ensuring a safe outcome with vacuum delivery nnepqin fall meeting november 14,2009 jerome...
TRANSCRIPT
Ensuring a Safe Ensuring a Safe Outcome With Outcome With
Vacuum DeliveryVacuum DeliveryNNEPQINNNEPQIN
Fall MeetingFall Meeting
November 14,2009November 14,2009
Jerome Schlachter, MD

No disclosures to No disclosures to reportreport

AcknowledgementAcknowledgement
Perinatal CommunityPerinatal CommunityVacuum Delivery BundleVacuum Delivery Bundle
Peter Cherouny, M.D.Peter Cherouny, M.D.
Division of Maternal-Fetal MedicineDivision of Maternal-Fetal Medicine
Department of Obstetrics and GynecologyDepartment of Obstetrics and Gynecology
University of Vermont College of MedicineUniversity of Vermont College of Medicine
Quality Care in ObstetricsPreventing Trauma with Vacuum Delivery
ObjectivesObjectives
1.1. Describe specific risks associated Describe specific risks associated with vacuum delivery.with vacuum delivery.
2.2. Describe technical considerations for Describe technical considerations for employing a vacuum device.employing a vacuum device.
3.3. Explain rationale for developing a Explain rationale for developing a clinical bundle of care elements for clinical bundle of care elements for vacuum delivery.vacuum delivery.
4.4. List 5 vacuum delivery bundle List 5 vacuum delivery bundle elements.elements.

Clinical Case Review: 20 y.o. G1 P0 at Clinical Case Review: 20 y.o. G1 P0 at 40 weeks presents in labor dilated 5-6 40 weeks presents in labor dilated 5-6
cm.cm.

Rapid progress to full dilatation, Rapid progress to full dilatation, pushing begins. Meconium is noted.pushing begins. Meconium is noted.

With concern about the fetal status, With concern about the fetal status, provider #1 applies a vacuum.provider #1 applies a vacuum.

Minimal descent occurs and provider Minimal descent occurs and provider #2 is called. With pulls over two #2 is called. With pulls over two
contractions there is descent to +1.contractions there is descent to +1.

The patient pushed for 10 minutes, bringing the The patient pushed for 10 minutes, bringing the vertex to +2 station. The vacuum was employed vertex to +2 station. The vacuum was employed
again over two contractions. The caput was again over two contractions. The caput was starting to crown. The position was noted to be OP.starting to crown. The position was noted to be OP.

Forceps were placed and delivery was Forceps were placed and delivery was accomplished with the first pull. A accomplished with the first pull. A
shoulder dystocia was encountered, shoulder dystocia was encountered, relieved easily with McRobert’s relieved easily with McRobert’s
position and gentle traction.position and gentle traction.
A live infant was delivered.Weight = 2940 grams
APGAR scores = 2, 6 and 8.
Arterial Cord pH = 7.07, BE = -14.1
A large 4th degree laceration was repaired.

The Whole StoryThe Whole StoryThe newborn spent 17 days in the NICU with The newborn spent 17 days in the NICU with
cephalohematoma, small subdural hematoma, cephalohematoma, small subdural hematoma, meconium aspiration, anemia, jaundice, r/o meconium aspiration, anemia, jaundice, r/o
sepsis, TPN. At 8 mo. there is residual sepsis, TPN. At 8 mo. there is residual calcification of the cephalohematoma, but calcification of the cephalohematoma, but
normal growth and development.normal growth and development.
The mother considers the delivery a traumatic experience and questions why a cesarean was not performed earlier.
She is requesting sterilization.
Elliot Hospital FY Elliot Hospital FY 20082008
32 babies were discharged 32 babies were discharged with a diagnosis of with a diagnosis of
““Birth trauma, injury to the Birth trauma, injury to the scalp”.scalp”.

