vol. 05 no 02 apr/may/jun. 2022 - sbed
TRANSCRIPT
BRAZILIAN JOURNAL OF PAINBRAZILIAN JOURNAL OF PAINBRAZILIAN JOURNAL OF PAINBrJPBrJPBrJP
capa brjp 2018.indd 1 08/05/2018 18:29:44
Vol. 05 No 02 Apr/May/Jun. 2022
ISSN 2595-3192


Volumen 5 – nº 2April to June, 2022
Trimestral Publication
SOCIEDADE BRASILEIRA PARA O ESTUDO DA DOR
DIRECTORYBiennium 2022-2023
PresidentJose Oswaldo de Oliveira Junior
http://lattes.cnpq.br/6744087111028320Vice-President
Luci Mara Franca Correiahttp://lattes.cnpq.br/8878925882317970
Scientific DirectorCarlos Marcelo de Barros
http://lattes.cnpq.br/5222329320430188Administrative DirectorRosimary Amorim Lopes
http://lattes.cnpq.br/1147309675795073Treasurer
Isabela Azevedo Freire Santoshttp://lattes.cnpq.br/3685635024799188
SecretaryPaola Palatucci Bello
http://lattes.cnpq.br/2464550062251493
Sociedade Brasileira para o Estudo da DorAv. Conselheiro Rodrigues Alves, 937
Cj. 2 – Vila Mariana04014-012 São Paulo, SPFone: 11 5904-2881/3959
www.dor.org.brE-mail: [email protected]
Quotations of Brazilian Journal of Pain shall be abbreviated to BrJP.
BrJP is not responsible whatosever by opinions.
Advertisements published in this edition do nogenerate conflict of interests.
Indexada na LILACSIndexada na SciELO
Publication edited and produced byMWS Design – Phone: (055) 11 98767-6188
Journalist In ChargeMarcelo Sassine - Mtb 22.869
Art EditorAnete Salviano
CONTENTS
EDITORIALAre we really translating pain knowledge to clinical practice? _____________________89Estamos mesmo translacionando o conhecimento da dor para a prática clínica?Josimari Melo DeSantana
ORIGINAL ARTICLESBrief multidisciplinary intervention for chronic pain management: pilot feasibility study __________________________________________________________________91Intervenção multidisciplinar breve para manejo da dor crônica: estudo piloto de viabilidadeYasmin Cardoso Metwaly Mohamed Ali, Áquila Lopes Gouvêa, Milena Santos de Oliveira, Sara Martini, Hazem Adel Ashmawi, Marina de Góes Salvetti
Nursing actions in the management of pain related to the use of a patient-controlled analgesia pump during the postoperative period of cardiac surgery ________________96Atuação da enfermagem no gerenciamento da dor relacionada ao uso da bomba de analgesia controlada pelo paciente durante o pós-operatório de cirurgia cardíacaLisa Catherine Miranda do Santos Pereira, Siomara Tavares Fernandes Yamaguti, Tatiane Gloria da Mota
Is cell phone use associated with neck pain and disability in skills of daily activities in young adults? __________________________________________________________100Há relação entre uso do celular com dor cervical e incapacidade nas habilidades das atividades diárias em adultos jovens?Felipe Maatalani Benini, Julia Franco Guidi, Maria Thereza Campagnolo, Maria Célia Cunha Ciaccia, Flavia Renata Dantas Alves Silva Ciaccia, Vera Esteves Vagnozzi Rullo
Use of sedatives and analgesics and hospital outcomes in pediatric intensive care: a cohort study _________________________________________________________________105Uso de sedativos e analgésicos e desfechos hospitalares em terapia intensiva pediátrica: estudo de coorteTayná Vieira, Arnildo Linck-Júnior, Mauren Teresa Grubisich Mendes Tacla, Rosângela Aparecida Pimenta Ferrari, Flávia Lopes Gabani
Does anodal transcranial direct current stimulation over left motor cortex show body side pain-related difference in fibromyalgia? ______________112A estimulação transcraniana por corrente contínua anódica sobre o córtex motor esquerdo apresenta diferença na dor entre os hemicorpos na fibromialgia?Monayane Grazielly Leite Matias, Antônio Felipe Lopes Cavalcante. Karime Andrade Mescouto, Edson Meneses Silva-Filho, Abrahão Fontes Baptista, Alexandre Hideki Okano, Rodrigo Pegado
Patients with fibromyalgia present different pain phenotypes compared to patients with generalized pain ________________________________________________________119Pacientes com fibromialgia apresentam fenótipos de dor diferentes em comparação com pacientes com dor generalizadaJuliana Valentim Bittencourt, Leticia Amaral Corrêa, Márcia Cliton Bezerra, Felipe José Jandre dos Reis, Katie de Luca, Leandro Alberto Calazans Nogueira
Exercise-based and pain education program for adults with chronic low back pain in Brazilian Primary Care: feasibility study _____________________________________127Programa de exercícios físicos e educação em dor para adultos com dor lombar crônica na Atenção Primária brasileira: estudo de viabilidadeAna Ellen do Nascimento Santos, Catharina Saraiva Nobre Cacau, Ana Carla Lima Nunes, Fabianna Resende de Jesus-Moraleida
Back pain prevalence and associated factors in Brazilian Unified Health System users __ 137Prevalência de dor nas costas e fatores associados em usuários do Sistema Único de SaúdeEduardo L Caputo, Daniele Fernandes da Silva de Souza, Vitor Häfele, Fernando Carlos Vinholes Siqueira
Submitted to articles online:https://www.gnpapers.com.br/brjp/default.asp
REVIEW ARTICLESNon-pharmacological methods for pain relief during mammography: integrative review _____________________________________________143Métodos não farmacológicos para o alívio da dor durante mamografia: revisão integrativaKatherine Olga Correia Alves Santos, Clarissa Lima Franco, Caique Jordan Nunes Ribeiro, Mariangela da Silva Nunes, Maria do Carmo de Oliveira
Acute pain in the critically ill patient: revisiting the literature __________147Dor aguda no paciente crítico: revisitando a literaturaJose Mauro Vieira Junior, Laura Herranz Prinz
Comorbidity between chronic headache and depression treated with botulinum toxin: literature review ________________________________154A comorbidade entre cefaleia crônica e depressão tratada com toxina botulínica: revisão da literaturaDenis Eduardo Bertini Bo, Eduardo de Melo Carvalho Rocha
Effect of neuromuscular electrical stimulation on muscle function in chronic low back pain patients: systematic review __________________________161Efeito da estimulação elétrica neuromuscular na função muscular em pacientes com dor lombar crônica: revisão sistemáticaAlessandra Linzmeyer, Camila Amaral Coracini, Gladson Ricardo Flor Bertolini, Alberito Rodrigo Carvalho
CASES REPORTSErector spinae plane block on pain management after thoracic surgical approaches due to COVID-19 complications. Case reports ____________168Bloqueio do plano dos músculos eretores da espinha no manejo de dor pós-abordagens cirúrgicas torácicas por complicações da COVID-19. Relato de casosLeonardo de Freitas Nascimento, Felipe Chiodini Machado, Adriana Madeleine Dominguez Gaibor, Lucas Snioka Zuretti, Hazem Adel Ashmawi
Psychotherapy in the treatment of chronic refractory orofacial pain. Case reports _________________________________________________172Psicoterapia no tratamento da dor orofacial crônica refratária. Relato de casosMarianna Barbosa Yamaguchi, Maria de Fatima Vidotto Oliveira, Silvia Regina DT de Siqueira
Phenotypic analysis of discordant monozygotic twins for pain-related temporomandibular joint disorder. Case report _____________________178Análise fenotípica de gêmeas monozigóticas discordantes para disfunção temporomandibular dolorosa. Relato de casoLais Valencise Magri, Melissa de Oliveira Melchior, Graziela Valle da-Silva, Edilaine Cristina Silva Gherardi-Donato, Christie Ramos Andrade Leite-Panissi
INSTRUCTIONS TO AUTHORS _______________________________183 Instruções aos Autores
EDITOR-IN-CHIEFJosimari Melo DeSantanaFederal University of Sergipe, Aracaju, SE, [email protected]://orcid.org/0000-0003-1432-0737http://lattes.cnpq.br/9819654988177433
COEDITORSAnamaria Siriani de OliveiraUniversity of São Paulo, Ribeirão Preto, Paulo, SP, [email protected]://orcid.org/0000-0001-5854-0016http://lattes.cnpq.br/0518357370991372Anita Perpetua Carvalho Rocha de CastroFederal University of Bahia, Salvador, BA, [email protected]://orcid.org/0000-0002-2957-6770http://lattes.cnpq.br/2863282043928410Caren Serra BavarescoLutheran University of Brazil, Canoas, RS, [email protected]://orcid.org/0000-0002-0730-3632http://lattes.cnpq.br/2237714828297776Célia Maria de OliveiraFederal University of Minas Gerais, Belo Horizonte, MG, [email protected]://orcid.org/0000-0002-1937-7364http://lattes.cnpq.br/9391711154551929Durval Campos KraycheteFederal University of Bahia, Salvador, BA, [email protected]://orcid.org/0000-0001-6561-6584http://lattes.cnpq.br/6008595426904260Eduardo GrossmannFederal University of Rio Grande do Sul, Porto Alegre, RS, [email protected]://orcid.org/0000-0002-1238-1707http://lattes.cnpq.br/4470378345964718Érica Brandão de MoraesSchool of Nursing at the Fluminense Federal University, Rio de Janeiro, RJ, [email protected]://orcid.org/0000-0003-3052-158Xhttp://lattes.cnpq.br/2265220151524135Henrique Ballassini Abdalla Leopoldo Mandic College, Campinas, SP, [email protected]://orcid.org/0000-0002-7517-2830http://lattes.cnpq.br/1401215034453544Irimar de Paula Posso University of São Paulo, São Paulo, SP, [email protected]://orcid.org/0000-0003-0337-2531http://lattes.cnpq.br/5789900900585872Isabela Freire Azevedo-SantosFederal University of Sergipe, SE, Aracajú, SE, [email protected]://orcid.org/0000-0001-8836-8640http://lattes.cnpq.br/3685635024799188João Batista Santos GarciaFederal University of Maranhão, São Luiz, MA, [email protected]://orcid.org/0000-0002-3597-6471http://lattes.cnpq.br/0424234103760462Josenilia Maria Alves GomesWalter Cantidio University Hospital, Fortaleza, CE, [email protected]://orcid.org/0000-0003-1031-9472http://lattes.cnpq.br/78133384727225202Josie Resende Torres da SilvaFederal University of Alfenas, Alfenas, MG, [email protected]://orcid.org/0000-0002-6679-2675http://lattes.cnpq.br/2678112119789338Juliana Barcellos de SouzaFederal University of Santa Catarina, Florianópolis, SC, [email protected]://orcid.org/0000-0003-4657-052Xhttp://lattes.cnpq.br/0009123389533752Lia Rachel Chaves do Amaral PellosoFederal University of Mato
Grosso, Cuiabá, MT, [email protected]://orcid.org/0000-0001-9594-9371http://lattes.cnpq.br/1267225376308387Lucas Vasconcelos LimaMcGill University, [email protected]://orcid.org/0000-0001-9662-6865http://lattes.cnpq.br/4856120017158903Luci Mara França CorreiaGraduate Program at Faculdade Einstein, Curitiba, PR, [email protected]://orcid.org/0000-0002-4977-255Xhttp://lattes.cnpq.br/8878925882317970Marcelo Lourenço da SilvaFederal University of Alfenas, Alfenas, MG, [email protected]://orcid.org/0000-0003-2319-9692http://lattes.cnpq.br/3885164141313284Maria Belén Salazar PossoChristian University Foundation, Pindamonhangaba, SP, [email protected]://orcid.org/0000-0003-3221-6124http://lattes.cnpq.br/4644641106395490Mariana Arias AvilaFederal University of São Carlos, São Carlos, SP, [email protected]://orcid.org/0000-0002-5081-5326http://lattes.cnpq.br/5905617922199364Mirlane Guimarães de Melo CardosoFederal University of Amazonas, Manaus, AM, Brazil [email protected]://orcid.org/0000-0001-9739-8235http://lattes.cnpq.br/1663863759459785Rafael Krasic AlaitiUniversity of São Paulo, São Paulo, SP, [email protected]://orcid.org/0000-0003-1830-7011http://lattes.cnpq.br/2213351462207411Telma Regina Mariotto ZakkaUniversity of São Paulo, São Paulo, SP, [email protected]://orcid.org/0000-0002-3222-2244http://lattes.cnpq.br/7210747586447129Thais Cristina ChavesFederal University of São Carlos, São Carlos, SP, [email protected]://orcid.org/0000-0002-6222-4961http://lattes.cnpq.br/6332531515878207Thiago Medina BrazolotoUniversity City of São Paulo, São Paulo, SP, [email protected]://orcid.org/0000-0003-4297-3241http://lattes.cnpq.br/7245353593408839Walter Lisboa OliveiraFederal University of Sergipe, Aracaju, SE, [email protected]://orcid.org/0000-0001-5798-6737http://lattes.cnpq.br/0512185167681269
INTERNACIONAL BOARDAllen FinleyDalhousie University, Halifax, Canadá.Antoon De LaatCatholic University of Leuven, Bélgica.Gary M. HeirMedicine and Dentistry University of New Jersey, New Jersey, EUA.Jeftrey P. OkesonKentucky University, Lexington, EUA.José Manoel Castro LopesUniversity of Porto, Porto, Portugal.Lee DongchulDepartment of Anesthesiology and Pain MedicineGuwol, Dong Mamdonggu, Incheon, Coreia.Mark JensenWashington University, Washington, EUA.Ricardo Plancarte SánchezNational Institute of Cancerology, México.
EDITORIAL PRODUCTIONEditorial CoordinationEvanilde Bronholi de [email protected]

89
Scientific research in health care takes many different forms, from preclinical laboratory research (basic research), observational studies and clinical trials (clinical research) to the direct application in the population (patients). It is not safe to make the direct transition from studying individual cells or organ systems and begin tests in patients, and this is where translational research comes in. Trans-lational research is designed to link basic research and innovation in health in order to generate products such as vaccines, drugs, non-pharmacological therapies, equipments, or services and policies that can benefit the population. In this context, the objective is to apply laboratory research findings and preclinical studies to the design and development of clinical trials, as well as the adoption of the best clinical practices1,2. Although the terminology is recent, this discussion about the link between basic scientific knowledge and the development of innova-tive products and processes has its origin in ancient research practices and was established after the Human Genome Project in 1990. The discussion strengthened after the publication of an editorial in the Journal of the American Medical Association (JAMA) in 2002, where it discussed the need to apply advancements acquired through basic research to improve patient health through new knowledge in the fields of disease prevention, diagnosis, prognosis, and treatment. In 2003, the National Institute of Health (NIH) in the United States began to prioritize translational research3 and, in 2022, the International Association for the Study of Pain (IASP) launched the worldwide campaign entitled Global Year for Translating Pain Knowledge to Practice, whose objective is to raise awareness about pain knowledge and how it can benefit individuals living with pain. In addition to the new terminology, a systematization for its practice has also been developed through improved methodologies and more effective information systems, such as network systems. But how can we ensure that the discoveries generated through basic research promotes gains for the health of the human population?In more clear terms, a basic pain researcher can identify, for example, an important receptor for a particular analgesic therapy. Based on this information, translational science researchers can evaluate a range of therapeutic combinations to develop a drug or a nonphar-macological intervention that achieves the expected effect by performing evaluations in laboratory animal models and determining a protocol with suggested dose, therapeutic effect, and adverse effects or toxicity. Next, after testing the effect and safety of the therapy, applied science researchers can initiate clinical trials in humans with specific pain conditions to test the efficacy, responsiveness, and clinical safety. Although translational research is considered to be this link between basic and applied science, in most cases, there is no articulation between the two.The knowledge produced via basic science is often not well utilized, or at best, its use occurs in a very slow and not promising manner. With the advent of translational research, there is a tendency for the researcher’s work to continue with the articulation between the laboratory and the clinic.However, in the current global scenario of translational research, there is a real gap between basic research, the ready access of patients to new products and the provision of care, which results in a great challenge to be overcome. In recent years, investment in this type of research has greatly grown and several discoveries about the neuroscience of pain have occurred, but the impact on the application of new pain diagnostics and treatments has not achieved corresponding progress regarding the development of new diagnostics and long-term interventions for the treatment of chronic pain, and therapeutic milestones have not been produced in the same proportion. This is a quintessential problem, since the prevalence of people affected by chronic pain has increased greatly in all age groups, increa-sing the global economic impact of pain, and, at the same time, no major advances in pain management interventions have occurred in the last 20 years. On the other hand, there has not been as much progress in methodological strategies of translational research from the development and evaluation of preclinical models to the design and execution of clinical trials.In what proportion does pain in laboratory animals resembles the human condition? Do preclinical pain models mimic the chronic pain condition to the same magnitude as acute pain? Are we becoming accommodated to existing models? Is it not now the time to reflect and seek new methodological options for a better comprehension of new concepts in pain in order to promote effective trans-lational optimization? Are the questions being asked and answered in preclinical studies relevant for diagnostic or clinical treatment studies? Have the most appropriate and relevant questions been asked by the scientists? Has the solution of real health problems been considered in contemporary basic science? Who is asking and testing the questions? What is the level of articulation between scientists and clinicians? These questions are important, and while there are no ready-made or unique answers in the different settings, they trigger important reflections.
Are we really translating pain knowledge to clinical practice?Estamos mesmo translacionando o conhecimento da dor para a prática clínica?
© Sociedade Brasileira para o Estudo da Dor
BrJP. São Paulo, 2022 apr-jun;5(2):89-90
DOI 10.5935/2595-0118.20220033-en
EDITORIAL

90
BrJP. São Paulo, 2022 apr-jun;5(2):89-90 DeSantana JM
Despite its importance, the knowledge acquired through basic science should not be assumed ipsis litteris to promote better pa-tient care, that is, it is not possible to ensure that the phenome-na that happen in laboratory animals replicate and reproduce exactly in the same way and to the same extent in human beings with clinical pain. It is not that simple! This shallow understan-ding perhaps contributes to the failure of the translational po-tential of science. All in all, caution is needed when criticizing translational scien-ce or scientists, as different factors affecting progress need to be considered, such as the lack of relevant pain models; limited stra-tegies of evaluation; species differences between laboratory ani-mals and humans; flaws in reporting, execution, analysis, and/or interpretation of clinical trials; regulatory constraints; and diffe-rences between countries.There is no doubt that the understanding of pathophysiologi-cal mechanisms of diseases, as well as the mechanisms of action of pharmacological and non-pharmacological interventions for pain, especially chronic pain, are important and add value and safety to the clinical reasoning of professionals, as well as induce the reasoning of scientists to create new hypotheses and inves-tigations in order to generate advances in the clinical area that reflect the investment of time and financial resources.However, in the current context, probably the most adequate and viable strategy is to perform the reverse translational reaso-ning, from the verification of occurrences with the patients and, then, the proposition of pain models and assessment methods consistent with the problem-situation. This feedback thinking (from clinic to science) favors the improvement of basic science, promoting progress and effective contribution to the health of the human population. Knowledge about pain cannot die on the bench of basic science. It needs continuity to be promising and actually influence, at some point, the assistance of patients with pain. On the other
hand, although clinical decision making is based on therapeutic efficacy derived from randomized clinical trials and, to a grea-ter extent, systematic reviews with meta-analysis, the knowledge produced by basic and translational sciences are essential to pro-vide pain specialists with accurate and reliable information about not only what works and how it works, but why it works.In this sense, clinical relevance must be the priority of decision making for translational pain science researchers. Simultaneou-sly, comprehending the complexity of the phenomena and the magnitude of health problems is necessary, assuming that fu-ture advances in clinical performance in the setting of chronic pain will have to be solved by teams that involve interdiscipli-narity, in a collaborative way, by means of multiple knowled-ge and complementation of skills, as well as scientists engaged together to seek the solution to a single problem. Furthermo-re, organizations, societies, institutions, and funding agencies must encourage and induce leadership so that scientists realize and focus on the need for innovative techniques and strategies with emphasis on real clinical goals for pain management. All these factors together tend to favor the future success of trans-lational pain research.
Josimari Melo DeSantanaFederal University of Sergipe, Physical Therapy Department,
Health Sciences Postgraduate Program, Physiological Sciences Post-graduate Program. Aracaju, SE, Brazil.
http://orcid.org/0000-0003-1432-0737 E-mail: [email protected]
REFERENCES
1. Translation Research | NIOSH | CDC. www.cdc.gov. 2020-02-24.2. What is Translational Research? | UAMS Translational Research Institute”. tri.uams.edu. 3. Zerhouni EA. Translational and clinical science time for a new vision. N Engl J Med.
2005;353(15):1621-3.

91
ABSTRACT
BACKGROUND AND OBJECTIVES: Chronic pain has a ne-gative impact on the quality of life of individuals and requires multidisciplinary attention. The aim of this study was to assess the feasibility of a brief multidisciplinary intervention for the management of chronic pain.METHODS: A pilot feasibility study. The participants were in-dividuals with chronic pain. The intervention had a psychoedu-cational focus and was carried out in a group for six weeks, with a two-hour weekly meeting. Participants received education on pain management, practiced stretching and relaxation techni-ques. The intervention was applied by two nurses, a psychologist and a physical therapist. The specific objective of this study was to assess the feasibility of the intervention through indicators of acceptability and feasibility.RESULTS: Forty-eight people with chronic pain eligible to participate in the study were identified. Among the accepta-bility indicators, the acceptance rate to participate in the in-tervention was 52% and the retention rate among participants was 60%. The rate of adherence to the recommendations was moderate for walking (53.3%) and satisfactory for stretching (100%) and relaxation (73.3%). As for the feasibility indica-tors, the following aspects were considered “great”: access to
Brief multidisciplinary intervention for chronic pain management: pilot feasibility study Intervenção multidisciplinar breve para manejo da dor crônica: estudo piloto de viabilidade
Yasmin Cardoso Metwaly Mohamed Ali1, Áquila Lopes Gouvêa2, Milena Santos de Oliveira3, Sara Martini1, Hazem Adel Ashmawi4, Marina de Góes Salvetti1
Yasmin Cardoso Metwaly Mohamed Ali – https://orcid.org/0000-0001-9254-8062; Áquila Lopes Gouvêa – https://orcid.org/0000-0002-0694-4470;Milena Santos de Oliveira – https://orcid.org/0000-0002-0431-3827; Sara Martini – https://orcid.org/0000-0001-9312-9740; Hazem Adel Ashmawi – https://orcid.org/0000-0003-0957-971X; Marina de Góes Salvetti – https://orcid.org/0000-0002-4274-8709.
1. University of São Paulo, Nursing School, Medical-Surgical Nursing Department, São Paulo, SP, Brazil.2. University of São Paulo, Medicine School, Teaching Hospital Central Institute, São Paulo, SP, Brazil. 3. Federal University of São Paulo, Biosciences Department, Santos, SP, Brazil.4. University of São Paulo, Medicine School, Anesthesiology Department, São Paulo, SP, Brazil.
Submitted on May 19, 2021.Accepted for publication on May 09, 2022.Conflict of interests: none – Sponsoring sources: Coordination of Improvement of Higher Education Personnel (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - CAPES).
Correspondence to:Yasmin Cardoso Metwaly Mohamed Ali E-mail: [email protected] [email protected]
© Sociedade Brasileira para o Estudo da Dor
the intervention site (83.3%), the intervention room (66.6%), the intervention content (86.6%) and the number of sessions (46.6%). All participants (100%) suggested increasing the number of sessions.CONCLUSION: The brief multidisciplinary intervention for chronic pain management was considered feasible and should be tested and implemented in primary care services and outpatient services specialized in pain management.Keywords: Chronic pain, Cognitive behavioral therapy, Feasibi-lity studies, Health education, Pain management, Self-efficacy.
RESUMO
JUSTIFICATIVA E OBJETIVOS: A dor crônica provoca im-pacto negativo na qualidade de vida dos indivíduos e requer atenção multidisciplinar. O objetivo deste estudo foi avaliar a viabilidade de uma intervenção multidisciplinar breve para ma-nejo da dor crônica.MÉTODOS: Estudo clínico de viabilidade. Os participantes foram pessoas com dor crônica. A intervenção teve foco psicoe-ducativo e foi realizada em grupo, por seis semanas, com um en-contro semanal de duas horas. Os participantes receberam edu-cação sobre manejo da dor, praticaram alongamento e técnicas de relaxamento. A intervenção foi aplicada por duas enfermeiras, uma psicóloga e uma fisioterapeuta. O objetivo específico deste estudo foi avaliar a viabilidade da intervenção por meio de indi-cadores de aceitabilidade e viabilidade. RESULTADOS: Identificaram-se 48 pessoas com dor crônica elegíveis para participar do estudo. Entre os indicadores de acei-tabilidade, a taxa de aceitação para participar da intervenção foi de 52% e a taxa de retenção foi de 60%. A taxa de adesão às recomendações foi moderada para caminhada (53,3%) e satisfa-tória para alongamento (100%) e relaxamento (73,3%). Quan-to aos indicadores de viabilidade, foram considerados “ótimos”: o acesso ao local da intervenção (83,3%), a sala da intervenção (66,6%), o conteúdo da intervenção (86,6%) e o número de ses-sões (46,6%). Todos os participantes (100%) sugeriram aumen-tar o número de sessões.CONCLUSÃO: A intervenção multidisciplinar breve para ma-nejo da dor crônica foi considerada viável e deve ser testada e implantada em serviços de atenção primária e serviços ambulato-riais especializados no tratamento da dor.Descritores: Autoeficácia, Dor crônica, Educação em saúde, Es-tudos de viabilidade, Manejo da dor, Terapia cognitivo-compor-tamental.
BrJP. São Paulo, 2022 apr-jun;5(2):91-5
DOI 10.5935/2595-0118.20220027-en
ORIGINAL ARTICLE

92
BrJP. São Paulo, 2022 apr-jun;5(2):91-5 Ali YC, Gouvêa AL, Oliveira MS, Martini S, Ashmawi HA and Salvetti MG
INTRODUCTION
Chronic pain causes physical, emotional and social losses1-6. Stu-dies performed in different populations indicate that the preva-lence of chronic pain in adults varies between 30% and 45%1,3-7. Studies developed in Brazil show an even higher prevalence, bet-ween 29.3% and 73.3%8. Interventions with a multidisciplinary approach, educational strategies and cognitive-behavioral therapy (CBT) have shown promising results in the management of chronic pain, contribu-ting to reduce pain intensity and depressive symptoms, impro-ving functionality and the perception of self-efficacy9-14.Self-efficacy has been shown to be an important variable in the context of chronic pain, since it is associated with better pain con-trol, better functionality, and fewer depressive symptoms15-17. In addition, the strengthening of self-efficacy can contribute to the behavioral changes required for chronic pain management17,18.There are several proposals of non-pharmacological interven-tions for chronic pain management that use educational and cognitive-behavioral strategies and can contribute to strengthen patients’ self-efficacy17,18. There are intensive, long-duration, and high workload approaches10,19-22 and there are “brief ” interven-tions, of short duration and reduced workload9,23. However, the optimal duration and/or mode of delivery for these interventions is not clear. Brief interventions may have lower costs of execution and lower dropout rates across sessions, but few studies have in-vestigated this approach.Therefore, the present study’s objective was to evaluate the accep-tability and feasibility of a multidisciplinary brief intervention for chronic pain management.
METHODS
This feasibility study followed the TiDier and CONSORT 2010-Checklist24 recommendations for pilot studies or feasibility trials and used Sidani and Braden’s methodology for developing and evaluating complex health interventions25.The present study was developed at the University of São Paulo Nursing School (Escola de Enfermagem da Universidade de São Paulo – EEUSP), in partnership with the Anesthesia Division Pain Control Outpatient Clinic (Ambulatório de Controle da Dor da Divisão de Anestesia – ACDDA) of the Central Institute of the University of São Paulo Medicine School Teaching Hospital (Ins-tituto Central do Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo – ICHC-FMUSP). The non-probabilistic sample was made up of people with chronic pain of different etiologies seen at the ACDDA, interested people reached through an announcement made on the social network Facebook® and others indicated by the EEUSP community who met the inclusion criteria and agreed to participate in the brief multidisciplinary intervention called “Chronic Pain Control Pro-gram” or CPCP (Programa de Controle da Dor Crônica – PCDC).The inclusion criteria were age between 18 and 65 years, pain complaint for more than 6 months and moderate to severe pain (pain intensity according to the Verbal Numerical Rating Sca-le)26. The exclusion criteria were pain related to oncologic origins,
communication and comprehension difficulties, motor deficits, and diagnosis of dementia.All potential participants were screened for eligibility to participate in the study. Patients who met the inclusion criteria were invited to participate, and those who agreed responded to an interview conducted by a nurse.In the interview, the objectives, and procedures of the CPCP were clarified and, with the expression of interest of the patients, they were asked to sign the Free and Informed Consent Term (FICT). The interview was guided by an instrument specially developed for the study and allowed the collection of sociodemographic and clinical data to characterize the sample.
Brief multidisciplinary intervention: chronic pain control pro-gramThe brief multidisciplinary intervention called Chronic Pain Con-trol Program (CPCP) tested in this pilot study was proposed by two nurses and is described in more detail in the Intervention Ma-nual (supplementary material), developed to guide and standardi-ze the intervention delivery.The CPCP was tested over a six-week period, including a weekly two-hour meeting, totaling 12h of intervention. The activities were conducted at the EEUSP Nursing Skills Lab by four health care professionals: a nurse with a master’s degree, a nurse with a PhD in nursing and CBT enhancement, a psychologist specialized in CBT, and a physical therapist specialized in Orthopedics and Traumatolo-gy, Global Postural Reeducation, and Myofascial Therapy.Each two-hour session included one hour of educational strate-gies, 45 minutes of supervised stretching, and 15 minutes of re-laxation. The nurses and the psychologist were responsible for the educational content, relaxation technique, and cognitive-behavio-ral strategies, and the physical therapist was responsible for the guidance and supervised practice of stretching.In the first session, the CPCP, the interventionists, and the parti-cipants were presented, and personal goals were established. The participants received a kit with an educational booklet and folder about chronic pain management, a notebook, and pen for notes. In all sessions, a central theme was explored and cognitive exercises were performed, oriented to the respective theme, always related to pain control (basic physiology of pain, manifestations of chro-nic pain, physical exercise, stress, rhythm in activities, energy con-servation and sleep hygiene). The patients did homework between sessions, including notes on stressful situations and negative thoughts, which would be wor-ked on by the psychologist and nurses in the following session. The tasks helped to promote cognitive restructuring through the comprehension between thought, emotion, and behavior in the context of chronic pains.The theoretical basis for the association of the different techniques used in this intervention was the Self-efficacy Theory, proposed by Bandura27, which explains that the perception of self-efficacy is based on four sources of information: personal accomplishments, observation of experiences, verbal persuasion, and emotional state, all managed in the intervention as described below. For personal accomplishments, individual goals were set regarding new skills learned in the intervention (stretching exercises, walking,

93
Brief multidisciplinary intervention for chronic pain management: pilot feasibility study
BrJP. São Paulo, 2022 apr-jun;5(2):91-5
and relaxation techniques throughout the week). Goal attainment was monitored and valued in order to promote improvement in perceived self-efficacy. For observation of experiences, group stret-ching and relaxation exercises were performed. Performing group activities allowed the observation of colleagues overcoming the challenge of retaking or learning a new skill, which contributes to promote improvement in perceived self-efficacy. For verbal persua-sion, guidelines and educational strategies used by the interventio-nists were conducted. These reinforce the involvement with the proposed activities and promote improvement in the perception of self-efficacy. Finally, for emotional state, a relaxation technique with music and directed imagination were performed. The individuals participated in 15 minutes of relaxation in all ses-sions and were instructed to practice the technique at home with the help of soft music in order to promote improvement in percei-ved self-efficacy. In the last session, the participants evaluated the intervention using acceptability and feasibility indicators, accor-ding to the theoretical framework of Sidani and Braden25.The outcomes of the study were acceptability and feasibility of the intervention. Acceptability indicators25 were evaluated through the acceptance rate of study participation (number of invited patients who agreed to participate), patient retention rate (number of patients who completed the CPCP) and adherence rate to the intervention re-commendations (use of the relaxation technique and practice of stret-ching/walking at home, from two to three times a week). The rate of adherence to the recommendations was obtained through questions about the weekly practice frequency of the recommended activities. Participants were expected to perform the relaxation technique, stret-ching, and walking two to three times a week. The feasibility indicators25 were the human resources to deliver the intervention (qualification and training of the interventionists), the material resources required (university chairs, multimedia pro-jector, mats for stretching and relaxation practice, stereo system, notebooks, and pen for notes), the context (access to the location of the sessions, room used, content offered, and number of ses-sions), and the reach of the intervention (ability to reach the target population)25. The feasibility indicators will be presented descriptively. To evalua-te the context, a printed instrument containing questions about the following items was used: access to the location, room used for the sessions, content, and number of sessions, rated by the partici-pants as great, good, fair, and poor, as well as space for suggestions and comments on each of the evaluated items.The project was approved by the Research Ethics Committee (Co-mitê de Ética em Pesquisa – CEP) of EEUSP (opinion number 2.831.470) and of the coparticipating institution, the Teaching Hospital (Hospital das Clínicas) of FMUSP (opinion number 3.339.401).
RESULTS
During the recruitment and selection period, 202 people were evaluated in order to be included in the study. Of these, 48 met the criteria and declared interest in participating. The interven-tion was applied to two consecutive groups (G1 and G2), with 10 and 15 patients, respectively, totaling 25 participants.
The analysis of the characteristics of the program participants (n=25) showed that 88% were women with a mean age of 55 years, living without a partner (52%) and with a mean pain du-ration of 10 years. The most frequent diagnoses were fibromyal-gia, bursitis, arthrosis, herniated disc, and rheumatoid arthritis. It is worth mentioning that 60% were unemployed, away from work or retired, most were sedentary (80%), and the average sleep time was of 5 hours and 30 minutes. The analysis of the acceptability indicators showed that, among the 48 patients invited, 25 attended one or more sessions of the intervention, characterizing an acceptance rate of 52%. Of the-se, 15 completed at least 5 sessions of the CPCP, resulting in a retention rate of 60%. The main reasons reported for failure to complete the program were personal commitments (caring for family members, court hearings, and previously scheduled travels), incompatibility with work schedules, severe pain, and financial difficulties to afford the transportation ticket costs.The adherence rate to the intervention recommendations (per-form the learned skills from two to three times a week at home) was 73.3% for the relaxation technique, 100% for stretching, and 53.3% for walking.The analysis of the feasibility indicators showed that the human resources available for the delivery of the intervention presented adequate availability and qualification, since the interventionists were present in all sessions and had experience in the area of pain, with training compatible with the objectives of the intervention. The training of the interventionists was standardized and occurred based on the Intervention Manual prepared by the nurses, who trained the other psychology and physical therapy professionals.The material resources available for the delivery of the interven-tion were university chairs, support table, mats, notebook, multi-media projector, USB flash drive, flipchart, colored pens for flip-chart, sound system, and CD with soft instrumental music. The educational strategies were performed using a table, notebook, projector and flash drive with a Microsoft Power Point®, which was used as a visual resource to present the planned content. The flipchart paper and pens were used for notes and schemes.For the muscle stretching activities and relaxation technique, mats and a sound system with soft music and nature sounds were used to promote a relaxing environment.The evaluation of the context of the intervention delivery showed that several items were evaluated by the participants as “great”: access to the location (83.3%), the room used for the interven-tion (66.6%), the content covered (86.6%), and the number of sessions (46.6%).Access to the location was considered adequate because of easy access to the intervention site by public transportation (buses, trains, and subway), but some participants, who lived further away from the location, reported that the time spent in transpor-tation was a negative point, generating fatigue.The room where the intervention sessions took place was con-sidered adequate, clean, and comfortable by most participants. However, one participant considered that the room was hot, and three said that the room was too small for practicing stretching. The content covered was considered great by all participants (100%), with reports that the learning was indeed impactful in

94
BrJP. São Paulo, 2022 apr-jun;5(2):91-5 Ali YC, Gouvêa AL, Oliveira MS, Martini S, Ashmawi HA and Salvetti MG
their lives due to the change in thoughts regarding the way they see the world and themselves. The new knowledge and skills pro-vided clarification of many doubts related to chronic pain and helped to better cope with pain. One of the participants, ho-wever, stated that he would’ve liked if the contents were deeper.Only 46.6% of the participants considered the number of ses-sions “great”, indicating that the program should have more ses-sions or could be offered continuously, because the contents were interesting and stimulated the desire to learn more about pain. Individuals reported that practicing the skills learned in a group setting was motivating, and they showed concerns of having dif-ficulties for practicing them on their own.Regarding the indicator of the intervention reach, the target population (individuals with chronic pain) was reached and the participants reported that the intervention provided a new treat-ment experience for chronic pain, in addition to the conventio-nal treatment already experienced.
DISCUSSION
The analysis of the participants’ characteristics showed a typical profile of individuals with chronic pain, with a predominance of women, mean age of 55 years old, unemployed or away from work, with pain for more than 10 years, sedentary and with impaired sleep pattern. Studies that analyzed populations with chronic pain describe a predominance of women, with ages bet-ween 40 and 58 years old, about 11 years of schooling and out of the labor market8,9,19,29,30.The mean time of pain among the participants of the present study was 10 years, similar to what is observed in other studies developed in populations with chronic pain19,21,31. Regarding the sleep pattern, the participants had around 5 hours of sleep per night, similarly to other studies on people with chronic pain32,33. A high rate of sedentary behavior was also observed, a common characteristic in populations with chronic pain34,35.In the present study, the main etiological diagnoses of pain were fibromyalgia, bursitis, arthrosis, herniated disc and arthritis, si-milar to other studies that analyzed populations with chronic pain9,21,29,30. The indicators of acceptability and feasibility of the interven-tion were positive, except for the number of sessions, which was evaluated as insufficient. This finding can be explained by the improvement in sociability and sense of belonging of the parti-cipants promoted by the group, which may have generated the desire to continue with the sessions. A similar national study, consisting of a psycho-educational program for chronic pain management applied by a multipro-fessional team, with cognitive-behavioral strategies, lasted eight weeks, with two weekly meetings and two hours long, totaling 32 hours9. The results were similar to those of the present study, which used similar strategies, but was offered briefly, lasting only 12 hours.The qualification of the interventionists in the present study was similar to that observed by other authors10,20,31. A systematic re-view that analyzed multidisciplinary interventions with educa-tion for chronic pain management highlighted that the interven-
tions were performed by at least two professionals from different disciplines, and physical therapists, psychologists and nurses were the most frequent ones31. As for the content of the intervention, pain education, cogni-tive restructuring strategies, stretching exercises and progressive muscle relaxation techniques were used, which are fundamental aspects for the quality of care of patients with pain32. Other stu-dies tested relaxation techniques, meditation and stress control in patients with chronic pain and found positive results9,33.A study that analyzed the effects of a four-week intervention with progressive muscle relaxation showed a reduction in anxiety and depression symptoms in people with chronic pain33. The sel-f-perception of the physiological state is one of the sources of information of the self-efficacy belief and it can favor the streng-thening of this belief, contributing to the success of treatment27.An intervention based on CBT that used relaxation as one of the program elements showed that the experimental group sho-wed an improvement in self-efficacy belief, which facilitated the control of chronic pain10. Stretching and relaxation techniques are elements that strengthen the intervention, providing more expressive changes, if compared to interventions that use only pain education34.The scope of the intervention was considered adequate, because it was able to reach the target population. However, the number of patients that left the program was high (40%) and should be minimized in future studies. Similar research has shown losses between 11% and 50% throughout similar programs20-22.To reduce patient losses throughout the intervention, this type of program should be offered in a location close to the partici-pants’ homes and with more than one option of time and day of the week. Studies highlight the value of group programs carried out in primary care, especially in units equipped with the Fa-mily Health Program (Estratégia Saúde da Família), because they promote health education and active participation of the indi-viduals, transforming their behavior in search of better health outcomes35-37.This study has limitations that must be noted: an unusual method for patient recruitment (Facebook® social network) was used due to the difficulty encountered in the availability and possibility of participation of ACDDA patients from ICHC-FMUSP. The difficulties reported by potential participants were related to the difficulty of access to the study location and financial difficulties to pay for transportation, which was also associated with losses throughout the intervention, resulting in a very small sample. Other limitations were that the intervention was offered on the second floor of the building and on only one day of the week, factors that may have hindered the participation of people with mobility difficulties and people who had other commitments on the dates of the intervention. Furthermore, the data collection instruments in this study were applied by the interventionists themselves, which may have influenced, in some way, the parti-cipants’ answers.The strengths of the study were the proposition of an acceptable and feasible intervention for the treatment of chronic pain, in a way that complements pharmacological treatment. This pilot study presents data that will allow refinement of the proposed

95
Brief multidisciplinary intervention for chronic pain management: pilot feasibility study
BrJP. São Paulo, 2022 apr-jun;5(2):91-5
brief multidisciplinary intervention for chronic pain manage-ment. Soon, it will be possible to test this intervention with more robust study designs and larger samples, as there are few national interventions of this nature for individuals with chronic pain.
CONCLUSION
The brief multidisciplinary intervention for chronic pain manage-ment was considered to be acceptable and feasible for patients with chronic pain and should be tested in larger samples, with more robust methods, in primary care or specialized outpatient services.
AUTHORS’ CONTRIBUTIONS
Yasmin Cardoso Metwaly Mohamed Ali Funding acquisition, Data Collection, Conceptualization, Re-source Management, Project Management, Research, Methodo-logy, Writing - Preparation of the original, Writing - Review and Editing, Supervision, Visualization Áquila Lopes Gouvea Conceptualization, Research, Validation Milena Santos de Oliveira Data Collection, Conceptualization, Research Sara Martini Data Collection, Research Hazem Adel Ashmawi Resource Management and final text reviewMarina de Góes Salvetti Conceptualization, Project Management, Methodology, Writing - Preparation of the original, Writing - Review and Editing, Su-pervision, Visualization
REFERENCES
1. de Moraes Vieira EB, Garcia JB, da Silva AA, Mualem Araújo RL, Jansen RC. Prevalen-ce, characteristics, and factors associated with chronic pain with and without neuropa-thic characteristics in São Luís, Brazil. J Pain Symptom Manage. 2012;44(2):239-51.
2. Rocha JR, Karloh M, Santos AR, Sousa TR. Characterization of biopsychosocial fac-tors of patients with chronic nonspecific low back pain. BrJP. 2021;4(4):332-8.
3. Raftery MN, Sarma K, Murphy AW, De La Harpe D, Normand C, McGuire B. Chro-nic pain in the Republic of Ireland—community prevalence, psychosocial profile and predictors of pain-related disability: results from the Prevalence, Impact and Cost of Chronic Pain (PRIME) study, Part 1. Pain. 2011;152(5):1096-103.
4. Nakamura M, Toyama Y, Nishiwaki Y, Ushida T, Prevalence and characteristics of chronic musculoskeletal pain in Japan: a second survey of people with or without chronic pain. J Orthop Sci. 2014;19(2):339-50.
5. Azevedo L, Costa-Pereira A, Mendonça L, Dias C. Epidemiology of chronic pain: a population-based nationwide study on its prevalence, characteristics and associated disability in Portugal. J Pain. 2020;13(8):773-83.
6. Wong WS, Fielding R. Prevalence and characteristics of chronic pain in the general population of Hong Kong. J Pain. 2011;12(2):236-45.
7. Grol-Prokopczyk H. undefined. Sociodemographic disparities in chronic pain, based on 12-year longitudinal data. Pain. 2017;158(2):313-22.
8. Vasconcelos FH, Araújo GC. Prevalence of chronic pain in Brazil: a descriptive study. BrJP. 2018;1(2):176-9.
9. Salvetti MG, Cobelo A, Vernalha PM, Vianna CI, Canarezi LC, Calegare RG. Effects of a psychoeducational program for chronic pain management. Rev Lat Am Enferma-gem. 2012;20(5):896-902.
10. Nash V, Ponto J, Townsend C, Nelson P, Bretz MN. Cognitive behavioral the-
rapy, self-efficacy, and depression in persons with chronic pain. Pain Manag Nurs. 2020;14(4):236-43.
11. Kawi J. Chronic low back pain patients’ perceptions on self-management, self-mana-gement support, and functional ability. Pain Manag Nurs. 2020;15(1):258-64.
12. Manias E, Gibson SJ, Finch S. Testing an educational nursing intervention for pain assessment and management in older people. Pain Med. 2020;12(8):1199-215.
13. Prevost V, Delorme C, Grach M-C, Le Chvetzoff G, Hureau M. Therapeutic edu-cation in improving cancer pain management: a synthesis of available studies. Am J Hosp Palliat Care. 2020;33(6):599-612.
14. Mehlsen M, Heegaard L, Counseling L. A prospective evaluation of the chronic pain Self-Management Programme in a Danish population of chronic pain patients. Pa-tient Educ Cous. 2015;98(5):677-80.
15. Salvetti MG, Pimenta CAM. Dor crônica e a crença de auto-eficácia. Rev Esc Enferm USP. 2020;41(1):135-40.
16. Salvetti MG, Pimenta CAM, Lage L V, Oliveira-Junior JO, Rocha JO. Auto-eficácia e sintomas depressivos em doentes com dor crônica. Rev Psiq Clin. 2020;34(3):111-7.
17. Martinez-Calderon J, Meeus M, Struyf F, Luque-Suarez A. The role of self-efficacy in pain intensity, function, psychological factors, health behaviors, and quality of life in people with rheumatoid arthritis: A systematic review. Vol. 36, Physiotherapy Theory and Practice. Taylor and Francis Ltd; 2020. 21-37p.
18. Martinez-Calderon J, Zamora-Campos C, Navarro-Ledesma S, Luque-Suarez A. The role of self-efficacy on the prognosis of chronic musculoskeletal pain: a systematic review. J Pain. 2018;19(1):10-34.
19. Gagnon CM, Scholten P, Atchison J. Multidimensional patient impression of change following interdisciplinary pain management. Pain Pract. 2018;18(8):997-1010.
20. Davin S, Lapin B, Mijatovic D, Fox R, Benzel E. Comparative effectiveness of an in-terdisciplinary pain program for chronic low back pain, compared to physical therapy alone. Spine. 2019;44(24):1715-22.
21. Casey MB, Cotter N, Kelly C, Mc Elchar L, Dunne C, Neary R, et al. Exercise and acceptance and commitment therapy for chronic pain: a case series with one-year follow-up. Musculoskeletal Care. 2020;18(1):64-73.
22. Dysvik E, Kvaløy JT, Natvig GK. The effectiveness of an improved multidisciplinary pain management programme: A 6- and 12-month follow-up study. J Adv Nurs. 2012;68(5):1061-72.
23. Moraes EB, Martins Júnior FF, Silva LB, Garcia JBS, Mattos-Pimenta CA. Autoeficá-cia e medo da dor ao movimento na lombalgia crônica: uma intervenção desenvolvida por enfermeiras. Rev Gaúcha Enferm. 2021;42.e20200180.
24. Eldridge SM, Chan CL, Campbell MJ, Bond CM, Hopewell S, Thabane L, Lancaster GA. CONSORT 2010 statement: extension to randomised pilot and feasibility trials. BMJ. 2016:355.
25. Sidani S, Braden CJ. Nursing and health interventions: design, evaluation, and imple-mentation. Oxford, John Wiley & Sons. 2021.
26. Hawker GA, Mian S, Kendzerska T, French M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF. Arthritis Care Res. 2011;63(Susppl 11):S.240-52.
27. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191-215.
28. Azzi RG, Bandura A, Polydoro SA. Teoria social cognitiva. São Paulo: Artmed; 2006. 29. Souza MS, Hortense P, Napoleão AA, Stefane T. Autoeficácia, intensidade de
dor e qualidade de vida em indivíduos com dor crônica. Rev Eletronica Enferm. 2020;18:20160331.
30. Carvalho RC, Maglioni CB, Machado GB, Araújo JE. Prevalence and characteristics of chronic pain in Brazil: a national internet-based survey study. BrJP. 2020;1(4):331-8.
31. Joypaul S, Kelly F, McMillan SS, King MA. Multi-disciplinary interventions for chro-nic pain involving education: a systematic review. PLoS One. 2019;(10):e0223306.
32. Gordon DB, Watt-Watson J, Reports BB. Interprofessional pain education—with, from, and about competent, collaborative practice teams to transform pain care. Pain. 2019;3(3):1-6.
33. Suri K, Pandey M. Effect of Jacobson Progressive Muscle Relaxation (JPMR) on psychopathological problems in chronic non-malignant pain patients. Indian J Heal Wellbeing. 2018;9:(4):630-33.
34. Louw A, Zimney K, Puentedura EL, Diener I. The efficacy of pain neuroscience edu-cation on musculoskeletal pain: a systematic review of the literature. Artic Physiother Theory Pract. 2020;32(5):332-55.
35. Thorn B, Campbell L, Van Dyke BP. Literacy-adapted cognitive behavioral therapy versus education for chronic pain at low-income clinics: a randomized controlled trial. Ann Intern Med. 2020;168(7):471-80.
36. Dias VP, Silveira DT, Witt RR. Educação em Saúde: o trabalho de grupos em atenção primária. Rev APS. 2009;12(2):221-7.
37. Cervera DPP, Pereira BDM, Goulart BF. Educação em saúde: percepção dos enfer-meiros da atenção básica em Uberaba (MG). Ciên Saúde Coletiva. 2011;16(Suppl 1):1547-54.

