fluid control and tissue managemtent
TRANSCRIPT

Charles J. Goodacre, DDS, MSD Professor of Restorative Dentistry
Loma Linda University School of Dentistry
This program of instruction is protected by copyright ©. No portion of this program of instruction may be reproduced, recorded or transferred by any means electronic, digital, photographic, mechanical etc., or by any information storage or retrieval system, without prior permission.
Fluid Control and Tissue Management for Fixed Prosthodontic Impressions

Reasons for Fluid Control • Fluid / moisture control is imperative to make a good impression • A good impression requires lateral displacement of the gingiva so the
impression material can be deposited on the finish line and also record some of the unprepared tooth located apical to the finish line
• The gingiva is moist and may bleed from the displacement, necessitating fluid control
• Fluid / moisture is also needed to prevent saliva from coating the gingiva and prepared tooth and thereby interfering with impression making
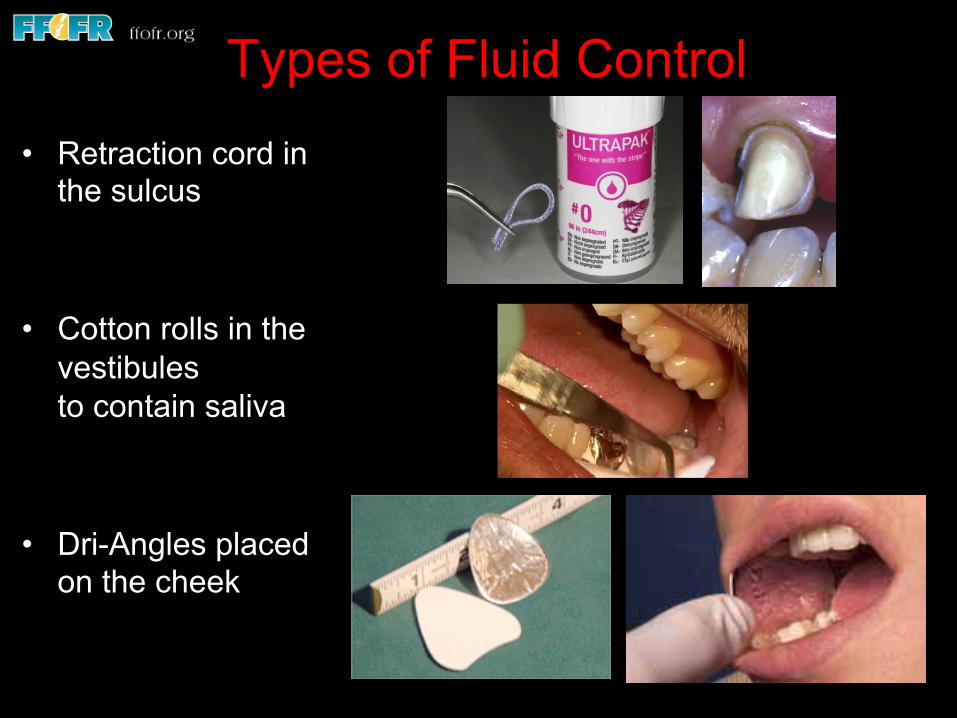
Types of Fluid Control • Retraction cord in
the sulcus
• Cotton rolls in the vestibules to contain saliva
• Dri-Angles placed on the cheek
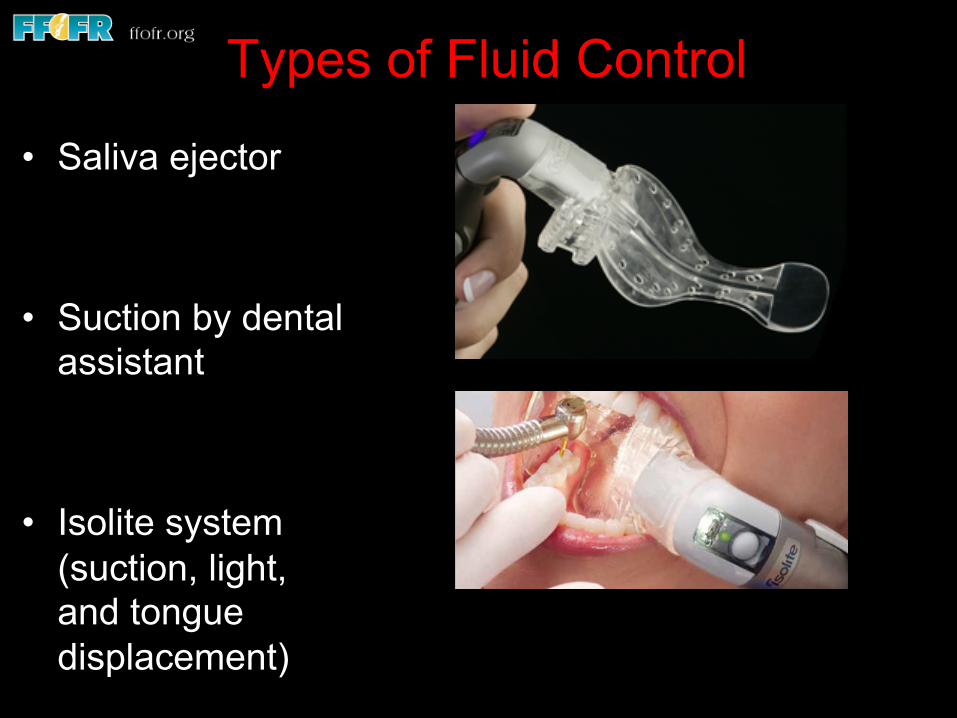
Types of Fluid Control
• Saliva ejector
• Suction by dental assistant
• Isolite system (suction, light, and tongue displacement)

