evolution of cancer treatment- hames - toparx.orgtoparx.org/resources/pictures/evolution of cancer...
TRANSCRIPT
9/21/2016
1
Evolution of Cancer Treatment: The Immune System Versus Cancer
Megan Hames Pollack, PharmD, BCOP, BCPSClinical Pharmacist, Outpatient Medical OncologyVanderbilt‐Ingram Cancer Center, Nashville, TNSeptember 24, 2016
1
Disclosures
Nothing to disclose at this time.
2
Objectives
• Discuss the evolution of treatment in solid tumor oncology.
• Explain the data supporting the use of immunotherapy agents in solid tumor malignancies.
• Recognize appropriate dosing and monitoring for the FDA approved immunotherapy agents.
• List the toxicities that are common among the various immunotherapy agents available.
3 4
Patient Case: RF
• 56yo Caucasian male
• No significant PMH
• Diagnosed with T3N1M1c (stage IV) melanoma in June 1990
5
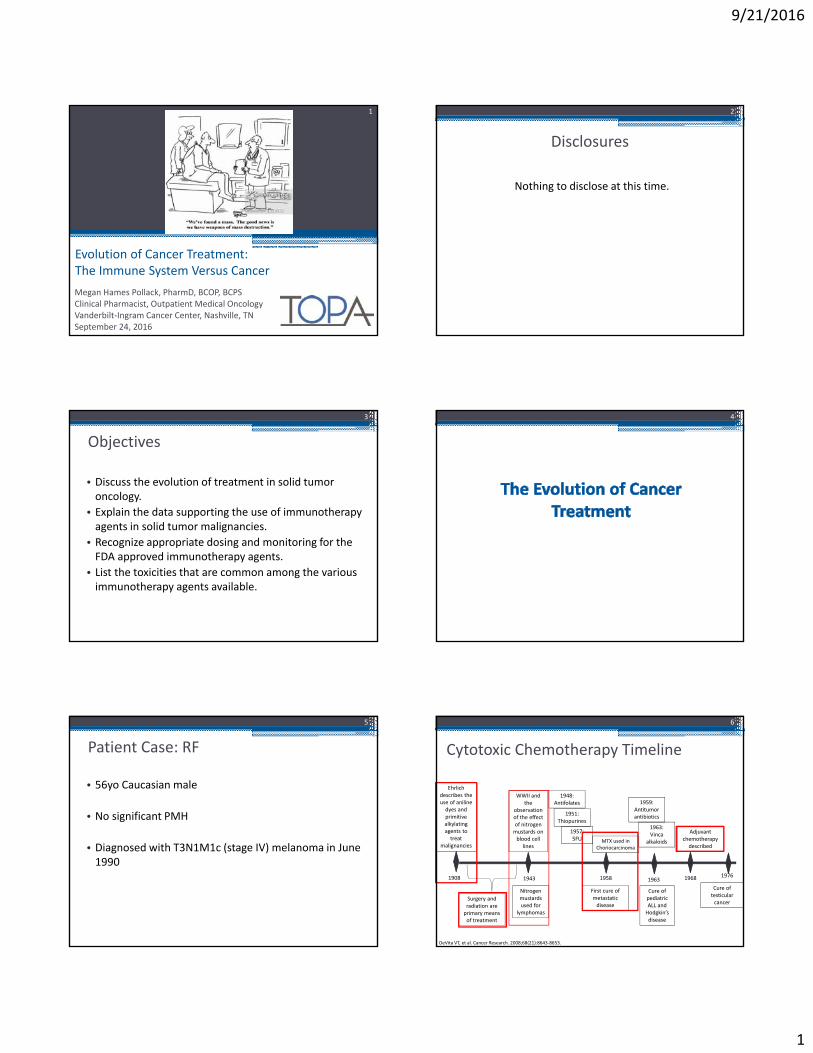
Cytotoxic Chemotherapy Timeline
6
Ehrlich describes the use of aniline dyes and primitive alkylating agents to treat
malignancies
1908
WWII and the
observation of the effect of nitrogen mustards on blood cell
lines
1943
Nitrogen mustards used for
lymphomas
MTX used in Choriocarcinoma
1958
Cure of pediatric ALL and Hodgkin’s disease
1963
Adjuvant chemotherapydescribed
1968
Cure of testicular cancer
1976
1948:Antifolates
1951:Thiopurines
1957:5FU
First cure of metastatic disease
1959:Antitumor antibiotics
1963:Vinca
alkaloids
Surgery and radiation are primary means of treatment
DeVita VT, et al. Cancer Research. 2008;68(21):8643‐8653.
