MRI’s referrals being our biggest concern. The GCC MRI is due to be operational mid-January 2015.
High volumes, significant access block, APU at capacity and staffing shortages exist. Solutions must come from in-patient escalation plans.
*
Patie
nt S
afet
y
*
Represents normal variation in the process around a mean (the target). Consideration is being given to changing this measure to a 12 month rolling average .
Auckland DHB Provider ScorecardFor October 2014
Measure Commentary
6.1
23

% DNA rate for outpatient appointments - Pacific PR058 17.5% <= 9% 18.2%Red Red
% Chemotherapy patients (Med Onc and Haem) attending FSA within 4 weeks of referral PR059 92% 100% 95.9%Red Red
% Radiation oncology patients attending FSA within 4 weeks of referral PR064 94.9% 100% 95.1%Red Red
% Cancer patients receiving radiation/chemo therapy treatment within 4 weeks of DTT PR070 100% 100% 100%Green Green
Average LOS for WIES funded discharges (days) PR074 3.04 <= 3 2.93Amber Green
28 Day Readmission Rate - Total PR078 N/A <= 6% 9.8%Grey Red
Breastfeeding rate on discharge excluding NICU admissions PR099 N/A >= 75% 78.4%Grey Green
Mental Health - 28 Day Readmission Rate (KPI Discharges) to Te Whetu Tawera PR119 N/A <= 10% 17.2%Grey Red
Mental Health Average LOS (KPI Discharges) - Te Whetu Tawera PR120 32.3 <= 21 22.3Red Amber
% Very good and excellent ratings for overall patient experience for inpatients (from physical health services, adult and paediatric) PR154 N/A >= 90% 87.8%
Grey Red
Number of CBU Outliers - Adult PR173 418 0 479Red Red
% Patients cared for in a mixed gender room at midday - Adult PR175 16% 0% 17.1%Red Red
Mental Health % long-term clients with relapse prevention plans in last 12 months (6-Monthly) PR125 94.6% >= 95% 97.4%
Amber Green
% Hospitalised smokers offered advice and support to quit PR129 97% >= 95% 95.9%Green Green
Amber
N/A
*PR125 (6-Monthly)Actual result is for the period ending June 2014. Previous period result is for period ending December 2013.PR143 (Quarterly)Actual result is for the period ending September 2014. Previous period result is for period ending June 2014.
= Variance from target not significant enough to report as non-compliant. This includes percentages/rates within 1% of target, or volumes within 1 value from target.
= Result not available, too soon to report
PR144 (4-Monthly)Actual result is for the period ending September 2014. Previous period result is for period ending June 2014.
PR154This measure is based on retrospective survey data, i.e. completed responses for patients discharged the previous month.
PR088, PR089, PR090Results are based on a manual process and complete test results not being available for the previous month.
= Quarterly, 4-Monthly or 6-Monthly Measure
PR078, PR119
A 35 day period is required to accurately report all acute re-admissions for the previous month's discharges. (35 days = 28 days post discharge as per MoH measures plus 5 working days to allow for coding).
*
Impr
oved
H
ealth
St
atus
Continued focus by Charge Nurses and Daily Ops team to provide same gender rooms. Variance due to extra.mixed gender acute observation units.
Continued volumes through October especially in Surgical areas contributed to outlier numbers.
While Average LOS at Te Whetu Tawera remains above target on a monthly and year to date basis, over the long run the trend is still downwards and positive.
Work continues to manage clinic capacity inorder to increase the number of FSA's seen.Virtual follow ups being used to monitor prostate cancer patients - where appropriate.
The drop in overal percentage reflects an increase in referrals particulary for the breast and melanoma tumour streams. Additional clinics are being run andr esources reallocated to manage this the current demand.
The team continues to support the implementation of the DNA strategies across the provider arm including the cancer and blood and cardiac patients / families followup.
24

Trend Information The following control charts plot process data in a time-ordered sequence to identify common cause and special cause variation.
• Expected Variation Region The area between the lower and upper control limits (LCL and UCL), where the process is expected to perform. This is also known as common cause variation and refers to occurrences that contribute to the natural variation in any process.
• Unexpected Variation Region The area beyond the control limits, also known as special cause variation. Special causes are unusual occurrences that are not normally (or intentionally) part of the process and create instability.
Upper Control Limit (UCL)
Lower Control Limit (LCL)
Target
Average
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
6.1
25

Falls with major harm per 1,000 bed days (PR095) The rate of falls resulting in major harm (SAC 1 or 2) per 1000 bed days.
Current Target Performance • ADHB has a 12 month Target of 0.09 Falls with Major Harm / 1,000 bed days. Recently
the hospital has experienced an unexplained increase in Major Harm Falls.
Current/Planned Improvements • Analysis of Falls by Directorates show there have been increases in most Directorates
outside of Adult Community & LTC. • We are increasing focus on these areas and rolling out lessons in the Concept Ward trial.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
26

% AED patients with ED stay < 6 hours (PR013) The amount of time a patient remains in Emergency Departments (ED) before leaving, regardless of their destination.
Current Target Performance • The key problem is a combination of high volumes with superimposed surges. The
surges exceed our capacity and push the 6-hour compliance below 95%.
Current/Planned Improvements • We are putting in place processes that will address surges. These include more front line
staff to process patients. We are also enhancing our processes to move patients and increasing our capacity to flex open beds to manage periods of high demand.
• We expect these processes will improve compliance by approximately 3-4% if demand does not increase further.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
6.1
27

% Outpatients & community referred MRI completed < 6 weeks (PR046) The percentage of accepted Outpatient & Community referred MRI's completed within six weeks.
Current Target Performance • MRI has been steady at around 75% for 3 months. • The waiting list for Paediatric MRI under GA is still the biggest concern.
Current/Planned Improvements • The new MRI installation at Greenlane Clinical Centre is due to be operational in mid-
January 2015. • Service Improvement Projects around outpatient CT & MRI bookings are also in
progress.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
28

% Outpatients & community referred CT completed < 6 weeks (PR047) The percentage of accepted Outpatient & Community referred CT's completed within six weeks.
Current Target Performance • The CT compliance has dropped from 78% to 66% in October as a result of the
installation of two new scanners on the GCC and ACH sites. We have effectively been down one scanner during each CT room replacement.
Current/Planned Improvements • The new scanner at GCC is now fully operational and once the new installations at ACH
are completed the compliance is expected to improve due to increased capacity. • Service Improvement Projects around outpatient CT & MRI bookings are also in
progress.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
6.1
29

% DNA rate for outpatient appointments – Maori (PR057) The percentage of appointments booked for Maori where the patients Did Not Attend (DNA).
Current Target Performance • The trend has been variable and shows a slight increase over the quarter albeit aided by
the positive September 2014 result. • He Kamaka Waiora have focussed their efforts within the cardiac and cancer & blood
services over this period. Extended Stay is now required.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
30

% DNA rate for outpatient appointments – Pacific (PR058) The percentage of appointments booked for Pacific People where the patients Did Not Attend (DNA).
Current Target Performance • DNA rate for Pacific people has trended downwards since December 2013 which is
pleasing to see. However there is on- opportunity to improve on current systems and practices in order to reach the 9% target.
Current/Planned Improvements • Tautai Fakataha are continuing to remind cancer and blood and cardiac patients of their
appointments. As a quality initiative we are working with the cardiac rehab team and Healthy Village Action Zone to ensure a continuity of care into the community, post discharge.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
6.1
31

% Chemotherapy patients (Med Onc and Haem) attending FSA within 4 weeks of referral (PR059) The percentage of patients attending Medical Oncology First Specialist Assessment (FSA) within four weeks of referral.
Current Target Performance • Performance remains in the 90+% range, fluctuation due to referral patterns. Increased
referrals to the normal in September for the breast and melanoma tumour stream in particular.
Current/Planned Improvements • Additional clinics performed and resource reallocation to support the tumour streams. • Production Planning work continues – good graphical illustrations available to the
tumour leads in medical oncology to demonstrate the current state and guide schedulers in their booking.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
32

% Radiation oncology patients attending FSA within 4 weeks of referral (PR064) The percentage of patients attending Radiation Oncology First Specialist Assessment (FSA) within 4 weeks of referral.
Current Target Performance • Performance remains in the 90+% range, fluctuation due to referral patterns.
Current/Planned Improvements • Virtual clinics are being used to monitor patients with prostate cancer, where
appropriate. This increases capacity for new patients. Will roll this model out to other tumour streams.
• Introduction of tumour stream Nurse Specialist in to radiation oncology – Head and Neck, GU and Gynaecology in particular have a supportive programme for the Nurse Specialist which will enable to NS to manage a cohort of patients who are currently being seen by a SMO.
• Radiation Oncology SMOs have structured themselves to be more tumour stream specific.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
6.1
33

Mental Health Average LOS (KPI Discharges) - Te Whetu Tawera (PR120) The monthly average length of stay (LOS) for Mental Health Adult Acute Unit - Te Whetu Tawera (limited to discharges meeting National KPI definition for inclusion).
Current Target Performance • While average length of stay at Te Whetu Tawera remains above target on a
monthly and year to date basis, over the long run the trend is still downwards and positive.
Current/Planned Improvements • Continued monitoring alongside the maintenance of a range of initiatives aimed
at improving length of stay.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
34

Number of CBU Outliers – Adult (PR173) The number of patients with an assigned CBU (Clinical Business Unit) that is not the CBU of the ward the patient was admitted or transferred to.
Current Target Performance • Continued high patient volumes through October especially in Surgical areas
contributed to outlier numbers.
Current/Planned Improvements • Reset of hospital when capacity allows. • Medium term review of bed modelling.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
6.1
35

% Patients cared for in a mixed gender room at midday – Adult (PR175) The percentage of patients cared for in a mixed gender room based on census at midday – Adult.
Current Target Performance • Variance due to extra mixed gender acute observation units.
Current/Planned Improvements • Continued focus by Charge Nurses and Daily Ops team to provide same gender rooms.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
36
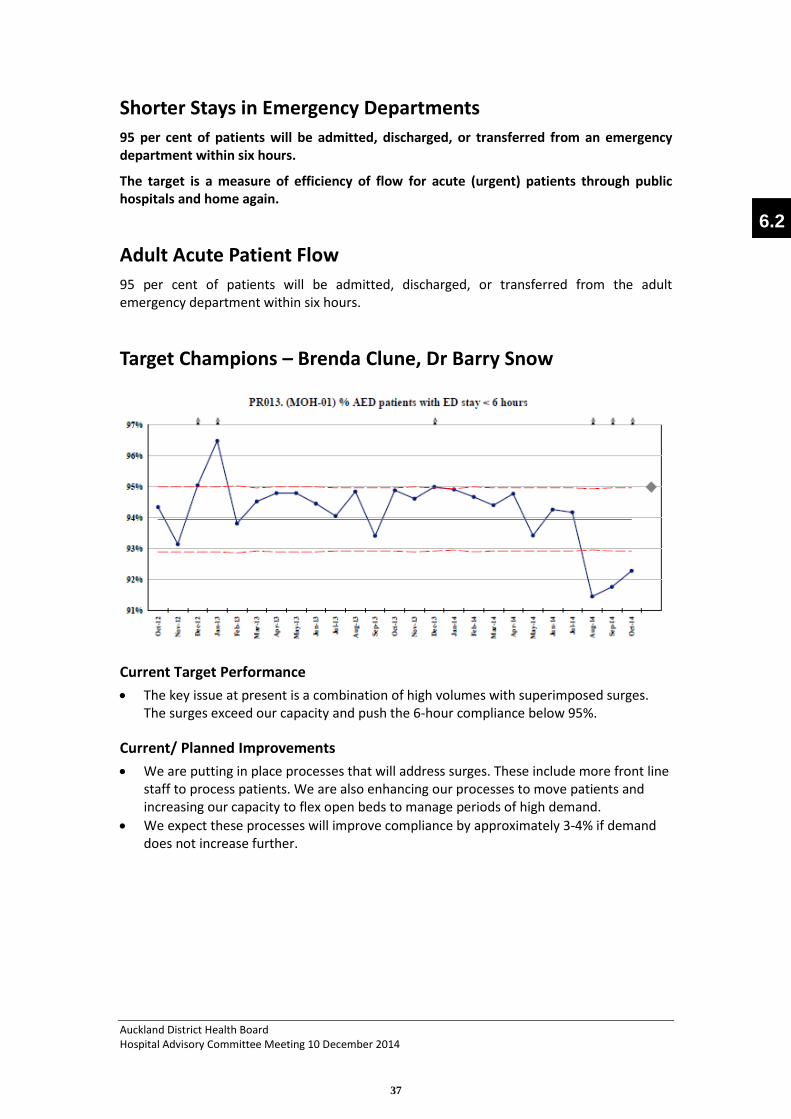
Shorter Stays in Emergency Departments 95 per cent of patients will be admitted, discharged, or transferred from an emergency department within six hours.
The target is a measure of efficiency of flow for acute (urgent) patients through public hospitals and home again.
Adult Acute Patient Flow 95 per cent of patients will be admitted, discharged, or transferred from the adult emergency department within six hours.
Target Champions – Brenda Clune, Dr Barry Snow
Current Target Performance • The key issue at present is a combination of high volumes with superimposed surges.
The surges exceed our capacity and push the 6-hour compliance below 95%.
Current/ Planned Improvements • We are putting in place processes that will address surges. These include more front line
staff to process patients. We are also enhancing our processes to move patients and increasing our capacity to flex open beds to manage periods of high demand.
• We expect these processes will improve compliance by approximately 3-4% if demand does not increase further.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
6.2
37

Children’s Acute Patient Flow 95 per cent of patients will be admitted, discharged, or transferred from the children’s emergency department within six hours.
Target Champion – Mike Shepherd
Current Target Performance • Higher than usual presentations (12% increase on last October), admissions (14%
increase on last October) and staff sickness in October contributed to inability to reach target for this month.
Current/Planned Improvements • Ensuring the aim of the Acute Patient Flow project – “ Valuing our patients time” – is
widely understood and acted upon by all staff at Starship, o Further Starship wide messaging. o CED Shift coordinator workshops focussing on managing acute patient flow.
• Improving the transfer of patients to inpatient wards by o Developing and reporting ward and service specific metrics based on median
time and the 6 hour target. o Develop and implement a process for transfer to the ward without nurse escort
for certain clinically appropriate patients. o Improve the utilisation of the existing policy to expedite admission of certain
patients to the ward. • Improve the utilisation of Clinical Short Stay in Children’s ED
o This facility is reserved for patients whose care is best delivered in CED but some opportunities for short staying patients are being missed currently.
Subsequent work will focus on • Medical staff activity – including discharge (CED) and admission (ward registrars) to
expedite patient care. • Winter planning for 2015
o It is possible that additional resource will be required to maintain acceptable acute patient flow over winter 2015, however this will be the focus of further work over the next 4 months.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
38

Improved Access to Elective Surgery The volume of elective surgery will be increased by at least 4000 discharges per year. DHBs have negotiated local targets taking into consideration the health needs of their communities. Collectively these targets contribute to a national increase in elective surgery discharges. ADHB’s objective is to deliver the MoH target for elective surgical discharges (13,872).
Target Champions – Wayne Jones, Vanessa Beavis, Mark Edwards
Current Target Performance • Total production (ADHB + IDF + Other) for Q1 has been very close to plan, we have re-
phased due to the following: o Our longer waiters had been skewed more than anticipated towards IDF
patients. This has meant we have been delivering more IDF discharges than planned YTD, to bring our ESPI compliance into line. This of course means a reduced number of ADHB discharges.
o Our acute load has been higher than expected, again reducing our capacity to deliver electives.
• However the IDF inflow demand remains high and we are working with the funder in key areas such as Ophthalmology to address the referral flow.
Current/Planned Improvements • Detailed planning by service, patient, and session is in place to manage our achievement
of the 120 day target, and this will ensure we maximise our resource use, bringing our discharge performance back in line.
• The scheduling horizon has been pushed out for FSA and elective surgery to improve visibility of capacity constraints.
• Countdown clock now live on the intranet showing days to the 120 day target. • We have put in place some measures to ensure we sustain the 120 day target, including:
o Shorter Christmas break. o Additional outsourcing in areas of constrained capacity such as Ophthalmology.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
6.2
39

Shorter Waits for Cancer Treatment All patients, ready for treatment, wait less than four weeks for radiotherapy or chemotherapy. The target is for patients who are ready to treat. It excludes patients who require other treatment prior to radiotherapy or chemotherapy, who are not fit to start treatment because of their medical condition or who choose to defer their treatment.
Target Champions – Giuseppe Sasso, David Porter, Richard Doocey
Current Target Performance
Chemotherapy • Continue to meet target for chemotherapy.
Radiation Therapy • Continue to meet target for radiation therapy.
Current/ Planned Improvements • Medical Oncology Day Stay scheduling trial put on hold due to unforeseen consequences
of using the new system. The various issues are being addressed and a new go live date will be established.
• New technologies in radiation oncology are being embedded in to our business as usual processes. The service continues to work towards a paperless system to reduce the time from DTT to treatment.
• Radiation Therapy project underway looking at the elective and acute patient flow through the unit.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
40

Increased Immunisation 95 per cent of eight-month-olds will have their primary course of immunisation (six weeks, three months and five month immunisation events) on time by December 2014.
The quarterly progress result includes children who turned eight months old during the three month period of the quarter and who were fully immunised at that stage.
Target Champion – Mike Shepherd
Current Target Performance • ADHB's coverage for target population at 30 September 2014 is 95% and achieving the
annual target. • Maori immunisation rate at 8 months is 95%; Pacific 97% Asian 97% Other 90% and NZE
95%, Maori coverage has increased 11% in the last quarter. Note: Data is reported quarterly.
Current/Planned Improvements • Work with PHOs to identify practices with higher Maori enrolments and provide
targeted support as required. • Addition of universal oral rotavirus vaccine, change to pneumococcal 13 and varicella
vaccine for special groups introduced from 1 July 2014. • Support ARPHS in Regional Measles Outbreak Response. • Six month milestone plan underway to improve on-time immunisations at 3 and 5
months. • Maternity / PHO enrolment data-match audit underway, outcomes will inform strategies
to increase new born enrolments with primary healthcare.
75%
80%
85%
90%
95%
100%
Sep-
13
Dec
-13
Mar
-14
Jun-
14
Sep-
14
Actu
al a
nd T
arge
t %
95% of 8 months olds are fully immunised - Total Actual vs Target - June 2013 to Sept 2014
Actual Percentage MOH Target %
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
6.2
41

Better Help for Smokers to Quit 95 per cent of hospitalised patients who smoke and are seen by a health practitioner in public hospitals and 90 per cent of enrolled patients who smoke and are seen by a health practitioner in general practice are offered brief advice and support to quit smoking.
Within the target a specialised identified group will include progress towards 90 per cent of pregnant women (who identify as smokers at the time of confirmation of pregnancy in general practice or booking with Lead Maternity Carer) are offered advice and support to quit.
Target Champions – Stephen Child, Margaret Dotchin, Karen Stevens
Current Target Performance • ADHB continues to meet the secondary care target. In October we achieved 97% of
current smokers being given brief advice to quit smoking. Indeed in the 3 month period Aug-Oct we were at 96.8%.
• In the maternal health target we came jointly 1st out of 20 DHBs. The MoH uses national data gathered from MMPO and LMC services into which dataset a high proportion of our midwives do not report. Our own data has even higher positive figures in relation to this target.
• Our ADHB catchment PHOs achieved 99.8% towards their target in Quarter 1.
Current/Planned Improvements • In secondary care we will keep supporting clinical areas with audit and analysis data to
highlight areas for improvement. • We are working on posters and brochures to trigger more patients into quitting. • We are working on a bar coded standard referral form to be used throughout clinics for
the New Year. • A Mental Health Smokefree Co-ordinator has started with us this month primarily to
enhance the smokefree work undertaken in ADHB Community satellite clinics.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
42

More Heart and Diabetes Checks 90 per cent of the eligible population will have had their cardiovascular risk assessed in the last five years.
Target Champion – Stephanie Muncaster
Current Target Performance • Provisional data from weekly Primary Health Organisations (PHO) reports show coverage
at 90%. • Ministry of Health will not provide provisional and final coverage data until November
2014. • Provisional PHO data shows that the DHB is on target at 90% coverage.
Current/ Planned Improvements • General practice has systematic processes in place to invite people to be assessed if they
move into the practice or move into the eligible age group. • General practice has systematic processes in place to recall patients for their five year
assessment if they have not been assessed in the last five years. • PHOs continue to work with cell groups providing information on cell group coverage
and discussion on how to make change in the practice to improve coverage. • PHOs use performance matrix to identify practices with low coverage and target
activities within though practices to increase coverage. • DHB and PHOs meet monthly to discuss matters arising in relation to the target and
proactively discuss solutions.
-
20,000
40,000
60,000
80,000
100,000
120,000
140,000
160,000
0%
20%
40%
60%
80%
100%
120%
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1
2012/13 2013/14 2014/15
Atua
l and
Tar
get V
olum
e
Actu
al a
nd T
arge
t %
More Heart and Diabetes ChecksActual vs Target - July 2012 - September 2014
Actual Percentage MOH Target % Actual Volume MOH Target Volume
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
6.2
43

Cardiac Bypass Surgery To enable timely access to cardiac bypass surgery, the wait list should be no greater than 104. To support the national cardiac bypass intervention target, 1038 bypasses should be completed in 2014/2015.
Target Champion – Dr Mark Edwards
Current Target Performance • During October the service delivered 90 eligible procedures against a plan of 82. The
service has had 10 cancellations. These cancellations were due to substitution by acute and bed unavailability in the CVICU. We have maintained a high level of production and reduced our cancellation rate which has enabled us to deliver over our production target for the month of October. The result of this has been a decrease in the waiting list from 101 to 71.
• The service continued to have ECMO activity over the month of October, although lower numbers. There was an increase in both acute work and thoracic cases throughout October.
• At month end there were 5 patients waiting in hospital, 38 waiting up to 60 days and 30 waiting between 60 and 120 days. There was 1 patient waiting beyond 120 days.
• The challenge for the service over the next few months is to maintain production during the lead up to and beyond the Christmas period. The service needs to be in a strong position prior to Christmas to continue the trend of the waitlist reducing. In addition the service needs to meet target times for P1 patients (inpatient) within 10 days), P2 patients within 30 days and P3 patients within 120 days. The service has remained ESPI 2 and 5 compliant.
Current/ Planned Improvements • Weekend contract cases continue the service has completed 8 cases during the month
of October. • The service has sent 1 patient to Waikato in October however due to Waikato’s increase
in their own waitlist no further patients have been sent. • Theatre cancellation data project is continuing. • Cardiac surgery referrals project/Patient experience work has commenced. Key
members of the team are meeting fortnightly to review the patient experience on the waitlist and identify potential improvements.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
44

Financial Performance Consolidated Statement of Financial Performance - October 2014 Provider Month YTD
$000s Actual Budget Variance Actual Budget Variance
Income Government and Crown Agency sourced 6,639 6,606 33 F 26,867 26,556 311 F
Non-Government & Crown Agency Sourced 7,274 8,274 (1,000)
U 28,862 30,039 (1,177) U
Inter-DHB & Internal Revenue 1,172 1,222 (50) U 5,168 5,051 117 F
Internal Allocation DHB Provider 96,543 95,085 1,457 F 387,770 386,171 1,599 F
111,628 111,188 441 F 448,667 447,817 850 F
Expenditure
Personnel 68,997 68,715 (283) U 271,523 271,544 22 F
Outsourced Personnel 2,127 1,297 (830) U 7,453 5,186 (2,268) U
Outsourced Clinical Services 2,027 2,113 87 F 8,009 8,161 152 F
Outsourced Other 3,554 3,651 97 F 14,256 14,814 558 F
Clinical Supplies 20,090 19,630 (460) U 78,763 79,688 925 F Infrastructure & Non-Clinical Supplies 14,661 14,089 (572) U 57,918 56,144 (1,774)
U Internal Allocations 803 796 (8) U 3,212 3,148 (64) U
Total Expenditure 112,258 110,289 (1,969) U 441,134 438,68
5 (2,450)
U
Net Surplus / (Deficit) (630) 899 (1,529) U 7,533 9,132 (1,599)
U
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
6.3
45

Consolidated Statement of Financial Performance – October 2014 Performance Summary by Directorate
Provider Variance Month
Variance FTE Month
Variance YTD
Variance FTE YTD
$000s $000’s $000’s
Adult Medical Services (471) U (16) U (1,469) U (5) U
Adult Community and LTC 202 F 13 F 987 F 22 F
Surgical Services (129) U 2 F 84 F 12 F
Women's Health & Genetics (121) U (11) U (203) U (13) U
Child Health (161) U 18 F 217 F 28 F
Cardiac Services 31 F (8) U (162) U (6) U
Clinical Support Services 566 F 63 F 2,206 F 54 F
Non-Clinical Support Services 106 F (4) U (279) U (13) U
Perioperative Services (332) U 36 F (659) U 40 F
Cancer & Blood Services 415 F (2) U 695 F 0 F
ACH Others (1,381) U 0 F (2,720) U 0 F
Mental Health 155 F 44 F 948 F 37 F
Ancillary Services (410) U (12) U (1,244) U 0 F
TOTAL (1,529) U 122 F (1,599) U 157 F
Consolidated Statement of Personnel By Professional Group – October 2014
Employee Group Actual FTE Month
Variance FTE
Month Variance Month
Actual FTE YTD
Variance FTE YTD
Variance YTD
$000’s $000’s
Medical Personnel 1,280 37 F (324) U 1,264 43 F (1,360) U
Nursing Personnel 3,410 (8) U (1,154) U 3,387 18 F (2,264) U
Allied Health Personnel 1,767 123 F 672 F 1,740 116 F 2,840 F
Support Personnel 492 43 F 184 F 497 38 F 329 F
Management/Admin Personnel 1,166 56 F 339 F 1,152 60 F 477 F
Total (before Outsourced) 8,116 251 F (283) U 8,041 274 F 22 F
Outsourced Medical 35 (1) U (24) U 29 5 F 218 F
Outsourced Nursing 6 (6) U (83) U 6 (6) U (62) U
Outsourced Allied Health 9 (7) U (95) U 9 (6) U (137) U
Outsourced Support 44 (44) U (148) U 46 (46) U (624) U
Outsourced Mgmt/Admin 80 (71) U (480) U 72 (63) U (1,662) U
Total Outsourced Personnel 175 (129) U (830) U 163 (117) U (2,268) U
Total Personnel 8,291 122 F (1,113) U 8,204 157 F (2,246) U
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
46

Month Result The Provider arm result for the month is $1.5M unfavourable.
Total revenue is $0.4M favourable – the key variance is $0.6M Research Grants – this income is offset by equivalent expenditure and is bottom line neutral.
Total expenditure is $1.9M unfavourable, with the key variances as follows: • Personnel costs $0.3M unfavourable – total expenditure is 0.4% above budget for the month, with
the key variance Nursing $1.1M unfavourable, reflecting planned average cost per FTE reductions not met. This unfavourable variance is offset by savings from total FTE across all categories being 251 below budget for the month.
• Outsourced Personnel $0.8M unfavourable - $0.2M of this relates to contract cleaning staff - a number of staff transferred to ADHB with very high leave balances and there has been a concerted effort to try and get as many staff off on leave as possible to reduce this leave liability, thus driving higher outsourced costs. Administration is $0.5M unfavourable - covering vacancies and project work in the Corporate area.
• Clinical Supplies $0.5M (2.3%) unfavourable primarily due to volumes for the month being higher than contract – latest estimated month performance is 4.5% above contact.
• Infrastructure & Non Clinical Supplies $0.6M (4.0%) unfavourable – due to timing of electricity and maintenance costs.
YTD Result The YTD Provider arm result is $1.6M unfavourable.
Overall volumes are reported at 99.0% of YTD base contract, however the latest estimate based on YTD 94% coded gives total contract performance at 99.7% - this equates to $1.1M below contract (not recognised in the YTD result).
YTD Provider arm revenue is $0.9M (0.2%) favourable, primarily due to non patient care revenue streams such as Research Grants (offset by equivalent expenditure and is bottom line neutral) and Interest Income.
YTD Provider arm expenditure is $2.5M (0.6%) unfavourable, with key variances as follows: • Personnel Costs are very close to budget – FTE are 274 below budget, largely due to Allied
Health/Technical vacancies. The favourable variance resulting from the lower FTE offsets planned average cost per FTE reductions not met and a $1.7M unfavourable variance for an increase in the valuation of retiring gratuities and CME liability.
• Outsourced Employee Costs $2.3M (43.7%) unfavourable - $0.6M of this relates to contract cleaning staff - a number of staff transferred to ADHB with very high leave balances and there has been a concerted effort to try and get as many staff off on leave as possible to reduce this leave liability, thus driving higher outsourced costs. The balance is Administration $1.7M unfavourable - covering vacancies and project work.
• Clinical Supplies $0.9M (1.2%) favourable, reflecting overall volume performance at 99.7% of contract.
• Infrastructure & Non Clinical Supplies $1.2M (3.2%) unfavourable – interest rate hedging costs are $1.2M unfavourable due to a downward revaluation of the Bond FRA reflecting increased long term interest rates.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
6.3
47

FTE Total FTE (including outsourced) for October is 8,291 which is 122 FTE below budget and 99 above last month – 63 of the increase from last month is due to the transfer of Anatomical Pathology staff from DML/LTA. Medical and Allied Health are below budget, and these are partly offset by Support, Nursing and Management/Administration all slightly above budget.
14/15 Savings Programme For 2014/15 one of our key priorities is to continue with a business transformation framework to deliver long-term financial and service sustainability in line with our strategic plan to live within our means. The recently established single point of accountability framework will provide the clinical leadership to deliver services in a cost efficient and productive manner.
The savings programme has been developed based on the Board’s decision to submit a zero deficit budget position in the 2014/15. The savings required to be found to close the budget gap is $49.5M. The Provider Arm savings represents $39.3M, categorised as either Business as Usual ($9.8M) or Business Transformation ($29.5M).
Key Strategies The savings target of $39.3M is linked to each directorate’s objective and fall into one of three key strategies being cost containment, model of service delivery changes and revenue growth in defined areas.
For HAC the Business Transformation target of $29.5M and monthly progress will be reported in this paper.
Table 1: Provider Arm Services Savings Target ($000’s) Cause of Change Revenue growth Cost Containment Model of service
delivery 14/15 Savings
Target
Business as Usual 848 7,405 1,580 9,832
Business Transformation 5,471 16,665 7,439 29,476
Grand Total $6,319 $23,970 $9,019 $39,308
FTE Impact on 14/15 budget 0.50 25.40 25.90 Business Transformation – October Update For the four months to October 2014, $10.3M savings were reported against budget of $9M, exceeding budget by $1.2M F.
The favourable variance of $1.2M is attributed to unbudgeted personnel savings in Clinical Support ($1.5M F) and Surgical ($657k F) as part of the cost containment strategy ($2.3M F). The $1.2M F unbudgeted savings has helped to mitigate the unfavourable performance in revenue growth initiatives $470 k U (Surgical $228k U, Children’s $202k U) and model of service delivery $640k U (Surgical $414k U, Women’s $57k U, Clinical Support $238k U and Non Clinical Support $108k U).
Note, some of the initiatives reporting unfavourable variances indicate timing factors between the budget phasing and when savings will be achieved. This applies mainly to Surgical Services where savings are expected to be achieved.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
48

Table 2: Business Transformation by Key Strategy – October 14 YTD ($000’s) Strategy Main Category 14/15 Savings
Budget YTD
Actual YTD
Budget Var.
Revenue growth Government and Crown Agency $3,387 $579 $1,084 -$505
Non-Government & Crown Agency $2,084 $730 $695 $35
Revenue growth in defined areas Total $5,471 $1,309 $1,779 -$470
Model of service Outsourced Services $2,058 $67 $613 -$546
Personnel $4,001 $1,144 $1,248 -$105
Clinical Supplies -$105 $35 -$34 $69
Infrastructure & Non-Clinical $575 $0 $108 -$108
Internal Alloc’n DHB Provider $910 $353 $303 $50
Model of service delivery changes Total $7,439 $1,599 $2,238 -$640
Cost Containment Personnel $5,296 $3,021 $1,467 $1,554
Clinical Supplies $10,579 $3,370 $3,372 $5
Infrastructure & Non-Clinical $690 $313 $230 $83
Internal Alloc’n DHB Provider $0 $657 $0 $657
Cost Containment Total $16,565 $7,361 $5,069 $2,299
Grand Total $29,476 $10,269 $9,087 $1,189
Key Points by Service
• Adult Medical – exceeded budget by $74k F. This is mainly attributed to adult emergency medicine laboratory cost reductions exceeding budget by $127k F which has helped to mitigate unfavourable variances in DCCM ($40k U) and IVIG ($13k U).
• Adult Community & LTC – exceeded budget by $38k F. This is mainly driven by the OPH skill mix review and reduction in 8 OPH beds. Both initiatives are progressing with savings being achieved.
• Adult Surgical – exceeded budget by $15k F. Higher savings in Personnel Costs due to improvement in recruitment processes. There are timing factors in the revenue related initiatives ($228k U) and service model changes ($414k U). Revenue initiatives include ACC, Non Residents, additional Renal transplants, Ophthamology acute revenue and co-payments for high cost patients. The model of service delivery initiatives are made up of the pathway design, scheduling and booking process and theatre productivity. Project work has commenced with the Pathway redesign and Theatre productivity initiatives which are in consultation phase and the Scheduling & Booking initiative is awaiting approval. The service is projecting to achieve budgeted savings for the year.
• Women’s – unfavourable variance $57k U. The key initiative is the Redesign of Community Midwifery model of care which will not proceed until after the collaboration with WDHB has been completed. This is expected to delay the programme and savings until fourth quarter. Therefore some of the savings will be expected to be achieved in 2015/16.
• Children’s – unfavourable variance $102k U. This is due to unfavourable variances from the partnership with Starship Foundation ($133k U) and TPN co-payments ($250k U). Some of this has been partially offset by better performing initiatives such as ACC income ($119k F), Non Resident income ($95k F) medical and nursing ($100K F).
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
6.3
49

