fusion and repeat discectomy following single … and repeat discectomy following single level open...
TRANSCRIPT
Fusion and repeat discectomy following single level open lumbar discectomies. Survival analysis
Dr John MortimerMr Chris Hoffman
CCDHB and TBI Health group
Sciatica = Leg Dominant Pain
• Patients referred for surgical review
• History of back and then leg-dominant pain
• Severe disability – unable to work and sleep
• Associated neurological disturbance
• Conservative care• Nortriptyline for sleep disturbance
• CT guided steroid injection
• NSAIDS/Opiates prn
• Physiotherapy
Failure of Resolution
• Indications for discectomy
• Leg dominant (CBI pattern 3) pain
• Positive tension signs – SLR to reproduce Leg Dominant Pain
• Concordant MRI scan – Disc prolapse at relevant level/side
• When should we operate?
• Must do - Cauda Equina Syndrome (rare)
• Should do - Progressive neurology (rare)
• Could do - Aim to reduce long term pain/disability
• Window of opportunity to intervene – 3 to 12 months

Surgical Goals
• Resolution of leg pain • Reduction in back pain• Preventing further disability
• Goal of surgery• Discectomy removes the displaced fragment• Removes the irritation/pressure on the relevant nerve
• Surgical technique• Cannot repair any nerve damage• Cannot repair the annular defect
• Problem of recurrent prolapse and/or chronic back pain• Conservative care initially• Repeat discectomy (fragment only)• Complete discectomy and spinal fusion
Aims and Methods
