guidelines in the acute management of ischemia stroke 0-3 hrs
TRANSCRIPT

Guidelines in the acute Guidelines in the acute management of Ischemia management of Ischemia
stroke 0-3 hrs.stroke 0-3 hrs.

INTRODUCTIONINTRODUCTION
Incidence of ABA :Incidence of ABA : 2.4 per 1000 people per year2.4 per 1000 people per year 0.2 % per year between 55-64 yrs of age0.2 % per year between 55-64 yrs of age 2 % per year for persons >85 yrs.2 % per year for persons >85 yrs. 1 per 1000 persons per year1 per 1000 persons per year 10,00,000 strokes per year in India10,00,000 strokes per year in India 3000 strokes a day3000 strokes a day In Chennai alone, 1000 cases a monthIn Chennai alone, 1000 cases a month 2% of all admissions2% of all admissions Crude prevalence rate is 220/100000.Crude prevalence rate is 220/100000.

Impact of ABA and economic Impact of ABA and economic burdenburden
Someone suffers a Brain Attack every 33 Someone suffers a Brain Attack every 33 secs.secs.
Every 3.3 mins., someone dies of a strokeEvery 3.3 mins., someone dies of a stroke Atleast 50,00,000 Indians are Stroke Atleast 50,00,000 Indians are Stroke
survivorssurvivors Stroke costs in India: Rs. 3000 – 4000 Stroke costs in India: Rs. 3000 – 4000
Crores a yearCrores a year

Rationale behind developing Rationale behind developing ABA teamABA team
1. Targets the unique needs of the Stroke victim1. Targets the unique needs of the Stroke victim2. A radical change has taken place in the way 2. A radical change has taken place in the way
stroke is managed. A stroke is managed. A ‘wait and hope’‘wait and hope’ approach has been replaced by a approach has been replaced by a ‘rapid ‘rapid diagnosis and intervention’diagnosis and intervention’ approach. approach.
3. A protocol driven, appropriately equipped 3. A protocol driven, appropriately equipped Stroke program run by a well-trained Stroke program run by a well-trained
staff is an absolute necessity to implement staff is an absolute necessity to implement the newer stroke treatments.the newer stroke treatments.
4. Acute Stroke units decrease length of hospital 4. Acute Stroke units decrease length of hospital stay.stay.

Rationale behind developing Rationale behind developing ABA teamABA team
Time is Brain!Time is Brain! ABA teams provide the most efficient and ABA teams provide the most efficient and
effective care during acute Hospitalization, effective care during acute Hospitalization, deliver thrombolytic therapy and improve deliver thrombolytic therapy and improve outcome.outcome.

Golden 90 Minutes
0 10 20 30 40 50 60 7080 90
minutes

Estimated thresholdsEstimated thresholds
Timemin
0 30 60 120 180 240 360 480 720 1080 1440
Penumbra
InfarctVolume
0 10 20 40 60 CBF ( ml/100g/min)
Core Oligemia
Normal range Hyperperfusion

Ischaemic core and Ischaemic core and penumbrapenumbra

One Hour from Onset
core
penumbra
Relationship of Ischemia over Time Relationship of Ischemia over Time
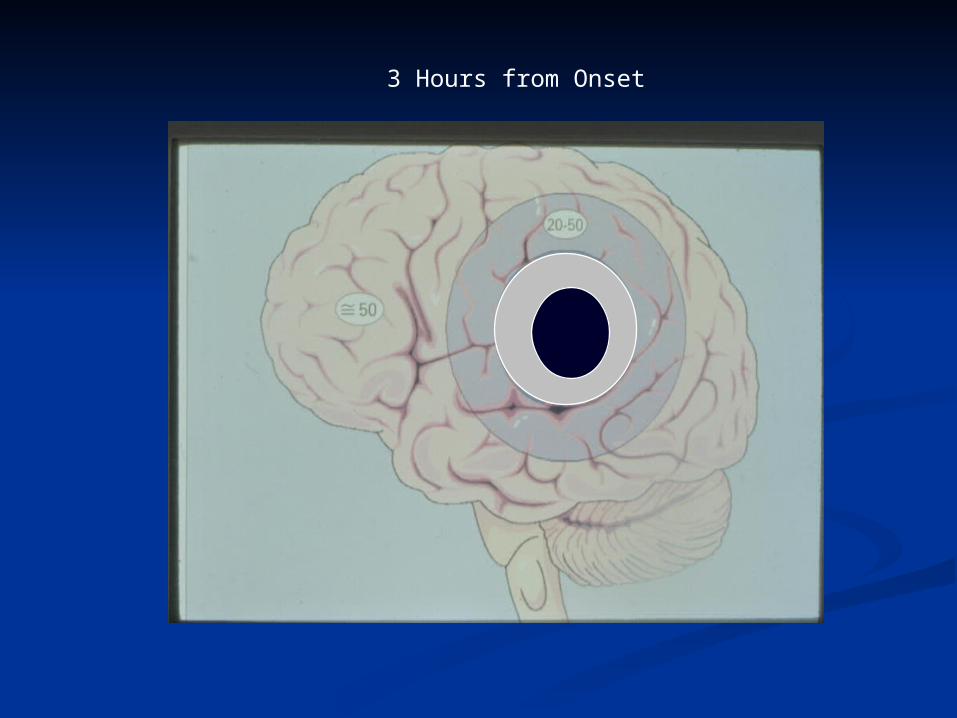
3 Hours from Onset
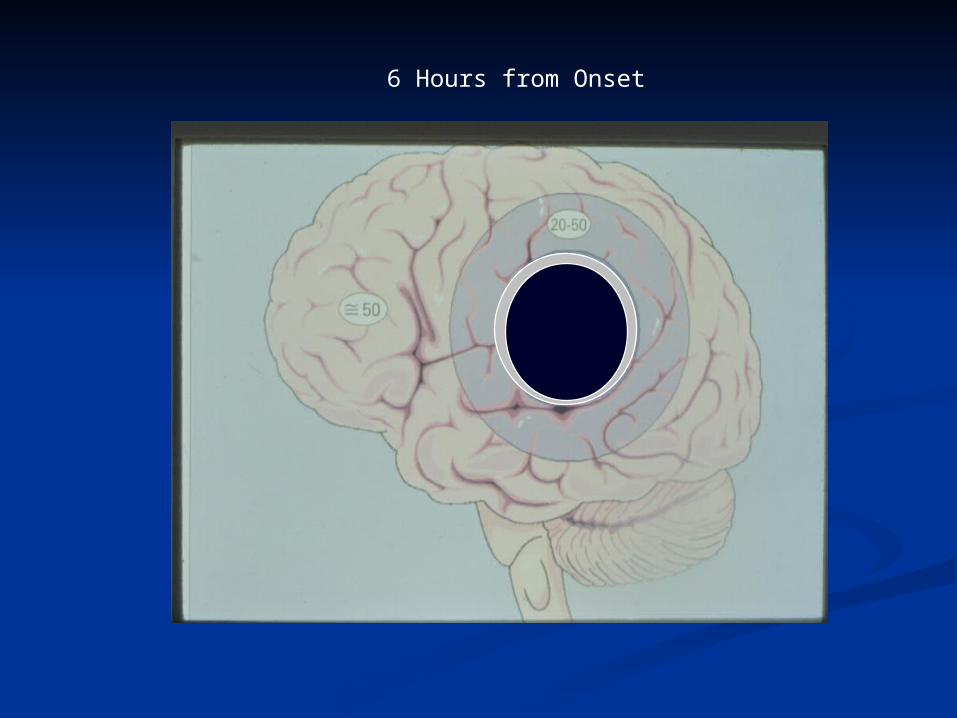
6 Hours from Onset

