for the evaluation of the radio distance learning evaluation draft... · report for the evaluation...
TRANSCRIPT

USAID/JHU Associate Cooperative Agreement No. 617‐A‐00‐07‐00005‐00
Report for the Evaluation of the Radio Distance Learning
Program, Mukono District
April 2012

Table of contents TABLE OF CONTENTS ............................................................................................................................................ I ACRONYMS ...............................................................................................................................................................II SUMMARY OF FINDINGS .................................................................................................................................... III 1.0 INTRODUCTION ................................................................................................................................................. 1
OBJECTIVES OF THE STUDY ........................................................................................................................................ 1 1.2 STUDY DESIGN AND METHODOLOGY: ....................................................................................................... 2 2.0 FINDINGS .............................................................................................................................................................. 4 2.1 QUANTITATIVE FINDINGS ............................................................................................................................. 4
2.1.1 NUMBER OF VHT RESPONDENTS INTERVIEWED ................................................................................................ 4 2.1.2 KNOWLEDGE OF VHT ROLES IN THE COMMUNITY ............................................................................................. 4 2.1.3 KNOWLEDGE OF FAMILY PLANNING .................................................................................................................. 5 2.1.4 KNOWLEDGE OF HIV AMONG VHTS ................................................................................................................. 6 2.1.5 KNOWLEDGE OF KEY PLHIV POSITIVE PRACTICES ............................................................................................ 8 2.1.6 KNOWLEDGE OF BENEFITS OF SAFE MALE CIRCUMCISION ................................................................................. 9 2.1.7 KNOWLEDGE OF VIOLENCE AND DANGERS OF ALCOHOL ABUSE ........................................................................ 9 2.1.8 SELF EFFICACY IN ADDRESSING KEY HEALTH TOPICS ...................................................................................... 10 2.1.9 VHT PERCEPTION ABOUT THE EFFECTIVENESS OF THE RDL PROGRAM ........................................................... 11
2.2 QUALITATIVE FINDINGS .............................................................................................................................. 14 2.2.1 KEY HEALTH CONCERNS/PROBLEMS IN THE COMMUNITY .............................................................................. 14 2.2.2 CURRENT SOURCES OF HEALTH INFORMATION ................................................................................................ 14 2.2.3 ROLES OF THE VILLAGE HEALTH TEAMS (VHTS) ........................................................................................... 15 2.2.4 LISTENERSHIP TO “OBBANYWA” RDL PROGRAM ........................................................................................... 16
2.2.5 KNOWLEDGE ABOUT PROGRAM CONTENT, FREQUENCY OF LISTENING AND RATING .... 16 2.2.6 TIMING OF THE PROGRAM ....................................................................................................................... 17 2.2.7 PROGRAM PRESENTATION ....................................................................................................................... 17 3.0 CONCLUSION AND RECOMMENDATIONS ............................................................................................... 18 3.1 CONCLUSIONS .................................................................................................................................................. 18 3.2 RECOMMENDATIONS .................................................................................................................................... 19 APPENDICES: DATA COLLECTION TOOLS ................................................................................................... 20
ii
Acronyms
ARVs Anti Retroviral Drugs DHE District Health Educator FGD Focus Group Discussion HCP Health Communication Partnership KI Key Informants LAPM Long Acting and Permanent family planning Methods MoH Ministry of Health PLHIV People Living with HIV RDL Radio Distance Learning program SMC Safe Male Circumcision VHT Village Health Teams

iii
Summary of findings
This evaluative study was designed to assess the effectiveness of the RDL program in improving the skills and knowledge of VHTs. The other objective was to establish the reach and effects of the RDL program among the general population beyond the VHT members. Results of the evaluative study are to be used in planning, refining as well as replicating the RDL program in other districts of Uganda. The study included a total of 230 and 194 VHT members at baseline and follow up respectively. For purposes of this report, we included 182 VHTs who had information collected at both baseline and follow up.
Knowledge of VHT roles in the community: Results indicate that the level of knowledge of at least three roles played by VHTs increased from 19% to 32% between the two data collection points. Notably, the most known role for VHTs was mobilization of the community, mentioned by 63 and 83 percent at baseline and follow up respectively.
Knowledge of family planning: Results indicate that knowledge of at least three benefits of family planning almost doubled from 22% at baseline to 40% at follow up while the proportion of VHT members who did not know any benefit of family planning drastically dropped to 0 percent at follow up down from six percent at baseline. The level of knowledge of all the four LAPM methods increased five fold from two percent upward to eleven percent at follow up.
Knowledge of HIV among VHTs: The percentage of VHTs who knew at least three benefits of HIV testing increased from 32 percent at baseline to 58 percent at follow up. Knowledge that pregnant women can prevent transmission of HIV to their unborn child was the least known benefit for HIV testing at follow up. With regard to level of knowledge of practices that couples can undertake to prevent HIV infection, there was an increase from 19 percent to 30 percent, while knowledge of signs of HIV infection among children increased from zero to two percent. The most known sign of HIV in children was recurrent and regular fever by 54 and 84 percent at baseline and follow up respectively. The least known sign was weight loss by five and four percent at baseline and follow up respectively. Knowledge of key PLHIV positive practices: VHT members were also asked about knowledge of key practices that PLHIVs should do in order to delay progression to AIDS. Knowledge of at least three practices increased almost two fold from 30% to 56%, while knowledge of all the six PLHIV practices to delay progression to AIDS rose from three to nine percent.
Knowledge of benefits of safe male circumcision: VHTs were also asked about the benefits of safe male circumcision during the survey. As can be observed, clearly the RDL program increased the level of knowledge of benefits for SMC among the VHTs enrolled in the program as the percentage of those who could mention all the three benefits correctly increased five fold from two percent to eleven percent. Knowledge of violence and dangers of alcohol abuse: Knowledge of all three types of violence increased more than two fold from 11 percent to 32 percent at baseline and follow up respectively. On the other hand, the percentage of those who do not know any type of violence decreased from twelve to five percent. Results obtained indicate that knowledge of at least three dangers of alcohol abuse more than doubled from 28% to 67%, while knowledge of all the dangers of alcohol also increased from two percent to four percent. Self efficacy in addressing key health topics: Results indicate that the RDL program increased self efficacy of VHTs in only two out of the eight health topics. The health topics for

iv
which self efficacy was increased were family planning; from 75% to 84% and HIV prevention and transmission; from 73% to 87% at baseline and follow respectively.
VHT perception about the effectiveness and relevancy of the RDL program: Overall, majority of the VHTs felt that the RDL program was effective for all the three elements asked; 83, 77 and 82 percent of the VHTs reporting that the weekly episodes on Radio, the listener’s guide and the listening groups were effective respectively. Results show that all the topics were very relevant. However the most relevant topics were benefits of HIV testing and causes and dangers of alcohol abuse with 91% of the VHTs saying that they were very relevant.
Qualitative findings: The general population mentioned VHTs and the radio were mentioned as the main sources of health information. Only a few community members interviewed reported to have listened to the program on Radio Dunamis partly because it was not one of their favorite radio FM stations, its signal was poor in some areas and that no community promotional activities were conducted before airing the program. Community members who had listened to the program described it as very interesting, engaging and not boring. Based on experiences from Mukono, future RDL programs are more likely to reach and influence the general population if radio stations with high listenership are identified to air the episodes, prior community awareness/promotional drives are conducted and proper timing of the different episodes is well thought out.