96
BrJP. São Paulo, 2022 apr-jun;5(2):96-9
ABSTRACT
BACKGROUND AND OBJECTIVES: Acute postoperative pain affects more than 80.0% of patients and approximately 75.0% of cases are described as moderate to severe. Effective pain relief after cardiac surgery has assumed an important role with the introduction of fast track protocols, requiring better monitoring and patient education for its effectiveness. The pre-sent study’s objective was to verify if nurses have been playing an active role during pain management, so that this brings positive impacts to the patient in pain control.METHODS: A cross-sectional, descriptive study with a quanti-tative approach, with data extracted and collected from the digi-tal platform Research Electronic Data Capture in March 2020, referring to data entered in the period between October 2018 and October 2019, totaling 326 patients in the postoperative period of cardiac surgery who used the electronic patient-con-trolled analgesia pump (PCA) model CADD-Legacy PCA.RESULTS: Predominantly male subjects (73.9%), with a mean age of 59.9±14.9 years. Among the characteristics of the PCA pump, intravenous infusion (98.8%) and bolus/PCA mode (98.5%) stood out. There was adequate monitoring of vital signs in compliance in 96.6% of cases, guidance by the nurse at the time of PCA pump installation in 85.9% and pain control after suspension of the PCA pump in 94.2%. With those who had pain controlled after the end of therapy, there was a predominan-ce of pain control in 95% of patients (p=0.11).CONCLUSION: The results show that well-established proto-cols, adequate monitoring, and the correct orientation of the pa-tient regarding the use of the device, bring positive impacts after suspension of PCA.
Nursing actions in the management of pain related to the use of a patient-controlled analgesia pump during the postoperative period of cardiac surgeryAtuação da enfermagem no gerenciamento da dor relacionada ao uso da bomba de analgesia controlada pelo paciente durante o pós-operatório de cirurgia cardíaca
Lisa Catherine Miranda do Santos Pereira1, Siomara Tavares Fernandes Yamaguti1, Tatiane Gloria da Mota1
Lisa Catherine Miranda do Santos Pereira – https://orcid.org/0000-0003-0641-918X;Siomara Tavares Fernandes Yamaguti – https://orcid.org/0000-0002-0617-0372;Tatiane Gloria da Mota – https://orcid.org/0000-0001-5743-3729. 1. Heart Hospital, São Paulo, SP, Brazil. Submitted on June 08, 2021.Accepted for publication on April 06, 2022.Conflict of interests: none – Sponsoring sources: none.
Correspondence to: Lisa Catherine Miranda do Santos PereiraE-mail: [email protected]
© Sociedade Brasileira para o Estudo da Dor
Keywords: Patient controlled analgesia, Postoperative care, Tho-racic surgery.
RESUMO
JUSTIFICATIVA E OBJETIVOS: A dor aguda pós-operatória acomete mais de 80% dos pacientes e, aproximadamente, em 75% dos casos, é descrita como moderada a intensa. O alívio efetivo da dor após cirurgia cardíaca assumiu um papel importante com a introdução de protocolos de via rápida, necessitando de melhor monitoramento e educação do paciente para sua efetividade. O objetivo deste estudo foi verificar se o enfermeiro vem desempe-nhando um papel ativo durante o gerenciamento da dor, de forma que isso traga impactos positivos ao paciente no controle álgico.MÉTODOS: Trata-se de um estudo transversal, descritivo e de abordagem quantitativa, com dados coletados da plataforma di-gital Research Electronic Data Capture em março de 2020, refe-rente aos dados inseridos no período entre outubro de 2018 e outubro de 2019, totalizando 326 pacientes em pós-operatório de cirurgia cardíaca que utilizaram bomba de infusão eletrônica modelo CADD-Legacy ACP.RESULTADOS: A média de idade foi de 59,9±14,9 anos (n=326), com um público predominantemente do sexo mascu-lino (73,9%). Dentre as características de bomba de analgesia controlada pelo paciente (ACP), destacaram-se via de infusão endovenosa (98,8%) e modo bolus/ACP (98,5%). Houve moni-torização adequada de sinais vitais em conformidade em 96,6% dos casos, orientação feita pelo enfermeiro no momento da ins-talação da bomba de ACP em 85,9% e controle da dor após sus-pensão da bomba de ACP em 94,2%. Com aqueles que tiveram dor controlada após término da terapia, observou-se predomi-nância do controle álgico em 95% dos pacientes (p=0,11).CONCLUSÃO: Os resultados mostraram que protocolos bem estabelecidos, monitoramento adequado e orientação correta do paciente quanto ao uso do dispositivo trazem impactos positivos após suspensão da ACP. Descritores: Analgesia controlada pelo paciente, Cirurgia toráci-ca, Cuidados pós-operatórios.
INTRODUCTION
The definition revised by the International Association for the Study of Pain (IASP) defines pain as “an unpleasant sensory and
DOI 10.5935/2595-0118.20220018
ORIGINAL ARTICLE

97
Nursing actions in the management of pain related to the use of a patient-controlled analgesia pump during the postoperative period of cardiac surgery
BrJP. São Paulo, 2022 apr-jun;5(2):96-9
emotional experience associated with, or resembling that asso-ciated with, actual or potential tissue damage”1. Cardiac surgery, which causes significant trauma in the thoracic region due to sternotomy, is considered one of the most painful surgeries2.Considered a common phenomenon, it can cause suffering by exposing patients to unnecessary risks, and one of the predomi-nant forms is acute pain, causing changes in various physiologi-cal mechanisms, injuries to the body and organic stress, affecting more than 80% of patients and, approximately, in 75% of cases, it is described as moderate to severe, according to the pain score3. The nurses, who are with the patient at bedside, frequently are responsible for pain control. Thus, the implementation of qua-lity improvement programs for pain management is recommen-ded to improve postoperative analgesia, enabling patient satisfac-tion and reducing the incidence of chronic pain4.Effective pain relief in the period after cardiac surgery has assu-med an important role with the introduction of fast track pro-tocols. The concept of patient-controlled analgesia (PCA) ena-bles the patient to supplement analgesia according to his or her needs. PCA is commonly considered an intermittent intravenous administration of opioids under patient control (with or without a continuous infusion)2,5.The guidance plans designed by the nursing team should in-clude information and clarifications about the causes and ex-planations of pain control procedures and instructions for the use of the pump during the postoperative period, favoring the education process2,5.Thus, the present study’s objective was to verify if nurses have been playing an active role in pain management, bringing positi-ve impacts to the patient’ pain control.
METHODS
A cross-sectional, descriptive study with a quantitative approach. The study was conducted based on Strengthening the Reporting of Observational Studies in Epidemiology (STROBE)6. Data collection was performed after approval by the Research Ethics Committee of Instituição Hospital do Coração/Associação Benefi-cência Síria (Heart Hospital Institution/Syrian Charity Associa-tion), with CAAE: 30711620.5.0000.0060.Data was collected from the digital data recording and manage-ment platform Research Electronic Data Capture (RedCap) of a philanthropic hospital specialized in cardiology, located in the south-center of the city of São Paulo. The sample was extracted in March 2020, referring to data entered in the period between October 2018 and October 2019.To compose the sample, the inclusion criteria comprised: in-dividuals of both genders; aged over 18 years; who underwent cardiac surgery; who started using the electronic infusion pump model CADD-Legacy PCA; and who received pre- and/or pos-toperative monitoring. Patients who used the mechanical PCA and who underwent other surgical procedures not classified as cardiac were excluded.The database was built containing information related to the fol-lowing variables: gender, age, infusion route, prescribed moda-
lity, control of vital signs, adverse effects, administered boluses, requested boluses and nurse guidance. The information related to the variables collected is filled in by the attending nurses every 6 hours, at bedside, and registered on the PCA pump’s own form. Later, the RedCap platform is fed with data entered by the pain specialist nurse.The benefit of evaluating the nurse’s performance through this study is being able to discuss the patients’ autonomy in mana-ging their pain, since they are responsible for activating the PCA device when they have pain, and the nurses responsible for edu-cating about the use of the equipment and monitoring the use and complaints reported by the patient.The main objective of the analysis was to identify the nurse’s performance in pain management in patients using PCA in the postoperative period of cardiac surgery. The specific objectives are: to gather the profiles of patients who use this therapy, identi-fy the most prevalent characteristics of programming, verify the relationship between the nurse’s guidance and pain control after suspension of therapy and the incidence of adverse effects during use of the PCA pump.For analysis, data were extracted from the RedCap database and entered into a Microsoft Office Excel database. The variables were described in absolute and relative frequencies. Current age was presented in mean and standard deviation, as well as with the median.Aspects such as: the attending nurse’s guidance now of PCA installation and the analgesic control after the PCA suspension were evaluated, and this data was analyzed in Fisher’s Exact test. Adverse effects were not considered for analysis since the data collected was insufficient.
RESULTS
From the total of 427 patients who used the PCA pump in the period intended for collection, 326 (76%) are cardiac surgery patients, from these 326 patients there was a predominance of 73.9% males, with mean age of 59.9±14.9 years (n=326).Regarding the prevalent characteristics related to the use of PCA, the infusion routes should be mentioned, predominating among them the venous infusion route (98.8%) through central venous catheter due to the postoperative condition. As for the other rou-tes, the use of spinal erector (0.3%) and epidural route (0.9%) were observed. Regarding the prescribed modalities, the following were identi-fied: continuous; continuous + bolus (continuous infusion as-sociated with triggering as needed by the patient); and bolus/ PCA (triggering only occurs as needed by the patient). From these modalities, there was a predominance of the bolus/PCA programming, representing 98.5% of cases. As for the others, the continuous mode was used by 0.3% of the sample, and the continuous + bolus mode by 1.2% of the configurations.Among the nurse’s attributions, the monitoring of vital signs performed by the nursing team was observed, which, according to the institutional protocol, is performed every 2 hours in the first 12 hours after the device is installed and, after this period, every 4 hours. The evaluation regarding the hemodynamic mo-

98
BrJP. São Paulo, 2022 apr-jun;5(2):96-9 Pereira LC, Yamaguti ST and Mota TG
nitoring is classified as compliant, non-compliant or partially compliant. Therefore, 96.6% of the cases were compliant, 0.6% non-compliant and 2.5% partially compliant.Regarding the installation and guidance of the nurse at the mo-ment of the PCA installation in the postoperative period, it was observed that in 314 (96.3%) of the cases the device was instal-led by the nurse, and in 12 (3.7%) by the anesthesiologist. As for the guidance, 280 patients (85.9%) received the guidance from the attending nurse, and 34 (10.4%) patients reported not having received guidance at the time of installation.After the PCA pump therapy was suspended, the presence of pain control was evaluated by checking the pain records made in the last 24 hours in the institutional control sheet. It was ob-served that 307 individuals (94.2%) had controlled pain after the removal of the device. When relating the guidance of the attending nurse at the time of the PCA installation (n=280) with those who had pain control after suspension of the pump, that is, a period of 24 hours after the removal of the PCA pump, a predominance of pain control in 95% of patients (p=0.11) was observed. Adverse effects had no relevance in the analysis, since the data collected was insufficient.
DISCUSSION
Pain is a frequent symptom with a high incidence in patients submitted to cardiac surgery. Since postoperative pain can in-fluence the recovery of the patient, its control involves adapting the analgesic treatment and the needs of each individual.The PCA pump with opioids through venous, epidural or sub-cutaneous route is an analgesic method used in the postoperative period for moderate to intense pain, characterized by self-admi-nistration, which respects the individuality of each patient be-cause it offers several modalities as to its programming in order to meet the patient’s needs7.The present study observed a high prevalence of the venous route by central venous catheter (98.8%), however, what is found in the literature refers to the epidural route, which is considered the most used, because the drug, when administered, has a stable concentration in the sites of action, avoiding “peaks and valleys” in concentration and effect, as in the case of morphine, which due to its low liposolubility, when given in bolus, can lead to respiratory depression8. Nevertheless, in the institution where the study was conducted, the standard was the venous route by a central venous catheter, sin-ce the pharmacological concentration is in a smaller volume due to its high dilution, thus avoiding the incidence of adverse effects.During the use of PCA, the patient actively participates in deter-mining the bolus of analgesic that will be administered, avoiding delays when medicating, and making it possible to schedule in-tervals between doses that avoid the probability of an overdose6.The most prescribed modality was the bolus/PCA method. The definition of the infusion modality is personalized to each pa-tient according to the knowledge of their tolerance to pain and to the opioid, which goes against the literature, which no longer recommends continuous infusion. This modality is indicated only for carefully selected patients with good tolerance to opioids
and/or who will remain in an intensive care unit, as well as the use of the continuous modality associated with the bolus, which is quite controversial in the literature6.As for the monitoring of vital signs, it was observed that most cases had adequate control. In a study, it was observed that the continuous pain assessment and the systematized data recording interfered positively in the pain experience9. The intention of offering autonomy to the patient in the use of PCA is to provi-de pain control instead of creating barriers between the patient and the team that assists him/her. Managing the patient’s pain is to actively participate in the follow-up, evaluation, and ree-valuation to make the necessary adjustments in the treatment, determining its efficacy and managing adverse effects until the suspension of treatment when necessary.Monitoring adverse effects is one of the attributions of nurses when dealing with patients who use PCA. In this sample, the data collected was insufficient and the justification is due to the change of routine for monitoring and recordings in this period, i.e., the nurses were in the process of adapting to the new form and, also, to the fact that the patient was being admitted to an intensive care unit bed, and there may be underreporting of ad-verse effects.As seen in the literature, the adverse effects expected during the use of PCA include itching, nausea, vomiting, urinary retention, decreased intestinal transit, and respiratory depression10. Often one of these symptoms end up being associated to low output and surgery, which justifies the incorrect recording of adverse effects.Thus, the team must be able to recognize the adverse effects and possible complications from the use of PCA associated with opioids, knowing how to differentiate the effects caused by phar-macological use from those associated with a worsening of the condition. Therefore, it is important to work on the continuing education of the team and the patient7.Providing information about the surgical procedure and gui-dance on the proper handling of a device of such complexity is important to reduce doubts, increase positive expectations about the surgery, and thus promote elements that implement the feeling of autonomy. Postoperative pain control is an im-portant aspect of care in the surgical setting, aiming to reduce and control postoperative complications and ensure faster reco-very without suffering11.Studies that address the patient’s experience in this pain ma-nagement process and the identification of adverse effects re-ported by the patient may add to the care offered during nu-rsing care. The present study has limitations, such as the use of secondary data analysis collected in a single institution, a factor that makes it difficult to generalize the findings. For this reason, it is suggested that other studies be carried out taking these limitations into consideration.
CONCLUSION
The results show that well-established protocols, adequate mo-nitoring, and the correct guidance of the patient regarding the use of the device bring positive impacts after suspension of PCA.

99
Nursing actions in the management of pain related to the use of a patient-controlled analgesia pump during the postoperative period of cardiac surgery
BrJP. São Paulo, 2022 apr-jun;5(2):96-9
AUTHORS’ CONTRIBUTIONS
Lisa Catherine Miranda do Santos Pereira Statistical Analysis, Funding Acquisition, Data Collection, Con-ceptualization, Resource Management, Research, Methodology, Writing - Preparation of the original, Writing – Review and Edi-ting, Visualization Siomara Tavares Fernandes Yamaguti Project Management, Supervision, Validation Tatiane Gloria da Mota Conceptualization, Research, Methodology, Supervision REFERENCES
1. Raja SN, Carr DB, Cohen M, Finnerup NB, Flor H, Gibson S, et al. The revised In-ternational Association for the Study of Pain definition of pain: concepts, challenges, and compromises. Pain. 2020;161(9):1976-82.
2. Andrade EV, Barbosa MH, Barichello E. Avaliação da dor em pós-operatório de cirur-
gia cardíaca. Acta Paulista Enferm. 2010;23(2):224-9. 3. Miranda AFA, Silva LF, Caetano JA, Sousa AC, Almeida PC. Avaliação da intensidade
de dor e sinais vitais no pós-operatório de cirurgia cardíaca. Rev Esc Enferm USP. 2011;45(2):327-33.
4. Duarte SCM, Stipp MAC, Mesquita MGR, Silva MM. O cuidado de enferma-gem no pós-operatório de cirurgia cardíaca: um estudo de caso. Esc Anna Nery. 2012;16(4):657-65.
5. Souza VS, Corgozinho MM. A enfermagem na avaliação e controle da dor pós-opera-tória. Rev Cient Sena Aires. 2016;5(1):70-8.
6. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. Int J Surg. 2014;12(12):1495-9.
7. Souza DC, Alves LB. Consequências da dor pós-operatória e implicações clínicas da dor pós-operatória não tratada. Rev Dor. 2017;18(1):14-9.
8. Lima LR, Stival MM, Barbosa M, Pereira LV. Controle da dor no pós-operatório de cirurgia cardíaca: uma breve revisão. Rev Eletr Enferm. 2008;10(2):521-9.
9. Silva MAS, Pimenta CAM, Cruz DALM. Treinamento e avaliação sistematizada da dor: impacto no controle da dor do pós-operatório de cirurgia cardíaca. Rev Esc En-ferm USP, 2013; 47(1):84-92.
10. Kraychete DC, Siqueira JT, Garcia JB. Recommendations for the use of opioids in Brazil: part I. Rev Dor. 2013;14(4):295-300.
11. Lima LR, Stival MM, Barbosa M, Pereira LV. Controle da dor no pós-operatório de cirurgia cardíaca: uma breve revisão. Rev Eletr Enferm. 2008;10(2):521-9.

100
BrJP. São Paulo, 2022 apr-jun;5(2):100-4
ABSTRACT
BACKGROUND AND OBJECTIVES: Some authors correla-te incorrect head and neck postures during cell phone use with cervical pain. The objective, therefore, is to correlate the constant use of cell phones with discomfort in the cervical region and the repercussion on daily activities in college students. METHODS: Cross-sectional study carried out between July 2019 and March 2020 using the questionnaires “Smartphone Addiction Inventory Instrument”, “Neck Disability Index” and “Young Spine Questionnaire”, and also a questionnaire about demographic and socioeconomic data. The nutritional status of the participants was also evaluated and the degree of anterioriza-tion of the head was measured in relation to the spinous process of the seventh cervical.RESULTS: The average age of the participants was 18.47±0.65 years. There was a significant statistical association between Smartphone dependence and cervical pain, and adolescents with Smartphone use dependency had the highest percentages of doctor visits for cervical pain. There was no association between smartphone dependence and absence from school or not playing sports due to pain in the spine; nutritional status; the angle of the neck and the father or mother having pain in the spine. Stu-dents with smartphone use dependency had the highest percen-tages of mild to moderate disability in the skills of daily activities.CONCLUSION: Dependence on cell phone use, in this study, is related to cervical pain and disability in the skills of daily activities.Keywords: Adolescent, Cell phone, Neck pain, Screen time.
Is cell phone use associated with neck pain and disability in skills of daily activities in young adults?Há relação entre uso do celular com dor cervical e incapacidade nas habilidades das atividades diárias em adultos jovens?
Felipe Maatalani Benini1, Julia Franco Guidi1, Maria Thereza Campagnolo1, Maria Célia Cunha Ciaccia1, Flavia Renata Dantas Alves Silva Ciaccia1, Vera Esteves Vagnozzi Rullo1
Felipe Maatalani Benini – https://orcid.org/0000-0003-4684-7605;Julia Franco Guidi – https://orcid.org/0000-0001-5228-6571;Maria Thereza Campagnolo – https://orcid.org/0000-0003-4333-5284; Maria Célia Cunha Ciaccia – https://orcid.org/0000-0003-3761-5060; Flavia Renata Dantas Alves Silva Ciaccia – https://orcid.org/0000-0002-4866-5621;Vera Esteves Vagnozzi Rullo – https://orcid.org/0000-0002-4754-6612. 1. Santos School of Medical Sciences, Lusiada University Center, Department of Pediatrics, Santos, SP, Brazil.
Submitted on June 24, 2021.Accepted for publication on April 20, 2022.Conflict of interests: none – Sponsoring sources: none.
Correspondence to: Felipe Maatalani BeniniE-mail: [email protected]
© Sociedade Brasileira para o Estudo da Dor
RESUMO
JUSTIFICATIVA E OBJETIVOS: Alguns autores correlacio-nam com dor cervical posturas de cabeça e pescoço durante o uso do celular consideradas incorretas. Objetivou-se, portanto, verificar a associação do uso constante de celular com descon-forto na região cervical e repercussão nas atividades diárias em estudantes universitários.MÉTODOS: Estudo transversal realizado entre julho de 2019 e março de 2020 através da aplicação dos questionários Smar-tphone Addiction Inventory Instrument, Neck Disability Index e Young Spine Questionnaire, além de um questionário contendo dados demográficos e socioeconômicos. Foi avaliado, ainda, o estado nutricional dos participantes e mensurado o grau de ante-riorização da cabeça em relação ao processo espinhoso da sétima vértebra cervical.RESULTADOS: A média etária dos participantes foi 18,47±0,65 anos. Houve associação estatística significativa entre o uso de ce-lular com dor cervical. Os adolescentes com tempo prolongado de uso do celular foram os que apresentaram maior frequência de consulta médica por dor na região cervical. Não houve asso-ciação entre uso de celular e ausência na escola ou não praticar esporte devido a dor na coluna, o estado nutricional, o ângulo do pescoço e o fato de pai ou mãe ter dor na coluna. Os adoles-centes com dependência de celular foram os que tiveram maior frequência de incapacidade leve a moderada nas habilidades das atividades diárias. CONCLUSÃO: A dependência do celular apresentou, neste es-tudo, uma relação com dores na coluna cervical e incapacidade nas habilidades das atividades diárias.Descritores: Adolescente, Dor cervical, Telefone celular, Tempo de tela.
INTRODUCTION
Nowadays, it is very common to see a person, whatever their age, using a cell phone1. During use, one can observe that the device is usually used at waist height, causing the person to bend his/her head downwards, so that there is a constant misalignment of the head support axis and an overload on the cervical spine2. This condition led to the creation of the terms “Text Neck” and “Turtle Neck Posture”, referring to the effect that the prolonged and repetitive neck flexion position causes to the cervical spine
DOI 10.5935/2595-0118.20220023-en
ORIGINAL ARTICLE

101
Is cell phone use associated with neck pain and disability in skills of daily activities in young adults?
BrJP. São Paulo, 2022 apr-jun;5(2):100-4
while the person uses electronic devices such as cell phones, com-puters, and tablets2.Moreover, using cell phones requires the user to look downward while extending the arms forward in order to read the screen. This causes the head to involuntarily move forward to maintain balance, causing excessive anterior curvature of the lower cervical vertebrae, as well as excessive posterior curvature of the upper thoracic vertebrae, putting pressure on the cervical spine and the muscles of the cervical region3. Some authors correlate this incorrect head and neck posture with chronic musculoskeletal pain4,5. Other studies also show that the prevalence of neck pain in late adolescence is almost the same as that found in adults, and as high as the prevalence of low back pain6-8.In recent years, the general population, especially the young, has been using cell phones in an addictive manner, potentially harmful to health and frequently associated with an increase in the prevalence of pain in the cervical region7,9. However, the current literature has heterogeneous information on the subject1,10, so that the conclusion that incorrect posture re-sults in neck pain remains uncertain and highlights the need for new studies to better understand the topic.Due to the increasing number of smartphone users, especially among young people who are in the growth leap phase, as-sociated with the scarce current literature on the subject, a study to evaluate the repercussions caused using cell phones on posture and pain in the cervical region is necessary. Thus, the present study’s objective was to verify the association of constant cell phone use with discomfort in the cervical region and with repercussions in daily activities among young uni-versity students.
METHODS
The project was approved by the Ethics Committee on Hu-man Research of the Lusíada University Center (CAAE: 14122919.6.0000.5436). After the approval, first-year un-dergraduate students were invited to participate in the study. The Free and Informed Consent Term (FICT) was presented, and, after approval, the application of the questionnaires and anthropometric measurements began.The STROBE Guideline (Strengthening the Reporting of Observational studies in Epidemiology) was used to guide the conduct of the study and the manuscript preparation11.This is a cross-sectional observational study conducted from July 2019 to March 2020. University students from the Lu-síada University Center in the city of Santos, SP, were invited to participate.University students between 18 and 20 incomplete years, duly enrolled in the first year of the Medical, Physical Therapy, and Nursing courses were included in the research. These courses were initially selected from among the nine higher education courses offered by the mentioned educational institution for being the three courses with the largest number of students in the age group of interest established in the inclusion cri-teria. The afore mentioned courses contained a total of 162 students in the studied age range. Of this total, 26 students
refused to participate in the research, resulting in a sample of 136 pre-selected student participants. All students interested in participating and who met the in-clusion criteria were conducted to a room offered by the uni-versity exclusively for data collection. The exclusion criteria were applied: university students with previously diagnosed back problems (e.g., scoliosis and lordosis). None of the 136 pre-selected students presented exclusion criteria, thus the fi-nal research sample totaled 136 participants.After signing the FICT, data collection began. The variables measured in this study were: dependence of college students on the use of smartphones, disability and pain in the cervical region, head anteriorization angle, and body mass index. The following instruments were applied for data collection: Smar-tphone Addiction Inventory (SPAI), Neck Disability Index (NDI), and Young Spine Questionnaire (YSQ). In addition, anthropometric measurements were obtained (weight, height and body mass index - BMI) and measurement of head ante-riorization of the participating students.The SPAI, developed to assess the dependence of Taiwanese college students on the use of smartphones, is composed of 26 items that validate five factors: time spent, compulsive-ness, interference with daily activities, craving, and interfe-rence with sleep. The Brazilian version of SPAI (SPAI-BR) has been validated and is reliable for detecting smartphone dependence in Brazilian college students between 18 and 35 years old12. Based on the values of sensitivity (79.05%), speci-ficity (75.66%), positive predictive value (64.29%), negative predictive value (86.70%) and accuracy (76.87%), the pre-sence of nine positive responses or more was established as the cut off point for determining dependence13.Next, the NDI was applied. This instrument was created to provide information on how the pain in the cervical region has affected the ability to perform daily activities14. It is divi-ded into 10 items, four related to subjective symptoms (pain intensity, headache, concentration, and sleep), four related to daily activities (lifting things, working, driving a car, and having fun), and two related to personal care and reading. Each of the items is scored from zero to five points14. Disa-bility was classified as: absent (total score between zero and 4 points); mild (total score between 5 and 14 points); moderate (total score between 15 and 24 points); severe (total score between 25 and 34 points); and complete (total score above 34 points)15.Evaluation of pain in the cervical region was performed with a body map and complemented with the following questions based on the YSQ15: “Have you had neck pain in the past week?” (Response options were “yes” or “no”); “How often have you had neck pain?” (Response options were “very of-ten”, “frequently”, “once in a while”, “rarely”, or “never”). For bivariate analysis, the variables were dichotomized into: very often, frequently, once in a while versus rarely or never.The YSQ contains questions assessing back pain and its con-sequences. The items were tested for content comprehension and concordance between the questionnaire scores and inter-view findings from the target respondents. These preliminary
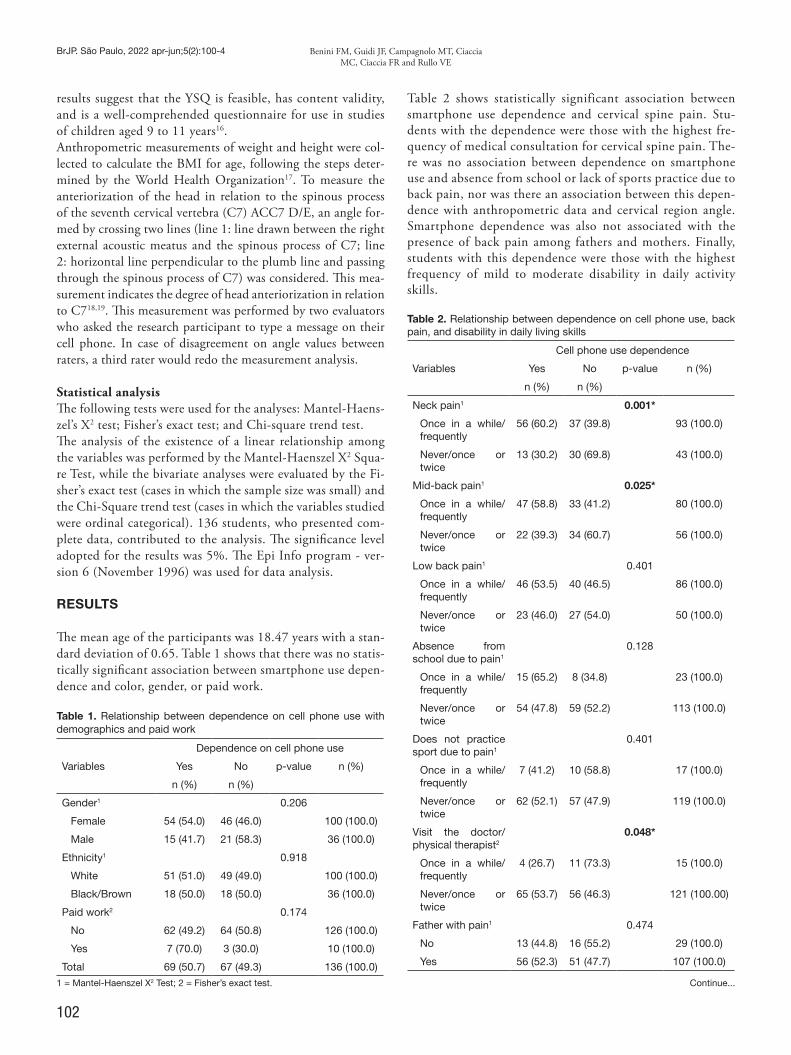
102
BrJP. São Paulo, 2022 apr-jun;5(2):100-4 Benini FM, Guidi JF, Campagnolo MT, Ciaccia MC, Ciaccia FR and Rullo VE
results suggest that the YSQ is feasible, has content validity, and is a well-comprehended questionnaire for use in studies of children aged 9 to 11 years16.Anthropometric measurements of weight and height were col-lected to calculate the BMI for age, following the steps deter-mined by the World Health Organization17. To measure the anteriorization of the head in relation to the spinous process of the seventh cervical vertebra (C7) ACC7 D/E, an angle for-med by crossing two lines (line 1: line drawn between the right external acoustic meatus and the spinous process of C7; line 2: horizontal line perpendicular to the plumb line and passing through the spinous process of C7) was considered. This mea-surement indicates the degree of head anteriorization in relation to C718,19. This measurement was performed by two evaluators who asked the research participant to type a message on their cell phone. In case of disagreement on angle values between raters, a third rater would redo the measurement analysis.
Statistical analysisThe following tests were used for the analyses: Mantel-Haens-zel’s X2 test; Fisher’s exact test; and Chi-square trend test.The analysis of the existence of a linear relationship among the variables was performed by the Mantel-Haenszel X2 Squa-re Test, while the bivariate analyses were evaluated by the Fi-sher’s exact test (cases in which the sample size was small) and the Chi-Square trend test (cases in which the variables studied were ordinal categorical). 136 students, who presented com-plete data, contributed to the analysis. The significance level adopted for the results was 5%. The Epi Info program - ver-sion 6 (November 1996) was used for data analysis.
RESULTS
The mean age of the participants was 18.47 years with a stan-dard deviation of 0.65. Table 1 shows that there was no statis-tically significant association between smartphone use depen-dence and color, gender, or paid work.
Table 1. Relationship between dependence on cell phone use with demographics and paid work
Dependence on cell phone use
Variables
Yes No p-value n (%)
n (%) n (%)
Gender1 0.206
Female 54 (54.0) 46 (46.0) 100 (100.0)
Male 15 (41.7) 21 (58.3) 36 (100.0)
Ethnicity1 0.918
White 51 (51.0) 49 (49.0) 100 (100.0)
Black/Brown 18 (50.0) 18 (50.0) 36 (100.0)
Paid work2 0.174
No 62 (49.2) 64 (50.8) 126 (100.0)
Yes 7 (70.0) 3 (30.0) 10 (100.0)
Total 69 (50.7) 67 (49.3) 136 (100.0)
1 = Mantel-Haenszel X2 Test; 2 = Fisher’s exact test.
Table 2 shows statistically significant association between smartphone use dependence and cervical spine pain. Stu-dents with the dependence were those with the highest fre-quency of medical consultation for cervical spine pain. The-re was no association between dependence on smartphone use and absence from school or lack of sports practice due to back pain, nor was there an association between this depen-dence with anthropometric data and cervical region angle. Smartphone dependence was also not associated with the presence of back pain among fathers and mothers. Finally, students with this dependence were those with the highest frequency of mild to moderate disability in daily activity skills.
Table 2. Relationship between dependence on cell phone use, back pain, and disability in daily living skills
Cell phone use dependence
Variables
Yes No p-value n (%)
n (%) n (%)
Neck pain1 0.001*
Once in a while/frequently
56 (60.2) 37 (39.8) 93 (100.0)
Never/once or twice
13 (30.2) 30 (69.8) 43 (100.0)
Mid-back pain1 0.025*
Once in a while/frequently
47 (58.8) 33 (41.2) 80 (100.0)
Never/once or twice
22 (39.3) 34 (60.7) 56 (100.0)
Low back pain1 0.401
Once in a while/frequently
46 (53.5) 40 (46.5) 86 (100.0)
Never/once or twice
23 (46.0) 27 (54.0) 50 (100.0)
Absence from school due to pain1
0.128
Once in a while/frequently
15 (65.2) 8 (34.8) 23 (100.0)
Never/once or twice
54 (47.8) 59 (52.2) 113 (100.0)
Does not practice sport due to pain1
0.401
Once in a while/frequently
7 (41.2) 10 (58.8) 17 (100.0)
Never/once or twice
62 (52.1) 57 (47.9) 119 (100.0)
Visit the doctor/physical therapist2
0.048*
Once in a while/frequently
4 (26.7) 11 (73.3) 15 (100.0)
Never/once or twice
65 (53.7) 56 (46.3) 121 (100.00)
Father with pain1 0.474
No 13 (44.8) 16 (55.2) 29 (100.0)
Yes 56 (52.3) 51 (47.7) 107 (100.0)
Continue...
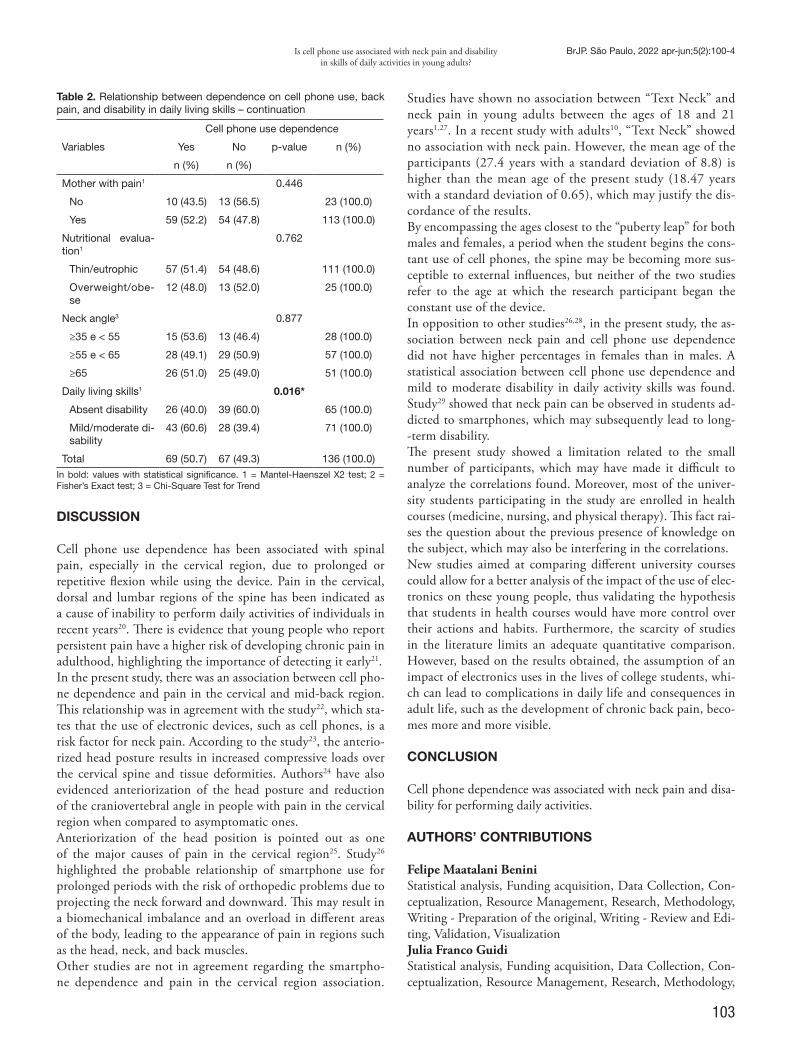
103
Is cell phone use associated with neck pain and disability in skills of daily activities in young adults?
BrJP. São Paulo, 2022 apr-jun;5(2):100-4
Cell phone use dependence
Variables
Yes No p-value n (%)
n (%) n (%)
Mother with pain1 0.446
No 10 (43.5) 13 (56.5) 23 (100.0)
Yes 59 (52.2) 54 (47.8) 113 (100.0)
Nutritional evalua-tion1
0.762
Thin/eutrophic 57 (51.4) 54 (48.6) 111 (100.0)
Overweight/obe-se
12 (48.0) 13 (52.0) 25 (100.0)
Neck angle3 0.877
≥35 e < 55 15 (53.6) 13 (46.4) 28 (100.0)
≥55 e < 65 28 (49.1) 29 (50.9) 57 (100.0)
≥65 26 (51.0) 25 (49.0) 51 (100.0)
Daily living skills1 0.016*
Absent disability 26 (40.0) 39 (60.0) 65 (100.0)
Mild/moderate di-sability
43 (60.6) 28 (39.4) 71 (100.0)
Total 69 (50.7) 67 (49.3) 136 (100.0)In bold: values with statistical significance. 1 = Mantel-Haenszel X2 test; 2 = Fisher’s Exact test; 3 = Chi-Square Test for Trend
DISCUSSION
Cell phone use dependence has been associated with spinal pain, especially in the cervical region, due to prolonged or repetitive flexion while using the device. Pain in the cervical, dorsal and lumbar regions of the spine has been indicated as a cause of inability to perform daily activities of individuals in recent years20. There is evidence that young people who report persistent pain have a higher risk of developing chronic pain in adulthood, highlighting the importance of detecting it early21.In the present study, there was an association between cell pho-ne dependence and pain in the cervical and mid-back region. This relationship was in agreement with the study22, which sta-tes that the use of electronic devices, such as cell phones, is a risk factor for neck pain. According to the study23, the anterio-rized head posture results in increased compressive loads over the cervical spine and tissue deformities. Authors24 have also evidenced anteriorization of the head posture and reduction of the craniovertebral angle in people with pain in the cervical region when compared to asymptomatic ones.Anteriorization of the head position is pointed out as one of the major causes of pain in the cervical region25. Study26 highlighted the probable relationship of smartphone use for prolonged periods with the risk of orthopedic problems due to projecting the neck forward and downward. This may result in a biomechanical imbalance and an overload in different areas of the body, leading to the appearance of pain in regions such as the head, neck, and back muscles.Other studies are not in agreement regarding the smartpho-ne dependence and pain in the cervical region association.
Studies have shown no association between “Text Neck” and neck pain in young adults between the ages of 18 and 21 years1,27. In a recent study with adults10, “Text Neck” showed no association with neck pain. However, the mean age of the participants (27.4 years with a standard deviation of 8.8) is higher than the mean age of the present study (18.47 years with a standard deviation of 0.65), which may justify the dis-cordance of the results. By encompassing the ages closest to the “puberty leap” for both males and females, a period when the student begins the cons-tant use of cell phones, the spine may be becoming more sus-ceptible to external influences, but neither of the two studies refer to the age at which the research participant began the constant use of the device.In opposition to other studies26,28, in the present study, the as-sociation between neck pain and cell phone use dependence did not have higher percentages in females than in males. A statistical association between cell phone use dependence and mild to moderate disability in daily activity skills was found. Study29 showed that neck pain can be observed in students ad-dicted to smartphones, which may subsequently lead to long--term disability.The present study showed a limitation related to the small number of participants, which may have made it difficult to analyze the correlations found. Moreover, most of the univer-sity students participating in the study are enrolled in health courses (medicine, nursing, and physical therapy). This fact rai-ses the question about the previous presence of knowledge on the subject, which may also be interfering in the correlations.New studies aimed at comparing different university courses could allow for a better analysis of the impact of the use of elec-tronics on these young people, thus validating the hypothesis that students in health courses would have more control over their actions and habits. Furthermore, the scarcity of studies in the literature limits an adequate quantitative comparison. However, based on the results obtained, the assumption of an impact of electronics uses in the lives of college students, whi-ch can lead to complications in daily life and consequences in adult life, such as the development of chronic back pain, beco-mes more and more visible.
CONCLUSION
Cell phone dependence was associated with neck pain and disa-bility for performing daily activities.
AUTHORS’ CONTRIBUTIONS
Felipe Maatalani Benini Statistical analysis, Funding acquisition, Data Collection, Con-ceptualization, Resource Management, Research, Methodology, Writing - Preparation of the original, Writing - Review and Edi-ting, Validation, Visualization Julia Franco Guidi Statistical analysis, Funding acquisition, Data Collection, Con-ceptualization, Resource Management, Research, Methodology,
Table 2. Relationship between dependence on cell phone use, back pain, and disability in daily living skills – continuation

