estudio de fracasos tras cirugías endodonticas evaluados por diversos métodos. rud y andreasen
TRANSCRIPT

Int, J. oral Surg. 1972: I: 311-328
( K e y w o r d s : endodontics; surgery, endodontic; radiology; hi~'tology)
A study of failures after endodontic by radiographic, histologic and stereomicroscopic methods
surgery
JORGEN RUD AND J. O. ANDREASEN
Dental Department, University Hospital, and Department o] Oral Pathology, Royal Dental College, Copenhagen, Denmark
ABSTRACT - - To study the causes of failures after endodontic surgery, individual cases with unsuccessful healing were examined radiographi- tally, histologically and stereomicroscopically. It was found that most failures could be related to an insufficient debridement and canal ob- turation. Comparing the results of histologie and radiographic exam- inations of failures it was found that insufficient canal obturations showed up in only one-third of the intraoral radiographs. Another cause of failure was incomplete removal of the cyst lining. The root filling materials used (Rickert's root canal sealer, guttapercha and amalgam) were found to be non-irritant to the periapical tissues. Of 12 cases of failures after endodontic surgery which were re-operated and followed-up again one or two years post-operatively, half showed complete healing. That is almost the same rate of success as is found in initially operated cases. A number of complications were found, such as root fractures and advanced periodontitis, which had no con- nection with the surgical endodonfic procedures.
(Received for publication 26 September, accepted 25 November 1972)
A useful way to evaluate a method of ope- ration is to study the causes of failures. In a large material this may be done by a sta- tistical analysis of the influence of various factors upon healing. This was made in a previous study (Rud, Andreasen & Jensen 1972b), and it was found that the type of root filling, as well as the presence of ad- vanced marginal periodontitis, seem to be significantly associated with the occurrence of failures after endodontic surgery.
A more direct approach to the study of causes of failures is to examine the indi-
vidual cases of unsatisfactory healing. A few attempts at such examinations have been made after conservative endodontic therapy (Tschamer 1955, Keresztesi 1955, Ingle 1965, Seltzer, Bender, Smidt, Freed- man & Nazimov 1967), but in the literature very little information on cases of endo- dontic surgery could be found.
The purpose of the present study has therefore been, by a radiographic, histo- logic and stereomicroscopic approach, to attempt to identify the possible causes of failures after endodontic surgery.

312 RUD AND ANDREASEN
Table 1. Type of teeth in 69 failures after endodontic surgery
Mandible Maxilla
Type of teeth 1 2 3 4 5 6 1 2 3 4 5 6
No. of cases 16 15 2 7 6 1 8 7 2 4 0 1
Table 2. N u m b e r of years between operation and latest follow-up of 69 failures after endodontic surgery
Years l 2 3 4 5 6 7 8 9 10 11 12 13 14 15
No. of cases 7 3 5 10 10 6 13 4 3 2 3 1 0 1 1
M A T E R I A L A N D M E T H O D S
The material for the radiographic study con- sisted of the 69 cases of failures (28 uncer- tain with observation periods of four years or mote and 41 unsatisfactory) Found in the material of 1,000 cases of endodontic surgery described in two previous studies (Rud, An- dreasen ,& Jensen 1972 a,b).
The type of teeth of the 69 failures and the number of years between the operation and the latest follow-ups of these cases are shown in Tables i and 2, respectively. Five of the failures had been re-operated previously by other dental practitioners. Of the 69 failures, the root was resected in 58 cases, while in 11 cases only a periapical curettage had been per- formed. Thirty cases (44 %) had been retro- grade filled. Of the 69 failures, 23 were later re-operated by one of the authors (J. R.); 10 were extracted. The ultimate fate of the re- maining 36 cases was unknown. Of the 23 re- operated teeth, 12 were followed-up again one year or more after re-operation. The results achieved by re-operations are shown in Table 3.
The material /or the histologic study con- sisted of 42 cases with moderate or severe periapical inf lammation described in a previ- ous study (Andreasen & Rud 1972a).
All biopsies included the root end, periodon- tal structures and surrounding bone. Step- serial sections were cut along the axis of the tooth. An average of 197 sections was avail- able f rom each biopsy. Every tenth section was stained with hematoxylin-eosin and evaluated
for the presence of left necrotic pulp tissue in the root canal. Furthermore, the presence of apical ramifications or lateral canals was reg- istered. Tissue reactions to the root filling ma- terial were evaluated in 12 cases, where rem- nants of either Rickert's root canal sealer or silver amalgam were found in the connective tissue. In order to compare histologic and ra- diographic findings, the radiographs of all cases in this material were evaluated.
The material /or the stereomicroscopic study consisted of 31 extracted teeth unsuc- cessfully treated by endodontic surgery. These teeth derived either from the 69 failures de- scribed above, or from the Dental Department, University Hospital, Copenhagen.
Examination of the apices was performed with a Reichert stereomicroscope®, using ;< 25 power magnification.
Table 3. Mode of radiographic healing found after re-operation of 12 cases of failures after endodontic surgery
Healing group No. Percent
Complete 6 50
Incomplete 3 25
Uncertain 2 17
Unsatisfactory 1 8