Elliot Hospital FY Elliot Hospital FY 20082008
109 Vacuum Deliveries 109 Vacuum Deliveries (4.7%)(4.7%)
5* Forceps Deliveries5* Forceps Deliveries
*3 of 5 followed use of vacuum*3 of 5 followed use of vacuum

Incidence of Operative Vaginal Incidence of Operative Vaginal Birth in U.S., 1989-1997Birth in U.S., 1989-1997

Vacuum Extraction: Vacuum Extraction: IndicationsIndications
Standard IndicationsStandard Indications Prolonged 2Prolonged 2ndnd stage of labor stage of labor Fetal compromise, non-reassuring fetal statusFetal compromise, non-reassuring fetal status Shortening of 2Shortening of 2ndnd stage for maternal benefit stage for maternal benefit
Nonstandard indicationsNonstandard indications Umbilical cord prolapseUmbilical cord prolapse Fetal compromise in multip, near fully dilatedFetal compromise in multip, near fully dilated Suspected borderline CPDSuspected borderline CPD Delivery of second twin above 0 stationDelivery of second twin above 0 station
Miksovski,OBGYN Surv. 2001
Vacuum Extraction: Vacuum Extraction: PrerequisitesPrerequisites
Cephalic presentationCephalic presentation Full cervical dilatationFull cervical dilatation Engaged fetal head (at or below 0 station)Engaged fetal head (at or below 0 station) Ruptured membranesRuptured membranes Experienced operator presentExperienced operator present Operator certain about the position of fetal Operator certain about the position of fetal
headhead Capability to perform emergency cesarean Capability to perform emergency cesarean
deliverydelivery Miksovski,OBGYN Surv. 2001
Vacuum Extraction: Vacuum Extraction: ContraindicationsContraindications
Premature fetus (GA < 34-36 weeks)Premature fetus (GA < 34-36 weeks) Fetus with bone demineralization condition Fetus with bone demineralization condition
(e.g. osteogenesis imperfecta)(e.g. osteogenesis imperfecta) Fetal hemorrhagic diathesisFetal hemorrhagic diathesis Face presentationFace presentation Cephalopelvic disproportionCephalopelvic disproportion Position of fetal head unknown (ACOG)Position of fetal head unknown (ACOG)
Miksovski,OBGYN Surv. 2001

Procedures That Procedures That Hasten DeliveryHasten Delivery
AmniotomyAmniotomy
VacuumVacuum

Quality Care in Obstetrics Quality Care in Obstetrics Birth Trauma related to Vacuum Birth Trauma related to Vacuum
DeliveryDelivery
What we causeWhat we cause– Scalp lacerationScalp laceration– Retinal hemorrhageRetinal hemorrhage– CephalohematomaCephalohematoma– Subgaleal hemorrhageSubgaleal hemorrhage– Intracranial hemorrhageIntracranial hemorrhage– HyperbilirubinemiaHyperbilirubinemia– Maternal traumaMaternal trauma
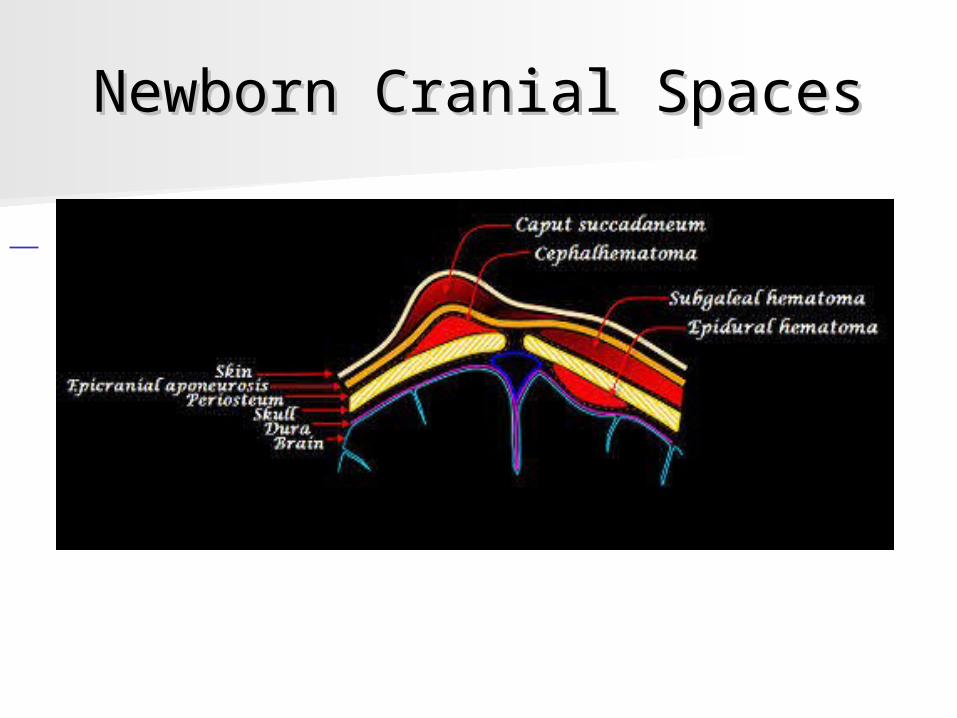
Newborn Cranial SpacesNewborn Cranial Spaces
Extracranial InjuriesExtracranial Injuries
Scalp bruisingScalp bruising 16%16% Usually resolve without sequellaeUsually resolve without sequellae
ChignonChignon highhigh Usually resolve without sequellaeUsually resolve without sequellae
CephalohematomaCephalohematoma 6-10%6-10% Usually resolve without sequellaeUsually resolve without sequellae
Subgaleal hemorrhageSubgaleal hemorrhage<1%<1%
Shock, DIC, organ failure, death in 25%Shock, DIC, organ failure, death in 25%Doumouchtsis, Clin.Perinat. 2008