104
BrJP. São Paulo, 2022 apr-jun;5(2):100-4 Benini FM, Guidi JF, Campagnolo MT, Ciaccia MC, Ciaccia FR and Rullo VE
Writing - Preparation of the original, Writing - Review and Edi-ting, Validation, Visualization Maria Thereza Campagnolo Statistical analysis, Funding acquisition, Data Collection, Con-ceptualization, Resource Management, Research, Methodology, Writing - Preparation of the Original, Writing - Review and Edi-ting, Validation, Visualization Maria Célia Cunha Ciaccia Statistical analysis, Funding acquisition, Data Collection, Con-ceptualization, Resource Management, Project Management, Research, Methodology, Writing - Preparation of the original, Writing - Review and Editing, Software, Supervision, Validation, Visualization Flavia Renata Dantas Alves Silva Ciaccia Statistical analysis, Conceptualization, Resource Management, Project Management, Research, Methodology, Writing - Prepa-ration of the original, Writing - Review and Editing, Software, Supervision, Validation, Visualization Vera Esteves Vagnozzi Rullo Funding acquisition, Project Management, Research, Writing - Preparation of the original, Writing - Review and Editing, Soft-ware, Supervision, Validation, Visualization
REFERENCES
1. Damasceno GM, Ferreira AS, Nogueira LAC, Reis FJJ, Andrade ICS, Mezia-t-Filho N. Text neck and neck pain in 18-21-year-old young adults. Eur Spine J. 2018;27(6):1249-54.
2. Cuéllar JM, Lanman TH. “Text neck”: an epidemic of the modern era of cell phones? Spine J. 2017;17(6):901-2.
3. Neupane S, Ali U, Matheus A. Text neck syndrome – systematic review. Imperial J Interdiscip Res. 2017(7):141-8.
4. AlAbdulwahab SS, Kachanathu SJ, AlMotairi MS. Smartphone use addiction can cau-se neck disability. Musculoskeletal Care. 2017;15(1):10-2.
5. Xie YF, Szeto G, Madeleine P, Tsang S. Spinal kinematics during smartphone texting - A comparison between young adults with and without chronic neck-shoulder pain. Appl Ergon. 2018;68:160-8.
6. Lau KT, Cheung KY, Chan KB, Lo KY, Chiu TT. Relationships between sagittal pos-tures of thoracic and cervical spine presence of neck pain, neck pain severity and disability. Man Ther. 2010;15(5):457-62.
7. Fejer R, Kyvik KO, Hartvigsen J. The prevalence of neck pain in the world popula-tion: a systematic critical review of the literature. Eur Spine J. 2016;15(6):834-48.
8. Hoy D, March L, Woolf A, Blyth F, Brooks P, Smith E, et al. The global burden of neck pain: estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis. 2014;73(7):1309-15.
9. Meziat Filho N, Azevedo e Silva G, Coutinho ES, Mendonça R, Santos V. Association between home posture habits and neck pain in High School adolescents. J Back Mus-
culoskellet Rehabil. 2017;30(3):467-75.10. Correia IM, Ferreira AS, Fernandez J, Reis FJ, Nogueira LAC, Meziat-Filho N.
Association Between Text Neck and Neck Pain in Adults. Spine (Phila Pa 1976). 2021;46(9):571-8.
11. Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344-9.
12. Lin YH, Lin YC, Lee YH, Lin PH, Lin SH, Chang LR, et al. Time distortion as-sociated with smartphone addiction: identifying smartphone addiction via a mobile application (App). J Psychiatr Res. 2015;65:139-45.
13. Kawamura T. Interpretação de um teste sob a visão epidemiológica: eficiência de um teste. Arq Bras Cardiol. 2002;79(4):437-41.
14. Vernon H, Mior S. The Neck Disability Index: A study of reliability and validity. J Manipulative Physiol Ther. 1991;14(7):409-15.
15. Falavigna A, Teles AR, Braga GL, Barazzeti DO, Lazzaretti L, Tregnago AC. Instru-mento de avaliação clínica e funcional em cirurgia da coluna vertebral. Coluna/Co-lumna. 2011;10(1):62-7.
16. Lauridsen HH, Hestbaek L. Development of the young spine questionnaire. BMC Musculoskelet Disord. 2013;14:185.
17. Agência Nacional de Saúde Suplementar. Manual de Diretrizes para o enfrentamento da Obesidade na Saúde Suplementar Brasileira. Rio de Janeiro, 2017.
18. Penha PJ, João SMA, Casarotto RA, Amino CJ, Penteado DC. Postural assessmentof girls between 7 and 10 years of age. Clinics. 2005;60(1):9-16.
19. Penha PJ, Baldini M, João SMA. Spinal Postural alignment variance accor-ding to sex and age in 7- and 8-year- old children. J Manipulative Physiol Ther. 2009;32(2):154-9.
20. Vos T, Barber RM, Bell B, Bertozzi-Villa A, Biryukov S, Bolliger I, et al. Global, regio-nal, and national incidence, prevalence, and Years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386(9995):743-800.
21. Jones GT, Silman AJ, Power C, Macfarlane GJ. Are common symptoms in childhood associated with chronic widespread body pain in adulthood? Results from the 1958 British Birth Cohort Study. Arthritis Rheum. 2007;56(5):1669-75.
22. Xie Y, Szeto G, Dai J. Prevalence and risk factors associated with musculoskeletal complaints among users of mobile handheld devices: a systematic review. Appl Ergon. 2017;59(Pt A):132-42.
23. Bonney RA, Corlett EN. Head posture and loading of the cervical spine. Appl Ergon. 2002;33(5):415-7.
24. Silva AG, Punt TD, Sharples P, Vilas-Boas JP, Johnson MI. Head posture and neck pain of chronic nontraumatic origin: a comparison between patients and pain-free persons. Arch Phys Med Rehabil. 2009;90(4):669-74.
25. Edmondston SJ, Chan HY, Ngai GC, Warren ML, Williams JM, Glennon S, et al. Postural neck pain: an investigation of habitual sitting posture, perception of ‘good’ posture and cervicothoracic kinaesthesia. Man Ther. 2007;12(4):363-71.
26. Areeudomwong P, Oapdunsalam K, Havicha Y, Tantai S, Buttagat V. Effects of shoul-der taping on discomfort and electromyographitc responses of the neck while texting on a touchscreen smartphone. Saf Health Work. 2018;9(3):319-25.
27. Saueressig IB, Oliveira VM, Xavier MK, Santos LRA, Silva KM, Araújo RC. Prevalen-ce of musculoskeletal pain in adolescents and its association with the use of electronic devices. Rev Dor. 2015;16(2):129-35.
28. Queiroz LB, Lourenço B, Silva LE, Lourenço DM, Silva CA. Musculoskeletal pain and musculoskeletal syndromes in adolescents are related to electronic. J Pediatr (Rio J). 2018;94(6):673-9.
29. Shah PP, Sheth MS. Correlation of smartphone use addiction with text neck syndro-me and SMS thumb in physiotherapy students. Int J Community Med Public Health. 2018;5(6):2512-6.

105
ABSTRACT
BACKGROUND AND OBJECTIVES: Continuous infusion sedoanalgesia may favor negative hospital outcomes, thus, the objective was to analyze the relationship between continuous infusion sedoanalgesia and factors such as duration of mecha-nical pulmonary ventilation (MPV), extubation failure, hospital infections, length of hospitalization, and death in a mixed pe-diatric intensive care unit (PICU). The aim of this study was to identify the association of the use of sedatives and analgesics in continuous infusion with hospital outcomes through the control of confounding variables.METHODS: Retrospective cohort with hospitalizations of chil-dren aged zero to 14 years, from 2012 to 2017. Use of continuous sedoanalgesia was considered a factor for the outcomes: duration of MPV, extubation failure, hospital infections (healthcare-asso-ciated infections - HCAI, fungal infection and catheter-related bloodstream infection), length of stay in the PICU and hospital, and death. Poisson regression was performed with adjustment by progressive models, with a significance level of 5%, calculation of relative risk (RR) and confidence interval (95% CI).RESULTS: A total of 894 hospitalizations were analyzed, with a predominance of males (54.3%), non-malnourished children (70.7%) and without a diagnosis of chronic disease (55.1%). Infants accounted for half of the population. The outcomes that were associated with continuous sedoanalgesia in the fi-nal model were: MPV time > 4 days (RR=2.74; 95%CI=1.90-3.93), HCAI (RR=1.91; 95%CI=.32-2.80), fungal infection
Use of sedatives and analgesics and hospital outcomes in pediatric intensive care: a cohort studyUso de sedativos e analgésicos e desfechos hospitalares em terapia intensiva pediátrica: estudo de coorte
Tayná Vieira1, Arnildo Linck-Júnior2, Mauren Teresa Grubisich Mendes Tacla1, Rosângela Aparecida Pimenta Ferrari1, Flávia Lopes Gabani1
Tayná Vieira – https://orcid.org/0000-0001-5743-7332;Arnildo Linck-Júnior – https://orcid.org/ 0000-0002-6813-019X;Mauren Teresa Grubisich Mendes Tacla – https://orcid.org/0000-0001-8928-3366;Rosângela Aparecida Pimenta Ferrari – https://orcid.org/0000-0003-0157-7461;Flávia Lopes Gabani – https://orcid.org/0000-0002-9442-4896.
1. State University of Londrina, Nursing Department, Londrina, PR, Brazil. 2. State University of Londrina, Pediatrics and Pediatric Surgery Department, Londrina, PR, Brazil.
Submitted on August 24, 2021. Accepted for publication on May 13, 2022.Conflict of interests: none – Sponsoring sources: none.
Correspondence to: Flávia Lopes Gabani E-mail: [email protected]
© Sociedade Brasileira para o Estudo da Dor
(RR=2.00; 95%CI=1.12-3.58), length of stay in the PICU > 3 days (RR=1.81; 95%CI=1.51 -2.17) and hospital stay > 10 days (RR=1.52; 95%CI=1.27-1.84), and death (RR=0.64; 95%CI=0.43-0.95).CONCLUSION: MPV time longer than four days, diagnosis of HCAI, diagnosis of fungal infection, length of stay in the PICU longer than three days, and hospitalization time longer than 10 days were factors more present in children who received continuous infu-sion of sedoanalgesia. Death, on the other hand, was more related to severity variables than to the use of psychoactive drugs. Keywords: Analgesia, Artificial ventilation, Cross infection, Deep sedation, Intensive Care Units, Length of stay.
RESUMO
JUSTIFICATIVA E OBJETIVOS: A sedoanalgesia em infusão contínua pode favorecer desfechos hospitalares negativos, assim, o objetivo foi analisar a relação entre sedoanalgesia em infusão contínua e fatores como tempo de ventilação pulmonar mecâni-ca (VPM), falha de extubação, infecções hospitalares, tempo de internação e óbito numa unidade de terapia intensiva pediátrica (UTIP) mista. Este estudo buscou identificar a associação do uso de sedativos e analgésicos em infusão contínua com desfechos hospitalares por meio do controle de variáveis de confusão.MÉTODOS: Coorte retrospectivo com internações de crianças de zero a 14 anos, de 2012 a 2017. Uso de sedoanalgesia contínua foi considerado fator para os desfechos tempo de VPM, falha de ex-tubação, infecções hospitalares (infecções relacionadas à assistência à saúde - IRAS, infecção fúngica e infecção de corrente sanguínea relacionada a cateter), tempo de internação em UTIP e no hospital e óbito. Foi realizada a regressão de Poisson com ajuste por mode-los progressivos com nível de significância de 5%, cálculo do risco relativo (RR) e intervalo de confiança (IC 95%). RESULTADOS: Foram analisadas 894 internações, predo-minando o sexo masculino (54,3%), crianças não desnutridas (70,7%) e sem diagnóstico de doença crônica (55,1%). Lac-tentes representaram metade da população. Os desfechos que se associaram à sedoanalgesia contínua no modelo final foram: tempo de VPM > 4 dias (RR=2,74; IC95%=1,90-3,93), IRAS (RR=1,91; IC95%=1,32-2,80), infecção fúngica (RR=2,00; IC95%=1,12-3,58), tempo de internação na UTIP > 3 dias (RR=1,81; IC95%=1,51-2,17) e hospitalar > 10 dias (RR=1,52; IC95%=1,27-1,84) e óbito (RR=0,64; IC95%=0,43-0,95). The aim of this study was to identify the association of the use of se-
BrJP. São Paulo, 2022 apr-jun;5(2):105-11
DOI 10.5935/2595-0118.20220030-en
ORIGINAL ARTICLE

106
BrJP. São Paulo, 2022 apr-jun;5(2):105-11 Vieira T, Linck-Júnior A, Tacla MT, Ferrari RA and Gabani FL
datives and analgesics in continuous infusion with hospital out-comes through the control of confounding variables.CONCLUSÃO: Tempo de VPM maior que quatro dias, diag-nóstico de IRAS, diagnóstico de infecção fúngica, tempo de in-ternação na UTIP maior que três dias e tempo de internação hospitalar maior que 10 dias foram mais incidentes nas crianças que receberam sedoanalgesia em infusão contínua. Já o óbito apresentou maior relação com as variáveis de gravidade do que com o uso de fármacos psicoativos. Descritores: Analgesia, Infecções nosocomiais, Sedação profun-da, Tempo de internação, Unidades de Terapia Intensiva Pediá-trica, Ventilação artificial.
INTRODUCTION
Intensive care units (ICU) are environments in which severely ill patients remain under multiprofessional care until their clinical condition improves or stabilizes. They must have technological resources for diagnosis, monitoring and treatment of the hospi-talized person. The ICU is classified according to age group as: neonatal, for patients between zero and 27 days of age; pediatric, for children between 28 days and 14 or 18 years of age; and mi-xed, when it cares for newborns and adolescents between 14 and 18 years of age, according to institutional norms1. ICU peculiarities, associated with invasive procedures inherent to the patient’s status of severity, culminate in higher levels of stress, anxiety, and agitation, especially in children2. Thus, seda-tion and analgesia are essential in the therapeutic processes of the pediatric ICU (PICU)3. However, adjusting the ideal dose in this population is a challenge due to the large difference in age groups of children admitted to PICU of mixed profile4. Sedoanalgesia can be performed continuously or intermittently, i.e., with mini-mal interval between doses. The most commonly used classes of drugs are benzodiazepines and opioids4,5. Adverse effects resulting from the continuous use of these drugs can be observed due to their cumulative effects, which result in higher incidence of withdrawal symptoms and delirium, as well as longer mechanical ventilation time and hospital stay. Howe-ver, the literature emphasizes these consequences by analyzing specific drugs and/or combinations of them4,6,7.In the case of children admitted to mixed profile PICU, com-prehending how the use of these drugs is associated with negative outcomes, regardless of the drug class, by controlling confoun-ding variables, will contribute to better direct the care provided, with the creation of protocols that allow differentiated manage-ment of these patients. Thus, the present study’s objective was to analyze the relationship between the use of continuous infusion sedoanalgesia and health outcomes in a mixed PICU.
METHODS
The study was conducted according to the international guide-lines for observational studies (Strengthening the Reporting of Observational Studies in Epidemiology - STROBE). A retros-pective cohort study composed of hospitalizations of children and adolescents from zero to 14 years of age in a tertiary care
hospital PICU, located in a city in southern Brazil. At the time of the research, the city had 36 PICU beds, of which seven were in the public network, the location of this research, and 31 in priva-te or philanthropic hospitals. The PICU studied is a reference for care provided to children and adolescents of the city and surrou-nding area, offering assistance in pediatric nephrology, child sur-gery, pediatric trauma, neurosurgery, major burns, and others.The hospitalizations covered the period between January 1st, 2012 and December 31, 2017, which were listed and provided by the hospital’s medical archive service. Cases of hospitalizations of chil-dren and adolescents who received continuous neuromuscular blockers and dissociative drugs (ketamine) intravenously were ex-cluded due to the pharmacokinetic particularities of these drugs. Infusions of sedatives and/or analgesics that lasted less than 24 hours, a period considered insufficient for association with the outcomes analyzed, were also not considered. Patients diagnosed with encephalic death were excluded for characterizing peculiar diagnostic conduct with the potential to interfere in the proposed analyses. Not located medical records and ignored information on continuous infusion of sedoanalgesia were considered losses.The variables analyzed in this research were: gender (male and female); age in years (< 1; 1 to 3; 4 to 6; 7 and more); Z-score classified according to weight measurement measured on admis-sion, by age (malnourished: < -2; non-malnourished: ≥ -2), diag-nosis of chronic disease on admission, considered as that with evolution longer than 30 days and in need of specialized pedia-tric follow-up (yes and no); main admission diagnoses, evaluated separately, such as respiratory failure, postoperative, sepsis, severe acute respiratory syndrome (SARS), and traumatic brain injury (TBI) (yes and no); need for mechanical pulmonary ventilation (MPV) (yes and no); and need for vasoactive drug (yes and no). These factors were assessed according to the need for sedatives and/or analgesics in continuous infusion (yes and no). The seda-tive drugs in this study were midazolam, thionembutal, clonidi-ne, propofol, and dexmedetomidine. Fentanyl, morphine, and remifentanil were the analgesics considered. The use of continuous sedoanalgesia (yes and no) was considered a factor for the following hospital outcomes: time of MPV, in days, according to the median (≤ 4 and > 4); extubation failure, that is, need for new tracheal intubation within 48h of withdra-wal of invasive ventilatory support (yes and no); hospital infec-tions, represented by healthcare-associated infections (HCAI), fungal infection, and catheter-related bloodstream infection (CRBI) (yes and no); length of ICU stay, according to the me-dian, greater than 3 days (yes and no); length of hospitalization, according to the median, greater than 10 days (yes and no); and death (yes and no).Data were obtained from medical records and transcribed to a form with the patients’ sociodemographic characteristics, health history, data on admission to the PICU, information on hospi-talization, and health outcomes. The data collection team was composed of nursing and medical students, as well as nursing residents in the field of child and adolescent health and medical residents in the field of pediatrics. All were trained by the resear-ch coordinators before the start of data collection. After this step, the forms were checked and coded for later typing.
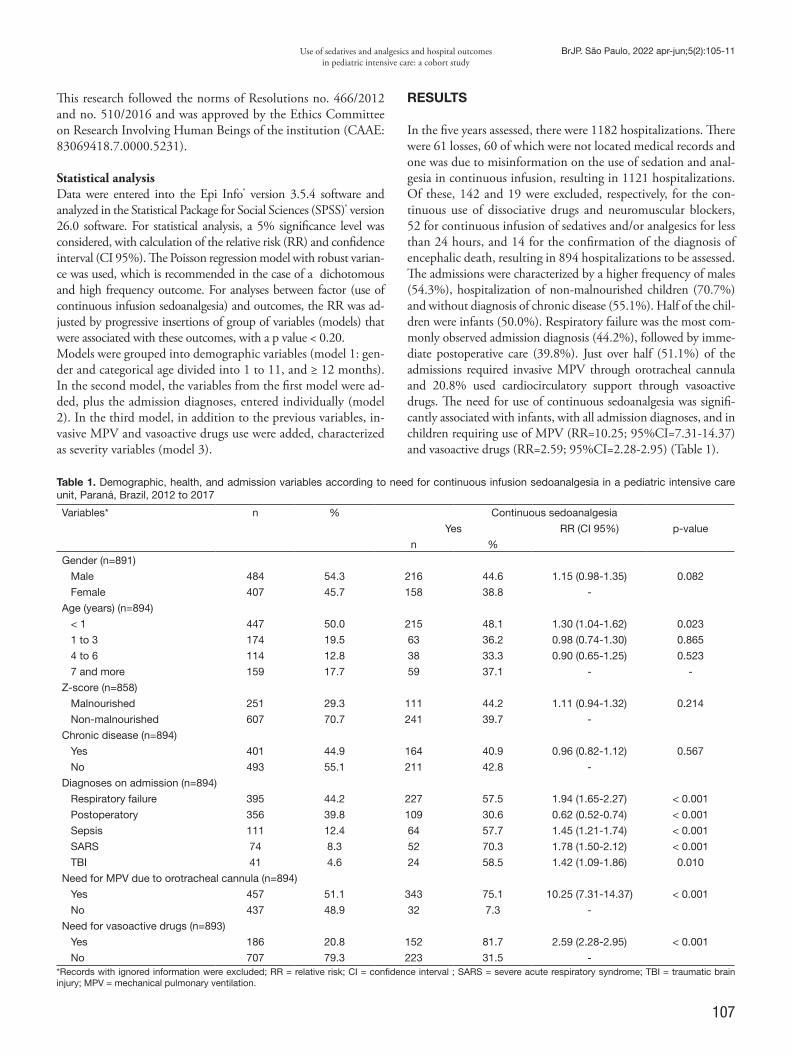
107
Use of sedatives and analgesics and hospital outcomes in pediatric intensive care: a cohort study
BrJP. São Paulo, 2022 apr-jun;5(2):105-11
This research followed the norms of Resolutions no. 466/2012 and no. 510/2016 and was approved by the Ethics Committee on Research Involving Human Beings of the institution (CAAE: 83069418.7.0000.5231).
Statistical analysisData were entered into the Epi Info® version 3.5.4 software and analyzed in the Statistical Package for Social Sciences (SPSS)® version 26.0 software. For statistical analysis, a 5% significance level was considered, with calculation of the relative risk (RR) and confidence interval (CI 95%). The Poisson regression model with robust varian-ce was used, which is recommended in the case of a dichotomous and high frequency outcome. For analyses between factor (use of continuous infusion sedoanalgesia) and outcomes, the RR was ad-justed by progressive insertions of group of variables (models) that were associated with these outcomes, with a p value < 0.20. Models were grouped into demographic variables (model 1: gen-der and categorical age divided into 1 to 11, and ≥ 12 months). In the second model, the variables from the first model were ad-ded, plus the admission diagnoses, entered individually (model 2). In the third model, in addition to the previous variables, in-vasive MPV and vasoactive drugs use were added, characterized as severity variables (model 3).
RESULTS
In the five years assessed, there were 1182 hospitalizations. There were 61 losses, 60 of which were not located medical records and one was due to misinformation on the use of sedation and anal-gesia in continuous infusion, resulting in 1121 hospitalizations. Of these, 142 and 19 were excluded, respectively, for the con-tinuous use of dissociative drugs and neuromuscular blockers, 52 for continuous infusion of sedatives and/or analgesics for less than 24 hours, and 14 for the confirmation of the diagnosis of encephalic death, resulting in 894 hospitalizations to be assessed.The admissions were characterized by a higher frequency of males (54.3%), hospitalization of non-malnourished children (70.7%) and without diagnosis of chronic disease (55.1%). Half of the chil-dren were infants (50.0%). Respiratory failure was the most com-monly observed admission diagnosis (44.2%), followed by imme-diate postoperative care (39.8%). Just over half (51.1%) of the admissions required invasive MPV through orotracheal cannula and 20.8% used cardiocirculatory support through vasoactive drugs. The need for use of continuous sedoanalgesia was signifi-cantly associated with infants, with all admission diagnoses, and in children requiring use of MPV (RR=10.25; 95%CI=7.31-14.37) and vasoactive drugs (RR=2.59; 95%CI=2.28-2.95) (Table 1).
Table 1. Demographic, health, and admission variables according to need for continuous infusion sedoanalgesia in a pediatric intensive care unit, Paraná, Brazil, 2012 to 2017
Variables* n % Continuous sedoanalgesia
Yes RR (CI 95%) p-value
n %
Gender (n=891)
Male 484 54.3 216 44.6 1.15 (0.98-1.35) 0.082
Female 407 45.7 158 38.8 -
Age (years) (n=894)
< 1 447 50.0 215 48.1 1.30 (1.04-1.62) 0.023
1 to 3 174 19.5 63 36.2 0.98 (0.74-1.30) 0.865
4 to 6 114 12.8 38 33.3 0.90 (0.65-1.25) 0.523
7 and more 159 17.7 59 37.1 - -
Z-score (n=858)
Malnourished 251 29.3 111 44.2 1.11 (0.94-1.32) 0.214
Non-malnourished 607 70.7 241 39.7 -
Chronic disease (n=894)
Yes 401 44.9 164 40.9 0.96 (0.82-1.12) 0.567
No 493 55.1 211 42.8 -
Diagnoses on admission (n=894)
Respiratory failure 395 44.2 227 57.5 1.94 (1.65-2.27) < 0.001
Postoperatory 356 39.8 109 30.6 0.62 (0.52-0.74) < 0.001
Sepsis 111 12.4 64 57.7 1.45 (1.21-1.74) < 0.001
SARS 74 8.3 52 70.3 1.78 (1.50-2.12) < 0.001
TBI 41 4.6 24 58.5 1.42 (1.09-1.86) 0.010
Need for MPV due to orotracheal cannula (n=894)
Yes 457 51.1 343 75.1 10.25 (7.31-14.37) < 0.001
No 437 48.9 32 7.3 -
Need for vasoactive drugs (n=893)
Yes 186 20.8 152 81.7 2.59 (2.28-2.95) < 0.001
No 707 79.3 223 31.5 -*Records with ignored information were excluded; RR = relative risk; CI = confidence interval ; SARS = severe acute respiratory syndrome; TBI = traumatic brain injury; MPV = mechanical pulmonary ventilation.
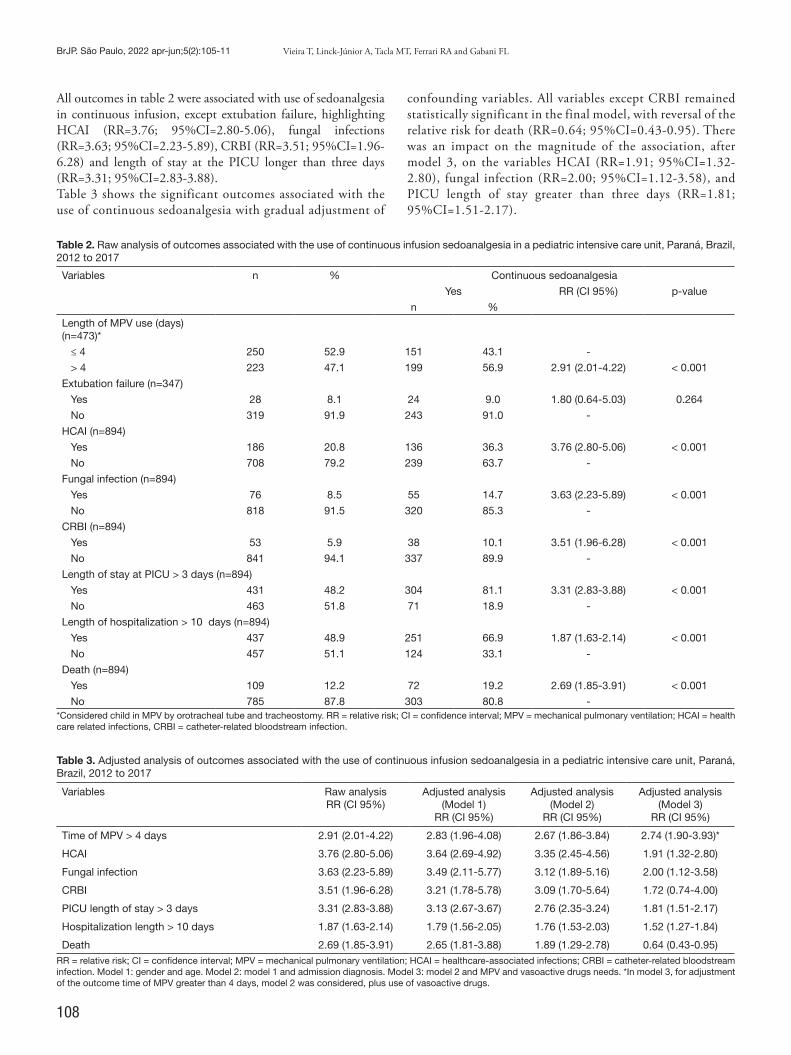
108
BrJP. São Paulo, 2022 apr-jun;5(2):105-11 Vieira T, Linck-Júnior A, Tacla MT, Ferrari RA and Gabani FL
All outcomes in table 2 were associated with use of sedoanalgesia in continuous infusion, except extubation failure, highlighting HCAI (RR=3.76; 95%CI=2.80-5.06), fungal infections (RR=3.63; 95%CI=2.23-5.89), CRBI (RR=3.51; 95%CI=1.96-6.28) and length of stay at the PICU longer than three days (RR=3.31; 95%CI=2.83-3.88).Table 3 shows the significant outcomes associated with the use of continuous sedoanalgesia with gradual adjustment of
confounding variables. All variables except CRBI remained statistically significant in the final model, with reversal of the relative risk for death (RR=0.64; 95%CI=0.43-0.95). There was an impact on the magnitude of the association, after model 3, on the variables HCAI (RR=1.91; 95%CI=1.32-2.80), fungal infection (RR=2.00; 95%CI=1.12-3.58), and PICU length of stay greater than three days (RR=1.81; 95%CI=1.51-2.17).
Table 2. Raw analysis of outcomes associated with the use of continuous infusion sedoanalgesia in a pediatric intensive care unit, Paraná, Brazil, 2012 to 2017
Variables n % Continuous sedoanalgesia
Yes RR (CI 95%) p-value
n %
Length of MPV use (days) (n=473)*
≤ 4 250 52.9 151 43.1 -
> 4 223 47.1 199 56.9 2.91 (2.01-4.22) < 0.001
Extubation failure (n=347)
Yes 28 8.1 24 9.0 1.80 (0.64-5.03) 0.264
No 319 91.9 243 91.0 -
HCAI (n=894)
Yes 186 20.8 136 36.3 3.76 (2.80-5.06) < 0.001
No 708 79.2 239 63.7 -
Fungal infection (n=894)
Yes 76 8.5 55 14.7 3.63 (2.23-5.89) < 0.001
No 818 91.5 320 85.3 -
CRBI (n=894)
Yes 53 5.9 38 10.1 3.51 (1.96-6.28) < 0.001
No 841 94.1 337 89.9 -
Length of stay at PICU > 3 days (n=894)
Yes 431 48.2 304 81.1 3.31 (2.83-3.88) < 0.001
No 463 51.8 71 18.9 -
Length of hospitalization > 10 days (n=894)
Yes 437 48.9 251 66.9 1.87 (1.63-2.14) < 0.001
No 457 51.1 124 33.1 -
Death (n=894)
Yes 109 12.2 72 19.2 2.69 (1.85-3.91) < 0.001
No 785 87.8 303 80.8 -*Considered child in MPV by orotracheal tube and tracheostomy. RR = relative risk; CI = confidence interval; MPV = mechanical pulmonary ventilation; HCAI = health care related infections, CRBI = catheter-related bloodstream infection.
Table 3. Adjusted analysis of outcomes associated with the use of continuous infusion sedoanalgesia in a pediatric intensive care unit, Paraná, Brazil, 2012 to 2017
Variables Raw analysisRR (CI 95%)
Adjusted analysis(Model 1)
RR (CI 95%)
Adjusted analysis(Model 2)
RR (CI 95%)
Adjusted analysis(Model 3)
RR (CI 95%)
Time of MPV > 4 days 2.91 (2.01-4.22) 2.83 (1.96-4.08) 2.67 (1.86-3.84) 2.74 (1.90-3.93)*
HCAI 3.76 (2.80-5.06) 3.64 (2.69-4.92) 3.35 (2.45-4.56) 1.91 (1.32-2.80)
Fungal infection 3.63 (2.23-5.89) 3.49 (2.11-5.77) 3.12 (1.89-5.16) 2.00 (1.12-3.58)
CRBI 3.51 (1.96-6.28) 3.21 (1.78-5.78) 3.09 (1.70-5.64) 1.72 (0.74-4.00)
PICU length of stay > 3 days 3.31 (2.83-3.88) 3.13 (2.67-3.67) 2.76 (2.35-3.24) 1.81 (1.51-2.17)
Hospitalization length > 10 days 1.87 (1.63-2.14) 1.79 (1.56-2.05) 1.76 (1.53-2.03) 1.52 (1.27-1.84)
Death 2.69 (1.85-3.91) 2.65 (1.81-3.88) 1.89 (1.29-2.78) 0.64 (0.43-0.95)RR = relative risk; CI = confidence interval; MPV = mechanical pulmonary ventilation; HCAI = healthcare-associated infections; CRBI = catheter-related bloodstream infection. Model 1: gender and age. Model 2: model 1 and admission diagnosis. Model 3: model 2 and MPV and vasoactive drugs needs. *In model 3, for adjustment of the outcome time of MPV greater than 4 days, model 2 was considered, plus use of vasoactive drugs.

109
Use of sedatives and analgesics and hospital outcomes in pediatric intensive care: a cohort study
BrJP. São Paulo, 2022 apr-jun;5(2):105-11
DISCUSSION
A total of 894 PICU admissions were analyzed. The need for sedoanalgesia was frequent in infants, in all analyzed admission diagnoses and in children who required MPV and vasoactive drugs. As for the outcomes, the duration of MPV use greater than four days, diagnosis of HCAI, diagnosis of fungal infection, length of stay in the PICU greater than three days and length of hospitalization greater than 10 days were more present among those who used these drugs. In the end, the use of sedatives and analgesics proved to be a protective factor for death. Continuous infusion sedoanalgesia is a common practice in in-tensive care settings, especially when there are clinical diagnoses of difficult management, requiring specific ventilatory strategies. However, the higher the dose and time of use, the higher the risk of adverse events related to these drugs5. In this context, iatrogenic abstinence stands out as a result of discontinuation of opioid and benzodiazepine drugs8. This condition, alone, can be associated with worse hospital outcomes by triggering, psycho-motor agitation, mental confusion, uncoordination for feeding, and breathing difficulty in children, among other situations that end up prolonging their length of stay in the PICU9. In this study, the greater need for psychoactive drugs in infants is consistent with the physiological disadvantages that can be aggravated in the presence of comorbidities. In addition, as it is the very characteristic of the sector to admit critically ill children who need ventilatory support and vasoactive drugs, it is expected that their use occurs more frequently, except in specific situa-tions, such as postoperative care, in which the length of stay in the sector ends up being inferior after a short observation period. Some strategies seek to minimize the adverse events of conti-nuous sedoanalgesia. The first one is the adequate choice of drugs to be used. A Chinese study, for example, compared the use of midazolam alone (Group 1) and combined with remifentanil (Group 2), concluding that satisfactory sedation was achieved in both groups, but Group 2 awoke faster and had a shorter time of extubation, duration of mechanical ventilation, and PICU stay. This is a good strategy for mechanically ventilated children to achieve better outcomes, with a lower dose for maintenance of sedation and analgesia6. Authors10 compared the sedative and anti-inflammatory effects of dexmedetomidine with midazolam in critically ill children with poly-trauma and found that dexmedetomidine decreased the level of pro-inflammatory cytokines, allowed shorter dura-tion of mechanical ventilation (4.7 days versus 6.6 days) and PICU stay (9.5 days versus 12.3 days), and reduced the propor-tion of sepsis (33.3% versus 53.1%). Another study compared the isolated use of midazolam and fentanyl (different solutions) with the combined use in the same solution and found that in the latter case there was a higher cumulative dose of these drugs, longer time of need for vasopressor drugs and a higher number of children who developed tolerance to the adopted treatment11. This study did not identify the hospital outcomes according to the drugs used, nor according to the form in which they were administered, although the service in which the data were col-lected did not adopt combined sedoanalgesia solutions. On the
other hand, the results consist of a large population of children in a PICU with a mixed profile, in which the use of sedatives and analgesics in continuous infusion, regardless of which was the chosen drug, favored longer MPV time, incidence of hospital in-fections and longer stays in the PICU and in the hospital, regar-dless of demographic factors, admission diagnosis and variables related to severity. Finding the balance between offering or restricting these drugs is a complex goal. A research performed in a PICU in the Nether-lands found a mean number of 11 painful and stressful procedu-res per patient per day. The most frequent were airway aspiration (endotracheal, oral and nasal), arterial and lumbar punctures and insertion of peripheral intravenous cannula. They also conclu-ded that mechanical ventilation patients undergo twice as many painful procedures as non-ventilated patients, and yet there is no adequate pain control in these situations12. Another study carried out in Philadelphia (USA) identified that severe children with cognitive impairment received less sedoa-nalgesia than the others, but it was not clear if there is a lower incidence of pain in this population or if there is an inadequacy of the behavioral assessment instruments in these patients regar-ding the clinical signs of discomfort13. This difficulty in assessing individual needs in pediatrics, especially due to the heterogeneity of the mixed profile PICU, according to age range, injury, and selection of safer drugs in each case, can hinder the work of pro-fessionals less experienced in clinical management in children’s intensive care environments12,14. This difficulty is also observed in the analyzed sector, because it is a teaching hospital with high turnover of professionals and less adherence to the practice of objective measurements through appropriate scales. Therefore, the indiscriminate use of certain psychoactive drugs for immediate sedoanalgesia ignores early and late pharmacological adverse effects, and its underuse has direct repercussions on the clinical and psychological condition of hospitalized children. A systematic review15 suggests that se-dation in the PICU is often not adequate to the demands of critically ill children and that there is a lack of assessment of this condition in this scenario. Excessive sedation is the most com-monly observed situation and can prolong hospitalization and increase the incidence of complications.In this research, it is noteworthy that continuous sedoanalgesia was a protective factor for death in the final adjustment model. This means that this outcome is related more to the severity con-ditions of the child than to the psychoactive drugs, which are often used as adjuvants to stabilize the clinical condition and better therapeutic management of more complex cases. A study16 recommends in its review, as a target for favorable hos-pital outcomes in PICU, the use of sedation guided by assess-ment scales, management of protocols for daily interruption of sedatives and analgesics, and assurance of spontaneous breathing tests for children under mechanic ventilation. These measures shorten the time of mechanical ventilation as well as the length of hospitalization, and help control withdrawal and delirium wi-thout increasing the risk of morbidity and mortality17.Planning the discontinuation of sedoanalgesia is as important as its use in order to reduce the incidence of negative outcomes in

110
BrJP. São Paulo, 2022 apr-jun;5(2):105-11 Vieira T, Linck-Júnior A, Tacla MT, Ferrari RA and Gabani FL
the pediatric population. Methadone, for example, is an allied drug in preventing withdrawal syndrome in patients who used opioids in continuous infusion during hospitalization, although the ideal therapeutic dose and treatment time are not so clear in the literature18. Another option to counteract the cumulative and adverse effects is drug rotation19. A study20 verified that the daily interruption of continuous psychoactive drugs in critically ill children is a viable therapeutic option that results in decreased use of sedation, favors early extubation and reduces the length of stay in the PICU. Despite the frequent use of these drugs in critically ill chil-dren, the choice must be based on criteria and evaluative sco-res to qualify care, facilitate mechanical ventilation, prevent accidental extubation, and minimize patient discomfort. A therapeutic plan should be established on an individual ba-sis, with constant review of the goals to be achieved, and the drugs should be rotated and appropriate to the children cli-nic. Strategies of regional anesthesia and analgesia controlled by the patient with appropriate cognitive conditions could reduce the need for continuous intravenous infusion and nu-rse-guided protocols should be incorporated into the routine of these sectors due to the advantages already well documen-ted in the literature5,21. There is also the possibility of titration of sedative and analge-sic agents to reach the desired therapeutic goal. These actions, together or separately, can reduce the negative impact of conti-nuous sedoanalgesia, regardless of the drug used, on the reported hospital outcomes5. In the research locus hospital, the rotation of sedatives and analgesics every 72h, as well as the daily inter-ruption of these drugs, were started in mid-2015, with further strengthening of these strategies from 2020 on, a period that was not contemplated in the data collection.The study presented some limitations, which can be improved in future methodological approaches. The first refers to the fact that the analysis was not classified according to the drug used and the combinations between them, which could iden-tify those potentially more associated with unfavorable hospi-tal outcomes. Also, relevant consequences associated with the use of continuous sedoanalgesia were not investigated, such as incidences of tolerance, abstinence, and delirium, which would allow a greater comparability of the intensity of this as-sociation with other scientific studies, since the applicability of objective scales to measure these diagnoses still does not occur routinely in the sector. Finally, it was not possible to use severity scores due to failure in the institutional records. Further prospective studies should be done covering these de-mands and following these patients after hospital discharge in order to identify potential long-term adverse effects on the developing human brain, especially in terms of neuropsycho-logical damage. These results reflect the features of a mixed PICU of a large uni-versity hospital in southern Brazil as to the outcomes associated with continuous sedoanalgesia, which may guide better plan-ning of care for children and adolescents in these conditions. Updating the professionals who work in the care of critically ill children is also imperative, enabling a better quality of care,
especially regarding pharmacodynamics, pharmacokinetics and caution in the administration of these drugs.
CONCLUSION
This study sought to identify the association of the use of sedatives and analgesics in continuous infusion with hospital outcomes. Af-ter all adjustments, MPV time greater than four days, diagnosis of HCAI, diagnosis of fungal infection, PICU length of stay greater than three days, and hospitalization time greater than 10 days were more present in these children. Death was more related to severity variables than to the use of psychoactive drugs.
AUTHORS’ CONTRIBUTIONS
Tayná Vieira Data Collection, Writing - Preparation of the original, Writing - Review and Editing Arnildo Linck-Júnior Statistical analysis, Data Collection, Project management, Wri-ting - Preparation of the original, Writing - Review and Editing Mauren Teresa Grubisich Mendes Tacla Conceptualization, Writing - Review and Editing, Visualization Rosângela Aparecida Pimenta Ferrari Conceptualization, Writing - Review and Editing, Visualization Flávia Lopes Gabani Statistical analysis, Data Collection, Project Management, Me-thodology, Writing - Preparation of the original, Writing - Re-view and Editing, Supervision
REFERENCES 1. AMIB. Associação de Medicina Intensiva Brasileira. Regulamento técnico para
funcionamento de unidades de terapia intensiva [Internet]. 2009 [Cited 2021 mar 19]. Available from: https://www.amib.org.br/fileadmin/user_upload/amib/2018/abril/23/RecomendacoesAMIB.pdf
2. Cardoso SB, Oliveira ICS, Martinez EA, Carmo SA, Moraes RCM, Santos MCO. Ambiente de terapia intensiva pediátrica: implicações para a assistência da criança e de sua família. Rev Baiana Enferm. 2019;33:e33545.
3. Taffarel P, Bonetto G, Jorro Barón F, Meregalli C. Sedación y analgesia en pacientes con asistencia ventilatoria mecánica en unidades de cuidados intensivos pediátricos de Argentina. Arch Argent Pediatr. 2018;116(2):e196-e203.
4. Telechea H, Idiarte L, Pardo L, Mondada S, Silva A, Silveira L, et al. Evaluación del uso de sedación y analgesia en niños con asistencia ventilatoria mecánica. Arch Pediatr Urug. 2019;90(1):6-11.
5. Minardi C, Sahillioglu E, Astuto M, Colombo M, Mauricio Ingelmo P. Sedation and analgesia in pediatric intensive care. Curr Drug Deliv. 2012;13(7):936-43.
6. Cai XF, Zhang FR, Zhang L, Sun JM, Li WB. Efficacy of analgesic and sedative treatments in children with mechanical ventilation in the pediatric intensive care unit. Zhongguo Dang Dai Er Ke Za Zhi. 2017;19(11):1138-44.
7. Meyburg J, Dill M-L, von Haken R, Picardi S, Westhoff JH, Silver G, et al. Risk fac-tors for the development of postoperative delirium in pediatric intensive care patients. Pediatr Crit Care Med. 2018;19(10):e514-e21.
8. Duceppe MA, Perreault MM, Frenette AJ, Burry LD, Rico P, Lavoie A, et al. Fre-quency, risk factors and symptomatology of iatrogenic withdrawal from opioids and benzodiazepines in critically ill neonates, children and adults: a systematic review of clinical studies. J Clin Pharm Ther. 2019;44(2):148-56.
9. Chiu AW, Contreras S, Mehta S, Korman J, Perreault MM, Williamson DR, et al. Iatrogenic opioid withdrawal in critically ill patients: a review of assessment tools and management. Ann Pharmacother. 2017;51(12):1099-111.
10. Tong W, Song C, Jin D, Sun J, Wang Y, Xu D. Effects of different sedation regimens on sedation and inflammatory response in critically ill children with multiple trauma. Zhonghua Eei Zhong Bing Ji Jiu Xi Xue. 2017;29(6):542-6.
11. da Silva PS, Reis ME, de Aguiar VE, Fonseca MC. Use of fentanyl and midazolam in mechanically ventilated children - does the method of infusion matter? J Crit Care. 2016;32:108-13.

