dr reema ayyash st7 james cook university hospital
TRANSCRIPT

Regional Anaesthesia Dr Reema Ayyash
ST7
James Cook University Hospital

Overview
• Past SAQs
• Anatomy and techniques for common blocks
• MCQ & SBA session
• Hot topics
• For nerve bloc videos: http://www.nysora.com

For any nerve block question
Preparation
• Pre-operative assessment and consent
• Aseptic technique
• Full monitoring as per AAGBI guidelines
• IV access
• Resuscitation equipment available
• Trained assistant
• Correct equipment available: needle, PNS, US
• Calculated dose of local anaesthetic

September 2014
a) Outline the basic principles of ultrasound signal and image generation. (6 marks)
b) How may physical factors influence the image quality of an ultrasound device? (6 marks)
c) Which two needling techniques are commonly used in ultrasound guided nerve blocks and what are the advantages and disadvantages of each? (8 marks)

Pass Rate 5.7%
“The very poor scores for this question were surprising given the widespread use of ultrasound imaging in current clinical practice”
“ Eight marks were attainable for discussing two types of needling technique, hence this question was deemed to be moderately difficult and not hard. Despite this, many candidates failed to score more than five marks.”
“ A “black box” approach was evident in the written answers and examiners questioned whether the candidates had any knowledge of the factors which affect the generation of a good quality ultrasound image.”
“Previous reports from the SAQ Group Chair have emphasised that knowledge acquired in preparation for the Primary FRCA examination can be tested in any element of the Final FRCA process. This advice seems to have been largely ignored. The question was of moderate discriminatory value as ignorance of the topic was widespread within the candidate cohort.”
a) Outline the basic principles of ultrasound signal and image generation. (6 marks) • Based on sound waves that are transmitted from, and received by, an US
transducer
• The transducer utilises frequencies of 2– 15 MHz
• Transducers use artificial polycrystalline ferroelectric materials (ceramics) which have piezoelectric properties
• Relies on piezo-electric effect: based on the conversion of sound to electrical energy
• This allows the transducer to act as both a sound transmitter and receiver
• Ultrasound waves are generated by a piezoelectric crystal transducer encased in the probe

a) Outline the basic principles of ultrasound signal and image generation. (6 marks) • A high frequency alternate voltage is applied to the crystal
• This changes the shape of the crystals generating oscillations
• The generated sound waves are propagated into the tissues and are either reflected or scattered at the tissue interface
• The reflected portion returns to the probe where it distorts the transducer material
• This creates an electrical charge which is then amplified and displayed on a monitor to produce an image
• Hyperechogenic: Highly reflective tissue e.g. bone – appear white
• Hypoechogenic: Poorly reflective tissue e.g. muscle – appear grey
• Anechogenic: Do not reflect at all e.g. blood/air – appear black

a) Outline the basic principles of ultrasound signal and image generation. (6 marks) Amplitude mode (A mode):
displays a single echo signal against time to measure depth
Brightness modulation (B mode): A 2D image using
multiple beam positions and a series of reflected echoes,
producing a black and white image similar to an anatomical
slice

a) Outline the basic principles of ultrasound signal and image generation. (6 marks)
Motion mode (M mode): M-line ensonified repeatedly to examine a moving structure.
Plots how the structure moves with time

b) How may physical factors influence the image quality of an ultrasound device? (6 marks)
Tissue interaction
• Ultrasound images produced depend on:
• Density of tissue imaged
• Echogenicity
• Axial resolution: refers to the ability to distinguish two structures that lie along the axis (i.e. parallel) of the ultrasound beam as separate and distinct.
• High frequency = low pulse duration thus better axial resolution
• Acoustic impedance: determines the amount of ultrasound reflected in the media/tissue

b) How may physical factors influence the image quality of an ultrasound device? (6 marks)
Tissue interaction
Attenuation

b) How may physical factors influence the image quality of an ultrasound device? (6 marks)
Tissue interaction
Refraction Scattering

b) How may physical factors influence the image quality of an ultrasound device? (6 marks)
Tissue interaction
Diffraction Speckle

b) How may physical factors influence the image quality of an ultrasound device? (6 marks)
Phenomena
Anisotropy Acoustic enhancement

b) How may physical factors influence the image quality of an ultrasound device? (6 marks)
Phenomena
Artifact Acoustic Shadowing

b) How may physical factors influence the image quality of an ultrasound device? (6 marks)
Phenomena
Reverberation

c) Which two needling techniques are commonly used in ultrasound guided nerve blocks and what are the advantages and disadvantages of each? (8 marks)
Out of plane technique
• Needle insertion perpendicular to transducer with the needle being identified as a hyperechoic dot on the screen as it crosses the beam
Advantages:
• Used when a short needle to nerve distance exists as this may minimize patient discomfort

c) Which two needling techniques are commonly used in ultrasound guided nerve blocks and what are the advantages and disadvantages of each? (8 marks)
Disadvantages:
• Accurate identification of needle tip challenging increasing risk of misplacement

c) Which two needling techniques are commonly used in ultrasound guided nerve blocks and what are the advantages and disadvantages of each? (8 marks)
In-plane technique
• Preferred technique
• Needle inserted parallel to the transducer and ultrasound beam allowing visualization of the needle shaft and tip throughout the procedure
Advantages:
• Insertion angle of needle relative to probe is fairly superficial making it very useful for superficial nerve blocks

c) Which two needling techniques are commonly used in ultrasound guided nerve blocks and what are the advantages and disadvantages of each? (8 marks)
Advantages:
• Needle visualization is better with accurate needle tip placement thus increasing potential for block success and limiting complications
Disadvantages:
• At steep angles identification of needle tip can be difficult with increased refraction/decreased reflection of ultrasound waves
• Increased needle to nerve distance may result in increased patient discomfort

September 2010
What are the
a) cardiovascular (25%),
b) respiratory (20%),
c) gastrointestinal (20%) and
d) haematological (25%)
potential benefits of local anaesthetic neuraxial blockade?

Pass Rate 21%
“Neuraxial blockade is a foundation of anaesthetic practice and the poor performance in this question was surprising.”
“Feedback from examiners suggests that the main reason for the poor performance in this question was not considering the potential benefits of neuraxial blockade through the entire perioperative period. “
Cardiovascular
• Improved coronary blood flow - reduced risk of myocardial ischaemia
• Myocardial oxygen supply:demand ratio is improved by reduction of sympathetic activity and reduced thrombotic tendency
• Patients with underlying cardiac disease appear to have a better cardiac outcome with lower catecholamine levels and reduced cardiac workload

Respiratory
• Improved pulmonary function particularly in patients with a poor pre-op pulmonary function
• Improved lung mechanics
• Reduced incidence of post-op atelectasis and therefore pulmonary infection
• Reduced side effects of opioid analgesia – respiratory depression
• Allows patients to comply with physio – deep breathing and coughing

Gastrointestinal
• Improved intestinal motility
• Blocking of nociceptive and sympathetic reflexes
• Limiting use of opioids and therefore post-op ileus
• Reduced side effects of opioids – nausea/vomiting/ileus
• Reduced hyperglycaemic response to surgery

Haematological
• Decreased incidence of post-op DVT by:
• Improved systemic blood flow
• Decreased platelet stickiness
• Decreased inhibition of fibrinolysis
• Increased mobility post-op
• Improved graft survival in vascular patients
• Reduced intra-operative blood loss and therefore blood transfusions

April 2002
a) Draw a diagram of the lumbar plexus.
b) Outline the anatomical basis of a ‘3 in 1’ block
c) Explain why the block may fail to provide reliable analgesia for hip surgery?

a) Draw a diagram of the lumbar plexus.

