Fusion and repeat discectomy following single level open lumbar discectomies. Survival analysis
Dr John MortimerMr Chris Hoffman
CCDHB and TBI Health group
Sciatica = Leg Dominant Pain
• Patients referred for surgical review
• History of back and then leg-dominant pain
• Severe disability – unable to work and sleep
• Associated neurological disturbance
• Conservative care• Nortriptyline for sleep disturbance
• CT guided steroid injection
• NSAIDS/Opiates prn
• Physiotherapy
Failure of Resolution
• Indications for discectomy
• Leg dominant (CBI pattern 3) pain
• Positive tension signs – SLR to reproduce Leg Dominant Pain
• Concordant MRI scan – Disc prolapse at relevant level/side
• When should we operate?
• Must do - Cauda Equina Syndrome (rare)
• Should do - Progressive neurology (rare)
• Could do - Aim to reduce long term pain/disability
• Window of opportunity to intervene – 3 to 12 months

Surgical Goals
• Resolution of leg pain • Reduction in back pain• Preventing further disability
• Goal of surgery• Discectomy removes the displaced fragment• Removes the irritation/pressure on the relevant nerve
• Surgical technique• Cannot repair any nerve damage• Cannot repair the annular defect
• Problem of recurrent prolapse and/or chronic back pain• Conservative care initially• Repeat discectomy (fragment only)• Complete discectomy and spinal fusion
Aims and Methods
• To describe the rates of reoperation following single level lumbar discectomies by one surgeon between 2000-2016
• To describe the complication rates