• To describe the rates of reoperation following single level lumbar discectomies by one surgeon between 2000-2016
• To describe the complication rates
• To describe the prevalence and association of patient factors and MRI reported disk disease on the incidence of repeat same level discectomy and lumbar fusions
Aims and Methods
• Inclusion
• Single level primary discectomy for MRI proven disk prolapse L1-S1
• No previous discectomy or fusion of any level
• Exclusion
• > one level discectomy
• Any previous spinal surgery
• Decompression for reasons other than HNP
• Any other combination of surgery fusion

Aims and Methods
• Single surgeon database 1998-2016 (Mana Orthopaedics)
• Private practice medical records
• MRI reports
• ACC coding
• ACC surgical request report - ARTP’s
• Operation notes
• Hutt, Wairarapa & Wellington Hospital medical records
• Pacific Radiology Records (PACS)
Aims and Methods
• Patient risk factors• Age• Gender• Level• Disk morphology type• Single level DDD versus multi level DDD• Duration of symptoms
• Outcomes• Indication for surgery – recurrent leg, leg/back or back pain• Patient undergoing same-level discectomy• Patient undergoing discectomy and lumbar fusion• Patient undergoing lumbar fusion• Time to repeat surgery• All complication/Deaths/ re-admission <30days
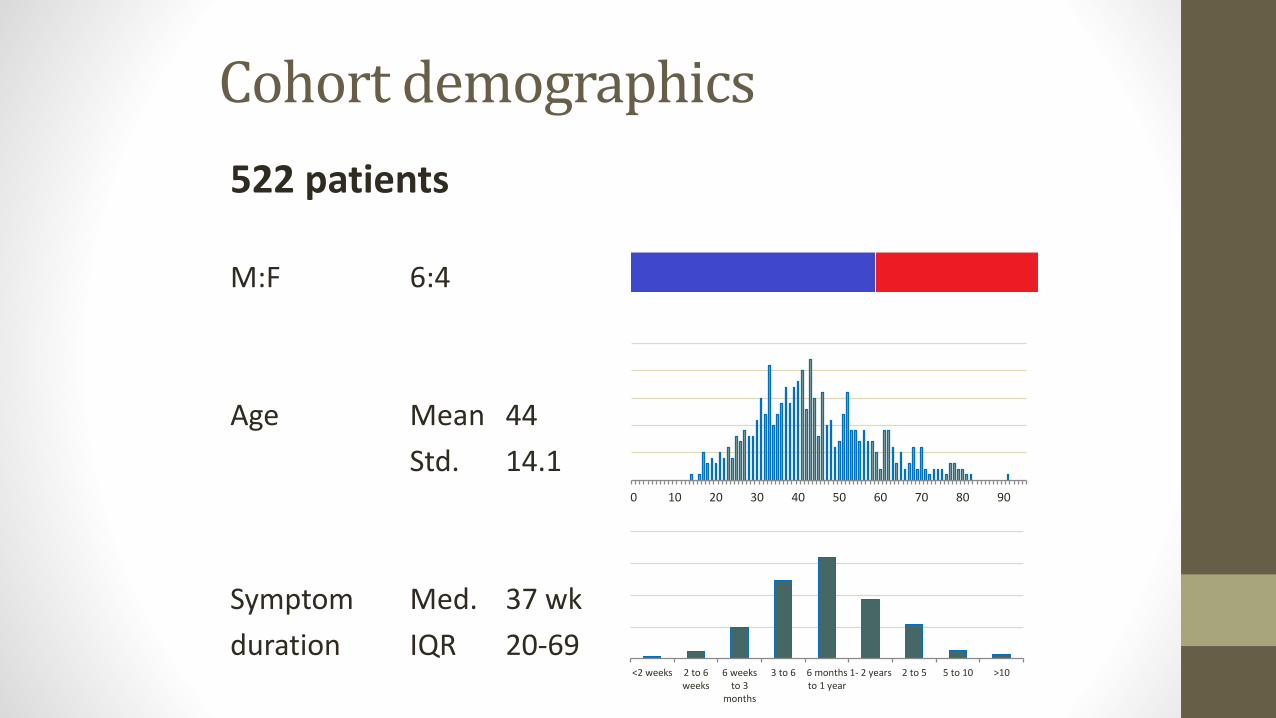
Cohort demographics
522 patients
M:F 6:4
Age Mean 44
Std. 14.1
Symptom Med. 37 wk
duration IQR 20-69
0 10 20 30 40 50 60 70 80 90
<2 weeks 2 to 6weeks
6 weeksto 3
months
3 to 6 6 monthsto 1 year