Heterogeneous Disease: Infarction at different rates 1 Hr 3 Hr
6 Hraverage
slow
fast

Acute Brain Attack TeamAcute Brain Attack Team
Objectives: Objectives: 1. To 1. To form a multi-disciplinary Strokeform a multi-disciplinary Stroke
team. 2. team. 2. To implement new advances that To implement new advances that
improve stroke outcome. improve stroke outcome. 3. To train Medical, 3. To train Medical, Neurological and Neurological and
Neurosurgical residents. Neurosurgical residents. 4. To participate in International 4. To participate in International ClinicalClinical
Research and Stroke trials.Research and Stroke trials.

Acute Brain Attack TeamAcute Brain Attack Team
Requirements:Requirements:1. 6 beds in Neuro Critical Care and 6 beds in1. 6 beds in Neuro Critical Care and 6 beds in
Stroke Unit Stroke Unit 2. E R Physicians interested in Stroke 2. E R Physicians interested in Stroke 3. 24 Hr/365 days ‘Full time’ Stroke/ 3. 24 Hr/365 days ‘Full time’ Stroke/ VascularVascular
Neurologists 4. Neurologists 4. Nursing staff trained in stroke careNursing staff trained in stroke care5. Stroke Rehab Programme 5. Stroke Rehab Programme 6. Physiotherapists 6. Physiotherapists 7. Speech Therapists 7. Speech Therapists 8. Dietitians 8. Dietitians

Anticoagulants and Antiplatelet Agents in Anticoagulants and Antiplatelet Agents in AcuteAcute
Ischemic StrokeIschemic Stroke
Report of the Joint Stroke Guideline Report of the Joint Stroke Guideline DevelopmentDevelopment
Committee of:Committee of: American Academy of NeurologyAmerican Academy of Neurology and the and the
American Stroke AssociationAmerican Stroke Association (a Division of the American Heart Association)(a Division of the American Heart Association)
B.M. Coull, MD; L.S. Williams, MD; L.B. B.M. Coull, MD; L.S. Williams, MD; L.B. Goldstein, MD; J.F. Meschia, MD; D. Goldstein, MD; J.F. Meschia, MD; D. Heitzman, M.S. Chaturvedi, MD; K.C. Heitzman, M.S. Chaturvedi, MD; K.C. Johnston, MD; S. Starkman, MD; L.B. Johnston, MD; S. Starkman, MD; L.B. Morgenstem, MD; J.L. Wilterdink,MD; S.R. Morgenstem, MD; J.L. Wilterdink,MD; S.R. Levine, MD &; J.L. Saver, MD.Levine, MD &; J.L. Saver, MD.

RecommendationsRecommendationsA tale of two drugsA tale of two drugs
1. Patients with acute ischemic stroke presenting 1. Patients with acute ischemic stroke presenting within 48 hours of symptom onset should be given within 48 hours of symptom onset should be given aspirin (160 to 325 mg/day) to reduce strokeaspirin (160 to 325 mg/day) to reduce strokemortality and decrease morbidity, providedmortality and decrease morbidity, providedcontraindications such as allergy and GI bleeding arecontraindications such as allergy and GI bleeding areabsent, and the patient has or will not be treated withabsent, and the patient has or will not be treated withrecombinant tissue-type Plasminogen Activator recombinant tissue-type Plasminogen Activator (Grade A). The data are insufficient at this time to (Grade A). The data are insufficient at this time to recommend the use of any other plateletrecommend the use of any other plateletantiaggregant in the setting of acute ischemic stroke.antiaggregant in the setting of acute ischemic stroke.

Recommendations (Contd.)Recommendations (Contd.)2. Subcutaneous unfractionated heparin, LMW2. Subcutaneous unfractionated heparin, LMW heparins, and heparinoids may be consideredheparins, and heparinoids may be considered for DVT prophylaxis in at-risk patients withfor DVT prophylaxis in at-risk patients with acute ischemic stroke, recognizing that non-acute ischemic stroke, recognizing that non- pharmacologic treatments for DVT preventionpharmacologic treatments for DVT prevention also exist (Grade A). A benefit in reducing thealso exist (Grade A). A benefit in reducing the incidence of PE has not been demonstrated.incidence of PE has not been demonstrated. The relative benefits of these agents must beThe relative benefits of these agents must be weighed against the risk of systemic and intra-weighed against the risk of systemic and intra- cerebral hemorrhage.cerebral hemorrhage.

Recommendations (Contd.)Recommendations (Contd.)
3. Although there is some evidence that fixed-dose,3. Although there is some evidence that fixed-dose,
subcutaneous, unfractionated heparin reduces early subcutaneous, unfractionated heparin reduces early
recurrent ischemic stroke, this benefit js negated by a recurrent ischemic stroke, this benefit js negated by a
concomitant increase in the occurrence of concomitant increase in the occurrence of
hemorrhage. Therefore, use of cutaneoushemorrhage. Therefore, use of cutaneous
unfractionated heparin is unfractionated heparin is not recommended not recommended forfor
decreasing the risk of death or related morbidity ordecreasing the risk of death or related morbidity or
for preventing early for preventing early Stroke recurrence Stroke recurrence (Grade A).(Grade A).

Suspected Acute Ischemic Stroke/TIA
DAY 1---1st 24hrs



Emergency Department ProtocolsAcute Stroke Nursing Protocolt-PA reconstitution and administration instructions
Acute Stroke Blood Draw and ED Order Sheet
Acute stroke Patient Clinical Examination Form
Neurologist Protocols
IV thrombolysis
Stroke scales
Post-thrombolysis Management
IA thrombolysis

NINDS - Stroke evaluation targets for NINDS - Stroke evaluation targets for potential Thrombolytic candidatespotential Thrombolytic candidates
Door to MD evaluationDoor to MD evaluation 10 min10 min Door to CT completionDoor to CT completion 25 min25 min Door to CT readDoor to CT read 45 min45 min Door to treatmentDoor to treatment 60 min60 min Access to neurological expertiseAccess to neurological expertise 15 min15 min Access to neurosurgical expertiseAccess to neurosurgical expertise 2 hrs2 hrs Admit to monitored bedAdmit to monitored bed 3 hrs3 hrs

Acute Brain Attack TeamAcute Brain Attack Team
OVERVIEW OF PROTOCOL:OVERVIEW OF PROTOCOL: 1.Creation of Public awareness about ABA1.Creation of Public awareness about ABA 2.Time 0 : Apollo Ambulance called for 2.Time 0 : Apollo Ambulance called for
3.Pre – arrival3.Pre – arrival 4.First hour after patient arrives in EMR4.First hour after patient arrives in EMR 5.Second Hour5.Second Hour 6. First 2 days6. First 2 days 7.Follow up.7.Follow up.