111
Use of sedatives and analgesics and hospital outcomes in pediatric intensive care: a cohort study
BrJP. São Paulo, 2022 apr-jun;5(2):105-11
12. Baarslag MA, Allegaert K, Knibbe CA, van Dijk M, Tibboel D. Pharmacological sedation management in the paediatric intensive care unit. J Pharm Pharmacol. 2017;69(5):498-513.
13. Best KM, Asaro LA, Curley MA, Wypij D, Allen GL, Angus DC, et al. Sedation Management for Critically Ill Children with Pre-Existing Cognitive Impairment. J Pediatr. 2019;206:204-11. e1.
14. Ismail A. The challenges of providing effective pain management for children in the pediatric intensive care unit. Pain Manag Nurs. 2016;17(6):372-83.
15. Vet NJ, Ista E, de Wildt SN, van Dijk M, Tibboel D, de Hoog M. Optimal seda-tion in pediatric intensive care patients: a systematic review. Intensive Care Med. 2013;39(9):1524-34.
16. Motta E, Luglio M, Delgado AF, Carvalho WB. Importance of the use of protocols for the management of analgesia and sedation in pediatric intensive carte unit. Rev Assoc Med Bras. 2016;62(6):602-9.
17. Smith HAB, Besunder JB, Betters KA, Johnson PN, Srinivasan V, Stormorken A et al. Society of Critical Care Medicine Clinical Practice Guidelines on Prevention and Ma-
nagement of Pain, Agitation, Neuromuscular Blockade, and Delirium in Critically Ill Pediatric Patients With Consideration of the ICU Environment and Early Mobility. Pediatr Crit Care Med. 2022;23(2):e74-e110.
18. Bichaff P, Setani KT, Motta EHG, Delgado AF, Carvalho WB, Luglio M. Opioid tapering and weaning protocols in pediatric critical care units: a systematic review. Rev Assoc Med Bras. 2018;64(10):909-15.
19. Sanavia E, Mencía S, Lafever SN, Solana MJ, Garcia M, López-Herce J. Sedative and analgesic drug rotation protocol in critically ill children with prolonged sedation: evaluation of implementation and efficacy to reduce withdrawal syndrome. Pediatr Crit Care Med. 2019;20(12):1111-7.
20. Verlaat CW, Heesen GP, Vet NJ, de Hoog M, van der Hoeven JG, Kox M, et al. Randomized controlled trial of daily interruption of sedatives in critically ill children. Paediatr Anaesth. 2014;24(2):151-6.
21. Neunhoeffer F, Kumpf M, Renk H, Hanelt M, Berneck N, Bosk A, et al. Nurse‐driven pediatric analgesia and sedation protocol reduces withdrawal symptoms in critically ill medical pediatric patients. Paediatr Anaesth. 2015;25(8):786-94.

112
BrJP. São Paulo, 2022 apr-jun;5(2):112-8
ABSTRACT
BACKGROUND AND OBJECTIVES: Fibromyalgia (FM) is a chronic widespread musculoskeletal pain resulting in central sensitization of nociceptive signaling. Transcranial direct current stimulation (tDCS) over the left motor cortex (M1) is a non-in-vasive neuromodulation technique indicated for a broad range of chronic pain disorders, including FM. Studies suggest that left and right M1 (contralateral and ipsilateral hemisphere of tDCS stimulation) are modulated. But it is necessary to clarify the dif-ferences in clinical pain perception comparing the right and left side of the body. This study aimed to evaluate the pain-related difference between right-left side of the body after five sessions of anodal tDCS in women with FM. METHODS: A double-blinded, parallel, randomized, sham--controlled trial with 30 women with FM was performed. Five sessions of anodal C3 and cathodal supraorbital (Fp2) tDCS were conducted (2 mA for 20 min). Pain, impact of FM and anxiety
Does anodal transcranial direct current stimulation over left motor cortex show body side pain-related difference in fibromyalgia?A estimulação transcraniana por corrente contínua anódica sobre o córtex motor esquerdo apresenta diferença na dor entre os hemicorpos na fibromialgia?
Monayane Grazielly Leite Matias1, Antônio Felipe Lopes Cavalcante3,5. Karime Andrade Mescouto2,3, Edson Meneses Silva-Filho3, Abrahão Fontes Baptista4, Alexandre Hideki Okano4, Rodrigo Pegado1,5
Monayane Grazielly Leite Matias – https://orcid.org/0000-0002-9132-6553;Antônio Felipe Lopes Cavalcante – https://orcid.org/0000-0003-0009-9197;Karime Andrade Mescouto – https://orcid.org/0000-0002-4107-6883;Edson Meneses Silva-Filho – https://orcid.org/0000-0002-0732-5049;Abrahão Fontes Baptista – https://orcid.org/0000-0001-7870-3820;Alexandre Hideki Okano – https://orcid.org/0000-0002-8995-1392;Rodrigo Pegado – https://orcid.org/0000-0002-7227-1075.
1. Federal University of Rio Grande do Norte, Postgraduate Program in Physical Therapy, Natal, RN, Brazil.2. The University of Queensland, School of Health and Rehabilitation Sciences, Brisbane, Australia.3. Federal University of Rio Grande do Norte, Postgraduate Program in Rehabilitation Sci-ences, Santa Cruz, RN, Brazil. 4. Federal University of ABC, Center of Mathematics, Computation and Cognition, São Bernardo, SP, Brazil.5. Federal University of Rio Grande do Norte, Postgraduate Program in Health Sciences, Natal, RN, Brazil.
Submitted on September 27, 2021.Accepted for publication on April 11, 2022.Conflict of interests: none – Sponsoring sources: This study was funded in part by the Coor-denação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001.
Correspondence to: Rodrigo PegadoE-mail: [email protected]
© Sociedade Brasileira para o Estudo da Dor
were evaluated. No statistically significant three-way interaction between time, stimulation type and body side were found. RESULTS: Active-tDCS showed significant improvement in pain, but impact of FM and anxiety did not show significant improvement. CONCLUSION: Five sessions of anodal tDCS over the left M1 improves pain in women with FM, however there was no diffe-rence between right-left body sides.Keywords: Chronic pain, Fibromyalgia, Motor cortex, Nonin-vasive brain stimulation, Transcranial direct current stimulation.
RESUMO JUSTIFICATIVA E OBJETIVOS: A fibromialgia (FM) é uma dor musculoesquelética crônica generalizada que resulta na sensibilização central da sinalização nociceptiva. A estimulação transcraniana de corrente contínua (eTCC) sobre o córtex motor esquerdo (M1) é uma técnica de neuromodulação não invasiva indicada para uma ampla gama de distúrbios de dor crônica, in-cluindo a FM. Estudos sugerem a modulação do M1 esquerdo e direito (hemisfério contralateral e ipsilateral da eTCC). Mas é necessário esclarecer as diferenças na percepção clínica da dor comparando os lados direito e esquerdo do corpo. Este estudo teve como objetivo avaliar a diferença relacionada à dor entre o lado direito e esquerdo do corpo após cinco sessões de eTCC anodal em mulheres com FM. MÉTODOS: Foi realizado um estudo duplo-cego, paralelo, ran-domizado e controlado por sham com 30 mulheres com FM. Foram realizadas cinco sessões de eTCC anodais C3 e supraor-bitais catodais (Fp2) (2 mA por 20 min). Foram avaliados a dor, o impacto da FM e a ansiedade. Não foi encontrada nenhuma interação de três vias estatisticamente significativa entre tempo, tipo de estimulação e lado do corpo. RESULTADOS: A eTCC-Ativa mostrou uma melhora signifi-cativa na dor, mas o impacto da FM e da ansiedade não mostrou uma melhora significativa. CONCLUSÃO: Cinco sessões de eTCC anodal sobre o M1 es-querdo melhoram a dor nas mulheres com FM, entretanto não houve diferença entre os lados direito e esquerdo do corpo.Descritores: Córtex motor, Dor crônica. Estimulação transcra-niana por corrente contínua, Fibromialgia, Síndrome de fadiga crônica.
DOI 10.5935/2595-0118.20220020
ORIGINAL ARTICLE

113
Does anodal transcranial direct current stimulation over left motor cortex show body side pain-related difference in fibromyalgia?
BrJP. São Paulo, 2022 apr-jun;5(2):112-8
INTRODUCTION
Fibromyalgia (FM) is a chronic pain syndrome associated with maladaptive plasticity in neural central circuits characterized by the presence of diffuse pain throughout the body, sleep distur-bance, mood dysfunction, musculoskeletal stiffness, and chronic fatigue1,2. Due to the central nervous system dysfunction, pain pathways seem to operate abnormally, resulting in central sen-sitization of pain signaling3. This mechanism leads to maladap-tive plastic changes in cortical activity from brain areas, inclu-ding pain neuromatrix2. Neuroimaging and electrophysiological approaches suggest that FM is a condition associated with brain dysfunction and rehabilitation programs should target the cen-tral nervous system2.Transcranial direct current stimulation (tDCS) is a non-inva-sive brain stimulation method that has been used to modula-te the excitability and the firing rate of individual neurons in a polarity-dependent fashion4,5. Several studies about FM and neuromodulation suggest promising results in pain relief6-9. Pain improvement has been demonstrated in other chronic pain syn-dromes such as traumatic spinal cord injury, cancer, migraine, and chronic post-stroke pain6-9. Anodal tDCS over the motor cortex (M1) is a promising in-tervention to relieve pain and improve general quality of life in FM9. Most studies used the anodal electrode over M1 or left dorsolateral prefrontal cortex (DLPFC), and the cathode over the contralateral supraorbital region6,10,11. In this sense, it has been suggested that M1 anode stimulation may reduce pain by activating neural circuits present in the precentral gyrus10. These connected structures are involved in the sensory and emotional component of pain processing, facilitating descending pain inhi-bitory control10. In most studies, anodal stimulation was applied over M1 in the contralateral hemisphere of pain (in case of focal or lateralized pain) or the dominant hemisphere (in case of widespread pain)10. A study demonstrated that tDCS applied over M1 was able to induce neuromodulatory effects on the corticospinal and cor-tical excitability indexes by measuring a single or left and right hemisphere through transcranial magnetic stimulation (TMS)12. Authors found that both anodal and cathodal tDCS induced an overall excitability increase compared to the baseline in the contralateral hemisphere of stimulation12. Anodal stimulation increased cortical response in both stimulated cortex and contra-lateral homotopic areas12. Moreover, another neuroimage study shows that tDCS not only modulates activity in the brain region directly underlying the sti-mulating electrode but also in a network of brain regions that are functionally related to the stimulated area13. This result supports a possible coupling of neural activity between motor regions13. However, for protocols involving specific pain syndromes such as migraine, phantom limb pain, and orofacial pain, the anodal stimulation was applied over M1 or DLPFC of the hemisphere contralateral to pain6,10.Following this assumption, the aim was to clarify the differences in clinical pain perception comparing the right and left side of the body after a short-term effect of bilateral bipolar-non ba-
lanced tDCS (C3/Fp2, 10/20 International EEG System™). The hypothesis is a global pain improvement with no pain-related difference between right-left side of the body. The primary ob-jective of the current study was to evaluate the left-right body pain-related difference using algometry threshold after five days of anodal tDCS over M1 in women with FM. The secondary outcomes were to assess pain, impact of FM and anxiety.
METHODS
This study was a single-center, double-blinded, parallel, rando-mized, sham-controlled trial that followed the recommendations of the CONSORT/201014 and TIDier15 checklist. This study complied with ethical standards based on Declaration of Helsin-ki and was approved by the local institutional ethics committee at Federal University of Rio Grande do Norte under registration number 2.932.953. The study was registered in clinicaltrials.gov with identifier NCT03084094. Data were collected in a Pesq-Clin Lab at Federal University of Rio Grande do Norte from Oc-tober 2016 to March 2017 and the recruitment was performed during the entire period since interventions were carried out. All patients were selected from a specialized outpatient service and evaluated by a rheumatologist before the trial.Participants were eligible to enter the study if they fulfilled the following inclusion criteria: women with FM according to the American College of Rheumatology (ACR, 2010)16, pain sco-re of at least 4 on the Numeric Rating Scale (NRS) in the two weeks preceding the clinical trial, and age between 18 and 70 years. Participants were excluded if they had another associa-ted rheumatic disease, such as lupus and rheumatoid arthritis, pregnancy or lactating, history of convulsive crises or intracra-nial implants. Patients who were receiving drugs for pain were not excluded and no changes in the medication were permitted throughout the trial. The G*Power (V. 3.1.9.4™, Kiel, Germany) was used to cal-culate sample size. Sample size was based on previous studies that investigated the effect of tDCS on FM6,11. A significance of 0.05 and power of 0.80 was assumed. Authors suggested in previous studies that a mean reduction of 3 points in the visual analogue scale (VAS) for the group under active stimula-tion was expected in contrast to no improvement in the sham group17. According to this method, the sample size resulted in two groups of 12 participants each. Three more patients were added in each group to prevent any reduction of power in case of patient dropout.Initially, 36 women were enrolled in the study (Figure 1). Six women were excluded for not meeting the inclusion criteria (n=2) or rejecting to participate (n=4). Patients were considered dropouts if they missed one day of treatment. Patients were ran-domized (1:1) and divided into two groups (M1 and Sham). All participants were blinded to the intervention allocation group.
InterventionsDirect current was administered by a trained physical therapist using a continuous electric stimulator, with three energy batteries (9 V) connected in parallel. The maximum energy output was

114
BrJP. São Paulo, 2022 apr-jun;5(2):112-8 Matias MG, Cavalcante AF, Mescouto KA, Silva-Filho EM, Baptista AF, Okano AH and Pegado R
10 mA and was controlled by a professional digital multimeter (DT832, WeiHua Electronic Co.™, Zhangzhou, Fujian, China) with a standard error of ±1.5%. Patients received five consecutive sessions (Monday-Friday) of either sham or anodal stimulation over left M1. The anode electrode was placed over C3 and the cathode was placed over the contralateral supraorbital area (Fp2) according to the 10–20 EEG system. Electrodes were placed into a 35 cm2 (5 cm x 7 cm) square sponge soaked in saline solution (150 mMols of NaCl diluted in Milli-Q water). Rubber banda-ges were used to hold the electrodes in place for the duration of stimulation. For the active tDCS, a constant current of 2 mA was applied for 20 min/day. For sham-tDCS, electrodes were placed at the same position as for the active tDCS, but the current was turned off after 30 seconds of stimulation, according to the me-thods of clinical studies in the brain stimulation10,18. Previous studies described this method of blinding as reliable11,19. Subjects felt the initial itching sensation but received no current for the rest of the stimulation period.
Outcome measuresSociodemographic data were assessed to characterize the sam-ple. Measures of pressure pain threshold (PPT) and NRS were collected one week before the first session (baseline), after the first stimulation (day 1) and after the last stimulation (day 5). For impact of FM and anxiety, data were assessed at baseline and on day 5.
Primary outcomePPT was quantified in kg/cm2 and measured by a digital pressure algometer through a 1-cm diameter rubber tip, (FDX™, Wagner Instruments, Greenwich, Connecticut, USA) on the 18 tender points recommended by the ACR/1990 (left and right low cer-vical, second rib, lateral epicondyle, knee, occiput, trapezius, su-praspinatus, gluteal and greater trochanter)20. The measurement was performed positioning the algometer perpendicularly to the skin, with an interval of 20 to 30 seconds between applications.
The examiner positioned the rubber tip above the area to be examined and gradually increased the pressure by 1 kg/cm2 per second. PPT was identified when the participant reported the beginning of an unpleasant sensation by stating “it started”. This method of evaluation records the initial pain sensation in-formed by participants in 18 different points throughout the body (9 points on the left and 9 on the right side). A mean of total tender points of each side of the body was used to statistical analysis. Furthermore, each pair of tender points (ipsilateral vs contralateral to stimulation) were compared. A second analysis was done with the mean of total pain threshold (mean of 18 tender points) of each time of evaluation.
Secondary outcomesNRS was used to assess the intensity of pain. This straight 10-cm scale is numbered from 0 to 10, in which 0 represents no pain and 10 the most pain. Subjects were instructed to mark the num-ber that best reflected the symptoms of pain at that moment. Ba-seline NRS was assessed one week before intervention for three consecutive days. For statistical analyses, a mean of these three days before the intervention was adopted. This method was used to measure the most real pain feeling before the intervention. The impact of FM was evaluated by using the Brazilian version of the Fibromyalgia Impact Questionnaire (FIQ), which is a sel-f-administered questionnaire that measures patients’ functional aspects21. FIQ contains three Likert-scale-type questions (levels of response) and seven visual analog questions. All scales vary from 1 to 10 and a high score indicates a negative impact and more severe symptoms. The total FIQ score is graded from 1 to 100 points. Higher scores are related to greater impact of the disease on patients’ functionality and a reduction in their quality of life21.The severity of anxiety symptoms was measured by using the Brazilian version of Hamilton Anxiety Scale (HAS). HAS was administered by an interviewer who asked a series of semi-struc-tured questions related to symptoms of anxiety22. The intervie-wer rated the individuals on a five-point scale for each of the 14 items. Seven items specifically address psychic anxiety and the remaining seven, somatic anxieties. The values on the scale range from zero to four: zero means that there is no anxiety, one indica-tes mild anxiety, two indicates moderate anxiety, three indicates severe anxiety, and four indicates very severe or grossly disabling anxiety. The total anxiety score ranges from 0 to 5622.
Statistical analysisDerived data supporting the findings of this study are available from the corresponding author. Analyses were performed using Graph Pad Prism 5 and SPSS software (V.19.0™, Chicago, Illi-nois, USA). Data were expressed as means and standard devia-tions. Shapiro-Wilk’s and Levene’s tests were applied to assess the normality of the distribution and homogeneity of variance of the data, respectively. Mauchly’s test of sphericity was used to valida-te the correlation of the repeated measures and if the assumption of sphericity was violated. The Greenhouse-Geisser correction was applied. Differences in sociodemographic data were calcula-ted using the unpaired t-test or Chi-square test.
Figure 1. Flowchart
Assessed for eligibility (n=36)
Randomized (n=30)
Analyzed
Enrollment
Allocation
Analysis
Active-tDCS (n=15)- Received allocated intervention (n=15)
- Decline to participate (n=0)
Excluded (n=6)Not meeting inclusion criteria (n=2)Rejected to participate (n=4)
Sham-tDCS (n=15)- Received allocated intervention (n=15)
- Decline to participate (n=0)
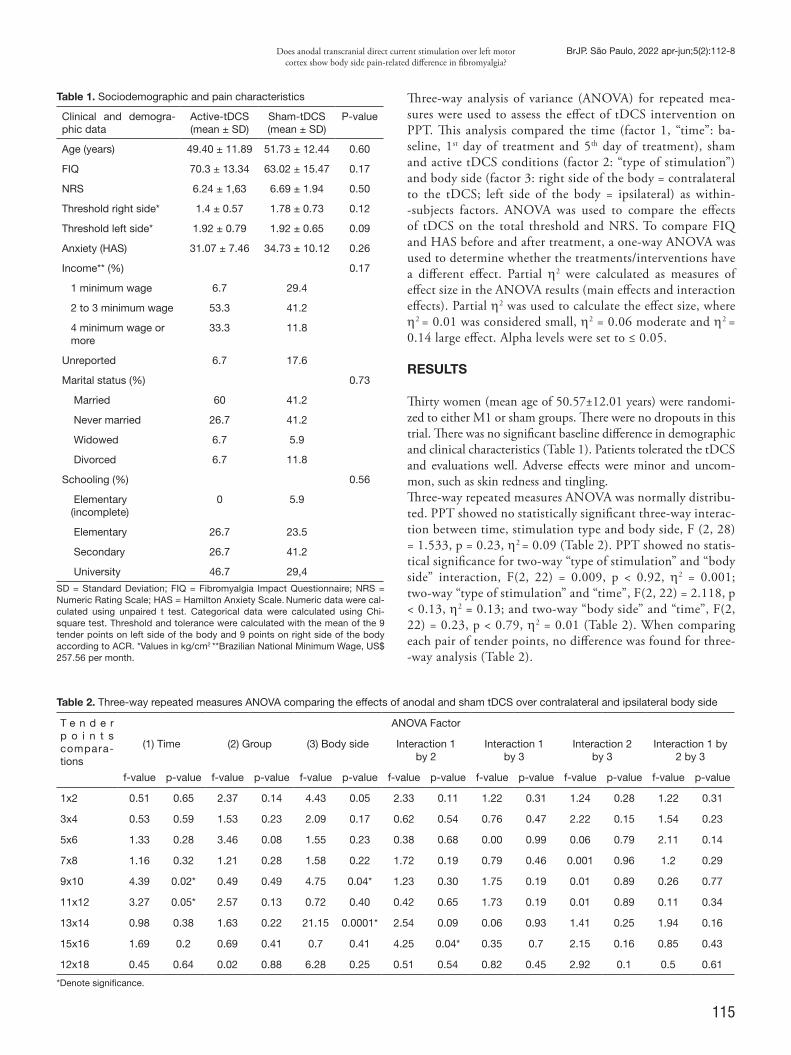
115
Does anodal transcranial direct current stimulation over left motor cortex show body side pain-related difference in fibromyalgia?
BrJP. São Paulo, 2022 apr-jun;5(2):112-8
Three-way analysis of variance (ANOVA) for repeated mea-sures were used to assess the effect of tDCS intervention on PPT. This analysis compared the time (factor 1, “time”: ba-seline, 1st day of treatment and 5th day of treatment), sham and active tDCS conditions (factor 2: “type of stimulation”) and body side (factor 3: right side of the body = contralateral to the tDCS; left side of the body = ipsilateral) as within--subjects factors. ANOVA was used to compare the effects of tDCS on the total threshold and NRS. To compare FIQ and HAS before and after treatment, a one-way ANOVA was used to determine whether the treatments/interventions have a different effect. Partial η2 were calculated as measures of effect size in the ANOVA results (main effects and interaction effects). Partial η2 was used to calculate the effect size, where η2 = 0.01 was considered small, η2 = 0.06 moderate and η2 = 0.14 large effect. Alpha levels were set to ≤ 0.05.
RESULTS
Thirty women (mean age of 50.57±12.01 years) were randomi-zed to either M1 or sham groups. There were no dropouts in this trial. There was no significant baseline difference in demographic and clinical characteristics (Table 1). Patients tolerated the tDCS and evaluations well. Adverse effects were minor and uncom-mon, such as skin redness and tingling. Three-way repeated measures ANOVA was normally distribu-ted. PPT showed no statistically significant three-way interac-tion between time, stimulation type and body side, F (2, 28) = 1.533, p = 0.23, η2 = 0.09 (Table 2). PPT showed no statis-tical significance for two-way “type of stimulation” and “body side” interaction, F(2, 22) = 0.009, p < 0.92, η2 = 0.001; two-way “type of stimulation” and “time”, F(2, 22) = 2.118, p < 0.13, η2 = 0.13; and two-way “body side” and “time”, F(2, 22) = 0.23, p < 0.79, η2 = 0.01 (Table 2). When comparing each pair of tender points, no difference was found for three--way analysis (Table 2).
Table 1. Sociodemographic and pain characteristics
Clinical and demogra-phic data
Active-tDCS(mean ± SD)
Sham-tDCS(mean ± SD)
P-value
Age (years) 49.40 ± 11.89 51.73 ± 12.44 0.60
FIQ 70.3 ± 13.34 63.02 ± 15.47 0.17
NRS 6.24 ± 1,63 6.69 ± 1.94 0.50
Threshold right side* 1.4 ± 0.57 1.78 ± 0.73 0.12
Threshold left side* 1.92 ± 0.79 1.92 ± 0.65 0.09
Anxiety (HAS) 31.07 ± 7.46 34.73 ± 10.12 0.26
Income** (%) 0.17
1 minimum wage 6.7 29.4
2 to 3 minimum wage 53.3 41.2
4 minimum wage or more
33.3 11.8
Unreported 6.7 17.6
Marital status (%) 0.73
Married 60 41.2
Never married 26.7 41.2
Widowed 6.7 5.9
Divorced 6.7 11.8
Schooling (%) 0.56
Elementary (incomplete)
0 5.9
Elementary 26.7 23.5
Secondary 26.7 41.2
University 46.7 29,4
SD = Standard Deviation; FIQ = Fibromyalgia Impact Questionnaire; NRS = Numeric Rating Scale; HAS = Hamilton Anxiety Scale. Numeric data were cal-culated using unpaired t test. Categorical data were calculated using Chi- square test. Threshold and tolerance were calculated with the mean of the 9 tender points on left side of the body and 9 points on right side of the body according to ACR. *Values in kg/cm2 **Brazilian National Minimum Wage, US$ 257.56 per month.
Table 2. Three-way repeated measures ANOVA comparing the effects of anodal and sham tDCS over contralateral and ipsilateral body side
T e n d e r p o i n t s compara-tions
ANOVA Factor
(1) Time (2) Group (3) Body side Interaction 1 by 2
Interaction 1 by 3
Interaction 2 by 3
Interaction 1 by 2 by 3
f-value p-value f-value p-value f-value p-value f-value p-value f-value p-value f-value p-value f-value p-value
1x2 0.51 0.65 2.37 0.14 4.43 0.05 2.33 0.11 1.22 0.31 1.24 0.28 1.22 0.31
3x4 0.53 0.59 1.53 0.23 2.09 0.17 0.62 0.54 0.76 0.47 2.22 0.15 1.54 0.23
5x6 1.33 0.28 3.46 0.08 1.55 0.23 0.38 0.68 0.00 0.99 0.06 0.79 2.11 0.14
7x8 1.16 0.32 1.21 0.28 1.58 0.22 1.72 0.19 0.79 0.46 0.001 0.96 1.2 0.29
9x10 4.39 0.02* 0.49 0.49 4.75 0.04* 1.23 0.30 1.75 0.19 0.01 0.89 0.26 0.77
11x12 3.27 0.05* 2.57 0.13 0.72 0.40 0.42 0.65 1.73 0.19 0.01 0.89 0.11 0.34
13x14 0.98 0.38 1.63 0.22 21.15 0.0001* 2.54 0.09 0.06 0.93 1.41 0.25 1.94 0.16
15x16 1.69 0.2 0.69 0.41 0.7 0.41 4.25 0.04* 0.35 0.7 2.15 0.16 0.85 0.43
12x18 0.45 0.64 0.02 0.88 6.28 0.25 0.51 0.54 0.82 0.45 2.92 0.1 0.5 0.61
*Denote significance.
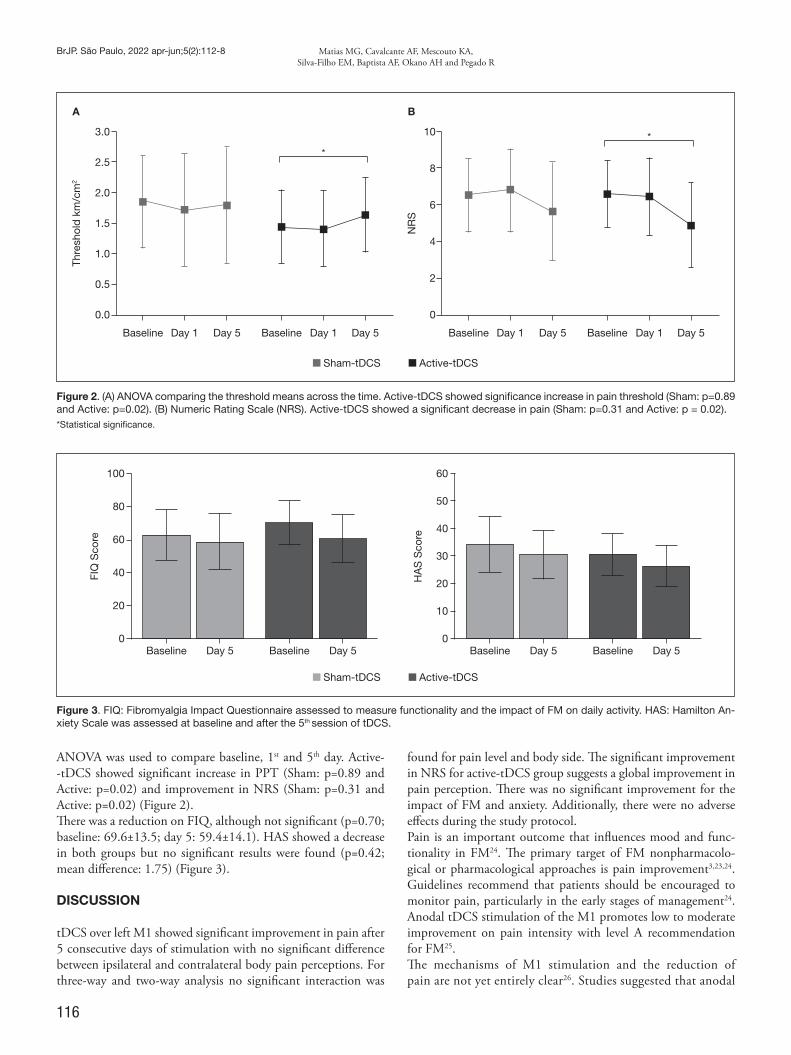
116
BrJP. São Paulo, 2022 apr-jun;5(2):112-8 Matias MG, Cavalcante AF, Mescouto KA, Silva-Filho EM, Baptista AF, Okano AH and Pegado R
ANOVA was used to compare baseline, 1st and 5th day. Active--tDCS showed significant increase in PPT (Sham: p=0.89 and Active: p=0.02) and improvement in NRS (Sham: p=0.31 and Active: p=0.02) (Figure 2). There was a reduction on FIQ, although not significant (p=0.70; baseline: 69.6±13.5; day 5: 59.4±14.1). HAS showed a decrease in both groups but no significant results were found (p=0.42; mean difference: 1.75) (Figure 3).
DISCUSSION
tDCS over left M1 showed significant improvement in pain after 5 consecutive days of stimulation with no significant difference between ipsilateral and contralateral body pain perceptions. For three-way and two-way analysis no significant interaction was
found for pain level and body side. The significant improvement in NRS for active-tDCS group suggests a global improvement in pain perception. There was no significant improvement for the impact of FM and anxiety. Additionally, there were no adverse effects during the study protocol.Pain is an important outcome that influences mood and func-tionality in FM24. The primary target of FM nonpharmacolo-gical or pharmacological approaches is pain improvement3,23,24. Guidelines recommend that patients should be encouraged to monitor pain, particularly in the early stages of management24. Anodal tDCS stimulation of the M1 promotes low to moderate improvement on pain intensity with level A recommendation for FM25. The mechanisms of M1 stimulation and the reduction of pain are not yet entirely clear26. Studies suggested that anodal
Sham-tDCS Active-tDCS
A B
Thre
shol
d k
m/c
m2
NR
S
3.0
2.5
2.0
1.5
1.0
0.5
0.0
10
8
6
4
2
0
Baseline BaselineDay 1 Day 1Day 5 Day 5Baseline BaselineDay 1 Day 1Day 5 Day 5
Sham-tDCS Active-tDCS
Baseline BaselineBaseline BaselineDay 5 Day 5Day 5 Day 5
100
80
60
40
20
0
60
50
40
30
20
10
0
FIQ
Sco
re
HA
S S
core
Figure 3. FIQ: Fibromyalgia Impact Questionnaire assessed to measure functionality and the impact of FM on daily activity. HAS: Hamilton An-xiety Scale was assessed at baseline and after the 5th session of tDCS.
Figure 2. (A) ANOVA comparing the threshold means across the time. Active-tDCS showed significance increase in pain threshold (Sham: p=0.89 and Active: p=0.02). (B) Numeric Rating Scale (NRS). Active-tDCS showed a significant decrease in pain (Sham: p=0.31 and Active: p = 0.02). *Statistical significance.

117
Does anodal transcranial direct current stimulation over left motor cortex show body side pain-related difference in fibromyalgia?
BrJP. São Paulo, 2022 apr-jun;5(2):112-8
tDCS over M1 has widespread effects on multiple cortical and subcortical areas, including cingulate, frontal areas, tha-lamus and striatum12,26. Moreover, after anodal stimulation over M1, studies observed an increase in the cortical response not only over the stimulated cortex but also over the contrala-teral homotopic areas12. This finding supports a possible cou-pling of neuroactivity of brain regions that are functionally related to the stimulated area13. Therefore, tDCS promotes a diffuse analgesic effect that could be used for diffuse pain syndromes such as FM27. For this reason, it is expected that M1 stimulation decreases pain in both sides of the body. Re-petitive transcranial magnetic stimulation (rTMS) seems to be analogous to pain reduction for FM and both neuromodu-lation modalities presented fewer side effects compared with pharmacological approach28. Some authors suggest FM as a centralized pain state and that the central nervous system could amplify nocicepti-ve input, even after a peripheral nociceptive input2. Brain networks involving pain perception seem to be altered in FM2. Patients exhibit multifocal pain in both sides with many cases of sensory hyperresponsiveness2. The impact of FM leads to a significant decrease in functional capacity and quality of life16,29. This study did not find significant differences in FIQ bet-ween groups. This may reflect the limited number of sessions and/or that the short period for participants’ evaluation was insufficient to induce changes in daily activities. Authors suggest that tDCS could be used with adjuvant therapy and multimodal treatment, including aerobic or strength exer-cises, which need to be encouraged27. Authors have shown better effects on pain with combined aerobic exercise and tDCS in FM1. On the other hand, associated therapy inclu-ding tDCS with functional exercises did not enhance the effects of physical exercise on pain, functionality and quality of life30. Further trials with multimodal therapy involving tDCS are necessary to clarify the effects for FM patients30. A complete understanding of FM requires a comprehensive assessment of pain, function and psychosocial context and the strategy of management should have a multidisciplinary approach2. The present results provide evidence that five sessions of anodal tDCS over M1 reduce pain with no body side difference in women with FM. No improvement was found for the impact of FM and anxiety. Methodological limitations could be appointed. First, the menstrual cycle of participants was not evaluated and tDCS was performed not at the same menstrual period. Secondly, no long-term effect was assessed and further clinical trials with two or three weeks of follow-up is encouraged. Future studies should include DLPFC stimulation to investigate ef-fects of tDCS on body side pain perception.
CONCLUSION
The use of five sessions of anodal tDCS over the left M1 improve pain with no body side difference in women with FM.
AUTHORS’ CONTRIBUTIONS
Monayane Grazielly Leite Matias Data Collection, Project Management Antônio Felipe Lopes CavalcanteWriting - Review and EditingKarime Andrade Mescouto Data Collection, Conceptualization, Visualization Edson Meneses Silva-Filho Statistical analysis, Writing - Preparation of the original Abrahão Fontes Baptista Writing - Review and Editing Alexandre Hideki Okano Conceptualization, Supervision Rodrigo Pegado Statistical analysis, Data Collection, Conceptualization, Writing - Preparation of the original
REFERENCES
1. Mendonca ME, Simis M, Grecco LC, Battistella LR, Baptista AF. Fregni F. Transcra-nial direct current stimulation combined with aerobic exercise to optimize analgesic responses in fibromyalgia: a randomized placebo-controlled clinical trial. Front Hum Neurosci. 2016;10:68.
2. Clauw DJ. Fibromyalgia: a clinical review. JAMA.2014;311(15):1547-55. 3. Clauw DJ, Arnold LM, McCarberg BH. The science of fibromyalgia. Mayo Clin Proc.
2011;86(9):907-11.4. Rossi S, Santarnecchi E, Valenza G, Ulivelli M. The heart side of brain neuromodula-
tion, Philos. Trans A Math. Phys Eng Sci. 2016;374(2067):20150187. 5. Heymann RE, Paiva Edos S, Helfenstein M Jr, Pollak DF, Martinez JE, Provenza JR,
Paula AP, et al. Brazilian consensus on the treatment of fibromyalgia. Rev Bras Reu-matol. 2010;50(1):56-66.
6. Lefaucheur JP. A comprehensive database of published tDCS clinical trials (2005-2016), Neurophysiol Clin. 2016;46(6):319-98.
7. Castillo-Saavedra L, Gebodh N. Bikson M, Diaz-Cruz C, Brandao R, Coutinho L, et al. Clinically effective treatment of fibromyalgia pain with high-definition trans-cranial direct current stimulation: Phase II Open-Label Dose Optimization. J Pain. 2016;17(1):14-26.
8. Nardone R, Höller Y, Leis S, Höller P, Thon N, Thomschewski A, et al. Invasive and non-invasive brain stimulation for treatment of neuropathic pain in patients with spinal cord injury : a review. 2014;37(1):19-31.
9. Zhu CE, Yu B, Zhang W, Chen WH, Qi Q, Miao Y. Effectiveness and safety of transcranial direct current stimulation in fibromyalgia: A systematic review and meta--analysis. J Rehabil Med. 2017;49(1):2-9.
10. Nasseri P, Nitsche MA, Ekhtiari H. A framework for categorizing electrode montages in transcranial direct current stimulation. Front Hum Neurosci. 2015;9:54.
11. Lefaucheur JP, Antal A, Ayache SS, Benninger DH, Brunelin J, Cogiamanian F, Co-telli M, et al. Evidence-based guidelines on the therapeutic use of transcranial direct current stimulation (tDCS). Clin Neurophysiol. 2017;128(1):56-92.
12. Pellicciari MC, Brignani D, Miniussi C. Excitability modulation of the motor system induced by transcranial direct current stimulation: a multimodal approach, Neu-roimage. 2013;83:569-80.
13. Zheng X, Alsop DC, Schlaug G. Effects of transcranial direct current stimulation (tDCS) on human regional cerebral blood flow. Neuroimage. 2011;58(1):26-33.
14. Schulz KF, Altman DG, Moher D. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. J Clin Epidemiol. 2010;63:834-40.
15. Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, et al. Better reporting of interventions: Template for intervention description and replication (TI-DieR) checklist and guide. BMJ. 2014;348:g1687.
16. Wolfe F, Clauw DJ, Fitzcharles MA, Goldenberg DL, Katz RS, Mease P, et al. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010;62(5):600-10.
17. Fregni F, Gimenes R, Valle AC, Ferreira MJ, Rocha RR, Natalle L, et al. A ran-domized, sham-controlled, proof of principle study of transcranial direct cur-rent stimulation for the treatment of pain in fibromyalgia. Arthritis Rheum. 2006;54(12):3988-98.
18. Bikson M, Grossman P, Thomas C, Zannou AL, Adnan T, Mourdoukoutas AP, et al. Safety of transcranial direct current stimulation: evidence based update 2016. Brain Stimul. 2016;9(5):641-61.
19. Riberto M, Marcon Alfieri F, Monteiro de Benedetto Pacheco K, Dini Leite V, Nemo-
118
BrJP. São Paulo, 2022 apr-jun;5(2):112-8 Matias MG, Cavalcante AF, Mescouto KA, Silva-Filho EM, Baptista AF, Okano AH and Pegado R
to Kaihami H, Fregni F, et al. Efficacy of transcranial direct current stimulation cou-pled with a multidisciplinary rehabilitation program for the treatment of fibromyalgia. Open Rheumatol J. 2011;5:45-50.
20. Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C, Goldenberg DL, et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum. 1990;33(2):160-72.
21. Marques AP, Barsante Santos AM, Assumpção A, Matsutani LA, Lage LV, Pereira CAB. Validação da versão Brasileira do Fibromyalgia Impact Questionnaire (FIQ), Rev Bras Reumatol. 2006;46(1):24-31.
22. Hamilton M. Hamilton Anxiety Rating Scale (HAM-A). J Med. 1959;261:81-82.23. Björkegren K, Wallander MA, Johansson S, Svärdsudd K. General symptom reporting
in female fibromyalgia patients and referents: a population-based case-referent study. BMC Public Health. 2009;9:402.
24. Ablin J, Fitzcharles MA, Buskila D, Shir Y, Sommer C, Häuser W. Treatment of fi-bromyalgia syndrome: Recommendations of recent evidence-based interdisciplinary guidelines with special emphasis on complementary and alternative therapies. Evid Based Complement Alternat Med. 2013;2013:485272.
25. Baptista AF, Fernandes AMBL, Sá KN, Okano AH, Brunoni AR, Lara-Solares A, et al. Latin American and Caribbean consensus on noninvasive central nervous system neuro-modulation for chronic pain management (LAC 2 -NIN-CP). Pain Rep. 2019;4(1):e692.
26. Jensen MP, Day MA, Miró J. Neuromodulatory treatments for chronic pain: efficacy and mechanisms. Nat Rev Neurol. 2014;10(3):167-78.
27. Morya E, Monte-Silva K, Bikson M, Esmaeilpour Z, Biazoli CE Jr, Fonseca A, Bocci T, et al. Beyond the target area: an integrative view of tDCS-induced motor cortex modulation in patients and athletes. J Neuroeng Rehabil. 2019;16(1):141.
28. Marlow NM, Bonilha HS, Short EB. Efficacy of transcranial direct current stimula-tion and repetitive transcranial magnetic stimulation for treating fibromyalgia syndro-me: a systematic review. Pain Pract. 2013;13(2):131-45.
29. Ceko M, Bushnell MC, Gracely RH. Neurobiology underlying fibromyalgia symp-toms. Pain Res Treat. 2012;2012:585419.
30. Matias MGL, Germano Maciel D, França IM, Cerqueira MS, Silva TCLA, Okano AH, et al. Transcranial direct current stimulation associated with functional exerci-se program for treating fibromyalgia: a randomized controlled trial. Arch Phys Med Rehabil. 2022;103(2):245-54.