• To describe the prevalence and association of patient factors and MRI reported disk disease on the incidence of repeat same level discectomy and lumbar fusions
Aims and Methods
• Inclusion
• Single level primary discectomy for MRI proven disk prolapse L1-S1
• No previous discectomy or fusion of any level
• Exclusion
• > one level discectomy
• Any previous spinal surgery
• Decompression for reasons other than HNP
• Any other combination of surgery fusion

Aims and Methods
• Single surgeon database 1998-2016 (Mana Orthopaedics)
• Private practice medical records
• MRI reports
• ACC coding
• ACC surgical request report - ARTP’s
• Operation notes
• Hutt, Wairarapa & Wellington Hospital medical records
• Pacific Radiology Records (PACS)
Aims and Methods
• Patient risk factors• Age• Gender• Level• Disk morphology type• Single level DDD versus multi level DDD• Duration of symptoms
• Outcomes• Indication for surgery – recurrent leg, leg/back or back pain• Patient undergoing same-level discectomy• Patient undergoing discectomy and lumbar fusion• Patient undergoing lumbar fusion• Time to repeat surgery• All complication/Deaths/ re-admission <30days
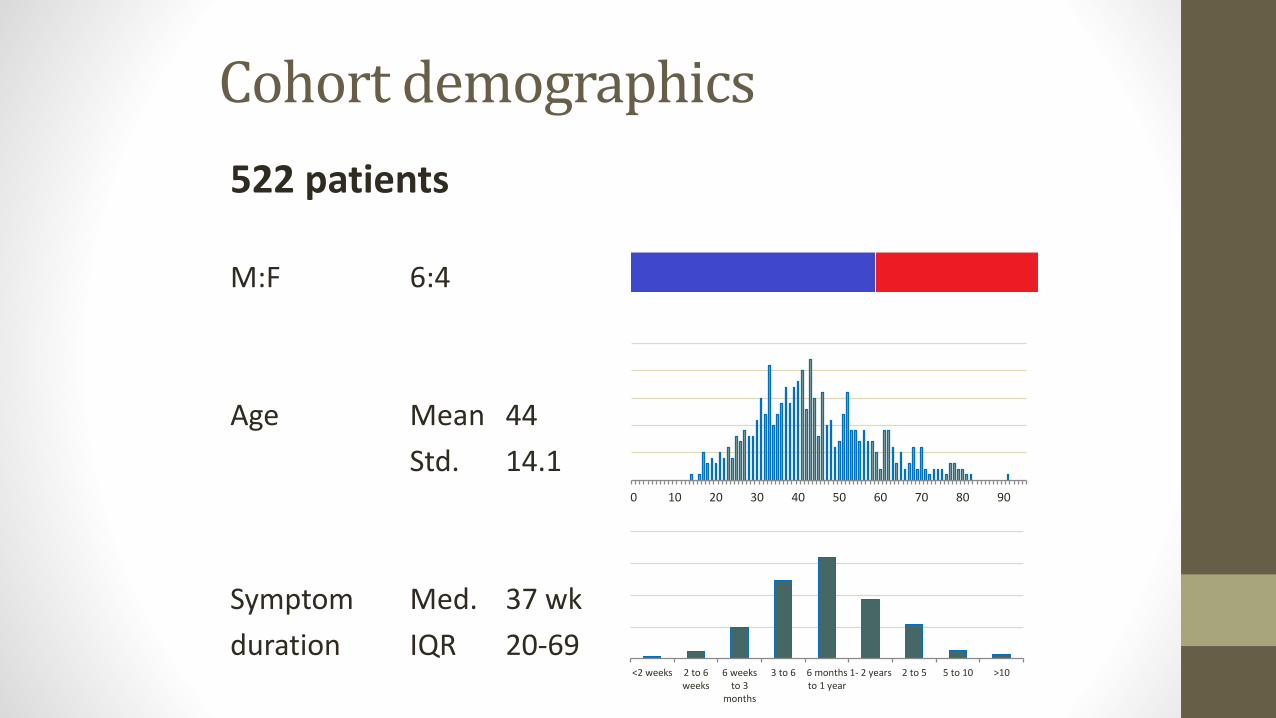
Cohort demographics
522 patients
M:F 6:4
Age Mean 44
Std. 14.1
Symptom Med. 37 wk
duration IQR 20-69
0 10 20 30 40 50 60 70 80 90
<2 weeks 2 to 6weeks
6 weeksto 3
months
3 to 6 6 monthsto 1 year
1- 2 years 2 to 5 5 to 10 >10
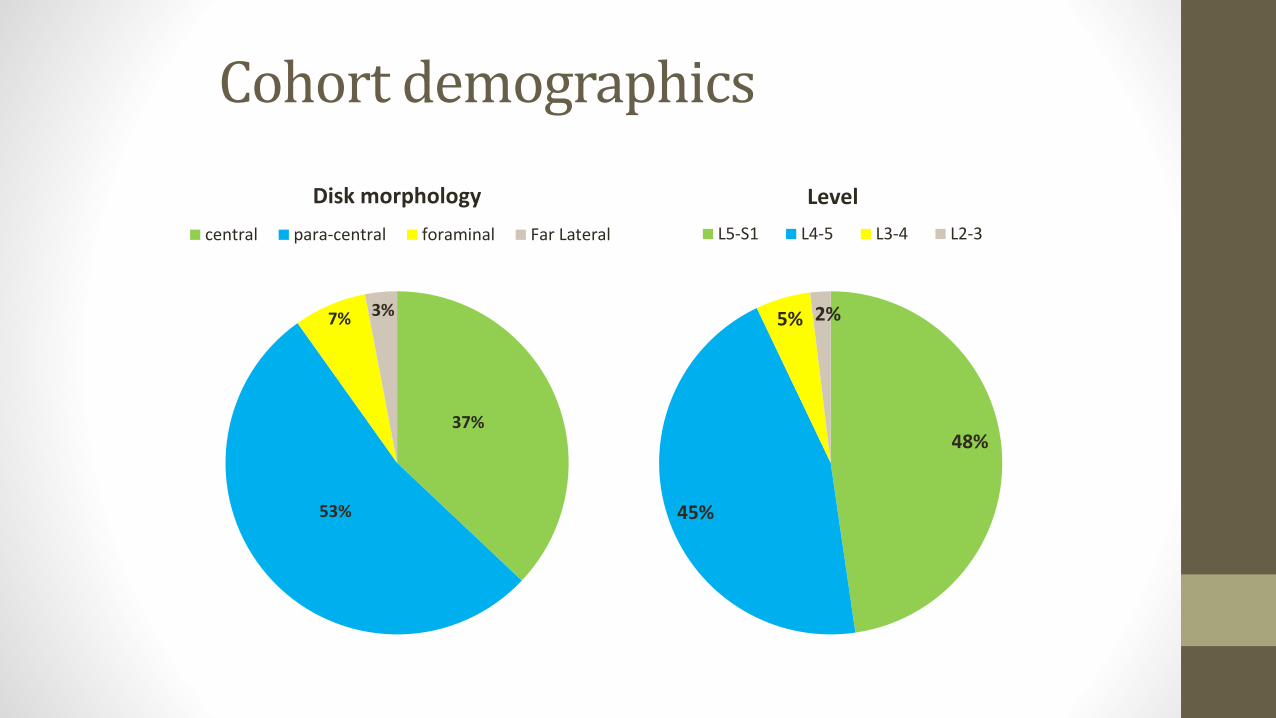
Cohort demographics
37%
53%
7% 3%
Disk morphology
central para-central foraminal Far Lateral
48%
45%
5% 2%
Level
L5-S1 L4-5 L3-4 L2-3
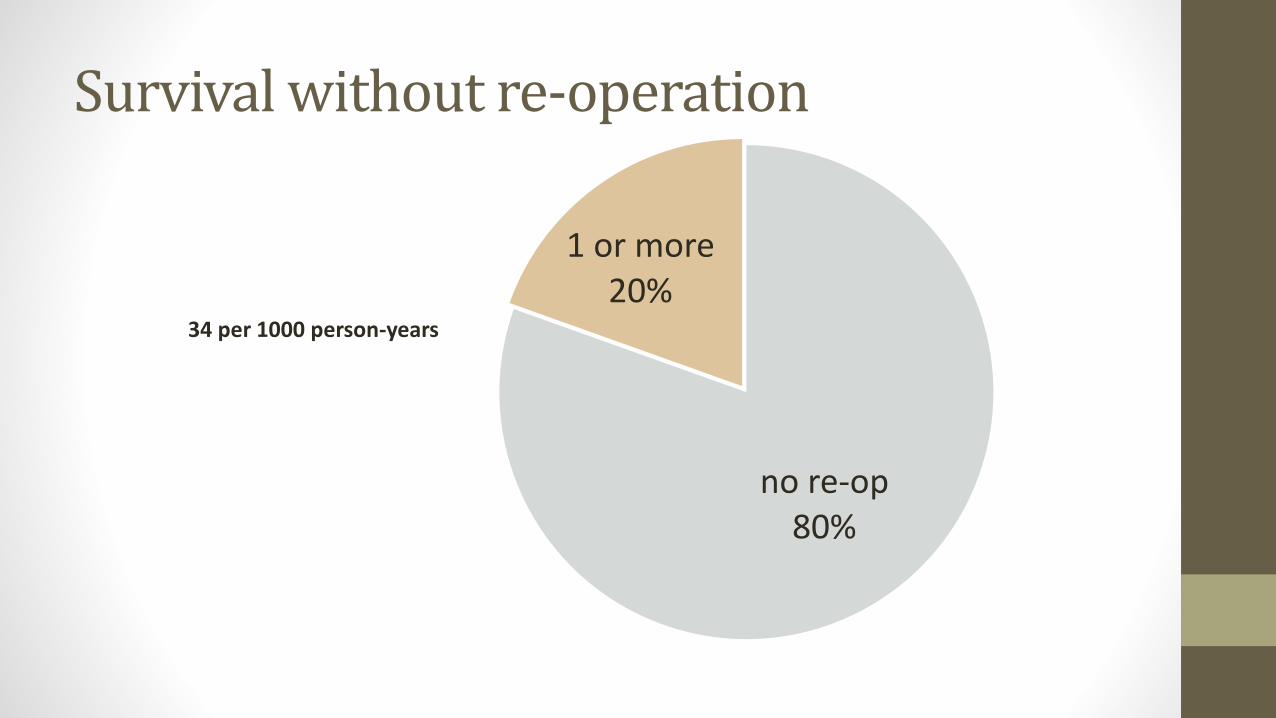
