gastrointestinal disorders. introduction the gastrointestinal (g.i.) tract comprises the oral...
TRANSCRIPT
Gastrointestinal disorders
Introduction
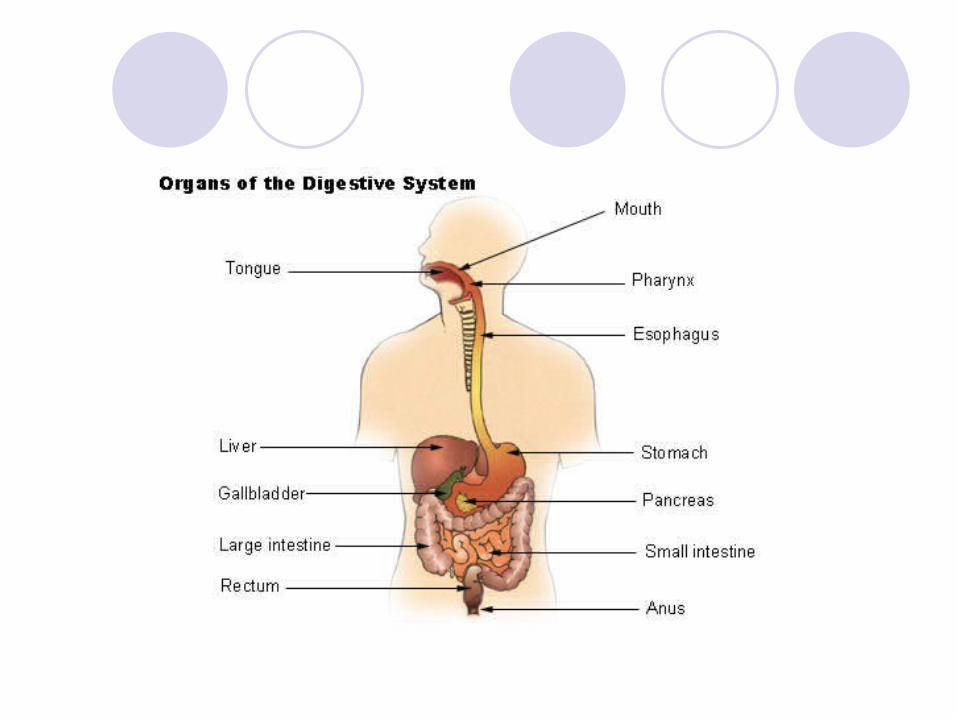
The gastrointestinal (G.I.) tract comprises the oral cavity, esophagus, stomach, small intestine (duodenum, jejunum, ileum) and large intestine (colon and rectum).
Accessory organs such as the pancreas, liver and gallbladder play an important role in the digestive process.
The process of digestion begins in the mouth with the mechanical grinding of food by the teeth.
Saliva produced by the salivary glands lubricates the food and contains amylase enzymes that begin the digestion of starches.
The chewed food or chyme now passes down the esophagus and enters the stomach. In the stomach, the chyme is further broken down by highly acidic gastric juice produced by the stomach lining.
The enzyme pepsin is released by cells in the stomach lining to begin digestion of proteins.
Muscular contractions of the stomach wall also serve to further grind the chyme into a smooth liquid. The chyme is now driven into the small intestine by contraction of the stomach.
In the small intestine, further digestion of proteins, sugars will occur via intestinal and pancreatic enzymes.
The small intestine is also where the majority of nutrient absorption occurs.
By the time the remaining chyme has reached the large intestine, most of the available nutrients have been absorbed from it.
The large intestine functions mainly in the absorption of water as well as the synthesis of vitamin K and certain B vitamins.
General Symptoms of G.I. Disease
Anorexia — loss of appetiteNauseaVomitingDiarrhea, constipationBleeding
Abnormalities of the esophagus
DysphagiaDifficulty swallowing that may be caused by obstruction
of the esophagus or impaired motility of the esophageal walls.
Obstruction may be caused by tumors, congenital narrowing .....etc
Neurologic disorders such as brain injury, stroke may affect voluntary swallowing or peristalsis of the esophagus.