• Cardiac Services – unfavourable variance $28k U. The unfavourable variance relates to the heart valve cost initiative ($81k U) partially offset by favourable savings in cardiac surgical efficiencies ($51k F). The service has negotiated reduced prices for heart valves and this is now being discussed with surgeons for approval for use.
• Clinical Support – exceeded budget by $1,237k F. The favourable year to date result is mainly attributed to unbudgeted personnel savings of $1,527k F. This has offset initiatives such as outsourcing reductions ($203k U), Scheduling & Booking process ($75k U) and other staff initiatives ($69k U).
• Non Clinical Support – unfavourable variance of $27k U. Unbudgeted photocopier and printer savings ($145k F) has offset HBL Food ($42k U), Waste volume ($67k U) and security savings ($63kU).
• Perioperative Services – exceeded budget by $4k F. The savings are attributed to cost containment of clinical supplies and waste management initiatives.
• Cancer & Blood – exceeded budget by $21k F. The savings relate to Haematology vacancies.
• Mental Health – exceeded budget by $13k F. The savings relate to managing excess leave and flexi-fund reduction initiatives.
• Functional – exceeded budget by $2k F. This is an improvement from the previous month. Savings reported in interest revenue ($67k) and capital charge ($168k).
• Human Resources – achieved budget with total savings of $936k. HR savings have been reported in SMO costs and sick leave savings.
• HealthAlliance – achieved budget with total savings of $2,600k. This is assessed based on the year to date result for spend on consumables and supplies.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
50

Table 3: Savings Summary by Service – October 14 YTD ($000’s)
Service Strategy
14/15 Savings Budget
YTD Actual
YTD Budget Variance
Adult Medical Model of service delivery changes $70 $11 $24 -$13 Cost Containment $177 $147 $60 $87 Adult Medical Total $247 $158 $84 $74 Adult Community & LTC Model of service delivery changes $810 $306 $268 $38 Adult Community & LTC Total $810 $306 $268 $38 Surgical Revenue growth in defined areas $2,821 $712 $940 -$228 Model of service delivery changes $1,262 $0 $414 -$414 Cost Containment $0 $657 $0 $657 Surgical Total $4,083 $1,369 $1,354 $15 Womens Model of service delivery changes $180 $3 $60 -$57 Womens Total $180 $3 $60 -$57 Childrens Revenue growth in defined areas $1,950 $448 $650 -$202 Model of service delivery changes $2,395 $899 $798 $101 Cost Containment $800 $266 $267 -$1 Childrens Total $5,145 $1,613 $1,715 -$102 Cardiac Model of service delivery changes $450 $51 $0 $51 Cost Containment $735 $10 $90 -$80 Cardiac Total $1,185 $62 $90 -$28 Clinical Support Revenue growth in defined areas $300 $82 $100 -$18 Model of service delivery changes $1,697 $328 $566 -$238 Cost Containment $1,879 $2,119 $626 $1,493 Clinical Support Total $3,876 $2,529 $1,292 $1,237 Non Clinical Support Model of service delivery changes $575 $0 $108 -$108 Cost Containment $190 $145 $63 $82 Non Clinical Support Total $765 $145 $172 -$27 Perioperative Cost Containment $400 $130 $133 $4 Perioperative Total $400 $130 $133 $4 Cancer & Blood Cost Containment $135 $65 $44 $21 Cancer & Blood Total $135 $65 $44 $21 Mental Health Revenue growth in defined areas $200 $0 $22 -$22 Cost Containment $249 $118 $83 $35 Mental Health Total $449 $118 $105 $13 Functional Revenue growth in defined areas $200 $67 $67 $0 Cost Containment $500 $168 $167 $1 Functional Total $700 $235 $233 $2 Human Resources Cost Containment $3,700 $936 $936 -$0 Human Resources Total $3,700 $936 $936 -$0 healthAlliance Cost Containment $7,800 $2,600 $2,600 $0 healthAlliance Total $7,800 $2,600 $2,600 $0 Grand Total $29,476 $10,269 $9,087 $1,189
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
6.3
51

Volume Performance
1) Combined DRG and Non-DRG Activity (All DHBs)
October 2014 Year to Date$000s $000s
Directorate Service Cont Act Var Prog % Cont Act Var Prog %A+ Links, HOP, Rehab 4,120 3,891 (228) 94.5% 16,400 15,223 (1,177) 92.8%Ambulatory Services 2,025 1,908 (117) 94.2% 8,237 7,649 (588) 92.9%
6,145 5,799 (346) 94.4% 24,638 22,873 (1,765) 92.8%
AED, APU, DCCM, Air Ambulance
1,892 1,886 (5) 99.7% 7,307 7,470 163 102.2%
Gen Med, Gastro, Resp, Neuro, ID, Renal
9,845 10,227 382 103.9% 41,371 42,122 752 101.8%
11,737 12,114 377 103.2% 48,678 49,592 914 101.9%
Elective, Interp 19 19 0 100.0% 76 76 0 100.0%Gen Surg, Trauma, Ophth, GCC, PAS
7,825 7,633 (192) 97.5% 31,937 30,614 (1,323) 95.9%
N Surg, Oral, ORL, Transpl, Uro
8,234 7,869 (365) 95.6% 33,433 33,296 (137) 99.6%
Orthopaedics Adult 4,127 4,360 233 105.6% 16,775 15,995 (780) 95.4%20,206 19,882 (324) 98.4% 82,220 79,980 (2,240) 97.3%
8,117 7,770 (347) 95.7% 32,535 30,910 (1,625) 95.0%
10,129 11,598 1,469 114.5% 41,821 43,647 1,826 104.4%
Child Health & Disability 904 887 (17) 98.1% 3,541 3,479 (61) 98.3%Medical & Community 6,269 7,128 859 113.7% 26,837 26,702 (135) 99.5%Paediatric Cardiac & ICU 3,642 3,313 (329) 91.0% 14,770 14,071 (699) 95.3%Surgical & Community 4,387 4,357 (30) 99.3% 17,669 18,024 356 102.0%
15,202 15,685 483 103.2% 62,816 62,276 (540) 99.1%
1,896 2,195 298 115.7% 7,652 8,428 776 110.1%
5,825 5,825 0 100.0% 22,687 22,687 0 100.0%
39 39 0 100.0% 154 154 0 100.0%
129 129 0 100.0% 503 503 0 100.0%
102 102 0 100.0% 398 398 0 100.0%
Genetics 220 212 (8) 96.4% 889 900 11 101.3%Women's Health 7,070 6,808 (262) 96.3% 28,102 27,239 (863) 96.9%
7,290 7,020 (270) 96.3% 28,991 28,139 (852) 97.1%
86,816 88,158 1,342 101.5% 353,093 349,588 (3,505) 99.0%
Women's Health
Women's Health Total
Grand Total
Clinical Support Services
DHB Funds
Mental Health & Addictions Total
Public Health Services
Support Services
Surgical Services Total
Cancer & Blood Services
Cardiac Services
Children's Health
Children's Health Total
Adult Community & LTC Total
Adult Medical Services
Adult Medical Services Total
Surgical Services
Adult Community & LTC
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
52

2) Total Discharges for the YTD October 2014
Directorate Service 2014 2015 Last YTD This YTD % Change Last YTD This YTD Last YTD This YTD
A+ Links, HOP, Rehab 0 0 833 784 (5.9%) 9 4 1.1% 0.5%Ambulatory Services 611 598 707 690 (2.4%) 646 618 91.4% 89.6%
Adult Community & LTC Total 611 598 1,540 1,474 (4.3%) 655 622 42.5% 42.2%
AED, APU, DCCM, Air Ambulance 3,637 3,647 3,637 3,649 0.3% 2,638 2,631 72.5% 72.1%
Gen Med, Gastro, Resp, Neuro, ID, Renal 6,821 6,722 6,910 6,786 (1.8%) 1,145 1,065 16.6% 15.7%
Adult Medical Services Total 10,458 10,369 10,547 10,435 (1.1%) 3,783 3,696 35.9% 35.4%
Cancer & Blood Total 1,687 1,645 1,919 1,805 (5.9%) 916 808 47.7% 44.8%
Cardiac Services Total 2,802 2,808 2,918 2,876 (1.4%) 733 715 25.1% 24.9%
Medical & Community 5,065 5,656 5,501 6,287 14.3% 3,140 3,556 57.1% 56.6%Paediatric Cardiac & 672 780 727 862 18.6% 164 174 22.6% 20.2%
Surgical & Community 3,163 3,298 3,383 3,490 3.2% 1,739 1,665 51.4% 47.7%
Children's Health Total 8,900 9,734 9,611 10,639 10.7% 5,043 5,395 52.5% 50.7%
Gen Surg, Trauma, Ophth, GCC, PAS 5,488 5,358 6,263 5,951 (5.0%) 3,473 3,186 55.5% 53.5%N Surg, Oral, ORL,
Transpl, Uro 3,709 3,644 3,955 3,916 (1.0%) 1,596 1,601 40.4% 40.9%Orthopaedics Adult 1,530 1,688 1,668 1,813 8.7% 314 322 18.8% 17.8%
Surgical Services Total 10,727 10,690 11,886 11,680 (1.7%) 5,383 5,109 45.3% 43.7%
Women's Health Total 7,423 7,475 7,728 7,730 0.0% 3,079 3,087 39.8% 39.9%
Grand Total 42,608 43,319 46,149 46,639 1.1% 19,592 19,432 42.5% 41.7%
Same Day as % of all discharges
Children's Health
Surgical Services
Adult Medical Services
Adult Community & LTC
Cases Subject to WIES PaymentInpatient
All Discharges Same Day discharges
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
6.3
53

3) Caseweight Activity for the YTD October 2014 (All DHBs)
Directorate Service Con Act Var Con Act Var Prog % Con Act Var Con Act Var Prog % Con Act Var Con Act Var Prog %
276 281 5 1,290 1,314 23 101.8% 39 38 (2) 184 176 (8) 95.7% 315 318 3 1,474 1,489 15 101.0%
AED, APU, DCCM, Air Ambulance
1,021 1,062 40 4,781 4,971 189 104.0% 0 0 0 0 0 0 0.0% 1,021 1,062 40 4,781 4,971 189 104.0%
Gen Med, Gastro, Resp, Neuro, ID, Renal
5,841 6,013 172 27,347 28,152 805 102.9% 1 0 (1) 7 0 (7) 0.0% 5,842 6,013 170 27,354 28,152 798 102.9%
6,862 7,075 212 32,128 33,123 995 103.1% 1 0 (1) 7 0 (7) 0.0% 6,864 7,075 211 32,135 33,123 988 103.1%
Gen Surg, Trauma, Ophth, GCC, PAS
2,936 2,678 (257) 13,745 12,540 (1,204) 91.2% 2,451 2,365 (86) 11,477 11,074 (403) 96.5% 5,387 5,044 (343) 25,221 23,614 (1,607) 93.6%
N Surg, Oral, ORL, Transpl, Uro
2,631 2,520 (111) 12,320 11,798 (522) 95.8% 2,368 2,479 111 11,085 11,605 520 104.7% 4,999 4,999 (1) 23,405 23,403 (2) 100.0%
Orthopaedics Adult
1,786 1,976 190 8,364 9,251 888 110.6% 1,419 1,077 (342) 6,646 5,043 (1,603) 75.9% 3,206 3,053 (153) 15,009 14,294 (715) 95.2%
7,353 7,174 (179) 34,429 33,590 (839) 97.6% 6,238 5,921 (317) 29,207 27,722 (1,486) 94.9% 13,592 13,095 (496) 63,636 61,311 (2,324) 96.3%
2,002 1,910 (92) 9,373 8,941 (432) 95.4% 0 0 0 0 0 0 0.0% 2,002 1,910 (92) 9,373 8,941 (432) 95.4%
5,028 5,496 469 23,539 25,733 2,194 109.3% 3,076 2,985 (91) 14,403 13,978 (426) 97.0% 8,104 8,482 378 37,942 39,710 1,769 104.7%
Medical & Community
3,954 3,922 (32) 18,512 18,363 (149) 99.2% 0 0 0 0 0 0 0.0% 3,954 3,922 (32) 18,512 18,363 (149) 99.2%
Paediatric Cardiac & ICU
1,984 1,836 (148) 9,288 8,594 (694) 92.5% 871 899 28 4,078 4,209 131 103.2% 2,855 2,734 (120) 13,366 12,803 (563) 95.8%
Surgical & Community
1,829 1,742 (87) 8,563 8,155 (408) 95.2% 1,479 1,633 153 6,926 7,644 717 110.4% 3,308 3,374 66 15,489 15,798 309 102.0%
7,767 7,499 (267) 36,363 35,112 (1,252) 96.6% 2,350 2,531 181 11,004 11,852 848 107.7% 10,117 10,031 (86) 47,367 46,964 (404) 99.1%
3,489 3,498 9 16,336 16,377 40 100.2% 736 629 (107) 3,447 2,945 (502) 85.4% 4,225 4,127 (98) 19,783 19,322 (461) 97.7%
32,776 32,932 156 153,458 154,188 730 100.5% 12,442 12,104 (337) 58,252 56,672 (1,580) 97.3% 45,218 45,037 (181) 211,710 210,860 (850) 99.6%Excludes caseweight Provision
$000s
Adult Medical Services
Adult Community & LTC
Adult Medical Services Total
Surgical Services
$000s Case Weighted Volume
Women's Health Service
Grand Total
Case Weighted Volume
$000sCase Weighted
Volume
Surgical Services Total
Cancer & Blood Service
Cardiac Service
Children's Health
Children's Health Total
Acute Elective Total
Acute - there is a continuing increase in delivery compared to the previous two months as acute WIES is now over contract (when previously it was 98.5% Sep YTD). Discharges are up 2.2% on the same period last year and average WIES is down 2% continuing the lower casemix trend this financial year. • Acute medical discharges are up 2.2%. Average WIES is up 2.6% compared with the same period last year (in contrast to Sep) while ALOS is the same as last month. • Acute surgical discharges are up 1.2%, while average WIES has increased from last month. ALOS has stayed stable. • Obstetric and newborn activity is still up and the average WIES has increased. ALOS has increased this month.
Elective discharges are down on last year by 0.7%, and still below contract, although there has been a 3% improvement against contract reflecting phasing impacts. However, average WIES has now increased above last year. Cardiothoracic has again improved and is now at 84% of the same period last year which is likely to be influencing the average WIES. Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
54

4) Non-DRG Activity (ALL DHBs)
Underperformance to contract is slowly improving but continues to be affected by Cancer & Blood services which are now contributing 44% of the variance, although their performance to contract has improved on last month. This is of concern because this service is subject to wash up and presents a financial risk.
The other major contributor is AT&R bed days which is continuing to track significantly below contract and is likely to do so for the rest of the financial year. If Cancer & Blood manage to reach contract, there is still likely to be under delivery against contract for the ADHB Funder. However, other performance to funding envelope for other Funders is likely to be over.
October 2014 Year to Date$000s $000s
Directorate Service Cont Act Var Prog % Cont Act Var Prog %A+ Links, HOP, Rehab 4,120 3,891 (228) 94.5% 16,400 15,223 (1,177) 92.8%Ambulatory Services 1,681 1,504 (177) 89.5% 6,764 6,160 (603) 91.1%
5,801 5,395 (406) 93.0% 23,164 21,383 (1,780) 92.3%
AED, APU, DCCM, Air Ambulance
624 630 6 100.9% 2,526 2,499 (27) 98.9%
Gen Med, Gastro, Resp, Neuro, ID, Renal
3,475 3,471 (4) 99.9% 14,017 13,971 (47) 99.7%
4,099 4,101 2 100.0% 16,543 16,470 (73) 99.6%
Elective, Interp 19 19 0 100.0% 76 76 0 100.0%Gen Surg, Trauma, Ophth, GCC, PAS
1,659 1,785 125 107.6% 6,716 7,000 284 104.2%
N Surg, Oral, ORL, Transpl, Uro 2,526 2,500 (27) 98.9% 10,027 9,893 (134) 98.7%
Orthopaedics Adult 437 467 30 106.8% 1,766 1,701 (65) 96.3%4,642 4,771 128 102.8% 18,584 18,669 85 100.5%
5,772 5,490 (282) 95.1% 23,162 21,969 (1,192) 94.9%
973 1,002 29 103.0% 3,879 3,937 58 101.5%
Child Health & Disability 904 887 (17) 98.1% 3,541 3,479 (61) 98.3%Medical & Community 2,072 1,986 (86) 95.9% 8,325 8,339 14 100.2%Paediatric Cardiac & ICU 349 313 (36) 89.7% 1,404 1,268 (135) 90.4%Surgical & Community 540 520 (20) 96.4% 2,179 2,226 47 102.1%
3,864 3,706 (158) 95.9% 15,449 15,312 (136) 99.1%
1,896 2,195 298 115.7% 7,652 8,428 776 110.1%
5,825 5,825 0 100.0% 22,687 22,687 0 100.0%
39 39 0 100.0% 154 154 0 100.0%
129 129 0 100.0% 503 503 0 100.0%
102 102 0 100.0% 398 398 0 100.0%
Genetics 220 212 (8) 96.4% 889 900 11 101.3%Women's Health 2,057 1,916 (141) 93.2% 8,319 7,917 (402) 95.2%
2,277 2,128 (149) 93.5% 9,208 8,817 (391) 95.8%
35,420 34,884 (536) 98.5% 141,383 138,728 (2,655) 98.1%
Clinical Support Services
DHB Funds
Children's Health Total
Adult Community & LTC
Adult Community & LTC Total
Adult Medical Services
Adult Medical Services Total
Surgical Services
Surgical Services Total
Children's Health
Cardiac Services
Cancer & Blood Service
Grand Total
Women's Health Total
Mental Health & Addictions
Public Health Service
Support Services
Women's Health
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
6.3
55


ADHB Compliments – Monthly Report October 2014 File ID Submission
Date Method Comments Category Submitting Unit
(physical location) Directorate (geographical site)
136244 06/10/2014 Feedback form
Nurse at Outpatients Clinic SSH is very kind, patient and helpful with child.
Attitude/Courtesy OUTPATIENTS - SCH
CHILDREN’S HEALTH
136245 06/10/2014 Feedback form
Hospital Aide in Ward 24B very hard working, friendly and looks after patients and their families well.
Attitude/Courtesy WARD 24B CHILDREN’S HEALTH
136246 06/10/2014 Feedback form
HCA in Ward 24B friendly, polite and smiling consistently.
Attitude/Courtesy WARD 24B CHILDREN’S HEALTH
136248 09/10/2014 Feedback form
Patient thanks all nurses in Ward 61 for their communication skills and effective care management, helped patient feel comfortable.
Care/Treatment WARD 61 ADULT SURGICAL SERVICES
136252 09/10/2014 Feedback form
Daughter of patient thanks staff of Ward 63 for helping her dad get better.
Care/Treatment WARD 63 ADULT MEDICAL SERVICES
136260 09/10/2014 Feedback form
Staff of Ward 97 compassionate, loving and caring. They connect with their patients.
Attitude/Courtesy WARD 97 WOMENS HEALTH
136262 09/10/2014 Feedback form
All Ward 97 staff caring and friendly. Attitude/Courtesy WARD 97 WOMEN’S HEALTH
09/10/2014 Feedback form
Meals fantastic but very large. Dietary WARD 97 CLINICAL SUPPORT SERVICES - COMMERCIAL SERVICES
136263 09/10/2014 Feedback form
Staff of Ward 63 friendly, helpful, attentive and empathetic. Explained things so patient could understand.
Attitude/Courtesy WARD 63 ADULT MEDICAL SERVICES
136292 09/10/2014 Feedback form
CED staff were helpful friendly and efficient. Treated family with respect and empathy.
Attitude/Courtesy EMERGENCY DEPARTMENT - CHILDRENS (CED)
CHILDREN’S HEALTH
136293 09/10/2014 Feedback form
CED provided wonderful care of 6 year old and great support for family.
Care/Treatment EMERGENCY DEPARTMENT -
CHILDREN’S HEALTH
7.1
56

File ID Submission Date
Method Comments Category Submitting Unit (physical location)
Directorate (geographical site)
CHILDRENS (CED)
136483 02/10/2014 Feedback form
Nurse in Ward 24B was very loving, kind and supported family whole time before and after baby’s operation.
Attitude/Courtesy WARD 24B CHILDREN’S HEALTH
136541 10/10/2014 Feedback form
Nurses and doctors and cooks were great made my pain go away faster when people are kind and cheerful. Thanks heaps.
Attitude/Courtesy WARD 97 WOMEN’S HEALTH
136542 10/10/2014 Feedback form
The care of the staff has been great, and most helpful.
Care/Treatment WARD 97 WOMEN’S HEALTH
136577 10/10/2014 Feedback form
HCA of Ward 24A very friendly and helpful. Attitude/Courtesy WARD 24A CHILDREN’S HEALTH
136579 10/10/2014 Telephone Patient found Eye Clinic staff kind, helpful, people focused.
Care/Treatment OPHTHALMOLOGY CLINIC
ADULT SURGICAL SERVICES
136580 13/10/2014 Feedback form
I was a support person to my daughter and found all staff to be exceptionally professional, helpful, caring and informative. I could not fault anything and my daughter was in agreement. Thank you for all your care and expertise. I did discuss the after procedure brochure with a nurse as nowhere did it mention to cease exercise for a 10 - 14 day period after termination and we think that should be mentioned. Only because there is a sentence that says "most women can go back to their usual activities the next day".
Care/Treatment EPSOM DAY UNIT WOMEN’S HEALTH
136582 13/10/2014 Feedback form
Great friendly help my friend found it an easy process with support from staff. Thank you for all your care.
Attitude/Courtesy EPSOM DAY UNIT WOMEN’S HEALTH
136583 13/10/2014 Feedback form
Day 1 - Fantastic service, ethical, empathetic and non-judgemental. Thank you. Day 2 - Once again outstanding service, care and after care. Thank you to the lovely
Attitude/Courtesy EPSOM DAY UNIT WOMEN’S HEALTH
57

File ID Submission Date
Method Comments Category Submitting Unit (physical location)
Directorate (geographical site)
and competent staff who made a hideous experience and choice bearable.
136584 13/10/2014 Feedback form
I was made to feel so comfortable and not judged in anyway what so ever. The nurses here are amazing - give them all a pay rise I reckon. Thank you so much.
Care/Treatment EPSOM DAY UNIT WOMEN’S HEALTH
13/10/2014 E-mail The staff members of ED, Ward 63 and Awatea Ward at all levels are the epitome of kindness and efficiency.
Attitude/Courtesy WARD 63 ADULT MEDICAL SERVICES
136585 13/10/2014 E-mail The facilities are modern, bright and clean and the food is more than adequate in both quantity and variety.
Environment Dietary
WARD 63 ADULT MEDICAL SERVICES
136586 15/10/2014 Feedback form
All staff of Ward 63 delivered excellent care every day to patient and made journey stress free for family.
Care/Treatment WARD 63 ADULT MEDICAL SERVICES
136588 13/10/2014 Feedback form
Really good. Staff were professional and informative. Nursing staff were excellent. Staff were very comforting during surgery. Partner support through the pill taking process could be a possibility for the future.
Care/Treatment EPSOM DAY UNIT WOMEN’S HEALTH
136593 13/10/2014 Feedback form
Nurses and doctors were really friendly and informative about everything. Very friendly and felt comfortable. Thank you all.
Attitude/Courtesy EPSOM DAY UNIT WOMEN’S HEALTH
136597 13/10/2014 Feedback form
Very friendly. Waiting too long but very good service.
Attitude/Courtesy EPSOM DAY UNIT WOMEN’S HEALTH
7.1
58

File ID Submission Date
Method Comments Category Submitting Unit (physical location)
Directorate (geographical site)
136672 17/10/2014 Feedback form
Nurse was a genuine comfort and clear light in supporting me through the immense and obviously traumatic experience. She was clear and informing, soft and understanding and had time to listen to me and formulate considered empathetic responses. Another nurse was similar to first nurse and she was incredible the nursing staffs finesse at managing and treating patients.
Care/Treatment EPSOM DAY UNIT WOMEN’S HEALTH
136872 22/10/2014 Feedback form
Social worker was fantastic, really took time to listen to me and my situation. Everyone from the staff made me feel welcome and were very kind explaining everything as we went through process
Attitude/Courtesy EPSOM DAY UNIT WOMEN’S HEALTH
136874 22/10/2014 Feedback form
Very good experience - ensures privacy and always made sure my concerns were addressed. Nurses and doctors are very patient, made me feel comfortable and helped me to make informed decisions. I want to say "thank you" to all nurses and doctors, the procedure is not as scary as I thought, really appreciate the support. Thank you all once again.
Care/Treatment EPSOM DAY UNIT WOMEN’S HEALTH
136875 22/10/2014 Feedback form
Nurses are very lovely I felt like crying and they made me feel so much better. Thank you.
Attitude/Courtesy EPSOM DAY UNIT WOMEN’S HEALTH
136876 22/10/2014 Feedback form
Efficient and friendly staff. Straight forward and helpful staff. Thank you.
Attitude/Courtesy EPSOM DAY UNIT WOMEN’S HEALTH
136877 22/10/2014 Feedback form
You guys are all awesome, friendly and caring. Thank you for looking after me. Great nurses and doctors.
Attitude/Courtesy EPSOM DAY UNIT WOMEN’S HEALTH
136878 17/10/2014 Letter Patient happy with the facilities, treatment and care.
Environment Care/Treatment
WARD 63 ADULT MEDICAL SERVICES
136879 22/10/2014 Feedback form
Everything was like clockwork. Very professional approach from the
Care/Treatment EPSOM DAY UNIT WOMEN’S HEALTH
59

File ID Submission Date
Method Comments Category Submitting Unit (physical location)
Directorate (geographical site)
nurses, showing a lot of caring and looking after patient, as well as following up on discomforts. Thank you.
136887 20/10/2014 E-mail Patient found staff of ED were friendly, professional and grateful for care
Attitude/Courtesy EMERGENCY DEPARTMENT - ADULT ( AED)
ADULT MEDICAL SERVICES
136889 21/10/2014 Feedback form
Family impressed with the facilities, friendliness and efficiency of staff
Attitude/Courtesy EMERGENCY DEPARTMENT - CHILDRENS (CED)
CHILD HEALTH
136892 17/10/2014 Letter Family in appreciation of the transplant and the care for the patient.
Care/Treatment WARD 27A/B - BMT CHILD HEALTH
136935 17/10/2014 Feedback form
Family acknowledges the staff for being caring it made a huge difference.
Attitude/Courtesy WARD 27A/B CHILD HEALTH
136939 17/10/2014 Feedback form
Mum is satisfied by the level of care, treatment and support given to her daughter.
Attitude/Courtesy WARD 27A/B CHILD HEALTH
136940 17/10/2014 Feedback form
Family thanks all the staff for care, treatment and support given to the patient.
Attitude/Courtesy WARD 27A/B CHILD HEALTH
136946 21/10/2014 Feedback form
Parents acknowledged the staff for being wonderful, caring and kind to the child and family.
Attitude/Courtesy EMERGENCY DEPARTMENT - CHILDRENS (CED)
CHILD HEALTH
136948 16/10/2014 Letter Patient compliments the doctor for being sensitive and providing practical, informative care and treatment.
Care/Treatment OPHTHALMOLOGY CLINIC
ADULT SURGICAL SERVICES
136950 17/10/2014 Letter Parents are thankful to the doctors for their professionalism, and the staff of Ward 72 for the care, expertise and treatment.
Care/Treatment <Not Specified> ADULT MEDICAL SERVICES
136998 24/10/2014 Letter Patient very thankful and grateful to the doctor, for his surgery, care and treatment.
Care/Treatment WARD 71 ADULT SURGICAL SERVICES
136997 20/10/2014 Letter Patient was very satisfied with the professionalism and compassion of the staff. Particularly impressed with a doctor for his first class medical care.
Care/Treatment EMERGENCY DEPARTMENT - ADULT ( AED)
ADULT MEDICAL SERVICES
7.1
60

File ID Submission Date
Method Comments Category Submitting Unit (physical location)
Directorate (geographical site)
137153 24/10/2014 Letter Patient is thankful to all the staff for the excellent care, treatment and support provided. Real Heroes.
Attitude/Courtesy MOTUTAPU WARD CANCER AND BLOOD
137154 24/10/2014 Letter Patient is thankful for the kind, sensitive and compassionate treatment received.
Care/Treatment COLPOSCOPY OUTPATIENTS
WOMENS HEALTH
137156 24/10/2014 Feedback form
Mum was thoroughly satisfied with the high level of care, treatment given to her son. Made the right decision to bring the baby in the hospital.
Care/Treatment WARD 25A/B CHILD HEALTH
137159 28/10/2014 Feedback form
Family was thankful to all the staff involved in the care and treatment of their child.
Care/Treatment WARD 24B CHILD HEALTH
137166 28/10/2014 Feedback form
Family is thankful to the staff for providing wonderful care, treatment and support to the patient, in his final days. "A sad and very painful situation was made much more bearable".
Care/Treatment WARD 76 ADULT SURGICAL SERVICES
137205 29/10/2014 Feedback form
Parents/Guardians were relaxed and happy to be in the ward. "Will always recommend ACH as a safe place with lovely staff".
Attitude/Courtesy WARD 23B CHILD HEALTH
137207 29/10/2014 Feedback form
Parents were satisfied for the exceptional care, treatment and support given to their son.
Care/Treatment WARD 23B CHILD HEALTH
61

7.1
62


Respect & Dignity As a health organisation we are bound by the Code of Health and Disability Services Consumers' Rights’ (the Code). Much of the Code deals with respect in some way but Rights 1,2 and 3 are the most specific. The Code states that patients have a right:
1. to be treated with respect 2. to freedom from discrimination, coercion, harassment, and
exploitation 3. to dignity and independence
From our survey we know that respect means different things to different people. For some it is about staff having good manners, for others it is about being caring, compassionate, listening to their point of view, sharing information and treating them as individuals. This report gives us a clearer idea of what respect looks like and further that in not treating people respectfully we leave them feeling disempowered and vulnerable.
A key point is that every interaction counts. In the eyes of our patients and families we are all caregivers and we should behave as such. From the person on the end of the phone in the contact centre, to the carpark attendant, the reception staff, and the rest of our clinical and non-clinical teams. Everyone who wears a badge makes a difference.
And it’s largely good news. Eighty-three percent of patients say that their views were always taken into account or respected, and 93% said that staff respected their values, cultural or religious views and needs. These are great results. The flipside is that for 1 in 6 patients, they feel we can do better in terms of taking their views into account and respecting them. This is one domain of care that really matters to people. If the food is not up to standard, or information isn’t provided well then those are issues, but if people feel disrespected then that destroys the therapeutic relationship and has a very real impact on their wellbeing and ultimately the outcome of the care we provide.
Some of areas patients are asking us to focus on are:
Be courteous and good mannered
Be kind, compassionate and friendly – they are not a body part or condition but an individual with a history, family and community, and would like to be treated as such.
Listen to them and respect their point of view. It is their health and they want to make decisions about their care and treatment. To do this they need to be treated respectfully, be given full information and be allowed time to consider options.
Dr Andrew Old Chief of Strategy, Participation & Improvement
Outpatients believe these things make the most difference to the quality of their care and treatment:
1 Getting good information about their condition and treatment
66%
2 Good organisation, including appointments and correspondence
55%
3 Feeling confident in the quality of their care and treatment
52%
(n= 1521)
TOP THREE
PATIENT VOICES
ADHB Outpatient Experience Report no. 6 September 2014:1
Rated overall care excellent “It was the first visit in a long time that I really felt like my concerns were being listened to. Even if (the doctor) might not have agreed with everything, he didn't show it and was completely respectful. Thank you.”
Rated overall care very good “My questions were respected and answered.”
Rated overall care good “Very understanding, respectful and did not treat me like a number and like I didn't know anything about my own condition.”
Rated overall care fair “Even if it is the 100th person that they have greeted they should be welcomed as if they were the first and only one for the day.”
“In the treatment of children, especially children with life-threatening conditions, some of the nursing staff would be better placed if they could remember that it is important for the parents and the children that they are not simply "doing a job" but that there is a level of empathy and respect/caring that goes beyond running through the motions.”
Rated overall care poor “(An improvement would be) the doctor respecting and listening to the patient.”
7.2
63