Acute Brain Attack TeamAcute Brain Attack Team
Education / Creation of awarenessEducation / Creation of awareness among the Public that: among the Public that:
1. Stroke is called Acute Brain Attack and 1. Stroke is called Acute Brain Attack and is a medical emergency.is a medical emergency.
2. Effective treatment is available if rushed 2. Effective treatment is available if rushed to Apollo Hospitals within the first 3-6 to Apollo Hospitals within the first 3-6 hours, after an ABA.hours, after an ABA.

CREATION OF AWARENESS AMONG CREATION OF AWARENESS AMONG THE PEOPLETHE PEOPLE
Stroke is “ACUTE BRAIN ATTACK" Stroke is “ACUTE BRAIN ATTACK" Exposure in TV channels as a video skit, Stroke Exposure in TV channels as a video skit, Stroke
information.information. Slide projection in Cinema theatres & other Slide projection in Cinema theatres & other
gatherings.gatherings. AIR (All India Radio) skits, small talks & AIR (All India Radio) skits, small talks &
announcements.announcements. Handouts in English,Tamil,Telugu & Hindi in Handouts in English,Tamil,Telugu & Hindi in
gatherings.gatherings. Posters in prominent places, road junctions & public Posters in prominent places, road junctions & public
places.places. Lectures - periodic at public places / functions / Lectures - periodic at public places / functions /
health meetings.health meetings.

Education / Creation of Education / Creation of awarenessawareness among the Public among the Public
Recognize the Recognize the warning signs warning signs of Stroke like:of Stroke like: 1.1.SuddenSudden numbness or weakness of the face, arm or numbness or weakness of the face, arm or
leg on one side of the body. leg on one side of the body.
2.2.SuddenSudden confusion, trouble speaking or confusion, trouble speaking or understanding.understanding.
3.3.SuddenSudden trouble seeing in one or both eyes. trouble seeing in one or both eyes.
4.4.SuddenSudden trouble walking, dizziness, loss of balance trouble walking, dizziness, loss of balance or Coordination. or Coordination.
5.5.SuddenSudden severe headache or coma. severe headache or coma.

The Chennai Acute Brain The Chennai Acute Brain Attack ConsortiumAttack Consortium
Formed on October 29, 2009, World Formed on October 29, 2009, World Stroke Day.Stroke Day.
Prof. M.R.SIVAKUMAR, MD, DM, FRCP, Prof. M.R.SIVAKUMAR, MD, DM, FRCP, FAAN, FAHA, is the Program Director FAAN, FAHA, is the Program Director and Co-ordinatorand Co-ordinator
ALL ALL 95000 17893 95000 17893 IF ANY OF THE IF ANY OF THE ABOVE SYMPTOMS ARE NOTED(24x7).ABOVE SYMPTOMS ARE NOTED(24x7).

Time Zero - Ambulance is calledTime Zero - Ambulance is called
The ambulance operator will be asked to rush The ambulance operator will be asked to rush the ambulance to the Stroke victim’s house.the ambulance to the Stroke victim’s house.
The Stroke patient will be transported to the The Stroke patient will be transported to the nearest scan center where facilities for CT/MRI nearest scan center where facilities for CT/MRI Scans are available.Scans are available.
After the Neuroimaging, the patient will be After the Neuroimaging, the patient will be admitted to the nearest Hospital equipped with admitted to the nearest Hospital equipped with Stroke Unit Stroke Unit and Acute Stroke Protocols.and Acute Stroke Protocols.

Pre -arrival: Before patient Pre -arrival: Before patient arrives at the ERarrives at the ER
The The ambulance operatorambulance operator should: should:1.Dispatch the ambulance immediately. 1.Dispatch the ambulance immediately. 2.Inform the Emergency Room/ Neurologist that a 2.Inform the Emergency Room/ Neurologist that a Stroke victim is on the way. Stroke victim is on the way.
EMR Medical OfficerEMR Medical Officer should: should:
1. Alert the Radiology Staff in the CT scan 1. Alert the Radiology Staff in the CT scan area/Duty Radiologist.area/Duty Radiologist. 2. Inform Stroke Neurologist2. Inform Stroke Neurologist

Pre-arrivalPre-arrival Phone contact eye-witnesses or family members Phone contact eye-witnesses or family members
to obtain:to obtain: - details of the event (time of onset)- details of the event (time of onset) - relevant medical history, medications, allergies- relevant medical history, medications, allergies - open discussion about risk/benefit of potential - open discussion about risk/benefit of potential
emergency therapiesemergency therapies - ensure open line of communication with next of - ensure open line of communication with next of
kinkin
Acute Stroke Nursing ProtocolAcute Stroke Nursing Protocol
T-PA reconstitution and administration T-PA reconstitution and administration instructionsinstructions
Acute Stroke Blood Draw Order SheetAcute Stroke Blood Draw Order Sheet Acute Stroke Patient Clinical Examination Acute Stroke Patient Clinical Examination
FormForm Acute Stroke Action PlanAcute Stroke Action Plan Acute Stroke Nursing ProtocolAcute Stroke Nursing Protocol

Acute Stroke Nursing ProtocolAcute Stroke Nursing Protocol
Record time of onset of symptomsRecord time of onset of symptoms Note patient’s PCP and primary Note patient’s PCP and primary
neurologistneurologist Notify ED attendingNotify ED attending Notify Stroke NeurologistNotify Stroke Neurologist Obtain vital signsObtain vital signs Ask the family medical history from patient Ask the family medical history from patient
or family: or family:

Acute Stroke Nursing ProtocolAcute Stroke Nursing Protocol
Recent trauma, datesRecent trauma, dates Recent surgery, datesRecent surgery, dates Recent procedure, datesRecent procedure, dates Prior stroke/TIA, datesPrior stroke/TIA, dates HTN; DM; CAD; AFHTN; DM; CAD; AF Bleeding disorder; coumadin useBleeding disorder; coumadin use Aspirin use ; GI, GU, or pulmonary hemorrhageAspirin use ; GI, GU, or pulmonary hemorrhage Migraine;Migraine; Metal fragments, or pacemakerMetal fragments, or pacemaker

First Hour - after the patient arrives in the ERFirst Hour - after the patient arrives in the ER::
The ER Medical Officer should note the time of The ER Medical Officer should note the time of arrival of the patient and:arrival of the patient and: 1.Inform CT scan room, Stroke Neurologist 1.Inform CT scan room, Stroke Neurologist
immediately.immediately. 2.ABC - Resuscitation if needed.2.ABC - Resuscitation if needed. 3.Quick History/Examination to confirm the initial 3.Quick History/Examination to confirm the initial
suspicion of ABA.suspicion of ABA. 4.Phlebotomy -->Send blood for Complete Blood 4.Phlebotomy -->Send blood for Complete Blood
Count, glucose, Creatinine, Urea, Electrolytes, PT, Count, glucose, Creatinine, Urea, Electrolytes, PT, PTT. Leave IV plug in.PTT. Leave IV plug in.
5.Check bedside glucose with a drop of blood from 5.Check bedside glucose with a drop of blood from the phlebotomy. Treat the phlebotomy. Treat
Hypoglycemia (<70mg/dl) immediately.Hypoglycemia (<70mg/dl) immediately.