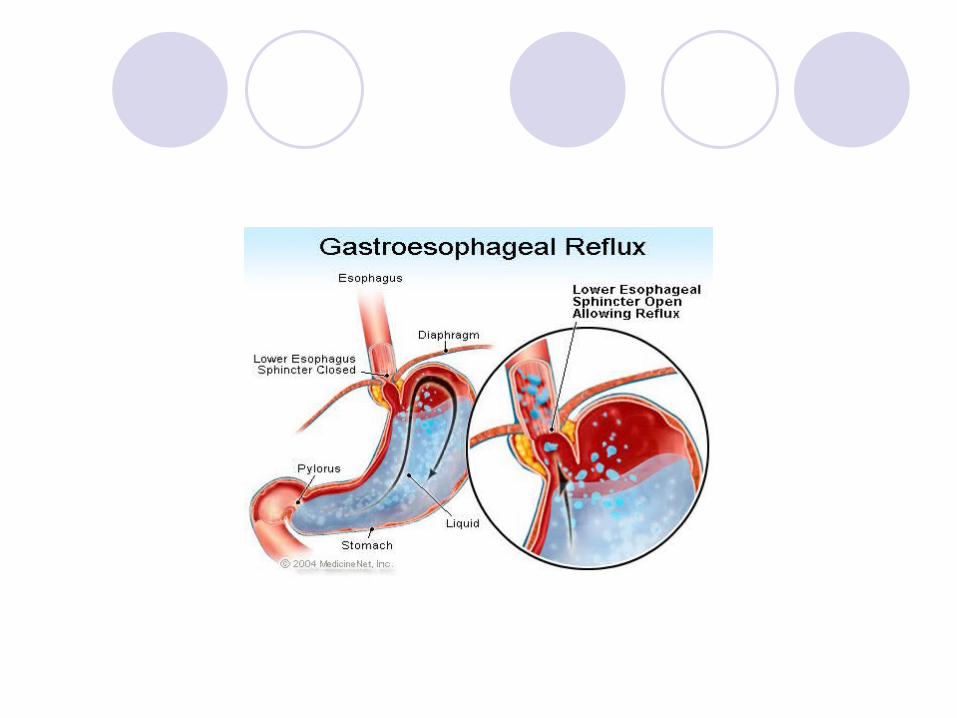
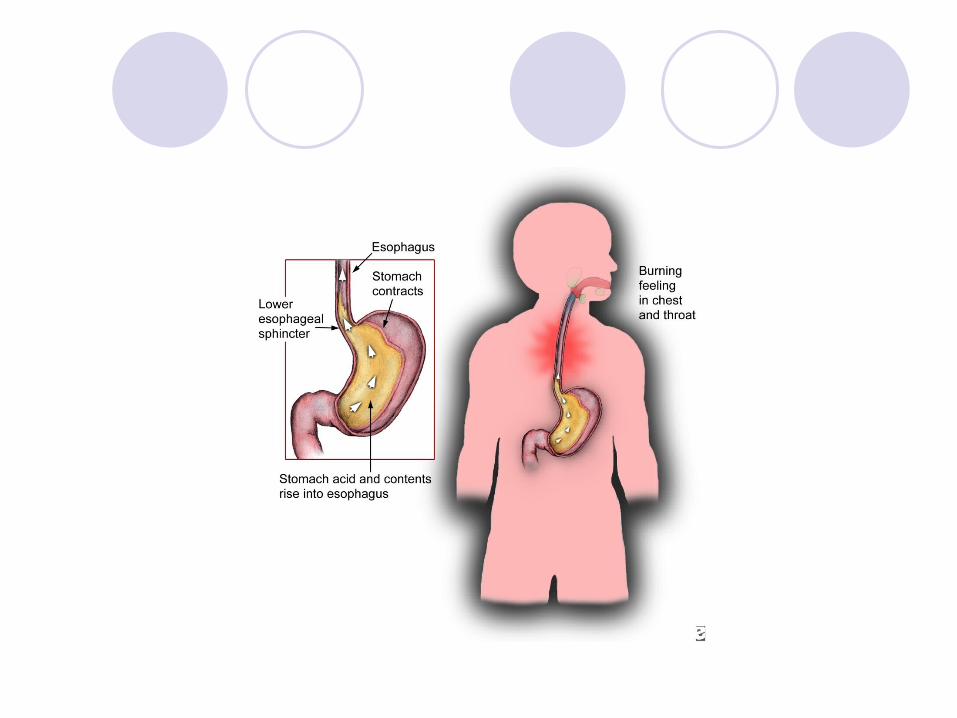
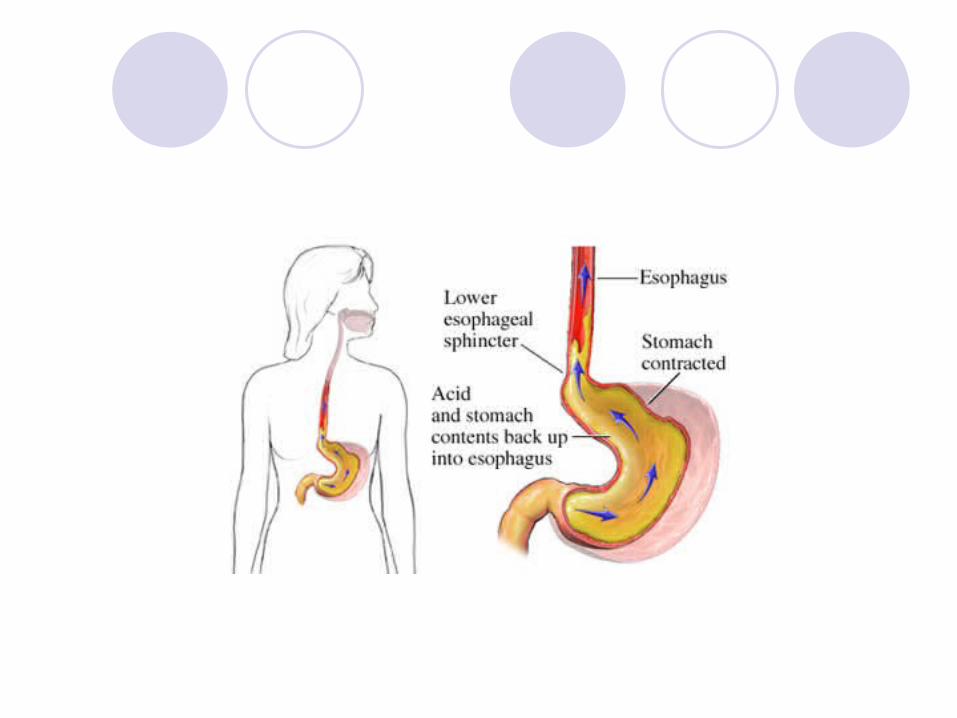
Gastroesophageal reflux diseaseGastroesophageal reflux is a condition caused by
the backflow of stomach contents into the esophagus.