Respect (Eleven point scale where 0 =poor and 10=excellent)
Rated highly (8-10) “These people really made you feel cared for, you were a person, not a statistic. There was no sense of being rushed through the system, so as to speak. I was treated with the highest dignity and respect, and always will carry memories of this.”
“Staff were considerate, listened attentively and were well mannered.”
Although I am old (over 80) I was not treated as if I would not understand the information I was being given.”
Rated well (5-7): “I felt that the doctor was distracted by something else. Some of what myself and my mother said, had to be repeated. This left us feeling bewildered. I felt that I wasn't quite sure that the doctor knew why we were there.”
“The nurse who took my weight/height/BP/SpO2 before the procedure was really perfunctory and didn't communicate. I felt like meat being examined in a laboratory.”
Rated as poor (0-4): “The nurse from the second waiting area was cold. She only answered my question with three cold words. Very brief , no greeting, no further explanation. I did not feel being respected at that moment. It made me think why I was not respected. Was is because my look? My race of being Chinese? I don't know.”
“Not being heard or taken seriously. Being belittled & compared to other patients who are more serious than me. Being talked over top of. Being rushed in my appointment because other patients were waiting and the doctor was running behind by an hour- not my problem.”
Respect This month we are focusing being treated with respect. One in five (20%) outpatients identified this as an aspect of our service that makes the most difference to their care and treatment.
These results are based on responses from over 3,300 outpatients who attended clinics between 1st October 2013 (the survey launch) and 31st August 2014.
Overall care and treatment The ADHB target is to have 90 per cent of patients rating their overall care and treatment as very good or excellent.
In the period up until August 2014, 86 per cent of outpatients rated their care as very good (33%) or excellent (53%).
The numbers in some of the Directorates are low, as the survey is being phased in. Surgical services in all directorates and Cancer & Blood patients were surveyed from January 1, 2014.
Overall care and treatment ratings by Health Service Group (%) n=3001
Overall n= 3390 (Women’s Health n=430, Children’s Health n=505, Cardiac services n=110, Cancer and Blood n=657, Adult Surgical n =1688
Overall
In August 87 per cent of patients rated their care as very good or excellent. This is an increase from ratings in February and March. Since October 2013 the very good and excellent ratings of overall care and treatment have ranged between 83 per cent and 93 per cent.
Note that the survey was not sent out over the Christmas period, and recommenced in January to a wider group of services. Consequently, the 2013 results are not directly comparable to the 2014 results.
Overall care and treatment ratings (outpatients) (%)
Overall n=3390
2
0
1
2
3
2
3
1
4
4
7
3
9
5
10
11
9
9
35
28
33
36
31
33
50
65
53
48
51
53
Surgical
Cancer & Blood
Cardiac
Children's Health
Women's Health
Overall
Poor Fair Good Very good Excellent
85
93
88
84 83
85
87 86
88 87
75
80
85
90
95
Oct '13 Nov '13 Jan '14 Feb '14 Mar '14 Apr '14 May '14 Jun'14 Jul' 14 Aug-14
PATIENT VOICES
ADHB Outpatient Experience Report no. 6 September 2014:2 64

Focus area Outpatients who selected being treated respect as an area that made a difference to their care, were asked to rate how well ADHB outpatient clinics performed on this dimension.
Overall, on an 11-point scale, where 0 is poor and 10 is excellent, most patients rated ADHB highly. The majority (80 per cent) rated respect highly (8-10.) Seven percent however rated it as poor (0-4).
Rating (%) n=798
Patient voices
“The doctor listened to my concerns and explained everything very clearly. I was treated with respect.”
“The staff greet each patient warmly every day, remember details of what they have done in their private lives on previous days and chat like old friends. They show respect for what the patient is going through and treat it with empathy as well as a professional respect.”
“The receptionist was very rude, we waited until she had finished her chit chat conversation with the other receptionist before saying 'next' and pointing at me to come forward. She did not say hello, she just said 'name' than she said 'you’re late' I attempted to offer an explanation but she did not appear to care.”
1 1 2 2 4 3 6
16
23
41
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%10excellent
9
8
7
6
5
4
3
2
1
0 poor
Respect Patients were asked about dignity and respect, in particular if their views were taken into account and respected, if they were given sufficient privacy at reception, during consultations and examinations, if their values were respected and if various members of staff treated them with dignity and respect.
How are we doing?
Between October 2013 (the start of the survey) and August 2014, 83% of patients said that their views were always taken into account or respected. However, one in six patients said this was not the case.
Views taken into account and respected (%) by directorate n=3409
Most (93%) said that staff respected their values, beliefs, cultural or religious views and needs. Seven percent said that this had not happened or had only happened in part.
Values, beliefs, cultural or religious needs respected (%) by directorate n=2051
Patients were asked whether they were given enough privacy at reception, during consultations and when examined or treated. Most felt that they had sufficient privacy. Those at reception were least likely to feel this way.
Privacy (%) n=3375
Although most patients said that staff treated them with dignity and respect, around one in ten patients indicated that this was not always the case.
Respect from staff (%) n=2740
3
3
2
2
1
3
14
13
16
13
11
15
83
83
82
85
88
81
Overall
Women's Health
Children's
Cardiac
Cancer & Blood
Adult surgical
No Sometimes Always
1
1
1
2
0
2
6
5
6
3
5
6
93
94
92
95
95
92
Overall
Women's Health
Children's
Cardiac
Cancer & Blood
Adult surgical
No In part Yes
3
1
1
13
5
8
83
94
91
Reception
Consultation
Examinations
No In part Yes
2
1
1
2
7
9
9
12
92
91
91
86
Doctors
Nurses/midwives
Allied staff
Reception
No In part Yes
PATIENT VOICES
ADHB Outpatient Experience Report no. 6 September 2014:3
7.2
65

response to patient feedback. We would like to share these stories Respect
Being treated with respect includes being treated with good manners, friendliness, compassion, and it means listening to patients, and respecting their views and decisions. Patients are asking us to:
Be courteous and good mannered
Be kind, compassionate and friendly – they are not a body part or condition but an individual with a history, family and community, and would like to be treated as such.
Listen to them and respect their point of view. It is their health and they want to make decisions about their care and treatment. To do this they need to be treated respectfully, be given full information and be allowed time to consider options.
Patient comments “I have been treated as a human being, with respect and admiration for what I am going through. The nurses are polite and efficient, which is great … I have felt very special when coming in, plus out of everyone in my life at this moment in time -they know what I am going through and how little things are really important.”
“All staff were polite and respectful, … all have taken the time to assist me as needed.”
“Being kept waiting at a nurses station for attention while they chat on the phone and eat their morning tea are frustrating - you're left feeling like you don't matter as much as their personal phone call.”
“Please close curtain completely when in a room examining an undressed patient. I can’t relax knowing someone could barge in. This should be standard practice.”
“Not listening to either my daughter or myself in what she wanted & taking in to account all her medical issues.”
“I had to have many different people look at me. I understand that it was needed for training purposes but still didn't like it very much.”
ACTIONS
ADHB Outpatient Experience Report no. 6 September 2014:4 :442014:4
A closer look at respect A total of 517 patients commented on respect. Patients have different views on the aspects of care that comprise respectful treatment. For some it is about having good manners, for others it is about being caring, compassionate, listening to their point of view, sharing information and treating them as individuals.
Three-quarters (78%) commented positively. One-quarter (24%) however, described poor experiences and gave suggestions of how we can improve this aspect of our care and treatment.
Positive comments (78%) Generally respectful (18%) Many patients observed that they appreciated staff treating them respectfully.
Well mannered (11%) One in ten patients (11%) described how they were treated respectfully by staff who introduced themselves, made eye contact and were generally polite and courteous.
Caring (9%) For some patients, respectful treatment meant treating them with gentleness, kindness, understanding and being sensitive to their situation and needs.
Friendly (7%) Some appreciated that staff were warm and friendly towards them.
Respect their point of view (7%) Some patients appreciated staff listening to them and respecting their point of view. Other comments relating to respectful treatment included:
Staff keeping them well informed and sharing information about treatments and test results, but also about waiting times etc. (6%);
Staff making them feel like individuals rather than numbers (6%);
Staff being helpful and proactive (5%);
Staff making them feel comfortable and at ease, particularly during procedures which they found potentially embarrassing ( 5%);
Staff taking time with patients (4%);
Staff answering questions, and reassuring them about worries and concerns (3%)
Patients cultural and religious beliefs being respected;
Patients given privacy both at reception and during examinations (2%);
Staff being aware of a patient’s history, reading their records and remembering them from previous appointments and showing an interest.
Improvements (24%) Reception (4%) Patients asked that receptionists consider their privacy and treat them respectfully. Some felt that receptionists spoke loudly about matters they considered private, were impolite or overly abrupt. Rushed (2%) Some patients felt that the consultations were rushed and that staff were more interested in getting them out the door than treating them. Listen (2%) Some patients felt that their concerns, opinions and views were ignored and asked that staff listen to them and respect their perspectives and points of view. Quiet voice (2%) Patients asked that staff use a quiet voice when giving them private and sensitive information in front of others. Wait times (2%) Patients asked to be kept up to date about wait times and to be treated respectfully when they asked about delays or wait times. Other comments relating to a perceived lack of respectful treatment included:
Patients feeling ‘prejudged’ on the basis of age or ethnicity and being spoken down to on that basis (1%);
A lack of private consultation areas, resulting in others overhearing private consultations (1%);
Decisions and actions being proposed or undertaken prior to either a consultation or agreement (1%);
Religious or cultural beliefs not being respected (1%);
Staff ignoring patients as they focus on non-work related activities (1%);
Students or other doctors being invited into a consultation before patients are asked for their consent (1%);
Being examined uncovered, or curtains being open during examinations resulting in a loss of dignity (1%);
66

Report on
R e p or t
O ct ob e r 2 0 1 4
33 Auckland District Health Board
Patient Experience
Pain and nausea All of us have experienced pain and nausea at some time in our lives and know how debilitating they can be. Both are very common symptoms and are often, pain in particular, a key reason our patients end up in hospital. Sometimes they can be overwhelming and for patients who are in pain, or are nauseous, then good management of their symptoms is an important part of their care.
Unsurprisingly, our approach to managing our patients’ pain and nausea has a significant impact on the way patients view their care and treatment, and on our overall ratings.
It is important to note that little has changed since the pain management report two years ago. Both our ratings and comments remain similar. The good news is that most people report we control their pain and nausea very well (74% and 70% respectively). However that leaves a significant minority for whom we can improve. What is really key from the comments is that it is less about how well their pain and nausea is controlled as it is about our staff showing kindness and compassion and doing everything they can to help control it.
There are three areas that patients have particularly highlighted:
1. Many patients are feeling undertreated, particularly on admission and discharge
On admission some patients have commented feeling overwhelmed by pain and not being attended to promptly. However, the main concern appears to be on discharge. Patients say they are being discharged without medication or prescriptions, and because there can be delays of several days before they can get a GP appointment, they are being left with inadequate relief. On wards some patients describe delays in being given relief, meaning that they experience unnecessary pain and nausea.
2. Lack of control
Patients want to be given information, options and choices. Some feel very unprepared for the level of pain they experience following a procedure and are having to take in information when they are overwhelmed with pain or nausea.
3. Compassion and care
As noted, the comments suggest it is less about controlling the pain and nausea, than staff showing kindness and compassion, and doing everything they can to help control the pain and nausea. They want us to listen to them when they are in pain, be proactive in giving information and relief, and help them when they need cleaning up if they or their loved ones have vomited.
This feedback from patients is entirely consistent with what we heard from both patients and staff during our Values Week at the end of July. Experience is less about the actual outcome than it is about the interpersonal relationship. The great news for us as an organisation is that this doesn’t mean we need a new blockbuster drug for pain or nausea. If we all pause to put ourselves in the shoes of our patients and families, and treat them as such, then together we’ll make a big difference.
Dr Andrew Old Chief of Strategy, Participation & Improvement
MATTERS MOST TO PATIENTS The survey asks patients what makes the most difference to their care and treatment.
Patients believe these things make the most difference to the quality of their care and treatment:
1 Communication (clear answers patients can understand)
50%
2 Feeling confident about the quality of their care and treatment
45%
3 Getting coordinated care in hospital 41%
ADHB’S PERFORMANCE The percentage of patients that rate ADHB care positively (as very good or excellent) on these dimensions of care are:
Communication 71%
Feeling confident 83%
Coordinated care 70%
Patient feedback: rated excellent “I was looked after very well during my hospital stay by all staff concerned. They were kind and understanding at all times and did everything within their capabilities to make me feel comfortable and to mitigate post-surgery pain.”
Patient feedback: rated very good “Nurses were of the highest standard and the backbone of the care given to me. Very caring, supportive and had empathy - most of all - they did not let you suffer with pain/nausea.”
Patient feedback: rated fair “No nursing staff came to me for long time. I cannot remember how long. The calling bell was not in reach. No relatives were with me. Felt nauseated. I was in helpless situation. Then one of my friend came to see me and helped me.”
Patient feedback: rated poor ‘The doctor on Saturday wrote my med cert and discharge but not my pain relief I had to wait 2 days for a doctor to write a script for my pain relief which is ridiculous.”
ADHB Patient Experience Report no.33 October 2014: 1
7.2
67

Most difference to care
Overall ratings Patients who selected pain and nausea as dimensions of care most important to them were then asked to rate ADHB’s performance on these dimensions.
Pain Overall, on an 11-point scale, where 0 is poor and 10 as excellent, 6 per cent rated their experience as poor. Most (72%) rated their care as very good or excellent.
Rating by Directorate % (n=692)
Poor
(0-4)
Moderate
(5-7)
Very Good
(8-10)
Overall 6 22 72
Women 4 21 75
Children 7 20 73
Cardiac 2 23 74
Cancer /Blood*
7 43 50
Surgical 6 23 71
Adult comm/ long term*
- - -
Adult medical
12 25 64
*The numbers were too small to analyse with confidence.
Nausea Most rated our care in respect to nausea control highly (70%). Nonetheless many (30%) felt that this was not always the case.
Rating % (n=127)
Poor
(0-4)
Moderate
(5-7)
Very Good
(8-10)
Overall 8 22 70
The numbers were too small to disaggregate further with confidence.
Why this matters Half (51%) of patients who felt that staff had done all they could to control their pain rated their overall care and treatment as excellent compared with only 6 per cent of those that said this was not the case. Similarly, only 3 per cent of patients who felt that staff had done all they could to control their pain rated our performance as fair or poor compared with 44 per cent of patients who felt staff had not.
The findings were similar in relation to staff assisting with nausea control.
ADHB Patient Experience Report no.33 October 2014: 2
How are we doing? This month the report is focusing on two areas of patient experience - pain and nausea control.
Pain and nausea control are important to our patients, with 18 per cent and 3 per cent respectively considering them be areas that makes the most difference their care and treatment. However, if looking at only those who experience pain, this rises to nearly one-quarter (23%) of patients. Similarly, when looking only at those who experience nausea, this rises to 7 per cent of patients.
For those experiencing pain and nausea, our care matters and makes a difference. And our overall ratings appear to be influenced by whether patients see us as doing all that we can to help control their pain and nausea.
Overall experience in the past 12 months (%) Each month patients are asked to rate their overall care and treatment. In the year to August 30
th 2014, 85 per cent of patients rated their care and treatment as
very good or excellent.
Overall ratings of care and treatment by Health Directorate (%) n=4072
*The differences between Directorates are significant p<.05
Overall experience month by month (%) ADHB’s target is for 90 per cent of patients to rate the overall care and treatment we have provided as very good or excellent. The percentage of patients that rated their overall care and treatment as very good or excellent fell in the month of August. The difference is significant. The fall has resulted from a decrease in positive ratings in all but Women’s Health Services.
Percentage of patients that rated their care as very good or excellent (each month) n=4127
2
0
2
1
1
2
1
1
6
4
3
3
1
4
5
4
13
7
10
11
4
13
9
10
39
43
39
35
32
41
38
39
40
45
47
50
61
40
46
46
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Adult medical
Adult comm/long term
Surgical
Cancer & Blood
Cardiac
Children's Health
Women's Health
Overall
Poor Fair Good Very good Excellent
84
83 82
88
85
88
84 84 84
86
83
85
80
75
77
79
81
83
85
87
89
Very good/excellent
68

*
Patient voices
Pain and Nausea (Eleven point scale where 0 =poor and 10=excellent)
Rated ADHB highly (8-10) “From recovery right through to the time the pain went away, I was constantly checked and monitored. I was advised at every level where my blood pressure sat and offered pain relief. The nurses told me how much I was taking, how long it would take to work and kept me informed. As soon as the pain left and I stopped the pain relief, the nurses didn't question my decision and I felt in control.”
“Very kind in helping clean up when vomited and provided anti-nausea medication.”
“They had to give me three different anti-nausea medications but they did not give up until I stopped throwing up.”
Rated ADHB well (5-7) “I was unsure why a certain pain regiment was withheld. I didn't find out until the end of my stay of the reason. I was also not aware I could inform them when the medication was insufficient.”
“Very slow responses from all medical staff on requests for anti-nausea medication for my very unwell child. Good response from theatre staff though who administered some medication post-operatively.”
Rated ADHB as poor (0-4) “I was in a lot of pain but the doctors and nurses seemed to treat me like I was over- exaggerating, well that's how I felt - however I felt like they didn't understand or want to understand what I was going through and that they down-played my symptoms although they were very stressful to me they weren't important to them.”
“I felt nauseous and rang for assistance. I had to request a vomit cup. When this was full and I had to ask for another one and it took a long time for full cups to be removed. I was given one tablet to help with the nausea so pharmacologically I was managed adequately but comfort wise I was not.”
Pain and Nausea Patients were asked if they were ever in any pain or nausea. Just under half (47%) said that they had experienced pain and around 21 per cent had experienced nausea. They were then asked if they felt that staff had done everything they could to help control the pain or nausea. Those who had experienced pain or nausea were asked about their experiences.
Pain Between September 2013 and August 2014, most (74%) felt that staff had done all they could to help control their pain. Four per cent felt that this was not the case. This is largely unchanged from ratings two years ago.
Did the hospital staff do everything they could to help control your pain (%) n= 2576
Over the past two years the percentage of patients who say that staff did everything they could to control their pain has ranged between 71 per cent and 78 per cent of patients.
Staff had definitely done everything to control their pain, by quarter (%) n= 5085
Nausea Similarly, between September 2013 and August 2014 most patients (74%) reported that staff did everything they could to help control their nausea they were feeling.
Did the hospital staff do everything they could to help control your nausea (%) n= 1543
(Adult community & long term patients – the numbers are too small to report)
Over the past two years the percentage of patients who say that staff did everything they could to control their pain has ranged between 70 per cent and 77 per cent of patients.
Staff had definitely done everything to control their nausea, by quarter (%) n= 3040
4 8
3 4 3 3 3 5
22 29
16 20 25
13 26
20
74 62
81 76
72 84
71 75
OverallAdult medical
Adult comm/long…Surgical
Cancer and BloodCardiac
Children'sWomen's
No
To someextent
Definitely
73 73 73
71
73 73
71
78
70
75
80
4 7
4 0 2 4 5
21 29
18 20
14 26
19
74 64
78 80
84 69
76
OverallAdult medical
Adult comm/long…Surgical
Cancer and BloodCardiac
Children'sWomen's
No
To someextent
Definitely
77
70
74
71
77 74
73 73
65
70
75
80
ADHB Patient Experience Report no.33 October 2014: 3
7.2
69
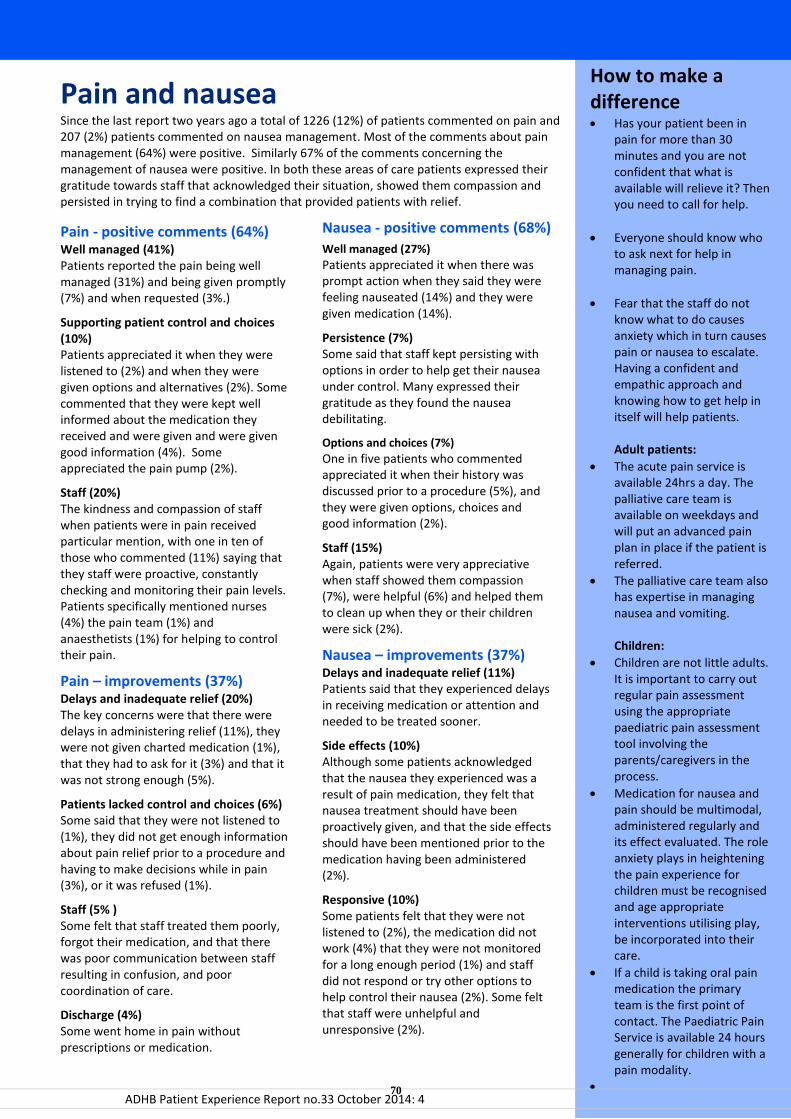
How to make a difference Has your patient been in
pain for more than 30 minutes and you are not confident that what is available will relieve it? Then you need to call for help.
Everyone should know who to ask next for help in managing pain.
Fear that the staff do not know what to do causes anxiety which in turn causes pain or nausea to escalate. Having a confident and empathic approach and knowing how to get help in itself will help patients. Adult patients:
The acute pain service is available 24hrs a day. The palliative care team is available on weekdays and will put an advanced pain plan in place if the patient is referred.
The palliative care team also has expertise in managing nausea and vomiting. Children:
Children are not little adults. It is important to carry out regular pain assessment using the appropriate paediatric pain assessment tool involving the parents/caregivers in the process.
Medication for nausea and pain should be multimodal, administered regularly and its effect evaluated. The role anxiety plays in heightening the pain experience for children must be recognised and age appropriate interventions utilising play, be incorporated into their care.
If a child is taking oral pain medication the primary team is the first point of contact. The Paediatric Pain Service is available 24 hours generally for children with a pain modality.
Pain and nausea Since the last report two years ago a total of 1226 (12%) of patients commented on pain and 207 (2%) patients commented on nausea management. Most of the comments about pain management (64%) were positive. Similarly 67% of the comments concerning the management of nausea were positive. In both these areas of care patients expressed their gratitude towards staff that acknowledged their situation, showed them compassion and persisted in trying to find a combination that provided patients with relief.
Pain - positive comments (64%)
Well managed (41%) Patients reported the pain being well managed (31%) and being given promptly (7%) and when requested (3%.)
Supporting patient control and choices (10%) Patients appreciated it when they were listened to (2%) and when they were given options and alternatives (2%). Some commented that they were kept well informed about the medication they received and were given and were given good information (4%). Some appreciated the pain pump (2%).
Staff (20%) The kindness and compassion of staff when patients were in pain received particular mention, with one in ten of those who commented (11%) saying that they staff were proactive, constantly checking and monitoring their pain levels. Patients specifically mentioned nurses (4%) the pain team (1%) and anaesthetists (1%) for helping to control their pain.
Pain – improvements (37%)
Delays and inadequate relief (20%) The key concerns were that there were delays in administering relief (11%), they were not given charted medication (1%), that they had to ask for it (3%) and that it was not strong enough (5%).
Patients lacked control and choices (6%) Some said that they were not listened to (1%), they did not get enough information about pain relief prior to a procedure and having to make decisions while in pain (3%), or it was refused (1%).
Staff (5% ) Some felt that staff treated them poorly, forgot their medication, and that there was poor communication between staff resulting in confusion, and poor coordination of care.
Discharge (4%) Some went home in pain without prescriptions or medication.
Nausea - positive comments (68%)
Well managed (27%)
Patients appreciated it when there was prompt action when they said they were feeling nauseated (14%) and they were given medication (14%).
Persistence (7%) Some said that staff kept persisting with options in order to help get their nausea under control. Many expressed their gratitude as they found the nausea debilitating.
Options and choices (7%)
One in five patients who commented appreciated it when their history was discussed prior to a procedure (5%), and they were given options, choices and good information (2%).
Staff (15%) Again, patients were very appreciative when staff showed them compassion (7%), were helpful (6%) and helped them to clean up when they or their children were sick (2%).
Nausea – improvements (37%)
Delays and inadequate relief (11%) Patients said that they experienced delays in receiving medication or attention and needed to be treated sooner.
Side effects (10%) Although some patients acknowledged that the nausea they experienced was a result of pain medication, they felt that nausea treatment should have been proactively given, and that the side effects should have been mentioned prior to the medication having been administered (2%).
Responsive (10%) Some patients felt that they were not listened to (2%), the medication did not work (4%) that they were not monitored for a long enough period (1%) and staff did not respond or try other options to help control their nausea (2%). Some felt that staff were unhelpful and unresponsive (2%).
ADHB Patient Experience Report no.33 October 2014: 4
ADHB Patient Experience Report no.11 October 2012: 3
70

Mental Health Directorate
Speaker: Clive Bensemann, Director
Service Overview This Directorate provides specialist community and inpatient mental health services to Auckland residents. Our team provide a range of services at various levels: sub-regional (adult inpatient rehabilitation & community psychotherapy), regional (youth forensics) and supra-regional (child and youth acute inpatient & eating disorders). The Mental Health Directorate is led by Director: Dr Clive Bensemann, with General Manager: Maria West, Director of Nursing: Anna Schofield and Director of Allied Health: Mike Butcher.
Scorecard
Mental HealthOct-14 Measure Target
Medication Errors 14 0 13
Number of reported adverse events causing harm (SAC 1&2) 0 TBC 1
Seclusion. All inpatient services - episodes of seclusion 0 <=7 0
Restraint. All services - incidents of restraint 76 <=86 58
7 day Follow Up post discharge 95.0% ≥95% 100.0%
Mental Health - 28 Day Readmission Rate (KPI Discharges) to Te Whetu Tawera N/A ≤10% 14.8%
Mental Health Average LOS (KPI Discharges) - Te Whetu Tawera 32.3 <=21 22.3
Mental Health Average LOS (All Discharges) - Child & Family Unit 8.9 <=15 8.9
Mental Health Average LOS (All Discharges) - Fraser McDonald Unit 36.8 <=35 48.9
Waiting Times. Provider arm only: 0-19Y - 3W Target 83.1% ≥80% 83.3%
Waiting Times. Provider arm only: 0-19Y - 8W Target 98.2% ≥95% 98.2%
Waiting Times. Provider arm only: 20-64Y - 3W Target 89.1% ≥80% 88.8%
Waiting Times. Provider arm only: 20-64Y - 8W Target 96.1% ≥95% 96.0%
Waiting Times. Provider arm only: 65Y+ - 3W Target 89.9% ≥80% 89.5%
Waiting Times. Provider arm only: 65Y+ - 8W Target 97.5% ≥95% 97.4%
% Hospitalised smokers offered advice and support to quit 96.4% ≥95% 96.8%
% long-term clients with relapse prevention plans in last 12 months (6 monthly) * 94.6% ≥95% 97.4%
Mental Health access rate - Maori 0-19Y 5.23% ≥5.5% 5.34%
Mental Health access rate - Maori 20-64Y 11.80% ≥12% 11.90%
Mental Health access rate - Maori 65Y+ 4.18% ≥4% 4.18%
Mental Health access rate - Total 0-19Y 2.95% ≥3% 2.99%
Mental Health access rate - Total 20-64Y 3.93% ≥4% 3.94%
Mental Health access rate - Total 65Y+ 3.65% ≥4% 3.71%
Impr
oved
Hea
lth S
tatu
s
Actual Prev Period
Incr
ease
d Pa
tient
Sa
fety
Bett
er Q
ualit
y Ca
re
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.1
71
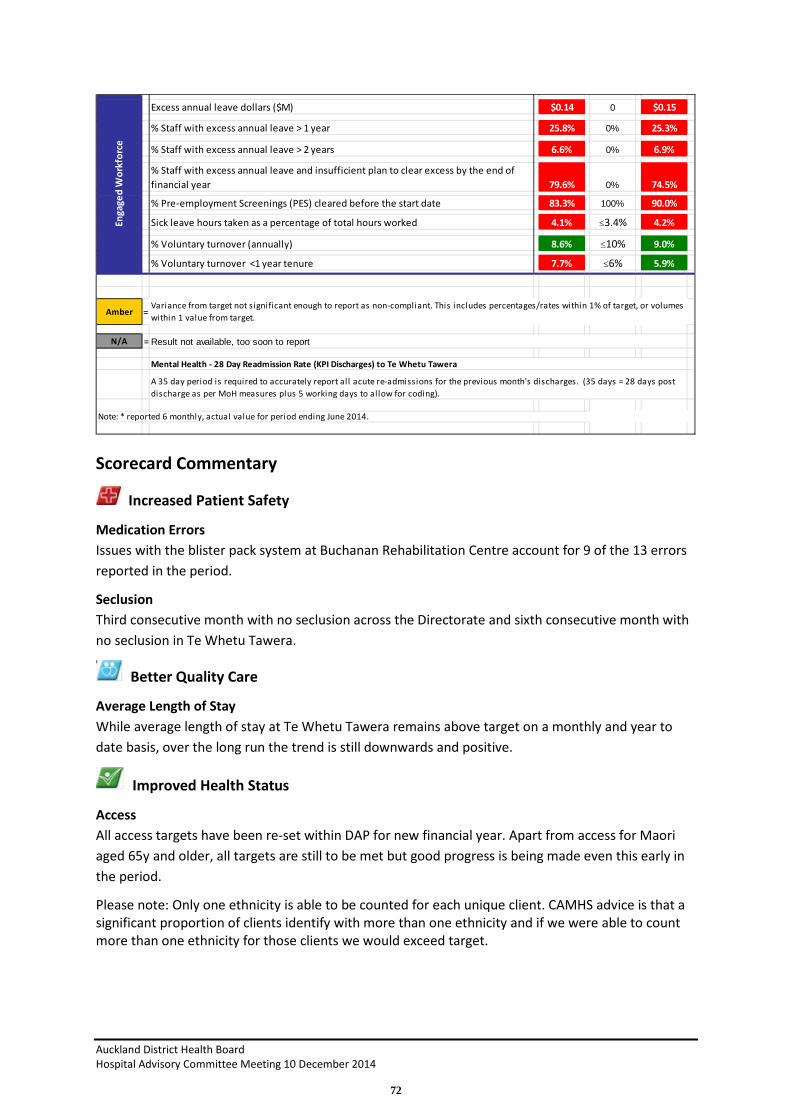
Scorecard Commentary
Increased Patient Safety
Medication Errors Issues with the blister pack system at Buchanan Rehabilitation Centre account for 9 of the 13 errors reported in the period.
Seclusion Third consecutive month with no seclusion across the Directorate and sixth consecutive month with no seclusion in Te Whetu Tawera.
Better Quality Care
Average Length of Stay While average length of stay at Te Whetu Tawera remains above target on a monthly and year to date basis, over the long run the trend is still downwards and positive.
Improved Health Status
Access All access targets have been re-set within DAP for new financial year. Apart from access for Maori aged 65y and older, all targets are still to be met but good progress is being made even this early in the period.
Please note: Only one ethnicity is able to be counted for each unique client. CAMHS advice is that a significant proportion of clients identify with more than one ethnicity and if we were able to count more than one ethnicity for those clients we would exceed target.
Excess annual leave dollars ($M) $0.14 0 $0.15
% Staff with excess annual leave > 1 year 25.8% 0% 25.3%
% Staff with excess annual leave > 2 years 6.6% 0% 6.9%
% Staff with excess annual leave and insufficient plan to clear excess by the end of financial year 79.6% 0% 74.5%
% Pre-employment Screenings (PES) cleared before the start date 83.3% 100% 90.0%
Sick leave hours taken as a percentage of total hours worked 4.1% ≤3.4% 4.2%
% Voluntary turnover (annually) 8.6% ≤10% 9.0%
% Voluntary turnover <1 year tenure 7.7% ≤6% 5.9%
Amber =
N/A =
Note: * reported 6 monthly, actual value for period ending June 2014.
Variance from target not significant enough to report as non-compliant. This includes percentages/rates within 1% of target, or volumes within 1 value from target.
Result not available, too soon to report
Mental Health - 28 Day Readmission Rate (KPI Discharges) to Te Whetu Tawera
A 35 day period is required to accurately report all acute re-admissions for the previous month's discharges. (35 days = 28 days post discharge as per MoH measures plus 5 working days to allow for coding).
Enga
ged
Wor
kfor
ce
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
72