1.0 Introduction
The Ministry of Health (MoH) is implementing the Village Health Team (VHT) strategy to ensure that every village in Uganda has village health teams who work together to mobilize individuals and households for better health. VHT members are community volunteers who are selected by communities to provide accurate health information and proper linkage to health services within their areas of jurisdiction. To supplement current VHT training efforts, the Uganda Ministry of Health and the Health Communication Partnership (HCP) established a radio distance learning (RDL) program for VHTs in Mukono district to provide them with continuing education on a regular basis. The overall purpose of the RDL program was to provide them with information and skills that would assist them to fulfill their roles and responsibilities including maintaining good health in the community, strengthening the capacity of family members to provide quality care and support in the home, and liaising with health facilities through referrals and data collection. The program was aired on Radio Dunamis and included radio drama series demonstrating how a VHT promotes key health practices in the fictitious village of ‘Obbanywa’. The drama series were broadcast twice a week over a 13 week period, and were accessible to VHTs as well as other community members.
Objectives of the Study The overall objective of the study was to assess the effectiveness of the radio distance learning program for VHTs in providing knowledge and skills to VHTs as well as establishing the reach and effects of the program among the general population beyond the VHT listening groups. The specific objectives were:
(i) Assess changes in knowledge, and attitudes of village health team members regarding key health issues especially those promoted by HCP;
(ii) Assess skills and practices of village health teams members regarding key health issues promoted by HCP;
(iii) Assess overall effectiveness of the radio distance learning program implemented by the Health Communication Partnership;
(iv) Establish the knowledge, practices, beliefs and attitudes related to the key health practices promoted by the RDL program among the general population.
(v) Gain an understanding the current sources of information about health services in their community. (vi) Assess community member`s knowledge about the roles of VHT roles in relation to the delivery of
health services. (vii) Collect information on community experiences about the RDL program including timing of the
program, topics listened to as well as appropriateness of the programs. (viii) Provide recommendations for developing, refining, and prioritizing the RDL program’s
interventions among VHT members in relation to the health issues promoted through the program.

2
1.2 Study design and methodology:
A longitudinal evaluative study design with two data points; baseline (during the launch of the program in each sub county) and a follow up 5 months afterwards was utilised. Both qualitative and quantitative research methods were employed to provide a range of opinions and conclusions regarding the RDL program. The study adopted a qualitative approach in which focus group discussions comprising of between 8 and 12 respondents were held with community members. A number of thematic areas following the specific objectives were adapted in order to extensively get feedback about the program.
1.2.1 Study population The study population consisted of VHT members residing in six sub-counties of the greater Mukono district who attended the launches of the radio distance program in the six sub-counties. The study focused only on VHT members who attended the launch because these were the one most likely to participate consistently in the program for purposes of follow up. In addition to the village health team members, the study population included the District Health Educator, VHT supervisors in each of the six sub-counties and the general population in Mukono district.
1.2.2 Study Sample Size and selection of respondents
Because the study needed to detect a 10% change in the proportion of respondents who are have full knowledge of family planning methods, with a power of 0.80 and an alpha of 0.05 assuming that 50% of VHT’s have full knowledge of family planning methods, a 10% non response rate and a loss to follow up of 20%, a sample of 255 VHT members were included in the study. For key informants, we interviewed the district health educator (DHE) and six sub county VHT supervisors. Within the general population, a total of twelve male and female FDGs were conducted each comprising of 8 to 12 participants.
VHT members included in the study were randomly selected from a list of participants attending the RDL launch in each of the six sub-counties with a minimum of 10 and a maximum of 43 VHT members being selected from each sub-county. For the key informants, the DHE and all the six VHT subcounty supervisors were interviewed. Within the community, 8 to 12 men and women were selected in each subcounty for inclusion into the focus group discussions.
1.2.3 Data Collection
Quantitative data among the VHTs was collected using a semi-structured questionnaire while qualitative data was collected using key informant and FGD guides. The key informant guide collected information from the District health education officer and VHT supervisors while the FGD guides collected information from community members in the general population.
The semi-structure VHT questionnaire: This questionnaire will include both close ended and open ended questions that will be posed to selected VHT members within the six sub-counties. The questionnaire will assess the knowledge and practices of VHT members and will include questions on the following

3
i HIV/AIDS knowledge and awareness;
ii Knowledge, attitudes and behaviors related to HIV testing and counseling (including couple counseling and testing);
iii Knowledge and practices about HIV care, support and treatment (both adult and pediatric);
iv Awareness, and knowledge of safe male circumcision;
v Knowledge about alcohol use;
vi Knowledge of family planning methods;
vii Gender norms;
viii Knowledge related to gender based violence;
ix Roles of VHT members; and
x Current practices in terms of training and holding of planning meetings
1.2.4 Data management and analysis Quantitative data analysis: The study collected data on a wide range of variables, including continuous, binary and ordinal variables and therefore univariate and bivariate analyses were conducted. To test changes in the knowledge, simple test of proportions were used. Only differences with p of 0.05 or less were considered statistically significant and treated as such in the analysis.
Qualitative analysis: Interview transcripts were analyzed by employing an iterative process of qualitative textual analysis. Open coding was utilized to code initial interviews by identifying and labeling discrete units of text that refer to one or more domains relevant to the key topics. Content of and appropriate names for the different concepts and working codebook of primary domains and emerging themes were developed.

4
2.0 Findings
2.1 Quantitative findings
2.1.1 Number of VHT respondents interviewed From table 1 below, the distribution of VHT was almost equal across all the sub counties at both of the data collection points. At the baseline, Goma had the least VHTS with 13% (30) of the VHTs interviewed while Nama had the most with 20% (46) of the VHTs interviewed. At the follow up study, there was a loss to follow up of 16 percent with 36 VHTs who were interviewed at the baseline not interviewed at follow up. In regard to VHT distribution at follow up, Ntenjeru subcounty had the least with 13% (25), while Nakisunga had the most VHTs (20 percent). In terms of loss to follow up, Nama had the highest number of VHTs interviewed at the baseline and were not interviewed at follow up. This report includes 182 unique VHT members who were interviewed both at baseline and follow up.
Table 1: Percentage distribution of VHTs interviewed by sub-county
Subcounty Pre-RDL (n=230)
Post-RDL (n=1941)
Goma 13 17 Kimenyedde-Nabaale 18 18 Nagojje 15 18 Nakisunga 19 20 Nama 20 14 Ntenjeru 16 13
Total 100 100
2.1.2 Knowledge of VHT roles in the community Knowledge of VHT roles among VHT members helps them understand their responsibilities within the communities so that they help in improving the health of the communities in which they work. During this evaluation study and between the two survey rounds, VHTs were spontaneously asked what roles the VHTs played in the community. Results indicate that the level of knowledge of at least three roles played by VHTs increased from 19% to 32% between the two data collection points. Notably, the most known role for VHTs was mobilization of the community which was mentioned by 63 and 83 percent at baseline and follow up respectively. It seems, most of the VHTs do not see record keeping as their responsibilities as it was least mentioned by six and eleven percent of the respondents at baseline and follow up respectively. However, the percentage of VHTs who did know the VHT roles decreased between the two periods from eleven percent before implementation of the RDL program to three percent at follow up after implementation of the program. For details please see table 2 below.
1 Only 182 unique VHT members interviewed both at baseline and follow up are included in this report.

5
Table 2: Percentage distribution of knowledge of VHT roles among VHT respondents
VHT Roles Baseline Follow up Keeping records 6 11 Saving lives 38 37 Mobilizing the community 63 83 Supporting people with problems 38 48 Role models in the community 16 36 Knows at least three VHT roles 19 32 Do not know any VHT roles 11 3
2.1.3 Knowledge of family planning One major objective of this evaluation study was to assess the change in level of knowledge of family planning among the VHTs enrolled into the VHT RDL program. Generally, when VHTs have increased and adequate knowledge and information about family planning, in turn they will convey correct family planning messages among their target communities and individuals. This will in turn help the communities and individuals to be able to develop a rational approach to use of family planning services. During the survey rounds, a series of questions were asked about the knowledge of family planning. Results indicate that knowledge of at least three benefits of family planning almost doubled from 22% at baseline to 40% at follow up. Similarly, the proportion of VHTs who did not know any benefit of family planning drastically dropped to 0 percent at follow up down from six percent at baseline. During the same survey, VHTs were asked about knowledge of long term acting and permanent contraceptive methods (LAPM). Results indicate that knowledge of all the four LAPM methods increased five fold from two percent upward to eleven percent at follow up. The most commonly mentioned LAPM method at baseline was female sterilization (45%) while at follow up it was IUD (87%). The least LAPM method was male sterilization at both survey rounds mentioned by 25 and 35 percent of the interviewed VHTs. For details see table 3 and figure 1 below. Table 3: Percentage distribution of Knowledge of long and acting family planning methods among VHTs
Methods Baseline Follow up IUD 41 87 Implants 41 59 Female sterilization 45 44 Male sterilization 25 35 Knows all four LAPM methods 2 11