It results from weakness or incompetence of the lower esophageal sphincter that normally blocks reflux of stomach contents into the esophagus.
Because of their high acid content (low pH), reflux of stomach contents will cause irritation and inflammation of the esophagus (esophagitis) that can lead to ulceration of the esophagus.
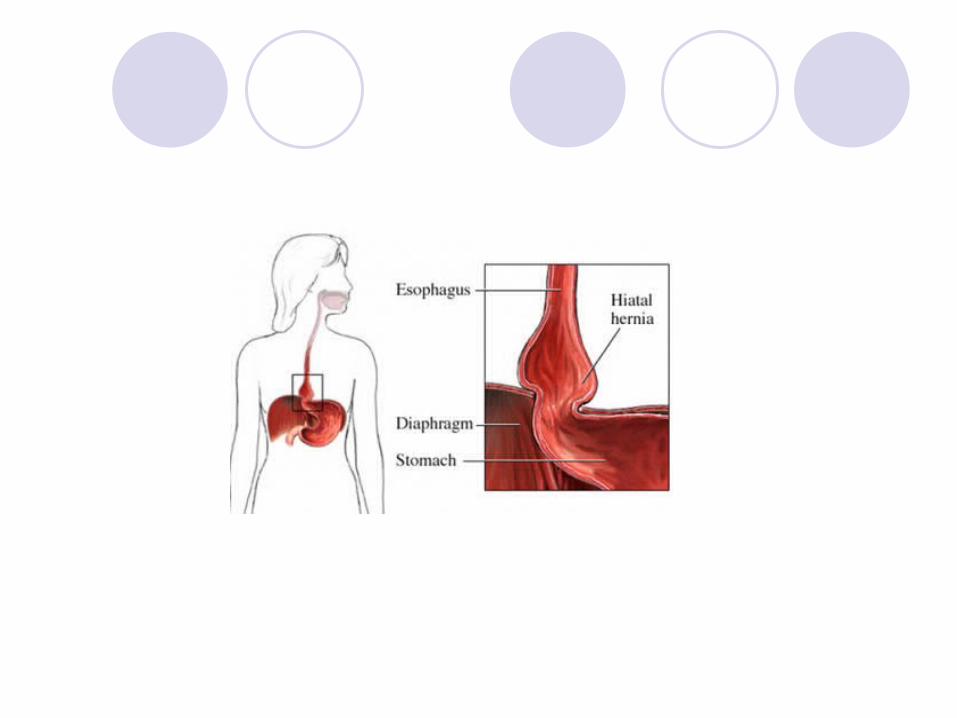
A hiatal hernia may also cause gastroesophageal reflux. A hiatal hernia is a protrusion of the top of the stomach through the opening of the diaphragm.
Manifestations
Burning pain in the epigastric region (“heartburn”) that may be worsened by alcohol consumption, caffeine, smoking, exercise and obesity.
Reflux may also be worsened by lying down.
Esophagitis, possible ulceration of esophagus.
Dysphagia, poor nutrition.
Possible increased risk of esophageal cancer with chronic esophagitis.
Treatment
Consumption of frequent small meals rather than large ones.
Sleeping with head elevated.Consumption of fluids with meals to wash food out of the
esophagus.Use of antacids or proton pump inhibitors to reduce pH
of stomach contents.Surgery if a hiatal hernia is present.
Disorders of the stomach
GastritisGastritis refers to inflammation of the gastric mucosa
(stomach lining). It may present as an acute or chronic disorder.
Acute gastritisTransient irritation and inflammation of the stomach
lining.May be caused by factors such as alcohol consumption,
aspirin use and stress.The inflammation associated with acute gastritis is a self-
limiting process that does not usually result in long-term injury to the gastric mucosa.
Chronic gastritisChronic irritation and inflammation of the stomach lining.
May be caused by bacterial infection, alcohol abuse or long-term aspirin and nonsteroidal anti-inflammatory drug (NSAID) use.
Can lead to atrophy and ulceration of the gastric mucosa.
