evergreen: a child and youth mental health framework for canada · dalhousie university, sun life...
TRANSCRIPT

Evergreen:
A Child and Youth Mental Health
Framework for Canada
A project of the Child and Youth Advisory
Committee of the
Mental Health Commission of Canada
July 2010

Evergreen Framework
- 2 -
Foreword
We did not want to push people to believe in our vision. We wanted to inspire
people to participate in the process of moving toward and creating the vision.
Appropriately, there is greater awareness and expectation today from people that they be
informed, and engaged in decisions that affect their lives. People want to see themselves
represented in decisions made.
From inception, the Evergreen Project has prioritized the active involvement of people from
across Canada in all aspects of creating a framework specific to child and youth mental health. In
this spirit of collaboration young people, parents, educators, mental health professionals, and
countless others involved in the lives of young people, came together using online technologies
to build Evergreen from the ground up.
The level of active involvement in Evergreen’s consultation process speaks to the interest in this
subject across Canada and underscores the concern Canadians have for matters related to child
and youth mental health and illness. The message surfacing throughout Evergreen’s development
was one of HOPE. The message offered by the Evergreen Framework is one of HOPE. Hope
gives young people, parents, families and professionals the ability to dream; an ability that is
truly healing. We hope that one day we will live in a world with a greater understanding of
mental health, a world equipped to best meet the needs of young people and their families, and a
world where the voice of young people and their families can be heard, respected, and acted
upon. In many ways, a world that reflects the inclusiveness and dreams of positive change for
child and youth mental health is embedded in the Evergreen Framework.
For too long, the mental health of young people has not been priority across Canada. For too
long, child and youth mental health has been orphaned within a mental health system that is itself
orphaned within Canadian health care. The time to act, to create positive change is now.
Evergreen can be part of that change. The recent publication of the Mental Health Commission
of Canada: Toward Recovery and Wellbeing: A Framework for a Mental Health Strategy for
Canada has outlined some possible directions toward this change. Evergreen can help provide
policy makers, planners, service providers, service users, families, advocates and the wider
public with nationally informed explicit values and strategic directions that can be used to help
frame and direct this needed change.
Together, young people, parents and professionals share a sense of urgency to transform the
child and youth mental health system. Being heard is a starting point, but being heard is not
enough. Young people, parents and families want to see practices, policies, programs and
services that reflect their values, values that are encapsulated in the Evergreen Framework. For
example, mental health is a right, not a privilege. If these values inform the transformation of the
child and youth mental health system, we feel certain that young people and families will engage
to assist in the creation of positive change, just as they engaged to help create the Evergreen
Framework.
Evergreen Framework
- 3 -
We hope that the values and strategic directions offered by the Evergreen Framework guide the
creation of practices, policies, and programs throughout Canada that truly reflect the needs
identified by those affected the most: young people and families. Indeed, such a paradigm shift is
endorsed by Goal One of Toward Recovery & Well Being, that people of all ages living with
mental health problems and illnesses are actively engaged and supported in their journeys. We
are hopeful that policy makers and service providers will wholeheartedly embrace such a shift.
As we have seen Evergreen develop using a national collaborative process we are confident that
this paradigm will be the way of the future. We will all, collectively, have to work together to
ensure absolute uptake of this vital and important paradigm shift.
We thank all those who participated in helping create the Evergreen Framework and
acknowledge the hard work of the leadership team of Dr. Stan Kutcher and Alan McLuckie and
the National and International Advisory Committees, Drafting Committee, Youth Advisory
Committee and members of the Mental Health Commission of Canada family. Most importantly,
we thank all the young people, parents, family members, mental health professionals, educators
and countless others across Canada who took the time and the risk to share their experiences and
ideas—without you Evergreen would not exist.
Bronwyn Loucks
Member, Youth Advisory Council,
Mental Health Commission of Canada
Keli Anderson
Parent Member, Child and Youth Advisory Committee,
Mental Health Commission of Canada
Dr. Simon Davidson
Chair, Child and Youth Advisory Committee,
Mental Health Commission of Canada
Evergreen Framework
- 4 -
AUTHORSHIP AND FUNDING
This project has been made possible through funding from the Mental Health Commission of
Canada. The work of the Mental Health Commission of Canada is supported by a grant from
Health Canada. Additional support for this project was provided by the IWK Health Centre,
Dalhousie University, Sun Life Financial, The Meighen Foundation, and The Weldon
Foundation.
Evergreen was directed, synthesized and created in its current form by Dr. Stan Kutcher and Mr.
Alan McLuckie. Members of the Drafting Committee (see Appendix B) contributed to the
writing of the drafts of Evergreen.
Recommended Citation:
Kutcher, S. and McLuckie, A. for the Child and Youth Advisory Committee, Mental Health
Commission of Canada. (2010). Evergreen: A child and youth mental health framework for
Canada. Calgary, AB: Mental Health Commission of Canada.
Evergreen Framework
- 5 -
Acknowledgements
On behalf of the Child and Youth Advisory Committee of the Mental Health Commission of
Canada (MHCC), we would like to thank those who helped develop Evergreen.
Particularly:
The members of the Child and Youth Advisory Committee of the MHCC
Ms. Brenda Leung, Dr. Gillian Mulvale, Ms. Janice Popp and the staff at the MHCC
Ms. Karleena Suppiah and the communications team at the MHCC, and Ms. Nicole
Fraughton and the communications team at the IWK Health Centre
Mr. Peter Dudding, and the staff of the Child Welfare League of Canada
Ms. Shaleen Jones, the staff and young people of Laing House in Halifax; Ms. Cathy
Dyer and the young people of the New Mentality; and Ms. Troy Stooke and the young
people of the Southern Alberta Child & Youth Health Network’s Child & Youth
Advisory Council
Ms. Maria Luisa Contursi http://www.mindyourmind.ca
Socialtext
Ms. Denise Nevo, Professional Certified Translator and Professor, Department of
Modern Languages, Mount Saint Vincent University
Ms. Tracy McKenzie, Mr. David Venn, Ms. Yifeng Wei, Ms. Magda Szumilas, Ms.
Jessica Wishart, Ms. Julie O’Grady, Ms. Christina Biluk and other members of the Sun
Life Financial Chair in Adolescent Mental Health Team
The Sun Life Financial Chair Youth Advisory Council
Members of the Evergreen Drafting Committee (see Appendix B)
Members of the Evergreen Advisory Committee (see Appendix B)
Members of the Evergreen International Advisory Committee (see Appendix B)
Today’s Parent magazine
All the young people, parents, family members, educators, health providers, professional
organizations, institutions, non-government organizations, policy makers and individuals
who shared their ideas, stories and encouragement throughout the creation of Evergreen

Evergreen Framework
- 6 -
Table of Contents
EXECUTIVE SUMMARY ...................................................................................................................................... - 7 -
PREAMBLE .......................................................................................................................................................... - 10 -
VALUES ................................................................................................................................................................ - 15 -
1. HUMAN RIGHTS ............................................................................................................................................ - 15 - 2. DIGNITY, RESPECT, AND DIVERSITY ........................................................................................................... - 15 - 3. BEST AVAILABLE EVIDENCE ........................................................................................................................ - 15 - 4. CHOICE, OPPORTUNITY AND RESPONSIBILITY ........................................................................................... - 16 - 5. COLLABORATION, CONTINUITY AND COMMUNITY .................................................................................... - 16 - 6. ACCESS TO INFORMATION, PROGRAMS AND SERVICES .............................................................................. - 16 -
STRATEGIC DIRECTIONS ............................................................................................................................... - 17 -
PROMOTION ....................................................................................................................................................... - 19 - PREVENTION ...................................................................................................................................................... - 23 - INTERVENTION & ONGOING CARE .................................................................................................................... - 28 - RESEARCH & EVALUATION ............................................................................................................................... - 33 -
SUGGESTED READINGS ................................................................................................................................. - 36 -
REFERENCES USED IN THE PREPARATION OF EVERGREEN ............................................................ - 36 -
APPENDIX A: EVERGREEN’S DEVELOPMENT PROCESS ..................................................................... - 50 -
EVERGREEN’S DEVELOPMENT TEAM .................................................................................................................. - 50 - CREATING THE EVERGREEN FRAMEWORK DOCUMENT ................................................................................... - 51 -
Phase 1: Values ............................................................................................................................................ - 52 - Phase 2: Strategic Directions ....................................................................................................................... - 54 -
APPENDIX B - EVERGREEN’S COMMITTEE MEMBERSHIP ................................................................... - 56 -
DRAFTING COMMITTEE .................................................................................................................................... - 56 - NATIONAL ADVISORY COMMITTEE ................................................................................................................. - 57 - YOUTH ADVISORY COMMITTEE ....................................................................................................................... - 61 - INTERNATIONAL ADVISORY COMMITTEE ........................................................................................................ - 61 -

Evergreen Framework
- 7 -
Executive Summary
“We must start treating people with mental health challenges with respect at all levels.”
-Mental Health Professional
Background & Context
In 2006, the Standing Senate Committee on Social Affairs, Science and Technology published its
report on mental health in Canada: Out of The Shadows at Last: Transforming Mental Health,
Mental Illness and Addiction Services in Canada (Kirby & Keon, 2006). Cognizant of the need
to transform how mental health care is delivered across Canada, it called for the creation of the
Mental Health Commission of Canada (MHCC), which was established by the Government of
Canada in 2008. Subsequently, the Child and Youth Advisory Committee (CYAC) of the MHCC
proposed to develop a national child and youth mental health framework that could be used by
governments, institutions and organizations to assist with the development of mental health
policies, plans, programs and services.
The purpose of Evergreen is twofold. One, is to provide the MHCC, through its CYAC,
information that can be used to support its national mental health mandate. The second, is to
provide a framework of values and strategic directions to assist governments and other
authorities responsible for child and youth mental health in Canada in their address of child and
youth mental health. This framework will also be made available to young people, parents,
service providers, professionals and the public to facilitate dialogue amongst all stakeholders
about what needs to be done to address child and youth mental health across Canada, and how
that could be accomplished. Thus, Evergreen is informing, supportive and encouraging of
collaborative action to deal with this urgent Canadian need.
Consultation and Development Process
Evergreen was developed by individuals from across Canada and around the world with
expertise (professional and lived experience) in child and youth health. Four committees
(Drafting, Advisory, International Advisory and Youth Advisory), an extensive on-line public
consultation and two conference-based public consultations informed Evergreen’s creation (see
Appendix A for a description of Evergreen’s development process).
Evergreen – What is it?
Evergreen is a resource that can be used by governments, institutions and organizations to help
develop child and youth mental health initiatives. It can also be used by young people, parents,
professionals and others to assist them in informing their thoughts, choices and priorities
regarding child and youth mental health policies, plans, programs and services.
Evergreen contains values as well as strategic directions meant to enhance and improve mental
health and mental health care across Canada. Each strategic direction can be fulfilled by one or
more specific initiatives (unique programs, services or activities) which should all be based on
the values of Evergreen. The strategic directions are not prescriptive, rather they provide a

Evergreen Framework
- 8 -
framework within which specific initiatives can be developed to help establish and maintain
mental health of populations, as well as effectively address mental disorders.
Evergreen explicitly states the values upon which it is based. Its strategic directions are meant to
be applied in a manner consistent with the following values:
1. Human Rights
2. Dignity, Respect and Diversity
3. Best Available Evidence
4. Choice, Opportunity and Responsibility
5. Collaboration, Continuity and Community
6. Access to Information, Programs and Services
Evergreen’s strategic directions are organized into the following four categories:
1. Promotion
2. Prevention
3. Intervention and Ongoing Care
4. Research and Evaluation
Evergreen is not a ―one size fits all‖ approach to child and youth mental health. The list of
strategic directions, although comprehensive, is not exhaustive. There may be additional strategic
directions not included here that can be identified and used. However, all strategic directions
chosen must be applied in a manner consistent with the values identified in Evergreen. Some
strategic directions may need to be adapted to conform to local realities and unique
circumstances. Additionally, there may be many different programs, services, or activities that
can be used to operationalize any strategic direction. Evergreen does not address which of the
many possibilities should be used to operationalize the strategic directions. Such a decision
should be made by those responsible for child and youth mental health policy, plans, programs
and services and should be further informed by local realities. The choice of specific programs,
services or activities however should likewise be based on Evergreen’s values. Evergreen also
recognizes that many programs, services and activities currently in use throughout Canada work
well, and need not be replaced, but may benefit from augmentation or enhancement. Existing,
augmented or enhanced programs, services and activities should also be consistent with
Evergreen’s values. A government official participating in Evergreen’s consultation process
underlined this point by stating:
“We should not lose sight of the success of community mental health, education,
youth justice and health services. There are countless examples of children, youth
and families whose needs are well met by existing services and supports. We need to
build upon strengths, enhance what exists and refrain from total re-invention…”
-Government Official
The contents of Evergreen are not set in stone. As new information and better understanding
develops, Evergreen can be amended to reflect these changes. While the values upon which
Evergreen is based will persist, some strategic directions currently suggested will stand the test

Evergreen Framework
- 9 -
of time, while others may not. These may need to be modified or changed over time. Others may
need to be added. As its name suggests, Evergreen is meant to be updated, perhaps every five to
seven years, and we therefore strongly encourage appropriate national bodies to assume this
challenge.

Evergreen Framework
- 10 -
Preamble
Participants in Evergreen’s consultation process expressed strong anticipation that this
framework would be useful in improving mental health of and mental health care for, children
and youth across Canada. Two recurrent themes: hope and commitment were consistently
voiced. Hope for a future where child and youth mental health is a national priority and
commitment from all stakeholders to work together to achieve this goal.
“I am pleased to see that a framework for infant, child and youth mental health
is being looked at with serious intentions, it may allow for better services and more
proactive intervention options rather than reactive measures that are in place now.”
-Friend of a young person with a mental illness
It is now well appreciated that mental disorders in young people are the most prevalent medical
conditions causing disability in this population. Most mental disorders begin prior to age twenty-
five and tend to be chronic, with substantial negative short and long term outcomes. They are
associated with poor academic and occupational success, substantial personal, interpersonal and
family difficulties, increased risk for many physical illnesses, shorter life expectancy and
economic burden. Good evidence exists to support specific interventions that can improve the
mental health and wellbeing of populations. Early interventions and easily accessed effective
treatments may improve both short and long-term outcomes. These outcomes include, but are not
limited to, the prevention of some disorders, reduction in disability and enhanced civic and
economic participation in a cost-effective manner. Presently, in Canada, few of these domains
have been adequately addressed.
Too many young people living in Canada are ―at risk‖ for poor mental health outcomes. The
majority of young people who require specialized mental health care do not receive it.
Historically, service silos have artificially segregated care provision, making it difficult to
address whole-person needs of young people and families. Some individuals and some groups
residing in Canada are not treated equally with regards to accessing quality and appropriately
responsive mental health programs and services. Research into child and youth mental health
lags behind other research activities within health care. Stigma against those living with a mental
disorder and their families may go unchallenged. Substantial discrepancies in funding for and
provision of mental health services exist across Canada. These are not newly discovered
concerns.
Recent initiatives have begun to elevate interest in addressing child and youth mental health
nationally. For example, child and youth mental health policies have been established in a few
provinces. A number of reports, including A Canada Fit for Children (Canada, 2004) and
Reaching for the Top, (Leitch, 2007) have recognized the need to priorize child and youth mental
health. The Standing Senate Committee on Social Affairs, Science and Technology, Out of the
Shadows at Last: Transforming Mental Health, Mental Illness and Addiction Services in
Canada, identified the need for immediate national action in mental health, especially with
regards to children and youth (Kirby & Keon, 2006). Recently, the Government of Canada
created the MHCC which in turn recognized the importance of child and youth mental health by
establishing the Child and Youth Advisory Committee of the MHCC Board. Under this mandate,

Evergreen Framework
- 11 -
a number of national child and youth mental health initiatives have been launched, including but
not limited to Evergreen.
Canadians have realized that meaningful changes must be made to how we approach child and
youth mental health. These range from how the social determinants of health are addressed all
the way to improving the provision of responsible and appropriate specialty mental health
services, based on best available evidence. Maintaining the status quo within Canada’s mental
health system is no longer an option as substantive changes in how we think about and address
child and youth mental health are required. As one mental health professional noted, “We can
not talk about how to fix the system – we have no system.” Another mental health professional
commented, “If we were going to start from scratch and build a child and youth mental health
system what we would create would be light years different from that which we have.”
Young people, parents and families are exercising their rights by becoming active participants in
all aspects of child and youth mental health. As identified in Evergreen, there is emerging
agreement about what needs to be done. Solid evidence about what works, and for whom, as well
as what does not work has raised awareness of how important it is to build all aspects of child
and youth mental health on the solid foundation of evidence (including cost effectiveness).
Increasing awareness of the influence of social determinants, genetics, brain development and
socio-cultural realities on risk and resiliency are reshaping prior conceptions of mental health
and mental well-being and traditional models of mental health services. Taken together, these
new ways of approaching mental health are encouraging us to rethink many aspects of child and
youth mental health, including the role of primary health care, educational institutions and non-
government organizations in the promotion of mental health and well-being and the delivery of
mental health care.
Purpose of Evergreen
Evergreen is meant to be a resource for those involved in, impacted by and responsible for, child
and youth mental health policy, plans, programs and services. Evergreen presents a set of values,
upon which child and youth mental health initiatives should be founded. These values should
inform and direct all child and youth mental health policies, plans, programs and services across
Canada.
Evergreen also provides a number of strategic directions. This component of the framework
should be used to guide the creation, development, implementation and review of mental health
policies, plans, programs and services for young people, parents and families residing in Canada.
These strategic directions should be found in all mental health policies and plans across Canada,
but they may need to be implemented over time and modified according to local conditions.
Within each strategic direction, each jurisdiction will select and apply specific programs,
services and activities. These should be guided by Evergreen’s values. Existing programs,
services and activities should be reviewed to ensure they are consistent with Evergreen’s values.
Evergreen is also meant to be a resource that can be used by young people, parents, caregivers,
service providers, professionals and others to examine or assess what child and youth mental
health strategies are available and to help determine if those programs and interventions that are