1- 2 years 2 to 5 5 to 10 >10
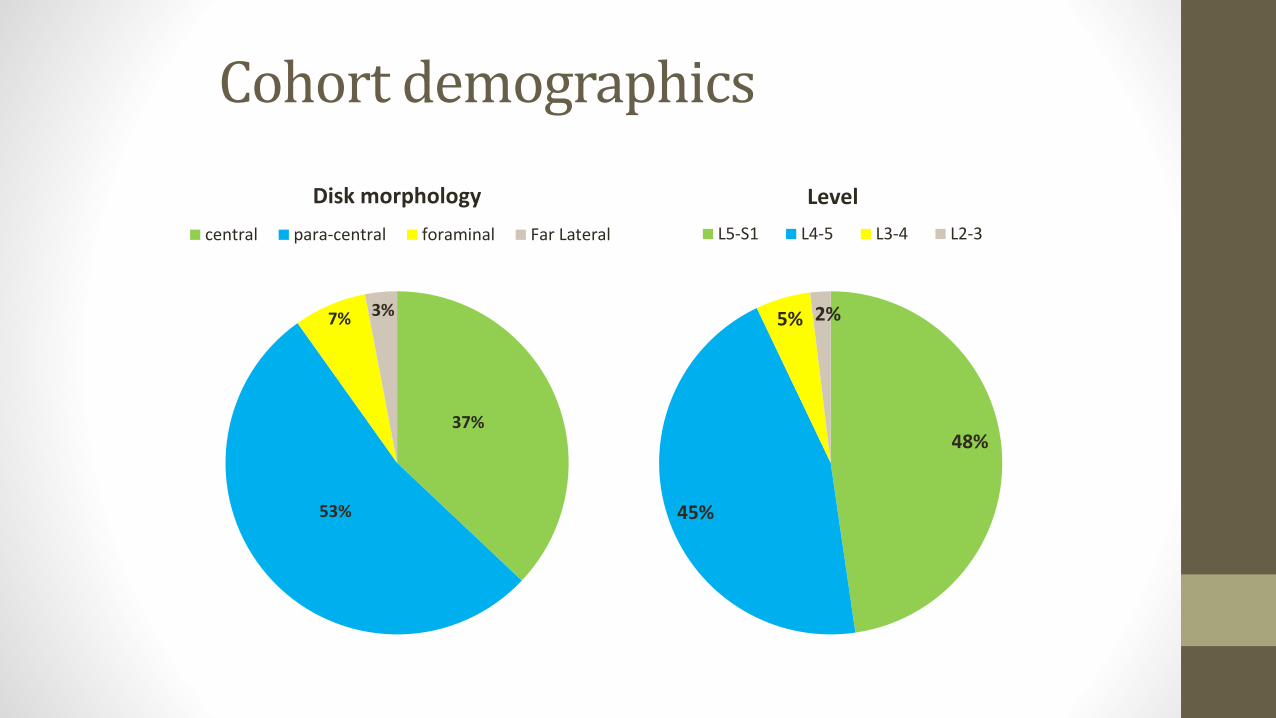
Cohort demographics
37%
53%
7% 3%
Disk morphology
central para-central foraminal Far Lateral
48%
45%
5% 2%
Level
L5-S1 L4-5 L3-4 L2-3
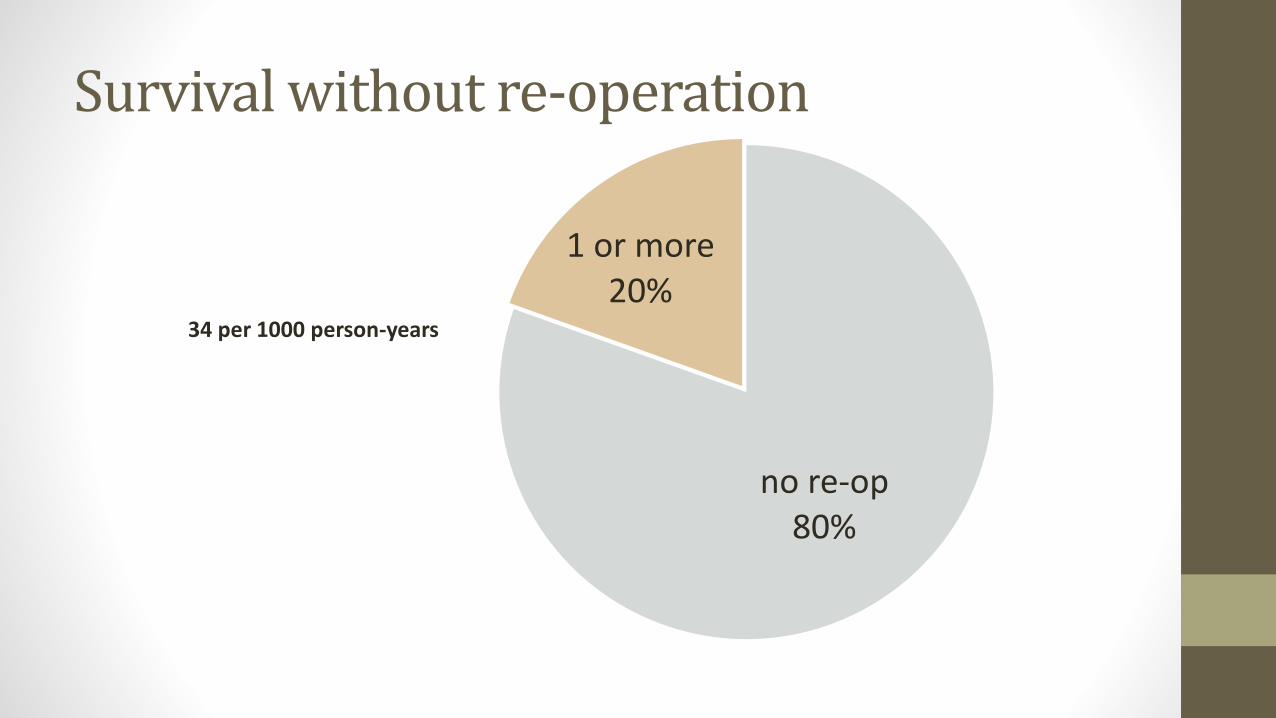
Survival without re-operation
no re-op80%
1 or more20%
34 per 1000 person-years
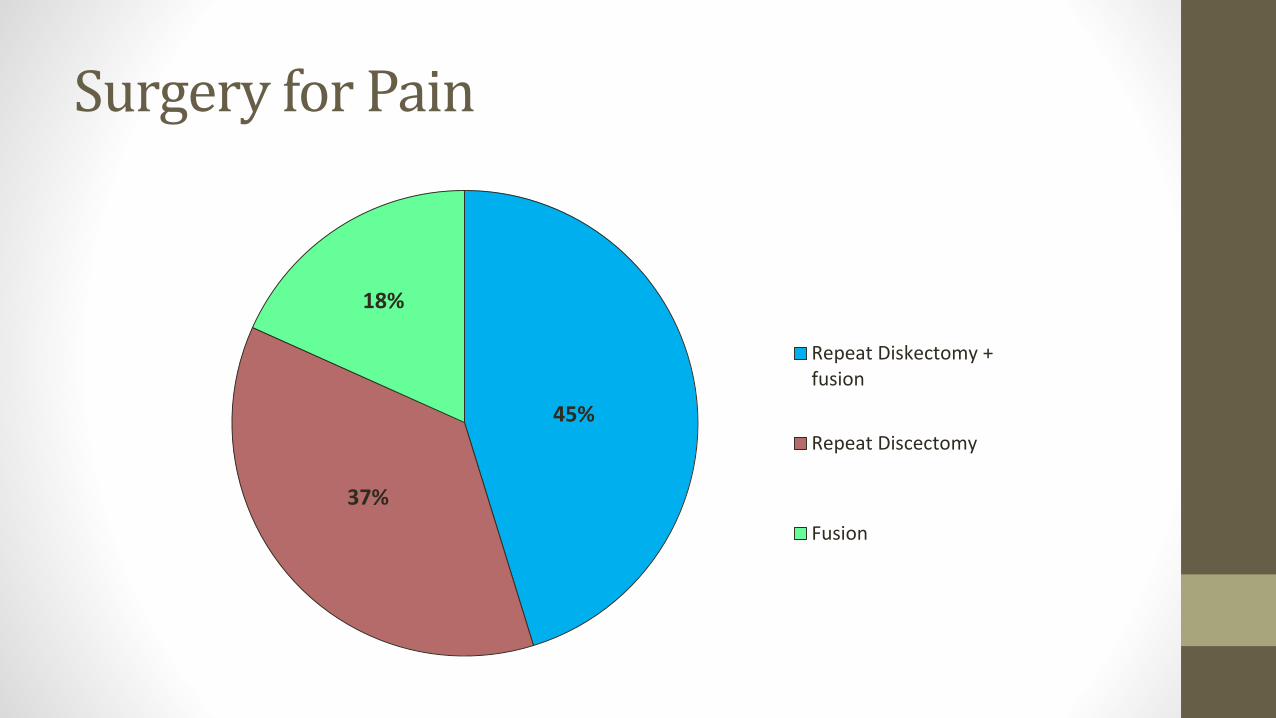
Surgery for Pain
45%
37%
18%
Repeat Diskectomy +fusion
Repeat Discectomy
Fusion
Recurrent Leg Dominant pain
• MRI with isolated recurrence
• 8.0 %
• 12 per 1000-person-years
• Mean age 44.6yr
• M:F 48 : 52
• Med. Symptom duration 46.5 wk
• Single : multi-level disease 60 : 40
• Mean time to re-operation 1.0 yr

0
100
200
300
400
500
600
700
0 1 2 3 4 5 6 7 8
Re
visi
on
rat
e
(p
er
10
00
pe
rso