The Purpose of Tissue Retraction is to Displace the Gingiva so:
• The finish line can be evaluated • The tooth structure apical to the finish line
can be examined • The gingiva is less likely to be traumatized by
rotary instruments • Impression material can record the finish line
plus some tooth structure apical to the finish line

Gingival Displacement (Retraction) Methods
• Mechanical Cord; Instrument; or Cord & Instrument

Gingival Displacement (Retraction) Methods
• Mechanical-Chemical Cord & Hemostatic agent
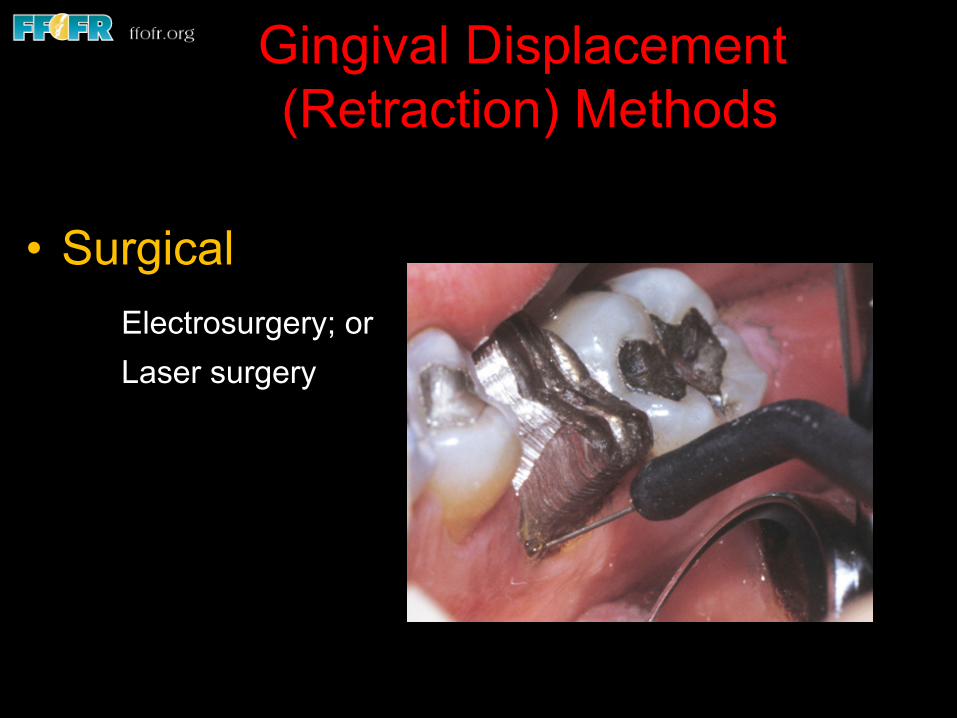
Gingival Displacement (Retraction) Methods
• Surgical Electrosurgery; or Laser surgery

Mechanical-Chemical-Hand Instrument To Minimize Gingival Trauma While
Smoothing A Tooth Preparation

