healthcare market access: vietnam - phamax · 1.3 demographics ... 2009 - 2012..... 22 table 15:...
TRANSCRIPT


2
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
1. COUNTRY LANDSCAPE ................................................................................................................................... 9
1.1 Economic environment ........................................................................................................... 9
1.2 Economic indicators ............................................................................................................. 10
1.2.1 Gross domestic product ................................................................................................ 10
1.2.2 Gross national income .................................................................................................. 12
1.2.3 Inflation ........................................................................................................................ 14
1.2.4 Foreign exchange reserves ............................................................................................ 16
1.2.5 Current account balance ............................................................................................... 17
1.2.6 Government net debt .................................................................................................... 17
1.2.7 Exchange rate ............................................................................................................... 18
1.2.8 Foreign direct investment ............................................................................................. 19
1.2.9 Trade balance ................................................................................................................ 22
1.3 Demographics ....................................................................................................................... 23
1.3.1 Population ..................................................................................................................... 23
1.3.2 Growth of middle class ................................................................................................. 25
1.3.3 Education and literacy .................................................................................................. 26
1.3.4 Access to internet.......................................................................................................... 27
1.3.5 Employment ................................................................................................................. 27
1.4 Political structure and environment ...................................................................................... 30
1.4.1 Current government ...................................................................................................... 31
1.5 Trade associations ................................................................................................................ 32
1.5.1 Vietnam Pharmaceutical Companies Association ........................................................ 32
1.6 Opportunity and challenges .................................................................................................. 33
2 HEALTHCARE INFRASTRUCTURE ............................................................................................................ 34
2.1 Healthcare system ................................................................................................................. 34
2.2 Health status ......................................................................................................................... 36
2.2.1 Life expectancy............................................................................................................. 36
2.2.2 Mortality rate ................................................................................................................ 37
2.3 Healthcare policy .................................................................................................................. 39
2.4 Healthcare financing and expenditure .................................................................................. 40
2.5 Pharmaceutical expenditure .................................................................................................. 45
TABLE OF CONTENTS
3
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
2.6 Shares of the public and private sectors ............................................................................... 47
2.7 Spending in pharmaceutical R&D ........................................................................................ 48
2.8 Health insurance ................................................................................................................... 49
2.9 Hospital sector ...................................................................................................................... 52
2.9.1 Major hospital profiles .................................................................................................. 55
2.9.1.1 Bach Mai Hospital .................................................................................................... 55
2.9.1.2 Cho Ray Hospital...................................................................................................... 56
2.9.1.3 Hue Central Hospital (HCH) .................................................................................... 56
2.9.1.4 Hanoi French Hospital (L’Hôpital Français de Hanoi) ............................................ 56
2.9.1.5 Hospital C in Da Nang .............................................................................................. 56
2.9.1.6 Viet Duc Hospital (Vietnam - Germany Hospital) ................................................... 57
2.9.1.7 Trieu An Hospital (TAH) ......................................................................................... 57
2.9.1.8 Hong Ngoc Hospital ................................................................................................. 57
2.10 Healthcare personnel ............................................................................................................ 58
3 OVERVIEW OF PHARMACEUTICAL MARKET ...................................................................................... 60
3.1 Market overview ................................................................................................................... 60
3.2 Industry structure .................................................................................................................. 61
3.3 Market segments ................................................................................................................... 64
3.4 Opportunities and challenges ................................................................................................ 65
3.5 Major players ........................................................................................................................ 67
3.6 Key products ......................................................................................................................... 70
3.7 Leading therapeutic segments .............................................................................................. 71
3.8 Supply chain ......................................................................................................................... 72
3.8.1 Distribution ................................................................................................................... 74
3.8.2 Retail ............................................................................................................................. 77
3.9 Sales and marketing .............................................................................................................. 78
3.10 FDI in pharmaceutical industry ............................................................................................ 80
3.11 Events ................................................................................................................................... 82
3.12 Major diseases ...................................................................................................................... 83
3.12.1 Stroke ............................................................................................................................ 83
3.12.2 Cancer ........................................................................................................................... 84
3.12.3 Road traffic accidents ................................................................................................... 84
3.12.4 Tuberculosis ................................................................................................................. 84
3.12.5 Diabetes mellitus .......................................................................................................... 85
4
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
3.12.6 HIV/AIDS ..................................................................................................................... 85
4 MARKET ACCESS............................................................................................................................................ 86
4.1 Stakeholder landscape .......................................................................................................... 86
4.2 Regulatory landscape ............................................................................................................ 88
4.2.1 Regulatory agencies ...................................................................................................... 88
4.2.2 Market authorization for pharmaceutical products ....................................................... 89
4.2.3 Clinical trial regulations ............................................................................................... 91
4.2.4 Licensing process for pharmaceutical manufacturing .................................................. 92
4.2.5 Licensing process for pharmaceutical imports ............................................................. 95
4.2.6 Post-marketing regulations ........................................................................................... 95
4.2.7 Advertising ................................................................................................................... 97
4.2.8 Labeling and packaging ................................................................................................ 97
4.2.9 Intellectual property rights ............................................................................................ 98
4.3 Pricing................................................................................................................................. 101
4.3.1 Pricing system............................................................................................................. 101
4.3.2 Pricing policy .............................................................................................................. 102
4.3.3 Price trends ................................................................................................................. 103
4.3.4 Discounts and margins ................................................................................................ 106
4.4 Reimbursement landscape .................................................................................................. 107
4.4.1 Reimbursement process .............................................................................................. 107
4.4.2 Insurance providers ..................................................................................................... 107
4.4.3 Co-payments ............................................................................................................... 108
4.5 Prescribing and dispensing ................................................................................................. 111
4.5.1 Prescribing guidelines ................................................................................................. 111
4.5.2 Prescribing influences ................................................................................................. 111
4.5.3 Dispensing .................................................................................................................. 112
4.6 Essential drug list ............................................................................................................... 113
4.7 Reimbursement drug list ..................................................................................................... 114
4.8 Drug procurement ............................................................................................................... 115
4.9 Hospital formulary .............................................................................................................. 117
5 APPENDIX........................................................................................................................................................ 118
5.1 Glossary .............................................................................................................................. 118
5.2 Bibliography ....................................................................................................................... 121
5.3 Methodology ....................................................................................................................... 125
5
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
5.3.1 Secondary research ..................................................................................................... 125
5.3.2 Primary research ......................................................................................................... 125
5.3.3 Data validation ............................................................................................................ 125
5.4 Disclaimer ........................................................................................................................... 126
5.5 Contact us ........................................................................................................................... 126
6
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Table 1: GDP ($bn), Vietnam, 2009 - 2013 ............................................................................................... 11 Table 2: GDP per capita ($), Vietnam, 2009 - 2013 ................................................................................... 11 Table 3: Real GDP growth (%), Vietnam, 2009 - 2013 ............................................................................. 12 Table 4: Gross national income ($bn), Vietnam, 2009 - 2013 ................................................................... 13 Table 5: GNI per capita ($), Vietnam, 2009 - 2013 .................................................................................... 13 Table 6: Inflation (%), Vietnam, 2009 - 2013 ............................................................................................ 15 Table 7: Consumer price index, Vietnam, 2009 - 2013 .............................................................................. 16 Table 8: Foreign exchange reserves ($bn), Vietnam, 2009 - 2013 ............................................................. 16 Table 9: Current account balance ($bn), Vietnam, 2009 - 2013 ................................................................ 17 Table 10: Government net debt (% to GDP), Vietnam, 2009 - 2013 ......................................................... 18 Table 11: Exchange rate (VND per USD), Vietnam, 2009 - 2013 ............................................................. 19 Table 12: Foreign direct investment, Vietnam, 2009 - 2013 ...................................................................... 20 Table 13: Foreign direct investment ($bn), Peer countries, 2009 - 2013 ................................................... 21 Table 14: Imports and Exports ($bn), Vietnam, 2009 - 2012 ..................................................................... 22 Table 15: Population (mn), Vietnam, 2009 - 2013 ..................................................................................... 23 Table 16: Urban and rural population (mn), Vietnam, 2009 - 2013 ........................................................... 24 Table 17: Population distribution by age groups (%), Vietnam, 2009 - 2013 ............................................ 25 Table 18: Gross enrolment ratio, Vietnam, 2009 - 2013 ............................................................................ 27 Table 19: Employment to population ratio (15+ age), Vietnam, 2009 - 2012 ........................................... 28 Table 20: Unemployment rate of labor force (%), Vietnam, 2009 - 2013 ................................................. 28 Table 21: Life expectancy at birth (years), Vietnam, 2008 - 2012 ............................................................. 36 Table 22: Mortality rate, Vietnam, 2008 - 2012 ......................................................................................... 37 Table 23: Mortality rate by gender, Vietnam, 2008–2012 ......................................................................... 38 Table 24: Healthcare expenditure, Vietnam, 2008 - 2012 .......................................................................... 40 Table 25: Healthcare expenditure per capita, PPP ($), Vietnam, 2008 - 2012 ........................................... 41 Table 26: Public healthcare expenditure (% of total), Vietnam, 2008 - 2012 ............................................ 41 Table 27: Out-of-pocket healthcare expenditure (% of total), .................................................................... 42 Table 28: Pharmaceutical expenditure, Vietnam, 2008 - 2012 .................................................................. 46 Table 29: Share of public - private healthcare expenditure (%), Vietnam, ................................................ 47 Table 30: Number of hospitals and beds by hospital, Vietnam, 2011 ........................................................ 53 Table 31: Number of hospitals, Vietnam, 2008 - 2012 .............................................................................. 54 Table 32: Number of beds (per 10,000 inhabitants), Vietnam, 2008 - 2012 .............................................. 54 Table 33: Number of doctors, Vietnam, 2008 - 2012 ................................................................................. 59 Table 34: Healthcare personnel, Vietnam, 2008 - 2012 ............................................................................. 59 Table 35: Summary of types of marketing activities allowed for............................................................... 79 Table 36: Illustrative price build up ranges for an imported pharmaceutical product in Vietnam ........... 106 Table 37: Benefit packages under CHI in Vietnam .................................................................................. 109
LIST OF TABLES
7
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Figure 1: GDP ($bn), Peer countries, 2013 .................................................................................................. 9 Figure 2: GDP ($bn), Peer countries, 2013 ................................................................................................ 10 Figure 3: GDP per capita ($), Vietnam, 2009 - 2013 ................................................................................. 11 Figure 4: Real GDP growth (%), Vietnam, 2009 - 2013 ............................................................................ 12 Figure 5: Gross national income ($bn), Vietnam, 2009 - 2013 .................................................................. 12 Figure 6: GNI per capita ($), Vietnam, 2009 - 2013 .................................................................................. 13 Figure 7: GNI, Peer countries, 2009 - 2013 ............................................................................................... 14 Figure 8: Inflation (%), Vietnam, 2009 - 2013 ........................................................................................... 15 Figure 9: Consumer price index, Vietnam, 2009 - 2013 ............................................................................ 15 Figure 10: Foreign exchange reserves ($bn), Vietnam, 2009 - 2013 ......................................................... 16 Figure 11: Current account balance ($bn), Vietnam, 2009 - 2012 ............................................................. 17 Figure 12: Government net debt (% to GDP), Vietnam, 2009 - 2013 ........................................................ 18 Figure 13: Exchange rate (VND per USD), Vietnam, 2009 - 2013............................................................ 19 Figure 14: Foreign direct investment, Vietnam, 2009 - 2013 ..................................................................... 20 Figure 15: Foreign direct investment ($bn), Peer countries, 2009 - 2013 .................................................. 20 Figure 16: GDP vs foreign direct investment, Peer countries, 2013 .......................................................... 21 Figure 17: Imports and Exports ($bn), Vietnam, 2009 - 2012 ................................................................... 22 Figure 18: Population (mn), Vietnam, 2009 - 2013.................................................................................... 23 Figure 19: Urban and rural population share (%), Vietnam, 2009 - 2013 .................................................. 24 Figure 20: Population distribution by age groups (%), Vietnam, 2009 - 2013........................................... 25 Figure 21: Gross enrolment ratio, Vietnam, 2009 - 2012 ........................................................................... 26 Figure 22: Employment to population ratio (15+ age), Vietnam, 2009 - 2012 .......................................... 27 Figure 23: Unemployment rate of labor force (%), Vietnam, 2009 - 2013 ................................................ 28 Figure 24: Employment by sectors (%), Vietnam, 2009 - 2013 ................................................................. 29 Figure 25: The structure of the healthcare system in Vietnam ................................................................... 35 Figure 26: Life expectancy at birth (years), Vietnam, 2008 - 2012............................................................ 36 Figure 27: Mortality rate, Vietnam, 2008 - 2012........................................................................................ 37 Figure 28: Mortality rate by gender, Vietnam, 2008–2012 ........................................................................ 38 Figure 29: Healthcare expenditure, Vietnam, 2008 - 2012 ........................................................................ 40 Figure 30: Healthcare expenditure per capita, PPP ($), Vietnam, 2008 - 2012 .......................................... 41 Figure 31: Public healthcare expenditure (% of total), Vietnam, 2008 - 2012 ........................................... 41 Figure 32: Out-of-pocket healthcare expenditure (% of total), .................................................................. 42 Figure 33: Share of sources of total health expenditure (%), Vietnam, 2010 ............................................. 43 Figure 34: Healthcare system financing, Vietnam ..................................................................................... 44 Figure 35: Pharmaceutical expenditure, Vietnam, 2008 - 2012 ................................................................. 45 Figure 36: Share of public-private healthcare expenditure (%), Vietnam, 2008 - 2012 ............................. 47 Figure 37: Health insurance coverage, Vietnam, 2002 - 2010 ................................................................... 49 Figure 38: Roadmap for universal healthcare in Vietnam .......................................................................... 50 Figure 39: Number of hospitals, Vietnam, 2008 - 2012 ............................................................................. 54 Figure 40: Number of beds (per 10,000 inhabitants), Vietnam, 2008 - 2012 ............................................. 54 Figure 41: Number of doctors, Vietnam, 2008 - 2012 ............................................................................... 58 Figure 42: Healthcare personnel, Vietnam, 2008 - 2012 ............................................................................ 59
LIST OF FIGURES
8
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Figure 43: Pharmaceutical market ($bn), Vietnam, 2008 - 2014 ............................................................... 60 Figure 44: Pharmaceutical imports, Vietnam, 2009 - 2013 ........................................................................ 61 Figure 45: Drug consumption distribution (%), Vietnam, 2013 ................................................................. 62 Figure 46: Revenues of notable domestic companies, Vietnam, 2013 ....................................................... 68 Figure 47: Market share of drugs by therapeutic area (%), Vietnam, 2010 ............................................... 71 Figure 48: Distribution channel for pharmaceuticals, Vietnam .................................................................. 73 Figure 49: Sales channel for domestic pharmaceutical companies, Vietnam ............................................. 75 Figure 50: Sales channel for foreign pharmaceutical companies, Vietnam ............................................... 76 Figure 51: Major diseases / conditions (DALY per 1,000,000), Vietnam .................................................. 83 Figure 52: Market authorization process, Vietnam .................................................................................... 90 Figure 53: Registration, evaluation and approval of clinical trial in Vietnam ........................................... 92 Figure 54: Process for obtaining pharmaceutical manufacturing license ................................................... 93 Figure 55: Process for obtaining GMP certificate for pharmaceutical manufacturing ............................... 94 Figure 56: The pharmacovigilance process ................................................................................................ 96 Figure 57: Organization structure of the IP management in Vietnam ........................................................ 99 Figure 58: Agencies involved in drug pricing policy in Vietnam ............................................................ 103 Figure 59: Price differential between Vietnam and IRP at different outlets, 2011 .................................. 104 Figure 60: Organization structure of Vietnam Social Security (VSS)...................................................... 108

9
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: World Bank
1. Country Landscape
1.1 Economic environment
Following its reunification in 1975, Vietnam went through a decade of economic stagnation. Post that era, Vietnam initiated a turnaround with an economic renovation in 1986, known as ‘Doi Moi’ to facilitate its transition from a centrally planned economy to a ‘socialist-oriented’ market economy. The country has since continued to experience strong growth in its economy and has gradually merged with the global community. The year 2013 proved to be a positive year for the Vietnamese economy in spite of posting its lowest growth rate in 2012 in more than a decade. The relatively stable economy in 2013 was attributed to the moderate inflation, stable exchange rates, current account surpluses and significant increase in forex reserves during the year. However, this growth was dampened due to unresolved issues in the banking sector and amongst State Owned Enterprises (SOEs). In an effort to resolve this issue of bad debts, the government did establish the Vietnam Asset Management Company (VAMC), a state owned enterprise in 2013. But, unless this process is hastened, the Non-performing Loan (NPL) crises that hovers over the banking sector will continue to undermine it and hinder Vietnam’s economic growth. The trade agreements that Vietnam signed with the European Union (EU) and other powers are expected to strengthen its economic capabilities, providing development opportunities, especially in the fields of economy, trade, science, technology, agriculture and tourism. According to the government’s directive on formulation of the next Socio-Economic Development plan for 2016 - 2020, Vietnam will target an annual growth of GDP between 6.5% and 7%. This is expected to help Vietnam become a modernized and industrialized country by 2020.
Figure 1: GDP ($bn), Peer countries, 2013
868
387 312 298 272
171
0
200
400
600
800
1,000
Indonesia Thailand Malaysia Singapore Philippines Vietnam
GD
P ($
bn)

10
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: World Bank
1.2 Economic indicators
1.2.1 Gross domestic product
The Gross Domestic Product (GDP) of Vietnam was $171.4 bn in 2013, witnessing a substantial growth of 5.4% compared to 2012, fuelled by a strong rise in final consumption. The GDP growth had reached an all-time high in 2010 and contrastingly slumped in 2012, attributable to the rising inflation in the country. Although Vietnam’s GDP growth was not as high as its peers (Indonesia, Malaysia, Philippines, Singapore and Thailand), the signs were greeted with optimism.
Between 2009 and 2013, the GDP of Vietnam grew at an annual average rate of 5.7%. Based on the findings of the International Monetary Fund (IMF), Vietnam’s growing economy is being supported by both exports and increased foreign investment in the country. The growth in 2013 was led by the Services sector (43% of the GDP), which grew by 6.6% while Manufacturing (38% of the GDP) and Agriculture sectors grew by 5.4% and 2.7% respectively. Taking into account all these factors, many analysts expected the GDP growth to rise slightly further to 5.6% in 2014 and grow further to 5.8% in 2015, in alignment with the upward trends in the US and European zones. The corresponding improvements in the developed zones were expected to help Vietnam address its domestic banking drawbacks.
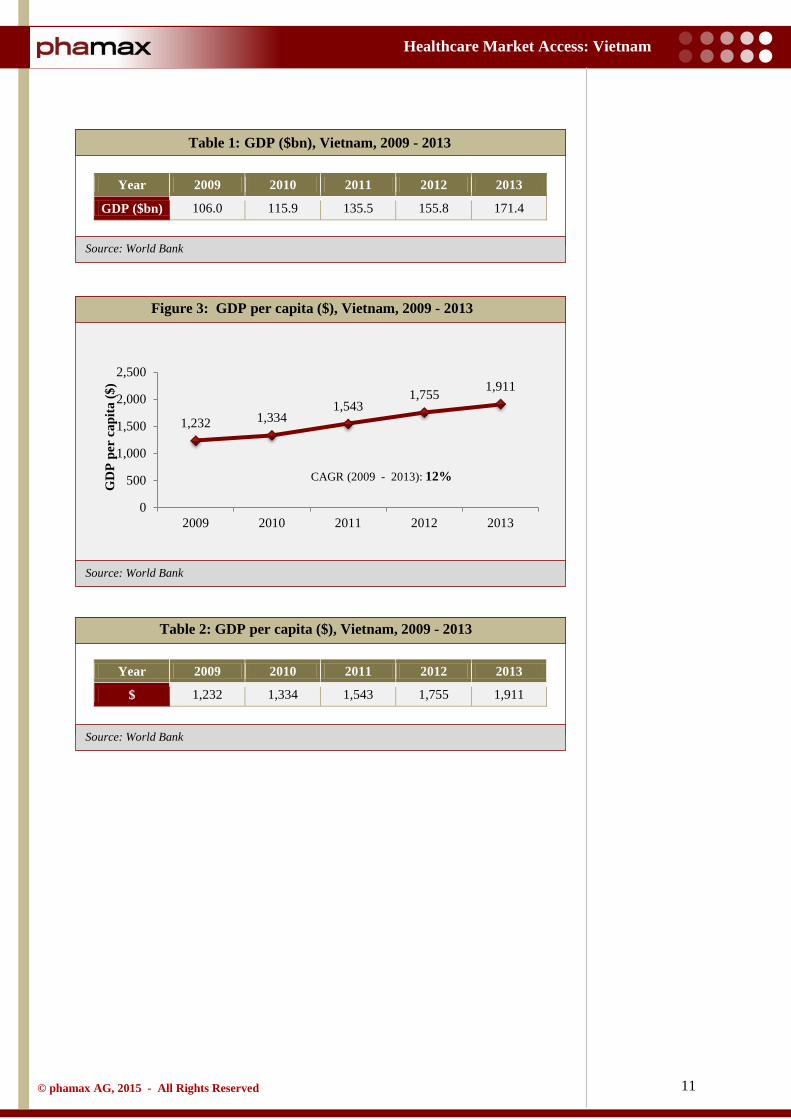
In 2010, Vietnam attained a per capita GDP of $1,333 and was categorized as a low middle-income country, based on guidelines designed by the World Bank. In 2013, Vietnam’s GDP per capita reached $1,911 and the National Congress (Ministry of Planning and Investment) expects to achieve its target of GDP per capita of $2,000 by 2015.
Figure 2: GDP ($bn), Peer countries, 2013
106.0 115.9 135.5
155.8 171.4
0
50
100
150
200
2009 2010 2011 2012 2013
GD
P ($
bn)
CAGR (2009 - 2013): 13%
The GDP of Vietnam has grown at an annual average rate of 5.7% over 2009 - 2013. Vietnam’s growing economy is being supported by both exports and increased foreign investment in the country.
GDP growth is estimated to be 5.8% in 2015 due to recovery in global economy.
11
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: World Bank
Source: World Bank
Source: World Bank
Table 1: GDP ($bn), Vietnam, 2009 - 2013
Year 2009 2010 2011 2012 2013
GDP ($bn) 106.0 115.9 135.5 155.8 171.4
Table 2: GDP per capita ($), Vietnam, 2009 - 2013
Year 2009 2010 2011 2012 2013
$ 1,232 1,334 1,543 1,755 1,911
Figure 3: GDP per capita ($), Vietnam, 2009 - 2013
1,232 1,334 1,543
1,755 1,911
0
500
1,000
1,500
2,000
2,500
2009 2010 2011 2012 2013
GD
P pe
r ca
pita
($)
CAGR (2009 - 2013): 12%
12
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: World Bank
Source: World Bank
Source: World Bank
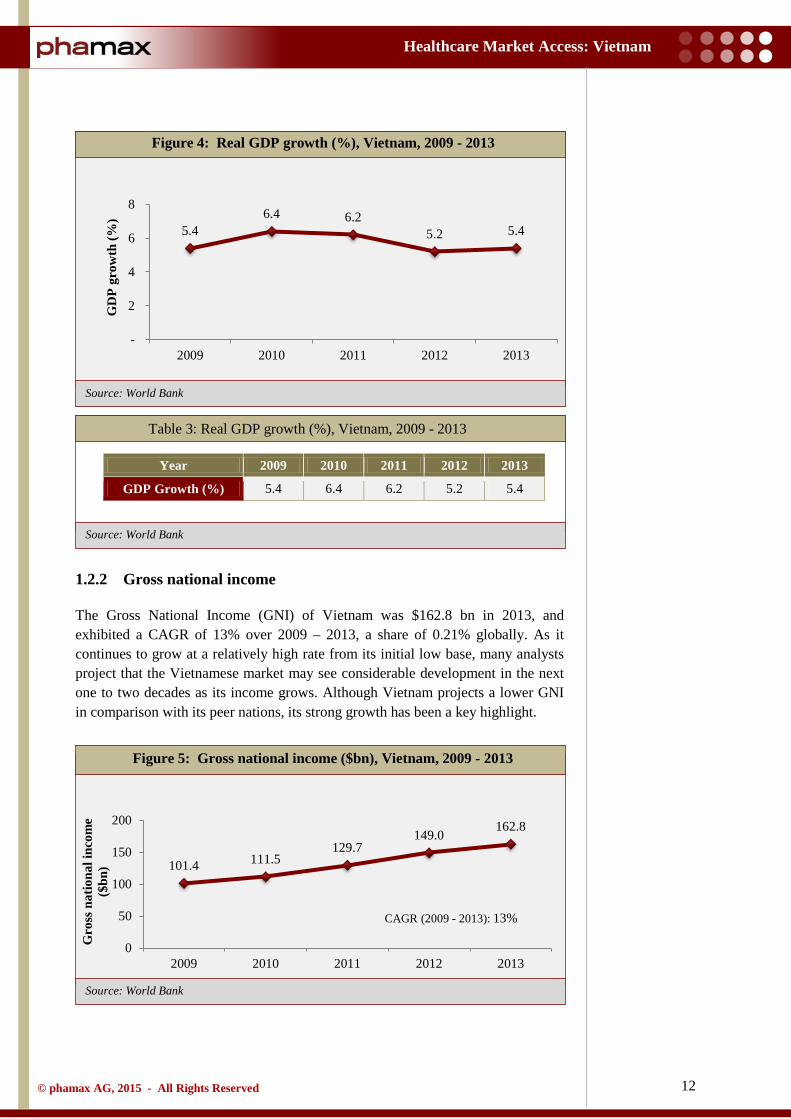
Table 3: Real GDP growth (%), Vietnam, 2009 - 2013
Year 2009 2010 2011 2012 2013
GDP Growth (%) 5.4 6.4 6.2 5.2 5.4
1.2.2 Gross national income
The Gross National Income (GNI) of Vietnam was $162.8 bn in 2013, and exhibited a CAGR of 13% over 2009 – 2013, a share of 0.21% globally. As it continues to grow at a relatively high rate from its initial low base, many analysts project that the Vietnamese market may see considerable development in the next one to two decades as its income grows. Although Vietnam projects a lower GNI in comparison with its peer nations, its strong growth has been a key highlight.
Figure 4: Real GDP growth (%), Vietnam, 2009 - 2013
Figure 5: Gross national income ($bn), Vietnam, 2009 - 2013
5.4 6.4 6.2
5.2 5.4
-
2
4
6
8
2009 2010 2011 2012 2013
GD
P gr
owth
(%)
101.4 111.5 129.7
149.0 162.8
0
50
100
150
200
2009 2010 2011 2012 2013
Gro
ss n
atio
nal i
ncom
e ($
bn)
CAGR (2009 - 2013): 13%
13
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: World Bank
Source: World Bank
Source: World Bank
Table 4: Gross national income ($bn), Vietnam, 2009 - 2013
Year 2009 2010 2011 2012 2013
$bn 101.4 111.5 129.7 149.0 162.8
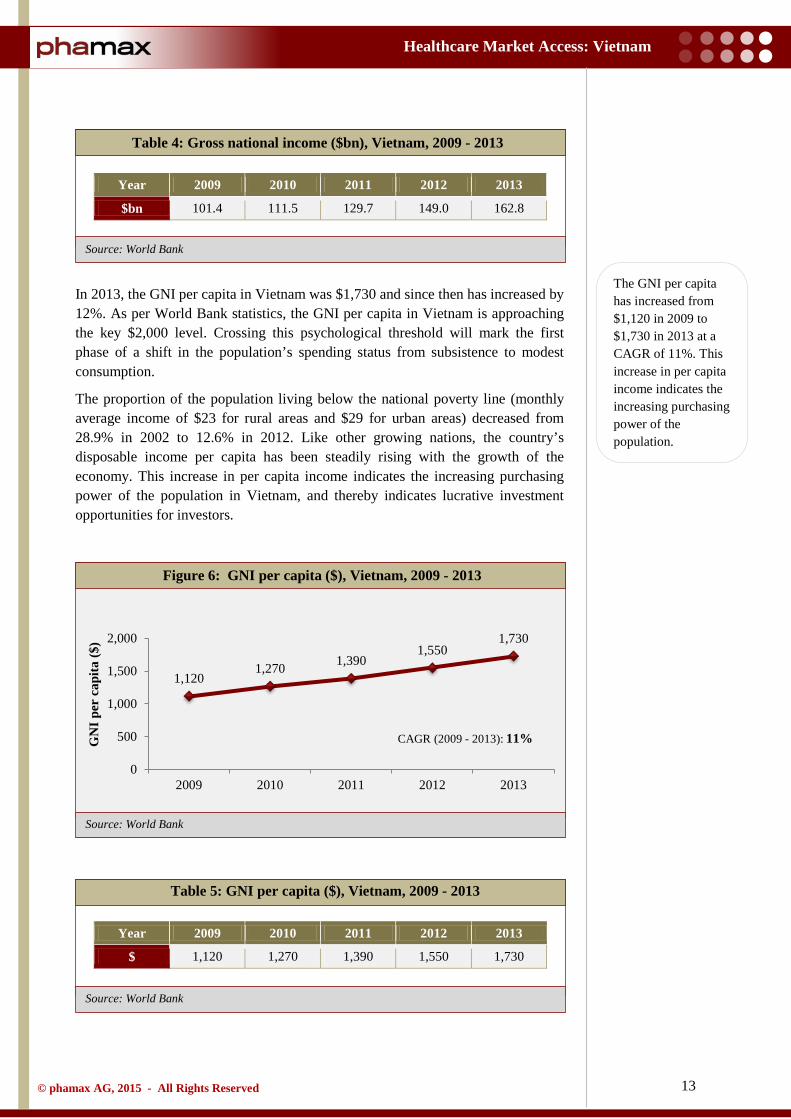
In 2013, the GNI per capita in Vietnam was $1,730 and since then has increased by 12%. As per World Bank statistics, the GNI per capita in Vietnam is approaching the key $2,000 level. Crossing this psychological threshold will mark the first phase of a shift in the population’s spending status from subsistence to modest consumption.
The proportion of the population living below the national poverty line (monthly average income of $23 for rural areas and $29 for urban areas) decreased from 28.9% in 2002 to 12.6% in 2012. Like other growing nations, the country’s disposable income per capita has been steadily rising with the growth of the economy. This increase in per capita income indicates the increasing purchasing power of the population in Vietnam, and thereby indicates lucrative investment opportunities for investors.
Table 5: GNI per capita ($), Vietnam, 2009 - 2013
Year 2009 2010 2011 2012 2013
$ 1,120 1,270 1,390 1,550 1,730
Figure 6: GNI per capita ($), Vietnam, 2009 - 2013
1,120 1,270 1,390
1,550 1,730
0
500
1,000
1,500
2,000
2009 2010 2011 2012 2013
GN
I per
cap
ita ($
)
CAGR (2009 - 2013): 11%
The GNI per capita has increased from $1,120 in 2009 to $1,730 in 2013 at a CAGR of 11%. This increase in per capita income indicates the increasing purchasing power of the population.
14
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: World Bank
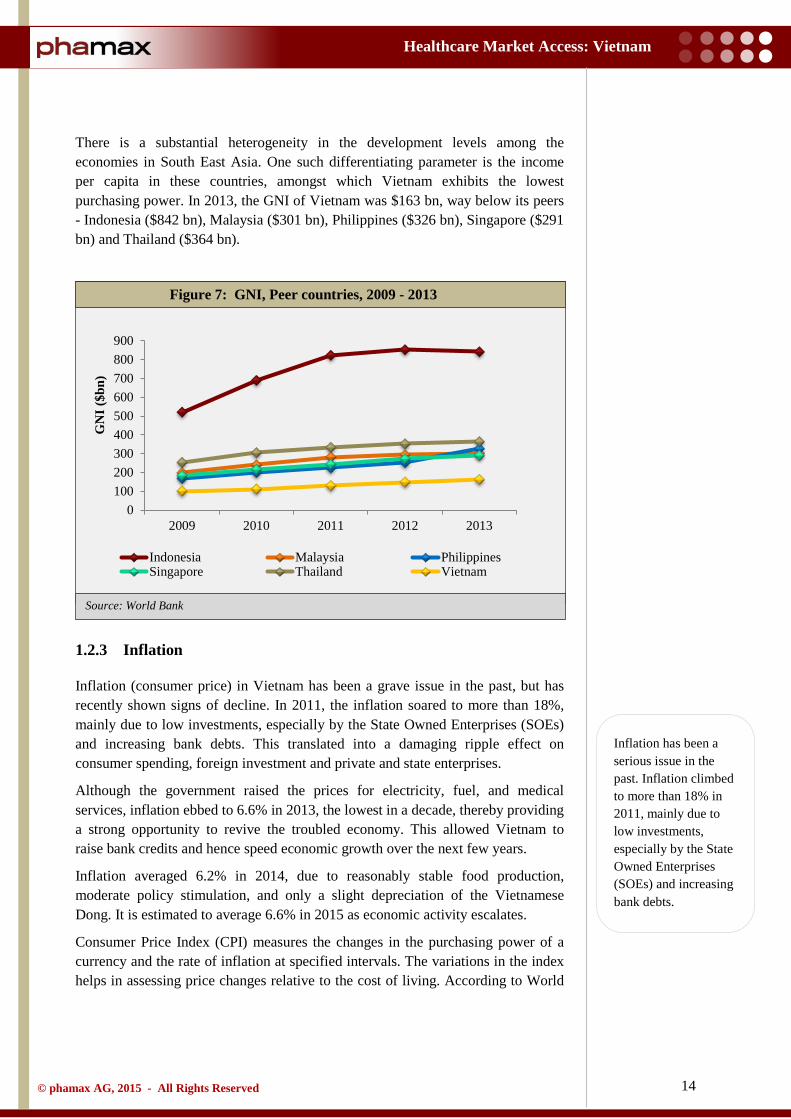
There is a substantial heterogeneity in the development levels among the economies in South East Asia. One such differentiating parameter is the income per capita in these countries, amongst which Vietnam exhibits the lowest purchasing power. In 2013, the GNI of Vietnam was $163 bn, way below its peers - Indonesia ($842 bn), Malaysia ($301 bn), Philippines ($326 bn), Singapore ($291 bn) and Thailand ($364 bn).
1.2.3 Inflation
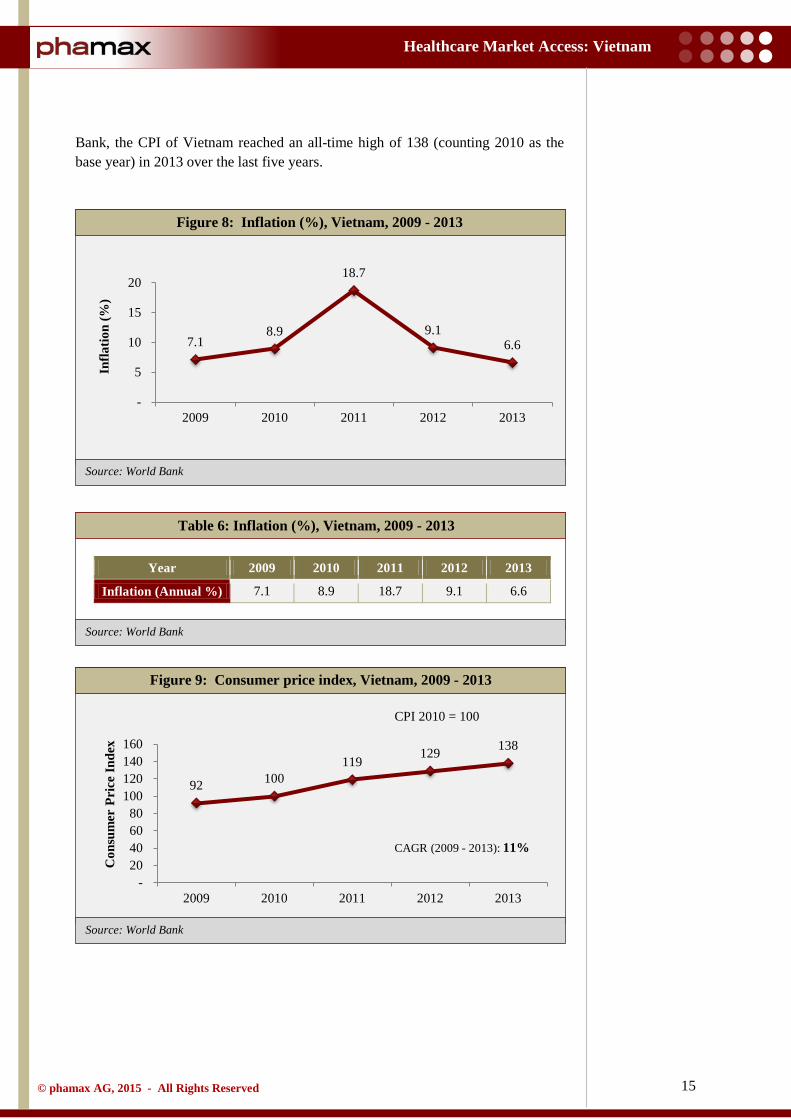
Inflation (consumer price) in Vietnam has been a grave issue in the past, but has recently shown signs of decline. In 2011, the inflation soared to more than 18%, mainly due to low investments, especially by the State Owned Enterprises (SOEs) and increasing bank debts. This translated into a damaging ripple effect on consumer spending, foreign investment and private and state enterprises.
Although the government raised the prices for electricity, fuel, and medical services, inflation ebbed to 6.6% in 2013, the lowest in a decade, thereby providing a strong opportunity to revive the troubled economy. This allowed Vietnam to raise bank credits and hence speed economic growth over the next few years.
Inflation averaged 6.2% in 2014, due to reasonably stable food production, moderate policy stimulation, and only a slight depreciation of the Vietnamese Dong. It is estimated to average 6.6% in 2015 as economic activity escalates.
Consumer Price Index (CPI) measures the changes in the purchasing power of a currency and the rate of inflation at specified intervals. The variations in the index helps in assessing price changes relative to the cost of living. According to World
Figure 7: GNI, Peer countries, 2009 - 2013
0100200300400500600700800900
2009 2010 2011 2012 2013
GN
I ($b
n)
Indonesia Malaysia PhilippinesSingapore Thailand Vietnam
Inflation has been a serious issue in the past. Inflation climbed to more than 18% in 2011, mainly due to low investments, especially by the State Owned Enterprises (SOEs) and increasing bank debts.
15
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: World Bank
Source: World Bank
Source: World Bank
Bank, the CPI of Vietnam reached an all-time high of 138 (counting 2010 as the base year) in 2013 over the last five years.
Table 6: Inflation (%), Vietnam, 2009 - 2013
Year 2009 2010 2011 2012 2013
Inflation (Annual %) 7.1 8.9 18.7 9.1 6.6
Figure 8: Inflation (%), Vietnam, 2009 - 2013
Figure 9: Consumer price index, Vietnam, 2009 - 2013
7.1 8.9
18.7
9.1 6.6
-
5
10
15
20
2009 2010 2011 2012 2013
Infla
tion
(%)
92 100 119 129 138
- 20 40 60 80
100 120 140 160
2009 2010 2011 2012 2013
Con
sum
er P
rice
Inde
x
CAGR (2009 - 2013): 11%
CPI 2010 = 100
16
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: World Bank
Source: World Bank
Source: World Bank
Table 7: Consumer price index, Vietnam, 2009 - 2013
Year 2009 2010 2011 2012 2013
Consumer Price Index 92 100 119 129 138
1.2.4 Foreign exchange reserves
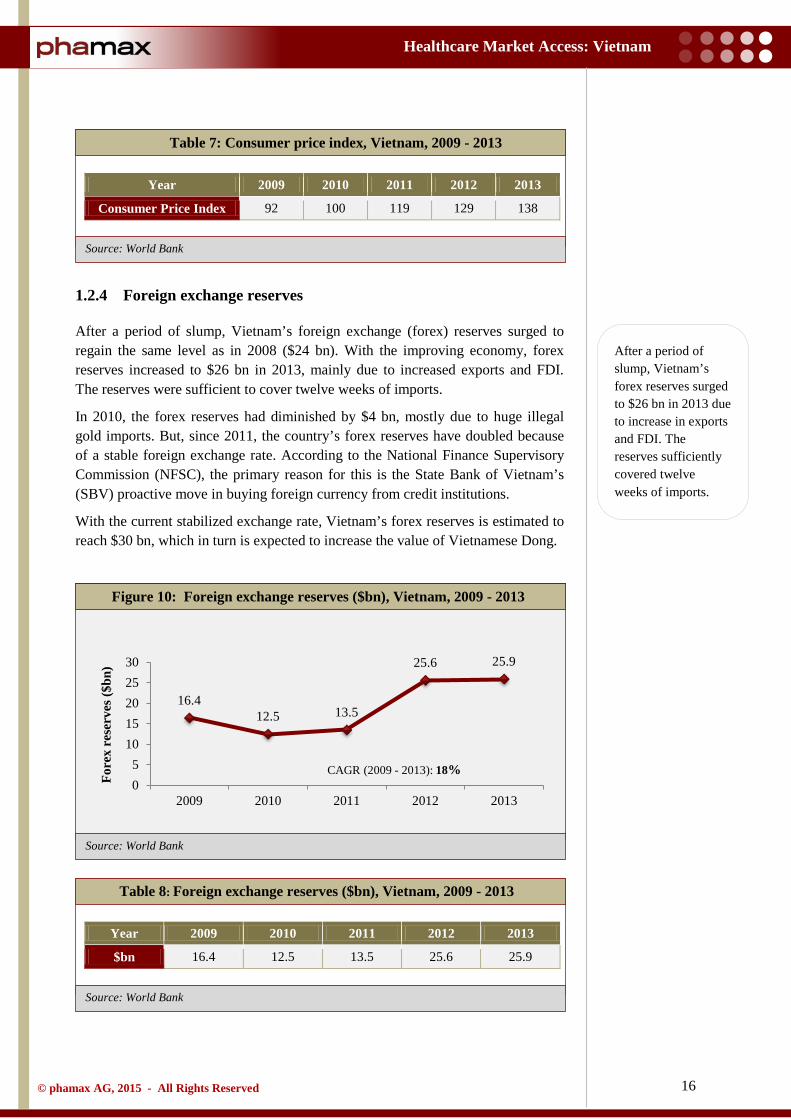
After a period of slump, Vietnam’s foreign exchange (forex) reserves surged to regain the same level as in 2008 ($24 bn). With the improving economy, forex reserves increased to $26 bn in 2013, mainly due to increased exports and FDI. The reserves were sufficient to cover twelve weeks of imports.
In 2010, the forex reserves had diminished by $4 bn, mostly due to huge illegal gold imports. But, since 2011, the country’s forex reserves have doubled because of a stable foreign exchange rate. According to the National Finance Supervisory Commission (NFSC), the primary reason for this is the State Bank of Vietnam’s (SBV) proactive move in buying foreign currency from credit institutions.
With the current stabilized exchange rate, Vietnam’s forex reserves is estimated to reach $30 bn, which in turn is expected to increase the value of Vietnamese Dong.
Table 8: Foreign exchange reserves ($bn), Vietnam, 2009 - 2013
Year 2009 2010 2011 2012 2013
$bn 16.4 12.5 13.5 25.6 25.9
Figure 10: Foreign exchange reserves ($bn), Vietnam, 2009 - 2013
16.4 12.5 13.5
25.6 25.9
05
1015202530
2009 2010 2011 2012 2013
Fore
x re
serv
es ($
bn)
CAGR (2009 - 2013): 18%
After a period of slump, Vietnam’s forex reserves surged to $26 bn in 2013 due to increase in exports and FDI. The reserves sufficiently covered twelve weeks of imports.
17
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: World Bank
Source: World Bank
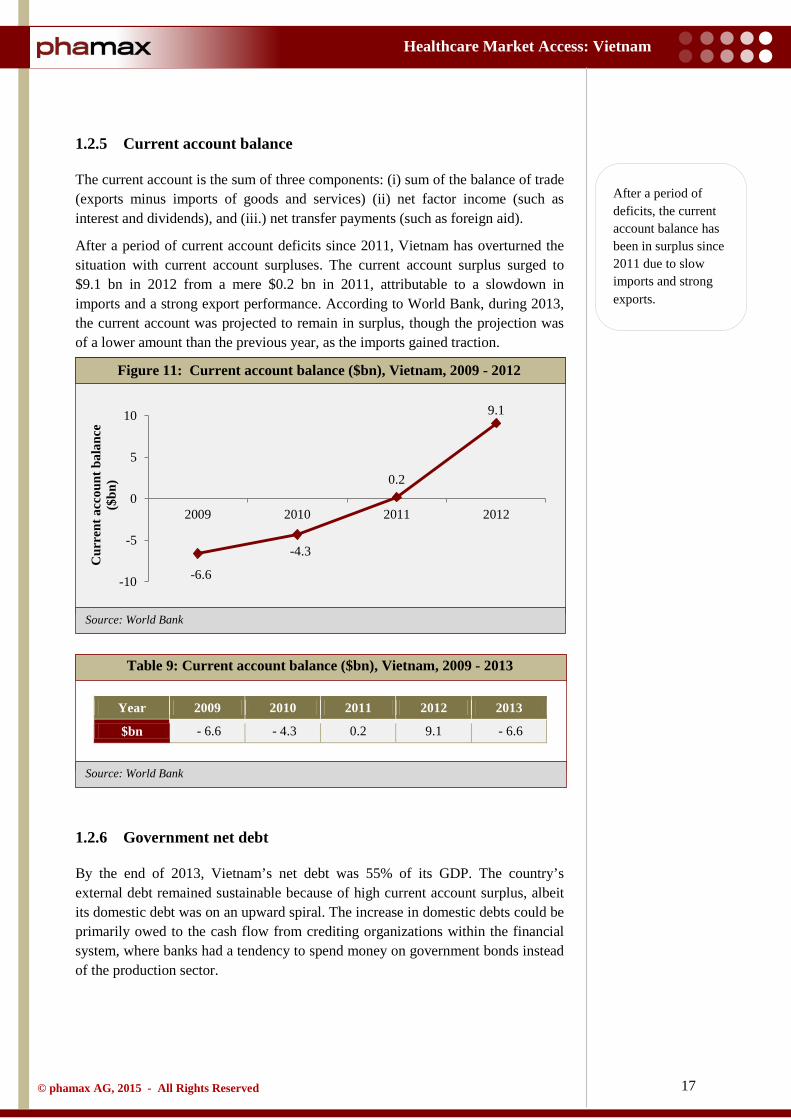
1.2.5 Current account balance
The current account is the sum of three components: (i) sum of the balance of trade (exports minus imports of goods and services) (ii) net factor income (such as interest and dividends), and (iii.) net transfer payments (such as foreign aid).
After a period of current account deficits since 2011, Vietnam has overturned the situation with current account surpluses. The current account surplus surged to $9.1 bn in 2012 from a mere $0.2 bn in 2011, attributable to a slowdown in imports and a strong export performance. According to World Bank, during 2013, the current account was projected to remain in surplus, though the projection was of a lower amount than the previous year, as the imports gained traction.
Table 9: Current account balance ($bn), Vietnam, 2009 - 2013
Year 2009 2010 2011 2012 2013
$bn - 6.6 - 4.3 0.2 9.1 - 6.6
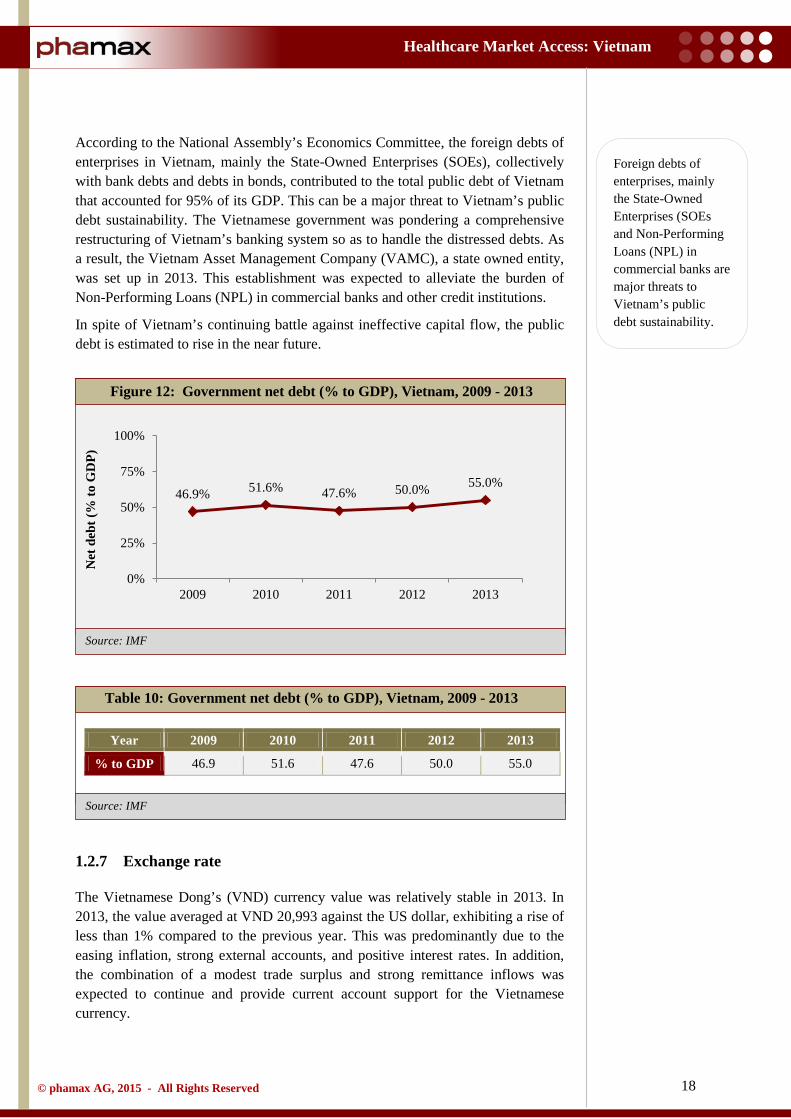
1.2.6 Government net debt
By the end of 2013, Vietnam’s net debt was 55% of its GDP. The country’s external debt remained sustainable because of high current account surplus, albeit its domestic debt was on an upward spiral. The increase in domestic debts could be primarily owed to the cash flow from crediting organizations within the financial system, where banks had a tendency to spend money on government bonds instead of the production sector.
Figure 11: Current account balance ($bn), Vietnam, 2009 - 2012
-6.6
-4.3
0.2
9.1
-10
-5
0
5
10
2009 2010 2011 2012
Cur
rent
acc
ount
bal
ance
($
bn)
After a period of deficits, the current account balance has been in surplus since 2011 due to slow imports and strong exports.
18
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: IMF
Source: IMF
According to the National Assembly’s Economics Committee, the foreign debts of enterprises in Vietnam, mainly the State-Owned Enterprises (SOEs), collectively with bank debts and debts in bonds, contributed to the total public debt of Vietnam that accounted for 95% of its GDP. This can be a major threat to Vietnam’s public debt sustainability. The Vietnamese government was pondering a comprehensive restructuring of Vietnam’s banking system so as to handle the distressed debts. As a result, the Vietnam Asset Management Company (VAMC), a state owned entity, was set up in 2013. This establishment was expected to alleviate the burden of Non-Performing Loans (NPL) in commercial banks and other credit institutions.
In spite of Vietnam’s continuing battle against ineffective capital flow, the public debt is estimated to rise in the near future.
Table 10: Government net debt (% to GDP), Vietnam, 2009 - 2013
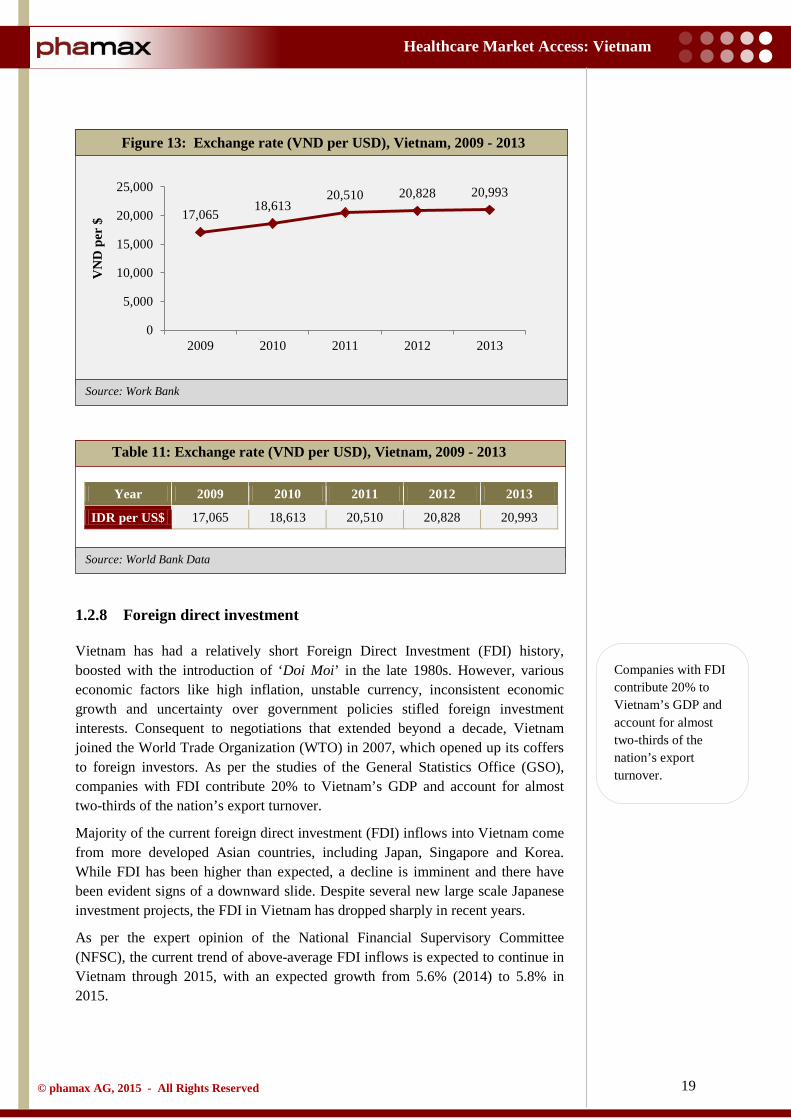
1.2.7 Exchange rate
The Vietnamese Dong’s (VND) currency value was relatively stable in 2013. In 2013, the value averaged at VND 20,993 against the US dollar, exhibiting a rise of less than 1% compared to the previous year. This was predominantly due to the easing inflation, strong external accounts, and positive interest rates. In addition, the combination of a modest trade surplus and strong remittance inflows was expected to continue and provide current account support for the Vietnamese currency.
Figure 12: Government net debt (% to GDP), Vietnam, 2009 - 2013
Year 2009 2010 2011 2012 2013
% to GDP 46.9 51.6 47.6 50.0 55.0
46.9% 51.6% 47.6% 50.0% 55.0%
0%
25%
50%
75%
100%
2009 2010 2011 2012 2013
Net
deb
t (%
to G
DP)
Foreign debts of enterprises, mainly the State-Owned Enterprises (SOEs and Non-Performing Loans (NPL) in commercial banks are major threats to Vietnam’s public debt sustainability.
19
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: World Bank Data
Source: Work Bank
Table 11: Exchange rate (VND per USD), Vietnam, 2009 - 2013
Year 2009 2010 2011 2012 2013
IDR per US$ 17,065 18,613 20,510 20,828 20,993
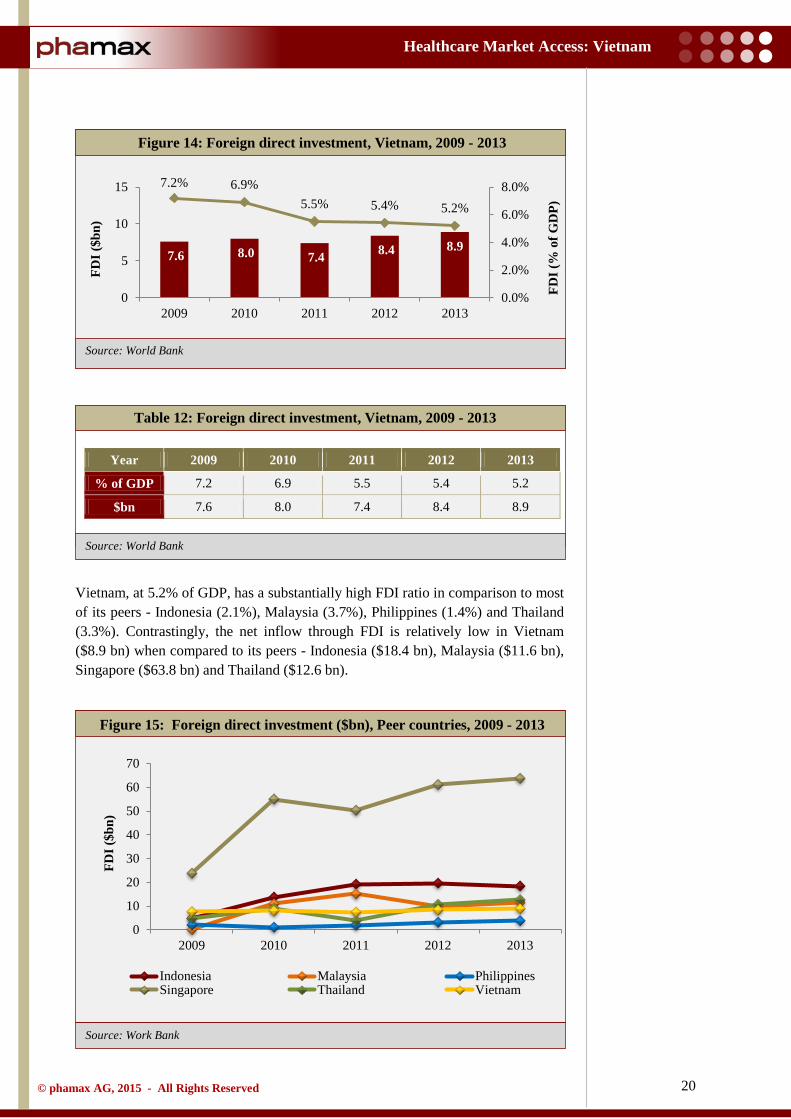
1.2.8 Foreign direct investment
Vietnam has had a relatively short Foreign Direct Investment (FDI) history, boosted with the introduction of ‘Doi Moi’ in the late 1980s. However, various economic factors like high inflation, unstable currency, inconsistent economic growth and uncertainty over government policies stifled foreign investment interests. Consequent to negotiations that extended beyond a decade, Vietnam joined the World Trade Organization (WTO) in 2007, which opened up its coffers to foreign investors. As per the studies of the General Statistics Office (GSO), companies with FDI contribute 20% to Vietnam’s GDP and account for almost two-thirds of the nation’s export turnover.
Majority of the current foreign direct investment (FDI) inflows into Vietnam come from more developed Asian countries, including Japan, Singapore and Korea. While FDI has been higher than expected, a decline is imminent and there have been evident signs of a downward slide. Despite several new large scale Japanese investment projects, the FDI in Vietnam has dropped sharply in recent years.
As per the expert opinion of the National Financial Supervisory Committee (NFSC), the current trend of above-average FDI inflows is expected to continue in Vietnam through 2015, with an expected growth from 5.6% (2014) to 5.8% in 2015.
Figure 13: Exchange rate (VND per USD), Vietnam, 2009 - 2013
17,065 18,613
20,510 20,828 20,993
0
5,000
10,000
15,000
20,000
25,000
2009 2010 2011 2012 2013
VN
D p
er $
Companies with FDI contribute 20% to Vietnam’s GDP and account for almost two-thirds of the nation’s export turnover.
20
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: World Bank
Source: World Bank
Source: Work Bank
Table 12: Foreign direct investment, Vietnam, 2009 - 2013
Year 2009 2010 2011 2012 2013
% of GDP 7.2 6.9 5.5 5.4 5.2
$bn 7.6 8.0 7.4 8.4 8.9
Vietnam, at 5.2% of GDP, has a substantially high FDI ratio in comparison to most of its peers - Indonesia (2.1%), Malaysia (3.7%), Philippines (1.4%) and Thailand (3.3%). Contrastingly, the net inflow through FDI is relatively low in Vietnam ($8.9 bn) when compared to its peers - Indonesia ($18.4 bn), Malaysia ($11.6 bn), Singapore ($63.8 bn) and Thailand ($12.6 bn).
Figure 14: Foreign direct investment, Vietnam, 2009 - 2013
Figure 15: Foreign direct investment ($bn), Peer countries, 2009 - 2013
7.6 8.0 7.4 8.4 8.9
7.2% 6.9% 5.5% 5.4% 5.2%
0.0%
2.0%
4.0%
6.0%
8.0%
0
5
10
15
2009 2010 2011 2012 2013
FDI (
% o
f GD
P)
FDI (
$bn)
0
10
20
30
40
50
60
70
2009 2010 2011 2012 2013
FDI (
$bn)
Indonesia Malaysia PhilippinesSingapore Thailand Vietnam