n-y
ears
)
Post-Op time (Years)
R² = 0.90
Rate of repeat discectomy leg pain
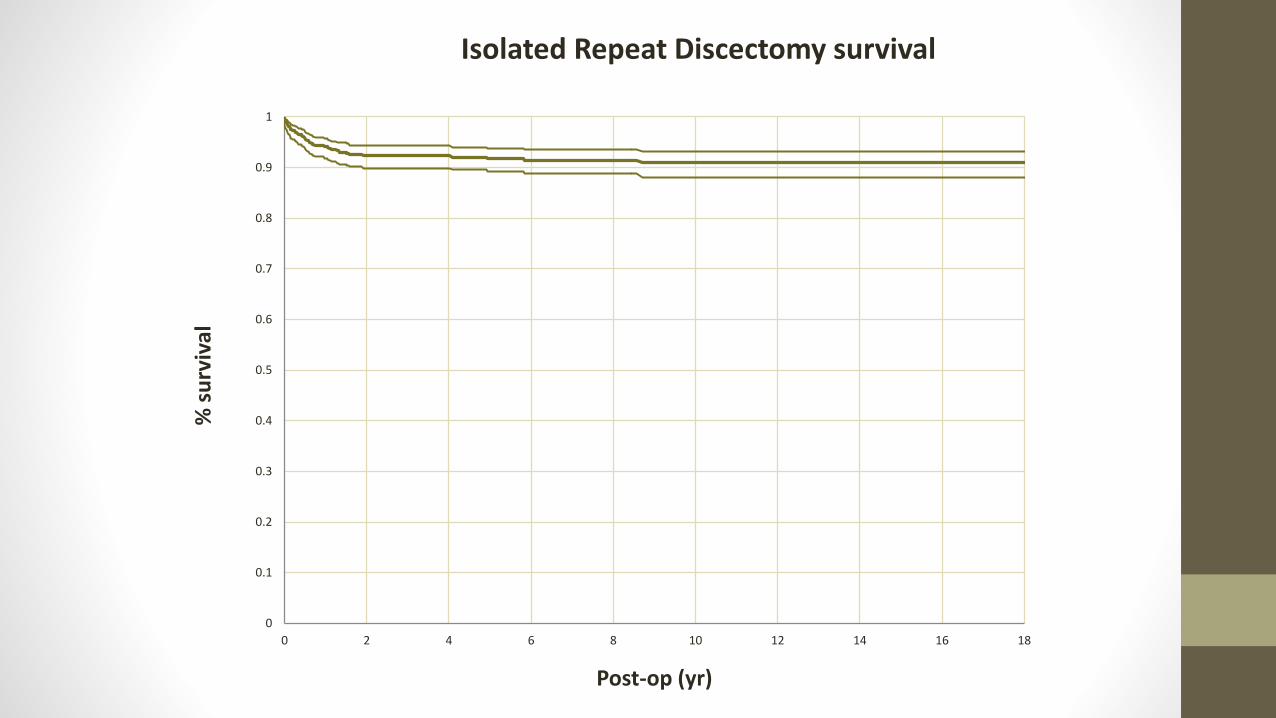
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 2 4 6 8 10 12 14 16 18
% s
urv
ival
Post-op (yr)
Isolated Repeat Discectomy survival
Recurrent Leg and Back pain
• MRI shows prolapse and further degeneration
• 5.0 %
• 3.3 per 1000-person-years
• Mean age 44
• M:F 65 : 35
• Med. Symptom duration 39 wk
• Single : multi-level disease 87 : 13
• Mean time to re-operation 1.5 yr

0
50
100
150
200
250
0 2 4 6 8 10 12 14
Rat
e (
10
00
-pe
rso
n-y
ear
s)
Time (yr)
Rate of Discectomy + Fusion
R² = 0.94
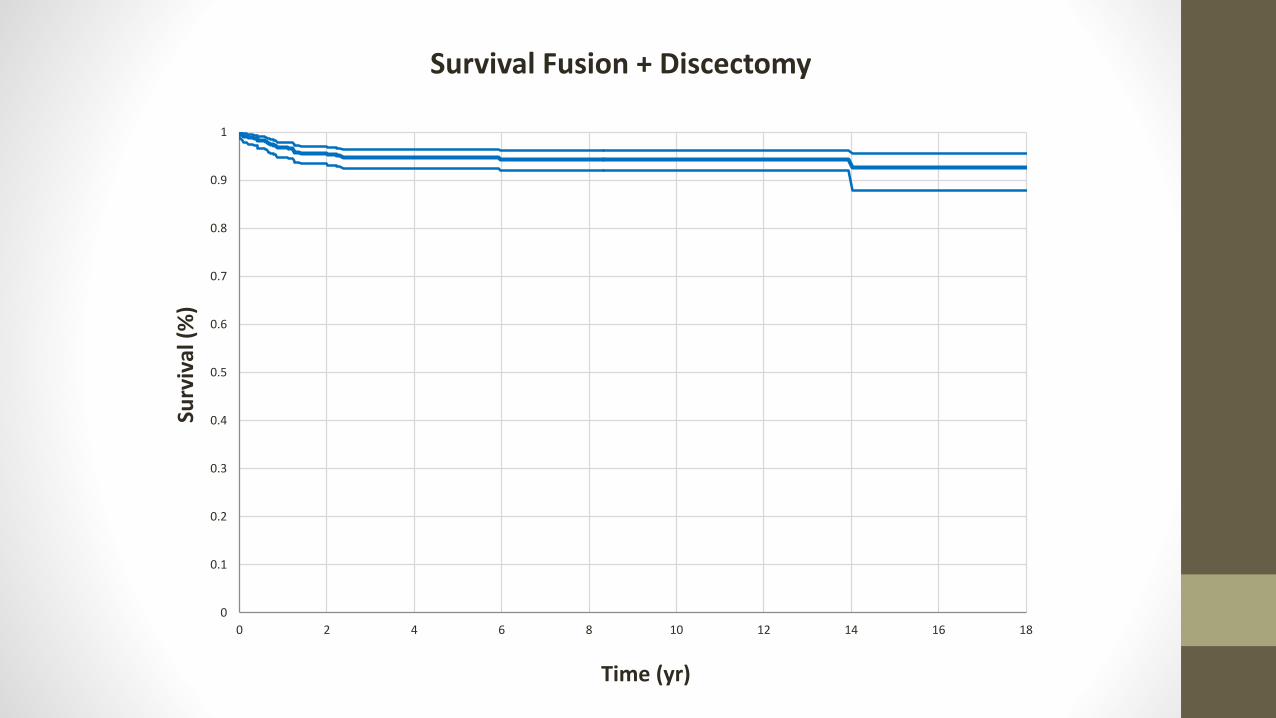
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 2 4 6 8 10 12 14 16 18
Surv
ival
(%
)
Time (yr)