ULTRAPAK Displacement Cords by Ultradent Products
Retraction Instruments • Smooth bladed instruments • Blades with perimeter serrations • Periodontal probe

Smooth-Sided & Serrated Perimeters

Curved Instruments Are Available That Can Hold The Tissue Out Of Contact With Rotary Instruments
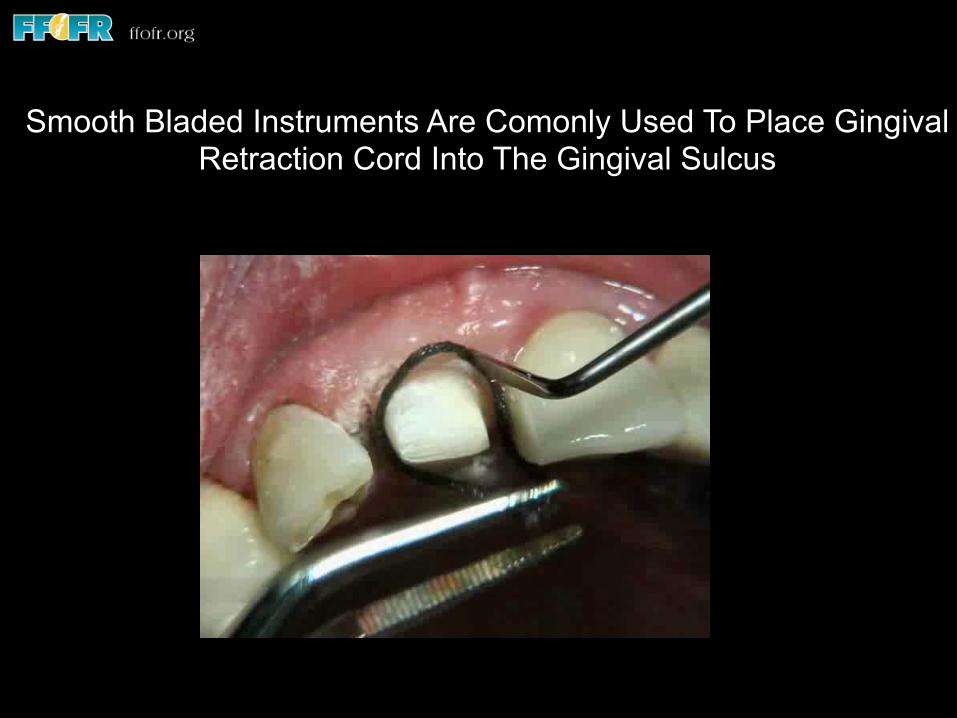
