endo vascular treatment of infected aa as is surgıcal draınage and debrıdement always necessary
TRANSCRIPT

KAMPHOL LAOHAPENSANG, MD, FACS,
Professor and Chief Division of Vascular and Endovascular Surgery,
Department of Surgery, Chiang Mai University Hospital,
Chiang Mai ,
Thailand
E-mail: [email protected]
ENDOVASCULAR TREATMENT OF INFECTED AAAS: IS SURGICAL DRAINAGE AND
DEBRIDEMENT ALWAYS NECESSARY?
14th Congress of Asian Society for Vascular and Endovascular Surgery , October 28, 2013
Lütfi Kırdar International Congress and Exhibiton Center- Rumeli Building / Istanbul, Turkey

• Missed and delayed diagnosis
• Immuno-compromised patients
• Located in para-visceral and thoraco-abdominal
aorta
Muller BT, et al. Mycotic aneurysms of the thoracic and abdominal aorta and iliac arteries. J Vasc Surg 2001; 33: 106-13.

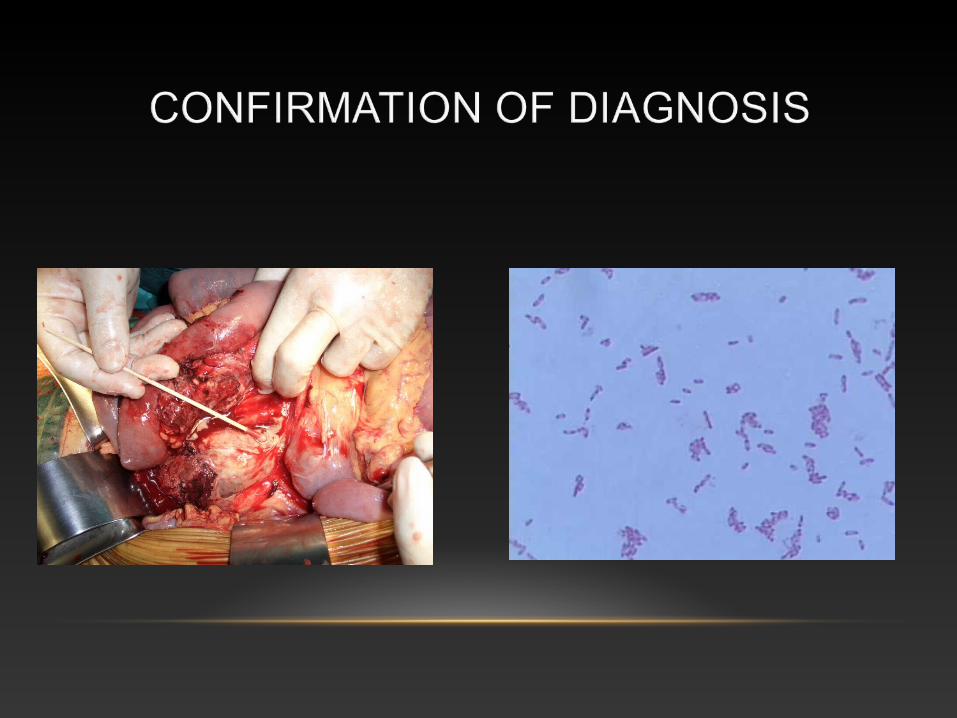
• Positive blood culture specimen
• First presentation of an aneurysm after bacterial sepsis
• Positive culture from aneurysmal wall, its content or the surrounding tissue with an associated infection
• Negative culture with : Image finding of eccentric aneurysms
: Signs of infection
: Preoperative treatment with antibiotics
Muller BT, et al. Mycotic aneurysms. J Vasc Surg 2001; 33:106-113.

• Antibiotics: initial and long term
• Prompt surgical treatment: rupture risk
- Excision of infected artery
- Removal of surrounding infected tissue
• Arterial reconstruction
- In-situ graft replacement
- Extra-anatomical bypass
• Pus collection or extended inflammatory change of the surrounding tissue
- Resection of the infected tissue
- Copious saline irrigation
- Closure of the aortic stump
- Extra-anatomical revascularization
• Low grade infection - Resection of the infected tissue
- Copious saline irrigation
- In-situ Revascularization
- Omental pedicle

• Antibiotic-coated (Rifampicin) Dacron grafts
• PTFE grafts
• Silver coated polyester grafts
• Autogenous material
• Cryopreserved allografts