Anterior and
Posterior Cutaneous
Innervation of Lumbar Plexus

Lumbar Plexus Block Patient Position • Lateral decubitus position • Side to be blocked
uppermost
Landmark • Posterior superior iliac crest • Spinous process (midline) • Posterior superior iliac
spine • 50-100mm needle insertion
site is 3-5 cm lateral intercristal line

Lumbar Plexus Block Technique • Needle inserted perpendicular
to skin
• Nerve stimulator set initially to 1.5 mA
• Needle advanced until twitches of quadriceps muscle is obtained (depth 6-8cm)
• Current then decreased to 0.5-1.0mA to produced stimulation
• After negative aspiration, inject LA

Lumbar Plexus Block: Complications • Infection: psoas abscess • Vascular puncture • Retro-peritoneal haematoma formation • Damage to abdominal viscera • Nerve injury and intra-neural injection • Haemodynamic consequences: spinal/epidural spread • Local anaesthetic toxicity

b) Outline the anatomical basis of a ‘3 in 1’ block • 3 in 1 = Single injection which aims to block
• Femoral nerve
• Obturator nerve
• Lateral femoral cutaneous nerve
• Uses the same technique as the femoral nerve block, however
• Larger volume of local anaesthetic injected 30-40mls
• Distal compression is performed as the local anaesthetic is being injected to force the solution cranially towards the lumbar plexus into the psoas compartment
c) Explain why the block may fail to provide reliable analgesia for hip surgery? • The obturator nerve has a more variable location as it passes to the
pelvis
• It is separated from femoral and lateral femoral cutaneous nerve by the psoas muscle
• This is why the “3-in-1 block” often fails to successfully block the obturator nerve

October 2008
a) Describe the surface anatomical landmarks for (i) the anterior (Beck’s) and (ii) one posterior approach to sciatic nerve block. (50%)
b) What practical advantages and disadvantages would you consider when choosing between these two approaches in an individual patient? (20%)
c) List the complications that may result from this block. (20%)

Sciatic Nerve Anatomy
• Largest nerve in body supplying lower limb
• Arises from sacral plexus L4-S3 • Exits pelvis through greater
sciatic foramen • Passes between the ischial
tuberosity and greater trochanter of the femur
• Runs down the posterior aspect of the thigh
• In the popliteal fossa it divides into tibial and common peroneal nerve

Sciatic Nerve Anatomy
Nerve Supply Motor • Posterior thigh muscles and biceps
femoris • Supplies NO structures in the
gluteal region Sensory • Skin of the leg and foot below the
knee except for the medial calf

a) Describe the surface anatomical landmarks for (i) the anterior (Beck’s) and (ii) one posterior approach to sciatic nerve block. (50%)
ANTERIOR APPROACH
Patient lies supine
Landmarks:
• Line 1 is drawn from the anterior
superior iliac spine to the pubic tubercle
• Line 2 is parallel to line 1
from the greater trochanter to
the medial border of the thigh

a) Describe the surface anatomical landmarks for (i) the anterior (Beck’s) and (ii) one posterior approach to sciatic nerve block. (50%)
ANTERIOR APPROACH
• At the junction of the medial
and middle thirds a perpendicular
line is dropped to meet line 2
• At this junction, a 150mm needle
is inserted perpendicular to the
skin and directed posteriorly
until it contacts the medial shaft
of the femur (lesser trochanter)

a) Describe the surface anatomical landmarks for (i) the anterior (Beck’s) and (ii) one posterior approach to sciatic nerve block. (50%)
ANTERIOR APPROACH
• When the lesser trochanter is
met, the needle is withdrawn
slightly and redirected to pass
under the medial border of the
femur, usually advanced 2-3cm
further (average depth 10-13cm)
• Aspirate to check for
intravascular injection

a) Describe the surface anatomical landmarks for (i) the anterior (Beck’s) and (ii) one posterior approach to sciatic nerve block. (50%)
POSTERIOR APPROACH
Patient lies in lateral position
Lower leg kept straight
Upper leg is flexed at the knee
Landmarks:
• A 1st line is drawn from the
greater trochanter to the
posterior superior iliac spine
• A 2nd line is drawn from the
Greater trochanter to sacral hiatus
(Winne’s modification)

a) Describe the surface anatomical landmarks for (i) the anterior (Beck’s) and (ii) one posterior approach to sciatic nerve block. (50%)
POSTERIOR APPROACH
• At the lines’ midpoint,
a perpendicular line is
dropped caudally by 3-5cm
• A 4th line is drawn along the
“furrow” formed by the medial
edge of gluteus maximus and
along the head of biceps femoris
• Triangle formed by the 1st, 2nd
and 4th lines identifies the point of needle insertion

b) What practical advantages and disadvantages would you consider when choosing between these two approaches in an individual patient? (20%) ANTERIOR APPROACH
Advantages • Performed supine – more
comfortable for patient
Disadvantages • Advanced nerve block, associated
with patient discomfort as the needle must traverse multiple muscle planes on its way to sciatic nerve (deeper block)
• Needle can become obstructed with tissue debris
• Sedation maybe required • Onset time 20-30min depending on
type and conc of LA used • Difficult to insert catheter for
continuous infusion due to perpendicular angulation of needle

b) What practical advantages and disadvantages would you consider when choosing between these two approaches in an individual patient? (20%) POSTERIOR APPROACH
Advantages • Readily identifiable landmarks in
most people • Onset time less at 10-25 minutes • Catheter easily inserted for
continuous infusion
Disadvantages • Significant discomfort as needle
traverses gluteus muscle • Sedation maybe required • Skin highly mobile therefore
palpating hand should not be moved during entire procedure
• Requires positioning in lateral decubitus position (trauma patients with uncleared or unstable spines therefore ruled out)
c) List the complications that may result from this block. (20%)
• Failure
• Drug error
• Nerve damage
• Intravascular injection
• Local anaesthetic toxicity
• Vascular puncture
• Haematoma - avoid multiple needle insertions particularly in patients receiving anticoagulation therapy
• Infection
• Neuronal ischaemia

Femoral Nerve: Anatomy
• Formed by dorsal divisions of anterior rami of L2–L4
• Largest terminal branch of lumbar plexus
• Travels through psoas muscle and leaves the psoas at its lateral border
• It then descends caudally into the thigh via the groove formed by the psoas and iliacus muscles, entering the thigh beneath the inguinal ligament

Femoral Nerve: Anatomy
• After emerging from the ligament, the femoral nerve divides into :
• Anterior branch
• Posterior branch
• At this level it is located lateral and posterior to the femoral artery
• Anterior branch:
• Motor innervation to sartorius and pectineus muscles
• Sensory innervation to skin of anterior and medial thigh

Femoral Nerve: Anatomy
• Posterior branch:
• Motor innervation to quadriceps muscle
• Sensory innervation to medial aspect of the lower leg via saphenous nerve

Femoral Triangle: Anatomy (Boundaries)
• Superiorly – inguinal ligament
• Laterally – medial border of sartorius
• Medially – medial border of adductor longus
• Base of triangle – inguinal ligament
• Apex - medial border of sartorius crosses the medial border of adductor longus
• Roof – fascia lata and cribiform fascia
• Floor (lateral to medial):
• Iliopsoas, Pectineus, Adductor longus

Femoral Triangle: Contents
Lateral to medial - NAVY
• Femoral nerve
• Femoral artery
• Femoral vein including great saphenous vein
• Femoral artery, vein, lymphatics and femoral canal are INSIDE the femoral sheath
• Femoral nerve and lateral cutaneous nerve lie OUTSIDE the femoral sheath

Femoral Nerve Block
Patient Position
• Supine, leg extended
Landmark
• Identify anterior superior iliac spine and pubic symphysis
• Draw a line between them = indicates inguinal ligament
• Palpate femoral artery

Femoral Nerve Block
Technique
• Needle is inserted 1-1.5cm lateral to artery and 1-2cm below inguinal ligament
• Needle directed cephalad at 30° to 45° angle to skin, at a depth of 3-4cm
• A brisk “patellar snap” with the current at or< 0.5 mA indicates successful localisation of needle near the femoral nerve

Femoral Nerve Block: Ultrasound
Landmark
• Palpate femoral pulse = useful landmark

Femoral Nerve Block: Ultrasound
Landmark
• Palpate femoral pulse = useful landmark
• Femoral nerve typically visualised at a depth of 2-4cm