Serrated Instruments Can Lift Cords Out Of The Sulcus Smooth Bladed Instruments Are Comonly Used To Place Gingival Retraction Cord Into The Gingival Sulcus
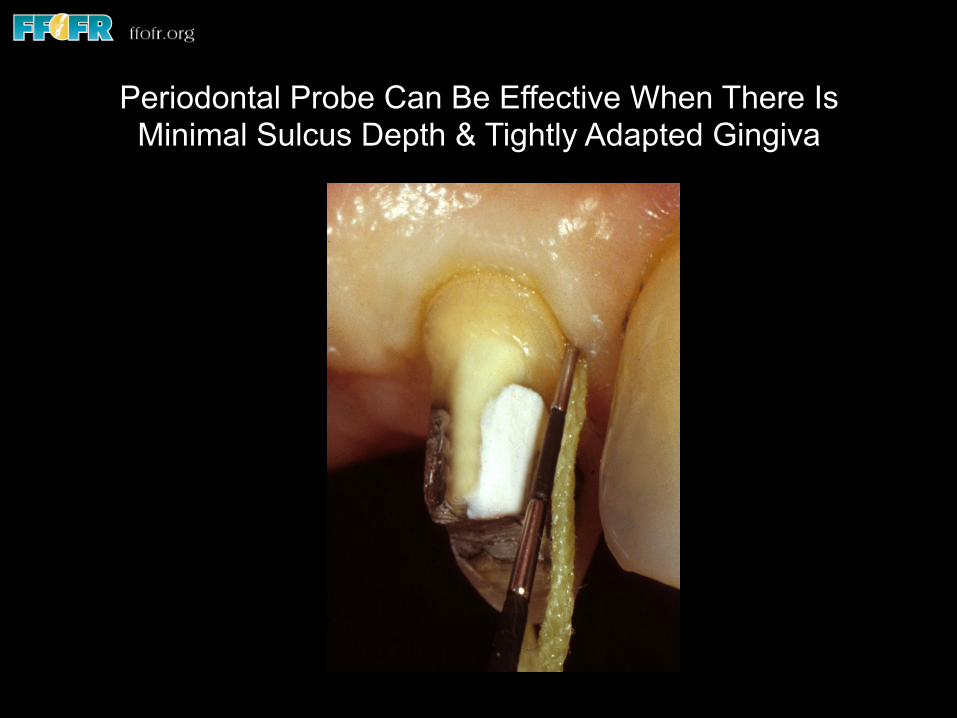
Periodontal Probe Can Be Effective When There Is Minimal Sulcus Depth & Tightly Adapted Gingiva
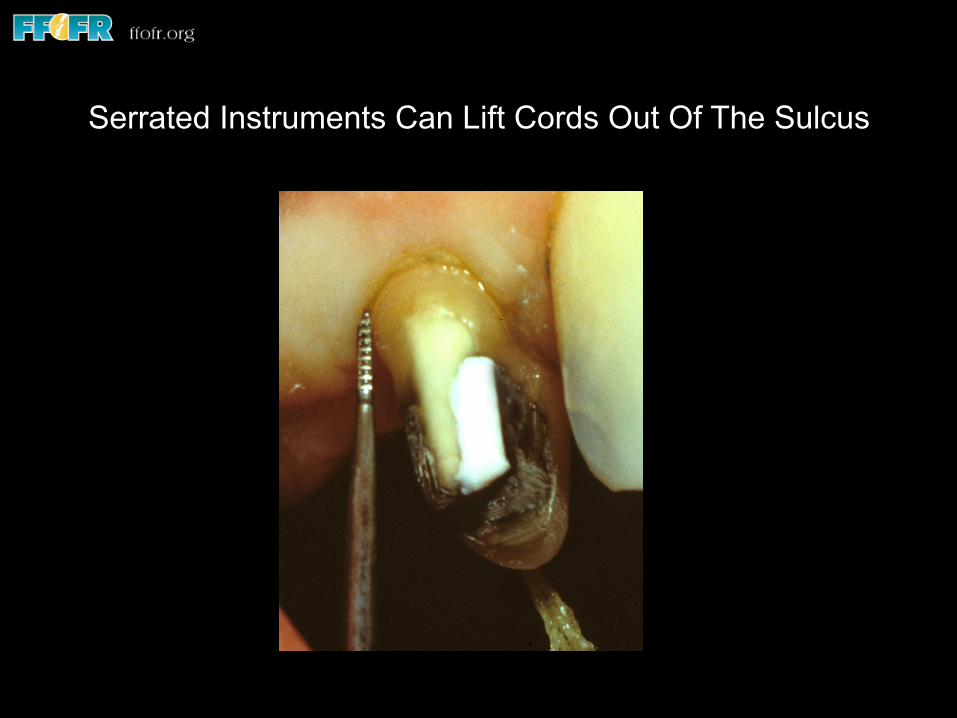
Serrated Instruments Can Lift Cords Out Of The Sulcus

