growth and development of cranial base
DESCRIPTION
summary of growth and development of cranial baseTRANSCRIPT

Puneet JainMDS 1st YEAR

Reasonably stable reference structure in cephalometric analysis
Basis to compare and understand abnormal growth patterns

Supports & protects the brain & spinal cord
Articulation of skull with vertebral column & mandible
Buffer zone between the brain, face & pharyngeal region

ANTERIOR CRANIAL FOSSA
MIDDLE CRANIAL FOSSA
POSTERIOR CRANIAL FOSSA

Cribriform plate of ethmoid
Orbital part of frontal bone
Anterior part of the body of sphenoid & lesser wing

1. THE SPHENOID BONE Anterior part of the upper surface of its
body is termed the JUGUM SPHENOIDALE

It separates the orbit and its contents from the
inferior surface of the frontal lobe of the brain
Its antero-medial part splits into 2 laminae :
FRONTAL SINUS

It is deeper than the anterior fossa
It shaped like a butterfly. In front it is bounded by posterior borders of the lesser wing of sphenoid
and the body of the sphenoid
Behind by superior borders of the temporal bones & Dorsum sellae of sphenoid bone


Centrally Optic Canal Hypophyseal Fossa
Laterally Superior Orbital Fissure Foramen Rotundum Foramen Ovale Foramen Spinosum Foramen Lacerum
MIDDLE CRANIAL FOSSA

Largest and deepest of the cranial fossa

FORAMEN MAGNUM JUGULAR FORAMINA INTERNAL ACOUSTIC MEATUS FACIAL CANAL HYPOGLOSSAL CANAL
POSTERIOR CRANIAL FOSSA

First three weeks of human development – The Pre-Embryonic period (three germ
layers).

Neuro-ectoderm forms the neural tube (eventually becoming the brain and spinal cord) & neural crest.
Neural crest cells are migratory and begin leaving the neural crest at about Week 5

As the development of the head progresses, neural crest cells and lateral plate mesoderm both migrate into rapidly forming pharyngeal arches, a series of bump-like structures on both sides of the embryonic head


Neural crest cells produce the bones of the cranial vault (neurocranium)
Within the pharyngeal arches, neural crest cells and lateral plate mesoderm give rise to bones of the jaw and lower face, the (viscerocranium)

NEURO / VISCERO / BASI CRANIUM

Earliest evidence of cartilage formation of cranial base is seen in the late somite period i.e. 4th week of intrauterine life.
Ectomeningeal capsule - Earliest evidence of
skull formation

Occipital sclerotomal mesenchyme concentrates around the notochord
Extends cephalically
Forms the floor of the brain
40th day of I. U. life mesenchyme starts converting into cartilage

PARACHORDAL CARTILAGE
HYPOPHYSEAL CARTILAGE
OTIC CAPSULE
NASAL CAPSULE


Chondrification centers forming around the cranial end of the notochord
Parachordal cartilages fuse with the
sclerotomes arising from occipital somites
surrounding the neural tube


Cranial to the oro-pharangeal membrane the hypophyseal pouch (Rathke’s pouch) arises from the stomodeum.
This pouch gives rise to the anterior lobe of pituitary gland (Adenohypophysis).

2 Hypophyseal cartilages - Post / Pasi sphenoid
* Sella turcica * Posterior part of body of sphenoid
`

Cranial to the pituitary gland fusion – 2 presphenoid or trabecular cartilages
Anterior part of the body of the sphenoid bone.
`

Orbitosphenoid (Lesser wing)
Alisphenoid (Greater wing)
Most anteriorly- presphenoid cartilage – Mesethmoid
Ossifies into perpendicular plate of ethmoid
Upper edge forms crista galli
This cartilage ossifies at birth


OTIC CAPSULE + PARACHORDAL CARTILAGES
Mastoid and petrous portions of the temporal bones
`
Otic capsule does not chondrify in humans

Nasal capsule chondrify in the 2nd month of I.U. life to form a box of cartilage with a roof and lateral walls divided by a median cartilage septum.
Chondrified nasal capsules form the cartilages of the nostrils and the nasal septal cartilage