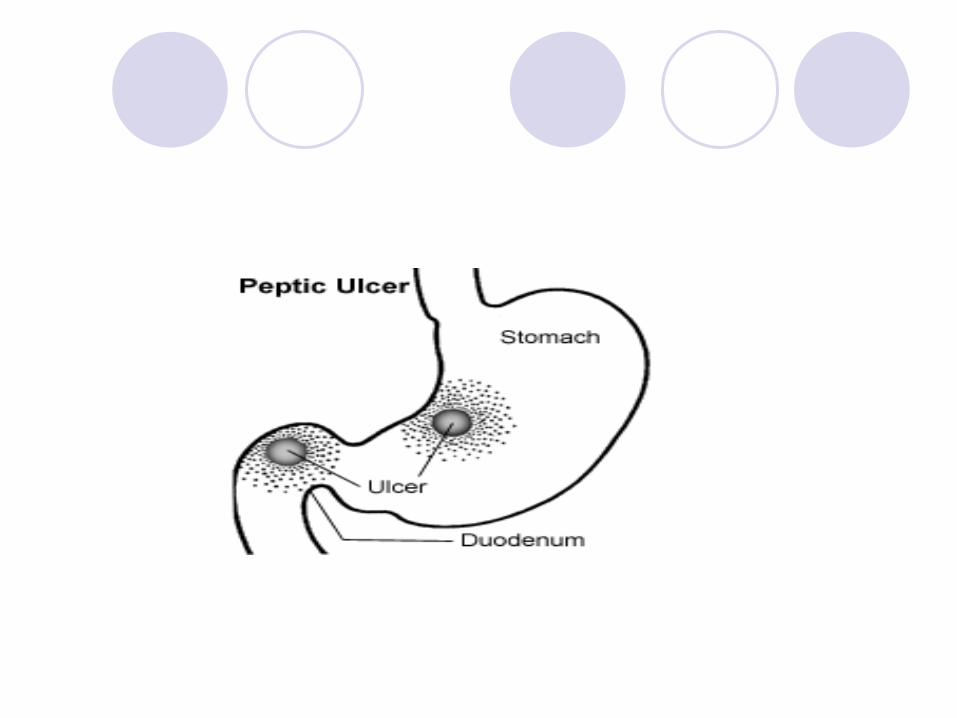
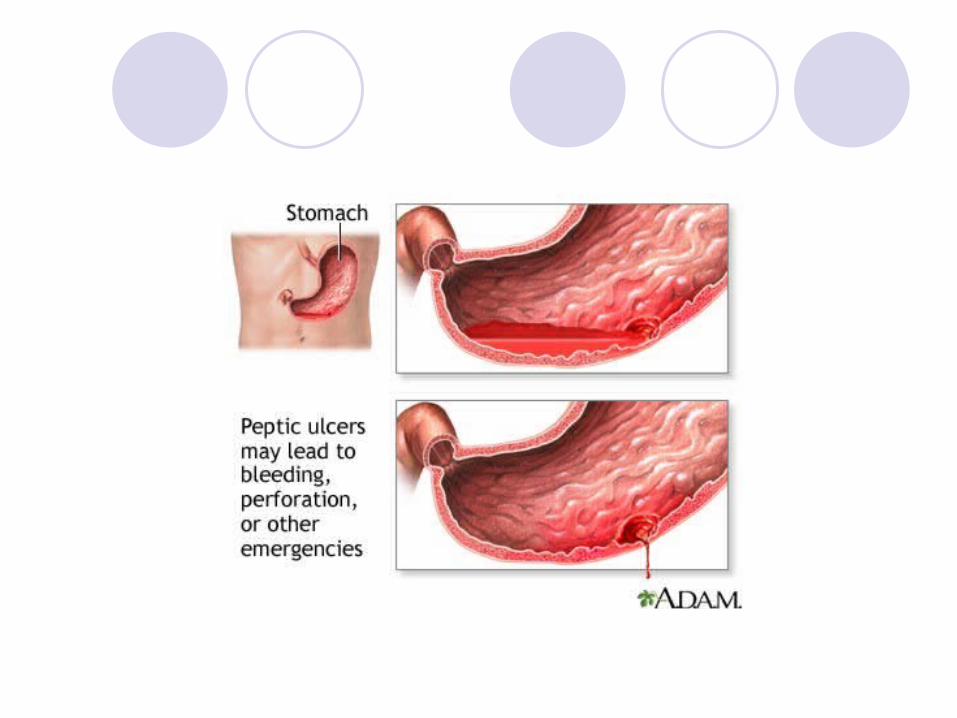
Peptic ulcersPeptic ulcer disease is a general term for ulcers that
occur in the stomach or duodenum (upper part of the small intestine).
If the ulcer occurs in the stomach lining, it is specifically referred to as a gastric ulcer.
In the United States most ulcers occur in the duodenum and in elderly patients.
Peptic ulcers that occur on the inside of the stomach are called gastric ulcers.
Peptic ulcers that occur inside the (esophagus) are called esophageal ulcers.
Peptic ulcers that affect the inside of the upper portion of small intestine (duodenum) are called duodenal ulcers.