Cephalhematoma vs. Subgaleal Cephalhematoma vs. Subgaleal HematomaHematoma

Cephalhematoma and Subdural Cephalhematoma and Subdural HematomaHematoma
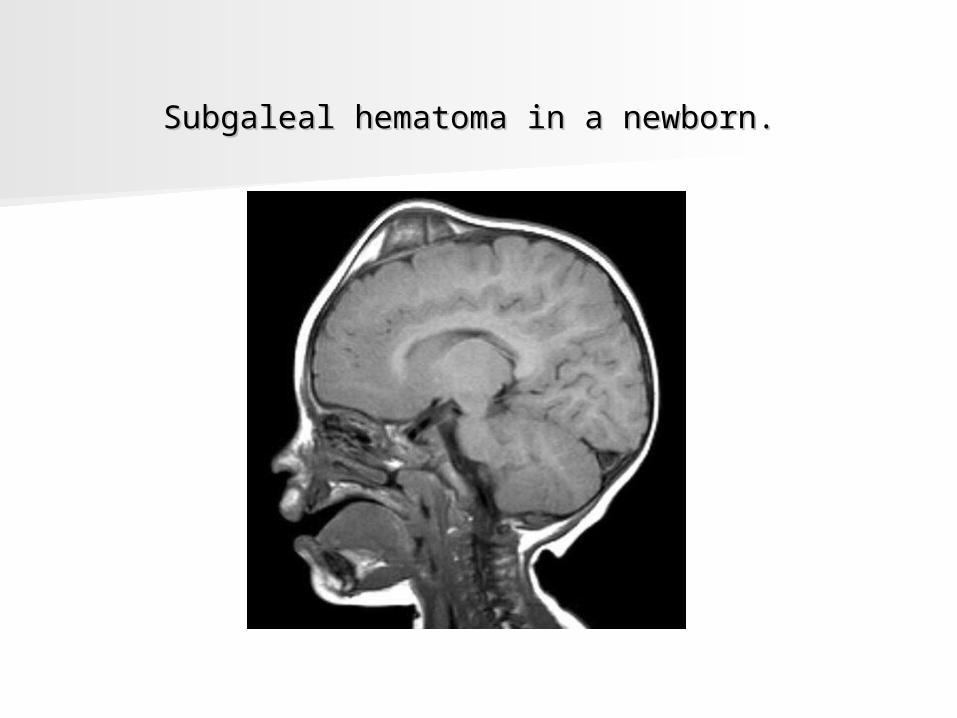
Subgaleal hematoma in a newborn. Subgaleal hematoma in a newborn.
Cranial InjuriesCranial InjuriesFracturesFractures
Linear skull fracturesLinear skull fractures 0.5% incidence estimated0.5% incidence estimated 5% incidence on screening x-ray5% incidence on screening x-ray Usually resolve without sequellaeUsually resolve without sequellae
Depressed skull fracturesDepressed skull fractures Rare with vacuum Rare with vacuum More common with forcepsMore common with forceps Associated with IC hemorrhage and Associated with IC hemorrhage and
neurologic complicationsneurologic complicationsDoumouchtsis, Clin.Perinat. 2008
Intracranial InjuriesIntracranial InjuriesIntracranial HemorrhageIntracranial Hemorrhage
Estimated incidence at term 0.11% - 0.34%. Estimated incidence at term 0.11% - 0.34%. Incidence with screening ultrasound after Incidence with screening ultrasound after
vacuum 0.87%.vacuum 0.87%. Similar incidence with cesarean alone.Similar incidence with cesarean alone. Associated with birth asphyxia, prematurity, Associated with birth asphyxia, prematurity,
infection, vascular abnormalities, infection, vascular abnormalities, hemorrhagic diathesis.hemorrhagic diathesis.
If VD, location is usually subdural or If VD, location is usually subdural or subarachnoid.subarachnoid.
Doumouchtsis, Clin.Perinat. 2008
Quality Care in ObstetricsQuality Care in Obstetrics Birth Trauma related to Vacuum Birth Trauma related to Vacuum
DeliveryDeliveryACOG ConclusionsACOG Conclusions
– ““Serious complication of vacuum device in Serious complication of vacuum device in approximately 5% of vacuum attempts.”approximately 5% of vacuum attempts.”
– ““Given the maternal and fetal risks Given the maternal and fetal risks associated with operative vaginal delivery, associated with operative vaginal delivery, it is important that the patient be made it is important that the patient be made aware of the potential complications of aware of the potential complications of the proposed procedure”the proposed procedure”
ACOG Practice Bulletin No. 17. ACOG Practice Bulletin No. 17. June, 2000June, 2000