21
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: World Bank
Source: Work Bank
Table 13: Foreign direct investment ($bn), Peer countries, 2009 - 2013
Year 2009 2010 2011 2012 2013
Indonesia 4.9 13.8 19.2 19.6 18.4
Malaysia 0.1 10.9 15.1 9.7 11.6
Philippines 2.1 1.1 2.0 3.2 3.9
Singapore 23.8 55.1 50.4 61.2 63.8
Thailand 4.9 9.1 3.9 10.7 12.6
Vietnam 7.6 8.0 7.4 8.4 8.9
Note: Size of the bubble indicate the 2013, FDI inflows in respective countries
Figure 16: GDP vs foreign direct investment, Peer countries, 2013
Indonesia, $18.4bn
Malaysia, $11.6bn
Philippines, $3.9bn
Singapore, $63.8bn
Thailand, $12.6bn
Vietnam, $8.9bn
0
200
400
600
800
1000
1200
0 5 10 15 20 25
GD
P (c
urre
nt $
bn)
Foreign Direct Investment, inflows (FDI, % of GDP)
22
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: Work Bank
Source: World Bank
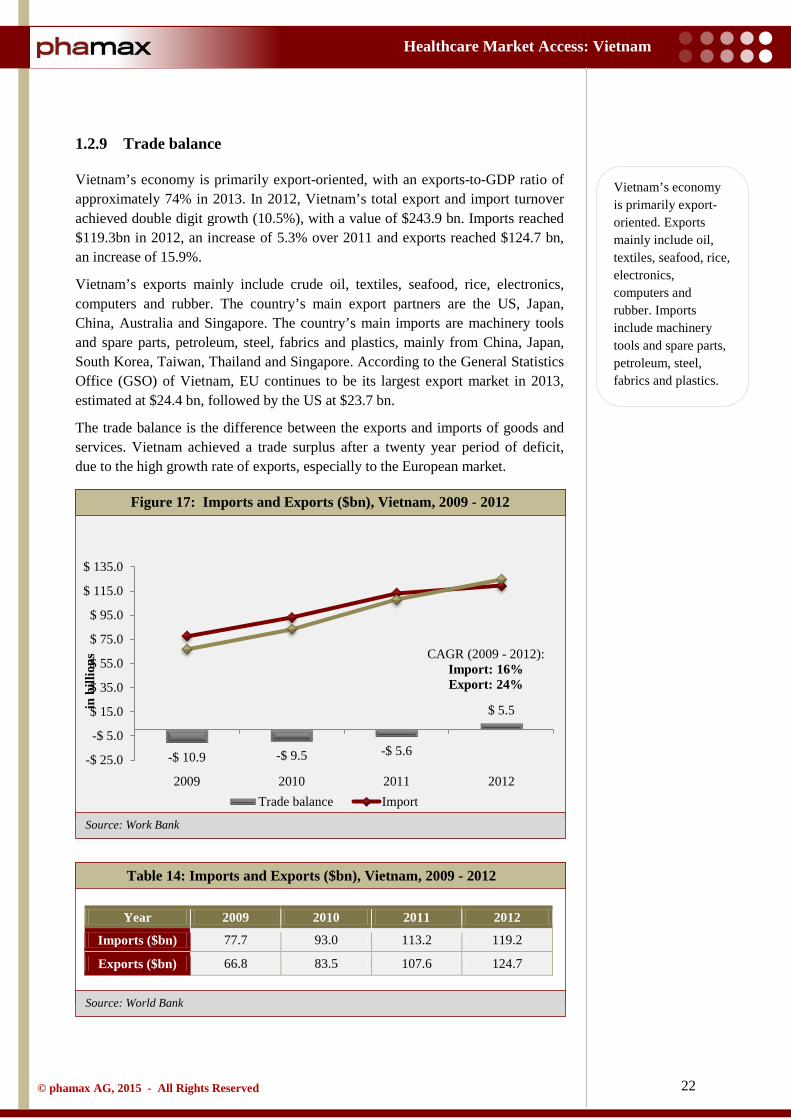
1.2.9 Trade balance
Vietnam’s economy is primarily export-oriented, with an exports-to-GDP ratio of approximately 74% in 2013. In 2012, Vietnam’s total export and import turnover achieved double digit growth (10.5%), with a value of $243.9 bn. Imports reached $119.3bn in 2012, an increase of 5.3% over 2011 and exports reached $124.7 bn, an increase of 15.9%.
Vietnam’s exports mainly include crude oil, textiles, seafood, rice, electronics, computers and rubber. The country’s main export partners are the US, Japan, China, Australia and Singapore. The country’s main imports are machinery tools and spare parts, petroleum, steel, fabrics and plastics, mainly from China, Japan, South Korea, Taiwan, Thailand and Singapore. According to the General Statistics Office (GSO) of Vietnam, EU continues to be its largest export market in 2013, estimated at $24.4 bn, followed by the US at $23.7 bn.
The trade balance is the difference between the exports and imports of goods and services. Vietnam achieved a trade surplus after a twenty year period of deficit, due to the high growth rate of exports, especially to the European market.
Table 14: Imports and Exports ($bn), Vietnam, 2009 - 2012
Year 2009 2010 2011 2012
Imports ($bn) 77.7 93.0 113.2 119.2
Exports ($bn) 66.8 83.5 107.6 124.7
Figure 17: Imports and Exports ($bn), Vietnam, 2009 - 2012
-$ 10.9 -$ 9.5 -$ 5.6
$ 5.5
-$ 25.0
-$ 5.0
$ 15.0
$ 35.0
$ 55.0
$ 75.0
$ 95.0
$ 115.0
$ 135.0
2009 2010 2011 2012
in b
illio
ns
Trade balance Import
CAGR (2009 - 2012): Import: 16% Export: 24%
Vietnam’s economy is primarily export-oriented. Exports mainly include oil, textiles, seafood, rice, electronics, computers and rubber. Imports include machinery tools and spare parts, petroleum, steel, fabrics and plastics.
23
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: World Bank
Source: World Bank
1.3 Demographics
1.3.1 Population
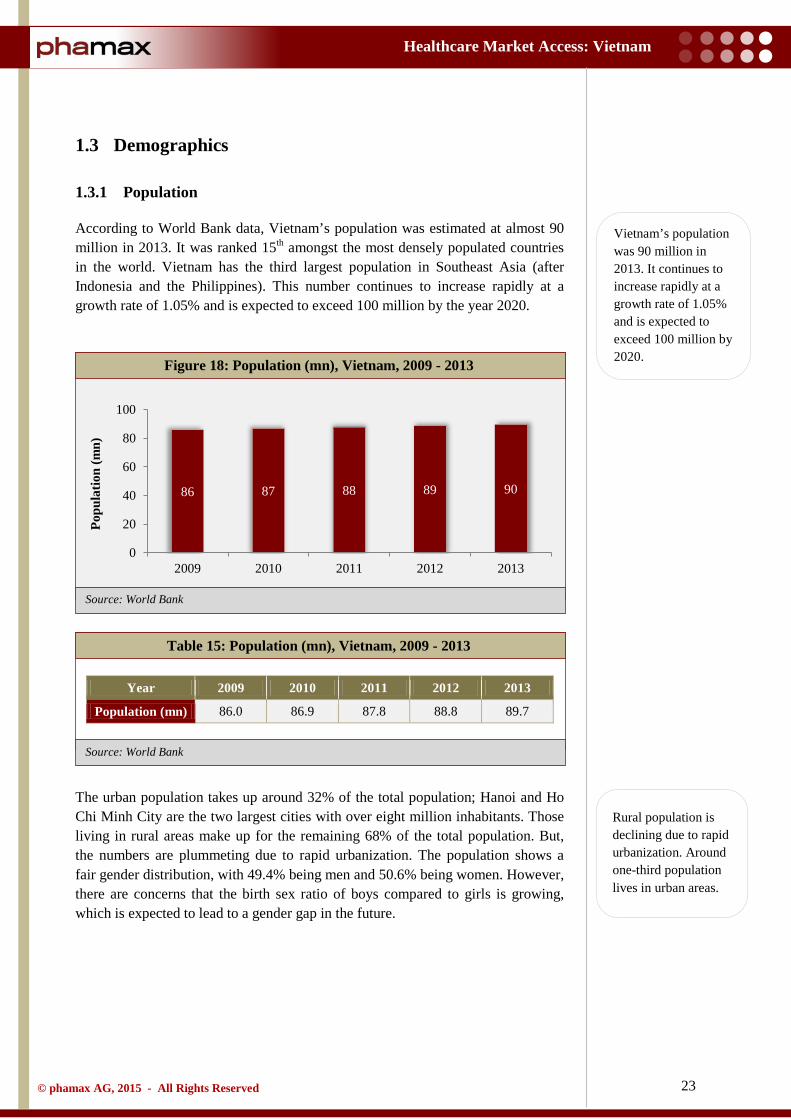
According to World Bank data, Vietnam’s population was estimated at almost 90 million in 2013. It was ranked 15th amongst the most densely populated countries in the world. Vietnam has the third largest population in Southeast Asia (after Indonesia and the Philippines). This number continues to increase rapidly at a growth rate of 1.05% and is expected to exceed 100 million by the year 2020.
Table 15: Population (mn), Vietnam, 2009 - 2013
Year 2009 2010 2011 2012 2013
Population (mn) 86.0 86.9 87.8 88.8 89.7
The urban population takes up around 32% of the total population; Hanoi and Ho Chi Minh City are the two largest cities with over eight million inhabitants. Those living in rural areas make up for the remaining 68% of the total population. But, the numbers are plummeting due to rapid urbanization. The population shows a fair gender distribution, with 49.4% being men and 50.6% being women. However, there are concerns that the birth sex ratio of boys compared to girls is growing, which is expected to lead to a gender gap in the future.
Figure 18: Population (mn), Vietnam, 2009 - 2013
86 87 88 89 90
0
20
40
60
80
100
2009 2010 2011 2012 2013
Popu
latio
n (m
n)
Vietnam’s population was 90 million in 2013. It continues to increase rapidly at a growth rate of 1.05% and is expected to exceed 100 million by 2020.
Rural population is declining due to rapid urbanization. Around one-third population lives in urban areas.

24
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: World Bank
Source: World Bank
Table 16: Urban and rural population (mn), Vietnam, 2009 - 2013
Year 2009 2010 2011 2012 2013
Rural (mn) 60.4 60.5 60.6 60.7 60.7
Urban (mn) 25.6 26.4 27.3 28.1 29.0
In 2012, the life expectancy in Vietnam was 75.6 years, with 80.4 years for women and 71.1 years for men.
Vietnam has a young population structure, with the age group of 14 - 64 years constituting almost 71% of the total population, with other age groups (0 - 14 years) and ( > 65 years) being 23% and 7% respectively. The United Nations with the General Statistics Office (GSO), released a publication with the general census of population in Vietnam in 2009, stating that the nation had a period of ‘golden population structure’, i.e., the number of working people exceeded the number of dependent people. This ratio clearly indicated a steady supply of labor for manufacturers and suppliers, which further reinforced Vietnam as a land of lucrative opportunities for foreign investment and outsourcing.
Figure 19: Urban and rural population share (%), Vietnam, 2009 - 2013
70% 70% 69% 68% 68%
30% 30% 31% 32% 32%
2009 2010 2011 2012 2013
% o
f tot
al p
opul
atio
n
Rural Urban
Vietnam has a young population. The age group of 14 to 64 years constitutes almost 71% of the total population.
25
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: World Bank
Source: World Bank
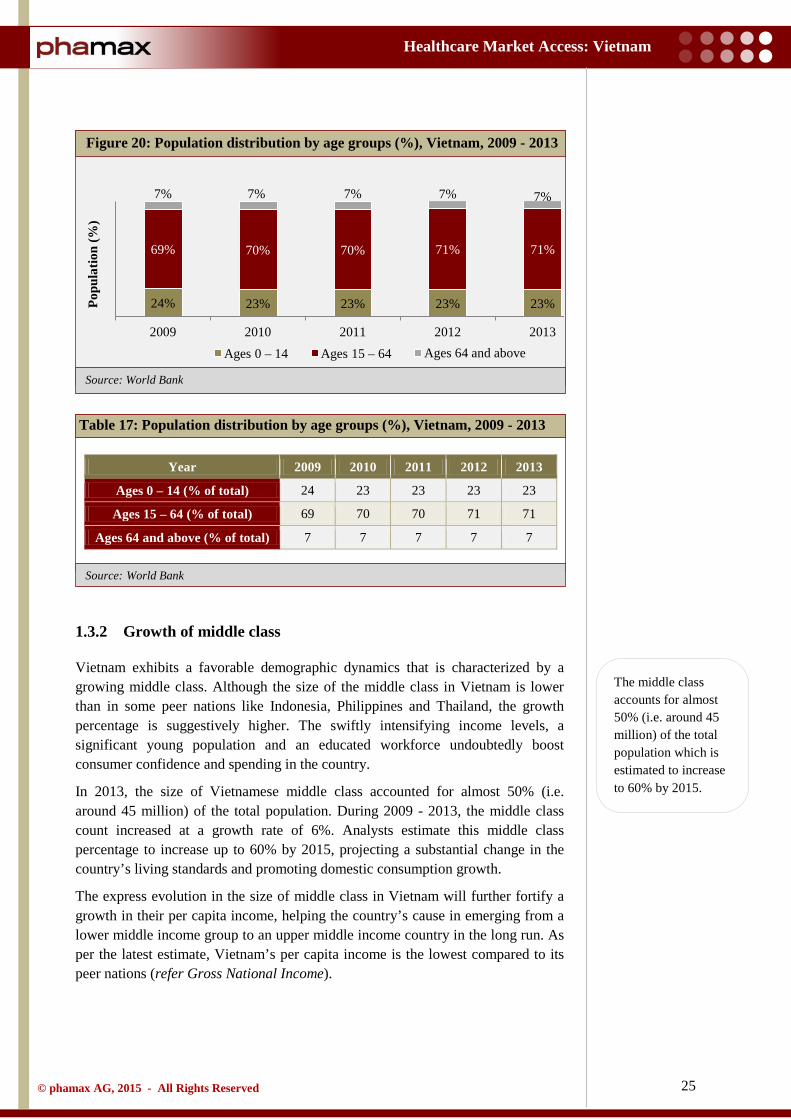
Table 17: Population distribution by age groups (%), Vietnam, 2009 - 2013
Year 2009 2010 2011 2012 2013
Ages 0 – 14 (% of total) 24 23 23 23 23
Ages 15 – 64 (% of total) 69 70 70 71 71
Ages 64 and above (% of total) 7 7 7 7 7
1.3.2 Growth of middle class
Vietnam exhibits a favorable demographic dynamics that is characterized by a growing middle class. Although the size of the middle class in Vietnam is lower than in some peer nations like Indonesia, Philippines and Thailand, the growth percentage is suggestively higher. The swiftly intensifying income levels, a significant young population and an educated workforce undoubtedly boost consumer confidence and spending in the country.
In 2013, the size of Vietnamese middle class accounted for almost 50% (i.e. around 45 million) of the total population. During 2009 - 2013, the middle class count increased at a growth rate of 6%. Analysts estimate this middle class percentage to increase up to 60% by 2015, projecting a substantial change in the country’s living standards and promoting domestic consumption growth.
The express evolution in the size of middle class in Vietnam will further fortify a growth in their per capita income, helping the country’s cause in emerging from a lower middle income group to an upper middle income country in the long run. As per the latest estimate, Vietnam’s per capita income is the lowest compared to its peer nations (refer Gross National Income).
Figure 20: Population distribution by age groups (%), Vietnam, 2009 - 2013
24% 23% 23% 23% 23%
69% 70% 70% 71% 71%
7% 7% 7% 7% 7%
2009 2010 2011 2012 2013
Popu
latio
n (%
)
Ages 0 – 14 Ages 15 – 64 Ages 64 and above
The middle class accounts for almost 50% (i.e. around 45 million) of the total population which is estimated to increase to 60% by 2015.

26
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: World Bank
1.3.3 Education and literacy
Although rated an underprivileged country with a low per capita income, Vietnam has persistently evolved in nurturing and preserving high literacy rates. According to the CIA World Fact book, the country’s literacy rate is 93.4% (95.4% for men and 91.4% for women). The literacy rate of Vietnam is higher than that of Malaysia and Indonesia, but lower than Singapore, Philippines and Thailand.
In 2005, the National Assembly of Vietnam approved a legislature, stating compulsory education at the primary and lower secondary levels. Demonstrating its keenness on the priority of education, the government of Vietnam has always allocated a part of its budget for the same. It had set substantial goals, under the Socio Economic Development Plan 2006 - 2010 and further reinforced it with the Resolution on Comprehensive and Fundamental Reform of Higher Education in Vietnam 2006 - 2020. The major objective of such plans was to increase enrolment in universities and colleges, increase proportion of qualified teachers and encourage private establishments with high-quality education and management.
Figure 21 displays the trends of Gross Enrolment Ratios for different levels of education in Vietnam. Gross Enrolment Ratio (GER) is the total enrolment, regardless of age, expressed as a percentage of the population. GER can exceed 100% based on the inclusion of over-aged and under-aged students because of early or late school entrances and grade repetitions.
The GER of pre-primary education in Vietnam has steadily increased from 66.7% in 2009 to 77.2% in 2012. The GER of primary education slightly decreased to 104.7% in 2012, although this decline was inconsistent. The Gross Enrolment Ratio of secondary education was not reflected whilst GER of tertiary education steadily increased during the period 2008 - 2012.
Figure 21: Gross enrolment ratio, Vietnam, 2009 - 2012
67 69 72 77
103 105 105 105
20 22 24 25 0
40
80
120
2009 2010 2011 2012
Gro
ss e
nrol
lmen
t ra
tio
Preprimary Primary Tertiary
In spite of a low per capita income, Vietnam has a high literacy rate of 93%.
27
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: World Bank
Source: World Bank
Table 18: Gross enrolment ratio, Vietnam, 2009 - 2013
Year 2009 2010 2011 2012
GER, pre - primary 44.8 40.4 41.5 47.6
GER, primary 109.9 109.9 109.1 108.5
GER, secondary 76.5 78.4 81.2 82.5
GER, tertiary 23.7 24.9 27.2 31.5
1.3.4 Access to internet
The Vietnam government made internet accessible in 1997. The access has since multiplied across all regions in Vietnam.
Based on the latest estimates, nearly 40% (around. 36 million) of Vietnamese population owns an individual internet connection. Vietnam ranks higher in terms of the number of internet users in comparison to its peers. The number of internet users has increase multifold (fifteen times) since 2000 and continues to grow at a rapid rate.
Recent years have seen the extensive growth of 3G networks in Vietnam. But, the progress has been stalling due to the lack of supporting infrastructure. Further, with an average household income of approximately $160 per month, the devices necessary for home and/or mobile data subscriptions remain out of reach of the majority. Also, approximately 70% of Vietnamese users are yet to migrate to a smartphone, thereby limiting the internet usage. But, in spite of such constraints, the numbers are predicted to improve with declining costs.
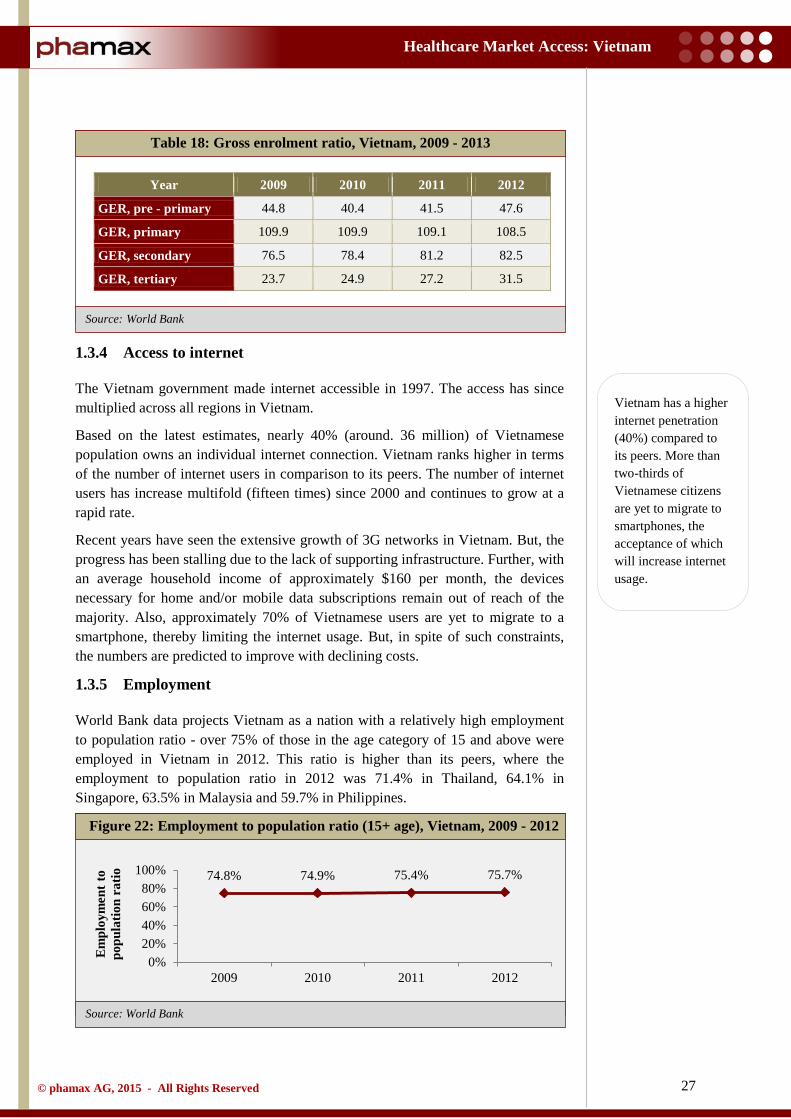
1.3.5 Employment
World Bank data projects Vietnam as a nation with a relatively high employment to population ratio - over 75% of those in the age category of 15 and above were employed in Vietnam in 2012. This ratio is higher than its peers, where the employment to population ratio in 2012 was 71.4% in Thailand, 64.1% in Singapore, 63.5% in Malaysia and 59.7% in Philippines.
Figure 22: Employment to population ratio (15+ age), Vietnam, 2009 - 2012
74.8% 74.9% 75.4% 75.7%
0%20%40%60%80%
100%
2009 2010 2011 2012
Em
ploy
men
t to
popu
latio
n ra
tio
Vietnam has a higher internet penetration (40%) compared to its peers. More than two-thirds of Vietnamese citizens are yet to migrate to smartphones, the acceptance of which will increase internet usage.
28
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: World Bank
Source: World Bank Data
Source: GSO Vietnam
Table 19: Employment to population ratio (15+ age), Vietnam, 2009 - 2012
Year 2009 2010 2011 2012
% of total labor force 74.8 74.9 75.4 75.7
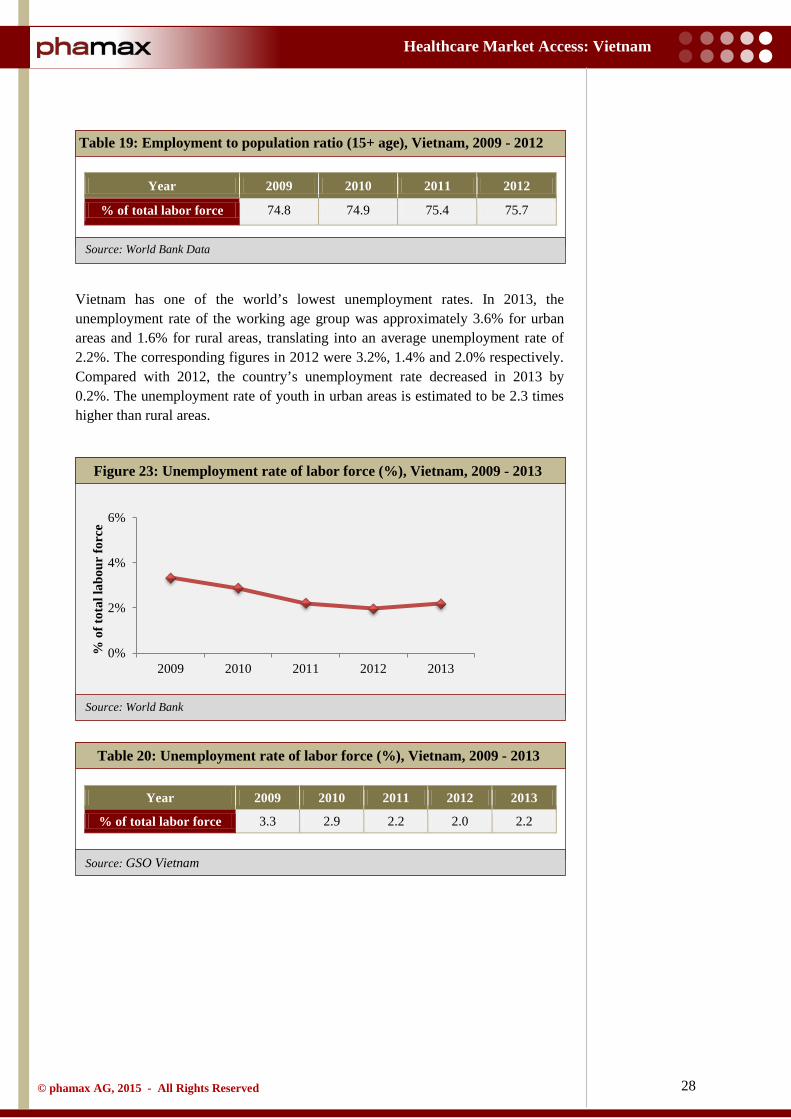
Vietnam has one of the world’s lowest unemployment rates. In 2013, the unemployment rate of the working age group was approximately 3.6% for urban areas and 1.6% for rural areas, translating into an average unemployment rate of 2.2%. The corresponding figures in 2012 were 3.2%, 1.4% and 2.0% respectively. Compared with 2012, the country’s unemployment rate decreased in 2013 by 0.2%. The unemployment rate of youth in urban areas is estimated to be 2.3 times higher than rural areas.
Table 20: Unemployment rate of labor force (%), Vietnam, 2009 - 2013
Year 2009 2010 2011 2012 2013
% of total labor force 3.3 2.9 2.2 2.0 2.2
Figure 23: Unemployment rate of labor force (%), Vietnam, 2009 - 2013
0%
2%
4%
6%
2009 2010 2011 2012 2013
% o
f tot
al la
bour
forc
e
29
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: GSO Vietnam
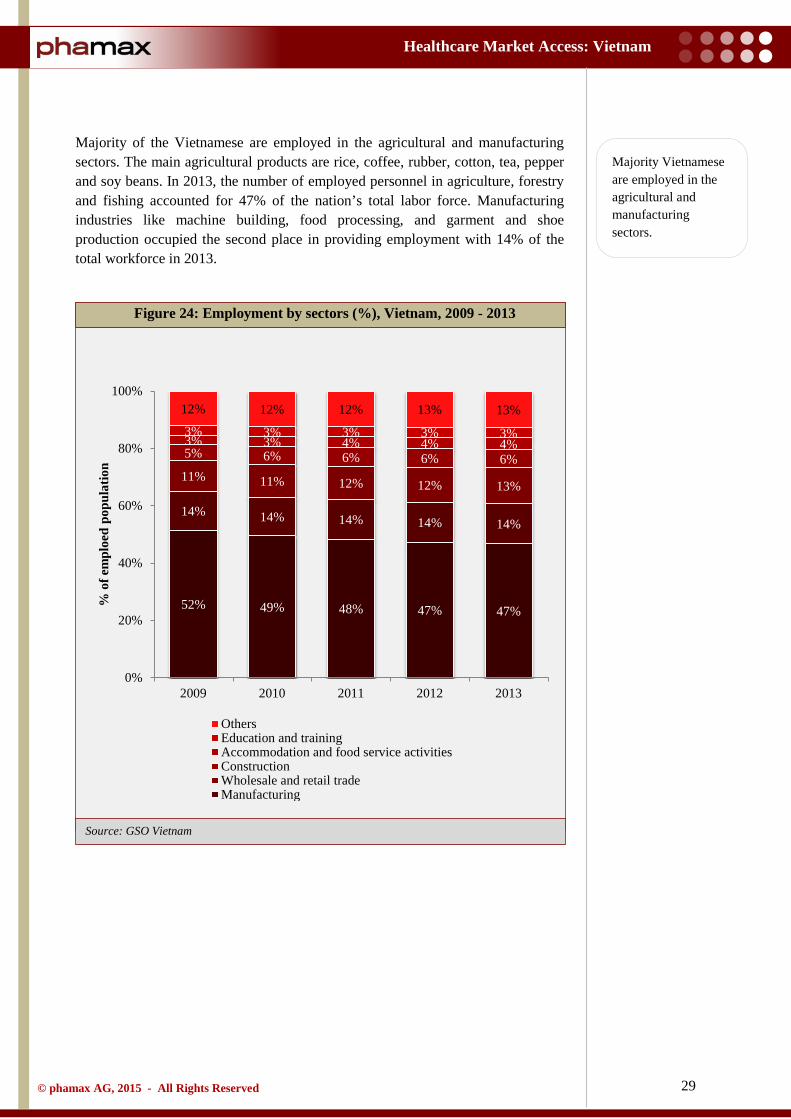
Majority of the Vietnamese are employed in the agricultural and manufacturing sectors. The main agricultural products are rice, coffee, rubber, cotton, tea, pepper and soy beans. In 2013, the number of employed personnel in agriculture, forestry and fishing accounted for 47% of the nation’s total labor force. Manufacturing industries like machine building, food processing, and garment and shoe production occupied the second place in providing employment with 14% of the total workforce in 2013.
Figure 24: Employment by sectors (%), Vietnam, 2009 - 2013
52% 49% 48% 47% 47%
14% 14% 14% 14% 14%
11% 11% 12% 12% 13%
5% 6% 6% 6% 6% 3% 3% 4% 4% 4% 3% 3% 3% 3% 3%
12% 12% 12% 13% 13%
0%
20%
40%
60%
80%
100%
2009 2010 2011 2012 2013
% o
f em
ploe
d po
pula
tion
OthersEducation and trainingAccommodation and food service activitiesConstructionWholesale and retail tradeManufacturing
Majority Vietnamese are employed in the agricultural and manufacturing sectors.