Median nasal septum remains cartilaginous except posteroinferiorly
On each side of the septum intramembraneous ossification centers forms the Vomer bone

Nasal septal cartilage serves the following functions:
A. It acts as a functional matrix in the downward and forward growth of the midface
B. It helps in transferring compressive forces from incisor region to the sphenoid bone

During the 4th month in utero there is an ingrowth of vascular elements into the various points of chondrocranium.
These areas become centers of ossification, at which cartilage is transformed into bone

Various foramina Related nerves and vessels
Perforations in the cribriform plate of ethmoid bone.
Fibres of Olfactory nerve (I)
Optic foramen (Formed by extensions of orbitosphenoid cartilage fuses with cranial part of basal plate)
Optic nerve (II) and ophthalmic artery.
Superior orbital fissure (space between the orbitosphenoid and alisphenoid cartilages)
Occulomotor (III)
Trochlear (IV)
Ophthalmic (V)
Abduceus (VI) and
Ophthalmic veins.

Various foramina Related nerves and vessels
Foramen rotundum Maxillary nerve (V2)
Foramen ovale Mandibular nerve (V3)
Foramen spindosum (Junction between the alisphenoid, presphenoid cartilages)
Middle meningeal artery
Foramen lacerum (At the junction of alisphenoid and postsphenoid cartilages and otic capsule)
Internal carotid artery

Various foramina Related nerves and vessels
Internal acoustic meatus (Nerves passes through otic capsule)
Facial (VII)
Vestibulocochlear (VIII)
Jugular foramen
(Passage of nerves and vessels
between the otic capsule and
the parachordal cartilage)
Glossopharyngeal (IX)
Vagus (X)
Spinal accessory (XI)
Internal jugular vein
Hypoglossal / anterior condylar canal (Nerve passing between the occipital sclerotomes)
Hypoglossal nerve (XII)

110 ossification centers appear in the embryonic human skull
45 bones in the neonatal skull
Young adult 22 skull bones

UNOSSIFIED CHONDROCRANIAL REMNANTS –
Alae & septum of the nose Spheno-occpital & spheno-petrous junctions The apex of the petrous bone Between the separate parts of the occipital
bone

OCCIPITAL BONE :
Derived from Basicranial cartilage, contributed by the occipital sclerotomes and the desmocranial membrane
7 centres - 2 Intramembranous 5 Endochondral

Supranuchal Squamous portion – 2 Intramembranous centres ( 8 th
week)
Infranuchal squamous portion – 2 Endochondral centres (10 th
week)
Kerckring centre

Basioccipital bone - Anterior to the foramen magnum and the anterior
1/3rd
of the occipital condyles.
Median Basicranial Endochondral ossification center - 11th week

Exoccipital bones (lateral to the foramen magnum, including posterior 2/3rd of the occipital condyles)
Pair of Endochondral ossification centers - 12th week form the,.
The Occipital Squame starts to fuse with the Exoccipital at the Posterior Intraoccipital Synchondrosis during 2nd or 3rd year postnatally.
The Exoccipital join the Basioccipital at the Anterior Intraoccipital Synchondroses and it disappears during the 3rd or 4th year
By the age of 7, the squamous, exoccipital and basilar portions have united into a single occipital bone

TEMPORAL BONE :
Squamous and Tympanic components of this bone ossify in membrane
Petrosal and Styloid elements ossify
endochondrally
21 ossification centers

Squamous portion - 1 intramembranous centre
(8 th week) Zygomatic process
Tympanic ring - 4 intramembranous centres (3 th month)

Petrosal part – 14 endochondral centres (16th week) Fusion occurs by 6th month IU
Styloid process – 2 endochochondral centres from
hyoid arch (at birth)

22 weeks of I.U. - Petrous & Tympanic ring fuse incompletely, leaving the Petrotympanic fissure
Petrous, Squamous & Styloid process - fuse
during the 1st year of life
The Mandibular (Glenoid) fossa is only a shallow depression at birth, deepening with development of articular eminance

ETHMOID BONE :
Endochondral bone
Forms the median floor of the anterior cranial fossa
Forms parts of the roof, lateral walls & median septum of the nasal cavity
Ossified from 3 centres

Single median center in the Mesethmoid cartilage forms the perpendicular plate and cristagalli just before birth.
A pair of centers for the lateral labyrinths appears in the nasal capsular cartilages at the 4th month I.U.