First Hour - after the patient arrives in the ER:First Hour - after the patient arrives in the ER:
6.Optimum MAP is 130 mm of Hg. If BP is low, start IV Normal 6.Optimum MAP is 130 mm of Hg. If BP is low, start IV Normal Saline and if BP is highSaline and if BP is high
( > 180/110 mm/Hg.), place a Nitrodisc (40 mg).( > 180/110 mm/Hg.), place a Nitrodisc (40 mg). 7.ECG - If ischemic changes are noted, request Cardiac 7.ECG - If ischemic changes are noted, request Cardiac
Enzymes in addition to other tests.Treat arrhythmias if noted.Enzymes in addition to other tests.Treat arrhythmias if noted. 8.Check vital signs every 10 minutes.8.Check vital signs every 10 minutes. 9.Wheel patient to CT scan area.9.Wheel patient to CT scan area. 10. Perform Transcranial Doppler at bedside, Carotid/Vertebral 10. Perform Transcranial Doppler at bedside, Carotid/Vertebral
/TC Doppler and ECHO Cardiogram in Vascular lab. /TC Doppler and ECHO Cardiogram in Vascular lab. Start collecting the result of investigations.Start collecting the result of investigations.

Transcranial Doppler in Transcranial Doppler in AISAIS
Can help identify intracranial vascular diseaseCan help identify intracranial vascular disease Useful to guide and monitor acute therapyUseful to guide and monitor acute therapy Useful for monitoring for emboli, and based on Useful for monitoring for emboli, and based on
location of MES (microembolic signals, nHITS), can location of MES (microembolic signals, nHITS), can differentiate between cardioembolic, large artery, differentiate between cardioembolic, large artery, medium vessel sources for strokemedium vessel sources for stroke
TCD performed 6 hours after stroke onset, if normal TCD performed 6 hours after stroke onset, if normal was predictive of early improvement, and if abnormal was predictive of early improvement, and if abnormal was predictive of early deterioration.was predictive of early deterioration.

TCD in Acute StrokeTCD in Acute Stroke
MES have been detected distal to intracranial MES have been detected distal to intracranial
arterial occlusions, and when found in high arterial occlusions, and when found in high numbers appear to herald the break-up of the numbers appear to herald the break-up of the thrombus.thrombus.
Some experimental evidence suggests that Some experimental evidence suggests that ultrasound (although at frequencies lower than ultrasound (although at frequencies lower than those used for TCD imaging) may enhance those used for TCD imaging) may enhance thrombolysis of intra-arterial thrombi.thrombolysis of intra-arterial thrombi.

Microembolic Signals (HITS)Microembolic Signals (HITS)
High intensityHigh intensity TransientTransient UnidirectionalUnidirectional Occur randomly in cardiac cycleOccur randomly in cardiac cycle Characteristic chirping soundCharacteristic chirping sound MES have particular characteristics that MES have particular characteristics that
distinguish them from the waveform, distinguish them from the waveform, background, and artifacts that move across the background, and artifacts that move across the monitoring screen. monitoring screen.
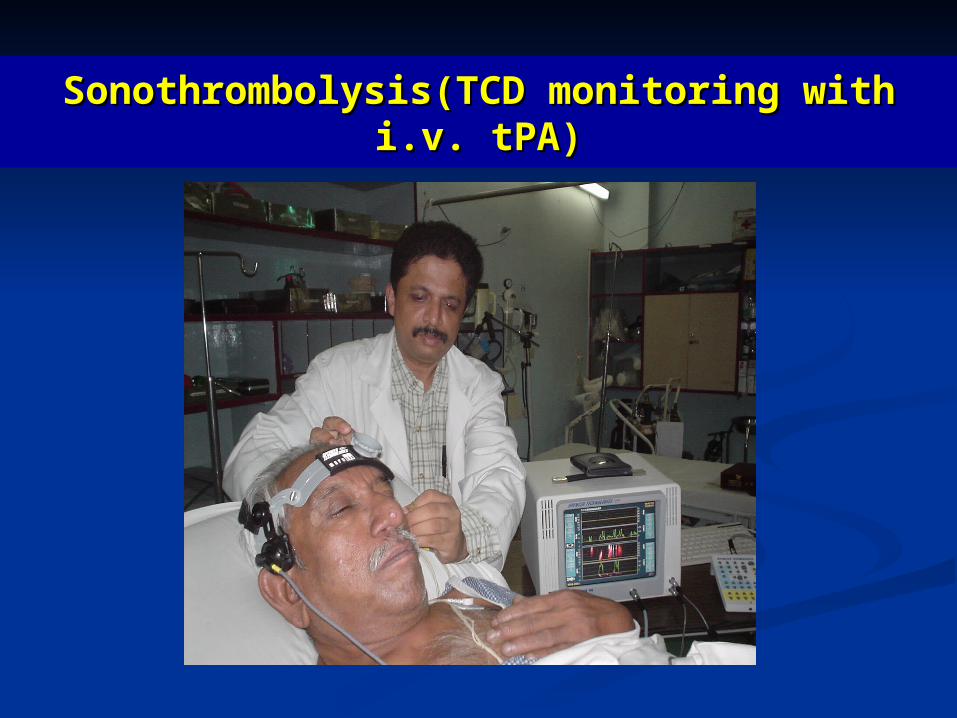
Sonothrombolysis(TCD monitoring with Sonothrombolysis(TCD monitoring with i.v. tPA)i.v. tPA)

TCD and Neuroimaging DataTCD and Neuroimaging Data
Pre-Sonothrombolysis
Post-Sonothrombolysis
49 yo presentedwith Rt. Sided Hemiplegia/Dysphasia since90 min.

Acute Brain Attack TeamAcute Brain Attack Team
The radiology technician should make The radiology technician should make him/herself available immediately.him/herself available immediately.
Should perform a non-contrast CT scan of the Should perform a non-contrast CT scan of the Brain as the ‘next case’ and the films should be Brain as the ‘next case’ and the films should be printed out as soon as possible.printed out as soon as possible.
The stroke Neurologist should make him/herself The stroke Neurologist should make him/herself available with the first call and arrive in the ER available with the first call and arrive in the ER as soon as the patient gets there.as soon as the patient gets there.