Survival Fusion + Discectomy

Fusion for back pain
• Back dominant pain
• Failed conservative care
• MRI with local progression of disc degeneration
• 3.6%
• 2.3 per 1000-person-years
• Mean age 43.6yr
• M:F 42 : 58
• Med. Symptom duration 37 wk
• Single : multi-level disease 82 : 18
• Mean time to re-operation 3.9 yr
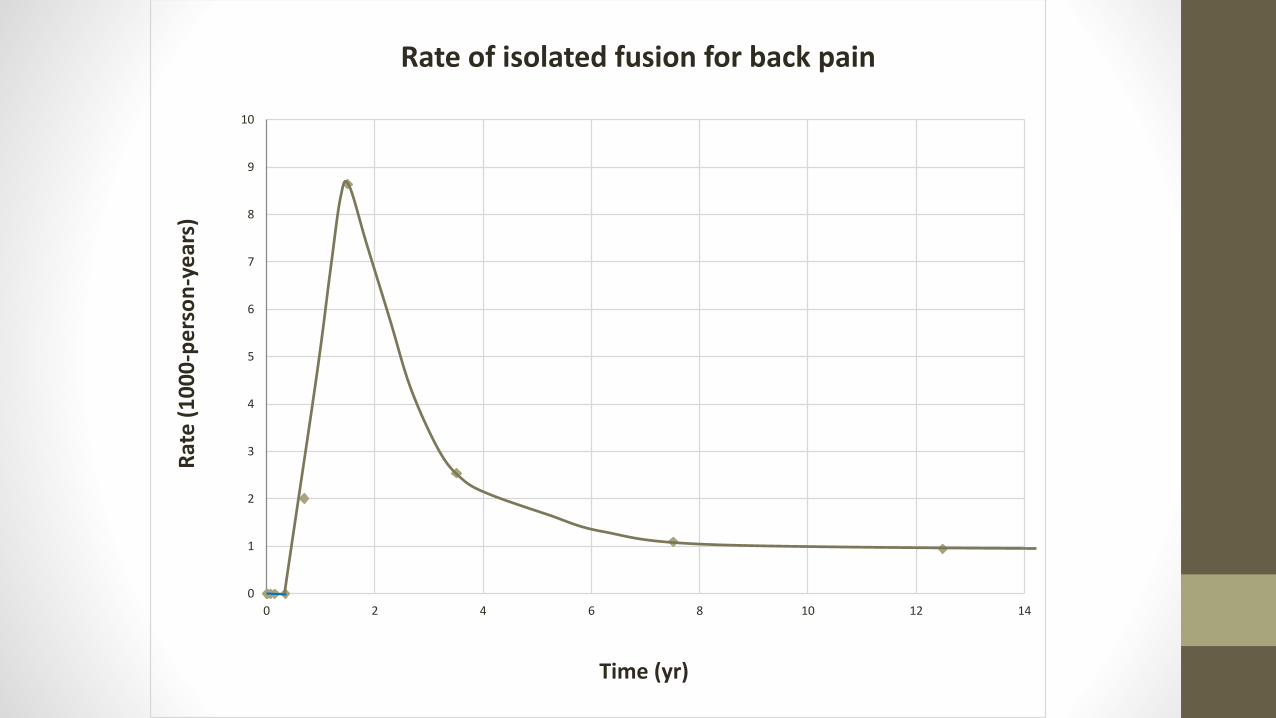
0
1
2
3
4
5
6
7
8
9
10
0 2 4 6 8 10 12 14
Rat
e (
10
00
-pe
rso
n-y
ear
s)
Time (yr)
Rate of isolated fusion for back pain
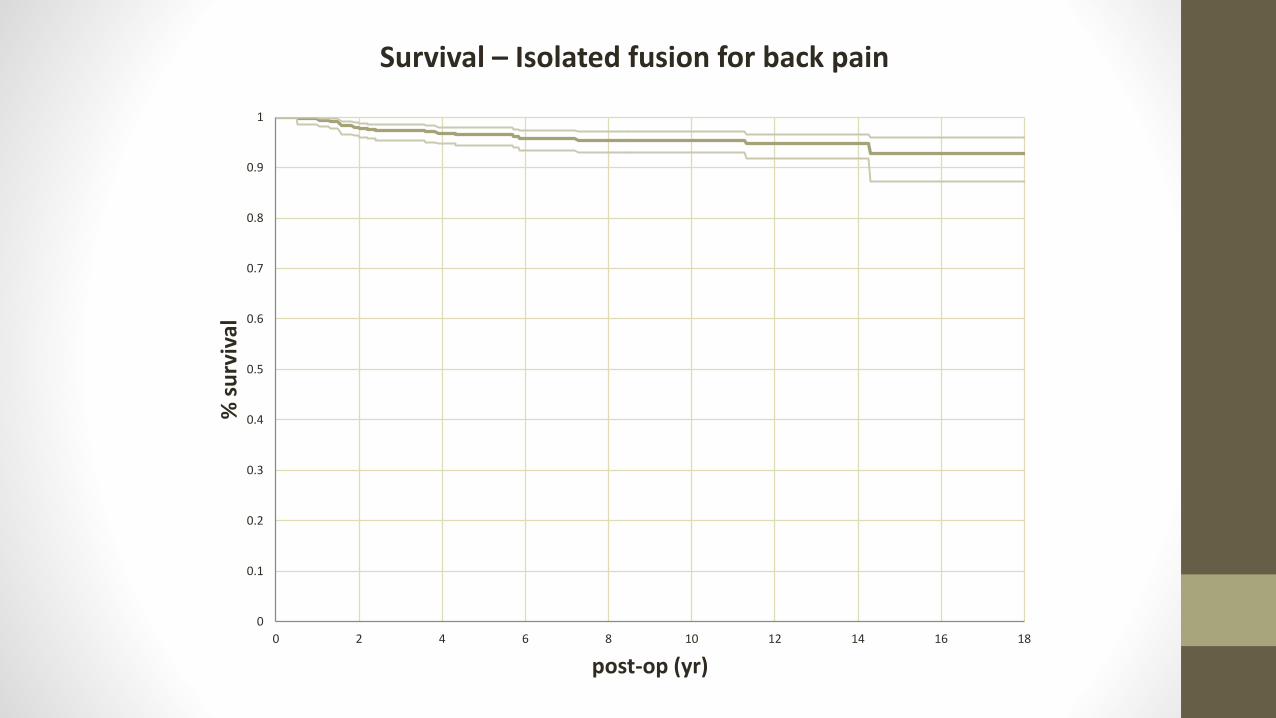
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 2 4 6 8 10 12 14 16 18
% s
urv
ival
post-op (yr)
Survival – Isolated fusion for back pain
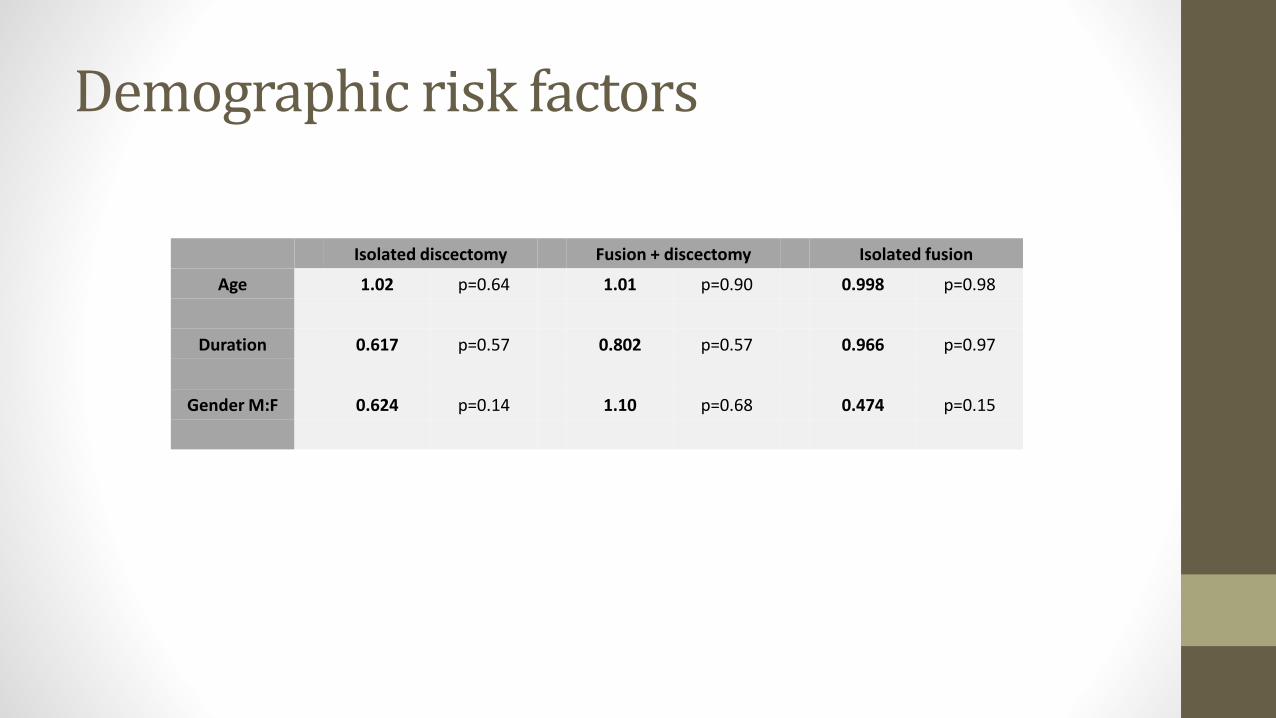
Demographic risk factors