Evergreen Framework
- 12 -
available are consistent with Evergreen’s values. This provides a democratic, transparent and
accountable approach to addressing the mental health needs of children and youth in Canada.
Policy makers and planners will now have the values and strategic directions that are important
to and expected by people living in Canada and can thus feel confident in their application of
Evergreen. In turn, people living in Canada can keep account of how policy makers are doing
and can use Evergreen as an advocacy tool and as a resource to direct constructive engagement
with policy makers and providers.
Evergreen is not prescriptive. Rather, it provides an opportunity for policy makers, planners and
providers to select among different options depending on local conditions, local needs and fiscal
realities. Ideally, every jurisdiction in Canada will develop and apply each of the strategic
directions in Evergreen. However, it is unrealistic to think that all of strategic directions will be
immediately applied everywhere. Those deemed most likely to be useful in specific locations or
circumstances should be applied first. It is recommended that a number of strategic directions
from each of the categories of promotion, prevention, intervention, and research/evaluation be
included in every child and youth mental health policy and plan. Regardless of the strategic
directions selected, it is expected that Evergreen’s values are used to inform all aspects of child
and youth mental health policy, plans, programs and services.
Possible Users of Evergreen:
Provincial or Territorial Governments
Federal Government
Regional or District Health Authorities
Institutions
Mental health policy writers, planners and program developers
Service providers
Advocates and advocacy groups
Professional organizations
Non-governmental organizations
Academics
Young people, parents, families, communities, and the public at large
International governments, organizations and associations

Evergreen Framework
- 13 -
Possible Uses for Evergreen (examples):
Guide the development or redesign of child and youth health/mental health policies,
plans, programs or services
Educate professionals, providers and those working with, or on behalf of young
people regarding mental health
Challenge the stigma related to mental health that exists within institutions,
organizations and the public at large
Inform advocacy initiatives targeting the development or redesign of policies,
programs, services and care practices related to, or impacting the mental health of
young people
Inform the development of youth-to-youth, or parent-to-parent initiatives pertaining
to mental health, mental disorders or mental illness occurring within the community
Inform and educate members of the general public regarding infant, child and youth
mental health in Canada
Encourage innovation in child and youth mental health promotion and mental health
care in primary care, schools and youth organizations
Challenge existing silo structures that have traditionally directed services pertaining
to child and youth mental health
Enhance the research enterprise for child and youth mental health
Improve the funding envelope for child and youth mental health from governments,
health care providers and other youth service providers
Evergreen’s Process
In 2008, the CYAC of the MHCC identified the creation of a child and youth mental health
framework as a priority, resulting in the launch of the Evergreen Project. Evergreen was
designed to enable broad national input combined with expertise (professional and lived
experience) in child and youth health to be collaboratively and transparently integrated using
online media, wiki-based document preparation and empirically guided thematic analysis. Input
to Evergreen was broadly invited as well as targeted to include those who may usually not
participate in policy discussions. Input was received as individual contributions rather than
organizational representation. Two distinct face-to-face consultations at national conferences
supplemented this approach.
Information garnered through the public consultation process was made available to three of
Evergreen’s committees: the Drafting Committee, the National Advisory Committee, and the
International Advisory Committee. A Youth Advisory Committee prepared and implemented a
youth engagement strategy that included online networking and the use of social media (i.e.,
Facebook). This information was also made available to the three Evergreen committees.
Advisory Committee inputs were used by the Drafting Committee to inform their collaborative
writing of the document. The computer program, Socialtext, provided the online wiki-technology
for Drafting Committee members to co-write components of Evergreen, and provided the
communication technology to allow all committee members to dialogue and share ideas in a
transparent manner. Repeat public consultation was sought regarding the appropriateness of
Evergreen’s values. Public and committee input was supported through an on-line library of
Evergreen Framework
- 14 -
relevant articles and child and youth mental health policies created specifically to support
Evergreen. An independent review of recent international and Canadian provincial/territorial
child and youth mental health strategies was prepared to help inform the strategic directions
portion of Evergreen. A thematic analysis, using the qualitative research software NVivo, was
conducted on information received through public consultation processes to help guide document
development. Detailed descriptions of Evergreen’s process and the composition of each of the
Committees are provided in Appendix A and Appendix B.
In accordance with privacy conditions outlined in Evergreen’s public consultation process, all
identifying information contained within public consultation materials, such as email addresses,
were removed prior to being made available to Evergreen’s Drafting Committee and Advisory
Committees.
Evergreen Framework
- 15 -
Values All institutions, organizations, legislation and governance are based on values. Sometimes these
values are manifest (i.e., open and clearly stated) and sometimes they are latent (i.e., unstated but
implied or even hidden). In the interests of transparency and the establishment of a common
national foundation for child and youth mental health, it was decided that Evergreen’s values
would be clearly stated. Evergreen’s national consultation process arrived at six values. Public
feedback regarding these values showed over 90 percent of consultation participants in favour.
These values are:
1. Human Rights
We believe that upholding human rights is key to improving the lives of young people.
Evergreen does so by endorsing the following human rights documents that have been accepted
by the Government of Canada:
United Nations Convention on the Rights of the Child (1989)
United Nations Convention on the Rights of Persons with Disabilities (2006)
United Nations Principles for the Protection of Persons with Mental Illness and for the
Improvement of Mental Health Care (1991)
United Nations A World Fit for Children (2002) and the Canadian response, A Canada
Fit for Children (2004)
Canadian Charter of Rights and Freedoms (1982)
Canadian Human Rights Act (1985)
Jordan’s Principle (2007)
2. Dignity, Respect, and Diversity
Young people and their families will receive equal access to opportunities, supports, programs,
services and care practices that match their diverse needs associated with age, gender, sexual
orientation, health status or ability, religion, legal status, social or economic status, geographic
location, language, culture, ethnicity, First Nations, Inuit or Métis identity, or other similar
personal, family or community characteristics.
3. Best Available Evidence
The Evergreen Framework promotes the use of interventions, programs, services and care
practices that are scientifically proven to be the most effective option and that take into account
cost-effectiveness. Knowing about the unique experiences, characteristics and needs of the
individual, family and community are also important in order to determine how well-suited
programs, services and care practices are to the specific young person, their family and their
particular community. Innovation is promoted by supporting research for programs, services and
care practices that are not yet proven effective but show promise and/or those believed to be
helpful in meeting outcomes important to young people, their families and their communities.
Options are increased for young people, families and communities through an ongoing
commitment to develop and implement best evidence-based programs, services and care
practices.

Evergreen Framework
- 16 -
4. Choice, Opportunity and Responsibility
Throughout their development, young people influence, and are influenced by, their families,
communities and environments. These lived experiences all play a role in a young person’s
health and development. Access to sufficient support, resources and opportunities may help to
address the social determinants of mental health, such as poverty, and may play a role in
preventing negative outcomes for young people, their families and communities. The Evergreen
Framework promotes a balanced approach between a child/youth-centered and a family-centered
approach to mental health that respects and supports the rights of the young person, as well as the
essential care-giving role that families play in the lives of young people. When young people and
families are provided with access to sufficient support, resources, education and opportunities,
they are empowered to be actively and meaningfully involved in decisions that affect their health
and development. Early in their development, youth rely on their families as their primary source
of support, protection and decision making. As young people mature into adolescents and young
adults, families will be empowered to function as supports and resources for the young person’s
decision making, taking a more or less active role based on the needs, circumstances and abilities
of the young person. Together, all participants need to have the opportunity to make informed
choices and to be responsible for the choices and actions that they take.
5. Collaboration, Continuity and Community
The mental health of young people can be positively affected by many parts of their lives
including their experiences with friends, family, caregivers as well as experiences in their
community, school or workplace. A benefit of the Evergreen Framework is to have young people
and all those who have a significant role in the lives of young people work together as a support
network to help every young person reach her or his potential. The complex needs of young
people are addressed through agencies, organizations, institutions and Ministries/Departments
working together with each other and alongside young people, their families and their
communities. The delivery of programs, services and care practices will be driven by, and
responsive to, the needs of young people, their families and their communities.
6. Access to Information, Programs and Services
The Evergreen Framework promotes the creation of methods and technologies to collect, store,
share and link together information relevant to the mental health of young people living in
Canada. These methods allow the public to easily receive and share information with
governments and organizations responsible for health and mental health care. These methods
must ensure that information is timely, accurate, unbiased and respectful of personal privacy.
Information must be available in all official languages, responsive to the information needs of
persons with different abilities and presented in a manner that is meaningful to the general
public. The Evergreen Framework also promotes access to mental health programs, services and
care practices for young people and families that is timely and provided in a manner consistent
with all of Evergreen’s values.

Evergreen Framework
- 17 -
Strategic Directions
Introduction
Young people, parents, family members, health care professionals, government officials,
educators, social service and justice professionals, advocates and other community members,
along with Evergreen’s advisory committee members shared strategic directions that they
perceived to be consistent with Evergreen’s values and essential to a child and youth framework
for Canada. Added to these were additional strategic directions gleaned from leading child and
youth mental health policy documents from across Canada and around the world. Each of these
strategic directions is consistent with one or more of Evergreen’s values. They were placed into
four conceptually separate but functionally overlapping categories including, promotion,
prevention, intervention and care, research and evaluation.
The first three categories are part of a continuum and while they are presented here as separate
categories, it is understood that they should be applied in a seamless manner rather than as stand
alone silos. The forth category, research and evaluation, is a component of each of the first three
categories as well as a unique focus of attention in its own right.
These strategic directions are the framework that specific programs, services and activities can
be operationalized within and as such should be used by those involved in, impacted by and
responsible for, child and youth mental health policy, plans, programs and services including
policy makers, program developers, funders, advocates, health and education providers, service
users, young people, parents/caregivers and others involved in the development of child and
youth mental health policies, plans, programs and services. Each strategic direction must be
implemented in a manner that upholds Evergreen’s values. The list of strategic directions is not
exhaustive. There may be some strategic directions not identified in Evergreen that those
responsible for child and youth mental health may wish to implement. In such cases, the selected
strategic direction should be consistent with Evergreen’s values. The broad and intentional
consultation process that resulted in the compilation of Evergreen’s strategic directions suggests
to those responsible for child and youth mental health that they should implement as many as are
feasible from each of the categories provided. Evergreen’s values acknowledge that these
strategic directions may be developed and applied somewhat differently in different situations,
depending on numerous local, financial and other factors.
Young people, parents/caregivers, advocates, service providers, service users, community
members and others can use Evergreen’s strategic directions to provide input to, or inform their
dialogue with, responsible decision makers regarding the nature of current programs, services
and activities and the prospects of future programs, services and activities.
Although many consultation participants suggested unique programs, services or activities in
support of a specific strategic direction, the Evergreen Framework provides only the broader
strategic direction. The reason for this is that for some strategic directions there may be more
than one validated and cost-effective unique program, service or activity available and for others
there may as yet be none available. It is not within the mandate of Evergreen to endorse any
unique program, service or activity but rather to provide the recognition of the strategic direction

Evergreen Framework
- 18 -
for which a unique program, service or activity can be considered – using Evergreen’s values to
help decide which will be chosen. Finally, no attempt has been made to create a hierarchy, or
prioritize the strategic directions – ideally, what should be implemented, when, and in what
manner is a decision to be made collaboratively between those involved in, impacted by and
responsible for, child and youth mental health policy, plans, programs and services.
Evergreen Framework
- 19 -
Promotion
“More children and adolescents need to learn about how mental disorders work, so
that they know…I am a real human, with feelings…We desire life. To get married.
Have children. Working a job we love doing. The better educated the kids of today
are, the less likely they are to be prejudicial.”
-A young person living with a mental illness
Promotion of mental health and addressing social determinants of health are increasingly
considered to be essential components in improving the well-being and mental health of
individuals and populations alike. Input into Evergreen reflected the high importance that
strategic directions for promotion play amongst people living in Canada. As one young person
with lived mental health experience stated, “Promotion & health literacy are especially
important due to the non-obvious nature of many mental health disorders.”
One of the most commonly recurring themes arising from Evergreen’s consultation was the need
to address stigma and increase mental health literacy. Social, professional and self-stigma were
all identified as important targets for mental health promotion.
“Efforts should be made to decrease stigma so that when mental health issues are
identified, children, youth and their families do not feel ashamed or discouraged to
seek support.”
- A young person
Consultation participants emphasized that addressing stigma will require active partnerships
amongst governments, non-governmental organizations, media, institutions (including schools)
and others. Young people and their families were considered to be front and centre in these
activities, not just as participants in promotional campaigns, but also as active partners in their
development and distribution. Consultation participants noted that promotion activities often
could not take a one-size-fits-all approach and may need to be designed to meet the needs of
different audiences. Furthermore, they pointed out that relying on traditional methods of reaching
people may not be most effective in today’s multi-media and digitally connected society. Young
people, parents and professionals noted the need for promotional strategies to keep pace with the
ever changing landscape of communication technologies. To effectively engage young people
with the message presented, promotional efforts need to embrace youth-friendly mediums.
Regardless of the medium, input from the consultation participants indicated a strong need for
information and education regarding positive mental health, mental disorders and mental illness
for infants, children and youth. A young person highlighted this sentiment by stating, “I think
the public does not believe kids when they tell them something is wrong… like we are just
making it up or lying.” This feeling was echoed by a parent of a young person living with a
mental illness who reported that “[s]ociety still does not want to believe that children have
mental health disorders.”
Overwhelmingly, the feedback regarding anti-stigma initiatives, mental health literacy and
mental health promotion activities focused on the use of school-based and youth organization-
based activities, and more specifically on programming embedded within the school curriculum.
The stigma associated with mental health problems and mental disorders was noted as being
particularly powerful in the school environment where jokes, teasing and bullying commonly

Evergreen Framework
- 20 -
occur. One young person helped identify a root of this problem in stating, “kids lack of
information about mental health… which leads to more stigma.” Stigma was identified as
strongly contributing to a culture of silence and shame in the school regarding mental health.
One youth with lived experience described the lack of education regarding mental health as,
“forcing me [him] to go through everything alone”, while another young person indicated
“only meeting one other person with my illness” not because others didn’t experience mental
health problems but “because no one feels comfortable discussing their illness.”
Young people, parents, health professionals, advocates, educators, government officials, social
service providers and others expressed the opinion that mental health programming should be an
integral part of what children and youth are exposed to in school. Educators, in particular,
identified that with the proper information, training and supports, they may be the best positioned
to challenge stigma, enhance mental health literacy and raise awareness of child and youth
mental health. Various strategies for addressing these issues, including establishing school
environments that may enable development of mental well-being were frequently suggested.
Regardless of the method of delivery, education for young people, parents, professionals and
community members regarding child and youth mental health was endorsed as key to promoting
mental health. Another frequently endorsed theme was that of enhancing the capacity of health
care providers, particularly those in primary care, to better address the mental health needs of
young people and their families. Young people often described a lack of knowledge by
physicians and other health professionals as contributing to poor service. For example, a young
person living with a mental illness described being “brushed off by professionals who don‟t
take your feelings seriously”. This feeling resonated with the friend of a young person living
with a mental illness who expressed exasperation at the perceived lack of understanding of
mental disorders by healthcare providers.
“So many kids have real issues of depression, anxiety, bipolar…
they need real help...its not growing blues or being „uncool and unhappy‟
…they deserve the treatment and the help.”
- A friend of a young person living with a mental illness
Another common theme was that of parental mental health literacy and acceptance of a mental
disorder in their child. One young person described herself as “living in secrecy” because her
family “doesn‟t understand about mental health and don‟t want to tell people” due to the
shame and the stigma. The value of young people accessing information and/or education
regarding mental health and mental illness was commonly invoked. The self-reported confusion
of one youth highlights the importance of validated knowledge regarding mental health:
“I had no concept of what mental illness was…I became ill when I was
16 years old. If I had known that I had a treatable and common problem
as opposed to being a bad person, things might have turned out differently.”
- A young person living with a mental illness
The importance of mental health promotion and literacy were punctuated by the words of one
young woman who identified the power associated with knowledge, stating that, “youth have a
right to know what is happening to them and those around them!”
Evergreen Framework
- 21 -
Identified Strategic Directions for Promotion
1. Develop and institute mental health awareness, anti-stigma and mental health literacy
campaigns for health providers, educators, parents/caregivers and the public that are
of proven effectiveness and that reflect and recognize the unique needs of the
audience to which they are directed
2. Develop and implement pro-social mental health promotion programs of
demonstrated effectiveness that reflect and recognize the unique needs of the
audience to which they are directed
3. Use a key stakeholder model (which includes representation and active participation
from young people, parents/caregivers and unique communities) in the development
and delivery of mental health promotion activities
4. Create valid sources of information related to child and youth mental health/mental
disorders. Widely distribute and promote such resources ensuring these materials are
free and accessible to the public
5. Establish mental health promotion activities that utilize online, digital and other
communication activities that appeal to and are used by young people and
parents/caregivers
6. Create, empower and support youth-led mental health promotion activities in multiple
contexts or venues (e.g., community settings, schools and youth serving
organizations)
7. Create a single-point-of-contact information service, mandated to provide information
on mental health activities, including how to access mental health care for each
community. Widely promote the availability of such resources
8. Embed mental health information into other health promotion activities and health
promotion campaigns
9. Enhance the public and professional reputation of mental health services and mental
health professionals
10. Encourage training in mental health as an integral part of all health and education-
related professional degree/diploma/certificate programs (e.g., medicine, social work,
nursing, child and youth worker, early childhood education, and teaching
certification)
11. Consider the creation and support of new mental health human resource designations
and professional regulatory bodies specializing in mental health (e.g., registered
mental health professional)
12. Encourage the provision of standardized, high quality and effective continuing
professional development programs in child and youth mental health for professionals
involved with young people and families (i.e., educators, child welfare professionals,
justice system professionals, daycare workers)
13. Expect and stipulate that all health providers are knowledgeable about child and
youth mental health, consistent with their role in the health care system
14. Educate teachers, students and parents/caregivers about mental health and mental
disorders through specific school mental health curriculum and community programs
15. Embed mental health promotion (including pro-social development programs) into all
school health promotion activities, requiring that mental health is given the same
degree of importance as ―physical health‖