NCCT pre and post t-PANCCT pre and post t-PA
CT CT AngiogramAngiogram
Acute Brain Attack TeamAcute Brain Attack Team
First Hour:First Hour: The Stroke Neurologist would evaluate the The Stroke Neurologist would evaluate the
clinical picture of the patient, review the CT clinical picture of the patient, review the CT Head and the results of the investigations.Head and the results of the investigations.
If the patient turns out to have an intracerebral If the patient turns out to have an intracerebral or subarachnoid bleed, follow appropriate or subarachnoid bleed, follow appropriate protocol. protocol.
If the patient has an infarct, a decision needs to If the patient has an infarct, a decision needs to be made if r-TPA could be safely used in the be made if r-TPA could be safely used in the patient.patient.
The pharmacy needs to be alerted immediately The pharmacy needs to be alerted immediately once a decision is made to use r-TPAonce a decision is made to use r-TPA

Acute Brain Attack TeamAcute Brain Attack Team
Intravenous r-TPA would be administered Intravenous r-TPA would be administered in the ER, only after getting an informed in the ER, only after getting an informed consent and under the direct supervision consent and under the direct supervision of the Neurologist.of the Neurologist.
The patient should be on ECG monitor The patient should be on ECG monitor and vital signs should be checked every and vital signs should be checked every 10 minutes during the r-TPA infusion.10 minutes during the r-TPA infusion.
The patient would be moved to the Acute The patient would be moved to the Acute Stroke Unit.Stroke Unit.

Second Hour:Second Hour:
The Stroke Neurologist would evaluate the clinical The Stroke Neurologist would evaluate the clinical picture of the patient, review the CT Head and the picture of the patient, review the CT Head and the results of the investigations.results of the investigations.
If the patient turns out to have an intracerebral or If the patient turns out to have an intracerebral or subarachnoid bleed, follow appropriate protocol. subarachnoid bleed, follow appropriate protocol.
If the patient has an infarct, a decision needs to be If the patient has an infarct, a decision needs to be made if r-TPA could be safely used in the patient.made if r-TPA could be safely used in the patient.
The pharmacy needs to be alerted immediately once a The pharmacy needs to be alerted immediately once a decision is made to use r-TPAdecision is made to use r-TPA

TPATPA
Intravenous r-TPAIntravenous r-TPA would be administered in would be administered in the ER, only after getting an informed consent the ER, only after getting an informed consent and under the direct supervision of the and under the direct supervision of the Neurologist.Neurologist.
The patient should be on ECG monitor and vital The patient should be on ECG monitor and vital signs should be checked every 10 minutes signs should be checked every 10 minutes during the r-TPA infusion.during the r-TPA infusion.
The patient would be moved to the Acute Stroke The patient would be moved to the Acute Stroke Unit.Unit.

Exclusion Criteria for Thrombolytic Exclusion Criteria for Thrombolytic TherapyTherapy: :
AbsoluteAbsolute:: 1. CT or MRI evidence of hemorrhage1. CT or MRI evidence of hemorrhage 2. Complete resolution of symptoms2. Complete resolution of symptoms RelativeRelative:: 1. CT changes > one-third of MCA territory1. CT changes > one-third of MCA territory 2. Hypertension (systolic 2. Hypertension (systolic >> 185, diastolic 185, diastolic >> 110) that remains unresponsive to 110) that remains unresponsive to
antihyperstensive management .antihyperstensive management . 3. History of GU or GI bleeding within three (3) weeks3. History of GU or GI bleeding within three (3) weeks 4. History of CPR, extensive trauma, or surgery within 2 weeks4. History of CPR, extensive trauma, or surgery within 2 weeks 5. History of stroke within two (2) weeks5. History of stroke within two (2) weeks 6. PT 6. PT >> 15, platelets 15, platelets << 100,000, INR 100,000, INR >> 1.7 1.7 7. LP or non-compressible arterial puncture within one week7. LP or non-compressible arterial puncture within one week 8. History of seizure at time of onset8. History of seizure at time of onset

Clinical CautionsClinical Cautions
1. Clinical presentation suggestive of SAH, 1. Clinical presentation suggestive of SAH, even if CT is negativeeven if CT is negative
2. Age 2. Age >> 80 80 3. Active pericarditis or pericardial infusion3. Active pericarditis or pericardial infusion 4. Glucose 4. Glucose << 50 or 50 or >> 400 400 5. NIH Stroke Scale 5. NIH Stroke Scale >> 22 22 6. Rapidly improving symptoms6. Rapidly improving symptoms

IV rt-PA reconstitution & DosingIV rt-PA reconstitution & Dosing
Dose: 0.9 mg/Kg ( Maximum: 90 mg.)Dose: 0.9 mg/Kg ( Maximum: 90 mg.) 10% bolus, rest as an infusion over 1 hour.10% bolus, rest as an infusion over 1 hour.

Intravenous/Intra-Arterial Intravenous/Intra-Arterial Therapy:Therapy:
Consider for the following patients:Consider for the following patients: Patients with suspected large vessel occlusive Patients with suspected large vessel occlusive
disease(carotid terminus, basilar artery, M1, disease(carotid terminus, basilar artery, M1, proximal M2)proximal M2)
Patients with a diffusion-perfusion mismatch on Patients with a diffusion-perfusion mismatch on MRMR
Patients being transferred from other institutionsPatients being transferred from other institutions Consent for IV/IA therapy should be obtained at Consent for IV/IA therapy should be obtained at
the institution initiating IV therapy.the institution initiating IV therapy.



TIBI TIBI ((Thrombolysis in Brain IschemiaThrombolysis in Brain Ischemia))
Grade 0Grade 0: : AbsentAbsent - absent flow signals are defined by - absent flow signals are defined by the lack of regular pulsatile flow signals despite the lack of regular pulsatile flow signals despite varying degrees of background noise.varying degrees of background noise.
Grade 1Grade 1: : Minimal Minimal - systolic spikes of variable velocity - systolic spikes of variable velocity and duration; absent diastolic flow during all cardiac and duration; absent diastolic flow during all cardiac cycles based on a visual interpretation of periods of no cycles based on a visual interpretation of periods of no flow during end diastole(reverberating flow is a type of flow during end diastole(reverberating flow is a type of minimal flow).minimal flow).
Grade 2Grade 2: : BluntedBlunted - flattened systolic flow acceleration of - flattened systolic flow acceleration of variable duration compared to control; positive end variable duration compared to control; positive end diastolic velocity and PI < 1.2.diastolic velocity and PI < 1.2.

TIBI TIBI ((Thrombolysis in Brain IschemiaThrombolysis in Brain Ischemia))
Grade 3Grade 3: : Dampened Dampened - normal systolic flow acceleration; - normal systolic flow acceleration; positive end-diastolic velocity; decreased MFVs by positive end-diastolic velocity; decreased MFVs by >30% compared to control.>30% compared to control.
Grade 4Grade 4: : StenoticStenotic - MFV >80 cm/s and velocity - MFV >80 cm/s and velocity difference >30% compared to control or; if both difference >30% compared to control or; if both affected and comparison sides have MFV <80 cm/s affected and comparison sides have MFV <80 cm/s due to low end-diastolic velocities, MFV >30% due to low end-diastolic velocities, MFV >30% compared to the control side and signs of turbulence.compared to the control side and signs of turbulence.
Grade 5Grade 5: : Normal Normal - <30% MFV difference compared to - <30% MFV difference compared to control; similar waveform shapes compared to control; similar waveform shapes compared to controls.controls.

