first- and second-generation antipsychotics for children and young adults
DESCRIPTION
First- and Second-Generation Antipsychotics for Children and Young Adults. Prepared for: Agency for Healthcare Research and Quality (AHRQ) www.ahrq.gov. Outline of Material. - PowerPoint PPT PresentationTRANSCRIPT
First- and Second-Generation Antipsychotics for Children and
Young AdultsPrepared for:
Agency for Healthcare Research and Quality (AHRQ)
www.ahrq.gov

Introduction to pediatric use of first-generation and second-generation antipsychotics, including approved and off-label indications.
Systematic review methods. The clinical questions addressed by the
comparative effectiveness review. Results of studies and evidence-based conclusions
about effectiveness and adverse effects of antipsychotics in pediatric use.
Gaps in knowledge. What to discuss with patients and their caregivers.
Outline of Material
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

Antipsychotics can be classified into two categories based on the timeline of their development, their mechanisms of action, and their anticipated adverse effect profiles. First-generation antipsychotics (FGAs), also
called conventional or typical antipsychotics Second-generation antipsychotics (SGAs), also
called atypical antipsychotics FGAs were the first successful pharmacological
treatments for primary psychotic disorders such as schizophrenia.
Introduction to Antipsychotics in Pediatric Use (1 of 4)
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

First-generation antipsychotics are associated with side effects that are difficult to manage and in some cases are irreversible. Neurological side effects include extrapyramidal system
movement disorders: Tardive dyskinesia: repetitive, involuntary muscle
movements Akathisia: restlessness Inability to initiate movement; Parkinson’s disease-
like symptoms
Development of the second-generation antipsychotics was driven by the need to limit neurological adverse effects.
Introduction to Antipsychotics in Pediatric Use(2 of 4)
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

Many first-generation and second-generation antipsychotics are approved by the U.S. Food and Drug Administration (FDA) for use in children and/or adolescents.
The FDA prohibits manufacturers from advertising or promoting the use of pharmaceuticals for indications that it has not approved. To do so is illegal.
Off-label prescribing by physicians is permitted.
Introduction to Antipsychotics in Pediatric Use (3 of 4)
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

Prescribing of antipsychotics for children with mental and behavioral disorders continues to increase and includes off-label use.
However, the effects of both first-generation (FGAs) and second-generation (SGAs) antipsychotics on patient-centered outcomes such as growth, development, and quality of life are not well understood.
Studies of efficacy, benefits, and adverse effects of FGAs and SGAs used in pediatric treatment are reported in the clinical literature.
Introduction to Antipsychotics in Pediatric Use (4 of 4)
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

Antipsychotics Approved for Pediatric Use:First-Generation Antipsychotics
Antipsychotic Indication Age Group
Chlorpromazine Schizophrenia
1–12 yearsBipolar disorder (mania)
Severe behavioral problems
Hyperactivity
Droperidol Agitation “children”
Loxapine Schizophrenia ≥12 years
Perphenazine Schizophrenia ≥12 years
Pimozide Tourette’s syndrome ≥12 years
Prochlorperazine Schizophrenia >2 years and >20 pounds
Thiothixene Schizophrenia ≥12 years
Thioridazine Schizophrenia “children”
Trifluoperazine Schizophrenia ≥6 years
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

Antipsychotics Approved for Pediatric Use:Second-Generation Antipsychotics
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.
Antipsychotic Indication Age Group
Aripiprazole
Schizophrenia 13–17 years
Autism irritability 10–17 years
Bipolar disorder (manic/mixed) 6–17 years
Olanzapine
SchizophreniaAdolescents (13–17 years)
Bipolar disorder (manic/mixed)
Bipolar disorder: depressive episode
QuetiapineSchizophrenia 13–17 years
Bipolar disorder (acute manic) 10–17 years
Risperidone
Schizophrenia 13–17 years
Autism irritability 5–16 years
Bipolar disorder (manic/mixed) 10–17 years

The clinical literature includes studies of pediatric use of first-generation and second-generation antipsychotics for treatment of these disorders: Pervasive developmental disorders Attention deficit hyperactivity disorder and disruptive
behavior disorders Bipolar disorder Schizophrenia and related psychosis Tourette’s syndrome Behavioral issues
No clinical studies were found for obsessive-compulsive disorder, post-traumatic stress disorder, or anorexia nervosa.
Disorders Treated by Antipsychotics inPediatric Use
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