Femoral Nerve Block: Ultrasound

October 2004
a) What are the indications for a popliteal fossa block? (10%)
b) List the nerves that are affected and describe their cutaneous innervation. (35%)
c) What responses would you get on stimulating these nerves? (25%)
d) Briefly describe one technique for performing this block. (30%)

a) What are the indications for a popliteal fossa block? (10%)
Indications
• Surgical procedures below the knee
• Foot/ankle Surgery
• Short saphenous vein stripping
• Corrective foot surgery
• Foot debridement
• Achilles tendon repair
• Sural nerve biopsy

Popliteal Fossa: Anatomy Boundaries
• Roof – skin and fascia
• Medially – tendon of
semimembranous and medial head
of gastrocnemius
• Laterally – tendon of biceps
femoris and lateral head
of gastrocnemius
• Site where sciatic nerve divides into: • Tibial Nerve • Common peroneal nerve
• Division occurs 4-7cm proximal to crease

b) List the nerves that are affected and describe their cutaneous innervation. (35%)
Sciatic Nerve (L4-S3)
• Supplies all cutaneous innervation except areas supplied by saphenous nerve L2–4 (branch of the femoral nerve)

b) List the nerves that are affected and describe their cutaneous innervation. (35%)
Tibial Nerve (L4-S3)
• Largest of 2 divisions
• Gives off terminal branches:
• Medial and Lateral Plantar Nerves
• Supplies anterior and medial parts of the sole of foot
• Posterior Tibial nerve calcaneal branch
• Supplies the heel

b) List the nerves that are affected and describe their cutaneous innervation. (35%)
Common Peroneal Nerve (L4-S2)
• Gives off terminal branches
• Superficial Peroneal Branch
• Supplies dorsum of foot
• Deep Peroneal Branch
• Supplies area between first and second toes

b) List the nerves that are affected and describe their cutaneous innervation. (35%)
Sural Nerve
• Formed from branches of tibial and common peroneal nerve
• Supplies:
• Lateral and posterior third of leg
• Lateral aspect of foot and heel and lateral ankle

c) What responses would you get on stimulating these nerves? (25%)
• Visible or palpable twitches of the foot or toes at 0.2-0.5 mA current
Common peroneal nerve stimulation
• Dorsiflexion and eversion
Tibial nerve stimulation
• Plantar flexion and inversion

d) Briefly describe one technique for performing this block. (30%) Patient Positioning
• Supine and flex knees to 30°
• Lateral decubitus
• Prone - allowing foot to extend
beyond the bed
Landmark
• Identify popliteal crease – Line 1
• Palpate the tendon of biceps
femoris muscle (laterally) – Line 2
• Palpate the tendons of
semitendinosus and
semimembranosus (medially) – Line 3

d) Briefly describe one technique for performing this block. (30%) Landmark
• Needle insertion point marked at 7 cm above popliteal fossa crease at midpoint between the two tendons

d) Briefly describe one technique for performing this block. (30%) Technique
• Stand at patients side
• Nerve stimulator should be initially set to deliver 1.5 mA current
• Insert a 22 G, 100 mm insulated needle posteriorly 25–30° and slightly caudad
• Needle is passed through bicep femoris to enter the popliteal fossa
• The nerves are located by identifying the responses
• Common peroneal nerve - Dorsiflexion and eversion
• Tibial nerve - Plantar flexion and inversion
• After initial stimulation is obtained, the current is gradually decreased until twitches are still seen or felt at 0.2 to 0.5 mA
• This typically occurs at a depth of 3 to 5 cm
• 10 - 20ml of LA is injected for each nerve

September 2014
a) List five nerves that can be blocked at ankle level for foot surgery? (5 marks)
b) For each of these nerves, describe the sensory distribution within the foot. (5 marks)
c) Give the anatomical landmarks for an ankle block which aid correct placement of local anaesthesia for each nerve. (5 marks)
d) What are the advantages and disadvantages of an ankle block? (5 marks)

Pass Rate 65.9%
“Common clinical subjects tend to score well in the SAQ paper and discriminate between strong and weak candidates as was the case for this question.”
“Weak candidates had poor anatomical knowledge or failed to list the advantages of this specific block, giving instead the features common to any local anaesthetic technique.”
“Poor candidates tended to describe features of blocks at the popliteal level, perhaps due to failing to read the question thoroughly as ankle level was highlighted. “
”The importance of candidates retaining knowledge of the basic sciences has been highlighted before”

a) List five nerves that can be blocked at ankle level for foot surgery? (5 marks)
• Sural nerve (L5-S2)
• Deep peroneal nerve (L4-S2)
• Superficial peroneal nerve (L4-S2)
• Saphenous nerve (L3-4)
• Tibial nerve (L5-S3)

b) For each of these nerves, describe the sensory distribution within the foot. (5 marks)

b) For each of these nerves, describe the sensory distribution within the foot. (5 marks)
Posterior Tibial Nerve (L5-S3)
• Branch of the sciatic nerve
• Lies posterior to the posterior tibial artery
• Supplies the anterior and medial aspect of sole of foot
Sural Nerve (L4-S2)
• Branch of the tibial nerve
• Accompanies short saphenous vein behind lateral malleolus
• Supplies the 5th toe, posterior aspect of sole, back of lower leg and lateral border of foot
b) For each of these nerves, describe the sensory distribution within the foot. (5 marks)
Superficial Peroneal Nerve (L4-S2)
• Branch of the common peroneal nerve
• Supplies the dorsum of the foot
Deep Peroneal Nerve (L4-S2)
• Branch of the common peroneal nerve
• Supplies the area between the 1st and 2nd toe
Saphenous Nerve (L3-4)
• Branch of the femoral nerve
• Supplies the medial side of the ankle joint

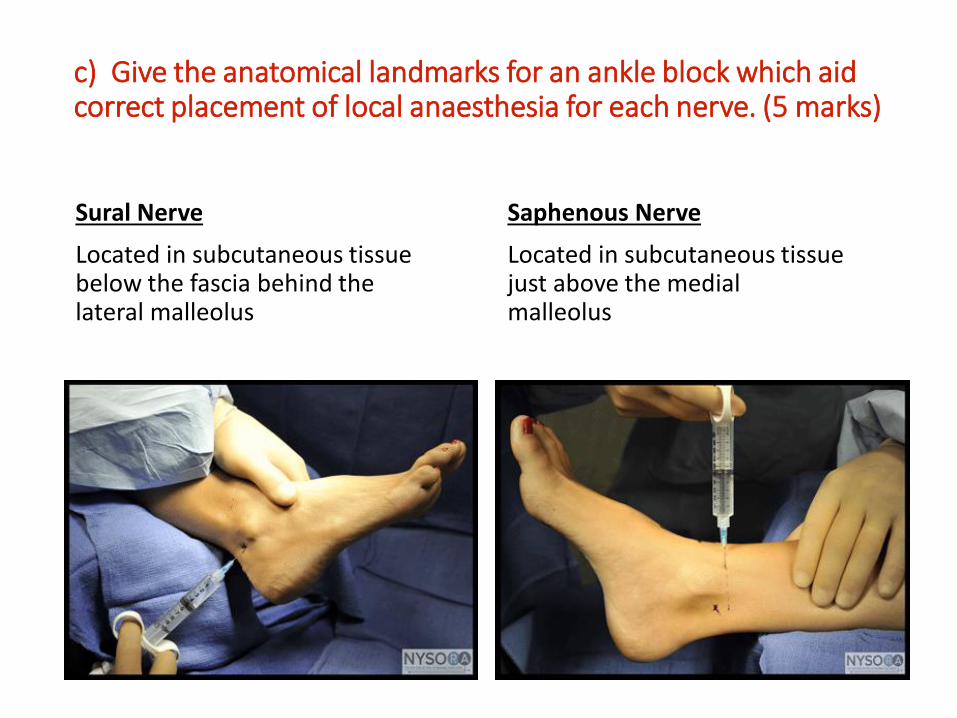
c) Give the anatomical landmarks for an ankle block which aid correct placement of local anaesthesia for each nerve. (5 marks)
Deep Peroneal Nerve
• Located immediately lateral to tendon of extensor hallucis longus muscle between extensor hallucis longus and the extensor digitorum longus
• Pulse of dorsalis pedis artery is felt
• The nerve is positioned immediately lateral to artery