Evergreen Framework
- 22 -
16. Enable schools to create mentally-healthy environments, including effective pro-
social behaviour programming, teacher education, parent/caregiver outreach, school-
based mental health supports and training for school administrators
17. Facilitate close collaboration and organizational linkages between schools,
parents/caregivers and health providers to enhance the exchange of knowledge and
information and to encourage the development of collaborative approaches to
promotion activities pertaining to child and youth mental health
18. Create and make available for national use, a compilation of child and youth mental
health programs of demonstrated effectiveness and cost-effectiveness
19. Establish appropriate regulatory frameworks that will provide national approval (or
national license) for child and youth mental health promotion programs and activities
based on effectiveness, cost effectiveness and safety
20. Create long-term sustainable funding to support child and youth mental health
promotion
Evergreen Framework
- 23 -
Prevention
“We have amazing workers and organization that are overtaxed…if we did
more prevention…maybe we could turn the curve on the continued rising
numbers of people reporting low levels of mental health.”
-Mental Health Professional
Prevention of mental disorders, where possible, and enhancing optimal development through
strategies designed to mitigate risk factors and building resiliency in young people, families and
communities, was viewed as consistent with a proactive approach to mental health. Engaging
secondary prevention measures to diminish the negative outcomes associated with mental health
problems or mental disorders was also recognized as essential to improving child and youth
mental health. Although, multiple ways exist to operationalize prevention, the consultation
revealed that the term prevention can carry both positive and negative connotations. Many
respondents viewed the term and concept in a positive light, perceiving prevention as an
investment in future generations and even as Canada’s preferred approach to mental health.
However, others, notably parents and young people with lived mental health experience,
suggested that when improperly applied, the concept of prevention implies a choice to be ill. One
parent stated that she “feels put out” by the implication “that there was something that I [she]
could have been done…and that‟s why my [her] child has a mental illness.”
There was also the realization that given our current state of knowledge that not all mental
disorders can be prevented (primary prevention) and that universal application of primary
prevention interventions in the absence of substantive evidence can raise unrealistic and even
harmful expectations. Youth with lived mental health experience attested to this by saying:
"Nothing could have prevented [my] bipolar disorder, as [I] inherited it
from [my] mother.”
- A young person living with a mental illness
Many youth described their frustration of how the facts surrounding genetic inheritance and the
biological underpinnings for mental illnesses are frequently discounted by the uninformed in
society, which can lead them to feel blamed by society for their illness, as well as face judgment
that they or their family members were somehow neglectful or negligent in not doing enough to
prevent their illness. Many respondents noted that the concept of prevention needs to be clarified
and that all aspects of prevention should be considered in the development of strategies. There
was strong endorsement for the use of secondary prevention initiatives aimed at mitigating
negative outcomes associated with mental disorders for young people and their families and for
the application of primary prevention strategies of proven efficacy and cost effectiveness.
Generally, the respondents to Evergreen’s consultation addressed the whole gamut of prevention
approaches, from universal population-based models to targeted interventions for specific sub-
groups or individuals. Throughout the consultation, the messages pertaining to prevention
emphasized the need to apply solid evidence of effectiveness when selecting prevention
initiatives, and the importance of tailoring prevention initiatives to the needs and unique
characteristics of populations, groups and individuals.

Evergreen Framework
- 24 -
A consistent theme emerging from the consultation was that of the need for accessible and
accurate information about mental health/mental disorders and mental health programs and
services. Many respondents commented that clear lines between promotion and prevention could
not always be drawn and suggested that specific strategies could be equally well placed in one or
another of these categories. The close association between the two was noted by one young
person who stated, “What is stopping the prevention of mental health in youth is
education…most people do not even realize they have a mental health problem/illness.”
Information targeting groups at-risk for mental health problems was viewed as particularly vital.
One young person of First Nations heritage noted with frustration that, “There isn‟t enough
emphasis, focus or relevant information/materials on health issues amongst Aboriginal
youth…many youth don‟t even know what mental health (good or bad) is, yet they have the
highest rates of suicide in the country.”
The need for early detection and intervention for mental disorders was noted to be dependent on
better information regarding mental health and mental illness (i.e., mental health literacy).
Training and education for parents and professionals working closely with young people (e.g.,
educators and youth organizations) was viewed as a priority. As voiced by a government official:
“The more aware parents, educators, and family physicians are about warning signs and
symptoms, the sooner mental health issues can be addressed.” Early detection and screening
was thought to be particularly beneficial for individuals who are at heightened risk for mental
disorders due to biological or social risk factors, such as genetics, trauma or poverty. Child and
youth mental health screening and early detection initiatives were noted by consultation
participants to include universal screening within the school system, or linking mental health
screening to prenatal visits or during well-baby/well-child examinations, and during child
immunization programs with family physicians or paediatricians.
The complex interplay between social determinants of health and their subsequent impact on
mental health and mental disorders were described by many respondents as a prime target for
prevention efforts. Centred out were factors such as poverty, family violence, abuse, bullying
homophobia, racism, maternal health (e.g., nutrition and prenatal care), and community health,
(i.e., the lingering trauma experienced by First Nations peoples associated with residential
schooling). One young person noted that addressing such factors should be a “first step” in any
approach to prevention. Rather than viewing these social risk factors at an individual level, many
respondents advocated for addressing of these risks at the population level through demonstrated
effective programs made widely available through accredited providers.
Consultation participants frequently identified primary, secondary and post-secondary schools as
key locations to implement prevention programs. As was the case with health promotion, the
school environment was viewed by young people, parents, mental health professionals, educators
and others as the ideal forum to implement a variety of prevention programs. This included
various strategies ranging from effective models of delivering mental health care in the school
setting to mental health literacy for teachers. Consultation participants also raised substantial
concerns about inadequate funding for prevention activities and identified the potential cost-
benefit impact of effective prevention initiatives across various domains: “For every $1 spent on
prevention [there is a] $8 dollar costs savings.” One government official issued a challenge by

Evergreen Framework
- 25 -
stating that as a country “we invest relatively small amounts into the mental health of children
and youth in comparison to many other countries in the world. We need to invest more and we
need to invest more carefully.”
In sum, there was a strong appreciation of the need to cast increasing focus on and funding into
the application of various effective and cost effective mental health prevention initiatives
tempered with the realization that not all mental disorders can be prevented given our current
state of knowledge. Consultation participants advocated for a mental health system that is more
balanced, one that provides appropriate preventive mental health applications while concurrently
strengthening mental health care and secondary prevention for those with mental disorders. It
was recognized that this re-balancing will require significant refocusing of current models of
mental health service, as well as increased funding to support this realignment. This challenge
was likened by a member of Evergreen’s National Advisory Committee to a “Gordian Knot”, an
intractable problem solved with a bold stroke, or more likely in this case, a series of bold strokes.

Evergreen Framework
- 26 -
Identified Strategic Directions for Prevention
1. Establish holistic maternal health care as a beginning point for mental health
prevention initiatives and provide education and training about maternal/child
mental health to all providers working in pre and post-natal care
2. Create and deliver prenatal educational programming and provide
parent/caregiver education that integrates infant, child and youth mental health
with physical health information
3. Provide well-established, proven effective and cost-effective prevention programs
designed to improve outcomes in at-risk populations. Locate these programs in
settings where young people and parents/caregivers can be most easily reached
(e.g., schools, community organizations)
4. Facilitate the provision of educational programs in infant, child and youth mental
health for all primary health care providers (e.g., doctors, nurses), social service
workers (e.g., social workers, child and youth workers, recreation staff) and
educators (teachers, early-childhood educators), and ensure they understand how
to identify mental health problems and provide appropriate resources, supports
and interventions
5. Include child and youth mental health as a key area for training for all child and
youth care providers (e.g., foster parents and justice workers)
6. Establish procedures through which all adult mental health services identify and
facilitate mental health evaluation of the children of patients/clients/service users
7. Enhance the development and delivery of school-based mental health services
either through directed onsite programming or collaboration with primary care
providers (i.e., family physicians, paediatricians) and specialty health care
providers (i.e., child psychiatrists, mental health therapists, family therapists)
8. Provide effective programs addressing social determinants of health for those
populations identified at risk (e.g., poverty) so that child development outcomes
can be improved
9. Make available and promote culturally specific activities to help young people,
parents/caregivers, families and communities to reconnect with or maintain a
connection with cultural traditions. Such activities may be especially important
for Aboriginal youth or young people new to Canada including immigrants and
refugees
10. Provide easily accessible, appropriately subsidized, high quality and regulated
(licensed) child care services to all who require them
11. Ensure that legislative, regulatory or policy barriers do not prevent youth from
obtaining the confidential health or social services that they may need
12. Encourage the availability of mentally healthy workplaces that support the needs
of parents/caregivers and families
13. Create and deliver age appropriate programs that empower and enable young
people to be socially active and integrated participants in civil society
14. Provide an easily available range of urgent access services to meet immediate
crisis needs of children and youth (e.g., 24/7 phone-based or web-based
counselling services, safe-houses and short-term crisis locations in the
community)
Evergreen Framework
- 27 -
15. Structure mental health services to provide a full range of care options, including
family respite care and prevention focused short-term residential interventions
16. Structure mental health and substance-abuse services for young people to be fully
integrated so that interventions in one of these domains can prevent the
development of problems in the other
17. Enhance linkages between specialty child and youth mental health services,
primary care, antenatal and obstetric services, paediatric health care and early
childhood services, child protection and justice agencies
18. Provide targeted initiatives for transitional-age young people (i.e., 16 to 25 years
of age) including funded community-based, social, vocational and educational
programs designed to mitigate the effects of mental disorders and enhance
secondary prevention
19. Establish long-term sustainable funding to support child and youth mental health
prevention initiatives
Evergreen Framework
- 28 -
Intervention & Ongoing Care
“I know I want better mental health care for me and my family. There can be
improvement on all levels of care.”
- A family member of a young person
living with a mental illness
Challenges faced by young people and families in accessing mental health services and the lack
of easily available, effective and respectful programs were two themes frequently identified.
While there was recognition that current services did demonstrate strengths, there was
overwhelming interest in improving all aspects of mental health care for young people and
families. Early effective intervention was identified as essential for addressing current mental
health problems, improving long-term outcomes, preventing disability and the onset of other
mental and physical disorders. Promotion, prevention and care services were not viewed as
separate components of a health system. Instead, consultation participants consistently reported
these areas of mental health service overlap in many ways, and should be seamlessly integrated
into an optimized model of mental health service. A parent addressed this need for integration:
“If parents don‟t know what mental health problems are, if parents don‟t know
where to go to access services, or worse yet, that service doesn‟t exist, and if
parents are „ashamed”, or don‟t acknowledge the child‟s mental health problems
then treatment and help can‟t occur.”
- A parent of a child with lived mental health experience
Another recurring theme was the importance of cross-sectoral collaboration to meet the needs of
young people and their families. These needs should drive the structure and function of services.
Consultation participants noted that the mental health system appears to be one of the few
service industries in Canada where the service user must cater to the wants of the system, rather
than the system catering to the needs of the service user. Many young people, parents and
professionals expressed concerns that cross-sectoral collaboration in support of young people
and families was not as seamless as it should be. As one mental health professional noted there is
a need for “better coordination and working relationship with the education, health care
system and community services.”
An indication of this was the focus on the need for effective mental health care to be delivered in
primary care particularly through family physicians. Many recommendations pertaining to
enhancing the role of family physicians in the prevention and treatment of common mental
disorders in young people were made. Building mental health capacity in primary care was noted
as necessary to decrease wait-lists for specialty mental health services, as well as contributing to
the provision of more effective and efficient mental health care in the community through
integration with usual health services. This was considered by many as having the additional
possible benefit of decreasing stigma about mental disorders. Caution was expressed however,
that family physicians and other providers would need training and additional supports to play an
increased role in the primary mental health care of young people.

Evergreen Framework
- 29 -
The balance between individual and parental responsibility for all aspects of mental health care
also emerged as a key theme. This was particularly pronounced in relation to initiating access to
services, decision making about treatments and other forms of care, and issues of privacy and
confidentiality. Youth frequently stressed the need to be active partners and decision makers in
matters related to their health and mental health. Input from parents highlighted the important
role they play in the lives of their children and emphasized their need to participate actively in all
aspects of mental health care for their children. There was a dynamic tension between these two
perspectives, one which is perhaps best described in this quote from a youth with lived mental
health experience:
“It is important to respect young people as experts on their own feelings
[while also realizing that] young people are not necessarily able to make
the decision to recover.”
- A young person with lived mental health experience
Concerns about system inefficiency and the lack of infrastructure and human resources were
frequently expressed. Contributors identified the cost inefficiency and burden of multiple
assessments for the same problem from different providers and the need for a single, secure, but
easily accessible, health data-base and information system. Many respondents expressed
concerns that funding cutbacks and limited resources create barriers to needed care. For example,
one young person with lived mental health experience noted, “I want to get better, but will I
have to be rich to do it?”
Although the need for a transformed mental health system was overwhelmingly articulated, there
was frequent praise for care that had been received, with adjectives such as “life saver” and
“miraculous” being used by parents and young people to describe their experiences. A frequent
refrain was that there were “some excellent services available through children‟s mental health
centers and hospitals”, but that there was difficulty finding services and accessing them once
they were discovered. Respondents also raised concerns about the quality of services. For
example, the system was described as offering “inadequate care”, with multiple barriers to
access including waiting lists described by young people, parents and professionals as
“horrendous”, “absurdly long”, “tedious”, “stressful”, and “virtually impossible”.
Consultation participants noted the lack of services available to rural or remote communities and
First Nations, Métis, or Inuit peoples and/or communities. A family member of a young person
with a mental illness summarized these concerns poignantly as follows: “The need is GREAT,
the availability of resources, LIMITED.”
Concerns about mental health services being welcoming and supportive were common. For
example, a mental health advocate wondered why mental health services for young people can’t
be “as user friendly and non-threatening as the fitness centre or library?” Several parents also
queried why appointment times could not be after school or after work hours. Young people,
parents and mental health professionals called for services that included online or telephone
counselling, or school-based programming. These concerns also included the physical and milieu
features of mental health services. Numerous young people commented on their negative
experiences with these components of mental health care. A young person described the system’s
lack of sensitivity to youth by saying, “When young people, put in hospital for having a mental

Evergreen Framework
- 30 -
illness, are put with older intimidating people…this can scare them away from seeking future
treatment.”
One of the most commonly raised concerns was that of the problems of accessing youth
friendly/transitional age services – for young people between 16 and 25 years of age. In the
words of one parent, “There are no good services for people between 17 and 25!” This gap
between needs and availability was noted by one youth service recipient who stated, “There are
no intermediate steps between sitting at home alone, or going to the hospital in crisis.” The
need to provide mental health services that are designed to specifically meet the needs of young
people in this age group, often referred to as the transitional age group, was one of the most
consistent themes appearing in the consultation.
Evergreen Framework
- 31 -
Identified Strategic Directions for Intervention and Ongoing Care
1. Provide youth-friendly and family-friendly mental health services that are accessible
(i.e., after school and weekend hours of operation)
2. Enhance the capacity of primary care services to meet child and youth mental health
needs by providing training to primary care physicians to diagnose and treat mental
disorders in children and youth and by providing family physician offices with the
human resource supports needed to provide care
3. Establish a full range of mental health services that meet the specific needs of young
people ages 16 to 25
4. Create community-based rehabilitation services that meet the needs of young people
(e.g., safe home-like atmosphere, vocational and educational assistance, health
directed, alcohol and drug prevention) and appropriately link these to institutional
facilities
5. Create appropriately staffed facilities in communities designed to be ―one stop
shopping‖ that meets the mental health and physical health needs of young people
and families in one location. Widely promote the availability of such resources
6. Enhance the development and delivery of ―first onset‖ programs in the major mental
disorders (e.g., psychosis and mood disorders)
7. Create services addressing the social determinants of mental health for young people
with early onset mental disorders (e.g., supported housing, employment and education
programs)
8. Create and efficiently operate effective cross-sectoral linkages that meet mental
health needs of young people across traditional government
ministries/agencies/departments
9. Support the development and activities of non-governmental organizations
representing parents/caregivers and young people
10. Include parents/caregivers and young people as active representatives in all aspects of
policy, planning, program development and evaluation of child and youth mental
health services
11. Establish and operate liaison/linkage programs between schools, primary health care
providers and mental health services
12. Establish and support school health with personnel trained to provide onsite mental
health interventions in secondary schools
13. Provide onsite mental health supports in junior high schools
14. Create common single-point-of-access patient and family databases using
standardized assessment materials that can be accessed by health providers, with
appropriate consent, to prevent unnecessary assessments
15. Invest in the development and delivery of effective training programs that enhance
the capacity of all primary health care providers to identify, diagnose and treat the
most common child and adolescent mental disorders
16. Support the development of new mental health human resources (e.g., mental health
workers) and the enhancement of mental health capacities within usual health care
providers (e.g., nurses and occupational therapists)

Evergreen Framework
- 32 -
17. Enhance access to specialty mental health services in rural areas through the use of
new communication technologies (e.g., telehealth psychiatric consultations,
telephone-based or web-based counselling)
18. Utilize innovative technologies (e.g., iPhone applications and web-based counselling)
to establish effective mental health services, including self-referral, counseling, and
educational/literacy programming, for young people and parents/caregivers
19. Integrate child and youth mental health into all existing health care services
20. Establish mechanisms that ensure that all interventions used are evidence-based and
preferentially provide programs and interventions where effectiveness and cost-
effectiveness has been proven for Canadian settings
21. Create mechanisms by which young people and parents/caregivers can obtain
information needed to help them determine which interventions, programs and
services are based on best scientific evidence
22. Establish joint service delivery/academic research teams that can provide systematic
reviews of best evidence in order to guide policy development, plans and programs
23. Provide opportunities and resources to young people and parents/caregivers to be
effective participants in their own mental health and recovery from mental disorders
24. Create sufficient numbers of long-term care facilities specializing in acute care with
low staff-to-young person ratios for those young people who require such services
25. Establish standards for staff training to ensure adequate knowledge and skill levels
related to child and youth mental health for professionals working in such areas as
juvenile justice facilities, child protection/children’s services agencies, first responder
organizations, group homes/residential treatment facilities, etc.
26. Establish and deliver appropriate cultural diversity training programs for all child and
youth mental health providers
27. Develop, monitor and enforce quality standards for child and youth mental health
care across all jurisdictions and provider organizations
28. Establish a national regulatory agency for the review and licensing of non-
pharmaceutical treatments based on the evidence requirements currently in place for
pharmaceutical treatments
29. Decrease duplication in services and streamline/co-ordinate service provider activities
30. Provide sustainable and sufficient funding to adequately meet the mental health care
needs of children and youth

Evergreen Framework
- 33 -
Research & Evaluation
“A resourced plan to shift toward evidence-based practice
has been a dream come true.”
- A Mental Health Professional
The Evergreen consultation produced numerous themes pertaining to research and evaluation in
child and youth mental health. Overall, it was noted that relative to other areas of child health,
research into child and youth mental health has not received the same attention, in development
or funding. It was recognized that all aspects of child and adolescent mental health had to be
built upon the best available research, as was noted by a mental health program director:
“Research and program evaluation is absolutely integral to the provision of well
grounded clinical care across the full continuum of cymh [child and youth mental
health] services ranging from health promotion and illness prevention to the expensive
intensive deep end services. We must know that what we do works and that it does no
harm.”
- Member of Evergreen’s Drafting Committee
Consultation participants consistently noted that all interventions should apply validated research
methods to direct and inform practice. One health professional stated candidly, “If you don‟t
measure it, you can‟t manage it.” Others noted that critical research inspired thinking must be a
core component of everything that is done and must be the foundation for ongoing learning. A
researcher noted that, ―The ultimate aim is for evaluation to become a normal part of planning
and managing programs, resulting in ongoing improvement and learning.‖
It is clear that people want programs and interventions to be effective and cost-effective. They do
not want to be exposed to interventions that do not work or might be more harmful than helpful,
and they expect that when it is offered, an intervention has undergone the appropriate evaluations
and has demonstrated its efficacy, safety and value. They expect governments to establish and
enforce research-based standards of care and they expect child and youth mental health research
to be a national priority for funding.