Carotid Carotid DopplerDoppler
Flow Velocity CriteriaFlow Velocity Criteria
Peak Systolic Velocity Diastolic Velocity ICA/CCA Peak Systolic Velocity Diastolic Velocity ICA/CCA % Diameter % Diameter(cm/sec) (cm/sec) (cm/sec) (cm/sec) Ratio Stenosis Ratio Stenosis
< 140 < 140 < 40 < 40 < 2 < 2 < 50% < 50% > 140 > 140 < 110 < 110 > 2 > 2 50-75% 50-75% >> 140 >> 140 > 110 > 110 > 3 > 3 75-95% 75-95%Variable Velocities Variable Variable Velocities Variable Variable 95-99% Variable 95-99%
(Subtotal occlusion)(Subtotal occlusion)No detectable flow N/A N/A Probable occlusionNo detectable flow N/A N/A Probable occlusion

Onset 3-6 hours: Intra-Arterial ThrombolysisOnset 3-6 hours: Intra-Arterial Thrombolysis ACT:ACT: Baseline, 1 hour, 2 hoursBaseline, 1 hour, 2 hours 1. Administer 2000 units heparin IV bolus if 1. Administer 2000 units heparin IV bolus if
thrombus is identified angiographically.thrombus is identified angiographically. 2. Start maintenance infusion of heparin at 450 2. Start maintenance infusion of heparin at 450
units/hour.units/hour. 3. Position 2.3 French microcatheter just distal to 3. Position 2.3 French microcatheter just distal to
occlusion.occlusion. 4. Infuse 2 mg TPA (2 mg/2 cc NS) over 4 4. Infuse 2 mg TPA (2 mg/2 cc NS) over 4
minutes minutes distaldistal to thrombus. to thrombus. 5. Retract catheter into thrombus.5. Retract catheter into thrombus.

Onset 3-6 hours: Intra-Arterial ThrombolysisOnset 3-6 hours: Intra-Arterial Thrombolysis 6. Infuse 2 mg TPA (2 mg/2 cc normal saline) over 4 minutes into 6. Infuse 2 mg TPA (2 mg/2 cc normal saline) over 4 minutes into
thrombus.thrombus. 7. Start maintenance infusion of 10 mg/hr TPA using infusion pump.7. Start maintenance infusion of 10 mg/hr TPA using infusion pump. 8. Perform control angiogram every 15 minutes (or as needed) after 8. Perform control angiogram every 15 minutes (or as needed) after
start of maintenance TPA infusion (option to mechanically disrupt start of maintenance TPA infusion (option to mechanically disrupt every 15 min.).every 15 min.).
9. Perform neurological examination every 15 minutes to assess level 9. Perform neurological examination every 15 minutes to assess level of consciousness and upper extremity motor functionof consciousness and upper extremity motor function
10. Infuse maintenance dose for a maximum of 2 hours to a maximum 10. Infuse maintenance dose for a maximum of 2 hours to a maximum time after onset of 8 hours.time after onset of 8 hours.
11. Consider more aggressive mechanical disruption (i.e., snare) if clot 11. Consider more aggressive mechanical disruption (i.e., snare) if clot has not resolved after 1 hour.has not resolved after 1 hour.
12. Terminate infusion prior to 2 hours if complete clot lysis is 12. Terminate infusion prior to 2 hours if complete clot lysis is achieved.achieved.
13. Total IA TPA dose = 24 mg.13. Total IA TPA dose = 24 mg.

tPA Dosing charttPA Dosing chartWeight (Lbs)Conv. to Kg) Total Dose t-PA Bolus t-PA Bolus Discard Dose Infusion dose Inf.rateWeight (Lbs)Conv. to Kg) Total Dose t-PA Bolus t-PA Bolus Discard Dose Infusion dose Inf.rate
Kg ( mg) (mg) (ml) ( mg) (mg) (ml/hr)Kg ( mg) (mg) (ml) ( mg) (mg) (ml/hr)
220+ 100.0 90.0 9.0 9.0 10.0 81.0 81.0220+ 100.0 90.0 9.0 9.0 10.0 81.0 81.0
210 95.5 85.9 8.6 8.6 14.1 77.3 77.3210 95.5 85.9 8.6 8.6 14.1 77.3 77.3
200200 90.9 81.8 8.2 8.2 18.2 73.6 73.6 90.9 81.8 8.2 8.2 18.2 73.6 73.6
190190 86.4 77.7 7.8 7.8 22.3 70.0 70.0 86.4 77.7 7.8 7.8 22.3 70.0 70.0
180 81.8 73.6 7.4 7.4 26.4 66.3 66.3180 81.8 73.6 7.4 7.4 26.4 66.3 66.3
170170 77.3 69.5 7.0 7.0 30.5 62.6 62.6 77.3 69.5 7.0 7.0 30.5 62.6 62.6
160160 72.7 65.5 6.5 6.5 34.5 58.9 58.9 72.7 65.5 6.5 6.5 34.5 58.9 58.9
150 150 68.2 68.2 61.4 61.4 6.1 6.1 6.1 6.1 38.6 38.6 55.2 55.2 55.2 55.2
140 63.6140 63.6 57.3 57.3 5.7 5.7 5.7 5.7 42.7 42.7 51.5 51.5 51.5 51.5
130130 59.1 53.2 5.3 5.3 46.8 47.9 47.9 59.1 53.2 5.3 5.3 46.8 47.9 47.9
120120 54.5 49.1 4.9 4.9 50.9 44.2 44.2 54.5 49.1 4.9 4.9 50.9 44.2 44.2
110 50.0 45.0 4.5 4.5 55.0 40.5 40.5110 50.0 45.0 4.5 4.5 55.0 40.5 40.5
100 45.5 40.9 4.1 4.1 59.1 36.8 36.8100 45.5 40.9 4.1 4.1 59.1 36.8 36.8