9/21/2016
2
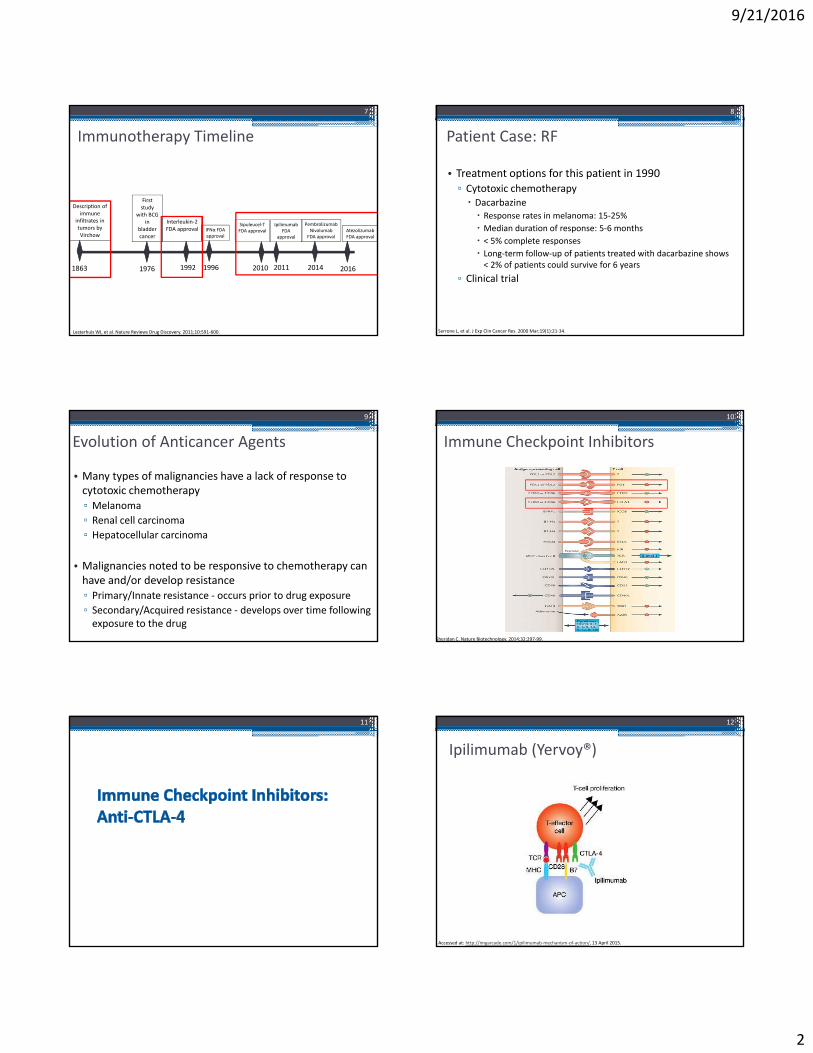
Immunotherapy Timeline
Description of immune
infiltrates in tumors by Virchow
1863
First study
with BCG in
bladder cancer
1976
Interleukin‐2FDA approval
1992
IFNα FDA approval
1996
Sipuleucel‐T FDA approval
2010
Ipilimumab FDA
approval
2011
PembrolizumabNivolumab
FDA approval
2014
Lesterhuis WJ, et al. Nature Reviews Drug Discovery. 2011;10:591‐600.
7
AtezolizumabFDA approval
2016
Patient Case: RF
• Treatment options for this patient in 1990▫ Cytotoxic chemotherapy Dacarbazine Response rates in melanoma: 15‐25%
Median duration of response: 5‐6 months
< 5% complete responses
Long‐term follow‐up of patients treated with dacarbazine shows < 2% of patients could survive for 6 years
▫ Clinical trial
8
Serrone L, et al. J Exp Clin Cancer Res. 2000 Mar;19(1):21‐34.
Evolution of Anticancer Agents
• Many types of malignancies have a lack of response to cytotoxic chemotherapy▫ Melanoma
▫ Renal cell carcinoma
▫ Hepatocellular carcinoma
• Malignancies noted to be responsive to chemotherapy can have and/or develop resistance▫ Primary/Innate resistance ‐ occurs prior to drug exposure
▫ Secondary/Acquired resistance ‐ develops over time following exposure to the drug
9
Immune Checkpoint Inhibitors
10
Sheridan C. Nature Biotechnology. 2014;32:297‐99.
11
Ipilimumab (Yervoy®)
12
Accessed at: http://imgarcade.com/1/ipilimumab‐mechanism‐of‐action/, 13 April 2015.

9/21/2016
3
Ipilimumab Indications and Dosage
• FDA approved indications▫ Unresectable or metastatic melanoma 3mg/kg IV q 3 weeks x 4 doses
▫ Adjuvant treatment of stage III or IV resected melanoma 10mg/kg IV q 3 weeks x 4 doses then q 12 weeks up to 3 years
Yervoy [package insert]. Princeton, NJ. Bristol‐Myers Squibb Co.; 2016.
Ipilimumab (Yervoy®)
14
Maio M., et al. Journal of Clinical Oncology. 2015; 33:1191‐1196.