Engaged Workforce
Excess Annual Leave A further reduction of 0.3% of staff with excess annual leave has been achieved with associated annual leave dollars reduced by $10k.
Pre-employment Screening 26 staff entered employment with the Directorate in the reporting period; 6 commenced employment prior to screening. 2 of these staff were internal recruits and a third had only left the DHB a month prior to returning into a different role and exemption was given to ensure continuity of service delivery in priority areas. All incidents of staff commencing prior to screening are followed up by the Service Manager.
Voluntary turnover <1yr tenure This reflects 5 staff exiting in the period. These are staff from across different teams and services.
Strategic Initiatives
Deliverable / Action Status
Ensure that people are engaged at the right level of service at the right time (using resources effectively/links to stepped care)
In progress √ √ √
Monitor consult liaison activity from secondary care to primary care, schools and other public agencies
In progress √ √ √
Continue to implement the long term restraint/seclusion minimisation strategy
In progress √ √ √
Implement actions from the Child and Youth MH&A Direction with interagency partners
In progress √ √
Implement enhancements to Maternal Mental Health continuum In progress √ √ √
Improve social inclusion through increased access to employment In progress √ √
Regional MoC Eating Disorders In progress √ √
Contribute to development of Regional Youth Forensic pathway and MoC
In progress √ √
Contribution to development of Localities Tamaki Project In progress √ √ √
Key achievements in the month
The Regional Mother and Baby Unit opened on schedule and commenced receiving patients on the 28th October.
Areas off track and remedial plans
A multidisciplinary working group are developing a plan to resolve issues regarding the medication system at Buchan Rehabilitation Centre. A review of the changing profile of the client group and their needs is in progress.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.1
73

New Initiatives The Directorate has begun a review of facilities across all services and is in early stages of developing a master site plan. The plan will align facilities and environments with future service model development for in-patient and community services.
Recruitment has commenced for a dedicated specialist FTE to support the Tamaki Localities Project. This allocated resource will be involved in delivery to the ‘Enabling General Practice’ project stream.
Financial Results Consolidated statement of financial performance
Paid FTE
Comments on Major Financial Variances Month of October The result for the month is a surplus of $122k against a budgeted surplus of $33k, a favourable variance of $155k.
The main drivers of this month's favourable variance of $155k are
• Internal revenue $85k U - Primarily revenue for the funding of the Regional Youth Forensic service, Maternal Mental health FTEs and Perinatal and Infant Mental Health beds not yet eligible for full month invoicing.
• Medical including outsourced $125k F- Primarily 5.8 FTE vacancies.
• Nursing including outsourced $72 F- Primarily due to vacancies of 26 FTE
• Allied Health including outsourced $131 F- Primarily due to vacancies of 20.5 FTE.
• Management/Administration including outsourced $10k F- Primarily due to vacancies of 1.9 FTE.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
74

• Other. Clinical supplies $9k U, Infrastructure and non-clinical supplies $20F and Internal allocation $20k F. Patient welfare and incentives $11k F, Pharmaceuticals $8k U. Rents $11k F, Maintenance $16k F.
Year to date The result for year to date is a surplus of $946k against a budgeted deficit of $2k, a favourable variance of $948k.
The main drivers of this are:
• Internal revenue $384k U - primarily revenue for the funding of the Regional Youth Forensic service and Maternal Mental health FTEs and beds for the Infant and Perinatal Mental Health beds not eligible for full invoicing.
• Medical including outsourced $711k F- primarily 5.9 FTE vacancies.
• Nursing including outsourced $317k F- primarily due to vacancies of 21.6 FTE.
• Allied Health including outsourced $600k F- primarily due to vacancies of 18.6 FTE.
• Management/Administration including outsourced $27k F primarily due to vacancies of 0.6 FTE.
• Other. Clinical supplies $12k U, Infrastructure and non-clinical supplies $46k U and Internal allocation $100k F. Predominately Patient welfare and incentives $22k F, Pharmaceuticals $26k U. Rents $46k F, Maintenance $46k F, Vehicle Depreciation and Loss on sale $27k U.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.1
75


Women’s Health Directorate
Speaker: Sue Fleming, Director
Service Overview The Women’s Health portfolio includes all Maternity and Gynaecology services plus Fertility and Termination services. The team is contracted to provide primary, secondary and tertiary services. The Maternal Fetal Medicine group provide quaternary services and are contracted to lead the National Maternal Fetal Medicine network.
The Northern Hub of the National Genetic service is also under the umbrella of the Women’s Healthcare Service Group.
Scorecard
Women's HealthOct-14 Measure Target
Number of healthcare-associated bloodstream infections N/A TBC 1
Number of healthcare-associated Staphylococcus aureus bacteraemia N/A TBC 0
Medication Errors 5 0 5
Falls with major harm. Days since last event 1101 0 1070
Number of reported adverse events causing harm (SAC 1&2) 1 0 0
HT2 Elective discharges cumulative variance from target 1.01 >=1 0.98
(ESPI-1) % Services acknowledging 90% of FSA referrals 100.0% 100% 100.0%
(ESPI-2) Patients waiting longer than 5 months for their FSA 0.10% 0% 0.27%
(ESPI-5) Patients given a commitment to treatment but not treated within 5 months 0.00% 0% 0.00%
% DNA rate for outpatient appointments - All Ethnicities 9.0% ≤9% 8.0%
% DNA rate for outpatient appointments - Maori 19.2% ≤9% 14.4%
% DNA rate for outpatient appointments - Pacific 16.4% ≤9% 17.0%
Elective day of surgery admission (DOSA) rate 84.1% TBC 81.4%
% Day Surgery Rate 58.3% TBC 54.9%
Inhouse Elective WIES through theatre - per day 8.00 TBC 6.39
Birthcare primary births (YTD) 125 200 92
Number of CBU outliers 8 0 2
% Very good and excellent ratings for overall patient experience for inpatients N/A ≥90% 91.9%
% Very good and excellent ratings for overall patient experience for outpatients N/A ≥90% 77.4%
Number of complaints received 8 TBC 12
28 Day Readmission Rate - Total N/A TBC 4.1%
Average Length of Stay for WIES funded discharges (days) - Acute 1.93 TBC 1.95
Average Length of Stay for WIES funded discharges (days) - Elective 1.23 TBC 1.07
Actual Prev Period
Incr
ease
d Pa
tient
Sa
fety
Bett
er Q
ualit
y Ca
re
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.2
76

Scorecard Commentary
Improved Health Status
We met our targets for this month.
Increased Patient Safety
We have had 5 minor medication errors this month none of which resulted in patient harm. We had 1 SAC 2 event in October which has been fully investigated and has resulted in a change of practice.
Better Quality Care
We have met ESPI 1 and 5 targets. We had one outpatient go non-compliant for ESPI 2 due to unforeseen sick leave of one of medical staff.
Maori and Pacific DNA rates continue to be high despite our active engagement with both Maori and community providers. A significant contribution of these DNA’s comes from women who need care from our Maternity Diabetes service. A formal green belt project is exploring ways of making our diabetes outpatient programme more responsive to the needs of women.
% Hospitalised smokers offered advice and support to quit 96.4% ≥95% 97.0%
Breastfeeding rate on discharge excluding NICU admissions N/A ≥75% 78.4%
Cervical Screening Rate (Quarterly) * N/A TBC N/A
NCSP DNA rates 6.0% TBC 12.0%
Excess annual leave dollars ($M) $0.25 0 $0.23
% Staff with excess annual leave > 1 year 32.6% 0% 31.7%
% Staff with excess annual leave > 2 years 11.7% 0% 11.2%
% Staff with excess annual leave and insufficient plan to clear excess by the end of financial year 89.1% 0% 84.4%
% Pre-employment Screenings (PES) cleared before the start date 100.0% 100% 40.0%
Sick leave hours taken as a percentage of total hours worked 3.4% ≤3.4% 3.4%
% Voluntary turnover (annually) 11.6% ≤10% 12.2%
% Voluntary turnover <1 year tenure 6.7% ≤6% 4.2%
Amber =
N/A =
Enga
ged
Wor
kfor
ceIm
prov
ed H
ealth
St
atus
Note: * reported quarterly.
These measures are based on retrospective survey data, i .e. completed responses for patients discharged or treated the previous month.
28 Day Readmission Rate - TotalA 35 day period is required to accurately report all acute re-admissions for the previous month's discharges. (35 days = 28 days post discharge as per MoH measures plus 5 working days to allow for coding).
Variance from target not significant enough to report as non-compliant. This includes percentages/rates within 1% of target, or volumes within 1 value from target.
Result not available, too soon to report
Number of healthcare-associated bloodstream infections, Number of healthcare-associated Staphylococcus aureus bacteraemiaResults are based on a manual process and complete test results not being available for the previous month.
% Very good and excellent ratings for overall patient experience for inpatients% Very good and excellent ratings for overall patient experience for outpatients
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
77

Engaged Workforce
Leave management continues to be a challenge. We have encouraged staff with excess leave balances to take leave. However, the combination of staff shortages, higher sick leave and workload demands meant some planned staff leave in October needed to be cancelled. A centralized approach to rostering and leave planning has been developed to help us better manage our staff and we are beginning to see the benefits from this approach. However our current Models of Care in Nursing and Midwifery do not accommodate full coverage of annual entitlements making it extremely difficult to manage excess leave whilst meeting service demands.
At present our midwifery vacancies are high. Recruitment of midwives is a challenge because we are reliant on new graduates to maintain our workforce and there is only one output from the AUT each year. We have aggressively recruited from overseas and other universities in New Zealand and have been successful in attracting seven new midwives who will start early next year.
Strategic Initiatives A summary of progress against WH strategic initiatives:
Work stream Objectives Progress
Consolidation of Women’s Health improvement programme
• Visibility of all improvement activity in women’s health
• Process to manage existing projects and prioritise new projects
• Improved allocation of resources
• New Service Clinical Directors in post. Work has commenced to review and prioritize our improvement projects against our agreed strategic direction as outlined in our “Excellence in Women’s Health” document.
Recovery after Obstetric Surgery (EROS)
• Optimize recovery after caesarean section to enable a smoother return to normal activities and better support breastfeeding
• Recovery after Obstetric Surgery (EROS) project which commence on August 1st and the regional work on maternity pathways.
Review of Women’s Acute pathways
• Develop a clear understanding of acute maternity pathways.
• Identify opportunities to improve the service for women and management of resources
• This project continues to remain on track with good engagement from all members of the team. A Flow Coordinator role has been recruited to and due to commence late Jan 15. This role will enable a more efficient patient flow through Womens Assessment Unit and assist in pulling patients from the Emergency Department.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.2
78
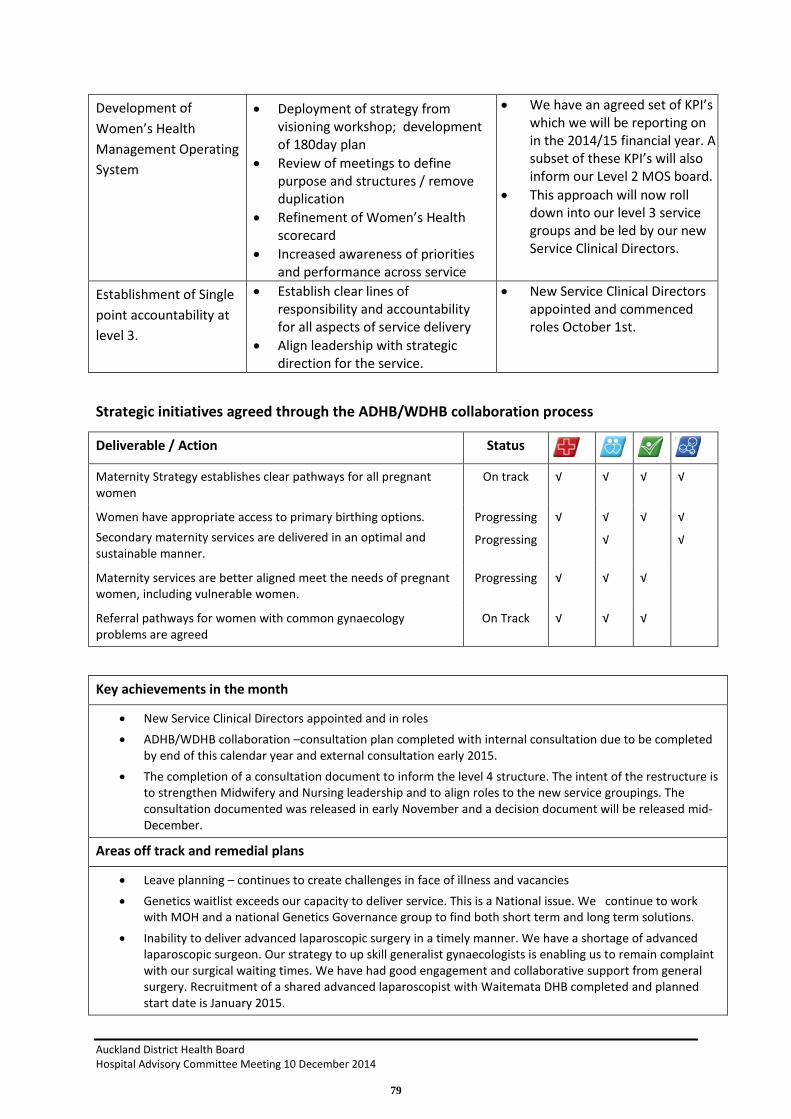
Development of Women’s Health Management Operating System
• Deployment of strategy from visioning workshop; development of 180day plan
• Review of meetings to define purpose and structures / remove duplication
• Refinement of Women’s Health scorecard
• Increased awareness of priorities and performance across service
• We have an agreed set of KPI’s which we will be reporting on in the 2014/15 financial year. A subset of these KPI’s will also inform our Level 2 MOS board.
• This approach will now roll down into our level 3 service groups and be led by our new Service Clinical Directors.
Establishment of Single point accountability at level 3.
• Establish clear lines of responsibility and accountability for all aspects of service delivery
• Align leadership with strategic direction for the service.
• New Service Clinical Directors appointed and commenced roles October 1st.
Strategic initiatives agreed through the ADHB/WDHB collaboration process
Deliverable / Action Status
Maternity Strategy establishes clear pathways for all pregnant women
On track √ √ √ √
Women have appropriate access to primary birthing options. Secondary maternity services are delivered in an optimal and sustainable manner.
Progressing
Progressing
√ √
√
√ √
√
Maternity services are better aligned meet the needs of pregnant women, including vulnerable women.
Progressing √ √ √
Referral pathways for women with common gynaecology problems are agreed
On Track √ √ √
Key achievements in the month
• New Service Clinical Directors appointed and in roles • ADHB/WDHB collaboration –consultation plan completed with internal consultation due to be completed
by end of this calendar year and external consultation early 2015. • The completion of a consultation document to inform the level 4 structure. The intent of the restructure is
to strengthen Midwifery and Nursing leadership and to align roles to the new service groupings. The consultation documented was released in early November and a decision document will be released mid-December.
Areas off track and remedial plans
• Leave planning – continues to create challenges in face of illness and vacancies • Genetics waitlist exceeds our capacity to deliver service. This is a National issue. We continue to work
with MOH and a national Genetics Governance group to find both short term and long term solutions.
• Inability to deliver advanced laparoscopic surgery in a timely manner. We have a shortage of advanced laparoscopic surgeon. Our strategy to up skill generalist gynaecologists is enabling us to remain complaint with our surgical waiting times. We have had good engagement and collaborative support from general surgery. Recruitment of a shared advanced laparoscopist with Waitemata DHB completed and planned start date is January 2015.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
79

Key issues / initiatives identified in coming • Strengthening of service delivery models under new Service Clinical Directors SpoA model.
SCD’s will develop strategic plans relevant to their areas of responsibility and a key set of KPI’s which relate to the overall Women’s KPI’s but are specific to the strategic focus of the service grouping.
• Work continues with the National Health Board to develop a national plan to reduce the genetics waitlist.
• Finalise level 4 structure and embed new Models of care across Midwifery and Nursing services
Financial Results
STATEMENT OF FINANCIAL PERFORMANCEWomens Health Services Reporting Date Oct-14
($000s) MONTH YEAR TO DATEActual Budget Variance Actual Budget Variance
REVENUEGovernment and Crown Agency 268 191 77 F 885 765 120 F
Funder to Provider Revenue 7,630 7,630 0 F 30,011 30,011 0 F
Other Income 137 164 27 U 774 654 120 F
Total Revenue 8,035 7,985 50 F 31,670 31,431 240 F
EXPENDITUREPersonnel Personnel Costs 3,127 3,048 80 U 12,358 12,077 281 U
Outsourced Personnel 75 69 6 U 307 275 32 U
Outsourced Clinical Services 13 12 1 U 112 49 63 U
Clinical Supplies 460 433 27 U 1,747 1,732 14 U
Infrastructure & Non-Clinical Supplies 162 89 73 U 590 356 234 U
Total Expenditure 3,838 3,651 187 U 15,113 14,490 623 U
Contribution 4,197 4,334 137 U 16,557 16,940 383 U
Allocations 688 704 16 F 2,683 2,864 181 F
NET RESULT 3,509 3,630 121 U 13,874 14,077 203 U
Paid FTEMONTH (FTE) YEAR TO DATE ( FTE)
Actual Budget Variance Actual Budget Variance Medical 63.8 65.5 1.8 F 62.6 65.4 2.8 F
Nursing 252.3 237.4 15.0 U 253.9 237.4 16.6 U
Allied Health 18.3 18.3 0.1 F 18.2 18.3 0.1 F
Support 0.0 0.0 0.0 F 0.0 0.0 0.0 F
Management/Administration 33.9 36.6 2.6 F 33.5 36.6 3.0 F
Other 0.0 0.0 0.0 F 0.0 0.0 0.0 F
Total excluding outsourced FTEs 368.3 357.7 10.6 U 368.3 357.6 10.7 U Total :Outsourced Services 3.2 2.6 0.6 U 5.0 2.6 2.4 U
Total including outsourced FTEs 371.5 360.3 11.2 U 373.3 360.2 13.1 U
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.2
80

Comments on Major Financial Variances The end result for the month was $121k U and $203k U YTD. The month’s results were impacted by Midwifery cost overruns and bad and doubtful debt write offs.
MOH base income is recognised at Directorate level as per 2014/15 budget. CWD volumes for the month and YTD were 98% of contract. Following trends from 13-14, for the month acute Gynae was 118% of contract and Specialist Neonates 121%. YTD Gynae acutes are 112% to contract. Total discharges from the service for the YTD are 7,730 which are not significantly different from the same period last year.
Year to date financial analysis:
Revenue • Private patient income is $184k F to budget. These patients are in the Fertility + service and
the revenue relates to treatments completed within the month. This revenue fluctuates from month to month depending on patients completing their treatment cycles
Expenses • Personnel $313k U. Midwifery costs are the main driver. The consultation on the New
Models of care has been delayed to enable the level 4 restructure process to progress first. It was recognised that changes to the MOC required the right leaders to be in place to drive the changes required. A decision will be made on the new level 4 structure before the end of the calendar year with implementation planned for February 2015.
• Infrastructure and nonclinical supplies $234k U – mainly a reflection of Doubtful Debt allocations which reflect invoiced but not paid. This will reduce as the debts are paid
• Allocations $181k F. This relates to Labs charges and relates to a change in clinical practice in gynecology that has led to a reduction surgery
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
81

Child Health Directorate
Speakers: Dr John Beca, Surgical Child Health Director, and Dr Michael Shepherd, Medical Child Health Director
Service Overview The Child Health Directorate is a dedicated paediatric healthcare service provider and major teaching centre. This Directorate provides family centred care to children and young people throughout New Zealand and the South Pacific. Care is provided for children up to their 15th birthday.
A comprehensive range of services are provided within the two directorate portfolios;
Surgical child health (Director, Dr John Beca) Paediatric and Congenital Cardiac Services, Paediatric Surgery, Paediatric ORL, Paediatric Orthopaedics, Paediatric Intensive Care, Neonatal Intensive Care, Neurosurgery, Consult Liaison.
Medical child health (Director, Dr Michael Shepherd) General Paediatrics, Te Puaruruhau, Paediatric Haematology/Oncology, Paediatric Medical Specialties (Dermatology, Developmental, Endocrinology, Gastroenterology, Immunology, Infectious Diseases, Metabolic, Neurology, Chronic Pain, Palliative Care, Renal, Respiratory, Rheumatology), Children's ED, Safekids and Community Paediatric Services (including Child Health and Disability, Family Information Service, Family Options, Audiology, Paediatric Homecare and Rheumatic Fever Prevention)
The leadership team members are: Dr Michael Shepherd, Director, Dr John Beca, Director, Emma Maddren, General Manager, Sarah Little, Nurse Director, Linda Haultain, Allied Health Director.
Scorecard Scorecard and financial data is for the month of October 2014.
Children's HealthOct-14 Measure Target
Number of healthcare-associated bloodstream infections N/A TBC 8
Number of healthcare-associated Staphylococcus aureus bacteraemia N/A TBC 0
Central line associated bacteraemia rate per 1,000 central line days 0.0 <=1 0.0
Medication Errors 30 0 26
Number of reported adverse events causing harm (SAC 1&2) 0 0 0
Actual Prev Period
Incr
ease
d Pa
tient
Sa
fety
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.3
82

(MOH-01) % CED patients with ED stay < 6 hours 93.7% ≥95% 94.6%
HT2 Elective discharges cumulative variance from target 1.13 >=1 1.16
(ESPI-1) % Services acknowledging 90% of FSA referrals 100.0% 100% 88.0%
(ESPI-2) Patients waiting longer than 5 months for their FSA 0.80% 0% 0.35%
(ESPI-5) Patients given a commitment to treatment but not treated within 5 months 0.50% 0% 1.73%
% DNA rate for outpatient appointments - All Ethnicities 10.4% ≤9% 11.1%
% DNA rate for outpatient appointments - Maori 17.0% ≤9% 19.3%
% DNA rate for outpatient appointments - Pacific 18.2% ≤9% 18.4%
Elective day of surgery admission (DOSA) rate 56.6% TBC 51.4%
% Day Surgery Rate 63.3% TBC 64.8%
Inhouse Elective WIES through theatre - per day 24.57 TBC 29.90
% Very good and excellent ratings for overall patient experience for inpatients N/A ≥90% 94.3%
% Very good and excellent ratings for overall patient experience for outpatients N/A ≥90% 78.9%
Number of complaints received 14 TBC 9
28 Day Readmission Rate - Total N/A ≤10% 12.6%
% Adjusted theatre utilisation 79.6% ≥80% 82.0%
Average Length of Stay for WIES funded discharges (days) - Acute 4.4 < 2.5 4.1
Average Length of Stay for WIES funded discharges (days) - Elective 1.4 < 1.5 1.3
Bett
er Q
ualit
y Ca
re
Immunisation at 8 months 95.0% ≥95% 96.0%
Excess annual leave dollars ($M) $0.44 0 $0.46
% Staff with excess annual leave > 1 year 33.0% 0% 33.1%
% Staff with excess annual leave > 2 years 8.6% 0% 8.8%
% Staff with excess annual leave and insufficient plan to clear excess by the end of financial year 100.0% 0% 98.9%
% Pre-employment Screenings (PES) cleared before the start date 71.4% 100% 61.1%
Sick leave hours taken as a percentage of total hours worked 3.8% ≤3.4% 3.8%
% Voluntary turnover (annually) 11.7% ≤10% 11.9%
% Voluntary turnover <1 year tenure 5.8% ≤6% 5.7%
Amber =
N/A =
These measures are based on retrospective survey data, i .e. completed responses for patients discharged or treated the previous month.
28 Day Readmission Rate - TotalA 35 day period is required to accurately report all acute re-admissions for the previous month's discharges. (35 days = 28 days post discharge as per MoH measures plus 5 working days to allow for coding).
Variance from target not significant enough to report as non-compliant. This includes percentages/rates within 1% of target, or volumes within 1 value from target.
Result not available, too soon to report
Number of healthcare-associated bloodstream infections, Number of healthcare-associated Staphylococcus aureus bacteraemiaResults are based on a manual process and complete test results not being available for the previous month.
% Very good and excellent ratings for overall patient experience for inpatients% Very good and excellent ratings for overall patient experience for outpatients
Enga
ged
Wor
kfor
ceIm
prov
ed
Heal
th
Stat
us
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
83

Scorecard Commentary
Health Targets
Shorter stays in ED Performance against the target was 93.7% for October. Whilst the number of presentations and acuity reduced somewhat during the early part of October, surges in demand and higher acuity in the latter part of the month impacted performance on this target. October 2014 had a 12% higher presentation rate and a 14% higher admission rate than the October 2013.
The acute flow steering group is addressing systemic issues to optimise flow throughout Starship and refocusing efforts on the patient experience. This work will continue through the spring and summer months and will inform winter 2015 planning.
Immunisation of 8 month olds
This target is consistently met with 95% performance for October 2014.
Access to elective surgery Elective performance continues to be actively managed although there was mixed performance during October. Time to FSA increased slightly from the previous period yet there was a significant improvement in time to surgery. The paediatric rheumatology service has significant resource constraints which impact ESPI 2 performance.
• ESPI 1 (acknowledgement of referral) was 100%. • ESPI 2 (time to FSA) performance was 0.80% non-compliant. 18 children waited greater than
150 days for a first specialist assessment during October. • ESPI 5 (time to surgery) performance was 0.50% non-compliant. 6 children waited greater than
150 days for surgery during October.
Active management of performance in the lead up to the 120 day target is underway. Paediatric ORL and Neurosurgery are compliant for ESPI 1, 2 and 5. Plans are in place for paediatric surgery and orthopaedics. Most medical specialties are already compliant for ESPI 2, a small quantum of additional clinics will be required to ensure all are fully compliant.
Increased Patient Safety
There were no Central Line Associated Bacteraemia (CLAB) events in October. It has been 92 days since the last CLAB event.
Medication errors for October were 30, all were minor in nature and no patient harm resulted. The error rate has increased slightly since September but remains considerably lower than earlier in the year. This reflects the presence of senior nursing staff in clinical areas and a persistent focus on this area of practice.
There were no adverse events causing harm (SAC 1 or 2) in the Child Health Directorate during October.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.3
84

Better Quality Care
Patient and family complaints There were 14 new complaints received in October. The key themes identified within the complaints remain communication, attitude and courtesy along with care and treatment. Where possible direct (face to face or telephone) contact is being made with family who have expressed concerns about the care provided for their child to discuss concerns and agree the best means of addressing these.
DNA rates Patient access and DNA rates are an important area of focus for the Child Health Directorate. The overall DNA rate reduced to 10.4% in October. DNA rates for Maori reduced from 19.3 to 17% and Pacific rates also reduced from, 18.4 to 18.2%.
A project was initiated in August to address DNA rates in respiratory and general surgery services. This work links to the Maori and Pacific DNA initiative and is being led by Allied Health Director, Linda Haultain. The current focus is on paediatric respiratory, paediatric general surgery and general paediatrics. The project leader has received a briefing on the sustainable transport project, and the links with parking, and its possible impact on DNA rates.
Improved Health Status
Immunisation of eight month olds The 2013/14 immunisation target is 95% of eight month old babies fully immunised by December 2014. ADHB remains at target with 95% coverage as at 31 October (Maori 92%, Pacific 97%). There was an increase for Pacific (2%) and a reduction for Maori (3%) in the October period. Work is ongoing to develop sustainability in closing the equity gap.
Immunisation of two year olds The total coverage rate at age two remains at target of 95% as at 31 October. Maori (94%) and Pacific (99%).
The current national coverage rates are 92% at eight months and 93% at two years.
These are good results for ADHB however the equity gap for Maori in the eighth month and two year old cohort has re-emerged. Sustaining high coverage is an ongoing challenge.
Rheumatic Fever Prevention Programme The Rheumatic Fever Prevention Programme is jointly funded by the Ministry of Health and Auckland DHB. This is managed through a Service Alliance between Auckland DHB and the four Auckland DHB PHOs. In addition to swabbing and treating sore throats, public health nurses and community health workers are identifying and treating skin infections. They are also referring families to the Auckland Wide Healthy Homes Initiative (AWHHI) for assistance with housing related issues.
4661 children have consented to engage in the Rheumatic Fever Prevention Programme. This represents a further 148 children consented in the targeted schools since July.
In term 4 2013 5 schools participated in whole school swabbing. The same 5 have just completed whole school swabbing through the months of October and November. A comparison will now be undertaken of the rates of GAS infection, skin infections and the resistance patterns of organisms between the 2013 and 2014 data.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
85

Family violence screening Family violence screening has reduced slightly to 41% for the quarter ended 31 July 2014. The next audit is currently being undertaken and will be finalised mid December 2014.
Engaged Workforce
Staff turnover reduced slightly to 11.7% in October, just above the organisational target.
Employees with excess annual leave (>2 years) reduced to 8.6% of the workforce. Active management of annual leave has continued and will remain a focus for the balance of 2014. There is an expectation that all staff will have a leave plan, with particular emphasis on use of all leave accrued for the year and any excess leave balances.
Strategic Initiatives The initiatives listed below have been developed as part of the Child Health Directorate Strategy and are heavily weighted to financial sustainability. The broader strategic programme for the Child Health Directorate is under review and initiatives targeting quality and safety will become a particular focus in 2015.
Deliverable / Action Status
Cost containment
FTE management On track √
Leave management In progress √ √
Capacity planning On track √ √
Reduce surgical outsourcing costs In progress √ √
Clinical supplies management On track √
Reduce medical staff costs In progress √
Pharmaceutical costs met by DHB of domicile In progress √
Reduce non-clinical operational costs On track √
Revenue growth in defined areas
Increase outreach clinic volume In progress √ √
Increase non-resident patient volume and pricing In progress √
Recover a greater portion of ACC funded volumes On track √
Secure new or additional funding for national services
In progress √ √
Strategic partnership with Starship Foundation In progress √ √
TPN co-payments In progress √
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.3
86

Model of service delivery
Transition planning In progress √ √
Review all non-clinically directed services and roles In progress √
Improved integration across inpatient – community In progress √ √
Medical specialties – pathway improvement project On track √ √
Productivity project In progress √ √
WDHB / ADHB collaboration In progress √ √
Community services review In progress √ √
New ways of working project In progress √ √ √ √
Development of child health transformation agenda
Development of child health strategy In progress √ √ √ √ √
Refresh tier 2 methodology In progress √ √ √
Identify sustainable suite of national services In progress √ √ √
Releasing time to care On Track √ √
Trend care pilot On track √ √
Increased Patient Safety - Better Quality Care - Economic Sustainability - Improved Health Status - Engaged Workforce
Key achievements in the month
• Consultation on the proposed service leadership structure for child health. Consultation began on 25th September and concluded on 22nd October.
• Completion of Phases 2 – 5 of the theatre re-development. This included pre-op, playroom, OR store room, anaesthesia offices, radio lollipop, PACU, OR reception, pharmacy, anaesthesia store, the OR corridor and the decontamination room. Phase 6 was also partially completed with OR 1 now refurbished and functioning.
• During the refurbishment of OR1 70 lists were displaced over a 7 week period, all were successfully decanted and surgical capacity maintained through close collaboration with adult surgical services.
• Successful roll out of Glamorgan Pressure Injury Risk Assessment and Prevention Tool and associated bundle of care.
Key issues / initiatives identified in coming months • Implementation of the new service level leadership structure for the Child Health
Directorate. • Phases 6 - 12 of the Starship Theatre Development Project. • Development of proposals for National funding and IDF funding for 2015/16. These will be
presented to the national planning and funding group in December 2014.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
87