Cords Should Be Moist & Immersed In A Hemostatic Agent

Never Pack Dry Cord
• Dry cords adhere to the crevicular epithelium and their removal tears the epithelium and elicits a wound healing reaction
Anneroth, Odontol Revy 1969;20:301-310
• Dry cord is harder to pack into the sulcus, leads to more bleeding upon cord removal and an unaccpetable impression, and makes it more likely that a less than ideal gingival response will follow

Preparing Cord For Placement Into The Sulcus
• Cut a segment of cord to the estimated circumference of the tooth plus a little extra
• Form into a circle and hold with cotton pliers
Preparing Cord For Placement Into The Sulcus
• Cut a segment of cord to the estimated circumference of the tooth plus a little extra
• Form into a circle and hold with cotton pliers • Immerse into hemostatic agent • Blot off excess hemostatic agent

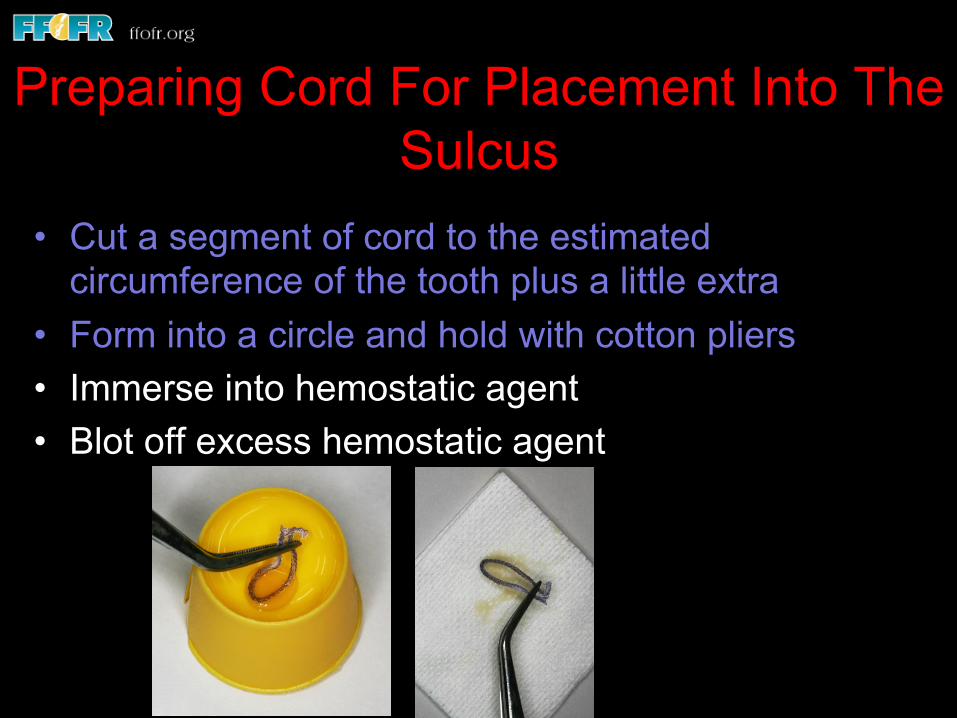
Preparing Cord For Placement Into The Sulcus
• Cut a segment of cord to the estimated circumference of the tooth plus a little extra
• Form into a circle and hold with cotton pliers
• Immerse into hemostatic agent • Blot off excess hemostatic
agent • Hold loop of cord over prepared
tooth

Preparing Cord For Placement Into The Sulcus • Cut a segment of cord to the
estimated circumference of the tooth plus a little extra
• Form into a circle and hold with cotton pliers
• Immerse into hemostatic agent • Blot off excess hemostatic
agent • Hold loop of cord over
prepared tooth • Place cord into sulcus with
instrument starting on the proximal surface

Minimizing Trauma When There Is Thin, Delicate Gingiva
Retraction Cord Placement Should Be Started Proximally Where Tissue Is More Easily Displaced

Gingival Retraction Techniques Commonly Used By Prosthodontists
• Results from 1,246 survey responses
• 98% of prosthodontists use retraction cord
• 43% of those using cord routinely use a two cord technique for more than half of their impressions Hansen, J Prosthod 1999;8:163-170

Cord Medicament Usage • 81% of prosthodontists soak cords before placing them
into sulcus
• 55% use aluminum chloride (like Hemodent)
• 23% use ferric sulfate / ferric subsulfate (like Astringedent)
• 70% use an additional agent after the cord is placed. Ferric sulfate with an infuser / burnisher was the most common additional agent Hansen, J Prosthod 1999;8:163-170
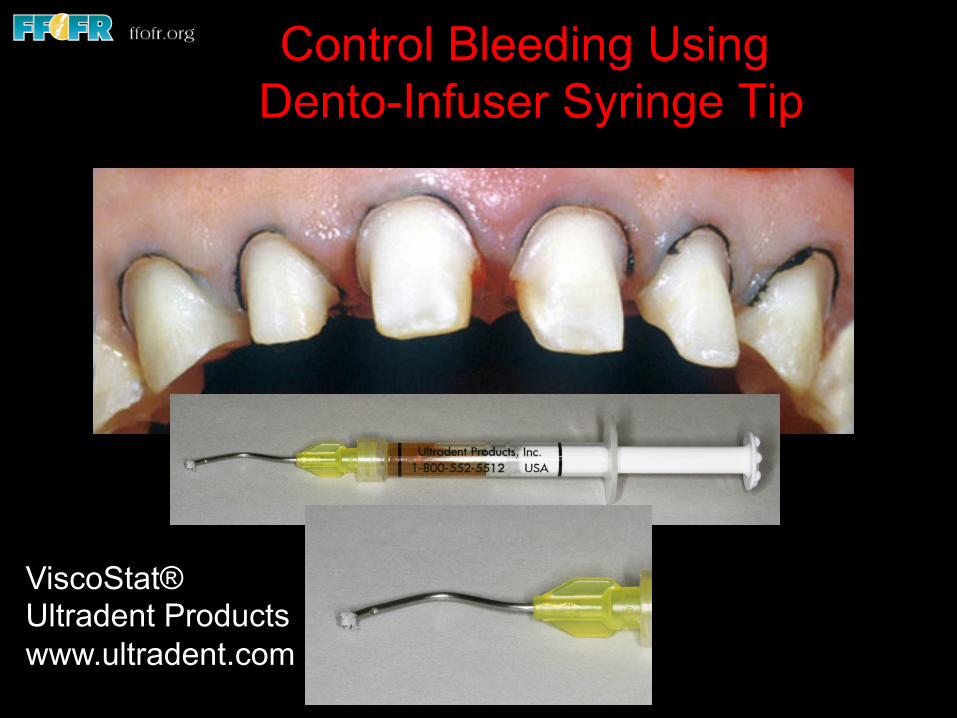
ViscoStat® Ultradent Products www.ultradent.com
Control Bleeding Using Dento-Infuser Syringe Tip