119
ABSTRACT
BACKGROUND AND OBJECTIVES: Fibromyalgia and ge-neralized pain represent a global health problem and are distinct musculoskeletal disorders, but there is an overlap in the clinical presentation between these conditions. However, no study has compared pain characteristics between patients with fibromy-algia and patients with generalized pain. Therefore, the present study aimed to compare pain characteristics and functional li-mitation of patients with fibromyalgia and patients with gene-ralized pain. METHODS: A pre-planned secondary analysis of data collec-ted from 311 patients with musculoskeletal pain was performed. Pain characteristics included pain intensity, pain duration, pain area, symptoms of central sensitization, presence of neuropathi-c-like symptoms, and the conditioned pain modulation. The Patient-Specific Functional Scale assessed functional limitation. RESULTS: 98 patients with generalized pain were identified, being 58 (59.18%) classified in the fibromyalgia group and 40 (40.82%) classified in the generalized pain group. Significant differences were found between groups for Widespread Pain Index, Symptom Severity Scale, and Polysymptomatic Distress Scale. Participants with fibromyalgia presented higher values of pain intensity (fibromyalgia = 7.29±2.07, generalized pain =
Patients with fibromyalgia present different pain phenotypes compared to patients with generalized painPacientes com fibromialgia apresentam fenótipos de dor diferentes em comparação com pacientes com dor generalizada
Juliana Valentim Bittencourt1, Leticia Amaral Corrêa1, Márcia Cliton Bezerra1, Felipe José Jandre dos Reis2, Katie de Luca3, Leandro Alberto Calazans Nogueira1,2
Juliana Valentim Bittencourt – https://orcid.org/0000-0001-9522-8523;Leticia Amaral Corrêa – https://orcid.org/0000-0002-8188-7111;Márcia Cliton Bezerra – https://orcid.org/0000-0003-3680-0969;Felipe José Jandre dos Reis – https://orcid.org/0000-0002-9471-1174;Katie de Luca – https://orcid.org/0000-0002-2763-771X;Leandro Alberto Calazans Nogueira – https://orcid.org/0000-0002-0177-9816. 1. Augusto Motta University Center, Rehabilitation Science Postgraduate Program, Rio de Janeiro, RJ, Brazil. 2. Federal Institute of Rio de Janeiro, Physiotherapy Department, Rio de Janeiro, RJ, Brazil. 3. Macquarie University, Department of Chiropractic, Sydney, New South Wales, Australia.
Submitted on October 02, 2021.Accepted for publication on April 12, 2022.Conflict of interests: none – Sponsoring sources: This study was financed in party by the Co-ordination of Improvement of Higher Education Personnel (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – CAPES) - Finance Code 001.
Correspondence to:Juliana Valentim BittencourtE-mail: [email protected]
© Sociedade Brasileira para o Estudo da Dor
6.05±2.47; p=0.008), neuropathic-like symptoms (fibromyalgia = 17.74±7.62, generalized pain = 12.17±6.41; p=0.005), and symptoms of central sensitization (fibromyalgia = 51.32±14.26, generalized pain = 33.97±14.65; p<0.001), when compared with generalized pain. There was no significant difference in conditio-ned pain modulation and functional limitation between groups. CONCLUSION: Patients with fibromyalgia exhibited unfavo-rable pain characteristics, including pain intensity, neuropathi-c-like symptoms, and symptoms of central sensitization compa-red to patients with generalized pain. However, pain duration, functional limitation, and conditioned pain modulation did not present meaningful differences between groups.Keywords: Chronic pain, Fibromyalgia, Pain measurement, Pain threshold.
RESUMO
JUSTIFICATIVA E OBJETIVOS: Fibromialgia e dor genera-lizada representam um problema de saúde global e são distúr-bios musculoesqueléticos distintos, mas há uma sobreposição na apresentação clínica entre essas condições. Entretanto, nenhum estudo comparou as características da dor entre os pacientes com estas condições. Portanto, o presente estudo teve como objetivo comparar as características da dor e a limitação funcional de pa-cientes com fibromialgia e dor generalizada. MÉTODOS: Realizou-se uma análise secundária pré-planejada de dados coletados de 311 pacientes com dor musculoesque-lética. As características da dor incluíram: intensidade da dor, duração da dor, área da dor, sintomas de sensibilização central, presença de sintomas neuropáticos e a modulação condicionada da dor. A escala de funcionalidade específica do paciente avaliou a limitação funcional. RESULTADOS: Identificou-se 98 pacientes com dor generali-zada, sendo 58 (59,18%) classificados no grupo de fibromialgia e 40 (40,82%) no grupo de dor generalizada. Diferenças sig-nificativas foram encontradas entre os grupos para o índice de dor generalizada, escala de severidade de sintomas e escala po-lissintomática de sofrimento. Os participantes com fibromialgia apresentaram maiores valores de intensidade da dor (fibromialgia = 7,29±2,07, dor generalizada = 6,05 ± 2,47; p=0,008), sinto-mas neuropáticos (fibromialgia = 17,74±7,62, dor generalizada = 12,17 ± 6,41; p=0,005) e sintomas de sensibilização central (fibromialgia = 51,32±14,26, dor generalizada = 33,97±14,65; p<0,001), quando comparados à dor generalizada. Não houve
BrJP. São Paulo, 2022 apr-jun;5(2):119-26
DOI 10.5935/2595-0118.20220031-en
ORIGINAL ARTICLE

120
BrJP. São Paulo, 2022 apr-jun;5(2):119-26 Bittencourt JV, Corrêa LA, Bezerra MC, Reis FJ, Luca K and Nogueira LA
diferença significativa na modulação condicionada da dor e na limitação funcional entre os grupos. CONCLUSÃO: Pacientes com fibromialgia exibiram caracterís-ticas de dor desfavoráveis, incluindo intensidade de dor, sinto-mas neuropáticos e sintomas de sensibilização central, quando comparados a pacientes com dor generalizada. Entretanto, a du-ração da dor, a limitação funcional e a modulação condicionada da dor não apresentaram diferença significativa entre os grupos.Descritores: Dor crônica, Dor musculoesquelética, Fibromial-gia, Limiar da dor, Medição da dor.
INTRODUCTION
Fibromyalgia and generalized pain are prevailing in musculoskele-tal health conditions. The prevalence of fibromyalgia was 4.7% in Europe1, 6.4% in the United States2, 4.4%3 in Brazil and 2%-3% in the general population4,5. The prevalence of chronic widespread pain was 24% in Brazilian women3, and 10.6%6, or one in ten in-dividuals, are affected by chronic widespread pain in the general population6. Patients with fibromyalgia present widespread muscu-loskeletal pain, fatigue, sleep disturbances, and cognitive changes7,8. Several instruments are available for the assessment of fibromyalgia and generalized pain. Preliminary criteria for the classification of fi-bromyalgia emerged in 19909. In the last update, a combination of the Widespread Pain Index (WPI), which was designed initially to assess pain distribution10, the Symptom Severity Scale (SSS), whi-ch evaluates cognitive and general somatic symptoms11, and the combination of WPI and SSS that results in the Polysymptomatic Distress Scale (PSD), which measures the severity of fibromyalgia symptoms, have been recommended as diagnostic criteria10. Fibromyalgia and generalized pain are distinct musculoskeletal di-sorders, but there is an overlap of the clinical presentation between these conditions. Likewise, chronic widespread pain and multisite pain present similar symptoms of fibromyalgia12. A previous study claimed that fibromyalgia and chronic widespread pain differ more in quantitative than qualitative measures13. Patients with fibrom-yalgia and generalized pain had higher symptoms of pain, anxiety and depression than those with regional pain14. Fibromyalgia pa-tients have more intense and persistent pain than patients with chronic widespread pain13. Moreover, fibromyalgia patients had more comorbidities, pain-related drugs, poorer health status, func-tion and sleep, lower productivity, and higher costs compared to patients without chronic widespread pain and with chronic wides-pread pain but without fibromyalgia15. Generalized pain may be associated with fatigue, psychological distress, and concentration problems, like fibromyalgia7,10. Still, while the two conditions were similarly disabling3, fibromyalgia has unfavorable clinical presen-tation when compared to chronic widespread pain13,16. However, the diagnosis of fibromyalgia and generalized pain remains trou-blesome, many redundancies exist17 and it is unclear whether the addition of the cognitive and somatic symptoms adds meaningful value to the clinical phenotype of these patients. The identification of particular pain characteristics of these overlapping conditions may contribute to tailored treatment. Fibromyalgia has distinct pain features when compared to other musculoskeletal conditions. A deficit of endogenous pain inhi-
bitory systems is observed in fibromyalgia but not in chronic low back pain18. Patients with fibromyalgia also present higher levels of neuropathic-like symptoms compared to patients with rheumatoid arthritis19. Likewise, reduced pain threshold13,20, increased temporal summation21, decreased conditioned pain modulation (CPM)21 and presence of central sensitization have been reported in patients with fibromyalgia22. However, no study has compared pain characteristics between patients with fibrom-yalgia and patients with generalized pain. Therefore, the present study aimed to compare pain characteristics and functional li-mitation of patients with fibromyalgia and patients with gene-ralized pain. The hypothesis was that patients with fibromyalgia would report more severe symptoms, higher levels of functional limitation and impaired pain modulation in the cold pressor test than patients with generalized pain.
METHODS
A pre-planned secondary analysis of data collected from a pre-vious study by the present group of authors was undertook23. The original study was a cross-sectional observational study that followed the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) criteria (Atachment 1)24. The study included 311 patients with musculoskeletal pain to compare the pain characteristics of patients with musculoskeletal pain classified according to PainDETECT as nociceptive pain, unclear and neuropathic-like symptoms. The current study ex-cluded 213 patients with musculoskeletal pain without genera-lized pain and had a final sample of 98 patients with generalized pain. The original study was approved by the Research Ethics Committee of Federal Institute of Rio de Janeiro (number: 02228818.0.3001.5258), following the Helsinki Declaration for research in humans. All patients who met the eligibility criteria signed the informed consent form before the study procedures.
Study participants Patients with musculoskeletal pain (aged 18 years and over) who sought treatment in the outpatient physiotherapy clinic of Gaffrée and Guinle University Hospital were enrolled bet-ween March and September 2019. The original study included patients with acute pain (pain duration less than three months) and chronic pain (pain duration greater than three months). Musculoskeletal pain was defined as pain perceived in a body region with muscular, ligament, bone, or joint origin25. The current study identified patients with generalized pain that could be classified as generalized pain or fibromyalgia accor-ding to the 2016 modified American College of Rheumatology (ACR) criteria. The study excluded patients who had a sur-gical procedure in the spine, pregnant women, patients with rheumatologic diagnosis in the acute inflammatory phase, with tumors, and patients who were illiterate or who could not com-plete the self-reported questionnaires.
Procedures Patients were referred for an evaluation consisting of a clinical history and physical examination. Participants completed a

121
Patients with fibromyalgia present different pain phenotypes compared to patients with generalized pain
BrJP. São Paulo, 2022 apr-jun;5(2):119-26
self-report questionnaire that included information on their sociodemographic characteristics (age, gender, weight, height, and body mass index), pain characteristics (pain intensity, pain duration, pain area, symptoms of central sensitization, presence of neuropathic-like symptoms, and CPM), func-tional limitation, and lifestyle factors (smoking, alcoholism, and physical activity). The completion of all questionnaires was supervised by one of the examiners for clarification, in case of uncertainties. The two examiners involved (J.V.B and M.C.B) had, respectively, two and 32 years of work experien-ce in treating patients with musculoskeletal disorders. The cli-nical history assessment lasted approximately 10 minutes per participant. Next, patients were referred for evaluation of the efficiency of the CPM.
Patient classificationFibromyalgia diagnosis was performed using the WPI and the SSS. WPI is a self-reported list of painful regions composed of 19 body areas, and the patient must mark the areas in which he or she felt pain during the last week. Each marked area is equivalent to 1 point. The final score varies between zero and 19 points. SSS is the sum of the severity scores of 3 symptoms (fatigue, waking unrefreshed, and cognitive symptoms) plus the totality of specific symptoms that occurred during the previous 6 months (headaches, pain or cramps in the lower abdomen, and depression). Fibromyalgia diagnosis was con-firmed when WPI≥7 and SSS score≥5 or WPI of 4-6 and SSS score≥9, according to the 2016 modified American College of Rheumatology criteria10. Fibromyalgia severity was measured by the Polysymptomatic Distress Scale (PDS). The sum of the WPI obtains this scale (zero-19) and the SSS (zero-12) with a final score that varies between zero-31. According to the 2016 modified ACR criteria, a PDS score of at least 12 represents an approximate level of fibromyalgia diagnosis10. The psycho-metric assessment of WPI demonstrated good construct and criterion validity between young patients with painful con-ditions26. Generalized pain was defined when the participant reported pain in at least 4 of 5 regions (upper left and right, lower left and right, and axial) of the WPI. Jaw, chest, and abdominal pain are not included in generalized pain definition10.
Main outcome measuresPain intensity was assessed by the numeric pain rating scale (NPRS). The Central Sensitization Inventory (CSI) was used for evaluating symptoms associated with central sensitization. Neuropathic-like symptoms were assessed by the PainDE-TECT questionnaire27. Functional limitation was measured using the Patient-Specific Functional Scale28 (PSFS). The cold pressor test assessed CPM. All questionnaires and tests were completed on the same day.
Pain characteristicsPain intensity was measured during the initial evaluation using the NPRS from zero (no pain) to 10 (worst pain pos-sible). Patients were oriented to rate their pain intensity now
of the initial evaluation. The duration of pain was recorded in months, and patients were classified with chronic muscu-loskeletal pain if they had pain for more than three months29. Pain area was measured using the WPI. The sum of the WPI (0-19) and the SSS (0-12) results in the polysymptomatic dis-tress (zero-31).The CSI is an instrument developed to identify patients with symptoms associated with central sensitization30. Part A as-sesses 25 health-related symptoms commonly observed in pa-tients with central sensitivity syndrome. Part A is scored on a 5-point Likert scale from 0 (never) to 4 (always), with a total of 100 points, and higher scores represent an increase in the severity of symptoms.Part B is not scored and encompasses ten previous diagnoses of an individual, including seven central sensitivity syndro-mes and three disorders related to central sensitization syn-drome. The optimal cut-off point was established at 40/100 in patients with central sensitivity syndrome31,32. The severity of symptoms related to central sensitization has been clas-sified into sub-clinical (0–29), mild (30-39), moderate (40-49), severe (50-59) and extreme (60-100)31,33, where higher scores indicate an increase in the severity of symptoms34. The Brazilian version of the CSI demonstrated strong psychome-tric properties35.PainDETECT is a self-administered questionnaire that en-compasses four domains as follows: the intensity of pain (three questions), pain course pattern (four graphs), areas of pain and the presence of radiating pain (body chart drawing), and sensory descriptor items of pain (seven questions). For each question, six different answers are possible, with scores from zero (never) to five (very strongly). By summing up the scores given in each domain, a final score between -1 to 38 can be achieved. The PainDETECT is validated for many neuropa-thic pain conditions. In the last years, it was also validated for the use in mixed pain conditions such as rheumatoid arthritis, osteoarthritis, cancer pain, and lumbar spondylolisthesis. The cut-off points for the original questionnaire indicate that in the scores≤12 a neuropathic component is unlikely, whereas, in the ≥19 scores, a neuropathic component is probable27,36. The Brazilian version of PainDETECT is indicated as useful to identify neuropathic components in the pain of Brazilian patients37.
Functional limitationFunctional limitation was investigated using the PSFS, which is a self-reported measure used to assess functional change in patients with musculoskeletal disorders. Patients should identify up to five important activities they are unable to per-form or are restrict because of their pain and classify on an 11-point scale the current level of difficulty associated with each activity. PSFS has easy applicability and can be used cli-nically as an outcome measure28,38.
Conditioned pain modulationCold pressor test is a psychophysical test used to assess the CPM, where the cold pain is the conditioning stimulus, and pressure

122
BrJP. São Paulo, 2022 apr-jun;5(2):119-26 Bittencourt JV, Corrêa LA, Bezerra MC, Reis FJ, Luca K and Nogueira LA
pain threshold (PPT) is the test stimulus. The cold pressor is an appropriate method to assess the descending nociceptive inhibi-tory system39. The conditioning stimulus was the immersion of the participants` hand in a bucket with temperature-controlled cold water (1ºC – 4ºC) monitored by a thermometer (5130 mo-del, IncotermTM, Hong Kong, Sha Tin, China), for up to one minute. The participant was instructed to remain with the hand immersed in water without making muscle contractions or chan-ges in position. The withdrawal of the side from the water was allowed when the patient could no longer tolerate the painful stimulus. Room temperature, humidity, lighting, and noise were maintained constant during the entire procedure. PPT measurement was performed before and after one minute of the cold pressor test, using a digital pressure algometer (model Force Ten FDX, Wagner InstrumentsTM, Greenwich, CT, USA). The distal part of the dorsal forearm and tibialis anterior mus-cle, which had not been immersed in water, were chosen to be evaluated due to the lack of relationship with participant’s mus-culoskeletal complaints. The two sites were assessed in the same order for all participants. The operation of the pressure algometer and measurement of PPT were explained to patients before the assessment. In addition, a familiarization procedure was carried out with the pressure algometer by applying pressure to the do-minant forearm to ensure that the test had been understood. The force was gradually increased (1 kilogram-force/s) until the feeling of pressure from the primary subject was changed to pain. PPT was recorded in kilograms-force (kgf) when the patient gave the verbal command “pain”. The classification of the CPM efficiency was based on the following strategy: evidence of impaired pain modulation in two sites. Only patients with the inefficiency of the CPM in both locations (the anterior tibialis muscle and the distal part of the dorsal forearm) were classified as impaired pain modulation40. Upper and lower limb sites were used to avoid the inclusion of the patients with peripheral sensitization according to recommendations for CPM40. Also, the efficiency of the CPM was assessed by calculating the difference between PPT values in the cold pressor test (differences between final and initial value). Negative values represented an inefficiency of CPM and null or positive values were considered a typical response of CPM.
Statistical analysisDemographic and clinical variables of the study population are presented as mean and standard deviation for continuous va-
riables. Categorical variables are presented numerically and as a percentage of the sample. For continuous variables, the normal distribution of the outcomes of the study was verified by the Sha-piro-Wilk test. The group of patients who presented fibromyalgia was compared with those with generalized pain. The comparison between groups according to the outcome’s measures: the unpai-red t-test performed pain intensity and pain duration due to the parametric distribution of the variables. The Chi-Square test was used to compare categorical variables: functional limitation, symptoms of central sensitization, neuropathic-like symptoms, and efficiency of the CPM. A significance level of less than 5% (p<.05) was considered for all analyses. The statistical analysis was performed using JASP version 0.10.2.0. Given the lack of sample size calculation due to the secondary analysis, a post hoc power analysis was performed to determine whether the sample size was large enough for the fin-dings to be statistically valid and to examine the potential for type II errors. The post hoc analysis was performed for estima-tion of the statistical power of the present study by unpaired t-test using G*Power 3.1.9.4 (Heinrich-Heine-Universität, Düs-seldorf, Germany).
RESULTS
A total of 98 participants with generalized pain was identified. Among the included participants, 83 (84.69%) were women. The mean age was of 57.94±11.64 years old, and the mean body mass index was 27.91±6.65 kg/m2. Forty-two (44.21%) participants reported practicing physical activities. All participants comple-ted the questionnaires and the cold pressor test with no adver-se events. Fifty-eight (59.18%) participants were classified with fibromyalgia and 40 (40.82%) participants were classified with generalized pain solely. Patients with fibromyalgia had higher number of pain areas in the WPI [fibromyalgia=11.39±3.52, generalized pain=8.67±3.35; p<0.001; power=0.96], more seve-re symptoms in the SSS [fibromyalgia=7.96±2.21, generalized pain=4.30±2.27; p<0.001; power =0.99], and in the PDS [fi-bromyalgia=16.75±5.29, generalized pain=12.97±3.75; p<0.001; power=0.98] than patients with generalized pain (Table 1). A comparison of pain characteristics and functional limitation between patients classified with fibromyalgia and patients clas-sified with generalized pain is presented in table 2. Participants with fibromyalgia presented higher values of pain intensity [fi-
Table 1. Characteristics of the study participants (n= 98)
Characteristics Fibromyalgian=58
Generalized pain n=40
p-value
Gender, n (%), female 52 (89.65%) 31 (77.50%) 0.102
Age, mean (SD) 58.94 (9.43) 56.46 (14.31) 0.305
Weight (kg), mean (SD) 72.59 (12.70) 73.07 (11.72) 0.855
Height (m), mean (SD) 1.61 (0.09) 1.59 (0.09) 0.323
Body mass index (kg/m²), mean (SD) 26.94 (7.30) 29.25 (5.45) 0.113
Physical activity (Yes), n (%) 27 (46.55%) 15 (37.50%) 0.453
WPI (0-19), mean (SD) 11.39 (3.52) 8.67 (3.35) <0.001Continue...
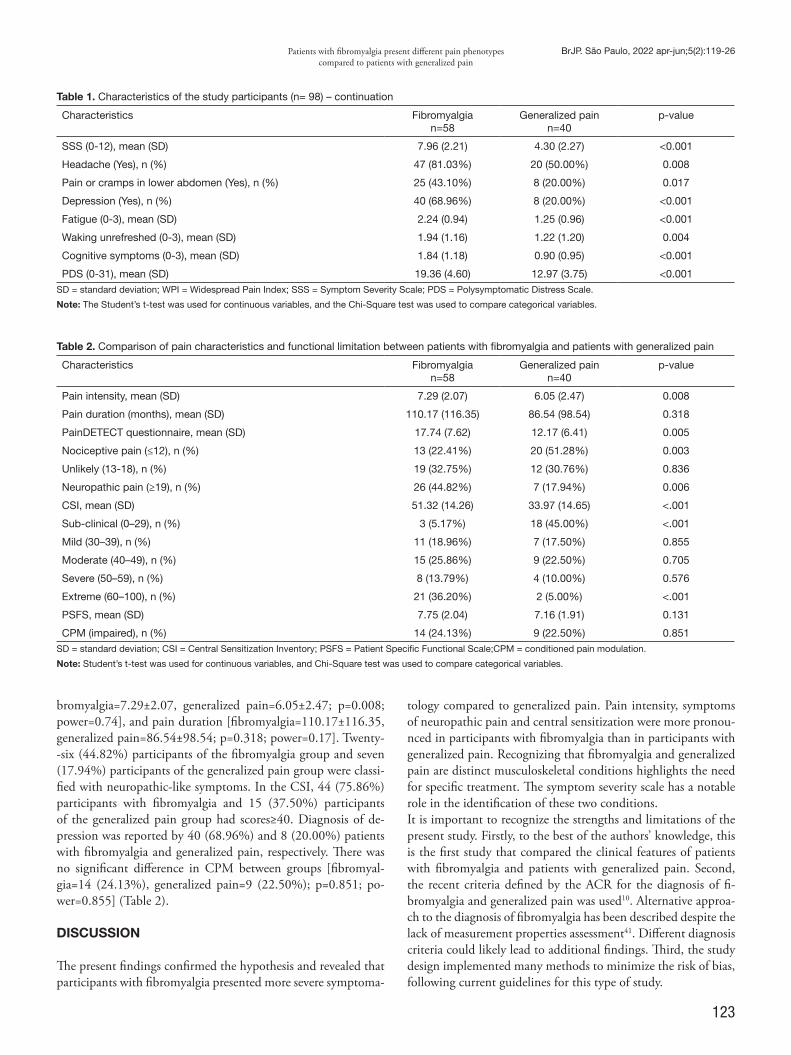
123
Patients with fibromyalgia present different pain phenotypes compared to patients with generalized pain
BrJP. São Paulo, 2022 apr-jun;5(2):119-26
bromyalgia=7.29±2.07, generalized pain=6.05±2.47; p=0.008; power=0.74], and pain duration [fibromyalgia=110.17±116.35, generalized pain=86.54±98.54; p=0.318; power=0.17]. Twenty--six (44.82%) participants of the fibromyalgia group and seven (17.94%) participants of the generalized pain group were classi-fied with neuropathic-like symptoms. In the CSI, 44 (75.86%) participants with fibromyalgia and 15 (37.50%) participants of the generalized pain group had scores≥40. Diagnosis of de-pression was reported by 40 (68.96%) and 8 (20.00%) patients with fibromyalgia and generalized pain, respectively. There was no significant difference in CPM between groups [fibromyal-gia=14 (24.13%), generalized pain=9 (22.50%); p=0.851; po-wer=0.855] (Table 2).
DISCUSSION
The present findings confirmed the hypothesis and revealed that participants with fibromyalgia presented more severe symptoma-
tology compared to generalized pain. Pain intensity, symptoms of neuropathic pain and central sensitization were more pronou-nced in participants with fibromyalgia than in participants with generalized pain. Recognizing that fibromyalgia and generalized pain are distinct musculoskeletal conditions highlights the need for specific treatment. The symptom severity scale has a notable role in the identification of these two conditions. It is important to recognize the strengths and limitations of the present study. Firstly, to the best of the authors’ knowledge, this is the first study that compared the clinical features of patients with fibromyalgia and patients with generalized pain. Second, the recent criteria defined by the ACR for the diagnosis of fi-bromyalgia and generalized pain was used10. Alternative approa-ch to the diagnosis of fibromyalgia has been described despite the lack of measurement properties assessment41. Different diagnosis criteria could likely lead to additional findings. Third, the study design implemented many methods to minimize the risk of bias, following current guidelines for this type of study.
Table 1. Characteristics of the study participants (n= 98) – continuation
Characteristics Fibromyalgian=58
Generalized pain n=40
p-value
SSS (0-12), mean (SD) 7.96 (2.21) 4.30 (2.27) <0.001
Headache (Yes), n (%) 47 (81.03%) 20 (50.00%) 0.008
Pain or cramps in lower abdomen (Yes), n (%) 25 (43.10%) 8 (20.00%) 0.017
Depression (Yes), n (%) 40 (68.96%) 8 (20.00%) <0.001
Fatigue (0-3), mean (SD) 2.24 (0.94) 1.25 (0.96) <0.001
Waking unrefreshed (0-3), mean (SD) 1.94 (1.16) 1.22 (1.20) 0.004
Cognitive symptoms (0-3), mean (SD) 1.84 (1.18) 0.90 (0.95) <0.001
PDS (0-31), mean (SD) 19.36 (4.60) 12.97 (3.75) <0.001SD = standard deviation; WPI = Widespread Pain Index; SSS = Symptom Severity Scale; PDS = Polysymptomatic Distress Scale.
Note: The Student’s t-test was used for continuous variables, and the Chi-Square test was used to compare categorical variables.
Table 2. Comparison of pain characteristics and functional limitation between patients with fibromyalgia and patients with generalized pain
Characteristics Fibromyalgian=58
Generalized pain n=40
p-value
Pain intensity, mean (SD) 7.29 (2.07) 6.05 (2.47) 0.008
Pain duration (months), mean (SD) 110.17 (116.35) 86.54 (98.54) 0.318
PainDETECT questionnaire, mean (SD) 17.74 (7.62) 12.17 (6.41) 0.005
Nociceptive pain (≤12), n (%) 13 (22.41%) 20 (51.28%) 0.003
Unlikely (13-18), n (%) 19 (32.75%) 12 (30.76%) 0.836
Neuropathic pain (≥19), n (%) 26 (44.82%) 7 (17.94%) 0.006
CSI, mean (SD) 51.32 (14.26) 33.97 (14.65) <.001
Sub-clinical (0–29), n (%) 3 (5.17%) 18 (45.00%) <.001
Mild (30–39), n (%) 11 (18.96%) 7 (17.50%) 0.855
Moderate (40–49), n (%) 15 (25.86%) 9 (22.50%) 0.705
Severe (50–59), n (%) 8 (13.79%) 4 (10.00%) 0.576
Extreme (60–100), n (%) 21 (36.20%) 2 (5.00%) <.001
PSFS, mean (SD) 7.75 (2.04) 7.16 (1.91) 0.131
CPM (impaired), n (%) 14 (24.13%) 9 (22.50%) 0.851SD = standard deviation; CSI = Central Sensitization Inventory; PSFS = Patient Specific Functional Scale;CPM = conditioned pain modulation.
Note: Student’s t-test was used for continuous variables, and Chi-Square test was used to compare categorical variables.

124
BrJP. São Paulo, 2022 apr-jun;5(2):119-26 Bittencourt JV, Corrêa LA, Bezerra MC, Reis FJ, Luca K and Nogueira LA
Regarding the limitations of the study, the main one is the rela-tively small number of participants included. Second, there is a lack of objective markers to diagnosis the two health conditions and other comorbidities. Moreover, chronic pain features may be reported dissimilarly using the questionnaire survey or interview survey method42. In comparison to patients with generalized pain, patients with fibromyalgia evidenced more impaired pain characteristics, cor-roborating previous studies13,16,43. In the same way, patients with fibromyalgia diagnosis or people whose symptoms met criteria for fibromyalgia had a greater symptom impact than people with chronic pain44. The present results showed that pain intensity was higher in patients with fibromyalgia compared to generalized pain. However, the findings revealed that pain duration showed no dif-ference between the groups. On the other hand, patients with fibromyalgia in several studies have reported more intense and persistent pain than patients with chronic widespread pain13,45-47. The current study revealed that patients with fibromyalgia pre-sented neuropathic-like symptoms measured by the PainDE-TECT questionnaire and higher levels of symptoms of central sensitization compared to patients with generalized pain. Like-wise, other authors found neuropathic-like symptoms in 67% of patients with fibromyalgia using the PainDETECT questionnai-re19. According to authors, abnormal wind-up and central sensi-tization have been reported in patients with fibromyalgia, which also relate to central pain processing abnormalities22. Interestingly, the level of functional limitation was similar bet-ween the patients with fibromyalgia and patients with genera-lized pain in the current study. There is evidence that patients with fibromyalgia and widespread pain were considered similarly disabling3. However, authors showed that participants with fi-bromyalgia had more pronounced pain-related interference in function and consequences for daily life compared to patients with chronic widespread pain47. The lack of difference in func-tional limitation between groups may be related to identical demographic and lifestyle features (gender, age, weight, height, body mass index and physical activity) of the participants. Fur-thermore, both groups had equivalent physical activity behavior. Individuals with chronic widespread pain with poor physical health and coping response to symptoms were identified as non‐engagers of physical activity48. The present study’s findings revealed that there are no signifi-cant differences in CPM between groups. Likewise, a previous study showed that patients with chronic widespread pain and fibromyalgia syndrome have equal CPM impairment49. On the other hand, a systematic review indicated that CPM seems to be dysfunctional in patients with chronic conditions, such as fi-bromyalgia50. It has been advocated that fibromyalgia syndrome is a condition that revealed clearly CPM impairment18,51. Authors showed that there was a deficit of endogenous pain inhibitory systems in fibromyalgia but not in chronic low back pain18. Similarly, a study showed that impairment in inhibitory pain modulation scores are likely antecedents to chronic wides-pread pain52. Although several studies observed the impairment in inhibitory pain modulation in participants with fibromyalgia and generalized pain, authors showed that results do not support
the idea that a general deficiency of central inhibitory mechanis-ms is a result of fibromyalgia53. Future research in fibromyalgia and generalized pain must em-phasize the use of the SSS as a clinical instrument for diagnosis that facilitates the distinction of these conditions. Although pa-tients with fibromyalgia have generalized pain, clinicians must be aware that fibromyalgia and generalized pain are not the same conditions, and thus they may require specific treatments. The presence of more severe symptomatology in patients with fibromyalgia reveals a need for appropriate therapeutic interven-tions for an assertive treatment for these patients.
CONCLUSION
Patients classified in the fibromyalgia group exhibited higher levels of pain intensity, neuropathic-like symptoms, and symp-toms of central sensitization compared to patients with generali-zed pain. Functional limitation and CPM demonstrated similar results between the two groups. Further studies should investiga-te the features of patients with fibromyalgia and generalized pain to facilitate the decision making of the clinicians.
AUTHORS’ CONTRIBUTIONS
Juliana Valentim Bittencourt Statistical analysis, Funding acquisition, Data Collection, Con-ceptualization, Resource Management, Project Management, Research, Methodology, Writing - Preparation of the original, Writing - Review and Editing, Software, Supervision, Validation, Visualization Leticia Amaral Corrêa Funding acquisition, Data Collection, Conceptualization, Re-source Management, Project Management, Research, Methodo-logy, Writing - Preparation of the original, Writing - Review and Editing, Software, Supervision Márcia Cliton Bezerra Statistical analysis, Funding acquisition, Data Collection, Con-ceptualization, Resource Management, Project Management, Research, Methodology, Writing - Preparation of the original, Writing - Review and Editing, Software, Supervision, Validation, Visualization Felipe José Jandre dos Reis Statistical analysis, Data Collection, Resource Management, Project Management, Methodology, Writing - Preparation of the original, Writing - Review and Editing, Software, Supervision, Validation, Visualization Katie de Luca Data Collection, Project Management, Methodology, Writing - Preparation of the original, Writing - Review and Editing, Soft-ware, Supervision, Validation, Visualization Leandro Alberto Calazans Nogueira Statistical analysis, Funding acquisition, Data Collection, Con-ceptualization, Resource Management, Project Management, Research, Methodology, Writing - Preparation of the original, Writing - Review and Editing, Software, Supervision, Validation, Visualization

125
Patients with fibromyalgia present different pain phenotypes compared to patients with generalized pain
BrJP. São Paulo, 2022 apr-jun;5(2):119-26
Atachment 1. STROBE Checklist of items that should be included in reports of cross-sectional studies
Item no Recommendation Page no
Title and abstract 1 (a) Indicate the study’s design with a commonly used term in the title or the abstract 01-02
(b) Provide in the abstract an informative and balanced summary of what was done and what was found
01-03
Introduction
Background/rationale 2 Explain the scientific background and rationale for the investigation being reported 03-04
Objectives 3 State specific objectives, including any prespecified hypotheses 05
Methods
Study design 4 Present key elements of study design early in the paper 05
Setting 5 Describe the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data collection
07
Participants 6 (a) Give the eligibility criteria, and the sources and methods of selection of participants 07
Variables 7 Clearly define all outcomes, exposures, predictors, potential confounders, and effect modifiers. Give diagnostic criteria, if applicable
09-13
Data sources/ mea-surement
8* For each variable of interest, give sources of data and details of methods of assessment (measu-rement). Describe comparability of assessment methods if there is more than one group
09-13
Bias 9 Describe any efforts to address potential sources of bias -
Study size 10 Explain how the study size was arrived at 13
Quantitative variables 11 Explain how quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen and why
13
Statistical methods 12 (a) Describe all statistical methods, including those used to control for confounding NA
(b) Describe any methods used to examine subgroups and interactions NA
(c) Explain how missing data were addressed NA
(d) If applicable, describe analytical methods taking account of sampling strategy NA
(e) Describe any sensitivity analyses NA
Results
Participants 13* (a) Report numbers of individuals at each stage of study—eg numbers potentially eligible, exa-mined for eligibility, confirmed eligible, included in the study, completing follow-up, and analysed
14
(b) Give reasons for non-participation at each stage NA
(c) Consider use of a flow diagram NA
Descriptive data 14* (a) Give characteristics of study participants (eg demographic, clinical, social) and information on exposures and potential confounders
14-16
(b) Indicate number of participants with missing data for each variable of interest 14-16
Outcome data 15* Report numbers of outcome events or summary measures 14-16
Main results 16 (a) Give unadjusted estimates and, if applicable, confounder-adjusted estimates and their pre-cision (eg, 95% confidence interval). Make clear which confounders were adjusted for and why they were included
13
(b) Report category boundaries when continuous variables were categorized 14-16
(c) If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period
NA
Other analyses 17 Report other analyses done—eg analyses of subgroups and interactions, and sensitivity analyses
NA
Discussion
Key results 18 Summarize key results with reference to study objectives 16
Limitations 19 Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both direction and magnitude of any potential bias
16-17
Interpretation 20 Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results from similar studies, and other relevant evidence
16-19
Generalizability 21 Discuss the generalizability (external validity) of the study results 16-19
Other information
Funding 22 Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on which the present article is based
19
Note: An Explanation and Elaboration article discusses each checklist item and gives methodological background and published examples of transparent reporting. The STROBE checklist is best used in conjunction with this article (freely available on the Web sites of PLoS Medicine at http://www.plosmedicine.org/, Annals of Internal Medicine at http://www.annals.org/, and Epidemiology at http://www.epidem.com/). Information on the STROBE Initiative is available at www.strobe-state-ment.org. *Give information separately for exposed and unexposed groups.
126
BrJP. São Paulo, 2022 apr-jun;5(2):119-26 Bittencourt JV, Corrêa LA, Bezerra MC, Reis FJ, Luca K and Nogueira LA
REFERENCES
1. Branco JC, Bannwarth B, Failde I, Abello Carbonell J, Blotman F, Spaeth M, et al. Prevalence of fibromyalgia: A survey in five European countries. Semin Arthritis Rheum. 2010;39(6):448-53.
2. Vincent A, Lahr BD, Wolfe F, Clauw DJ, Whipple MO, Oh TH, et al. Prevalence of fibromyalgia: a population-based study in Olmsted County, Minnesota, utilizing the Rochester epidemiology project. Arthritis Care Res. 2013;65(5):786-92.
3. Assumpção A, Cavalcante AB, Capela CE, Sauer JF, Chalot SD, Pereira CAB, et al. Pre-valence of fibromyalgia in a low socioeconomic status population. BMC Musculoskelet Disord. 2009;10(1):1-7.
4. Sarzi-Puttini P, Giorgi V, Marotto D, Atzeni F. Fibromyalgia: an update on clinical cha-racteristics, aetiopathogenesis and treatment. Nat Rev Rheumatol. 2020;16(11):645-60.
5. Souza JB, Perissinotti DMN. The prevalence of fibromyalgia in Brazil–a population-ba-sed study with secondary data of the study on chronic pain prevalence in Brazil. BrJP. 2018;17(1):345-8.
6. Mansfield KE, Sim J, Jordan JL, Jordan KP. A systematic review and meta-analysis of the prevalence of chronic widespread pain in the general population. Pain. 2016;157(1):55-63.
7. Shresher NM, Mohamed AE, Elshahaly MH. Performance of 2016 revised fibrom-yalgia diagnostic criteria in patients with rheumatoid arthritis. Rheumatol Int. 2019;39(10):1703-10.
8. Galvez-Sánchez CM, Montoro CI, Duschek S, Del Paso GA. Depression and trait-an-xiety mediate the influence of clinical pain on health-related quality of life in fibromyal-gia. J Affect Disord. 2020;265:486-95.
9. Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C, Goldenberg DL, et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum. 1990;33(2):160-72.
10. Wolfe F, Clauw DJ, Fitzcharles MA, Goldenberg DL, Häuser W, Katz RL, et al. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin Arthritis Rheum. 2016;46(3):319-29.
11. Wolfe F, Clauw DJ, Fitzcharles MA, Goldenberg DL, Katz RS, Mease P, et al. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010;62(5):600-10.
12. Dean LE, Arnold L, Crofford L, Bennett R, Goldenberg D, Fitzcharles M, et al. Impact of moving from a widespread to multisite pain definition on other fibromyalgia symp-toms. Arthritis Care Res (Hoboken). 2017;69(12):1878-86.
13. Toda K. Comparison of symptoms among fibromyalgia syndrome, chronic wides-pread pain, and an incomplete form of chronic widespread pain. J Musculoskelet Pain. 2011;19(1):52-5.
14. Santos AM, Burti JS, Lopes JB, Scazufca M, Marques AP, Pereira RM. Prevalence of fibromyalgia and chronic widespread pain in community-dwelling elderly subjects living in São Paulo, Brazil. Maturitas. 2010;67(3):251-5.
15. Schaefer C, Mann R, Masters ET, Cappelleri JC, Daniel SR, Zlateva G, et al. The com-parative burden of chronic widespread pain and fibromyalgia in the United States. Pain Pract. 2016;16(5):565-79.
16. White KP, Nielson WR, Harth M, Ostbye T, Speechley M. Chronic widespread mus-culoskeletal pain with or without fibromyalgia: Psychological distress in a representative community adult sample. J Rheumatol. 2002;29(3):588-94.
17. Stewart JA, Mailler-Burch S, Müller D, Studer M, von Känel R, Grosse Holtforth M, et al. Rethinking the criteria for fibromyalgia in 2019: The ABC indicators. J Pain Res. 2019;12:2115-24.
18. Julien N, Goffaux P, Arsenault P, Marchand S. Widespread pain in fibromyalgia is rela-ted to a deficit of endogenous pain inhibition. Pain. 2005;114(1-2):295-302.
19. van Bemmel PF, Voshaar MAO, Klooster PMT, Vonkeman HE, van de Laar MA. De-velopment and preliminary evaluation of a short self-report measure of generalized pain hypersensitivity. J Pain Res. 2019;12:395-404.
20. Cagnie B, Coppieters I, Denecker S, Six J, Danneels L, Meeus M. Central sensitization in fibromyalgia? A systematic review on structural and functional brain MRI. Semin Arthritis Rheum. 2014;44(1):68-75.
21. O’Brien AT, Deitos A, Pego YT, Fregni F, Carrillo-de-la-Peña MT. Defective endoge-nous pain modulation in fibromyalgia: a meta-analysis of temporal summation and conditioned pain modulation paradigms. J Pain. 2018;19(8):819-36.
22. Staud R, Smitherman ML. Peripheral and central sensitization in fibromyalgia: pathoge-netic role. Curr Pain Headache Rep. 2002;6(4):259-66.
23. Bittencourt JV, Bezerra MC, Pina MR, Reis FJJ, de Sá Ferreira A, Nogueira LAC. Use of the painDETECT to discriminate musculoskeletal pain phenotypes. Arch Physiother. 2022;12(1):7.
24. Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Bull World Health Organ. 2007;85(11):867-72.
25. Murray CJ, Atkinson C, Bhalla K, Birbeck G, Burstein R, Chou D, Dellavalle R, et al. The state of US health, 1990-2010: burden of diseases, injuries, and risk factors. JAMA. 2013;310(6):591-608.
26. Dudeney J, Law EF, Meyyappan A, Palermo TM, Rabbitts JA. Evaluating the psycho-metric properties of the Widespread Pain Index and the Symptom Severity Scale in youth with painful conditions. Can J Pain. 2019;3(1):137-47.
27. Freynhagen R, Tölle TR, Gockel U, Baron R. The painDETECT project - Far more than a screening tool on neuropathic pain. Curr Med Res Opin. 2016;32(6):1033-57.
28. Horn KK, Jennings S, Richardson G, Vliet DV, Hefford C, Abbott JH. The patient-spe-cific functional scale: Psychometrics, clinimetrics, and application as a clinical outcome measure. J Orthop Sports Phys Ther. 2012;42(1):30-42.
29. Treede RD, Rief W, Barke A, Aziz Q, Bennett MI, Benoliel R, et al. Chronic pain as a symptom or a disease: the IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain. 2019;160(1):19-27.
30. Mayer TG, Neblett R, Cohen H, Howard KJ, Choi YH, Williams MJ, et al. The deve-lopment and psychometric validation of the Central Sensitization Inventory. Pain Pract. 2012;12(4):276-85.
31. Neblett R, Hartzell MM, Mayer TG, Cohen H, Gatchel RJ. Establishing clinically rele-vant severity levels for the Central Sensitization Inventory. Pain Pract. 2017;17(2):166-75.
32. Neblett R, Hartzell MM, Cohen H, Mayer TG, Williams M, Choi YH, et al. Ability of the central sensitization inventory to identify central sensitivity syndromes in an outpa-tient chronic pain sample. Clin J Pain. 2015;31(4):323-32.
33. Tanaka K, Murata S, Nishigami T, Mibu A, Manfuku M, Shinohara Y, et al. The central sensitization inventory predict pain-related disability for musculoskeletal disorders in the primary care setting. Eur J Pain (United Kingdom). 2019;23(9):1640-8.
34. Scerbo T, Colasurdo J, Dunn S, Unger J, Nijs J, Cook C. Measurement properties of the central sensitization inventory: a systematic review. Pain Pract. 2018;18(4):544-54.
35. Caumo W, Antunes LC, Elkfury JL, Herbstrith EG, Busanello Sipmann R, Souza A, et al. The central sensitization inventory validated and adapted for a Brazilian population: psychometric properties and its relationship with brain-derived neurotrophic factor. J Pain Res. 2017;10:2109-22.
36. Freynhagen R, Baron R, Gockel U, Tölle TR. Pain DETECT: a new screening ques-tionnaire to identify neuropathic components in patients with back pain. Curr Med Res Opin. 2006;22(10):1911-20.
37. Rio JPMD, Bittencourt JV, Corrêa LA, Freynhagen R, Reis FJJD, Melo TB, et al. Cros-s-cultural adaptation of the PainDETECT Questionnaire into Brazilian Portuguese Language. Braz J Anesthesiol. 2022;72(1):44-8.
38. Abbott JH, Schmitt J. Minimum important differences for the patient-specific func-tional scale, 4 region-specific outcome measures, and the numeric pain rating scale. J Orthop Sports Phys Ther. 2014;44(8):560-4.
39. Lewis GN, Heales L, Rice DA, Rome K, McNair PJ. Reliability of the conditioned pain modulation paradigm to assess endogenous inhibitory pain pathways. Pain Res Manag. 2012;17(2):98-102.
40. Yarnitsky D, Bouhassira D, Drewes AM, Fillingim RB, Granot M, Hansson P, et al. Recommendations on practice of conditioned pain modulation (CPM) testing. Eur J Pain (United Kingdom). 2015;19(6):805-6.
41. Arnold LM, Bennett RM, Crofford LJ, Dean LE, Clauw DJ, Goldenberg DL, et al. AAPT Diagnostic Criteria for fibromyalgia. J Pain. 2019;20(6):611-28.
42. Steingrímsdóttir ÓA, Landmark T, Macfarlane GJ, Nielsen CS. Defining chro-nic pain in epidemiological studies: a systematic review and meta-analysis. Pain. 2017;158(11):2092-107.
43. Pamuk ÖN, Yethil Y, Çakir N. Factors that affect the number of tender points in fi-bromyalgia and chronic widespread pain patients who did not meet the ACR 1990 Cri-teria for Fibromyalgia: are tender points a reflection of neuropathic pain? Semin Arthritis Rheum. 2006;36(2):130-4.
44. Doebl S, Hollick RJ, Beasley M, Choy E, Macfarlane GJ. Comparing people who have and have not received a diagnosis of fibromyalgia: a cross‐sectional survey within the PACFiND study. Arthritis Care Res (Hoboken). 2021;3 Epub ahead of print.
45. Cöster L, Kendall S, Gerdle B, Henriksson C, Henriksson KG, Bengtsson A. Chronic widespread musculoskeletal pain - A comparison of those who meet criteria for fibrom-yalgia and those who do not. Eur J Pain. 2008;12(5):600-10.
46. White KP, Speechley M, Harth M, Ostbye T. The London Fibromyalgia Epidemiology Study: comparing the demographic and clinical characteristics in 100 random commu-nity cases of fibromyalgia versus controls. J Rheumatol. 1999;26(7):1577-85.
47. Staud R. Chronic widespread pain and fibromyalgia: two sides of the same coin? Curr Rheumatol Rep. 2009;11(6):433-6.
48. Martin KR, Druce KL, Murdoch SE, D’Ambruoso L, Macfarlane GJ. Differences in long-term physical activity trajectories among individuals with chronic widespread pain: a secondary analysis of a randomized controlled trial. Eur J Pain (United Kingdom). 2019;23(8):1437-47.
49. Gerhardt A, Eich W, Treede RD, Tesarz J. Conditioned pain modulation in patients with nonspecific chronic back pain with chronic local pain, chronic widespread pain, and fibromyalgia. Pain. 2017;158(3):430-9.
50. Lewis GN, Rice DA, McNair PJ. Conditioned pain modulation in populations with chronic pain: a systematic review and meta-analysis. J Pain. 2012;13(10):936-44.
51. Jensen KB, Kosek E, Petzke F, Carville S, Fransson P, Marcus H, et al. Evidence of dysfunctional pain inhibition in Fibromyalgia reflected in rACC during provoked pain. Pain. 2009;144(1-2):95-100.
52. Tan AC, Jaaniste T, Champion D. Chronic widespread pain and fibromyalgia syndro-me: life-course risk markers in young people. Pain Res Manag. 2019;2019:6584753.
53. Staud R, Robinson ME, Vierck Jr CJ, Price DD. Diffuse noxious inhibitory controls (DNIC) attenuate temporal summation of second pain in normal males but not in normal females or fibromyalgia patients. Pain. 2003;101(1-2):167-74.