Financial Results
Comments on Major Financial Variances The Child Health Directorate was $161k U for the month and $217k F YTD October. Inpatient WIES for the month was 106% to contract and 99% YTD October.
Factors impacting on the YTD performance are:
Revenue: • Non-resident income is $95k F to budget. The majority of the patients have been discharged
from Paediatric Cardiac Service. • Donation income is $1.097m U to budget. The budget has been set in the 2014-15 financial
year to reflect additional income from the Starship Foundation in relation to donations for the Starship Theatres rebuild. These will come at different points in time throughout the financial year as parts of the project are completed. A funding submission of $1m for the first two phases of the project has been tabled with the Foundation. This will be reflected in the next month’s financials.
STATEMENT OF FINANCIAL PERFORMANCEChild Health Services Reporting Date Oct-14
($000s) MONTH YEAR TO DATEActual Budget Variance Actual Budget Variance
REVENUEGovernment and Crown Agency 690 773 83 U 3,073 3,091 17 U
Funder to Provider Revenue 16,907 16,907 0 F 69,452 69,452 0 F
Other Income 475 1,089 615 U 2,909 4,357 1,447 U
Total Revenue 18,072 18,769 697 U 75,434 76,899 1,465 U
EXPENDITUREPersonnel Personnel Costs 9,346 9,599 252 F 37,405 37,996 592 F
Outsourced Personnel 118 147 29 F 463 587 124 F
Outsourced Clinical Services 192 213 21 F 944 851 93 U
Clinical Supplies 1,833 2,122 288 F 7,306 8,486 1,181 F
Infrastructure & Non-Clinical Supplies 287 255 32 U 1,144 1,019 125 U
Total Expenditure 11,777 12,335 558 F 47,262 48,941 1,679 F
Contribution 6,294 6,434 140 U 28,173 27,958 214 F
Allocations 925 903 21 U 3,687 3,690 3 F
NET RESULT 5,370 5,531 161 U 24,486 24,269 217 F
Paid FTEMONTH (FTE) YEAR TO DATE ( FTE)
Actual Budget Variance Actual Budget Variance Medical 216.6 220.7 4.1 F 215.4 220.4 5.0 F
Nursing 609.3 606.8 2.5 U 599.5 606.8 7.3 F
Allied Health 115.7 129.1 13.5 F 116.8 129.1 12.4 F
Support 0.0 0.0 0.0 F 0.0 0.0 0.0 F
Management/Administration 80.9 83.3 2.4 F 79.4 83.3 3.9 F
Total excluding outsourced FTEs 1,022.5 1,040.0 17.5 F 1,011.1 1,039.7 28.6 F Total :Outsourced Services 5.5 5.5 0.0 F 5.7 5.5 0.2 U
Total including outsourced FTEs 1,028.0 1,045.5 17.5 F 1,016.9 1,045.2 28.3 F
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.3
88

• Other Income is $467k U to budget. This relates to projects for the 2014-15 year which are currently underway. These projects aim to increase funding for TPN by way of co-payments and increased funding for national services to recognise the additional unfunded work being achieved. Broadening of the scope of these projects is underway while other potential income streams are being recognised.
Costs: • Personnel costs $716k F YTD. Main drivers for the variance are:
o Medical costs $320k F to budget and 6.1 FTE F to budget which is helping drive the YTD F cost variance
o Nursing $176k F and 7.3 FTE F to budget. Active recruitment is in place with positions set aside for new graduates. This includes clinical workload sharing within the directorate.
o Allied Health $150k F and 12.3 FTE F. The vacant FTE are mainly in the child community services and recruitment is on-going for these positions
o Overall active management of FTE for the whole Directorate includes: Weekly FTE reconciliation (actual-budget) and review by the Directors Rationalisation of all FTE pending approval and being sourced Delayed start of replacement FTE.
• Clinical supply costs $1.2m F. The patient mix for the last 4 months appears to be the key driver as reflected in the following data:
o Decreases in the average WIES per discharge e.g. Paed Medical down 3%, Paed Cardiac down 9% and Paed Surgical down 2%.
o Inpatient discharges have increased and are 111% of the same period last year. o Costs associated with high cost procedures e.g. catheters, blood products and
implants are all significantly less than the same period last year.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
89

Surgical Services Directorate
Speaker: Dr Wayne Jones, Director Surgical Services
Service Overview The Surgical Services Directorate is responsible for the provision of surgical services for the adult population. The Directorate leadership consists of Director -Surgical Services Wayne Jones, Nurse Director Anna MacGregor, Allied Health Director Kristine Nicol and General Manager Tara Argent. Supported by Emma Moss (HR), Justin Kennedy-Good (Service Improvement) and Lynette Hagenson (Finance)
The services in the Directorate are structured into the following portfolios:
• Orthopaedics, ORL, Neurosurgery, Oral Health • General Surgery, Trauma, Transplant, Urology • Ophthalmology Clinic Facilities, Clinic Nursing, Pre Admit
Scorecard
Surgical ServicesOct-14 Measure Target
Number of healthcare-associated bloodstream infections N/A TBC 7
Number of healthcare-associated Staphylococcus aureus bacteraemia N/A TBC 3
Nosocomial pressure injury point prevalence (% of in-patients) 4.3% 0% 0.0%
Medication Errors 22 0 21
Falls with major harm per 1,000 bed days 0.14 TBC 0.00
Number of reported adverse events causing harm (SAC 1&2) 1 0 2
Actual Prev Period
Incr
ease
d Pa
tient
Saf
ety
HT2 Elective discharges cumulative variance from target 0.92 >=1 0.92
(ESPI-1) % Services acknowledging 90% of FSA referrals 100.0% 100% 85.0%
(ESPI-2) Patients waiting longer than 5 months for their FSA 0.10% 0% 0.31%
(ESPI-5) Patients given a commitment to treatment but not treated within 5 months 0.35% 0% 0.67%
% DNA rate for outpatient appointments - All Ethnicities 10.12% ≤9% 10.16%
% DNA rate for outpatient appointments - Maori 21.8% ≤9% 19.7%
% DNA rate for outpatient appointments - Pacific 17.7% ≤9% 19.4%
Elective day of surgery admission (DOSA) rate 78.6% ≥68% 79.7%
% Day Surgery Rate 59.0% ≥70% 60.1%
Inhouse Elective WIES through theatre - per day 64.10 TBC 64.47
Number of CBU outliers 180 0 242
% Patients cared for in a mixed gender room at midday - Adult 15.0% TBC 10.0%
% Very good and excellent ratings for overall patient experience for inpatients N/A ≥90% 80.2%
% Very good and excellent ratings for overall patient experience for outpatients N/A ≥90% 87.8%
Number of complaints received 26 TBC 32
28 Day Readmission Rate - Total N/A ≤10% 10.3%
Average Length of Stay for WIES funded discharges (days) - Acute 3.64 TBC 3.34
Average Length of Stay for WIES funded discharges (days) - Elective 1.42 TBC 1.35
31/62 day target - % of non-surgical patients seen within the 62 day target N/A 85% 70.0%
31/62 day target - % of surgical patients seen within the 62 day target N/A 85% 50.0%
62 day target - % of patients treated within the 62 day target N/A 85% 60.0%
Bette
r Qua
lity C
are
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.4
90

Scorecard Commentary
Health Targets
Smoking Cessation Performance to target in September 99%, staff continue to offer the advice and support service to smokers to ensure that the target is sustained.
Elective Discharges Elective discharges have been delivered 93% of the ADHB target (-206, of which -100 = General Surgery, -92 = Ophthalmology) and 106% of the IDF target (+96 of which +37 = General Surgery , +52 = Ophthalmology) to the end of October.
At the end of October patients waiting longer than 5 months for their FSA is (ESPI 2) 0.19% or 24 patients (target is <0.4%), however the service managers are working with the production planners and bookers to ensure that patients are booked within the breach dates. All parties are now working towards the 4 month target and additional capacity is being delivered according to demand on a sub speciality level. The overall ESPI 2 position for September is moderately non-compliant.
The ESPI 5 position is 0.62% of patients or 27 patients in total (target is <1.0%) receiving a date for surgery over 5 months, both of these are improvements on the September position which demonstrates the hard work being undertaken by all administrative and clinical teams to deliver the 4 month target.
% Hospitalised smokers offered advice and support to quit 99.0% ≥95% 98.2%
Excess annual leave dollars ($M) $1.02 0 $0.97
% Staff with excess annual leave > 1 year 31.6% 0% 34.1%
% Staff with excess annual leave > 2 years 15.1% 0% 14.9%
% Staff with excess annual leave and insufficient plan to clear excess by the end of financial year 100.0% 0% 100.0%
% Pre-employment Screenings (PES) cleared before the start date 63.6% 100% 72.4%
Sick leave hours taken as a percentage of total hours worked 3.3% ≤3.4% 3.2%
% Voluntary turnover (annually) 8.2% ≤10% 8.2%
% Voluntary turnover <1 year tenure 0.0% ≤6% 0.0%
Amber =
N/A =
Enga
ged
Wor
kfor
ceIm
prov
ed
Heal
th
Stat
us
These measures are based on retrospective survey data, i .e. completed responses for patients discharged or treated the previous month.
28 Day Readmission Rate - TotalA 35 day period is required to accurately report all acute re-admissions for the previous month's discharges. (35 days = 28 days post discharge as per MoH measures plus 5 working days to allow for coding).
Variance from target not significant enough to report as non-compliant. This includes percentages/rates within 1% of target, or volumes within 1 value from target.
Result not available, too soon to report
Number of healthcare-associated bloodstream infections, Number of healthcare-associated Staphylococcus aureus bacteraemiaResults are based on a manual process and complete test results not being available for the previous month.
% Very good and excellent ratings for overall patient experience for inpatients% Very good and excellent ratings for overall patient experience for outpatients
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
91

Increased Patient Safety
A total of 20 falls (with no harm) incidents reported for October, which is a reduction of 16 compared to the September position, we continue to undertake a review of all incidents as we believe that some are being dual reported.
Pressure Injuries – 20 incidents reported for October. There were:
• 10 Category 1 (Non-blanchable erythema) • 8 Category 2 (Partial thickness) • Category 3 (Full thickness skin Loss) acquired • Category 4 (Full thickness tissue loss)
Total of 22 medication errors. These were of low risk; including omission, documentation and duplication. We are reviewing the themes and ensuring that that these are raised at the daily ward MOS meetings.
Adverse Events - There was 1 SAC 2 event reported in October; the incident is being investigated.
Better Quality Care
The DNA rate for appointments for all ethnicities remains above target at 10.12% and it is unclear what is driving this. Work is on-going to improve communication and contact with patients to reduce the number of DNAs.
The number of outliers has reduced from 242 to 180 in October. This issue remains linked to the high surgical acute load for the month. The directorate continue to review the bed configuration across all specialties, to be able to align the capacity to the demand, cohorting and repatriating patients to reduce the outliers across the surgical bed base. We continued to have 31 East open during the beginning of October which contributed to the reduction in outliers.
Improved Health Status
Smoking performance – achieved target again in October.
Engaged Workforce
Mind Over Manner Training - on the 30th of October we held a customer service workshop for the Ophthalmology admin and clerical team. This training was developed and provided in conjunction with a patient advocate who had complained about their experience when asking for directions and support in the clinic environment. Mind over Manner is an interactive workshop where a skilled MoM facilitator uses hypothetical and real life scenarios that are played out by actors and then improved, shaped and altered using the input and suggestions of the audience. It was extremely well received by the team and allowed them to come together to identify areas for improvement and change in ways in which we interact with our patients and improve customer service.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.4
92

Strategic Initiatives
Deliverable / Action Status
Reduce average LOS
Long stay patients
ERAS in Ortho / Gen surg
Rollout
In progress
√ √ √
Outpatient Service Improvement Programme
Review / Standardise of Communications
Standardised Processes
31/62 day cancer target
In progress
√ √ √ √
Adult savings programme
ACC and Non Resident funding
Outsourcing reduction
DTC reduction in line with Concord programmes
On Track
On Track
On Track
√
Orthopaedic Service review
Capacity v Demand
Outsourcing review
ESPI compliance
In progress √ √ √ √
Key achievements in the month
• ADHB delivered 100.3% for quarter 1 (Discharge target) • 4 month countdown clock “live” on the intranet for all staff to see • 4 month communication – posters sent to all admin areas • Delivery of the Mind over Manner workshop • Continue to work towards the delivery of the 4 month target • Closure of 31 East (short stay surgical ward) after the agreed period, against a
reduction in the number of outliers in October
Areas off track and remedial plans
• ESPI Compliance (moderately non-compliant) – All teams continue to deliver the additional capacity required to achieve the 4 month target.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
93

Financial Results
Comments on Major Financial Variances We are unfavourable to budget in October with a net result of $129k U.
Current Month The key variances in the month are:-
• Revenue $136k U due to delay in maximisation of revenue projects. We are currently forecasting to meet targets for year overall
• Outsourcing $126k F reflecting low outsourcing for Orthopaedics but this is offset by low volumes.
• Clinical Supplies $189k U mainly due to the costs of high acuity Transplant patients including two high cost retrieval flights from Australia and delayed realisation of expected healthAlliance (hA) procurement projects.
YTD We are favourable for the YTD ($84k F). This is primarily driven by staffing vacancies ($663k F) and decreased outsourcing ($554k F) which is in turn driving lower volumes.
Business Improvement Savings We are currently delivering on our Business Improvement Savings.
STATEMENT OF FINANCIAL PERFORMANCESurgical Services Reporting Date Oct-14
($000s) MONTH YEAR TO DATEActual Budget Variance Actual Budget Variance
REVENUEGovernment and Crown Agency 849 844 5 F 3,289 3,375 86 U
Funder to Provider Revenue 21,409 21,409 0 F 85,763 85,763 0 F
Other Income 388 529 141 U 1,503 2,116 613 U
Total Revenue 22,646 22,782 136 U 90,554 91,253 699 U
EXPENDITUREPersonnel Personnel Costs 7,275 7,198 78 U 27,899 28,561 663 F
Outsourced Personnel 184 235 51 F 884 940 56 F
Outsourced Clinical Services 194 320 126 F 725 1,278 554 F
Clinical Supplies 2,422 2,233 189 U 9,557 8,933 624 U
Infrastructure & Non-Clinical Supplies 122 213 91 F 760 856 96 F
Total Expenditure 10,197 10,198 1 F 39,824 40,569 745 F
Contribution 12,449 12,584 135 U 50,730 50,684 46 F
Allocations 2,353 2,359 6 F 9,538 9,576 38 F
NET RESULT 10,096 10,225 129 U 41,192 41,108 84 F
Paid FTEMONTH (FTE) YEAR TO DATE ( FTE)
Actual Budget Variance Actual Budget Variance Medical 192.6 200.8 8.2 F 190.8 201.2 10.4 F
Nursing 474.1 471.6 2.5 U 470.1 471.6 1.5 F
Allied Health 42.0 38.5 3.5 U 38.1 38.5 0.4 F
Support 0.0 0.0 0.0 F 0.0 0.0 0.0 F
Management/Administration 63.8 65.0 1.2 F 65.8 65.0 0.8 U
Total excluding outsourced FTEs 772.5 775.9 3.4 F 764.7 776.3 11.6 F Total :Outsourced Services 15.2 14.0 1.2 U 13.1 14.0 0.9 F
Total including outsourced FTEs 787.7 789.9 2.2 F 777.8 790.3 12.5 F
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.4
94


Perioperative Services Directorate
Speaker: Vanessa Beavis, Director
Service Overview The Perioperative Service provides services for all patients who need anaesthesia care and operating room facilities. All surgical specialties in ADHB use our services. Patients needing anaesthesia in non-operating room environments are also cared for by our teams. There are five suites of operating rooms on two campuses, and includes five (or more) all day preadmission clinics every weekday. We provide the (24/7) acute pain services for the whole hospital. We also assist other services with line placement and other interventions when high level technical skills are needed.
Scorecard
Scorecard Commentary
Health Targets Improved access to electives Session usage for the month of October (i.e. the number of available sessions vs. those used) remains consistent at 97%. The top three reasons for non-use of sessions were: ‘unfilled by service’; ‘surgeon unavailable’ and ‘session released, not filled’.
Adjusted utilisation for all OR suites remains consistent at 86.7%. The international benchmark for adjusted utilisation (i.e. a measure of how efficiently the available time in the session is used) is 85%.
Perioperative ServicesOct-14 Measure Target
% Acute index operation within acuity guidelines 73% ≥ 95% 73%
Wrong site surgery 0 0 0
% antibiotics within 60 mins of operation 85% ≥ 80% 82%
Surgical safety checklist compliance 84% 100% 88%
# Same surgery rescheduled N/A ≤ 3% N/A
30 day mortality rate 0.7% ≤ 2% 0.8%
CSSD incidents 2.14% ≤ 2% 1.85%
Elective sessions planned vs actual 97% 97% 98%
Adjusted utilisation 86.7% 85% 85%
Late starts 12% ≤ 5% 12%
% Sick leave 4.2% ≤ 3.9% 4.09%
Turnover 0.30% ≤ 10% 0.92%
Excess annual leave > 2 years 9.7% 0% 10.4%
Finishing on time 94% ≥ 90% 90%
Amber =
N/A =
Variance from target not significant enough to report as non-compliant. This includes percentages/rates within 1% of target, or volumes within 1 value from target.
Result not available, too soon to report
Actual Prev Period
Incr
ease
d Pa
tient
Sa
fety
Bett
er Q
ualit
y Ca
reIm
prov
ed
Heal
th S
tatu
sEn
gage
d W
orkf
orce
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.5
95

‘All cause’ cancellations rate for patients was 13.8%. The predominant reasons for patient cancellations/deferment in October were all related to the heavy acute load: ‘acute substitution by acute’; ‘acute cancellation’; ‘substitution by acute’.
This continues the trend of the past few months whereby it is unusual for acute patients to be so affected by cancellations. This reflects the heavy acute load in the hospital.
Increased Patient Safety
Timely access to acute surgery is at 73%. This reflects the heavy acute load in the hospital. As nearly all elective sessions were filled, acute patients were restricted to acutes only sessions.
The new Surgical Safety Checklist process change has been rolled out throughout Level 8 Operating Rooms. Training and education sessions for all areas has been completed through all of the Surgical and Anaesthetic Departments. Roll out for other Operating Room Departments is planned for late January, early February 2015.
There have been no incidents of wrong site surgery.
There were no SAC 1 or SAC 2 adverse events in October.
Across Perioperative Services in October there were five medication errors (with no sequelae); ‘allergic reaction’, ‘extra dose/duplication’.
There were no falls or pressure injuries reported in October.
There was one patient complaint attributed to Perioperative Services in October related to a less than satisfactory communication between a staff member and a patient.
All risks have appropriate mitigation plans and are manageable.
Better Quality Care
30 day mortality rate remains low at 0.7%.
CSSD incidents have risen slightly in October to 2.14%. Contamination reduction is a priority focus for the department with a number of initiatives underway.
Improved Health Status
Late starts remain at 6% largely due to rescheduling requirements related to high hospital occupancy and some logistical issues related to consent.
For the month of October there were 1,553 planned sessions, of those, 36 sessions were not used. In addition, 87 sessions were recycled.
Engaged Workforce
We are encouraging staff to reduce their excess annual leave where possible, as production is the first priority.
A proposed reduced break over the Christmas holidays means people need to work so leave must be planned differently.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
96

List over runs and consequent late finishes continue, although this has remained above target at 94%. Late finishes have consistently been shown to be the single most important determinant of staff morale for Operating Room staff.
Our staff turnover rate remains low at 0.30%. Sick leave was slightly over target at 4.2%, and is being addressed.
Strategic Initiatives
Deliverable / Action Status
• Starship Operating Rooms rebuild
All decanting has been completed. Re-commissioning of refurbished OR 1 complete and operational.
New OR 7 is on track as per schedule - first list booked for 10.12.14.
Other auxiliary work still underway regarding refurbishment.
√
√
√
√
√
• Hybrid Operating Room, Level 4
Building has started and ordering of equipment is slowly progressing. Projected end date - mid Feb 2015.
The PACU build will be completed 25.11.14.
√
√
√
√
• Single Instrument tracking system
The business case is being fine-tuned and will be submitted by IT to CAMP in December (or January at the latest).
The work between the performance improvement specialists and project manager is now complete and being collated to form part of the business case.
√
√
√
√
• GSU – Optimisation of usage to maximise case mix and capacity
This has progressed to the point where there are only 11 vacant sessions over a four week period.
Work continues with the surgical services to make use of all available time.
√
√
√
√
Key achievements in the month
• Starship decanting completed. Upgrading of storage areas in Starship ORs has commenced and will be ongoing.
• CSSD selected as a finalist in the clinical excellence section of the ADHB Healthcare Excellence Awards.
• Surgical Safety Checklist changes rolled out in Level 8 Operating Rooms.
Areas off track and remedial plans
• Delays to the hybrid rebuild.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.5
97

Key issues / initiatives identified in coming months Hand Hygiene Project – introduction of “4 opportunities” for the Operating Room. We are continuing to develop promotional strategies to increase compliance with increasing audit success in all areas and continued feedback to clinical areas.
A greenbelt project has commenced to look at breakages and damage to the rigid scopes.
This (repair/replace issue) is an area of significant cost for the service. The project will hopefully result in considerable savings.
The pre-admission clinic is being re-organised at present which is a large piece of work and will align better with the surgical services and the outpatient project also underway at present.
Financial Results
STATEMENT OF FINANCIAL PERFORMANCEPerioperative Services Reporting Date Oct-14
($000s) MONTH YEAR TO DATEActual Budget Variance Actual Budget Variance
REVENUEGovernment and Crown Agency 194 214 20 U 771 855 84 U
Funder to Provider Revenue 0 0 0 F 0 0 0 F
Other Income 14 19 5 U 71 75 4 U
Total Revenue 208 232 25 U 842 930 88 U
EXPENDITUREPersonnel Personnel Costs 7,253 7,312 58 F 28,755 28,962 208 F
Outsourced Personnel 97 43 54 U 251 172 80 U
Outsourced Clinical Services 0 0 0 F 0 0 0 F
Clinical Supplies 3,533 3,240 293 U 13,561 12,960 601 U
Infrastructure & Non-Clinical Supplies 166 147 18 U 691 590 101 U
Total Expenditure 11,049 10,742 307 U 43,258 42,684 574 U
Contribution (10,842) (10,510) 332 U (42,416) (41,754) 662 U
Allocations 27 27 0 U 107 110 3 F
NET RESULT (10,869) (10,537) 332 U (42,523) (41,864) 659 U
Paid FTEMONTH (FTE) YEAR TO DATE ( FTE)
Actual Budget Variance Actual Budget Variance Medical 157.2 164.3 7.1 F 158.8 164.3 5.5 F
Nursing 394.0 413.8 19.9 F 390.3 413.8 23.5 F
Allied Health 93.7 107.2 13.4 F 95.3 107.2 11.8 F
Support 114.8 111.8 3.0 U 113.0 111.8 1.1 U
Management/Administration 23.1 24.4 1.3 F 22.8 24.4 1.6 F
Total excluding outsourced FTEs 782.7 821.4 38.7 F 780.2 821.4 41.3 F Total :Outsourced Services 3.8 1.3 2.5 U 3.1 1.3 1.8 U
Total including outsourced FTEs 786.5 822.7 36.2 F 783.2 822.7 39.5 F
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
98

Comments on Major Financial Variances Net Result The net results for October were $332k U ($659k U YTD).
The key driver of the current month unfavorable result is clinical supplies $293kU, due to:-
• Depreciation ($44k U) offset by the pool depreciation budget held at corporate level • Treatment disposables $191k U budget phasing forecasted to be offset by year end and • Clinical supplies target savings unmet for the month ($47k U) with projects commencing
later in the year
The YTD unfavourable result was driven by clinical supplies $601k U phasing U as above and unmet target savings $189k U, depreciation $190k U to be offset by the pool depreciation budget held at corporate level and the premium staffing costs of backfilling vacancies.
OR activity for the year, including virtual, measured by theatre minutes for the period is 1% more than the same period last year.
FTE The 39 FTE favorable in October is primarily due to operating room model of care nursing and anesthetic technician’s vacancies as the operating rooms transition to resourcing full capacity sessions. The favorable FTE variance is offset by the higher costs of backfill and lower ADHB revenue. Action – Perioperative and Surgical Service Managers to work to maximise surgical production.
Business Improvement Savings We are forecasting to achieve Perioperative Business Improvement savings by year end. The Perioperative team is focussed on implementing further projects which will reduce prices for consumables over and above healthAlliance savings by approximately $0.8M pa. This will offset the unmet target savings in the YTD unfavourable result. This remains an area of high risk for the Directorate.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.5
99


Cancer and Blood Directorate
Speaker: Richard Sullivan, Director
Service Overview Cancer is a major health issue for New Zealanders. One in three New Zealanders will have some experience of cancer, either personally or through a relative or friend. Cancer is the country’s leading cause of death (29.8%) and a major cause of hospitalisation.
The ADHB Cancer and Blood Service provide active and supportive cancer care to the 1.5 million population of the greater Auckland region. This is currently achieved by seeing approximately 5000 new patients a year and 46000 patients in follow-up/or on treatment assessment appointments.
The leadership within this directorate consists of Richard Sullivan, Director, Brenda Clune, Nurse Director, Carolyn Simmons Carlsson, Allied Health Director and Kelly Teague, General Manager.
Scorecard
Cancer and Blood ServicesOct-14 Measure Target
Number of healthcare-associated bloodstream infections N/A TBC 6
Number of healthcare-associated Staphylococcus aureus bacteraemia N/A TBC 1
Medication Errors 9 0 21
Falls with major harm. Days since last event 62 0 31
Number of reported adverse events causing harm (SAC 1&2) 0 0 0
(ESPI-1) % Services acknowledging 90% of FSA referrals 100.0% 100% 100.0%
% DNA rate for outpatient appointments - All Ethnicities 5.8% ≤9% 6.1%
% DNA rate for outpatient appointments - Maori 10.9% ≤9% 11.0%
% DNA rate for outpatient appointments - Pacific 9.9% ≤9% 9.6%
% Cancer patients receiving radiation/chemotherapy treatment within 4 weeks of DTT 100.0% 100% 100.0%
% Chemotherapy patients (Med Onc and Haem) attending FSA within 4 weeks of referral 92.0% 100% 95.9%
% Radiation oncology patients attending FSA within 4 weeks of referral 94.9% 100% 95.1%
Number of CBU outliers 18 0 29
% Very good and excellent ratings for overall patient experience for inpatients N/A ≥90% 100.0%
% Very good and excellent ratings for overall patient experience for outpatients N/A ≥90% 95.6%
Number of complaints received 5 0 0
28 Day Readmission Rate - Total N/A TBC 15.0%
Average Length of Stay for WIES funded discharges (days) - Acute 4.55 TBC 4.25
% Patients from referral to FSA within 7 days 24.0% TBC 27.8%
31/62 day target - % of non-surgical patients seen within the 62 day target N/A 85% 70.0%
31/62 day target - % of surgical patients seen within the 62 day target N/A 85% 50.0%
62 day target - % of patients treated within the 62 day target N/A 85% 60.0%
Actual Prev Period
Incr
ease
d Pa
tient
Sa
fety
Bett
er Q
ualit
y Ca
re
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.6
100
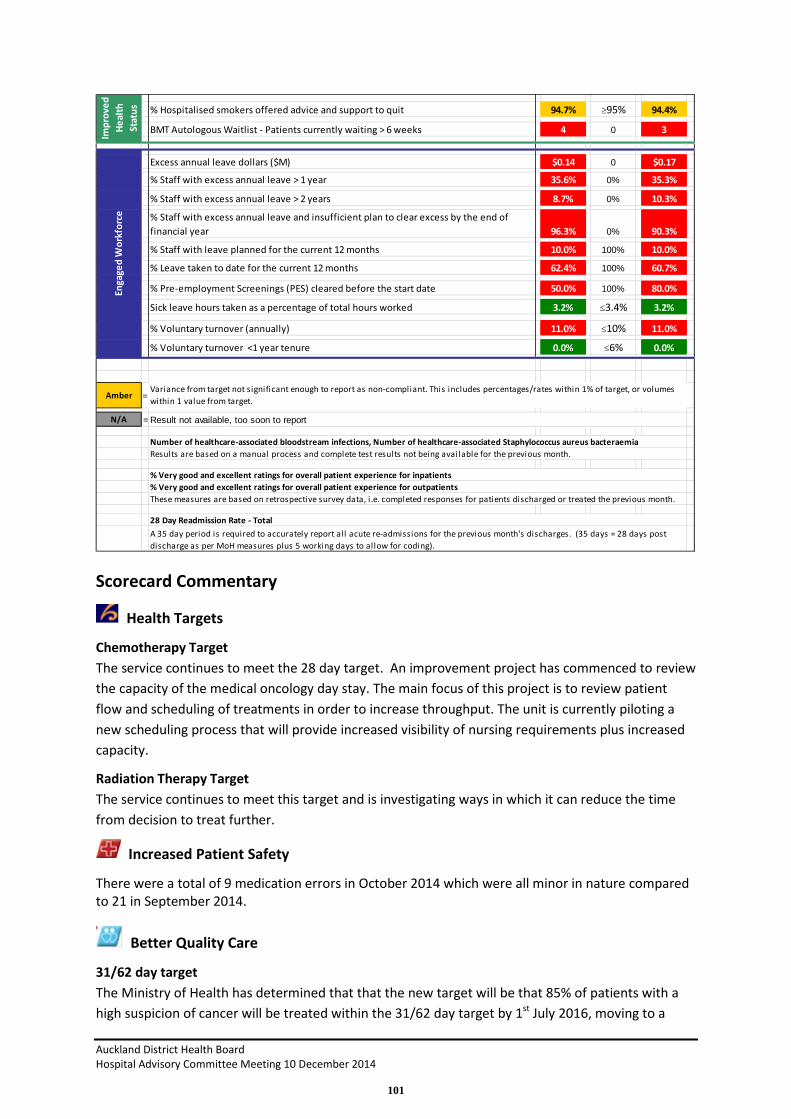
Scorecard Commentary
Health Targets
Chemotherapy Target The service continues to meet the 28 day target. An improvement project has commenced to review the capacity of the medical oncology day stay. The main focus of this project is to review patient flow and scheduling of treatments in order to increase throughput. The unit is currently piloting a new scheduling process that will provide increased visibility of nursing requirements plus increased capacity.
Radiation Therapy Target The service continues to meet this target and is investigating ways in which it can reduce the time from decision to treat further.
Increased Patient Safety
There were a total of 9 medication errors in October 2014 which were all minor in nature compared to 21 in September 2014.
Better Quality Care
31/62 day target The Ministry of Health has determined that that the new target will be that 85% of patients with a high suspicion of cancer will be treated within the 31/62 day target by 1st July 2016, moving to a
% Hospitalised smokers offered advice and support to quit 94.7% ≥95% 94.4%
BMT Autologous Waitlist - Patients currently waiting > 6 weeks 4 0 3
Excess annual leave dollars ($M) $0.14 0 $0.17
% Staff with excess annual leave > 1 year 35.6% 0% 35.3%
% Staff with excess annual leave > 2 years 8.7% 0% 10.3%
% Staff with excess annual leave and insufficient plan to clear excess by the end of financial year 96.3% 0% 90.3%
% Staff with leave planned for the current 12 months 10.0% 100% 10.0%
% Leave taken to date for the current 12 months 62.4% 100% 60.7%
% Pre-employment Screenings (PES) cleared before the start date 50.0% 100% 80.0%
Sick leave hours taken as a percentage of total hours worked 3.2% ≤3.4% 3.2%
% Voluntary turnover (annually) 11.0% ≤10% 11.0%
% Voluntary turnover <1 year tenure 0.0% ≤6% 0.0%
Amber =
N/A =
These measures are based on retrospective survey data, i .e. completed responses for patients discharged or treated the previous month.
28 Day Readmission Rate - TotalA 35 day period is required to accurately report all acute re-admissions for the previous month's discharges. (35 days = 28 days post discharge as per MoH measures plus 5 working days to allow for coding).
Variance from target not significant enough to report as non-compliant. This includes percentages/rates within 1% of target, or volumes within 1 value from target.
Result not available, too soon to report
Number of healthcare-associated bloodstream infections, Number of healthcare-associated Staphylococcus aureus bacteraemiaResults are based on a manual process and complete test results not being available for the previous month.
% Very good and excellent ratings for overall patient experience for inpatients% Very good and excellent ratings for overall patient experience for outpatients
Enga
ged
Wor
kfor
ceIm
prov
ed
Heal
th
Stat
us
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
101

target of 90% by 1st July 2017.The 31 day target is measured from decision to treat to first definitive treatment and 62 days is measured from an urgent General Practitioner referral for suspected cancer to first definitive treatment.
Progress against compliance for Auckland District Health Board for the last quarter ending 30th September 2014 was 44.6% and has deteriorated since the previous quarter which was 64.7%. A regional steering group has been established to review individual tumour stream pathways in order to agree them regionally and implement locally to improve performance. High suspicion data collection is also being reviewed to ensure all patients are being captured.
% Chemotherapy patients (medical oncology and haematology) attending FSA within 4 weeks of referral In light of the 31/62 day target, work is being undertaken to reduce FSA waiting times by 50% within the next year with a view to all FSA’s being seen within 7 working days from receipt of referral by July 2016.
Discussions are also underway with the medical and senior nurse workforce to enable Nurse Specialists within tumour streams to run dedicated clinics, removing this workload from medical staff and again increasing capacity for FSA.
Number of CBU outliers The key drivers for this are delays to discharge on ward 64. A process has been implemented whereby the long stay patients (over 14 days) are being reported to the directorates on a daily basis and appropriate action is being taken. The structures of ward rounds are also being reviewed as they are currently taking too long which means patients are frequently not being discharged until late afternoon.
% Radiation oncology patients attending FSA within 4 weeks of referral All patients accepted by the service received their FSA within 4 weeks. In light of the 31/62 day target, work is being undertaken to reduce FSA waiting times by 50% within the next year with a view to all FSA’s being seen within 7 working days from receipt of referral by July 2016.
Improved Health Status
Smoking Cessation Advice Throughout October 2014 there has been a slight improvement in compliance of 94.7% compared to September 2014 of 94.4%.
BMT Autologous waitlist patients waiting > 6 weeks The new Northern Region Bone Marrow Transplant Unit opened in mid-August 2014. Bed capacity has increased from 7-10 on the unit. However there was a 2 month delay in recruiting sufficient staff to support this which is reflected in our waiting list position. In October 2014 there were 4 patients waiting over 6 weeks.
Engaged Workforce
Excess annual leave management The service continues to work with staff with excess leave balances. Plans are in place to ensure that staff take this year’s leave allocation within the 12 month period and 62.4% have taken their leave within the allocated 12 months.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.6
102