Procedure consent formProcedure consent form ----------Hospitals, Chennai.----------Hospitals, Chennai. Patient’s name :Patient’s name : Unit No. :Unit No. : Procedure:Procedure: I have explained to the patient / family / guardian the nature of the patient’s condition, I have explained to the patient / family / guardian the nature of the patient’s condition,
the nature of the procedure, the benefits to be reasonably expected compared with the nature of the procedure, the benefits to be reasonably expected compared with alternative approaches. I have discussed the likelihood of major risks or alternative approaches. I have discussed the likelihood of major risks or complications of this procedure including (if applicable) but not limited to loss of limb complications of this procedure including (if applicable) but not limited to loss of limb function, brain damage, paralysis, hemorrhage, infection, complications from function, brain damage, paralysis, hemorrhage, infection, complications from transfusion of blood components, drug reactions, blood clots, and transfusion of blood components, drug reactions, blood clots, and loss of lifeloss of life. I have . I have also indicated that with any procedure there is always the possibility of an unexpected also indicated that with any procedure there is always the possibility of an unexpected complication. complication.
Dr.Dr. has explained to me (or my family member) has explained to me (or my family member) why they believe a stroke is happening and which of the available methods would be why they believe a stroke is happening and which of the available methods would be most likely to improve my condition. They have explained the risks and benefits of the most likely to improve my condition. They have explained the risks and benefits of the drugs and techniques available to dissolve blood clots in the brain and possible drugs and techniques available to dissolve blood clots in the brain and possible alternative treatments. They have recommended use of the INTRAVENOUS DRUG, alternative treatments. They have recommended use of the INTRAVENOUS DRUG, recombinant Tissue Plasminogen Activator (clot – dissolver) to dissolve the blood recombinant Tissue Plasminogen Activator (clot – dissolver) to dissolve the blood clot.clot.
INTRAVENOUS THROMBOLYSIS:INTRAVENOUS THROMBOLYSIS:

Procedure consent Procedure consent ( contd.)( contd.)
The risks include:The risks include: 1. Death, Stroke or permanent neurologic injury (paralysis, 1. Death, Stroke or permanent neurologic injury (paralysis, coma,etc) 2. Worsening of stroke symptoms from swelling or bleeding in the brain 3. coma,etc) 2. Worsening of stroke symptoms from swelling or bleeding in the brain 3. Bleeding in other parts of the body 4. Need for blood transfusions to replace blood or Bleeding in other parts of the body 4. Need for blood transfusions to replace blood or clotting factors 5. Other unexpected complications.clotting factors 5. Other unexpected complications.
All questions were answered and the patient / family / guardian consents to the All questions were answered and the patient / family / guardian consents to the procedure.procedure.
(Physician’s Signature)(Physician’s Signature) Date :Date : Dr.Dr. has explained the above to me and I consent to the has explained the above to me and I consent to the
procedure. I understand that APOLLO HOSPITALS is an academic medical center procedure. I understand that APOLLO HOSPITALS is an academic medical center and that residents, registrars, fellows and students in medical and allied disciplines and that residents, registrars, fellows and students in medical and allied disciplines may participate in this procedure. In addition, I understand that tissue, blood or other may participate in this procedure. In addition, I understand that tissue, blood or other specimens removed for necessary diagnostic or therapeutic reasons may specimens removed for necessary diagnostic or therapeutic reasons may subsequently be used by the Hospital or members of its professional staff for subsequently be used by the Hospital or members of its professional staff for research or educational purposes. research or educational purposes.
( patient’s / family’s / guardian’s signature)( patient’s / family’s / guardian’s signature)

Symptomatic hemorrhage after t-PASymptomatic hemorrhage after t-PA STAT head CT, if ICH suspected STAT head CT, if ICH suspected Consult Neurosurgery for ICH Consult Neurosurgery for ICH Check CBC, PT, PTT, platelets, fibrinogen and D-dimer. Repeat q 2 h until Check CBC, PT, PTT, platelets, fibrinogen and D-dimer. Repeat q 2 h until
bleeding is controlled bleeding is controlled Give FFP 2 units every 6 hours for 24 hours after dose Give FFP 2 units every 6 hours for 24 hours after dose Give cryoprecipitate 20 units. If fibrinogen level < 200 mg/dL at 1 hr, repeat Give cryoprecipitate 20 units. If fibrinogen level < 200 mg/dL at 1 hr, repeat
cryoprecipitate dose. cryoprecipitate dose. Give platelets 4 units Give platelets 4 units Give protamine sulfate 1 mg/100 U heparin received in last 3 hours (give Give protamine sulfate 1 mg/100 U heparin received in last 3 hours (give
inital 10 mg test dose. Maximum dose :50 mg) inital 10 mg test dose. Maximum dose :50 mg) Institute frequent neurochecks and therapy of acutely elevated ICP, as Institute frequent neurochecks and therapy of acutely elevated ICP, as
needed needed May give aminocaproic acid (Amicar) 5 g in 250 cc NS IV over 1 hr as a last May give aminocaproic acid (Amicar) 5 g in 250 cc NS IV over 1 hr as a last
resort. resort.
NIH Stroke ScaleNIH Stroke ScaleThe NINDS t-PA Stroke Trial No. ___ The NINDS t-PA Stroke Trial No. ___ Pt. Date of Birth ___ ___/___ ___/___ ___Pt. Date of Birth ___ ___/___ ___/___ ___ Date of Exam ___ ___/___ ___/___ ___Date of Exam ___ ___/___ ___/___ ___ Intervals : Intervals :
1[ ] Baseline 1[ ] Baseline
2[ ] 2 hours post treatment 2[ ] 2 hours post treatment
3[ ] 24 hours post onset of symptoms ±20 mins.3[ ] 24 hours post onset of symptoms ±20 mins.
4[ ] 7-10 days4[ ] 7-10 days
5[ ] 3 months 5[ ] 3 months
6[ ] Other 6[ ] Other
Total Score : 42 Total Score : 42

Baseli
ne
30
Min.
1 hr
2 hr
24 hr
48 hr
7-10 days
1a. Level of Consciousness
Alert 0 Drowsy 1 Stuporous 2 Coma 3
1b. LOC Questions
Answers both correctly 0 Answers one correctly 1 Incorrect 2
1c. LOC Commands
Obeys both correctly 0 Obeys one correctly 1 Incorrect 2
2. Best Gaze
Normal 0 Partial gaze palsy 1 Forced deviation 2
3. Best Visual
No visual loss 0 Partial hemianopia 1 Complete hemianopia 2 Bilateral hemianopia 3
4. Facial Palsy
Normal 0 Minor 1 Partial 2 Complete 3
5. Best Arm Movement
No drift 0 Drift 1 Can’t resist gravity 2 No effort against gravity 3 No movement 4
6. Other Arm For brainstem strokeuse same scale as above
0-4
7. Best Motor Leg
No drift 0 Drift 1 Can’t resist gravity 2 No effort against gravity 3 No movement 4
8. Other Leg For brainstem strokeuse same scale as above
0-4
9. Limb Ataxia
Absent 0 Present in upper or lower
1 Present in both 2
10. Sensory
Normal 0 Partial loss 1 Dense loss 2
11. Neglect
No neglect 0 Partial neglect 1 Complete neglect 2
12. Dysarthria
Normal articulation 0 Mild to moderate dysarthria
1 Near unintelligible or worse
2 13. Best Language
No aphasia 0 Mild to moderate aphasia
1 Severe aphasia 2 Mute 3
14. Change from Previous Exam
Same S Better B Worse W
15. Change from Baseline
Same S