127
ABSTRACT
BACKGROUND AND OBJECTIVES: Low back pain is the leading cause of disability in Brazil. Most of the evidence on in-terventions for chronic low back pain (CLBP) comes from high income countries. The objective was to investigate the feasibility of conducting a program based in exercise and pain education in Primary Health Care supported by low-cost mobile technology for adults with CLBP (versus waiting list) and to explore the profile of patients who adhered compared to those who did not adhere. METHODS: This is a feasibility study with adult residents of Fortaleza, Brazil with CLBP. The Intervention Group consisted of strategies such as physical exercises, pain education, phone calls and support messages to participants. The Control Group was based on a waiting list. Primary outcomes included retention and adherence rates, comprehension of the intervention, credibi-lity, and satisfaction with the intervention. Secondary outcomes included clinical and demographic factors such as pain intensity, disability, recovery prognosis, and physical activity, described ac-cording to adherence behavior.RESULTS: Forty-five individuals were allocated to the Interven-tion Group and 24 to the Control Group. Overall, 57.8% of participants adhered to the intervention. Retention rates were 53.33% and 58.3% for intervention and control, respectively.
Exercise-based and pain education program for adults with chronic low back pain in Brazilian Primary Care: feasibility studyPrograma de exercícios físicos e educação em dor para adultos com dor lombar crônica na Atenção Primária brasileira: estudo de viabilidade
Ana Ellen do Nascimento Santos1, Catharina Saraiva Nobre Cacau2, Ana Carla Lima Nunes3, Fabianna Resende de Jesus-Moraleida4
Ana Ellen do Nascimento Santos – https://orcid.org/0000-0001-8429-324X;Catharina Saraiva Nobre Cacau – https://orcid.org/0000-0002-3374-5522;Ana Carla Lima Nunes – https://orcid.org/0000-0002-7380-6537;Fabianna Resende de Jesus-Moraleida – https://orcid.org/0000-0002-3797-949X. 1. Federal University of Ceará, Master’s Program in Physical Therapy and Functioning, For-taleza, CE, Brazil.2. Public Health School of Ceará, Pediatrics Multiprofessional Residency Program, For-taleza, CE, Brazil.3. Federal University of Ceará, School of Medicine, Physical Therapy Department, Fortaleza, CE, Brazil.4. Federal University of Ceará, School of Medicine, Master’s Program in Physical Therapy and Functioning, Physical Therapy Department, Fortaleza, CE, Brazil.
Submitted on December 22, 2021.Accepted for publication on May 09, 2022.Conflict of interests: none – Sponsoring sources: This study was supported by the Coordina-tion of Improvement of Higher Education Personnel (CAPES) - code 001, the Institutional Scientific Initiation Scholarship Program (PIBIC) and by the Federal University of Ceará Dean’s Office of Extension.
Correspondence to: Ana Ellen do Nascimento Santos E-mail: [email protected]
© Sociedade Brasileira para o Estudo da Dor
The other primary feasibility outcomes were satisfactory. Longer time spent sitting and level of schooling differed the profile of those who adhered to the intervention from those who did not. Higher pain intensity and poorer recovery prognosis, measured at baseline, influenced non-adherence to home exercises. CONCLUSION: The feasibility of the protocol was adequate for the comprehension of the components, however, adherence to the protocol and the follow-up of the participants were low. The profile of individuals adhering to the intervention includes higher schooling and more time spent sitting at baseline. Cha-racteristics such as higher pain intensity and the influence of psychosocial factors influenced non-adherence to home exerci-ses. Brazilian Registry of Clinical Trials (REBEC RBR-5wqr2j).Keywords: Low back pain, Primary Health Care, Treatment adherence and compliance.
RESUMO
JUSTIFICATIVA E OBJETIVOS: A dor lombar é a principal causa de incapacidade no Brasil. A maior parte da evidência so-bre intervenções para dor lombar crônica (DLC) advém de países desenvolvidos. O objetivo deste estudo foi investigar a viabilida-de de conduzir um programa baseado em exercícios e educação em dor na Atenção Primária à Saúde para adultos com DLC (versus lista de espera) e explorar o perfil dos pacientes que aderi-ram comparado aos que não aderiram à intervenção. MÉTODOS: Este é um estudo de viabilidade. Foram incluídos adultos com DLC e residentes em Fortaleza, CE, no Brasil. O Grupo Intervenção foi composto por estratégias como exercícios físicos, educação em dor, ligações telefônicas e mensagens de suporte aos participantes. O Grupo Controle consistiu em lista de espera. Os desfechos primários incluíram taxas de retenção e adesão, entendimento da intervenção, credibilidade e satisfação com a intervenção. Os desfechos secundários incluíram fatores clínicos e demográficos, como intensidade de dor, incapacidade, prognóstico de recuperação e atividade física, descritos segundo comportamento de adesão.RESULTADOS: Quarenta e cinco indivíduos foram alocados para o Grupo Intervenção e 24 para o Grupo Controle. Em ge-ral, 57,8% dos participantes aderiram à intervenção. As taxas de retenção foram 53,33% e 58,3% para intervenção e controle, respectivamente. Os demais desfechos primários de viabilidade foram satisfatórios. Maior tempo sentado e o grau de instrução diferiam o perfil dos aderentes dos não aderentes à intervenção. Maior intensidade de dor e pior prognóstico de recuperação,
BrJP. São Paulo, 2022 apr-jun;5(2):127-36
DOI 10.5935/2595-0118.20220032-en
ORIGINAL ARTICLE

128
BrJP. São Paulo, 2022 apr-jun;5(2):127-36 Santos AE, Cacau CS, Nunes AC and Jesus-Moraleida FR
mensurados na avaliação, influenciaram a não adesão aos exer-cícios domiciliares. CONCLUSÃO: A viabilidade do protocolo apresentou-se ade-quada para entendimento dos componentes. Entretanto, a adesão ao protocolo e o seguimento dos participantes foram baixos. O perfil dos indivíduos aderentes à intervenção incluiu maior instru-ção e mais tempo sentado na sua avaliação inicial. Características como maior intensidade de dor e influência de fatores psicossociais influenciaram a não adesão aos exercícios domiciliares. Registro Brasileiro de Ensaios Clínicos (REBEC RBR-5wqr2j).Descritores: Atenção Primária à Saúde, Cooperação e adesão ao tratamento, Dor lombar.
INTRODUCTION
Low back pain (LBP) is the leading cause of disability in the world. In the last decades, the growth of this condition’s global burden has been alarming, mainly due to the increased disability of individuals in low and middle income countries1. In Brazil, the data points to an annual prevalence of more than 50% of LBP in adults, and a prevalence of chronic low back pain (CLBP) of up to 14.7%2. The impact of LBP in the Brazilian population has resulted in an increase of 79.9% in the total number of years lived with disability in the last 30 years, making this condition responsible for the largest number of years lived with disability and the most frequent reason for absenteeism3. In order to reduce disability, international clinical guidelines recommend the management of CLBP in primary care and emphasize the use of multifaceted approaches based on the biopsychosocial model4. Therapeutic exercise, education, coun-seling for self-management, and psychological therapies are re-commended for the first line of care for LBP5. In Brazil, multi-faceted strategies involving education and group exercises have not been the target of investigations in primary care. Currently, most national studies focus on investigating manual techni-ques6-8, specific exercise modalities9-14 and physical agents15,16, usually delivered individually in specialized outpatient services. This scenario shows the need for exploration regarding how transferable this evidence from the first line of care in the Bra-zilian primary health care system is, since this approach would have the potential to reduce the impact of LBP on functioning and generate less costs.As much as multifaceted strategies show good results for pa-tients with LBP around the world17,18, treatment adherence is a major challenge. According to the World Health Organization (WHO), the rates of non-adherence to long-term treatment for musculoskeletal conditions are high, around 50%19. In ad-dition, the international literature also points out that intrin-sic and extrinsic factors to the individual with CLBP interfere with adherence to an education and exercise therapy program, such as low level of physical activities, anxiety and depression, increased pain during exercise, and a greater number of bar-riers20. However, little is known about adherence, acceptance, and factors related to adult participation within a program ba-sed on the first line of care in low-income communities in the Brazilian context.
Given the scarcity of national evidence on implementation of the first line of care for CLBP, as well as lack of information on adherence and acceptance rates of a multifaceted intervention in the primary care setting in Brazil, a feasibility study is necessary. From this perspective, the primary objective of the present feasi-bility study was to investigate the feasibility related to adherence, retention, and acceptability of a multifaceted program based on exercise and pain education in Primary Health Care in indivi-duals with CLBP supported by low-cost mobile technology. The aim was also to explore the sociodemographic and clinical profile of patients who adhere to the intervention compared to those who do not. Describing clinical measures of this type of proposal configured the secondary objectives of the study.
METHODS
The present research is a two-arm parallel feasibility study with a 2:1 allocation ratio, reported according to the CONSORT gui-delines for feasibility studies of clinical trials21 and registered in the Brazilian Registry of Clinical Trials (REBEC RBR-5wqr2j). The present study is linked to the Project Movement of the Federal University of Ceará (UFC) Physical Therapy Depart-ment. This project is an extension action that aims at the free treatment and follow-up of people with chronic musculoskele-tal pain through physical exercises combined with educational strategies for the adoption of an active lifestyle with the objec-tive of managing pain. Project Movement has a team of stu-dents and volunteer physical therapists who perform assistance actions in a group format in the Physical Therapy Department of UFC and in a primary care unit in Fortaleza/Ceará.Participants were selected between August 2018 and August 2019. Participants were recruited by active search in health centers of Fortaleza, referral by health professionals, telephone contact, and announcement on social networks (Facebook and Instagram). Individuals interested in participating in the study were contacted by the research team and screened for eligibi-lity. Individuals with a primary musculoskeletal complaint of LBP (between the 12th thoracic vertebra to the gluteal fold) for three or more months, with or without irradiation of symp-toms to the lower limbs, aged over 18 years, of both genders and residing in the city of Fortaleza were included.The exclusion criteria were: individuals with severe auditory or cognitive deficits that prevented them from answering the questionnaires, those who complained of LBP with a specific diagnosed origin (fracture, tumor, vertebral stenosis), severe associated systemic or neurological disease, history of spinal surgery, or in concomitant physical therapy treatments for CLBP, or who did not have a cell phone. Those using drugs with analgesic action were not excluded from the project, but the amount and type of drug used were recorded in the pre- and post-intervention periods.
InterventionThis program was described according to the Template for In-tervention Description and Replication (TIDieR)22. The In-tervention Group consisted of a weekly group program (4-6
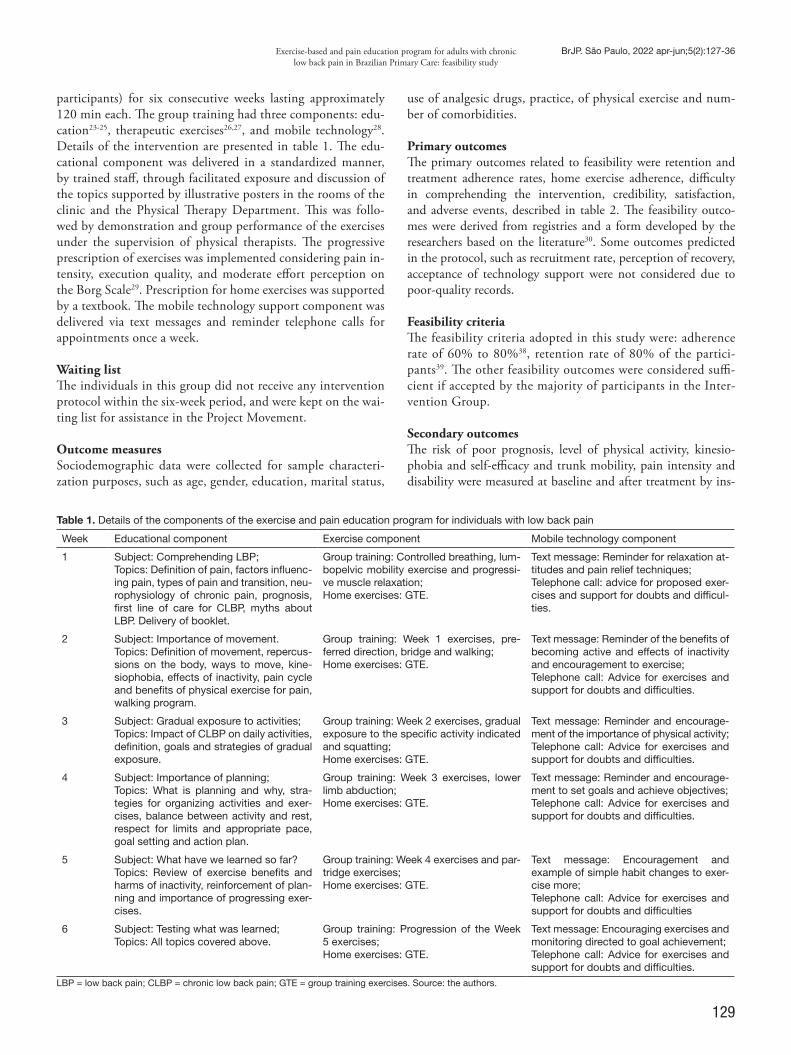
129
Exercise-based and pain education program for adults with chronic low back pain in Brazilian Primary Care: feasibility study
BrJP. São Paulo, 2022 apr-jun;5(2):127-36
participants) for six consecutive weeks lasting approximately 120 min each. The group training had three components: edu-cation23-25, therapeutic exercises26,27, and mobile technology28. Details of the intervention are presented in table 1. The edu-cational component was delivered in a standardized manner, by trained staff, through facilitated exposure and discussion of the topics supported by illustrative posters in the rooms of the clinic and the Physical Therapy Department. This was follo-wed by demonstration and group performance of the exercises under the supervision of physical therapists. The progressive prescription of exercises was implemented considering pain in-tensity, execution quality, and moderate effort perception on the Borg Scale29. Prescription for home exercises was supported by a textbook. The mobile technology support component was delivered via text messages and reminder telephone calls for appointments once a week.
Waiting listThe individuals in this group did not receive any intervention protocol within the six-week period, and were kept on the wai-ting list for assistance in the Project Movement.
Outcome measures Sociodemographic data were collected for sample characteri-zation purposes, such as age, gender, education, marital status,
use of analgesic drugs, practice, of physical exercise and num-ber of comorbidities.
Primary outcomesThe primary outcomes related to feasibility were retention and treatment adherence rates, home exercise adherence, difficulty in comprehending the intervention, credibility, satisfaction, and adverse events, described in table 2. The feasibility outco-mes were derived from registries and a form developed by the researchers based on the literature30. Some outcomes predicted in the protocol, such as recruitment rate, perception of recovery, acceptance of technology support were not considered due to poor-quality records.
Feasibility criteria The feasibility criteria adopted in this study were: adherence rate of 60% to 80%38, retention rate of 80% of the partici-pants39. The other feasibility outcomes were considered suffi-cient if accepted by the majority of participants in the Inter-vention Group.
Secondary outcomesThe risk of poor prognosis, level of physical activity, kinesio-phobia and self-efficacy and trunk mobility, pain intensity and disability were measured at baseline and after treatment by ins-
Table 1. Details of the components of the exercise and pain education program for individuals with low back pain
Week Educational component Exercise component Mobile technology component
1 Subject: Comprehending LBP;Topics: Definition of pain, factors influenc-ing pain, types of pain and transition, neu-rophysiology of chronic pain, prognosis, first line of care for CLBP, myths about LBP. Delivery of booklet.
Group training: Controlled breathing, lum-bopelvic mobility exercise and progressi-ve muscle relaxation;Home exercises: GTE.
Text message: Reminder for relaxation at-titudes and pain relief techniques;Telephone call: advice for proposed exer-cises and support for doubts and difficul-ties.
2 Subject: Importance of movement.Topics: Definition of movement, repercus-sions on the body, ways to move, kine-siophobia, effects of inactivity, pain cycle and benefits of physical exercise for pain, walking program.
Group training: Week 1 exercises, pre-ferred direction, bridge and walking;Home exercises: GTE.
Text message: Reminder of the benefits of becoming active and effects of inactivity and encouragement to exercise;Telephone call: Advice for exercises and support for doubts and difficulties.
3 Subject: Gradual exposure to activities;Topics: Impact of CLBP on daily activities, definition, goals and strategies of gradual exposure.
Group training: Week 2 exercises, gradual exposure to the specific activity indicated and squatting;Home exercises: GTE.
Text message: Reminder and encourage-ment of the importance of physical activity;Telephone call: Advice for exercises and support for doubts and difficulties.
4 Subject: Importance of planning;Topics: What is planning and why, stra-tegies for organizing activities and exer-cises, balance between activity and rest, respect for limits and appropriate pace, goal setting and action plan.
Group training: Week 3 exercises, lower limb abduction;Home exercises: GTE.
Text message: Reminder and encourage-ment to set goals and achieve objectives;Telephone call: Advice for exercises and support for doubts and difficulties.
5 Subject: What have we learned so far?Topics: Review of exercise benefits and harms of inactivity, reinforcement of plan-ning and importance of progressing exer-cises.
Group training: Week 4 exercises and par-tridge exercises;Home exercises: GTE.
Text message: Encouragement and example of simple habit changes to exer-cise more;Telephone call: Advice for exercises and support for doubts and difficulties
6 Subject: Testing what was learned;Topics: All topics covered above.
Group training: Progression of the Week 5 exercises; Home exercises: GTE.
Text message: Encouraging exercises and monitoring directed to goal achievement;Telephone call: Advice for exercises and support for doubts and difficulties.
LBP = low back pain; CLBP = chronic low back pain; GTE = group training exercises. Source: the authors.
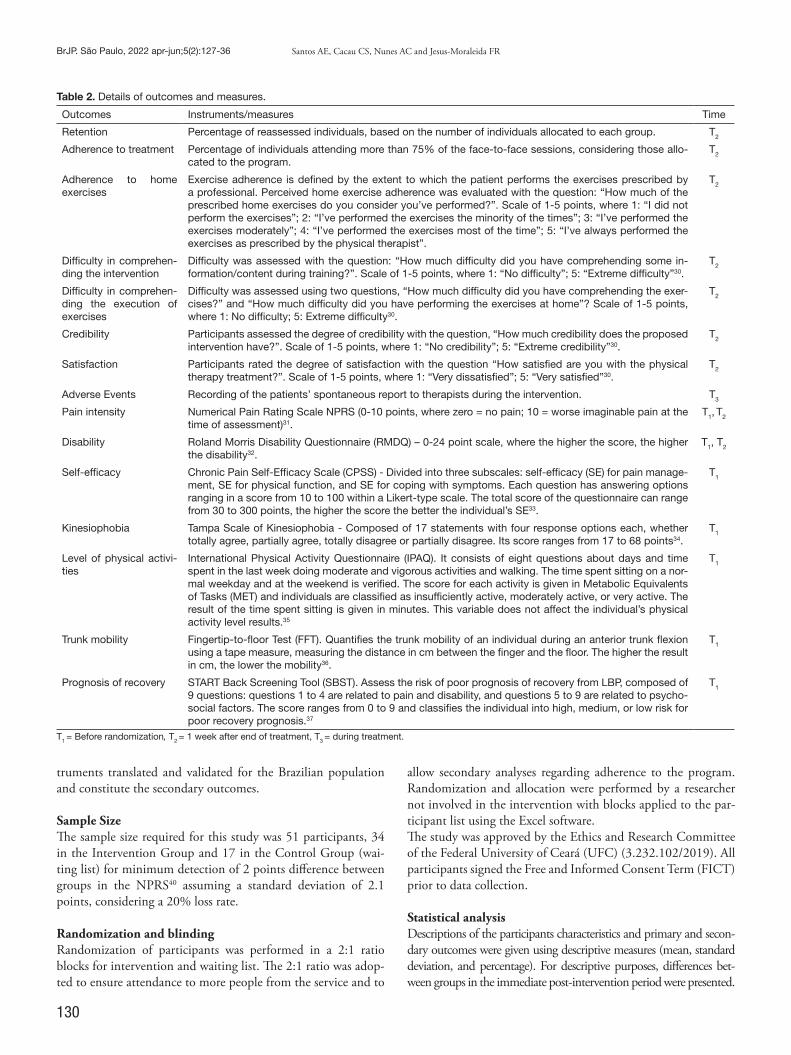
130
BrJP. São Paulo, 2022 apr-jun;5(2):127-36 Santos AE, Cacau CS, Nunes AC and Jesus-Moraleida FR
truments translated and validated for the Brazilian population and constitute the secondary outcomes.
Sample SizeThe sample size required for this study was 51 participants, 34 in the Intervention Group and 17 in the Control Group (wai-ting list) for minimum detection of 2 points difference between groups in the NPRS40 assuming a standard deviation of 2.1 points, considering a 20% loss rate.
Randomization and blindingRandomization of participants was performed in a 2:1 ratio blocks for intervention and waiting list. The 2:1 ratio was adop-ted to ensure attendance to more people from the service and to
allow secondary analyses regarding adherence to the program. Randomization and allocation were performed by a researcher not involved in the intervention with blocks applied to the par-ticipant list using the Excel software.The study was approved by the Ethics and Research Committee of the Federal University of Ceará (UFC) (3.232.102/2019). All participants signed the Free and Informed Consent Term (FICT) prior to data collection.
Statistical analysisDescriptions of the participants characteristics and primary and secon-dary outcomes were given using descriptive measures (mean, standard deviation, and percentage). For descriptive purposes, differences bet-ween groups in the immediate post-intervention period were presented.
Table 2. Details of outcomes and measures.
Outcomes Instruments/measures Time
Retention Percentage of reassessed individuals, based on the number of individuals allocated to each group. T2
Adherence to treatment Percentage of individuals attending more than 75% of the face-to-face sessions, considering those allo-cated to the program.
T2
Adherence to home exercises
Exercise adherence is defined by the extent to which the patient performs the exercises prescribed by a professional. Perceived home exercise adherence was evaluated with the question: “How much of the prescribed home exercises do you consider you’ve performed?”. Scale of 1-5 points, where 1: “I did not perform the exercises”; 2: “I’ve performed the exercises the minority of the times”; 3: “I’ve performed the exercises moderately”; 4: “I’ve performed the exercises most of the time”; 5: “I’ve always performed the exercises as prescribed by the physical therapist”.
T2
Difficulty in comprehen-ding the intervention
Difficulty was assessed with the question: “How much difficulty did you have comprehending some in-formation/content during training?”. Scale of 1-5 points, where 1: “No difficulty”; 5: “Extreme difficulty”30.
T2
Difficulty in comprehen-ding the execution of exercises
Difficulty was assessed using two questions, “How much difficulty did you have comprehending the exer-cises?” and “How much difficulty did you have performing the exercises at home”? Scale of 1-5 points, where 1: No difficulty; 5: Extreme difficulty30.
T2
Credibility Participants assessed the degree of credibility with the question, “How much credibility does the proposed intervention have?”. Scale of 1-5 points, where 1: “No credibility”; 5: “Extreme credibility”30.
T2
Satisfaction Participants rated the degree of satisfaction with the question “How satisfied are you with the physical therapy treatment?”. Scale of 1-5 points, where 1: “Very dissatisfied”; 5: “Very satisfied”30.
T2
Adverse Events Recording of the patients’ spontaneous report to therapists during the intervention. T3
Pain intensity Numerical Pain Rating Scale NPRS (0-10 points, where zero = no pain; 10 = worse imaginable pain at the time of assessment)31.
T1, T2
Disability Roland Morris Disability Questionnaire (RMDQ) – 0-24 point scale, where the higher the score, the higher the disability32.
T1, T2
Self-efficacy Chronic Pain Self-Efficacy Scale (CPSS) - Divided into three subscales: self-efficacy (SE) for pain manage-ment, SE for physical function, and SE for coping with symptoms. Each question has answering options ranging in a score from 10 to 100 within a Likert-type scale. The total score of the questionnaire can range from 30 to 300 points, the higher the score the better the individual’s SE33.
T1
Kinesiophobia Tampa Scale of Kinesiophobia - Composed of 17 statements with four response options each, whether totally agree, partially agree, totally disagree or partially disagree. Its score ranges from 17 to 68 points34.
T1
Level of physical activi-ties
International Physical Activity Questionnaire (IPAQ). It consists of eight questions about days and time spent in the last week doing moderate and vigorous activities and walking. The time spent sitting on a nor-mal weekday and at the weekend is verified. The score for each activity is given in Metabolic Equivalents of Tasks (MET) and individuals are classified as insufficiently active, moderately active, or very active. The result of the time spent sitting is given in minutes. This variable does not affect the individual’s physical activity level results.35
T1
Trunk mobility Fingertip-to-floor Test (FFT). Quantifies the trunk mobility of an individual during an anterior trunk flexion using a tape measure, measuring the distance in cm between the finger and the floor. The higher the result in cm, the lower the mobility36.
T1
Prognosis of recovery START Back Screening Tool (SBST). Assess the risk of poor prognosis of recovery from LBP, composed of 9 questions: questions 1 to 4 are related to pain and disability, and questions 5 to 9 are related to psycho-social factors. The score ranges from 0 to 9 and classifies the individual into high, medium, or low risk for poor recovery prognosis.37
T1
T1 = Before randomization, T2 = 1 week after end of treatment, T3 = during treatment.
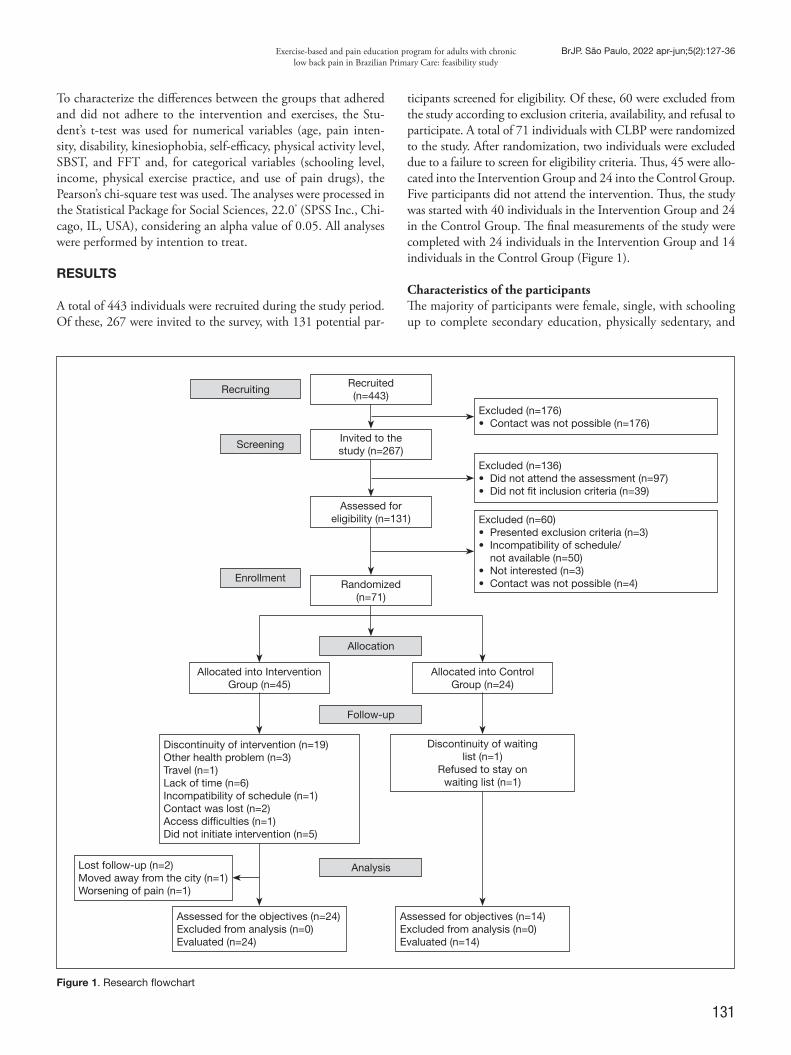
131
Exercise-based and pain education program for adults with chronic low back pain in Brazilian Primary Care: feasibility study
BrJP. São Paulo, 2022 apr-jun;5(2):127-36
To characterize the differences between the groups that adhered and did not adhere to the intervention and exercises, the Stu-dent’s t-test was used for numerical variables (age, pain inten-sity, disability, kinesiophobia, self-efficacy, physical activity level, SBST, and FFT and, for categorical variables (schooling level, income, physical exercise practice, and use of pain drugs), the Pearson’s chi-square test was used. The analyses were processed in the Statistical Package for Social Sciences, 22.0® (SPSS Inc., Chi-cago, IL, USA), considering an alpha value of 0.05. All analyses were performed by intention to treat.
RESULTS
A total of 443 individuals were recruited during the study period. Of these, 267 were invited to the survey, with 131 potential par-
ticipants screened for eligibility. Of these, 60 were excluded from the study according to exclusion criteria, availability, and refusal to participate. A total of 71 individuals with CLBP were randomized to the study. After randomization, two individuals were excluded due to a failure to screen for eligibility criteria. Thus, 45 were allo-cated into the Intervention Group and 24 into the Control Group. Five participants did not attend the intervention. Thus, the study was started with 40 individuals in the Intervention Group and 24 in the Control Group. The final measurements of the study were completed with 24 individuals in the Intervention Group and 14 individuals in the Control Group (Figure 1).
Characteristics of the participantsThe majority of participants were female, single, with schooling up to complete secondary education, physically sedentary, and
Figure 1. Research flowchart
Recruiting
Screening
Enrollment
Recruited (n=443)
Excluded (n=176)• Contact was not possible (n=176)
Excluded (n=136)• Did not attend the assessment (n=97)• Did not fit inclusion criteria (n=39)
Excluded (n=60)• Presented exclusion criteria (n=3)• Incompatibility of schedule/
not available (n=50)• Not interested (n=3)• Contact was not possible (n=4)
Invited to the study (n=267)
Assessed for eligibility (n=131)
Allocated into Intervention Group (n=45)
Discontinuity of intervention (n=19)Other health problem (n=3)Travel (n=1)Lack of time (n=6)Incompatibility of schedule (n=1)Contact was lost (n=2)Access difficulties (n=1)Did not initiate intervention (n=5)
Assessed for the objectives (n=24)Excluded from analysis (n=0)Evaluated (n=24)
Lost follow-up (n=2)Moved away from the city (n=1)Worsening of pain (n=1)
Allocated into Control Group (n=24)
Discontinuity of waiting list (n=1)
Refused to stay on waiting list (n=1)
Assessed for objectives (n=14)Excluded from analysis (n=0)Evaluated (n=14)
Randomized (n=71)
Allocation
Follow-up
Analysis
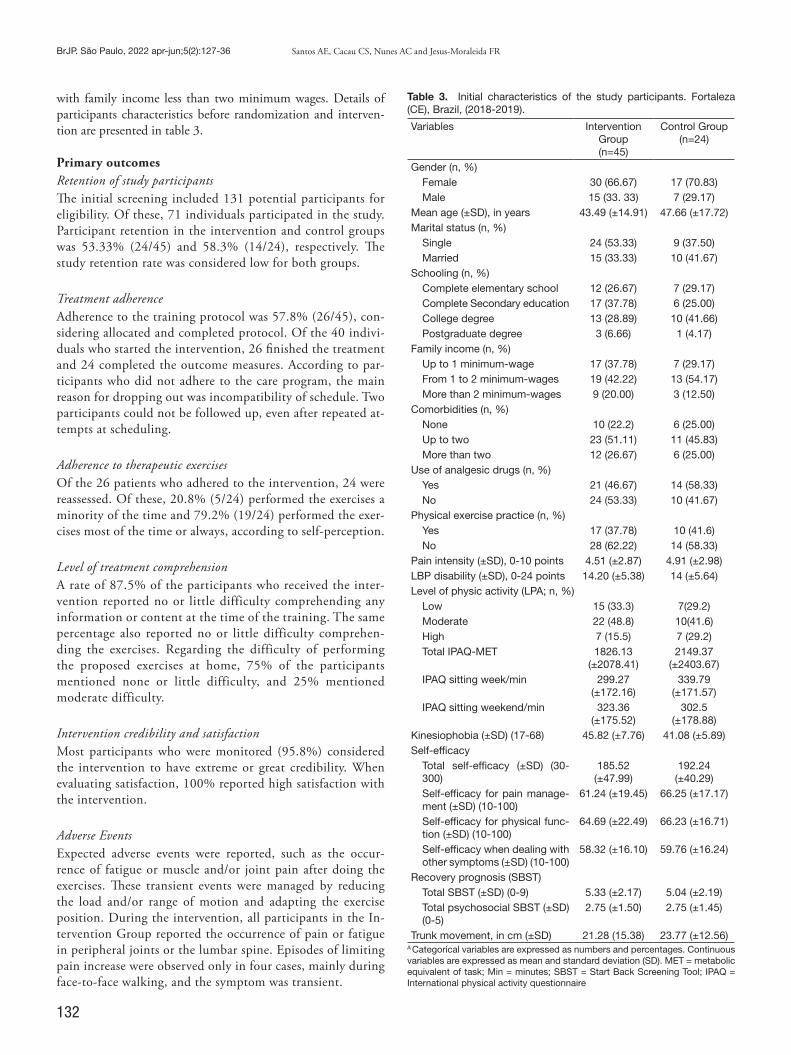
132
BrJP. São Paulo, 2022 apr-jun;5(2):127-36 Santos AE, Cacau CS, Nunes AC and Jesus-Moraleida FR
with family income less than two minimum wages. Details of participants characteristics before randomization and interven-tion are presented in table 3.
Primary outcomesRetention of study participantsThe initial screening included 131 potential participants for eligibility. Of these, 71 individuals participated in the study. Participant retention in the intervention and control groups was 53.33% (24/45) and 58.3% (14/24), respectively. The study retention rate was considered low for both groups.
Treatment adherenceAdherence to the training protocol was 57.8% (26/45), con-sidering allocated and completed protocol. Of the 40 indivi-duals who started the intervention, 26 finished the treatment and 24 completed the outcome measures. According to par-ticipants who did not adhere to the care program, the main reason for dropping out was incompatibility of schedule. Two participants could not be followed up, even after repeated at-tempts at scheduling.
Adherence to therapeutic exercisesOf the 26 patients who adhered to the intervention, 24 were reassessed. Of these, 20.8% (5/24) performed the exercises a minority of the time and 79.2% (19/24) performed the exer-cises most of the time or always, according to self-perception.
Level of treatment comprehensionA rate of 87.5% of the participants who received the inter-vention reported no or little difficulty comprehending any information or content at the time of the training. The same percentage also reported no or little difficulty comprehen-ding the exercises. Regarding the difficulty of performing the proposed exercises at home, 75% of the participants mentioned none or little difficulty, and 25% mentioned moderate difficulty.
Intervention credibility and satisfactionMost participants who were monitored (95.8%) considered the intervention to have extreme or great credibility. When evaluating satisfaction, 100% reported high satisfaction with the intervention.
Adverse EventsExpected adverse events were reported, such as the occur-rence of fatigue or muscle and/or joint pain after doing the exercises. These transient events were managed by reducing the load and/or range of motion and adapting the exercise position. During the intervention, all participants in the In-tervention Group reported the occurrence of pain or fatigue in peripheral joints or the lumbar spine. Episodes of limiting pain increase were observed only in four cases, mainly during face-to-face walking, and the symptom was transient.
Table 3. Initial characteristics of the study participants. Fortaleza (CE), Brazil, (2018-2019).
Variables Intervention Group(n=45)
Control Group(n=24)
Gender (n, %)Female 30 (66.67) 17 (70.83)Male 15 (33. 33) 7 (29.17)
Mean age (±SD), in years 43.49 (±14.91) 47.66 (±17.72)Marital status (n, %)
Single 24 (53.33) 9 (37.50)Married 15 (33.33) 10 (41.67)
Schooling (n, %)Complete elementary school 12 (26.67) 7 (29.17)Complete Secondary education 17 (37.78) 6 (25.00)College degree 13 (28.89) 10 (41.66)Postgraduate degree 3 (6.66) 1 (4.17)
Family income (n, %)Up to 1 minimum-wage 17 (37.78) 7 (29.17)From 1 to 2 minimum-wages 19 (42.22) 13 (54.17)More than 2 minimum-wages 9 (20.00) 3 (12.50)
Comorbidities (n, %)None 10 (22.2) 6 (25.00)Up to two 23 (51.11) 11 (45.83)More than two 12 (26.67) 6 (25.00)
Use of analgesic drugs (n, %)Yes 21 (46.67) 14 (58.33)No 24 (53.33) 10 (41.67)
Physical exercise practice (n, %)Yes 17 (37.78) 10 (41.6)No 28 (62.22) 14 (58.33)
Pain intensity (±SD), 0-10 points 4.51 (±2.87) 4.91 (±2.98)LBP disability (±SD), 0-24 points 14.20 (±5.38) 14 (±5.64)Level of physic activity (LPA; n, %)
Low 15 (33.3) 7(29.2)Moderate 22 (48.8) 10(41.6)High 7 (15.5) 7 (29.2)Total IPAQ-MET 1826.13
(±2078.41)2149.37
(±2403.67)IPAQ sitting week/min 299.27
(±172.16)339.79
(±171.57)IPAQ sitting weekend/min 323.36
(±175.52)302.5
(±178.88)Kinesiophobia (±SD) (17-68) 45.82 (±7.76) 41.08 (±5.89)Self-efficacy
Total self-efficacy (±SD) (30-300)
185.52 (±47.99)
192.24 (±40.29)
Self-efficacy for pain manage-ment (±SD) (10-100)
61.24 (±19.45) 66.25 (±17.17)
Self-efficacy for physical func-tion (±SD) (10-100)
64.69 (±22.49) 66.23 (±16.71)
Self-efficacy when dealing with other symptoms (±SD) (10-100)
58.32 (±16.10) 59.76 (±16.24)
Recovery prognosis (SBST)Total SBST (±SD) (0-9) 5.33 (±2.17) 5.04 (±2.19)Total psychosocial SBST (±SD) (0-5)
2.75 (±1.50) 2.75 (±1.45)
Trunk movement, in cm (±SD) 21.28 (15.38) 23.77 (±12.56)A Categorical variables are expressed as numbers and percentages. Continuous variables are expressed as mean and standard deviation (SD). MET = metabolic equivalent of task; Min = minutes; SBST = Start Back Screening Tool; IPAQ = International physical activity questionnaire
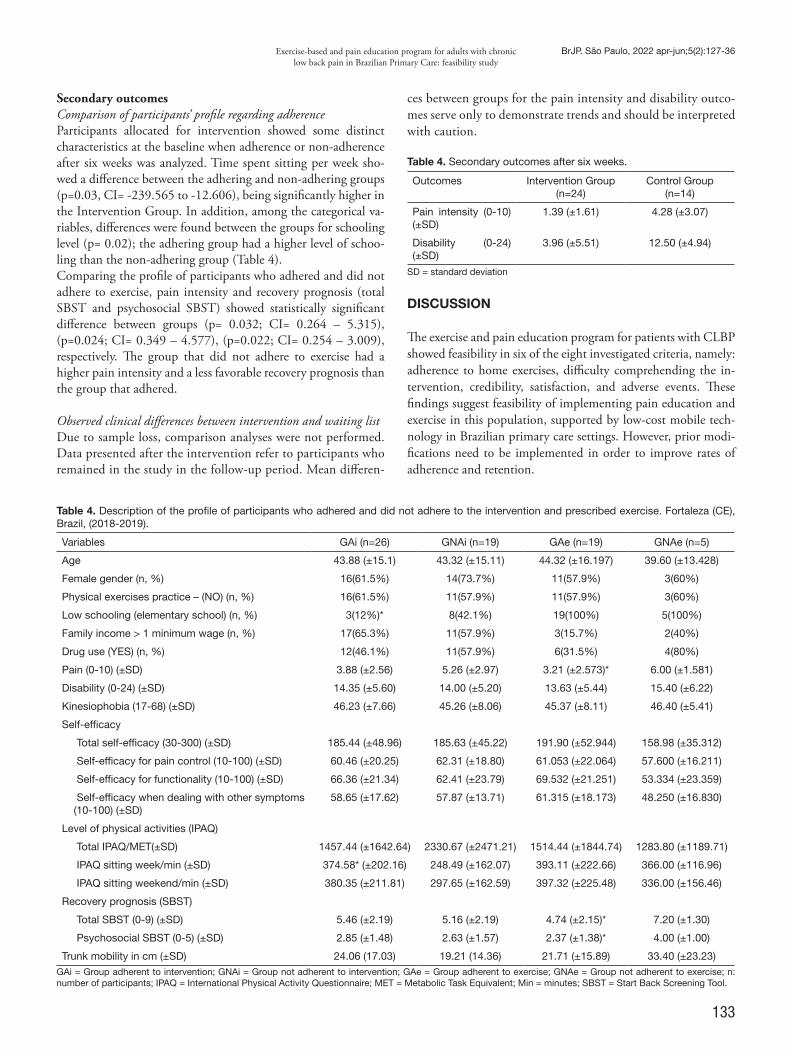
133
Exercise-based and pain education program for adults with chronic low back pain in Brazilian Primary Care: feasibility study
BrJP. São Paulo, 2022 apr-jun;5(2):127-36
Secondary outcomesComparison of participants’ profile regarding adherenceParticipants allocated for intervention showed some distinct characteristics at the baseline when adherence or non-adherence after six weeks was analyzed. Time spent sitting per week sho-wed a difference between the adhering and non-adhering groups (p=0.03, CI= -239.565 to -12.606), being significantly higher in the Intervention Group. In addition, among the categorical va-riables, differences were found between the groups for schooling level (p= 0.02); the adhering group had a higher level of schoo-ling than the non-adhering group (Table 4).Comparing the profile of participants who adhered and did not adhere to exercise, pain intensity and recovery prognosis (total SBST and psychosocial SBST) showed statistically significant difference between groups (p= 0.032; CI= 0.264 – 5.315), (p=0.024; CI= 0.349 – 4.577), (p=0.022; CI= 0.254 – 3.009), respectively. The group that did not adhere to exercise had a higher pain intensity and a less favorable recovery prognosis than the group that adhered.
Observed clinical differences between intervention and waiting listDue to sample loss, comparison analyses were not performed. Data presented after the intervention refer to participants who remained in the study in the follow-up period. Mean differen-
ces between groups for the pain intensity and disability outco-mes serve only to demonstrate trends and should be interpreted with caution.
Table 4. Secondary outcomes after six weeks.
Outcomes Intervention Group (n=24)
Control Group (n=14)
Pain intensity (0-10) (±SD)
1.39 (±1.61) 4.28 (±3.07)
Disability (0-24) (±SD)
3.96 (±5.51) 12.50 (±4.94)
SD = standard deviation
DISCUSSION
The exercise and pain education program for patients with CLBP showed feasibility in six of the eight investigated criteria, namely: adherence to home exercises, difficulty comprehending the in-tervention, credibility, satisfaction, and adverse events. These findings suggest feasibility of implementing pain education and exercise in this population, supported by low-cost mobile tech-nology in Brazilian primary care settings. However, prior modi-fications need to be implemented in order to improve rates of adherence and retention.
Table 4. Description of the profile of participants who adhered and did not adhere to the intervention and prescribed exercise. Fortaleza (CE), Brazil, (2018-2019).
Variables GAi (n=26) GNAi (n=19) GAe (n=19) GNAe (n=5)
Age 43.88 (±15.1) 43.32 (±15.11) 44.32 (±16.197) 39.60 (±13.428)
Female gender (n, %) 16(61.5%) 14(73.7%) 11(57.9%) 3(60%)
Physical exercises practice – (NO) (n, %) 16(61.5%) 11(57.9%) 11(57.9%) 3(60%)
Low schooling (elementary school) (n, %) 3(12%)* 8(42.1%) 19(100%) 5(100%)
Family income > 1 minimum wage (n, %) 17(65.3%) 11(57.9%) 3(15.7%) 2(40%)
Drug use (YES) (n, %) 12(46.1%) 11(57.9%) 6(31.5%) 4(80%)
Pain (0-10) (±SD) 3.88 (±2.56) 5.26 (±2.97) 3.21 (±2.573)* 6.00 (±1.581)
Disability (0-24) (±SD) 14.35 (±5.60) 14.00 (±5.20) 13.63 (±5.44) 15.40 (±6.22)
Kinesiophobia (17-68) (±SD) 46.23 (±7.66) 45.26 (±8.06) 45.37 (±8.11) 46.40 (±5.41)
Self-efficacy
Total self-efficacy (30-300) (±SD) 185.44 (±48.96) 185.63 (±45.22) 191.90 (±52.944) 158.98 (±35.312)
Self-efficacy for pain control (10-100) (±SD) 60.46 (±20.25) 62.31 (±18.80) 61.053 (±22.064) 57.600 (±16.211)
Self-efficacy for functionality (10-100) (±SD) 66.36 (±21.34) 62.41 (±23.79) 69.532 (±21.251) 53.334 (±23.359)
Self-efficacy when dealing with other symptoms (10-100) (±SD)
58.65 (±17.62) 57.87 (±13.71) 61.315 (±18.173) 48.250 (±16.830)
Level of physical activities (IPAQ)
Total IPAQ/MET(±SD) 1457.44 (±1642.64) 2330.67 (±2471.21) 1514.44 (±1844.74) 1283.80 (±1189.71)
IPAQ sitting week/min (±SD) 374.58* (±202.16) 248.49 (±162.07) 393.11 (±222.66) 366.00 (±116.96)
IPAQ sitting weekend/min (±SD) 380.35 (±211.81) 297.65 (±162.59) 397.32 (±225.48) 336.00 (±156.46)
Recovery prognosis (SBST)
Total SBST (0-9) (±SD) 5.46 (±2.19) 5.16 (±2.19) 4.74 (±2.15)* 7.20 (±1.30)
Psychosocial SBST (0-5) (±SD) 2.85 (±1.48) 2.63 (±1.57) 2.37 (±1.38)* 4.00 (±1.00)
Trunk mobility in cm (±SD) 24.06 (17.03) 19.21 (14.36) 21.71 (±15.89) 33.40 (±23.23)GAi = Group adherent to intervention; GNAi = Group not adherent to intervention; GAe = Group adherent to exercise; GNAe = Group not adherent to exercise; n: number of participants; IPAQ = International Physical Activity Questionnaire; MET = Metabolic Task Equivalent; Min = minutes; SBST = Start Back Screening Tool.