FAILURES AFTER ENDODONTIC SURGERY 313
RESULTS
Radiographic findings
Table 4 shows the findings of the attempt
to determine a possible cause for the fail- ures by radiography.
In two cases, root fractures were suspect- ed because of corrosion of pins or posts. It was not possible in either case to observe a fracture directly, but a unilateral blurring
of the periodontal space (Fig. 1) and cor- rosion products from the pin (Fig. 2) sug-
gested a root fracture (Rud & Omnell
1970). Advanced marginal periodontitis was ob-
served in six cases. In some of these cases, the loss of bone extended to the apex. Com- parison with the marginal condition of the neighboring teeth revealed that periapical
inflammation had derived from the margi- nal periodontium (Fig. 3).
Mechanical per~orations of the root were
found in two cases, a maxillary lateral in- cisor with a curved root, and a mandibular first premolar. In both cases the root filling deviated from the main canal in the apical part of the root (Fig. 9).
Table 4. Radiographic findings of possible causes of failures in 69 cases with unsuccess- ful healing after endodontic surgery
No. of cases
Signs of root fracture 2
Advanced marginal periodontitis 6
Mechanical perforation of root 2
Insufficient root filling 8
Supernumerary root canals 7
Lateral canals 2
External resorption of root 5
In eight cases an insufficient guttapercha root filling was found, due to an insufficient technique (Fig. 4). I t proved impossible to determine radiographically whether a retro-
grade amalgam filling was insufficient, ex- cept in a case with severe root resorption.
Supermtmerary root canals were found
in six cases: one maxillary first premolar
with three root canals and one mandibular central and one mandibular lateral incisor,
Fig. 1. Root fracture suspected in a maxillary left second premolar because of localized bone destruc- tion mesially along the root. No direct signs of the fracture may be seen.

314 RUD A N D ANDREASEN
Fig. 2. Recurrence of perlapical inflammation due to root fracture. A, post-operative radiogra- phic condit ion of a maxil lary second left premolar. B, follow-up one year after the operation shows comple te bone repair. C, four years after the operation a recurrence of the periapical in- f lammation has occurred, caused by a root fracture.
Fig. 3. Progressive marginal periodontitis leading to recurrence of periapicat inflammation. A, pre-operative radiographic condition of a maxillary left first premolar. B, follow-up one year after the operation shows almost complete bone regeneration. C, condition four years after the operation shows a generalized marginal bone resorption.
Fig. 4. Failure of endodontic surgery of a max- illary left lateral incisor, probably due to an insufficient root filling.
two mand ibu la r premolars (Fig. 5) and one maxi l la ry lateral incisor, all with two root
canals. Supe rnumera ry canals were usual ly visible radiographical ly on ly when filled more o r less with root canal sealer.
Lateral canals were found radiographic- ally in two cases in maxi l la ry central inci- sors. Lateral canals could be seen on a
rad iograph only when they were filled with root canal sealer. Indirect ly , the presence
of lateral canals could be suspected by a
localized rarefact ion on the side of the root
(Fig. 6). External resorption of the root was found
in five cases, where the root fil l ing was seen
extending outside the root. F o u r of these
cases had a re t rograde root filling.

FAILURES AFTER ENDODONTIC SURGERY 315
Fig. 5. Supernumerary root canal in a mandibular left first premolar filled with root canal sealer only.
Histologic findings
The findings of the histologically examined cases are listed in Table 5. In 18 cases a defective canal obturation was found; be- tween the root filling and the canal walls, necrotic pulp tissue and debris from the
Fig. 6. Presence of a lateral canal is indicated by a localized widening of the periodontal mem- brane space mesially (arrow) on the root of a maxillary right central incisor. Note periapical rarefaction and partial obliteration of root canal.
mechanical canal preparation had accumu- lated (Figs. 7-8). In two of these cases, a mandibular lateral incisor with two root canals and a maxillary first premolar, mi- croscopy showed that a thin communication between the canals had not been filled by the retrograde amalgam filling.
In two cases an accidental root perfora- tion resulted in the main canal at the apex being left without root filling (Fig. 9). In one case an unfilled lateral canal was the probable cause of re-inflammation (Fig. 10). In three cases, cyst epithelium was diag- nosed histologically at the time of opera- tion, and again when the cases were re- operated because of unsuccessful healing 6, 4 and 2 years, respectively, after the ini- tial operations.
A filamentous material, similar to dental calculus, was found covering the root sur- face in two cases (Fig. 11). Deposits on the roots of a similar structure were also found when both cases were initially operated on for radicular cysts. At that time the de- posits were carefully removed.
In one case a spread of a marginal peri- odontitis appeared to be the cause of peri- apical inflammation (Fig. 12).