6
9
2218
11
20
40
2
36
11
05
1015202530354045
Does not knowany benefits of
FP
Knows at least3 benefits of
FP
Does not knowany LAPMmethods
Know at least 3LAPM methods
Knows all 4LAPM methods
Knowledge of benefits of familyplanning
Knowledge of long acting and permanent familyplanning methods
Perc
ent
BaselineFollow up
Figure 1: Knowledge of benefits of family planning and long term acting and permanent family planning methods
2.1.4 Knowledge of HIV among VHTs One of the key activities for VHTs is to provide HIV prevention, care and treatment information to the general community. During this evaluation, the VHT members were asked both at baseline and follow up questions concerning knowledge of HIV prevention, care and treatment. In particular, VHT members were asked whether they knew the benefits of HIV testing, key practices couples should do to prevent infecting each other with HIV, and whether they know the key signs that could signify that children below 5 years had HIV. With regard to knowledge of benefits of testing for HIV, results indicate that the percentage of VHTs who knew at least three benefits for HIV testing increased from 32 percent at baseline to 58 percent at follow up. The percentage of those who do not know any benefit for HIV testing dropped from 10 percent at baseline to just 1 percent at follow up. The most known benefit at both baseline and follow up was for PLHIVs to start treatment early mentioned by 54% of the VHTs, while the least known was testing reveal HIV discordance among couples mentioned by 14 percent of the VHTs at baseline and 21 percent at follow up. Similarly knowledge that pregnant women can prevent transmission of HIV to their unborn child was also the least known benefit for HIV testing at follow up. With regard to knowledge of practices that couples can do to prevent HIV transmission, when asked among VHTs, the least mentioned at both baseline and follow up was abstaining from sex by 3 and 6 percent at baseline and follow up respectively. The most known practice was consisitent and correct condom use mentioned by 89 and 90 percent of VHTs at baseline and follow up respectively. In order to measure whether there was change in knowledge between the baseline and follow up, a composite indicator was computed to find out the percentage that mentioned correctly at least three practices that couples should do to for prevention of HIV infection. Results show that knowledge of at least three practices increased from 19 percent at baseline to 30 percent at follow up. Furthermore, results indicate that the percentage of VHTs who do not know any practice that prevents HIV infection among couples dropped to just one percent at follow up from three percent at baseline. Refer to table 4 and figure 2 below for details.
7
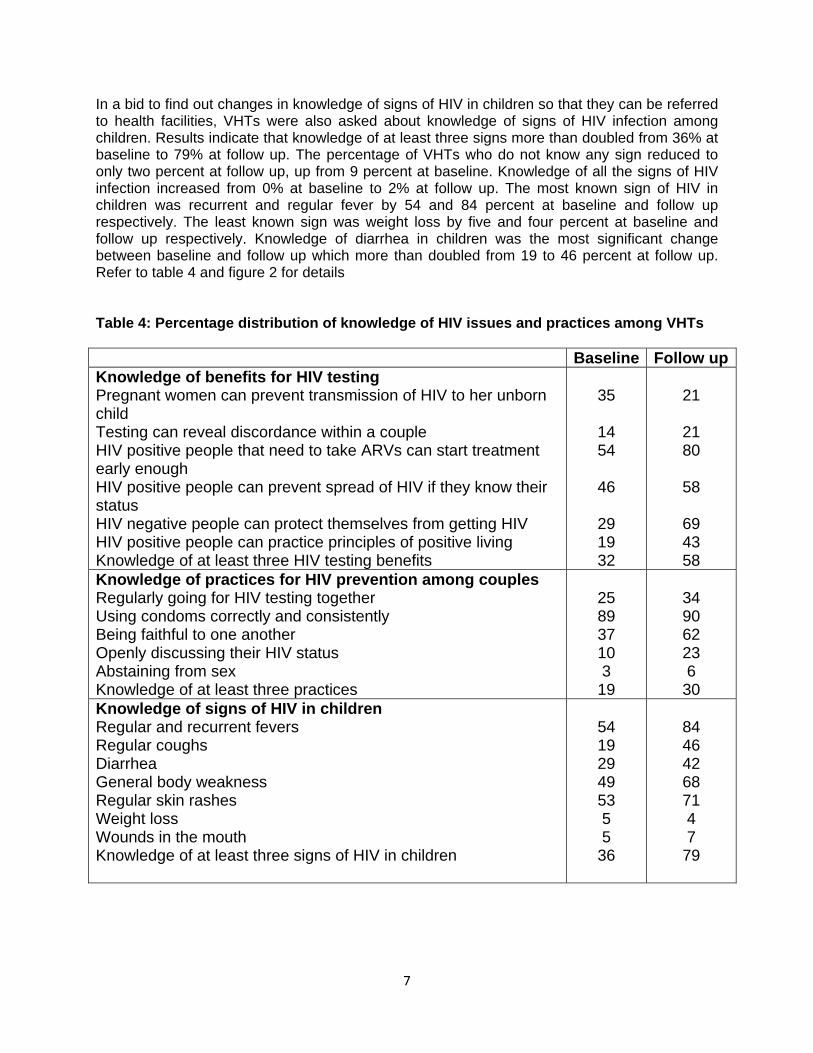
In a bid to find out changes in knowledge of signs of HIV in children so that they can be referred to health facilities, VHTs were also asked about knowledge of signs of HIV infection among children. Results indicate that knowledge of at least three signs more than doubled from 36% at baseline to 79% at follow up. The percentage of VHTs who do not know any sign reduced to only two percent at follow up, up from 9 percent at baseline. Knowledge of all the signs of HIV infection increased from 0% at baseline to 2% at follow up. The most known sign of HIV in children was recurrent and regular fever by 54 and 84 percent at baseline and follow up respectively. The least known sign was weight loss by five and four percent at baseline and follow up respectively. Knowledge of diarrhea in children was the most significant change between baseline and follow up which more than doubled from 19 to 46 percent at follow up. Refer to table 4 and figure 2 for details Table 4: Percentage distribution of knowledge of HIV issues and practices among VHTs Baseline Follow upKnowledge of benefits for HIV testing Pregnant women can prevent transmission of HIV to her unborn child Testing can reveal discordance within a couple HIV positive people that need to take ARVs can start treatment early enough HIV positive people can prevent spread of HIV if they know their status HIV negative people can protect themselves from getting HIV HIV positive people can practice principles of positive living Knowledge of at least three HIV testing benefits
35
14 54
46
29 19 32
21
21 80
58
69 43 58
Knowledge of practices for HIV prevention among couples Regularly going for HIV testing together Using condoms correctly and consistently Being faithful to one another Openly discussing their HIV status Abstaining from sex Knowledge of at least three practices
25 89 37 10 3
19
34 90 62 23 6
30 Knowledge of signs of HIV in children Regular and recurrent fevers Regular coughs Diarrhea General body weakness Regular skin rashes Weight loss Wounds in the mouth Knowledge of at least three signs of HIV in children
54 19 29 49 53 5 5
36
84 46 42 68 71 4 7
79

8
Figure 2: Importance of HIV testing, key practices to protect couples from infecting each other with HIV and signs of HIV infection among children.
2.1.5 Knowledge of key PLHIV positive practices VHT members were also asked about knowledge of key practices that PLHIVs should do to delay progression to AIDS. Results indicate that the most mentioned practice PLHIV should do at baseline was regular exercising mentioned by 71% whereas at follow up, the most mentioned practice was seeking early treatment mentioned by 91% of the VHTs. The least mentioned practice was disclosing their HIV status by 13 percent and regular exercising by 8 percent at baseline and follow up respectively. Knowledge of at least three practices increased almost two fold from 30% at baseline to 56% at follow up. Knowledge of all the six PLHIV practices to delay progression to AIDS rose from three percent at baseline to nine percent at follow up. The percentage of VHTs who do not know any practice reduced from six percent at baseline to only one percent at follow up. For details refer to figure 3.