Hemorrhage Control
Epinephrine Cords vs. Others
• 22 students & 8 faculty could not tell difference (epinephrine vs. aluminum sulfate in a blind study) Jokstad, J Prosthet Dent 1999;81:258-261
• Epinephrine did not produce superior displacement to
Hemodent (AlCl3) Weir, J Prosthet Dent 1984;51:326-329
• No practical difference between aluminum sulfate,
epinephrine, and aluminum chloride Gennaro, J Prosthet Dent 1982;47:384-386

My Preferred Technique

STEP 1: Cut a segment of a smaller diameter cord to the estimated circumference of the tooth plus a little extra. Form into a circle and hold with cotton pliers
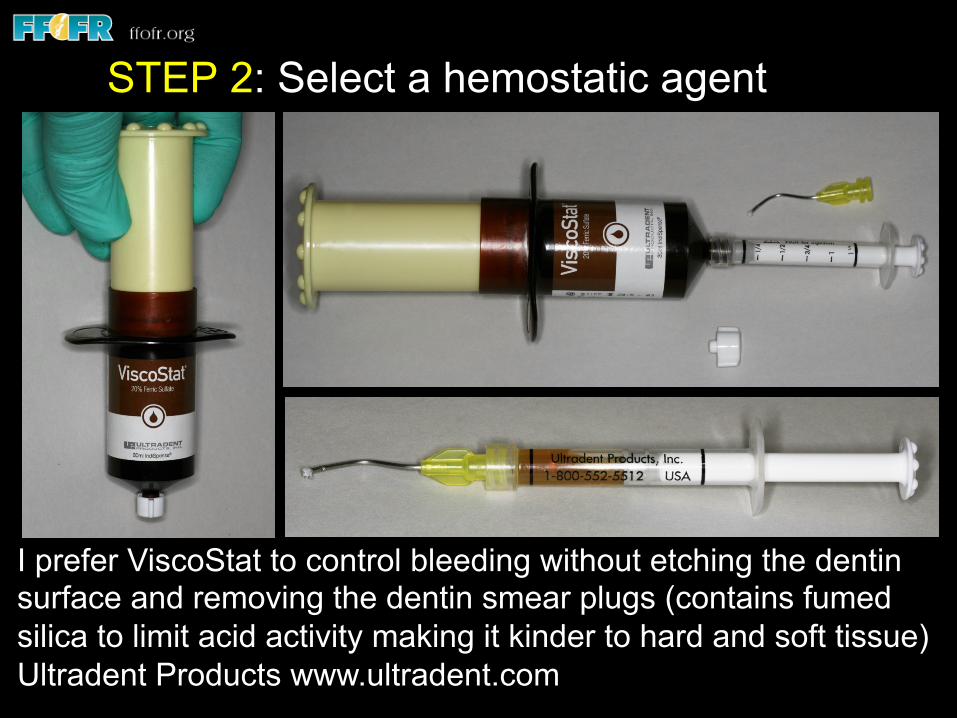
I prefer ViscoStat to control bleeding without etching the dentin surface and removing the dentin smear plugs (contains fumed silica to limit acid activity making it kinder to hard and soft tissue) Ultradent Products www.ultradent.com
STEP 2: Select a hemostatic agent