316 RUD A N D ANDREASEN
Table 5. Causes of fai lures after 42 cases of endodontic surgery found by histologic and radio- graphic methods
Histologic Radiographic examination examinat ion
Leak between root filling and canal walls 18 5
Root fi l l ing not extended to apex 2 1
Unfi l led lateral canal 1 0
Recurrence of cyst 3 0
"Calculus" deposited on root surface 2 1
Spread of marginal periodonti t is to apical area 1 0
No f indings 15 35
J
Fig. 7. Bacter ia in roo t canal and dentin tubules of a maxillary right lateral incisor, seven months af ter endodont ic surgery. A, surgical specimen. The apical foramen is filled partly with gutta- percha and part ly wi th root canal sealer (black outlined triangle). XI00. B, a leak is present be- tween the roo t canal, sealer and canal wall (arrow). X70. C, bacteria present in the root canal and dent in tubules (arrow). X195.

FAILURES AFTER ENDODONTIC SURGERY 317
A
B
Fig. 8. A maxillary left lateral incisor with periapical inflammation, probably due to necrotic tis- sue remnants in root canal. A, surgical specimen. X 10. B, necrotic remnants within root canal. X 195. C, Gram-stain of the same area reveals no bacteria in the tissue remnants (black area is root canal sealer). X195.
A comparison between the findings in the present series, using histologic and radiographic methods, may be seen in Table 5. Of 18 cases where incomplete obturatlon of the root was found histologically, only five could be demonstrated radiographic- ally. Of the two root perforations with only partial obturation of the main root canal found histologically, only one could be diagnosed by radiography. Other histologic findings in this series showed no radio- graphic signs.
The results of the histologic evaluation of tissue reactions to dislodged particles of silver amalgam and Rickert's root canal sealer are listed in Table 6. It appears from the figures that both materials are generally well accepted in the periapical tissue, and
that Rickert's root canaI sealer apparently causes the least reaction (Fig. 13).
Stereomicroscopic /indings
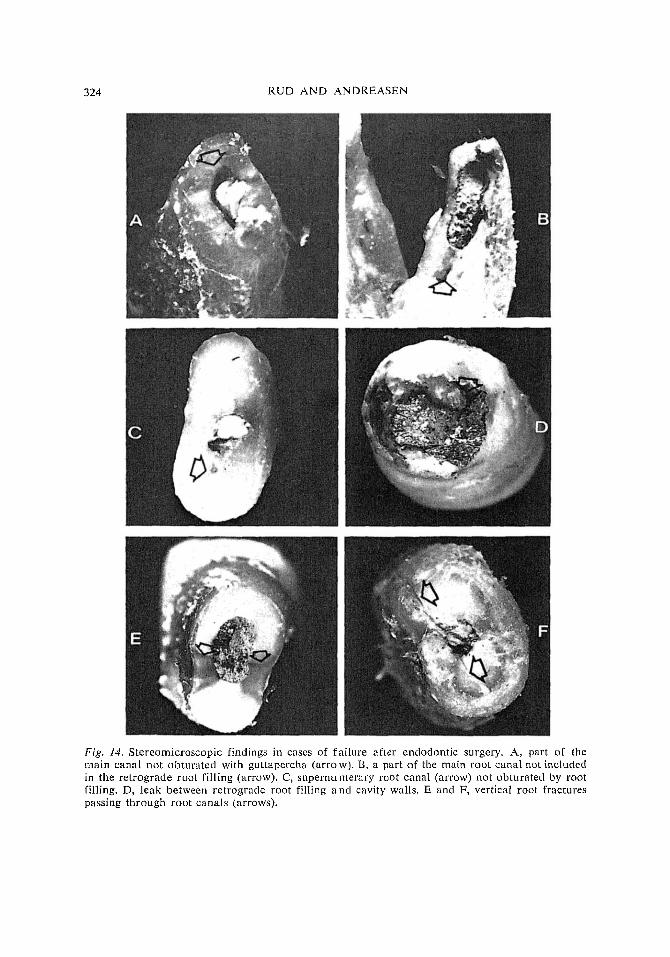
The results of the 31 cases where stereo- microscopic examinations were made are given in Table 7. It appears that insufficient canal instrumentation and obturation was the most frequent finding among unsuccess- ful orthograde fillings (Fig, 14A-C) . Fur- thermore, a leak often was found between root filling and canal walls in teeth treated by a retrograde technique (Fig. '14D). In one case, the retrograde filling was found to perforate through the lateral surface of the root. Only one case was found where an unfilled lateral canal terminated close to the apical area. Fractures in the root were