INFERIOR NASAL CONCHA :
Endochondral bone ossification
Single center
Appears in the 5th month I.U.

SPHENOID BONE :
19 Intramembranous & Endochondral ossification centers
Central body (Basisphenoid) have both Cartilaginous and Intramembranous ossification centers derived from Pre & Post sphenoid centers

A single median and 2 paired Presphenoid ossification centers (4th month I.U.) in the mesethmoid portion of basicranial cartilage
The Postsphenoid bone arising from 2 sets of paired centers in the basisphenoid cartilage on either side of the unpwardly projecting hypophyseal pouch (Rathke’s) during the 4th month I.U.

Endochondral ossification centers for the greater wings of the sphenoid appear in the alisphenoid cartilages and for the lesser wings in the orbitosphenoid cartilages.
Intramembranous ossification centers appear in the 8th week for some parts of greater wings and for the medial and lateral pterygoid plates

Intramembranous ossification centres
Medial pterygoid plates – 2 Lateral pterygoid plates -2
Endochondral ossification centres
Presphenoid – 3 Postsphenoid – 4 Orbitosphenoids - 2 Alisphenoids - 2 Pterygoid hamuli - 2

VOMER :2 Intramembranous centres

BONE - SITE & NUMBER OF OSSIFICATION INTRAMEMBRANOUS ENDOCHONDRAL
OCCIPITAL _ Supranuchal Infranuchal squamous (2)
squamous (2) Basilar (1) Exoccipital
(2)
TEMPORAL _ Squamous (1) Petrosal (14) Tympanic (4) Styloid (2)
ETHMOID _ Lateral labrynths (2)
Perpendicular plate Crista(1)

BONE - SITE & NUMBER OF OSSIFICATION INTRAMEMBRANOUS ENDOCHONDRAL VOMER _ Alae (2)
SPHENOID _ Medial pterygoid Presphenoid (3) plates (2) Postsphenoid (4) Lateral pterygoid Orbitosphenoid (2) plates (2) Alisphenoids (2) Pterygoid hamulus
(2) Sphenoidal conchae
(2)
INFERIOR NASAL CONCHA _ Lamina (1)
The central region of the cranial base is composed of prechordal and chordal parts which meet at an angle at the hypophyseal fossa (sella turcia).

Between 8-10 weeks as the whole head is raised by extension of the neck,
lifting the face from the thorax).

Growth of the cranial base - highly uneven
Anterior cranial base increases its length and width by 7 folds between the 10th and 40thweek of I.U life
Posterior cranial base grows only 5 fold

Cephalic index is the ratio of the maximum width of the head to its maximum length.
Sometimes used for estimating the age of fetuses for legal and obstetrical reasons, in which case the differences in skull shapes between different populations are still of interest

The cephalic index was defined by Swedish professor of anatomy Anders Retzius (1796-1860) and first used in physical anthropology to classify ancient human remains found in Europe.
Martin & Saller (1957) substantiated the use of cephalic index

The measured factors are defined as the maximum width of the bones that surround the head, above the supramastoid crest (behind the cheekbones), and the maximum length from the most easily noticed part of the glabella (between the eyebrows) to the most easily noticed point on the back part of the head.

Females Males Scientific term Meaning Alternative term
< 75% < 65% dolichocephalic 'long-headed' mesocranial
75% to 80% 65% to 75% mesocephalic 'medium-headed' mesaticephalic
> 80% > 75% (male) brachycephalic 'short-headed' brachycranial

PROSENCEPHALY…………….?????????
Growth and development though closely related are not synonymous.
In simple English growth refers to a process of change where as development as a process of increasing degree of organization.
Growth refers to an increase in size and number whereas development refers to increase in complexity.
Growth is an anatomic phenomenon where as development is an physiologic and behaviourial phenomenon.