Topics are nominated through a public process, which includes submissions from health care professionals, professional organizations, the private sector, policymakers, members of the public, and others.
A systematic review of all relevant clinical studies is conducted by independent researchers, funded by AHRQ, to synthesize the evidence in a report summarizing what is known and not known about the select clinical issue. The research questions and the results of the report are subject to expert input, peer review, and public comment.
The results of these reviews are summarized into Clinician Research Summaries and Consumer Research Summaries for use in decisionmaking and in discussions with patients. The Summaries and the full report, with references for included and excluded studies, are available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.
Agency for Healthcare Research and Quality (AHRQ) Comparative Effectiveness Review (CER) Development
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

The strength of evidence was classified into four broad categories:
Rating the Strength of Evidence From the Comparative Effectiveness Review
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

The reviewed literature was limited to studies performed in children, adolescents, and young adults from 1 to 24 years of age.
What is the comparative efficacy or effectiveness of first-generation (FGAs) and second-generation (SGAs) antipsychotics for treating disorder-specific and nonspecific symptoms?
Do FGAs and SGAs differ in short-term (within 6 months) and long-term (after 6 months) outcomes, including: Response rate and relationship to dosage; speed of response; duration of response;
remission; relapse; time to discontinuation; and adherence Growth and maturation; cognitive and emotional development Suicidal behaviors and ideation Work-related functional capacity; school performance Patient insight into illness Patient- or caregiver–reported outcomes Health-related quality of life Legal or justice system interactions Health care system utilization
Clinical Questions Addressed by theComparative Effectiveness Review (1 of 2)
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

Do first-generation (FGAs) and second-generation (SGAs) antipsychotics differ in the following medication-associated adverse events: Overall adverse events? Specific adverse events? Withdrawals and time to withdrawal due to adverse events? Persistence and reversibility of adverse events?
Do the efficacy and risks of FGAs and SGAs vary in differing subpopulations including: Sex, age group, and race? Comorbidities? Cotreatment versus monotherapy First episode versus prior episodes (for schizophrenia)? Duration of illness?
Treatment naïve versus history of antipsychotic use?
Clinical Questions Addressed by theComparative Effectiveness Review (2 of 2)
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

Clinically Significant Outcomes of Interest in the Comparative Effectiveness Review Both core illness symptoms and nonspecific symptoms were of interest. A wide variety of psychiatric assessment instruments are used to evaluate symptoms in studies of
pediatric use of antipsychotics. Lower scores indicate less severity. The assessments included:
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.
Instrument Application
Aberrant Behavior Checklist (ABC)Treatment effects on profoundly mentally retarded participants
Brief Psychiatric Rating Scale–Children (BPRS-C)
Childhood psychiatric disorders and response to treatment
Children’s Depression Rating Scale (CDRS) Severity of depression in children 6–12 years of age
Children’s Global Assessment Scale (CGAS)
Overall measure of disturbance; children 4–16 years of age
Clinical Global Impressions (CGI)Global rating of severity (-S), improvement (-I), or overall impression
Nisonger Child Behavior Rating Form (NCBRF)
Childhood problems because of mental retardation
Overt Aggression Scale (OAS) Physical and verbal aggressive behaviors
Positive and Negative Syndrome Scale (PANSS)
Positive and negative symptoms in schizophrenia
Young Mania Rating Scale (YMRS) Severity (not diagnosis) of mania

Adverse Events of Interest in theComparative Effectiveness Review Adverse events data extracted
from published studies included: Mortality Cardiac and cerebrovascular
events Weight and body
composition Dyslipidemia Insulin resistance and
diabetes Prolactin-related and sexual
effects Neuromotor
(extrapyramidal) Sedation
Liver toxicityNeutropenia and agranulocytosisThyroid dysfunctionSeizuresNeuroleptic malignant syndromeConstipationExercise intolerancePrecocious pubertyBehavioral effectsDermatological effects
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.
For adverse events reporting, standardized instruments that evaluate extrapyramidal symptoms are also used in clinical trials.

Population: Children to age 12 years, adolescents ages 12–17 years, and young adults ages 18–24 years with these diagnosed mental disorders: PDD, ADHD, DBD, bipolar disorder, schizophrenia or related psychosis, Tourette’s syndrome, or other behavioral symptoms
Interventions: Any FGAs and SGAs approved by the FDA Comparators: Other FGAs or SGAs, placebo Outcomes: Core and nonspecific symptoms; response; remission;
growth and maturation; cognitive and emotional development; suicide-related behaviors; adherence; school and work capacity and performance; patient insight; patient-, parent-, or caregiver-reported outcome; health-related quality of life; legal system interaction; health care system utilization; adverse events (e.g., weight; dyslipidemia; insulin and blood glucose effects and diabetes; extrapyramidal symptoms; prolactin effects)
Timing: No minimum or maximum duration specified Setting: Community and hospitalized care
Summary of Study Characteristics Evaluated in the Effectiveness Review: PICOTS
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