30
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
1.4 Political structure and environment
The Socialist Republic of Vietnam is a law governed state and one of the world's few remaining one-party communist states. The current political system of Vietnam encompasses the Communist Party of Vietnam (CPV), political organizations, socio-political organizations, socio-professional organizations, and mass associations.
The Communist Party of Vietnam (CPV) includes the Central Committee, which is a very powerful institution in Vietnam and formally vests much of the political power. It comprises 175 full and 25 alternate members elected at the Party Congress, held every five years (the Twelfth Party Congress is scheduled for 2016). The Central Committee meets twice a year and acts as the CPV's supreme decision-making body. The Central Committee elects a Politburo (currently sixteen members), which runs Party affairs. The three most powerful political positions in Vietnam are those of the General Secretary of the CPV, the Prime Minister and the President.
The President is elected by the National Assembly for a five year term and acts as the Commander-in- Chief of the Armed Forces and Chairman of the Council for Defense and Security. The government is the main executive power in Vietnam and is headed by the Prime Minister. The Prime Minister is elected by a proposal of the President of Vietnam to the National Assembly. The Prime Minister is responsible to the National Assembly, which elects all ministers of the government.
The country has a unicameral National Assembly, whose 450 members are elected every five years. The National Assembly exercises three main functions: to legislate, to decide on important national issues, to exercise supreme supervision over all activities of the state. In the last held election for the National Assembly in 2011, 92% of those elected were members from the CPV. In recent years, the National Assembly has been increasingly active and influential in setting national priorities and has become more assertive in exercising its authority over law making. However, it is still subject to the Communist Party directions.
Vietnam has an independent judicial system governed by the Constitution of Vietnam. However, lawyers are not available in ample numbers and the judicial system does not have the relevant power to administer law.
The increasing role of the National Assembly in reviewing legislation and policies and a more incisive media has contributed to greater transparency in Vietnam. On the flip side, individuals can incur long prison terms for broadly framed charges, such as spying, minor acts against national security and propaganda against the state.
Vietnam is one of the world's few remaining one-party communist states with the Communist Party of Vietnam (CPV) in power.
31
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
1.4.1 Current government
The government is the executive body of the National Assembly, the highest body of state administration in Vietnam. It manages the overall political, economic, cultural, social and national (defense, security and external duties) duties of the state.
The government is accountable to the National Assembly and reports to it, its Standing Committee, and the country's President. The government consists of the Prime Minister, who is a designated National Assembly deputy as declared by the Constitution, Deputy Prime Ministers, Ministers and other members.
In 2011, the CPV’s central committee re-elected Prime Minister Nguyen Tan Dung to the Politburo for a second five year term. In 2010, he was under tremendous public pressure to resign after a scandal involving a prominent ship building group, Vinashin. Several Vinashin officials were jailed for their roles in the scandal. But, he was spared disciplinary action by the Communist Party. Analysts believe that despite concerns about economic instability, Dung is widely expected to be re-appointed as Prime Minister for another term. However, the leaders will need to tame the inflation and mitigate further risks in the economic growth to justify re-election.
Earlier, under Dung's leadership, international human rights groups had accused Vietnam of taking a more than usual tougher stance against political rebels, including those peacefully expressing their views online. But the government has minimum any threat to its one - party rule, and people can be jailed for publicly demanding a multiparty system.
Truong Tan Sang was elected as the President in July 2011, winning 97% of the votes in parliament. Meanwhile, the Communist Party appointed Nguyen Phu Trong as its Secretary General in January 2011, replacing Nong Duc Manh, who retired after ten years of active service.
The government is the executive body of the National Assembly, the highest body of state administration in Vietnam.
The CPV’s central committee re-elected Prime Minister Nguyen Tan Dung to a second five year term in 2011. Truong Tan Sang was elected as the President in July 2011.
32
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
1.5 Trade associations
1.5.1 Vietnam Pharmaceutical Companies Association
Vietnam Pharmaceutical Companies Association (VNPCA) is a trade association that invites pharmaceutical companies to join its community and represents them. The main motive of the association is to benefit the community in alignment with the growth and nurture of the enterprises, enhance the Vietnamese pharmaceutical brands in the domestic and global markets and ultimately contribute to the development of the nation and the pharmaceutical industry
After nine years of operations, the association has assembled nearly hundred top Vietnamese pharmaceutical firms, assisted them in updating industry and legal information, accelerated trade promotion activities, provided consultancy and training, and acted as a bridge between enterprises and government organizations and the community.

33
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
1.6 Opportunity and challenges
Vietnam is a growing economy in the Asia Pacific region, and therefore provides lucrative opportunities for investors.
In 2013, the macroeconomic conditions in Vietnam were relatively stable and the country’s economy fought back to recover from earlier slumps. However, the struggle to boost the economy remains, In 2012, the decline in bank lending affected domestic demand, mounting pressure on the government to overhaul the financial system, thus deferring the economic growth. Added to this, a corrupt and bureaucratic administration was ineffective in taking the relevant measures to curtail entrepreneurs and investors.
Vietnam’s economy is bound to face adversities in the coming years, due to bad debts, liquidity of commercial banks and a shrinking market for locally manufactured goods. Unless domestic enterprises take initiatives to restructure themselves, cut production costs, develop strategies to multiply their business, seize opportunities as they arise, find means to access economical fund supplies, the supply and value chain in both domestic and international markets will remain affected. This, in turn, will pose risks in controlling inflation, reducing trade and budget deficit, attracting more foreign investment, reducing unemployment and ensuring social security.
In accordance with its economy boosting initiatives, in 2012, Vietnam revealed a broad ‘three pillar’ economic reform program, proposing the restructuring of public investment, State Owned Enterprises (SOEs) and the banking sector. However, the progress has been at a snail’s pace under the program.
The Vietnamese government initiatives under the Socio-Economic Development plan for the period 2011 - 2020 outlines a group of effective measures to accelerate the economic restructuring process. In line with this plan, in 2013, the government persisted in tightening the monetary policy, prioritizing macro stability and managing inflation at moderately low levels. Additionally, the government’s prime focus areas have always been clearing bad debts and restructuring state owned enterprises, two strategies that are imperative to drive economic growth in the upcoming years. But, the modifications are destined to happen only gradually.
A survey by the American Chamber of Commerce (AmCham) in Singapore reveals that American companies intend to slot Vietnam after Indonesia in Southeast Asia for investments in the coming years, replacing China. Notable trade agreements like the Trans-Pacific Partnership Agreement (TPP) and the EU - Vietnam Free Trade Agreement (EVFTA) are also positive moves to augment trade and boost investment activities in Vietnam.
Moreover, the large and increasingly affluent population represents a large workforce and an under-served consumer market providing an attractive avenue for foreign investors.
Vietnam’s economy is bound to face adversities in the coming years, due to bad debts, liquidity of commercial banks and a shrinking market for locally manufactured goods. However, recently signed trade agreements with the West will have a favorable impact on trade and investments.

34
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
2 Healthcare Infrastructure
2.1 Healthcare system
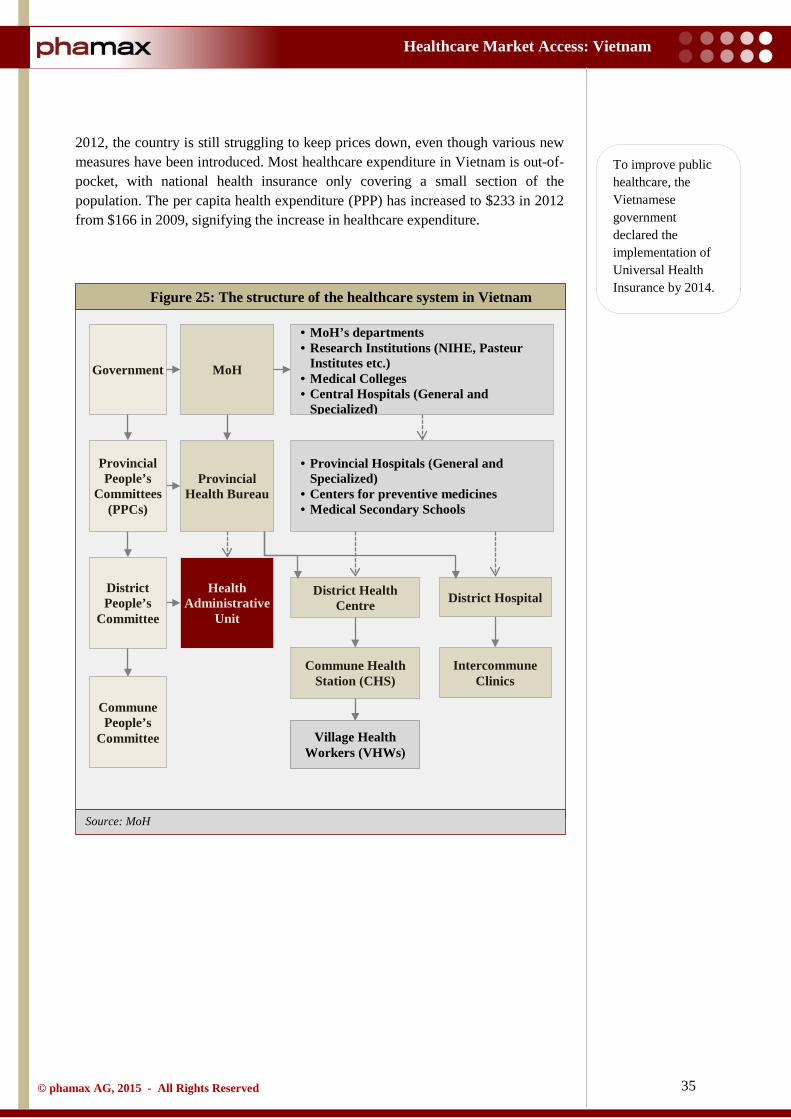
Since the introduction of the economic reforms initiated by ‘Doi Moi’ in 1986, Vietnam has made steady progress in healthcare. The country’s health indicators are better, and continue to improve at rates that equal or surpass its peers. The health sector is seeing a dramatic transformation due to programs concentrated on alleviating poverty and growing the economy. Twenty years ago, the country’s healthcare was firmly controlled by the central government, like any other socialist healthcare system. But, due to the rapid growth of the private sector, larger role of out-of-pocket expenditures, and the ongoing decentralization process, the role of the Ministry of Health (MoH) to shape activities has diminished significantly.
Vietnam healthcare system is a mix of public and private systems, in which the public system plays a key role, especially in policy, prevention, research and training. The public healthcare administration is organized at three levels - central, principal and local. At the central level, the Ministry of Health (MoH) formulates and executes health policies. It also directly controls and finances research institutions, and general and specialized hospitals. At the provincial level, there are 63 provincial health bureaus that follow the MoH policies, but are a part of local provincial governments under the Provincial People’s Committees (PPCs). These provincial health bureaus manage the provincial hospitals and Centers for Preventive Medicine, while the PPCs control their administration and financial aspects. At the primary level, there are Commune Health Stations (CHS), Village Health Workers (VHW) and district hospitals. They provide basic services like primary care, including preventive care, access to drugs, family planning and overall health promotion in the community.
The public healthcare expenditure in Vietnam is funded by the state’s limited budget because it is still a developing country. State hospitals do not have access to modern equipment because of restricted budgets. Consequently, the quality of service in state hospitals is weak, and not enough to cover the demand of patients, especially from the province levels to commune levels. Hence, the optimum choice for healthcare is the private sector. For example, in 2012, the health expenditure accounted for 6.6% of GDP, wherein government expenditure was just 42.6% and the rest was private expenditure.
To counter the inclination towards the private healthcare sector, in 2009, the Vietnamese Government declared the implementation of Universal Health Insurance by 2014. Since 2010, the government has been working for universal coverage with Vietnamese Social Security, a government affiliated agency responsible for implementation of health insurance policy in the country.
The chief concern for the Vietnamese government is to make healthcare universal and affordable to its population, especially in the case of pharmaceutical prices, which account for a significant portion of annual expenditure on health. But, since
The public sector is unable to cater to patient demands and lacks quality due to limited budgets. Hence, private expenditure is comparatively higher.
Vietnam healthcare system is a mix of public and private systems. In the public sector, the healthcare administration is organized at three levels: central, provincial and local.
35
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: MoH
2012, the country is still struggling to keep prices down, even though various new measures have been introduced. Most healthcare expenditure in Vietnam is out-of-pocket, with national health insurance only covering a small section of the population. The per capita health expenditure (PPP) has increased to $233 in 2012 from $166 in 2009, signifying the increase in healthcare expenditure.
Figure 25: The structure of the healthcare system in Vietnam
To improve public healthcare, the Vietnamese government declared the implementation of Universal Health Insurance by 2014.
Government
Provincial People’s
Committees (PPCs)
District People’s
Committee
Commune People’s
Committee
MoH
Intercommune Clinics
Commune Health Station (CHS)
District Hospital District Health Centre
Provincial Health Bureau
• MoH’s departments • Research Institutions (NIHE, Pasteur
Institutes etc.) • Medical Colleges • Central Hospitals (General and
Specialized)
• Provincial Hospitals (General and Specialized)
• Centers for preventive medicines • Medical Secondary Schools
Health Administrative
Unit
Village Health Workers (VHWs)
36
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: World Bank
Source: World Bank
2.2 Health status
The health status in Vietnam has shown improvement in the recent years, which is clearly evident in health indicators like average life expectancy at birth, mortality rate under the age of five years, maternal mortality ratio and malnutrition. These progresses are consequences of widespread healthcare delivery networks, increased number of qualified health workers and the expanding national public health programs.
2.2.1 Life expectancy
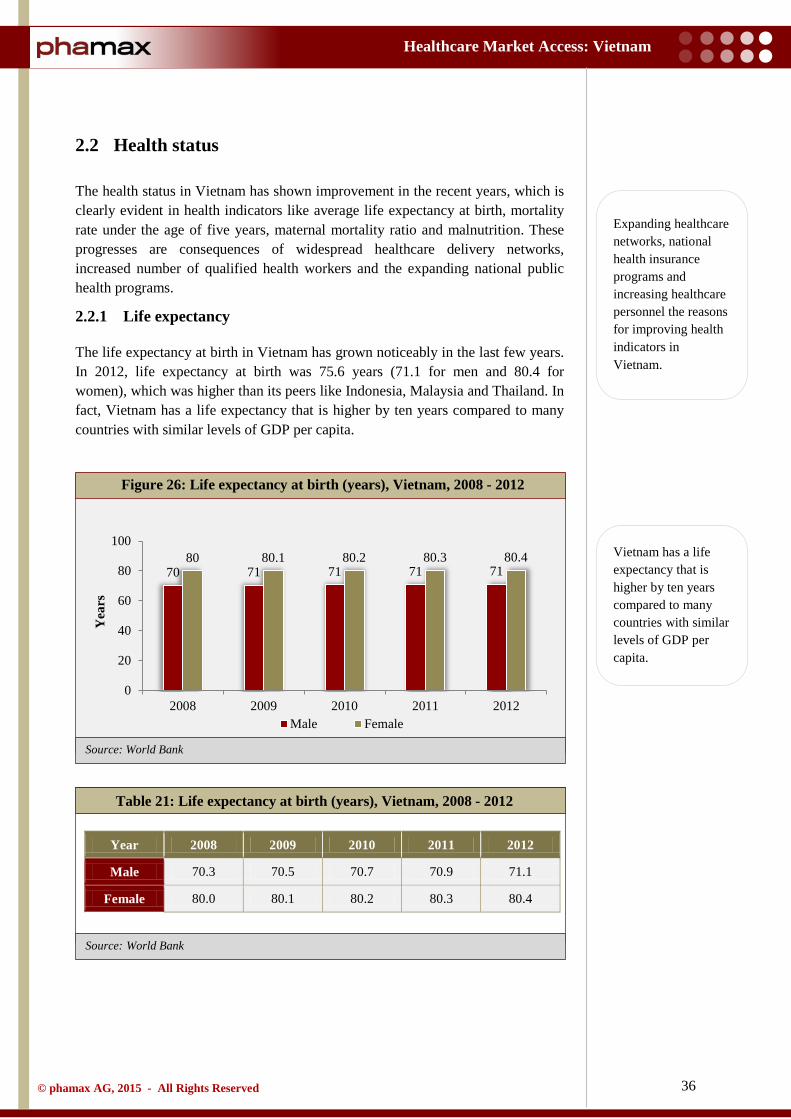
The life expectancy at birth in Vietnam has grown noticeably in the last few years. In 2012, life expectancy at birth was 75.6 years (71.1 for men and 80.4 for women), which was higher than its peers like Indonesia, Malaysia and Thailand. In fact, Vietnam has a life expectancy that is higher by ten years compared to many countries with similar levels of GDP per capita.
Table 21: Life expectancy at birth (years), Vietnam, 2008 - 2012
Year 2008 2009 2010 2011 2012
Male 70.3 70.5 70.7 70.9 71.1
Female 80.0 80.1 80.2 80.3 80.4
Figure 26: Life expectancy at birth (years), Vietnam, 2008 - 2012
70 71 71 71 71 80 80.1 80.2 80.3 80.4
0
20
40
60
80
100
2008 2009 2010 2011 2012
Yea
rs
Male Female
Vietnam has a life expectancy that is higher by ten years compared to many countries with similar levels of GDP per capita.
Expanding healthcare networks, national health insurance programs and increasing healthcare personnel the reasons for improving health indicators in Vietnam.
37
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: World Bank
Source: World Bank
2.2.2 Mortality rate
In confirmation with World Bank data, infant mortality rate (per 1,000 live births) during 2008 - 2012 declined from 19.2% to 18.7% in Vietnam. Although infant mortality rates have dropped in all regions, there are variations - the Northwest and Central Highlands have higher infant mortality rates and slower reductions in infant mortality compared to the national average. The rapid decline in the infant mortality rate has also contributed in reducing the mortality rate in the under-five age group in the country.
Currently, the under-five mortality rate is similar to that of countries with GDP per capita three to four times higher than Vietnam. The country had managed to reduce the under-five mortality rate from 24% in 2008 to 23% in 2012, and the goal for 2015 is to reduce it to 19%.
Table 22: Mortality rate, Vietnam, 2008 - 2012
Year 2008 2009 2010 2011 2012
Infant 19.2 18.9 18.7 18.6 18.4
Under 5 24.0 23.6 23.4 23.2 23.0
Largely, the mortality rate is on an unceasing decline. Many communicable diseases, especially vaccine preventable diseases (diphtheria, pertussis, encephalitis etc.), gastro-intestinal diseases (typhoid, dysentery etc.) and meningitis have plunged markedly compared to the former decade. On the other hand, morbidity and mortality patterns are displaying increased incidence and prevalence of chronic and non-communicable diseases. Also, accidents and injuries account for a large proportion of adult mortality in the country. In 2012, mortality rate of males in Vietnam was as high as 189 per 1,000 adults, while female mortality rate was a moderate 69 per 1,000 adults.
Figure 27: Mortality rate, Vietnam, 2008 - 2012
19.2 18.9 18.7 18.6 18.4
24.0 23.6 23.4 23.2 23.0
0
10
20
30
2008 2009 2010 2011 2012
Mor
talit
y ra
te
(per
1,0
00)
Infant Under 5
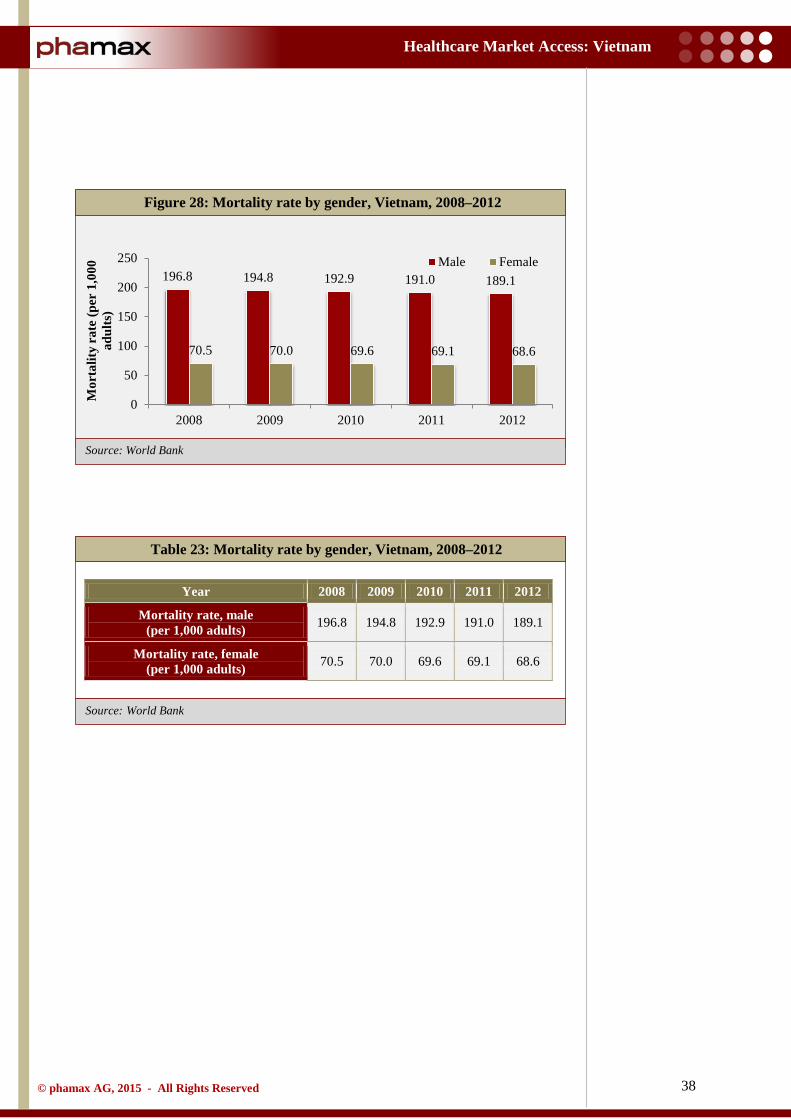
38
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: World Bank
Source: World Bank
Table 23: Mortality rate by gender, Vietnam, 2008–2012
Year 2008 2009 2010 2011 2012
Mortality rate, male (per 1,000 adults) 196.8 194.8 192.9 191.0 189.1
Mortality rate, female (per 1,000 adults) 70.5 70.0 69.6 69.1 68.6
Figure 28: Mortality rate by gender, Vietnam, 2008–2012
196.8 194.8 192.9 191.0 189.1
70.5 70.0 69.6 69.1 68.6
0
50
100
150
200
250
2008 2009 2010 2011 2012
Mor
talit
y ra
te (p
er 1
,000
ad
ults
)
Male Female
39
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
2.3 Healthcare policy
The health sector of Vietnam has been effective enough in providing crucial anticipatory health services, specifically for controlling crucial communicable diseases. But, there are still challenges to surmount and reforms to bring in. At the same time, although there is clarity over the goals of government policy on health, there is also an ongoing debate on strategies to achieve these goals.
Health policy goals in Vietnam are reflected in a number of documents, including the Socio-Economic Development Plan 2011 – 2020. The goals align with the four basic health system goals defined by the World Health Organization, which are:
• Improve people’s health • Improve system responsiveness • Protect people from financial risks • Raise the efficiency of the entire system
Vietnam’s Five Year Health Sector Development Plan 2011 - 2015 provides a framework for the government’s health policy. It was developed keeping in mind major socio-economic development orientations and tasks undertaken by the government focused towards the health sector. The key aims of the government’s policy are to achieve universal health insurance cover, improve healthcare infrastructure, address the discriminations in healthcare provisions and inefficiencies in delivery of healthcare and financing of healthcare. General objectives under this plan are to: • Consolidate the healthcare network at all levels, and continue to invest in
upgrading the healthcare system capabilities, with priority to healthcare networks in remote and isolated areas
• Promote preventive medicine and primary healthcare, assuring access to the best basic healthcare services
• Develop the quality of health examinations and treatments with balanced basic and universal healthcare services
• Create awareness on population control and family planning, reproductive health and mitigating imbalance of sex ratio
• Promote the healthcare human resources sector in terms of quality and quantity as per the actual needs of the healthcare industry, with vital focus on remote and isolated areas and specialties like paraclinical, preventive medicine and pediatric care, health education and communications, and counseling
• Concentrate the healthcare financing mechanism towards increased public expenditure to develop the universal health insurance scheme, leading to an increased budget allocation for healthcare and hence increase in public sector healthcare facilities
• Cultivate the pharmaceutical industry and domestic production of medical equipment, strengthening effective use and management of drugs, bio-medical products and medical devices • Strengthen management capacity to tackle health sector reforms and bring
in developments adhering to the modern demands
Vietnam’s Five Year Health Sector Development Plan 2011 - 2015 provides a framework of the government’s health policy.
The key aims of the government’s policy are to achieve universal health insurance cover, improve healthcare infrastructure, and address the discriminations in healthcare provisions and inefficiencies in delivery of healthcare and financing of healthcare.
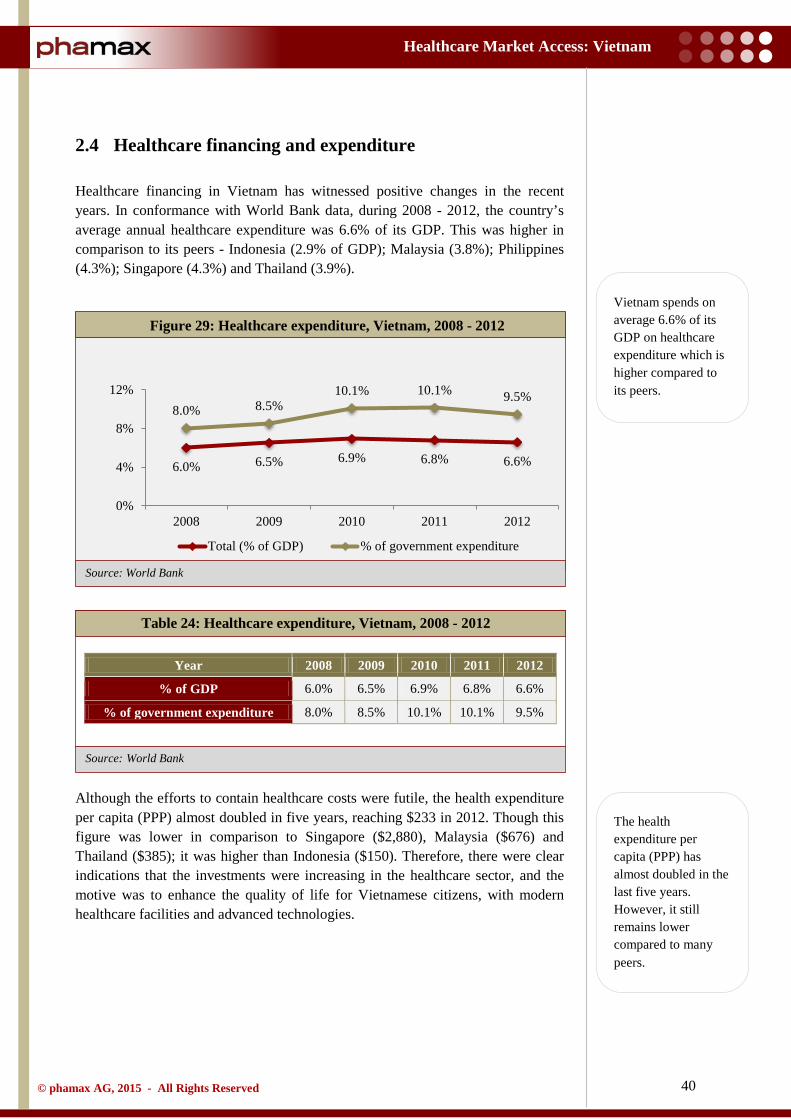
40
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: World Bank
Source: World Bank
2.4 Healthcare financing and expenditure
Healthcare financing in Vietnam has witnessed positive changes in the recent years. In conformance with World Bank data, during 2008 - 2012, the country’s average annual healthcare expenditure was 6.6% of its GDP. This was higher in comparison to its peers - Indonesia (2.9% of GDP); Malaysia (3.8%); Philippines (4.3%); Singapore (4.3%) and Thailand (3.9%).
Table 24: Healthcare expenditure, Vietnam, 2008 - 2012
Year 2008 2009 2010 2011 2012
% of GDP 6.0% 6.5% 6.9% 6.8% 6.6%
% of government expenditure 8.0% 8.5% 10.1% 10.1% 9.5%
Although the efforts to contain healthcare costs were futile, the health expenditure per capita (PPP) almost doubled in five years, reaching $233 in 2012. Though this figure was lower in comparison to Singapore ($2,880), Malaysia ($676) and Thailand ($385); it was higher than Indonesia ($150). Therefore, there were clear indications that the investments were increasing in the healthcare sector, and the motive was to enhance the quality of life for Vietnamese citizens, with modern healthcare facilities and advanced technologies.
Figure 29: Healthcare expenditure, Vietnam, 2008 - 2012
6.0% 6.5% 6.9% 6.8% 6.6%
8.0% 8.5% 10.1% 10.1% 9.5%
0%
4%
8%
12%
2008 2009 2010 2011 2012
Total (% of GDP) % of government expenditure
Vietnam spends on average 6.6% of its GDP on healthcare expenditure which is higher compared to its peers.
The health expenditure per capita (PPP) has almost doubled in the last five years. However, it still remains lower compared to many peers.
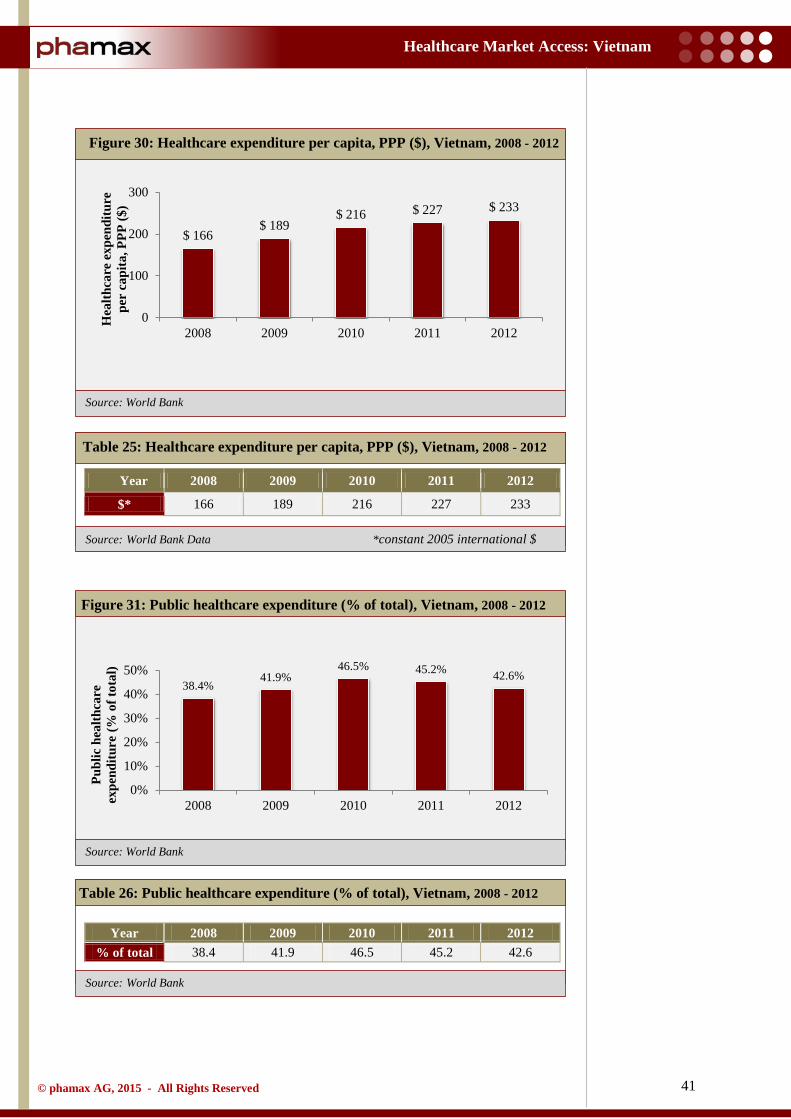
41
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: World Bank
Source: World Bank Data *constant 2005 international $
Source: World Bank
Source: World Bank
Table 25: Healthcare expenditure per capita, PPP ($), Vietnam, 2008 - 2012
Table 26: Public healthcare expenditure (% of total), Vietnam, 2008 - 2012
Year 2008 2009 2010 2011 2012 % of total 38.4 41.9 46.5 45.2 42.6
Figure 30: Healthcare expenditure per capita, PPP ($), Vietnam, 2008 - 2012
Year 2008 2009 2010 2011 2012
$* 166 189 216 227 233
Figure 31: Public healthcare expenditure (% of total), Vietnam, 2008 - 2012
$ 166 $ 189
$ 216 $ 227 $ 233
0
100
200
300
2008 2009 2010 2011 2012
Hea
lthca
re e
xpen
ditu
re
per
capi
ta, P
PP ($
)
38.4% 41.9%
46.5% 45.2% 42.6%
0%
10%
20%
30%
40%
50%
2008 2009 2010 2011 2012
Publ
ic h
ealth
care
ex
pend
iture
(% o
f tot
al)
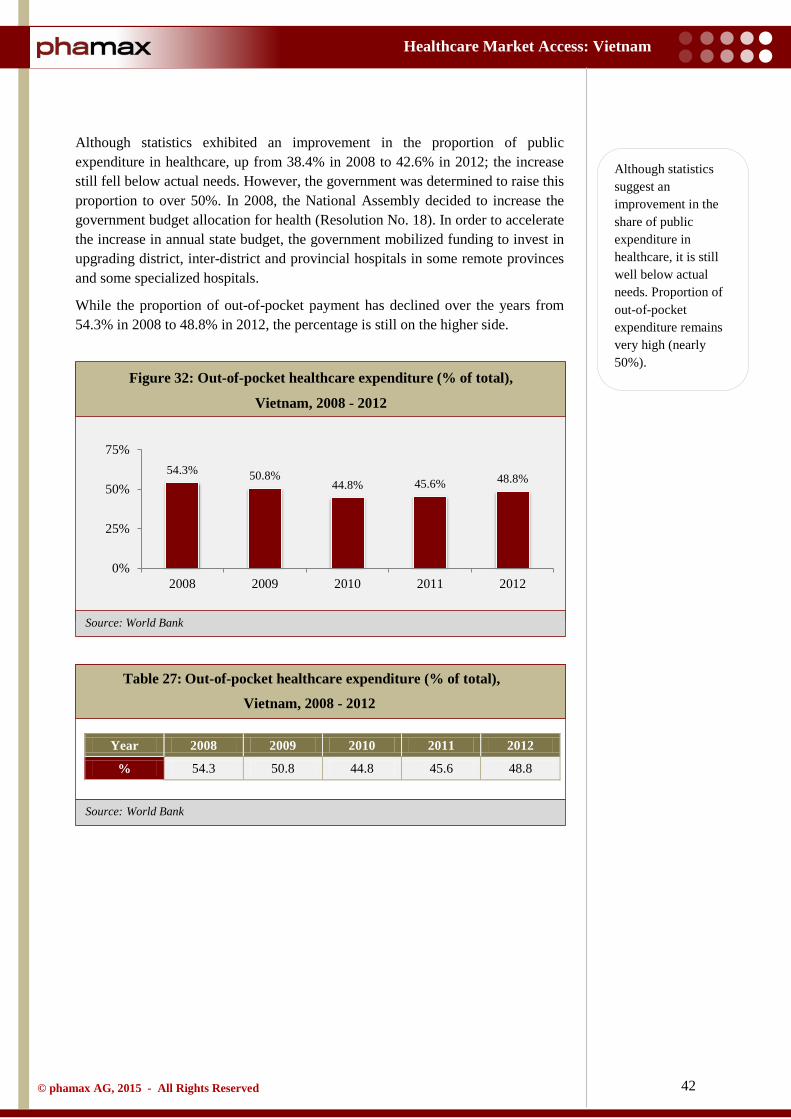
42
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: World Bank
Source: World Bank
Although statistics exhibited an improvement in the proportion of public expenditure in healthcare, up from 38.4% in 2008 to 42.6% in 2012; the increase still fell below actual needs. However, the government was determined to raise this proportion to over 50%. In 2008, the National Assembly decided to increase the government budget allocation for health (Resolution No. 18). In order to accelerate the increase in annual state budget, the government mobilized funding to invest in upgrading district, inter-district and provincial hospitals in some remote provinces and some specialized hospitals.
While the proportion of out-of-pocket payment has declined over the years from 54.3% in 2008 to 48.8% in 2012, the percentage is still on the higher side.
Table 27: Out-of-pocket healthcare expenditure (% of total),
Vietnam, 2008 - 2012
Year 2008 2009 2010 2011 2012
% 54.3 50.8 44.8 45.6 48.8
Figure 32: Out-of-pocket healthcare expenditure (% of total),
Vietnam, 2008 - 2012
54.3% 50.8% 44.8% 45.6% 48.8%
0%
25%
50%
75%
2008 2009 2010 2011 2012
Although statistics suggest an improvement in the share of public expenditure in healthcare, it is still well below actual needs. Proportion of out-of-pocket expenditure remains very high (nearly 50%).
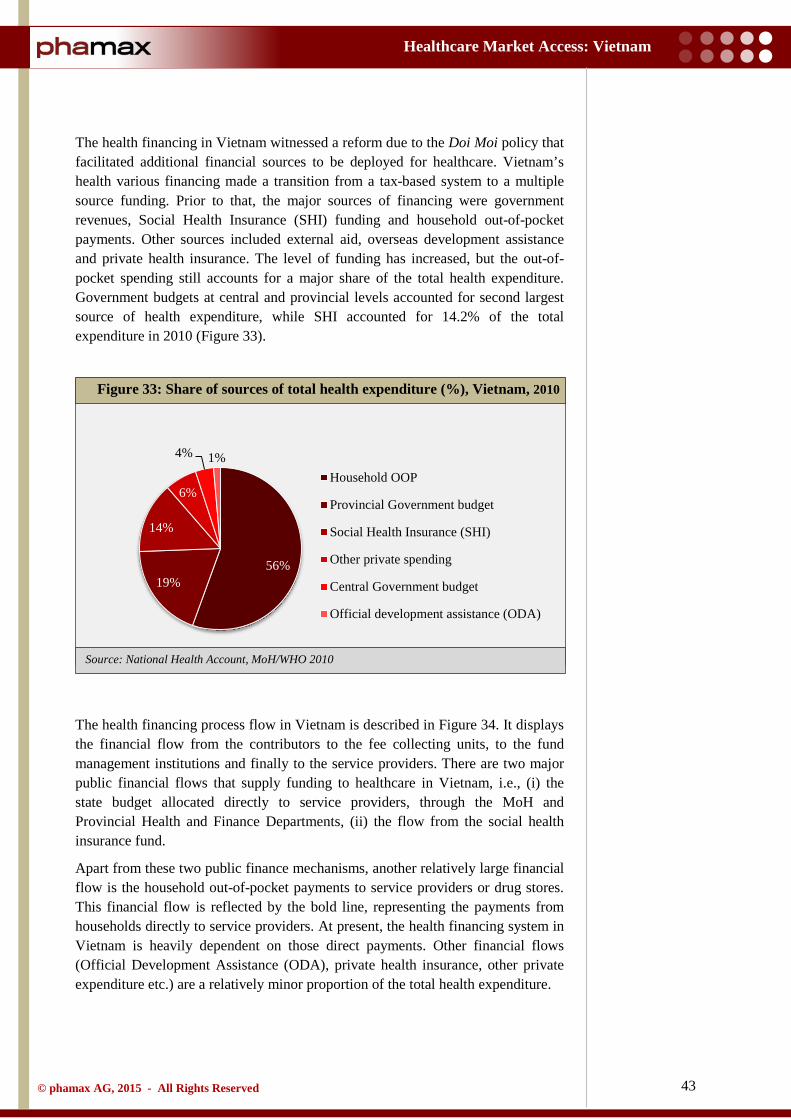
43
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: National Health Account, MoH/WHO 2010
The health financing in Vietnam witnessed a reform due to the Doi Moi policy that facilitated additional financial sources to be deployed for healthcare. Vietnam’s health various financing made a transition from a tax-based system to a multiple source funding. Prior to that, the major sources of financing were government revenues, Social Health Insurance (SHI) funding and household out-of-pocket payments. Other sources included external aid, overseas development assistance and private health insurance. The level of funding has increased, but the out-of-pocket spending still accounts for a major share of the total health expenditure. Government budgets at central and provincial levels accounted for second largest source of health expenditure, while SHI accounted for 14.2% of the total expenditure in 2010 (Figure 33).
The health financing process flow in Vietnam is described in Figure 34. It displays the financial flow from the contributors to the fee collecting units, to the fund management institutions and finally to the service providers. There are two major public financial flows that supply funding to healthcare in Vietnam, i.e., (i) the state budget allocated directly to service providers, through the MoH and Provincial Health and Finance Departments, (ii) the flow from the social health insurance fund.
Apart from these two public finance mechanisms, another relatively large financial flow is the household out-of-pocket payments to service providers or drug stores. This financial flow is reflected by the bold line, representing the payments from households directly to service providers. At present, the health financing system in Vietnam is heavily dependent on those direct payments. Other financial flows (Official Development Assistance (ODA), private health insurance, other private expenditure etc.) are a relatively minor proportion of the total health expenditure.
Figure 33: Share of sources of total health expenditure (%), Vietnam, 2010
56% 19%
14%
6%
4% 1% Household OOP
Provincial Government budget
Social Health Insurance (SHI)
Other private spending
Central Government budget
Official development assistance (ODA)
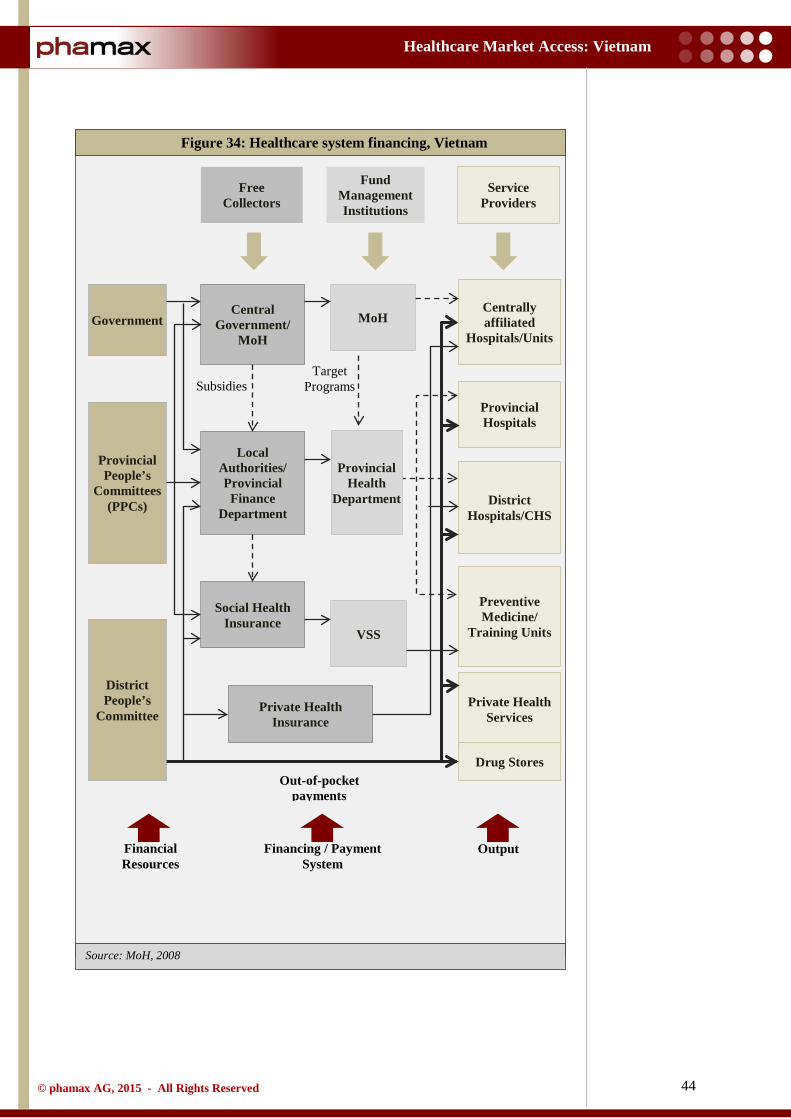
44
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: MoH, 2008
Figure 34: Healthcare system financing, Vietnam
Government
Provincial People’s
Committees (PPCs)
Central Government/
MoH
Social Health Insurance
Local Authorities/ Provincial
Finance Department
MoH
VSS
Private Health Insurance
Free Collectors
Service Providers
Fund Management Institutions
Centrally affiliated
Hospitals/Units
Provincial Hospitals
District Hospitals/CHS
Private Health Services
Preventive Medicine/
Training Units
Drug Stores
District People’s
Committee
Provincial Health
Department
Subsidies Target
Programs
Out-of-pocket payments
Financial Resources
Financing / Payment System
Output
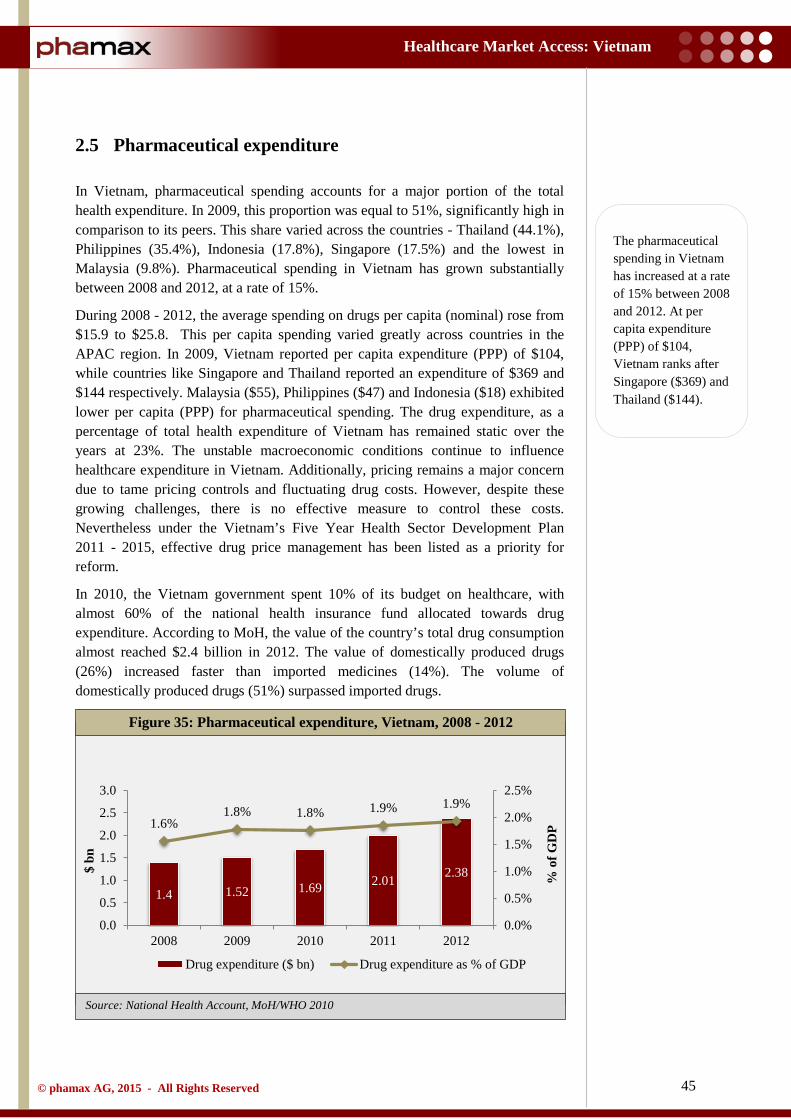
45
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: National Health Account, MoH/WHO 2010
2.5 Pharmaceutical expenditure
In Vietnam, pharmaceutical spending accounts for a major portion of the total health expenditure. In 2009, this proportion was equal to 51%, significantly high in comparison to its peers. This share varied across the countries - Thailand (44.1%), Philippines (35.4%), Indonesia (17.8%), Singapore (17.5%) and the lowest in Malaysia (9.8%). Pharmaceutical spending in Vietnam has grown substantially between 2008 and 2012, at a rate of 15%.
During 2008 - 2012, the average spending on drugs per capita (nominal) rose from $15.9 to $25.8. This per capita spending varied greatly across countries in the APAC region. In 2009, Vietnam reported per capita expenditure (PPP) of $104, while countries like Singapore and Thailand reported an expenditure of $369 and $144 respectively. Malaysia ($55), Philippines ($47) and Indonesia ($18) exhibited lower per capita (PPP) for pharmaceutical spending. The drug expenditure, as a percentage of total health expenditure of Vietnam has remained static over the years at 23%. The unstable macroeconomic conditions continue to influence healthcare expenditure in Vietnam. Additionally, pricing remains a major concern due to tame pricing controls and fluctuating drug costs. However, despite these growing challenges, there is no effective measure to control these costs. Nevertheless under the Vietnam’s Five Year Health Sector Development Plan 2011 - 2015, effective drug price management has been listed as a priority for reform.
In 2010, the Vietnam government spent 10% of its budget on healthcare, with almost 60% of the national health insurance fund allocated towards drug expenditure. According to MoH, the value of the country’s total drug consumption almost reached $2.4 billion in 2012. The value of domestically produced drugs (26%) increased faster than imported medicines (14%). The volume of domestically produced drugs (51%) surpassed imported drugs.
Figure 35: Pharmaceutical expenditure, Vietnam, 2008 - 2012
1.4 1.52 1.69 2.01 2.38
1.6% 1.8% 1.8% 1.9% 1.9%
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
0.0
0.5
1.0
1.5
2.0
2.5
3.0
2008 2009 2010 2011 2012
% o
f GD
P
$ bn
Drug expenditure ($ bn) Drug expenditure as % of GDP
The pharmaceutical spending in Vietnam has increased at a rate of 15% between 2008 and 2012. At per capita expenditure (PPP) of $104, Vietnam ranks after Singapore ($369) and Thailand ($144).
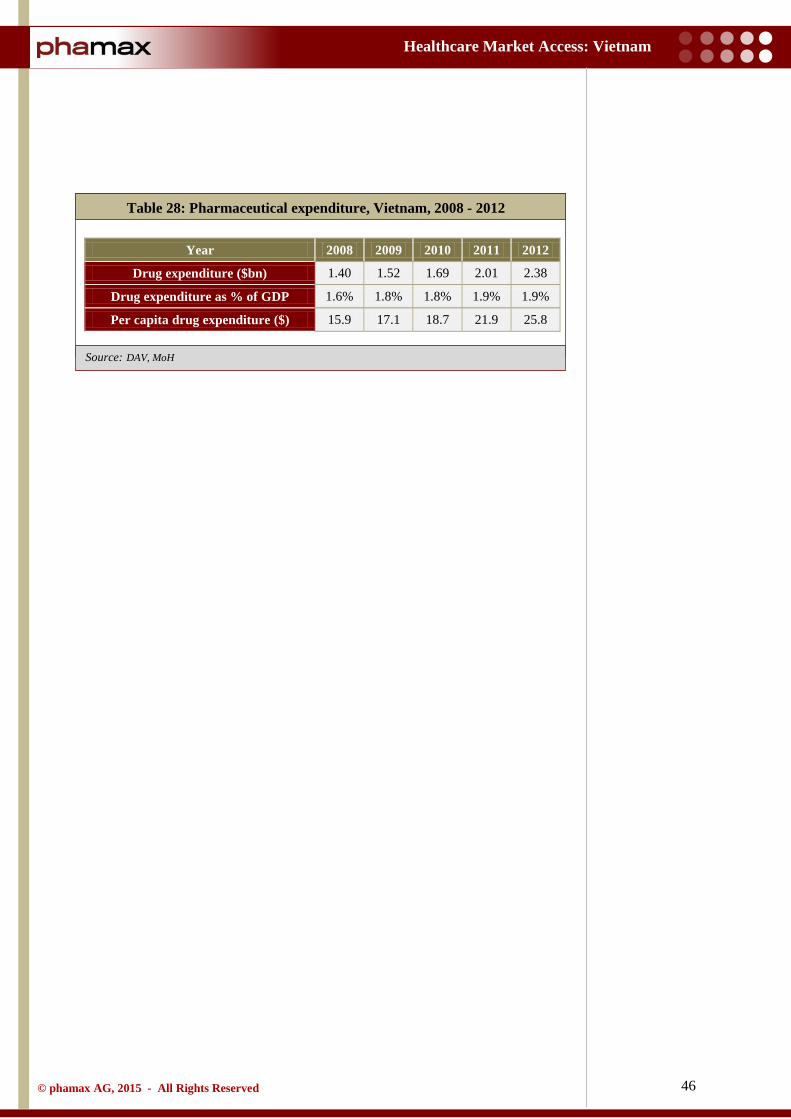
46
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: DAV, MoH
Table 28: Pharmaceutical expenditure, Vietnam, 2008 - 2012
Year 2008 2009 2010 2011 2012
Drug expenditure ($bn) 1.40 1.52 1.69 2.01 2.38
Drug expenditure as % of GDP 1.6% 1.8% 1.8% 1.9% 1.9%
Per capita drug expenditure ($) 15.9 17.1 18.7 21.9 25.8
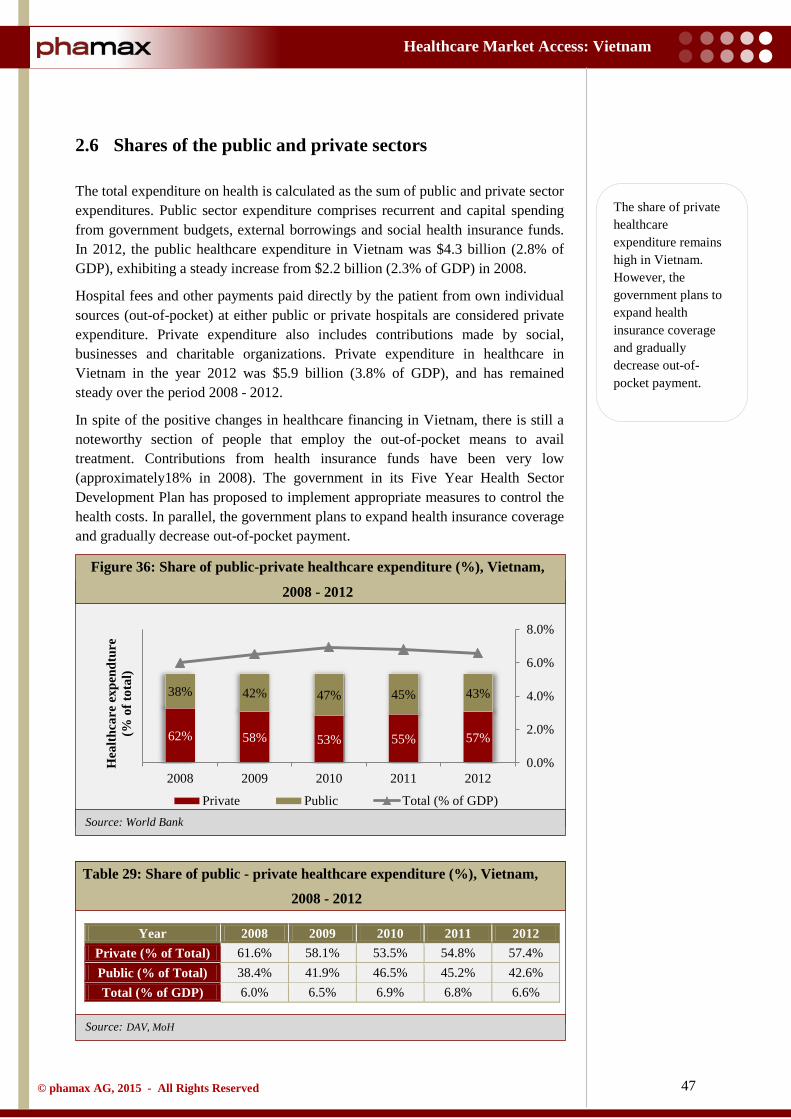
47
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: World Bank
Source: DAV, MoH
2.6 Shares of the public and private sectors
The total expenditure on health is calculated as the sum of public and private sector expenditures. Public sector expenditure comprises recurrent and capital spending from government budgets, external borrowings and social health insurance funds. In 2012, the public healthcare expenditure in Vietnam was $4.3 billion (2.8% of GDP), exhibiting a steady increase from $2.2 billion (2.3% of GDP) in 2008.
Hospital fees and other payments paid directly by the patient from own individual sources (out-of-pocket) at either public or private hospitals are considered private expenditure. Private expenditure also includes contributions made by social, businesses and charitable organizations. Private expenditure in healthcare in Vietnam in the year 2012 was $5.9 billion (3.8% of GDP), and has remained steady over the period 2008 - 2012.
In spite of the positive changes in healthcare financing in Vietnam, there is still a noteworthy section of people that employ the out-of-pocket means to avail treatment. Contributions from health insurance funds have been very low (approximately18% in 2008). The government in its Five Year Health Sector Development Plan has proposed to implement appropriate measures to control the health costs. In parallel, the government plans to expand health insurance coverage and gradually decrease out-of-pocket payment.
Table 29: Share of public - private healthcare expenditure (%), Vietnam,
2008 - 2012
Year 2008 2009 2010 2011 2012 Private (% of Total) 61.6% 58.1% 53.5% 54.8% 57.4% Public (% of Total) 38.4% 41.9% 46.5% 45.2% 42.6% Total (% of GDP) 6.0% 6.5% 6.9% 6.8% 6.6%
Figure 36: Share of public-private healthcare expenditure (%), Vietnam,
2008 - 2012
62% 58% 53% 55% 57%
38% 42% 47% 45% 43%
0.0%
2.0%
4.0%
6.0%
8.0%
2008 2009 2010 2011 2012
Hea
lthca
re e
xpen
dtur
e (%
of t
otal
)
Private Public Total (% of GDP)
The share of private healthcare expenditure remains high in Vietnam. However, the government plans to expand health insurance coverage and gradually decrease out-of-pocket payment.