Evergreen Framework
- 34 -
Identified Strategic Directions for Research and Evaluation
1. Support research in the areas of health promotion, prevention and intervention so that
the effectiveness and cost effectiveness of health promotion, prevention and
intervention activities are clearly established prior to programs being launched
2. Support child and youth mental health systems research and apply its findings to
guide development and application of mental health care
3. Create a national repository of mental health promotion, prevention and intervention
activities and/or programs that meet an acceptably high standard of evidence for
access by policy makers, planners, service providers, service users, parents/caregivers
and advocates
4. Establish criteria and expectations for the inclusion of cost-effectiveness evaluations
into research when appropriate, so that all scientifically validated interventions
include cost-effectiveness evaluations
5. Demand that appropriate processes have occurred to ensure the effectiveness, safety,
and cost-effectiveness, as well as to ensure the comparator efficacy, safety, and cost-
effectiveness analyses have been conducted for all interventions and ongoing care
programming
6. Create processes that actively include young people, parents/caregivers and advocates
in the identification of national and/or provincial/territorial child and youth mental
health research priorities, as well as in the evaluation of interventions, programs, and
other activities
7. Provide education to young people, parents/caregivers, advocates and others on the
value and purpose of research
8. Create specific programs and incentives to increase the number and quality of
researchers working in child and youth mental health
9. Create research partnerships in each province and territory involving policy makers,
service providers, academics, young people and parents/caregivers in order to
identify, fund, create and deliver research that is relevant and meaningful to all
stakeholders
10. Establish evaluations that are mindful of multiple ways of knowing and apply them
appropriately
11. Create comprehensive and easily accessible national and provincial/territorial
research data-bases that are linked and which will allow for data capture and research
into child and youth development and child and youth mental health
12. Provide directions that stipulate that research is conducted with participants that are
reflective of the national population
13. Promote research into groups of people traditionally excluded or under-represented in
child and youth mental health domains
14. Create professional development and training programs for health providers that
emphasizes research principles and the application of research evidence to the
development and delivery of policy, plans, programs and interventions
15. Establish program funding mechanisms whereby funding is directly tied to
completion of outcome evaluation
16. Create a national child and youth research repository in which validated tools and
measures can be compiled and made easily accessible to researchers at minimal cost
Evergreen Framework
- 35 -
17. Create or support knowledge translation nodes that can apply best evidence to
develop products such as, programs and activities useful for practitioners, policy
makers, young people, parents/caregivers, and others
18. Establish an international child and youth mental health research liaison group that
can facilitate joint international projects and enhance international research
collaborations
19. Create dedicated funding for child and youth mental health research within the
Canadian Institutes of Health Research or other appropriate granting agencies
(including provincial/territorial health research funding bodies)

Evergreen Framework
- 36 -
SUGGESTED READINGS
Canada (2004). A Canada Fit for Children: Canada’s plan of action in response to the May 2002
United Nations Special Session on Children. Ottawa: Canada. Retrieved on February 1, 2010,
from http://www.rhdcc-hrsdc.gc.ca/eng/cs/sp/sdc/socpol/publications/2002-
002483/canadafite.pdf
Kirby, M.J.L. & Keon, W.J. (2006). Out of the shadows at last: Transforming mental health,
mental illness and addiction services in Canada. Ottawa: Standing Senate Committee on
Social Affairs, Science and Technology. Retrieved on December 4, 2009, from
http://parl.gc.ca/39/1/parlbus/commbus/senate/Com-e/SOCI-E/rep-e/pdf/rep02may06high-
e.pdf
Leitch, K.K. (2007). Reaching for the top: A report by the advisor on healthy children and youth.
Ottawa: Health Canada. Retrieved on February 2, 2010, from
http://www.hc-sc.gc.ca/hl-vs/alt_formats/hpb-dgps/pdf/child-enfant/2007-advisor-
conseillere/advisor-conseillere-eng.pdf
RELEVANT ARTICLES AND POLICIES USED IN THE PREPARATION OF EVERGREEN
Many of the following materials used in the preparation of the Evergreen Framework can be
accessed from http://www.teenmentalhealth.org/initiatives/evergreen
Ad Hoc Working Group on Women, Mental Health, Mental Illness and Addictions (2008).
Women, mental health and mental illness and addiction in Canada: An overview. Canadian
Women’s Health Network. Retrieved on January 19, 2009, from
www.cwhn.ca/PDF/womenMentalHealth.pdf
Adelman, H. & Taylor, L. (1999). Policy leadership cadre from mental in schools. Expanding
policy leadership for mental health in schools: Report from the mini-summit. Retrieved on
January 19, 2008, from http://smhp.psych.ucla.edu/pdfdocs/Report/minisum.pdf
Agic, B. & Scheffer, R. (2003). Health promotion programs on mental health/illness and
addiction issues in ethno-racial/cultural communities. Toronto: Centre for Addictions and
Mental Health. Retrieved on January 19, 2009, from
http://www.camh.net/education/ethnocult_healthpromores02.pdf
Alberta Health Services (2004). Advancing the mental health agenda: A provincial mental health
plan for Alberta. Edmonton: Alberta Health Services. Retrieved on January 13, 2008, from
www.amhb.ab.ca/Publications/reports/Documents/MentalHealthPlan.pdf
Alberta Health and Wellness (2006). Positive futures-optimizing mental health for Alberta’s
children & youth. Edmonton: Alberta Health and Wellness. Retrieved on January 13, 2008,
from www.assembly.ab.ca/lao/library/egovdocs/2006/alhw/156586_01.pdf
Alberta Mental Health Board (2005). A call to action: The Alberta suicide prevention strategy.
Edmonton: Alberta Mental Health Board. Retrieved on January 13, 2008, from
http://www.amhb.ab.ca/Initiatives/suicidePrevention/Documents/A%20call%20to%20action.

Evergreen Framework
- 37 -
Alberta Mental Health Board (2006). Aboriginal mental health: A framework for Alberta-
Health Aboriginal people in health communities. Edmonton: Alberta Mental Health Board.
Retrieved on January 13, 2009, from
http://www.amhb.ab.ca/Initiatives/aboriginal/Documents/Aboriginal_%20%20Framework.pd
f
Alberta Mental Health Research Partnership Program (2007). Child and adolescent mental
health research: Alberta research activity and leadership: Environmental scan. Edmonton:
Alberta Health Services. Retrieved on January 13, 2008, from
http://www.mentalhealthresearch.ca/Publications/Documents/CA%20E-Scan09_FINAL.pdf
Alberta Health and Wellness (2008). Children’s mental health plan for Alberta. Edmonton:
Alberta Health and Wellness. Retrieved on January 13, 2008, from
http://www.mentalhealthresearch.ca/Publications/Documents/CA%20E-Scan09_FINAL.pdf
Alianait Inuit-Specific Mental Wellness Task Group (2007). Alianait Inuit mental health action
plan. Retrieved on February 1, 2010, from
http://www.itk.ca/sites/default/files/alainait_action_plan_english.pdf
Ajunnginiq Centre (2007). Substance use/abuse issues among Inuit in Canada. Presentation to
the Standing Committee of the Conference of Parliamentarians of the Arctic Region Ottawa-
October, 19, 2007. Retrieved on April 9, 2009, from
http://www.naho.ca/inuit/e/resources/documents/2007-10-
19ParliamentarianSubstanceAbuse-FINAL-NAHO-AC.pdf
American Academy of Pediatrics Policy Statement, Committee on school health (2004). School-
based mental health services. Pediatrics, 113(6), 1839-1845.
Andreychuk, R. & Fraser, J. (2007). The silenced citizens-effective implementation of Canada’s
international obligations with respect to the rights of children: Final report of the Standing
Senate Committee on Human Rights. Ottawa: Senate Committees Directorate. Retrieved on
December 8, 2008, from http://www.parl.gc.ca/39/1/parlbus/commbus/senate/com-e/huma-
e/rep-e/rep10apr07-e.htm
Assembly of First Nations (2005). First Nations action plan for non-insured health benefits.
Ottawa: Assembly of First Nations. Retrieved on January 13, 2009, from
http://afn.ca/cmslib/general/NIHB%20Action%20Plan_Fe.pdf
Australian Health Promoting Schools Association (2000). A national framework for health
promoting schools (2000-2003): National health promoting schools initiative.
Commonwealth Department of Health and Family Services. Retrieved on January 22, 2009,
from http://newsite.ahpsa.org.au/media/framework.pdf
Aubé, D., Vallée C., Fournier L., Poirier, L.R., Roberge, P., & Lessard, L. (2008). Influences of
Quebec’s ministerial mental health action plan on organizational models in social and health
Service centres: Study of 15 local service networks. National Conference on Collaborative
Mental Health Care, Victoria, Canada. Retrieved on May 9, 2009, from
http://www.qualaxia.org/mental-health-information/publications-results.php?lg=en
Bakermans-Kranenburg, M.J., van IJzendoorn, M.H., Juffer, F. Less is more: Meta-analyses of
sensitivity and attachment interventions in early childhood. Psychological Bulletin, 129(2),
195-215.
Barwick, M.A., Boydell, K.M. & Omrin, C. (2002). A knowledge transfer infrastructure for
children’s mental health in Ontario: Building capacity for research and practice. Toronto,
ON: The Hospital for Sick Children. Retrieved on April 9, 2009, from
http://www.kidsmentalhealth.ca/documents/KT_full_report.pdf

Evergreen Framework
- 38 -
Benoit, C. & Shumka, L. (2009). Gendering the health determinants framework: Why girls’ and
women’s health matters. Vancouver: Women’s Health Research Network. Retrieved on
January 22, 2009, from http://www.whrn.ca/why-girls-and-womens-health-matters-
download.php
Bird, C.M. & Lawson, A. (n.d.). Mental health in middle childhood: Policy report. Calgary:
National Children’s Alliance. Retrieved on January 7, 2009, from
http://www.nationalchildrensalliance.com/nca/pubs/2006/Mental%20Health%20in%20Middl
e%20Childhood%20Policy%20Brief.pdf
Blackstock, C., Bruyere, D., Moreau, E. (2005) Many hands, one dream: Principles for a new
perspective on the health of First Nations, Inuit and Métis children and youth. Summary of
the conference of the same title held in Victoria, B.C., Dec. 3, 2005. Retrieved on December
8, 2008, from http://www.manyhandsonedream.ca/english/manyhands-principles.pdf
Blackstock, C. (2009). General comment No. 11: Indigenous children and their rights under the
convention. Office of the High Commission for Human Rights. Retrieved on December 8,
2008, from http://www2.ohchr.org/english/bodies/crc/docs/GC.11_indigenous_New.pdf
British Columbia Centre of Excellence for Women’s Health. Mainstreaming women’s mental
health: Building a Canadian strategy. Vancouver: BC Centre of Excellence for Women’s
Health. Retrieved on March 10, 2009, from http://www.bccewh.bc.ca/publications-
resources/documents/mainstreamingwomensmentalhealth.pdf
British Columbia Ministry of Children and Family Development (2003). Child and youth mental
health plan for British Columbia. Victoria: British Columbia Ministry of Children and
Family Development. Retrieved on December 8, 2008, from
http://www.mcf.gov.bc.ca/mental_health/pdf/cymh_plan.pdf
British Columbia Ministry of Health, Mental Health and Addictions (2007). Planning guidelines
for…mental health & addiction services for children, youth & adults with developmental
disability. Victoria: British Columbia Ministry of Health, Mental and Addictions. Retrieved
on January 13, 2009, from
http://www.health.gov.bc.ca/library/publications/year/2007/MHA_Developmental_Disability
_Planning_Guidelines.pdf
Brookman-Frazee, L., Baker-Ericzen, M., Stahmer, A., Mandell, D., Haine, R.A., Hough, R.L.
(2009). Involvement of youths with autism spectrum disorders or intellectual disabilities in
multiple public service systems. Journal of Mental Health Research, 2, 201-219.
Bryan, T., Burstein, K., Ergul, C. (2004). The Social-emotional side of learning disabilities: A
science-based presentation of the state of the art. Learning Disability Quarterly, 27(Winter),
45-51.
Burns, B.J., Costello, E.J., Angold, A., Tweed, D., Stangl, D., Farmer, E.M.Z., & Erkanli, A.
(1995). Children’s mental health use across service sectors. Health Affairs, 14(3), 148-159.
Campbell, D.M., Redman, S., Jorm, L., Cooke, M., Zwi, A.B. & Rychetnik, L. (2009).
Increasing the use of evidence in health policy: Practice and views of policy makers and
researchers. Australia and New Zealand Health Policy, 6 (21), doi: 10.1186/1743-8462-6-
21.
Canada (1982). Charter of Rights and Freedoms. Ottawa: Ministry of Heritage, Government of
Canada. Retrieved on January 20, 2009, from
http://www.cejamericas.org/doc/legislacion/constituciones/can-rights-freedoms.pdf

Evergreen Framework
- 39 -
Canada (1985). Canadian Human Rights Act. Ottawa: Ministry of Heritage. Retrieved on
January 20, 2009, from http://www.ilo.org/wcmsp5/groups/public/---ed_protect/---protrav/---
ilo_aids/documents/legaldocument/wcms_127704.pdf
Canada (2004). A Canada Fit for Children: Canada’s plan of action in response to the May 2002
United Nations Special Session on Children. Ottawa: Government of Canada. Retrieved on
January 7, 2009, from www.phac-aspc.gc.ca/dca-dea/publications/ncd-
jna/canada_fit_for_children.pdf
Canada (2005). Aboriginal horizontal framework. Ottawa: Government of Canada. Retrieved on
January 7, 2009, from http://www.tbs-sct.gc.ca/aaps-aapd/pdf/poverview_e.pdf
Canadian Alliance on Mental Illness and Mental Health (2006). Framework for action on mental
illness and mental health. Canadian Alliance on Mental Illness and Mental Health. Retrieved
on January 20, 2009, from
http://www.cmha.ca/data/1/rec_docs/601_CAMIMH%20English%20Lowres.pdf
Canadian Association of Paediatric Health Centres (2006). Reclaiming the mental health of our
children & youth “A national call to action”. CAPHC Annual Meeting Vancouver (October
15-18, 2006). Retrieved on January 20, 2009, from
http://www.caphc.org/documents_annual/2006/concurrent_session_proceedings.pdf
Canadian Collaborative Mental Health Initiative (2006). Working together towards recovery:
Consumers, families, caregivers and providers. Mississauga, ON: Canadian Collaborative
Mental Health Initiative. Retrieved on December 23, 2008, from
http://www.ccmhi.ca/en/products/toolkits/documents/EN_Workingtogethertowardsrecovery.
Canadian Collaborative Mental Health Initiative (2007/2008). CCMHI provincial consultations:
Nova Scotia, Manitoba, Saskatchewan final report. Mississauga, ON: Canadian
Collaborative Mental Health Initiative. Retrieved on December 23, 2008, from
http://www.ccmhi.ca/en/documents/CCMHIPROVINCIALCONSULTATIONSFINAL.pdf
Canadian Collaborative Mental Health Initiative (2006). Pathways to healing: A mental health
guide for First Nations People- A toolkit. Mississauga: Canadian Collaborative Mental
Health Initiative. Retrieved on December 23, 2008, from
http://www.ccmhi.ca/en/products/toolkits/documents/EN_PathwaystoHealing.pdf
Canadian Human Rights Commission (2008). Policy and procedures on the accommodation of
mental illness. Ottawa: Canadian Human Rights Commission. Retrieved on December 25,
2008, from http://www.chrc-ccdp.ca/pdf/policy_mental_illness_en.pdf
Canadian Institute of Child Health (1980). The rights of the child in the health care system.
Ottawa: Canadian Institute of Child Health. Retrieved on March 2, 2009, from
http://www.cich.ca/PDFFiles/RightHospitalizedENG.pdf
Canadian Institute for Health Information (2008). Mental health, delinquency and criminal
activity. Ottawa: Canadian Institute for Health Information. Retrieved on December 22,
2008, from http://secure.cihi.ca/cihiweb/products/mh_crime_full_report_apr11_08_e.pdf
Centre for Addictions and Mental Health. Strategy to build relationships and partnerships with
LGTTTQQI communities. Toronto: CAMH. Retrieved on January 15, 2009, from
http://www.camh.net/About_CAMH/Diversity_Initiatives/final%20LGBTQ%20strategy.pdf
Center on the Developing Child at Harvard University (2007). A science-based framework for
early childhood policy: Using evidence to improve outcomes in learning, behavior, and
health for vulnerable children. Retrieved on May 8, 2009, from
http://developingchild.harvard.edu/files/7612/5020/4152/Policy_Framework.pdf