Definitions:
Change in any morphological parameter that is measureable.
“by Moss”
The self multipication of living substance. “by Huxely”
Increase in size and change in proportion and progressive complexity.
“by Krogman”

An increase in size. “by Todd”
Entire series of anatomic and physiologic changes taking place from the beginning of prenatal life to senility.
“by Meridth”
The naturally occurring unidirectional changes in the life of and individual from its existence as single cell to its elaboration as a multifunctional unit terminating to death.
“by Moyer’s” Progress towards maturity. “by Todd”
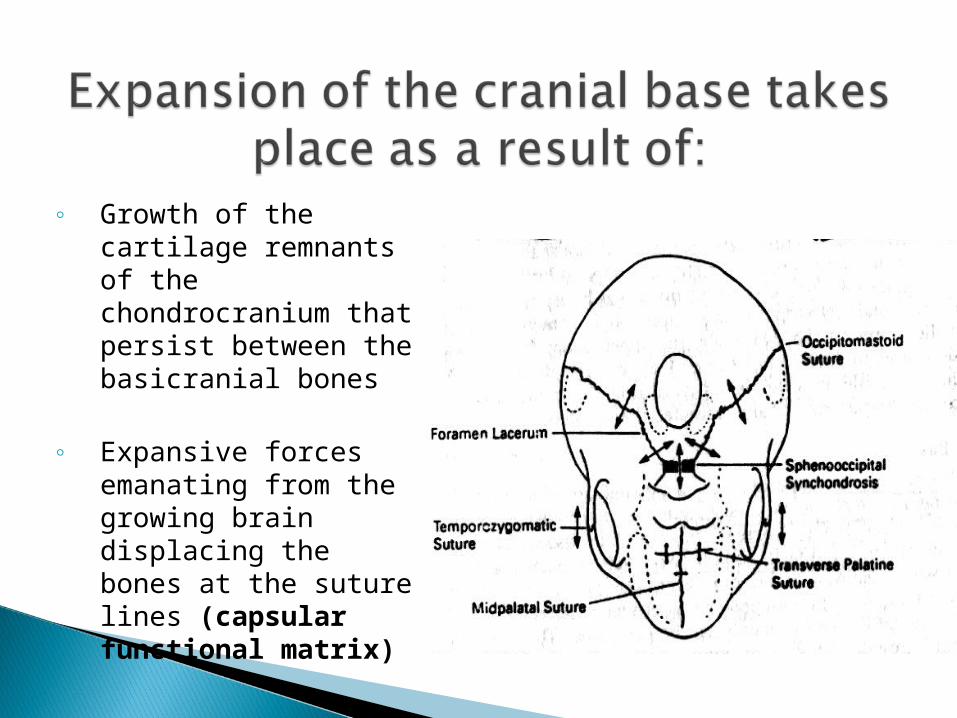
◦ Growth of the cartilage remnants of the chondrocranium that persist between the basicranial bones
◦ Expansive forces emanating from the growing brain displacing the bones at the suture lines (capsular functional matrix)

Cranial base acts as a template from which the face develops
The endocranial surface of the basicranium is resorptive in most areas
Remodeling is required to accommodate the massively enlarged human brain