9
Figure 3: Percentage distribution of VHT’s level of knowledge of key PLHIV positive living practices
2.1.6 Knowledge of benefits of safe male circumcision VHTs were also asked about the benefits of safe male circumcision during the survey. The least mentioned benefits at both baseline and follow up were reduction of worries during sex and improvement in cleanness of the male genitals mentioned by 8 and 14 percent of the VHTs respectively. On the other had, the most mentioned was reduction in the chances of getting HIV mentioned by 72 and 91 percent of the VHTs at baseline and follow up respectively. As can be observed in the table xx below, clearly the RDL program increased the level of knowledge of benefits for SMC among the VHTs enrolled in the program as the percentage of those who could mention all the three benefits correctly increased five fold from two percent at baseline to eleven percent at follow up.
Table 5: Percentage distribution of VHT’s knowledge of the benefits of safe male circumcision
Benefits of safe male circumcision Baseline Follow upReduces chances of getting HIV Reduces chance of getting other STDs Reduces worry during sex Improves on the cleanness of the genitals Correct knowledge of all the three benefits for SMC Do not know any benefits for SMC
72 55 8 8 2
4.4
91 73 14 14 11 1.1
2.1.7 Knowledge of violence and dangers of alcohol abuse Among the key topics covered during the radio distance learning program for VHTs was types of violence and these occur within the communities. VHTs therefore have a role in educating community members about violence and its associated dangers. Increased VHT knowledge about violence implies that the target communities where VHT operate will get accurate information and in turn reduce the prevalence of violence in the general population. During the

10
evaluation study, VHT respondents were spontaneously asked at baseline and at follow up the types of violence they knew. Knowledge of types of violence clearly increased between the baseline and follow up. For instance, knowledge of all three types of violence increased more than two fold from 11 percent to 32 percent at baseline and follow up respectively. On the other hand, the percentage of those who do not know any type of violence decreased from twelve percent to five percent at baseline and follow up respectively. The most known type of violence was physical at both baseline (74%) and follow up (83%).
Recognition of the causes, signs and dangers of alcohol abuse is one of the topics covered in the RDL program with the objective of helping the VHT members in educating their communities on the dangers of alcohol abuse. During this study VHTs were asked whether to the name the dangers of alcohol intake at the two data collection points. Results obtained indicate that knowledge of at least three dangers of alcohol abuse more than doubled from 28% at baseline (before RDL implementation) to 67% at follow up. Knowledge of all the dangers of alcohol also increased from two percent at baseline to four percent at follow up. The percentage of the VHTs who did not know any danger of alcohol intake reduced from six percent at baseline to just two percent at follow up. Furthermore, the most mentioned consequence of alcohol abuse was the inability to fulfill work and domestic responsibilities mentioned by 45 and 71 percent of the VHTs at baseline and follow up respectively. For details see table 6 Table 6: Percentage distribution of level of knowledge of dangers of alcohol abuse and types of violence among VHTs
Baseline Follow up Knowledge of dangers of alcohol intake Mentioned none 6 2 Mentioned at least three 28 67 Mentioned all 2 4 Knowledge of types of violence Mentioned none 12 5 Economic 44 56 Physical 73 83 Emotional 27 57 Mentioned all 11 32
2.1.8 Self efficacy in addressing key health topics In addition to making monthly home visits to their community members, VHTs have a duty to conduct monthly sensitization meetings. In these meetings the VHTs sensitize community members about different health topics and answer any questions that arise about topics so that everyone in the community has basic knowledge concerning health. In order to determine self efficacy among VHTs in addressing health topics, VHTs were spontaneously asked at baseline and at follow up how confident they felt in addressing certain health topics with community members. The health topics included family planning, HIV prevention, HIV testing and counseling, HIV care and treatment, safe medical male circumcision, violence against women, among others. To measure self efficacy, only the VHTs that said they were very confident in addressing a given health topic were considered.

11
Results indicate that the RDL program increased self efficacy of VHTs in only two out of the eight health topics. To test the changes in self efficacy, the test of proportions was utilized. The health topics for which the self efficacy was increased were family planning; from 75% to 84% of VHT who said they were confident in addressing the topic. The other topic was HIV prevention and transmission; from 73% to 87% at baseline and follow respectively (all p-values<0.05). On the contrary, results indicate that the self efficacy for addressing violence against women decreased from 88% to 80% of the VHTs saying they were confident to address violence against women as a topic. Refer to table 7 below for details.
Table 7: Self efficacy among VHTs in addressing topics with community members before and after the RDL program
Topic Baseline Follow up
P-value
Family Planning 75 84 0.0391 Modes of HIV Transmission and Prevention 73 87 0.0011 HIV Testing 67 68 0.9110 Safe Male Circumcision for HIV Prevention 58 55 0.5972 Antiretroviral Drugs 64 67 0.5086 Stigma against PLHIV 81 83 0.6033 Causes and Dangers of Alcohol Abuse 83 80 0.5863 Violence against Women 88 80 0.0329
2.1.9 VHT perception about the effectiveness of the RDL program The RDL program used different components in helping VHTs acquire accurate and consistent health information. These include the weekly radio episodes that aired twice every week, a listener`s guide that contains questions about health topics being discussed in the episodes and the listening groups that were made up of the VHTs enrolled into the weekly radio program. During the follow up survey, the program was interested in collecting information about VHT members opinion about the effectiveness of the program in providing accurate information and knowledge to VHTs. Overall, majority of the VHTs felt that the RDL program was effective for all the three elements asked; 83, 77 and 82 percent of the VHTs reporting that the weekly episodes on Radio, the listener’s guide and the listening groups were effective respectively.
Table 8: Percent distribution of VHT’s perception about the effectiveness of the RDL program
Very effective
Somewhat effective
Not effective at all
Weekly Episodes on Radio 83 14 3 Listener`s Guide 77 17 6 Listening Groups 82 11 7

12
2.1.10 VHT recommendation for future programming purposes
The VHTs were also asked whether the timing of the program was conducive for all the VHTs to listen in and all those that said it was not were further asked to recommend different time for future programming purposes. Results indicate that seventy percent of the VHTs said the timing was conducive. The most recommended time for those that said it was not conducive was 4:00pm mentioned by 33% followed by 8:00pm which was mentioned by 26%.
The radio program also aired twice every week and the VHTs were asked whether these two slots were enough. Majority of them (84%) said that the two slots were enough. Only 16% said the slots were not enough.
The VHTs were also expected to listen in to the program in groups and each of these groups had a leader. The VHTs were asked to rate the competence of these leaders. Results indicate that seventy percent of the leaders were very competent, twenty six percent of the leaders were somewhat competent and only four percent of the leaders were not competent at all.
Relevance of topics that were discussed during the RDL Program
Different health topics were discussed on the radio program in order for the VHTs to gain more information about each of the topics. The VHTs were asked to rate the relevance of each topic that was discussed. Results show that all the topics were very relevant. However the most relevant topics were benefits of HIV testing and causes and dangers of alcohol abuse with 91% of the VHTs saying that they were very relevant. For details refer to figure xx
very relevant somewhat relevant not relevant at all
Figure 4: VHT’s perception of the relevancy of the health topics covered

13
Average number of home visits and referrals for VHTs
The VHTs were asked how many people on a monthly basis they refer to the health centres, how many home visits they make per month and the number of sensitization meetings they carry out. Results indicate that the average monthly numbers for referrals, home visits and sensitization meetings were 7.4, 14.4 and 1.3 respectively at baseline. However at follow up the average monthly numbers did not change much as the average monthly numbers for referrals home visits and sensitization meetings were 7.5, 15.1 and 1.4 respectively. The similarity in number of home visits, referrals and sensitizations made between the baseline and follow up may have been due to the short time period between pre implementation and post implementation and the fact that the program did focus on the number of activities VHT had to do but rather providing them with accurate knowledge.
Table 9: Average number of home visits, referrals and sensitization meetings per month among VHTs
Baseline Follow up
Average monthly refferals made 7.4 7.5
Average home visits per month 14.4 15.1
Average sensitization meetings per month 1.3 1.4