c) Give the anatomical landmarks for an ankle block which aid correct placement of local anaesthesia for each nerve. (5 marks)
Posterior Tibial Nerve
• Located just behind and distal to medial malleolus
• Pulse of posterior tibial artery is felt
• The nerve is just posterior to the artery

c) Give the anatomical landmarks for an ankle block which aid correct placement of local anaesthesia for each nerve. (5 marks)
Superficial Peroneal Nerve
Located in subcutaneous tissue along a circular line at the level of the lateral malleolus and extending from anterior to posterior
c) Give the anatomical landmarks for an ankle block which aid correct placement of local anaesthesia for each nerve. (5 marks)
Sural Nerve
Located in subcutaneous tissue below the fascia behind the lateral malleolus
Saphenous Nerve
Located in subcutaneous tissue just above the medial malleolus

d) What are the advantages and disadvantages of an ankle block? (5 marks)
Advantages
• Generally well tolerated • Low risk of systemic LA toxicity • Low risk of neurological damage • Facilitates variety of surgical
procedures • Avoidance of GA, esp in high risk pts • Post-operative analgesia, allowing
earlier mobilisation & facilitating physiotherapy
• Avoids complications associated with neuraxial blockade
• Avoids use of opioids and their subsequent side effects
• Provides intra-operative cardiovascular stability
Disadvantages
• Multiple injections required – can be uncomfortable for patient
• Risk of vascular injection / injury • Potential failure of block /
inadequate block • Time consuming • Sedation maybe required • Unable to use a proximal tourniquet
for extended periods (thigh/calf)

March 2013
a) Which specific nerves must be blocked to achieve effective local anaesthesia for shoulder surgery? (30%)
b) What are the possible neurological complications of an interscalene block? (30%)
c) Outline the measures available to reduce all types of neurological damage during shoulder surgery? (40%)

Pass Rate 69.2%
“This question was answered well.”
“If an open question is asked on the possible neurological complications of a block then this will include damage to both the peripheral and central nervous system. Some candidates focused on the peripheral nerves only.”
“The answer to part c) required an account of both anaesthetic and surgical factors that would reduce neurological damage. This included “avoiding interscalene block” in the first place.”
“The question was a very good discriminator. “

April 2009
An adult patient is scheduled for shoulder surgery under an interscalene brachial plexus block.
a) Outline the possible unwanted neurological sequelae that may occur with interscalene block and their associated symptoms & signs? (60%)
b) What steps may be taken while performing the block to reduce the incidence of these problems? (40%)

Brachial Plexus: Anatomy

Interscalene Block: Indications • Shoulder surgery
• Surgery on clavicle
• Upper arm surgery
• Reduction of dislocated shoulder
• Analgesia for distal structures in the upper limb

Interscalene Block: Anatomy

Interscalene Block: Landmark Technique
• Modified Winnie’s technique
Patient Position
• Patient lies supine - head turned slightly away from side to the blocked
Landmark
• White arrow: Clavicle
• Red arrow: Posterior border of SCM
• Blue arrow: External jugular vein

Interscalene Block: Landmark Technique
Landmark
• Palpate interscalene groove between scalenous anterior and medius
• Infiltrate skin with LA
• 5cm 50mm short bevelled block needle attached to PNS
• Insert needle at 30° aiming for contralateral elbow
• Directed in the planes caudally, medially and posteriorly to the transverse processes of C6
• Look for stimulation of deltoid or biceps muscle

Interscalene Block: Ultrasound Technique
Ultrasound Probe
• Linear probe, Frequency 10-15 MHz, Depth setting 2-4 cm

a) Which specific nerves must be blocked to achieve effective local anaesthesia for shoulder surgery? (30%) • Shoulder area innervated by
nerves of both cervical and brachial plexuses
Superficial cervical plexus (C3-4):
• Supplies skin above clavicle, shoulder tip, and first two intercostal spaces anteriorly

a) Which specific nerves must be blocked to achieve effective local anaesthesia for shoulder surgery? (30%)
Brachial plexus:
• Motor supply C5-7

a) Which specific nerves must be blocked to achieve effective local anaesthesia for shoulder surgery? (30%) Brachial plexus:
• Supplies skin over deltoid muscle through upper lateral cutaneous branch of the axillary nerve
• Supplies medial side of arm and axilla through medial cutaneous nerve of the arm and the intercostobrachial nerve (T2)

a) Which specific nerves must be blocked to achieve effective local anaesthesia for shoulder surgery? (30%) • Acromioclavicular joint,
capsule and glenohumeral joint: supplied by the suprascapular nerve
• The inferior aspect of the capsule and glenohumeral joint: supplied by axillary nerve

a) Outline the possible unwanted neurological sequelae that may occur with interscalene block and their associated symptoms & signs? (60%)
Neurological Sequelae Inadvertent epidural or subarachnoid injection
Phrenic nerve block
Symptoms & Signs • Total Spinal • Anxiety/nausea, arm or hand
dysaesthesia or paralysis, cranial nerve involvement, LOC with profound cardiorespiratory compromise
• Paralysis of the hemi-diaphragm leading to reduced FVC/FEV1
• May have considerable impact on patients who are obese or with underlying respiratory problems

a) Outline the possible unwanted neurological sequelae that may occur with interscalene block and their associated symptoms & signs? (60%)
Neurological Sequelae Recurrent laryngeal nerve block
Vagal nerve block Cervical sympathetic blockade Nerve injury
Symptoms & Signs • Hoarseness of voice secondary to
unilateral vocal cord palsy
• Hoarseness of voice • Reduced cough reflex
• Horner’s syndrome
• Paresthesia (permanent/temporary)

b) What steps may be taken while performing the block to reduce the incidence of these problems? (30%) • Full monitoring as per AAGBI
• Education and sound understanding of anatomy
• Only perform unilateral blocks, STOP BEFORE YOU BLOCK
• Awake patient so patient can report pain or paresthesia on injection
• Do not inject against resistance
• USS guidance
• USS guidance plus nerve stimulator
• Experienced practitioner
• A practitioner who is experienced in one or 2 upper limb blocks
• Repeated aspiration during injection to ensure needle tip has not moved into a vascular space

c) Outline the measures available to reduce all types of neurological damage during shoulder surgery? (40%) Anaesthetic Factors • Thorough preoperative history and examination
• Identify conditions that predispose to nerve injury and existing neurological dysfunction
• Avoidance of block • Avoid intraoperative hypotension, hypothermia, and dehydration • Careful positioning of patient
• Protective padding and padded arm boards • Avoidance of contact with hard surfaces or supports that may
apply direct pressure to susceptible peripheral nerves • Arm abduction limited to < 900 in supine position to prevent brachial
plexus lesions • Protection of ulnar and median nerves: padding should be mandatory
and forearm kept in supine or neutral position • Flexion/extension of the elbow should be < 900

c) Outline the measures available to reduce all types of neurological damage during shoulder surgery? (40%) Surgical Factors
• Head and neck should be secure and care should be taken throughout the pro-cedure to ensure that excessive stretching of the brachial plexus does not occur as a result of the excessive surgical traction
• Avoidance of direct nerve injury through surgical laceration and nerve contusion
• Avoidance of traction on nerve particularly with arthroscopic surgery
• Avoidance of excess arm manipulation

November 1996
• Describe how you would carry out an axillary brachial plexus block

Axillary Block: Anatomy

Axillary Block: Landmark Technique
Patient Position
• Supine position with head
turned away to the opposite side
• Arm abducted to 90 and
the hand under the head or
externally rotated
Landmark
• Palpate axillary artery in axilla as high as possible at the lateral border of pectoralis major