318 RUD A N D A N D R E A S E N
H :
, , ~ , ,
F ,¢
,2
G

FAILURES AFTER ENDODONTIC SURGERY 319
C
Fig. 10. Endodontic failure probably due to an unfilled lateral canal. A and B, condition im- mediately after the operation and 10 years later. C, low-power view of surgical specimen. Note lateral canal close to the apex. X t0 . D, minimal inf lammation in relat ion to the retrograde fill- ing. X70. E, lateral canal in direct communication with infected and necrotic pulp tissue in main canal. X170. F, bacteria present in necrotic tissue in main canal. X195.
Fig. 9. Endodontic failure probably due to a lateral perforation. A and B, condition immediately after the operation and three years later. C, low-power view of surgical specimen. Note tha t the mechanical preparation has caused a lateral perforation, whereas the apical part of the root ca- nal has remained, without any root filling. Xl0 . D, scar tissue. ×20. E, apical part of root canal filled with necrotic material. X20. F, higher magnification of E. X70. G, Gram stain of this area revealing clusters of bacteria. × 195. I-I, new cementum deposited on lateral root surface. XT0.

320 RUD AND ANDREASEN
Fig. 11. "Calculus" deposited on root surface of a maxillary lateral incisor after an infected radi- cular cyst was removed. A and B, condition immediately after the operation and l l years later. C, low-power view of surgical specimen. X 10. D, filamentous material deposited on root sur- face in close connection to squamous epithelium and a marked periapical inflammation. × 30. E, Gram stain reveals that the "calculus" consists of Gram-positive as well as Gram-negative bacteria, x 30.
found at the root ends in three cases (Fig. 14 E, F).
DISCUSSION
Following cases of endodontic surgery for a long time after the operation (in the pres- ent study up to 15 years), may reveal com- plications which have no connection with the surgical endodontic therapy as such. These secondary complications may be root fractures, advanced periodontitis with deep pocket formation, removal or dislodging of the root filling, or a mechanical perforation of the root for a post. These complications may occur at any time after the operation.
Vertical or oblique root fractures caused by corrosion of pins or posts (Angmar- Maansson, Omnell & Rud 1969) are found quite frequently. Thus, 468 cases were diag- nosed in a 15-year period in the same pri- vate practice from which the 1,641 cases of endodontic surgery derived during a nine- year period (Rud et al. 1972a). The diagno- sis oC root fracture caused by corrosion may be difficult, as a fracture is discernible in a radiograph in only 36% of the cases. When a fracture is not to be seen, the diagnosis can be made on the presence of corrosion products or can be suspected when a wide- ning o~ the periodontM space is found (Fig. 1) (Rud & Omnell 1970). If only the last-

FAII .URES AFTER ENDODONTIC SURGERY 321
A
Fig. 12. Periapical inflammation of maxillary right cuspid possibly caused by spread of a mar- ginal periodontitis. A, low-power view of surgical specimen shows dental calculus on left side of the root (arrows). X10. B, periapical inflammation and root resorption. X 30. C, section of per- ipheral part of root apex reveals dental calculus and bacteria (arrow) close to root filling. X70.
ment ioned sign is present, an expIorat ive
operat ion should be m a d e to ver i fy the diagnosis. I f a root f rac ture is no t discov- ered and the tooth is treated with endodont- ic surgery, this would inevitably result in a
failure. As the f requency of root f rac tures
is so high, at least in Denmark , fa i lure to
recognize this condi t ion before or at the t ime of surgery will result in a high fa i lu re rate. In the study (Rud et al. 1972a,b), a
Table 6. Tissue reactions in the periodontal soft tissue to dislodged root-filling material
Rickert's root Silver amalgam canal sealer
Collagenous fibers in direct relation + 4 6 to root filling material -- 0 2
Histiocytes adjacent to q- 3 2 root filling material -- 1 6
+ 0 2 Lymphocytes and plasma cells adjacent to root filling material -- 4 6

322 RUD AND ANDREASEN
Fig. 13. Tissue reaction to Rickert's root canal sealer and silver amalgam. A, root canal sealer surrounded by dense collagenous tissue without foreign body reaction. X70. B, slight histiocytic reaction adjacent to root canal sealer (arrow). X70. C, amalgam surrounded by dense collagenous tissue without foreign body reaction. >(70. D, amalgam partly embedded in hone without in- flammatory reactions. X70. E, amalgam surrounded by lymphocytes, histiocytes, and giant cells (arrow). XT0. F, amalgam surrounded by lymphocytes. XT0.
large n u m b e r of the roots in patients re- ferred for endodoatic surgery were found to be fractured. The majori ty of these were diagnosed before the operation and extract- ed. Eight cases o[ root fracture were diag- nosed during endodontic surgery, and seven
cases were found during follow-up. These cases were excluded from the material and replaced by other cases. In two of the un- satisfactory cases in the present study of failures, indirect signs of root fractures were present radiographically (Figs. 1-2),