14
2.2 Qualitative findings
This section highlights an analysis of focus group discussion findings from the six sub counties in Mukono district, conclusions and recommendations.
2.2.1 Key Health Concerns/Problems in the Community The respondents were asked about the key health concerns/problems they face in the community as a way of introducing the key study topics. Findings show that community members consider malaria, malnutrition, common colds, cough and HIV as their key health problems. Other health concerns mentioned include drug stock outs, lack of clean water, poor disposal of waste resulting into poor hygiene and sanitation, lack of drugs in health units, lack of adequate health information and sensitization on health matters among others.
“Scarcity of water is a big problem with few wells and people have to make long queues to access water. The other problem we have is that whenever it rains the water in our wells gets dirty because it is not protected thereby spreading diseases” (Male Respondent, Naama).
“We don’t have drugs in our health centres and hospitals yet VHTs don’t have a solution for this problem” (Female Respondent, Nagojje)
Malaria featured prominently as one of the key health problems accounting for high levels of morbidity with many households lacking insecticide treated mosquito nets coupled with lack of drugs at the health facilities.
“Many of us here suffer from malaria because we do not have mosquito nets to protect us. You may be suffering from malaria but when you visit a health unit; health workers will refer you to pharmacies to buy medicine” (Female Respondent, Kimenyedde)
2.2.2 Current sources of health information Understanding sources of information for the target population is important for any program that implements health interventions. Results show that interpersonal communication (involving VHTs, health workers, local leaders, peer educators) and radio are the most common sources of health information.
Specifically VHTs were mentioned as a key source of information because they conduct home visits giving information on a number of health issues and making appropriate referrals. VHTs and health workers were also viewed as key health information sources because face to face communication with them was interactive and was followed by instant feedback as indicated in the quote below:
“Generally we get health information through VHTs and health workers in that they are able to sensitize us on key health issues and allow us to ask questions there and then” (Female Respondent, Seeta –Nazigo)
However, female respondents in Naama Sub County indicated that access to health information by the community was still a problem due to scarcity of health personnel inspite of the existence of VHTs in the

15
community. Among male respondents in the same Sub county, only one community member mentioned VHTs as the main source of health information.
Radio was mentioned as the second most important source of health information with talk shows and radio spots promoting key health practices mainly malaria prevention by sleeping under ITNs and use of family planning. Majority of participants who happen to be regular radio listeners acknowledged Radio Simba and Dunamis for having a number of health talk shows and radio spots that air regularly although the ‘Obbanywa’ drama series were not mentioned at this point.
I hear a number of health programs and adverts about sleeping under mosquito nets and family planning on Radio Simba and Dunamis. (Male Respondent, Naama)
2.2.3 Roles of the Village Health Teams (VHTs) Since the Ministry of Health VHT strategy is aimed at ensuring that every village in Uganda has VHTs who work together to mobilize individuals and households for better health, it was important for this study to assess whether community members understood VHT roles. Majority of the respondents had a clear understanding of the roles VHTs play in relation to improving their health status. The key roles mentioned include sensitization and mobilization of the communities on health issues, essential drug distribution, mobilization for immunization, provision of counseling, referral and reporting disease outbreaks.
“VHTs sensitize us about hygiene and sanitation, how to prevent malaria, the importance of constructing latrines, utensil drying stands and kitchens (Female Respondent, Seeta-Nazigo)
Regarding essential drug distribution in the community, VHTs are currently playing a key role syndromic management of malaria by distributing and prescribing drugs to people with malaria signs. The Ministry of Health and other partner organizations have been supplying malaria drugs (tablets) to VHTs for distribution to manage and control malaria at the grass roots. A male participant of Bukerere in regard to that role said that,
“What I know about those VHTs is that they supply malaria drugs to children. When a child gets sick of malaria, the VHT will come immediately to provide treatment” (Male Respondent, Bukerere)
VHTs have been active in mobilizing communities to adopt other healthy practices like immunizing their children from six killer diseases and utilizing modern family planning methods.
“Every time the Ministry of Health announces the child days plus immunization campaign, I see VHTs moving from household to household encouraging families with young children to take them for immunization”. (Female Respondent, Nagojje)
“They have been sensitizing us about the dangers of bearing so many children and encouraging us to consider using modern contraceptives” (Female Respondent, Seeta Nazigo)

16
Respondents in Naama Sub County however noted that some VHTs were old and hence find it quite difficult to make good use of some of the equipment supplied to facilitate their operations which require physical strength such as bicycles.
The findings also show more women than men were most likely to report that they had been visited by a VHT in the last three months. This could be explained by the fact that more men than women spend a lot of their time out of the household during the day since they are normally the bread winners.
During their visits, the Village Health Teams are reported to have sensitized the communities on general cleanliness of homes, malaria prevention using of mosquito nets and how to treat malaria.
2.2.4 Listenership to “Obbanywa” RDL Program In order to assess the effect of the radio distance learning program on the general population, respondents were asked whether themselves or their peers had listened to the drama series that aired on a local FM station called Radio Dunamis between July and October 2011. Only a few community members reported to have listened to the program on Radio Dunamis. The main reasons advanced for not listening to the drama series were that Radio Dunamis was not one of their favorite radio FM stations, it was faith based, in some areas its signal was poor and that no community promotional activities were conducted before airing the program.
“Some of us do not listen to Radio Dunamis because we consider it to be a station for born again Christians yet we are not” (Male Respondent, Nagojje)
“Dunamis is not reliable, the signal is not stable sometimes it is and other times it is off” (Female Respondent, Seeta-Nazigo).
“First of all we were not informed about the program before its airing; secondly people listen to different programs on different radio stations. If people do not know that Radio Dunamis has a program at a given time on a given day they will not listen to it” (Male Respondent, Ntenjeru)
A few more respondents intimated that they were able to listen to the program on Radio Simba because it has interesting programs, a good signal and a wide coverage.
“We listen to Radio Simba, and majority of the people here listen to Simba because of their interesting programs” (Female Respondent, Seeta Nazigo).
These findings clearly show that listenership to a health program is mainly influenced by the popularity of the radio station, the strength of the signal, community awareness about the program and its coverage.
2.2.5 Knowledge about Program Content, Frequency of Listening and Rating
Community members who had listened to the program before were asked to mention some of the topics discussed in the drama series, frequency of listening, their rating of the program and some of the key messages they recalled. Family planning, HIV prevention and the roles of VHTs were the only topics mentioned. One respondent who had listened to the program had this to say;

17
“In Obbanywa I heard about family planning, they also talked about the methods of family planning like using injections, pills, condoms and others” (Male Respondent, Nagojje)
Other topics like safe male circumcision, anti retroviral therapy, HIV stigma, dangers of alcohol abuse and violence against women were not mentioned by any of the respondents.
2.2.6 Timing of the Program
The ‘Obbanywa’ program aired on Radio Dunamis every Sunday at 2.00pm with a repeat every Thursday at 11.00am. Majority of the respondents found Sunday afternoon convenient for them to tune in whereas the timing for Thursday was considered to be unfavorable because many would be listeners are preoccupied with work. Below are some of their comments;
“As a market vendor, Sunday afternoon is good timing for me because I have already come back from church and just relaxing at home, whereas Thursday morning there are many customers that I am attending to. I think a repeat of the program should be aired in the evening for example from 7:00 pm onwards” (Female Respondent, Seeta-Nazigo).
“Airing the program on Thursday morning is wrong timing because most of us are working and have little time to tune in. If it could be changed to about 8:00 pm or any time after then many of us can tune in since we are back home“ (Male Respondent, Nagojje)
2.2.7 Program Presentation
The way a radio health program is presented influences listener`s interest in the topics presented and health practices being promoted. The radio distance learning program used serial drama with 13 episodes that were aired over a period of 3 months. Each episode tackled a different topic in a dramatized format allowing listeners to be intimately engaged in the lives of the characters featured. The drama series used real life scenarios, examples and challenges that communities are faced with and combined them with key health messages on family planning, HIV testing, safe male circumcision, and violence against women among others. Community members who had listened to the program described it as very interesting, engaging and not boring as shown by one of the quotes below;
“I loved listening to the program because it had a lot of drama which made it interesting. I do not remember ever getting bored” (Male Respondent, Nakifuma)