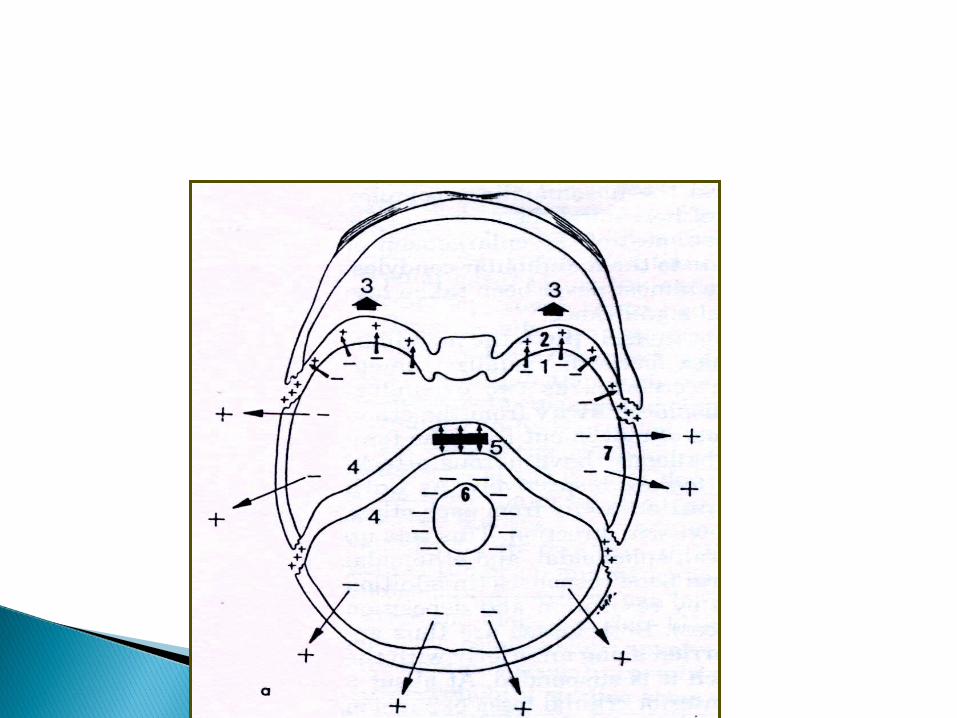
Key remodeling process
Provides for the direct expansion of the various endocranial fossae in conjunction with sutural growth and growth at synchondrosis

• Middle & Posterior fossae – petrous elevation
• Olfactory fossae – crista galli
• Right & Left middle fossae – Sphenoidal elevation
• Right & left anterior & posterior fossae – Longitudinal midline bony ridge

Fossa expands outward by resorption Partitions between them enlarge inward by
deposition

Mid ventral segments of cranial floor grows more slowly than the floor of the laterally located fossae.
This accommodates the slower development of the medulla, pons, hypothalamus, optic chiasma in contrast to the massive rapid expansion of the hemispheres

Foramen Drift process (Re-
location)
Spinal Cord Differential re-modelling

Bands of cartilage at the junction of various bones.
Bony union brought about by cartilage interstitial growth.
The cartilages between bones in the ventral midline.
Contribute to growth of the cranial base in elongation and lateral expansion.

Retention left from the primary cartilages of the chondrocranium after
the endocranial ossification centers appear during fetal development

Fronto-ethmoidal synchondrosis
Spheno-ethmoidal synchondrosis
Inter-sphenoidal
Spheno-occipital.

Fronto-ethmoidal & Spheno-ethmoidal synchondrosis ceases contributing to the antero-posterior elongation after the age 7 years.
Further growth of anterior cranial base is associated with expansion of the developing frontal air sinuses

Spheno-occipital synchondrosis (major contributor)
Last of all synchondrosis to fuse
Starts fusing at 12-13 years in girls, & 14-15 years in boys and completing ossification by 20 years of age.
This prolonged growth period allows for
continued posterior expansion of the maxilla to accommodate last erupting molar teeth and provides space for growing nasopharynx.
All growth cartilages are associated with (directly) bone development, the SOS
provides a pressure adapted bone growth mechanism
(provides for the elongation of the midline portion of the cranial floor)
The lateral suture areas shows tension adapted mechanism

Because cranial base supports the mass of the brain and face SOS in the midline is subjected to cervical and masticatory
muscle forces
Endochondral ossification is pressure adapted mechanism &
Intramembranous bone growth is tension adapted

Familiar reserve zone
Cell division zone
Hypertrophic zone
Calcified zone.

Bipolar direction of growth
2 epiphyseal plates positioned back to back and separated by a common
zone of reserve cartilage

The resorption occurs from the lining side of the forward walls of the middle cranial fossa.
Deposition on the orbital face of the sphenoid and in the sphenofrontal suture.
Forward displacement of the anterior cranial fossae as the frontal lobes are displaced anteriorly.
The petrous elevation increases by deposition on the endocranial surface.
Lengthening of clivus occurs by growth at SOS.
The foramen magnum is progressively lower by resorption on the endocranial surface and deposition on the ectocranial side.
Endocranial fossa enlarge by a combination of endocranial resorption and ectocranial deposition.