FAILURES AFTER ENDODONTIC SURGERY 323
Table 7, Stereomicroscopic findings in 31 teeth treated unsuccessfully by surgical endodontics
Orthograde fillings Retrograde with guttapercha
fillings with and Rickert's root silver amalgam canal sealer*
A separate root canal left unfilled 3 1
Main canal not filled to apical foramen 5
Leak between root filling and canal walls 6 2
Lateral perforation of retrograde root fillings 1
Lateral canal not obliterated by root filling material 1
Fracture lines extending from the root filling 2 l
No observable cause 9 3
* Ten of these teeth were root-resected
but as no definite diagnosis of root fracture could be made radiographically, these cases were not excluded from the material. Ster- eomicroscopic examination revealed three cases of fracture in the root.
Advanced periodontitis with deep pocket formation was found in a previous study to be significantly associated with periapical inflammation (Rud et al. 1972b). The mech- anism for this relation appeared in this study to be a direct spread of marginal in- flammation to the apical area. Thus, the endodontic surgical treatment cannot be blamed for the unsuccessful results in these cases.
Among the causes of failures which may be attributed to the endodontic surgical operation as such, inferior technique or in- sufficient technique due to anomalies of the root can also be included.
The findings made in this study seem to indicate that an insufficient cleansing and filling of the root canal is the most com- mon cause of periapical re-inflammation. The same factors were claimed to be re-
sponsible for 59% of the failures recorded after conservative endodontic therapy (Ingle 1961, 1965).
The frequent insufficiency in removal of all necrotic pulp tissue during the mechan- ical preparation of the root canal has been demonstrated in several studies (Ullik 1929, Hagman 1948, Waechter 1955, Biichs & Reul 1962). An irregular shape of the root canal is usuaily responsible for a deficiency in cleans- ing and mechanical preparation, resulting in a leak between the root filling material and the canal walls. This leak may harbor necrotic pulp tissue with or without bacteria. In a previous study it was found that tis- sue remnants were seen frequently when severe periapical inflammation was present but not at all in the cases without inflam- mation (Andreasen & Rud 1972b). The in- flammatory potentials of cellular debris, whether sterile or infected, have been shown in an experimental study by Torneck (1967). Furthermore, it has been found that a peri- apical rarefaction may occur among teeth with pulp necrosis, even when bacteria cul-
324 RUD AND ANDREASEN
Fig. 14. Stereomicroscopic findings in cases of fa i lure after endodontic surgery. A, part of the main canal not obturated with guttapereha (afro w). B, a part of the main root canal not included in the re t rograde root filling (arrow). C, supernumerary root canal (arrow) not obturated by root filling. D, leak between re t rograde root filling a n d cavity wails. E and F, vertical root fractures passing through root canals (arrows).

FAILURES AFTER ENDODONTIC SURGERY 325
tures gave negative results (Sommer 1954, Chirnside 1957). These findings, together with the results found in this study, support the assumption that products of tissue de- composition following pulp necrosis may cause a periapical inflammation (Chirnside 1957, Shovelton & Sidaway 1964).
A recent study by Harty, Parkins & Wen- graf (1970) has revealed that insufficiently condensed root fillings were significantly associated with failure after conservative endodontic therapy. Experiments on ex- tracted teeth have shown penetration of a radioactive solution from outside into the root canal along an insufficient root filling (Dow & Ingle 1955). I t has been supposed that tissue fluid in the same way may in- vade the leak between the root filling and the canal wall and act as a culture medium for bacteria (Rickert & Dixon 1931). How- ever, the value of this assumption has re- cently been questioned based on "hollow tube" experiments in animals (Goldman & Pearson 1965, Torneck 1967).
I t may therefore be concluded that the role of an insufficient root filling in peri- apical inflammation apparently is due first of all to the presence of necrotic tissue remnants, infected or not, in the leak be- between the root filling and the canal walls.
In extracted teeth an insufficient root filling may be detected radiographically, using both a vestibulo-lingual and a mesio- distal projection (Ingle 1956, Heilscher 1956). Unfortunately, the findings in the present study showed that with the teeth in situ, using a vestibulo-lingual projection, only one-third of the histologically insuffi- cient root fillings were detected.
In the present study, one case of an in- sufficient root filling was observed histo- logically to be due to an accidental perfo- ration of the canal wali because of an apical curvature. In two other failure cases, acci- dental perforations were diagnosed by radio- graphy. Such cases have also been reported
by other investigators (Luebke, Glick & Ingle 1964, Ingle 1965). If the perforations were in the apical part of the root, failures could have been avoided if a proper api- ectomy had been carried out.
Lateral canals apparently were the cause of failures in a number of cases. While these canals often were filled with root canal sealer when orthograde root filling with guttapercha was made using high pressure condensation, the lateral canals in cases with retrograde root filling were found to be the leaks through which infected mate- rial could escape from the unfilled root canal to the periodontal structures (Fig. 10).
Aberrant main canals, like lateral canals, were sometimes found to be filled with root canal sealer. However, as these canals were not always cleansed, the obturation with the sealer was apparently not always sufficient and failures occurred in seven cases.
Apical ramifications of the root canal are frequently found in the permanent dentition (Meyer & Scheele 1955, Meyer 1960, Selt- zer, Soltanoff, Bender & Ziontz 1966, Ai- namo & Erie 1968). It has been supposed that they may constitute an important cause of endodontic failures. However, previous studies as well as the present one have shown that this apparently is not true (Ingle 1965, Seltzer et al. 1967). These ramifications may well contain vital pulp tissue nourished from the periodontal membrane, or they may be obturated by root canal sealer. On the other hand, if they should contain ne- crotic tissue, this would be in a l imited quantity and would cause only a small in- f lammatory response by the periapical tis- sue, which may be difficult to observe on a radiograph.
External resorption of the root occurred in 60 of the 1,000 cases of endodontic sur- gery described in two previous studies (Rud et al. 1972a,b). Of these, five cases were failures, four of which occurred in teeth with retrograde root fillings. In these cases