48
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
2.7 Spending in pharmaceutical R&D
Local pharmaceutical companies in Vietnam have a shortage in expertise and the relevant financial support to facilitate pharmaceutical Research and Development (R&D). Furthermore, these companies are reluctant on investing on R&D because of the vast spending involved and the time frame that is usually associated with the development cycle of a new, patented drug.
The funds allocated for R&D in 2010 in Vietnam was less than 3% of the total revenue, lower than other Asian countries (about 5%) and global average (12% -16%). Although the government made declarations in the Five Year Socio-Economic Development Plan 2005 - 2010 that they ‘plan to accelerate research and apply technological advances to increase productivity, generate jobs and produce goods for consumption, production and export’, no quantifiable objectives have been set as yet. Consequently with no facility, subsidy, expertise, money and long-term vision, Vietnamese pharmaceutical companies have zero or no interest in the R&D sector. This scenario is not expected to change very soon.
Local pharmaceutical companies lack the expertise as well as the finance for R&D.
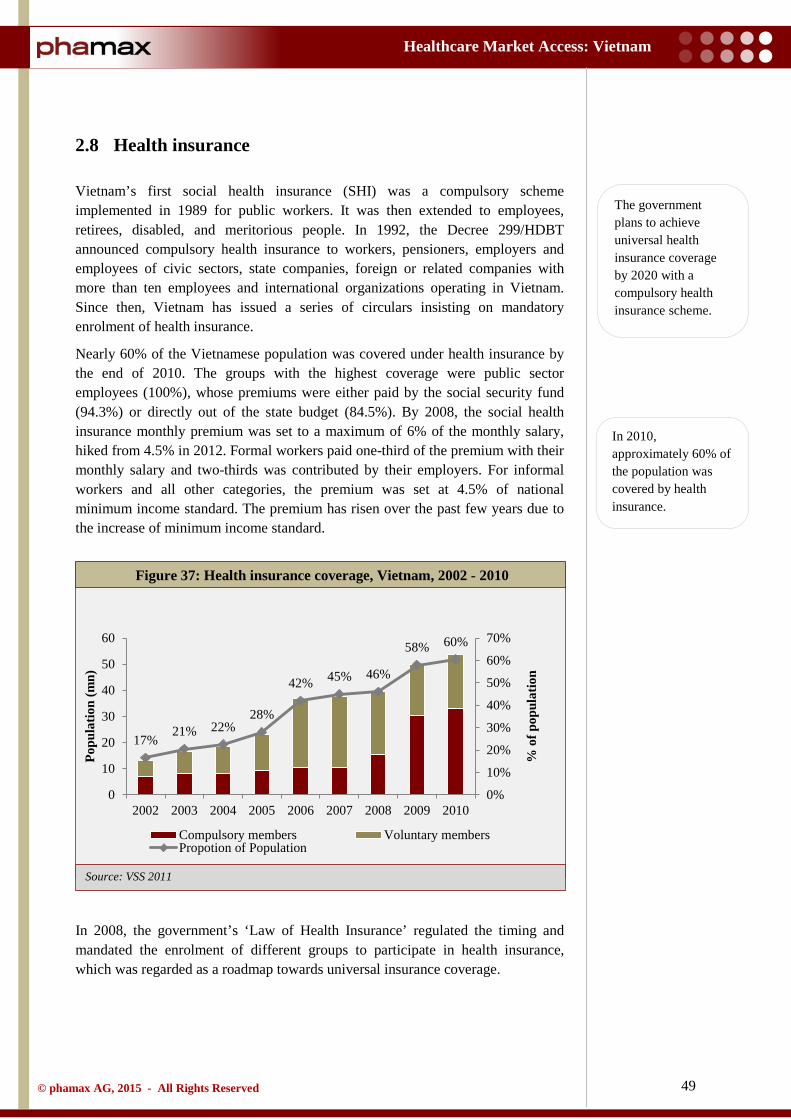
49
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: VSS 2011
2.8 Health insurance
Vietnam’s first social health insurance (SHI) was a compulsory scheme implemented in 1989 for public workers. It was then extended to employees, retirees, disabled, and meritorious people. In 1992, the Decree 299/HDBT announced compulsory health insurance to workers, pensioners, employers and employees of civic sectors, state companies, foreign or related companies with more than ten employees and international organizations operating in Vietnam. Since then, Vietnam has issued a series of circulars insisting on mandatory enrolment of health insurance.
Nearly 60% of the Vietnamese population was covered under health insurance by the end of 2010. The groups with the highest coverage were public sector employees (100%), whose premiums were either paid by the social security fund (94.3%) or directly out of the state budget (84.5%). By 2008, the social health insurance monthly premium was set to a maximum of 6% of the monthly salary, hiked from 4.5% in 2012. Formal workers paid one-third of the premium with their monthly salary and two-thirds was contributed by their employers. For informal workers and all other categories, the premium was set at 4.5% of national minimum income standard. The premium has risen over the past few years due to the increase of minimum income standard.
In 2008, the government’s ‘Law of Health Insurance’ regulated the timing and mandated the enrolment of different groups to participate in health insurance, which was regarded as a roadmap towards universal insurance coverage.
Figure 37: Health insurance coverage, Vietnam, 2002 - 2010
17% 21% 22%
28%
42% 45% 46%
58% 60%
0%
10%
20%
30%
40%
50%
60%
70%
0
10
20
30
40
50
60
2002 2003 2004 2005 2006 2007 2008 2009 2010
% o
f pop
ulat
ion
Popu
latio
n (m
n)
Compulsory members Voluntary membersPropotion of Population
The government plans to achieve universal health insurance coverage by 2020 with a compulsory health insurance scheme.
In 2010, approximately 60% of the population was covered by health insurance.
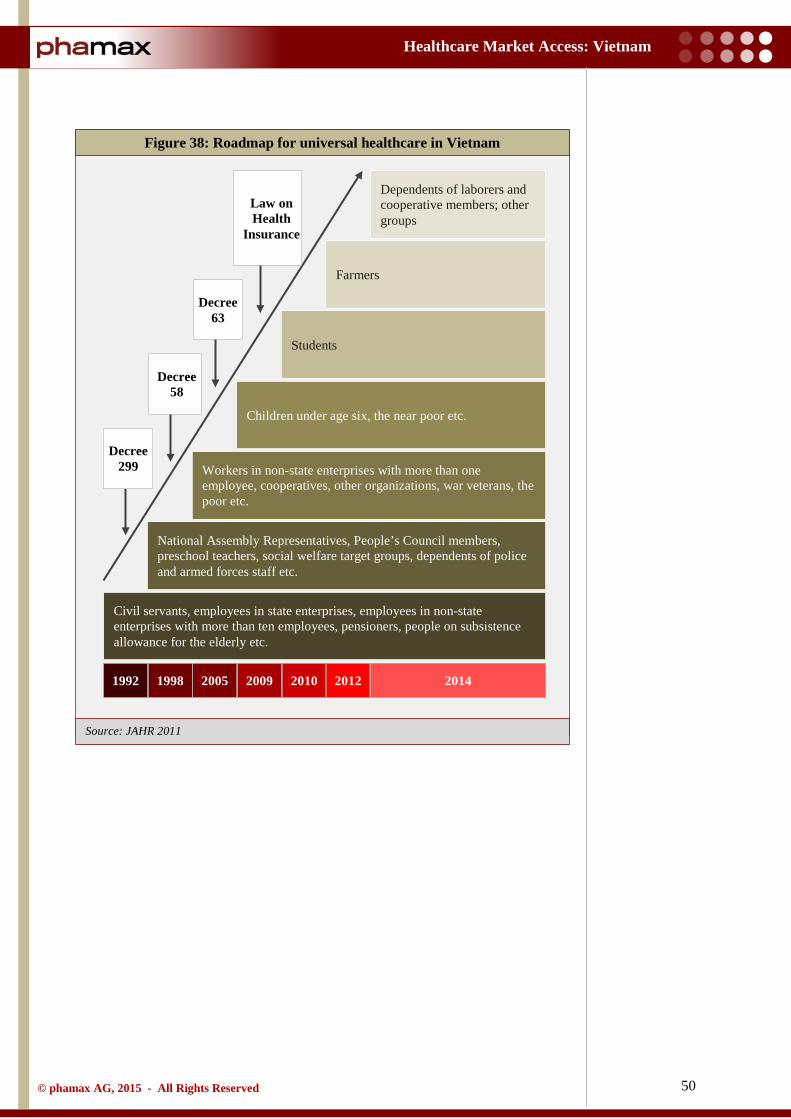
50
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: JAHR 2011
Figure 38: Roadmap for universal healthcare in Vietnam
Civil servants, employees in state enterprises, employees in non-state enterprises with more than ten employees, pensioners, people on subsistence allowance for the elderly etc.
1992 1998 2005 2009 2010 2012
National Assembly Representatives, People’s Council members, preschool teachers, social welfare target groups, dependents of police and armed forces staff etc.
Workers in non-state enterprises with more than one employee, cooperatives, other organizations, war veterans, the poor etc.
Children under age six, the near poor etc.
Students
Farmers
Dependents of laborers and cooperative members; other groups
2014
Decree 299
Decree 58
Decree 63
Law on Health
Insurance
51
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
The government has been promoting social health insurance, both through compulsory and voluntary schemes, with the ultimate goal of achieving universal health insurance coverage by 2020. However, the expectations were that the voluntary scheme would be discarded and completely replaced by the compulsory insurance scheme before 2014.
Since 2010, the government has been working towards universal health insurance coverage with Vietnam Social Security, a government-affiliated agency, responsible for implementing health insurance policy. In spite of the introduction of the ‘Law of Health Insurance’ in 2009, the extent of population coverage has been below expectations. In 2010, the number of the insured increased by 1.8% compared to 2009, which further went up to 3.1% in 2011.
Approximately 34 million people who were not a part of the health insurance schemes, mainly belonged to low participation groups, i.e., the near poor (even though the state provided a partial subsidy, participation only reached 13.1% amongst this group), farmers, dependents of workers, workers in cooperatives (33.4%) and workers in non-state enterprises (53.4%). For children under the age of six, even though 100% of their contribution was paid by the state budget, only 77.6% of the group was covered. School students who were entitled to a 30% subsidy, also had 76% coverage.
The Five Year Health Sector Plan (2011 - 2015) had set the goal to provide health insurance to 76% of Vietnam’s population by 2014 and 80% by 2015. But, fulfilling the objectives set as a part of the goal are hindered by some major challenges. Like other developing countries, majority of Vietnam’s population works in the informal sector. The share of household out-of-pocket (OOP) payments for health, despite its rapid decrease in recent years, is still on the higher side. Added to this, there are other bottlenecks in terms of institutional design and organizational practice. These may act as barriers to the ultimate goal of achieving universal health coverage.
The government expected several challenges in surpassing its goal of health insurance to 76% of population by 2014 and 80% of the population by 2015.

52
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
2.9 Hospital sector
The hospital system in Vietnam is organized widely based on convenience and accessibility. The hospital system is largely managed by the State. By the end of 2012, there were a total of 1,189 hospitals in the country (excluding the army hospital under the Department of Defense Management).
In 2012, the Vietnam healthcare system incorporated 13,630 large public and growing private curative care facilities that mainly included hospitals and clinics. The public sector dominated with a share of almost 90% of the total hospitals in the country, a remarkably large number compared to the private sector. The public health sector provided in-patient healthcare services with 1,030 hospitals and 178,401 patient beds. The private sector comprised 132 hospitals and 6,941 patient beds. As reported by General Statistics Office (GSO), Vietnam, the number of patient beds available per 10,000 inhabitants was 24.9 in 2012.
On the other hand, there has been substantial growth in the number of private hospitals in Vietnam since the government of Vietnam permitted private investment in the health segment. But, private hospitals still contribute less than 5% of the total hospital beds, and are unlikely to reach the projected target of 20% hospital beds (5 beds /10,000 persons) by 2020. The encouragement of the growth of private hospitals is a crucial aspect of the government’s ‘social mobilization’ policy, which has led to increased private investment in state hospitals. The ambition of this policy is to mobilize resources from within the society to invest in key public services, and allow all members of the community to reap the benefits.
Public hospitals are heavily subsidized in the state. They are usually backed with financial resources from the state budget allocation and health insurance, usually forming 60 - 70% of their revenues. In addition, public hospitals, especially the leading ones in Ho Chi Minh City and Hanoi, boast of a long history and enjoy a trustworthy reputation because of the finest trained, experienced doctors in the country. Contrarily, the private hospitals in Vietnam have a shorter history. The oldest ones were established in the late 90s. The perception about private hospitals is that they deliver superior services but they do not have good doctors as their public counterparts. Thus, private hospitals have to collaborate with doctors from public hospitals, especially in the early years of their operation, to attract clients before they build their own team of doctors and create their own portfolio of clients. Privatization of public hospitals in Vietnam has been a raging topic for more than a decade now, but the change is highly improbable because of strong opposition from doctors.
Despite the mushrooming number of private hospitals, public hospitals are still plagued by overcapacity. Many public hospitals are constantly operating at full capacity, with four to five patients allocated to a single bed. The bed capacity in Cho Ray Hospital in Ho Chi Minh City, stretched to 135% in 2013, while at the Ho Chi Minh City Oncology Hospital, there were 560 inpatients per 160 beds. On the other hand, private hospitals, though they are equipped with modern technology
Public hospitals are operating at full capacity and mostly overcrowded with many hospitals overburdened with four to five patients per bed.
The public sector dominates with almost 90% of the total hospitals in the country. The private hospitals contribute less than 5% of total hospital beds.
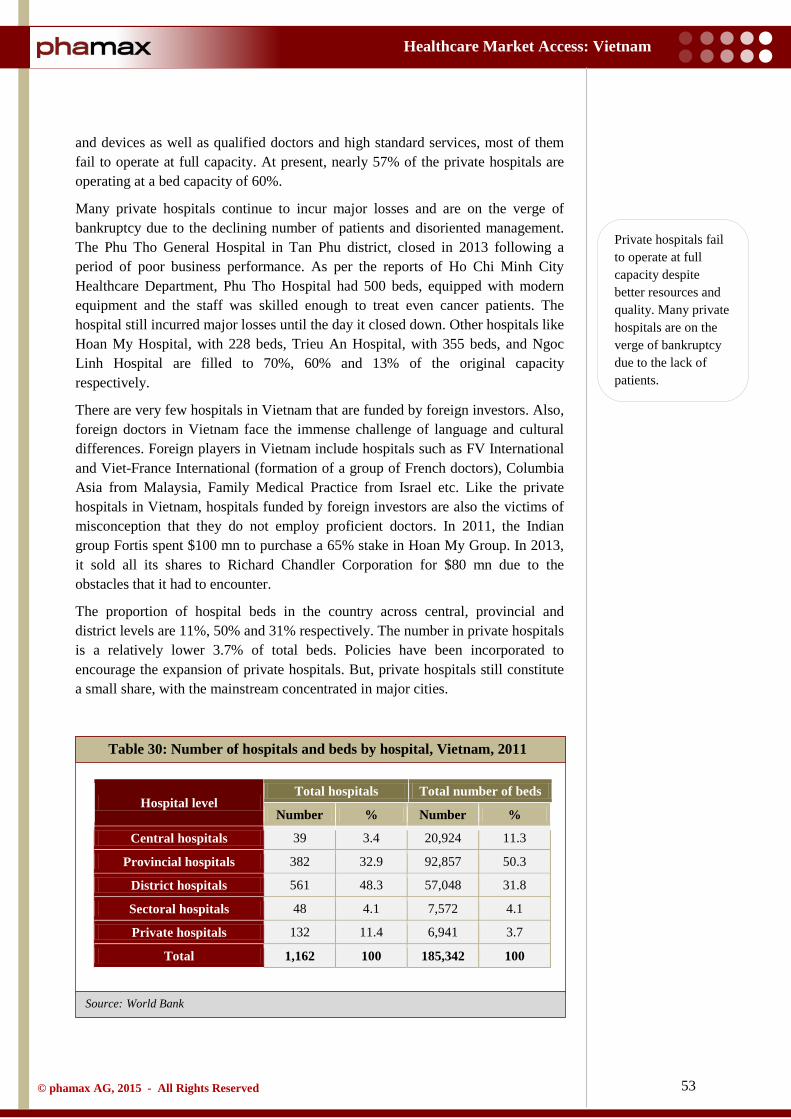
53
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: World Bank
and devices as well as qualified doctors and high standard services, most of them fail to operate at full capacity. At present, nearly 57% of the private hospitals are operating at a bed capacity of 60%.
Many private hospitals continue to incur major losses and are on the verge of bankruptcy due to the declining number of patients and disoriented management. The Phu Tho General Hospital in Tan Phu district, closed in 2013 following a period of poor business performance. As per the reports of Ho Chi Minh City Healthcare Department, Phu Tho Hospital had 500 beds, equipped with modern equipment and the staff was skilled enough to treat even cancer patients. The hospital still incurred major losses until the day it closed down. Other hospitals like Hoan My Hospital, with 228 beds, Trieu An Hospital, with 355 beds, and Ngoc Linh Hospital are filled to 70%, 60% and 13% of the original capacity respectively.
There are very few hospitals in Vietnam that are funded by foreign investors. Also, foreign doctors in Vietnam face the immense challenge of language and cultural differences. Foreign players in Vietnam include hospitals such as FV International and Viet-France International (formation of a group of French doctors), Columbia Asia from Malaysia, Family Medical Practice from Israel etc. Like the private hospitals in Vietnam, hospitals funded by foreign investors are also the victims of misconception that they do not employ proficient doctors. In 2011, the Indian group Fortis spent $100 mn to purchase a 65% stake in Hoan My Group. In 2013, it sold all its shares to Richard Chandler Corporation for $80 mn due to the obstacles that it had to encounter.
The proportion of hospital beds in the country across central, provincial and district levels are 11%, 50% and 31% respectively. The number in private hospitals is a relatively lower 3.7% of total beds. Policies have been incorporated to encourage the expansion of private hospitals. But, private hospitals still constitute a small share, with the mainstream concentrated in major cities.
Table 30: Number of hospitals and beds by hospital, Vietnam, 2011
Hospital level Total hospitals Total number of beds
Number % Number %
Central hospitals 39 3.4 20,924 11.3
Provincial hospitals 382 32.9 92,857 50.3
District hospitals 561 48.3 57,048 31.8
Sectoral hospitals 48 4.1 7,572 4.1
Private hospitals 132 11.4 6,941 3.7
Total 1,162 100 185,342 100
Private hospitals fail to operate at full capacity despite better resources and quality. Many private hospitals are on the verge of bankruptcy due to the lack of patients.
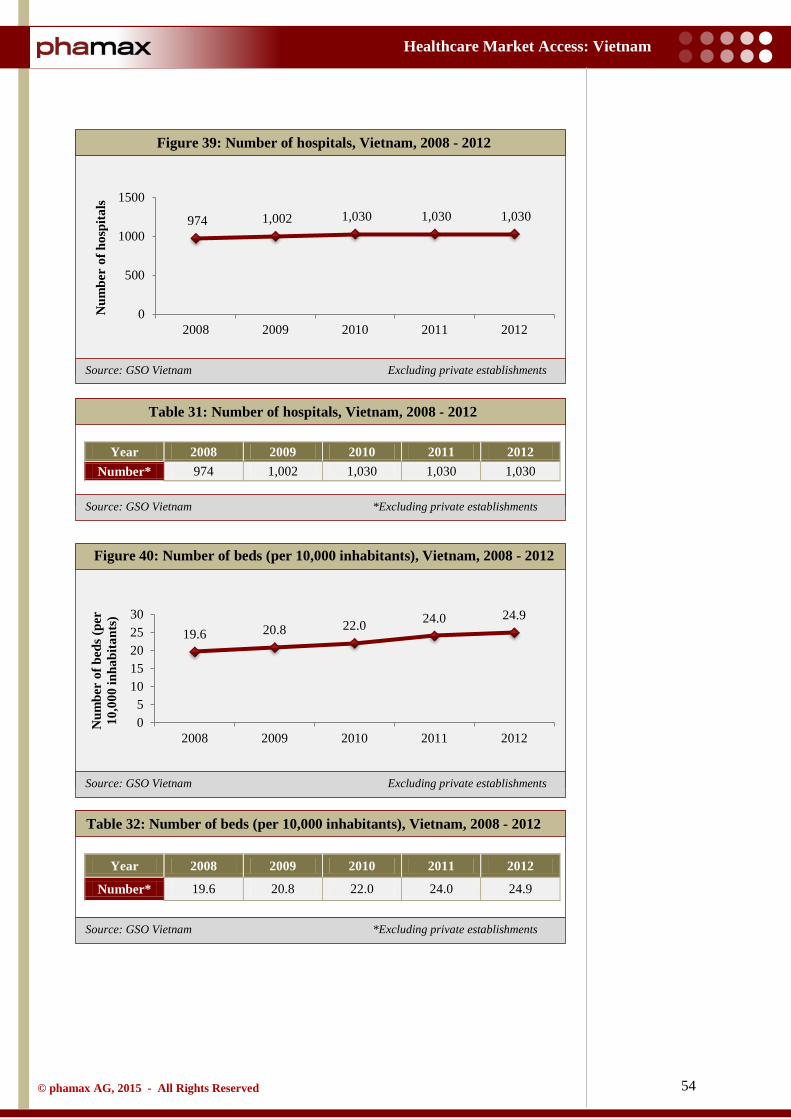
54
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: GSO Vietnam Excluding private establishments
Source: GSO Vietnam *Excluding private establishments
Source: GSO Vietnam Excluding private establishments
Source: GSO Vietnam *Excluding private establishments
Table 31: Number of hospitals, Vietnam, 2008 - 2012
Year 2008 2009 2010 2011 2012 Number* 974 1,002 1,030 1,030 1,030
Table 32: Number of beds (per 10,000 inhabitants), Vietnam, 2008 - 2012
Year 2008 2009 2010 2011 2012
Number* 19.6 20.8 22.0 24.0 24.9
Figure 39: Number of hospitals, Vietnam, 2008 - 2012
Figure 40: Number of beds (per 10,000 inhabitants), Vietnam, 2008 - 2012
974 1,002 1,030 1,030 1,030
0
500
1000
1500
2008 2009 2010 2011 2012
Num
ber
of h
ospi
tals
19.6 20.8 22.0 24.0 24.9
05
1015202530
2008 2009 2010 2011 2012
Num
ber
of b
eds (
per
10,0
00 in
habi
tant
s)
55
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
The number of clinics and hospital beds has increased relatively steadily over the years. As mentioned earlier in the report, most in-patient care is provided by public hospitals. But, recently there has been a budding number of private hospitals in major cities, increasing rivalry. Tertiary care is still principally provided by national hospitals, granting that there are a few provincial and private hospitals that have the capacity to provide highly specialized care. Private clinics account for a large share of out-patient care, but the majority still resorts to public hospitals. Thus, the Ministry of Health continues to channelize resources to counter the surplus and improve the quality of care and treatment.
Traditional medicine continues to be an integral part of the healthcare system in Vietnam. It is strongly backed by the Prime Minister’s directive issued in 2010, in conformance with the development of Vietnamese traditional medicine until the year 2020. Currently, there are 58 traditional medicine hospitals in the country. All provincial general hospitals and 90% of the district hospitals have a preventive medicine department or division and 85% of the commune health stations provide traditional medicine services. Three private hospitals and more than 10,000 traditional medicine clinics provide private traditional medicine services. Traditional medicine has expanded at a quick rate, accounting for 8.8% at the provincial level, 9.1% at the district level and 24.6% at the commune level as a share of total medical examinations, treatments and consultations in the country.
2.9.1 Major hospital profiles
As cited in the previous pages, Vietnam healthcare market is dominated by public hospitals. Private hospitals only account for 5% of the total hospital beds in the country. Only 102 (8%) of the 1,189 hospitals in Vietnam are private hospitals. Also, in 2011, private hospitals only accounted for 4.2% and 5.1% of the inpatient and outpatient count respectively. Few notable hospitals in the country are summarized below:
2.9.1.1 Bach Mai Hospital
It is a multi-field medical facility in Hanoi and is considered one of the largest in Vietnam. It has two institutes covering 21 clinical departments, six paraclinical departments, nine functional departments and one nursing school. The hospital specializes in examination and treatment of patients with quality care, training, guiding lower level hospitals, scientific research, international cooperation for healthcare, epidemic prevention and health-economic management. In 2012, the hospital had 1,900 beds and employed 2,100 staff members, including 470 doctors, 1,020 nurses, technicians, mid-wives and 55 pharmacists.
Traditional medicine continues to be an integral part of the healthcare system in Vietnam.