Axillary Block: Landmark Technique
Landmark
• Needle is inserted at 45° just above the axillary artery pulsation
• Inject LA when a click in the perivascular sheath is felt or muscle stimulation is apparent
Radial Nerve = Wrist and finger extension
Ulnar Nerve = Thumb adduction, and flexion of 5th finger
Median Nerve = Flexion of fingers
Musculocutaneous Nerve = Elbow flexion

Axillary Block: Ultrasound Technique
Ultrasound Probe
• Linear probe, Frequency 10-15 MHz, Depth setting 2-4 cm

September 2012
a) Describe the innervation of the anterior abdominal wall. (20%)
b) In which types of surgery would a transversus abdominus plane (TAP) block be used and what are the potential benefits? (25%)
c) Outline how you would perform a TAP block. (40%)
d) What are the specific complications of a TAP block? (15%)

Pass Rate 67.4%
“The question was relevant and topical.”
“Many candidates had poor knowledge of the innervation of the anterior abdominal wall.”
“Overall was answered well.”

a) Describe the innervation of the anterior abdominal wall. (20%) • Innervation of anterolateral abdominal
wall arises from anterior rami of spinal nerves T7 to L1
• Intercostal nerves: T7-T11
• Subcostal nerves: T12
• Iliohypogastric and ilioinguinal: L1

a) Describe the innervation of the anterior abdominal wall. (20%) • Anterior divisions of T7-T11
continue from the intercostal space
• Enter abdominal wall between internal oblique and transversus abdominis muscles until they reach the rectus abdominis
• Here they perforate and supply the skin of the front of the abdomen via anterior cutaneous branches

a) Describe the innervation of the anterior abdominal wall. (20%) • Midway along their course, they
pierce external oblique muscle giving off lateral cutaneous branch
• This divides into:
• Anterior branch – supplies external oblique
• Posterior branch – supplies latissmus dorsi
a) Describe the innervation of the anterior abdominal wall. (20%) • Anterior branch of T12 communicates with iliohypogastric nerve
• Gives off a branch to pyramidalis muscle
• Lateral cutaneous branch perforates internal and external oblique muscles
• Descends over the iliac crest
• Supplies sensation to front part of gluteal region

a) Describe the innervation of the anterior abdominal wall. (20%) • Iliohypogastric and ilioinguinal nerve form part of the lumbar plexus
• Enter the transverse abdominis plane near to the iliac crest
• Iliohypogastric nerve (L1) divides into lateral and anterior cutaneous branches
• Lateral cutaneous branch supplies skin over gluteal region
• Anterior cutaneous branch supplies skin over hypogastric region
• Ilioinguinal nerve (L1) travels within the inguinal canal
• Supplies the upper and medial part of the thigh and part of the skin covering the genitalia

b) In which types of surgery would a transversus abdominus plane (TAP) block be used and what are the potential benefits? (25%)
Uses
Upper/Lower abdominal surgery • Open inguinal/umbilical hernia • Open appendicectomy • Midline Laparotomy • Open cholecystectomy
Gynaecological/Obstetric surgery • Hysterectomy via pfannenstiel
incision • LSCS via pfannenstiel incision
Urology • Prostatectomy • Renal transplant • Nephrectomy
Potential Benefits
• Role in decreasing analgesia requirements
• Used where epidural is contraindicated
• Used in ambulatory surgery to improve the quality of analgesia
• Reduce postoperative opioid requirements

c) Outline how you would perform a TAP block. (40%) Patient Position • Supine
Landmark
• TAP found in triangle of petit
• Posterior – latissamus dorsi
• Anterior – external oblique
• Inferior – iliac crest
• Triangle of petit identified on lateral aspect of abdominal wall, mid axillary point

c) Outline how you would perform a TAP block. (40%) Blind Technique
• 50-100mm blunt needle inserted perpendicular to skin within triangle of petit
• Advanced through the skin and 2 distinct “pops” are felt as needle traverses the external oblique and internal oblique muscles
• = transvusus abdominus plane
• After negative aspiration, inject 20mL of LA

c) Outline how you would perform a TAP block. (40%) Ultrasound Technique
• High frequency linear probe (10-5 MHz)
• Patient in supine position
• Probe placed transverse to abdominal wall between costal margin and iliac crest

c) Outline how you would perform a TAP block. (40%)

c) Outline how you would perform a TAP block. (40%)

d) What are the specific complications of a TAP block? (15%)
Complications • Intraperitoneal injection/haematoma • Bowel hematoma • Transient femoral nerve palsy • Intrahepatic injection • Local anaesthetic toxicity - due to large volumes required to perform
block especially if bilateral

April 2008
a) Describe the anatomy of the thoracic paravertebral space. (35%)
b) What are the indications for paravertebral nerve blockade? (25%)
c) List the complications of a paravertebral nerve block. (30%)

a) Describe the anatomy of the thoracic paravertebral space. (35%) • Wedge shaped potential space that
Space
• Extends from T1 to T12
• Found on each side
lateral to the bony
vertebral column

a) Describe the anatomy of the thoracic paravertebral space. (35%) BOUNDARIES
Anterolateral (Posterior to anterior)
• Parietal pleura
• Pleural space
• Visceral pleura
• Lung parenchyma
Medial
• Vertebral body
• Vertebral disc
• Vertebral foramina

a) Describe the anatomy of the thoracic paravertebral space. (35%) BOUNDARIES
Posterior
• Transverse process
• Costo-transverse ligament
Superior
• Head of adjacent rib
Laterally
• Posterior intercostal membrane
• Intercostal space

a) Describe the anatomy of the thoracic paravertebral space. (35%) CONTENTS
• Spinal nerve roots
• Sympathetic chain
• White and grey communicates
• Lymph nodes
• Fat
• Intercostal vessels

b) What are the indications for paravertebral nerve blockade? (25%)
Unilateral Surgical Procedure in Thoraco-abdominal Region
• Breast surgery • Thoracic surgery • Cholecystectomy • Renal surgery • Appendicectomy • Inguinal hernia repair
Relief of Acute Pain • Fractured ribs • Liver capsule pain (trauma/ruptured
cysts)
Relief of Chronic Pain • Neuropathic chest or abdominal pain
(post-surgical or post-herpetic) • Complex regional pain syndrome • Refractory angina pectoris • Relief of cancer pain
Sympathetic Blockade • Therapeutic control of hyperhydrosis • SVT

c) List the complications of a paravertebral nerve block. (30%) General Complications • Hypotension (4.6%) • Vascular puncture (3.8%) • Pleural puncture (1.1%) • Pneumothorax (0.5%)
Specific Complications • Nerve trauma • Pleural tap with seeding of malignant
cells • Intra-pleural block • Lumbar spread with quadriceps
weakness • Epidural spread • Bilateral spread of local anaesthetic • Ipsilateral Horner’s syndrome

Contraindications to Block
Absolute • Patient refusal • local sepsis (cutaneous or
intrathoracic) • Tumours in the paravertebral space
at the level of injection • Allergy to local anaesthetic drugs
Relative • Severe coagulopathy • Severe respiratory disease (where
the patient depends on intercostal muscle function for ventilation)
• Ipsilateral diaphragmatic paresis

Paravertebral Block: Technique Patient Position
• Sitting
• Lateral decubitus
Landmarks
• Spinal processes main landmark
• Represent midline
• C7 – T7