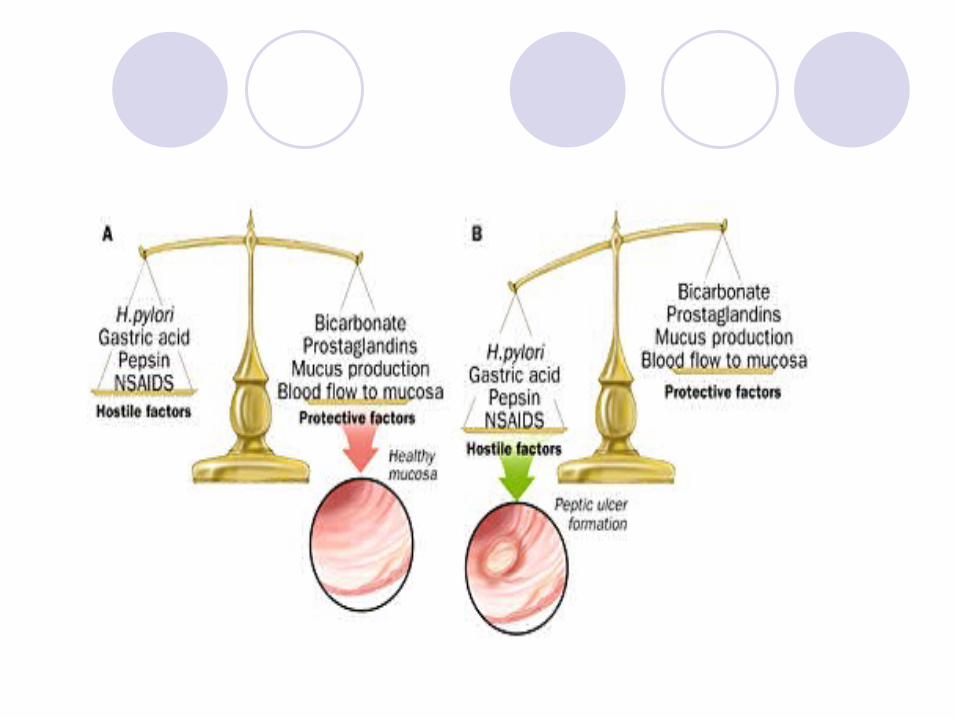
Pathogenesis of peptic ulcer
Peptic ulcers are produced by an imbalance between the
Protective Factors and Hostile Factors
The causes of peptic ulcer disease include the following: Infection with the bacteria Helicobacter pylori occurs in 80 to 95% of
patients with peptic ulcer disease.
Excess acid production from gastrinomas, tumors of the acid producing cells of the stomach that increases acid output .
Chronic use of aspirins and NSAIDs.
Manifestations of peptic ulcer disease
Episodes of remission and exacerbation
Pain
G.I. bleeding and possible hemorrhage (20 to 25% of patients)
Perforation of ulcers with significant mortality
Obstruction of G.I. tract
Treatment of peptic ulcer disease
Avoidance of alcohol, smoking and NSAIDs
Antibiotics for eradication of H. pylori if present
Antacids (Examples: magnesium hydroxide , aluminum hydroxide )
H 2 receptor antagonists (examples: Ranitidine ,Cimetidine )
Proton-pump inhibitors (example: Omeprazole)
Mucosal protective agents (examples: bismuth , sucralfate )
Disorders of the intestines
Disorders of the intestines
Irritable bowel syndromeMay be one of the most common G.I. disorders.
Patients present with symptoms of G.I. pain, gas, bloating and altered bowel function (diarrhea or constipation). Most symptoms are localized to the lower intestine and colon.
No underlying pathophysiologic processes have yet to be identified in these patients. “Hyperreactivity” and excessive motility of the bowels may be contributing factors.
Emotional factors and diet may exacerbate the symptoms.
Treatment may include psychological counseling, dietary changes such as increased fiber consumption. Antidiarrhea, anticholinergic and antispasmodic agents might also be of value.
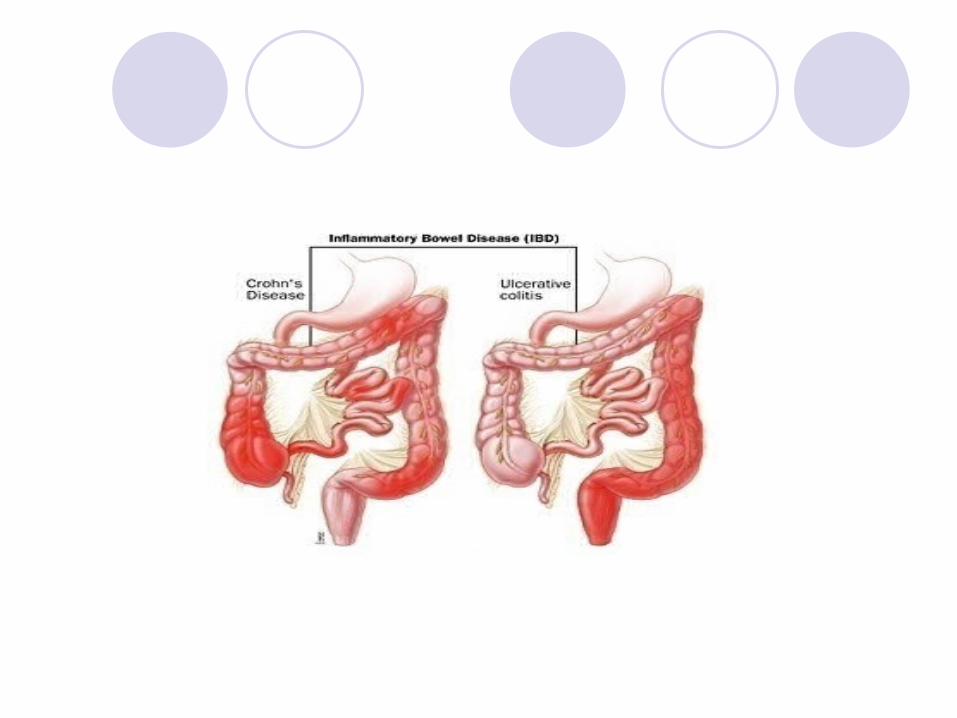
Inflammatory bowel disease
The term inflammatory bowel disease includes the conditions Crohn’s disease and ulcerative colitis . Both of these diseases are characterized by chronic inflammation of various regions of the G.I. tract
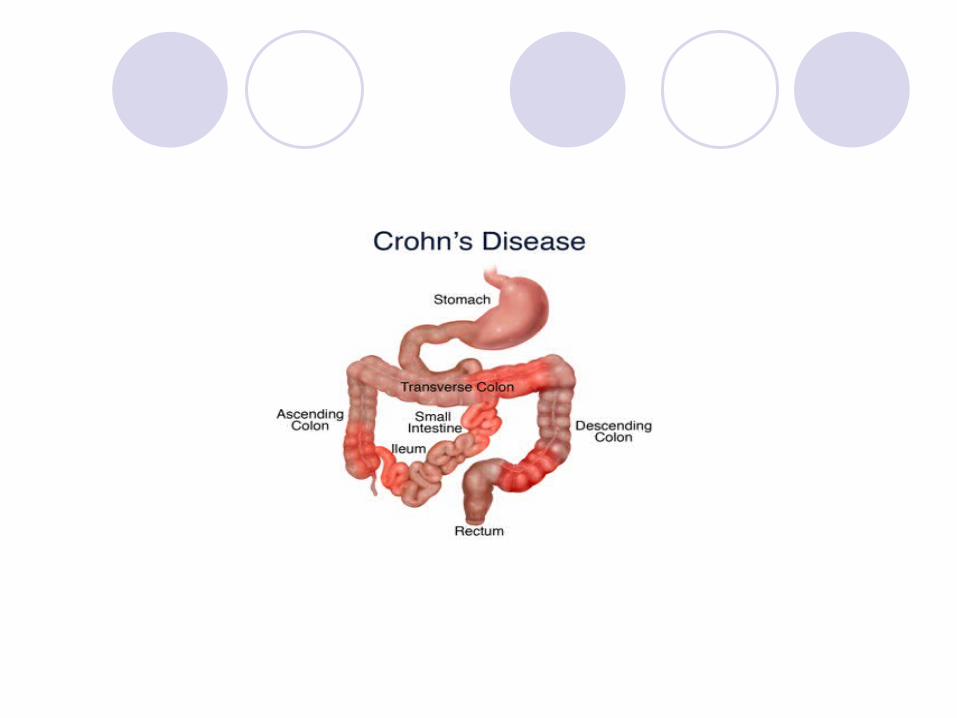
Crohn’s disease
Although the exact etiology of Crohn’s disease in unknown, there appears to be a significant autoimmune component. Much recent interest has focused on the possible role of pro-inflammatory cytokines in the pathogenesis of this disorder.