CTLA‐4 Inhibitor Toxicities
Toxicity Percentage of Patients
Fatigue 41
Diarrhea 32
Pruritus 31
Rash 29
Colitis 8
15
Most Common Adverse Reactions CTCAE Grade 1‐5
Severe to Fatal Immune‐Related Adverse Events (irAEs)
Toxicity Percentage of Patients
Enterocolitis 7
Hypopituitarism 4
Dermatitis 2
Nephritis 1
Hepatotoxicity 1
Neuropathy 1
Eosinophilia 1
Pericarditis < 1
Pneumonitis < 1
Meningitis < 1
Hodi FS, et al. N Engl J Med. 2010;363(8):711‐23.
Patient Case: RF
• Diagnosed with T1a (stage I) melanoma February 2001▫ Surgical resection – 3/2001
• Remained disease free until March 2010▫ Nodal recurrence▫ T3N3 (stage III)
• Complete surgical resection and left axillary lymph node dissection March 2010
16
Patient Case: RF
• Presents to medical oncology clinic to discuss options to prevent recurrence▫ Interferon alfa‐2b▫ Clinical trial
• Enrolled on MEL0823▫ Ipilimumab versus placebo
17
Patient Case: RF
18
6/21/10 7/12/10
9/21/2016
4
Patient Case: RF
• Patient presents to the ED on 7/14/2010▫ Bloody diarrhea with 8‐12 bowel movements per day and febrile to 101.5F
• Vital signs▫ Temp 100.6F
▫ HR 92▫ BP 130/72▫ RR 20
19
137
4.3
104
24
21
1.291 6.2 232
15.2
45
ANC = 2.85
Patient Case: RF
• Colonoscopy report▫ Evidence of moderately severe colitis in the entire colon The mucosa appeared edematous, erythematous, and friable with bleeding on contact
• Pathology report▫ There is a marked mononuclear infiltrate within the lamina properia that also focally involves glandular epithelium
20
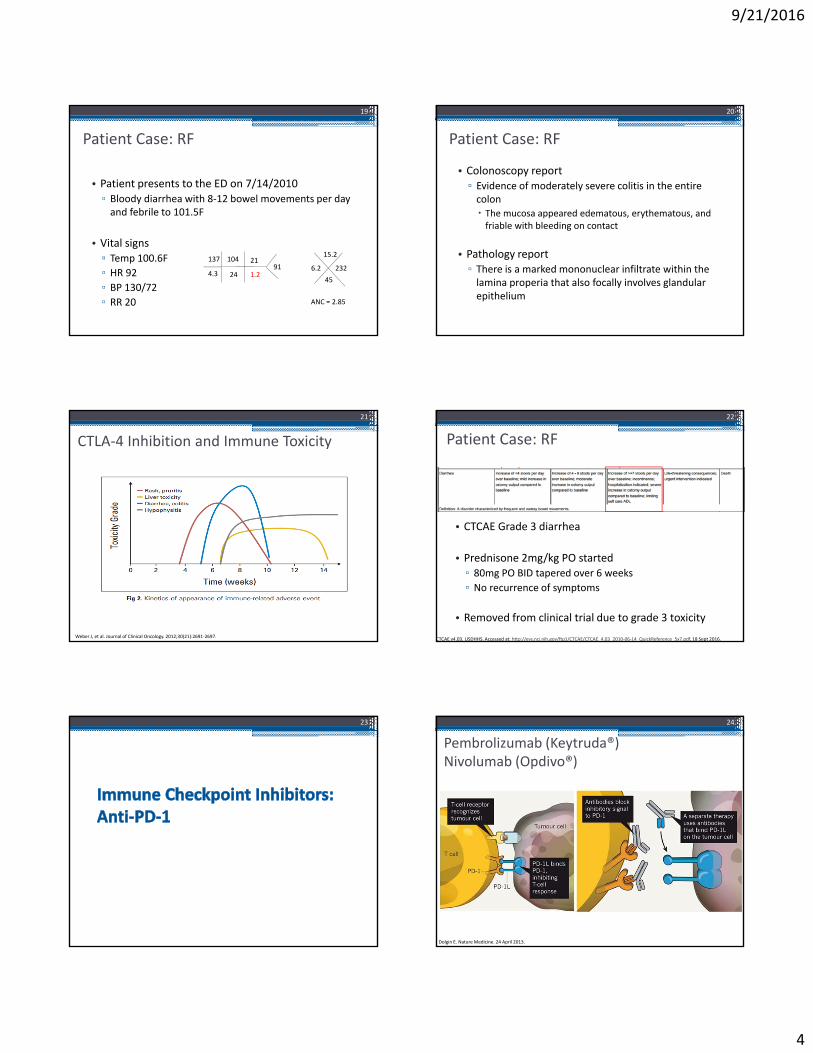
CTLA‐4 Inhibition and Immune Toxicity
21
Weber J, et al. Journal of Clinical Oncology. 2012;30(21):2691‐2697.
Patient Case: RF
• CTCAE Grade 3 diarrhea
• Prednisone 2mg/kg PO started▫ 80mg PO BID tapered over 6 weeks
▫ No recurrence of symptoms
• Removed from clinical trial due to grade 3 toxicity
22
CTCAE v4.03. USDHHS. Accessed at: http://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03_2010‐06‐14_QuickReference_5x7.pdf, 18 Sept 2016.