Isolated discectomy Fusion + discectomy Isolated fusion
Age 1.02 p=0.64 1.01 p=0.90 0.998 p=0.98
Duration 0.617 p=0.57 0.802 p=0.57 0.966 p=0.97
Gender M:F 0.624 p=0.14 1.10 p=0.68 0.474 p=0.15
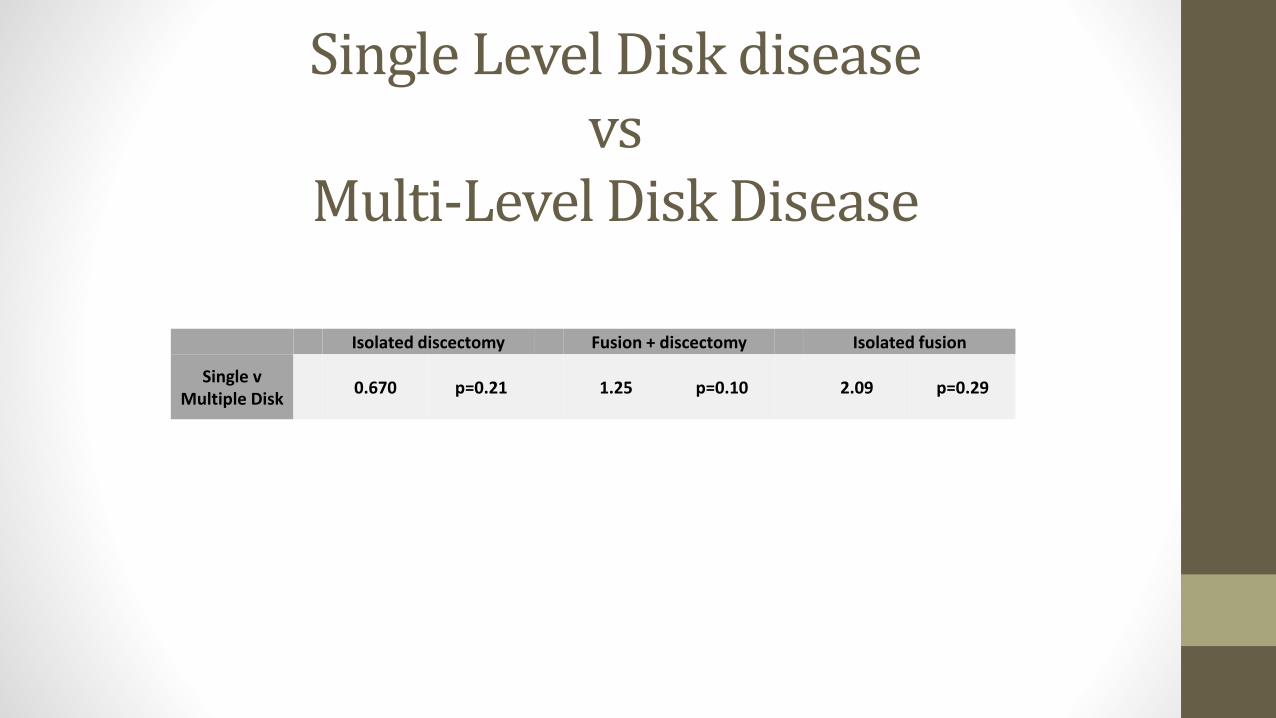
Single Level Disk diseasevs
Multi-Level Disk Disease
Isolated discectomy Fusion + discectomy Isolated fusion
Single v Multiple Disk
0.670 p=0.21 1.25 p=0.10 2.09 p=0.29

Flaws and future
• Subjective markers of patient outcomes influenced by surgically candidacy and surgical decision making
• Doesn’t objectively measure pre or post op leg/back pain and quality of life measures (SF-36, ODI)
• Loss to F/U
• Next Step: Spine Surgery Registry• Prospective collection of Patient outcomes – VAS, EQ5D and ODI
• Revision procedures recorded on registry