Evergreen Framework
- 40 -
Chalmers, J., Cayen, L., Snowshoe, S. (2002). “A state of emergency…”: A report on the
delivery of addictions services in the NWT-Final report. Yellowknife: Department of Health
and Social Services and Community Wellness Programs and Services. Retrieved on
December 22, 2008, from
http://www.hlthss.gov.nt.ca/pdf/reports/mental_health_and_addictions/2002/english/a_state_
of_emergency_evaluation_of_addiction_services_in_the_nwt.pdf
Chalmers, J., Cayen, L., Bradbury, C., & Snowshoe, S. (2006). Stay the course…and together we
can secure the foundation that has been built”- An interim report on the mental health and
addictions services in the NWT. Yellowknife: The Department of Health and Social Services.
Retrieved on December 22, 2008, from
http://www.hlthss.gov.nt.ca/pdf/reports/mental_health_and_addictions/2005/english/stay_the
_course/chalmers_full_report_december_2005.pdf
Child and Youth Initiative of the Canadian Medical Association, Canadian Paediatric Society &
The College of Family Physicians of Canada (2007). Child and youth health: Our challenge.
Canada’s child and youth health charter. Canadian Medical Association, Canadian
Paediatric Society & The College of Family Physicians of Canada. Retrieved on April 4,
2009, from http://www.ourchildren.ca/images/charter.pdf
Children’s Mental Health Ontario (n.d.). A summary of discussions regarding Ontario’s policy
framework for child and youth mental health. Toronto: Ministry of Children and Youth
Services. Retrieved on January 13, 2009, from
http://www.kidsmentalhealth.ca/documents/Res_CMHOPolicyFrameworkDiscussions.pdf
Copage, C. & Broom, B. (2008). First Nations & Inuit child-youth mental health & addictions:
building bridges in Atlantic Canada. Retrieved on March 3, 2009, from
http://download.cmha.ab.ca/ns/Barbara%20Broom%20and%20Cheryl%20Copage%20-
%20First%20Nation%20and%20Inuit%20Child-
Youth%20Mental%20Health%20&%20Addictions%20Building%20Bridges%20in%20Atlan
tic%20Canada.ppt
Core Working Group- Public Health Institute of Scotland (2003). Needs assessment report on
child and adolescent mental health: Final report- May 2003. Edinburgh: Scotland National
Health Services. Retrieved on December 18, 2009, from
http://www.headsupscotland.co.uk/documents/SNAP1.pdf
Costello, E.J., Farmer, E.M., Angold, A., Burns, B.J., & Erkanli, A. (1997). Psychiatric disorders
among American Indian and white youth in Appalachia: The Great Smoky Mountains study.
American Journal of Public Health, 87(5), 827-32.
Dababnah, S. & Cooper, J. (2006). Challenges and opportunities in children’s mental health: A
view from families and youth. New York City, NY: National Centre for Children in Poverty,
Columbia University Mailman School of Public Health. Retrieved on January 8, 2009, from
http://www.nccp.org/publications/pdf/download_9.pdf
Danese, A., Moffitt, T.E., Harrington, H., Milne, B.J., Polanczyk, G., Pariante, C.M., Poulton,
R., & Caspi, A. (2009). Adverse childhood experiences and adult risk factors for age-related
disease. Archives of Pediatric Adolescent Medicine, 163(12), 1135-1143.
Dean, R.G. (2001). The Myth of Cross-Cultural Competence. Families in Society, 82(6), 623-
630.

Evergreen Framework
- 41 -
Dunnachie, B. (2007). Evidence-based age-appropriate interventions – A guide for child and
adolescent mental health services (CAMHS). Auckland: The Werry Centre for Child and
Adolescent Mental Health Workforce Development. Retrieved on May 10, 2009, from
http://www.werrycentre.org.nz/site_resources/library/Workforce_Development_Publications/
Evidence_Based_Intervention_Final_Doc.pdf
Durlack, J.A. & Wells, A.M. (1997). Primary Prevention Mental Health Programs for Children
and Adolescents: A Meta-Analytic Review. American Journal of Community Psychology,
25(2), 115-152.
Emerson, E. & Hatton, C. (2007). Mental health of children and adolescents with intellectual
disabilities in Britain. British Journal of Psychiatry, 191, 493-499.
Epstein, D., Jimenez-Rubio, D. Smith, P.C., & Suhrcke, M. (2009). An economic framework for
analyzing the Social Determinants of Health and Health Inequalities. York, UK: University
of York Centre for Health Economics. Retrieved on February 1, 2010 from
http://www.york.ac.uk/inst/che/pdf/rp52.pdf
European Union Health & Consumer Protection Directorate-General (2005). Green paper:
improving the mental health of the population: Towards a strategy on mental health fro the
European Union. Brussels: EU Health & Consumer Protection Directorate-General.
Retrieved on January 22, 2009, from
http://ec.europa.eu/health/ph_determinants/life_style/mental/green_paper/mental_gp_en.pdf
Findlay, S.S. (2004). Knowledge-brokers: Linking researchers and policy makers. Edmonton:
Alberta Heritage Foundation for Medical Research. Retrieved on March 2, 2009, from
http://www.ihe.ca/documents/HTA-FR14.pdf
Fleming, M. & Towey, K., (Eds.) (2002). Educational forum on adolescent health: Youth
bullying. Chicago: American Medical Association. Retrieved on April 4, 2009, from
www.ama-assn.org/ama1/pub/upload/mm/39/youthbullying.pdf
Fournier, L. & Poirier, L.R. (2006). Transformation of mental health primary care in Quebec: A
research program. Paper presented at the 7th
National Conference on Shared Mental Health
Care, Calgary. Retrieved on December 23, 2008, from http://www.qualaxia.org/mental-
health-information/publications-results.php?lg=en
Girls Action Foundation (2008). The need for a gender-sensitive approach to the mental health
of young Canadians. Girls Action Foundation. Retrieved on March 17, 2009, from
http://www.whc.ie/publications/gender_manual.pdf
Glied, S. & Cuellar, A.E. (2003). Trends and issues in child and adolescent mental health, Health
Affairs, 22(5), 39-50.
Government of Newfoundland and Labrador (2005). Working together for mental health: A
provincial policy framework for mental health & addictions services in Newfoundland and
Labrador. St. John’s: Government of Newfoundland and Labrador. Retrieved on January 7,
2009, from
http://www.health.gov.nl.ca/health/publications/pdfiles/Working%20Together%20For%20M
ental%20Health.pdf
Hawaii Child and Adolescent Mental Health Division (2009). “Blue Menu”- Evidence-based
child and adolescent psychosocial interventions. Honolulu: Hawaii Child and Adolescent
Mental Health Division. Retrieved on May 10, 2009, from http://hawaii.gov/health/mental-
health/camhd/library/pdf/ebs/ebs022.pdf

Evergreen Framework
- 42 -
Health Canada (2000). Aboriginal Health Start Initiative: Children making a community whole:
A review of Aboriginal head start in urban and northern communities. Ottawa: Health
Canada. Retrieved on January 7, 2009, from http://www.phac-aspc.gc.ca/dca-
dea/publications/pdf/cmacw_final_e.pdf
Health Canada (2000). Children Making a Community Whole: A review of Aboriginal head start
in urban and northern communities- Executive summary. Ottawa: Health Canada. Retrieved
on December 8, 2008, from http://www.phac-aspc.gc.ca/dca-
dea/publications/pdf/cmacw_exec_sum_final_e.pdf
Health Canada (2006). Brighter futures & building healthy community initiatives: Evaluation
summary. Ottawa: Health Canada. Retrieved on December 8, 2008, from http://www.hc-
sc.gc.ca/fniah-spnia/alt_formats/fnihb-dgspni/pdf/pubs/mental/2006-sum-rpt-eng.pdf
Health Council of Canada. (2006). Their future is now: Healthy choices for Canada’s children &
youth. Toronto: Health Council of Canada. Retrieved on May 10, 2009, from
http://www.healthcouncilcanada.ca/docs/rpts/2006/HCC_ChildHealth_EN.pdf
Hill, L.D. & Nelson, P. (2000). Communication is the key: Review of deaf mental health services
in British Columbia. Victoria: Inter-Ministry Jericho Coordinating Committee, Ministry for
Children and Families, Ministry of Health,
Ministry of Attorney General, Ministry of Education. Retrieved on April 9, 2009, from
http://www.mcf.gov.bc.ca/mental_health/pdf/deaf_mental_health.pdf
Institute for Health Economics (2008). Effective dissemination of findings from research.
Edmonton: Institute for Health Economics. Retrieved on March 2, 2009, from
http://www.ihe.ca/documents/Dissemination_0.pdf
Institute for Health Economics (2007). Mental health economic statistics in your pocket-Revised.
Edmonton: Alberta Mental Health Board. Retrieved on March 2, 2009, from
http://www.assembly.ab.ca/lao/library/egovdocs/2007/alpmh/165627.pdf
Institute for Health Economics (2008). How much should we spend on mental health?
Edmonton: Institute for Health Economics. Retrieved on March 2, 2009, from
http://www.ihe.ca/documents/Spending%20on%20Mental%20Health%20Final.pdf
Irish Mental Health Commission (2001). Quality framework: Mental health services in Ireland.
Dublin, Ireland: Mental Health Commission. Retrieved on April 9, 2009, from
http://www.hiqa.ie/media/pdfs/news/hiqa_qfwork_mh.pdf
Jordan’s Principle Fact Sheet. (n.d.). Retrieved on January 7, 2009, from
http://www.fncfcs.com/docs/JordansPrincipleFactSheet.pdf
Jezzard, B. (n.d.). Development of child and adolescent mental health services (CAMHS) in
England. London, UK: Department of Health. Retrieved on January 7, 2009, from
http://www.kidsmentalhealth.ca/documents/Res_Bob_Jezzard.pdf
Kendall-Taylor, N. & Mikulak, A. (2009). Child mental health: A review of the scientific
discourse. Washington, DC. FrameWorks Institute. Retrieved on December 22, 2008, from
http://www.frameworksinstitute.org/assets/files/PDF_childmentalhealth/childmentalhealthrev
iew.pdf
Kiefer, H., Cohen, N. & Pape, B. (2004). Handle with care: Strategies for promoting the mental
health of young children in community-based child care. Toronto: Canadian Mental Health
Association. Retrieved on December 22, 2008, from
http://www.cmha.ca/data/1/rec_docs/156_handle_with_care.pdf

Evergreen Framework
- 43 -
Kirby, M.J.L. & Keon, W.J. (2006). Out of the shadows at last: Transforming mental health,
mental illness and addiction services in Canada. Ottawa: Standing Senate Committee on
Social Affairs, Science and Technology. Retrieved on December 4, 2008, from
http://parl.gc.ca/39/1/parlbus/commbus/senate/Com-e/SOCI-E/rep-e/pdf/rep02may06high-
e.pdf
Kutcher, S., Davidson, S., & Manon, I., (2009). Child and Youth Mental Health Integrated
Health Care Using Contemporary Competency Based Teams. Paediatrics and Child Health,
14(5), 315-318.
Kutcher, S. (2007). Improving mental health outcomes in Canadian youth: Values, knowledge
and participation. Originally presented at the National Invitational Symposium on Child and
Youth Mental Health. Ottawa. Retrieved on December 8, 2008, from
http://www.cwlc.ca/files/file/events/Kutcher%20Presentation.pdf
Korhonen, M. (2004). Alcohol problems and approaches: Theories, evidence and northern
practice. Ottawa: National Aboriginal Health Organization. Retrieved on April 9, 2009, from
http://www.naho.ca/english/pdf/alcohol_problems_approaches.pdf
Lavis, J.N., Moynihan, R., Oxman, A.D., & Paulsen, E.J. (2008). Evidence-informed health
policy 4 – Case descriptions of organizations that support the use of research evidence.
Implementation Science, 3 (56). doi: 10.1186/1748-5908-3-56.
Lavis, J.N. (2009). How can we support the use of systematic reviews in policymaking? PLoS
Medicine, 6(11) e1000141.doi: 10.1371/journal.pmed.1000141.
Leadbeater, B., Lynch, A., Smith, A., Podmore, S., Martin, S., Simon, S., Peled, M., Clark, N. et
al., (2008). Listening to vulnerable youth: Transitioning to adulthood in British Columbia.
Victoria: BC Child and Youth Health Research Network. Retrieved on January 7, 2009, from
http://www.cyhrnet.ca/documents/ListeningtoVulnerableYouth-
TransitioningtoAdulthoodinBC.pdf
Leitch, K.K. (2007). Reaching for the top: A report by the advisor on healthy children & youth.
Ottawa: Health Canada. Retrieved on December 22, 2008, from http://www.hc-sc.gc.ca/hl-
vs/alt_formats/hpb-dgps/pdf/child-enfant/2007-advisor-conseillere/advisor-conseillere-
eng.pdf
Manitoba Healthy Living (2009). Reclaiming hope: Manitoba’s youth suicide prevention
strategy. Winnipeg: Manitoba Healthy Living. Retrieved on December 19, 2008, from
www.gov.mb.ca/healthyliving/mh/docs/suicide_prevention_framework.pdf
Manitoba Healthy Living (n.d.). A framework for suicide prevention planning in Manitoba.
Winnipeg: Manitoba Healthy Living. Retrieved on December 19, 2008, from
http://www.gov.mb.ca/health/mh/docs/suicide_prevention_framework.pdf
Manitoba Ministry of Health (2008). Breaking the chains of addictions: Manitoba’s five-point
strategic plan. Winnipeg: Manitoba Ministry of Health. Retrieved on December 19, 2008,
from www.gov.mb.ca/healthyliving/mh/plan.html
Marshall, K., Lewsley, P., Towler, K. & Aynsely., A. (2008). UK children’s commissioners’
report to the UN committee on the rights of the child. UK Children’s Commissioner.
Retrieved on January 22, 2009, from
http://www.sccyp.org.uk/UK_Childrens_Commissioners_UN_Report.pdf

Evergreen Framework
- 44 -
McCain, M.N., Mustard, J.F. & Shanker, S. (2007). Early years study 2: Putting science into
action. Toronto: Council for Early Child Development. Retrieved on December 22, 2008,
from
http://www.founders.net/fn/home.nsf/d600c375dbd231ab8525673a00539121/f6fee16051f10
b268525693b006b7c7a/$FILE/Early%20Years%20Study%202%20-
%20Putting%20Science%20into%20Action%20March%202007.pdf
McEwan, K. & Goldner, E.M. (2001). Accountability and performance indicators for mental
health services and supports: A resource kit. Ottawa: Health Canada. Retrieved on January 7,
2009, from http://www.phac-aspc.gc.ca/mh-sm/pdf/apimhss.pdf
McGorry, P. (2008). Strengthening the system where it’s weakest…Early intervention for young
people aged 12-25 in Australia. Retrieved on December 22, 2008, from
http://www.nucleusnetwork.com.au/Upload/Content/File/2008%20Docs/CRX08%20Speaker
%20Presentations/Australasia/Prof%20Patrick%20McGorry.pdf
McKee, M. (2009). Together into the future: A transformed mental health system for New
Brunswick. Fredericton: New Brunswick Department of Health. Retrieved on March 12,
2009, from http://www.gnb.ca/cnb/Promos/MentalHealth/NBMHS-e.pdf
Mental Health Commission of Canada (2009). Toward recovery and wellbeing: A framework for
a mental health strategy for Canada. Ottawa: Mental Health commission of Canada.
Retrieved on February 21, 2009, from
http://www.mentalhealthcommission.ca/SiteCollectionDocuments/boarddocs/15507_MHCC
_EN_final.pdf
Milliken, A.D., (2007). Bringing services for mental illness “Out of the Shadows”: First steps
towards a coherent policy for British Columbians with psychiatric illnesses. Retrieved on
January 9, 2009, from
http://www.health.gov.bc.ca/library/publications/year/2007/conversation_on_health/media/B
ringing_Services_for_Mental_Illnesses_Out_of_the_Shadows.pdf
Morrow, M. & Chappell, M. (1999). Hearing women’s voices: Mental health care for women.
Vancouver: BC Centre of Excellence for Women’s Health. Retrieved on March 10, 2009,
from http://synthesis.womenshealthdata.ca/uploads/topic197_0.pdf
National Aboriginal Health Organization (2006). Youth knowledge needs assessment project
report. Ottawa: NAHO. Retrieved on January 13, 2009, from www.naho.ca/firstnations/
english/documents/youth/FNC_YouthKnowledgeNeedsAssessmentReport.pdf
National Aboriginal Health Organization (2008). An overview of traditional knowledge and
medicine and public health in Canada. Ottawa: National Aboriginal Health Organization.
Retrieved on January 13, 2009, from
http://www.naho.ca/publications/tkOverviewPublicHealth.pdf
National Assembly for Wales (2001). Child and adolescent mental health services. Everybody’s
business: Strategy document. Cardiff: Wales. National Assembly for Wales, Primary &
Community Healthcare Division. Retrieved on January 22, 2009, from
http://www.wales.nhs.uk/publications/men-health-e.pdf
National Centre for Children in Poverty (2006). Children’s mental health: Facts for
policymakers. New York City, NY: National Centre for Children in Poverty, Columbia
University Mailman School of Public Health. Retrieved on January 8, 2009, from
http://www.nccp.org/publications/pdf/text_687.pdf