18
3.0 Conclusion and recommendations
3.1 Conclusions
This evaluative study was designed to assess the effectiveness of the RDL program in improving the skills and knowledge of VHTs. The other objective was to establish the reach and effects of the RDL program among the general population beyond the VHT members. Results of the evaluative study are to be used in planning, refining as well as replicating the RDL program in other districts of Uganda.
Findings of this evaluative study indicate that the RDL program clearly increased the knowledge of VHTs who participated in the program as knowledge in all the health topics addressed increased from the baseline to follow up post implementation of the RDL program. However, the focus group discussions showed that there was a very low reach of the radio program among the general population.
Knowledge of VHT roles in the community increased almost two fold with most VHTs knowing community mobilization as their key role. Benefits of family planning knowledge also doubled from baseline to follow up. Notably, knowledge of all four long term methods increased five fold from 2 to 11%, with the level of knowledge of IUD improving the most between the two survey rounds.
In regard to HIV prevention knowledge, similar trends were observed with the knowledge of at least three benefits of HIV testing doubling, knowledge of practices that couples need to undertake to prevent HIV infection increasing by 11%, with the most mentioned practice being use of condoms consistently and correctly. Knowledge of key PLHIV positive practices also increased but knowledge of exercising as a key PLHIV positive practice decreased from baseline to follow up. Other health topics were there was an observed increase in level of knowledge included benefits of safe male circumcision, violence against women and the dangers of alcohol abuse.
Whereas there was increase in knowledge of all the health topics included in the RDL program, this evaluation showed that for self efficacy among VHTs to deliver messages to the communities was in the reverse direction or did not change at all. In addition no changes were observed in the number of home visits, referrals and sensitization meetings undertaken by the VHTs as a result of the RDL program. The probable explanation to this could have been the short time period between the start and completion of the program and maybe most VHTs took off the time for the other activities to attend to the RDL program.
Among the general population, results indicated that the general reach was very low as few community members who were interviewed reported to have listened to the program partly because the radio used was not their favorite FM radio stations, its signal was poor in some areas and that no community promotional activities were conducted before airing the program. The few community members who had listened to the program described it as very interesting, engaging and not boring.

19
3.2 Recommendations
• A very small percentage of VHTs viewed record keeping at one of the key roles they play. Future programs need to emphasis record keeping as a key role in addition to other roles mentioned in the program. One way would be to include more time about record keeping as well as including extra exercises about record keeping.
• Study findings clearly show that listenership to a health program is greatly influenced by the popularity and listenership of the chosen radio station, the strength of the signal, and its coverage. For future RDL programming purposes, there is need to use media monitoring statistics from Synovate Uganda (formerly Steadman Group) to choose radio stations with high listenership rates and wider coverage.
• There is need to conduct community promotional activities in order to raise community awareness and interest in future RDL programs before their launch.
• Given the success of the program in increasing the knowledge of VHTs as observed in this evaluative study, such interventions should be scaled up in order to build the capacity of VHTs to reach more individuals and households with accurate health information and ensure proper linkage to health services.
• Well as there was increase in knowledge across all the health topics, the results showed that knowledge of dangers of alcohol abuse (4%), knowledge of long term family planning methods (11%) and the knowledge of benefits of SMC (11%) is still low. Future RDL programs need to review the content and place more emphasize on these health topics so as to increase the levels of knowledge among the VHTs.
• The timing of the program on Sunday afternoon 3.00pm should be maintained whereas a repeat of the program during week days should be shifted from morning to evening hours to have more listeners tuned in.
• During the discussions, messages about HIV/AIDS prevention and family planning were the most frequently recalled by respondents who listened to Obbanywa whereas other key health topics including safe male circumcision, anti retroviral therapy, HIV stigma, dangers of alcohol abuse and violence against women did not feature any where. There is need to re-emphasize these messages on radio and distribution of relevant IEC materials.
• The RDL program did not increase the self efficacy of the VHTs in addressing the key health issues and therefore future RDL programs need to include modules or exercises that can increase their self efficacy in addressing the topics covered by the programs.
• Lastly, future evaluative studies need to include more in depth interviews with selected VHT members who listened and fully participated(by doing the exercises) in the radio program to get a better and deeper understanding of the effectiveness of the training materials used so as to improve on the training materials. This was outside the scope of the evaluative study.

Appendices: Data collection tools
OBBANYWA: RADIO DISTANCE LEARNING POST TEST ASSESSEMENT TOOL FOR VHTs
Interviewer’s Name_______ ________ Date of interview ________________________
District_________________ Sub county___________________ ____
Parish__________ ______________ Village__________________ ______
SECTION A: VHT Knowledge on Health Issues
Question Response 1. What are the roles of a VHT in the
community?
Keeping records………………………………..….1 Saving lives…………………………………….……..2Mobilizing the community……………….……3 Supporting people with problems…….…..4Role models in the community……………..5Others(specify)……………………………………..6
2. Should men be involved in family planning? Yes……………………………………..…….………….1
No………………………….…………….…….………..2
3.
What are the benefits of family planning (CIRCLE ALL THAT ARE MENTIONED)
Gives the mother enough time to recover from previous pregnancy……………………..1 Some methods protect from STDs/HIV…2 Allows mother to breastfeed fully….……..3There is more money for the family……..4 Reduces worry and overwork……………….5 Children enjoy fill love from parents…….6 Other (specify)………………………….………….7

21
4. What long acting and permanent family planning methods do you know? (CIRCLE ALL THAT ARE MENTIONED)
IUD‐Coil………………………………..….………….1 Implants………………………………..….………...2 Tubal Ligation………………………..…………….3 Vasectomy……………………………..……………4 Others (specify)……………………………………5
5. What is the difference between HIV and
STDs? (CIRCLE ALL THAT ARE MENTIONED)
HIV has no cure but some types of STDs can be treated if found early………………1 A person suffering from STDs has a high chance of contracting HIV………………….2 Many of the ways of preventing sexual transmission of HIV and STDs are similar……..3 All people suffering from STDs are advised to go for early treatment to reduce chances of getting HIV……..……..4 Don’t know………………………………………….5
6. Why is it important for everyone to go for HIV
testing in your community?
A pregnant woman can prevent transmission of HIV to her unborn child………………………………………..………..…1 Testing can reveal discordance within a couple………………………………………………….2 An HIV positive person that needs to be on ARVs can start treatment early enough……………………..………..………….…….3An HIV positive person can prevent spread of the virus to others if they know their status…………………….……………….……4 An HIV negative person can protect themselves from getting the diseases……………………………….……….…….5 An HIV positive person can practice principles of positive living…………………..6
Others (specify)………………………………….7

22
7. Is it possible for a couple to have different HIV statuses?
Yes……………………………………………………1 No…………………………………………………….2
8. What are the practices couples should do
together to protect from infecting each other from HIV infection? (CIRCLE ALL THAT ARE MENTIONED)
Regularly going for HIV testing together ………………………………………………………….…1 Using condoms correctly and consistently………………………………………….2 Being faithful to one another……….………3 Openly discussing their HIV status……….4 Others (Specify)………………..…………….…..5 Don’t know……………….………………………….6
9. What are the types of violence in your community? (Circle all that are mentioned)
Physical violence………….………..…………….1 Emotional Abuse……..……………..……………2 Economic abuse………..…………..…………….3 Don’t know………………………………..………...4Others (specify)…….……………………………..5
10. What are the key practices that PLHIV should
do to delay the progression to AIDS?
Eating nutritious foods………………….……..1 Disclosing their HIV status………..…….……2 Joining support groups…………………………3 Regularly exercising ……….…………………..4 Seeking early treatment ………….………….5 Practicing safe sex………………….……………6 Others (specify)…………………………………..7 Don’t know………………………………………….8
11. Can a person taking ARVs still transmit HIV?
Yes………………………………………………..…….1 No…………………………………………….…………2
12. What are the benefits of medical male circumcision
Reduces chances of getting HIV…………..1 Reduces chance of getting other STDs.…2 Reduces worry during sex…………….………3 Other (specify)……...................................4 Don’t know……..…………………………………..5
13. If a man is circumcised is he still at risk of Yes……………………..……….……………………….1