If you have to inform a mother of a If you have to inform a mother of a 5% risk of serious complications 5% risk of serious complications associated with vacuum delivery, associated with vacuum delivery, can you do anything to reduce the can you do anything to reduce the
risk?risk?
What are the factors that are What are the factors that are associated with increased risk associated with increased risk
of trauma?of trauma?
Quality Care in Obstetrics Quality Care in Obstetrics Birth Trauma related to Vacuum Birth Trauma related to Vacuum
DeliveryDelivery
How we cause itHow we cause it– Unnecessary procedureUnnecessary procedure– High risk procedureHigh risk procedure– Inadequate skill of providerInadequate skill of provider– Unknown fetal parametersUnknown fetal parameters– Prolonged application or multiple pop-Prolonged application or multiple pop-
offsoffs– No alternative delivery options availableNo alternative delivery options available

Vacuum ApplicationVacuum Application


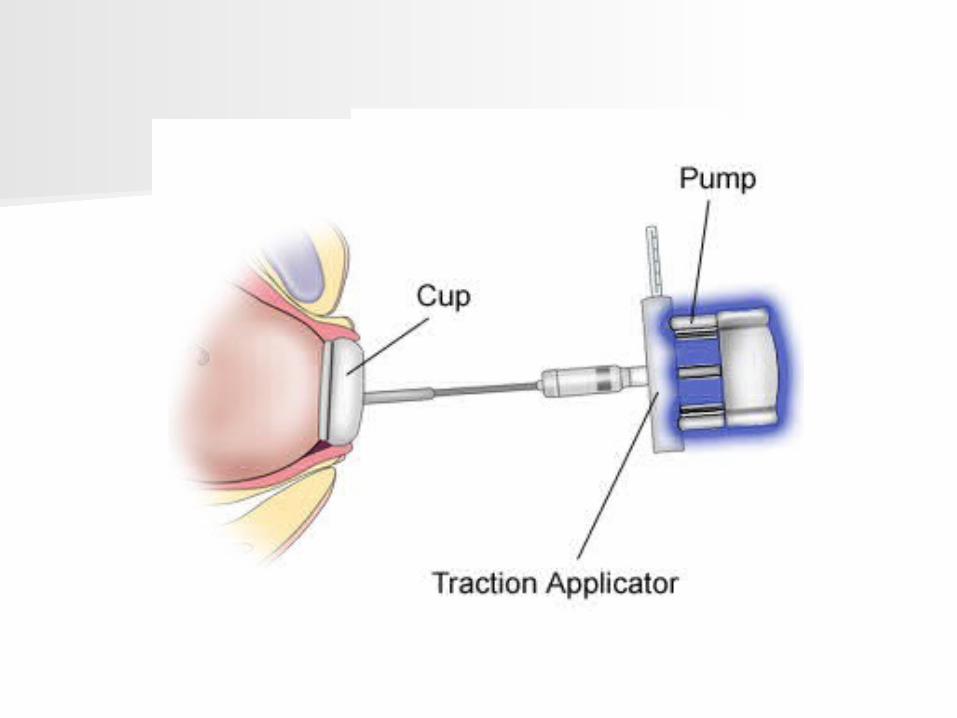
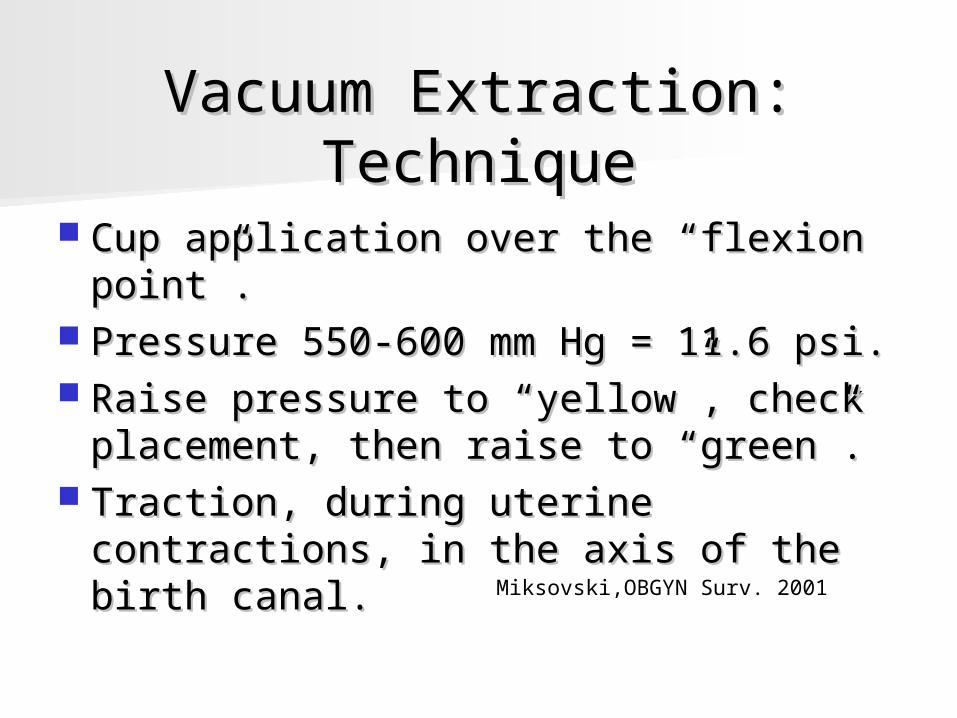
Vacuum Extraction: Vacuum Extraction: TechniqueTechnique
Cup application over the “flexion Cup application over the “flexion point”.point”.
Pressure 550-600 mm Hg = 11.6 psi.Pressure 550-600 mm Hg = 11.6 psi. Raise pressure to “yellow”, check Raise pressure to “yellow”, check