The disease may affect any region of the G.I. tract but is most commonly seen in the distal ileum and colon.
Distribution of Crohn’s disease shows a distinct predisposition to certain populations including Jews and individuals from the United States, Western Europe and Scandinavia.
The disease often presents in the late teens to early 20s and is present for the life of the patient with intermittent periods of remission and exacerbation.
The inflammation of Crohn’s disease is particularly evident in the submucosal layer of the intestine.
The inflammatory lesions are not constant along the length of the intestine but rather present with a “skip” pattern that disperses areas of inflammation with normal looking, non-inflamed tissue.
Manifestations of Crohn’s disease
Diarrhea (blood is usually not evident in the stool but may be occult, i.e., detected by clinical assay)
Intestinal pain similar to indigestion
Fever
Weight loss from intestinal malabsorption
Nausea, anorexia, vomiting
Complications: intestinal obstruction, formation of fistulas (abnormal connections between the colon and other abdominal organs)
Toxic megacolon
Toxic megacolonLife-threatening distention of the colon.May lead to perforation of the colon, septicemia and
peritonitis.Mortality associated with a perforated colon is on the
order of 40% or more.
Treatment of Crohn’s disease
Nutritional supplementation to offset the poor nutrition that can result from anorexia and intestinal malabsorption. Total parenteral nutrition may be indicated in severe cases.
Anti-inflammatory drugs.
Recently, considerable research has focused on the role of pro-inflammatory cytokines in Crohn’s disease and the possibility that drugs or antibodies that block cytokine action might be of benefit in treating the disease.
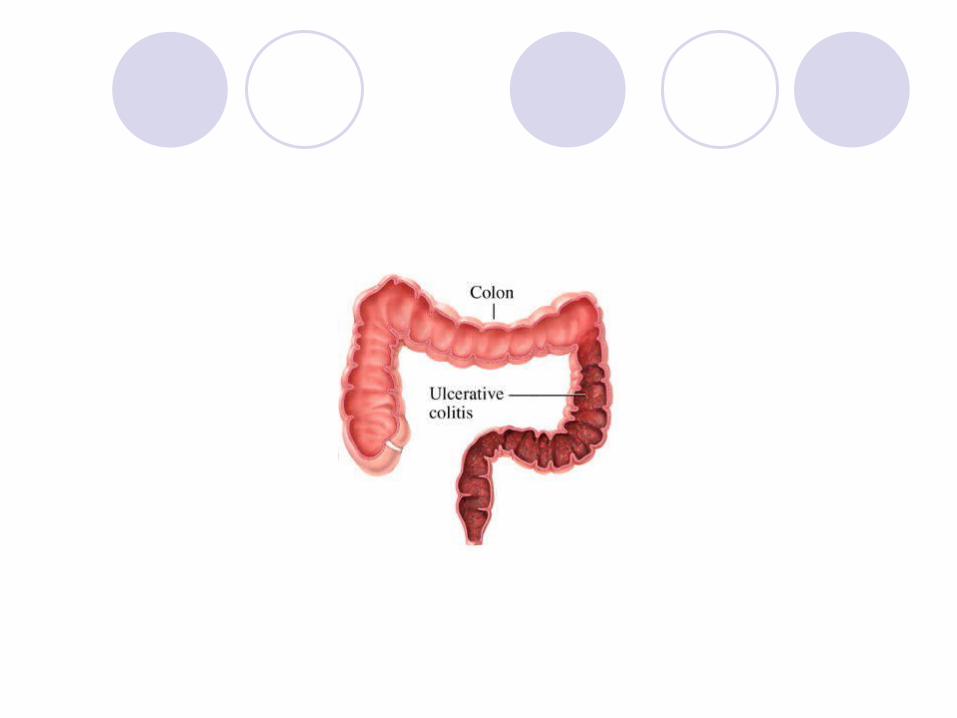
Ulcerative colitis
Inflammatory disease of the rectum and colon.The disease primarily affects the submucosa layer of the
intestines.Unlike Crohn’s disease the pattern of inflammation is
continuous throughout the affected area.Like Crohn’s disease, ulcerative colitis also presents with
periods of remission and exacerbation.