95-Percent Confidence Interval: The range of statistically valid results that will include the true population mean in 95 of 100 repeated experiments.
Mean Difference (MD): The difference between treatment and comparison group means. To determine a standardized mean difference (SMD), results
from different scales are normalized to a common, “standardized” scale before calculating the mean difference.
For MD and SMD, the result is statistically significant (p < 0.05) when the 95-percent confidence interval does not include 0.0, which is the point of no difference between groups.
Relative Risk (RR): The ratio of the rate (absolute risk, probability) of an event in the treatment group, to the rate of the event in the comparison group. For RR, the result is statistically significant at p < 0.05 when the
95-percent confidence interval does not include 1.0, which is the point of equal risk for both groups.
Modes of Results Reporting and Statistical Analysis in the Comparative Effectiveness Review (1 of 2)
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

Absolute Risk Difference: The absolute value of the mathematical difference between the rates (risk) of an event in the treatment and comparison groups. ARD = |ARC-ART|
Number Needed to Treat or Harm (NNT, NNH): The number of patients to be treated to observe benefit or harm in one patient more than seen in the comparison group. The number of patients to be treated in order to find a benefit or harm attributable to the intervention. NNT or NNH = |ARC-ART|-1 for a benefit or adverse event,
respectively Number of attributable events per 1000 = 1000 x |ARC-ART| The smaller the NNT or NNH, the greater the attributable
effect.
Modes of Results Reporting and Statistical Analysis in the Comparative Effectiveness Review (2 of 2)
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.
.

Efficacy studies Are randomized, controlled trials (RCTs) designed to demonstrate a
clinical benefit Enroll participants based on restrictive inclusion and exclusion criteria The comparator is usually placebo
Effectiveness studies May be RCTs but can include retrospective cohort studies and other study
formats Are designed to examine clinical effects of treatments in typical medical
practice Inclusion and exclusion criteria are not as restrictive as in efficacy trials The comparator is usually an active control or “usual care,” rather than
placebo The treatment setting may vary widely among the participants
Effectiveness and Efficacy of Antipsychotics
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.
.

The included studies were limited to those that enrolled children (≤12 years of age), youth (12–18 years of age), and young adults (19–24 years of age).
Comparisons of second-generation antipsychotics (SGAs) with placebo were the most commonly reported studies.
Too few placebo comparison studies of first-generation antipsychotics (FGAs) for treatment of psychiatric disorders of children were reported to permit conclusions about effect sizes and statistical significance.
Head-to-head comparisons of FGAs with other FGAs included in this review (two studies) were studies about treatment of schizophrenia.
Head-to-head comparisons of FGAs versus SGAs that met the criteria for inclusion in this review (17 studies) were investigations for treatment of schizophrenia, pervasive developmental disorder (autism), and Tourette’s syndrome.
Head-to-head comparisons of SGAs with other SGAs (46 studies) were investigated for treatment of bipolar disorder, schizophrenia, and behavioral issues.
Summary of Efficacy and Effectiveness Studies of Antipsychotics in Pediatric Use
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

Efficacy of Second-Generation Antipsychotics: Placebo Comparisons, by Indication (1 of 3)
Outcome(n studies, n participants)
Meta-analytic Result (Mean Difference) and Statistically Valid Range (95% CI)
Strength of Evidence
Bipolar Disorder
CGI (6, 978) Pooled SGA results (aripiprazole, olanzapine, quetiapine, and risperidone): CGI score is 0.67 points lower with SGAs when compared with placebo (0.51 to 0.84 points lower)
●●○
YMRS No meta-analysis of SGAs as a class due to statistical heterogeneity
●○○
YMRS (3, 328) Aripiprazole: 7.22 points lower than placebo (5.17 to 9.28 points)
YMRS (1, 159) Olanzapine: 7.66 points lower than placebo (5.68 to 9.74 points)
YMRS (3, 339) Quetiapine: No pooled result due to statistical heterogeneity among reports
YMRS (1, 163) Risperidone: 8.31 points lower than placebo (4.88 to 11.74 points)
YMRS (1, 218) Ziprasidone: 5.22 points lower than placebo (2.36 to 8.08 points)
CDRS (4, 532) NSD (No pooled values) ●○○
Strength of Evidence Symbols: High = ●●●Moderate = ●●○Low = ●○○Insufficient = ○○○
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