56
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
2.9.1.2 Cho Ray Hospital
Cho Ray Hospital is the largest general hospital in Ho Chi Minh City. The facility is constructed on an area of 53,000 square meters. The hospital has 35 clinical, 11 subclinical and 8 functional departments. It organizes practice and postgraduate training for more than 2,500 medical students and 600 doctors each year. The hospital has 1200 beds, employs 2,270 health workers including 500 medical doctors and pharmacists, and provides treatment for about 457,000 outpatients and 67,000 inpatients per year.
2.9.1.3 Hue Central Hospital (HCH)
Hue Central Hospital (HCH) is the first western hospital in Vietnam, established in 1894. It is situated in an area of 120,000 square meters, and is one of the three largest in the country along with Bạch Mai Hospital and Cho Ray Hospital. It is managed by the Ministry of Health. Positioned as a top referral hospital, it is a central medical institution for the 15.3 million constituting the central Vietnamese population. It is also the primary training facility for the Hue Medical College. The hospital has 2,078 beds and has a total staff of 2,500, including 431 doctors and pharmacists and 42 professors. They are supplemented by 152 staff and 2,500 students of the Hue Medical College and around 300 doctors and interns pursuing their professional engagements. The hospital is organized into 52 clinics and para-clinic departments, notably the Cardiovascular Centre (co–funded by Atlantic Philanthropies and East Meets West Foundation), the Blood Transfusion Centre (co–funded by World Bank and the World Health Organization) and the Training Centre.
2.9.1.4 Hanoi French Hospital (L’Hôpital Français de Hanoi)
Hanoi French Hospital (L’Hôpital Français de Hanoi) is the first international hospital, not only in Hanoi, but also across the North of Vietnam. It incorporates multidisciplinary medical French-Vietnamese experts. The hospital supports emergencies and treatment of all common diseases, both in terms of medical as well as surgical techniques. The infrastructure comprises 68 beds, with 42 full-time doctors, 20 rotation doctors, 114 qualified nurses, midwives and technicians.
2.9.1.5 Hospital C in Da Nang
Hospital C in Da Nang is a first class facility under the Ministry of Health, located in central Da Nang city. In recent years, the state has invested in building facilities and modern equipment, and as a result, the hospital often gets professional assistance from leading experts. Along with improving the quality of care and timely support for emergencies, the hospital has successfully deployed a variety of techniques in cranial operations such as hematoma and brain tumor surgery. The hospital is now investing in advanced systems for laparoscopic surgery and
57
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
interventions for gastrointestinal, respiratory and urology related diseases. In 2011, the hospital staffed 550 employees.
2.9.1.6 Viet Duc Hospital (Vietnam - Germany Hospital)
Viet Duc Hospital (Vietnam - Germany Hospital) is the largest surgical center in Vietnam, situated in Hanoi. This privately held hospital has around 1,400 beds and 30 operating rooms and performs over 800 open heart surgeries annually. It has collaborations for exchange and training programs with medical facilities in France, Germany, Australia and other countries.
2.9.1.7 Trieu An Hospital (TAH)
Trieu An Hospital (TAH) was founded in July 2001, with a total construction area of 21,200 square meters. It is the most technologically advanced private hospital in Ho Chi Minh City. Trieu An Hospital, in collaboration with Medic Medical Center, has started offering radiotherapy for cancer patients using HDR (High-dose Rate) in a brand new facility at the healthcare park in the city. This is only the third hospital in the city to be equipped with HDR.
2.9.1.8 Hong Ngoc Hospital
Founded in 2003, Hong Ngoc General Hospital is one of the first private hospitals in central Hanoi. After ten years in operation, Hong Ngoc Hospital has built a strong reputation for quality healthcare with exceptional customer service. The hospital is located at Ba Dinh, Hanoi with an area of more than 700 square meters, spreading to sixteen floors.
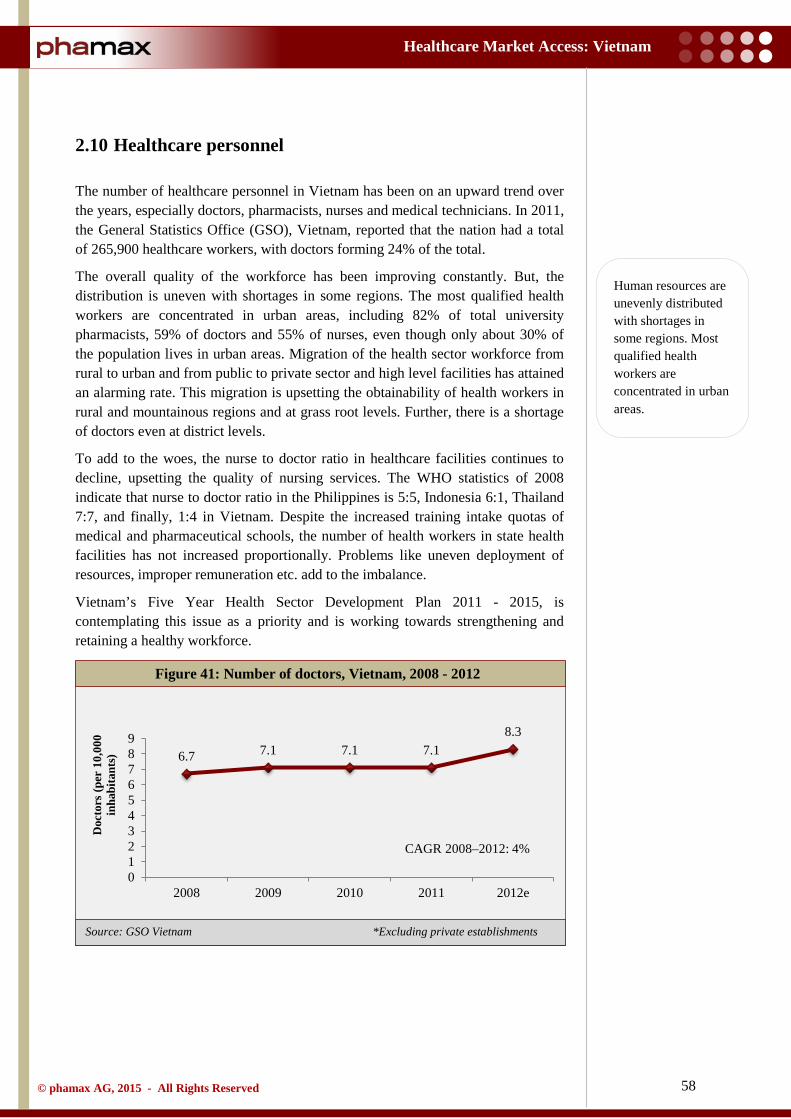
58
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: GSO Vietnam *Excluding private establishments
2.10 Healthcare personnel
The number of healthcare personnel in Vietnam has been on an upward trend over the years, especially doctors, pharmacists, nurses and medical technicians. In 2011, the General Statistics Office (GSO), Vietnam, reported that the nation had a total of 265,900 healthcare workers, with doctors forming 24% of the total.
The overall quality of the workforce has been improving constantly. But, the distribution is uneven with shortages in some regions. The most qualified health workers are concentrated in urban areas, including 82% of total university pharmacists, 59% of doctors and 55% of nurses, even though only about 30% of the population lives in urban areas. Migration of the health sector workforce from rural to urban and from public to private sector and high level facilities has attained an alarming rate. This migration is upsetting the obtainability of health workers in rural and mountainous regions and at grass root levels. Further, there is a shortage of doctors even at district levels.
To add to the woes, the nurse to doctor ratio in healthcare facilities continues to decline, upsetting the quality of nursing services. The WHO statistics of 2008 indicate that nurse to doctor ratio in the Philippines is 5:5, Indonesia 6:1, Thailand 7:7, and finally, 1:4 in Vietnam. Despite the increased training intake quotas of medical and pharmaceutical schools, the number of health workers in state health facilities has not increased proportionally. Problems like uneven deployment of resources, improper remuneration etc. add to the imbalance.
Vietnam’s Five Year Health Sector Development Plan 2011 - 2015, is contemplating this issue as a priority and is working towards strengthening and retaining a healthy workforce.
Figure 41: Number of doctors, Vietnam, 2008 - 2012
6.7 7.1 7.1 7.1 8.3
0123456789
2008 2009 2010 2011 2012e
Doc
tors
(per
10,
000
inha
bita
nts)
CAGR 2008–2012: 4%
Human resources are unevenly distributed with shortages in some regions. Most qualified health workers are concentrated in urban areas.
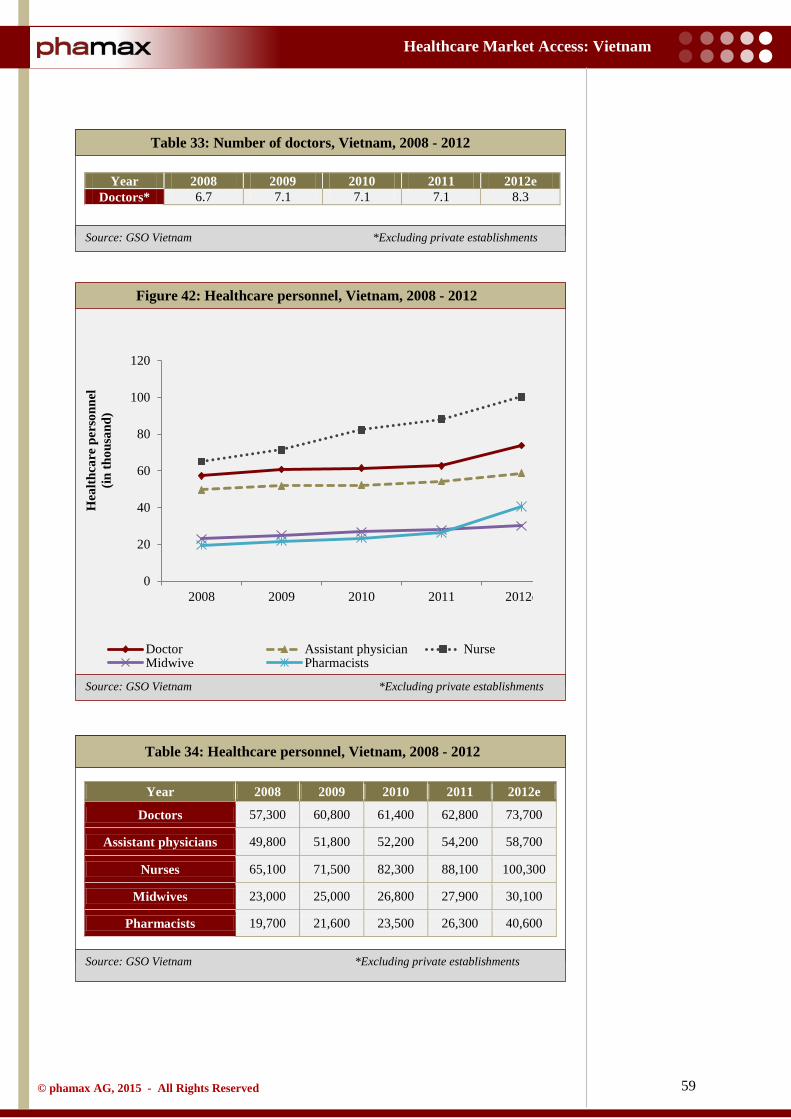
59
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: GSO Vietnam *Excluding private establishments
Source: GSO Vietnam *Excluding private establishments
Source: GSO Vietnam *Excluding private establishments
Table 33: Number of doctors, Vietnam, 2008 - 2012
Year 2008 2009 2010 2011 2012e Doctors* 6.7 7.1 7.1 7.1 8.3
Table 34: Healthcare personnel, Vietnam, 2008 - 2012
Figure 42: Healthcare personnel, Vietnam, 2008 - 2012
Year 2008 2009 2010 2011 2012e
Doctors 57,300 60,800 61,400 62,800 73,700
Assistant physicians 49,800 51,800 52,200 54,200 58,700
Nurses 65,100 71,500 82,300 88,100 100,300
Midwives 23,000 25,000 26,800 27,900 30,100
Pharmacists 19,700 21,600 23,500 26,300 40,600
0
20
40
60
80
100
120
2008 2009 2010 2011 2012e
Hea
lthca
re p
erso
nnel
(in
thou
sand
)
Doctor Assistant physician NurseMidwive Pharmacists

60
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: MoH, DAV
3 Overview of Pharmaceutical Market
3.1 Market overview
Although the global pharmaceutical industry has slackened in the last two years, the industry in developing countries, including Vietnam, still has potential to exhibit strong growth in the near future. The pharmaceutical market in Vietnam reached $3.1 bn in 2013, making it a fairly small market by South-East Asian standards, after Indonesia ($7.3bn), Thailand ($6.3bn) and the Philippines ($4.9bn). However, pharmaceutical sales in Vietnam increased by 17% compared to 2013, and is therefore considered one of the fastest growing sectors of the country. Driven by the expanding population, higher levels of health awareness, and increased access to medicines across the country, Vietnam promises healthy prospects as a pharmaceutical market. The country’s Ministry of Health (MoH) predicts that the pharmaceutical market is expected to grow at a rate of 16% by 2017.
Though there are indigenous pharmaceutical companies that produce medicines for local consumption, the country is characterized by a strong dependence on imports of raw materials (90% are imported). The local pharmaceutical companies mostly produce generics and account for less than 50% of the nation’s annual drug consumption. Poor technology and lack of qualified human resources are impediments to the country’s self-sufficiency. Additionally, the inability of local firms to source raw materials from domestic sources further hinders the flow of foreign investments from global pharmaceutical companies. The Vietnamese pharmaceutical market is also renowned for oriental medicine, mainly because of its inclination towards herbal products.
.
Figure 43: Pharmaceutical market ($bn), Vietnam, 2008 - 2014
1.5 1.8 1.9 2.2 2.7 3.1 3.5
0.0
1.0
2.0
3.0
4.0
2008 2009 2010 2011 2012 2013 2014e
Mar
ket (
$bn)
The pharmaceutical market in Vietnam reached $3.1 bn in 2013. It is expected to grow at a rate of 16% by 2017.
Increasing population, health awareness, and increased access to medicines across the country and universal health coverage will drive the Vietnamese pharma market.
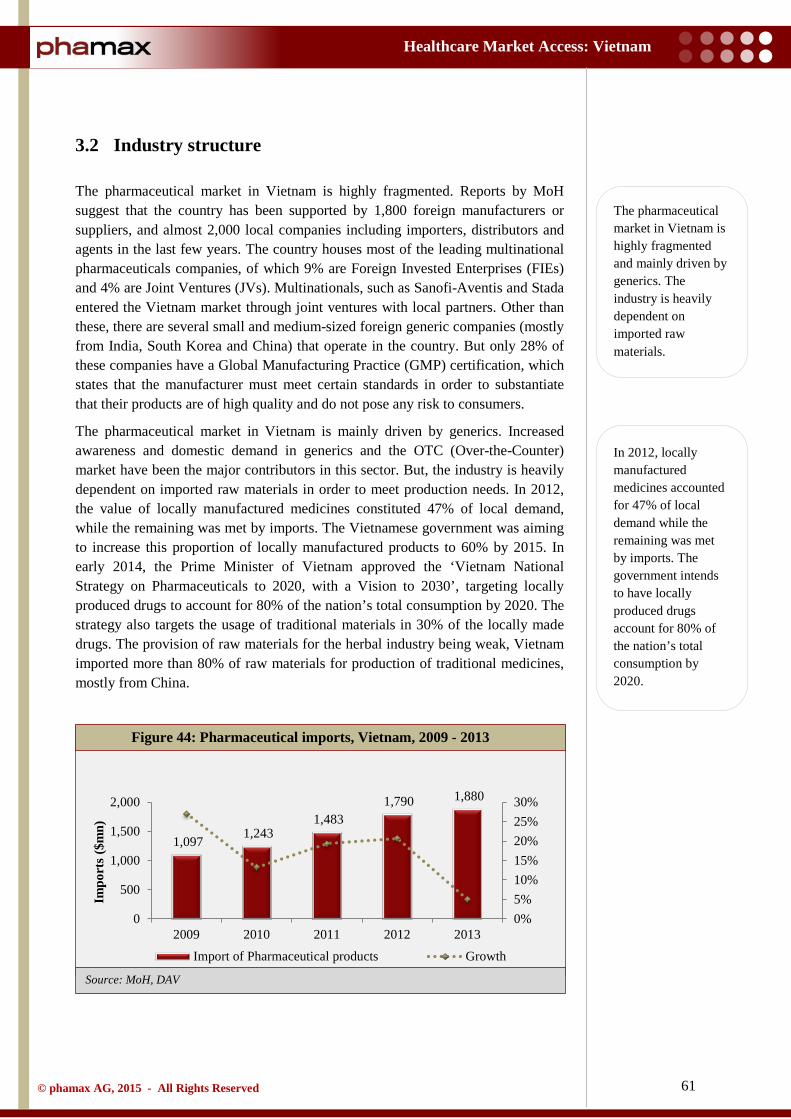
61
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: MoH, DAV
3.2 Industry structure
The pharmaceutical market in Vietnam is highly fragmented. Reports by MoH suggest that the country has been supported by 1,800 foreign manufacturers or suppliers, and almost 2,000 local companies including importers, distributors and agents in the last few years. The country houses most of the leading multinational pharmaceuticals companies, of which 9% are Foreign Invested Enterprises (FIEs) and 4% are Joint Ventures (JVs). Multinationals, such as Sanofi-Aventis and Stada entered the Vietnam market through joint ventures with local partners. Other than these, there are several small and medium-sized foreign generic companies (mostly from India, South Korea and China) that operate in the country. But only 28% of these companies have a Global Manufacturing Practice (GMP) certification, which states that the manufacturer must meet certain standards in order to substantiate that their products are of high quality and do not pose any risk to consumers.
The pharmaceutical market in Vietnam is mainly driven by generics. Increased awareness and domestic demand in generics and the OTC (Over-the-Counter) market have been the major contributors in this sector. But, the industry is heavily dependent on imported raw materials in order to meet production needs. In 2012, the value of locally manufactured medicines constituted 47% of local demand, while the remaining was met by imports. The Vietnamese government was aiming to increase this proportion of locally manufactured products to 60% by 2015. In early 2014, the Prime Minister of Vietnam approved the ‘Vietnam National Strategy on Pharmaceuticals to 2020, with a Vision to 2030’, targeting locally produced drugs to account for 80% of the nation’s total consumption by 2020. The strategy also targets the usage of traditional materials in 30% of the locally made drugs. The provision of raw materials for the herbal industry being weak, Vietnam imported more than 80% of raw materials for production of traditional medicines, mostly from China.
Figure 44: Pharmaceutical imports, Vietnam, 2009 - 2013
1,097 1,243 1,483
1,790 1,880
0%5%10%15%20%25%30%
0
500
1,000
1,500
2,000
2009 2010 2011 2012 2013
Impo
rts
($m
n)
Import of Pharmaceutical products Growth
The pharmaceutical market in Vietnam is highly fragmented and mainly driven by generics. The industry is heavily dependent on imported raw materials.
In 2012, locally manufactured medicines accounted for 47% of local demand while the remaining was met by imports. The government intends to have locally produced drugs account for 80% of the nation’s total consumption by 2020.
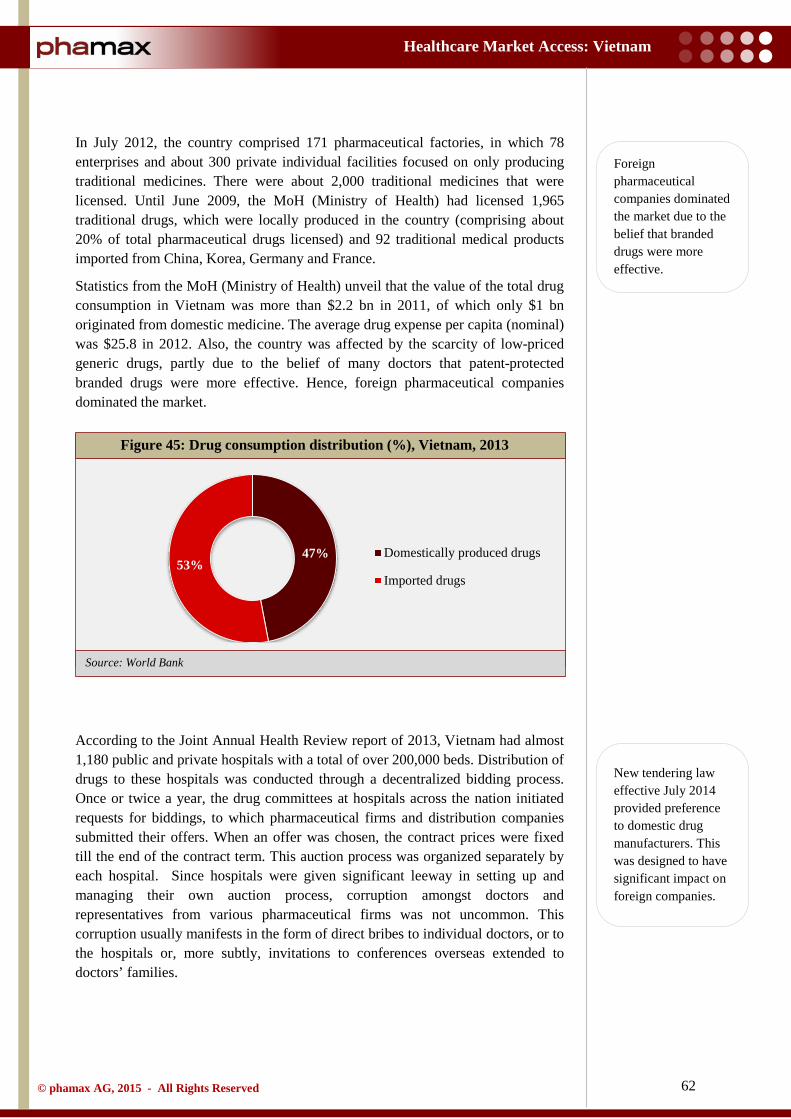
62
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: World Bank
In July 2012, the country comprised 171 pharmaceutical factories, in which 78 enterprises and about 300 private individual facilities focused on only producing traditional medicines. There were about 2,000 traditional medicines that were licensed. Until June 2009, the MoH (Ministry of Health) had licensed 1,965 traditional drugs, which were locally produced in the country (comprising about 20% of total pharmaceutical drugs licensed) and 92 traditional medical products imported from China, Korea, Germany and France.
Statistics from the MoH (Ministry of Health) unveil that the value of the total drug consumption in Vietnam was more than $2.2 bn in 2011, of which only $1 bn originated from domestic medicine. The average drug expense per capita (nominal) was $25.8 in 2012. Also, the country was affected by the scarcity of low-priced generic drugs, partly due to the belief of many doctors that patent-protected branded drugs were more effective. Hence, foreign pharmaceutical companies dominated the market.
According to the Joint Annual Health Review report of 2013, Vietnam had almost 1,180 public and private hospitals with a total of over 200,000 beds. Distribution of drugs to these hospitals was conducted through a decentralized bidding process. Once or twice a year, the drug committees at hospitals across the nation initiated requests for biddings, to which pharmaceutical firms and distribution companies submitted their offers. When an offer was chosen, the contract prices were fixed till the end of the contract term. This auction process was organized separately by each hospital. Since hospitals were given significant leeway in setting up and managing their own auction process, corruption amongst doctors and representatives from various pharmaceutical firms was not uncommon. This corruption usually manifests in the form of direct bribes to individual doctors, or to the hospitals or, more subtly, invitations to conferences overseas extended to doctors’ families.
Figure 45: Drug consumption distribution (%), Vietnam, 2013
47% 53%
Domestically produced drugs
Imported drugs
Foreign pharmaceutical companies dominated the market due to the belief that branded drugs were more effective.
New tendering law effective July 2014 provided preference to domestic drug manufacturers. This was designed to have significant impact on foreign companies.
63
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
The National Assembly’s new law on Tendering was initiated in July 2014. The law prohibited those offering tenders from providing imported drugs if there were domestic drugs available that could fully satisfy the requirements on medical treatment, price and availability. This law explicitly provided preference to domestic manufacturers, and was expected to have a deep impact on foreign companies active in this market.
The efforts to encourage local medicines and raise awareness about domestic pharmaceutical companies and their products are encouraging healthcare providers to use these products. At the same time, the domestic industry has to face challenges such as the need to meet quality standards, competition from branded generics in a highly crowded market and tight hospital budgets putting pressure on prices.
The Vietnam pharmaceutical market is expected to remain attractive, especially in view of the perception that foreign branded generics are superior to those produced locally. However, in the longer run, they are bound to come under greater pressure from cheaper locally produced generics. Vietnam encompasses over 150 sizeable domestic pharmaceutical manufacturers. DHG is currently the largest domestic drug manufacturer while other notable domestic companies are Domesco, Imexpharm, Pymepharco, and Traphaco.
In the longer run, foreign branded generics will come under greater pressure from cheaper, locally produced generics.
64
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
3.3 Market segments
The Vietnamese pharmaceutical market supplies almost every drug available, from cheap, very specialized and traditional Asian medicines to the top selling drugs derived from plants or food supplements as well as antibiotics. On the other hand, Vietnamese pharmaceutical production is limited. The domestic companies manufacture mostly generics, low-value medicines, antibiotics and pain-relievers
The market share of generics (including branded generics) in Vietnam is higher than its peers. As per the Drug Administration of Vietnam (DAV), in 2011, the share of generics in Vietnam accounted for 71% of the total market, against Singapore (35%), Thailand (46%), Malaysia (38%) and Philippines (59%).
The generics market in Vietnam is very competitive, and the first to penetrate can claim to have the first recognized drug to be embraced by customers. To survive and attract more clients, companies resort to advertising and differentiation tactics by developing new medicines. Unfortunately, the local companies are inhibited by smaller advertisement budgets and limited R&D expenses.
Local pharmaceutical companies in Vietnam are not very keen on investing in R&D. Primarily, the operational costs associated with the discovery of new patented drugs and the duration required discourage these organizations. Therefore, they are content in producing generic drugs and holding patents for trade names instead of drug formulations.
Even though manufacturing generics is the mainstream trend in Vietnam, the quality of these products vary depending on the technology used and the development cycles involved in different companies. To reduce production costs, many local pharmaceutical companies resort to low quality and cheap raw materials, regardless of the low efficacy of their products. Taking counter measures to stem this, the MoH (Ministry of Health), initiated the Decision 3886/2004, under which all domestic pharmaceutical manufacturers were mandated to obtain WHO-GMP certification from the MoH by the end of 2010. But, contrary to expectations, in 2013, there were only 120 companies out of the total 171 complying with this requirement.
The OTC (Over-the-Counter) segment in Vietnam accounts for almost one-third of the total market. Vietnamese patients usually purchase medicines based on advice from clerks in drug stores or peers and friends. Patients go to clinics only in case of serious diseases. Therefore, if symptoms are not severe, people choose to use the same treatment as previously used, or drugs advertised on television, or recommended by friends or family. This approach is largely seen in low-income groups and is affecting the pharmaceutical market.
The market is primarily driven by generics. Generics (including branded generics) accounted for 71% of the market, substantially higher than peers.
The OTC (Over-the-Counter) segment in Vietnam accounts for almost one-third of the total market.

65
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
3.4 Opportunities and challenges
Being a rapidly developing market in Asia, Vietnam offers lucrative opportunities for pharmaceutical companies keen on tapping this market. Vietnam has indigenous pharmaceutical factories that produce medicine for local consumption. However, there are many products that are either produced scarcely or not manufactured at all, due to lack of adequate facilities. Such products are hence imported from foreign pharmaceutical companies to serve the market requirement. But, the actual annual supply of imported drugs is far less than the demand. Thus, considering the growth opportunities in the market, and the need for high quality and effective medicines, the country offers a productive opportunity for the foreign companies to market their drugs.
Considering the increasing medicine consumption in the country, Vietnam represents a lucrative opportunity for drug manufacturers pursuing high returns. This demand for medicines is supported by a thriving economy, political stability, growing private consumption and expanding health insurance coverage. The country is heavily dependent on imported drugs (53%). But, the devaluation of its currency is a major area of concern. The pharmaceutical prices are on the rise and patients continue to struggle with the inflationary pressure that is predominantly affecting essential drugs.
Even though Vietnam’s healthcare service space is dominated by the public sector, there is a high number spending out-of-pocket to avail treatment. The ongoing expansion of healthcare insurance in the country, together with the increasing private spending provides an environment conducive to pharmaceutical companies and hospitals offering more products and services.
Amongst the rising optimism, the domestic pharmaceutical sector continues to face challenges, most notable of which are:
Low affordability of drugs
Vietnam’s low per capita pharmaceutical spending (1.9% of GDP per capita in 2013), highlights the country’s poor access to medical drugs, caused by the high prices of imported drugs. The MoH (Ministry of Health) reports that imported medicines constitute 80% of the total medicines used in hospitals.
Incompetent drug price management and intellectual property protection
The prices of medicines are inconsistent across the supply chain due to arbitrary price hikes by drug distributors and retail stores, thus eroding the affordability of medicines. Also, a large section of the country’s generics market represents low-quality replicas with unproven bioequivalence. Despite the fact that Vietnam’s agreement to the World Trade Organization (WTO) in January 2007 resulted in an overall improvement in the Intellectual Property (IP) legal framework, the IP enforcement is still patchy and disorganized. Therefore, companies venturing into the market have to be on vigil. Again, local manufacturers are skeptical about R&D and hence are more prone towards the production of imitation drugs.
Pharma companies will continue to face challenges due to low affordability of drugs, inadequate price controls, weak IP protection, corruption and counterfeit drugs.
Growing population, economic growth, private healthcare spending and government’s plan for universal health coverage make Vietnam an attractive destination for pharmaceutical companies.
66
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Widespread corruption amongst healthcare officials
There have been numerous allegations regarding the collusion between foreign drug-makers and local distributors to keep prices high and doctors accepting commissions for prescribing certain drugs. The modes of bribes are usually direct bribes to individual doctors or hospitals or, more subtly, invitations extended to doctors’ families to overseas conferences. Such practices are putting patient lives in jeopardy by making treatments inaccessible, especially to the layman.
Presence of counterfeits in the market
In a market that directly affects patients and where pharmaceutical companies have an inclination to manufacture spurious drugs, counterfeit medicines are naturally bound to thrive. The Drug Administration of Vietnam (DAV) pointed out that the percentage of substandard medicines was 3.1% in 2012, up by 0.2% from 2011. The counterfeit menace is a grave one, especially given the fact that pharmacy distribution is essentially controlled by private dealers. The counterfeit drug trade is rampant on the borders of Laos, China and Cambodia and is increasingly intimidating for the Vietnamese drug market.
Amidst all pros and cons, Vietnam is still an attractive prospect for pharmaceutical firms, purely because of its growing affluence, an ageing population and the continuing presence of non-communicable diseases.
In addition, the National Assembly’s new law on Tendering, passed in July, 2014, prohibits tenders offering imported drugs if there are domestic drugs available that can fulfill the criteria for treatment and price. The law is explicitly built to help local manufacturers. The law will strongly affect the penetration strategies of foreign investors.
Preferential treatment given to local manufacturers by the new tendering law will directly impact foreign pharma companies.
67
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
3.5 Major players
Foreign pharmaceutical companies have continued to exhibit a mounting interest to launch sales and production facilities in Vietnam in spite of the ever increasing user-friendly policies that support the domestic firms. These firms also carry on buying shares in their Vietnamese counterparts. In 2012, Netherlands based Stada Service Holdings bought a 25% stake in Pymepharco a Vietnamese manufacturer. This transaction helped Stada boost its share up to a total of 49%.
In another partnership, in 2010, GlaxoSmithKline (GSK) signed an agreement with the leading Vietnamese pharmaceutical company Savipharm. Under this agreement, GSK is responsible for marketing authorization, technical support and quality control, while Savipharm is responsible for manufacturing and distribution. Also, Fresenius Kabi signed a joint venture agreement with the state-owned company Bidiphar and manufactures infusion solutions and liquid medications under the tag Fresenius Kabi Bidiphar JSC.
In 2012, Vietnam had 170 pharmaceutical companies, 10% of which were owned by foreign investors, and around 4% operated as joint ventures. The largest drug companies in terms of market share were GlaxoSmithKline (GSK), Bristol Myers Squibb (BMS), Novartis and Sanofi Aventis.
Sanofi Aventis has been operating in Vietnam for over 50 years, with over 1,000 employees. Boasting a strong infrastructure constituting two distributing centers in Tan Binh Industrial zone and two factories adhering to WHO–GMP (World Health Organization – Good Manufacturing Practice) standards, Sanofi continues to have a strong base in Vietnam. Their chief products include Calcium Corbiere (nutritional supplement), Plavix (coagulation prevention), Taxotere (cancer), Enterogermina (digestion) and Amaryl (diabetes). In 2013, Sanofi officially announced the construction of its third pharmaceutical factory in Saigon hi-tech park, citing a total investment of $75 mn. This plant has a key role to play in advancing the country’s manufacturing capabilities.
Notable domestic players in the market include Hau Giang Pharmaceutical Company (DHG), Domesco Medical Import Export JSC (DMC), Traphaco, and Imexpharm. To hike the domestic production of quality drugs, Vietnam has lately encouraged manufacturers to acquire a Good Manufacturing Practice (GMP) certification. Yet, only about one-third of the Vietnamese pharmaceutical companies have complied with a GMP certification.
DHG pharmaceutical is the largest domestic drug manufacturer in Vietnam in terms of sales volume and operation network. The company’s portfolio chiefly consists of Over-the-Counter (OTC) drugs in the antibiotic and pain relief segments. In 2012, the revenues from these two OTC categories contributed 38% and 19% respectively. In 2013, the company successfully completed the installation of its two new production plants, raising its total annual production capacity. The company posted a net revenue of VND 3.5 trillion in 2013, with a
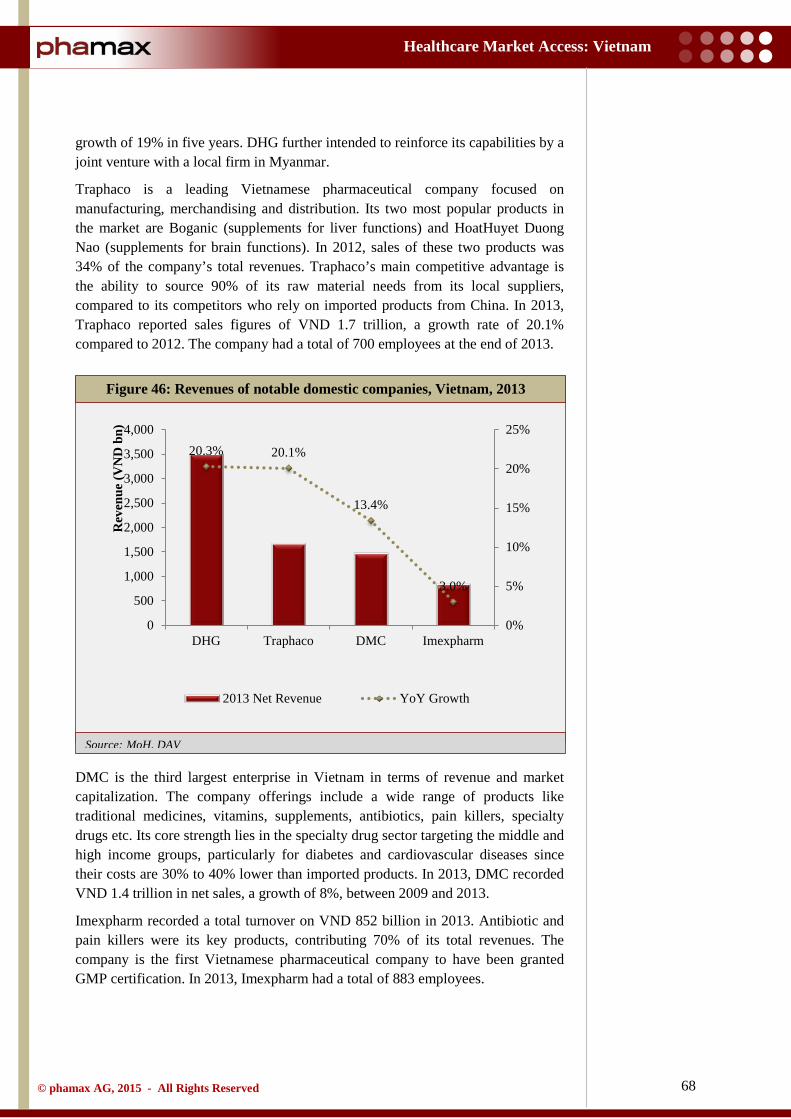
68
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: MoH, DAV
growth of 19% in five years. DHG further intended to reinforce its capabilities by a joint venture with a local firm in Myanmar.
Traphaco is a leading Vietnamese pharmaceutical company focused on manufacturing, merchandising and distribution. Its two most popular products in the market are Boganic (supplements for liver functions) and HoatHuyet Duong Nao (supplements for brain functions). In 2012, sales of these two products was 34% of the company’s total revenues. Traphaco’s main competitive advantage is the ability to source 90% of its raw material needs from its local suppliers, compared to its competitors who rely on imported products from China. In 2013, Traphaco reported sales figures of VND 1.7 trillion, a growth rate of 20.1% compared to 2012. The company had a total of 700 employees at the end of 2013.
DMC is the third largest enterprise in Vietnam in terms of revenue and market capitalization. The company offerings include a wide range of products like traditional medicines, vitamins, supplements, antibiotics, pain killers, specialty drugs etc. Its core strength lies in the specialty drug sector targeting the middle and high income groups, particularly for diabetes and cardiovascular diseases since their costs are 30% to 40% lower than imported products. In 2013, DMC recorded VND 1.4 trillion in net sales, a growth of 8%, between 2009 and 2013.
Imexpharm recorded a total turnover on VND 852 billion in 2013. Antibiotic and pain killers were its key products, contributing 70% of its total revenues. The company is the first Vietnamese pharmaceutical company to have been granted GMP certification. In 2013, Imexpharm had a total of 883 employees.
Figure 46: Revenues of notable domestic companies, Vietnam, 2013
20.3% 20.1%
13.4%
3.0%
0%
5%
10%
15%
20%
25%
0
500
1,000
1,500
2,000
2,500
3,000
3,500
4,000
DHG Traphaco DMC Imexpharm
Rev
enue
(VN
D b
n)
2013 Net Revenue YoY Growth

69
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
OPV Pharmaceutical (OPV) is a leading domestic generics manufacturer in Vietnam. It attained WHO GMP (World Health Organization - Good Manufacturing Practice) and WHO GLP (World Health Organization - Good Laboratory Practice) certifications from the Vietnam MoH (Ministry of Health) in 2005. The same year, GSK (GlaxoSmithKline), after stringent quality audits, approved OPV to manufacture its products. In 2008, the contract was extended. OPV also has a joint venture with Otsuka Pharmaceutical Company, Japan. In 2010, the company registered 693 pharmaceutical products, of which 280 products were manufactured and marketed.