Strategic Initiatives
Deliverable / Action Status/Deadline
Implementation of tumour streams across the directorate
30th June 2015 √ √ √ √ √
Develop protocols for the management of paediatric patients
31st Dec 2014 √ √ √
Re-design the directorate structure Design complete Implement February
2015
√ √ √
Develop a regional cancer strategy alongside colleagues at neighbouring District Health Boards
June 2015 √ √ √
Develop a business case for a Comprehensive Cancer Centre
March 2015 √ √ √ √
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
103

Financial Results
STATEMENT OF FINANCIAL PERFORMANCECancer & Blood Services Reporting Date Oct-14
($000s) MONTH YEAR TO DATEActual Budget Variance Actual Budget Variance
REVENUEGovernment and Crown Agency 716 741 25 U 2,893 2,965 71 U
Funder to Provider Revenue 8,377 8,377 0 F 33,316 33,316 0 F
Other Income 36 93 57 U 190 372 181 U
Total Revenue 9,129 9,211 82 U 36,399 36,652 253 U
EXPENDITUREPersonnel Personnel Costs 2,686 2,793 107 F 10,529 11,034 505 F
Outsourced Personnel 64 67 3 F 245 268 23 F
Outsourced Clinical Services 134 190 56 F 735 759 24 F
Clinical Supplies 2,752 2,883 132 F 11,396 11,533 137 F
Infrastructure & Non-Clinical Supplies 91 83 7 U 366 334 32 U
Total Expenditure 5,726 6,016 291 F 23,271 23,928 657 F
Contribution 3,403 3,195 208 F 13,128 12,724 404 F
Allocations 411 618 207 F 2,220 2,510 290 F
NET RESULT 2,992 2,577 415 F 10,908 10,213 695 F
Paid FTEMONTH (FTE) YEAR TO DATE ( FTE)
Actual Budget Variance Actual Budget Variance Medical 60.4 61.1 0.8 F 59.3 61.1 1.8 F
Nursing 142.8 138.2 4.6 U 139.8 138.2 1.5 U
Allied Health 79.4 79.6 0.2 F 80.8 79.6 1.2 U
Support 1.4 1.0 0.4 U 1.8 1.0 0.8 U
Management/Administration 10.8 13.3 2.5 F 11.0 13.3 2.3 F
Total excluding outsourced FTEs 294.7 293.2 1.5 U 292.6 293.2 0.5 F Total Outsourced Services 1.6 1.3 0.3 U 1.6 1.3 0.3 U
Total including outsourced FTEs 296.4 294.5 1.8 U 294.3 294.5 0.2 F
YTD ResultThe result for the YTD October is a surplus of $10,908k against a budgeted surplus of $10,213k , a favourable variance of $695k.
Total Revenue - $253k unfavourable mainly due Haemophilia blood product reimbursement driven by patient deman.d $119k U (offset by reduced blood product costs) and timing of donation income $128k U (pledges received for the BMT/Haematology ward still to be received).
Total Expenditure- $657k favourable mainly due to- Personnel and Outsourced Personnel combined $528k F. This is primarily due to favourable variances in
- Medical costs $149k F ( Oncology $108k F and Haematology $41k F due to vacancies and the impact of expired CPEwritten off in July) and
- Nursing costs $212k F driven by vacancies combined with the favourable impact of annual leave taken
- Clinical Supplies $137k F primarily due to instruments and equipment. $186k F due to timing of depreciation and RT machine repairs and maintenance and Pharmaceuticals $116k F offset by treatment disposable and blood products $124k U . Treatment disposables are made up of Haematology blood products $108k U, Oncology blood product $91k U offset by Haemophilia blood costs $138 F (demand driven).
Internal Allocations - $290k F - mainly due to the timing of research overhead recovery $160k F and radiology charges $101k F.
S i T t A hi d $2 000
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.6
104

Savings Plan Demonstrated below is the Directorates performance against our savings plan.
144 335 464
859
0 0 0 0 0 0 0 0 $144 $288 $432 $576 $720 $864 $1,008 $1,152 $1,296 $1,442 $1,586 $1,728
$-
$2,000
41821 41852 41883 41913 41944 41974 42005 42036 42064 42095 42125 42156
Financial Savings vs Target October 2014
Actuals
Planned
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
105

Community and Long Term Conditions Directorate
Speaker: Judith Catherwood, Director
Service Overview The Community and Long Term Conditions Directorate is responsible for the provision of care of Older People’s Health Services, Rehabilitation Services, Palliative Care Services, Community Based Nursing and Allied Health Services and Ambulatory Services for the adult population. The Directorate Leadership Team consists of Directorate Director, Judith Catherwood, Medical Director, Barry Snow, Jim Kriechbaum, Primary Care Director, Nurse Director Jane Lees and Allied Health Director Anna McRae.
The services in the Directorate are structured into 2 portfolios:
• A+ Links, Health of Older Persons, Rehab Plus, Needs Assessment and Service Coordination, Home Based Support, Residential Care, Care Navigation, Dementia, End of Life Care including Palliative Care
• Dermatology, Immunology, Rheumatology, Diabetes, Endocrinology, Chronic Pain, Sexual Health
Scorecard
Adult Community and Long Term ConditionsOct-14 Measure Target
Nosocomial pressure injury point prevalence (% of in-patients) 7.1% 0% 10.3%
Medication Errors 4 0 6
Falls with major harm per 1,000 bed days 0 0.09 0
Number of reported adverse events causing harm (SAC 1&2) 1 0 0
(ESPI-1) % Services acknowledging 90% of FSA referrals 100.0% 100% 100.0%
(ESPI-2) Patients waiting longer than 5 months for their FSA 0.00% 0% 0.00%
% Inpatients on Older Peoples Health waiting list for 4 days or less 91.2% ≥80% 88.7%
% DNA rate for outpatient appointments - All Ethnicities 10.3% ≤9% 11.7%
% DNA rate for outpatient appointments - Maori 16.1% ≤9% 21.3%
% DNA rate for outpatient appointments - Pacific 25.5% ≤9% 26.0%
% Patients cared for in a mixed gender room at midday - Adult 2.0% 2% 4.0%
% Very good and excellent ratings for overall patient experience for inpatients N/A ≥90% 100.0%
% Very good and excellent ratings for overall patient experience for outpatients N/A ≥90% N/A
Number of complaints received 6 TBC 3
Average Length of Stay for all patient discharges (days) 10.83 TBC 10.80
% Hospitalised smokers offered advice and support to quit 100.0% ≥95% 100.0%
Prev PeriodActual
Incr
ease
d Pa
tient
Sa
fety
Bett
er Q
ualit
y Ca
reIm
prov
ed
Heal
th
Stat
us
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.7
106

Scorecard Commentary
Increased Patient Safety
There were 17 pressure injuries reported in October. There were 4 medication errors for the month. There were no falls with harm reported in the month.
There was one SAC 2 event. A patient in OPH developed a pressure injury on the right heel and a full investigation is taking place to determine the cause.
Better Quality Care
The Directorate was 100% compliant for ESPI 1 and 2 targets. No patient waited longer than 5 months for their FSA.
The DNA rate for appointments is above target and remains a concern. Our Directorate action plan to address this is progressing and will be monitored closely over the coming months. We have set targets to reduce DNAs across our services and focus specific attention on activities to reduce Maori and Pacifica DNA rates. There has been a small reduction in DNAs from our September data and we will continue to monitor our progress in this area.
The Directorate remains committed to minimising the number of patients in mixed gender rooms and the rate in September was 2% and within our agreed tolerance range.
OPH waiting time performance and patient flow has remained within targets. The escalation plans are being implemented as required. We are also working on plans to reduce the number of patients with longer than average length of stay with clinical teams across the hospital.
Patient experience surveys have not been fully implemented across our Directorate by the patient experience team. At present only in patient areas in our directorate are targeted and completion rates post discharge are low. Current feedback is reviewed by all staff. We are working with the patient experience team to increase the number of patients providing feedback through this service.
Complaints are being actively managed within our Directorate meetings and action plans to address any learning points have been created and are being monitored. There were 6 complaints received in the month of October and all were responded to within the agreed target.
Excess annual leave dollars ($M) $0.12 0 $0.11
% Staff with excess annual leave > 1 year 33.1% 0% 33.3%
% Staff with excess annual leave > 2 years 8.8% 0% 8.1%
% Staff with excess annual leave and insufficient plan to clear excess by the end of financial year 83.7% 0% 93.6%
% Pre-employment Screenings (PES) cleared before the start date 83.3% 100% 88.9%
Sick leave hours taken as a percentage of total hours worked 3.7% ≤3.4% 3.6%
% Voluntary turnover (annually) 7.6% ≤10% 7.8%
% Voluntary turnover <1 year tenure 0.0% ≤6% 0.0%
N/A =
Enga
ged
Wor
kfor
ce
Result not available, too soon to report
% Very good and excellent ratings for overall patient experience for inpatients
These measures are based on retrospective survey data, i .e. completed responses for patients discharged or treated the previous month.% Very good and excellent ratings for overall patient experience for outpatients
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
107

Improved Health Status
Performance on the smoking advice metric is 100% this month.
Engaged Workforce
We have a number of staff members with excess annual leave. Current plans are not sufficient to reduce these leave balances this year and are being reviewed on a weekly basis. There has been an improvement in the percentage of staff with plans to clear excess leave balances within the year. Plans to support planned leave across clinical services continue to be progressed.
Sick leave is marginally above target and is being reviewed across the directorate applying the ADHB Wellness guide.
Strategic Initiatives Deliverable / Action Status
Service review and integration programme across Older Peoples Health, Rehab + and community services.
On track √ √ √ √
Patient Flow and Intermediate Care Work Stream including: • Gerontology and community service presence within ED • Rapid response team model • Early discharge team model • Reduce admissions from ARRC • Streamline NASC and Service Coordination process
On Track √ √ √ √ √
Dementia Care Pathway On Track √ √
Infusion Services Work Stream On track √ √ √ √
Stroke Pathway (in partnership with Acute Medical Directorate) On Track √ √ √
Sexual health review with WDHB. Being reconfigured for ADHB / WDHB sexual health review
On Track √ √ √
Talent Management and Leadership Development Work Stream On track √ √
Directorate operational performance and savings programme including:
• ACC revenue • Skill mix • Leave Management • Service and job sizing
On Track √
Directorate structure review to progress single point of accountability principles
On track √ √ √
Directorate team development On track √ √ √
Management Operation System Development Programme On track √ √ √
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.7
108

Key achievements in the month
• The Directorate has commenced consultation on its proposed clinical leadership structure to support SPoA and service development in line with our vision for services. Consultation concludes on the 5th of December.
• OPH launched a stroke specific rehabilitation unit in Rangitoto ward on the 10th of November. This unit cohorts all older adult stroke rehabilitation patients into one area, with the aim of improving team coordination of care and outcomes for this population. This is the first step in a plan to develop consistent care pathways for all stroke patients in ADHB.
• Two workshops have been held to support integrated service and pathway planning for patients across service groups. Over 60 staff attended and plans will be progressed to support service change based on the outcome in the New Year.
• The ADHB Palliative Care Governance Group has been re-established and a workshop to develop a revised strategic plan for the group was held in October. The group engages all partners across the health sector in Auckland.
• The pilot of “Wander Search” was successful and plans are progressing to implement this system. This is an electronic tracking system to reduce the risk of harm in those with Dementia or other cognitive impairment and at risk of wandering.
• The Dementia Care Governance Group is progressing plans to support the Dementia Friendly Hospital project. The aim is to improve care for patients admitted to hospital with cognitive impairment and improve access to specialist and support services in hospital and community settings.
• The Directorate Leadership Team visited CMDHB in October. Our visit provided an opportunity to develop professional links and explore areas of joint working or sharing of approaches between teams.
• The Short Term Home Based Support Service had a successful certification audit by the DAA.
Areas off track and remedial plans
• There has been an increase in number of complex patients requiring home based support. A proposal to change from the current in hospital assessment to a post discharge assessment model is being implemented. The entire NASC service model and pathway is being reviewed to improve the patient experience and flow.
• DNA action plan for the Directorate has been developed and is being implemented across all services.
• Leave management is being monitored on a weekly basis, specific targets have been set in high risk areas and action plans to address high leave balances within teams are being put in place across the service.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
109

Key issues / initiatives identified in coming months • Develop the Directorate Leadership team and embed management operating system across
the directorate at service and ward/team level. • Continue work on the Directorate Work Programme with partners across the sector and
develop the Directorate Strategic Plan. • Further development of community services including the review of the NASC process,
model of care within district nursing and allied health services, integration of our community rehabilitation services to ensure equity of care and further development of a locality multi-disciplinary model of service to reduce duplication and enhance community responsiveness.
• Continue skill mix reviews across the directorate. • Complete a preliminary feasibility study for an infusion centre at Green Lane. • Implementation of the revised Directorate structure under the principles of clinician led
SPoA. • Continue the development of work streams to improve the quality and outcome of the
patient’s journey including intermediate care, dementia care, stroke pathway and avoidable admissions.
• Development of a capital planning programme for the Directorate and the facilities our services utilise. A number of our buildings are in need of refurbishment. Plans are progressing for OPH and we will consider Rehab Plus and Community Service areas shortly. Our future requirements need to be informed by our clinical services plans and support a whole of ADHB approach.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.7
110

Financial Results
Comments on Major Financial Variances The YTD result is $987k F.
Revenue YTD is $169k F. This is largely due to Inter RAI revenue $75k F from June 2014 and Nurses Training reimbursement $115k F and ACC $80k F offset by the timing of recovery in some side contracts with the MoH $104k U.
Total Expenditure YTD is $695k F. Mainly due to: • Personnel and Outsourced Personnel combined are $428k F due to 22.3F in FTE. Outsourcing
includes $46kU for Mobility Solutions which is recovered from the Ministry. • Outsourced Clinical Services YTD is $9k U mainly in NZ Familial GI which is recovered under
contract from the Ministry. • Clinical Supplies are $221k F mainly due to under budget expenditure in Immunology Blood
$168k F and Rheumatology Pharmaceuticals $78k F. • Internal Allocations are $123k F, mainly due to reduced Lab charges in Ambulatory $111k F. • FTE is 22.3F YTD.
STATEMENT OF FINANCIAL PERFORMANCEAdult Community and LTC Reporting Date Oct-14
($000s) MONTH YEAR TO DATEActual Budget Variance Actual Budget Variance
REVENUEGovernment and Crown Agency 1,324 1,268 57 F 5,237 5,070 166 F
Funder to Provider Revenue 6,181 6,181 0 F 24,746 24,746 0 F
Other Income 28 19 9 F 77 75 2 F
Total Revenue 7,533 7,467 66 F 30,060 29,891 169 F
EXPENDITUREPersonnel Personnel Costs 3,992 4,074 82 F 15,639 16,150 511 F
Outsourced Personnel 92 55 37 U 302 219 83 U
Outsourced Clinical Services 104 133 29 F 541 532 9 U
Clinical Supplies 720 734 14 F 2,714 2,935 221 F
Infrastructure & Non-Clinical Supplies 149 187 38 F 693 748 55 F
Total Expenditure 5,057 5,182 125 F 19,889 20,584 695 F
Contribution 2,476 2,285 191 F 10,170 9,307 864 F
Allocations 343 354 11 F 1,318 1,441 123 F
NET RESULT 2,133 1,930 202 F 8,853 7,866 987 F
Paid FTEMONTH (FTE) YEAR TO DATE ( FTE)
Actual Budget Variance Actual Budget Variance Medical 70.5 69.8 0.7 U 68.3 69.9 1.6 F
Nursing 271.2 274.1 2.9 F 268.8 274.1 5.3 F
Allied Health 129.3 137.7 8.5 F 126.5 137.7 11.3 F
Support 0.0 0.0 0.0 F 0.0 0.0 0.0 F
Management/Administration 49.1 55.3 6.2 F 49.3 55.3 6.0 F
Total excluding outsourced FTEs 520.2 537.0 16.9 F 512.9 537.1 24.2 F Total :Outsourced Services 5.8 2.3 3.5 U 4.3 2.3 2.0 U
Total including outsourced FTEs 526.0 539.4 13.4 F 517.2 539.4 22.3 F
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
111

Non-Clinical Support Services
Speaker: Clare Thompson, General Manager
Service Overview This service delivery group is comprised of Corporate Support Services including Commercial Contract management, Clinical Education Centre, Sustainability, Security, Retail, Health Alliance Procurement & Supply Chain relationship, Health Benefits –Food & Linen programmes, Fleet Management, Car-parking, Mailroom, and Crèche. It also covers Non-Clinical Support Services within the Provider Arm including, Bed Management, Cleaning, Contact Centre, Food Services, Volunteers and Waste Collection.
Leadership team includes: Clare Thompson, General Manager, Manjula Sickler, Business Manager, Leanne Gatman, Finance Manager, Shankara Amurthalingam, Operations Manager Non-Clinical Support Services, Penny King, Service Manager- Food & Nutrition, Jane Woolford, Operations Manager Procurement & Supply Chain, Stuart Almao, HR Manager.
Scorecard
Scorecard Commentary
The Non Clinical Support Service continues to strengthen and enhance its overall service delivery across the organisation including quality improvement, enhancing staff training, building our team with the skills and expertise to manage the wide range of service under its portfolio.
A large number of service improvement work-streams are progressing well with team leaders fully engaged with all stakeholders including the clinical services to meet their requirements. Planning for the Christmas/New Year period is also underway to ensure supplies and staff resourcing is aligned with the clinical services plan during this period. We are also working with healthAlliance, Waitemata and Counties Manukau DHBs in a number of areas to help us achieve more service efficiencies and savings that are already underway in other DHBs. This also includes the contact centre collaboration project and the benchmarking on performance and standards is being initiated.
Non-Clinical Support ServicesOct-14 Measure Target
Excess annual leave dollars ($M) $0.11 0 $0.10
% Staff with excess annual leave > 1 year 36.2% 0% 37.9%
% Staff with excess annual leave > 2 years 11.1% 0% 10.7%
% Staff with excess annual leave and insufficient plan to clear excess by the end of financial year 97.3% 0% 97.5%
% Pre-employment Screenings (PES) cleared before the start date NULL 100% 100.0%
Sick leave hours taken as a percentage of total hours worked 5.9% ≤3.4% 6.0%
% Voluntary turnover (annually) 13.0% ≤10% 13.0%
% Voluntary turnover <1 year tenure 25.0% ≤6% 25.0%
NULL =No employee required pre-employment screening for the month of October.
Actual Prev Period
Enga
ged
Wor
kfor
ce
Not applicable
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.8
112

The weekly MOS sessions are now fully embedded into the service with weekly updates and progress on key actions. The team is building its capability in managing the service demand pressures by way of systems and protocols.
The improved quality of cleaning with the introduction of the Victorian Cleaning Standards continues. The latest audit for October reveals that both Grafton and Greenlane sites are achieving an average of 87% (last month 82%). The highest score was in the Support Building at 89%. Other sites with high scores were Starship building at 85% and ACH building at 81%. Overall, this is a significant achievement against the standards compared to the 42-50% when the cleaning service was outsourced and reflects the commitment and willingness of cleaning staff to become part of a team and embrace change with benchmarking standards.
The new security contract with First Security will take effect from 1st December. This will be followed by a new team structure and new roster which aligns with the recent electronic security and surveillance system installed in the ACH building Level 4.
The national business case for the Food Service continues to be negotiated with the preferred Service Provider (Compass Group Ltd). Staff consultation has been completed. There was a high level of participation in all stakeholder forums and the findings from the consultation will be presented to the Board on 10th December 2014.
The commentary below highlights the month’s activities:
Engaged Workforce
• Workforce Central Training – all cleaning staff training has been completed. It was noted that approx. 85% of staff had a lack of computer literacy. Further computer training is being explored to improve computer confidence.
• Language Literacy & Numeracy Course continues to progress with further sessions scheduled in 2015 if required
• NZQA Level 3 Cleaners Qualification – discussions with Auckland Metro DHBs to establish a centralised single Level 3 certification for NCS units and standard modules.
• Inductions for new volunteer recruits have been conducted. Continued recruitment progress underway focusing on Blue Coats.
• A second Volunteers newsletter has been published in October following the September publication which has been well received.
• Training for Waste Orderlies scheduled for 14th November.
Increased Patient Safety
• Business case for the upgrade to replace existing the access control and CCTV systems will be submitted to Board on 10th December 2015.
• Additional cameras, the video management system (VMS) and voice over internet protocol (VOIP) cameras are now active.
• Number of Patient Watches: Patient watches were down slightly with 122 in October compared to 124 in September. The increase in patient watches remains a concern and will require further focus when the new contract with First Security takes effect from 1st December 2015.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
113

• Code Orange: Conversely, code orange responses increased with 83 in October, up from 69 in September.
• New security contract due to be signed with First Security and expected go live date is 1st December. Once this is signed a team restructure will take place and the new shift roster will be initialised.
• Preparations for Ebola contingency underway and impact on non-clinical support services for example Cleaners, Waste, Security and Linen Services. Staff training, stock management and equipment and sealed trolley stock specifications factored into the overall Ebola plan.
Better Quality Care
• In October, the cleaning service achieved 87% against the benchmarking standards - an improvement from the previous month.
• New T2 Mini Jumbo toilet paper dispensers have been installed in staff/public toilets at Grafton and GCC to address the wastage, cleaning and maintenance issues experienced with the previous T3 dispensers.
• Awaiting the outcome of the RFP for Pest Control. • Cleaning Services are actively monitoring slips and trips with a goal of 0 incidents per month. • OH&S are assisting the service in assisting cleaning staff to achieve 100% compliant with
Virus and Hep vaccinations.
Cleaning Audit scores graph:
020406080
100120140160180
Janu
ary
Febr
uary
Mar
ch
April
May
June July
Augu
st
Sept
embe
r
Oct
ober
Code OrangePatient Watch
020406080
100
April
May
June July
Augu
st
Sept
embe
r
Oct
ober
Cleaning Audit Scores (%) at GCC & Grafton Target 100%
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.8
114

Current Month’s Activity
Car-park A
• Board Approved - Business case to construct the roof top parking in Car-park A adding 69 public car-parks to the ACH site. Construction to be completed by April 2015.
Contact Centre
• ADHB Collaboration meeting held with key stakeholder Management • Improvements in key SLA’s in October compared to previous month
Cleaning
• Workforce Central training is due to Go Live on 17th November for both weekly and fortnightly pay.
• Fire Safety Training confirmed for 26th November for members of Cleaning Services, Waste and Volunteer Services as well as DX Mailroom, Konica Minolta and Taylors Linen.
Food & Nutrition Service
• Telarc SAI Ltd has completed their annual review of the ADHB‘s food safety programme which covers the main kitchen and the three in-house cafes and achieved an A+ rating. The executive summary noting ‘the overall finding of the audit was that the food safety programme is being very well managed with a high standard of compliance throughout”.
• Patients now have a choice of side salads on the dinner menu, and the uptake has been 150-200 patients per night taking that option.
• Groups of nurses continue to visit the main kitchen to better understand where their patient meals are prepared and to discuss issues around correct ordering of meals for their wards. Totara ward staff members visited this month.
Linen and Laundry Services
• There has been a reduction in the total cost of linen and laundry of $76k in October 2014 compared to prior year and $48k is attributable to a reduction in non-sterile linen. Year to date credit adjustments totalling $64k relate to the one-off stock-take variance.
• A reduction of 4% in utilisation for the month of October has been observed across ADHB for month of October 2014. Departmental utilisation rates to be reviewed, with a view to reducing imprest levels for some items in consultation with end users is planned. Decreased utilisation rates are potentially related to seasonal fluctuations and occupancy and introduction of the larger sheet (eliminating the requirement for 2 bottom sheets for bed making).
• Disposable Curtain Trial – on track to commence over the next 4 weeks on ward 71 for a period of 3 months. The supplier is developing an assessment tool to establish the suitability of the product with approval by Infection Control.
• Reporting – Further investigation and work is required to progress reporting of occupied bed day costs for linen due to difficulty aligning the RC codes with the Business Unit volumes supplied by Business Intelligence Unit.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
115

Non Sterile Linen costs graph:
Procurement & Supply Chain Procurement and supply chain initiatives this month include;
• The appointment of a Dock Manager is underway. This appointment will help to address the daily demand pressures on dock space which is a major risk to the organisation as well as mitigation of Health & Safety issues.
• Service level agreements (SLA) between Service providers and ADHB are now underway. These include the Annual Operating Plan (Procurement) and SLA with Health Alliance. The SLAs will help to improve vendor performance and collaboration with key DHB stakeholders (eg. inventory management practice, shortage reports, data integrity and monitoring procurement savings).
• Planning is underway to implement the ADHB New Product Committee for both clinical/non clinical products. Monthly Clinical meetings to commence February 2015 and the non-clinical in December 2014. The brief for the clinical committee has been broadened to include product and supplier recommendations from Health Alliance and Pharmac. In the interim, all requests from the Clinical Product Coordinators (CPC) are being reviewed by the ADHB Supply Chain and Procurement team to ensure that the product once approved, is implemented correctly into the organisation.
• The daily congestion around Level Five Dock, Support Building on the Grafton site has been addressed by restricting staff in using this dock as a thoroughfare. Other measures being considered to mitigate the risk include reducing the number of vehicles parking around the area, and encouraging pedestrians to use the footpaths once better sign posted and repaired.
• The dock review and materials flows to wards and theatres with recommendations will be completed by end of January 15 with the following key objectives:
• That ADHB supply chain deliveries processes and the day to day operation of the Docks are in line with documented, agreed SOPs
o That the current congestion of loading docks and surrounding roadways is resolved o That workflow of clean/dirty goods though the hospital is improved o That the ADHB supply chain delivery process is compliant with OSH best practice o That the agreed SOPs support the best utilization of ADHB resources physically and
financially
0
200,000
400,000
600,000
800,000
1,000,000
1,200,000
July Aug Sept Oct Nov Dec Jan Feb Mar April May June
Mon
thly
Cos
t ex
GST
Total Monthly Linen Costs 12/13 vs 13/14 vs 1415
2012/13
2013/14
2014/15
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.8
116

Sustainability A number of sustainability initiatives are underway for the 14/15 financial year. These include;
• The installation of hand-dryers into all non-clinical areas (staff and public). • 6-month trial of a waste convertor (see comment above). • Recycling of glass and plastics.
o Level 4, level 8 & 9 theatres roll out of PVC Re-cycling as well as Day Surgery at Greenlane.
o Staff engagement includes rolling out staff kitchen recycling as well as looking at a larger recycling programme on site.
• Updated sustainability Communications plan with Communications team.
Volunteer Services • Hospital Grandparents programme under review. Key focus over the next 6 months will be:
o Induction and Training review o Review procedures child/HGP allocation o Marketing of Family Support, Hospital Grandparent and Pet Outreach Program
aimed at parents/caregivers o Improvement of communication between Starship and Volunteer Coordinator by
direct contact in case of specific/urgent issues o Volunteer Co-ordinator quarterly participation in Charge Nurse meetings o Improved child care information from nursing staff to HGP’s
Commercial Contract Management
Commercial Contract Status
Contract Status
Taylors (Linen) Expired - In Negotiation (HBL)
Ecolab Pest Control & Hygiene Expired - In Negotiation (healthAlliance)
First Security Expired - In Negotiation (healthAlliance)
Konica Minolta (Print) Concluded
DX Mail Expires 30th April 2016
OCM Expired - In Negotiation
Transpacific International Expired – In Negotiation
Auckland Co-op Taxis Expires 31st May 2016
Community Site Cleaning Expired – In Negotiation
SCA (Paper products) Expires 31st November 2014
Alpha Recruitment No variation
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
117

Management Operating System • The (MOS board) reporting has been fully embraced by the team in terms of transparency
and visibility. The MOS provides both staff and suppliers a range of performance against KPI’s and other benchmarking indicators.
Photocopier and Printer Refresh Project (Konica) • This project is expected to be completed by 30th October 2014. All project printer
installations have been completed at all sites. • A secondary label, audit and reconciliation of Grafton and outlying sites to commence 11th
August 14 for every device (approx. 2,000). GCC secondary audit completed. Grafton and outlying areas to be completed by end October 14
• This information will be held in the Konica database and will be made available to ADHB and healthAlliance (from November 14). Estimated savings of $2m over 5 years.
• Savings achieved for four months YTD 14/15 $356k.
Hand-Dryers in Non Clinical Toilets • Currently awaiting the signing of the new contract for 288 hand-dryers. • The final price negotiated reduced unit cost per machine by $123 resulting in total capital
savings of $25k. • Delivery is early expected to be December and installation commencing thereafter in
January 15.
Non Sterile Examination Gloves • The clinically approved non sterile examination glove new pricing takes effect from February
2015. Further savings of $60k in 14/15 and $44k in 15/16.
Greenlane Car-parking • Seed funding for apex approved $150k. • Council pre-application meeting booked for 12 November 2014. • Consultants engaged to prepare soil contamination, drainage and traffic reports.
HBL Facilities Management Service Stream (FMSS) • Food Service - Consultation regarding the proposed contracting out of food and nutrition
services to Compass Group commenced on 28th October, as part of an Auckland Metro initiative to enter into an early regional implementation of the proposed National Food Services contract. Following the initial announcement of the proposal to affected staff and unions, consultative forums and clinical impact briefings were facilitated by senior representatives of ADHB, HBL and Compass Group, followed by three days of Steamplicity demonstrations at ACH. The demonstrations were very well received by those who attended, and feedback was mainly positive with strongly positive feedback from the Charge Nurse Group. Consultation concluded on 14th November for feedback and submissions. The consultation feedback and outcome will be presented to the Board on 10th December 14. An ADHB steering group has been established, and has co-ordinated to plan and manage the activities associated with pre and post consultative processes, and commence mobilisation planning via establishment of work streams, should the project be approved to proceed.
• Linen & Laundry Services – A detailed business case has been presented at the August Audit & Finance Committee meeting and was approved in principle.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.8
118