23
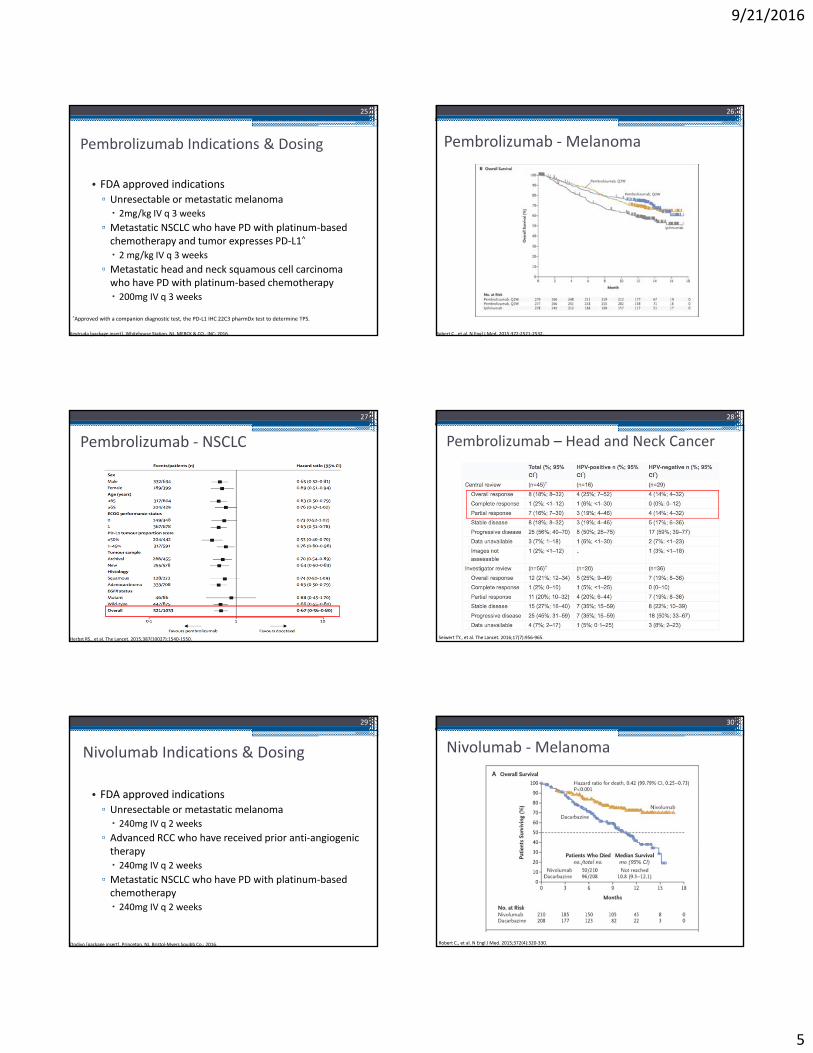
Pembrolizumab (Keytruda®)Nivolumab (Opdivo®)
24
Dolgin E. Nature Medicine. 24 April 2013.
9/21/2016
5
Pembrolizumab Indications & Dosing
• FDA approved indications▫ Unresectable or metastatic melanoma 2mg/kg IV q 3 weeks
▫ Metastatic NSCLC who have PD with platinum‐based chemotherapy and tumor expresses PD‐L1^
2 mg/kg IV q 3 weeks
▫ Metastatic head and neck squamous cell carcinoma who have PD with platinum‐based chemotherapy 200mg IV q 3 weeks
25
^Approved with a companion diagnostic test, the PD‐L1 IHC 22C3 pharmDx test to determine TPS.
Keytruda [package insert]. Whitehouse Station, NJ. MERCK & CO., INC; 2016.
Pembrolizumab ‐Melanoma
26
Robert C., et al. N Engl J Med. 2015;372:2521‐2532.
Pembrolizumab ‐ NSCLC
27
Herbst RS., et al. The Lancet. 2015;387(10027):1540‐1550.
Pembrolizumab – Head and Neck Cancer
28
Seiwert TY., et al. The Lancet. 2016;17(7):956‐965.
Nivolumab Indications & Dosing
• FDA approved indications▫ Unresectable or metastatic melanoma 240mg IV q 2 weeks
▫ Advanced RCC who have received prior anti‐angiogenic therapy 240mg IV q 2 weeks
▫ Metastatic NSCLC who have PD with platinum‐based chemotherapy 240mg IV q 2 weeks
29
Opdivo [package insert]. Princeton, NJ. Bristol‐Myers Squibb Co.; 2016.
Nivolumab ‐Melanoma
30
Robert C., et al. N Engl J Med. 2015;372(4):320‐330.