ViscoStat® Is Very Effective At Controlling Bleeding But It Can Leave A Brown Residue When There Is A Lot Of Bleeding. The Residue Can Be Removed Using A Cotton Pellet Soaked In Hemodent
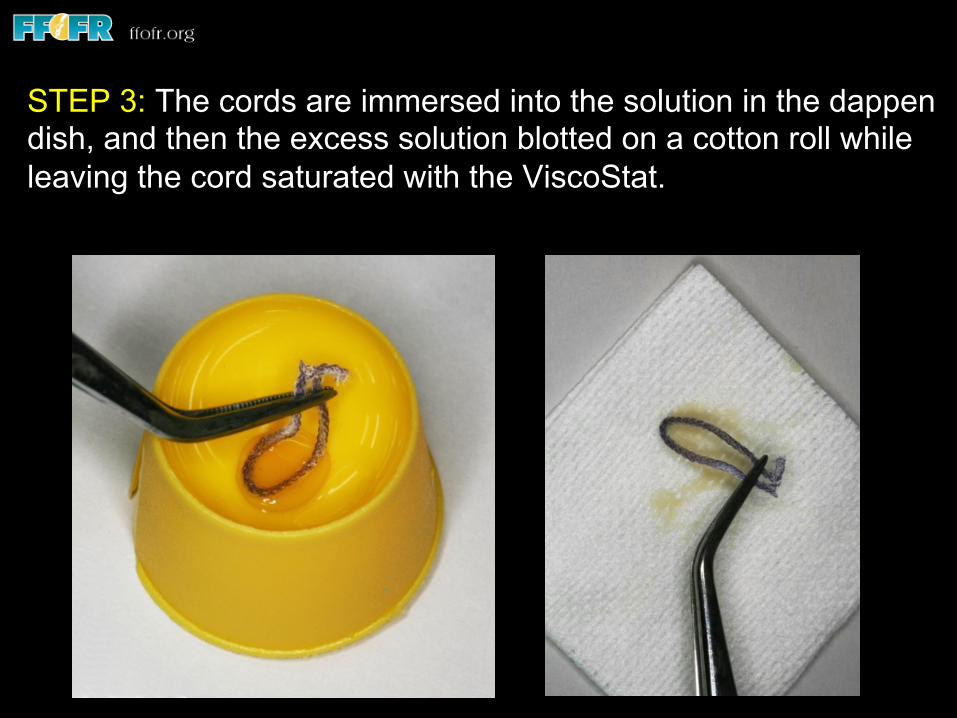
STEP 3: The cords are immersed into the solution in the dappen dish, and then the excess solution blotted on a cotton roll while leaving the cord saturated with the ViscoStat.
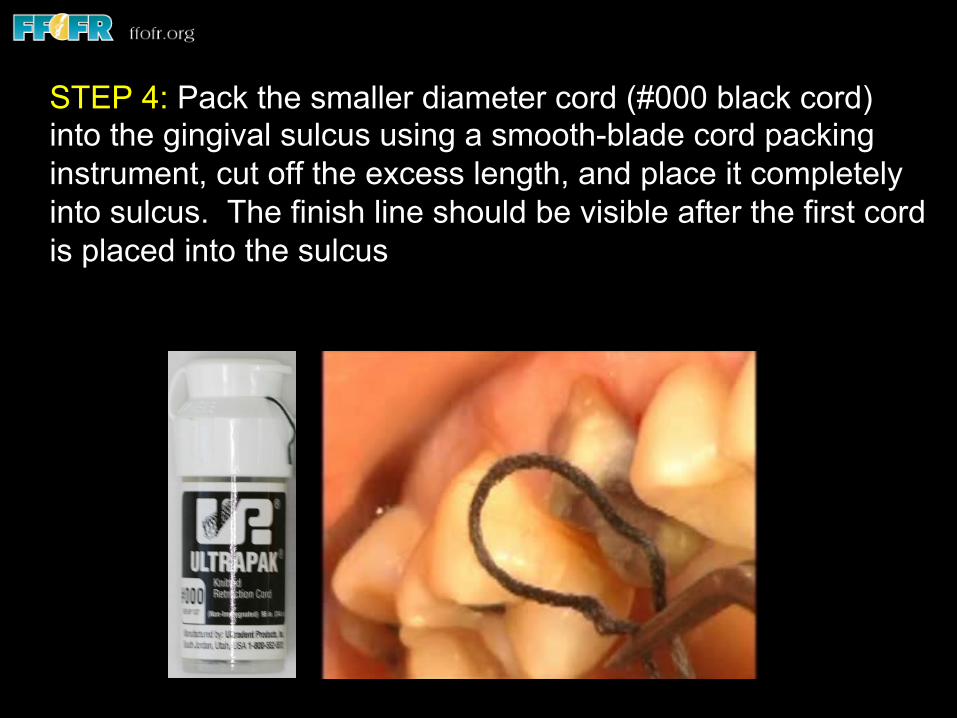
STEP 4: Pack the smaller diameter cord (#000 black cord) into the gingival sulcus using a smooth-blade cord packing instrument, cut off the excess length, and place it completely into sulcus. The finish line should be visible after the first cord is placed into the sulcus
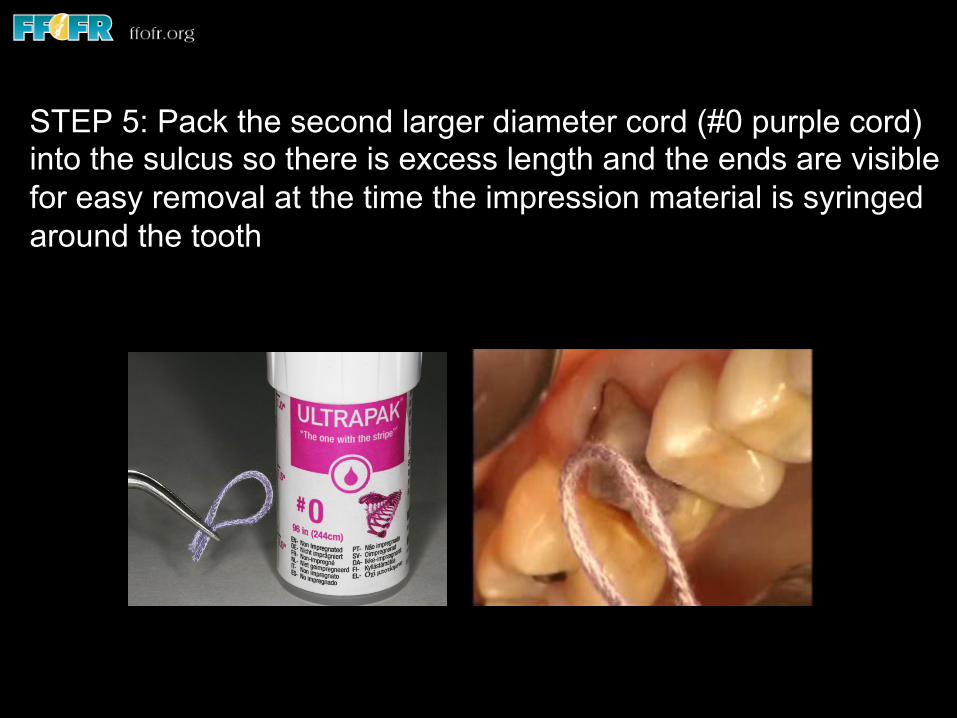
STEP 5: Pack the second larger diameter cord (#0 purple cord) into the sulcus so there is excess length and the ends are visible for easy removal at the time the impression material is syringed around the tooth

STEP 6: Use compressed air to dry the tooth but do not dessicate the gingiva and cord as that will cause fusion of the cord to the gingiva and instantaneous bleeding when the cord is removed

Remove the 2nd cord (leaving the 1st cord to control moisture and hemorrhage) and syringe impression material directly behind the exiting second cord to minimize the opportunity for moisture or hemorrhage to reach the finish line before the impression material
Syringe Tip Access To Interproximal Finish Line
Thank You For Your Kind Attention
Charles J. Goodacre, DDS, MSD Professor of Restorative Dentistry
Loma Linda University School of Dentistry

v Visit ffofr.org for hundreds of additional lectures on Complete Dentures, Fixed Prosthodontics, Implant Dentistry, Removable Partial Dentures, Esthetic Dentistry and Maxillofacial Prosthetics.
v The lectures are free. v Our objective is to create the
best and most comprehensive online programs of instruction in Prosthodontics