Business Transformation Savings • For the four months year to October 2014, the service reported a total of $614K savings,
exceeding budget by $207k F. • The favourable variance is mainly attributed to Linen savings of $277k F, Photocopier/printer
project $145k F, Security $45k F and CEC Centre $27kF. These savings have offset other initiatives that are tracking under budget largely due to timing factors.
Economic Sustainability
Financial Results
STATEMENT OF FINANCIAL PERFORMANCENon-Clinical Support Services Reporting Date Oct-14
($000s) MONTH YEAR TO DATEActual Budget Variance Actual Budget Variance
REVENUEGovernment and Crown Agency 0 0 0 F 0 0 0 F
Funder to Provider Revenue 0 0 0 F 0 0 0 F
Other Income 49 31 18 F 173 124 49 F
Total Revenue 49 31 18 F 173 124 49 F
EXPENDITUREPersonnel Personnel Costs 1,283 1,461 178 F 5,453 5,740 287 F
Outsourced Personnel 185 14 171 U 812 56 756 U
Outsourced Clinical Services 0 0 0 F 13 0 13 U
Clinical Supplies 63 56 8 U 236 223 13 U
Infrastructure & Non-Clinical Supplies 1,487 1,559 72 F 6,128 6,235 107 F
Total Expenditure 3,018 3,089 71 F 12,642 12,254 388 U
Contribution (2,969) (3,058) 89 F (12,469) (12,130) 339 U
Allocations (824) (807) 17 F (3,287) (3,227) 60 F
NET RESULT (2,145) (2,251) 106 F (9,182) (8,903) 279 U
Paid FTEMONTH (FTE) YEAR TO DATE ( FTE)
Actual Budget Variance Actual Budget Variance Medical 0.0 0.0 0.0 F 0.0 0.0 0.0 F
Nursing 0.2 0.0 0.2 U 0.2 0.0 0.2 U
Allied Health 3.5 4.8 1.3 F 3.2 4.8 1.6 F
Support 266.0 316.9 50.8 F 272.2 316.9 44.6 F
Management/Administration 52.3 45.2 7.1 U 51.7 45.2 6.5 U
Total excluding outsourced FTEs 322.1 366.9 44.8 F 327.3 366.9 39.6 F Total :Outsourced Services 49.1 0.0 49.1 U 52.2 0.0 52.2 U
Total including outsourced FTEs 371.1 366.9 4.3 U 379.5 366.9 12.6 U
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
119

Comments on Major Financial Variances YTD Result is $279K U. The key drivers of this result are:
1. The key driver of this result is Personnel costs and outsourced personnel costs related to leave. This is due to the valuation of cleaner’s annual leave transferred from OCS which is $260K more than valued by OCS. A number of staff have transferred across with very high leave balances. There has been a concerted effort to try and get as many staff off on leave as possible to reduce this leave liability. This is driving higher outsourced costs. For the month of October however, the total personnel costs offset with outsourced personnel were in line with budget.
2. Infrastructure and Non–Clinical Supplies are favourable to budget due to a $75K one off rebate in regard to the security contract. Linen savings of $277K are contributing to this F variance. These are offset by some savings initiatives which will not be implemented until the second half of the financial year.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.8
120


Clinical Support Services
Speaker: Frank Tracey, General Manager, Acting Director
Service Overview This service delivery group is comprised of Daily Operations (including daily operations, transit, resource, bureau, volunteers & reception), Greenlane Clinical Centre (including Outpatient facilities, Patient Administration, Contact Centre & Interpreter services), Radiology, Laboratory, Clinical Engineering, Commercial Services, Nutrition, Emergency Management, Pharmacy and Allied Health Services (including Physiotherapy, Occupational Therapy, Speech Language Therapy, Social Work and Hospital Play Specialist services).
Scorecard
Scorecard Commentary
Health Targets
The new Ministry of Health targets are now reflected in our dashboard.
The installation of an additional MRI scanner at GCC is nearing completion and will be operational in January 2015. This will improve available capacity. Paediatric MRI has a significant impact on waitlist times due to the need for anaesthesia. We are working on ways to improve access to anaesthesia resource and are exploring outsourcing options to address the backlog of MRI GA paediatric scans.
The Radiology department is currently undertaking a major project to install and resite 3 CT scanners, consequently, outpatient capacity will be impacted for approximately 3 months (October – December 2014). Additional sessions are being booked on available equipment to minimise the
Clinical Support ServicesOct-14 Measure Target
Medication Errors 4 0 8
Number of reported adverse events causing harm (SAC 1&2) 0 0 1
Number of complaints received 4 0 3
% Outpatients & community referred MRI completed < 6 weeks 75.0% ≥80% 75.0%
% Outpatients & community referred CT completed < 6 weeks 66.0% ≥90% 78.0%
% Outpatient & community referred US completed < 6 weeks 48.0% ≥75% 51.0%
Excess annual leave dollars ($M) $0.42 0 $0.41
% Staff with excess annual leave > 1 year 33.9% 0% 32.6%
% Staff with excess annual leave > 2 years 8.4% 0% 8.1%
% Staff with excess annual leave and insufficient plan to clear excess by the end of financial year 97.6% 0% 96.7%
% Pre-employment Screenings (PES) cleared before the start date 84.1% 100% 74.2%
Sick leave hours taken as a percentage of total hours worked 3.7% ≤3.4% 3.7%
% Voluntary turnover (annually) 7.6% ≤10% 8.3%
% Voluntary turnover <1 year tenure 0.9% ≤6% 1.7%
Enga
ged
Wor
kfor
ce
Actual Prev Period
Incr
ease
d Pa
tient
Sa
fety
Bett
er Q
ualit
y Ca
re
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.9
121

impact on wait times. It is anticipated that CT will be at full capacity in December 2014 which will clear the backlog by mid-February 2015.
MRI While performance against the MRI target has improved over recent months (75%) we are 5% short of the MoH required 80%. We have put in place additional evening sessions on Starship MRI for both adults and paediatrics. The main issue remains access to anaesthetic time for paediatric MRI, this is our largest area of waitlist. We are actively working on the prospect of outsourcing additional GA paediatric sessions through the Centre for Advanced MRI (UoA).
CT As a consequence of the new CT scanner installation at GCC a downturn in productivity was expected. Performance against MoH 90% target of out-patients completed within six weeks has fallen to 66%. We have increased sessions for adult patients on the Starship CT scanner during this time, which will help manage the impact on wait times. Once the new CTs and resited old CTs has been completed (Dec/Jan), our capacity for CT outpatient exams will be increased by four sessions per week which will be dedicated to cardiac scanning and working towards maximising patient throughput for outpatients.
Ultrasound Performance is currently 48% against our internal 75% target, we are working on long term solutions to manage demand. Approximately 50% of the waitlist is vascular and GP referrals. Vascular referrals are time consuming and have grown by up to 20% year on year. GP referrals have increased significantly since early 2014. We are in communication with referrers (internal and GPs) to help manage volumes. A sustainable model to deliver out of hours US is in development, this includes the prospect of outsourcing volumes. While we are impacted by FTE vacancy (sonographers) and are actively recruiting to these roles to increase capacity. Four (4) additional weekend US sessions were undertaken in September/October and this has provided service for in excess of 200 patients from the current waitlist. The Department is piloting an after-hours service for inpatients which should have a positive impact on wait – times and the wait list.
Increased Patient Safety
There were no SAC 1 or 2 incidents reported for October. There were 4 medication errors reported-damaged medicationx1, delay in delivery x1 and unordered medicationx2 (Pharmacy). Each incident has been investigated at service level and improvement and training provided where required. There was no reported harm to the patients.
Better Quality Care
There have been 4 complaints in the month of October. These include issues with booking and scheduling (appointment times, delays in notification via letter), Discharge procedures (incomplete script, breakdown in communication re transfer by ambulance). All complaints have been reviewed, contact has been undertaken with some patients by telephone, written responses including explanation and apology provided to patients and recommended actions implemented.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
122

Engaged Workforce
The daily operations team in the hospital continue to coordinate a hospital wide response to unprecedented numbers of presentations and admissions. We are in the process of finalising our Escalation Planning (Seasonal Plan for Summer) which will focus on ensuring continuity of key activity in service delivery (hospital flow) for the coming 6 months.
Each service is actively managing staff Leave balances (annual leave, sick leave and excess annual leave). Service leave plans are aligned with planning for hospital flow and seasonal variation.
Strategic Initiatives
Deliverable / Action Status
PC3 Lab build Detailed planning underway – contingent on Lab shell.
Tender let
Due for completion Aug/Sep 2016
√
Level 4 Lab shell Tender closed
Site works to begin in December 2014
Due for completion Aug/Sep 2016
√
ADHB programme for AP project (DML/LTA)
Transition of daily operations to ADHB has taken place as of Oct 1.
Work is underway to refurbish a suitable site in Mt Wellington for location of the service by
March 2015
√
√
√
Consolidate Nuclear Medicine scans at ACH
ADHB have engaged with the Regional Radiology Group to develop a regional
response to provision of NM services in the region over the longer term.
√
√
√
3rd MRI scan at GCC Building commenced due date for completion Oct/Nov 2014 some delay due to site works and weather (approximately 3 weeks.
Full capacity by Feb 2015.
√ √ √
MOJ - ROI initiated for delivery of a National Forensic Pathology Service
Process on hold as per advice from MOJ – likely to be reinitiated in early 2015
x x
Pharmacy: PAPU (Pharmacy
Aseptic Production Unit)
Application for License to
manufacture medicines
Project underway
Application to Medsafe in development.
Project position paper under development currently
x
x
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.9
123

Radiology: Service Excellence II A series of service improvement initiatives/projects including a MoH funded
project are in development
√
√
√
√
Call Centre Collaboration
(WDHB/ADHB)
The implementation / project plan has been finalised and a decision document and associated communication has been provided to staff and key stakeholders.
Recruitment for joint CC Manager in train.
A tender for an updated Telephony solution has been issued.
√
√
√
√
Key achievements in the month Radiology
• Successful recruitment of new graduate MRT’s to fill vacancies • Service Excellence II underway including an after-hours US pilot • Project work on the new GLC MR build advancing
Clinical Engineering • Work is underway to determine how we can collaborate regionally with WDHB/CMDHB on
areas that are mutually beneficial.
Laboratory Services • The Regional community based AP project (DML/LTA transition) is on track ADHB took
responsibility for delivery of the service as of 1st October 2014. • ADHB is in the process of acquiring the Gynaecological Cytology Service (Cervical Screening)
currently provided by DML. Work is underway to finalise the contract for service and to plan for the recruitment of staff.
• Work is advancing on the refurbishment of Laboratory premises at Mt Wellington to accommodate the AP and recently potentially the Gynaecological Cytology Service (Cervical Screening)
Contact Centre Collaboration • The contact centre implementation / project plan has been finalised and a decision
document and associated communication has been provided to staff, Unions and key stakeholders.
• Recruitment for a joint (ADHB/WDHB) contact centre Manager has commenced with a view to appointment in early January 2015.
• A tender for an updated telephony solution has been issued. • A site visit to Auckland Council call centre has been scheduled for November 2014.
Forensic Pathology review • Terms of reference finalised and external panel of experts and key stakeholders established. • Review to commence early December 2014
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
124

Areas off track and remedial plans Radiology
• A series of initiatives are currently underway in radiology to better understand and ultimately address the capacity and demand issues associated with meeting new Ministry of Health Targets (CT under 6 weeks 90% and MRI under 6 weeks 80%).
Daily Operations • A review of booking and scheduling processes is underway across the organisation, our aim
is to improve the patient experience and assist accelerate admissions and relieve wait times for outpatient clinics.
• Planning is underway with the Adult Medical Services Directorate to develop and establish a service model to improve patient flow through Adult ED.
Key initiatives for the next six months
Area Timeframe
Radiology • Reduction of Ultrasound and MR waitlists. • Build programme and Installation of MRI at GCC has commenced • Additional after hours ultrasound
On-going
Oct/Nov 2014 October 2014
LabPLUS • Progress transformation initiatives including reducing operating costs. • Discussions re a National Integrated Forensic and Coronial Pathology Service on
hold pending communication from MOJ • Establish a cohesive regional Anatomical Pathology service through establishment
of ADHB Hospital and community based AP services. • Finalise contractual arrangements and planning for delivery of a Gynaecological
Cytology Service (Cervical Screening) by ADHB.
On-going On hold –
October 2014
March 2015
Pharmacy • Improvement projects in drug management (imprest, waste, safety) and
dispensing to continue. • Project underway to obtain a manufacturing licence. This could allow for increased
ability to manufacture/compound specific products on behalf of ACH, other DHBs and the private sector.
On-going
Dec 2014
Clinical Engineering • Implement transformational change programme and consolidate and stabilise
existing core services.
December 2014
Daily Operations • Complete ACH planning for seasonal trends (Escalation planning) and establish a
directorate wide support function to aid decision making.
June 2014 and
on-going
Forensic Pathology • Planning is advanced regarding a review of the Department of Forensic Pathology
and the National Coronial service (provided under contract to the MoJ). The aim is to assist the department develop a contemporary service delivery model and robust and sustainable infrastructure to support a national service.
October 2014 –
Jan 2015
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.9
125

Financial Results
Comments on Major Financial Variances YTD Result is $2,206K F. The key drivers of this result are: 1. Personnel Costs $2,465K F. This is part of a planned process which sees skill mix and vacancies
carefully managed to support service delivery in key areas. Delayed recruitment due to delay in MRI and CT scanner implementation is another contributing factor, however, this is offset by increased outsourced personnel ($278K).
2. Outsourced Clinical Services were $459K U of which $187K was due to CT and MRI project being delayed. These costs are being offset by savings in depreciation and employee costs. The remainder was in Laboratories due to cost of send away tests being higher than budget and targeted savings not achieved. This is being actively managed.
3. Clinical Supplies were F in Radiology and Laboratories. Savings in Laboratories due to savings for demand management being achieved and volumes being lower than budget. $313K savings in Radiology due to depreciation savings.
4. Service Billing Income U in Laboratories and Radiology due to volumes which is in line with overall provider arm volumes being lower than contract.
5. Funder to provider revenue is above budget due to the budget for Anatomical Pathology contract revenue being included in other income.
STATEMENT OF FINANCIAL PERFORMANCEClinical Support Services Reporting Date Oct-14
($000s) MONTH YEAR TO DATEActual Budget Variance Actual Budget Variance
REVENUEGovernment and Crown Agency 900 792 108 F 3,492 3,101 392 F
Funder to Provider Revenue 2,932 1,865 1,066 F 8,596 7,530 1,066 F
Other Income 1,802 2,844 1,043 U 7,099 8,461 1,362 U
Total Revenue 5,634 5,502 132 F 19,188 19,092 96 F
EXPENDITUREPersonnel Personnel Costs 9,935 10,470 535 F 36,912 39,377 2,465 F
Outsourced Personnel 401 262 139 U 1,327 1,049 278 U
Outsourced Clinical Services 748 634 114 U 3,052 2,593 459 U
Clinical Supplies 3,716 3,765 49 F 14,141 14,796 656 F
Infrastructure & Non-Clinical Supplies 473 483 10 F 1,606 1,767 161 F
Total Expenditure 15,274 15,615 341 F 57,039 59,583 2,544 F
Contribution (9,640) (10,113) 473 F (37,851) (40,491) 2,640 F
Allocations (7,546) (7,453) 93 F (29,884) (30,319) 435 U
NET RESULT (2,094) (2,660) 566 F (7,966) (10,172) 2,206 F
Paid FTEMONTH (FTE) YEAR TO DATE ( FTE)
Actual Budget Variance Actual Budget Variance Medical 126.6 139.6 13.0 F 117.5 129.0 11.6 F
Nursing 66.3 69.6 3.3 F 68.1 69.6 1.5 F
Allied Health 794.3 845.7 51.5 F 770.3 812.2 41.9 F
Support 70.7 68.4 2.3 U 71.4 68.4 3.0 U
Management/Administration 271.3 279.0 7.7 F 254.4 268.6 14.2 F
Total excluding outsourced FTEs 1,329.1 1,402.3 73.2 F 1,281.6 1,347.8 66.1 F Total :Outsourced Services 13.7 3.2 10.5 U 15.1 3.2 11.9 U
Total including outsourced FTEs 1,342.8 1,405.5 62.7 F 1,296.7 1,351.0 54.3 F
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
126

Cardiovascular Directorate
Speaker: Mark Edwards, Director
Service Overview The Cardiovascular Directorate comprises Cardiothoracic Surgery, Cardiology, Vascular Surgery, CVICU, Organ Donation New Zealand, the New Zealand Heart and Lung Transplant Unit and Hearty Towers. Mark Edwards is Director of the Directorate, Anna MacGregor is Nurse Director, Kristine Nicol is Allied Health Director and Tara Argent is General Manager. Jim Kriechbaum is the Primary Care Director. They are supported by Emma Moss (HR), Justin Kennedy-Good (Service Improvement), Sam Titchener (Service Manager) and Laurie Pharo (Finance).
Scorecard
Cardiac ServicesOct-14 Measure Target
Number of healthcare-associated bloodstream infections N/A TBC 2
Number of healthcare-associated Staphylococcus aureus bacteraemia N/A TBC 0
Nosocomial pressure injury point prevalence (% of in-patients) 11.5% 0% 7.1%
Medication Errors 22 0 22
Falls with major harm. Days since last event 3 0 526
Number of reported adverse events causing harm (SAC 1&2) 1 0 0
(ESPI-1) % Services acknowledging 90% of FSA referrals 100.0% 100% 100.0%
HT2 Elective discharges cumulative variance from target 1.04 >=1 1.01
% DNA rate for outpatient appointments - All Ethnicities 9.4% TBC 5.3%
% DNA rate for outpatient appointments - Maori 16.8% TBC 11.0%
% DNA rate for outpatient appointments - Pacific 25.3% TBC 16.0%
Elective day of surgery admission (DOSA) rate 41.6% TBC 39.1%
% Day Surgery Rate 35.4% TBC 42.9%
Inhouse Elective WIES through theatre - per day 39.26 TBC 31.18
Number of CBU outliers 43 0 50
% Very good and excellent ratings for overall patient experience for inpatients N/A ≥90% 96.9%
% Very good and excellent ratings for overall patient experience for outpatients N/A ≥90% 76.5%
Number of complaints received 2 0 3
28 Day Readmission Rate - Total N/A TBC 11.0%
Cardiac Bypass Surgery Waiting List 71 52-104 96
% Accepted referrals for elective angiography treated within 3 months 99.0% ≥90% 99.0%
% Adjusted theatre utilisation 82.2% ≥80% 92.6%
% Theatre cancellations 5.2% TBC 11.1%
Average Length of Stay for WIES funded discharges (days) - Acute 5.25 TBC 5.66
Average Length of Stay for WIES funded discharges (days) - Elective 3.12 TBC 3.24
Actual Prev Period
Incr
ease
d Pa
tient
Saf
ety
Bett
er Q
ualit
y Ca
re
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.10
127

Scorecard Commentary
Health Targets
Cardiac Surgery Bypass Waiting List At the end of October the waiting list totalled 71. There was 1 patient waiting over the 120 day target and 38 patients waiting up to 60 days. During the month there were 90 patients operated on against a plan of 82. There were 10 cancellations during the month of October which is a continued improvement on the previous month which saw 14 patients cancelled. During October the service has seen an increase in production and a decrease in the waitlist predominately due to an ability to get patients through both CVICU and the ward. The service completed 8 weekend contract cases and outsourced 1 patient to Waikato Hospital.
Increased Patient Safety
11 patients had falls which is a decrease from the previous month, none with significant harm.
There were 8 pressure injuries in October, 5 of these were Category/Stage I: Non-blanchable erythema and 3 were Category/Stage II: Partial thickness.
There was one SAC 2 event reported in October This was a fall and is following the usual examination process.
There were 22 medication errors, a decrease from last month; of these 8 were omissions, 3 delivery errors, 8 incorrect dose/order, 2 dose duplication and 1 damaged unusable medication.
% Hospitalised smokers offered advice and support to quit 98.9% ≥95% 98.6%
Vascular surgical waitlist - longest waiting patient (days) 121 <=150 134
Outpatient wait time for chest pain clinic patients (% compliant against 42 day target) 93.0% ≥70% 100.0%
CVD risk assessment 91.0% ≥95% 90.0%
Excess annual leave dollars ($M) $0.49 0 $0.48
% Staff with excess annual leave > 1 year 33.2% 0% 34.2%
% Staff with excess annual leave > 2 years 14.5% 0% 13.5%
% Staff with excess annual leave and insufficient plan to clear excess by the end of financial year 96.2% 0% 97.3%
% Pre-employment Screenings (PES) cleared before the start date 100.0% 100% 100.0%
Sick leave hours taken as a percentage of total hours worked 4.5% ≤3.4% 4.5%
% Voluntary turnover (annually) 6.2% ≤10% 6.8%
% Voluntary turnover <1 year tenure 9.7% ≤6% 8.8%
N/A =
28 Day Readmission Rate - TotalA 35 day period is required to accurately report all acute re-admissions for the previous month's discharges. (35 days = 28 days post discharge as per MoH measures plus 5 working days to allow for coding).
Result not available, too soon to report
Number of healthcare-associated bloodstream infections, Number of healthcare-associated Staphylococcus aureus bacteraemiaResults are based on a manual process and complete test results not being available for the previous month.
% Very good and excellent ratings for overall patient experience for inpatients
These measures are based on retrospective survey data, i .e. completed responses for patients discharged or treated the previous month.% Very good and excellent ratings for overall patient experience for outpatients
Enga
ged
Wor
kfor
ceIm
prov
ed H
ealth
St
atus
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
128

There were 2 complaints in October, 1 has been closed and 1 remains open and is being reviewed.
Better Quality Care
The Cardiovascular Service is maintaining the 4 month target in both ESPI2 and ESPI 5 in Cardiology and Vascular services. The service continues to monitor and validate the cardiac waitlist weekly and reviews all patients waiting longer than 90 days. We have commenced a Cardiac surgery patient experience project reviewing both patient experience and the impact of having surgery cancelled while on the waiting list. Focus areas have been identified and includes contact points for patients on waiting list, impact of cancellation on patients, letters and information provided to patients while waiting for surgery.
Clinicians have now finalised options and requirements for the imaging equipment in room 2 of the Cardiology Investigation Unit. We are proceeding to final quote and will then order the equipment. Installation is expected to begin in March 2015. Due to similar projects due to commence at Starship Children’s Hospital and CMDHB, communication has begun to ensure all 3 facilities are not out of commission concurrently.
Targets for interventional work continue to be met with 89% of ADHB-domicile patients with acute coronary syndrome undergoing coronary angiography within 3 days (target is >=70%).
Improved Health Status
The Cardiovascular Directorate achieved 98.9% for smoking cessation in October.
Engaged Workforce
Management of excess annual leave remains challenging despite manager’s actively managing leave within the constraints of maintaining service delivery. We have seen leave plans being submitted for the January and February period for 2015 and the service has been working with Clinical Directors and RC managers to maintain focus on addressing high leave balances.
Strategic Initiatives Deliverable / Action Status
• Bypass intervention rates 6.5 per 10,000 population Lack of demand
• Angiogram discharges rates 34.73 per 10,0000 (98.2% of target YTD)
On Track √ √
• PCI (angioplasty) + Cardiac Surgery rates 18.90 per 10,000 (99% of target year to date)
On Track √
• 100% patients receive elective angiogram < 90 days On Track √ √ √
• Primary angioplasty “Door to balloon time” On Track √ √ √ √
• Acute coronary syndrome diagnostic angiogram > 70% On Track √ √ √
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.10
129

Key achievements in the month
• Cardiac surgery cancellations continue to decrease each month • Improved production for the month of October • 1 patient was outsourced to Waikato District Health Board, the service no longer requires
this outsourcing • MOH weekly teleconference ceased • Patient experience on waiting list project has been meeting fortnightly. • Plans to return to full production on 12th January 2015, 1 week earlier than previous years
to enable sustained production during Christmas/New year period
Areas off track and remedial plans
• Identification of full savings initiative target for 14/15 – work underway • Hybrid OR build behind schedule, but building work has commenced. • CIU imaging equipment installation later than anticipated; scheduled for March 2015.
Key issues / initiatives identified in coming months Continued focus on achieving the 4 month target across the Cardiovascular Directorate by December.
Careful management of the cardiac waitlist as we move towards Christmas which historically has seen an increase in inflow of patients added to the waiting list.
Continuing to manage financial performance, in particular the financial implications of the hybrid operating theatre build.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
130

Financial Results
Comments on Major Financial Variances The YTD result is $162k U
Revenue YTD is $59k F. Revenue from other DHBs is $100k U YTD mainly due to Cardiology, which is below budget YTD in Northland $53k U, Waitemata $25kU ,Hawkes Bay $14k U and Counties $5k U. Non Resident income YTD is $177k F offset by ACC YTD which is $65k U mainly in Cardiology.
Total Expenditure YTD is $247k U. Mainly due to: • Outsourcing Clinical $142k F, all work was done in house in July and August. • Personnel and Outsourced Personnel are net $127k F. Outsourced personnel are $102k F
YTD including a $72k favourable prior year adjustment. • Clinical Supplies $278k U. Overall Clinical Supplies was higher than budgeted, mainly
because CTSU Blood usage was $172k U. YTD October 4 patients have consumed $252k of blood.
• Infrastructure and non-clinical supplies are $238k U reflecting an increase in doubtful debts.
STATEMENT OF FINANCIAL PERFORMANCECardiac Services Reporting Date Oct-14
($000s) MONTH YEAR TO DATEActual Budget Variance Actual Budget Variance
REVENUEGovernment and Crown Agency 108 87 21 F 329 347 18 U
Funder to Provider Revenue 10,484 10,484 0 F 42,886 42,886 0 F
Other Income 687 558 129 F 2,309 2,232 78 F
Total Revenue 11,279 11,129 151 F 45,525 45,465 59 F
EXPENDITUREPersonnel Personnel Costs 5,133 5,139 6 F 20,348 20,373 25 F
Outsourced Personnel 45 52 7 F 105 208 102 F
Outsourced Clinical Services 142 141 1 U 422 564 142 F
Clinical Supplies 2,547 2,477 70 U 10,212 9,934 278 U
Infrastructure & Non-Clinical Supplies 253 133 120 U 770 532 238 U
Total Expenditure 8,120 7,941 178 U 31,857 31,611 247 U
Contribution 3,160 3,187 28 U 13,667 13,855 187 U
Allocations 925 984 59 F 3,978 4,002 25 F
NET RESULT 2,234 2,203 31 F 9,690 9,852 162 U
Paid FTEMONTH (FTE) YEAR TO DATE ( FTE)
Actual Budget Variance Actual Budget Variance Medical 88.4 88.4 0.0 U 89.1 88.4 0.8 U
Nursing 313.5 305.2 8.3 U 310.8 305.2 5.7 U
Allied Health 65.3 66.5 1.2 F 65.0 66.5 1.5 F
Support 3.0 3.0 0.0 F 3.0 3.0 0.0 F
Management/Administration 30.2 30.1 0.1 U 31.6 30.1 1.5 U
Total excluding outsourced FTEs 500.5 493.1 7.3 U 499.5 493.1 6.4 U Total Outsourced Services 2.4 1.7 0.6 U 1.5 1.7 0.2 F
Total including outsourced FTEs 502.8 494.9 8.0 U 501.0 494.8 6.2 U
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.10
131

FTE Employed/Contracted – YTD Var 6.2 FTE U The base budget includes reductions in FTE on the assumption that vacancies will occur as they have in the past. YTD Medical, Nursing and Allied Health were reduced by 3.0, 6.8 and 2.5 FTE respectively, a total of 12.3 FTE.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
132

Adult Medical Directorate
Speaker: Barry Snow
Service Overview The Adult Medical Service is responsible for the provision of emergency care, medical services and sub specialties for the adult population. The leadership within this directorate consists of Barry Snow, Director, Brenda Clune, Nurse Director, Carolyn Simmons Carlsson, Allied Health Director and Kelly Teague, General Manager.
The services in the Adult Medical Directorate are structured into 2 portfolios:
Group 1 General Medicine, Infectious Diseases, Neurology, Renal, Respiratory and Gastroenterology
Group 2 Adult Emergency, APU, Critical Care, Air Ambulance
Scorecard
Adult Medical ServicesOct-14 Measure Target
Number of healthcare-associated bloodstream infections N/A TBC 2
Number of healthcare-associated Staphylococcus aureus bacteraemia N/A TBC 0
Nosocomial pressure injury point prevalence (% of in-patients) 9.8% 0% 9.8%
Medication Errors 18 0 25
Falls with major harm per 1,000 bed days 0.16 TBC 0.16
Number of reported adverse events causing harm (SAC 1&2) 1 0 3
(MOH-01) % AED patients with ED stay < 6 hours 92.3% ≥95% 91.8%
(ESPI-1) % Services acknowledging 90% of FSA referrals 100.0% 100% 100.0%
(ESPI-2) Patients waiting longer than 5 months for their FSA 0.00% 0% 0.00%
% DNA rate for outpatient appointments - All Ethnicities 9.0% ≤9% 11.0%
% DNA rate for outpatient appointments - Maori 19.9% ≤9% 20.0%
% DNA rate for outpatient appointments - Pacific 15.3% ≤9% 19.0%
Number of CBU outliers 144 0 152
% Patients cared for in a mixed gender room at midday - Adult 18.0% TBC 22.0%
% Very good and excellent ratings for overall patient experience for inpatients N/A ≥90% 76.9%
% Very good and excellent ratings for overall patient experience for outpatients N/A ≥90% N/A
Number of complaints received 13 0 11
28 Day Readmission Rate - Total N/A ≤10% 12.8%
% Urgent Diagnostic colonoscopy procedures treated < 14 days 100.0% ≥75% 77.0%
% Non urgent colonoscopy procedures treated < 42 days 99.0% ≥60% 77.0%
% Surveillance Colonoscopies Treated 98.0% ≥60% 88.0%
Average Length of Stay for WIES funded discharges (days) - Acute 3.69 TBC 3.62
Actual Prev Period
Incr
ease
d Pa
tient
Saf
ety
Bett
er Q
ualit
y Ca
re
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.11
133

Scorecard Commentary
Health Targets
Acute Flow Adult acute flow performance for October 2014 was at 92.3% which demonstrates a very slight increase in performance compared to September 2014 at 91.8% of which both figures are below the Ministry of Health Target at 95%. A 5% increase in presentations over the last 12 months has made it increasingly difficult to maintain the target with no additional investment into the service. An additional 5.4 nursing staff and 4 additional medical staff have been approved in the 2014/15 budget.
Escalation plans have been put into place and Directors and General Managers are contacted early each morning by the Flow Manager if patients are waiting in ED/APU in order to ensure appropriate action in a timely manner. This includes enhanced discharging and freeing up specific resources such as side rooms.
We expect to return to 95% compliance as the residual effects of the winter load and influenza resolve.
Further investment is required alongside improvement initiatives in order to meet the target due to the increased volume of presentations. This is being considered by the ADHB Executive Team.
Smoking Cessation Performance for October 2014 was 95.2%.
% Hospitalised smokers offered advice and support to quit 95.2% ≥95% 94.7%
Excess annual leave dollars ($M) $0.59 0 $0.60
% Staff with excess annual leave > 1 year 39.4% 0% 36.4%
% Staff with excess annual leave > 2 years 14.5% 0% 15.8%
% Staff with excess annual leave and insufficient plan to clear excess by the end of financial year 84.1% 0% 90.0%
% Staff with leave planned for the current 12 months 13.3% 100% 7.0%
% Leave taken to date for the current 12 months 53.3% 100% 55.0%
% Pre-employment Screenings (PES) cleared before the start date 62.5% 100% 78.6%
Sick leave hours taken as a percentage of total hours worked 3.7% ≤3.4% 3.7%
% Voluntary turnover (annually) 5.6% ≤10% 5.5%
% Voluntary turnover <1 year tenure 7.0% ≤6% 4.8%
Amber =
N/A =
These measures are based on retrospective survey data, i .e. completed responses for patients discharged or treated the previous month.
28 Day Readmission Rate - TotalA 35 day period is required to accurately report all acute re-admissions for the previous month's discharges. (35 days = 28 days post discharge as per MoH measures plus 5 working days to allow for coding).
Variance from target not significant enough to report as non-compliant. This includes percentages/rates within 1% of target, or volumes within 1 value from target.
Result not available, too soon to report
Number of healthcare-associated bloodstream infections, Number of healthcare-associated Staphylococcus aureus bacteraemiaResults are based on a manual process and complete test results not being available for the previous month.
% Very good and excellent ratings for overall patient experience for inpatients% Very good and excellent ratings for overall patient experience for outpatients
Enga
ged
Wor
kfor
ceIm
prov
ed
Heal
th
Stat
us
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
134