9/21/2016
6
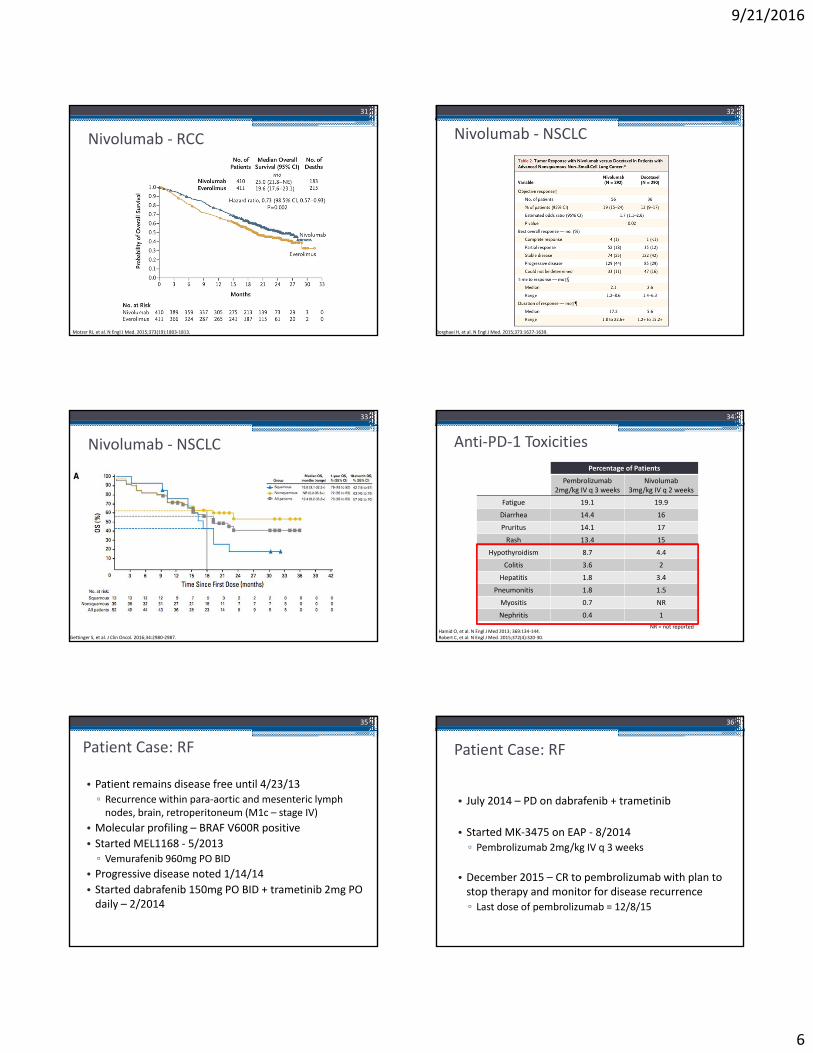
Nivolumab ‐ RCC
31
Motzer RJ, et al. N Engl J Med. 2015;373(19):1803‐1813.
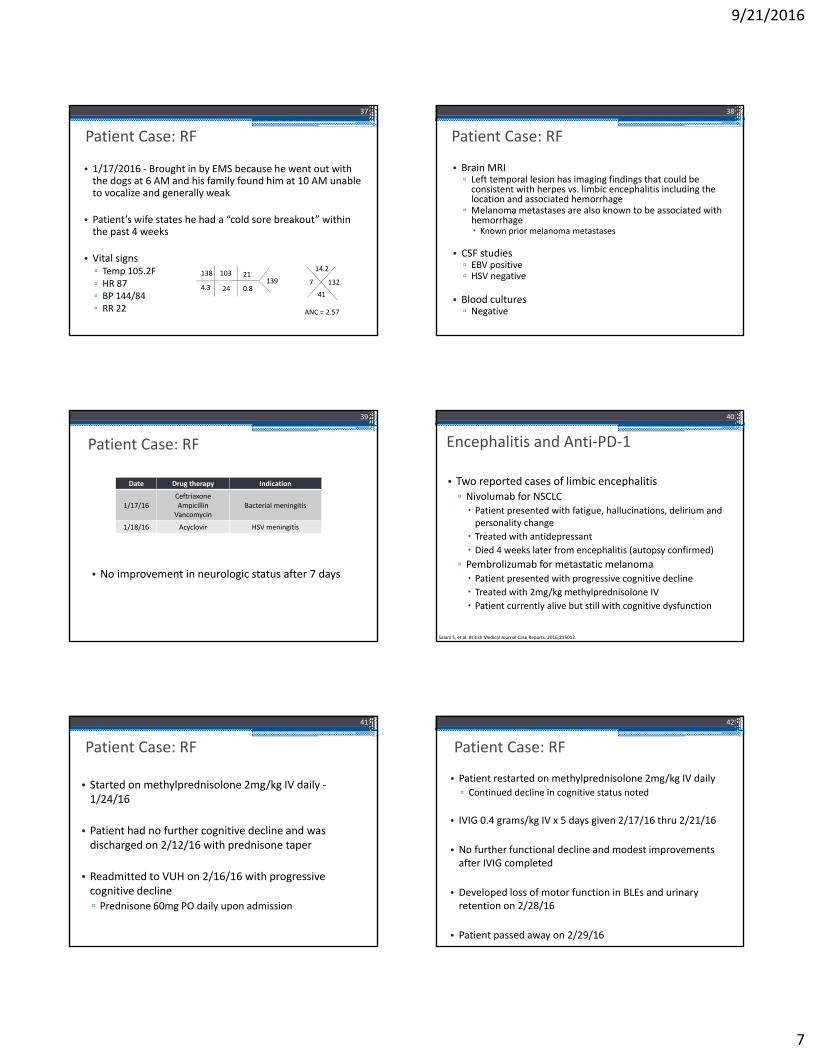
Nivolumab ‐ NSCLC
32
Borghaei H, et al. N Engl J Med. 2015;373:1627‐1639.