326 RUD AND ANDREASEN
resorption had apparently extended to such a degree that a communication was estab- lished to the infected unfilled root canal. In this context it is interesting that external root resorption in one case apparently was the cause of an ultimate complete healing. In this case a periapical rarefaction had been present for a ~ery long time after the operation. At the final follow-up, it was noted that the guttapercha point extended outside the root, but otherwise a normal periodontal space was found. It may be that a small leak containing necrotic tissue had existed between the root filling and the canal wall and prevented normal bone re- generation. After resorption of the root, the insufficiently filled part of the apex had disappeared, and because the root filling in the lower parts of the root canal was tight, normal healing ensued.
An important question may be raised: is the root filling material directly responsible for inflammatory changes in the periodon- tium? The findings in the present study do not support this view and a review of the literature gives the same resutt. Thus, Ric- kert's root canal sealer used in this study has repeatedly been found to inflict no or a very mild response in the connective tissue in implantation experiments in animals (Dixon & Rickert 1933, Hunter 1957, Ste- wart 1958, Guttoso 1963, Rappaport, Lilly & Kapsimalis 1964, Curson & Kirk 1968). The same conclusion can be drawn from studies dealing with tissue tolerance to- wards silver amalgam (Rickert & Dixon 1931, Pilz 1956, Mitchell 1959, Nagai & Imazeki 1960, Feldmann & Nyborg 1962, Kellner & Keresztesi 1965, Lyon, Water- strat & Paffenbarger 1966, Sperber 1966, Friend & Browne 1968, Friend 1969, Spaangberg 1.969) and guttapercha (Rickert & Dixon 3931, Boulger 1933, Bernhardt & Eulig 1953, Hunter 1957, Mitchell 1959, Feldmann & Nyborg 1962, Spaangberg 1968, 1969).
Another problem which shouId be con- sidered: do changes occur in the root filling material when placed in the tissues.'? In several in vitro studies it has been shown that amalgam has excellent sealing proper- ties when used as a retro-filling (Nyberg 1958, Herd 1968). However, the question may be raised as to whether later dimen- sional changes or corrosion may invalidate the adaptation between the amalgam and the canal walls. The findings of the stereo- microscopic examination in this and other studies (Driak 1952), as well as implant ex- periments (Nagai & Imazeki 1960), seem to indicate that such changes may actually occur. A proper filling technique is there- fore essential.
In three cases in which a cyst was diag- nosed at the time of operation, a later biop- sy showed recurrence of the cyst. Apparent- ly some cyst epithelium had been left du- ring the initial operation. This emphazises the importance of a careful removal of all cyst lining.
It was interesting to note how long a time the patients retained teeth unsuccessfully treated with surgical endodontic procedures. When the 69 failures were radiographically followed-up for the last time, more than three-fourths were from three to 15 years old. Several patients refused re-operation or extraction, preferring to keep the clinically symptomless teeth.
The results found after re-operation of 12 failures after endodontic surgery showed complete healing in half of the cases. As 60% of the re-operated cases with follow- up had had a retrograde root filling, and as the follow-up periods were for only one or two years, the results obtained after re- operation do not differ much from the re- sults of the main material This shows that re-operation of failures after endodontic surgery may be attempted, with a reason- able hope of success.