70
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
3.6 Key products
Natively manufactured, inexpensive products are prevalent amidst the low income population in Vietnam. Most of these highest selling products are antibiotics, food supplements, complementary products like eye and ear drops and vitamins. Foreign players focus more on the creamy layer of high-priced products, rather than these high selling products that are not part of their portfolio.
However, Vietnamese consumers favor foreign products, generally from Europe and the US. Products from international firms are chosen because of brand recognition and the perception that western products are of dependable value. GSK's Augmentin continued to generate the highest sales in the country despite stiff competition from DHG Pharma’s domestic version of this broad-spectrum antibiotic. Other products of GSK, namely Zinnat (cefuroxime), Panadol (analgesic) and Ventolin (albuterol) own a major share of the market. In addition, BMS’s Efferalgan (acetaminophen) also tops the list of major products sold in Vietnam.
The only companies with a sizeable budget for marketing expenses and money to advertise in the country are foreign pharmaceutical companies. Regulations that cap domestic pharmaceutical firms’ advertising expenditures at ten percent of their annual budgets, limit their ability to advertise. Domestic companies only do some direct marketing and focus more on building customer relationships. Doctors also prefer prescribing foreign drugs to local ones due to heavy commissions and kickbacks offered by foreign pharma companies. But, domestic products still retain their popularity amongst the low-income population. But, in spite of the sale of these domestic drugs in large volumes, the revenue generated remains low. Product sales also fluctuate as per tender purchases in public hospitals.
Foreign drugs dominate the Vietnam market since they are perceived to have better quality, are supported by advertising and the companies owning them offer more commissions to doctors.
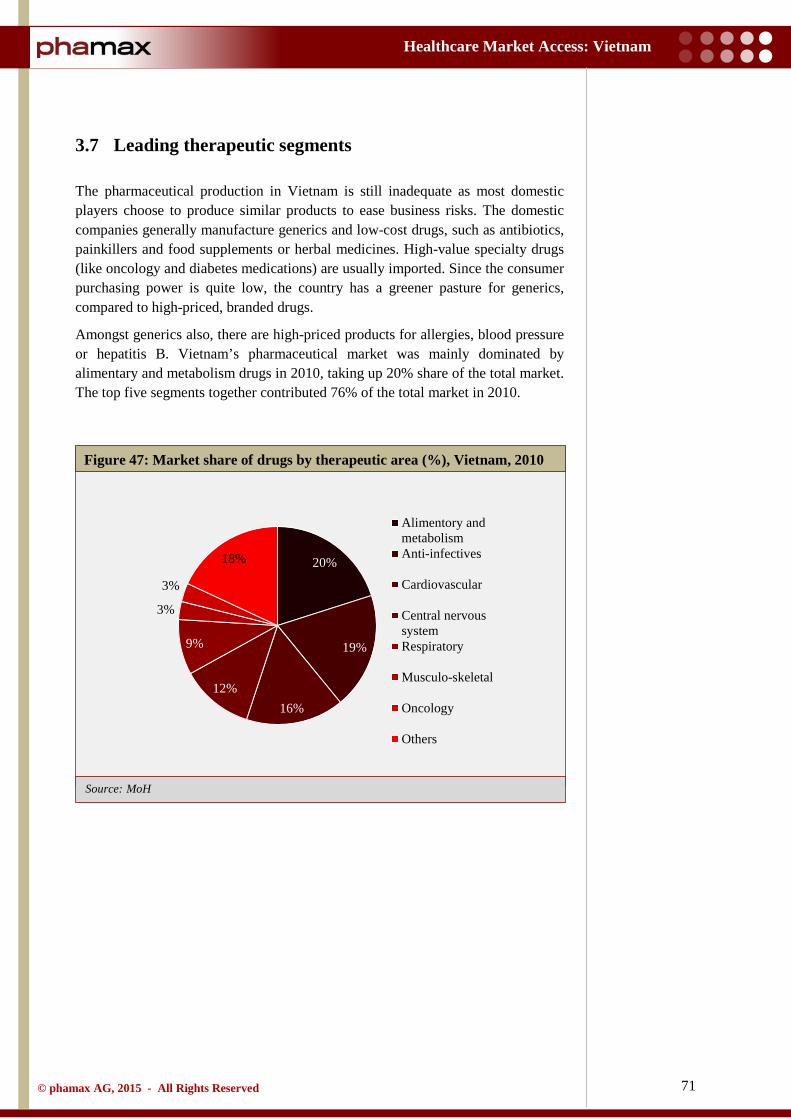
71
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: MoH
3.7 Leading therapeutic segments
The pharmaceutical production in Vietnam is still inadequate as most domestic players choose to produce similar products to ease business risks. The domestic companies generally manufacture generics and low-cost drugs, such as antibiotics, painkillers and food supplements or herbal medicines. High-value specialty drugs (like oncology and diabetes medications) are usually imported. Since the consumer purchasing power is quite low, the country has a greener pasture for generics, compared to high-priced, branded drugs.
Amongst generics also, there are high-priced products for allergies, blood pressure or hepatitis B. Vietnam’s pharmaceutical market was mainly dominated by alimentary and metabolism drugs in 2010, taking up 20% share of the total market. The top five segments together contributed 76% of the total market in 2010.
Figure 47: Market share of drugs by therapeutic area (%), Vietnam, 2010
20%
19%
16% 12%
9%
3%
3%
18%
Alimentory andmetabolismAnti-infectives
Cardiovascular
Central nervoussystemRespiratory
Musculo-skeletal
Oncology
Others

72
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
3.8 Supply chain
Unlike most of the global pharmaceutical market, where manufacturing and distributing companies are independent units that focus on a certain area of specialization, drug distribution in Vietnam is complex. The structure involves many levels like:
• Professional drug distributing enterprises o State-owned distributing companies: Mostly, these state-owned
pharmaceutical companies are distributors of imported products. For instance, Vinapharm, a state-owned company under the Ministry of Health, has seventeen companies responsible for trade across the country.
o Private distributing companies: Private distributing companies also act as distributors for imported products.
o Foreign distributing companies: There are only three foreign distributors in the market, namely, Zuellig Pharma, Diethelm and Megaproduct.
• Manufacturing cum distributing companies: Pharmaceutical enterprises in Vietnam are still young in comparison to the global industry. Thus, there is only one state-owned drug company that is a manufacturer cum distributor, although there are approximately 170 drug manufacturers in the generics market.
• Wholesale markets: Wholesale markets are capable of manipulating both foreign and domestic distributing companies. Wholesalers, backed by strong finance, purchase discounted drug products, creating a false shortage of supply in the market and later redistribute them in times of dire need to the market at much higher prices hoping to make bigger profits. Wholesale markets are also home to drugs of uncertain origins, counterfeits, low quality products, and samples or almost expired drugs without certification.
• Public and private hospitals: There are 1,030 hospitals (central, provincial and district hospitals) run by the Ministry of Health, around 47 hospitals run by other ministries and approximately 28 private hospitals in Vietnam.
• Drugstores: This is the most popular distribution channel in Vietnam, mostly because of purchasing convenience. It is also a conventional habit in developing countries to go to drugstores in case of a malady, and only consult doctors if they cannot find the remedy in drugstores. In remote areas, drugstores are almost the singular, default choice. 39,016 registered pharmacies have been reported nationwide. Most of them are small, single owner pharmacies, run by a pharmacist. The number of drugstore retail chains is very less compared to peers. Out of total drugstores, only 83 are GPP (Good Pharmacies Practice) accredited.
• Private clinics: The MoH has reported that there are more than 30,000 private clinics in the entire country, with the number tending to increase

73
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: MoH
over the years. These are mostly located in the two major cities, namely, Ho Chi Minh City and Hanoi. The Ministry of Health also cited that there are about 25,000 doctors engaged in private business practices and these private clinics are an important part of the drug distribution chain in Vietnam. The reasons are as follows:
o Most of the doctors working in hospitals also work overtime in their own clinics to boost their income, given the fact that monthly average earning per doctor in Vietnam is only around VND 3 mn.
o State-owned hospitals are unable to satisfy the persistent demands of patients while private hospitals are already a trustworthy source for patients.
Figure 48: Distribution channel for pharmaceuticals, Vietnam
Domestic / Foreign Manufacturers
Domestic / Foreign
Distributors Wholesalers
Pharmacies / Drug retailers Hospitals Private clinics
74
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
3.8.1 Distribution
After Vietnam joined the WTO in 2007, foreign pharmaceutical companies were allowed to open branches and import their products into the country. However, they were prohibited from distributing their products directly and had to partner with local distributors to sell their products. In Vietnam, the pharmaceutical industry gets access to consumers through two different channels - treatment distribution network and commercial distribution network.
Treatment distribution network: This channel includes hospitals and other treatment units at diverse levels. Almost all pharmaceutical companies promote this distribution channel because of its consumption capabilities in large quantities. In this channel, pharmaceutical companies get access to customers and expand their market shares by giving commissions or discounts to doctors and pharmacists.
Although this channel brings advantages with high turnover, it entails difficulties when it comes to domestic pharmaceutical companies, such as,
• Primarily, selling through hospitals occupies a high amount of working capital because hospitals normally settle payment at the end of the year.
• Secondly, foreign pharmaceutical companies with financial advantages give high commissions and discounts across the treatment network, creating considerable competition for domestic companies.
Commercial distribution network: The commercial distribution network involves agents, distributors and pharmacies. The domestic pharmaceutical companies promote this channel to reduce their dependence on the treatment distribution network, which comes with intense competition.
In this channel, working capital is turned over faster. Besides, product brand names are easily recognized, particularly because domestic companies mainly produce generic drugs. However, pharmaceutical companies also face challenges in this distribution channel:
• In order to expand their branches, pharmaceutical companies have to construct warehouses that meet Good Supply Practice (GSP) standards.
• On the other hand, the new guideline mandates the drug stores and agents to meet Good Pharmacy Practice (GPP) standards. Those which fail to meet the standards are permitted to sell prescription drugs.
Foreign pharmaceutical companies are prohibited from distributing their products directly and have to partner with local distributors.
There are two main distribution channels: Treatment channel (mainly include hospitals) and Commercial channel (includes retail pharmacies and drug stores).
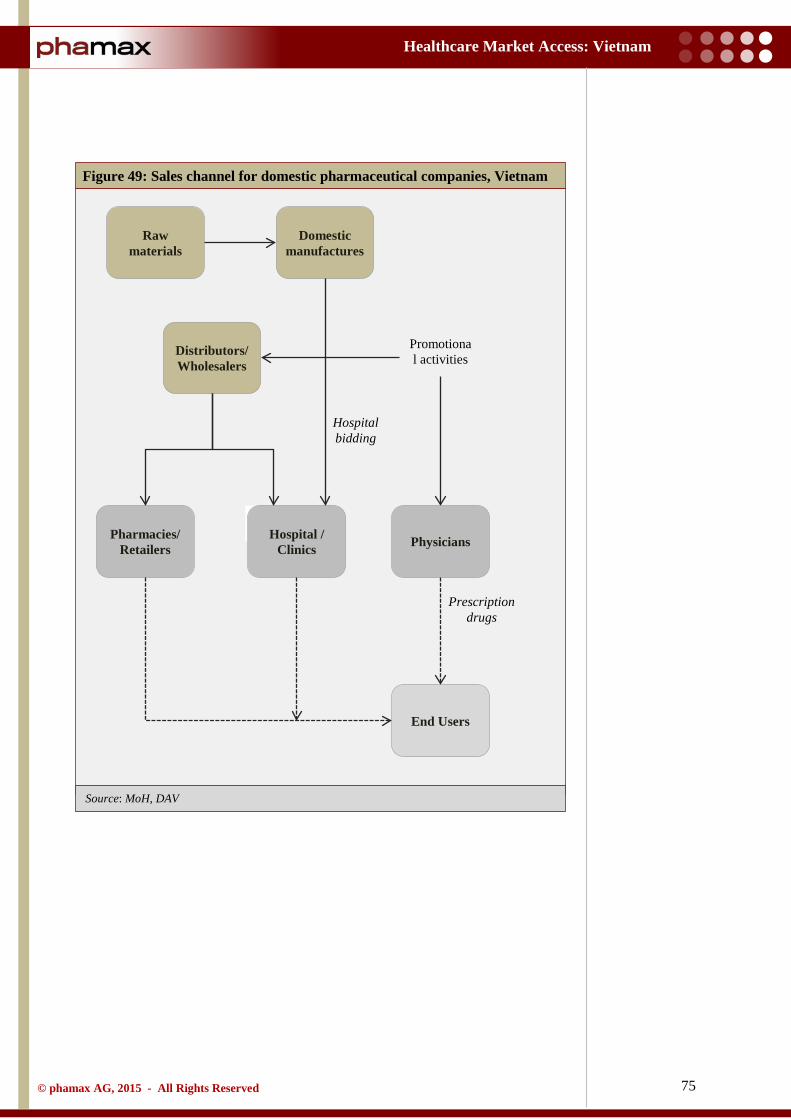
75
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: MoH, DAV
Figure 49: Sales channel for domestic pharmaceutical companies, Vietnam
Raw materials
Domestic manufactures
Distributors/ Wholesalers
Promotional activities
Hospital bidding
Hospital / Clinics
Pharmacies/ Retailers
End Users
Physicians
Prescription drugs
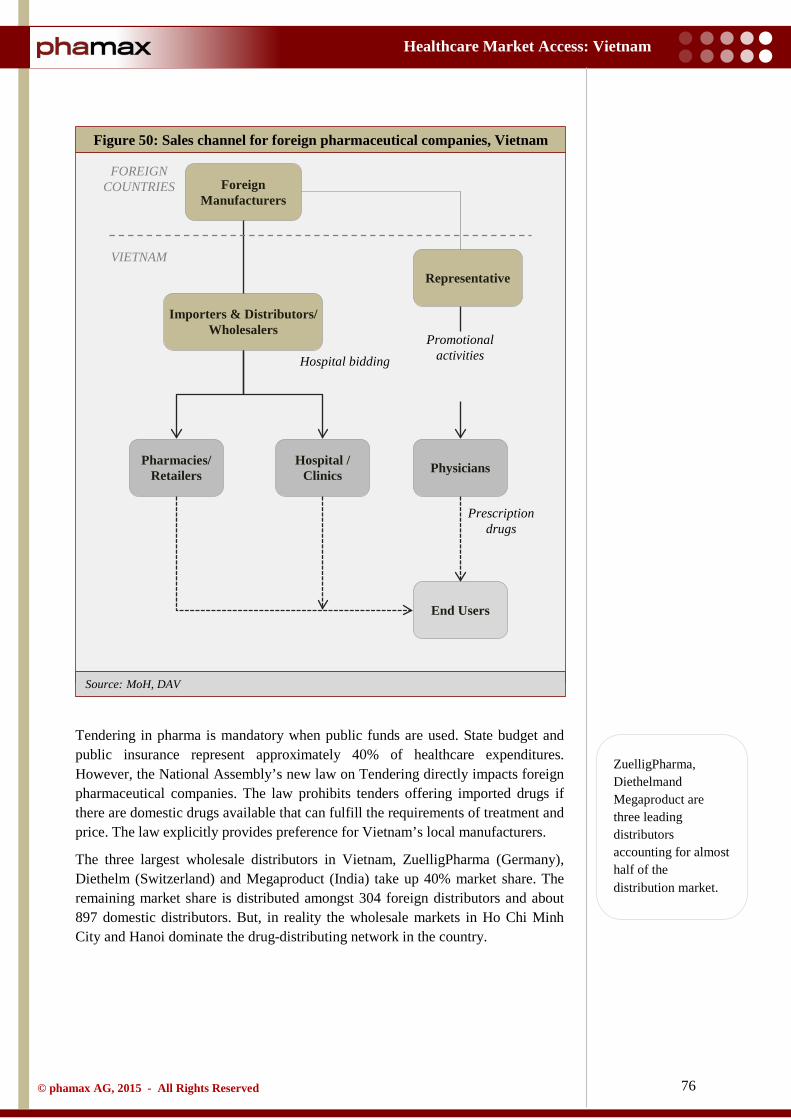
76
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: MoH, DAV
Tendering in pharma is mandatory when public funds are used. State budget and public insurance represent approximately 40% of healthcare expenditures. However, the National Assembly’s new law on Tendering directly impacts foreign pharmaceutical companies. The law prohibits tenders offering imported drugs if there are domestic drugs available that can fulfill the requirements of treatment and price. The law explicitly provides preference for Vietnam’s local manufacturers.
The three largest wholesale distributors in Vietnam, ZuelligPharma (Germany), Diethelm (Switzerland) and Megaproduct (India) take up 40% market share. The remaining market share is distributed amongst 304 foreign distributors and about 897 domestic distributors. But, in reality the wholesale markets in Ho Chi Minh City and Hanoi dominate the drug-distributing network in the country.
Figure 50: Sales channel for foreign pharmaceutical companies, Vietnam
Foreign Manufacturers
Representative
Importers & Distributors/ Wholesalers
Promotional activities Hospital bidding
Hospital / Clinics
Pharmacies/ Retailers
End Users
Physicians
Prescription drugs
VIETNAM
FOREIGN COUNTRIES
ZuelligPharma, Diethelmand Megaproduct are three leading distributors accounting for almost half of the distribution market.
77
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
3.8.2 Retail
In 2012, there were approximately 54,000 pharmacies and drug stores in Vietnam, representing an average of six outlets for every 10,000 people. Patients had access to most of the drugs even without prescriptions at private pharmacies or retail establishments, although they charged higher than pharmacies located within hospitals. As per the information from various news sources, retail prices offered to end users are three or four times the wholesale prices set by drug manufacturers. Despite rules and counter measures imposed by the MoH to counter this, only a few outlets are examined and audited by the MoH. This phenomenon is likely to persist in the future. But, in spite of the drawbacks, the retail segment is seeing upward trends.
The majority of the drug outlets in Vietnam have individual owners and are small-scale in nature. The largest retail chains (e.g. My Chau Pharmacies) claim to have around 20 – 30 stores. In contrast, drug retail chains in Vietnam’s more developed neighboring countries are much larger. In Philippines, Mercury drug retail chain owns more than 500 stores (60% of the country’s total market share in 2010). Operating at a small scale helps Vietnamese pharmacies and retail drug stores to escape the regulator’s attention. So, they continue to adjust the retail price of drugs at their will.
As per Ministry of Health statistics, in 2011, there were 10,250 private pharmacies nationwide and a total of 44,000 drug retailers in both public and private sectors. The quality of the pharmaceutical supply network has been strengthened by the promulgation and implementation of standards like Good Distribution Practice (GDP), Good Storage Practice (GSP), and Good Pharmacy Practice (GPP). By 2012, there were 3,950 GPP pharmacies in Vietnam, representing 39% amongst all pharmacies nationwide.
The domestic pharma distributors are gearing up to compete with the small private pharmacies that currently dominate the market. Domestic enterprises like Eco, Sapharco and others are planning to close stores that have proven to be ineffective and invest more capital in expansion across the country. Sapharco (a retail chain set up by Saigon Pharmaceuticals) in Ho Chi Minh City is expected to have over 3,000 pharmacies with GPP standards by 2019.
Patients have access to drugs without prescriptions at private pharmacies or retail establishments. But, drugs are priced higher compared to pharmacies located within hospitals.
The retail segment is growing at a rapid rate and has been exhibiting a strong growth over the years. The domestic pharma distributors are gearing up to compete with small private pharmacies.

78
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
3.9 Sales and marketing
Like many other countries, marketing of drugs in Vietnam is also subjected to strict regulations. Prescription drugs are not directly marketed to the general public. They may be only marketed to Medical Professionals (MPs), including pharmacists through certain approved methods. Predominant among these is marketing through licensed medical representatives (called drug introducers in Vietnam). Other methods include distribution of drug information documents, introduction seminars for MPs and promotion programs.
Pharmaceutical sales in Vietnam is very complex and unstructured, mostly because the sale relies on personal relationships between medical sales representative and doctors, hospital directors, pharmacists etc. The budget for marketing in pharmaceutical companies is restricted, further limiting advertisements. The expense incurred mostly includes the cost of manpower, as in the case of medical representatives. All pharmaceutical companies, foreign and local in Vietnam, have a strong network of medical sales representatives. DHG Pharma has 700 medical representatives, DMC around 350, Sanofi has approximately 200 representatives and Zuellig Pharma has 120 medical representatives. Foreign pharmaceutical companies have strong advantages, considering their well-known brands and products that are not manufactured in Vietnam. Therefore, hospitals, doctors, pharmacies etc. are mandated to purchase from them. The lobbying costs represent around 5 - 6% of their total revenue. On the contrary, it local companies have to build a strong network and relationships to thrive.
Vietnam’s Wholly Foreign Owned Enterprises (WFOE), who are licensed to import drugs, are allowed to engage in all marketing activities. But, if a foreign company is present in Vietnam as a RO (as per the law, a Representative Office is a cost center with no revenue), it is technically prohibited from all marketing activities except for conducting seminars and distribution of information to medical representatives. The choice to opt for one of these legal entities is often driven by political or financial motives. RO is not taxed as it doesn’t have revenue. Building a factory needs high initial capital investment while a joint venture requires trust and reliability on an unknown company. Considering all these advantages, most of the foreign companies choose to have a representative office as a legal representation in Vietnam.
A sales promotion program for pharmaceuticals cannot be directed at consumers, but must be directed only at pharmaceutical traders. Sampling is prohibited because of past abuses, where companies used samples as incentives for dispensing doctors. Promotion within the hospital premises is also forbidden. Any gifts or incentives received must be declared to the tax authorities by physicians.
Prescription drugs cannot be advertised directly to consumers. They can be promoted only via healthcare professionals via medical representatives and other approved means. OTC drugs can be advertised directly via print media. However, marketing via radio and Television requires prior approval from DAV.
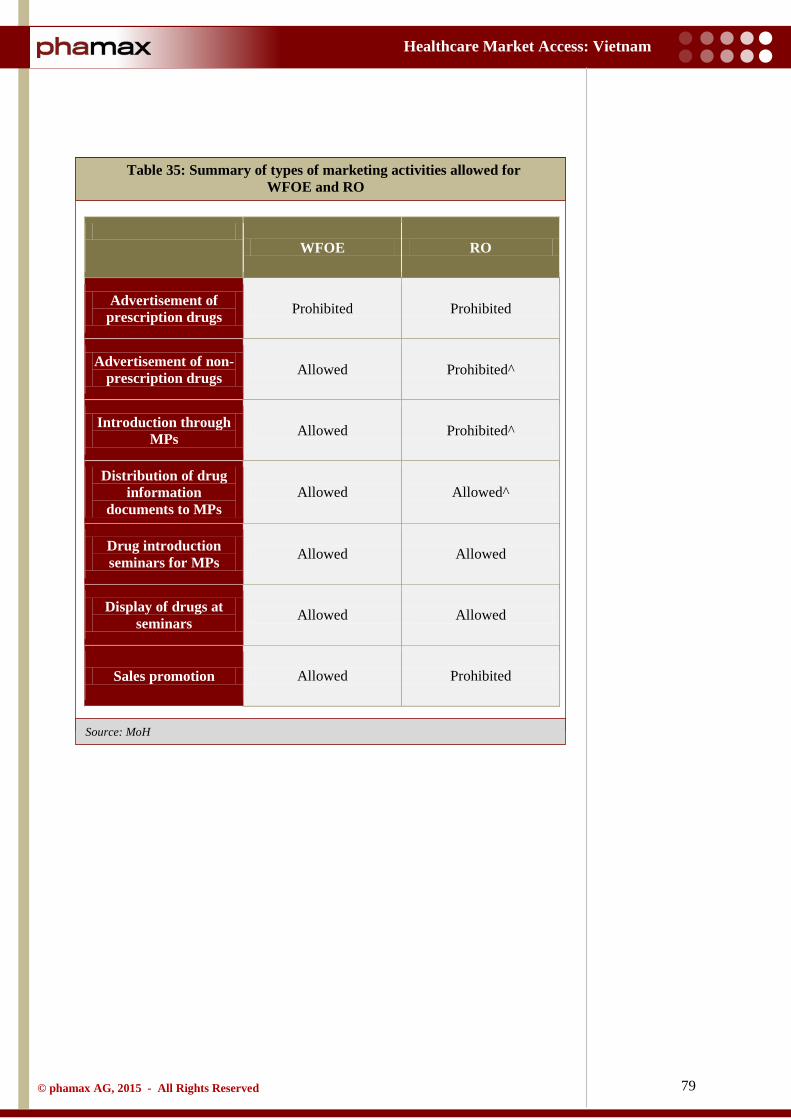
79
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: MoH
Table 35: Summary of types of marketing activities allowed for WFOE and RO
WFOE RO
Advertisement of prescription drugs Prohibited Prohibited
Advertisement of non-prescription drugs Allowed Prohibited^
Introduction through MPs Allowed Prohibited^
Distribution of drug information
documents to MPs Allowed Allowed^
Drug introduction seminars for MPs Allowed Allowed
Display of drugs at seminars Allowed Allowed
Sales promotion Allowed Prohibited
80
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
3.10 FDI in pharmaceutical industry
Based on the Investment Law of 2005, a foreign pharmaceutical company can enter the Vietnam market in three ways:
• A foreign pharmaceutical company can establish a 100% foreign-owned enterprise, where local manufacturing is mandatory. This legal entity is normally a factory, which can distribute its own manufactured products. This does not allow the company to distribute its imported products that are not locally manufactured. Therefore, in this set up, the company has to use a distributor for the imported products. The main constraint of this set up is the huge investment needed to construct a factory
• A foreign company can enter the Vietnamese pharmaceutical market with a joint venture with a local Vietnamese partner, who has at least 51% stakes in the company. This setup is complicated, time consuming and mandates trust between the parties
• Finally, a foreign company is allowed to be present in Vietnam as a Representative Office (RO). According to the Vietnamese law, a RO cannot generate revenue and therefore needs to go through a distributor for selling
The Ministry of Health (MoH) introduced a draft circular (Draft 13), citing guidelines for pharmaceutical enterprises with foreign direct investment (FDI) interests and implement import-export rights for these firms. The category of FDI enterprises in the pharmaceutical field that are permitted to carry out drug import-export activities is defined under Decree No. 79/2006. As per this provision, for drug import and export rights, FDI enterprises must invest in one of the following activities - drug manufacturing, drug storage or drug testing services.
In addition to the aforementioned business conditions, FDI pharmaceutical enterprises have to mandatorily comply with other conditions to be granted a Certificate of Satisfaction of Conditions (CSC) for drug import activities. These include:
• Drug import rights included in the investment certificate • Ownership of a CSC to implement drug manufacturing, drug storage or
drug testing services, and • Possession of a drug storage warehouse with (Good Supply Practices)
GSP standards
In complying with these obligations, firms with an FDI interest not only have to have a larger investment capital, but also have to spend more time than usual, which can be spent on more productive activities. Apart from this, the choices are limited in terms of business partners in Vietnam. According to Article 7.3 of Draft 13, FDI enterprises are only permitted to carry out trading activities with certain selected Vietnamese pharmaceutical entrepreneurs who meet the distribution criteria as regulated by the MoH, i.e.,
Regulations require enterprises with FDI interests to invest in one of the following activities - drug manufacturing, drug storage or drug testing services.

81
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
• A chain of GPP pharmacies • Distribution centers as regulated by the MoH, or • Warehouse(s) and a drug distribution system complying with GSP
standards
FDI enterprises are still not allowed to engage in any drug distribution activities in the country, except for distributing drugs that are manufactured by them locally (Articles 9.1 and 9.2 of Draft 13). It is explicit that these regulations on drug import-export activities etched out the MoH are prone to decrease the competitiveness of FDI enterprises in the Vietnamese pharmaceutical market. To sum up, FDI enterprises face numerous hurdles in expanding their business.
But, notwithstanding the bureaucratic interventions and legal compliances that make life difficult for them, foreign drug companies continue to establish sales and production facilities in Vietnam. Looking at a prime example, in 2012, Japan’s Nipro Pharma Corporation invested around $250 mn in a manufacturing plant for new drugs and medical equipment. The facility specializes in high quality, low-priced injectable drugs produced for export to developed countries, including Japan itself. There are other companies who buy shares in their Vietnamese counterparts to establish a foothold in the country. Based on reports filed by the Drug Administration of Vietnam (DAV), the country had 39 FDI projects in the pharmaceutical sector in 2013, with a collective registered capital of $303 mn. 26 of these 39 projects are categorized under operations, comprising 24 manufacturing facilities and two storage facilities. As mentioned in the earlier parts of the report, the National Assembly’s new law on Tendering, passed in July, 2014, also will have a restrictive impact on foreign investors. The law prohibits foreign firms from distributing imported drugs if the same criteria are fulfilled by local firms. The law was created with a predilection towards local firms.

82
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
3.11 Events
The last few years have seen an escalating interest shown by foreign drug companies in Vietnam due to its mounting capabilities. To substantiate the fact, there are several foreign investors holding big stakes in local pharmaceutical enterprises. The country is also unveiling a new trend in Mergers and Acquisitions (M&A), in which a group of shareholders offer to sell their stakes in a company to a foreign strategic investor. In 2013, local pharmaceutical company EuviPharm sold a 65% stake to Canada’s Valeant Pharmaceuticals International for $20 mn, giving Valeant an opportunity to manage the local firm actively. In the same year, Chilean company CFR International acquired a 44% stake in Domesco.
In 2012, Netherlands based Stada Services Holding bought a 25% stake in a Vietnamese drug maker Pymepharco, providing Stada a total share of 49%. In the same year, private equity firm Navis Capital Partners completed an investment in a leading domestic generics manufacturer, OPV Pharmaceutical Holdings, which in turn controls the shareholders of OPV Pharmaceutical Joint Stock Company.
In 2010, GlaxoSmithKline (GSK) atained manufacturing capability through a joint venture with leading Vietnamese pharmaceutical company Savipharm. Under this agreement, GSK is responsible for marketing, technical support and quality control (including the upgrade of Savipharm’s quality control systems), while Savipharm handles manufacturing and distribution. This partnership marked the beginning of the business cooperation model for manufacturing and trading firms in the Vietnamese pharmaceutical domain.
Sanofi is another brand that has made sizeable investments in its own production facilities in Vietnam. It recently announced an investment sum of $75 mn for its third facility in the Saigon Hi-Tech Park in outer Ho Chi Minh City, its largest project in the country so far. This facility is expected by 2016.
Adversely, Vietnam has imposed bans on at least 45 Indian pharmaceutical companies from supplying medicines to its market, some of them being Strides Arcolab, Medley Pharmaceuticals, Marksans Pharma and UMedica Laboratories. The Drug Administration of Vietnam (DAV) stated that the drugs of these companies were 'Not of Standard Quality' (NSQ), and were therefore banned. Some Indian companies, nine from Korea, two from Bangladesh, two from France, and one each from the US, Philippines, Pakistan, Russia, Indonesia, Germany, Cyprus and Canada have been banned.
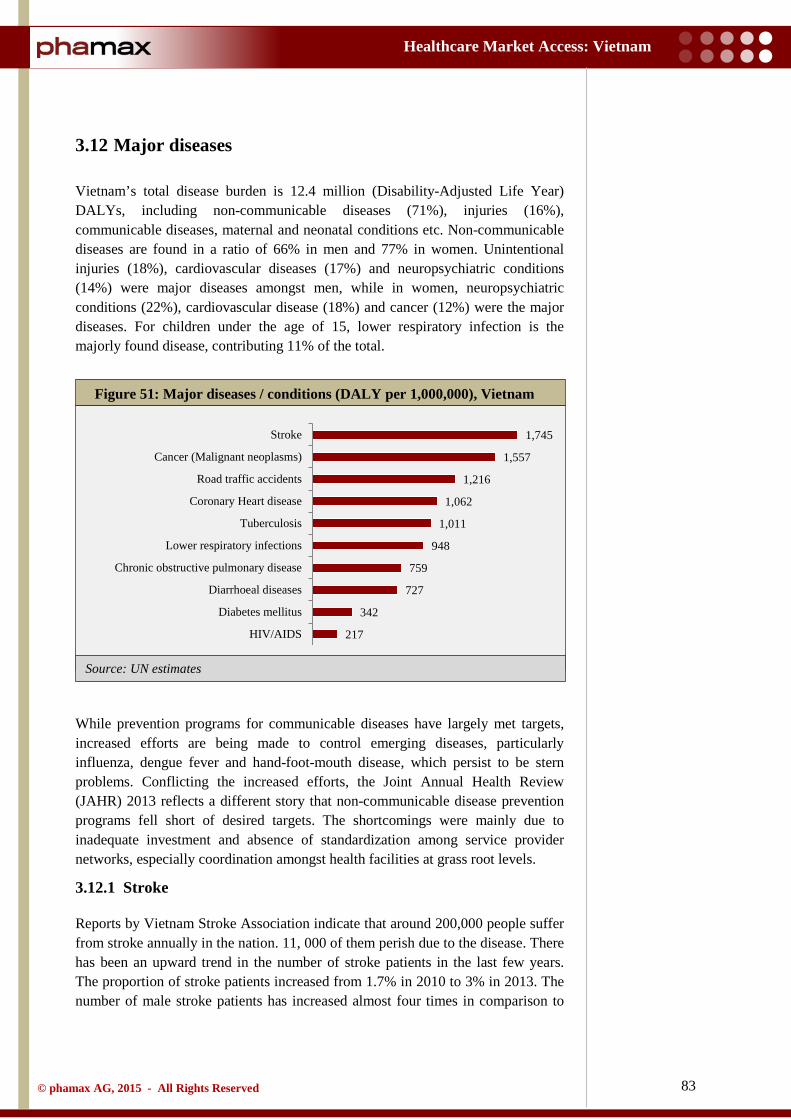
83
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: UN estimates
3.12 Major diseases
Vietnam’s total disease burden is 12.4 million (Disability-Adjusted Life Year) DALYs, including non-communicable diseases (71%), injuries (16%), communicable diseases, maternal and neonatal conditions etc. Non-communicable diseases are found in a ratio of 66% in men and 77% in women. Unintentional injuries (18%), cardiovascular diseases (17%) and neuropsychiatric conditions (14%) were major diseases amongst men, while in women, neuropsychiatric conditions (22%), cardiovascular disease (18%) and cancer (12%) were the major diseases. For children under the age of 15, lower respiratory infection is the majorly found disease, contributing 11% of the total.
While prevention programs for communicable diseases have largely met targets, increased efforts are being made to control emerging diseases, particularly influenza, dengue fever and hand-foot-mouth disease, which persist to be stern problems. Conflicting the increased efforts, the Joint Annual Health Review (JAHR) 2013 reflects a different story that non-communicable disease prevention programs fell short of desired targets. The shortcomings were mainly due to inadequate investment and absence of standardization among service provider networks, especially coordination amongst health facilities at grass root levels.
3.12.1 Stroke
Reports by Vietnam Stroke Association indicate that around 200,000 people suffer from stroke annually in the nation. 11, 000 of them perish due to the disease. There has been an upward trend in the number of stroke patients in the last few years. The proportion of stroke patients increased from 1.7% in 2010 to 3% in 2013. The number of male stroke patients has increased almost four times in comparison to
Figure 51: Major diseases / conditions (DALY per 1,000,000), Vietnam
1,745
1,557
1,216
1,062
1,011
948
759
727
342
217
Stroke
Cancer (Malignant neoplasms)
Road traffic accidents
Coronary Heart disease
Tuberculosis
Lower respiratory infections
Chronic obstructive pulmonary disease
Diarrhoeal diseases
Diabetes mellitus
HIV/AIDS
84
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
females. The Vietnam Association against Stroke (VAAS) states that the country’s inadequate healthcare infrastructure that affects timely treatment is one of the key reasons for the upward trends. Further, there are no official statistics available for treatment expenses for stroke patients. However, in an effort to minimize complications, the health sector had put into operation two more anti-stroke centers in October 2011, increasing the total number of these centers to sixteen across the country.
3.12.2 Cancer
Around 100,000 to 150,000 new cancer cases and 75,000 cancer deaths are reported each year in Vietnam (seven times higher than road injuries). These numbers have seen a sizeable increase in the decade from 2000 to 2010. In 2000, the occurrence of cancer in men was 141.6/100,000, which increased to 181.3/100,000 in 2010. Amongst women, cancer incidence in 2000 was 101.6/100,000, increasing to 139.9/100,000 in 2010. Stomach cancer, Lung cancer and Liver cancer were found to be most prevalent in men as well as women. According to JAHR, a national program for cancer prevention and treatment was initiated for the period 2012 - 2015, aimed to increase awareness of cancer, train healthcare workers in cancer detection and monitor the cancer care system. The frequency of cancer is on the rise in Vietnam, and delayed detection of the disease is thwarting effective therapy. The Vietnam Cancer Association has specified that controlling cancer will be a challenge since there are only six public hospitals specializing in cancer treatment and polyclinics with oncology departments in the state, indicating the scarcity of resources to meet the demands. Nonetheless, Vietnam is aided under the International Atomic Energy Authority’s technical cooperation Program of Action for Cancer Therapy, which offers technical expertise and backs government efforts for a national cancer control program.
3.12.3 Road traffic accidents
The number of accidents and deaths due to road traffic incidents has proliferated over the years. On an average, Vietnam reports around 30 deaths and 70 injuries due to accidents each day. According to the Health Statistics Yearbook 2010, the mortality rate for road traffic accidents was 17.9 per 100,000 of the population (men: 28.3/100,000, 3 times higher than women: 7.8/100,000).
3.12.4 Tuberculosis
Tuberculosis (TB) has been on a constant decline in the realm over the years. Vietnam’s National Tuberculosis Control Program, including activities to diagnose the disease in children, covers 100% of the population. Granting that the prevalence has come down from 225/100,000 in 2011 from 375/100,000 in 2000, the disease is yet to be effectively controlled. Vietnam needs to strive harder if it has to achieve the nation’s goal for tuberculosis control. The WHO-WPRO (Western Pacific Region) announced the goal to reduce tuberculosis prevalence and mortality by 50% from 2000 to 2015, yet Vietnam has currently achieved only a 40% reduction in prevalence and 38% reduction in mortality rates compared to
85
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
2000. Vietnam also introduced the Vietnam Stop TB Partnership (VSTP), officially established in the country in 2010. It has collaborated with various partners including government institutions, community institutions and international organizations for advocacy and awareness campaigns for the general population.
3.12.5 Diabetes mellitus
Diabetes is one of the more serious threats bothering Vietnam. As per a survey carried out by the National Hospital of Endocrinology, the prevalence of diabetes has increased to almost 6% from 2.7% in the last decade. To improve diagnosis and prompt treatment, the government plans to step up diabetes screening and setup specialty wards at provincial hospitals. Dearth of awareness of diabetes is a common problem, contributing to late detection and serious complications arising from the ailment. A diabetes care program is underway in the country as a collaborative initiative between the MoH and Novo Nordisk Vietnam, aimed at raising awareness, improving screening for those at risk, training doctors in diabetes management, improving access to diabetes care, and improving control of the disease in patients being treated.
3.12.6 HIV/AIDS
In June 2012, the HIV count in Vietnam was 204,019 and the number of AIDS patients was 58,569. HIV/AIDS prevalence in the community has increased from 187 to 224.3 per 100, 000 of the population in the last five years. About 41% of this HIV/AIDS infection is due to injections. To counter this prevalence, in 2012, the Prime Minister approved the National scheme (Decision No. 608/2012) for the control and prevention of HIV/AIDS.
86
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
4 Market Access
4.1 Stakeholder landscape
The healthcare system is swiftly changing as the stakeholder landscape in pharmaceutical industry continues to reshape itself. Like many other countries, payers and patients are taking a lead in driving the decision making process in Vietnam and its healthcare infrastructure continues to strengthen. It is taking bold steps with health financing reforms like universal coverage of health insurance across the country within a few years. Amidst the rising optimism, there are also challenges like poor coordination of activities within the fragmented healthcare system.
While social health insurance had steadily expanded to cover over 60% of the population by the end of 2012, voluntary participation by vulnerable groups such as the near poor still remained low. Thus, the National General Assembly had significantly scaled efforts to accelerate this transition towards universal access to affordable and quality healthcare services. Regardless of the path chosen, successful implementation requires many resources and institutions to be in place. The World Bank is supporting the efforts of the country in the transition towards universal health coverage with objectives like improving health outcomes, reducing financial risks associated with ill health, and increasing equity.
The pharmaceutical market in Vietnam is bound to see rapid growth in the coming years due to the numerous reforms that have come in. But, the industry is still heavily dependent on imported raw materials for domestic manufacturing, which continues to hamper drug prices. Further, the country lacks expertise and resources to manufacture pioneering medicines and therefore just focuses on generic drug manufacturing. However, imported products continue to relish higher sales owing to the local perception of imported products being of high quality. The new tendering laws are expected to favor sales of local generics, and also control the extortionate drug prices in the country.
The pharmaceutical companies are key stakeholders and one of the main beneficiaries in terms of revenue generation. Recent trends clearly exhibit the increasing role of pharmaceutical companies in the country’s policy shaping and decision making process, together with the regulatory agencies, payers and physicians. Companies no longer want to be perceived as only profit oriented, but as partners in providing healthcare solutions to the government and the community at large.
Furthermore, along with the complex healthcare system, the government of Vietnam also faces the intricacies of the pharmaceutical distribution system across the country. The chain includes wholesalers, retailers and pharmacies that widely vary across the region. These distributors not only have a strong impact on how margins and discounts are applied, but also have the power to influence policy making processes.
Like many other countries, payers and patients are taking a lead in driving decision making process in Vietnam.
Although health insurance has steadily expanded to cover over 60% of the population, the government faces challenges to achieve universal coverage as it requires many resources to be in place.
Foreign pharma companies have enjoyed dominance owing to the local perception of imported products being of high quality and lack of expertise of local companies. New tendering law favoring locally produced generics will force them to rethink strategy and engage more with regulatory agencies in policy shaping and decision making.

87
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Market dynamics for physicians in Vietnam reveal that the geographic preference for most physicians is the advanced urban localities while there is a lack of physicians in the rural areas. Although physician concentration is higher in urban healthcare centers, most juggle with dual jobs and therefore the availability again becomes an issue. Dual practice is prominent with almost one-third of physicians. Physician-patient relationship has also been hampered in the recent years due to the collusion between physicians and pharmaceutical representatives or pharmacies in the form of commission to prescribe certain drugs, private clinic sales of drugs with no prescriptions and many such incidents that affect the safety of patients. Vietnam pharmaceutical market also reports a high rate of self-medication, with prevalence around 40% - 60%. Nonetheless, despite being a neglected component of the healthcare system, physicians still play a crucial role in the country’s healthcare landscape.
Corruption is a misery that will continue to affect Vietnam's pharmaceutical and healthcare environment. Corruption continues to manifest itself in various forms, mainly, political influence in defining drug policies, illegal collusion of physicians and drug stores or pharmacies to influence prescriptions, bribery in influencing the drug procurement processes etc. The government has designed a series of reforms directly aimed at improving the country’s healthcare system. But, an unbiased assessment of the impact of these reforms is still deficient.
Although collusion between physicians and pharmaceutical companies remain an open secret, physicians still continue to play significant roles.
Corruption at various levels remains a critical issue and hinders patients’ access to cost-effective and quality healthcare processes.
88
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
4.2 Regulatory landscape
Vietnam has a legal framework for pharmaceuticals and continues to relentlessly improve it. The Pharmacy Law, issued in June 2005, implements regulations that govern the management of drugs and biologicals in Vietnam. The regulations provide guidelines on:
• Pharmaceutical business. • Registration and distribution of drugs. • Traditional herbal medicines and drugs from pharmaceutical materials. • Prescriptions and use of drugs. • Advertisement of drugs. • Provision of drugs in health facilities. • Clinical trials of drugs. • Management of addictive drugs, mental health medications, radioactive
materials etc. • Standards for quality of drugs and drug quality assurance.
The law, however, does not cover issues such as financial and economic mechanisms, monitoring and evaluation methods, or roles of health professionals.
The Vietnamese regulations on market authorization are in line with the Association of Southeast Asian Nations (ASEAN) Common Technical Dossier and ASEAN Common Technical Requirements. But, market authorization still faces challenges such as lack of tests for bio-equivalence and bio-availability of drugs, paving way to difficulties in the scientific assessment of drug efficacies.
The National Drug Policy was issued by the Vietnamese government in 1996 to ensure regular and sufficient supply of quality drugs for the population and the rational and safe use of these. This policy has not been updated since 1996.
4.2.1 Regulatory agencies
In Vietnam, the Ministry of Health (MoH) is the main regulatory authority. Under the MoH, the Drug Administration of Vietnam (DAV), established in 1996, is responsible for the regulation of pharmaceuticals. It evaluates pharmaceutical applications for their compliance with the 2005 Pharmaceutical Law. It has specific responsibilities which mainly include:
• Develop and issue legal documents on pharmaceuticals. • Manage the registration and circulation of pharmaceuticals. • Permit, suspend or revoke certificates of pharmaceutical trading,
manufacturing, import, export and circulation of drugs. • Coordinate with the Science and Training Department, under the MoH,
regarding clinical trials in Vietnam. • Manage drug advertising.
Under The Ministry of Health (MoH), Drug Administration of Vietnam (DAV) is the main agency responsible for the regulation of pharmaceuticals.
89
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
• Manage and coordinate with competent authorities for drug prices, carry out measures to stabilize the drug market, and manage tenders in hospitals.
• Inspect the implementation of provisions relating to drugs and punish violations.
4.2.2 Market authorization for pharmaceutical products
Under the MoH, DAV is responsible for reviewing the dossiers for market authorization. It has the rights to provide a valid duration as well as withdraw market authorization numbers if necessary. Establishments registering drugs are obligated to pay a fee upon filing of dossiers according to the provisions of law.
Some of the basic compliances for market authorization in Vietnam are as follows:
• Clinical trial results on the effectiveness and safety of drugs, except for those exempt from clinical trials provided by the Pharmacy Law.
• Technical documents on drugs. • Vietnam's national policies on drugs.
Within six months after receiving complete and valid dossiers, the MoH grants market authorization numbers. In case of refusal to grant authorization numbers, the MoH must reply in writing, clearly stating the reasons.
During the process, the companies themselves are required to take responsibilities for matters relating to intellectual property (viz. industrial design, brand name and inventions), since the Vietnamese regulation does not require checking of industrial design, brand name or inventions. The companies applying for market authorization can submit IP related documents in collaboration with the National Office of Intellectual Office of Vietnam (NOIP).
If any company violates IP regulations, the DAV may, after obtaining conclusions from the relevant authorities, withdraw the authorization number and suspend the company’s pharmaceutical products from the market.
The MoH encourages pharmaceutical companies to study all IP regulations thoroughly before marketing their products so as to avoid any non-compliance with the law. Foreign traders supplying drugs without authorization number in Vietnam must have licenses for operation in Vietnam granted by the MoH. In case the foreign traders with such operation licenses do not supply drugs which are needed for disease prevention and treatment, the MoH will consider the alternative to permit the import of these drugs from other drug suppliers in the world.
The process of receiving and evaluating market authorization dossiers is as follows:
Obtain the dossiers: The Drug Registration Department (DRD) receives the market authorization dossiers. Name of drugs and related information are numbered in sequence and accordingly recorded by the DRD.
DAV is responsible for providing market authorization (known as Visa) which is valid for five years.