134
BrJP. São Paulo, 2022 apr-jun;5(2):127-36 Santos AE, Cacau CS, Nunes AC and Jesus-Moraleida FR
FeasibilityAn adherence rate of 57.8% of participants was recorded in this program, a value below the expected threshold, even with the use of a motivational strategy to reinforce attendance. Other physi-cal therapy interventions based on active treatments for CLBP have adherence rates ranging from 60% to 80%38,41 and reinforce the challenge of adherence in programs for the management of CLBP. On the other hand, the adherence rate for exercise was found to be adequate. A systematic review pointed out that the use of motivational strategies aimed at behavior change may fa-vor the adherence to home exercises in individuals with CLBP42.A retention rate below the recommended values was recorded. Although the criterion was more flexible (80%), the general re-commendation is that clinical trials have a retention rate of 85% of participants. Since this is evaluated in clinical trial methodolo-gical quality scales, such as the Physiotherapy Evidence Database Scale (PEDro Scale)39, it’s necessary to understand which aspects of the research context or protocol interfered with this rate. The literature already points out this difficulty, however, little is kno-wn about strategies to improve this participation rate, especially in countries like Brazil, in which no monetary incentive is allo-wed for participation in researches43.Despite the problems of adherence and retention, satisfactory viability of the comprehension of the intervention components, credibility, and satisfaction were recorded. In the criterion of in-tervention comprehension, the educational content comprehen-sion was assessed as positive. A study based on neuroeducation found that most participants (75%) found that the educational component was easy44. It is worth noting that the language used in the program was adapted and clarified for the schooling level of the population.
Adherence profileIn the present study, the level of schooling of individuals with CLBP was related to adherence to the proposed intervention, whi-ch indicates that the higher the level of literacy, the higher the likelihood of adherence. A meta-analysis showed that there is a po-sitive association between adherence and schooling, in which peo-ple with higher schooling levels have higher treatment adherence, a relationship observed specially in chronic conditions45. Another aspect observed was the difference between the groups, such as the time spent sitting, in which the less active routine pre-intervention predominated in the adherent group. Unlike what was observed in this study, the literature has shown that physically active indi-viduals at baseline are more likely to adhere to interventions with physical exercise20. This finding suggests that less active individuals identified more with the proposed biopsychosocial group inter-vention, in which one of the main goals is to stimulate changes in lifestyle habits and encourage regular physical exercise.The group of participants who self-reported minimal adherence to home exercises had higher pain intensity and higher risk of poor recovery prognosis than the group that adhered. Although greater pain intensity was found in the group reporting minimal adhe-rence, it is not well established in the literature whether baseli-ne pain intensity really influences the adherence of individuals to exercise interventions, with conflicting results in the evidence20,46.
It is known that psychosocial factors such as pain catastrophizing, depressive symptoms, and false beliefs about the condition may influence poor prognosis and exercise adherence46. Not all patients who adhered to the intervention were adherent to home exercise. Based on the present results and with what is available in the li-terature, the belief is that insecurity related to lack of supervision during home exercise, as well as failure to align the exercises in the daily life routine, influenced non-adherence to home exercise42,47.
Potential Clinical ImpactThe short-term results of this study on the outcomes of pain and disability for the group involved in the multifaceted pro-gram suggest potential for relevant changes in these outcomes. Although the literature shows that programs of this nature are beneficial to those with this health condition18, there is limita-tion of the data when investigated in settings such as the present analysis. The literature points out that unfavorable socioecono-mic contexts are associated with worse outcomes in CLBP48. Thus, the preliminary results add strength to the feasibility re-sults. However, it is important to remember that the results of this study do not allow clinical differences to be detected.
Limitations and strengths of the studySome limitations of this feasibility study should be listed. The main limitation was related to sample loss. A possible contri-buting factor was the fact that, in this study, users were not al-located immediately after evaluation. As for the Control Group participants, they may have missed the follow-up because they did not receive intervention during the proposed program pe-riod. Regarding the pain and disability outcomes, these findings should be interpreted with limitations considering the sample size. Furthermore, due to insufficient data quality, some outco-mes predicted in the protocol, such as recruitment rate, percep-tion of recovery, and acceptance of technology support were not reported, leading to a deviation from the protocol.The present study was the first to investigate the feasibility of a multifaceted, mobile technology-supported intervention in a li-mited socioeconomic setting for CLBP. The protocol considered the latest primary care line recommendations for CLBP5. The pro-gram showed potential applicability in primary care as it is a strate-gy that does not require the primary health care facility to invest in hard or high cost technology. The literature points out that group format programs are favorable in community settings, since they have similar efficacy to individual programs and potentially lower health care costs49. The approaches described in this study are also in accordance with the practices recommended in the 35º Caderno de Atenção Básica (35th Basic Care Booklet), entitled Strategies for the care of chronic disease patients, however, the document does not bring specifications for chronic pain50. This study anticipates some possibilities and challenges to imple-ment strategies described in the international literature or tested only in the outpatient setting in Brazilian Primary Care. The pre-sent study also made it possible to identify the profile of those with a greater tendency to adhere and not adhere to the inter-vention, which can favor the indication of this and other possible protocol formats. In addition, a trend toward positive clinical

135
Exercise-based and pain education program for adults with chronic low back pain in Brazilian Primary Care: feasibility study
BrJP. São Paulo, 2022 apr-jun;5(2):127-36
outcomes was observed for the Intervention Group, showing the potential for implementation.
RecommendationsThe present results point to improvements to be made to the study protocol before its expanded implementation. To increa-se the protocol adherence rates, participants should be offered chances to make up for their absences, more appointment times, and more access points in the network. So that the protocol has a higher number of engaged participants, it is necessary for the group to become even closer to the flow of services offered in the primary health care network so that the protocol has a higher number of engaged participants, as well as flexibility in the way data is collected during follow-up. As some of the participants dropped out of the protocol due to availability or absences exceeding 30% of the protocol, similar groups should monitor participants not only in person, but also through the phone via telephone calls or a text message app, so that the main study outcomes are monitored. The teams involved should continue to receive monitoring throughout the protocol weeks to ensure that there are no factors associated with the na-ture of the intervention and with dropout. Future studies should focus on large-scale implementation of interventions with pro-ven efficacy in the healthcare system and on assisting people with CLBP to engage in these proposed interventions.
CONCLUSION
The feasibility of the protocol was adequate for the comprehen-sion of the components, however, adherence to the protocol and follow-up of participants were low. The profile of individuals adhering to the intervention includes higher schooling levels and more time spent sitting during their day to day. Characteristics such as higher pain intensity and the influence of psychosocial factors influenced the non-adherence to home exercises. Preli-minary results indicate benefits of the program for individuals with CLBP and suggest the expansion of the implementation as long as there are previous modifications for the improvement of actions of this nature in contexts similar to the present study.
ACKNOWLEDGMENTS
To the extensionists, the physical therapists from Project Mo-vement, the volunteers, and the coordination and professionals from the Anastácio Magalhães Primary Health Care Unit in For-taleza/Ceará.
AUTHORS’ CONTRIBUTIONS
Ana Ellen do Nascimento Santos Data Collection, Project Management, Research, Methodology, Writing - Preparation of the original, Writing - Review and Editing Catharina Saraiva Nobre Cacau Data Collection, Project Management, Research, Methodology, Writing - Preparation of the original manuscript, Writing - Re-view and Editing
Ana Carla Lima Nunes Statistical analysis, Conceptualization, Resource Management, Project Management, Methodology, Writing - Review and Edi-ting, Supervision Fabianna Resende de Jesus-Moraleida Statistical analysis, Conceptualization, Resource Management, Project Management, Methodology, Writing - Review & Edi-ting, Supervision
REFERENCES
1. Hartvigsen J, Hancock MJ, Kongsted A, Louw Q, Ferreira ML, Genevay S, et al. What low back pain is and why we need to pay attention. Lancet. 2018;391(10137):2356-67.
2. Nascimento PRC, Costa LOP. Prevalência da dor lombar no Brasil: uma revisão siste-mática. Cad Saude Publica. 2015;31(6):1141-56.
3. Marinho F, de Azeredo Passos VM, Carvalho Malta D, Barboza França E, Abreu DMX, Araújo VEM, et al. Burden of disease in Brazil, 1990–2016: a systematic subnational analysis for the Global Burden of Disease Study 2016. Lancet. 2018;392(10149):760-75.
4. Koes BW, van Tulder M, Lin CW, Macedo LG, McAuley J, Maher C. An updated overview of clinical guidelines for the management of non-specific low back pain in primary care. Eur Spine J. 2010;19(12):2075-94.
5. Foster NE, Anema JR, Cherkin D, Chou R, Cohen SP, Gross DP, et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet. 2018;391(10137):2368-83.
6. de Oliveira RF, Costa LOP, Nascimento LP, Rissato LL. Directed vertebral manipu-lation is not better than generic vertebral manipulation in patients with chronic low back pain: a randomised trial. J Physiother. 2020;66(3):174-9.
7. de Oliveira RF, Liebano RE, Costa Lda C, Rissato LL, Costa LO. Immediate effects of region-specific and non–region-specific spinal manipulative therapy in patients with chronic low back pain: a randomized controlled trial. Phys Ther. 2013;93(6):748-56.
8. Added MA, Costa LO, de Freitas DG, Fukuda TY, Monteiro RL, Salomão EC, et al. Kinesio taping does not provide additional benefits in patients with chronic low back pain who receive exercise and manual therapy: a randomized controlled trial. J Orthop Sport Phys Ther. 2016;46(7):506-13.
9. França FR, Burke TN, Caffaro RR, Ramos LA, Marques AP. Effects of muscular stret-ching and segmental stabilization on functional disability and pain in patients with chronic low back pain: a randomized, controlled trial. J Manipulative Physiol Ther. 2012;35(4):279-85.
10. Franca FR, Burke TN, Hanada ES, Marques AP. Segmental stabilization and muscular strengthening in chronic low back pain - a comparative study. Clinics. 2010;65(10):1013-7.
11. Magalhães MO, Comachio J, Ferreira PH, Pappas E, Marques AP. Effectiveness of graded activity versus physiotherapy in patients with chronic nonspecific low back pain: midterm follow up results of a randomized controlled trial. Braz J Phys Ther. 2018;22(1):82-91.
12. Garcia AN, Costa Lda C, da Silva TM, Gondo FL, Cyrillo FN, Costa RA, et al. Effec-tiveness of back school versus McKenzie exercises in patients with chronic nonspecific low back pain: a randomized controlled trial. Phys Ther. 2013;93(6):729-47.
13. Miyamoto GC, Costa LO, Galvanin T, Cabral CM. Efficacy of the addition of modi-fied Pilates exercises to a minimal intervention in patients with chronic low back pain: a randomized controlled trial. Phys Ther. 2013;93(3):310-20.
14. Magalhães MO, Muzi LH, Comachio J, Burke TN, Renovato França FJ, Vidal Ramos LA, et al. The short-term effects of graded activity versus physiotherapy in patients with chronic low back pain: a randomized controlled trial. Man Ther. 2015;20(4):603-9.
15. Ramos LAV, Callegari B, França FJR, Magalhães MO, Burke TN, Carvalho e Silva APMC, et al. Comparison between transcutaneous electrical nerve stimulation and stabilization exercises in fatigue and transversus abdominis activation in patients with lumbar disk herniation: a randomized study. J Manipulative Physiol Ther. 2018;41(4):323-31.
16. Guimarães LS, Costa LDCM, Araujo AC, Nascimento DP, Medeiros FC, Avanzi MA, et al. Photobiomodulation therapy is not better than placebo in patients with chronic nonspecific low back pain: a randomised placebo-controlled trial. Pain. 2021;162(6):1612-20.
17. Hayden JA, Ellis J, Ogilvie R, Malmivaara A, van Tulder MW. Exercise therapy for chronic low back pain. Cochrane Database Syst Rev. 2021;(9):CD009790.
18. Kamper SJ, Apeldoorn AT, Chiarotto A, Smeets RJ, Ostelo R, Guzman J, et al. Mul-tidisciplinary biopsychosocial rehabilitation for chronic low back pain. Cochrane sys-tematic review and meta-analysis. BMJ. 2015;350:h444.
19. World Health Organization (WHO). Adherence to Long-Term Therapies: Evidence for Action [Internet]. Geneva:WHO; 2003.[Acessado em 29 set 2021]. Disponível em: https://apps.who.int/iris/bitstream/handle/10665/42682/9241545992.pdf
20. Jack K, McLean SM, Moffett JK, Gardiner E. Barriers to treatment adherence in physiotherapy outpatient clinics: a systematic review. Man Ther. 2010;15(3):220-8.
21. Eldridge SM, Chan CL, Campbell MJ, Bond CM, Hopewell S, Thabane L, Lancaster
136
BrJP. São Paulo, 2022 apr-jun;5(2):127-36 Santos AE, Cacau CS, Nunes AC and Jesus-Moraleida FR
GA; PAFS consensus group. CONSORT 2010 statement: extension to randomised pilot and feasibility trials. BMJ. 2016;355:i5239.
22. Hoffmann T, Glasziou P, Boutron I, Milne R, Perera R, Moher D, et al. Better repor-ting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. 2014;348:g1687.
23. Nijs J, Paul van Wilgen C, Van Oosterwijck J, van Ittersum M, Meeus M. How to explain central sensitization to patients with “unexplained” chronic musculoskeletal pain: practice guidelines. Man Ther. 2011;16(5):413-8.
24. Gatchel RJ, Rollings KH. Evidence-informed management of chronic low back pain with cognitive behavioral therapy. Spine J. 2008;8(1):40-4.
25. Du S, Hu L, Dong J, Xu G, Chen X, Jin S, et al. Self-management program for chronic low back pain: a systematic review and meta-analysis. Patient Educ Couns. 2017;100(1):37-49.
26. Macedo LG, Smeets RJ, Maher CG, Latimer J, McAuley JH. Graded activity and graded exposure for persistent nonspecific low back pain: a systematic review. Phys Ther. 2010;90(6):860-79.
27. Hayden JA, Wilson MN, Stewart S, Cartwright JL, Smith AO, Riley RD, et al. Exerci-se treatment effect modifiers in persistent low back pain: an individual participant data meta-analysis of 3514 participants from 27 randomised controlled trials. Br J Sports Med. 2019;54(21):1277-8.
28. Fritsch CG, Ferreira PH, Prior JL, McLachlan AJ, Ferreira ML. Effects of using text message interventions for the management of musculoskeletal pain: a systematic re-view. Pain. 2020;161(11):2462-75.
29. Borg G. Escalas de Borg para dor e esforço percebido. 1ª ed. Manole, São Paulo; 2000. 30. Sharma S, Jensen MP, Moseley GL, Abbott JH. Pain education for patients with non-
-specific low back pain in Nepal: protocol of a feasibility randomised clinical trial (PEN-LBP Trial). BMJ Open. 2018;8(8):e022423.
31. Childs JD, Piva SR, Fritz JM. Responsiveness of the numeric pain rating scale in patients with low back pain. Spine (Phila Pa 1976). 2005;30(11):1331-4.
32. Nusbaum L, Natour J, Ferraz MB, Goldenberg J. Translation, adaptation and valida-tion of the Roland-Morris questionnaire - Brazil Roland-Morris. Braz J Med Biol Res. 2001;34(2):203-10.
33. Salvetti MG, Pimenta CAM. Validação da Chronic Pain Self-Efficacy Scale para a língua portuguesa. Arch Clin Psychiatry (São Paulo). 2005;32(4):202-10.
34. Siqueira FB, Teixeira-Salmela LF, Magalhães LC. Análise das propriedades psicométricas da versão brasileira da escala tampa de cinesiofobia. Acta Ortop Bras. 2007;15(1):19-24.
35. Matsudo S, Araújo T, Marsudo V, Andrade D, Andrade E, Braggion G. Questionário internacional de atividade física (IPAQ): estudo de validade e reprodutibilidade no Brasil. Rev Bras Ativ Fís Saúde. 2001;5-18.
36. Perret C, Poiraudeau S, Fermanian J, Lefèvre Colau MM, Mayoux Benhamou MA, Revel M. Validity, reliability, and responsiveness of the fingertip-to-floor test. Arch Phys Med Rehabil. 2001;82(11):1566-70.
37. Pilz B, Vasconcelos RA, Marcondes FB, Lodovichi SS, Mello W, Grossi DB. The Bra-zilian version of STarT Back Screening Tool - translation, cross-cultural adaptation and reliability. Braz J Phys Ther. 2014;18(5):453-61.
38. Dhondt E, Van Oosterwijck J, Cagnie B, Adnan R, Schouppe S, Van Akeleyen J, et al. Predicting treatment adherence and outcome to outpatient multimodal rehabilitation in chronic low back pain. J Back Musculoskelet Rehabil. 2020;33(2):277-93.
39. Macedo LG, Elkins MR, Maher CG, Moseley AM, Herbert RD, Sherrington C. There was evidence of convergent and construct validity of Physiotherapy Evidence Database quality scale for physiotherapy trials. J Clin Epidemiol. 2010;63(8):920-5.
40. Kamper SJ, Maher CG, Mackay G. Global rating of change scales: A review of strengths and weaknesses and considerations for design. J Man Manip Ther. 2009;17(3):163-70.
41. Stevens ML, Lin CC, Hancock MJ, Wisby-Roth T, Latimer J, Maher CG. A physio-therapist-led exercise and education program for preventing recurrence of low back pain: a randomised controlled pilot trial. Physiotherapy. 2018;104(2):217-23.
42. Beinart NA, Goodchild CE, Weinman JA, Ayis S, Godfrey EL. Individual and inter-vention-related factors associated with adherence to home exercise in chronic low back pain: a systematic review. Spine J. 2013;13(12):1940-50.
43. Gillies K, Kearney A, Keenan C, Treweek S, Hudson J, Brueton VC, et al. Stra-tegies to improve retention in randomised trials. Cochrane Database Syst Rev. 2021;6(3):MR000032.
44. Sharma S, Jensen MP, Moseley GL, Abbott JH. Results of a feasibility randomised clinical trial on pain education for low back pain in Nepal: the Pain Education in Nepal-Low Back Pain (PEN-LBP) feasibility trial. BMJ Open. 2019;9(3):e026874.
45. DiMatteo MR. Variations in patients’ adherence to medical recommendations: a quantitative review of 50 years of research. Med Care; 2004;42(3):200-9.
46. Boutevillain L, Dupeyron A, Rouch C, Richard E, Coudeyre E. Facilitators and bar-riers to physical activity in people with chronic low back pain: A qualitative study. PLoS One. 2017;12(7):e0179826.
47. Palazzo C, Klinger E, Dorner V, Kadri A, Thierry O, Boumenir Y, et al. Barriers to home-based exercise program adherence with chronic low back pain: Patient expecta-tions regarding new technologies. Ann Phys Rehabil Med. 2016;59(2):107-13.
48. Carr JL, Klaber Moffett JA, Howarth E, Richmond SJ, Torgerson DJ, Jackson DA, et al. A randomized trial comparing a group exercise programme for back pain pa-tients with individual physiotherapy in a severely deprived area. Disabil Rehabil. 2005;27(16):929-37.
49. O’Keeffe M, Hayes A, McCreesh K, Purtill H, O’Sullivan K. Are group-based and in-dividual physiotherapy exercise programmes equally effective for musculoskeletal condi-tions? A systematic review and meta-analysis. Br J Sport Med. 2017;51(2):126-32.
50. Brasil. Ministérios da Saúde (MS). Estratégias para o cuidado da pessoa com doença crônica (Cadernos de Atenção Básica, n. 35) [Internet]; Brasília: MS; 2014. [Acessado 22 Abr 2021]. Disponível emhttps://bvsms.saude.gov.br/bvs/publicacoes/estrategias_cuidado_pessoa_doenca_cronica_cab35.pdf.

137
ABSTRACT
BACKGROUND AND OBJECTIVES: Back pain is one of the main causes of disability worldwide, resulting in higher rates of work absenteeism and years lived with disability. This study ai-med to evaluate back pain prevalence and its associated factors in Primary Health Units (PHU) users.METHODS: A community-based cross-sectional study was conducted at PHU located in Pelotas, Brazil. Fifteen individuals of each PHU, aged 18 years or more, were interviewed (n=540). Back pain was defined as pain in one to three back areas (neck, dorsal and lumbar). Demographic, economic, behavioral, nutri-tional status (body mass index) and health characteristics were assessed as covariates. Poisson regression was used to estimate the prevalence ratio and 95% confidence intervals. RESULTS: Prevalence of back pain in PHU users was 20% (95%CI 16.8 - 23.6). Fair (PR 2.66 95%CI 1.00 - 7.09) and poor (PR 3.65 95%CI 1.31 - 10.16) self-perceived health, mus-culoskeletal disease (RP 2.71 95%CI 1.84 - 3.98) and current smoking (PR 1.71 95%CI 1.18 - 2.47) were associated with back pain. CONCLUSION: Back pain is a common problem in PHU users in Brazil. Patients with musculoskeletal disease, who are current smokers and have a poor self-perceived health, are more likely to experience back pain.Keywords: Back pain, Chronic pain, Unified Health System.
Back pain prevalence and associated factors in Brazilian Unified Health System usersPrevalência de dor nas costas e fatores associados em usuários do Sistema Único de Saúde
Eduardo L Caputo1, Daniele Fernandes da Silva de Souza1, Vitor Häfele1, Fernando Carlos Vinholes Siqueira1
Eduardo L Caputo – https://orcid.org/0000-0002-3515-9308;Daniele Fernandes da Silva de Souza – https://orcid.org/0000-0001-5752-048;Vitor Häfele – https://orcid.org/0000-0001-6812-2002;Fernando Carlos Vinholes Siqueira – https://orcid.org/0000-0002-2899-3062.
1. Federal University of Pelotas, Postgraduate Program of Physical Education, Pelotas, RS, Brazil.
Submitted on February 02, 2021. Accepted for publication on April 12, 2022.Conflict of interests: none – Sponsoring sources: none.
Correspondence to:Eduardo L Caputo E-mail: [email protected]
© Sociedade Brasileira para o Estudo da Dor
RESUMO
JUSTIFICATIVA E OBJETIVOS: A dor nas costas é uma das principais causas de incapacidade em todo o mundo, resultando em maiores taxas de absenteísmo no trabalho e anos vividos com incapacidade. Este estudo teve como objetivo avaliar a prevalên-cia de dor nas costas e seus fatores associados em usuários de Unidades Básicas de Saúde (UBS). MÉTODOS: Foi realizado um estudo transversal de base comu-nitária em UBS localizadas em Pelotas, Brasil. Foram entrevista-dos 15 indivíduos de cada UBS, com idade igual ou superior a 18 anos (n=540). A dor nas costas foi definida como dor em uma a três áreas das costas (pescoço, dorsal e lombar). Características demográficas, econômicas, comportamentais, nutricionais (índi-ce de massa corporal) e de saúde foram avaliadas como covariá-veis. A regressão de Poisson foi utilizada para estimar a razão de prevalência e os intervalos de confiança de 95%. RESULTADOS: A prevalência de dor nas costas em usuários de UBS foi de 20% (IC95% 16,8 - 23,6). Autopercepção de saúde regular (RP 2,66 IC95% 1,00 - 7,09) e ruim (RP 3,65 IC95% 1,31 - 10,16), doença musculoesquelética (RP 2,71 IC95% 1,84 - 3,98) e tabagismo atual (RP 1,71 IC95% 1,18 - 2,47) foram associados à dor nas costas. CONCLUSÃO: A dor nas costas é um problema comum em usuários de UBS. Pacientes com doença musculoesquelética, fumantes atuais e com autopercepção de saúde ruim são mais propensos a sentir dor nas costas.Descritores: Dor crônica, Dor nas costas, Sistema Único de Saúde.
INTRODUCTION
Back pain is one of the main causes of disability worldwide, resulting in higher rates of work absenteeism and years lived with disability1. In Southern Latin America, low back pain (LBP) and neck pain have a prevalence of 8.0% and 5.6%, respectively2. Furthermore, chronic back pain prevalence, de-fined as pain in cervical, thoracic or lumbar area, is 17.7%3.LBP etiology includes myofascial pain, facet joint pain, disco-genic pain, spinal stenosis, and might be worsened by psycho-logical and disease related factors4. Approximately 80% of pa-tients who experience LBP seek a healthcare professional to manage their pain. The general practitioner is the healthcare professional most sought by LBP patients5,6.The Brazilian Unified Health System (SUS – Sistema Único de Saúde) was founded based on a new political and orga-nizational formulation, aiming to reorganize health actions
BrJP. São Paulo, 2022 apr-jun;5(2):137-42
DOI 10.5935/2595-0118.20220022
ORIGINAL ARTICLE

138
BrJP. São Paulo, 2022 apr-jun;5(2):137-42 Caputo EL, Souza DF, Häfele V and Siqueira FC
and services established in Brazil’s 1988 Constitution7. This system emerges as a decentralized strategy for attention and healthcare, using primary care as users main gateway8,9. Addi-tionally, communication with SUS’ entire healthcare network takes place through Primary Health Units (PHU)10.PHU are strategically located close to people’s home, school, and work. They are composed of multidisciplinary teams which play an important role to provide quality primary care to Brazilian public health system users10. Simple and cheap procedures are performed at PHU, where staff members are capable of solving most of the community’s common health problems. However, their organization, applicability and development demand complex studies and deep knowledge regarding po-pulation reality11. Users who seek care in PHU are, in general, individuals from a less privileged social level and can also be in vulnerability, who need equity in healthcare12. As PHU are the community closest option of health care, this study aimed to 1) evaluate the prevalence of back pain (cervical, thoracic and lumbar) in PHU users and 2) to evaluate what factors were associated with back pain prevalence in this population.
METHODS
A community-based cross-sectional study was conducted at PHU located in the city of Pelotas, RS, Brazil. The structure of the manuscript agreed with STROBE requirements13. Ac-cording to 2010 Demographic Census (IBGE), Pelotas is a city with approximately 327,778 inhabitants. Overall, there are 38 PHU located in the city urban area. Two PHU for specific populations (prisoners and children) were excluded. Following the worldwide prevalence of chronic pain (i.e., 35.5%)14, a sample size of 540 participants was calculated, with 80% power and 95% confidence level. In each PHU (i.e., 36 in urban Pelotas), 15 individuals, aged 18 or more, were interviewed (n=540). Participants were asked to take part in the study regardless of the reason they sought care in the PHU.After the Municipal Health Department authorized the study, the PHU were contacted. Interviews were scheduled with the PHU head chief aiming not to disturb the unit’s normal ope-ration. Data collection took place between March and June 2018, and interviews were conducted individually.The first subject located on the right side of the room, starting from the entrance door was the first person asked to partici-pate in the study. Then, the next subject located on the left side of the first participant was the next and so on, until the predetermined number of 15 participants was reached15,16. Individuals who were accompanying patients, who were not PHU users, as well as people unable to express themselves due to a health disability, did not participate in the study.Back pain was defined as pain in one to three back areas (neck, dorsal and lumbar). Participants were asked about pain experience by the question: “Did you feel any pain this week”? If participants answered positively, a human body image in supine position was showed, and participants were then asked
to point the pain location on the image. Participants who pointed one or more back areas on the image were considered as experiencing back pain.
Covariates Demographic (age and gender), economic (wage), behavio-ral (smoking, alcohol intake, physical activity level and TV watching), nutritional status (body mass index) and health (self-perceived health, depression, musculoskeletal disea-se and drug treatments) characteristics were assessed. Age was divided into three categories: 18-39, 40-59, 60 or more years. Economic level was determined by the number of sel-f-reported wages and classified in less than one wage, one to two wages and more than three (one minimal wage was R$ 954,00). Medical diagnostic of depression and musculoskele-tal disorders were assessed by the questions of a Brazilian na-tional survey17. Self-perceived health was classified in excel-lent/very good, good, fair and poor. Participants were asked about alcohol intake and had three response options: “no”; “yes, sometimes”; and “yes, every day’’. For analysis purposes, participants who reported alcohol intake sometimes or every day were classified by “yes”. The number of continuously used drugs was classified in none, one or two and three or more.Body mass index was calculated from self-reported height and weight, following the World Health Organization recom-mendation (normal <25 kg/m2, overweight 25-29.9 kg/m2 and obese ≥30 kg/m2). Smoking was categorized into never smoked, former-smoker and current smoker (one or more ci-garettes per day for more than one month). Leisure-time phy-sical activity was assessed through the International Physical Activity Questionnaire long version (IPAQ). A cut-off point of 150 minutes per week was used to classify subjects as active (150 min/week or more) or insufficiently active (below 150 min/week)18. Television time was calculated considering three or more hours per day. The study was approved by the Research Ethics Committee from the Physical Education Faculty, Federal University of Pelotas (protocol number: 2.496.718).
Statistical analysisEpiData 3.1 was used to structure the dataset. Descriptive analyzes of the sample, according to back pain report, are pre-sented as relative and absolute frequencies. Prevalence ratio and 95% confidence interval between back pain and independent variables were estimated with crude and adjusted analyzes, using Poisson regression. A p<0.2 was considered aiming to control for potential confounders. Analyzes were conducted using Stata statistical software (StataCorp. 2012, Stata Statis-tical Software: Release 12, Version 12.1, StataCorp LP, College Station, TX, USA) with the significance level set at 0.05.
RESULTS
Overall, data of 540 users in 36 PHU from Pelotas were analyzed. Back pain prevalence was 20.0% (95%CI 16.8; 23.6). Higher frequencies of back pain were observed in

139
Back pain prevalence and associated factors in Brazilian Unified Health System users
BrJP. São Paulo, 2022 apr-jun;5(2):137-42
those participants who were female, aged 40-59, smokers, with fair and poor self-perceived health, reported muscu-loskeletal disorders, depression, and continued use of drugs (Table 1).The crude analyzes between back pain and covariates is displa-yed in Table 1. Mid-age adults were 71% (95%CI 1.11; 2.65) more likely to report back pain. Regarding health characteris-tics, those who perceived their health as fair or poor (PR 3.88 95%CI 1.46; 10.32; PR 6.75 95%CI 2.51; 18.19, respecti-vely), who reported depression (PR 1.85 95%CI 1.31; 2.56)
and musculoskeletal disease (PR 3.41 95%CI 2.43; 4.78) were more likely to experience back pain. Smoking (PR 1.73 95%CI 1.15; 2.60) and using one or more drugs (PR 1.83 95%CI 1.16; 2.89; PR 1.98 95%CI 1.27 - 3.10, for 1-2 and ≥ 3, respectively) were also associated with back pain.Table 2 shows the adjusted analyzes between back pain and covariates. No association was observed with gender, age, in-come, depression, alcohol intake, BMI, TV watching and lei-sure-time physical activity. Fair (PR 2.66 95%CI 1.00 - 7.09) and poor (PR 3.65 95%CI 1.31 - 10.16) self-perceived health
Table 1. Descriptive characteristics, and crude analysis of back pain of Brazil Primary Health Unit users, 2018 (n=540)
Variables Total samplen
Back pain%
PR CI 95% p-value
Gender 0.131 Male 147 15.7 1.0 – Female 393 21.6 1.38 (0.91 – 2.10)Age (years) 0.051 18-39 179 14.0 1.0 – 40-59 213 23.9 1.71 (1.11 – 2.65) 60-90 147 21.8 1.56 (0.97 – 2.51)Income 0.401 < 1 wage 205 21.0 1.0 – 1-2 wages 274 20.4 0.97 (0.68 – 1.39) > 3 wages 60 15.0 0.72 (0.37 – 1.38)Health self-perception <0.001 Excellent/very good 63 6.4 1.0 – Good 199 12.1 1.90 (0.68 – 5.27) Fair 215 24.7 3.88 (1.46 – 10.32) Poor 63 42.9 6.75 (2.51 – 18.19)Depression <0.001 No 388 16.2 1.0 – Yes 151 29.8 1.84 (1.31 – 2.56)Musculoskeletal disease <0.001 No 374 11.5 1.0 – Yes 166 39.2 3.41 (2.43 – 4.78)Smoking 0.007 Never smoker 276 15.9 1.0 – Former smoker 155 21.9 1.38 (0.92 – 2.06) Smoker 109 27.5 1.73 (1.15 – 2.60)Alcohol intake 0.785 No 359 20.3 1.0 – Yes 181 19.3 0.95 (0.66 – 1.37)Leisure-time physical activity 0.172 0-149 minutes 432 21.2 1.0 – ≥ 150 minutes 106 15.1 0.71 (0.44 – 1.16)TV watching 0.306 < 3 hours 339 18.9 1.0 – ≥ 3 hours 195 22.6 1.20 (0.85 – 1.68)Body mass index 0.577 Normal 174 20.1 1.0 – Overweight 186 22.6 1.12 (0.75 – 1.67) Obesity 154 17.5 0.87 (0.55 – 1.37)Use of drugs 0.002 None 197 12.7 1.0 – 1-2 172 23.3 1.83 (1.16 – 2.89) ≥ 3 171 25.2 1.98 (1.27 – 3.10)
PR = Prevalence ratio; CI = Confidence interval of 95%.
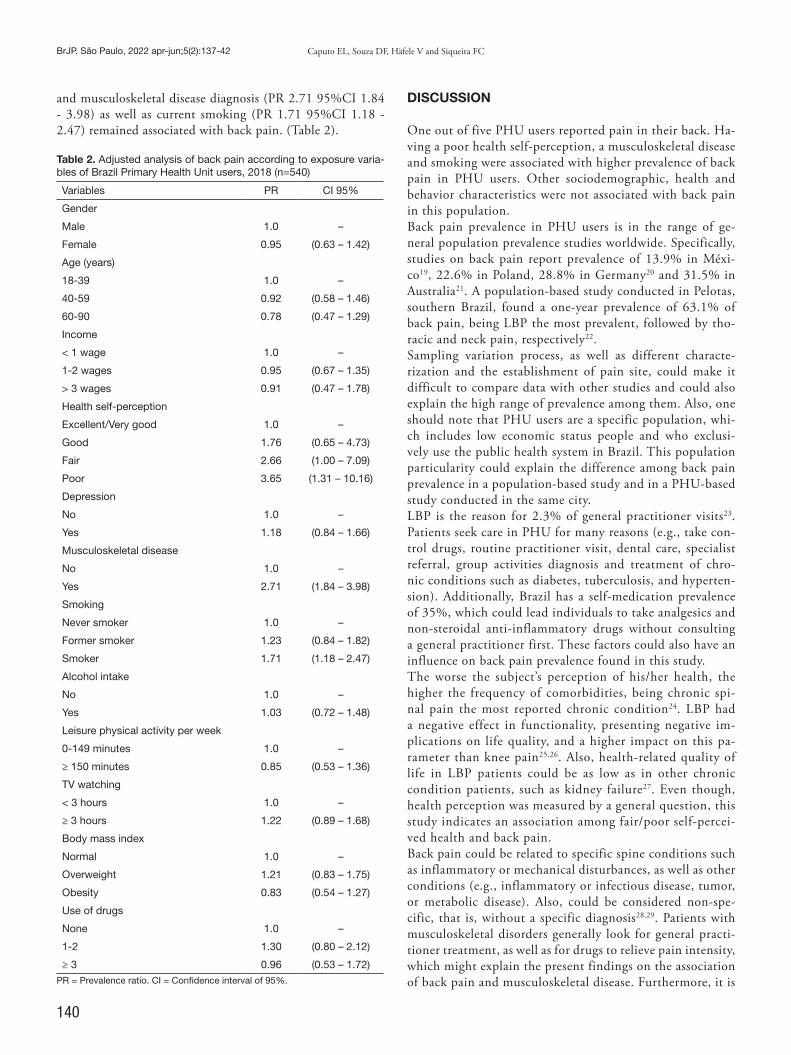
140
BrJP. São Paulo, 2022 apr-jun;5(2):137-42 Caputo EL, Souza DF, Häfele V and Siqueira FC
and musculoskeletal disease diagnosis (PR 2.71 95%CI 1.84 - 3.98) as well as current smoking (PR 1.71 95%CI 1.18 - 2.47) remained associated with back pain. (Table 2).
Table 2. Adjusted analysis of back pain according to exposure varia-bles of Brazil Primary Health Unit users, 2018 (n=540)
Variables PR CI 95%
Gender
Male 1.0 –
Female 0.95 (0.63 – 1.42)
Age (years)
18-39 1.0 –
40-59 0.92 (0.58 – 1.46)
60-90 0.78 (0.47 – 1.29)
Income
< 1 wage 1.0 –
1-2 wages 0.95 (0.67 – 1.35)
> 3 wages 0.91 (0.47 – 1.78)
Health self-perception
Excellent/Very good 1.0 –
Good 1.76 (0.65 – 4.73)
Fair 2.66 (1.00 – 7.09)
Poor 3.65 (1.31 – 10.16)
Depression
No 1.0 –
Yes 1.18 (0.84 – 1.66)
Musculoskeletal disease
No 1.0 –
Yes 2.71 (1.84 – 3.98)
Smoking
Never smoker 1.0 –
Former smoker 1.23 (0.84 – 1.82)
Smoker 1.71 (1.18 – 2.47)
Alcohol intake
No 1.0 –
Yes 1.03 (0.72 – 1.48)
Leisure physical activity per week
0-149 minutes 1.0 –
≥ 150 minutes 0.85 (0.53 – 1.36)
TV watching
< 3 hours 1.0 –
≥ 3 hours 1.22 (0.89 – 1.68)
Body mass index
Normal 1.0 –
Overweight 1.21 (0.83 – 1.75)
Obesity 0.83 (0.54 – 1.27)
Use of drugs
None 1.0 –
1-2 1.30 (0.80 – 2.12)
≥ 3 0.96 (0.53 – 1.72)PR = Prevalence ratio. CI = Confidence interval of 95%.
DISCUSSION
One out of five PHU users reported pain in their back. Ha-ving a poor health self-perception, a musculoskeletal disease and smoking were associated with higher prevalence of back pain in PHU users. Other sociodemographic, health and behavior characteristics were not associated with back pain in this population. Back pain prevalence in PHU users is in the range of ge-neral population prevalence studies worldwide. Specifically, studies on back pain report prevalence of 13.9% in Méxi-co19, 22.6% in Poland, 28.8% in Germany20 and 31.5% in Australia21. A population-based study conducted in Pelotas, southern Brazil, found a one-year prevalence of 63.1% of back pain, being LBP the most prevalent, followed by tho-racic and neck pain, respectively22. Sampling variation process, as well as different characte-rization and the establishment of pain site, could make it difficult to compare data with other studies and could also explain the high range of prevalence among them. Also, one should note that PHU users are a specific population, whi-ch includes low economic status people and who exclusi-vely use the public health system in Brazil. This population particularity could explain the difference among back pain prevalence in a population-based study and in a PHU-based study conducted in the same city.LBP is the reason for 2.3% of general practitioner visits23. Patients seek care in PHU for many reasons (e.g., take con-trol drugs, routine practitioner visit, dental care, specialist referral, group activities diagnosis and treatment of chro-nic conditions such as diabetes, tuberculosis, and hyperten-sion). Additionally, Brazil has a self-medication prevalence of 35%, which could lead individuals to take analgesics and non-steroidal anti-inflammatory drugs without consulting a general practitioner first. These factors could also have an influence on back pain prevalence found in this study. The worse the subject’s perception of his/her health, the higher the frequency of comorbidities, being chronic spi-nal pain the most reported chronic condition24. LBP had a negative effect in functionality, presenting negative im-plications on life quality, and a higher impact on this pa-rameter than knee pain25,26. Also, health-related quality of life in LBP patients could be as low as in other chronic condition patients, such as kidney failure27. Even though, health perception was measured by a general question, this study indicates an association among fair/poor self-percei-ved health and back pain.Back pain could be related to specific spine conditions such as inflammatory or mechanical disturbances, as well as other conditions (e.g., inflammatory or infectious disease, tumor, or metabolic disease). Also, could be considered non-spe-cific, that is, without a specific diagnosis28,29. Patients with musculoskeletal disorders generally look for general practi-tioner treatment, as well as for drugs to relieve pain intensity, which might explain the present findings on the association of back pain and musculoskeletal disease. Furthermore, it is

141
Back pain prevalence and associated factors in Brazilian Unified Health System users
BrJP. São Paulo, 2022 apr-jun;5(2):137-42
important to highlight that PHU are the easiest and nearest health facility to seek care. Association between smoking and back pain has been well established in literature. Data from a meta-analysis study indicate higher odds of back pain in former smokers (OR 1.27) and ever smokers (OR 1.26), in comparison with ne-ver smokers30. Additionally, a study with US adults observed that back pain prevalence in current smokers is higher when compared to former and never smokers. Also, back pain pre-valence of former smokers is higher than never smokers31. However, only ever smoker category was associated with back pain in the present study.Even tough there is evidence on the protective effect of lei-sure-time physical activity on back pain32, the present study did not show an association between these variables. Ho-wever, people who experience pain might be less likely to engage in physical activity to avoid worsening their pain16. This might explain the lack of association found in this stu-dy. However, future studies in PHU users should focus on physical activity and back pain. Limitations of this study should be listed. First, different types of PHU (standard, Family Health, or mixed) offer different health care treatments. Actions and resources are more adequate in Family Health Program, because they are directed to programmatic actions, home activities and grea-ter involvement with the community. On the other hand, in standard PHU, treatment depends on the patient’s initia-tive to seek care, which could interfere in their pain condi-tion33. Second, pain was assessed only in the last week, whi-ch doesn’t allow to make inferences about pain chronicity. However, to the authors knowledge this is the first study to evaluate back pain prevalence in PHU user’s population. In addition, the study assessed a representative sample of PHU users, providing information on a well-represented sample of such population.
CONCLUSION
In summary, the conclusion is that back pain is a common problem among PHU users, and is associated with muscu-loskeletal disease, smoking behavior and a poor health per-ception. Further studies are necessary to elucidate pain out-comes in this population, such as pain intensity, duration and disability.
CONTRIBUTIONS OF THE AUTHORS
Eduardo L Caputo Conceptualization, Project Management, Writing - Preparation of the original Daniele Fernandes da Silva de Souza Data Collection, Methodology, Writing - Review and Editing Vitor Häfele Statistical analysis, Writing - Review and Editing Fernando Carlos Vinholes Siqueira Project Management, Writing - Review and Editing
REFERENCES
1. Hartvigsen J, Hancock MJ, Kongsted A, Louw Q, Ferreira ML, Gene-vay S, et al. What low back pain is and why we need to pay attention. Lancet. 2018;391(10137):2356-67.
2. March L, Smith EU, Hoy DG, Cross MJ, Sanchez-Riera L, Blyth F, et al. Burden of disability due to musculoskeletal (MSK) disorders. Best Pract Res: Clin Rheumatol. 2014;28(3):353-66.
3. Gerhardt A, Hartmann M, Blumenstiel K, Tesarz J, Eich W. The prevalence rate and the role of the spatial extent of pain in nonspecific chronic back pain--a population--based study in the south-west of Germany. Pain Med. 2014;15(7):1200-10.
4. Urits I, Burshtein A, Sharma M, Testa L, Gold PA, Orhurhu V, et al. Low back pain, a comprehensive review: pathophysiology, diagnosis, and treatment. Curr Pain Hea-dache Rep. 2019;23(3)23.
5. Freburger JK, Holmes GM, Agans RP, Jackman AM, Darter JD, Wallace AS, et al. The rising prevalence of chronic low back pain. Arch Int Med. 2009;169(3):251-8.
6. Ferreira ML, Machado G, Latimer J, Maher C, Ferreira PH, Smeets RJ. Factors defi-ning care-seeking in low back pain--a meta-analysis of population based surveys. Eur J Pain. 2010;14(7):747.e1-7.
7. Brazil. ABC do SUS: Doutrina e Princípios. 1990. 8. Brazil. Política Nacional de Gestão Estratégica e Participativa no SUS - Participa SUS.
2009. 9. Paim J, Travassos C, Almeida C, Bahia L, MacInko J. The Brazilian health system:
history, advances, and challenges. Lancet. 2011;377(9779):1778-97. 10. Brazil. Política Nacional de Atenção Básica. 2012. 11. Plano Municipal de Saúde de Pelotas. 2013. 12. Brazil. Política de Promoção de Equidade em Saúde. 2013. 13. Vandenbroucke JP, von Elm E, Altman DG, Gøtzsche PC, Mulrow CD, Pocock SJ,
et al. Strengthening the Reporting of Observational Studies in Epidemiology (STRO-BE): explanation and elaboration. PLoS Med; 2022;4(10):1628-54.
14. IASP. How prevalent is chronic pain? . Clinical Updates. 2003;11(2). 15. Häfele V, Siqueira FV. Aconselhamento para atividade física e mudança de com-
portamento em Unidades Básicas de Saúde. Rev Bras Ativ Física & Saúde. 2022;21(6):581-92.
16. Souza DF da S, Häfele V, Siqueira FV. Dor crônica e nível de atividade físi-ca em usuários das unidades básicas de saúde. Rev Bras Ativ Física & Saúde. 2019;11(24);1-10.
17. Brasil M da S. VIGITEL Brasil 2019: vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico: estimativas sobre frequência e distribuição sociodemográfica de fatores de risco e proteção para doenças crônicas nas capitais dos 26 estados br. SVS/MS Brasília; 2019.
18. Craig CL, Marshall AL, Sjöström M, Bauman AE, Booth ML, Ainsworth BE, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports and Exerc. 2003;35(8):1381-95.
19. Peláez-Ballestas I, Flores-Camacho R, Rodriguez-Amado J, Sanin LH, Valerio JE, Na-varro-Zarza E, et al. Prevalence of back pain in the community. A COPCORD-based study in the Mexican population. J Rheumatol Suppl. 2011;;86:26-30.
20. Henn L, Schier K, Brian T, Hardt J. Back pain in Poland and Germany: a survey of prevalence and association with demographic characters. BioMed Research Internatio-nal. Hindawi Publishing Corporation; 2014.
21. Dennis D, Tampin B, Jacques A, Hebden-Todd T, Carter V, McLintock M, et al. The prevalence of back pain in patients in one Australian tertiary hospital population. Musculoskeletal Care. 2018;16(1):112-7.
22. Ferreira GD, Silva MC, Rombaldi AJ, Wrege ED, Siqueira FV, Hallal PC. Prevalence and associated factors of back pain in adults from southern Brazil: a population-based study. Rev Bras Fisioter. 2011;15(1):31-6.
23. Deyo RA, Mirza SK, Martin BI. Back pain prevalence and visit rates: estimates from U.S. national surveys, 2002. Spine (Phila Pa 1976). 2006;31(23):2724-7.
24. Araujo MEA, Silva MT, Galvao TF, Nunes BP, Pereira MG. Prevalence and patterns of multimorbidity in Amazon Region of Brazil and associated determinants: a cross--sectional study. BMJ Open. 2018;1;8(11):e023398.
25. Muraki S, Akune T, Oka H, En-Yo Y, Yoshida M, Saika A, et al. Health-related quality of life in subjects with low back pain and knee pain in a population-based cohort study of Japanese men: the Research on Osteoarthritis Against Disability study. Spine. 2011;36(16):1312-9.
26. Horng YS, Hwang YH, Wu HC, Liang HW, Mhe YJ, Twu FC, et al. Predicting heal-th-related quality of life in patients with low back pain. Spine. 2005;30(5):551-5.
27. Yamada K, Matsudaira K, Takeshita K, Oka H, Hara N, Takagi Y. Prevalence of low back pain as the primary pain site and factors associated with low health-related qua-lity of life in a large Japanese population: a pain-associated cross-sectional epidemiolo-gical survey. Mod Rheumatol. 2014;24(2):343-8.
28. Broonen JP, Marty M, Legout V, Cedraschi C, Henrotin Y. Is volition the missing link in the management of low back pain? Vol. 78, Joint Bone Spine. 2011;78(4):364-7.
29. Endean A, Palmer KT, Coggon D. Potential of magnetic resonance imaging findings to refine case definition for mechanical low back pain in epidemiological studies: a systematic review. Spine (Phila Pa 1976). 2011;36(2):160-9.
30. Shiri R, Karppinen J, Leino-Arjas P, Solovieva S, Viikari-Juntura E. The association between smoking and low back pain: a meta-analysis. Am J Med. 2010;123(1):87.e7-87.e35.