FAILURES AFTER ENDODONTIC SURGERY 327
Acknowledgments - This study has been sup- ported by a grant from the Danish Dental As- sociation ("Fonden til st6tte for videnskabelige og praktiske unders~gelser inden for tandlaege- kunsten") Dentalaktieselskabet af 1934's Fond, and the Danish State Research Foundation.
R E F E R E N C E S
AINAMO, J. ,& L~SE, H.: A stereomicroscopic in- vestigation of the anatomy of the root apices of 910 maxillary and mandibular teeth. Odont. T. 1968: 76: 419-426.
ANDREASEN, J. O. ~, ROD, J.: Modes of heal- ing histologically after endodontic surgery in 70 cases. Int. Y. oral Surg. 1972a: 1: 148-160.
ANDREASEN, J. O. ,& RUD, J.: A histobacteri- ological study of dental and periapical struc- tures after endodontic surgery. 1at. J. oral Surg. 1972b: 1: 272-281.
ANGMAR-MAANSSON, B., OMNELL, K.-AA. & ROD, I.: Root fractures due to corrosion. 1. Metallurgical aspects. Odont. Revy 1969: 20: 245-266.
BERNHARDT, H. & EULm, H.-G.: Die Reaktion des Knochengewebes auf die MarkhShle bei Meerschweinchen implantierte Guttapercha. Dtsch. Zahniirztebl. 1953: 7: 295-297.
BOULGER, E. P.: The foreign body reaction of rat tissue and human tissue to guttapercha. J. Amer. dent. Ass. 1933: 20: 1473-1481.
BOCHS, I-I. & REUL, L : Zur Frage der Kno- chenregeneration nach Wurzelspitzenresek- tion mit retrograder Abffillung. Dtsch. zahn- i'h'ztl. Z. 1962: 17: 1635-1644.
Crllm,~SlDE, I. M.: A bacteriological and hist- ological study of traumatized teeth. N. Z. dent. J. 1957: 53: 176-191.
Cr.rRSON, I. & KIRK, E. E. J.: An assessment of root canal-sealing cements. Oral Sttrg. 1968: 26: 229-236.
DIxor~, C. M. & RICKERT, U. G.: Tissue tol- erance to foreign materials. J. Amer. dent Ass. 1933: 20: 1458-1472.
D o w , P. R. & INGLE, J. I.: Isotope determi- nation of root canal failure. Oral Sttrg. 1955: 8: 1100-1104.
DlUAK, F.: Vergleich einer normalen und rctro- graden Zahnwurzelfii1iung an Schliffpriipa- raten. Mikroskopie 1952: 7: 354-358.
FIgLDMANN, G. & NYBORG H,: Tissue reactions to root filling materials. I. Comparison be- tween gutta percha and silver amalgam im- planted in rabbit. Odont. Revy 1962: 13: 1-14.
FELDMANN, G. 8.c NYBORG, I'{.I Tissue reactions to root filling materials. II. A comparison o f implants of silver and root filling material A H 26 in rabbits' jaws. Odont, Revy 1964: 15: 33-40.
FRIEND, L. A.: Tissue reactions to some root filling materials in the bone of rabbits. Arch. oral Biol. 1969: 14: 629-638.
FRmND, L. A. & BROWNE, R. M.: Tissue reac- tions to some root filling materials. Brit. dent. J. 1968: 125: 291-297.
GOLI~MAN, M. & PEARSON, A. H.: A prelimi- nary investigation of the "hollow tube" theory in endodontics: studies with neo-tetra- zolium. J. oral Ther. & Phavm. 1965: 1: 618- 626.
Gu'rruso, J.: Histopathologic study of rat con- nective tissue responses to endodontie mate- rials. Oral Sm'g. 1963: 16: 713-727.
HAO~ANN, H.: l~Iber die I-Iistologie des aufbe- reiteten, iufizierten Wurzelkanalen. Schweiz. Mschr. Zahnheilk. 1948: 58: 4-16.
HARTY, F. J., PA~dNS, B. L & W~NOaAF, A. M.: Success rate in root canal therapy. A retrospective study of conventional cases. Brit. dent. J. 1970: 128: 65-70.
HERD, I. R.: Apicoectomy! - Why7 Aust. dent. J. 1968: 13: 57-64.
HEILSCHER, W.: Eine kritische Betrachtung zur Interpretation der rarefizierenden circum- apikalen Prozesse. Dtsch. zahniirztl. Z. 1956: 11: 1354-1370.
HUNTER, H. A.: The effect of gutta percha, sil- ver points, and Rickert 's root sealer on bone healing. J. Camtd. dent. Ass. 1957: 23: 385- 388.
INGLE, J. I.: Root canal obturatioa. J. Amer . dent. Ass'. 1956: 53: 47-55.
INOLE, J. L: A standardized endodontic tech- nique utilizing newly designed instruments and filling materials. Oral Surg. 1961: 14: 83-91.
INOLE, I. I. Endodontics. Lea & Febiger, Phi- ladelphia 1965; p. 54-77.
KELLNF.R, G. & KBI~ESZ'nZSI, K.: Die Wirkung metalliseher Wurzelftillmaterialien auf Zell- kulturen. Dtsch. zahniirztl. Z. 2965: 20: 978- 988.
KERESZ-rESI, K.: Ergebnisse klinischer und r~Snt- genologischer Nachuntersuchungen yon Wur- zelspitzenresektionen. Ost. Z. Stomat. 1955: 52: 429-435.
LUEBKE, R. G., GLJCK, D. H. & INGLE, J. I.: Indications and contraindieations for endo- dontic surgery. Oral Surg. 1964: 18: 97-113,