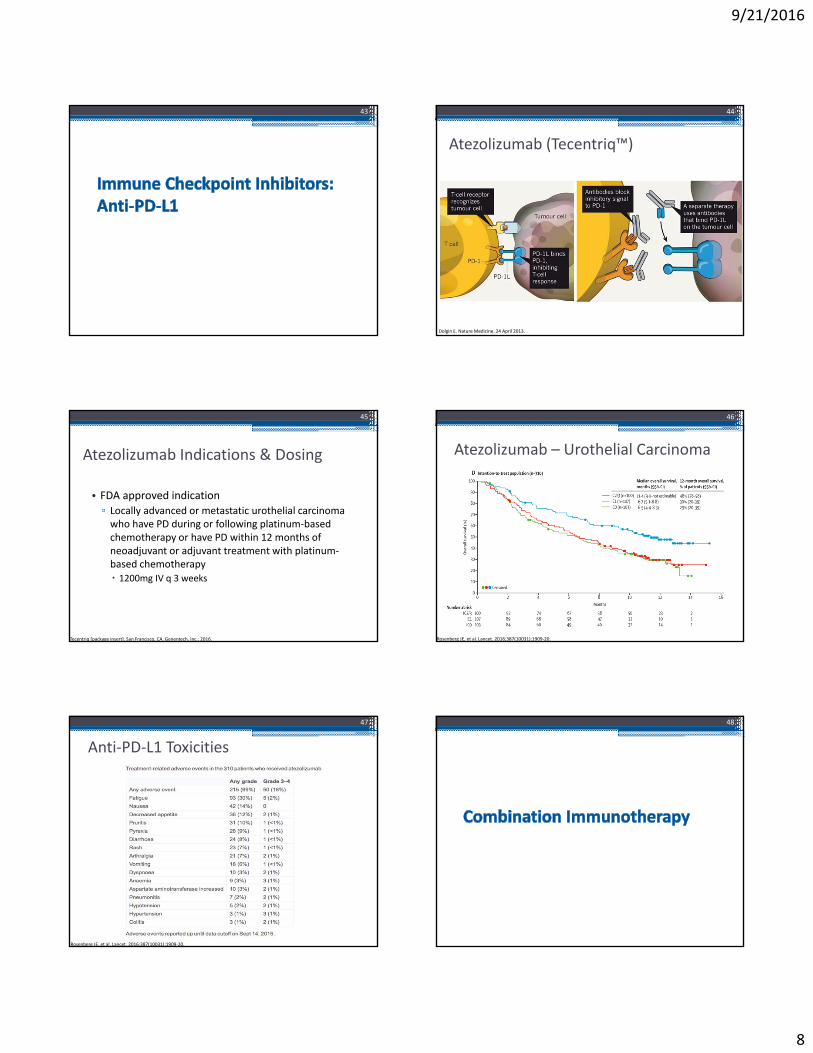
Nivolumab ‐ NSCLC
33
Gettinger S, et al. J Clin Oncol. 2016;34:2980‐2987.