Survival without re-operation
no re-op80%
1 or more20%
34 per 1000 person-years
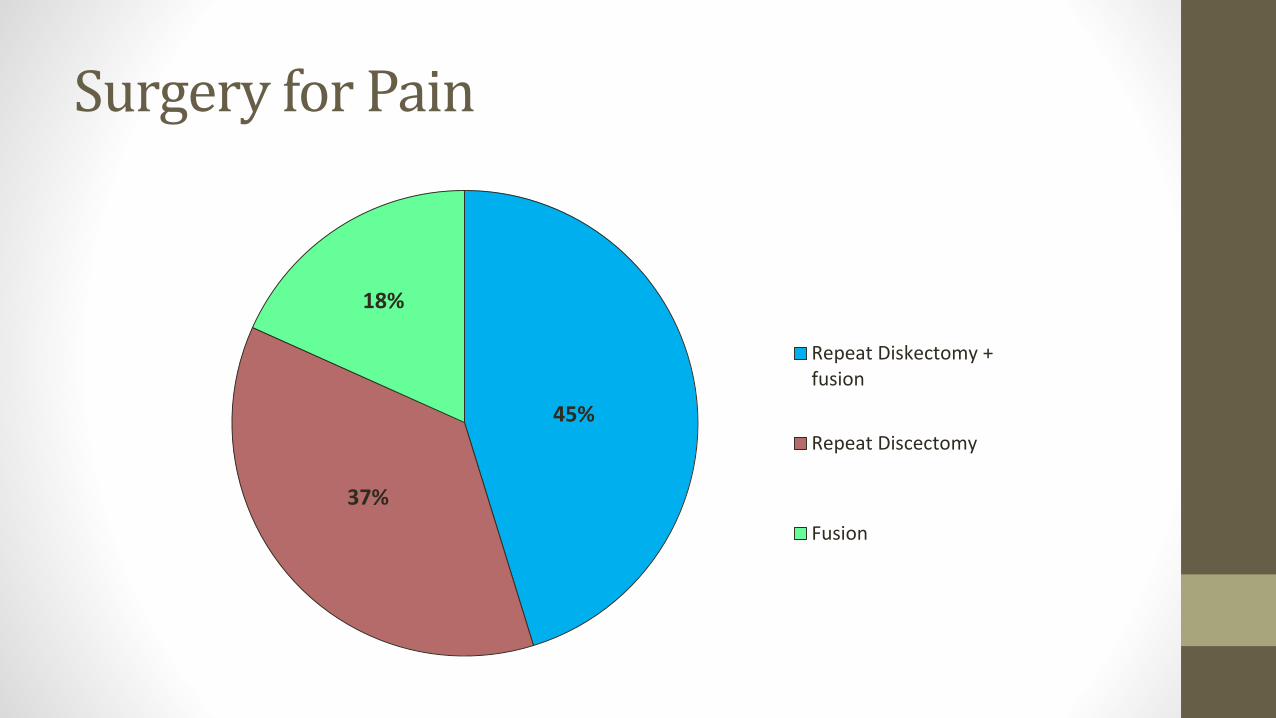
Surgery for Pain
45%
37%
18%
Repeat Diskectomy +fusion
Repeat Discectomy
Fusion
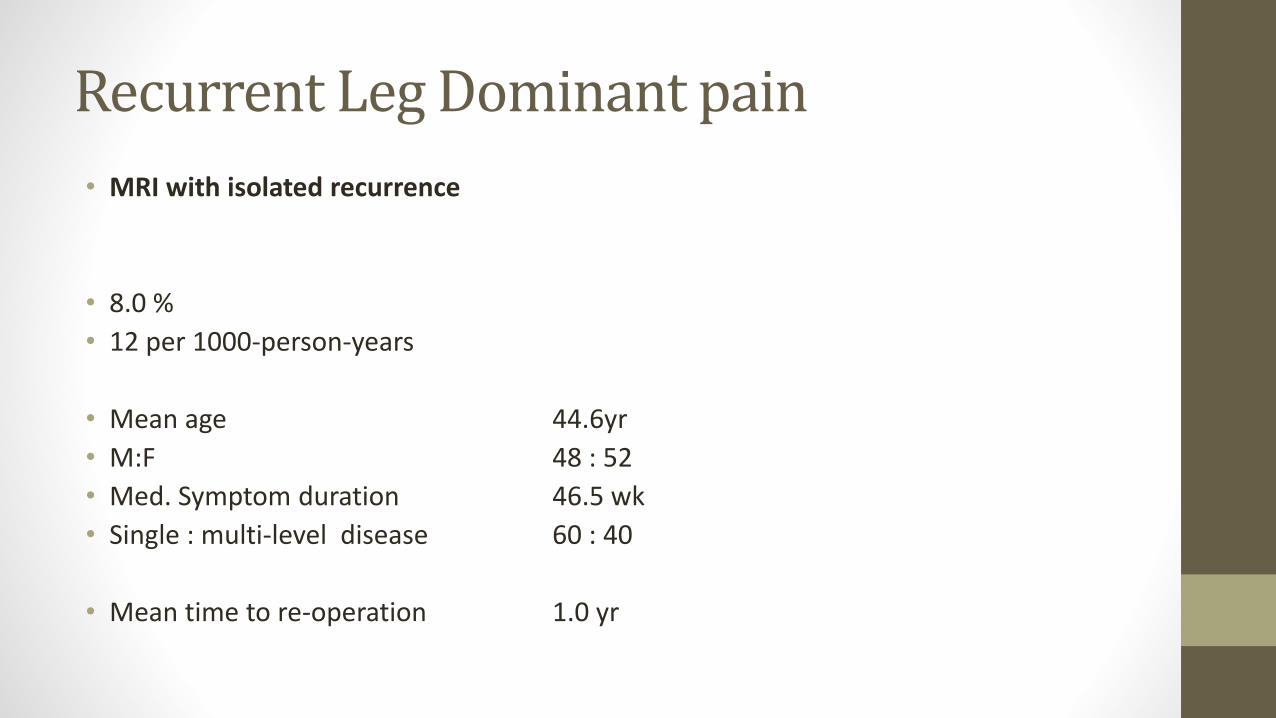
Recurrent Leg Dominant pain
• MRI with isolated recurrence
• 8.0 %
• 12 per 1000-person-years
• Mean age 44.6yr
• M:F 48 : 52
• Med. Symptom duration 46.5 wk
• Single : multi-level disease 60 : 40
• Mean time to re-operation 1.0 yr

0
100
200
300
400
500
600
700
0 1 2 3 4 5 6 7 8
Re
visi
on
rat
e
(p
er
10
00
pe
rso
n-y
ears
)
Post-Op time (Years)
R² = 0.90
Rate of repeat discectomy leg pain
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 2 4 6 8 10 12 14 16 18
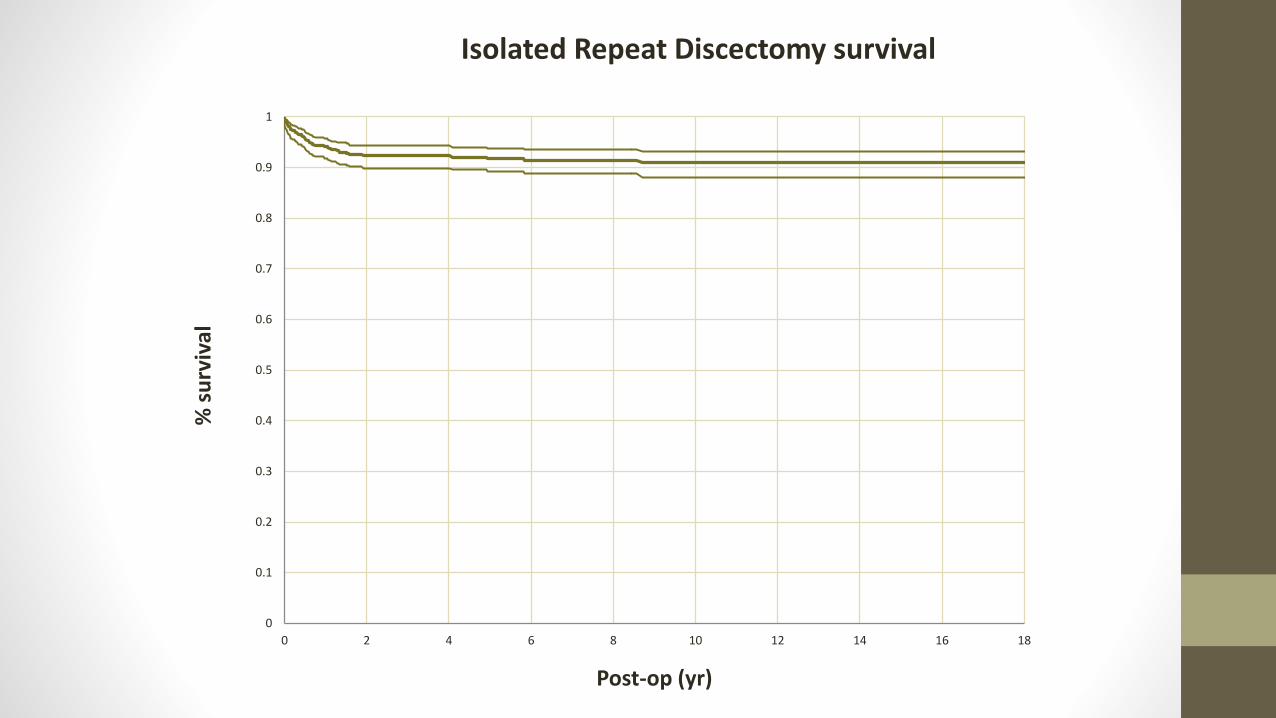
% s
urv
ival
Post-op (yr)