Evergreen Framework
- 45 -
National Public Health Partnership (2005). Healthy children – Strengthening promotion and
prevention across Australia: National public health strategic framework for children 2005–
2008. NPHP, Melbourne: National Public Health Partnership. Retrieved on January 22, 2009,
from
http://www.dhs.vic.gov.au/nphp/workprog/chip/documents/CHIPFramework14Sept05web.p
df
New Brunswick Ministry of Health (2008). Transforming New Brunswick’s health-care system:
The provincial health plan 2008-2012 major initiatives. Fredericton: New Brunswick
Ministry of Health. Retrieved on January 9, 2009, from
http://www.gnb.ca/cnb/promos/php/Initiatives-e.pdf
New South Wales Department of Health, Centre for Mental Health (1997). NSW Aboriginal
mental health policy: A strategy for the delivery of mental health services for Aboriginal
people in New South Wales. North Sydney, Australia: NSW Department of Health. Retrieved
on January 22, 2009, from http://www.health.nsw.gov.au/policy/cmh/publications/
Aboriginal%20Mental%20Health%20Policy.pdf
New South Wales Department of Health (2007). NSW Aboriginal mental health and well being
policy 2006-2010. North Sydney, Australia: NSW Department of Health Retrieved on
January 22, 2009 from http://www.health.nsw.gov.au/policies/pd/2007/pdf/PD2007_059.pdf
New South Wales Department of Health (n.d.). Prevention initiatives for child and adolescent
mental health. North Sydney, Australia: NSW Department of Health. Retrieved on January 7,
2009, from www.health.nsw.gov.au/policy/cmh/publications/Child_AdolesMH.pdf
New York State Office of Mental Health (2008). The children’s plan: Improving the social and
emotional well being of New York’s children and their families. Albany, NY: New York
State Office of Mental Health. Retrieved on January 7, 2008, from
http://www.niusileadscape.org/lc/Record/894
New Zealand Ministry of Health (2002). Te Puawaitanga Mäori mental health national
strategic framework. Wellington, New Zealand: Ministry of Health. Retrieved on May 8,
2009, from
http://www.moh.govt.nz/moh.nsf/0/76bcfc62ef772291cc256baa000f2ae0/$FILE/MaoriMent
alHealthNationalStrategicFramework.pdf
New Zealand Ministry of Health (2007). Te Raukura-Mental health and alcohol and other
drugs: Improving outcomes for children and youth. Wellington, New Zealand: Ministry of
Health. Retrieved on May 8, 2009, from
http://www.moh.govt.nz/moh.nsf/pagesmh/7461/$File/te-raukura.pdf
New Zealand Ministry of Health (n.d.). United future: Health policy. Wellington, New Zealand:
Ministry of Health. Retrieved on January 22, 2009, from
http://www.unitedfuture.org.nz/assets/sm/982/46/HealthPolicy-Final.pdf
Northwest Territories Health and Social Services (2004). Action plan: Mental health and
addictions services. Yellowknife: Northwest Territories Health and Social Services.
Retrieved on January 7, 2009, from
http://www.hlthss.gov.nt.ca/pdf/reports/mental_health_and_addictions/2004/english/action_p
lan_mental_health_and_addiction_services.pdf
Nova Scotia Department of Health (2003). Standards for mental health services in Nova Scotia.
Halifax: Nova Scotia Department of Mental Health. Retrieved on January 7, 2009, from
http://www.gov.ns.ca/health/mhs/pubs/Standards_Mental_Health_Services_2009.pdf

Evergreen Framework
- 46 -
Nova Scotia Department of Justice: Policy, Planning and Research (2006). Perspectives on youth
crime in Nova Scotia. Halifax: Nova Scotia Department of Justice. Retrieved on December
23, 2008, from http://www.gov.ns.ca/just/publications/documents/Youth_FinalMay906.pdf
Ontario Ministry of Children and Youth Services (2006). A shared responsibility: Ontario’s
policy framework for child and youth mental health. Toronto: Ontario Ministry of Children
and Youth Services. Retrieved on January 13, 2009, from
http://www.children.gov.on.ca/htdocs/English/documents/topics/specialneeds/mentalhealth/fr
amework.pdf
Ontario Ministry of Children and Youth Services (2008). Realizing potential: Our children, our
youth, our future. Toronto: Ministry of Children and Youth Services. Retrieved on
December 7, 2009, from
http://www.children.gov.on.ca/htdocs/English/documents/about/StrategicFramework.pdf
Pape, B. (2006). Discussion paper on mental health promotion. The Ontario Prevention
Clearinghouse. Retrieved on March 3, 2009, from
http://www.healthnexus.ca/policy/mhp_report_nov06.pdf
Pereira, N. (2007). Ready... set... engage! Building effective youth/adult partnerships
for a stronger child and youth mental health system. Toronto: Children’s Mental Health
Ontario & Ottawa: The Provincial Centre of Excellence for Child and Youth Mental Health
at CHEO. Retrieved on March 24, 2009, from
http://www.thenewmentality.ca/documents/Ready%20Set%20engage.pdf
Prince Edward Island Department of Health and Social Services (2001). Strategic plan for the
Prince Edward Island health and social services system. Charlottetown: Prince Edward
Island Department of Health and Social Services. Retrieved on December 23, 2008, from
http://www.gov.pe.ca/photos/original/hss_stratplan.pdf
Proulx, J. & Nighswander, M.R. (2007). Manitoba provincial forum on trauma recovery.
Winnipeg: RESOLVE Manitoba. Retrieved on December 18, 2008, from
http://www.suicideline.ca/traumafiles/Trauma%20Report%20September%2013%202007.pdf
Provincial Strategic Framework Development Committee (2006). Nova Scotia strategic
framework to address suicide. Halifax: Nova Scotia Department of Health. Retrieved on
January 7, 2009, from http://www.gov.ns.ca/hpp/publications/SuicideFramework.pdf
Richard, B. (2008). Connecting the dots: A report on the condition of youth-at-risk and youth
with very complex needs in New Brunswick. Fredericton: New Brunswick Ombudsman and
Child and Youth Advocate. Retrieved on December 19, 2008, from
http://www.gnb.ca/0073/PDF/ConnectingtheDots-e.pdf
Ro, M. & Shum, L. (2001). Forgotten policy: An examination of mental health in the U.S - A
series of community voices publications. Bottle Creek, MI: W.K. Kellogg Foundation.
Retrieved on January 13, 2009, from
http://www.communityvoices.org/Uploads/4c2xne45g5ezjq45414wni55_20020826102804.p
df
Romanow, R.J. (2002). Building on values: The future of health care in Canada. Ottawa:
Commission on the Future of Health Care in Canada. Retrieved on January 19, 2008, from
http://publications.gc.ca/pub?id=237274&sl=0
Rosenthal, E. & Sundram, C.J. (2004). The role of international human rights in national mental
health legislation. Geneva: World Health Organization. Retrieved on December 25, 2008,
from
http://www.who.int/mental_health/policy/international_hr_in_national_mhlegislation.pdf
Evergreen Framework
- 47 -
Rutter, M. (2008). Biological implications of gene-environment interaction. Journal of
Abnormal Child Psychology, 36, 969-975.
Salmon, A., Poole, N., Morrow, M., Greaves, L., Ingram, R. & Pederson, A. (2006). Improving
conditions: Integrating sex and gender into federal mental health and addictions policy.
Vancouver: The British Columbia Center of Excellence for Women’s Health. Retrieved on
March 10, 2009, from http://www.cwhn.ca/PDF/ImprovingConditions.pdf
Saskatchewan Health (n.d.). A better future for youth: Saskatchewan’s plan for child & youth
mental health services. Regina: Saskatchewan Health. Retrieved on December 8, 2008, from
http://www.health.gov.sk.ca/better-future-youth
Saskatchewan Health Organization Research and Evaluation (2007). Child and youth mental
health services in Saskatchewan: In search of applicable outcome indicators. Regina:
Community Care Branch Saskatchewan Health. Retrieved on December 25, 2008, from
http://www.medicine.usask.ca/psychiatry/downloads-reports/Child%20-
%20Youth%20Mental%20Health%20Services.pdf
Scotland Health Department (2004). Children and young people’s mental health: A framework
for promotion, prevention and care – Draft for consultation. Edinburgh: Health Department.
Retrieved on January 22, 2009, from
http://www.scotland.gov.uk/Resource/Doc/77843/0018686.pdf
Shonkoff, J.P., Boyce, T.W., McEwen, B.S. (2009). Neuroscience, molecular biology, and the
childhood roots of health disparities; Building a new framework for health promotion and
disease prevention. Journal of the American Medical Association, 301(21), 2252-2259.
Sub-committee on Self-regulating Systems for the Federal/Provincial/Territorial Working Group
on the Mental Health and Well-being of Children Youth (n.d.). Celebrating success: A self-
regulating service delivery system for children and youth. Ottawa: Health Canada. Retrieved
on January 7, 2009, from http://www.phac-aspc.gc.ca/dca-
dea/publications/pdf/celebrating_e.pdf
The Provincial Centre of Excellence for Child and Youth Mental Health at CHEO (2006).
Indicators of quality for child and youth mental healthcare in Ontario. Ottawa: The
Provincial Centre of Excellence for Child and Youth Mental Health at CHEO. Retrieved on
January 7, 2009, from http://www.onthepoint.ca/publications/reports/Indicators.pdf
Trainor, J., Pomeroy, E., & Pape, B. (2004). A framework for support: 3rd
Edition. Toronto:
Canadian Mental Health Association. Retrieved on December 22, 2008, from
http://www.cmha.ca/data/1/rec_docs/120_Framework3rdEd_Eng.pdf
Tremblay, R.E., Nagin, D.S., Seguin, J.R., Zoccolillo, M. Zelazo, P.D., Boivin, M. Perusse, D. &
Japel, C. (2004). Physical aggression during early childhood: Trajectories and predictors.
Pediatrics, 114(1), e43-e56.
United Kingdom Department for Education and Skills (2001). Promoting mental health within
early years and school settings. Sherwood Park, UK: Department for Education and Skills.
Retrieved on January 22, 2009, from
http://www.teachernet.gov.uk/_doc/12605/promoting%20mental%20health%20guidance%20
2001.pdf
United Kingdom Department of Health (2004). Executive summary, national service framework
for children. London: UK Department of Health. Retrieved on December 22, 2009, from
http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digital
asset/dh_4090552.pdf

Evergreen Framework
- 48 -
United Kingdom Department of Health (2004). The mental health and psychological well-being
of children and young people: National service framework for children, young people and
maternity services. London: UK Department of Health. Retrieved on December 22, 2009,
from
http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digital
asset/dh_4090560.pdf
United Kingdom Child and Adolescent Mental Health Services (2008). Children and young
people in mind: The final report of the national CAMHS review. London: UK Department of
Health. Retrieved on December 22, 2008, from
http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digital
asset/dh_090398.pdf
United Kingdom Department of Health (2009). New horizons: A shared vision for mental health.
London, UK: Department of Health. Retrieved on February 10, 2010, from
http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digital
asset/dh_109708.pdf
United Nations (1989). Convention on the rights of the child. New York: United Nations
Retrieved on January 5, 2009 from http://www2.ohchr.org/english/law/crc.htm
United Nations (2002). A world fit for children. New York: United Nations. Retrieved on
January 5, 2009 from
http://www.unicef.org/specialsession/docs_new/documents/A-RES-S27-2E.pdf
United Nations (2006). Convention on the rights of persons with disabilities and optional
protocol. New York: United Nations. Retrieved on January 5, 2009, from
http://www.un.org/disabilities/documents/convention/convoptprot-e.pdf
United Nations (2007). Declaration on the rights of Indigenous Peoples. New York: United
Nations. Retrieved on January 5, 2009, from
http://www.un.org/esa/socdev/unpfii/documents/DRIPS_en.pdf
United Nations (1991). Principles for the protection of persons with mental illness and for the
improvement of mental health care. New York: United Nations: Retrieved on January 5,
2009 from http://www.un.org/documents/ga/res/46/a46r119.htm
Vancouver Coastal Health (n.d.). A mental health and addiction framework for services:
Vancouver. Vancouver: Vancouver Coastal Health. Retrieved on January 7, 2009, from
http://vancouver.ca/commsvcs/housing/supportivehousingstrategy/pdf/StrategyFramework.p
df
Volpe, R., Batra, A., Bomio, S., & Costin, D. (1999). Third generation school-linked services
for at risk children. Toronto: Institute of Child Study. Retrieved on May 10, 2009, from http://fcis.oise.utoronto.ca/~rvolpe/thirdgen.html
Waddell, C., McEwan, K., Shepherd, C.A., Offord, D.R. & Josephine, M.H. (2005). A public
health strategy to improve the mental health of Canadian children. Canadian Journal of
Psychiatry, 50(4), 226-233.
Waddell, C. McEwan, K. & Peters, R.D. (2007). Preventing mental disorders in children: A
public health priority. Canadian Journal of Public Health, 98(3), 174-178.
Welsh Assembly Government (n.d.). Mental health policy: Implementation guidance for child
and adolescent mental health services. Retrieved on January 8, 2009, from
http://www.wales.nhs.uk/documents/commioning-child-mh.pdf
Evergreen Framework
- 49 -
Wener, P. (2003). Consultation on disordered eating/eating disorders draft report. Winnipeg:
The Winnipeg Regional Health Authority: Mental Health Program and The Winnipeg
Regional Health Authority: Child and Adolescent Mental Health Program. Retrieved on
December 25, 2008, from
http://www.wrha.mb.ca/community/mentalhealth/files/EatingDisorders_May03.pdf
Winnipeg Regional Health Authority (2003). Development of a suicide prevention strategy.
Winnipeg: Winnipeg Regional Health Authority. Retrieved on January 7, 2009, from
http://www.gov.mb.ca/health/mh/docs/hope.pdf
Winnipeg Regional Health Authority (2004). Position statement on mental health promotion and
prevention. Winnipeg: Winnipeg Regional Health Authority. Retrieved on December 25,
2008, from http://www.wrha.mb.ca/community/mentalhealth/files/PS_MentalHealth.pdf
White, J. (2005). Preventing suicide in youth: Taking action with imperfect knowledge.
Vancouver: Children’s Mental Health Policy Research Program, University of British
Columbia. Retrieved on January 7, 2009, from
http://www.childhealthpolicy.sfu.ca/research_reports_08/rr_pdf/RR-9-05-full-report.pdf
World Health Organization (2005). Assessment instrument for mental health (AIMS). Geneva:
WHO. Retrieved on February 28, 2009, from
http://www.who.int/mental_health/evidence/AIMS_WHO_2_2.pdf
World Health Organization (2005). WHO resource book on mental health, human rights and
legislation: Stop exclusion, dare to care. Geneva: WHO. Retrieved on December 25, 2008,
from http://www.who.int/mental_health/policy/who_rb_mnh_hr_leg_FINAL_11_07_05.pdf
World Health Organization (2005). Child and adolescent mental health policies and plans:
Mental health policy and service guidance package. Geneva: WHO. Retrieved on January 8,
2009, from http://www.who.int/mental_health/policy/Childado_mh_module.pdf
World Health Organization (2007). Action needed on improving mental health for adolescents.
European forum on social cohesion for mental well-being among adolescents. Paper
presentation in Viareggio, Italy, October 2, 2007. Retrieved on May 8, 2009, from
http://www.euro.who.int/__data/assets/pdf_file/0005/84623/E91921.pdf
World Health Organization-Europe (2008). European pact for mental health and well-being. EU
High-level Conference ―Together for Mental Health and Wellbeing‖ Brussels, 12-13 June,
2008). Retrieved on February 28, 2009, from
http://ec.europa.eu/health/ph_determinants/life_style/mental/docs/pact_en.pdf

Evergreen Framework
- 50 -
Appendix A: Evergreen’s Development Process
Evergreen’s Development Team
Evergreen’s Development Team, responsible for planning, project oversight and final document
preparation is comprised of Dr. Stan Kutcher, project lead and chair of Evergreen’s Drafting
Committee and Mr. Alan McLuckie, Project Coordinator. Ms. Jessica Wishart, Youth
Engagement Coordinator, assisted the Development Team with the youth engagement activities.
Following receipt of the MHCC grant, used to support the development of Evergreen, the
Development Team actively recruited advisory committee members, established the
technological platform for the on-line development of Evergreen (i.e., Socialtext) and began to
compile a resource library that would inform its creation. Subsequently, the Development Team
elicited stakeholder engagement; established the processes by which consultations would occur
and how consultation materials would be analyzed; finalized the resource library; assisted in the
writing of the draft versions of Evergreen; and provided technical support to members of the
drafting and advisory committees. Finally, the Development Team maintained ongoing contact
with the CYAC and MHCC, participated in face-to-face conference-based discussions and
produced the Evergreen document following final input from the CYAC.
Drafting, National Advisory, International Advisory and Youth Advisory Committees
A multi-stage recruitment process was used to construct Evergreen’s Drafting and Advisory
committees. Committee members were invited to participate in Evergreen’s development with
the explicit understanding that they did not represent any organizations or interest groups.
In the initial recruitment stage, the chair of the Drafting Committee, along with key informants
from the CYAC of the MHCC, nominated committee members, including young people and
parents with interest in, or lived experience with, child and youth mental health. An additional
on-line search was conducted by Evergreen’s Project Coordinator of institutions, organizations
and programs servicing young people and families, as well as policy and research documents to
identify additional professionals, parents and young people with expertise with child and youth
mental health who could be potentially recruited to one of Evergreen’s advisory committees.
Recruitment efforts placed emphasis on identifying young people and parents from a diverse
range of geographic regions and social circumstances. For example, contact was established with
young people previously recognized with community advocacy awards related to mental health.
The subsequent recruitment stage asked those committee members identified in the first round of
recruitment, to nominate additional committee members whose skill set, area of expertise,
geographic location, or social circumstance would enhance the scope and expertise of
Evergreen’s advisory committees. For example, efforts were made to engage with professionals
working with street-youth in several cities in order to utilize these advisors both for their
expertise and as a conduit to a hard-to-reach population. In the final recruitment stage, committee
members were specifically requested to review the existing membership to ensure that the
committees demonstrated diversity and a wide range of expertise.