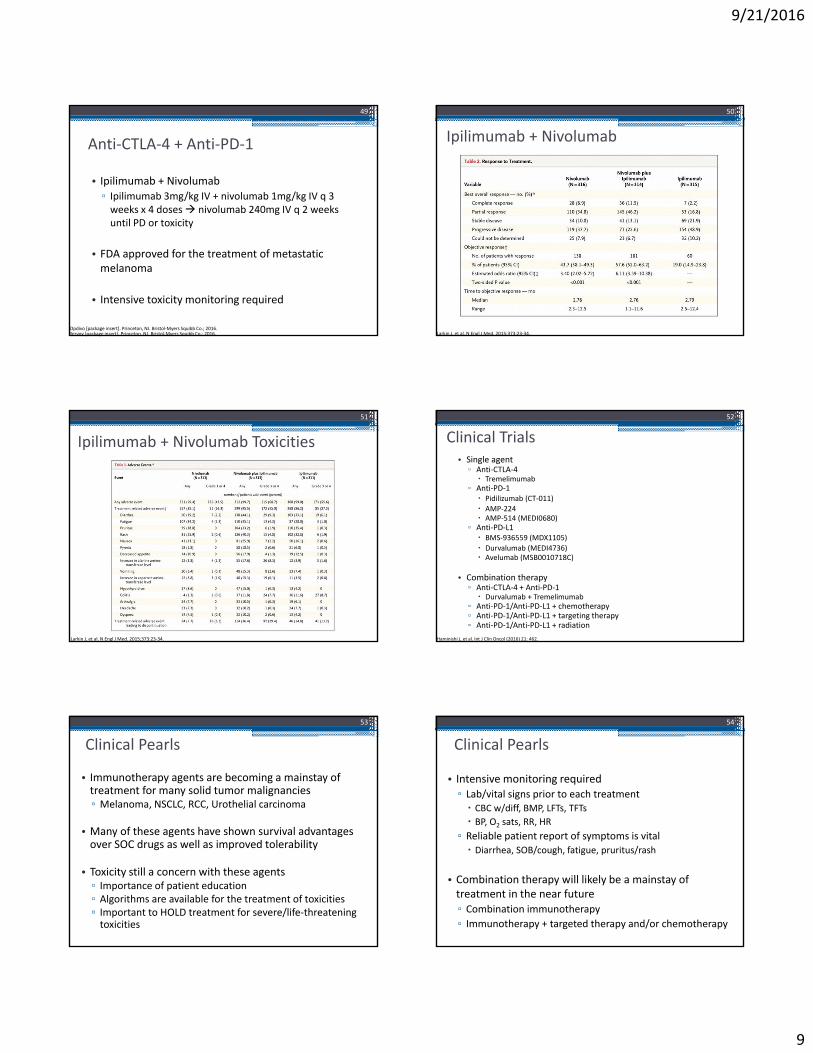
Anti‐PD‐1 Toxicities
Percentage of Patients
Pembrolizumab2mg/kg IV q 3 weeks
Nivolumab3mg/kg IV q 2 weeks
Fatigue 19.1 19.9
Diarrhea 14.4 16
Pruritus 14.1 17
Rash 13.4 15
Hypothyroidism 8.7 4.4
Colitis 3.6 2
Hepatitis 1.8 3.4
Pneumonitis 1.8 1.5
Myositis 0.7 NR
Nephritis 0.4 1
34
NR = not reportedHamid O, et al. N Engl J Med 2013; 369:134‐144.Robert C, et al. N Engl J Med. 2015;372(4):320‐30.
Patient Case: RF
• Patient remains disease free until 4/23/13▫ Recurrence within para‐aortic and mesenteric lymph nodes, brain, retroperitoneum (M1c – stage IV)
• Molecular profiling – BRAF V600R positive
• Started MEL1168 ‐ 5/2013▫ Vemurafenib 960mg PO BID
• Progressive disease noted 1/14/14• Started dabrafenib 150mg PO BID + trametinib 2mg PO daily – 2/2014
35
Patient Case: RF
• July 2014 – PD on dabrafenib + trametinib
• Started MK‐3475 on EAP ‐ 8/2014▫ Pembrolizumab 2mg/kg IV q 3 weeks
• December 2015 – CR to pembrolizumab with plan to stop therapy and monitor for disease recurrence▫ Last dose of pembrolizumab = 12/8/15
36
9/21/2016
7
Patient Case: RF
• 1/17/2016 ‐ Brought in by EMS because he went out with the dogs at 6 AM and his family found him at 10 AM unable to vocalize and generally weak
• Patient’s wife states he had a “cold sore breakout” within the past 4 weeks
• Vital signs▫ Temp 105.2F▫ HR 87▫ BP 144/84▫ RR 22
37
138
4.3
103
24
21
0.8139 7 132
14.2
41
ANC = 2.57
Patient Case: RF
• Brain MRI▫ Left temporal lesion has imaging findings that could be consistent with herpes vs. limbic encephalitis including the location and associated hemorrhage
▫ Melanoma metastases are also known to be associated with hemorrhage Known prior melanoma metastases
• CSF studies▫ EBV positive▫ HSV negative
• Blood cultures▫ Negative
38
Patient Case: RF
• No improvement in neurologic status after 7 days
39
Date Drug therapy Indication
1/17/16CeftriaxoneAmpicillinVancomycin
Bacterial meningitis
1/18/16 Acyclovir HSV meningitis
Encephalitis and Anti‐PD‐1
• Two reported cases of limbic encephalitis▫ Nivolumab for NSCLC Patient presented with fatigue, hallucinations, delirium and personality change
Treated with antidepressant
Died 4 weeks later from encephalitis (autopsy confirmed)
▫ Pembrolizumab for metastatic melanoma Patient presented with progressive cognitive decline
Treated with 2mg/kg methylprednisolone IV
Patient currently alive but still with cognitive dysfunction
40
Salam S, et al. British Medical Journal Case Reports. 2016;215012.
Patient Case: RF
• Started on methylprednisolone 2mg/kg IV daily ‐1/24/16
• Patient had no further cognitive decline and was discharged on 2/12/16 with prednisone taper
• Readmitted to VUH on 2/16/16 with progressive cognitive decline▫ Prednisone 60mg PO daily upon admission
41
Patient Case: RF
• Patient restarted on methylprednisolone 2mg/kg IV daily▫ Continued decline in cognitive status noted
• IVIG 0.4 grams/kg IV x 5 days given 2/17/16 thru 2/21/16
• No further functional decline and modest improvements after IVIG completed
• Developed loss of motor function in BLEs and urinary retention on 2/28/16
• Patient passed away on 2/29/16
42
9/21/2016
8
43
Atezolizumab (Tecentriq™)
44
Dolgin E. Nature Medicine. 24 April 2013.