Efficacy of Second-Generation Antipsychotics: Placebo Comparisons, by Indication (2 of 3)
Outcome(n studies, n participants)
Meta-analytic Result (Mean Difference) and Statistically Valid Range (95% CI)
Strength of Evidence
Schizophrenia
CGAS (5, 880)
Score is 4.56 points higher (2.55 to 6.57 points higher) with SGAs (aripiprazole, olanzapine, paliperidone, quetiapine, and risperidone)
●○○CGI-I (3, 505) Score is 0.75 points lower (0.38 to 1.12 points lower) with SGAs (aripiprazole, olanzapine, and risperidone)
PANSS (6, 987)
Score is 8.69 points lower (5.61 to 11.76 points lower) with SGAs (aripiprazole, olanzapine, paliperidone, quetiapine, and risperidone)
Tourette’s Syndrome
YGTSS (2, 54)
Score is 6.98 points lower (3.62 to 10.34 points lower) with SGAs (risperidone and ziprasidone)
●○○
Strength of Evidence Symbols: High = ●●●Moderate = ●●○Low = ●○○Insufficient = ○○○
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.
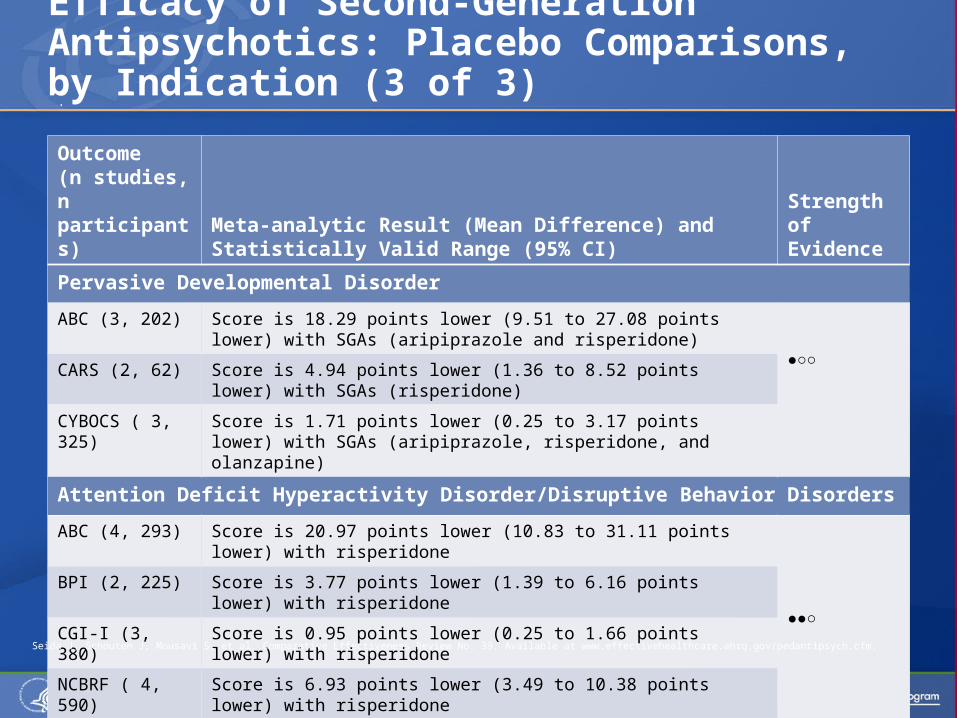
Efficacy of Second-Generation Antipsychotics: Placebo Comparisons, by Indication (3 of 3)
Outcome(n studies, n participants)
Meta-analytic Result (Mean Difference) and Statistically Valid Range (95% CI)
Strength of Evidence
Pervasive Developmental Disorder
ABC (3, 202) Score is 18.29 points lower (9.51 to 27.08 points lower) with SGAs (aripiprazole and risperidone)
●○○CARS (2, 62) Score is 4.94 points lower (1.36 to 8.52 points lower) with
SGAs (risperidone)
CYBOCS ( 3, 325)
Score is 1.71 points lower (0.25 to 3.17 points lower) with SGAs (aripiprazole, risperidone, and olanzapine)
Attention Deficit Hyperactivity Disorder/Disruptive Behavior Disorders
ABC (4, 293) Score is 20.97 points lower (10.83 to 31.11 points lower) with risperidone
●●○
BPI (2, 225) Score is 3.77 points lower (1.39 to 6.16 points lower) with risperidone
CGI-I (3, 380) Score is 0.95 points lower (0.25 to 1.66 points lower) with risperidone
NCBRF ( 4, 590)
Score is 6.93 points lower (3.49 to 10.38 points lower) with risperidone
Strength of Evidence Symbols: High = ●●●Moderate = ●●○Low = ●○○Insufficient = ○○○
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.
.