Paravertebral Block: Technique

May 2007
a) Describe the anatomy of an intercostal nerve. (25%)
b) How does this influence your technique of intercostal nerve blockade for a fractured rib? (35%)
c) List the complications that may arise and explain the anatomical reasons for these complications. (30%)

a) Describe the anatomy of an intercostal nerve. (25%) • Thoracic nerve roots arise
from ventral rami of T1-T11
• After emerging from intervertebral
foramina - gives off:
• Anterior primary ramus
• Posterior primary ramus

a) Describe the anatomy of an intercostal nerve. (25%) Anterior primary ramus
• Continues laterally as the intercostal nerve
• Pierces the posterior intercostal membrane lateral to intervertebral foramen
• Enters subcostal groove of rib, and travels inferiorly to intercostal artery and vein

a) Describe the anatomy of an intercostal nerve. (25%) Anterior primary ramus
• Initially, lies between parietal pleura and inner most intercostal muscle
• Proximal to angle of rib, passes into space between innermost and internal intercostal muscles
• At mid-axillary line, gives rise to lateral cutaneous branch which perforates to supply muscles and skin of lateral trunk

a) Describe the anatomy of an intercostal nerve. (25%) Anterior primary ramus
• Continuation of intercostal nerve terminates as the anterior cutaneous branch
• Supplies skin and muscles of anterior trunk, skin overlying the sternum and rectus abdominis

a) Describe the anatomy of an intercostal nerve. (25%) Posterior primary ramus
• Runs in neurovascular bundle below the intercostal artery and vein
• Provides innervation to:
• Skin
• Paravertebral region muscles

a) Describe the anatomy of an intercostal nerve. (25%) Typical intercostal nerve
Collateral branches
- Arises at angle of the rib
- Supplies the underlying muscle
Lateral cutaneous branch
- Arises from mid-axillary line
- Supplies sensation to overlying
skin

a) Describe the anatomy of an intercostal nerve. (25%) Typical intercostal nerve
Anterior cutaneous branch
- Arise from anterior chest/
abdominal wall
- Supplies sensation to overlying skin
muscles

a) Describe the anatomy of an intercostal nerve. (25%) Atypical intercostal nerve
T1 : No lateral or anterior cutaneous branch
Supplies lower part of brachial plexus
T2 : Has an atypical lateral cutaneous branch: intercostal-brachial nerve
T7-T1 : Has an abdominal course
T12 :Referred to as subcostal nerve

b) How does this influence your technique of intercostal nerve blockade for a fractured rib? (35%)
• Perform block at angle of the rib at the posterior axillary line
• Nerve most superficial
• Ensures lateral cutaneous nerve is blocked
• Protects the intercostal space, thus reducing the risk of passing the needle into the lung
• Sometimes block performed anterior to this point especially above the 6th rib because of the presence of the scapula, resulting in inadequate posterior analgesia
• Bony scapula may impede access to higher (T1–7) intercostal nerves
• Risk of pneumothorax – close proximity of pleura
• A perpendicular or caudad angulation of the needle can cause the block failure; maintenance of the 20° cephalad angle increases the chances that the needle tip will be placed in close proximity to the intercostal nerve
• Beware of neurovascular bundle

c) List the complications that may arise and explain the anatomical reasons for these complications. (30%)
Complication Pneumothorax Neural/Vascular Injury LA toxicity Spinal anaesthesia Paravertebral spread
Anatomical Reason • Close proximity of parietal pleura
• Advancement into neurovascular
bundle which lies immediately inferior to rib
• Increased systemic absorption
• Dural sleeve can extend up to 8cm from the midline leading to a small risk of subarachnoid spread if needle contacts dural sleeve
• More medial injection

Intercostal Nerve Block: Indications Anaesthesia
• Chest drain insertion
• Gastrostomy insertion
• Minor thoracic/breast and upper abdominal procedures
Analgesia
• Fractured ribs
• Acute herpes zoster
• Chronic pain syndromes

Intercostal Nerve Block: Technique
Patient Position • Sitting • lateral decubitus • Prone
Landmarks
• 7th rib (lowest rib covered by angle of scapula)
• 12th rib (last rib palpable inferiorly)
• Identify inferior border of rib to be blocked
• 6-7cm lateral from spinous process (midline)

Intercostal Nerve Block: Technique
Technique • Infiltrate 1-2 mL of dilute LA S/C at
each planned injection site • Apply traction to fix skin • Advance needle 20° cephalad until
lower border of rib encountered • Walk off inferior border, skin allowed
to retract • Advance needle 2-3cm until it
punctures the innermost intercostal muscle
• After negative aspiration, inject 3-5mL of LA

Hot Topics Guidelines

Regional Anaesthesia and Patients with Abnormal Coagulation (2013)

September 2012
a) List the implications for the patient of an inadvertent wrong-sided peripheral nerve block. (25%)
b) Summarise the recommendations of the “Stop Before You Block’’ campaign and list factors that
have been identified as contributing to the performance of a wrong-sided block. (45%)
c) Define the term “never event” as described by the National Patient Safety Agency and list three never events of relevance to anaesthetic or intensive care practice. (30%)

The Management of Hip Fractures in Adults – NICE 2011

Stop Before You Block
• Wrong sided block can lead to wrong sided surgery = Never Event
• Nov’2010 – 67 inadvertent wrong sided blocks over a 15 month period
• SLAG recommended checking surgical site had been marked by surgical team before performing a peripheral nerve block
• Nottingham University Hospitals investigated 5 wrong sided blocks
• Contributing factors were:
• Distraction in anaesthetic room
• Time delay between WHO check list and performing block
• Covering up of surgical mark in an attempt to keep patients warm
STOP BEFORE YOU BLOCK CAMPAIGN We introduce a national patient safety initiative called Stop Before You Block. The campaign is aimed at reducing the incidence of inadvertent wrong-sided nerve block during regional anaesthesia. BACKGROUND Inadvertent wrong-sided peripheral nerve blocks are uncommon but can have serious consequences including complications from the unnecessary block such as nerve injury and local anaesthetic toxicity. Hospital discharge may also be delayed due to reduced mobility or dexterity. At worst, a wrong-sided nerve block may lead the team to continue to wrong-site surgery. The National Patient Safety Agency (NPSA) describe a ‘Never Event’ as a serious, largely preventable patient safety incident that should not occur if the available preventative measures have been implemented [1]. Whilst inadvertent wrong-sided nerve blocks are not yet classified by the NPSA as ‘Never Events’, they are certainly unacceptable and preventative measures are required to help reduce their incidence. In November 2010, the Safe Anaesthesia Liaison Group (SALG) published an alert highlighting details and learning points from 67 inadvertent wrong-sided nerve blocks reported via the National Reporting and Learning Service (NRLS) over a 15-month period [2]. The recommendation from this alert was to check that the surgical site had been marked by the surgical team before performing a peripheral nerve block, as per the World Health Organisation (WHO) checklist [3]. At Nottingham University Hospitals NHS Trust, we had already conducted a local investigation in response to 5 reported wrong-sided blocks during a 12-month period. Analysis revealed that in ALL of these cases the surgical site had been marked appropriately and the WHO ‘sign in’ performed correctly. We identified several important factors contributing to the performance of the wrong-sided nerve blocks that were common in most cases. These included:
Distraction in the anaesthetic room
Time delay between the WHO sign and performance of the nerve block (e.g. a femoral block performed after a difficult and time-consuming spinal anaesthetic)
Covering-up of the surgical mark with blankets in an attempt to keep the patient warm These factors were also found to be recurring themes throughout the 67 incident reports received by the NRLS. We felt that the initial advice from the SALG, whilst important, needed to be bolder and therefore introduced a local STOP BEFORE YOU BLOCK campaign. We requested that anaesthetists and operating department personnel conduct an additional ‘stop moment’; in addition to the WHO checklist, IMMEDIATELY BEFORE NEEDLE INSERTION when performing a peripheral nerve block. The conduct of the STOP BEFORE YOU BLOCK process is described below.
STOP BEFORE YOU BLOCK CAMPAIGN We introduce a national patient safety initiative called Stop Before You Block. The campaign is aimed at reducing the incidence of inadvertent wrong-sided nerve block during regional anaesthesia. BACKGROUND Inadvertent wrong-sided peripheral nerve blocks are uncommon but can have serious consequences including complications from the unnecessary block such as nerve injury and local anaesthetic toxicity. Hospital discharge may also be delayed due to reduced mobility or dexterity. At worst, a wrong-sided nerve block may lead the team to continue to wrong-site surgery. The National Patient Safety Agency (NPSA) describe a ‘Never Event’ as a serious, largely preventable patient safety incident that should not occur if the available preventative measures have been implemented [1]. Whilst inadvertent wrong-sided nerve blocks are not yet classified by the NPSA as ‘Never Events’, they are certainly unacceptable and preventative measures are required to help reduce their incidence. In November 2010, the Safe Anaesthesia Liaison Group (SALG) published an alert highlighting details and learning points from 67 inadvertent wrong-sided nerve blocks reported via the National Reporting and Learning Service (NRLS) over a 15-month period [2]. The recommendation from this alert was to check that the surgical site had been marked by the surgical team before performing a peripheral nerve block, as per the World Health Organisation (WHO) checklist [3]. At Nottingham University Hospitals NHS Trust, we had already conducted a local investigation in response to 5 reported wrong-sided blocks during a 12-month period. Analysis revealed that in ALL of these cases the surgical site had been marked appropriately and the WHO ‘sign in’ performed correctly. We identified several important factors contributing to the performance of the wrong-sided nerve blocks that were common in most cases. These included:
Distraction in the anaesthetic room
Time delay between the WHO sign and performance of the nerve block (e.g. a femoral block performed after a difficult and time-consuming spinal anaesthetic)
Covering-up of the surgical mark with blankets in an attempt to keep the patient warm These factors were also found to be recurring themes throughout the 67 incident reports received by the NRLS. We felt that the initial advice from the SALG, whilst important, needed to be bolder and therefore introduced a local STOP BEFORE YOU BLOCK campaign. We requested that anaesthetists and operating department personnel conduct an additional ‘stop moment’; in addition to the WHO checklist, IMMEDIATELY BEFORE NEEDLE INSERTION when performing a peripheral nerve block. The conduct of the STOP BEFORE YOU BLOCK process is described below.