Although the exact etiology of ulcerative colitis is unknown, genetic and immunological factors are likely contributors to the disease.
Individuals between the ages of 20 and 40 are most susceptible, particularly those with a family history of the disorder or who are of Jewish descent.
Manifestations of ulcerative colitis
Chronic, bloody diarrheaFever, painWeight lossPossible anemia from blood lossPossible complications: toxic megacolon , perforation of
the intestine, significant blood loss; an increased incidence of colon cancer has also been documented in patients with ulcerative colitis
Treatment of ulcerative colitis
Anti-inflammatory drugs and salicylates suppress the inflammatory response.
Sulfasalazine
Nicotine appears to exert a protective effect in ulcerative colitis but not Crohn’s disease.
Severe malnutrition may require nutritional supplementation.
Surgical resection of diseased bowel may be required.
Disorders of the gall bladder
The gall bladder is a saclike structure that stores the bile that is produced by the liver.
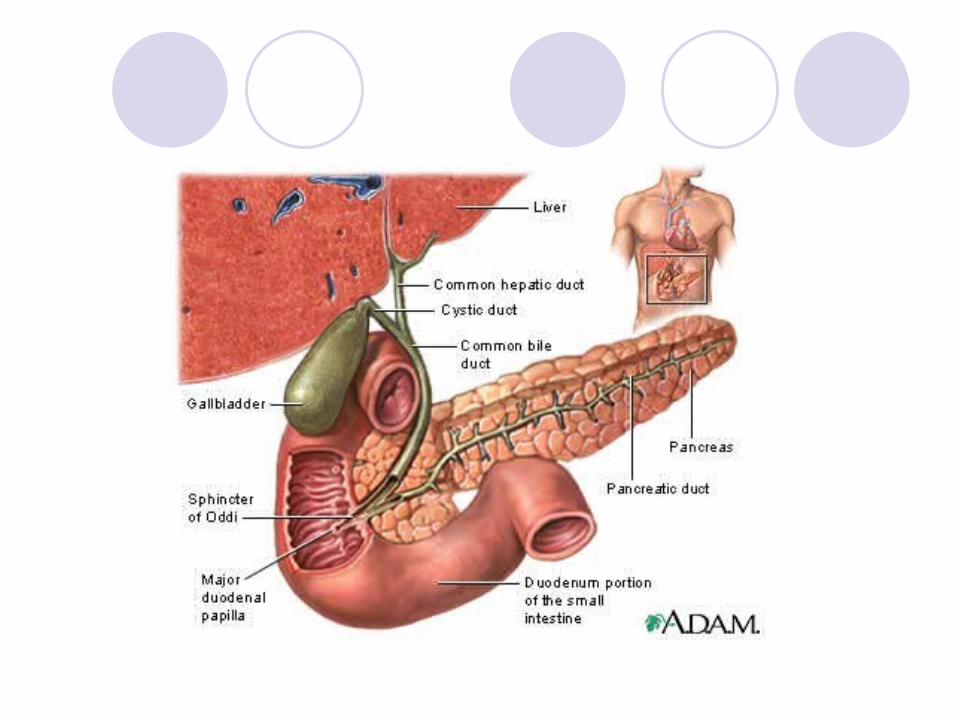
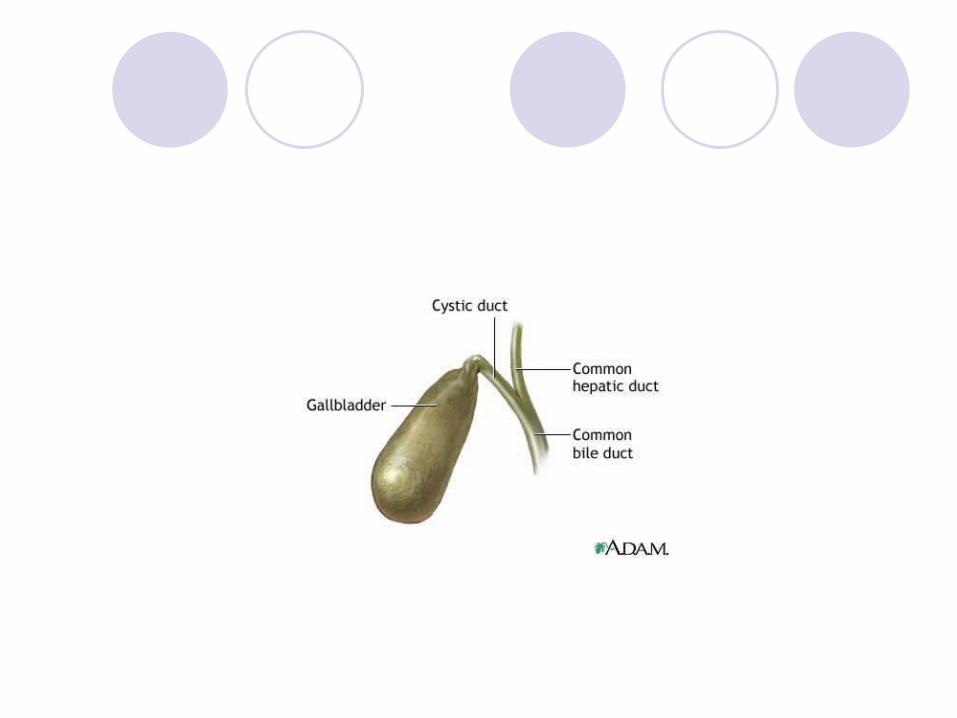
The walls of the gall bladder contain smooth muscle and, under the stimulus of the duodenal hormone cholecystokinin , can contract to eject bile down the bile duct and into the duodenum.
In the duodenum, bile salts emulsify fats to aid in their absorption. Bile is composed primarily of water, bile salts, cholesterol and bilirubin.