placement, then raise to “green”.placement, then raise to “green”. Traction, during uterine contractions, Traction, during uterine contractions,
in the axis of the birth canal.in the axis of the birth canal.Miksovski,OBGYN Surv. 2001

Vacuum Extraction: Vacuum Extraction: TechniqueTechnique
Duration of vacuumDuration of vacuum– 15-30 minutes, most favoring 15-20.15-30 minutes, most favoring 15-20.– 10 minutes of high pressure if pressure 10 minutes of high pressure if pressure
lowered between contractions.lowered between contractions. Pop-offsPop-offs
– One occurs in 16-38% of casesOne occurs in 16-38% of cases– Limits of 3 recommendedLimits of 3 recommended– Likely is a sign of misapplication or CPDLikely is a sign of misapplication or CPD
Miksovski,OBGYN Surv. 2001

Baskett T, JOGC, July 2008Baskett T, JOGC, July 2008
ParameterParameter Total (N = 1000)Total (N = 1000)
Spines + 2 or +3Spines + 2 or +3 75%75%
Spines + 4Spines + 4 15%15%
Occiput anterior at applicationOcciput anterior at application 87%87%
Occiput anterior at deliveryOcciput anterior at delivery 93%93%
Applied at flexion pointApplied at flexion point 50%50%
Applied paramedian Applied paramedian 47%47%
Duration of application < 10 minDuration of application < 10 min 97%97%
Number of pulls > 3Number of pulls > 3 4%4%
Number of pop-offs >1Number of pop-offs >1 7%7%
Successful vacuum deliverySuccessful vacuum delivery 87%87%