23
getting HIV?
No………………………………..………………………2
14. What are the short and long term dangers of taking alcohol?
Inability to fulfill work and domestic responsibilities ………………………………..…..1Deterioration of one’s health…………….…2 Increased chances of getting HIV……….…3 Can cause you to make bad choices……..4 abuse of your spouse or partner…………..5 Others (specify)………..…………………………6 Don’t know………………………………………….7
15. Should children with HIV be given ARVs? Yes……………………………………..………..……….1No………………………………….……………..………2
16. What are the signs that a child could be infected with HIV?
TB……………………………………..………...……...1 Regular and recurrent fevers………..….…..2Regular coughs……………………………………..3Diarrhea……………………………………….……..4 General body weakness………………..………5Regular skin rashes……………………..…..…..6 Others(specify)…………………………..…..……7 Don’t Know…………….………………………….…8
17. I would like you to tell me how confident you feel in addressing the following topics with community members in your village; Please note that I’m only asking you to tell me whether you can address the topics it or not. I’m not asking you whether you actually do it or not.
Interviewer: First read the statement and then ask:
Would you say you are: Very confident, Somewhat confident, Or Not confident at all in addressing this topic?
Very confiden
t
Somew
hat con
fiden
t
Not con
fiden
t at a
ll
Not sure/ Refused
Family Planning 3 2 1 0
Modes of HIV Transmission and Prevention 3 2 1 0
Benefits of HIV Testing 3 2 1 0

24
Importance of Couple HIV Counselling and Testing 3 2 1 0
Safe Male Circumcision for HIV Prevention 3 2 1 0
Antiretroviral Drugs 3 2 1 0
Stigma against PLHIV 3 2 1 0
Causes and Dangers of Alcohol Abuse 3 2 1 0
Violence against Women 3 2 1 0
18. I would like you to tell me how effective the different materials/components of the Radio Distance Learning program were in helping you acquire accurate and consistent health information as a VHT.
Interviewer: First read the statement and then ask:
Would you say this material/component was very effective, somewhat effective or not effective at all?
Very Effective
Somew
hat E
ffective
Not Effective
at a
ll
Weekly Episodes on Radio 3 2 1
Listener`s Guide 3 2 1
Listening Groups 3 2 1
19. As you might be aware, the Radio Distance Learning program also known as OBBANYWA has been airing every Sunday at 3.00pm on Rhino FM with repeats on Tuesday at 8.00pm for the last four months. Was the timing of the program conducive for you to listen in?
Yes...............1 No................2
2→Q21
20. What time would you recommend for future programming purposes?
Time of the day: ....................
21. OBBANYWA has been airing twice every week (Sunday and Tuesday). Are these slots enough?
Yes..................................1No...................................2

25
22. How would you rate the competence of the leaders of
OBBANYWA listening groups?
Very competent.............1 Somewhat competent....2 Not competent at all......3
23. I would like to get your views on the topics that were discussed on OBBANYWA over the last four months and how they relate to your role as a VHT.
Interviewer: Read the name of the topic below and then ask; Would you say this topic was very relevant, somewhat relevant or not relevant at all?
Very Relevant
Somew
hat
Not Relevant a
t all
Family Planning 3 2 1
Modes of HIV Transmission and Prevention 3 2 1
Benefits of HIV Testing 3 2 1
Importance of Couple HIV Counselling and Testing 3 2 1
Safe Male Circumcision for HIV Prevention 3 2 1
Antiretroviral Drugs 3 2 1
Stigma against PLHIV 3 2 1
Causes and Dangers of Alcohol Abuse 3 2 1
Violence against Women 3 2 1
SECTION B: VHT Situational Analysis and Practices
24. What are your current sources of knowledge/ information on health issues in your village?
………………………………………………………………………………………………
………………………………………………………………………………………………
25. How many people do you send to the health centre every month?……………………
26. How many homes do you visit as a VHT per month……………………………….
27. How many sensitization meetings do you carry out as a VHT every month? ……………………
26
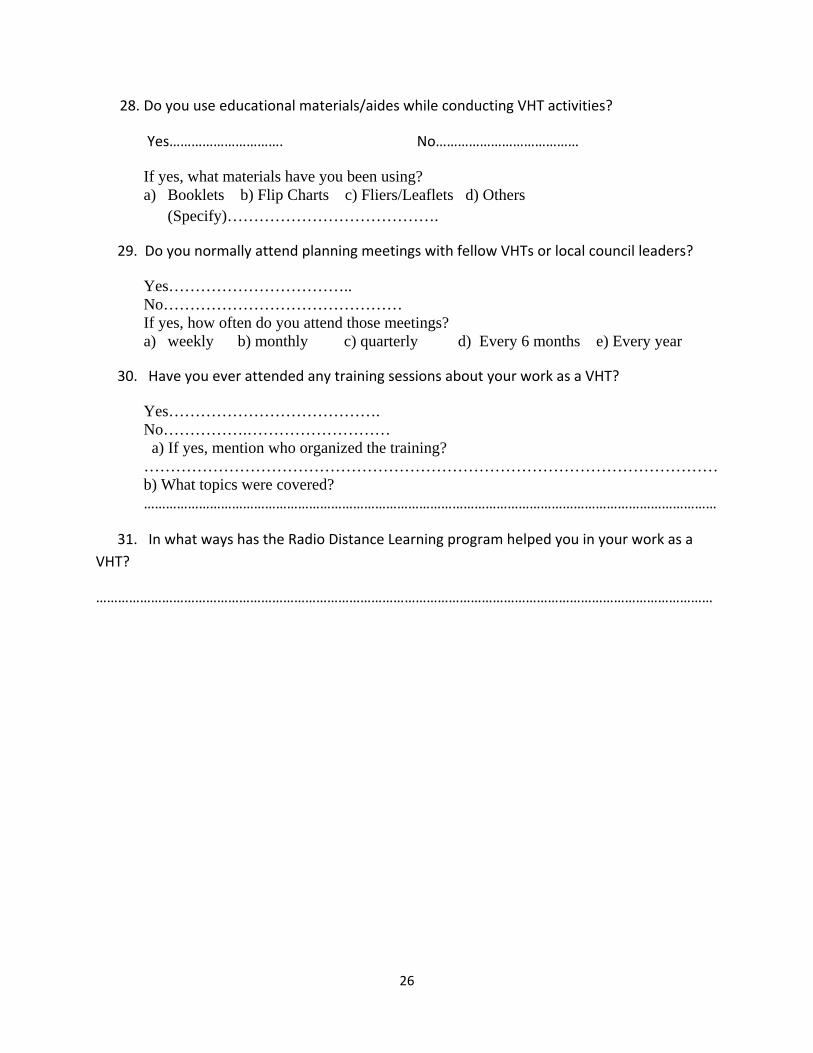
28. Do you use educational materials/aides while conducting VHT activities?
Yes…………………………. No…………………………………
If yes, what materials have you been using? a) Booklets b) Flip Charts c) Fliers/Leaflets d) Others
(Specify)………………………………….
29. Do you normally attend planning meetings with fellow VHTs or local council leaders?
Yes…………………………….. No……………………………………… If yes, how often do you attend those meetings? a) weekly b) monthly c) quarterly d) Every 6 months e) Every year
30. Have you ever attended any training sessions about your work as a VHT?
Yes…………………………………. No…………….……………………… a) If yes, mention who organized the training? ……………………………………………………………………………………………… b) What topics were covered? …………………………………………………………………………………………………………………………………………
31. In what ways has the Radio Distance Learning program helped you in your work as a VHT?
……………………………………………………………………………………………………………………………………………………

27
OBBANYWA: RADIO DISTANCE LEARNING PRE TEST ASSESSEMENT TOOL FOR VHTs
Interviewer’s Name_______ ________ Date of interview ________________________
District_________________ Sub county___________________ ____
Parish__________ ______________ Village__________________ ______
SECTION A: VHT Knowledge on Health Issues
Question Response 1. What are the roles of a VHT in the
community?
Keeping records………………………………..….1 Saving lives…………………………………….……..2 Mobilizing the community……………….……3 Supporting people with problems…….…..4 Role models in the community……………..5 Others(specify)……………………………………..6
2. Should men be involved in family planning? Yes……………………………………..…….………….1
No………………………….…………….…….………..2 3.
What are the benefits of family planning (CIRCLE ALL THAT ARE MENTIONED)
Gives the mother enough time to recover from previous pregnancy……………………..1 Some methods protect from STDs/HIV…2 Allows mother to breastfeed fully….……..3 There is more money for the family……..4 Reduces worry and overwork……………….5 Children enjoy fill love from parents…….6 Other (specify)………………………….………….7
4. What long acting and permanent family planning methods do you know? (CIRCLE ALL THAT ARE MENTIONED)
IUD‐Coil………………………………..….………….1 Implants………………………………..….………...2 Tubal Ligation………………………..…………….3 Vasectomy……………………………..……………4 Others (specify)……………………………………5
5. What is the difference between HIV and
STDs? (CIRCLE ALL THAT ARE MENTIONED)
HIV has no cure but some types of STDs can be treated if found early………………1 A person suffering from STDs has a high