Batt M, et al. In situ revascularization with silver-coated polyester grafts to treat aortic infection. J Vasc Surg 2003;38: 983-9.
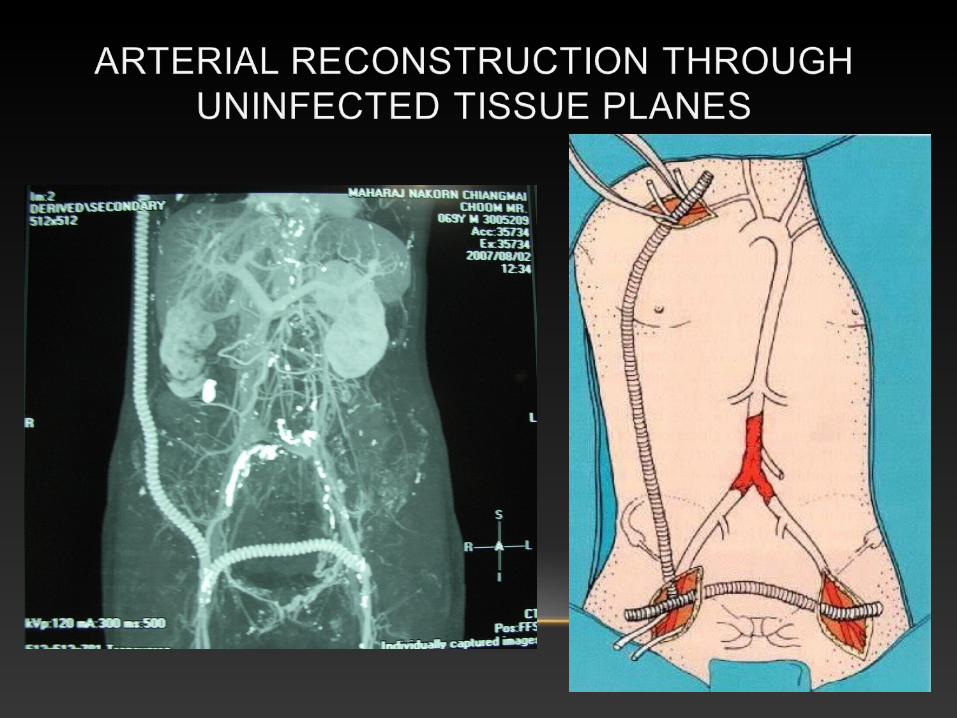

• Advantage of extra-anatomical bypass
- Decrease the risk of graft infection
• Advantage of in-situ graft replacement
- Possible in special anatomic sites
- Aortic arch
- Thoraco-abdominal aorta
- Para-visceral aorta

• Disadvantages of extra-anatomical bypass
- Shorter graft patency
- Aortic stump disruption 20%
- Amputation 20-29%
- Infection 20%
Oderich GS, Panneto JM, Bower TC, et al. Infected aortic aneueysms. J Vasc Surg 2001; 34 : 900-8.

ENDOGRAFTS FOR THE TREATMENT OF INFECTED AORTIC ANEURYSMS
• An alternative to open surgery
• Less invasive, rapid aneurysm exclusion Prompt control of bleeding in the face of hemodynamic instability
• The better choice for critically ill patients with hostile abdomen

ENDOGRAFTS FOR THE TREATMENT OF INFECTED AORTIC ANEURYSMS

• Advantages
• Decrease surgical morbidity and mortality
• Temporary measure in ruptured infected AAA
• Disadvantages
• Retained foreign body in infected tissue
• Tissue arterial wall morphology could not be obtained.
• Uncertain long term outcomes

THE SUCCESSFUL USE OF EVAR IN MYCOTIC AORTIC ANEURYSMS
1. Broad-spectrum antibiotics are administered as soon as a mycotic aortic aneurysm is suspected
2. No microbes could be isolated from blood and tissue cultures in 25 % to 40 % of mycotic aortic aneurysms
3. The use of antibiotic-coated grafts to reduce the source of infection
4. Adjunct procedures such as surgical debridement and percutaneous drainage are an important step in eliminating the source of infection
5. Prolonged postoperative antibiotic therapy is a key component for success
Lee KH, et al. J Endovasc Ther 2006; 13: 338-45. Kan CD, Lee HL, Yang YJ. Outcome after endovascular stent graft treatment for mycotic aortic aneurysm: A systematic review. J Vasc Surg 2007; 46: 906-12.

THE QUESTIONS TO BE ADDRESSED
1. When is endovascular repair only palliative therapy?
2. When does it serve as a bridge to staged definitive surgical therapy?
3. When is endovascular repair the preferred, definitive therapy?

THE ROLE OF EVAR FOR TREATMENT OF INFECTED AORTIC ANEURYSMS
• Well- controlled of an active infection by broad-spectrum antibiotics and with the patient without fever and with stable hemodynamic parameters
• Acute presentation with fever, positive blood culture, active bleeding and hemodynamic in-stability from aneurysm rupture
• Treatment is followed by specific appropriate antibiotics

CHIANG MAI UNIVERSITY REVIEW(FROM JANUARY 2009 DECEMBER 2011)
Elective EVAR for stable Infected AAAsCase no.
Gender/Age Organisms Procedures Complications 2nd Procedures Status
1. 71/ M Salmonella Bifurcated Graft
Infected Graft Explantation 10 months after EVAR
Alive
2. 69/ M B. pseudomallei AUI - FFbx No No Alive
3. 72/ M E. coli Bifurcated Graft
No Surgical Drainage
Alive
4. 83/ F Salmonella Tube Graft No No Alive
5. 57/ M B. pseudomallei Tube Graft No No Alive
All survived patients have a lifelong antibiotics treatment