When compared with placebo, second-generation antipsychotics (SGAs) result in greater improvement of disorder-specific symptoms.
SGAs (aripiprazole, olanzapine, paliperidone, quetiapine, and risperidone) improve both clinical global impressions and positive and negative symptoms of schizophrenia (an approved indication). Strength of Evidence = Moderate
SGAs (aripiprazole, olanzapine, quetiapine, and risperidone) improve clinical global impressions (CGIs) of bipolar disorder and manic but not depressive symptoms of bipolar disorder. Strength of Evidence = Moderate for CGIs Strength of Evidence = Low for manic and depressive
symptoms
Summary of Results: Efficacy of Antipsychotics in Placebo Comparisons (1 of 2)
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

Risperidone and ziprasidone improve tics in Tourette’s syndrome.Strength of Evidence = Moderate
Risperidone improves behavioral symptoms and clinical global impressions of attention deficit hyperactivity disorders/ disruptive behavior disorders.Strength of Evidence = Moderate
Second-generation antipsychotics (aripiprazole and risperidone) improve behavioral (irritability, an approved indication), obsessive-compulsive, and autistic symptoms of pervasive developmental disorders.Strength of Evidence = Low
Summary of Results: Efficacy of Antipsychotics in Placebo Comparisons (2 of 2)
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

Results of Comparative Effectiveness Studies:FGAs Versus SGAs
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.
The evidence from comparisons of first-generation (FGAs) and second-generation (SGAs) antipsychotics in Tourette’s syndrome is insufficient to permit conclusions about effect size or statistical significance.
Comparison
Outcome(n studies,
n participants)
Mean Difference and Statistically Valid Range Defined by the 95% CI
Strength of Evidence
FGAs vs. SGAs for Pervasive Developmental Disorders
Haloperidol vs. Olanzapine
Autistic Symptoms
(CPRS) (1, 12)
Anger and hyperactivity factors reduced only in the
olanzapine group (p ≤ 0.05)*●○○
Haloperidol vs. Risperidone
Autistic Symptoms
(ABC, CGI) (1, 30)
Behavior, impulsivity, and language skills improved
to a greater degree with risperidone (p ≤ 0.05)*●○○
FGAs vs. SGAs for Schizophrenia
Haloperidol vs. SGAs
(clozapine, olanzapine, and
risperidone]
BPRS (3 , 71)
Score is 11.44 points lower with SGAs(Statistically valid range is 3.52 to 19.35 points lower)
●○○
CGI-I(3, 87)
Score is 0.76 points lower with SGAs (Statistically valid range is 0.26 to 1.25 points lower)
●○○
PANSS(2, 27)
NSD (Statistically valid range is 33.85 points lower to 14.08 points greater)
●○○
*Single study; no meta-analysis. 95% CI = 95-percent confidence interval: the range of statistically valid results; mean difference = the difference between treatment and control group means; NSD = No statistically significant difference (p ≥ 0.05). Strength of Evidence Symbols: High = ●●●Moderate = ●●○Low = ●○○Insufficient = ○○○

Results of Comparative Effectiveness Studies: SGAs Versus SGAs
Comparison
Outcome (n studies, n participants)
Mean Difference and Statistically Valid Range Defined by the 95% CI
Strength of Evidence
SGAs vs. SGAs for Schizophrenia
Olanzapine vs. Risperidone
BPRS (3, 136) NSD
●○○CGI-S (2, 111) NSD
PANSS (3, 143) NSD
Olanzapine vs. Clozapine
BPRS (2, 27) NSDStatistically valid range from 10.82 points less to 0.64 points more
●○○CGI-S (2, 64) NSD
Statistically valid range from 1.01 points less to 0.08 points more
SANS (2, 64) NSDStatistically valid range from 15.45 points less to 5.36 points more
95% CI = 95-percent confidence interval: the range of statistically valid results; mean difference = the difference between treatment and control group means; NSD = no statistically significant difference (p ≥ 0.05)Strength of Evidence Symbols: High = ●●●Moderate = ●●○Low = ●○○Insufficient = ○○○
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pediantipsych.cfm.