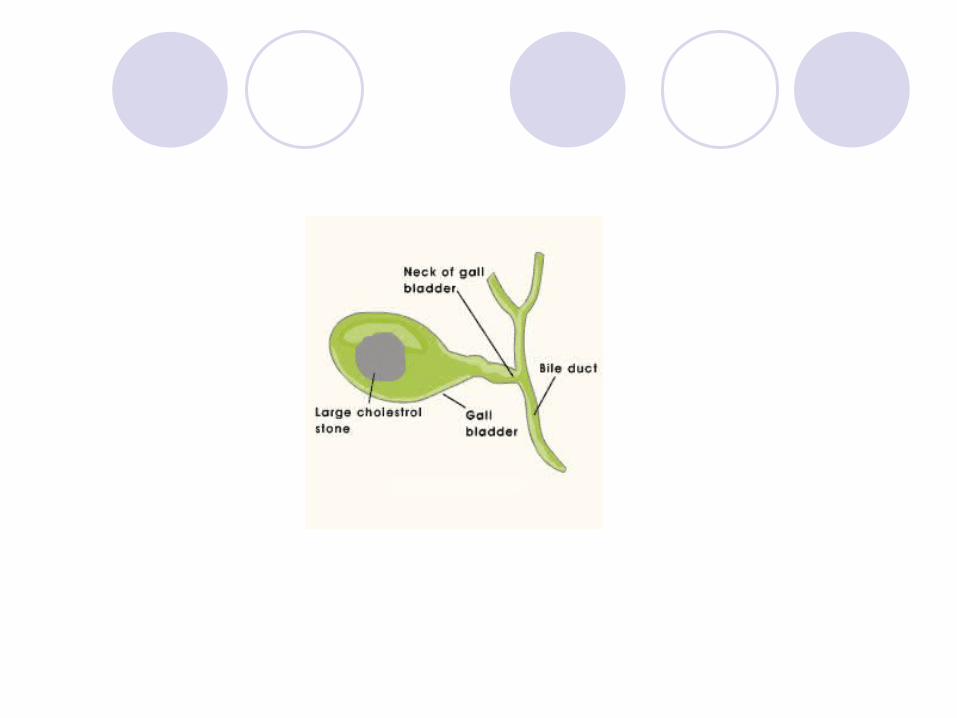
Gallstone formation (cholelithiasis)
The gallstones that form in the gall bladder are hardened precipitates of bile that contain predominantly cholesterol.
The size of gallstones can range from the size of a grain of sand to several inches in diameter.
Factors such as aging, excess cholesterol, obesity, sudden dietary changes or abnormal fat metabolism may contribute to gallstone formation.
Gallstones may be detected by a number of techniques including radiography, ultrasonography and cholecystoscopy.
Manifestations of gallstone formation
Symptoms of gallstone formation will generally not occur until the stones have reached sufficient size to block the bile ducts.
Acute and severe abdominal pain.
Nausea, vomiting, fever, chills.
Jaundice from obstruction of bile outflow.
Treatment
Surgical removal of gall bladder ( cholecystectomy )
Endoscopic removal of gallstones
Lithotripsy — The use of sound waves to break up the gallstones in the gall bladder
Low-fat diet for prevention of additional stone formation
Cholecystitis
Cholecystitis is an acute or chronic inflammation of the gall bladder.
It is most commonly caused by the presence of gallstones in the gall bladder, but may also result from infection or reduced blood flow to the gall bladder.
Signs and symptoms are similar to those observed with cholelithiasis.
Treatment involves removal of gallstones and antibiotics for treatment of infection if present.
Thank you