Stop Before You Block
Recommendations
• Poster alerts in anaesthetic rooms
• WHO checklist sign in as usual
• Particular vigilance to:
• Delay between sign in and block performance
• After turning patient – block site moved relative to anaesthetist
• Distractions in anaesthetic room
• Lower limb nerve blocks are performed
• Personnel performing block do not perform blocks on a regular basis
• STOP MOMENT occurs IMMEDIATELY before needle insertion and correct site confirmed AGAIN
• Double check surgical site marking AND side of block
STOP BEFORE YOU BLOCK CAMPAIGN We introduce a national patient safety initiative called Stop Before You Block. The campaign is aimed at reducing the incidence of inadvertent wrong-sided nerve block during regional anaesthesia. BACKGROUND Inadvertent wrong-sided peripheral nerve blocks are uncommon but can have serious consequences including complications from the unnecessary block such as nerve injury and local anaesthetic toxicity. Hospital discharge may also be delayed due to reduced mobility or dexterity. At worst, a wrong-sided nerve block may lead the team to continue to wrong-site surgery. The National Patient Safety Agency (NPSA) describe a ‘Never Event’ as a serious, largely preventable patient safety incident that should not occur if the available preventative measures have been implemented [1]. Whilst inadvertent wrong-sided nerve blocks are not yet classified by the NPSA as ‘Never Events’, they are certainly unacceptable and preventative measures are required to help reduce their incidence. In November 2010, the Safe Anaesthesia Liaison Group (SALG) published an alert highlighting details and learning points from 67 inadvertent wrong-sided nerve blocks reported via the National Reporting and Learning Service (NRLS) over a 15-month period [2]. The recommendation from this alert was to check that the surgical site had been marked by the surgical team before performing a peripheral nerve block, as per the World Health Organisation (WHO) checklist [3]. At Nottingham University Hospitals NHS Trust, we had already conducted a local investigation in response to 5 reported wrong-sided blocks during a 12-month period. Analysis revealed that in ALL of these cases the surgical site had been marked appropriately and the WHO ‘sign in’ performed correctly. We identified several important factors contributing to the performance of the wrong-sided nerve blocks that were common in most cases. These included:
Distraction in the anaesthetic room
Time delay between the WHO sign and performance of the nerve block (e.g. a femoral block performed after a difficult and time-consuming spinal anaesthetic)
Covering-up of the surgical mark with blankets in an attempt to keep the patient warm These factors were also found to be recurring themes throughout the 67 incident reports received by the NRLS. We felt that the initial advice from the SALG, whilst important, needed to be bolder and therefore introduced a local STOP BEFORE YOU BLOCK campaign. We requested that anaesthetists and operating department personnel conduct an additional ‘stop moment’; in addition to the WHO checklist, IMMEDIATELY BEFORE NEEDLE INSERTION when performing a peripheral nerve block. The conduct of the STOP BEFORE YOU BLOCK process is described below.


March 2012
A 90-year-old woman sustains a fractured neck of femur following a fall. She is scheduled for surgery. a) What aspects of this patient’s care will have the highest impact on outcome? (45%) b) Outline the recommendations made by The National Institute for Heath and Clinical Excellence (2011) on the management of pain in this patient. (30%) c) What causes of a fall in this patient might impact on the anaesthetic management? (25%)

MULTIPLE CHOICE
QUESTIONS

The following nerves arise from the lumbar plexus:
a) Lateral Cutaneous Nerve of the Thigh
b) Obturator nerve
c) Tibial nerve
d) Saphenous nerve
e) Sural nerve

The following nerves arise from the lumbar plexus:
a) Lateral Cutaneous Nerve of the Thigh T
b) Obturator nerve T
c) Tibial nerve F
d) Saphenous nerve T
e) Sural nerve F

Which one of the following statements is incorrect?
a) The paravertebral space communicates laterally with
the intercostal space and medially with the intervertebral foramen
b) When performing a thoracic paravertebral block sympathetic blockade is essential for reliable postoperative analgesia
c) In a 70kg patient 5 dermatomes can safely be anaesthetised
using 5 injections, each of 5ml 0.5% bupivacaine
d) The superior aspect of the tip of the spine of T2 lies adjacent
to the transverse process of T2

Which one of the following statements is incorrect?
a) The paravertebral space communicates laterally with T
the intercostal space and medially with the intervertebral foramen
b) When performing a thoracic paravertebral block sympathetic T blockade is essential for reliable postoperative analgesia
c) In a 70kg patient 5 dermatomes can safely be anaesthetised T
using 5 injections, each of 5ml 0.5% bupivacaine
d) The superior aspect of the tip of the spine of T2 lies adjacent F
to the transverse process of T2

Regarding the properties of sound waves, which of the following statements is correct? a) ‘Wavelength’ refers to the time taken for one complete
wave cycle to occur
b) The speed of a sound wave is unrelated to the medium through
which it travels
c) Frequency is inversely related to wavelength
d) Frequency is directly related to the period
e) The SI unit of frequency is the candela

Regarding the properties of sound waves, which of the following statements is correct? a) ‘Wavelength’ refers to the time taken for one complete F
wave cycle to occur
b) The speed of a sound wave is unrelated to the medium through F
which it travels
c) Frequency is inversely related to wavelength T
d) Frequency is directly related to the period F
e) The SI unit of frequency is the candela F

Interscalene block is suitable for the following surgeries a) Shoulder arthroplasty
b) Hand surgery
c) Acromio-clavicular joint surgery
d) Sterno-clavicular joint surgery
e) Proximal humerus surgery

Interscalene block is suitable for the following surgeries a) Shoulder arthroplasty T
b) Hand surgery F
c) Acromio-clavicular joint surgery T
d) Sterno-clavicular joint surgery F
e) Proximal humerus surgery T

Before surgery, under general anaesthetic and 20 minutes after insertion of a paravertebral block a patient has a cardiac arrest. Which of the following are possible causes? a) Local anaesthetic toxicity
b) Hypotension due to sympathetic blockade
c) Anaphylaxis
d) Tension pneumothorax

Before surgery, under general anaesthetic and 20 minutes after insertion of a paravertebral block a patient has a cardiac arrest. Which of the following are possible causes? a) Local anaesthetic toxicity T
b) Hypotension due to sympathetic blockade T
c) Anaphylaxis T
d) Tension pneumothorax T

Regarding ultrasound guided interscalene block
a) The plexus may be approached with an in-plane or
out-of-plane needling technique
b) The ideal ultrasound probe frequency is 5-10 MHz
c) Out-of-plane technique is preferred for insertion
of continuous catheter techniques
d) Shallow angle to the skin aids in needle visualisation
e) On testing, loss of motor component is the most reliable
indicator of block success