90
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: MoH
Process: The DRD processes dossiers in a first-in-first-out (FIFO) sequence. After having received comments from all groups of specialists, the DRD prepares letters signed by the Director of the DAV (or deputy director on his behalf) informing the applicants of the evaluation results.
Though there are no separate regulations on authorization of biologicals (including vaccines), the procedures can vary from those for typical market authorization. All vaccines must undergo clinical trials in Vietnam for authorization purposes.
Figure 52: Market authorization process, Vietnam
Registration Request
Generic name
Trade name
Trade name protection at NoIP Vietnam
Pre-submission preparation
Manufacturer sign & stamp on dossier
Dossier submission to DAV
Dossier evaluation of jury
Evaluation result
VISA number
Passed Not yet passed
6 months
Supplementary Resubmit dossier Within
3 months from date of notice
91
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Finally, the MoH reviews the application and if approved, it issues the approval license (locally known as a VISA). Under the current regulations, although the review and approval process should be complete by six months, in practice the timeline for issuing a market authorization can range from one to two years. The market authorization of a product is valid for five years.
The MoH currently necessitates pharmaceutical firms to reapply for product approval through product visas every five years. This requirement has become a significant administrative liability since the process for renewal or to obtain a product visa can take anywhere between eight months to more than one year. Additionally, under Circular 22, it is not possible to submit a dossier for the renewal of market authorization earlier than six months before the expiry of the product’s existing authorization. Thus it leads to an off period for a product for several months. During this period, import of the product is not permitted and providing information to doctors about the product (promotions) is restricted. Moreover, the participation in hospital tenders during this period is also not allowed.
There are also concerns with carrying out domestic clinical trials in Vietnam for the marketing approval of all pharmaceuticals that have not been made available in their country of origin for more than five years. The member companies of Pharmaceutical Research and Manufacturers of America (PhRMA) state that this practice is unnecessary, considering that development and manufacture of drugs already follow stringent rules and rigorous protocols under USFDA and other regulatory agencies before introduction in Vietnam. This process is also applicable for vaccines and biologicals. The member companies ascertain that a change in the aforementioned amendment could quickly improve patient access to essential medicines.
4.2.3 Clinical trial regulations
In order to grant marketing authorization, MoH necessitates pharmaceutical companies to conduct clinical trials in Vietnam for drugs which have not been in the market of their origin for more than five years. At present, there are two main regulations generally governing clinical trials that apply to finished pharmaceuticals, vaccines and biological products:
• Circular No. 03/2012 of the MoH, providing guidance on clinical trials. • Decision No. 799 of the MoH, promulgating guidelines of Good Clinical
Practice.
The key regulatory authorities responsible for evaluating and approving applications for clinical trials include the MoH, the Department of Science and Training and the Department of Biomedical Research Ethics Council.
Although the review and approval process for granting VISA completes in six months, in reality it ranges from one to two years.
Regulations for renewing VISA often lead to an off-visa period on non-compliance for drugs during which imports and participation in tenders is not allowed, and marketing is also restricted.
In order to grant marketing authorization, MoH necessitates pharmaceutical companies to conduct clinical trials in Vietnam for drugs which have not been in the market of their origin for more than five years.
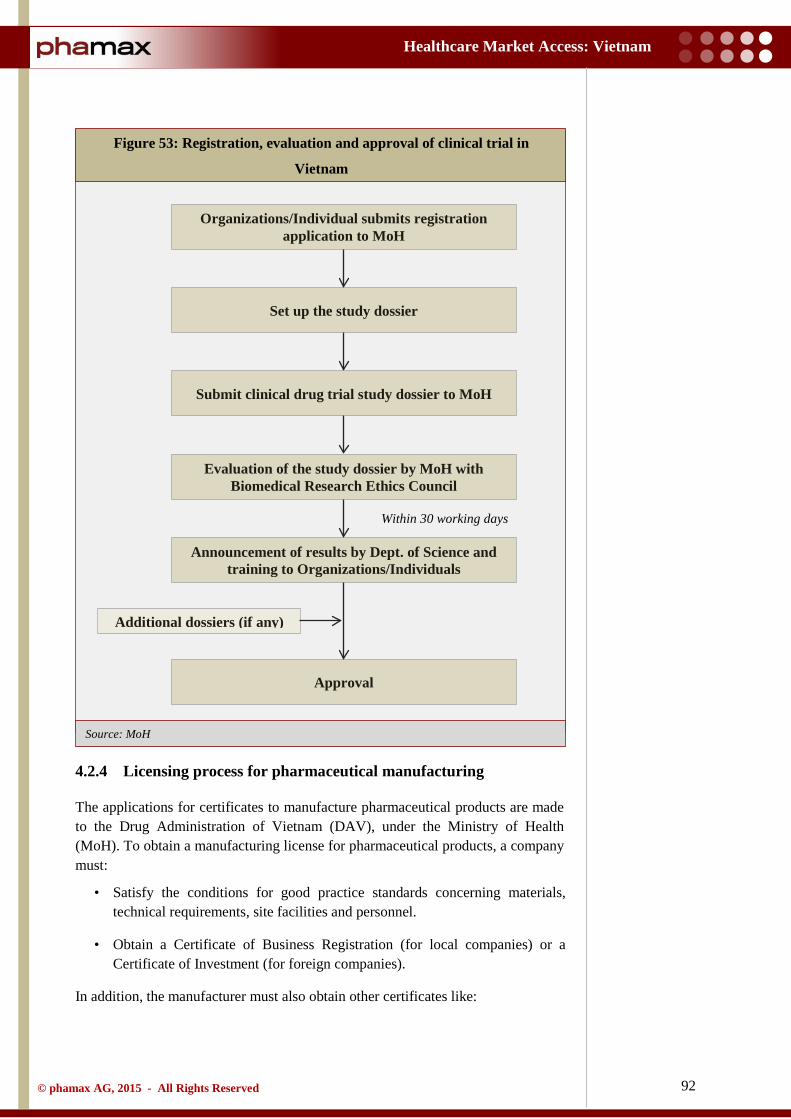
92
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: MoH
4.2.4 Licensing process for pharmaceutical manufacturing
The applications for certificates to manufacture pharmaceutical products are made to the Drug Administration of Vietnam (DAV), under the Ministry of Health (MoH). To obtain a manufacturing license for pharmaceutical products, a company must:
• Satisfy the conditions for good practice standards concerning materials, technical requirements, site facilities and personnel.
• Obtain a Certificate of Business Registration (for local companies) or a Certificate of Investment (for foreign companies).
In addition, the manufacturer must also obtain other certificates like:
Figure 53: Registration, evaluation and approval of clinical trial in
Vietnam
Organizations/Individual submits registration application to MoH
Set up the study dossier
Submit clinical drug trial study dossier to MoH
Evaluation of the study dossier by MoH with Biomedical Research Ethics Council
Announcement of results by Dept. of Science and training to Organizations/Individuals
Approval
Additional dossiers (if any)
Within 30 working days
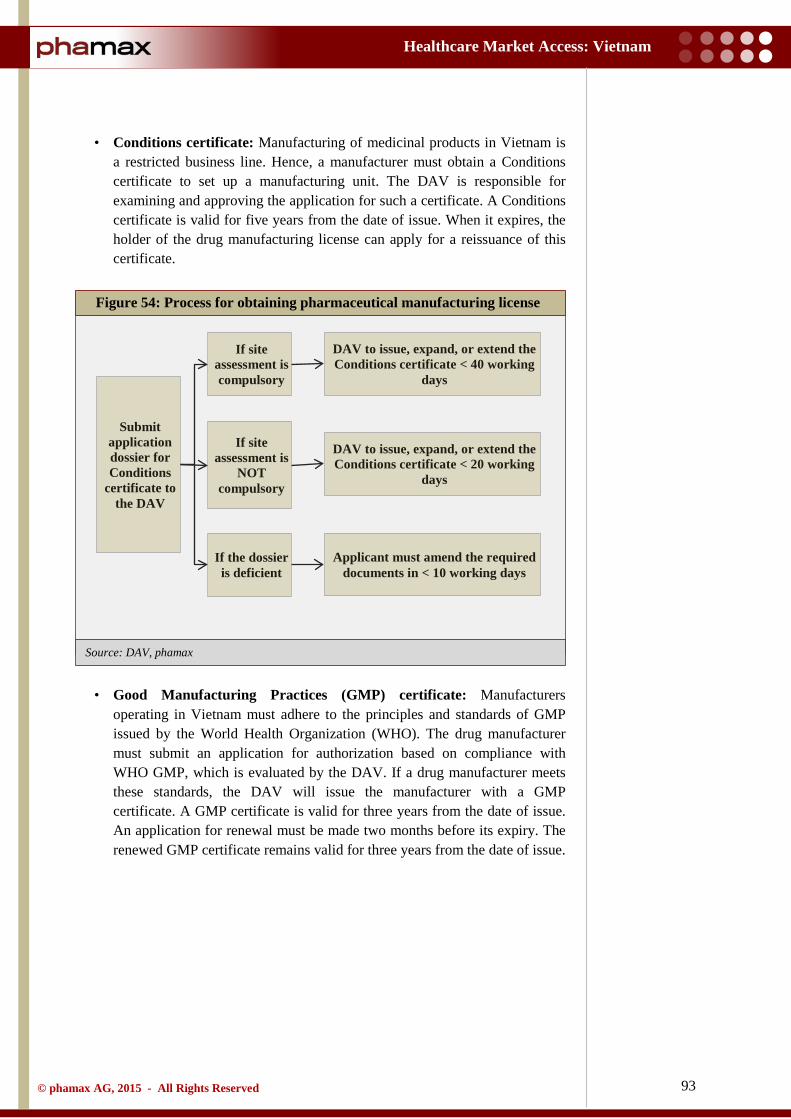
93
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: DAV, phamax
• Conditions certificate: Manufacturing of medicinal products in Vietnam is a restricted business line. Hence, a manufacturer must obtain a Conditions certificate to set up a manufacturing unit. The DAV is responsible for examining and approving the application for such a certificate. A Conditions certificate is valid for five years from the date of issue. When it expires, the holder of the drug manufacturing license can apply for a reissuance of this certificate.
• Good Manufacturing Practices (GMP) certificate: Manufacturers operating in Vietnam must adhere to the principles and standards of GMP issued by the World Health Organization (WHO). The drug manufacturer must submit an application for authorization based on compliance with WHO GMP, which is evaluated by the DAV. If a drug manufacturer meets these standards, the DAV will issue the manufacturer with a GMP certificate. A GMP certificate is valid for three years from the date of issue. An application for renewal must be made two months before its expiry. The renewed GMP certificate remains valid for three years from the date of issue.
Figure 54: Process for obtaining pharmaceutical manufacturing license
Submit application dossier for Conditions
certificate to the DAV
If site assessment is compulsory
If the dossier is deficient
If site assessment is
NOT compulsory
DAV to issue, expand, or extend the Conditions certificate < 40 working
days
Applicant must amend the required documents in < 10 working days
DAV to issue, expand, or extend the Conditions certificate < 20 working
days
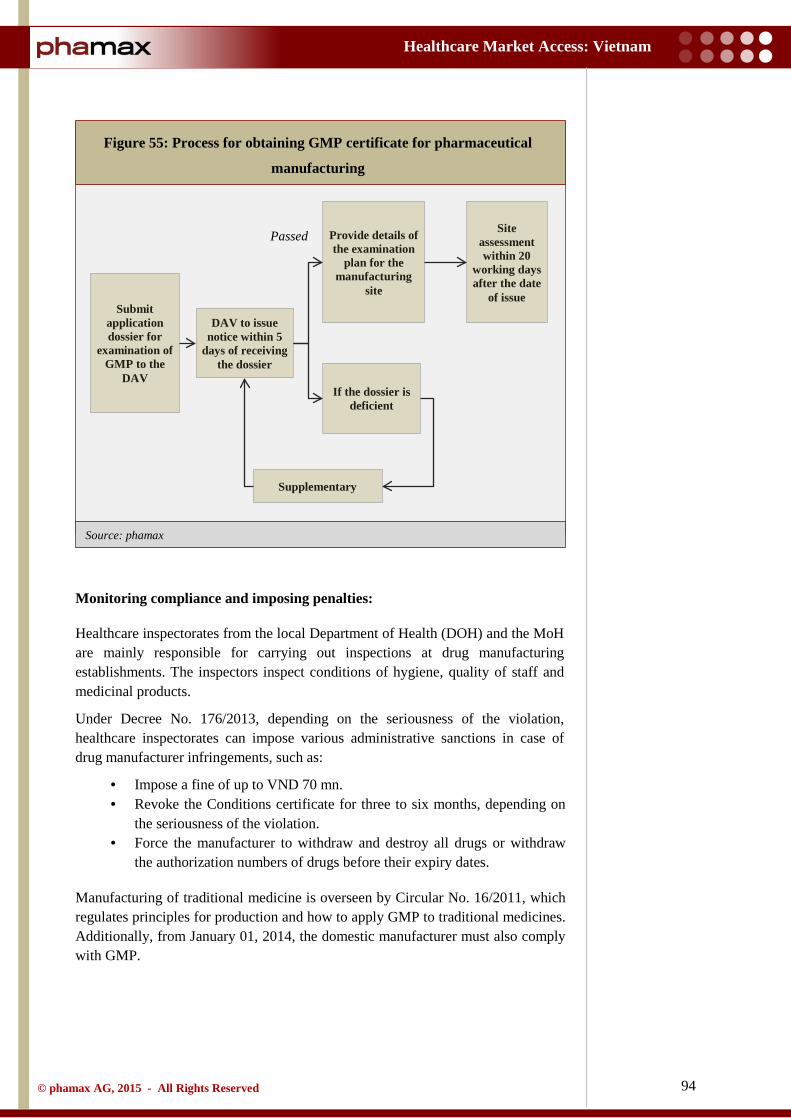
94
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: phamax
Monitoring compliance and imposing penalties:
Healthcare inspectorates from the local Department of Health (DOH) and the MoH are mainly responsible for carrying out inspections at drug manufacturing establishments. The inspectors inspect conditions of hygiene, quality of staff and medicinal products.
Under Decree No. 176/2013, depending on the seriousness of the violation, healthcare inspectorates can impose various administrative sanctions in case of drug manufacturer infringements, such as:
• Impose a fine of up to VND 70 mn. • Revoke the Conditions certificate for three to six months, depending on
the seriousness of the violation. • Force the manufacturer to withdraw and destroy all drugs or withdraw
the authorization numbers of drugs before their expiry dates.
Manufacturing of traditional medicine is overseen by Circular No. 16/2011, which regulates principles for production and how to apply GMP to traditional medicines. Additionally, from January 01, 2014, the domestic manufacturer must also comply with GMP.
Figure 55: Process for obtaining GMP certificate for pharmaceutical
manufacturing
Submit application dossier for
examination of GMP to the
DAV
Provide details of the examination
plan for the manufacturing
site
If the dossier is deficient
DAV to issue notice within 5
days of receiving the dossier
Site assessment within 20
working days after the date
of issue
Passed
Supplementary
95
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
4.2.5 Licensing process for pharmaceutical imports
The Drug Administration of Vietnam (DAV) regulates the import and export of pharmaceutical products in the country. The Pharmacy Law, issued in June 2005, under Article 63, defines that drugs with authorization numbers in Vietnam can be imported without quantity limitations, except for vaccines, biological products and specially controlled drugs (e.g. habit‐forming drugs, psychotropic drugs etc.).
Drug trading establishments have rights to import and delegate the import or export of drug types specified by the MoH. The allocation of export or import of drugs must comply with the provisions of the Commercial Law and other relevant provisions of law.
However, there is a special case for importing drugs without authorization numbers in Vietnam for the special medical treatment needs of hospitals. Drugs without authorization numbers may be imported in specified quantities in the following cases:
• They contain pharmaceutical ingredients with or without authorization numbers, which are, however, insufficient to fully meet treatment needs.
• They are imported to meet urgent needs of disease or epidemic prevention, overcome consequences of natural calamities or catastrophes and for special treatment needs.
• They are imported in service of national health programs. • They are donations. • They are imported for clinical trials, for use as registration samples or for
exhibitions or trade fairs. • The Prime Minister authorizes the import of drugs without authorization
numbers.
4.2.6 Post-marketing regulations
In Vietnam, an organization must comply with the quality and safety requirements as agreed to during the marketing authorization. The maximum duration of validity for marketing authorization is five years from the date of approval. However, the duration of valid marketing authorization is one year for special cases (e.g. for narcotics or anti-depressants).
The DAV mandates manufacturers and distributors to report adverse drug reactions to the National Center for Drug Information (NDI) and Adverse Drug Reactions (ADR) Centre (process given in the figure below). Once a year, all adverse drug reactions must be reported to the respective authorities. In case of any serious or unexpected adverse drug reactions, the DAV mandates companies to report the occurrence within ten working days from the date of receipt of information. Also, notifications of withdrawal of any market authorization in any country must be reported to the DAV, immediately after receiving the information.
Drugs with authorization numbers in Vietnam can be imported without quantity limitations except for vaccines, biological products and specially controlled drugs.
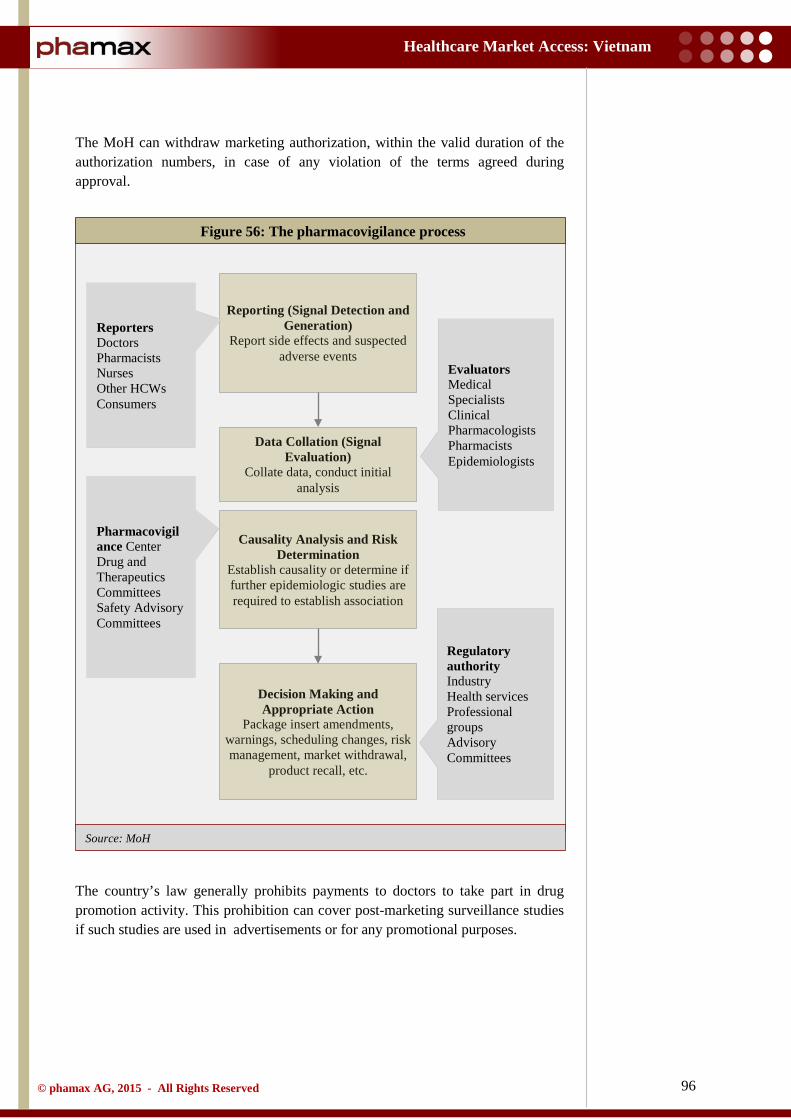
96
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: MoH
The MoH can withdraw marketing authorization, within the valid duration of the authorization numbers, in case of any violation of the terms agreed during approval.
The country’s law generally prohibits payments to doctors to take part in drug promotion activity. This prohibition can cover post-marketing surveillance studies if such studies are used in advertisements or for any promotional purposes.
Figure 56: The pharmacovigilance process
Reporting (Signal Detection and Generation)
Report side effects and suspected adverse events
Data Collation (Signal Evaluation)
Collate data, conduct initial analysis
Causality Analysis and Risk Determination
Establish causality or determine if further epidemiologic studies are required to establish association
Decision Making and Appropriate Action
Package insert amendments, warnings, scheduling changes, risk management, market withdrawal,
product recall, etc.
Reporters Doctors Pharmacists Nurses Other HCWs Consumers
Pharmacovigilance Center Drug and Therapeutics Committees Safety Advisory Committees
Evaluators Medical Specialists Clinical Pharmacologists Pharmacists Epidemiologists
Regulatory authority Industry Health services Professional groups Advisory Committees
97
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
4.2.7 Advertising
In Vietnam, advertising of pharmaceuticals are controlled by stringent regulations. There are numerous rules regulating advertisement in general, and a number of laws specifically governing advertisements in the healthcare sector. The primary legislation regulating the advertisement of drugs in Vietnam is promulgated under Circular No. 13/2009.
Under Circular 13, ‘Drug Advertising’ is defined as the introduction of drugs by a drug trader to promote the prescription, supply, sale, and/or use of drugs in a proper, safe, and effective manner. Such introduction also includes introductions made through sponsorship or authorization by the drug trader to another individual or organization or collaboration between the parties.
The DAV is the prime regulatory authority which examines and approves drug advertisement records with other authorities (People’s Committee, the Department of Culture, Sports and Tourism, the Department of Health etc.). In general, information provided to health professionals must be submitted to the DAV for approval. The only exception to this requirement is for information that has previously been submitted to and approved by the DAV in market authorization dossiers, including drug labels and instructions of use.
Prescription drugs cannot be directly advertised to the general population in Vietnam. Companies are permitted to introduce and provide information on prescription drugs distributed to medical professionals including pharmacists and administrators. This generally takes place through either of these channels - licensed medical representatives (locally known as drug introducers), distribution of information through documents or by seminars and conferences.
4.2.8 Labeling and packaging
Packaging and labeling of pharmaceuticals follows guidelines as drafted in Circular 04/2008. This legislation is enforced by the MoH, particularly the DAV.
A label of a drug circulated in the market must satisfy the following content requirements:
• The names of the drug. • The form and composition of the drug. • Packing specifications. • Information on manufacturers, importers, distributors etc. • The authorization number, serial number of the manufacture lot, date of
manufacture and expiry (if applicable). • Conditions for drug preservation and other necessary information. • Drug use instructions (must be in Vietnamese).
If the original labels of medical products imported into Vietnam do not bear, or fail to adequately bear mandatory content in Vietnamese, they must have auxiliary
98
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
labels bearing the mandatory content in Vietnamese, while the original labels must be kept intact. Label content and use instruction inserts must:
• Be truthful, clear and accurate. • Not be misleading about the true nature and effect of the medicine.
4.2.9 Intellectual property rights
In June 2009, the National Assembly of Vietnam adopted a new law on Intellectual Property (Amended IP Law), to amend a number of articles of the existing IP Law passed in November 2005. The Amended IP Law aims at encouraging innovation, improving IP management system and bringing it into compliance with the Trade Related Aspects of Intellectual Property Rights (TRIPS). The Amended IP Law came into force on January 01, 2010. The National Office of Intellectual Office of Vietnam (NOIP) holds the chief coordinator role in the amended law.
Vietnam has been a member of the World Trade Organization (WTO) since 2007. In accordance with the WTO regulations, the Vietnamese legislation outlines a patent protection for an invention in Vietnam for 20 years and data protection against unfair commercial use of a product.
Subsequently, the ongoing negotiations by Vietnam to join the Trans Pacific Partnership (TPP) free trade agreement will require the country to allow an additional period of data protection, undoubtedly resulting in a rearrangement of the existing situation.
Pursuant to its WTO requirements in respect to TRIPS, Vietnam has also joined a number of international IPR conventions. Until now, Vietnam has been party to four international agreements in the field of industrial property:
• The Paris Convention for the Protection of Industrial Property. • The Convention establishing the World Intellectual Property
Organization. • The Patent Cooperation Treaty. • The Madrid Agreement on the International Registration of Marks .
Similarly, Vietnam has committed to the following Bilateral Agreements:
• Agreement between the United States of America and the Socialist Republic of Vietnam on Trade Relations (BTA).
• Agreement between the Government of the Socialist Republic of Vietnam and the Swiss Federal Council on the Protection of Intellectual Property and on Cooperation in the Field of Intellectual Property.
Being a member of WTO, legislation outlines a patent protection for an invention in Vietnam for 20 years and data protection against unfair commercial use of a product.
Ongoing negotiations by Vietnam to join the Trans Pacific Partnership (TPP) free trade agreement will require it to allow an additional period of data protection.
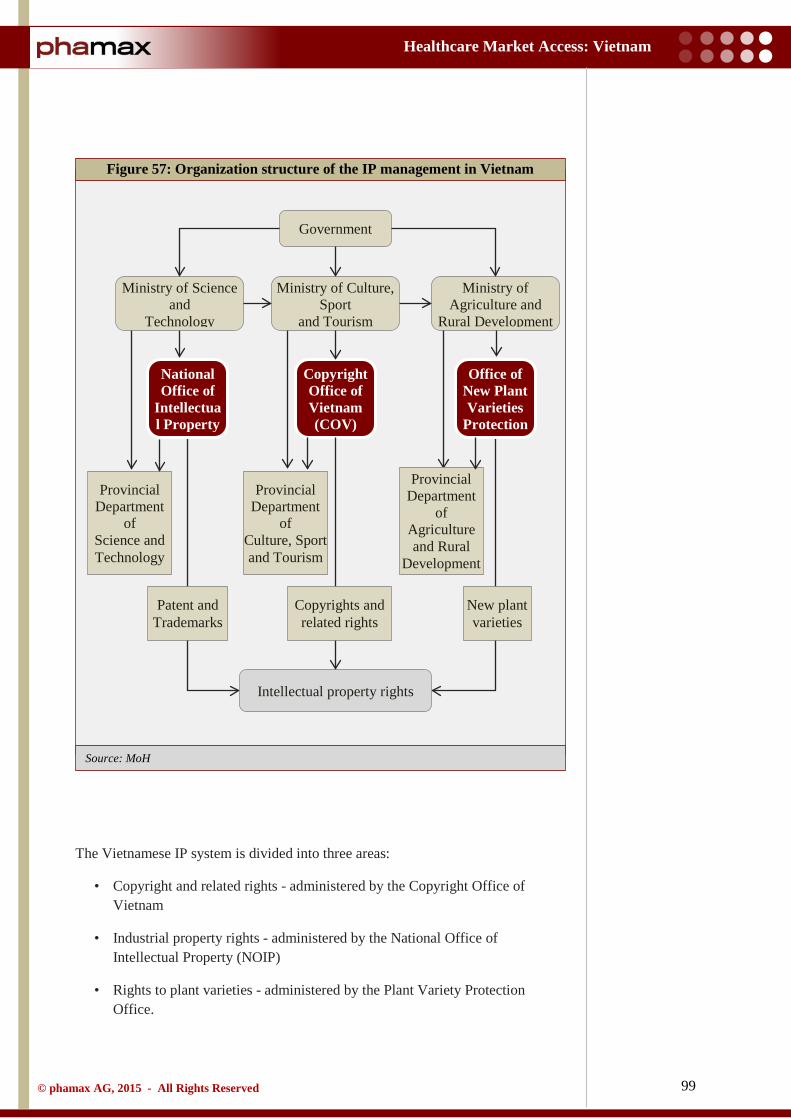
99
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
The Vietnamese IP system is divided into three areas:
• Copyright and related rights - administered by the Copyright Office of Vietnam
• Industrial property rights - administered by the National Office of Intellectual Property (NOIP)
• Rights to plant varieties - administered by the Plant Variety Protection Office.
Figure 57: Organization structure of the IP management in Vietnam
Government
Ministry of Science and
Technology
Ministry of Agriculture and
Rural Development
Ministry of Culture, Sport
and Tourism
National Office of
Intellectual Property
Copyright Office of Vietnam (COV)
Office of New Plant Varieties
Protection
Provincial Department
of Culture, Sport and Tourism
Provincial Department
of Agriculture and Rural
Development
Provincial Department
of Science and Technology
Patent and Trademarks
New plant varieties
Intellectual property rights
Copyrights and related rights
Source: MoH
100
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Despite all comprehensive legislation, covering every aspect of IP protection in accordance with international standards, Vietnam still faces significant concerns related to IP. Violations of these rights are increasing in number, as they get more difficult to identify. A major share of Vietnam’s generic drug market constitutes low-quality copies of unproven bioequivalent products. Though Vietnam’s pact with WTO did provide some improvements in this regard, stricter enforcement is required, otherwise any improvement of Vietnam’s IP protection regime is likely to remain disorganized. Although Vietnam has issued a circular granting a five-year term of regulatory data protection, it is not clear whether it applies to generic products relying on or referencing innovator data in support of its marketing approval application. Furthermore, the circular conditions require that:
• Member companies submit a separate application for data protection rather than receive automatic protection upon marketing approval as per WTO’s TRIPS requirements.
• Data be classified as ‘trade secret’ under Vietnamese law. • The innovator proves ‘ownership’ of the data in cases of dispute, rather
than the third party or government challenger. Thus, the conditions make it virtually impossible for innovator drugs to have data protection.
According to the report published by Pharmaceutical Research and Manufacturers of America (PhRMA), innovator companies continue to face delays in the grant of patents, which is eroding the rights available for innovative medicines. In addition, PhRMA has also highlighted that the reasons for such delays is prominently the insufficient personnel capacity at the respective regulatory bodies. The association further suggested that Vietnam should adopt more effective mechanisms in preventing the infringement of patents prior to the granting of marketing approval for follow-on products.
Violations of IP, weak data protection and delays in granting patents are some of the major concerns for pharma companies, especially foreign MNCs. The government will have to do more to fall in line with international best practices.
101
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
4.3 Pricing
Pricing of medicines in Vietnam still remains a controversial issue. During 2008 - 2012, the average spending on drugs per capita rose from $15.9 to $25.8. Expenditure on medicines in Vietnam currently accounts for 40% of total healthcare spending. Consequently, both availability and affordability of drugs are low, particularly in the public sector. According to market reports, the prices to patients for some medicines were up to ten times their imported prices, which conclude that low adherence to medicine pricing regulations is a key factor impacting prices. In addition, heavy dependence on imported drugs and decentralized drug procurement process fuel the drug prices.
Although a pharmaceutical law was introduced, the current pharmaceutical regulation system has not kept its pace with rapid changes in the pharmaceutical market, especially the rise of the private health sector. Vietnam’s legislation and regulations regarding medicine prices are numerous and quite complex. These regulations were intended to ensure transparency of medicine prices along the supply chain, through the mechanism of price declaration and publication of price information. However, these initiatives have not been successful as expected, as they failed to address all the preconditions necessary for the laws to operate effectively.
In 2006, the MoH assigned the DAV to assist the Minister of Health to fulfill the task of State management of medicine prices regulated by the pharmaceutical law. Accordingly, the Drug Price Management Division was established. This division at present has only four staff members and faces difficulties in the management of prices of 20,066 medicines, especially when the medicine pricing policies are in the starting phase. This task has become even more difficult in the absence of a strong regulation enforcement capacity, with a shortage of pharmaceutical inspectorate personnel and a weak, inconsistent and unclear sanction system.
Furthermore, the ongoing negotiation for the Trans Pacific Partnership (TPP) by Vietnam and several other countries is expected to allow additional data exclusivity period which will delay the generics entry and thus restrict the country’s ability to contain the rising drug costs.
4.3.1 Pricing system
The regulatory framework for medicine pricing in Vietnam is based on a modified free market pricing structure. Pharmaceutical law no. 34/2005 states that medicine suppliers and distributors are free to set prices of their products based on market forces, subject to stabilization by the state.
Establishments are required to declare the projected wholesale, retail and import prices of the drugs to the DAV while applying for market authorization. Once the price is stated, the enterprise is not allowed to sell their products at prices higher than the declared value. In cases where they hike prices, the organizations are expected to declare the value again before applying. On the other hand, in case the
In absence of an adequate price control policy, drug prices remain high due to heavy dependence on imported drugs and a decentralized drug procurement process.
The regulatory framework for medicine pricing in Vietnam is based on a modified free market pricing structure. Suppliers and distributors are free to set prices of their products based on market forces, subject to stabilization by the state.

102
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
organization sells drugs at prices lower than the declared price, it must also follow the anti-dumping regulations of the country.
According to the pharmacy law, drug prices that are declared must not be higher than those of drugs imported into regional countries with healthcare and commercial conditions similar to those of Vietnam (reference pricing). The MoH has announced these reference countries for comparison lists to set medicine prices. These countries include Thailand, Malaysia, Indonesia, the Philippines and Cambodia. However, there is a lack of clarity over price definitions, with regulations not explicitly defining the type of prices for international comparisons (i.e. ex-factory price or wholesale price or retail price, inclusive of taxes etc.). The DAV announces the price list for drugs produced in Vietnam on its website.
4.3.2 Pricing policy
In 2003, the Vietnamese Government requested that the Ministry of Health, in cooperation with the Ministry of Finance, issue a joint circular guiding price management for essential medicines to stabilize medicine prices. Subsequently, Joint Circular 08 was issued that came into force on August 21, 2003. The circular met with limited success as medicine prices continued to increase.
Following the criticisms of the weakness of Circular 08, mainly about its inadequacy to manage drug prices and also that an effective policy was needed to stabilize drug price margins, the Ministry of Finance collaborated with the Ministry of Health to develop a government decree on managing drug prices. In 2004, Decree No. 120 was passed including ceilings on mark-ups and requirements that declared prices to be compared to international reference prices (indirectly referred to ex-factory prices for comparison) to determine reasonableness.
However, a study in 2005 by World Health Organization (WHO) discovered another problem with drug prices in Vietnam. Not only was there rapid inflation, but drug price levels in Vietnam were extremely high. So much so that the prices in Vietnam were 8.3 times higher than international reference prices for the same drugs. Evidence from this study was used to constrict the drug price policy, replacing Decree 120 with Decree 79 in 2006 and Circular 11 (2007) to guide its implementation. These revisions encompassed ceilings on drug price margins, which had proven difficult to implement, and clarified on prices that were to be used for comparison.
Circular 11 used average cost, insurance, and freight (CIF) price of the medicine as a benchmark for comparison with regional comparable countries. But, it did not specify what type of prices declared in Vietnam should be used for comparison. According to the PhRMA member companies, this system of pricing was creating unequal opportunities and restrictions for imported products against locally manufactured products. This was mainly because trade in Vietnam relied on third party arrangements (requires mandatory local firms for distribution rights), which resulted in exorbitant CIF prices within Vietnam. Moreover, this system applied to imported products and not on locally manufactured drugs which were priced based on manufacturing costs.
Establishments are required to declare the projected wholesale, retail and import prices of the drugs to the DAV while applying for market authorization. However, declared prices must not be higher than those of drugs imported into regional countries with healthcare and commercial conditions similar to those of Vietnam.
Currently, Vietnam uses cost, insurance, and freight (CIF) price for reference pricing, which foreign pharma companies claim to be unfair for imported products.
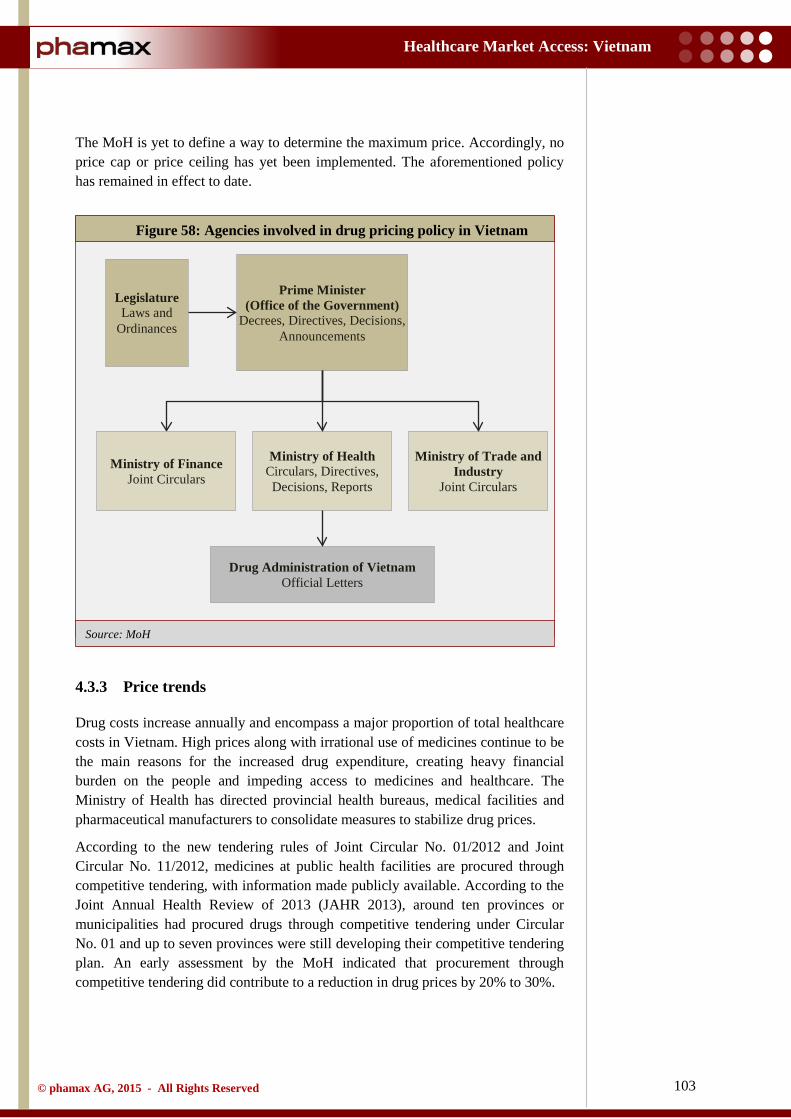
103
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: MoH
The MoH is yet to define a way to determine the maximum price. Accordingly, no price cap or price ceiling has yet been implemented. The aforementioned policy has remained in effect to date.
4.3.3 Price trends
Drug costs increase annually and encompass a major proportion of total healthcare costs in Vietnam. High prices along with irrational use of medicines continue to be the main reasons for the increased drug expenditure, creating heavy financial burden on the people and impeding access to medicines and healthcare. The Ministry of Health has directed provincial health bureaus, medical facilities and pharmaceutical manufacturers to consolidate measures to stabilize drug prices.
According to the new tendering rules of Joint Circular No. 01/2012 and Joint Circular No. 11/2012, medicines at public health facilities are procured through competitive tendering, with information made publicly available. According to the Joint Annual Health Review of 2013 (JAHR 2013), around ten provinces or municipalities had procured drugs through competitive tendering under Circular No. 01 and up to seven provinces were still developing their competitive tendering plan. An early assessment by the MoH indicated that procurement through competitive tendering did contribute to a reduction in drug prices by 20% to 30%.
Figure 58: Agencies involved in drug pricing policy in Vietnam
Legislature Laws and
Ordinances
Drug Administration of Vietnam Official Letters
Prime Minister (Office of the Government)
Decrees, Directives, Decisions, Announcements
Ministry of Finance Joint Circulars
Ministry of Health Circulars, Directives, Decisions, Reports
Ministry of Trade and Industry
Joint Circulars
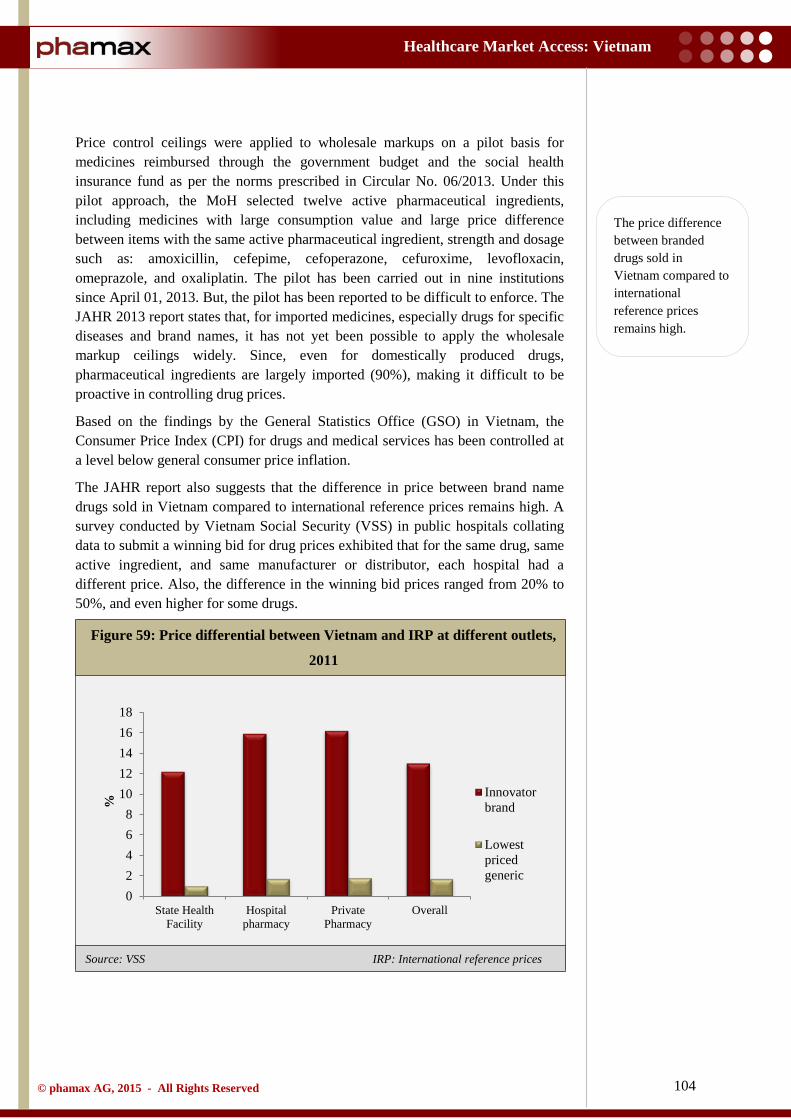
104
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: VSS IRP: International reference prices
Price control ceilings were applied to wholesale markups on a pilot basis for medicines reimbursed through the government budget and the social health insurance fund as per the norms prescribed in Circular No. 06/2013. Under this pilot approach, the MoH selected twelve active pharmaceutical ingredients, including medicines with large consumption value and large price difference between items with the same active pharmaceutical ingredient, strength and dosage such as: amoxicillin, cefepime, cefoperazone, cefuroxime, levofloxacin, omeprazole, and oxaliplatin. The pilot has been carried out in nine institutions since April 01, 2013. But, the pilot has been reported to be difficult to enforce. The JAHR 2013 report states that, for imported medicines, especially drugs for specific diseases and brand names, it has not yet been possible to apply the wholesale markup ceilings widely. Since, even for domestically produced drugs, pharmaceutical ingredients are largely imported (90%), making it difficult to be proactive in controlling drug prices.
Based on the findings by the General Statistics Office (GSO) in Vietnam, the Consumer Price Index (CPI) for drugs and medical services has been controlled at a level below general consumer price inflation.
The JAHR report also suggests that the difference in price between brand name drugs sold in Vietnam compared to international reference prices remains high. A survey conducted by Vietnam Social Security (VSS) in public hospitals collating data to submit a winning bid for drug prices exhibited that for the same drug, same active ingredient, and same manufacturer or distributor, each hospital had a different price. Also, the difference in the winning bid prices ranged from 20% to 50%, and even higher for some drugs.
Figure 59: Price differential between Vietnam and IRP at different outlets,
2011
02468
1012141618
State HealthFacility
Hospitalpharmacy
PrivatePharmacy
Overall
% Innovator
brand
Lowestpricedgeneric
The price difference between branded drugs sold in Vietnam compared to international reference prices remains high.