Isolated Repeat Discectomy survival
Recurrent Leg and Back pain
• MRI shows prolapse and further degeneration
• 5.0 %
• 3.3 per 1000-person-years
• Mean age 44
• M:F 65 : 35
• Med. Symptom duration 39 wk
• Single : multi-level disease 87 : 13
• Mean time to re-operation 1.5 yr

0
50
100
150
200
250
0 2 4 6 8 10 12 14
Rat
e (
10
00
-pe
rso
n-y
ear
s)
Time (yr)
Rate of Discectomy + Fusion
R² = 0.94
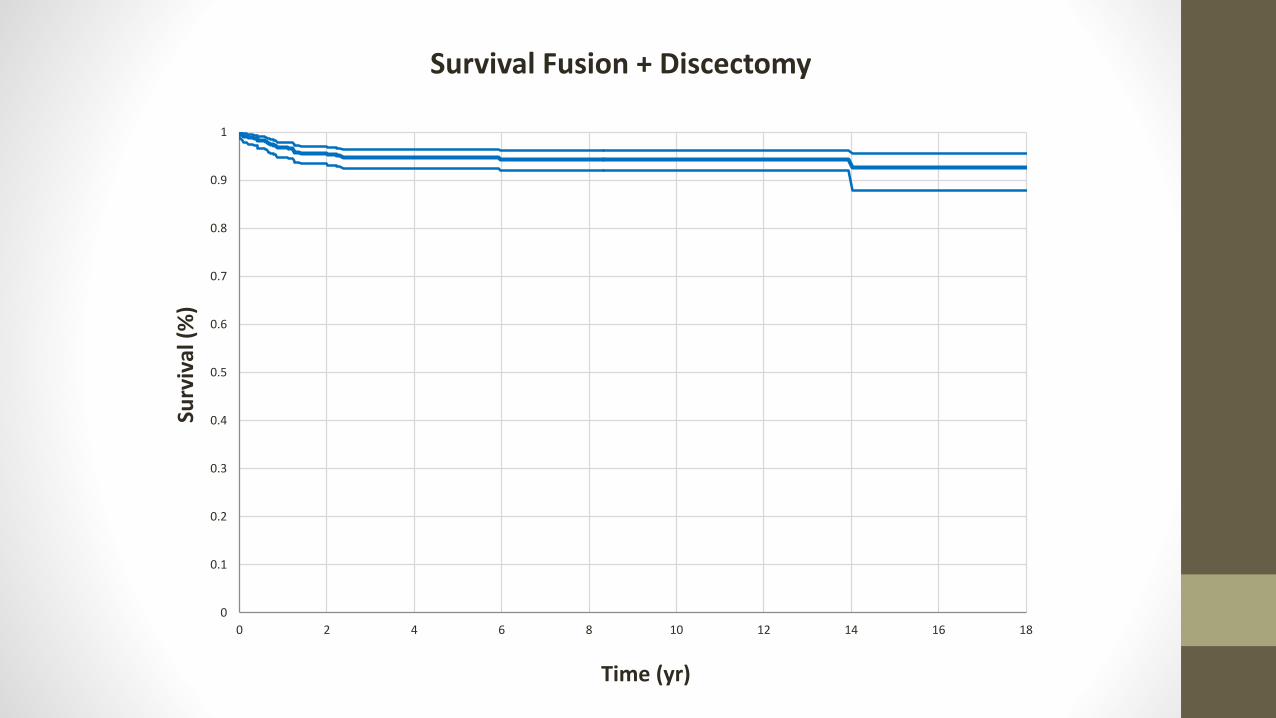
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 2 4 6 8 10 12 14 16 18
Surv
ival
(%
)
Time (yr)
Survival Fusion + Discectomy

Fusion for back pain
• Back dominant pain
• Failed conservative care
• MRI with local progression of disc degeneration
• 3.6%
• 2.3 per 1000-person-years
• Mean age 43.6yr
• M:F 42 : 58
• Med. Symptom duration 37 wk