Baskett T, JOGC, July 2008Baskett T, JOGC, July 2008
Outcome MeasureOutcome Measure Total (N = 1000)Total (N = 1000)
3rd/4th Degree Tear : Epis./No Epis.3rd/4th Degree Tear : Epis./No Epis. 16%/6%16%/6%
Scalp “markings”Scalp “markings” 65%65%
Minor scalp traumaMinor scalp trauma 11.4%11.4%
Shoulder dystociaShoulder dystocia 5.6%5.6%
BP injuryBP injury 0.3%0.3%
ICHICH 0.4%0.4%
Subgaleal hemorrhageSubgaleal hemorrhage 0.1%0.1%
Forceps following vacuumForceps following vacuum 9.8%9.8%
Cesarean following vacuumCesarean following vacuum 2%2%

Simonsen, et. al.Simonsen, et. al.
913 successful term vacuum births.913 successful term vacuum births. Limits: Vacuum discontinued ifLimits: Vacuum discontinued if
no progress in 3 pulls, no progress in 3 pulls, no delivery in 8 pulls, or no delivery in 8 pulls, or 2 pop-offs.2 pop-offs.
All infants evaluated by All infants evaluated by transfontanellar ultrasound and skull transfontanellar ultrasound and skull x-rayx-ray
Obstet.Gynecol, 2007, 109, 626-33
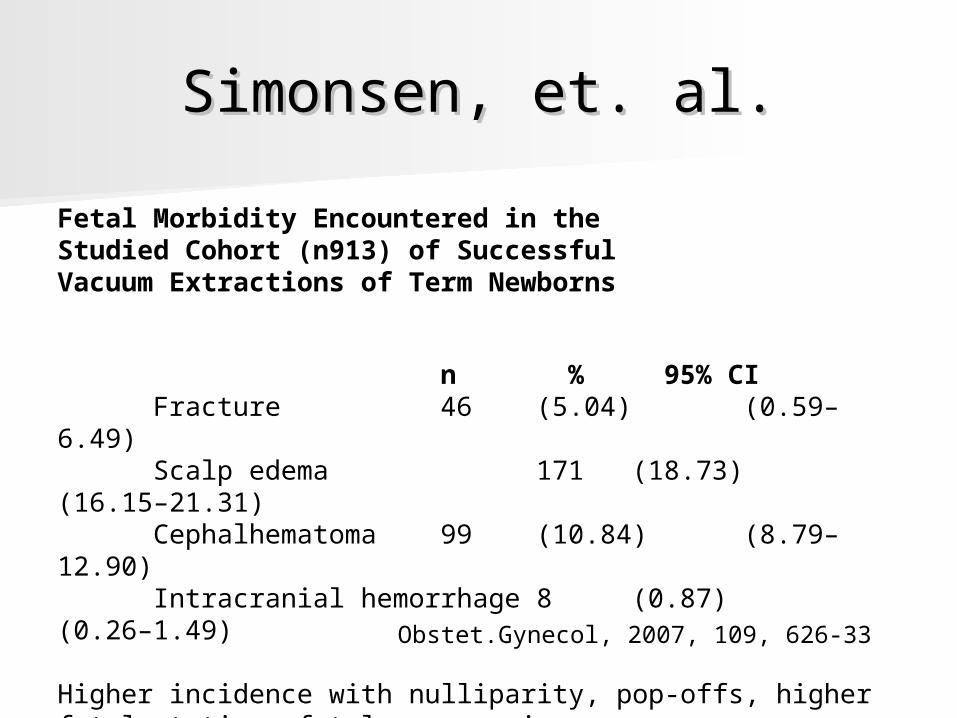
Simonsen, et. al.Simonsen, et. al.
Fetal Morbidity Encountered in theStudied Cohort (n913) of SuccessfulVacuum Extractions of Term Newborns
n % 95% CIFracture 46 (5.04) (0.59–6.49)Scalp edema 171 (18.73) (16.15–21.31)Cephalhematoma 99 (10.84) (8.79–12.90)Intracranial hemorrhage 8 (0.87) (0.26–1.49)
Higher incidence with nulliparity, pop-offs, higher fetal station, fetal macrosomia
Obstet.Gynecol, 2007, 109, 626-33
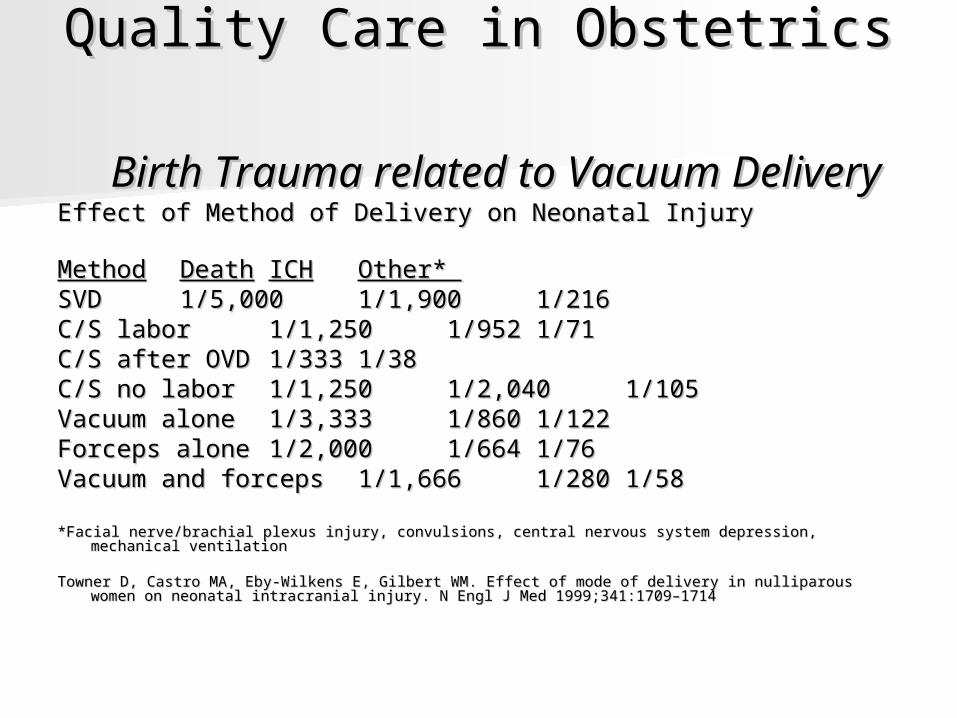
Quality Care in ObstetricsQuality Care in Obstetrics Birth Trauma related to Vacuum Birth Trauma related to Vacuum
DeliveryDeliveryEffect of Method of Delivery on Neonatal InjuryEffect of Method of Delivery on Neonatal Injury
MethodMethod DeathDeath ICHICH Other* Other* SVDSVD 1/5,0001/5,000 1/1,9001/1,900