Modified Rankin ScaleModified Rankin Scale Patient NamPatient Name: e: RANKIN Rater Name: SCALE (MRS) Date: RANKIN Rater Name: SCALE (MRS) Date: ____Score DescriptionScore Description 0 No symptoms at all0 No symptoms at all 1 No significant disability despite symptoms; able to carry out all usual duties 1 No significant disability despite symptoms; able to carry out all usual duties
and activitiesand activities 2 Slight disability; unable to carry out all previous activities, but able to look after 2 Slight disability; unable to carry out all previous activities, but able to look after
own affairs without assistanceown affairs without assistance 3 Moderate disability; requiring some help, but able to walk without assistance3 Moderate disability; requiring some help, but able to walk without assistance 4 Moderately severe disability; unable to walk without assistance and unable to 4 Moderately severe disability; unable to walk without assistance and unable to
attend to own bodily needs without assistanceattend to own bodily needs without assistance 5 Severe disability; bedridden, incontinent and requiring constant nursing care 5 Severe disability; bedridden, incontinent and requiring constant nursing care
and attentionand attention 6 Dead6 Dead TOTAL (0–6): _______TOTAL (0–6): _______ ReferencesReferences Rankin J. “Cerebral vascular accidents in patients over the age of 60.”Rankin J. “Cerebral vascular accidents in patients over the age of 60.” Scott Med J Scott Med J 1957;2:200-151957;2:200-15 Bonita R, Beaglehole R. “Modification of Rankin Scale: Recovery of motor Bonita R, Beaglehole R. “Modification of Rankin Scale: Recovery of motor
function after stroke.” function after stroke.” Stroke Stroke 1988 Dec;19(12):1497-15001988 Dec;19(12):1497-1500

Barthel IndexBarthel Index

First day:First day:
Transcranial doppler repeated after 6 hours if Transcranial doppler repeated after 6 hours if abnormal earlier.abnormal earlier.
Repeat CT Scan if I.V. r-TPA has been used. Repeat CT Scan if I.V. r-TPA has been used.
Continuous ECG monitor. Hourly vital signs and Continuous ECG monitor. Hourly vital signs and neurological status examination.neurological status examination.
Swallowing/nutrition status assessed and treated Swallowing/nutrition status assessed and treated appropriately. appropriately.
DVT prophylaxis instituted.DVT prophylaxis instituted. Physiotherapy/ Speech therapy started, if Physiotherapy/ Speech therapy started, if
condition is stable.condition is stable.

Acute Brain Attack TeamAcute Brain Attack Team
Second day:Second day: Continue medical management and Continue medical management and
monitoring.monitoring. Ensure that detailed case evaluation Ensure that detailed case evaluation
notes, NIHSS, mRS and Barthel notes, NIHSS, mRS and Barthel Index are documented.Index are documented.


Standard treatment with Alteplase to Standard treatment with Alteplase to Reverse Stroke ( STARS) studyReverse Stroke ( STARS) study
STARS STARS CVRFCVRFNo.No. 389389 174174Mean age(yrs.)Mean age(yrs.) 6969 60.3(23-78)60.3(23-78)Time to treatment(%)Time to treatment(%)
0-90 mins.0-90 mins. 4.2 4.2 21.4021.4091-180 mins.91-180 mins. 82.382.3 75.0075.00180 - 270 mins.180 - 270 mins. 13.513.5 3.60 3.60
Median time from stroke Median time from stroke onset to tPA Rx.onset to tPA Rx. 2 h 44 m2 h 44 m 2h,22m2h,22mMedian time from ER Median time from ER arrival to tPA Rx.arrival to tPA Rx. 1 h 36m1 h 36m 1h28m1h28m
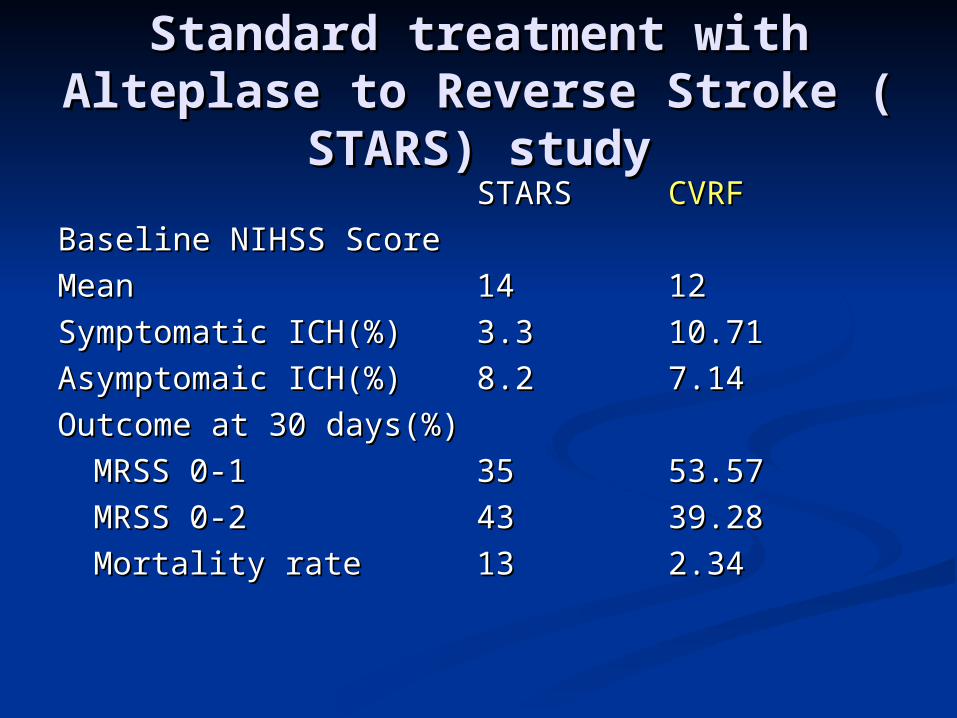
Standard treatment with Alteplase to Standard treatment with Alteplase to Reverse Stroke ( STARS) studyReverse Stroke ( STARS) study
STARS STARS CVRFCVRF
Baseline NIHSS ScoreBaseline NIHSS Score
MeanMean 1414 1212
Symptomatic ICH(%)Symptomatic ICH(%) 3.33.3 10.7110.71
Asymptomaic ICH(%)Asymptomaic ICH(%) 8.28.2 7.147.14
Outcome at 30 days(%)Outcome at 30 days(%)
MRSS 0-1MRSS 0-1 3535 53.5753.57
MRSS 0-2MRSS 0-2 4343 39.2839.28
Mortality rateMortality rate 1313 2.342.34

STROKE packageSTROKE package
Costs about Rs. 8 – 17000/- for investigations.Costs about Rs. 8 – 17000/- for investigations. The cost of 50 mg of r-TPA is around The cost of 50 mg of r-TPA is around
Rs.44,000/-( 0.9 mg/Kg. Body wt.).Rs.44,000/-( 0.9 mg/Kg. Body wt.). The cost for stay in the Hospital for 1 week will The cost for stay in the Hospital for 1 week will
depend on the type of room and will be around depend on the type of room and will be around Rs. 5,000 to Rs.20,000.Rs. 5,000 to Rs.20,000.