Regarding ultrasound guided interscalene block
a) The plexus may be approached with an in-plane or T
out-of-plane needling technique
b) The ideal ultrasound probe frequency is 5-10 MHz F
c) Out-of-plane technique is preferred for insertion T
of continuous catheter techniques
d) Shallow angle to the skin aids in needle visualisation T
e) On testing, loss of motor component is the most reliable F
indicator of block success

Complications of lumbar plexus block include:
a) Epidural block
b) Sub arachnoid/intrathecal injection
c) Cardiovascular collapse
d) Psoas muscle haematoma
e) Renal capsular haematoma

Complications of lumbar plexus block include:
a) Epidural block T
b) Sub arachnoid/intrathecal injection T
c) Cardiovascular collapse T
d) Psoas muscle haematoma T
e) Renal capsular haematoma T

Regarding the sacral plexus
a) The sciatic nerve exits the pelvis via the greater sciatic notch
b) The superior gluteal nerve supplies gluteus maximus
c) The lateral cutaneous nerve of the thigh arises from
from the sacral plexus
d) The sciatic nerve only innervates muscles distal to the
popliteal fossa
e) The inferior gluteal nerve supplies semitendinosus and
semimembranosus

Regarding the sacral plexus
a) The sciatic nerve exits the pelvis via the greater sciatic notch T
b) The superior gluteal nerve supplies gluteus maximus F
c) The lateral cutaneous nerve of the thigh arises from F
from the sacral plexus
d) The sciatic nerve only innervates muscles distal to the F
popliteal fossa
e) The inferior gluteal nerve supplies semitendinosus and F
semimembranosus

Regarding the lumbar plexus
a) The block provides good analgesia for a fractured NOF
b) To perform the block, the patient lies prone
c) The needle insertion point is where Tuffier’s line crosses
a line drawn parallel to the spinous processes passing through
the posterior superior iliac crest
d) The standard needle depth to lumbar plexus is 8-12cm
e) If the hamstring muscles are stimulated, the needle is
too medial

Regarding the lumbar plexus
a) The block provides good analgesia for a fractured NOF T
b) To perform the block, the patient lies prone F
c) The needle insertion point is where Tuffier’s line crosses T
a line drawn parallel to the spinous processes passing through
the posterior superior iliac crest
d) The standard needle depth to lumbar plexus is 8-12cm T
e) If the hamstring muscles are stimulated, the needle is T
too medial

Which of the following are relative contraindications to thoracic paravertebral block?
a) Ipsilateral empyema
b) Mesothelioma
c) Competent adults declining the procedure
d) Previous anaphylaxis to procaine

Which of the following are relative contraindications to thoracic paravertebral block?
a) Ipsilateral empyema T
b) Mesothelioma T
c) Competent adults declining the procedure F
d) Previous anaphylaxis to procaine T

Some of the side-effects/complications of interscalene block are:
a) Hemi-diaphragmatic palsy
b) Mydriasis
c) Nasal stuffiness
d) Epidural injection
e) Ptosis

Some of the side-effects/complications of interscalene block are:
a) Hemi-diaphragmatic palsy T
b) Mydriasis F
c) Nasal stuffiness T
d) Epidural injection T
e) Ptosis T

When considering clinical ultrasound, which of the following statements are correct?
a) Clinical ultrasound uses sound waves in the frequency
range 1 – 20 MHz.
b) The average velocity of clinical ultrasound through the
soft tissues of the body is 1540 m/s
c) B-mode is the most commonly used image modality
d) Piezo-electrical materials are unaffected by pressure changes
e) The Doppler effect refers to the change in frequency for
an observer moving relative to the source of the sound wave

When considering clinical ultrasound, which of the following statements are correct?
a) Clinical ultrasound uses sound waves in the frequency T
range 1 – 20 MHz.
b) The average velocity of clinical ultrasound through the T
soft tissues of the body is 1540 m/s
c) B-mode is the most commonly used image modality T
d) Piezo-electrical materials are unaffected by pressure changes F
e) The Doppler effect refers to the change in frequency for T
an observer moving relative to the source of the sound wave

SINGLE BEST ANSWERS

You are anaesthetising a 67 year old make for a transurethral resection of a bladder tumour under general anaesthetic. Midway through the operation the surgeon complains that the patients right id moving as he resects the right side of his bladder tumour. Which of the following blocks would have been the most likely to prevent this occurring?
a) A spinal anaesthetic
b) A lumbar plexus block
c) A femoral nerve block
d) A sciatic nerve block
e) A caudal block

You are anaesthetising a 67 year old make for a transurethral resection of a bladder tumour under general anaesthetic. Midway through the operation the surgeon complains that the patients right id moving as he resects the right side of his bladder tumour. Which of the following blocks would have been the most likely to prevent this occurring?
a) A spinal anaesthetic
b) A lumbar plexus block
c) A femoral nerve block
d) A sciatic nerve block
e) A caudal block

Which of the following statements regarding approaches to blocking of the brachial plexus is TRUE?
a) The axillary approach alone is sufficient for all aspects of awake hand surgery
b) The interscalene approach blocks the plexus at the level of the trunks
c) The vertical infra-clavicular approach has the highest rate of pneumothorax
d) An advantage of the supra-clavicular approach is being more distal, phrenic nerve block is not a complication
e) The subclavian perivascular approach relies on the plexus being immediately posterior to the subclavian artery as it crosses the first rib in between scalenus anterior and medius

Which of the following statements regarding approaches to blocking of the brachial plexus is TRUE?
a) The axillary approach alone is sufficient for all aspects of awake hand surgery
b) The interscalene approach blocks the plexus at the level of the trunks
c) The vertical infra-clavicular approach has the highest rate of pneumothorax
d) An advantage of the supra-clavicular approach is being more distal, phrenic nerve block is not a complication
e) The subclavian perivascular approach relies on the plexus being immediately posterior to the subclavian artery as it crosses the first rib in between scalenus anterior and medius

Regarding the anatomy and regional anaesthesia of the lumbar plexus, the following statements are true EXCEPT which one?
a) The lumbar plexus is described as being derived from spinal nerve roots T12-L4
b) The genitofemoral nerve is of L1-2 spinal root origin
c) The lumbar plexus is embedded in the psoas major muscle
d) A lumbar plexus block combined with a proximal sciatic nerve block can provide complete anaesthesia for all leg and foot surgery
e) As the skin on the back is less sensitive, a lumbar plexus block is one which is better tolerated by patients without the need for sedation/analgesia

Regarding the anatomy and regional anaesthesia of the lumbar plexus, the following statements are true EXCEPT which one?
a) The lumbar plexus is described as being derived from spinal nerve roots T12-L4
b) The genitofemoral nerve is of L1-2 spinal root origin
c) The lumbar plexus is embedded in the psoas major muscle
d) A lumbar plexus block combined with a proximal sciatic nerve block can provide complete anaesthesia for all leg and foot surgery
e) As the skin on the back is less sensitive, a lumbar plexus block is one which is better tolerated by patients without the need for sedation/analgesia

Which one of the following statements regarding the anatomy of the brachial plexus is TRUE?
a) The median nerve derives contribution from spinal nerve roots C5 to C8
b) The upper, middle and lower trunks each have divisions that unite to form the posterior cord
c) The axillary and radial nerves are both derived from the lateral cord
d) The medial cutaneous nerves of the arm and forearm are branches of the ulnar nerve
e) The lateral cutaneous nerves of the forearm is a terminal branch of the radial nerve

Which one of the following statements regarding the anatomy of the brachial plexus is TRUE?
a) The median nerve derives contribution from spinal nerve roots C5 to C8
b) The upper, middle and lower trunks each have divisions that unite to form the posterior cord
c) The axillary and radial nerves are both derived from the lateral cord
d) The medial cutaneous nerves of the arm and forearm are branches of the ulnar nerve
e) The lateral cutaneous nerves of the forearm is a terminal branch of the radial nerve

Summary