328 RUD AND ANDREASEN
LYON, H. W., WA.TERSTRAT, R. M. & PAFFEN- BARGER, G . C.: Soft tissue response to im- plants o~ gallium alloys and silver amalgam alloys. J. Amer. dent. Ass. 1966: 72: 659- 664.
MEYER, W.: Die anatomischen Grundlagen der Wurzelbehandlung. Dtsch. zahni~rztL Z. 1960: 15: 777-786.
MEYER, W. & SCnEELE, E.: Die Anatomic der Wurzelkan~le der oberen Frontzilhne. Dtsch. zahniirztl. Z. 1955: 10: 1041-1045.
MITCHELL, F.: The irritational qualities of den- tal materials, d. Amer. dent. Ass. 1959: 59: 955-966.
]NAGM, K. & IMAZEKI, T.: Correlational study be- tween metallographical findings of metals and their tissue reactions in vital body. J. Nihon Univ. Sch. Dent. 1960: 2: 66-74.
Nennao, M.: Retrograd rotfyllning. Fordringar p~, materialets anslutningst~thet och sterilitet. Svensk Tandl~iL-T. 1958: 51: 537-548.
Pmz, W.: Histologische Studien fiber die dutch Fremdk~Srper beeinflusste periapikale Wund- heilung nach operativer Wurzelbehandlung. Dtsch. zahn~irztl. Z. 1956: 11: 1175-1186.
RAPPAPORT, I-I. M., LILLY, G. E. & KAPSIMALIS, P.: Toxity of endodontic filling materials. Oral Surg. 1964: 18: 785-801.
RICKERT, U. G. & DIXON, C. M.: The control- ling of root surgery. 80 Congr6ss Dentaire International 1931, p. 15-22.
RUD, J., ANDREASEN, J'. O. & JENSEN, J. E. M.: A follow-up study of 1000 cases treated by endodontie surgery. Int. J. oral Stlrg. 1972a: 1: 215-228.
ROD, J., ANDRF_,ASEN, J. O. & JENSEN, J. E. M.: A multivariate analysis of the influence of various factors upon healing after endodon- tic surgery, lnt. J. oral Surg. 1972b: 1: 258- 271.
RUb, J. ~,: OMNELL, K.-AA.: Root fractures due to corrosion. Diagnostic aspects. Scand. J. dent. Res. 1970: 78: 397-403.
SELTZER, S., BENDER, 1. B., SMITH, J., FREED- MAN, I. & NAZIMOV, H.: Endodontic failures - An analysis based on clinical, roentgen- ographic, and histologic findings. Oral Surg. 1967: 23: 500-530.
SELTZER, S., SOLTANOFF, W., BENDER, I. B. & ZIO~TZ, M.: Biologic aspects of endodontics. I. Histologic observations of the anatomy and morphology of root apices and sur- rounding structures. Oral Surg. 1966: 22: 375-385.
SHOVELTON, D. S. & SIDAWA¥, D. A.: Infec- tion in root canals. Brit. dent. J. 1964: 108: 115-118.
SOMMgR, R. F.: Clinical evaluation of diagno- stic aids, Dent. Radiography and Photo- graphy 1954: 27: 17-23, 31-36.
SPERBER, G . H.: Biological reactions to experi- mental dental amalgams. J. dent. Res. 1966: 45: 99-105.
SPAANGIIERG, L,: Comparison between tissue reactions to guttapercha and polytetrafluor- ethylene implanted in the mandible of the rat. Svensk Tandliik.-T. 1968: 61: 705-714.
SPAANGBERG, L.: Biological effects of root canal filling materials. 7. Reaction of bony tissue to implanted root canal filling materials in guinea pigs. Odont. T. 1969: 77: 501-527.
STEWART, (~. G.: A comparative study of three root canal sealing agents. Oral Stlrg. 1958: 11: 1029-1041, 1074-1078.
TORNECK, C. I3.: Reaction of rat connective tissue to polyethylene tube implants. Oral Surg. 1957: 24: 674-683.
TSCHArvmR, /ft.: Das Ergebnis der Nachkontrolle yon 160 Wurzelspitzenamputationen. Zahn- &'ztl. Rdsch. 1955: 64: 432-436.
ULLm, R.: Die histologische Kontrolle yon ver- schiedenen Methoden der Wurzelkanalreini- gung. Z. Stomat. 1929: 27: 1037-1051.
WAECHTER, R.: I-tistologische Untersuchungen zur Aufbereitung des infizierten Wurzelka- nals. Zahtl&'ztl. Welt. 1955: 10: 20-22.
Addresses: Y. Andreasen 4 Universitetsparken DK-2IO0 Copelthagen 0 Denmark
J. Rud Nikola] Plads DK-1067 CopeJzhagen K Denmark