The evidence from within-class comparisons of FGAs with FGAs is insufficient to permit conclusions about effect sizes and statistical significance.
In between-class comparisons of FGAs with SGAs: Olanzapine and risperidone are more effective than
haloperidol for reducing autistic symptoms (anger, hyperactivity, and Aberrant Behavior Checklist scores) in pervasive developmental disorders. Strength of Evidence = Low
In pooled analyses, SGAs (clozapine, olanzapine, and risperidone) are more effective than haloperidol in treating schizophrenia, as assessed by clinical global impressions, but not by effects on positive and negative symptoms. Strength of Evidence = Low
Summary of Comparative Effectiveness Results (1 of 2)
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

In within-class comparisons of second-generation antipsychotics with each other: Olanzapine is not statistically different from
risperidone or clozapine in treating schizophrenia, as assessed by clinical global impressions and positive and negative symptoms. Strength of Evidence = Low
Summary of Comparative Effectiveness Results (2 of 2)
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

Adverse events were examined across all indications in total: adverse events are not expected to be dependent on diagnosis.
Several adverse events of interest had no data reported. The analysis focused on key adverse event categories
reported in at least one study: Weight and body composition Blood lipids Blood glucose, insulin, and diabetes Neuromotor effects (e.g., extrapyramidal symptoms,
akathisia, tardive dyskinesia) Prolactin and related sexual adverse effects Sedative effects
Adverse Effects of Antipsychotics In Children
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

Placebo Comparisons: There are few comparisons of first-generation
antipsychotics (FGAs) with placebo that report differences in adverse events in children.
The evidence is insufficient for all key adverse events.
FGAs versus FGAs: The evidence is insufficient for all head-to-head
comparisons of FGAs.
Adverse Effects: First-Generation Antipsychotics
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

Adverse Effects: FGAs Compared With SGAsFGAs versus SGAs:
The evidence from comparisons of FGAs as a class versus SGAs as a class, and for FGAs compared with the SGA clozapine, is insufficient to permit conclusions.
Comparisons of haloperidol with two SGAs, olanzapine and risperidone, yielded the following results in a meta-analysis:
Comparison
Weight (95% CI) [n studies, n participants]
Extrapyramidal Symptoms (95% CI)[n studies, n participants]
Sedation (95% CI)[n studies, n participants]
Haloperidol vs. Olanzapine
5.79 kg greater with olanzapine(from 3.0 to 8.6 kg higher) [4, 132] ●○○
3.53-fold greater risk with haloperidol (from 1.1-fold to 10.9-fold) [3, 62] ●○○
Not reported
Haloperidol vs. Risperidone
NSD(statistically valid range is from 8.9 kg lower with haloperidol to 16.76 kg greater with haloperidol)[3, 130] ●○○
No meta-analysis.Two different scales used; both show statistically significant, greater severity of extrapyramidal symptoms with haloperidol.[1, 34] ●○○
6- fold greater risk of fatigue with haloperidol (from 1.5-fold to 24.2-fold)[1, 24] ˜™™
Strength of Evidence Symbols: High = ●●●Moderate = ●●○Low = ●○○Insufficient = ○○○Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

For comparisons between FGAs or with placebo, the evidence is insufficient to permit conclusions about the degree of risk or severity of adverse effects.
In direct comparisons of the FGA haloperidol with SGAs: When compared with olanzapine:
Haloperidol is associated with a lower risk for adverse effects on weight and body composition but with a greater risk of extrapyramidal symptoms.
No statistically significant differences are noted for prolactin-related measures or sedation. Strength of Evidence = Low
When compared with risperidone: Haloperidol is associated with greater severity of extrapyramidal
symptoms. No statistically significant differences in risk are noted for adverse
effects on weight and body composition or prolactin-related effects. Strength of Evidence = Low
Summary of Adverse Effects ofFirst-Generation Antipsychotics
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

Adverse Effects: Second-Generation Antipsychotics Versus Placebo (1 of 2)
The risk and severity of key adverse events was examined in a meta-analysis of individual SGAs compared with placebo, in pediatric use. SGAs showed these effects:
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.
Adverse Effects
Relative Risk or Mean Difference (95% CI)
Aripiprazole Olanzapine Quetiapine Risperidone Ziprasidone
Dyslipidemia†
Elevated cholesterol
Risk is elevated 2.5x (range from 1.4x to 4.4x )
NNH = 4 ●○○
Elevated cholesterol
Risk is elevated 10x (range from 1.4x to 73.2x)
NNH = 6 ●○○
Triglyceride level
Triglycerides are 29.1 mg/dL higher (range from 7.3 to 50.9 mg/dL higher)
●○○
Insufficient ○○○
No Data
Weight Gain*
Weight is 0.77 kg greater (range from 0.4 to 1.2 kg)●●○
Weight is 4.60 kg greater (range from 3.07 to 6.13 kg)●●○
Weight is 1.8 kg greater (range from 1.1 to 2.5 kg)●●○
Weight is 1.8 kg greater (range from 1.5 to 2.1 kg)●●○
NSD●○○
Strength of Evidence Symbols: High = ●●●Moderate = ●●○Low = ●○○Insufficient = ○○○95% CI = 95-percent confidence interval (the range of statistically valid results); NNH = number needed to harm (the number of patients to be treated to affect one patient more than in the control group); NSD = no statistically significant difference*Most studies that measured changes in weight ranged from 4 to 8 weeks duration, but some were in the range of 6 months to 1 year. † Dyslipidemia includes abnormalities in total cholesterol and triglycerides.