105
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
In addition, the pharmaceutical companies declare higher prices at the time of authorization, so as to avoid having to declare gain for an increase. As long as the price rise stays below the declared prices, they are not penalized. However, these artificial higher prices pose a problem when a product goes off patent, and it becomes difficult to reduce the prices.
The government has shown no signs to overhaul the pricing system, expecting the new tendering rules to have desired results. But, the stringent control of prices throw forth many difficulties. The competitive tendering for drug procurement has exposed shortcomings such as excessive attention to price criteria, lack of balance between price and quality etc. Further, classification of drugs into groups by technical standards lacks clarity and is ambiguous.
The prices vary in the range of 20% to 50% among the winning bids even for the same drug and same manufacturer or distributor.
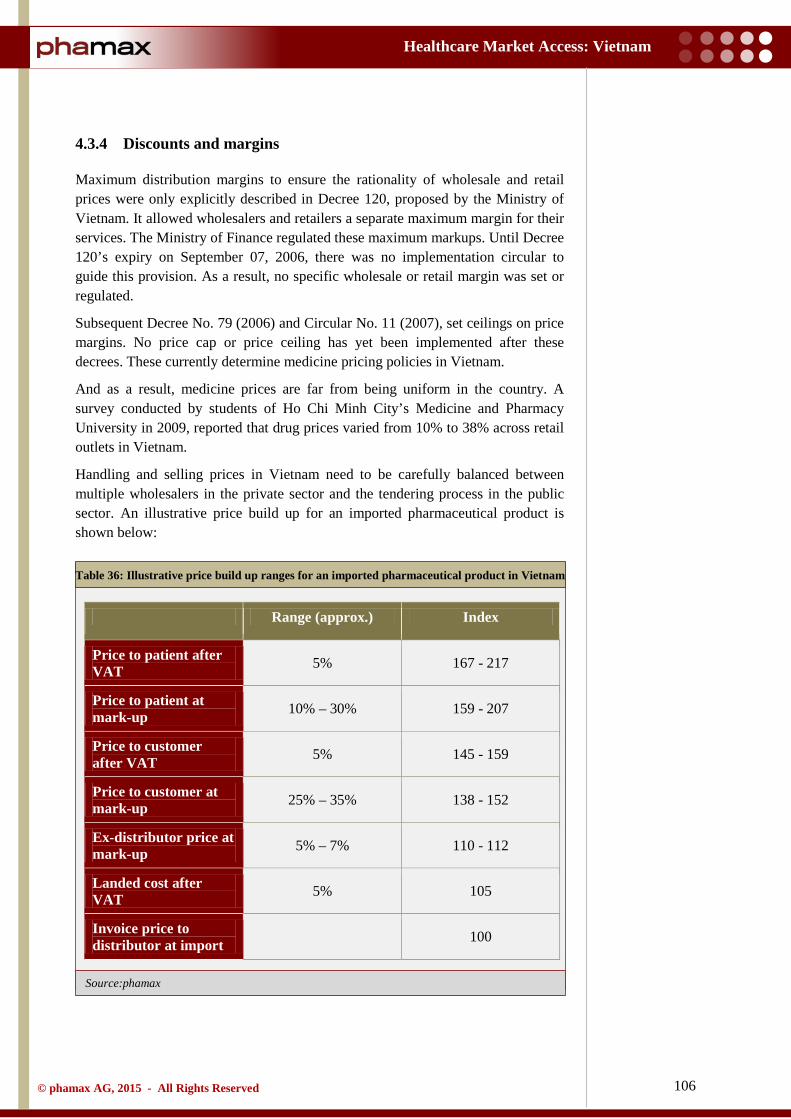
106
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source:phamax
4.3.4 Discounts and margins
Maximum distribution margins to ensure the rationality of wholesale and retail prices were only explicitly described in Decree 120, proposed by the Ministry of Vietnam. It allowed wholesalers and retailers a separate maximum margin for their services. The Ministry of Finance regulated these maximum markups. Until Decree 120’s expiry on September 07, 2006, there was no implementation circular to guide this provision. As a result, no specific wholesale or retail margin was set or regulated.
Subsequent Decree No. 79 (2006) and Circular No. 11 (2007), set ceilings on price margins. No price cap or price ceiling has yet been implemented after these decrees. These currently determine medicine pricing policies in Vietnam.
And as a result, medicine prices are far from being uniform in the country. A survey conducted by students of Ho Chi Minh City’s Medicine and Pharmacy University in 2009, reported that drug prices varied from 10% to 38% across retail outlets in Vietnam.
Handling and selling prices in Vietnam need to be carefully balanced between multiple wholesalers in the private sector and the tendering process in the public sector. An illustrative price build up for an imported pharmaceutical product is shown below:
Table 36: Illustrative price build up ranges for an imported pharmaceutical product in Vietnam
Range (approx.) Index
Price to patient after VAT 5% 167 - 217
Price to patient at mark-up 10% – 30% 159 - 207
Price to customer after VAT 5% 145 - 159
Price to customer at mark-up 25% – 35% 138 - 152
Ex-distributor price at mark-up 5% – 7% 110 - 112
Landed cost after VAT 5% 105
Invoice price to distributor at import 100
107
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
4.4 Reimbursement landscape
4.4.1 Reimbursement process
In Vietnam, reimbursement of prescription drugs is determined by the reimbursement drug list issued by the MoH (issued in 2008). The Vietnam Social Security (VSS) is the main entity that reimburses services provided to patients covered by social health insurance (SHI).
The SHI constitutes three types of provider payment mechanisms, namely fee-for-service, capitation, and payment by diagnosis-related groups (DRGs). Fee-for-service payment was officially introduced as a payment method for the social health insurance agency in 1995, after the collection of user fees had been legalized at government health facilities. It is now the dominant payment mechanism at all health facilities, both public and private and is used to pay provincial and central (tertiary) hospitals and referral health services.
Capitation payment is used to pay for primary healthcare, i.e., outpatient and inpatient healthcare at commune health stations and district hospitals that switched to capitation payment. Capitation was first piloted in 2004 at a low scale. By 2009, about 40 district hospitals (out of more than 600 district hospitals), functioned on the capitation model.
Payment by DRGs is only at a pilot stage. Since hospitals have the rights to choose between capitation and fee-for-service, most hospitals still prefer payment based on fee-for-service. To contain costs, the MoH issued a Circular in 2009 that aimed at gradually expanding capitation with the goal of applying this payment mechanism in all district hospitals and commune health stations by 2015.
The Health Insurance Law (effective 2009) set up an insurance fund functioning on premium payments. This was used to cover costs of medical care for the insured, managerial costs of health insurance institutions and other lawful costs related to health insurance. There are three levels of benefits under health insurance schemes - complete coverage or 100% of expenses at nominated medical facilities, 95% and 80% of the expenses with the patient making up the rest. Since there are no reimbursements for drugs dispensed at retail pharmacies, discussions are in process to introduce this for drugstores that comply with Good Pharmacy Practice (GPP).
4.4.2 Insurance providers
Healthcare in Vietnam is financed through various sources, including individual out-of-pocket payments, central and provincial government tax revenues, supply-side subsidies, and to a smaller extent, private insurance and external aid. To curb the high incidence of catastrophic household spending, Vietnam has introduced various reforms, culminating in the 2003 introduction of the Healthcare Fund for the Poor (HCFP). The HCFP provides care for the poor, ethnic minorities, and the disadvantaged. Initially implemented as a separate social program, HCFP was
The Vietnam Social Security (VSS) is the main entity that reimburses services provided to patients covered by social health insurance (SHI). It constitutes three types of provider payment mechanisms, namely fee-for-service, capitation and payment by diagnosis-related groups.
Currently, drugs dispensed at retail pharmacies are not reimbursed.
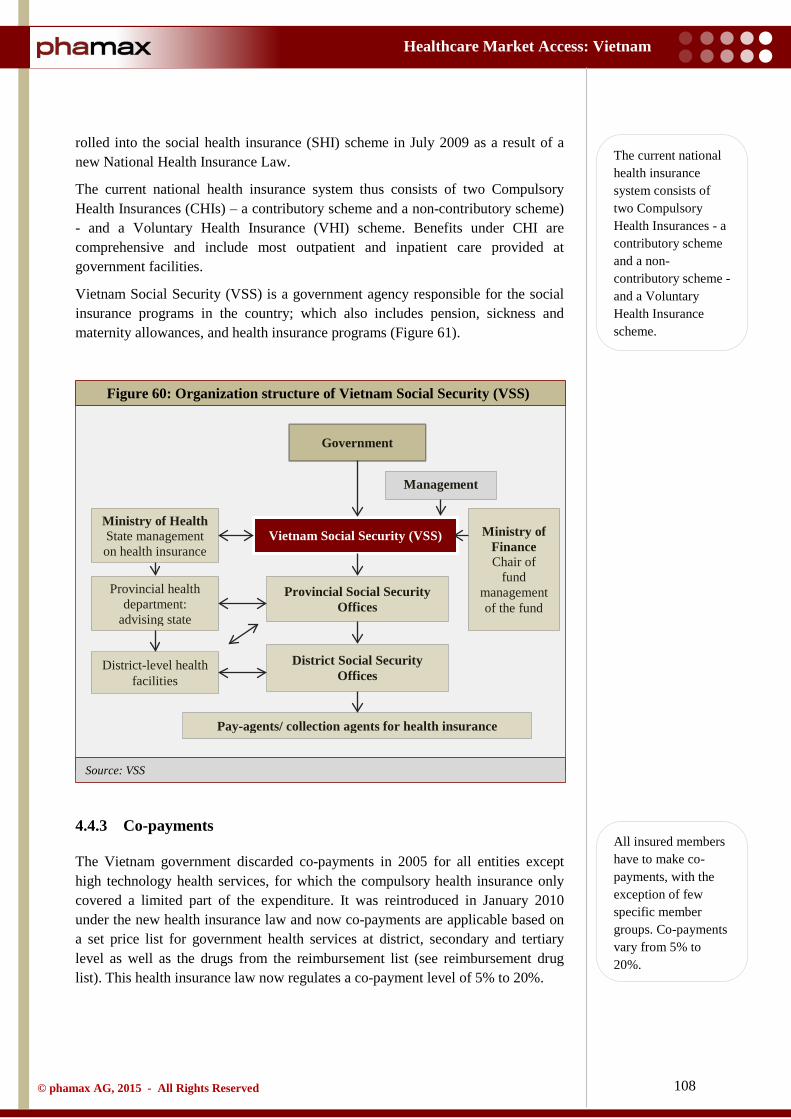
108
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: VSS
rolled into the social health insurance (SHI) scheme in July 2009 as a result of a new National Health Insurance Law.
The current national health insurance system thus consists of two Compulsory Health Insurances (CHIs) – a contributory scheme and a non-contributory scheme) - and a Voluntary Health Insurance (VHI) scheme. Benefits under CHI are comprehensive and include most outpatient and inpatient care provided at government facilities.
Vietnam Social Security (VSS) is a government agency responsible for the social insurance programs in the country; which also includes pension, sickness and maternity allowances, and health insurance programs (Figure 61).
4.4.3 Co-payments
The Vietnam government discarded co-payments in 2005 for all entities except high technology health services, for which the compulsory health insurance only covered a limited part of the expenditure. It was reintroduced in January 2010 under the new health insurance law and now co-payments are applicable based on a set price list for government health services at district, secondary and tertiary level as well as the drugs from the reimbursement list (see reimbursement drug list). This health insurance law now regulates a co-payment level of 5% to 20%.
Figure 60: Organization structure of Vietnam Social Security (VSS)
Government
Ministry of Finance Chair of
fund management of the fund
Vietnam Social Security (VSS)
Provincial Social Security Offices
Management
District Social Security Offices
Pay-agents/ collection agents for health insurance
Ministry of Health State management on health insurance
Provincial health department:
advising state
District-level health facilities
The current national health insurance system consists of two Compulsory Health Insurances - a contributory scheme and a non-contributory scheme - and a Voluntary Health Insurance scheme.
All insured members have to make co-payments, with the exception of few specific member groups. Co-payments vary from 5% to 20%.
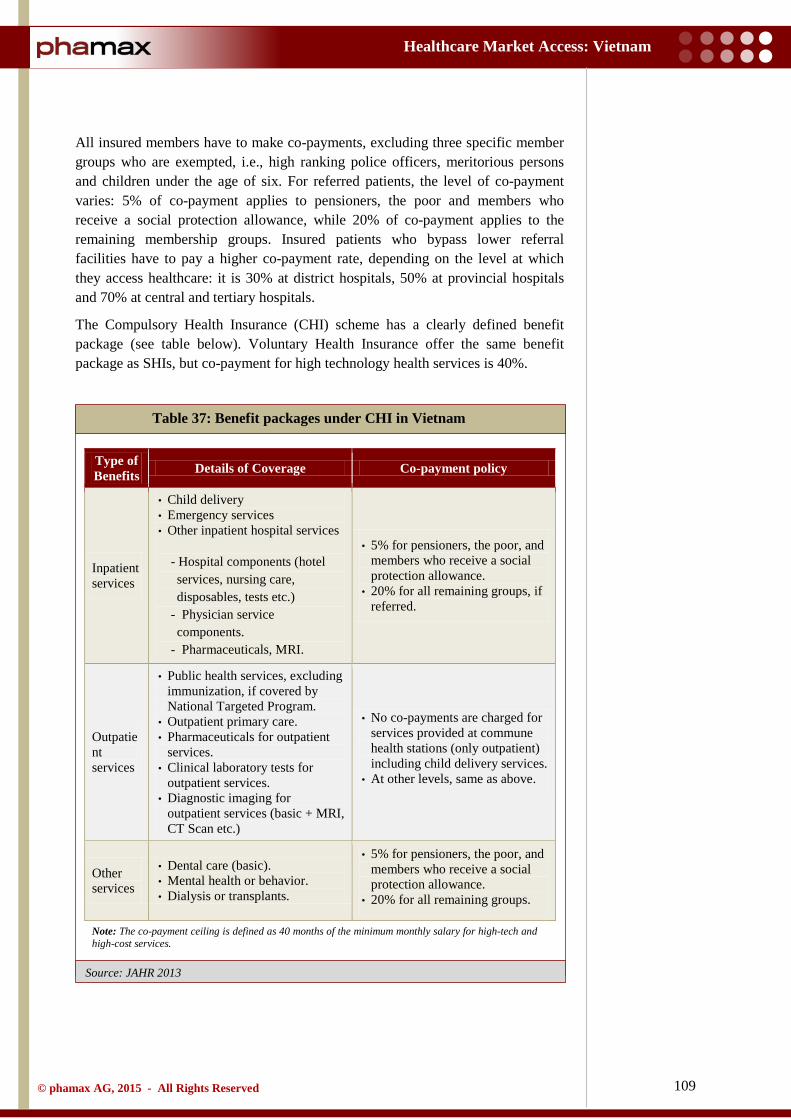
109
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Source: JAHR 2013
All insured members have to make co-payments, excluding three specific member groups who are exempted, i.e., high ranking police officers, meritorious persons and children under the age of six. For referred patients, the level of co-payment varies: 5% of co-payment applies to pensioners, the poor and members who receive a social protection allowance, while 20% of co-payment applies to the remaining membership groups. Insured patients who bypass lower referral facilities have to pay a higher co-payment rate, depending on the level at which they access healthcare: it is 30% at district hospitals, 50% at provincial hospitals and 70% at central and tertiary hospitals.
The Compulsory Health Insurance (CHI) scheme has a clearly defined benefit package (see table below). Voluntary Health Insurance offer the same benefit package as SHIs, but co-payment for high technology health services is 40%.
Table 37: Benefit packages under CHI in Vietnam
Type of Benefits Details of Coverage Co-payment policy
Inpatient services
• Child delivery • Emergency services • Other inpatient hospital services
- Hospital components (hotel services, nursing care, disposables, tests etc.)
- Physician service components.
- Pharmaceuticals, MRI.
• 5% for pensioners, the poor, and members who receive a social protection allowance.
• 20% for all remaining groups, if referred.
Outpatient services
• Public health services, excluding immunization, if covered by National Targeted Program.
• Outpatient primary care. • Pharmaceuticals for outpatient
services. • Clinical laboratory tests for
outpatient services. • Diagnostic imaging for
outpatient services (basic + MRI, CT Scan etc.)
• No co-payments are charged for services provided at commune health stations (only outpatient) including child delivery services.
• At other levels, same as above.
Other services
• Dental care (basic). • Mental health or behavior. • Dialysis or transplants.
• 5% for pensioners, the poor, and members who receive a social protection allowance.
• 20% for all remaining groups.
Note: The co-payment ceiling is defined as 40 months of the minimum monthly salary for high-tech and high-cost services.

110
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Under the current health insurance policy, co-payment might become a financial burden for patients with low income, to counter high healthcare costs, since there is no ceiling for co-payment and the accumulation of co-payments, even at rates of 5% or 20% of healthcare costs, might become a huge expenditure for households. In addition, there is a ceiling on the maximum benefit that the health insurance fund covers for each episode requiring costly high-tech services.
About 30% of the people with health insurance for the poor still face high healthcare costs. Co-payments (5% for the poor) still cause financial hardships for the poor because of their low ability to pay. For instance, if kidney dialysis is needed for more than an year, a poor person would have to pay VND 4 to 5 mn in co-payments (while GNI per capita is approximately VND 25 mn in 2013). Because the financial protection is still inadequate, people facing financial difficulties are likely to delay seeking care until their health problems become severe.
In summary, the co-payment policy substantially limits the risk protection function of health insurance. Uninsured patients are particularly at risk as they pay user charges (fee for service) i.e. 100% of the price described in the set price list.
111
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
4.5 Prescribing and dispensing
4.5.1 Prescribing guidelines
In Vietnam, prescribing at public hospitals continues to be determined by their formularies (see hospital formulary), based on the Essential Drug List. However, the liberty of prescribing remains influenced by the Social Health Insurance cover and patient’s ability to pay out-of-pocket.
A prescription and drug dispensing regulation has been in place since 1995 and includes detailed information regarding prescription-only drugs. Under the new Pharmacy Law, Article 46 defines the guidelines for prescription and use of drugs. It states that:
i) Prescriptions serve as a lawful basis for the sale, dispensing, preparation, weighing and use of drugs. The name of a drug written in a prescription must include its original brand name or international generic name, except for drugs containing many active ingredients.
ii) The Health Minister shall specify prescriptions, groups of prescription drugs and the sale of drugs according to prescriptions.
Subsequently, Article 48 provides guidelines for dispensing drugs in Vietnam. The conditions for supply of drugs are given below:
i) The supply of drugs in medical examination and treatment establishments must comply with regulations on good practice in distribution, preservation of drugs and other relevant provisions of law.
ii) Drug dispensers in medical examination and treatment establishments must dispense drugs strictly according to medical orders or drug prescriptions, clearly write the names and concentrations of drugs on their packing and give instructions to drug users.
iii) Doctors, assistant doctors, nurses, midwives and convalescent attendants must not sell drugs to patients, except for traditional medicines.
Hospitals define ceiling for prescribing costs and quota for branded drugs. It mandates physicians to obtain authorization to prescribe such drugs. The guidelines also have certain prescribing restrictions for specialty products.
4.5.2 Prescribing influences
Vietnam suffers from an irrational use of medicines. A lack of enforcement on prescribing and dispensing and inappropriate profit-driven prescribing behavior has further hampered the situation. Many physicians use prescribing for revenue generation to cross-subsidize their low government paid salary. As a result, medicine prices at the patient level are grossly inflated.
Prescribing at public hospitals continues to be determined by their formularies, based on the Essential Drug List. However, the liberty of prescribing remains influenced by the Social Health Insurance cover and patient’s ability to pay out-of-pocket.
Physicians in the private sector have the liberty to prescribe. Generally, branded drugs are their first choice.
112
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
Physicians in private practice have retained the liberty to prescribe and branded drugs are their first choice. Mostly, prescriptions in public hospitals are generics, while brands are only prescribed for patients who can afford the medicines. However, since physicians in Vietnam often work in both public and private set ups, there is a major influence on their prescribing patterns.
Physicians teaming up with pharmacies to obtain commissions for prescribing specific drugs is common in the country. Bribes to doctors to prescribe particular medicines, persuading hospital purchasing officers to buy is one of the key reasons for booming drug prices. Private clinics continue to sell drugs at specific points of treatment without prescriptions.
In 2009, the rights and obligations of patients were stipulated in the Law on Examination and Treatment (effective since January, 2011). Enforcing the regulation was a decree for violation in medical examination and treatment. This decree stipulates prohibitions on prescribing drugs or services exceeding those required by the patient in order to gain financial benefits or bribes; prescribing unnecessarily expensive branded drugs to gain commission from drug representatives.
4.5.3 Dispensing
In the district and central hospitals in the country, pharmacy departments are primarily responsible for dispensing medicines to hospitalized patients, supported hospital pharmacies that dispense medicines to outpatients. Alternatively, many pharmacies operate like clinics, dispensing drugs without prescriptions (patients purchase drugs for self-treatment based on ‘prescriptions’ created by drug sellers). Doctors are not permitted to dispense in Vietnam. Nonetheless, illegal dispensing of prescription drugs without a doctor’s prescription remains common practice in Vietnam.
Physicians teaming up with pharmacies to earn commissions, bribes to prescribe specific brands and bribes to hospitals to purchase certain drugs largely influence prescribing behavior.
Physicians often work in both public and private set ups, influencing their prescribing habits.
Illegal dispensing of prescription drugs without a doctor’s prescription remains common practice.
113
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
4.6 Essential drug list
This Essential Drug List is developed by the Drug Administration of Vietnam (DAV), approved by the Minister of Health, and supported by guidelines and recommendations of the World Health Organization (WHO). Drugs listed on the Essential Drug List must be available in specific health establishments that include any healthcare facility that supplies essential drugs directly to the patients. The essential drug list also covers drugs used in the national target health programs (for instance tuberculosis, leprosy etc.). Essential drugs are not directly distributed through pharmacists.
The first Essential Drug list of Vietnam was adopted in 1985 and so far has been revised five times, responding to Vietnam's practical situation and illness patterns in each period. This list hence was subsequently updated in 1989, 1995, 1999 and 2005. The new edition was released in 2014. This replaced the previous list in Decision No. 17/2005 dated July 01, 2005.
The fifth edition (2005) comprised 355 medicines with 314 active substances and 94 traditional medicines. Starting with the third edition, essential drugs were categorized to allow different drugs to be allowed for use in different level facilities depending on technical capacity. The drugs, including dosages and route of administration, have changed over time in relation to changes in morbidity patterns and socio-economic conditions over time.
The process of selecting, adding and eliminating drugs from the list is not based on scientific evidence but primarily on proposals from healthcare service providers. This has also led to inclusion of some drugs that economically developed countries do not use in their country.
The drug list used at grassroots facilities, issued by the MoH, is considered as the recommended version. But, each locality can develop a more appropriate drug list based on morbidity patterns in their locality. Criteria for selecting drugs include existence of generic versions, availability, efficacy, limited side effects, low toxicity, low cost etc. Additionally, the selection criteria includes ensuring the quality of essential drugs in the supply chain, considering the numerous intermediates involved in the process.

114
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
4.7 Reimbursement drug list
The list of drugs covered by the Social Health Insurance (SHI) for reimbursement is issued by the MoH. The most recent reimbursement drug list was issued in February 2008 under Decision No.5/2008.
The most recent reimbursement drug list for health insurance members consisted of 750 medicines and 237 traditional herbal medicines. Recently, an additional 54 drugs for children under six years have been added to the list. The 750 medicines are listed by their international non-proprietary name (INN) and providers can prescribe generic and/or branded products. While this gives doctors some flexibility and medical autonomy, it makes them susceptible to pressure from pharmaceutical suppliers to prescribe the more expensive branded drugs.
Hospitals have the right to set up their own drug list according to the Major Drug list (see hospital formulary). There is a concern that the reimbursement drug list has not been sufficiently developed, based on cost-effectiveness and inclusion of some drugs that are rarely used even in some developed countries. The process for adding new drugs or removing drugs from the list does not have well-defined steps that ensure selection based on cost-effectiveness. The biggest concern is, however, that the prices for drugs are neither monitored nor regulated. Therefore, it remains under the discretion of the hospital to set prices. The co-payment rates are thus unregulated and lead to high drug prices. The root cause of this problem is the fact that suppliers are allowed to set the drug prices on a competitive basis, as prescribed by the Law on Pharmaceuticals.
There is a concern that the reimbursement drug list has not been sufficiently developed, based on cost-effectiveness and inclusion of some drugs that are rarely used even in some developed countries.

115
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
4.8 Drug procurement
Vietnam is yet to have a central procurement office to administer drug purchases for government healthcare facilities. At present, drug procurement is decentralized to individual healthcare facilities or to the provinces, leading to unnecessary duplication as well as poorer opportunities in larger bulk purchases.
Like most of the other countries, public drug procurement is established by tender, so as to secure the lowest price for a product through a transparent and competitive bidding process. The lists for tender procurement are drawn from the reimbursement drug list issued by the MoH. The local hospitals customize their tender in consensus with the basic MoH list and individual hospital needs. Typically, around 40% of the budget is allocated to domestic products and around 20% share to innovator brands. A minimal tender fee is mandatory on the submission of both provincial and hospital tenders. Tender intervals may vary from six months to one year, and in some circumstances may be extended up to two years.
The out-of-pocket payment in Vietnam accounts for approximately 50% of the national health spending. Given the lack of universal healthcare coverage, patients are forced to pay for the treatment. The fluctuations in the drug prices continue to increase the affliction. Bribes and unhealthy influences in drug procurement are common occurrences in the country. Collusion to influence specification of the bids and tender process also has been severely impacting the access to appropriate medicines. The adverse consequence has been an increased use of imported expensive drugs. All the efforts to address the problems have been ineffective. Concerned with the ever-increasing lack of transparency and rising drug prices, the MoH introduced a new tendering law in 2012.
The new regulations on competitive tendering for drug procurement were implemented under the Joint Circular No. 01/2012 and Circular No. 11/2012. These regulations required the healthcare facilities to plan their competitive tendering at least once every year. Each drug category is allowed to have one bid winner, who meets specific technical requirements. The winning price for each drug cannot be higher than the price in the approved competitive tendering plan. The circular also states that drug procurement involving the state budget or the health insurance fund would involve a ceiling on the profit margin, allowed between import and wholesale prices for twelve active ingredients. This is expected to help the drug price control in the country.
Prior to this enactment, there was no clear preference given to domestic drugs in Vietnam. Under the circular issued, the criteria for selecting the winning bid are based on both price and the quality of the pharmaceutical products. The new law prohibits tenders offering imported drugs, if there are domestic drugs available that can satisfy the requirements. Generic drugs have begun to receive attention in competitive tendering for drug procurement. This has also lead to relatively stable drug prices with the growth in drug prices being slower.
Most public drug procurements are established by tender. The lists for tender procurement are drawn from the reimbursement drug list issued by the MoH.
Collusion to influence specification of the bids and tender process has been severely impacting the access to appropriate medicines.
The new tendering law prohibits tenders offering imported drugs if there are domestic drugs available that can satisfy the requirements, clearly providing preference to domestic pharma companies.

116
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
However, there is a downside to the new tendering law. It is expected to have a direct impact on foreign MNCs in the market. Moreover, this new arrangement will also have a major impact on hospital purchasing and prescribing behaviors. Since the MoH’s new Major Drug list (see hospital formulary) for purchasing by tender will restrict the choice for hospital formularies, affecting both branded and generic drugs.

117
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
4.9 Hospital formulary
In Vietnam, the hospitals have the right to set up their own drug list according to the Major Drug list (also an expanded essential drug list). This Major Drug List constitutes therapeutic drugs appropriate to the disease patterns in Vietnam. This list is developed by the Department of Therapy and circulated by the MoH and has been revised four times, with the 4th edition published in 2005. Hospitals use the Major Drug list as a basis to choose drugs to include in their formulary, and it may be different for different hospital departments and units.
In addition, the hospital formulary also derive information from the Essential Drug list, developed by DAV (see Essential Drug List). It is mandatory that these essential drugs be available in any Vietnam health facility (even if the facility is without doctors).
In the future, the major drug list is expected to be replaced with the drug formulary for health insurance reimbursement. But as mentioned before in drug procurement section, the new tender regulations will also affect the formulary listing in public hospitals.
It is expected that hospital formularies will be replaced with a single formulary for health insurance reimbursement.

118
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
5 Appendix
5.1 Glossary
ADR Adverse Drug Reactions
AIDS Acquired Immunodeficiency Syndrome
ASEAN Association of Southeast Asian Nations
CDHP Consumer-Driven Health Plans
CHI Compulsory Health Insurance
CHS Commune Health Station
CIA Central Intelligence Agency
CIF Cost, Insurance and Freight
CPI Consumer Price Index
CPV Communist Party of Vietnam
CSC Certificate of Satisfaction of Conditions
DALY Disability-Adjusted Life Year
DAV Drug Administration of Vietnam
DHG Hau Giang Pharmaceutical Company
DMC Domesco Medical Import Export JSC
DOH Department of Health
DRD Drug Registration Department
DRG Diagnosis-Related Group
EU European Union
EVFTA European Union - Vietnam Free Trade Agreement
FDI Foreign Direct Investment
FIE Foreign Invested Enterprises
GDP Gross Domestic Product
GER Gross Enrolment Ratio
GLP Good Laboratory Practice
GMP Good Manufacturing Practice
GNI Gross National Income
GPP Good Pharmacy Practice
GSK GlaxoSmithKline
119
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
GSO General Statistics Office
GSP Good Supply Practice
HCFP The Healthcare Fund for the Poor
HIV Human Immunodeficiency Virus
HMO Health Maintenance Organization
IMF International Monetary Fund
INN International Non-proprietary Name
IPR Intellectual Property Right
JAHR Joint Annual Health Review
JV Joint Venture
MoH Ministry of Health
MP Medical Professional
NDI National Center for Drugs
NFSC National Financial Supervisory Committee
NOIP National Office of Intellectual Property of Vietnam
NPL Non-Performing Loans
NSQ Not of Standard Quality
ODA Official Development Assistance
OOP Out-of-pocket (Payment)
OTC Over-the-counter
PhRMA Pharmaceutical Research and Manufacturers of America
PPC Provincial People’s Committee
PPP Purchasing Power Parity
R&D Research and Development
RO Representative Office
SEDP Socio-Economic Development Plan
SHI Social Health Insurance
SOE State-Owned Enterprise
TPP Trans-Pacific Partnership
TRIPS Trade-Related Aspects of Intellectual Property Rights
USD United States Dollar
VAMC Vietnam Asset Management Company
120
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
VHI Voluntary Health Insurance
VHW Village Health Workers
VND Vietnamese Dong
VNPCA Vietnam Pharmaceutical Companies Association
VSS Vietnam Social Security
WFOE Wholly Foreign-Owned Enterprises
WHO World Health Organization
WTO World Trade Organization

121
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
5.2 Bibliography
• Annual Report 2012; DHG Pharmaceutical Joint Stock Company; Available from: http://www.dhgpharma.com.vn/dhgen/images/stories/quan - he - co - dong/Annual%20Report%202012.pdf [Accessed August, 2014]
• Annual Report 2013; Traphaco Joint Stock Company; Available from: http://www.traphaco.com.vn/en/sites/traphaco.vn.en/files/attachment/quan - he - co - dong/20140522 - traphaco - ar - 2013 - en.pdf [Accessed September, 2014]
• Annual Report 2014; Imexpharm: Available from: http://www.imexpharm.com/Download/File%202014/Bao%20cao%20thuong%20nien/Bao%20cao%20thuong%20nien%202013.pdf [Accessed September, 2014]
• Assessing Provincial Health Systems in Vietnam: Lessons From Two Provinces; 2009; Health systems 2020; Available from: http://www.healthsystems2020.org/files/2347_file_Vietnam_HSA_FIN14_with_logo.pdf. [Accessed October, 2014]
• Circular - Guidelines for clinical drug trial; 2010; Ministry of Health; Available from: http://www.tbtvn.org/Ti%20liu%20upload%20cho%20QCKT/TT%20Bo%20Yte.doc.pdf [Accessed November, 2014]
• Circular - Guiding the management of Medicine Quality; 2010; Ministry of Health; Available from: http://haiquanbinhduong.gov.vn/EN/vanban/Thongtu09kiemtrachatluongthuoc.doc [Accessed November, 2014]
• Circular - Stipulating the regulations on classification and chemical labeling; 2012; Ministry of Industry and Trade; Available from: http://www.customs.gov.vn/Lists/EnglishDocuments/Attachments/1178/Circular%2004.12.BCT.doc [Accessed November, 2014]
• Company Report 2014; Domesco Medical Import Export JSC (DMC); Available from: https://www.tvs.vn/images/2014/document/DMC___INDEPTH_REPORT_25062014_EN.pdf%20%20 [Accessed September, 2014]
• Country Strategy For Development Cooperation With Vietnam 2013–2016; 2014; Ministry For Foreign Affairs Of Finland; Available from: http://formin.finland.fi/doc/kytmaaohjelmat/Vietnam/files/assets/basic - html/index.html#1[Accessed August, 2014]
• Fiscal Policy for Inclusive Growth - Economic trends and prospects in developing Asia: Southeast Asia; 2014; Asian Development Outlook; Available from: http://www.adb.org/publications/asian - development - outlook - 2014 - fiscal - policy - inclusive - growth [Accessed August, 2014]
• Five - Year Health Sector Development Plan 2011 - 2015; Ministry of Health Vietnam; Available from: http://www.wpro.who.int/health_services/viet_nam_nationalhealthplan.pdf [Accessed October, 2014]
• Health at a Glance: Asia/Pacific 2012; 2012; OECD; Available from: http://www.oecd - ilibrary.org/docserver/download/8112131e.pdf?expires=1417090895&id=id&accname=guest&checksum=699D715B4DF8F1A45A9141DBAC24ADA8 [Accessed September, 2014]
• Health Financing And Delivery In Vietnam - Looking Forward; 2009; World Bank Available from:

122
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
https://openknowledge.worldbank.org/bitstream/handle/10986/2594/473880PUB0VN0H101OFFICIAL0USE0ONLY1.pdf?sequence=1 [Accessed October, 2014]
• Health Service Delivery Profile Vietnam 2012; 2012; WHO and the Ministry of Health, Vietnam; Available from: http://www.wpro.who.int/health_services/service_delivery_profile_vietnam.pdf [Accessed October, 2014]
• Huyen, Le Thu; Exploring Medical Representatives’ Strategies To Influence Doctors’ Prescribing Decisions In Vietnam; 2012; Department of Public Health and Clinical Medicine Epidemiology and Global health, Umeå University, Sweden; Available from: http://www.phmed.umu.se/digitalAssets/104/104566_huyen - le - thu.pdf [Accessed November, 2014]
• Implementing clinical research in Vietnam: A dialogue on the current regulations of the Ministry of Health; 2007; MoH; Available from: http://www.fhi360.org/sites/default/files/media/documents/Implementing%20Clinical%20Research%20in%20Vietnam.pdf [Accessed November, 2014]
• Intellectual Property Rights in Vietnam; 2013; Intellectual Property Office, Vietnam; Available from: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/306015/ipvietnam.pdf [Accessed November, 2014]
• Introduction to the IP administration system of Vietnam; 2008; The Inspectorate of Science and Technology; Available from: http://iprenforcement.most.gov.vn/ckfinder/userfiles/files/Introduction%20to%20the%20IP%20administration%20system%20of%20Vietnam(2).pdf[Accessed November, 2014]
• Joint Annual Health Review 2009; Vietnam Ministry of Health; Available from: jahr.org.vn/downloads/JAHR2009 - EN.pdf [Accessed September, 2014]
• Joint Annual Health Review 2010; Vietnam Ministry of Health; Available from: jahr.org.vn/downloads/JAHR2010 - EN.pdf [Accessed September, 2014]
• Joint Annual Health Review 2011; Vietnam Ministry of Health; Available from: jahr.org.vn/downloads/JAHR2011/JAHR2011_Fullversion_English.pdf [Accessed September, 2014]
• Joint Annual Health Review 2012; Vietnam Ministry of Health; Available from: jahr.org.vn/downloads/JAHR2012/JAHR2012_Eng_Full.pdf [Accessed September, 2014]
• Joint Annual Health Review 2013; Vietnam Ministry of Health; Available from: jahr.org.vn/downloads/JAHR2013/JAHR2013_Final_EN.pdf [Accessed September, 2014]
• Key Indicators for Asia and the Pacific 2013 Country Tables; 2013; Asian Development Bank; Available from: http://www.adb.org/publications/key - indicators - asia - and - pacific - 2014 [Accessed August, 2014]
• Law on Pharmacy; 2005; The National Assembly of Vietnam; Available from: http://www.vertic.org/media/National%20Legislation/Vietnam/VN_Law_on_Pharmacy.pdf [Accessed November, 2014]
• Market Economy For A Middle - Income Vietnam; Joint Donor Report to the Vietnam Consultative Group Meeting;2012; Vietnam Development Report; Available from: http://www - wds.worldbank.org/external/default/WDSContentServer/WDSP/IB/2011/12/13/000333037_20111213003843/Rendered/PDF/659800AR00PUBL0elopment0Report02012.pdf [Accessed August, 2014]
• Matsushima, Midori; Yamada, Hiroyuki; Public Health Insurance in Vietnam Towards Universal Health Coverage; 2013; Osaka University of Commerce

123
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
• Medicines Prices: Policy Options for Vietnam; 2010; WHO; Available from: http://www.who.int/medicines/areas/nextgen_essentialmeds/7MedicinesPrices_NA3.pdf [Accessed November, 2014]
• MoH – Scheme to reduce hospital overcrowding period 2012 - 2020 - VN [Recd. through email from Hoan My Hospital, Saigon on September 16, 2014]
• New tendering law challenges foreign pharma producers; 2014; Available from: http://www.vir.com.vn/new - tendering - law - challenges - foreign - pharma - producers.html [Accessed September, 2014]
• Nguyen Thi Dan Thanh; The Vietnamese social health insurance for the near - poor - A health capability approach; 2013; Department of Sociology and Human Geography, University of Oslo
• Nguyen Thi Trang Nhung, Vietnam Burden of Disease and Injury Study 2008; 2011; Hanoi School of Public Health, Vietnam
• Nguyen, Anh Tuan, Medicine pricing policies: Lessons from Vietnam; 2010; School of Public Health and Community Medicine, University of New South Wales, Sydney
• Nguyen, Duc Hinh; Hoang, Van Minh; Lucia, D’Ambruoso; Public health in Vietnam: here’s the data, where’s the action?; 2013; Hanoi Medical University
• Nguyen, Hang T.; Vietnam Pharmaceutical Industry Report; 2014; VietinbankSc • Nguyen, Tuan Anh; Medicine Prices And Pricing Policies In Vietnam; 2011; School of Public
Health & Community Medicine Faculty of Medicine, University of New South Wales, Australia; Available from: http://apps.who.int/medicinedocs/documents/s19038en/s19038en.pdf [Accessed November, 2014]
• OPV Pharmaceuticals joint stock company; 2014; Available from: http://opv.com.vn/opven/index.php?option=com_content&view=article&id=1522:history - from - the - 1950s&catid=111:category - aboutusopv&Itemid=487 [Accessed November, 2014]
• Pharma Pro and Pack Article: Rising drug demand in Vietnam - Opportunities & Challenges in front of Vietnam pharma sector; Available from: http://www.gpeexpo.com/mar2013/part_3.pdf [Accessed September, 2014]
• Pharmaceutical Research and Manufacturers of America (PhRMA), Special 301 Submission; 2014; PhRMA; Available from: http://www.phrma.org/sites/default/files/pdf/2014 - special - 301 - submission.pdf [Accessed August, 2014]
• Regulation On Herbal Medicines In Vietnam; 2013; Drug Administration of Vietnam; Available from: http://apps.who.int/medicinedocs/collect/medicinedocs/pdf/whozip57e/whozip57e.pdf [Accessed November, 2014]
• Robin Thompson, Sophie Witter, Nguyen Thi Thuy Nga; Strategic options for financing health system modernization and development: what can Vietnam learn from international experiences; 2011; Development Strategy Institute, Ministry of Planning and Investment
• Simonet, Daniel; Entry Modes of European Firms in Vietnam Volume 2 (2012); 2012; American University of Sharjah; Available from: http://emaj.pitt.edu/ojs/index.php/emaj/article/view/27/121 [Accessed November, 2014]
• Somanathan, Aparnaa; Ajay Tandao; Moving toward Universal Coverage of Social Health Insurance in Vietnam; 2013; World Bank Available from: https://openknowledge.worldbank.org/bitstream/handle/10986/18885/890660PUB0Univ00Box385269B00PUBLIC0.pdf?sequence=1 [Accessed September, 2014]
• Somanathan, Aparnaa; Huong, Lan Dao; Tran, Van Tien; Integrating the Poor into Universal Health Coverage in Vietnam; 2013; World Bank Available from:
124
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
https://openknowledge.worldbank.org/bitstream/handle/10986/13314/74945.pdf?sequence=1 [Accessed October, 2014]
• Somanathan, Aparnaa; Vietnam’s Universal Health Coverage; 2011; World Bank; Available from: https://www.kdevelopedia.org/mnt/idas/asset/2013/11/19/DOC/SRC/04201311190129112013305.PDF [Accessed October, 2014]
• Taking Stock An Update On Vietnam’s Recent Economic Developments;2014; World Bank; Available from: http://www.worldbank.org/content/dam/Worldbank/document/EAP/Vietnam/Taking_Stock_July2014_EN_final.pdf [Accessed August, 2014]
• Towards a Comprehensive Generic Policy: Vietnam; 2009; WHO; Available from: http://www.who.int/medicines/areas/nextgen_essentialmeds/6GenericPolicy.pdf [Accessed November, 2014]
• Tran, Van Tien; Hoang, Thi Phuong; Inke Mathauer; Nguyen Thi Kim Phuong; A Health Financing Review of Vietnam with a Focus on Social Health Insurance; 2011; WHO; Available from: http://www.who.int/health_financing/documents/oasis_f_11 - vietnam.pdf [Accessed October, 2014]
• Vietnam’s Healthcare System: A Macroeconomic Perspective; 2005; International Monetary Fund Available from: http://www.imf.org/external/country/vnm/rr/sp/012105.pdf [Accessed October, 2014]
• Vietnam’s Rapid Economic Changes And Its Implications On The Regulatory Affairs; 2011; Drug Administration of Vietnam; Available from: http://www.who.int/medicines/areas/quality_safety/regulation_legislation/icdra/2_ImplicationsRapidSocioeconomicChanges.pdf [Accessed August, 2014]
• World Development Indicators; 2014; World Bank; Available from: http://data.worldbank.org/country/indonesia [Accessed October, 2014]
• World Economic Outlook Database; 2014; International Monetary Fund; Available from: Available from: http://www.imf.org/external/pubs/ft/weo/2014/02/weodata/weoselgr.aspx [Accessed September, 2014]
125
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
5.3 Methodology
5.3.1 Secondary research
In-depth and extensive secondary research was conducted to capture quantitative and qualitative information by a team of experienced consultants with advanced analytical skills and expertise in the pharmaceutical industry. The data was collected from multiple credible and authentic sources within public domain, including but not limited to:
• Websites of Ministry of Health and its affiliates as well as various regulatory and government bodies.
• Company websites, annual reports, investor presentations and press releases of various pharmaceutical companies and hospitals.
• Reports of various healthcare and pharmaceutical trade associations. • Reports published by various internationally recognized bodies such as World Health
Organization (WHO), United Nations (UN), and others. • Reports and articles published by globally accredited institutions such as the World Bank,
International Monetary Fund (IMF), Asian Development Bank (ADB), the Organization for Economic Cooperation and Development (OECD), Central Banks of respective countries and many more.
• News, press releases and bulletins of domestic as well as foreign newspapers and magazines. • Publications in various scientific, healthcare and other related journals.
5.3.2 Primary research
To address the data gaps and further consolidate the secondary research findings, phamax collected primary data through e-mails, telephone calls and interviews with various sources including:
• Ministry of Health officials. • Key officials serving in government agencies. • Healthcare and Pharmaceutical trade associations and other similar bodies. • Pharmaceutical distributors/stockists/retailers. • Hospitals and their affiliates. • KOLs in therapy area and disease management. • Industry experts. • Executives of both domestic and foreign pharmaceutical companies.
In addition to the above mentioned primary sources, phamax leveraged the experience and expertise of its ‘Dendron Network’, which comprises top KOLs and scientific experts in respective countries.
5.3.3 Data validation
Both the primary and secondary data was validated by a panel of experts including industry experts, KOLs, thought leaders and members of phamax Dendron Network.
126
Healthcare Market Access: Vietnam
© phamax AG, 2015 - All Rights Reserved
5.4 Disclaimer
All information contained in this publication has been thoroughly researched and compiled from various sources that are believed to be accurate and credible at the time of publishing. However, in view of the natural scope for human and/or mechanical error, either at source or during production, phamax accepts no liability whatsoever for any loss or damage resulting from errors, inaccuracies or omissions from any part of the publication. All information is provided without warranty, and phamax makes no representation of warranty of any kind as to the accuracy or completeness of any information hereto contained.
The information contained in this report is strictly confidential and has been provided to the client under a non-exclusive and non-transferable license for the client’s direct benefit and use only. The report should not be copied, electronically transmitted, sold or divulged to any other party without the prior written consent of phamax.
© 2015 phamax AG. All rights reserved.
5.5 Contact us
All communications pertaining to this report should be addressed to:
SWITZERLAND OFFICE
phamax AG Passage 6, 4104 Oberwil (BL), SWITZERLAND Phone: +41 61821 5687 Fax: +41 61821 5836 E-mail: [email protected]
INDIA OFFICE
phamax Analytic Resources Pvt. Ltd. #19, “KMJ Ascend”, 1st Cross, 17th C Main, 5th Block, Koramangala, Bangalore 560 095, INDIA Phone no: +91 80 6745 1100 Fax no: +91 80 6745 1122 E-mail: [email protected]