28
chance of contracting HIV………………….2 Many of the ways of preventing sexual transmission of HIV and STDs are similar……..3 All people suffering from STDs are advised to go for early treatment to reduce chances of getting HIV……..……..4 Don’t know………………………………………….5
6. Why is it important for everyone to go for HIV
testing in your community?
A pregnant woman can prevent transmission of HIV to her unborn child.…1 Testing can reveal discordance within a couple………………………………………………….2 An HIV positive person that needs to be on ARVs can start treatment early enough…….3An HIV positive person can prevent spread of the virus to others if they know their status…………………….…………………..……….……4 An HIV negative person can protect themselves from getting the diseases……….5An HIV positive person can practice principles of positive living…………….………..6
Others (specify)…………………….…..…………….7
7. Is it possible for a couple to have different HIV statuses?
Yes……………………………………………………1 No…………………………………………………….2
8. What are the practices couples should do
together to protect from infecting each other from HIV infection? (CIRCLE ALL THAT ARE MENTIONED)
Regularly going for HIV testing together .…1 Using condoms correctly and consistently………………………………………….2 Being faithful to one another……….………3 Openly discussing their HIV status……….4 Others (Specify)………………..…………….…..5 Don’t know……………….………………………….6
9. What are the types of violence in your community? (Circle all that are mentioned)
Physical violence………….………..…………….1 Emotional Abuse……..……………..……………2 Economic abuse………..…………..…………….3 Don’t know………………………………..………...4 Others (specify)…….……………………………..5
10. What are the key practices that PLHIV should Eating nutritious foods………………….……..1

29
do to delay the progression to AIDS?
Disclosing their HIV status………..…….……2 Joining support groups…………………………3 Regularly exercising ……….…………………..4 Seeking early treatment ………….………….5 Practicing safe sex………………….……………6 Others (specify)…………………………………..7 Don’t know………………………………………….8
11. Can a person taking ARVs still transmit HIV?
Yes………………………………………………..…….1 No…………………………………………….…………2
12. What are the benefits of medical male circumcision
Reduces chances of getting HIV…………..1 Reduces chance of getting other STDs.…2 Reduces worry during sex…………….………3 Other (specify)……...................................4 Don’t know……..…………………………………..5
13. If a man is circumcised is he still at risk of getting HIV?
Yes……………………..……….……………………….1 No………………………………..………………………2
14. What are the short and long term dangers of taking alcohol?
Inability to fulfill work and domestic responsibilities ………………………………..…..1 Deterioration of one’s health…………….…2 Increased chances of getting HIV……….…3 Can cause you to make bad choices……..4 abuse of your spouse or partner…………..5 Others (specify)………..…………………………6 Don’t know………………………………………….7
15. Should children with HIV be given ARVs? Yes……………………………………..………..……….1 No………………………………….……………..………2
16. What are the signs that a child could be infected with HIV?
TB……………………………………..………...……...1 Regular and recurrent fevers………..….…..2 Regular coughs……………………………………..3 Diarrhea……………………………………….……..4 General body weakness………………..………5 Regular skin rashes……………………..…..…..6 Others(specify)…………………………..…..……7 Don’t Know…………….………………………….…8

30
I would like you to tell me how confident you feel in addressing the following topics with community members in your village; Please note that I’m only asking you to tell me whether you can address the topics it or not. I’m not asking you whether you actually do it or not.
Interviewer: First read the statement and then ask:
Would you say you are: Very confident, Somewhat confident, Or Not confident at all in addressing this topic?
Very con
fiden
t
Somew
hat con
fiden
t
Not con
fiden
t at a
ll
Not sure/ Refused
Family Planning 3 2 1 0
Modes of HIV Transmission and Prevention 3 2 1 0
Benefits of HIV Testing 3 2 1 0
Importance of Couple HIV Counselling and Testing 3 2 1 0
Safe Male Circumcision for HIV Prevention 3 2 1 0
Antiretroviral Drugs 3 2 1 0
Stigma against PLHIV 3 2 1 0
Causes and Dangers of Alcohol Abuse 3 2 1 0
Violence against Women 3 2 1 0
SECTION B: VHT Situational Analysis and Practices
1. What are your current sources of knowledge/ information on health issues in your village?
………………………………………………………………………………………………
………………………………………………………………………………………………
2. How many people do you send to the health centre every month? ………………………
3. How many homes do you visit as a VHT per month? …………………………………….
4. How many sensitization meetings do you carry out as a VHT every month? …………………

31
5. Do you use educational materials/aides while conducting VHT activities?
Yes…………………………. No…………………………………
If yes, what materials have you been using? b) Booklets b) Flip Charts c) Fliers/Leaflets d) Others
(Specify)………………………………….
6. Do you normally attend planning meetings with fellow VHTs or local council leaders?
Yes…………………………….. No……………………………… If yes, how often do you attend those meetings? b) weekly b) monthly c) quarterly d) Every 6 months e) Every year
7. Have you ever attended any training sessions about your work as a VHT?
Yes…………………………………. No…………….……………………… a) If yes, mention who organized the training? ……………………………………………………………………………………………… b) What topics were covered? …………………………………………………………………………………………………………………………………………

32
FGD GUIDE FOR COMMUNITY MEMBERS Date: ___________________
District___________________________Location: ___________________________
FGD Facilitator: __________________ Note Taker: _____________________
No of Respondents: ______________
INTRODUCTION: Good morning/ afternoon my name is ___________ and my colleague is ___________ we are working with Health Communication Partnership (HCP). In July 2011, HCP supported the Ministry of Health to launch a Radio Distance Learning (RDL) program for Village Health Teams (VHTs) in Mukono district. The program code named “Obbanywa” aired every Sunday at 2 pm with a repeat on Thursday at 11 am on Dunamis FM for three months (July to early October 2011). It was aimed at providing basic information on a number of health issues that affect our community. Today we are here to collect feedback from you about the program. Remember this is just a discussion and therefore there are no wrong or right answers. We therefore expect you to tell us everything you think about the program. The information you will share with us will remain confidential and only be used for research purposes.
Please speak right up but also respect others when they are talking. Some of the discussion questions will solicit information on your individual knowledge, while others will seek information on the community as a whole. As indicated in the consent form, all information shared in this group is confidential. Your full name also will not be reported in any reports resulting from this group. During this meeting, we would like to tape record the discussion and take written notes. The recording and notes are only to help us remember everything that we “hear.” Only people who are working on this project will ever hear any of the recordings or read the notes we take. Does anyone have any objections to being tape-recorded? I anticipate that this discussion will last not more than one and half hours. Is there anyone who can’t stay for this time?
. The following rules shall apply in the group:
• There are no silly questions, answers or comments.
• Everyone's opinion counts.
• All information is to be kept confidential.
• Do not judge other participants' responses.
• Respect each other, and try to talk one at a time.
• Relax.
• Speak loudly.

33
• Cell phones should be put on silent mode.
• Don’t hesitate to ask if you don’t understand the question
Are there any questions before we begin?
Instructions for the Facilitator:
Proceed to ask the questions listed below while ensuring that all participants are involved throughout the discussion. The Note taker should be able to record the responses in a note book.
Discussion Questions:
1. What are some of the key health issues/problems that affect your community? (warm up question)
2. How do you get information about the key health issues in your community?
3. In your own view, what are the roles of VHTs in the delivery of health information and services in your community?
4. How many of you were visited by a VHT in your home in the last three months? (For those who were visited, probe for the support provided or health issues addressed by the VHT)
5. How many of you listened to the “Obbanywa” radio program that aired on Dunamis FM?
6. Do you know any body in this community who has listened to the “Obbanywa” radio program that aired on Dunamis FM? If so, who?
7. For those who listened, probe for the topics they heard, the frequency of listening in, how they rate the program (was it interesting, informative, boring?) and the key messages they recall whereas for those who did not, probe why)
8. What is your view about the timing of the program? (Sunday at 2 pm with a repeat on Thursday at 11 am)
9. How would you like us to improve the “Obbanywa” radio program?