Adverse Effects: Second-Generation Antipsychotics Versus Placebo (2 of 2)
Adverse Events
Relative Risk or Mean Difference (95% CI)
Aripiprazole Olanzapine
Quetiapine Risperidone Ziprasidone
EPS Risk is elevated 4.2x (from 2.4x to 7.2x)
NNH = 4 ●●○
Not Reported NSD●○○
Risk is elevated2.7x (from 1.4x to 4.9x)
NNH = 15 ●●○
Risk is elevated 10.3x (from 1.4 x to 75x)
NNH = 9 ●○○
Somnolence
Risk is elevated 2.7x (from 1.1x to 6.5x)
NNH = 10 ●○○
NSD●○○
Risk is elevated 3.4x (from 2.0x to 5.8x)
NNH = 4 ●○○
Risk is elevated 2.9x (from 1.5x to 5.5x)
NNH = 4 ●●○
Risk is elevated 3.0x (from 1.7x to 5.2x)
NNH = 7 ●●○
ProlactinLevels
4.1 ng/mL lower (from 1.8 ng/mL to 6.3 ng/mL)
●●○
11.5 ng/nL higher(from 8.8 ng/mL to 14.1 ng/mL)●●○
NSD ●○○
22.6 ng/mL higher(from 10.7 to 34.5 ng/mL)
●○○
Insufficient ○○○
Strength of Evidence Symbols: High = ●●●Moderate = ●●○Low = ●○○Insufficient = ○○○95% CI = 95-percent confidence interval (the range of statistically valid results); EPS = extrapyramidal symptoms; NNH = number needed to harm (the number of patients to be treated to affect one patient more than in the control group); NSD = no statistically significant differenceSeida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

Adverse Effects: SGAs Versus SGAs (1 of 2)The risk and severity of key adverse events were examined in a meta-analysis of individual SGAs compared with other SGAs in head-to-head evaluations in pediatric use. The analysis found the following summary effects and statistically valid range of values for the effects, as defined by the 95-percent confidence interval (95% CI):
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.
Comparison
Dyslipidemia Weight
Olanzapine vs. Quetiapine
The risk with olanzapine is 3.5 times that of quetiapine (from 1.1x to 11.2x). ●○○
No summary estimate.
Olanzapine vs. Risperidone
Triglycerides are 17.3 mg/dL higher, on average, with olanzapine (from 3.5 to 31.1 mg/dL higher). ●●○
Weight is 2.39 kg greater, on average, with olanzapine (from 1.5 kg to 3.3 kg greater).●●○
Olanzapine vs. Aripiprazole
The risk with olanzapine is 4 times that of aripiprazole (from 1.25x to 12.5x). ●○○
Weight is 4.1 kg greater, on average, with olanzapine (from 2.7 kg to 5.5 kg greater).●○○
Aripiprazole vs. Quetiapine
Triglycerides are 39.4 mg/dL lower with aripiprazole (from 7.4 to 71.3 mg/dL lower). ●○○
Weight is 1.62 kg greater, on average, with quetiapine (from 0.3kg to 3.0 kg greater).●○○
Strength of Evidence Symbols: High = ●●●Moderate = ●●○Low = ●○○Insufficient = ○○○
For other adverse events in direct comparisons, there is limited evidence of no statistically significant difference between second-generation antipsychotics (SGAs) for effects on insulin levels and glucose control, extrapyramidal symptoms, and sedative effects. Strength of Evidence = Low
The risk of elevated prolactin is 2.6 times greater with risperidone than with olanzapine (from 1.7x to 5x). Strength of Evidence = Moderate
The evidence from other head-to-head comparisons is insufficient to permit conclusions about differences in prolactin levels.
Study durations were typically too short to evaluate adverse effects on some important outcomes such as insulin and glycemic control.
Adverse Effects: SGAs Versus SGAs (2 of 2)
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