1/2161/216C/S laborC/S labor 1/1,2501/1,250 1/9521/952 1/711/71C/S after OVDC/S after OVD 1/3331/333 1/381/38C/S no laborC/S no labor 1/1,2501/1,250 1/2,0401/2,040
1/1051/105Vacuum aloneVacuum alone 1/3,3331/3,333 1/8601/860 1/1221/122Forceps aloneForceps alone 1/2,0001/2,000 1/6641/664 1/761/76Vacuum and forcepsVacuum and forceps 1/1,6661/1,666 1/2801/280 1/581/58
*Facial nerve/brachial plexus injury, convulsions, central nervous system depression, mechanical ventilation*Facial nerve/brachial plexus injury, convulsions, central nervous system depression, mechanical ventilation
Towner D, Castro MA, Eby-Wilkens E, Gilbert WM. Effect of mode of delivery in nulliparous women on neonatal Towner D, Castro MA, Eby-Wilkens E, Gilbert WM. Effect of mode of delivery in nulliparous women on neonatal intracranial injury. N Engl J Med 1999;341:1709–1714 intracranial injury. N Engl J Med 1999;341:1709–1714
ACOG RecommendationsACOG Recommendations
Unless the preoperative assessment Unless the preoperative assessment is is highly suggestivehighly suggestive of a successful of a successful outcome, trial of operative vaginal outcome, trial of operative vaginal delivery is best avoided.delivery is best avoided.
The weight of available evidence The weight of available evidence appears to be against attempting appears to be against attempting multiple efforts at OVD with different multiple efforts at OVD with different instruments, instruments, unless there is a unless there is a compelling and justifiable reason.compelling and justifiable reason.
ACOG Practice Bulletin 17, June 2000

Knowing what you Knowing what you know, what know, what
interventions could be interventions could be considered to ensure considered to ensure
the safest outcome for the safest outcome for vacuum delivery at your vacuum delivery at your
hospital?hospital?