Sphenoid and the occipital bones become moved apart by the Primary displacement process
Post border of N-Mcomplex coincides with
boundary between ant and middle cranial fossa
Secondary displacement effect (Anterior cranial floor , nasomaxillary complex
& mandible)

Frontal lobe growth completes by 5years.
Temporal lobes continue to enlarge for several more years and displaces the frontal lobe forward.

In this study growth and development of the cranial bone in children who were treated orthodontically were compared with children who were not.
Mixed longitudinal study of 153 boys and 167 girl samples, 7-14 years of age.

No significant differences could be demonstrated between children with or without treatment.
Cranial base displayed sexual dimorphism in absolute size, timing and amount of growth.
All C.B. dimensions examined in this study were greater in boys than in girls

Anencephaly – Absence of calvaria
Characterized by :
A short, narrow chondrocranium in many cases with notochordal anomalies.
Patients retain the acute cranial base flexure typical of early fetuses.
Brain growth contributes to flattening of the cranial base.
Afflictions of cartilage growth produce a reduced cranial base with increased angulation which is seen in conditions like Achondroplasia, Cretinism and Down’s syndrome (Trisomy 21)

Disturbance in endochondral bone formation
Deficient growth at the synchondrosis
Maxilla is not translated forward This results in abnormal depression of the
bridge of the nose Relative midface deficiency


Premature ossification / Synostosis of the suture between the presphenoid and post sphenoid parts and of the sphenooccipital suture.
Consists of an abnormal depression of the bridge of the nose.

Anomalous development of the Presphenoidal elements may lead to an excessive separation between the orbit and abnormally broad nasal bridge.

Coalescence of the ossification centers in the body of sphenoid obliterates the orohypopharyngeal track.
Persistence of the track as a craniopharyngeal canal in the sphenoid body gives rise to craniopharyngeal tumours.

INADEQUATE GROWTH OF CHONDROCRANIUM
Impacted eruption of third molars
CLIEDOCRANIAL DISOSTOSIS
Abnormalities of the skull, teeth, jaws and shoulder girdle

Skull frontanelles remain open or atleast exhibit delayed closing.
Frontal, parietal and occipital bones are prominent
The paranasal sinuses are undeveloped and narrow.

Keriborg Bjork and Skieller conducted a qualitative screening for abnormal morphological traits in the cranial base.
(AJO May 1981)
The sample comprised seventeen patients with CCD (8 males and 9 females):

The anterior and posterior cranial base was significantly shorter and the C.B. angle smaller in the syndrome groups than in the control groups.
Clivus distorted.
All patients showed small pituitary fossae and bulbous dorsum sellae.
The amount of bone resorption was lesser than normal, so abnormalities in remodeling pattern is seen.

The configuration of the neurocranium (and brain) determines a person’s headform type.
A long and narrow basicranium (Dolicocephalic)
A rounder basicranium (Brachycephalic)

Basicranium, is the template that establishes the shape and perimeter of
the facial growth field

Craniosynostosis, the premature fusion of calvarial sutures, is a common developmental anomaly that causes abnormal skull shape.
The locus for one autosomal dominant form of craniosynostosis has been mapped to chromosome 5

Roberts phocomelia syndrome (RS) is an autosomal recessive disorder of symmetric limb defects, craniofacial abnormalities, pre- and postnatal growth retardation, and mental retardation.
Craniofacial abnormalities of this case were typical; he showed mild hypertelorism, mandibular hypoplasia, dysplastic helix of ear, narrowing of external auditory canal, and cleft palate with wide gap.

Primary abnormality in Crouzon syndrome appears to be premature fusion of sutures and synchondroses.
Very early release of the coronal suture areas with advancement of the frontal bone is advocated in this syndromes

Craniofacial Embryology -G.H.SPERBER
Essencials Of Facial Growth -D.H.ENLOW
Contemporary orthodontics W.R.PROFFIT
Anatomy –Gray
Human Embryology – Inderbir Singh
Grants Atlas
Abnormalities Of Cleidocranial Disostosis – Kreiborg,bjork& Skeiller (Ajo May; 1981 )
Cranial Base Growth For Dutch Boys & Girls – M.Herneberke,b.P. Andersen (Ajo November; 1994 )
Various Links