Current evidence indicates that there are differences between individual second-generation antipsychotics (SGAs) in the risk and severity of key adverse effects.
However, in the absence of direct comparisons, only subjective interpretations of relative risk and severity can be made using data from placebo comparisons.
In the current evidence base of direct comparisons of SGAs, statistically significant differences are noted in rate or severity of dyslipidemia and in adverse changes in weight and body composition.
Among the SGAs, olanzapine exhibits the most severe adverse effects on weight and blood lipids, and risperidone has the strongest effect for elevating prolactin levels, both in placebo comparisons and when compared with olanzapine.
There is limited evidence of no statistically significant difference between SGAs in other direct comparisons of adverse effects (insulin and glucose control, extrapyramidal symptoms, and sedative effects).
Summary of Adverse Effects ofSecond-Generation Antipsychotics
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

Evidence about the use of antipsychotics in children and adolescents is inadequate to support strong conclusions about their comparative effectiveness.
Moderate-strength evidence indicates that second-generation antipsychotics (SGAs) as a class improve clinical global impressions in bipolar disorder, and low-strength evidence supports benefits for treating mania.
Moderate-strength evidence shows that SGAs as a class improve both clinical global impressions and positive and negative symptoms of schizophrenia.
Moderate-strength evidence shows that risperidone is effective for attention deficit hyperactivity disorder and disruptive behavior disorders, and that risperidone and ziprasidone can reduce tics in Tourette’s syndrome.
Limited evidence suggests that SGAs are more effective than first-generation antipsychotics for improving some autistic symptoms of pervasive developmental disorders.
Conclusions About the Benefits and Adverse Effects of Antipsychotics (1 of 2)
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

Adverse effects of second-generation antipsychotics (SGAs) include extrapyramidal symptoms (EPS), somnolence, weight gain, dyslipidemia, and elevated prolactin levels.
In head-to-head comparisons of SGAs, the risk and severity of abnormalities of weight and blood lipids are greatest with olanzapine.
Risperidone raises prolactin levels more than olanzapine. There is low-strength evidence of no differences between SGAs in
effects on insulin and glucose control, EPS, and sedation. The long-term safety of both first-generation antipsychotics (FGAs)
and SGAs and their effectiveness for improving quality-of-life outcomes are not established.
Although SGAs have been perceived as having fewer side effects than FGAs, data are very limited to compare the relative risks of adverse effects. The spectrum of adverse effects should be taken into account, along with possible alternatives, when considering use of these drugs.
Conclusions About the Benefits and Adverse Effects of Antipsychotics (2 of 2)
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.
The effectiveness review revealed areas where the evidence about the effectiveness of first-generation (FGAs) and second-generation (SGAs) in treating pediatric psychiatric disorders is limited or absent, including: Few head-to-head comparisons of FGAs and SGAs exist, either
within or between classes, to demonstrate their effectiveness, benefits, and adverse effects for use in pediatric and young adult populations.
No studies were found that reported pediatric use of antipsychotics to treat obsessive-compulsive disorder, post-traumatic stress disorder, or anorexia nervosa.
Studies of young adults (ages 19–24) were rare. Few studies reported outcomes that are important to patients
(e.g., health-related quality of life, school performance, and legal interactions), and there is no consensus on the minimal clinically important effects to be produced by treatments.
Gaps in Knowledge (1 of 2)
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

Evidence about efficacy and safety over several years is unavailable.
Standardized scales and methods for systematically investigating adverse events are needed.
How the characteristics of key patient subpopulations affect patient-centered outcomes is not understood.
Large-scale effectiveness studies that apply few patient restrictions and closely match typical clinical practice are needed to inform clinical decisionmaking.
Gaps in Knowledge (2 of 2)
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.

The role that antipsychotics may play as one component in the broader array of treatments for child and adolescent psychiatric disorders.
The ability of both first-generation and second-generation antipsychotics to improve symptoms of psychiatric disorders in children, and the differences in strength of evidence for benefits in particular indications.
The risks of extrapyramidal effects, weight gain, and blood lipid abnormalities, and the evidence about differences in risk among drugs in both classes.
The limited evidence about long-term benefits and adverse effects on health and quality of life.
What To Discuss With Your Patients andTheir Caregivers
Seida J, Schouten J, Mousavi S, et al. Comparative Effectiveness Review No. 39. Available at www.effectivehealthcare.ahrq.gov/pedantipsych.cfm.