• Single : multi-level disease 82 : 18
• Mean time to re-operation 3.9 yr
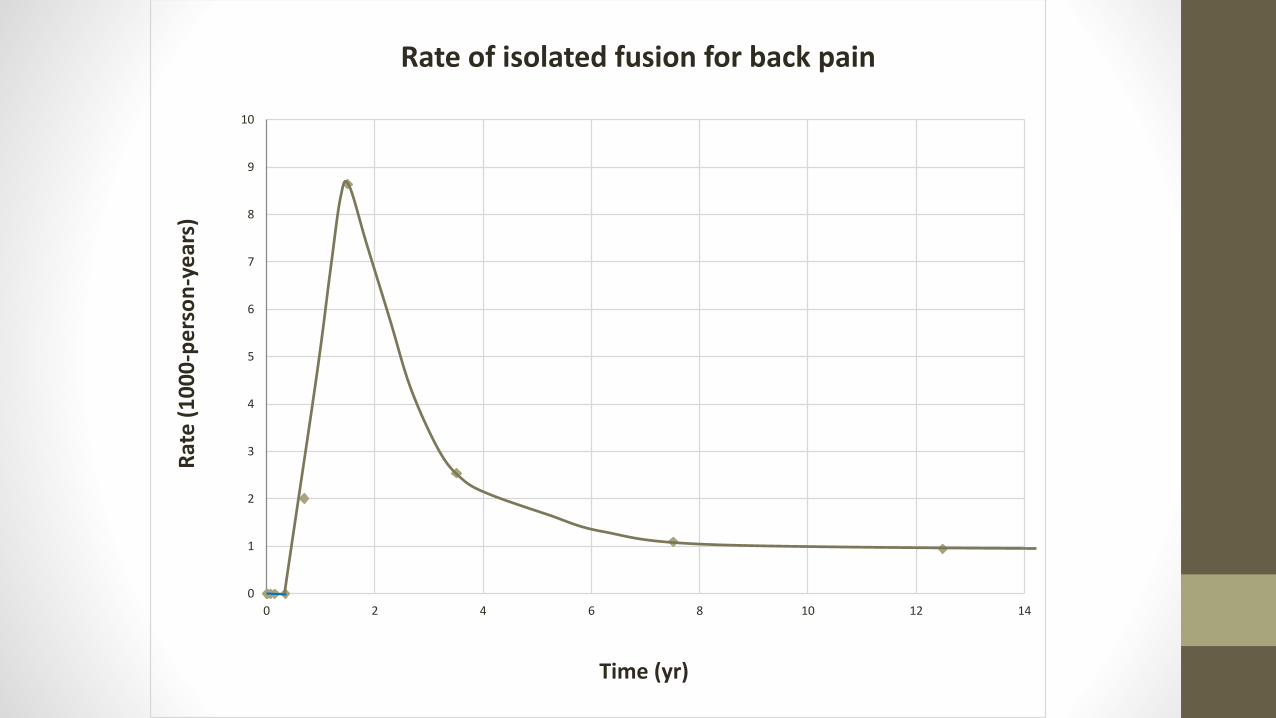
0
1
2
3
4
5
6
7
8
9
10
0 2 4 6 8 10 12 14
Rat
e (
10
00
-pe
rso
n-y
ear
s)
Time (yr)
Rate of isolated fusion for back pain
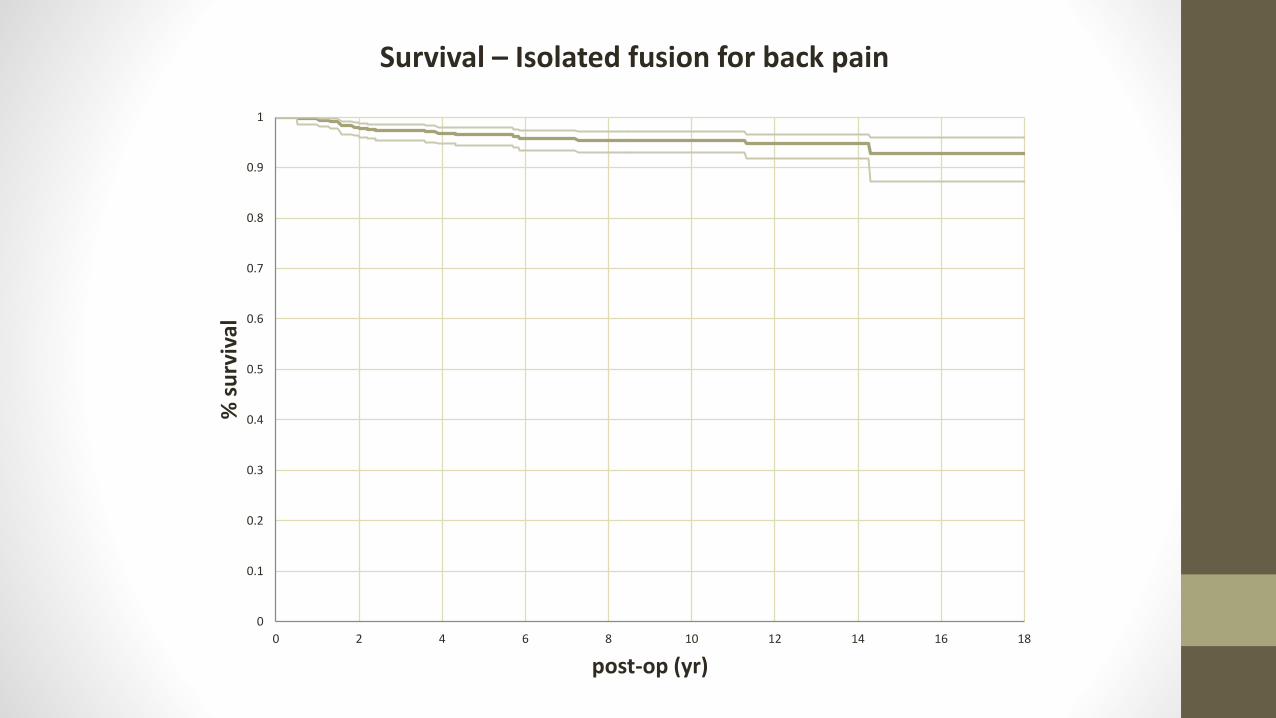
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 2 4 6 8 10 12 14 16 18
% s
urv
ival
post-op (yr)
Survival – Isolated fusion for back pain
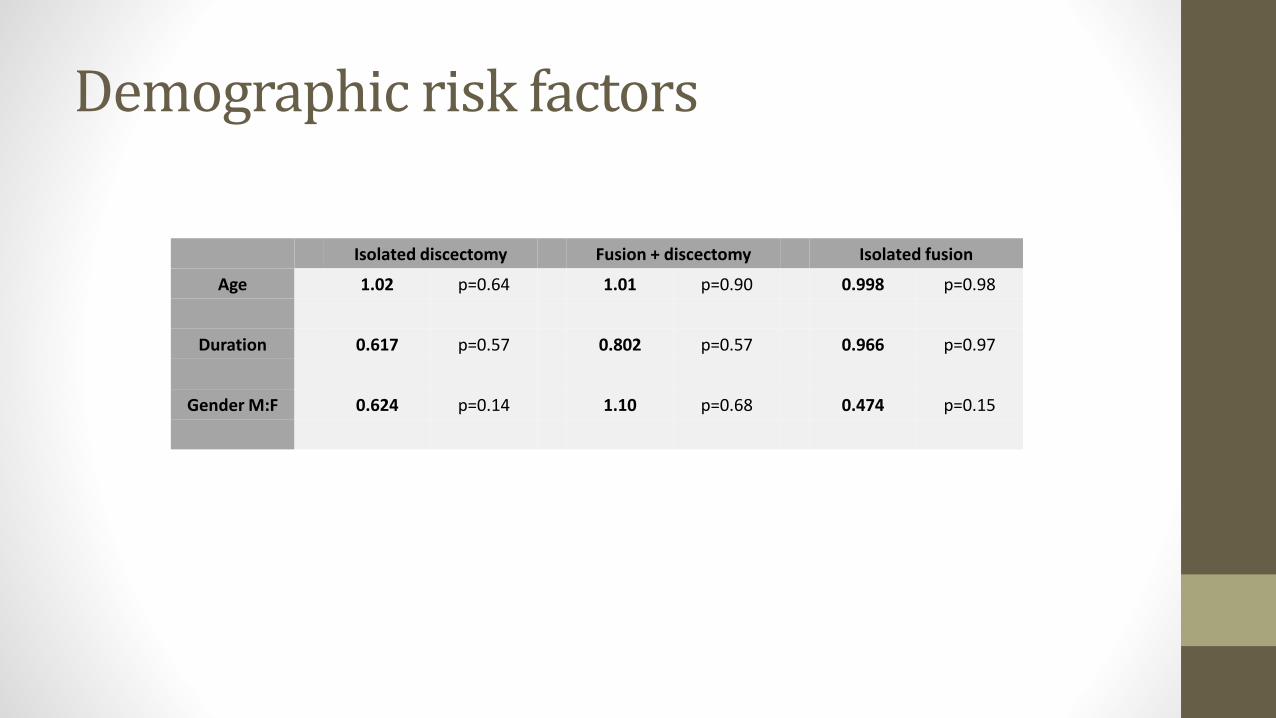
Demographic risk factors
Isolated discectomy Fusion + discectomy Isolated fusion
Age 1.02 p=0.64 1.01 p=0.90 0.998 p=0.98
Duration 0.617 p=0.57 0.802 p=0.57 0.966 p=0.97
Gender M:F 0.624 p=0.14 1.10 p=0.68 0.474 p=0.15
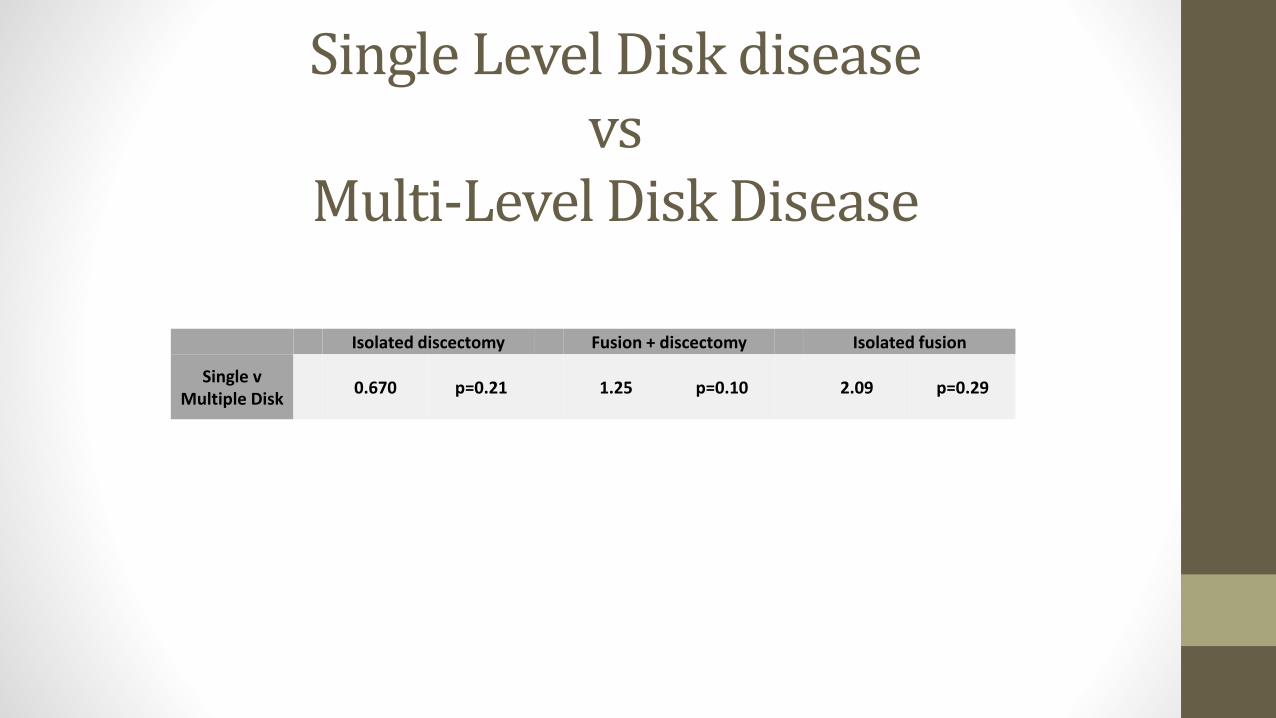
Single Level Disk diseasevs
Multi-Level Disk Disease
Isolated discectomy Fusion + discectomy Isolated fusion
Single v Multiple Disk
0.670 p=0.21 1.25 p=0.10 2.09 p=0.29

Flaws and future
• Subjective markers of patient outcomes influenced by surgically candidacy and surgical decision making
• Doesn’t objectively measure pre or post op leg/back pain and quality of life measures (SF-36, ODI)
• Loss to F/U
• Next Step: Spine Surgery Registry• Prospective collection of Patient outcomes – VAS, EQ5D and ODI
• Revision procedures recorded on registry
![Incidence of Low Back Pain After Lumbar Discectomy for ...discectomy [5, 10]. In 2003, 2.1 per 1000 Medicare en-rollees received a lumbar discectomy/laminectomy [92]. Although the](https://cdn.vdocuments.mx/doc/165x107/600b85aa673f433b006b3d0b/incidence-of-low-back-pain-after-lumbar-discectomy-for-discectomy-5-10-in.jpg)