Increased Patient Safety
There were 18 medication errors in October 2014 compared to 23 in September 2014 relating to omissions and data collection. Service level focus and education continues.
Throughout October 2014 there have been 4 grade 1 pressure injuries. Focus continues on assessment and monitoring in all clinical areas.
There was one fall with harm which was an un-witnessed fall in a bathroom. This incident is currently being investigated.
The graphs below demonstrate a slight increase in complaints, 13 in October 2014 compared to 11 in September 2014. The increase predominately relates to the Accident and Emergency Department and the increase in volumes. The themes largely relate to the attitude (actions plans are in place to address these areas of concern) of staff and cost of treatment.
Number of Complaints, July – October 2014:
Number of Complaints by Speciality, July – October 2014:
0
5
10
15
20
25
Jul-14 Aug-14 Sep-14 Oct-14
23
9 11
13
No
of C
ompl
aint
s
Month
No of Complaints
0123456789
1
9
5
2 1
2 3
0 0
3 2
0 0 0
4
0 0
8
1 0 0 0
2
0 0
6
2 1
0 1
2 1
Jul-14
Aug-14
Sep-14
Oct-14
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.11
135

Better Quality Care
ESPI-2 compliance Is compliant with 0% of patients waiting greater than 3 months.
DNA rates There has been an improvement in DNA rates for all ethnicities within the directorate, 9% for October 2014 compared to 11% in September 2014. There is a slight improvement in the Maori and Pacific DNA rates.
As part of the outpatient redesign project, a plan has been developed to roll out a partial booking service across the organisation (to provide patients with a choice of appointments which is convenient for them). The services with the highest DNA rates will be targeted in the first instance. In relation to the Adult Medical Directorate, a partial booking system has now been implemented in Gastroenterology with a view to roll out in Respiratory in January 2015. Patient feedback has been extremely positive as they now receive a choice of date and time of appointment.
Improved Health Status
Capacity and demand modelling has been undertaken to ensure the correct number of training lists for our Gastroenterology and Colorectal Surgical trainees are delivered within the college guidelines. In addition, there is now an established training programme for Nurse Endoscopists but we are not in a position to commence training due to the capacity restrictions. A paper describing the issues and potential solutions will be presented to the Executive Team on the 25th November 2014.
Regional work is also being undertaken to determine the type of capacity required to deliver the increased colonoscopy volumes over the next 5 years.
Engaged Workforce
Excess annual leave plans have slightly improved but this is a result of the wards, Admission & Planning Unit and the Emergency Department not having the flexibility to enable staff to take their planned leave. Plans are in place to continue to address excess leave balances across the directorate.
In addition, plans are in place to ensure that staff take this year’s leave allocation within the 12 month period and 53.3% has been achieved to date.
Key Challenges Key challenges for the directorate over the next two months are outlined below:
Challenges Deadline
Re-design the Directorate structure 31st January 2015
Continue close watch on bed demand and maintain bed closure disciplines where possible
Monthly
Capacity and demand modelling to ensure that training lists are delivered for Gastroenterology and Colorectal Surgical trainees
31st December 2014
Continue to deliver on acute flow performance Monthly
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
136

Review models of care for patient attenders. A project has commenced to assess the criteria and utilisation and observation units to determine the most appropriate utilisation of patient attenders
1st December 2014
Roll out of e-referrals for our services. Neurology, General Medicine, Infectious Diseases are all now using e-referrals
31st December 2014
Strategic Initiatives
Deliverable / Action Status/Deadline Develop a 5 year strategy for the directorate Draft complete √ √ √ √
Scoping exercise for the re-design for the Emergency Department
28th February 2015 √ √ √ √
Write a business case for the development/expansion of the renal dialysis services at Green Lane
31st December 2014 √ √ √
Continue work with the Ngati Whatua O Orakei Health Board to develop a business case for a community dialysis unit
31st January 2015 √ √ √ √
Implement a partial booking system Deadline for all services within our Directorate is 28th
February 2015
√ √
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.11
137

Financial Results
STATEMENT OF FINANCIAL PERFORMANCEAdult Medical Services Reporting Date Oct-14
($000s) MONTH YEAR TO DATEActual Budget Variance Actual Budget Variance
REVENUEGovernment and Crown Agency 261 286 25 U 1,032 1,144 112 UFunder to Provider Revenue 12,498 12,498 0 F 50,961 50,961 0 FOther Income 350 378 27 U 1,239 1,510 271 U
Total Revenue 13,109 13,161 53 U 53,232 53,615 384 U
EXPENDITUREPersonnel Personnel Costs 7,634 7,454 180 U 30,127 29,545 582 U
Outsourced Personnel 170 103 67 U 404 412 8 FOutsourced Clinical Services 27 26 1 U 144 102 42 UClinical Supplies 1,748 1,685 63 U 7,145 6,742 404 UInfrastructure & Non-Clinical Supplies 186 182 5 U 733 726 7 U
Total Expenditure 9,765 9,449 316 U 38,554 37,528 1,027 U
Contribution 3,344 3,712 369 U 14,678 16,088 1,410 U
Allocations 1,855 1,752 102 U 7,180 7,120 59 U
NET RESULT 1,489 1,960 471 U 7,498 8,967 1,469 U
Paid FTEMONTH (FTE) YEAR TO DATE ( FTE)
Actual Budget Variance Actual Budget Variance Medical 183.3 183.7 0.3 F 181.4 183.6 2.2 F Nursing 521.4 499.1 22.3 U 516.3 501.7 14.7 U All ied Health 47.4 51.7 4.3 F 47.2 51.7 4.5 F Support 6.0 6.0 0.0 F 6.1 6.0 0.1 U Management/Administration 51.8 54.2 2.4 F 51.4 54.2 2.8 FTotal excluding outsourced FTEs 809.9 794.6 15.3 U 802.3 797.1 5.3 U Total :Outsourced Services 5.2 4.2 1.0 U 3.5 4.2 0.7 F
Total including outsourced FTEs 815.1 798.9 16.3 U 805.9 801.3 4.6 U
YTD ResultThe result for YTD October is a surplus of $7,498k against a budgeted surplus of $8,967k, an unfavourable variance of $1,469k.
Total Revenue - $384k unfavourable mainly due to the timing of Non Residents income $193k U and IDF revenue from WDHB for Renal $56k U.
Total Expenditure - $1,086 k unfavourable due to : - Personnel Costs including outsourced personnel- $ 574k U - This is mainly due to unfavourable variances in Medical costs $153k U and Nursing costs $642k U offset by Allied Health $103 F and Admin $116k F.The Medical employee cost variance of $153k U is primarily driven by Gen Med Registrars $219k U due to unbudgeted Relievers (full year impact estimated to be $500k unfav - mitigation strategies are being worked up to offset this impact). The Nursing unfavourable variance of $ 642k U is spread across most of the services mainly DCCM $110k U, APU $141k U (offset by ED $167k F), Adult Medical Management $121k U,Gen Med $170k U and Gastro $110k U. This was due to DCCM (an increase in ICU patient numbers and call back) , APU ( high attendances), Adult Medical Management- Bureau staff to cover Ward 31 and Ward 62 for all patients across the organisation and Gastro due to additional colonoscopy lists.
- Clinical Supplies Clinical supplies $404k U primarily due to DCCM $310k U (volume driven), Gastro $204k U (high administration of Infl iximab drugs), Neurology $32k U, IVIG and Adult Medical Management (timing of hA procurement savings $46k U ).
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
138

Financial pressures
Savings Plan Demonstrated below is the directorates savings plan vs actual monthly performance.
Full Year YTD
Description
Annual Budget
$k
Annual Forecast
$k
Budget Shortfall
$kBudget
$kActual
$kVariance
$k
IVIG 1,036 1,245 -209 383 418 -35
Infliximab 935 1,230 -295 312 410 -98
0.25 FTE for Nurse Advisor 0 25 -25 0 8 -8
X3 endoscopy nurses 0 230 -230 0 77 -77
Cadaver transplants -65 0 -65 -22 0 -22
Ward 62 0 37 -37 0 37 -37
Ward 31 79 79 0 13 29 -16
Gen Med registrar relievers 3,206 3,706 -500 1,069 1,235 -167
WDHB Haemodialysis Revenue -160 0 -160 -53 0 -53
Fingolimod and Natalizumab 0 TBA 0 0 0 0
5,031 6,552 -1,522 1,702 2,214 -513
84147
231294
0 0 0 0 0 0 0 0$70 $140
$211 $275
$332 $389
$445 $501
$555 $608
$658 $706
$-
$200
$400
$600
$800
41821 41852 41883 41913 41944 41974 42005 42036 42064 42095 42125 42156
Financial Savings vs TargetOctober 2014
Actuals
Planned
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
8.11
139

Reduction in follow ups Demonstrated below is a reduction in follow ups for neurology as this speciality had over performing in 2013/14.
Neurology – Actual vs Contracted Volume, July – October 2014:
0123456789
1
9
5
2 1
2 3
0 0
3 2
0 0 0
4
0 0
8
1 0 0 0
2
0 0
6
2 1
0 1
2 1
Jul-14
Aug-14
Sep-14
Oct-14
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
140

Management of Slow Moving and Due-to-Expire Inventory and Stock
Recommendation That the Committee:
1. Receives the report. 2. Notes the update on Slow Moving Inventory and Pandemic stock at the DHB 3. Notes for information purposes
Prepared by: Matt Riesterer (Improvement Specialist) Endorsed by: Jane Woolford (Operations Manager, Procurement and Supply Chain), and
Clare Thompson (General Manager, Commercial Services and Non Clinical Support Services)
Purpose This report provides an update to the report submitted in July 14 regarding the status of slow moving inventory and Pandemic stock for the ADHB as well as a brief overview of the current situation both regionally and nationally.
Slow Moving Inventory At the end of FY14/15 a provision of $1.027m was carried forward for the potential write-off of inventory identified either with no purchase history, and or no usage.
Items identified with the above criteria have now been verified by clinicians; • $357k identified as still able to be used • $423k identified as obsolete requiring write –off • $247k is still under review
Key actions include; • healthAlliance and DHB staff are reviewing stock levels for slow moving products which are
still active to ensure appropriate inventory volumes are maintained. • Items identified as obsolete will be written-off, and healthAlliance will endeavour to on-sell
these items where possible. • A process to reduce risk of expiring product has been implemented. However, further work
remains to proactively manage slow moving inventory. • ADHB and healthAlliance team members will continue to investigate the root causes of slow
moving stock, and implement learnings from other DHBs.
Management of Slow moving inventory at other DHBs Waitemata and Counties-Manukau DHBs currently expense stock at point of order. Notification of slow moving products is provided manually by the clinicians. A healthAlliance initiative now includes implementing an inventory model at these DHBs to align with Auckland DHB practices. This is referred to as the Extended Inventory Project.
Other DHBs outside the Auckland metro region have various inventory systems in place and generate reports that provide information relating to slow moving products. These products are either relocated to areas where the product will be consumed more quickly, or ultimately written off against the service. Other DHBs have retained their own staff to manage the inventory function and
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
9.1
141

indications are that our write-offs are higher than other DHBs outside the region. This is being addressed with healthAlliance.
Pandemic Stock N95 Masks During September the ADHB were advised of a potential supply issue with N95 masks due to unusually high national demand. The ADHB Infection Control team arranged for the N95 masks held as part of the Pandemic supply, to be tested by Airlab to determine their suitability. Based on the results, it was determined that these masks could be used if required. Meanwhile the supplier had sourced additional inventory which prevented any out-of-stocks.
Pandemic stock review The Pandemic stock schedule currently has 29 items totalling $721k (see Appendix 1). Five items totalling $605k (shaded yellow) can be used but the balance totalling $116k will be written off.
The stock is currently 7 to 8 years old and while it can be used, it is in excess of demand and whilst some of these items are fit for purpose, this will diminish over time.
The pandemic inventory is locally owned but held regionally. Therefore Waitemata and Counties Manukau DHBs are also in a similar situation and have limited ability to use stock before it expires.
The volume of Pandemic stock held throughout the remainder of the country is significantly less and this has enabled those DHBs to rotate Pandemic stock with regular business-as-usual activity.
The ADHB is seeking an opinion from the Ministry of Health on a list of Pandemic stock to be held regionally and locally. A decision will be made then on any stock that remains excess to requirements.
Any stock excess to ADHB’s requirements and still fit for purpose could be donated to Medical Aid Abroad. The remainder would be disposed of.
Discussions have commenced to review holding pandemic stock regionally to reduce the risk of obsolescence and expired stock.
Planned Actions to Address Slow Moving and Pandemic Stock
Action Timeframe
ADHB and healthAlliance Supply Chain teams to implement a process that identifies and address slow moving inventory
March ‘15
Pandemic stocks confirmed as excess to requirements is written off Stock levels are reset taking into account regional requirement.
March ‘15
Develop and implement a regional solution for Pandemic stock which addresses storage locations, rotation and replenishment
March ‘15
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
142

Appendix 1 – ADHB Pandemic Stock Holding Item VPN Description UOM Cost SOH Value Months Cover
M107452 ADM203 CANNULA LEVER LOCK INTERLINK B.D.303370 EA $0.43 2,326 $1,000.18
M50966 ADM042 CATHETER IV 24G X 3/4 INCH INSYTE 381212 BD EA $1.02 538 $548.76
M12224 SYR135 SYRINGE HYPO DISP 50ML NO NEEDLE LUER LOCK CONCENTRIC BD EA $0.69 0 $0.00
M12226 SYR134 SYRINGE HYPO DISP 5ML NO NEEDLE LUER LOCK BD EA $0.08 5,000 $400.00
M107456 MEA861 GOWN ISOLATION 40GSM YELLOW EA $0.94 66,950 $63,093.68 310
M56925 AIB573 NEEDLE HYPO DISP 24G 1 INCH LEUR LOCK EA $0.04 80,100 $3,040.44
M12215 SYRINGE HYPO DISP 10ML NO NEEDLE LUER LOCK BD EA $0.11 21,429 $2,357.19
M41302 MEC538 GLOVE EXAM DERMAGRIP LATEX POWDER FREE LARGE BX100 1666 BOX $5.77 50 $288.50
M54957 GEN1128 HAND GEL ANTIMICROBIAL MICROSHIELD 500ML EA $10.41 0 $0.00
M107454 MASK FACE FLUIDSHEILD TECNOL ADHB ONLY BOX $31.26 8,094 $253,018.44 76
M11788 ADM047 CATHETER IV 18G X 1 1/4 INCH BD INSYTE EA $1.02 538 $548.76
M107453 ADM206 CANNULA THREADED LOCK INTERLINK EA $0.43 1,163 $500.09
M40598 ADM411 CANNULA PLASTIC BLUNT 303345 PK100 INTERLINK EA $0.21 11,800 $2,478.00
M107460 GEN432 EXAM GLOVE L LATEX PF DERMAGRIP BOX $5.24 3,739 $19,592.36
M41301 MEC537 GLOVE EXAM DERMAGRIP LATEX POWDER FREE MEDIUM BX100 1665 BOX $5.77 15 $86.55
H10256 MEC161 PAPER TISSUE FACIAL 2 PLY PK100 PREMIUM TORK PKT $0.77 1,000 $770.00
M107450 MASK N95 PARTICULATE RESPIRATOR REGULAR SURGICAL BOX $19.89 7,503 $149,271.35 151
M54511 AHB1324 SODIUM CHLORIDE 0.9PC 1000ML EA $1.80 4,068 $7,322.40
M41300 MEC536 GLOVE EXAM DERMAGRIP LATEX POWDER FREE SMALL BX100 1664 BOX $5.77 50 $288.50
M70478 SYRINGE LUER LOCK 20CC TERUMO 3SS-20LA EA $0.19 3,077 $584.63
M56566 ADM361 ADMIN SET IV BURETROL 2 INJ SITE 2.1M CA48 INTERLINK EA $15.78 259 $4,087.02
M107459 GEN431 EXAM GLOVE M LATEX P/FREE DERMAGRIP BOX $5.24 6,339 $33,216.36
M107458 GEN430 EXAM GLOVE SMALL LATEX P/FREE NON-STERILE DERMAGRIP BOX $5.24 6,178 $32,372.72
M107451 RFD029 SOLUTION IV GLUCOSE 4% 0.18% SALINE 1000ML EA $0.00 0 $0.00
M107457 ADM199 IV SET INTERLINK W/SIDE ARM LUER LOCK FNC1112 EA $2.04 2,696 $5,499.84
M11786 ADM040 CATHETER IV 16G X 1 1/4 INCH BD INSYTE EA $1.02 538 $548.76
M58356 MEA860 GLASSES SAFE VIEW EYE PROTECTION ASSEMBLED PK10 EA $3.09 32,910 $101,586.81 4,897
M57307 MEA899 MASK RESPIRATOR/TB SUB-MICRON BX20 N95 SMALL 3M 1860S BOX $45.44 828 $37,624.32 24
M107455 SYRINGE HYPO 50ML LUER LOCK EA $0.61 658 $401.38
Items shaded in yellow are potentially able to be used (subject to testing). Months cover is based on current usage. $720,527.04
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
9.1
143


National Services Update
Recommendation That the Committee:
1. Receives the report. 2. Notes the current progress and status of the work programme for National Services
provided by Auckland District Health Board with the National Health Board.
Prepared by: Fionnagh Dougan (Director Provider Services), and Jo Brown (Hospitals Funding and Development Manager)
Glossary CLT Clinical Leadership Team DNA Did Not Attend GHSNZ Genetic Health Service New Zealand NHB National Health Board PBFF Population Based Funding Formula
Executive Summary This report provides an update to the Committee regarding the current progress and status of the work programme to address issues relating to, or development and funding of, National Services provided by Auckland District Health Board (ADHB) with the National Health Board (NHB).
The document outlines the work plan agreed with the NHB for National Services provided by ADHB over the 2014/15 year.
Background National Services are services that are planned and/or funded nationally, and provided through a lead DHB. The lead DHB plans, coordinates, and delivers the National Service for the populations of all or most DHBs. Lead DHBs for National Services have the same obligations to their external and local DHB populations.
ADHB provides a number of National Services for the New Zealand population, through contracts with the NHB on behalf of all DHBs nationally. The ADHB Provider Services team and the Funding team have been working with the NHB to prioritise a work plan to manage the portfolio of National Services provided by ADHB and ensure funding is secured where appropriate.
These services are:
• heart transplants • heart–lung transplants • lung transplants • donor coordination and retrieval • liver transplants • paediatric cardiac and adult congenital heart defect service • paediatric and adult metabolic services
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
9.2
144

Services nationally provided by two or more lead DHBs on behalf of all other DHBs (including ADHB):
• clinical genetic services • paediatric and perinatal pathology • major trauma
Services for which ADHB receives supplementary funding:
• paediatric rheumatology
Progress Regular face-to-face meetings and teleconferences take place with NHB National Services personnel to achieve the work plan below. Our clinicians are an integral part of the process.
National Services Service Definition Activity Update Progress/ADHB comments
National Paediatric & Adult Metabolic Services
Provide national consultation and advisory service, plan treatment and oversight for patients with (often rare) metabolic disease. 24/7 on call service.
Proposal submitted for other funders for additional funding for Additional clinician resource for 2015/16 – final feedback awaited
Growing demand for services, especially adult (due to new technologies and improved life expectancy and outcomes). Need for additional SMO resource with Adult focus/expertise. Succession planning. Need to identify associated costs that are additional to WIES price.
National Paediatric & Perinatal Pathology (ADHB, CCDHB, CDHB & SDHB)
Urgent routine and specialised paediatric and perinatal medical laboratory services for inpatients, outpatients and day patients.
Further discussion with NHB regarding resources and reporting. Ministry of Justice Review completed – feedback from NHB awaited
Original process included setting up formal MOU arrangements with other three DHBs and SDHB – this remains outstanding and needs to be finalised. Cost pressures for pathologist and mortuary technician salaries – need to be factored in as cost increase for 2014/15. No formal reporting at present as never confirmed/finalised with MOH/NHB.
National Renal Transplantation Service
Solid Organ Transplant Service (Renal) Hospital Service to treat patients undergoing a transplant procedure. Includes:
• all transplant procurement process nationally
• coordinators for transplants • retrievals • on-call clinicians
Additional funding confirmed for three years from 2014/15
National priority recognised. Funding for 2014/15 confirmed for 10 live donor additional transplants. Funding confirmed for Paired Kidney Exchange Coordinator role 2014-2017. Funding confirmed 2014-2017 for 11 Additional Donor Liaison Coordinators nationally to support increase in Donor numbers. Capacity planning for 2015/2016 inclusive of revised assumptions
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
145

Organ Donation NZ Service Organ Coordination Education and Information Service Clinical director, donor coordinators, and other staff as required.
National Intestinal Failure Service
National coordination service for Intestinal Failure.
Contract signed and Implementation Plan developed.
Funding and contract arrangements confirmed for 2014/15 – 2016/17.
Paediatric Cardiac and Adult Congenital Service
Paediatric Cardiac Service National service for infants and children with congenital and acquired heart disease. Also provides a foetal cardiology service and the investigation and treatment of those people born with congenital heart disease who are now adults. 24/7 cardiac surgical service and 24/7 cardiology medical team cover for inpatient ward. Adult Congenital Service Outpatient and Network of Outreach clinics. Transition clinic for patients transferring from paediatric to the adult service. Educational resources for patients and families. Services include: Single national hub DHB-based with a tertiary inpatient service, multidisciplinary day stay and OP facilities. This includes provision of cardiology investigation; cardiac surgery and its ancillary components; paediatric and cardiac intensive care; neonatal intensive care; child and adult cardiac inpatient beds. Spoke level outreach clinics with face to face and virtual/distant consultations, professional relationships using clinical networks in the two areas of paediatric cardiac and adult congenital cardiac services.
Proposal submitted NHB for other funders for additional funding for 2015/16. This includes pricing issues and capacity pressures, and is required to sustain the national service and reduce the rate of cancellation.
Implementation planning underway. Overarching demand and capacity pressures mean frequent cancellations. Pricing of our services to Pacific nations purchasers is impacting flow and overarching sustainability.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
9.2
146

Genetic Health New Zealand Service (CCDHB, CDHB & ADHB)
National service includes:
• Advice • Education • Inpatient consults • Outpatient clinics • Outreach clinics
Additional funding agreed for 2014/15 and 2015/16 in principle to address waiting list backlog. Northern Hub (ADHB) Project Plan developed and approved for implementation. Targets and outcomes to be agreed.
Development of plans for addressing waiting list backlog. NHB Project underway to review service model to ensure clinical and financial sustainability going forward.
Paediatric Rheumatology (HVDHB & ADHB)
Service includes specialist diagnosis and care, information, education services in a range of clinical settings, including outreach clinics, to meet the needs of children and young people with rheumatologic disease.
Proposal submitted for other funders for additional funding for 2015/16 – final feedback awaited.
Resource pressures can be due to vulnerable service – limited SMO capacity.
Major Trauma Contracts for Clinical Lead and Clinical Network, and development/implementation of the Major Trauma Registry.
Funding for 15/16 and activities to be confirmed
Increased clarity and visibility of service in progress
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
147

ADHB and WDHB Contact Centre Collaboration Update
Recommendation That the Committee:
1. Receives the report. 2. Notes the on-going project work and operational management of both Contact Centres
under a single joined-up management structure and technology solution. 3. Notes the commitment to the implementation of a continuous improvement framework
across the joint Contact Centre (ADHB/WDHB) to enable the realisation of identified benefits to both DHBs and to the populations served.
Prepared by: Frank Tracey (General Manager, Acting Director Clinical Support Services) Endorsed by: Fionnagh Dougan (Director Provider Services)
Glossary ADHB Auckland District Health Board WDHB Waitemata District Health Board CRO Central Referrals Office DR Disaster Recovery hA health Alliance KPI Key Performance Indicator MOS Management Operating System PAS Patient Administration System PSC Patient Services Centre RFP Request for Proposal
Executive Summary This report provides a progress update on the joint Contact Centre project which is part of the collaboration between Auckland and Waitemata DHB. The joint initiative came into effect on October 1st 2014. A change management process has been put in place to amalgamate the functions of both contact centres.
Current call volume per DHB:
DHB Call volume
ADHB Approximately 120,000 calls per month (includes appointment confirmation)
WDHB Approximately 70 – 80,000 calls per month (does not include appointment confirmation)
The Clinical Support Service Directorate of ADHB assumed management responsibility for the joint Contact Centre from Non-clinical Support on 1st of October 2014. The change in management reporting is designed to enable better alignment and integration of Contact Centre activities with a range of other administrative and service support functions at both DHBs. At ADHB, this includes the Central Referrals Office, Patient Administration Service which fall under the service cluster of the ‘Patient Services Centre’.
A targeted performance improvement process has been initiated in ADHB to improve Contact Centre performance. As part of this performance improvement process a set of benchmarks and associated
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
9.3
148

key performance indicators (KPIs) for the service and individual staff have been established. Initial research into comparable health systems regionally, nationally and internationally resulted in a requirement for ‘80% - first time response and resolution to a call’ being set as a performance indicator. Reporting against this and other indicators at ADHB demonstrates incremental improvement in service delivery (responsiveness) since implementation.
A similar approach is being considered for implementation at WDHB as a means of aligning performance expectations and deliverables for the joint entity.
Regular progress reports regarding the joint Contact Centre collaboration will be provided through the monthly Hospital Advisory Committee (HAC) report.
Background In July 2013 Auckland and Waitemata DHBs commenced a project to propose a joint contact centre to serve both DHBs from a single location within the Greenlane Clinical Centre. The rationale being there were various service issues and risks identified on both DHB sites.
A joint contact centre approach was deemed the best model by which to improve customer service levels for both DHB contact centres and to address issue related to business continuity planning, lack of quality framework, poor performance reporting and technology limitations.
Following consultation with staff and stakeholders and a detailed investigation and assessment of options, a business case was prepared recommending the best option as a standardised decentralised contact centre with a single management structure supported by a new software solution and would continue to operate from its two current contact centres sites.
This option best addressed the concerns about staff relocation, limitations of current technology systems, business continuity and disaster recovery, emergency management and 777 call handling, and management of other non-core contact centre duties.
A standardised decentralised Contact Centre has the following features:
• A virtual combined ADHB-WDHB Contact Centre located on the two DHB sites, but providing a synchronised, seamless service by staff who work in one DHB but may respond to calls from either DHB
• One contact centre technology solution, including call recording and reporting, automated call distributor and quality programme creating consistency across all contact points
• A Disaster Recovery (DR) site as back-up in the event that one of the Contact Centre sites is unavailable due to loss of power, telephones, data network or facilities.
• One quality framework and training approach focused on improvement of customer experience and up-skilling of the staff for excellence in service and career development
• A clear continuous improvement framework to action year-on-year volume reduction activities
• Option to centralise to a single site or multiple sites should business needs or environment change in the future.
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
149

Project Update The following table provides a summary of key activities undertaken as part of the joint Contact Centre initiative.
Milestone Progress Completion Date
Governance approval • The ADHB-WDHB Collaboration Governance Group approval and CEO signoff on decision
Sept 2014
Consultation on the new operating model and change process
• Consultation undertaken with staff and union representatives
• retaining both contact centre sites with a single joined-up management structure and technology solution
Sept/Oct 2014
Management • Recruitment to a new joint Contact Centre Manager role is underway
Oct 2014
Operating Systems • A Request for Proposal (RFP) to seek a suitable technology provider and software solution has been released through hA
Nov/Dec 2014
Operational improvement
• A detailed improvement plan and process established for ADHB
Aug 2014 ongoing
• A detailed performance analysis to be undertaken WDHB
Dec 2014 – Mar 2015
• A formal linkage with ADHBs website refresh program has been established. Integration of CC and Website functionality to be accelerated in an effort to actively manage call volumes and increase responsiveness.
Oct 2014 – Mar 2015
• Initial site visit to Auckland City Council contact Centre has taken place
Nov 2014
• Further visit for joint contact centre staff and management planned for Jan 2015
Jan 2015
ADHB Performance improvement update Efficiency gaps were identified as part of an assessment of function at the ADHB contact centre. These are being addressed as part of a focused plan to improve service performance and build staff capability. A similar functional and quality assessment of the WDHB contact centre is being planned and will be undertaken in early 2015. In order to establish consistency the key performance indicators (KPIs) and benchmarks established for ADHB will be used as a guiding framework.
The following KPIs and benchmark indicators have been established to guide improvement and efficiency of the service;
Benchmarking and measurement of performance • Establish an accountability framework and individual KPIs to manage operator performance;
including benchmarking activity to assess calls processed per hour • Establish individual KPIs for each operator (also pro-rated in cases for part time staff) at 40 calls
per hour and report monthly • Monthly individual and consolidated centre ‘performance report’ developed and presented to
General Manager • Integrate on-going performance monitoring as part of analysis and feedback to assist individuals
achieve targets • Establish tracking of sickness levels for centre and individuals and report monthly
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
9.3
150

Staff Management • Proactively manage performance through individual and team processes • Proactively manage sick and annual leave to ensure a healthy workforce • On-going staff development program established with HR support • Identify technology, call-type and user response to assess competency and behavioural
issues. • On-going project to boost morale and motivation e.g. a recognition program within the
centre for consistent achievement of SLA & KPI Systems improvement
• Establish monthly ‘Benchmarking meetings’ to address and establish focused action plans • Review the handling of OAS calls and the on-going coordination of this particular queue • Create a platform for staff to raise issues/obstacles in achieving results • Establish a Management Operating System (MOS) board to provide visibility of performance
vs. benchmarks
The graph below illustrates system performance improvement against KPIs as of October 2014. These metrics are now shared with staff as part of their weekly and monthly operational meetings.
Contact Centre KPI Graph
Contact Centre Performance Target 80% Oct 2014 Target 80% Sep 2014 Target 80% Aug 2014
777 100% 100% 100%
Mental Health 80% 77% 79%
GP Helpdesk 78% 76% 78%
On Call 76% 75% 75%
Whisper 78% 76% 77%
General 63% 61% 63%
OAS 56% 54% 56%
Patient Enquiries 68% 57% 59%
SSH Online Confirmation 382 422 415
20
40
60
80
100
MAY JUNE JULY AUGUST SEPT OCT
Contact Centre Key Statistics % Mental Health
GP Helpdesk
On Call
Whisper
General
OAS
Patient Enquiries
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
151

The table below illustrates the impact of improved staff engagement and operational management on sick leave.
Recommendations The following recommendations are made:
1. That the committee note the ongoing project work and operational management of both Contact Centres under a single joined-up management structure and technology solution.
2. That the committee note the commitment to the implementation of a continuous improvement framework across the joint Contact Centre (ADHB/WDHB) to enable the realisation of identified benefits to both DHBs and to the population served.
0
10
20
30
40
50
JULY AUGUST SEPTEMBER OCTOBER NOVEMBER
Sick / days
Sick / days
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
9.3
152


Resolution to exclude the public from the meeting
Recommendation That in accordance with the provisions of Clauses 32 and 33, Schedule 3, of the New Zealand Public Health and Disability Act 2000 the public now be excluded from the meeting for consideration of the following items, for the reasons and grounds set out below:
General subject of item to be considered
Reason for passing this resolution in relation to the item
Grounds under Clause 32 for the passing of this resolution
1. Confirmation of Confidential Minutes 29 October 2014
Confirmation of Minutes As per resolution(s) from the open section of the minutes of the meeting, in terms of the NZPH&D Act 2000.
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
2. Confidential Action Points 29 October 2014
Confirmation of Action Points As per resolution(s) from the open section of the minutes of the meeting, in terms of the NZPH&D Act 2000.
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
3. Health and Safety Commercial Activities To enable the Board to carry out, without prejudice or disadvantage, commercial activities [Official Information Act 1982 s9(2)(i)] Obligation of Confidence The disclosure of information would not be in the public interest because of the greater need to protect information which is subject to an obligation of confidence [Official Information Act 1982 s9(2)(ba)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
4. External Reviews Commercial Activities To enable the Board to carry out, without prejudice or disadvantage, commercial activities [Official Information Act 1982 s9(2)(i)] Obligation of Confidence The disclosure of information would not be in the public interest because of the greater need to protect information which is subject to an obligation of confidence [Official Information Act 1982 s9(2)(ba)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
10
153

5. Medicines Governance
Commercial Activities To enable the Board to carry out, without prejudice or disadvantage, commercial activities [Official Information Act 1982 s9(2)(i)] Obligation of Confidence The disclosure of information would not be in the public interest because of the greater need to protect information which is subject to an obligation of confidence [Official Information Act 1982 s9(2)(ba)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
6. Risk Report Negotiations To enable the Board to carry on, without prejudice or disadvantage, negotiations (including commercial and industrial negotiations) [Official Information Act 1982 s9(2)(j)] Commercial Activities To enable the Board to carry out, without prejudice or disadvantage, commercial activities [Official Information Act 1982 s9(2)(i)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
7. Complaints Report Negotiations To enable the Board to carry on, without prejudice or disadvantage, negotiations (including commercial and industrial negotiations) [Official Information Act 1982 s9(2)(j)] Obligation of Confidence The disclosure of information would not be in the public interest because of the greater need to protect information which is subject to an obligation of confidence [Official Information Act 1982 s9(2)(ba)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
Auckland District Health Board Hospital Advisory Committee Meeting 10 December 2014
154