EXPLANTANTATION OF THE INFECTED AORTIC STENT GRAFT

EVAR for Mycotic Aortoiliac Aneurysm with Surgical Drainage

EVAR for Mycotic Aortoiliac Aneurysm with Surgical Drainage

CHIANG MAI UNIVERSITY REVIEW(FROM JANUARY 2009 DECEMBER 2011)
All 5 cases ( 1 E. coli, 1 B. pseudomalei and 3 Salmonella )
• No operative and 30 days mortality
• Significant postoperative complications 40 %
-Renal failure, MI, respiratory failure, etc
• Surgical complications 21 %
-Bleeding, wound, ischemic colitis, etc
Elective Open repair for stable Infected AAAs
All survived patients have a lifelong antibiotics treatment
Laohapensang K, et al. Management of the Infected Aortoiliac Aneurysms. Annals of Vascular Disease 2012: 5 : 1-8.

CHIANG MAI UNIVERSITY REVIEW(FROM JANUARY 2009 DECEMBER 2011)
Case no. Gender/Age Organisms Procedures Complications 2nd Procedures Status
1. 75/ F Salmonella Bifurcated Graft
Left Graft Limb Occlusionb
Thrombo-embolectomy
Alive
2. 58/ M E. coli Tube Graft No No Alive
3. 81/ M Salmonella AUI , F-F bx No No Alive
4. 61/ F Salmonella Tube Graft No No Alive
Emergency EVAR for un-stable Infected AAAs
Emergency Open repair for un-stable Infected AAAs
All 5 case had Salmonella infection with 30 days mortality rate of 60 % (3/5)
All survived patients have a lifelong antibiotics treatmentLaohapensang K, et al. Management of the Infected Aortoiliac Aneurysms. Annals of Vascular Disease 2012: 5 : 1-8.
Laohapensang K, et al. Infected aneurysms. Annals of Vascular Disease 2010: 3 : 16-23.
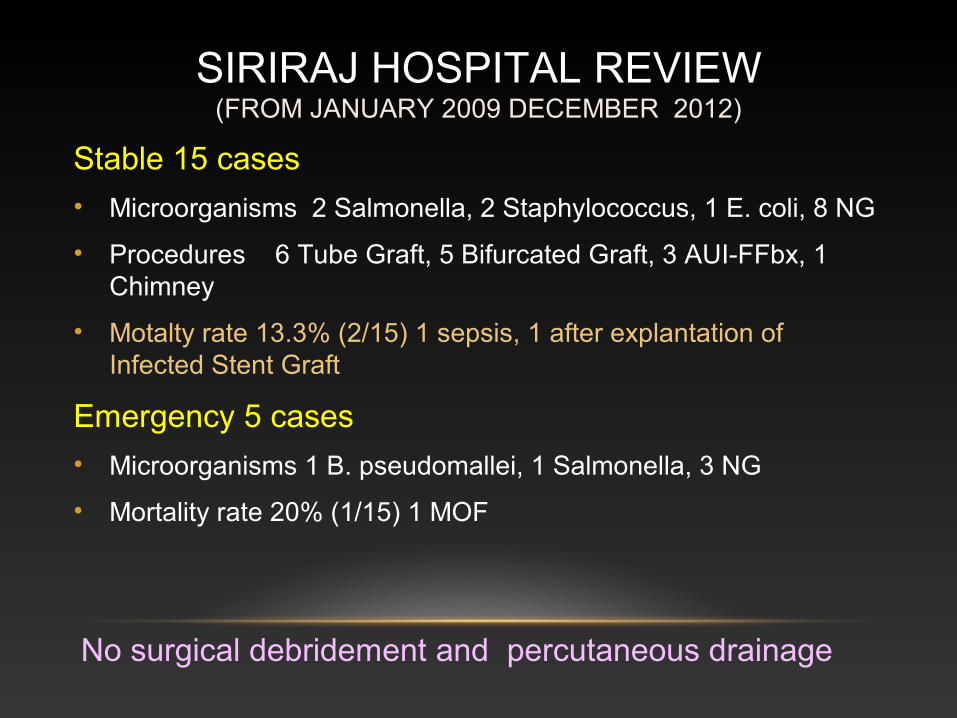
SIRIRAJ HOSPITAL REVIEW(FROM JANUARY 2009 DECEMBER 2012)
Stable 15 cases
• Microorganisms 2 Salmonella, 2 Staphylococcus, 1 E. coli, 8 NG
• Procedures 6 Tube Graft, 5 Bifurcated Graft, 3 AUI-FFbx, 1 Chimney
• Motalty rate 13.3% (2/15) 1 sepsis, 1 after explantation of Infected Stent Graft
Emergency 5 cases
• Microorganisms 1 B. pseudomallei, 1 Salmonella, 3 NG
• Mortality rate 20% (1/15) 1 MOF
No surgical debridement and percutaneous drainage

IS SURGICAL DRAINAGE AND DEBRIDEMENT ALWAYS NECESSARY?
THE ANSWER IS
NO

THANK YOU FOR ATTENTION
Chiang Mai,Thailand