Evergreen Framework
- 51 -
The Drafting Committee was comprised of individuals with nationally or internationally
recognized expertise in the areas of child and youth mental health, health care, child welfare,
human rights, culture, economics and education. Young people and parents who had lived
experience with mental illness who had been active in national child and youth mental health
initiatives were also invited to be members of this committee. The role of the Drafting
Committee was to work collaboratively, using online technologies to co-write the nucleus of the
Evergreen document using their own knowledge and input from the National Advisory
Committee, the International Advisory Committee and the public consultations. Refer to
Appendix B for a list of Drafting Committee members.
Members of Evergreen’s National Advisory Committee have recognized experience and
expertise across a wide variety of domains including mental health, child health, health,
education, justice, social service, human rights, culture, business, economics and other areas
relevant to child and youth mental health. Young people, parents and family members with lived
experienced with mental health were also members of this committee. The role of the National
Advisory Committee was to provide input on child and youth mental health to the Drafting
Committee as well as to review and provide critical feedback on materials created by the
Drafting Committee. A secondary role of this committee was to function as a conduit to engage
organizations and the public in Evergreen’s on-line consultations. Refer to Appendix B for a list
of this committee’s membership.
The International Advisory Committee was comprised of leaders in the area of child and youth
mental health policy, promotion, prevention, intervention and research across the globe. Many of
these individuals have had direct experience developing mental health policies, plans, programs
and services in their respective countries. The role of the International Advisory Committee was
to provide input to the Drafting Committee on child and youth mental health issues and to review
and provide critical feedback on various materials created by the Drafting Committee. Refer to
Appendix B for a comprehensive list of this committee’s membership.
A Youth Advisory Committee (YAC) was formed following Evergreen’s national consultation at
the Second National Invitational Symposium on Child and Youth Mental Health, hosted by the
Child Welfare League of Canada in Ottawa. There, youth noted that they would benefit from
having a separate youth-only advisory group, in addition to youth sitting on Evergreen’s other
committees. Evergreen’s YAC was thus established and was actively involved in the design and
dissemination of youth-specific materials related to Evergreen’s public consultation, including
the use of a ―community champions‖ model, whereby members of the YAC would engage young
people from their respective communities in Evergreen’s online public consultations. Refer to
Appendix B for a list of this committee’s membership.
Creating the Evergreen Framework Document
Evergreen was developed in three phases beginning in the winter of 2008, concluding in the
spring of 2010. The preliminary phase of the project focused on forming advisory committees
and constructing an online library designed to help inform the work of Evergreen’s Drafting and
Advisory Committees and to support the public consultation.

Evergreen Framework
- 52 -
The initial library compilation was created by the Evergreen development team. Each Evergreen
committee member was also asked to provide suggestions for materials to be included in the
library. As new materials relevant to Evergreen were published during Evergreen’s development
these were added to the library. The library’s holdings included Canadian policy (national as
well as provincial/territorial) documents as well as policies and plans from the World Health
Organization and governments around the globe. Seminal research articles and recent reviews
pertaining to child mental health were also included. Library contents were posted on-line in
PDF formats and were made available to all Committee members as well as to any member of
the public who wished to access them.
An independent review of numerous child and youth mental health policies and plans from
across Canada and around the world that had been placed in the library, was commissioned to
identify strategic directions found in those documents. These were used to help inform
Evergreen’s strategic directions.
Phase 1: Values
Evergreen articulates the values upon which it is based and these are expected to be used to
inform its strategic directions and the programs, services and activities that are developed to
operationalize each strategic direction. To identify these values, the Evergreen Development
Team engaged in a values consultation from spring 2009 to spring 2010 that included: multiple
online discussions among Evergreen committee members, face-to-face discussions at national
conferences in Ottawa and Vancouver and multiple on-line public consultations.
Step 1: Online consultation with Evergreen’s committee members seeking
examples of values pertinent to a national child and youth mental health
framework.
Step 2: Evergreen’s Drafting Committee used an online wiki-forum to co-write a draft
version of Evergreen’s values, incorporating the input gathered in step one.
Step 3: An extensive public awareness campaign was conducted drawing attention to the
opportunity to participate. Traditional and non-traditional means of engaging the
public were employed. Traditional routes included sending posters advertising the
public consultation process via regular mail. These posters were mass-mailed to
every school-board and all major children’s mental health centres and community
recreational programs across Canada. The consultation was also advertised
through letter-to-the-editor submissions to national health care journals, and in
Today’s Parent magazine. Materials were mailed to all federal and
provincial/territorial ministries involved with young people and families. In
addition to this mail out, consultation materials were emailed through distribution
lists of large health care and social service institutions, organizations and
associations, including the MHCC, Canadian Association of Paediatric Health
Centres, Canadian Psychiatric Association, Canadian Paediatric Society, and
others. Links to the surveys were also hosted on the websites of multiple
associations and organizations, such as the MHCC, as well sites frequented by
young people, such as www.mindyourmind.ca. A Facebook group was also
established, which at its high point had a membership of over 1500 individuals,
Evergreen Framework
- 53 -
allowing for ongoing dialogue between members in addition to hosting a link to
the online consultations. The National Advisory Committee and the Youth
Advisory Committees were instrumental in distributing hard copies and email
copies to their friends, family members and members of their communities.
Step 4: An online written public consultation was conducted resulting in over 1000
distinct inputs from all regions of Canada. A separate online consultation
specifically targeting young people received input from over 200 youth. Specific
attempts were made to engage with young people, individuals with lived mental
health experience, individuals from rural or remote regions and other vulnerable
groups. Consultation was based on individual not on organizational input, thus
avoiding the lobby group models commonly seen in government consultations.
For additional information regarding the composition of the participant group,
please refer to Table 1. Input from the public consultation process was made
available to Evergreen’s committees to be used in the creation of Evergreen. Step 5: Simultaneous to the public consultation process, Evergreen’s National and
International Advisory Committees engaged in an online values discussion using
Socialtext, a computer program well-suited to collaborative projects. Step 6: A researcher experienced with qualitative research methods and tools provided
support to the Drafting Committee by analyzing and synthesizing information
obtained from the public consultation. NVivo, a computer program for qualitative
research, was used to help thematically organize consultation materials which
were made available to the various committees. Step 7: Using all the above inputs, the Drafting Committee created a draft of Evergreen’s
values. Step 8: Face-to-face consultations pertaining to the Evergreen values draft were held at
two national conferences: the Second National Invitational Symposium on Child
and Youth Mental Health, hosted by the Child Welfare League of Canada (held in
Ottawa), and the Into the Light Conference, hosted by the Mental Health
Commission of Canada, Vancouver Coastal Health and Simon Fraser University’s
Centre for Applied Research in Mental Health and Addiction (held in Vancouver).
These consultations took the form of focus groups and small group discussions
with participants from across Canada with diverse perspectives on child and youth
mental health, including policy writers, researchers, practitioners, Aboriginal
Peoples, educators, health care workers, young people, and others with interest or
expertise in child and youth mental health.
Step 9: Feedback from the national conferences was used by Evergreen’s committees to
further inform the development of Evergreen’s values including the identified
need for the final version to be constructed in a ―plain English‖ format.
Step 10: The modified values document was posted for public feedback and review for
further suggestions. Over 800 individuals participated, sharing written feedback,
as well as providing a quantitative ranking of their agreement. Using a numeric
scale, participants ranked Evergreen’s values out of a possible score of 7, where 1
denoted no acceptance and 7 indicated complete acceptance of the values. Over
90 percent of participants noted their positive acceptance of the values (e.g.,
scores 5 to 7).
Step 11: Evergreen’s values were finalized.
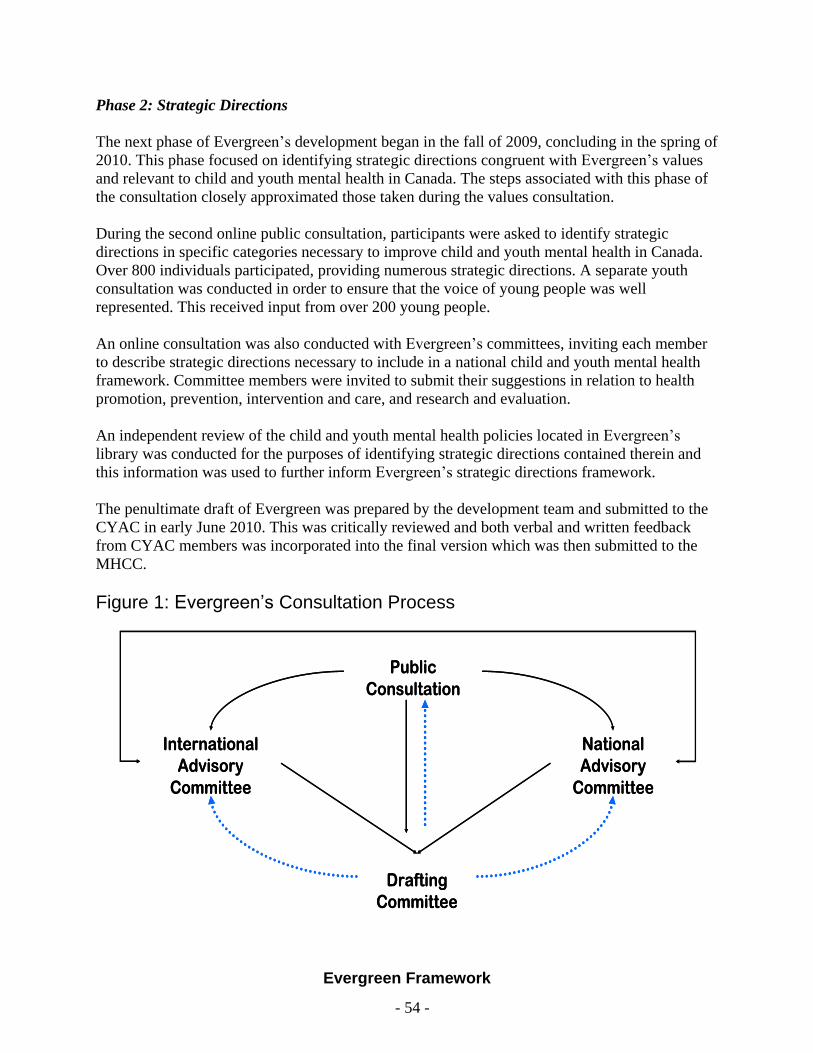
Evergreen Framework
- 54 -
Phase 2: Strategic Directions
The next phase of Evergreen’s development began in the fall of 2009, concluding in the spring of
2010. This phase focused on identifying strategic directions congruent with Evergreen’s values
and relevant to child and youth mental health in Canada. The steps associated with this phase of
the consultation closely approximated those taken during the values consultation.
During the second online public consultation, participants were asked to identify strategic
directions in specific categories necessary to improve child and youth mental health in Canada.
Over 800 individuals participated, providing numerous strategic directions. A separate youth
consultation was conducted in order to ensure that the voice of young people was well
represented. This received input from over 200 young people.
An online consultation was also conducted with Evergreen’s committees, inviting each member
to describe strategic directions necessary to include in a national child and youth mental health
framework. Committee members were invited to submit their suggestions in relation to health
promotion, prevention, intervention and care, and research and evaluation.
An independent review of the child and youth mental health policies located in Evergreen’s
library was conducted for the purposes of identifying strategic directions contained therein and
this information was used to further inform Evergreen’s strategic directions framework.
The penultimate draft of Evergreen was prepared by the development team and submitted to the
CYAC in early June 2010. This was critically reviewed and both verbal and written feedback
from CYAC members was incorporated into the final version which was then submitted to the
MHCC.
Figure 1: Evergreen’s Consultation Process
International
Advisory
Committee
National
Advisory
Committee
Drafting
Committee
Public
Consultation
International
Advisory
Committee
National
Advisory
Committee
Drafting
Committee
Public
Consultation
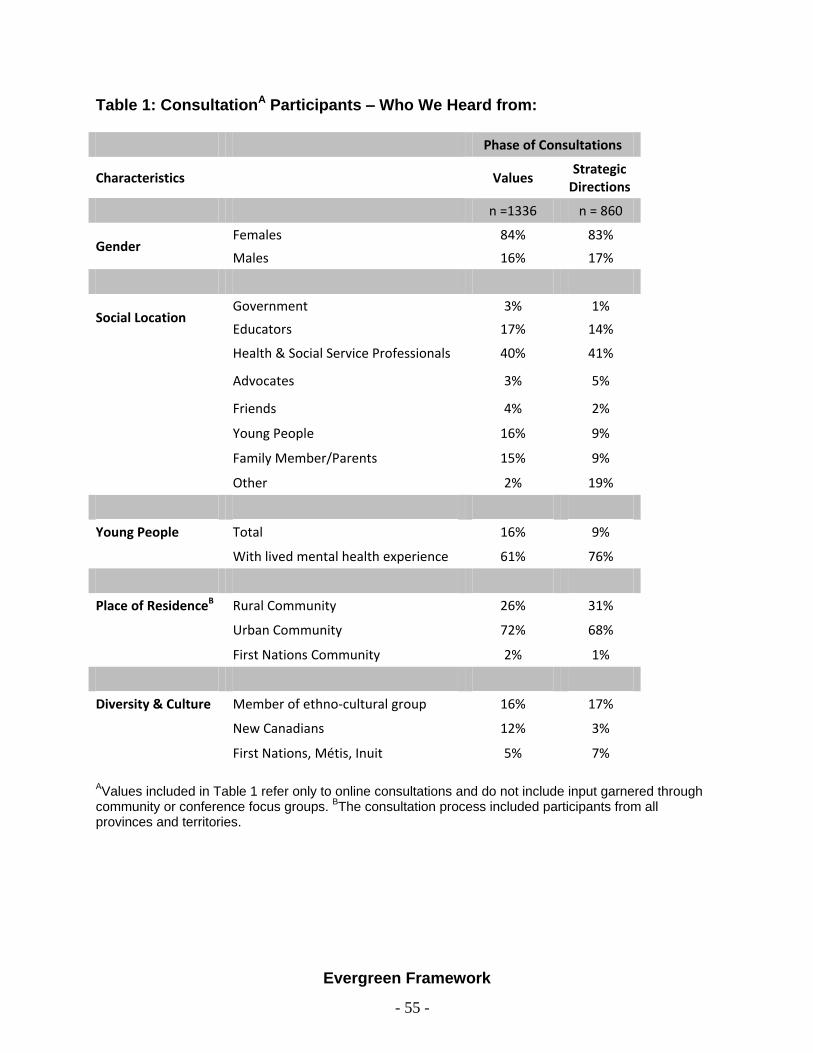
Evergreen Framework
- 55 -
Table 1: ConsultationA Participants – Who We Heard from:
Phase of Consultations
Characteristics Values Strategic
Directions
n =1336 n = 860
Gender Females 84% 83%
Males 16% 17%
Social Location Government 3% 1%
Educators 17% 14%
Health & Social Service Professionals 40% 41%
Advocates 3% 5%
Friends 4% 2%
Young People 16% 9%
Family Member/Parents 15% 9%
Other 2% 19%
Young People Total 16% 9%
With lived mental health experience 61% 76%
Place of ResidenceB Rural Community 26% 31%
Urban Community 72% 68%
First Nations Community 2% 1%
Diversity & Culture Member of ethno-cultural group 16% 17%
New Canadians 12% 3%
First Nations, Métis, Inuit 5% 7%
AValues included in Table 1 refer only to online consultations and do not include input garnered through
community or conference focus groups. BThe consultation process included participants from all
provinces and territories.
Evergreen Framework
- 56 -
Appendix B - Evergreen’s Committee Membership
Drafting Committee
Dr. Stan Kutcher – Chair, Evergreen Drafting Committee; Sun Life Chair in Adolescent Mental
Health; Director of the World Health Organization Collaborating Center in Mental Health
Training and Policy Development, Halifax, NS, Canada
Ms. Keli Anderson - Member, Child & Youth Advisory Committee, Mental Health Commission
of Canada; Executive Director, F.O.R.C.E., Society for Kids’ Mental Health, Vancouver,
BC, Canada
Dr. Ramona Alaggia - Associate Professor, Factor-Inwentash Faculty of Social Work,
University of Toronto, ON, Canada
Dr. Cindy Blackstock - Executive Director, First Nations Child and Family Caring Society of
Canada, Ottawa, ON, Canada
Dr. Katherine Boydell - Senior Scientist, Population Health Sciences, The Hospital for Sick
Children, Toronto, ON, Canada
Dr. Simon Davidson - Chair, Child and Youth Advisory Committee, Mental Health
Commission of Canada; Regional Chief of Specialized Psychiatric and Mental Health
Services, Children’s Hospital of Eastern Ontario, Ottawa, ON, Canada
Dr. Margaret Clarke - Fraser Mustard Chair in Childhood Development; Professor of
Psychiatry and Pediatrics, Department of Psychiatry and Pediatrics, University of
Calgary, Canada
Ms. Pat Brimblecombe - Parent Advocate, Barrie, ON, Canada
Mr. Irwin Elman - Chief Advocate, Office of the Ontario Provincial Advocate, Toronto,
Canada
Dr. Bruce Ferguson - Director, Community Health Systems Resource Group, The Hospital for
Sick Children, Toronto, ON, Canada
Dr. Eric Fombonne - Canada Research Chair in Child and Adolescent Psychiatry; Director of
the Department of Psychiatry at the Montreal Children’s Hospital, Montreal, QC, Canada
Ms. Michelle Forge - Education Advocate and Consultant; Former Co-director of the Ontario
Council of Directors of Education, Meaford, ON, Canada
Dr. Jaswant Guzder - Associate Professor, Department of Psychiatry, McGill University; Head
of Child Psychiatry and Director of Child Day Treatment at the Jewish General Hospital,
Montreal, QC, Canada
Ms. Susan Hess - Mental Health Advocate; Past President of Parents for Children’s Mental
Health, Windsor, ON, Canada
Dr. Philip Jacobs - University of Alberta School of Public Health Sciences; Fellow of the
Institute of Health Economics, Edmonton, AB, Canada
Mr. Chris Korvela - Youth Mental Health Advocate, Calgary, AB, Canada
Dr. John LeBlanc – Assistant Professor of Pediatrics, Psychiatry, and Community Health and
Epidemiology, Dalhousie University, Halifax, NS, Canada
Dr. Kellie Leitch - Associate Professor, Faculty of Medicine, University of Toronto; Chair,
Centre for Health Innovation & Leadership, Richard Ivey School of Business, Toronto,
Canada
Ms. Bronwyn Loucks - Youth Mental Health Advocate, Kingston, ON, Canada
Evergreen Framework
- 57 -
Dr. Harriet MacMillan – Professor, Department of Psychiatry & Behavioural Neurosciences
and Pediatrics, McMaster University, Hamilton, ON, Canada
Mr. Mat Marchand - Youth Mental Health Advocate, Vancouver, BC, Canada
Dr. Ian Manion - Associate Director, Research Institute at Children's Hospital of Eastern
Ontario; Clinical Professor in the School of Psychology, University of Ottawa, Ottawa,
ON, Canada
Dr. Gillian Mulvale - Senior Policy Advisor, Mental Health Commission of Canada; Assistant
Professor, Department of Clinical Epidemiology & Biostatistics, McMaster University,
Hamilton, ON, Canada
Dr. Pratibha Reebye - Clinical Director, Infant Psychiatry Clinic, Children’s & Women’s
Health Centre of BC, Vancouver, BC, Canada
Ms. Nancy Reynolds – Member, Child and Youth Advisory Committee, Mental Health
Commission of Canada; President and CEO of the Alberta Centre for Child, Family and
Community Research, Edmonton, AB, Canada
Ms. Catherine Pringle - Youth Mental Health Advocate, Toronto, ON, Canada
Dr. Tom Ward - Former Deputy Minster of Health, Province of Nova Scotia, Victoria, BC,
Canada
Dr. Jean Wittenberg - Associate Professor, Faculty of Medicine, the University of Toronto;
Head of the Psychotherapies Program at the Hospital for Sick Children, Toronto, ON,
Canada
National Advisory Committee
Dr. Jean Addington – Department of Psychiatry, University of Calgary, Calgary, AB, Canada
Dr. Robert Armstrong – Chief of Pediatric Medicine, BC Children’s Hospital, Vancouver, BC,
Canada
Dr. Linda Baker – Executive Director, Centre for Children and Families in the Justice System,
London, ON, Canada
Dr. Melanie Barwick – Assistant Professor in the Department of Psychiatry and the Dalla Lana
School of Public Health at the University of Toronto; Director of Knowledge Translation,
Child Health Sciences Program, The Hospital for Sick Children, Toronto, ON, Canada
Ms. Nancy, Beck – Director of Connections Clubhouse, Halifax, NS, Canada
Ms. Heidi Bernhardt – Executive Director, Canadian ADHD Resource Alliance, Toronto, ON,
Canada
Dr. Cheri Bethune - Faculty of Medicine, Memorial University, St. John’s, NL, Canada
Ms. Ann Blackwood - Director of English Program Services, Nova Scotia Department of
Education and Culture, Halifax, NS, Canada
Ms. Leanne Boyd – Director of Policy, Development, Research and Evaluation, Healthy Child
Manitoba, Winnipeg, MB, Canada
The Hon. Judge Alfred Brien- Mental Health Court, Saint John, NB, Canada
Dr. Elsa Broder - Psychiatrist, Hincks-Dellcrest Treatment Centre, Toronto, ON, Canada
Dr. Russell Callaghan - Scientist, Social, Prevention and Health Policy Research Department
and Assistant Professor, Department of Public Health Sciences, The University of
Toronto, Toronto, ON, Canada
Evergreen Framework
- 58 -
Ms. Melissa Campbell - Child, Family and Community Consultant, Provincial Services for the
Deaf and Hard of Hearing, Ministry of Children and Family Development, Vancouver,
BC, Canada
Dr. David Cawthorpe - Research & Evaluation Coordinator, Child & Adolescent Mental Health
Program, Alberta Health Services, Calgary, AB, Canada
Dr. Michael Chandler – Professor, Department of Psychology, University of British Columbia,
Vancouver, BC, Canada
Dr. Alice Charach - Head of Outpatient Neuropsychiatry, The Hospital for Sick Children,
Toronto, ON, Canada
Ms. Sandi Carmichael - Educational Consultant & Advocate, Port Williams ,NS, Canada
Ms. Gloria Chaim - Deputy Clinical Director, Child Youth and Family Program, Centre for
Addictions and Mental Health, Toronto, ON, Canada
Dr. Connie Coniglio - Director of Health Literacy at BC Mental Health and Addiction Services,
Vancouver, BC, Canada
Ms. Marion Cooper – Department of Mental Health Promotion, Winnipeg Regional Health
Authority; President of the Canadian Association for Suicide Prevention, Winnipeg, MB,
Canada
Dr. Penny Corkum – Associate Professor, Department of Psychology, Dalhousie University,
Halifax, NS, Canada
Mr. Andy Cox - Member, Board of Directors, Mental Health Commission of Canada; Mental
Health Patient Advocate for children and youth, IWK Health Centre, Halifax, NS,
Canada
Dr. Janice Currie - Vice President, Counselling Services, Kids Help Phone, Toronto, ON,
Canada
Dr. Dell Ducharme – Psychologist, Manitoba Adolescent Treatment Centre; Department of
Clinical Health Psychology, University of Manitoba, Winnipeg, MB, Canada
Ms. Catherine Dyer - Project coordinator for the New Mentality Project, Toronto, ON, Canada
Ms. Marie Fast- Clinical Manager, Whitehorse Mental Health Services, Whitehorse, YT,
Canada
Ms. Jane Fitzgerald - Executive Director, Children’s Aid Society of London & Middlesex,
London, ON, Canada
Dr. Roger Freeman - Department of Psychiatry, University of British Columbia, Vancouver,
BC, Canada
Ms. Ruth daCosta - Executive Director of Covenant House, Toronto, ON, Canada
Ms. Laurie Dart - Executive Director Griffin Centre, Toronto, ON, Canada
Dr. Marie-Josée Fleury - Assistant Professor, Department of Psychiatry, McGill University,
Montreal, QC, Canada
Dr. E. Jane Garland – Clinical Professor, Department of Psychiatry, University of British
Columbia, Vancouver, BC, Canada
Dr. Eudice Goldberg - Staff Paediatrician, Adolescent Medicine, The Hospital for Sick
Children, Toronto, ON, Canada
Mr. Yude Henteleff - Senior counsel, Pitblado Barristers and Solicitors; Member of the
Advisory Council, Canada Lawyers for International Human Rights, Winnipeg, MB,
Canada
Dr. Audrey Ho - Staff Psychologist, BC Children’s Hospital, Vancouver, BC, Canada