Atezolizumab Indications & Dosing
• FDA approved indication▫ Locally advanced or metastatic urothelial carcinoma who have PD during or following platinum‐based chemotherapy or have PD within 12 months of neoadjuvant or adjuvant treatment with platinum‐based chemotherapy 1200mg IV q 3 weeks
45
Tecentriq [package insert]. San Francisco, CA. Genentech, Inc.; 2016.
Atezolizumab – Urothelial Carcinoma
46
Rosenberg JE, et al. Lancet. 2016;387(10031):1909‐20.
Anti‐PD‐L1 Toxicities
47
Rosenberg JE, et al. Lancet. 2016;387(10031):1909‐20.
48
9/21/2016
9
Anti‐CTLA‐4 + Anti‐PD‐1
• Ipilimumab + Nivolumab▫ Ipilimumab 3mg/kg IV + nivolumab 1mg/kg IV q 3 weeks x 4 doses nivolumab 240mg IV q 2 weeks until PD or toxicity
• FDA approved for the treatment of metastatic melanoma
• Intensive toxicity monitoring required
49
Yervoy [package insert]. Princeton, NJ. Bristol‐Myers Squibb Co.; 2016.Opdivo [package insert]. Princeton, NJ. Bristol‐Myers Squibb Co.; 2016.
Ipilimumab + Nivolumab
50
Larkin J, et al. N Engl J Med. 2015;373:23‐34.
Ipilimumab + Nivolumab Toxicities
51
Larkin J, et al. N Engl J Med. 2015;373:23‐34.
Clinical Trials• Single agent▫ Anti‐CTLA‐4 Tremelimumab
▫ Anti‐PD‐1 Pidilizumab (CT‐011)
AMP‐224 AMP‐514 (MEDI0680)
▫ Anti‐PD‐L1 BMS‐936559 (MDX1105)
Durvalumab (MEDI4736) Avelumab (MSB0010718C)
• Combination therapy▫ Anti‐CTLA‐4 + Anti‐PD‐1 Durvalumab + Tremelimumab
▫ Anti‐PD‐1/Anti‐PD‐L1 + chemotherapy▫ Anti‐PD‐1/Anti‐PD‐L1 + targeting therapy▫ Anti‐PD‐1/Anti‐PD‐L1 + radiation
52
Haminishi J, et al. Int J Clin Oncol (2016) 21: 462.
Clinical Pearls
• Immunotherapy agents are becoming a mainstay of treatment for many solid tumor malignancies▫ Melanoma, NSCLC, RCC, Urothelial carcinoma
• Many of these agents have shown survival advantages over SOC drugs as well as improved tolerability
• Toxicity still a concern with these agents▫ Importance of patient education▫ Algorithms are available for the treatment of toxicities▫ Important to HOLD treatment for severe/life‐threatening toxicities
53
Clinical Pearls
• Intensive monitoring required▫ Lab/vital signs prior to each treatment CBC w/diff, BMP, LFTs, TFTs
BP, O2 sats, RR, HR
▫ Reliable patient report of symptoms is vital Diarrhea, SOB/cough, fatigue, pruritus/rash
• Combination therapy will likely be a mainstay of treatment in the near future▫ Combination immunotherapy
▫ Immunotherapy + targeted therapy and/or chemotherapy
54
9/21/2016
10
Question 1
• Ipilimumab is a anti‐CTLA‐4 monoclonal antibody and is the first drug to improve OS in metastatic melanoma.A. True
B. False
55
Question 2
• Which agents are FDA approved for the first line treatment of metastatic melanoma?A. Nivolumab
B. Pembrolizumab
C. Atezolizumab
D. All of the above
E. A and B only
56
Question 3
• Patient AD presents to the ED complaining of SOB and new onset cough. She states that she has “lung cancer” and is being treated with “chemo” by Dr. Horn. She is currently febrile to 101F, otherwise her labs and vital signs are all within normal limits. What is the next step for treatment of this patient?A. Assume she is being treated with cytotoxic chemotherapy;
draw cultures and start antibiotics immediately
B. Determine what treatment she is actually getting as this will help with determining the cause of SOB/cough
C. Do nothing – lung cancer patients often have this problem
57
Question 4
• Atezolizumab has data supporting its use in patients with urothelial carcinoma that have had a recurrence of disease within 6 months of platinum based chemotherapy.A. True
B. False
58
Evolution of Cancer Treatment: The Immune System Versus Cancer
Megan Hames Pollack, PharmD, BCOP, BCPSClinical Pharmacist, Outpatient Medical OncologyVanderbilt‐Ingram Cancer Center, Nashville, TNSeptember 24, 2016
59