Quality Care in ObstetricsQuality Care in ObstetricsPreventing Trauma with Vacuum DeliveryPreventing Trauma with Vacuum Delivery
Preliminary considerationsPreliminary considerations– Consider alternative managementConsider alternative management– High chance of successHigh chance of success– Exit strategy preparedExit strategy prepared– Prepared patientPrepared patient
Informed consentInformed consent
– Resuscitation team availableResuscitation team available

Quality Care in ObstetricsQuality Care in ObstetricsPreventing Trauma with Vacuum DeliveryPreventing Trauma with Vacuum Delivery
Technical considerationsTechnical considerations– Fetal parameters known and consideredFetal parameters known and considered
EFW, Station, PositionEFW, Station, Position
– Application time and pop-offs limitedApplication time and pop-offs limited– Traction in direct line of birth canalTraction in direct line of birth canal
No rocking movementsNo rocking movements

How could you How could you “package” a plan of “package” a plan of
care?care?
Quality Care in ObstetricsQuality Care in ObstetricsPreventing Trauma with Vacuum DeliveryPreventing Trauma with Vacuum Delivery
Bundle ComponentsBundle Components– Individual components supported by Individual components supported by
sciencescience– Required to be performed for every Required to be performed for every
patient, every timepatient, every time– Bundle compliance measured by Bundle compliance measured by
fulfilling all parts of the bundlefulfilling all parts of the bundle– Focus on systemFocus on system
Quality Care in ObstetricsQuality Care in ObstetricsPreventing Trauma with Vacuum DeliveryPreventing Trauma with Vacuum Delivery
Vacuum BundleVacuum Bundle– Alternative labor strategies consideredAlternative labor strategies considered– Prepared patientPrepared patient
Informed consent discussed and documentedInformed consent discussed and documented
– High probability of successHigh probability of success EFW, fetal position and station knownEFW, fetal position and station known
– Maximum application time and number of Maximum application time and number of pop-offs predeterminedpop-offs predetermined
– Exit strategy availableExit strategy available Cesarean and resuscitation team availableCesarean and resuscitation team available

Bundle Elements Applied to our Bundle Elements Applied to our Clinical Case Clinical Case
Alternative strategies considered Alternative strategies considered – Should cesarean have been done initially?Should cesarean have been done initially?
Informed consent of the patient Informed consent of the patient – Didn’t document, didn’t occur.Didn’t document, didn’t occur.
EFW, position, station known EFW, position, station known – Not really known, not documented.Not really known, not documented.
Vacuum time and pop-offs predetermined Vacuum time and pop-offs predetermined – No policy in place, was not monitored during application.No policy in place, was not monitored during application.
Exit strategy in place Exit strategy in place – Was move to forceps “compelling and justifiable”?Was move to forceps “compelling and justifiable”?– C/S team was not prepared.C/S team was not prepared.

What tools do you need What tools do you need to implement your to implement your
“package”?“package”?

Vacuum CommunicationVacuum Communication“Time Out”“Time Out”
Pre-procedure briefing:Pre-procedure briefing:– In the presence of the patient?In the presence of the patient?
Alternative strategies?Alternative strategies? Informed consent?Informed consent? High probability of success?High probability of success? Limits clear?Limits clear? Exit strategy in place?Exit strategy in place?
Post-procedure debriefing: “What went Post-procedure debriefing: “What went well? What could be done differently?”well? What could be done differently?”

Vacuum ChecklistVacuum Checklist
Alternative labor strategies discussedAlternative labor strategies discussedInformed consent discussed and Informed consent discussed and
documenteddocumentedDocument before deliveryDocument before delivery
EFW EFW Fetal positionFetal positionStation Station
Document during deliveryDocument during deliveryapplication time (limit pre-determined)application time (limit pre-determined)number of pop-offsnumber of pop-offs
Cesarean and resuscitation team availableCesarean and resuscitation team available