Evergreen Framework
- 59 -
Dr. Jeanette Holden - Director of the Cytogenetics & DNA Research Lab and the Autism
Research Laboratory at Ongwanada Resource Centre; Department of Psychiatry and
Physiology, Queen’s University, Kingston, ON, Canada
Dr. Roy Holland - Clinical Director of the Maples Adolescent Treatment Centre, Burnaby, BC,
Canada
Dr. Wade Junek - Clinical and consulting psychiatrist, Child & Adolescent Mental Health
Program, IWK Health Centre; President, the Canadian Academy of Child and Adolescent
Psychiatry, Halifax, NS, Canada
Dr. Abel Ickowicz - Psychiatrist-in-Chief, Hospital for Sick Children, Toronto, ON, Canada
Dr. Umesh Jain - Head of the Adolescent ADHD Program and Director of the Children’s
Medication Clinic, the Centre for Addiction and Mental Health, Toronto, ON, Canada
Mr. Malcolm Johnson - Editor-in-Chief, SBC Surf Magazine, Toronto, ON, Canada
Ms. Shaleen Jones - Executive Director, Laing House, Halifax, NS, Canada
Dr. Llewellyn Joseph – Director, Disruptive Behaviours Program, South Lake Regional
Hospital, Newmarket, ON, Canada
Dr. Debra Katzman - Medical Director Eating Disorders Program, The Hospital for Sick
Children, Toronto, ON, Canada
Ms. Marianne Kobus-Matthews - Senior Health Promotion Consultant, Centre for Addiction
and Mental Health, Toronto, ON, Canada
Ms. Patricia Kyle - Manger, Mental Health & Addictions Services, Beaufort Delta Health and
Social Services Authority, Inuvik, NT, Canada
Mr. David Langtry - Deputy Chief Commissioner, Canadian Human Rights Commission
Ottawa, ON, Canada
Dr. Jeffery Landine - Director, Accessibility Services, University of New Brunswick.
Fredericton, NB, Canada
Mr. Harold Lipton - Manager, Healthy Minds/Healthy Children, Calgary, AB, Canada
Ms. Charlotte Lombardo - Coordinator Youth Voices/TeenNet, Department of Public Health
Sciences, University of Toronto, Toronto, ON, Canada
Dr. Jane Matheson – CEO, Wood’s Homes Children Services, Calgary, AB, Canada
Dr. Derrick MacFabe - Director, Kilee Patchell-Evans Centre for Autism, The University of
Western Ontario, London, ON, Canada
Mr. Robert MacNeil - Instructor, Ontario Police College Criminal Investigations Section;
President of The Committee of Youth Officers-Province of Ontario, Alymer, ON, Canada
Mr. Doug McCall - Executive Director, Canadian Association for School Health, Vancouver,
BC, Canada
Dr. Faye Mishna – Dean and Professor, Factor-Inwentash Faculty of Social Work, University of
Toronto, Toronto, ON, Canada
Mr. Gordon Matheson - President of the National Board of Directors of the Canadian Mental
Association, Stratford, PE, Canada
Dr. Patrick McGrath - Vice President of Research, IWK Health Centre; Professor of
Psychology, Pediatrics and Psychiatry, Dalhousie University, Halifax, NS, Canada
Ms. Susan Morris - Clinical Director of the Dual Diagnosis Program at the Centre for Addiction
and Mental Health, Toronto, ON, Canada
Dr. Marina Morrow - Associate Professor, Faculty of Health Sciences, Simon Fraser
University, Burnaby, BC, Canada
Evergreen Framework
- 60 -
Dr. David Mykota - Head of the Department of Educational Psychology and Special Education,
University of Saskatchewan, Saskatoon, SK, Canada
Ms. Winona Polson-Lahache - Policy Analyst, Mental Health & Addictions Assembly of First
Nations Health Secretariat, Ottawa, ON, Canada
Dr. Marjory Phillips - Clinical Director, Integra Foundation for Learning Disabilities, Toronto,
ON, Canada
Dr. Declan Quinn - Associate Professor, Faculty of Medicine, the University of Saskatchewan,
Saskatoon, SK, Canada
Dr. Rémi Quirion - Scientific Director of Research, Canadian Institute of Health Research;
Professor and Scientific Director at the Douglas Institute, McGill University, Montreal,
QC, Canada
Mr. Mark Rayter - Manager, Child and Youth Mental Health Services in Vancouver
Community, Vancouver, BC, Canada
Dr. Darcy Santor – Professor, School of Psychology, University of Ottawa, Ottawa, Canada
Ms. Alyse Schacter - Youth Mental Health Advocate, Ottawa, ON, Canada
Mr. Brent Seal - Youth Mental Health Advocate, Langley, BC, Canada
Ms. Sylvia Sikakane - Clinical Manager, Geneva Centre for Autism, Toronto, ON, Canada
Dr. Purnima Sundar - Research and Knowledge Exchange Consultant, The Provincial Centre
of Excellence for Child and Youth Mental Health at CHEO, Ottawa, ON, Canada
Dr. Sherry Stewart - Department of Psychiatry, Psychology, and Community Health, and
Epidemiology, Dalhousie University, Halifax, NS, Canada
Ms. Linda Smith - Executive Director, Mental Health, Children's Services and Addictions
Treatment, Government of Nova Scotia, Halifax, NS, Canada
Mr. Steven Solomon - Social Worker, Human Sexuality Program, Department of Social
Services, Toronto District School Board, Toronto, ON, Canada
Ms. Marg Synyshyn - Member, Child & Youth Advisory Committee, Mental Health
Commission of Canada; Program Director, Child and Adolescent Mental Health Program
Winnipeg Regional Health Authority, Winnipeg, MB, Canada
Dr. Rosemary Tannock - Canada Research Chair in Special Education; Senior Scientist, The
Hospital for Sick Children, Toronto, ON, Canada
Mr. Don Tapscott - Author, Growing Up Digital and Wikinomics, Toronto, Canada
Ms. Krista Thompson - Executive Director Covenant House, Vancouver, BC, Canada
Dr. Kate Tilleczek - Canada Research Chair in Youth Cultures and Transitions; Associate
Professor, Department of Sociology, University of Prince Edward Island, Charlottetown,
PE, Canada
Dr. Brenda Toner - Co-Head for the Social Equity & Health Research Unit, Centre for
Addictions and Mental Health; Professor and Head of the Women’s Mental Health
Program, and Director of Fellowship Program in the Department of Psychiatry,
University of Toronto, Toronto, ON, Canada
Prof. Paula Tognazzini - Senior Instructor, School of Nursing, University of British Columbia,
Vancouver, BC, Canada
Ms. Michelle Wong - Director, Evaluation and Strategic Directions, Monitoring, Research and
Evaluation, Representative for Children and Youth, Province of British Columbia,
Vancouver, BC, Canada
Dr. Michael Ungar – Professor, School of Social Work, Dalhousie University, Halifax, NS,
Canada
Evergreen Framework
- 61 -
Dr. Tracy Vaillancourt - Canada Research Chair in Children’s Mental Health and Violence
Prevention; Associate Professor, School of Psychology, University of Ottawa, Ottawa,
ON, Canada
Dr. Jeannette Waegemakers Schiff - Assistant Professor, Faculty of Social Work, University
of Calgary, Calgary, AB, Canada
Ms. Shelly Watkins – Project Coordinator, Inuit Tapiriit Kanatami, Ottawa, ON, Canada
Dr. Margaret Weiss – Clinical Professor, Department of Psychiatry, University of British
Columbia; Director of Research, Child Psychiatry Division of the University of British
Columbia, Vancouver, BC, Canada
Dr. Christopher Wilkes - Associate Professor, Faculties of Psychiatry and Pediatrics,
University of Calgary, Calgary, AB, Canada
Dr. David Wolfe- RBC Investments Chair in Children's Mental Health and Developmental
Psychopathology, Centre for Addiction & Mental Health, Toronto, ON, Canada
Youth Advisory Committee
Ms. Jessica Wishart – Chair, Evergreen’s Youth Advisory Committee, Halifax, NS, Canada
Ms. Faye Bronte - Member of the Youth Council for the CYAC for the MHCC, Halifax, NS,
Canada
Ms. Olivia Fischer – Member, Southern Alberta Child & Youth Health Network’s, Child &
Youth Advisory Council, Calgary, AB, Canada
Mr. Aaron Goodwin - Member of the Youth Council for the MHCC, Halifax, NS, Canada
Mr. Kyle Haddow – Member of the Youth Council for the MHCC, Calgary, AB, Canada
Mr. Joe Leger – Chair, Youth Council for the MHCC, Halifax, NS, Canada
Ms. Bronwyn Loucks – Member of the Youth Council for the MHCC, Kingston, ON, Canada
Ms. Alyse Schacter – Youth Mental Health Advocate, Ottawa, ON, Canada
Ms. Meredith Pritchard – Member, Southern Alberta Child & Youth Health Network’s, Child
& Youth Advisory Council, Calgary, AB, Canada
International Advisory Committee
Dr. Wendel Abel - Head for the Section of Psychiatry, Department of Community Health and
Psychiatry, Faculty of Medical Sciences, The University of the West Indies, Jamaica
Dr. Leah Andrews – Senior Lecturer in Clinical Psychological Medicine, School of Medicine,
The University of Auckland, New Zealand
Dr. Alan Apter - Schneiders Children’s Medical Center of Israel, Israel
Dr. Myron Belfer - Professor of Psychiatry, Department of Global Health and Social Medicine,
Harvard Medical School, USA
Dr. Gary Blau - Branch Chief, Child, Adolescent, Substance and Mental Health Services
Administration (SAMHSA), USA
Dr. David Brent – Departments of Psychiatry, Pediatrics and Epidemiology, The University of
Pittsburgh, USA
Dr. Barbara Burns - Director of Services, Effectiveness Research Program and Professor,
Department of Psychiatry and Behavioral Sciences, Duke University School of Medicine,
USA
Evergreen Framework
- 62 -
Dr. Ian Goodyer – Professor, Department of Child & Adolescent Psychiatry, University of
Cambridge, Great Britain
Dr. Tiffany Farchione – Assistant Professor, Department of Psychiatry, University of
Pittsburgh, USA
Dr. Joerg Fegert – Professor, Department of Child and Adolescent Psychiatry, University of
Ulm, Germany
Dr. Alan Flisher – Professor and Head of the Division of Child and Adolescent Psychiatry,
University of Cape Town, South Africa
Dr. Katherine Grimes – Assistant Professor, Department of Psychiatry, Harvard Medical
School, USA
Dr. Megan Gunnar – Professor, Institute of Child Development, University of Minnesota, USA
Dr. Joel Hetler - Director, The Centre for Excellence in Children’s Mental Health, University of
Minnesota, USA
Mrs. Devora Kestel – Regional Advisor, Pan American Health Organization, Barbados
Dr. Cristina Marques - National Mental Health Coordinating Board, Lisbon, Portugal
Dr. Andrés Martin – Professor, Department of Psychiatry, Yale University; Editor-in-Chief,
Journal of the American Academy of Child and Adolescent Psychiatry Center, USA
Dr. Patrick McGorry – Professor, Department of Psychiatry, University of Melbourne;
Executive Director, ORYGEN Research Centre, Australia
Dr. Merete Nordentoft – Professor, Department of Psychiatry, Copenhagen University,
Denmark
Dr. Helmut Remschmidt – Professor, Department of Child and Adolescent Psychiatry,
Philipps-University, Germany
Sir Michael Rutter – Professor, Institute of Psychiatry, Kings College, England, Great Britain
Dr. Luis Augusto Rohde – Associate Professor, Department of Psychiatry, Federal University
of Rio Grande du Sul, Brazil
Dr. Stephen Suomi - Chief of the Laboratory of Comparative Ethology, National Institute of
Child Health and Human Development, USA
Dr. Garry Walter – Professor, Department of Psychological Medicine, Northern Clinical
School at the University of Sydney, Australia
Ms. Deborah Wan - Chief Executive Officer, New Life Psychiatric Rehabilitation Association,
Hong Kong, China
Dr. Robert Wrate - Former Head of the Young Peoples’ Unit, in Edinburgh, Scotland, Great
Britain