142
BrJP. São Paulo, 2022 apr-jun;5(2):137-42 Caputo EL, Souza DF, Häfele V and Siqueira FC
31. Green BN, Johnson CD, Snodgrass J, Smith M, Dunn AS. Association bet-ween smoking and back pain in a cross-section of adult Americans. Cureus. 2016;8(9):e806.
32. Alzahrani H, Mackey M, Stamatakis E, Zadro JR, Shirley D. The association between physical activity and low back pain: a systematic review and meta-analysis of observa-
tional studies. Sci Rep. 2019;9(1):8244.33. Facchini LA, Piccini RX, Thumé E, Silveira DS, Siqueira FV, Rodrigues MA, et
al. Performance of the PSF in the Brazilian South and Northeast: Institutional and epidemiological Assessment of Primary Health Care. Ciencia e Saude Coletiva. 2006;11(3):669-81.

143
ABSTRACT
BACKGROUND AND OBJECTIVES: Mammography is an examination of images of the breasts, obtained through radio-graphy with compression of the breast tissue. Pain is a factor constantly reported by patients undergoing the procedure and, for this reason, there is a need to establish alternative non-phar-macological strategies that reduce the sensation of pain. The aim of this study was to carry out an integrative review on non-phar-macological methods used for pain relief during mammography examination. CONTENTS: The search was carried out in April 2021 in four databases (Pubmed, Medline, Scopus and CINAHL) using the descriptors “pain”, “pain management”, “mammography”, “mu-sic therapy” and “complementary therapies “. After reading and final analysis, four articles met the pre-established criteria, ad-dressing the non-pharmacological management of pain during mammography. The studies showed different methods to reduce pain, such as the use of pads and changes in the compression protocol, as well as the intervention with music. CONCLUSION: Evidence on the non-pharmacological mana-gement of mammography-related pain is still scarce. Among the strategies found, the customized compression protocol and the use of compressible pads showed analgesic efficacy, while the use of music did not result in a significant reduction in procedural pain. However, as this is an integrative review, there is a need to carry out evidence syntheses with greater methodological rigor to estimate the size of the analgesic effect of these interventions. Keywords: Complementary therapies Mammography, Pain, Pain management.
Non-pharmacological methods for pain relief during mammography: integrative reviewMétodos não farmacológicos para o alívio da dor durante mamografia: revisão integrativa
Katherine Olga Correia Alves Santos1, Clarissa Lima Franco2, Caique Jordan Nunes Ribeiro2,3, Mariangela da Silva Nunes1, Maria do Carmo de Oliveira1,2
Katherine Olga Correia Alves Santos – https://orcid.org/0000-0002-3819-0917;Clarissa Lima Franco – https://orcid.org/0000-0002-4462-3408;Caique Jordan Nunes Ribeiro – https://orcid.org/0000-0001-9767-3938;Mariangela da Silva Nunes – https://orcid.org/0000-0003-0693-5790;Maria do Carmo de Oliveira – https://orcid.org/0000-0003-4719-3893. 1. Federal University of Sergipe, Nursing Department, Aracaju, SE, Brazil.2. Federal University of Sergipe, Postgraduate Program in Nursing, São Cristóvão, SE, Brazil.3. Federal University of Sergipe, Nursing Departament, Lagarto, SE, Brasil.
Submitted on July 14, 2021.Accepted for publication on 19 May, 2022.Conflict of interests: none – Sponsoring sources: none.
Correspondence to: Katherine Olga Correia Alves SantosE-mail: [email protected]
© Sociedade Brasileira para o Estudo da Dor
RESUMO
JUSTIFICATIVA E OBJETIVOS: A mamografia é um exame de imagens das mamas, obtidas por meio de radiografia com realização da compressão do tecido mamário. A dor é um fator constantemente relatado pelas pacientes submetidas ao procedi-mento e, por esse motivo, evidencia-se a necessidade de estabe-lecer estratégias alternativas não farmacológicas que reduzam a sensação dolorosa. O objetivo deste estudo foi realizar uma re-visão integrativa sobre os métodos não farmacológicos utilizados para o alívio da dor durante o exame mamográfico.CONTEÚDO: A busca foi realizada no mês de abril de 2021 em quatro bases de dados (Pubmed, Medline, Scopus e CINAHL) utilizando os descritores “dor”, “manejo da dor”, “mamografia”, “musicoterapia” e “terapias complementares”. Após a leitura e análise final, quatro artigos atenderam aos critérios preestabele-cidos, abordando o manejo não farmacológico da dor durante a mamografia. Os estudos evidenciaram diferentes métodos para redução da dor, como a utilização de almofada e a alteração no protocolo de compressão, bem como a intervenção com música.CONCLUSÃO: Evidências sobre o manejo não farmacológico da dor relacionada à mamografia ainda são escassas. Entre as es-tratégias encontradas, o protocolo personalizado de compressão e o uso de almofadas compressíveis apresentaram eficácia analgé-sica, enquanto o uso da música não resultou em redução signi-ficativa da dor procedimental. No entanto, por se tratar de uma revisão integrativa, destaca-se a necessidade da realização de sín-teses de evidências com maior rigor metodológico para estimar o tamanho do efeito analgésico dessas intervenções.Descritores: Dor, Mamografia, Manejo da dor, Terapias com-plementares.
INTRODUCTION
Mammography is the most effective and low-cost procedure for early identification of breast alterations1. Among these is breast cancer, whose occurrence in women is the leading cause of can-cer mortality in the world, as well as in Brazil, where there is an estimation of 66280 new cases for the period of 2020-20222,3. The compression performed by the mammography unit reduces breast thickness in order to separate the overlapping structures and minimize the absorbed radiation4. Despite its importance in the identification of these changes in the breast tissue, the literature contains reports claiming that the receptivity to mam-mography is negatively influenced by procedural pain, discoura-
BrJP. São Paulo, 2022 apr-jun;5(2):143-6
DOI 10.5935/2595-0118.20220029-en
REVIEW ARTICLE
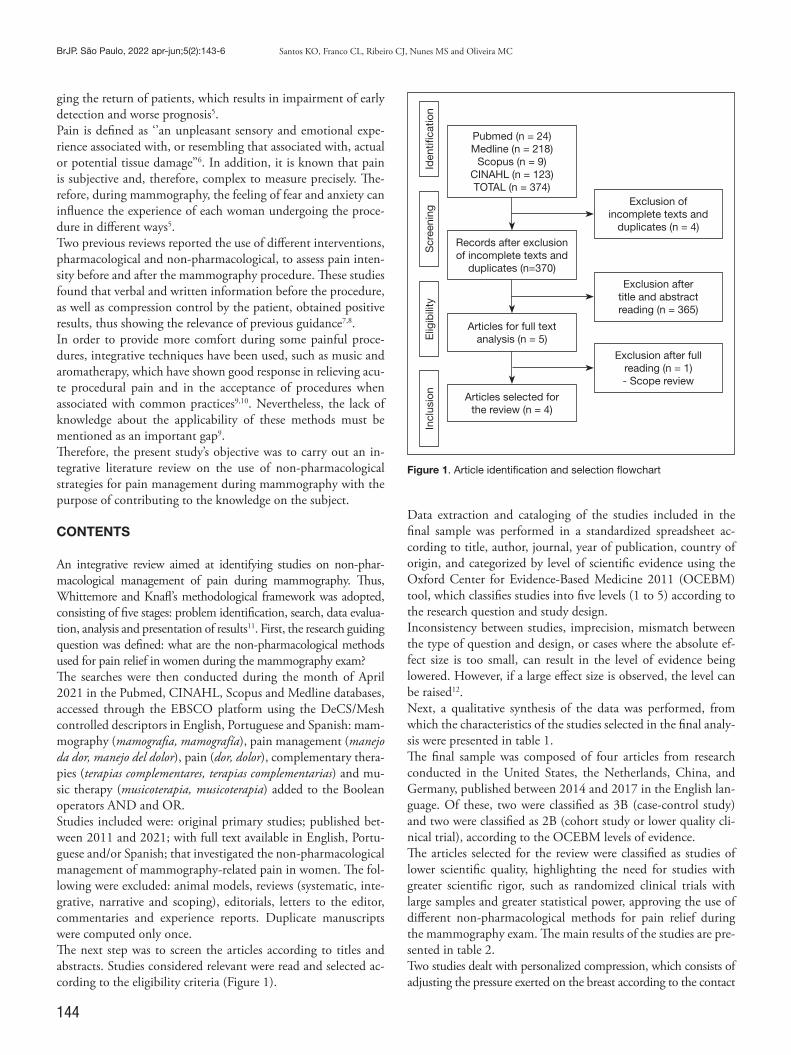
144
BrJP. São Paulo, 2022 apr-jun;5(2):143-6 Santos KO, Franco CL, Ribeiro CJ, Nunes MS and Oliveira MC
ging the return of patients, which results in impairment of early detection and worse prognosis5.Pain is defined as ‘’an unpleasant sensory and emotional expe-rience associated with, or resembling that associated with, actual or potential tissue damage’’6. In addition, it is known that pain is subjective and, therefore, complex to measure precisely. The-refore, during mammography, the feeling of fear and anxiety can influence the experience of each woman undergoing the proce-dure in different ways5. Two previous reviews reported the use of different interventions, pharmacological and non-pharmacological, to assess pain inten-sity before and after the mammography procedure. These studies found that verbal and written information before the procedure, as well as compression control by the patient, obtained positive results, thus showing the relevance of previous guidance7,8.In order to provide more comfort during some painful proce-dures, integrative techniques have been used, such as music and aromatherapy, which have shown good response in relieving acu-te procedural pain and in the acceptance of procedures when associated with common practices9,10. Nevertheless, the lack of knowledge about the applicability of these methods must be mentioned as an important gap9. Therefore, the present study’s objective was to carry out an in-tegrative literature review on the use of non-pharmacological strategies for pain management during mammography with the purpose of contributing to the knowledge on the subject.
CONTENTS
An integrative review aimed at identifying studies on non-phar-macological management of pain during mammography. Thus, Whittemore and Knafl’s methodological framework was adopted, consisting of five stages: problem identification, search, data evalua-tion, analysis and presentation of results11. First, the research guiding question was defined: what are the non-pharmacological methods used for pain relief in women during the mammography exam?The searches were then conducted during the month of April 2021 in the Pubmed, CINAHL, Scopus and Medline databases, accessed through the EBSCO platform using the DeCS/Mesh controlled descriptors in English, Portuguese and Spanish: mam-mography (mamografia, mamografía), pain management (manejo da dor, manejo del dolor), pain (dor, dolor), complementary thera-pies (terapias complementares, terapias complementarias) and mu-sic therapy (musicoterapia, musicoterapia) added to the Boolean operators AND and OR.Studies included were: original primary studies; published bet-ween 2011 and 2021; with full text available in English, Portu-guese and/or Spanish; that investigated the non-pharmacological management of mammography-related pain in women. The fol-lowing were excluded: animal models, reviews (systematic, inte-grative, narrative and scoping), editorials, letters to the editor, commentaries and experience reports. Duplicate manuscripts were computed only once.The next step was to screen the articles according to titles and abstracts. Studies considered relevant were read and selected ac-cording to the eligibility criteria (Figure 1).
Data extraction and cataloging of the studies included in the final sample was performed in a standardized spreadsheet ac-cording to title, author, journal, year of publication, country of origin, and categorized by level of scientific evidence using the Oxford Center for Evidence-Based Medicine 2011 (OCEBM) tool, which classifies studies into five levels (1 to 5) according to the research question and study design. Inconsistency between studies, imprecision, mismatch between the type of question and design, or cases where the absolute ef-fect size is too small, can result in the level of evidence being lowered. However, if a large effect size is observed, the level can be raised12.Next, a qualitative synthesis of the data was performed, from which the characteristics of the studies selected in the final analy-sis were presented in table 1.The final sample was composed of four articles from research conducted in the United States, the Netherlands, China, and Germany, published between 2014 and 2017 in the English lan-guage. Of these, two were classified as 3B (case-control study) and two were classified as 2B (cohort study or lower quality cli-nical trial), according to the OCEBM levels of evidence.The articles selected for the review were classified as studies of lower scientific quality, highlighting the need for studies with greater scientific rigor, such as randomized clinical trials with large samples and greater statistical power, approving the use of different non-pharmacological methods for pain relief during the mammography exam. The main results of the studies are pre-sented in table 2. Two studies dealt with personalized compression, which consists of adjusting the pressure exerted on the breast according to the contact
Incl
usio
nE
ligib
ility
Scr
eeni
ngId
entifi
catio
n
Pubmed (n = 24)Medline (n = 218)
Scopus (n = 9)CINAHL (n = 123)TOTAL (n = 374)
Exclusion after title and abstract reading (n = 365)
Exclusion after full reading (n = 1)- Scope review
Exclusion of incomplete texts and
duplicates (n = 4)
Records after exclusion of incomplete texts and
duplicates (n=370)
Articles for full text analysis (n = 5)
Articles selected for the review (n = 4)
Figure 1. Article identification and selection flowchart

145
Non-pharmacological methods for pain relief during mammography: integrative review
BrJP. São Paulo, 2022 apr-jun;5(2):143-6
area, i.e., its size14,16. This is an important factor to be evaluated, since in many places the compression force is the same in all proce-dures, regardless of the size and density of the examined breast.When comparing the standard compression protocol with the customized one, authors found that pain scores were reduced. The compression time resulted in an increase from 23% to 50% in the number of women who had severe pain in the clamping or immobilization phase of compression, showing that prolonged compression also interferes with the perception of pain14.Furthermore, another study addressed the fact that 60% of women reported pain in the axilla and not in the compression site16. These studies pointed out the customization of the compression protocol as the best method for pain relief during mammography, since both reported more intense pain for women with less voluminous breasts, a problem that was solved by customizing compression.The use of a radiotransparent, compressible pad (MammoPad, Hologic Inc, Bedford MA, USA) was tested in one of the studies. The use of this device as support for the breasts during com-pression presented good results for pain reduction as well as for
image quality, 92% of which were similar to the group that did not use the device. However, unlike the other studies, this one did not present an association between the incidence of pain and breast size15. The use of integrative and complementary therapies was one of the least investigated topics. Only one of the studies evaluated the efficacy of musical intervention in the management of pain during mammography. Although the group that received music therapy presented lower pain intensity initially, music did not reduce pain after adjustments for analgesic use and clinical con-ditions of the patients. Nevertheless, a significant relationship between pain and anxiety was identified, alerting to the need for more specific studies about integrative practices and pain percep-tion during mammography13.
CONCLUSION
The analysis of the results of this review revealed some non--pharmacological strategies for pain management during
Table 1. Description of studies included in the review.
Authors Country of Origin
Design and Level of Evidence
Sample Size Objectives
Zavotsky et al.13
United States of America
Prospective quasi-experimental study2B
100 women Examine the relationship between screening mammography and music intervention.
de Groot et al.14
Netherlands Observational Study3B
117 women Gain insight into existing and potential mammography pain preven-tion strategies by simultaneously recording breast mechanics and pain throughout the breast compression cycle.
Chan, Lo and Cheung15
China Cohort Study2B
100 women Evaluate the effectiveness of a radiotransparent pad (MammoPad; Ho-logic Inc, Bedfor [MA], US) during screening mammography to reduce pain in Chinese patients and the possibility of glandular dose reduction.
Ferder and Grunert16
Germany Prospective observational study3B
199 women Determine how to reduce the presence of pain during mammographic compression. In doing so, the authors evaluated its association with compression force, compressed breast surface area, breast density (ACR), and previous operations.
ACR = American College of Radiology.
Table 2. Results of evaluated studies
Authors Results
Zavotsky et al.13
The mean unadjusted pain scores (X) were lower for the music therapy group (X = 4.38 ± 2.58) compared to the control group (X = 4.44 ± 2.93), which received no music. A statistical calculation was performed to evaluate the association between an-xiety and pain scores. A significant, moderate, positive relationship was found between participants’ anxiety and pain scores (r = 0.54; p < 0.01). These results support an association between anxiety and pain in this population that may influence pain perception in both groups.
de Groot et al.14
Breast compressions consisted of a deformation phase for flattening and a clamping phase for immobilization. The clamping pha-se lasted 12.8 ± 3.6 seconds (mean ± standard deviation), 1.7 times longer than the deformation phase of 7.5 ± 2.6 seconds. Du-ring the clamping phase, the mean pain intensity increased from 4.75 to 5.88 (24%) on the numerical rating scale (NRS) from 0 to 10, and the proportion of women presenting severe pain (NRS ≥ 7) increased from 23% to 50%. Moderate pain (NRS ≥ 4) was reported up to four days after mammography. Multivariate analysis showed that pain memory from the previous mammogram and pain in the breast prior to compression are significant predictors of pain. Women with smaller breasts experienced more pain.
Chan, Lo and Cheung15
Of the 100 patients, 66.3% of women reported at least a 10% reduction in the level of discomfort with the use of the Mammo-Pad. No statistical differences were found for age, breast size, and discomfort level. The mean pain score was 5.7 ± 2.5 without the MammoPad vs 4.2 ± 1.8 with the use of the device.
Ferder and Grunert16
The thickness of the compressed breast was 65.2% of the uncompressed breast at a force of 10 daN (57.8% at 15 daN). When the force was increased from 10 daN to 15 daN, the average glandular dose (AGD) decreased by 17%. Compression tolerance was associated with breast size. More than 50% of mammograms with compression less than 9 daN were associated with higher pain levels. In the oblique projection, 60% of the women specified the axilla as the area of most pain.
NRS = Numerical Rating Scale; AGD = average glandular dose.

146
BrJP. São Paulo, 2022 apr-jun;5(2):143-6 Santos KO, Franco CL, Ribeiro CJ, Nunes MS and Oliveira MC
mammography, such as customization of the compression protocol, use of a radiotransparent compressible pad and mu-sic. Both customization of compression and use of the com-pressible pad showed satisfactory results for reducing proce-dural pain in the original studies. On the other hand, music was not effective for analgesia. The results of this review show that robust scientific evidence that can support the non-phar-macological management of pain during mammography is scarce, highlighting the need for additional studies with grea-ter methodological rigor.
AUTHORS’ CONTRIBUTION
Katherine Olga Correia Alves Santos Data Collection, Conceptualization, Project Management, Re-search, Methodology, Writing - Preparation of the original, Wri-ting - Review and Editing, Visualization Clarissa Lima Franco Methodology, Writing - Review and Editing Caique Jordan Nunes Ribeiro Conceptualization, Methodology, Writing - Review and Editing, Supervision Mariangela da Silva Nunes Conceptualization, Methodology, Writing - Review and Editing, Supervision Maria do Carmo de Oliveira Conceptualization, Methodology, Writing - Review and Editing, Supervision
REFERENCES
1. Serwan E, Matthews D, Davies J, Chau M. Mammographic compression practices of force- and pressure-standardisation protocol: A scoping review. J Med Radiat Sci. 2020; 67(3):233-42.
2. GLOBOCAN - Cancer Incidence and Mortality Worldwide: IARC Cancer. Lyon, France: International Agency for Research on Cancer. 2020. Disponível em: http://globocan.iarc.fr. Acesso em: 26/05/2021.
3. INCA - Instituto Nacional do Câncer José Alencar Gomes da Silva. Estimativa 2020. Incidência do Câncer no Brasil. Rio de Janeiro: INCA, 2019.
4. INCA - Instituto Nacional do Câncer José de Alencar Gomes da Silva. Ministério da Saúde. Atualização em mamografia para técnicos em radiologia. 2ª ed. rev. atual. Rio de Janeiro: INCA, 2019.
5. Gomes EA, Jesus MCP, Silva MH, Merighi MAB, Campos SEM. Motivos da não realiza-ção da mamografia por mulheres com idades entre 60 e 69 anos. Revista APS, 2018;21:2.
6. DeSantana JM, Perissinotti DM, Oliveira Junior JO, Correia LM, de Oliveira CM, Fonseca PR para a língua portuguesa da definição revisada de dor pela Sociedade Bra-sileira para o Estudo da Dor. BrJP. 2020;3(3):197-8.
7. Ribeiro NFP, Ribeiro CJN, Oliveira ALC, Dias EMF, Silva Santos, M, Santos AD et. al. Efeito analgésico da música durante a fotocoagulação retinal a laser em diabéticos: Um es-tudo cruzado, randomizado e controlado por placebo. Res Soc Develop. 2021;10(6):1-12.
8. Lakhan SE, Sheafer H, Tepper D. The effectiveness of aromatherapy in reducing pain: a systematic review and meta-analysis. Pain Res Treat. 2016;2016:8158693.
9. Whittemore R, Knafl K. The integrative review: Updated methodology. J Adv Nurs. 2005;52(5):546-53.
10. CEBM. The Centre for Evidence-Based Medicine develops. OCEBM Levels of Evi-dence. 2011;287-95.
11. Zavotsky KE, Banavage A, James P, Easter K, Pontieri-Lewis V, Lutwin L. The effects of music on pain and anxiety during screening mammography. Clin J Oncol Nurs. 2014;18(3):E45-9.
12. de Groot JE, Broeders MJM, Grimbergem CA, den Heeten GJ. Pain-preventing strategies in mammography: an observational study of simultaneously recorded pain and breast mechanics throughout the entire breast compression cycle. BCM Womens Health. 2015;15:26.
13. Chan HH, Lo G, Cheung PS. Is pain from mammography reduced by the use of a radiolucent MammoPad? Local experience in Hong Kong. Hong Kong Med J. 2016;22(3):210-5.
14. Ferder K, Grunert JH. Is individualizing breast compression during mammography useful? investigations of pain indications during mammography relating to compres-sion force and surface area of the compressed breast. Rofo. 2017;189(1):39-48.

147
ABSTRACT
BACKGROUND AND OBJECTIVES: According to the re-definition, acute pain is a somatic experience, with individual perception of physical or existential threat, comprising affective, cognitive and behavioral components. In critically ill patients, pain is a frequent and poorly controlled symptom, causing worse outcomes. The objective of this study was to explore the topic of acute pain in critically ill adult patients, focusing on some aspects of pathophysiology, in addition to updates regarding diagnosis, multimodal therapy and discussion of its control as a marker of good care practice. CONTENTS: A search strategy was performed with the descriptors previously defined in the Pubmed and Cochrane portals, in the pe-riod from 2011 to 2021, without a language restriction filter. Acute pain represents a physiological response to a nociceptive stimulus, with high relevance due to its ability to activate complex pathways (inflammatory, hormonal and immune), with systemic repercus-sions. Pain assessment is often performed using recognized scales, but with limited validation in patients with traumatic brain injury, burns and patients with severe delirium and/or dementia. Studies considering these patients point to the use of new technologies in an attempt to target this diagnosis, such as bedside pupillometry and the use of platforms capable of integrating multiparametric measu-rements. Regarding therapy, the concept of analgosedation, aiming at prioritizing analgesia in critically ill patients, presents an approach capable of improving clinical outcomes. In addition, there is a pre-ference for multimodal therapy as a good medical practice through the association of different drugs with different mechanisms of no-ciceptive blockade as a strategy to achieve pain control and facilitate the reduction of opioid consumption.CONCLUSION: Due to its systemic effects and prevalence, acute pain is still a relevant problem in intensive care units. New diagnostic methods are being marketed with the aim of targeting this evaluation in complex patients. The approach to acute pain
Acute pain in the critically ill patient: revisiting the literatureDor aguda no paciente crítico: revisitando a literatura
Jose Mauro Vieira Junior1, Laura Herranz Prinz1
Jose Mauro Vieira Junior – https://orcid.org/0000-0002-8607-8145;Laura Herranz Prinz – https://orcid.org/0000-0002-1944-6980.
1. Syrian-Lebanese Hospital, Education and Research Institute, São Paulo, SP, Brazil.
Submitted on July 21, 2021.Accepted for publication on April 22, 2022.Conflict of interests: none – Sponsoring sources: none.
Correspondence to: Laura Herranz PrinzE-mail: [email protected]
© Sociedade Brasileira para o Estudo da Dor
should prioritize the use of multimodal techniques, which pre-sent more consistent clinical responses, in addition to reducing the consumption of opioids. The existence of multidisciplinary teams specialized in pain control in the hospital environment is able to assist in difficult cases and help in quality audits.Keywords: Acute pain, Critical care, Analgesia, Opioids analge-sics, Pain management, Quality of health care.
RESUMO
JUSTIFICATIVA E OBJETIVOS: Conforme redefinição, a dor aguda é uma experiência somática, com percepção individual de ameaça física ou existencial, compreendendo componentes afeti-vos, cognitivos e comportamentais. Em pacientes críticos, a dor representa um sintoma frequente e mal controlado, ocasionando piores desfechos. O objetivo deste estudo foi explorar a temática da dor aguda nos pacientes críticos adultos, com enfoque em alguns aspectos de fisiopatologia, além de atualizações em relação a diagnóstico, terapêutica multimodal e discussão de seu controle como um marcador de boa prática assistencial. CONTEÚDO: Foi realizada estratégia de busca com os descri-tores previamente definidos nos portais Pubmed e Cochrane, no período de 2011 a 2021, sem filtro de restrição para idioma. A dor aguda representa uma resposta fisiológica a um estímulo no-ciceptivo, tendo alta relevância por sua capacidade de ativar vias complexas (inflamatórias, hormonais e imunes), com repercussões sistêmicas. A avaliação da dor é frequentemente realizada através de escalas reconhecidas, porém com validação limitada em pacien-tes com trauma cranioencefálico, queimados e portadores de de-lirium e/ou demência acentuados. Os estudos considerando esses pacientes apontam para o uso de novas tecnologias na tentativa de objetivar esse diagnóstico, como a pupilometria à beira leito e o uso de plataformas capazes de integrar medidas multiparamétricas. Em relação à terapêutica, o conceito de analgossedação, objetivan-do priorização de analgesia nos pacientes críticos, apresenta abor-dagem capaz de melhorar desfechos clínicos. Além disso, há prefe-rência da terapêutica multimodal como boa prática médica através da associação de diferentes fármacos com diversos mecanismos de bloqueio nociceptivo como estratégia para alcançar controle álgico e facilitar a redução do consumo de opioides. CONCLUSÃO: Por seus efeitos sistêmicos e sua prevalência, a dor aguda ainda é problemática relevante nas unidades de terapia intensiva. Novos métodos diagnósticos estão sendo comerciali-zados com a proposta de objetivar essa avaliação em pacientes complexos. A abordagem da dor aguda deve priorizar o emprego de técnicas multimodais, que apresentam respostas clínicas mais consistentes, além de redução no consumo de opioides. A exis-
BrJP. São Paulo, 2022 apr-jun;5(2):147-53
DOI 10.5935/2595-0118.20220024-en
REVIEW ARTICLE
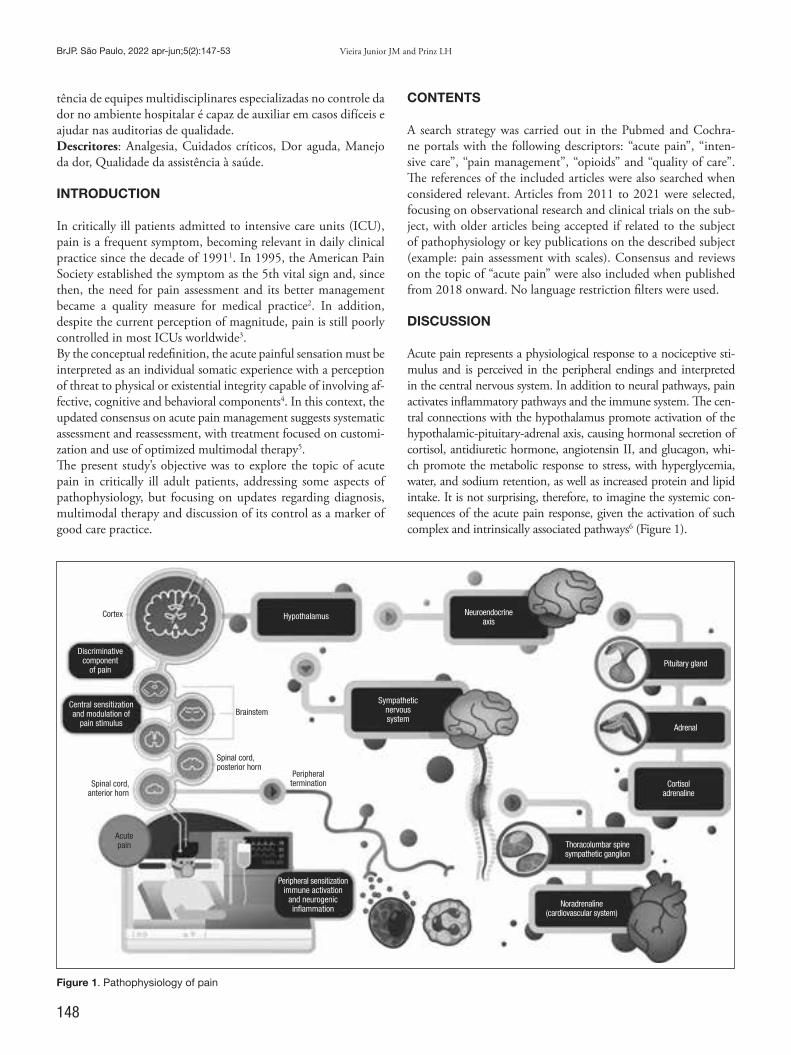
148
BrJP. São Paulo, 2022 apr-jun;5(2):147-53 Vieira Junior JM and Prinz LH
tência de equipes multidisciplinares especializadas no controle da dor no ambiente hospitalar é capaz de auxiliar em casos difíceis e ajudar nas auditorias de qualidade.Descritores: Analgesia, Cuidados críticos, Dor aguda, Manejo da dor, Qualidade da assistência à saúde.
INTRODUCTION
In critically ill patients admitted to intensive care units (ICU), pain is a frequent symptom, becoming relevant in daily clinical practice since the decade of 19911. In 1995, the American Pain Society established the symptom as the 5th vital sign and, since then, the need for pain assessment and its better management became a quality measure for medical practice2. In addition, despite the current perception of magnitude, pain is still poorly controlled in most ICUs worldwide3.By the conceptual redefinition, the acute painful sensation must be interpreted as an individual somatic experience with a perception of threat to physical or existential integrity capable of involving af-fective, cognitive and behavioral components4. In this context, the updated consensus on acute pain management suggests systematic assessment and reassessment, with treatment focused on customi-zation and use of optimized multimodal therapy5. The present study’s objective was to explore the topic of acute pain in critically ill adult patients, addressing some aspects of pathophysiology, but focusing on updates regarding diagnosis, multimodal therapy and discussion of its control as a marker of good care practice.
CONTENTS
A search strategy was carried out in the Pubmed and Cochra-ne portals with the following descriptors: “acute pain”, “inten-sive care”, “pain management”, “opioids” and “quality of care”. The references of the included articles were also searched when considered relevant. Articles from 2011 to 2021 were selected, focusing on observational research and clinical trials on the sub-ject, with older articles being accepted if related to the subject of pathophysiology or key publications on the described subject (example: pain assessment with scales). Consensus and reviews on the topic of “acute pain” were also included when published from 2018 onward. No language restriction filters were used.
DISCUSSION
Acute pain represents a physiological response to a nociceptive sti-mulus and is perceived in the peripheral endings and interpreted in the central nervous system. In addition to neural pathways, pain activates inflammatory pathways and the immune system. The cen-tral connections with the hypothalamus promote activation of the hypothalamic-pituitary-adrenal axis, causing hormonal secretion of cortisol, antidiuretic hormone, angiotensin II, and glucagon, whi-ch promote the metabolic response to stress, with hyperglycemia, water, and sodium retention, as well as increased protein and lipid intake. It is not surprising, therefore, to imagine the systemic con-sequences of the acute pain response, given the activation of such complex and intrinsically associated pathways6 (Figure 1).
Figure 1. Pathophysiology of pain
Cortex
Discriminative component
of pain
Central sensitization and modulation of
pain stimulus
Hypothalamus Neuroendocrine axis
Pituitary gland
Adrenal
Cortisol adrenaline
Thoracolumbar spine sympathetic ganglion
Noradrenaline (cardiovascular system)
Sympathetic nervous system
Acute pain
Peripheral sensitization immune activation
and neurogenic inflammation
Spinal cord, anterior horn
Brainstem
Spinal cord, posterior horn
Peripheral termination

149
Acute pain in the critically ill patient: revisiting the literature BrJP. São Paulo, 2022 apr-jun;5(2):147-53
The exact prevalence of pain in ICUs is difficult to assess, given the variability of studies, however, a systematic review indica-ted that approximately 50% of critically ill patients report pain and more than 35% experience severe pain at some point during their hospital stay7. The ICU is clearly an environment of mul-tiple potentials for pain and, although advances have occurred in the last years, its approach is still a challenge, especially in patients that are female, on mechanical ventilation, chronically critical, young people with low resilience, psychiatric disorders (depression, anxiety, bulimia and alcohol abuse) and previous users of benzodiazepines8,9. In addition, the literature shows growing evidence associating poor pain control to worse clinical outcomes10. Poorly controlled pain in the ICU is already known to be associated with longer mechanical ventilation time, hospitalization, and delirium11-13. In a systematic review from 2015, critically ill patients evaluated for pain had outcomes related to ICU length of stay, complications, adverse events, duration of mechanical ventilation and mortality analyzed14. Despite methodological differences, the study con-firms that systematic pain assessment seems to have a favorable impact in the short term. In the long term, it is known that patients may also develop chronic pain and post-traumatic stress syndrome15. If pain is responsible for these worse outcomes, on the other hand, its adequate control with epidural analgesia, for example, can reduce cardiovascular events, pulmonary throm-boembolism and promote faster recovery of organic functions in selected critically ill patients16.
Pain assessment in the intensive care unit – from known sca-les to new technologies The use of pain scales in the ICU comes from a heterogeneous implementation process, with validation and training of sca-les in different patient profiles. Because the sensorial expe-rience of pain is absolutely personal, the health professional’s own perception is usually flawed, tending to underestimate pain, while the caregivers and/or family members of these pa-tients tend to overestimate it17. A multicenter, prospective, and observational study reported that more than 50% of the analyzed ICUs had pain measurement instruments and anal-gesia protocols, but the application of both was less than 30% of the cohorts18. Although no scale alone is sensitive enough to correctly assess pain, the recommendation is that patients able to verbally re-port their pain must be assessed by the verbal numeric rating scale (vNRS zero – 10)19. The biggest challenge lies in critically ill patients with difficulties in self-expression. In the literatu-re, it is already known that isolated fluctuations of vital signs are poor predictors of pain assessment and must be seen as an adverse event associated with severe pain20. In these cases, the Behavior Pain Scale21 and the Critical-Care Pain Observational Tool (CPOT)22 are both validated, having robust psychometric properties and similar reproducibility in published studies, both for clinical, surgical and polytraumatized patients. It is important to consider that pain assessment in patients with traumatic brain injury, burns, patients with acute delirium and/or dementia is still a challenge. The studies considering this
profile of patients, especially those comatose or deeply sedated, point to the use of the bispectral index and the use of pupillome-try as an attempt to objectify this assessment23. In a study with 100 immediate postoperatory (PO) patients, a high correlation (0.88 p<0.001) was found between pain intensity measured by pain vNRS and the pupillary reflex measured with a bedside pu-pillometer as a guide for the titration of intravenous morphine24.Recently, the use of a new analgesia monitoring (Analgesia No-ciception Index) was published, using electrocardiogram elec-trodes integrated with a computer model of data interpretation, including subcortical functions, bronchial receptor reflexes, the vagus nerve nucleus and the sinoatrial node stimuli25. Studies have been published in an attempt to validate this new modality in order to reduce opioid consumption in the PO26. Using simi-lar technology, a monitor that integrates cardiac variability data with temperature, plethysmography, and skin conductance res-ponse on a multiparametric platform (Nociception Level Index), via a device placed on a chiropractor, was developed.Through advanced artificial intelligence algorithms, nociception is presented on a scale of zero to 100, ranging from no pain to severe pain. Its validation has also been performed in periope-rative patients27 with more severe profiles. Still using artificial intelligence, a recent publication described the development of algorithms specialized in facial expression image analysis, con-figuring a potential tool in detection and analysis of pain and its intensity28 at bedside in patients incapable of expressing their pain.
Pain in the intensive care unit and the (excessive) use of opioidsOpioids are the most commonly used drugs for pain manage-ment in critically ill patients, despite the current knowledge of their adverse effects, such as tolerance, dependence, and with-drawal syndrome. Tolerance seems to be an even greater problem in burn patients, patients with prolonged mechanical ventilation and pediatric patients29. Its use has acquired such significant di-mensions that it has become a public health issue in the US. In 2017, analyzing the impact of this situation in the country’s ICUs, the number of deaths due to opioid abuse has reportedly increased substantially in recent years within ICU30. Opioids still have formal indication for moderate to severe pain control5, and the choice of drug and dose should be titrated ac-cording to the patient’s profile. Besides inducing metabolic ileus and hypotension, the use of opioids can be related to delirium and immunosuppression29,31. In critically ill patients, particular attention should be paid to those with altered body distribution volume, polypharmacy, and renal and hepatic alterations. The prolonged use of opioids causes persistent stimulation of neuroreceptors, promoting desensitization and signaling of pro-nociceptive pathways29, resulting in dose escalation due to tolerance. In addition, the use of opioids in association with inflammatory states, infections and stress promotes neuroin-flammation by activating glial receptors in the central nervous system32, a factor related to the induction of hyperalgesia. Accor-ding to the literature, these events seem even worse in critically ill patients when compared to other patients.

150
BrJP. São Paulo, 2022 apr-jun;5(2):147-53 Vieira Junior JM and Prinz LH
Due to this current evidence, there is an academic effort in the strategic use of analgesic measures that spare opioids. When ne-cessary and indispensable, opioids should be used in the lowest possible doses and in a short period of time, with daily adjust-ments, and in association with the use of other analgesic drugs. Remifentanil, for example, should be avoided because of its po-tent induction of hyperalgesia. In critically ill patients with a history of opioid abuse and tolerance, rotation of opioids may be necessary to subvert desensitization of active receptors or me-tabolites (the use of methadone, for example). In patients with hyperalgesia, the use of opioids can cause worsening of pain, re-quiring the use of multimodal therapy, with activation of other nociceptive receptors for pain control29.
Acute pain approach and multimodal therapy The concept of analgosedation emerged in recent years, aiming at analgesia instead of sedation in acute critically ill patients, allowing minimal or no sedation, including during mechanical ventilation, with better outcomes, such as shorter ICU stay33. This process also promoted rationalization in the negative effects of sedatives, especially benzodiazepines.The current broader concept of good practice is patient-centered care34,35, allowing comfort with adequate analgesia, minimum
sedation, and maximum humanization (besides open visitation policies and mobilization protocols). The logic is to customize the level of comfort (total pain)36, trying to evaluate the pain component not in an isolated and numerical manner, but en-compassing the psychosocial and affective components of pa-tients through qualitative and functionality analysis.Multimodal analgesia, which is characterized by pain control through the association of different drugs with several nocicepti-ve blocking mechanisms, should be valued for being highly effi-cient in the treatment of pain when compared to the use of only one high-dose analgesic, besides facilitating the opioid sparing strategy, even in trauma patients37,38. Multimodal therapy inclu-des the combined use of common analgesics (dipyrone and para-cetamol) and controlled doses of nonsteroidal anti-inflammatory drugs (NSAIDs), besides the adjuvant use of other drugs, such as alpha-adrenergic agonists (dexmedetomidine), as well as ketami-ne and lidocaine, in combinations tailored to the patient’s profile and analgesic needs39,40 (Table 1).Dexmedetomidine is a highly selective central alpha2-agonist agent with a short half-life that promotes sedative effects without central nervous system depression and has analgesic potential via modulation of the posterior horn of the spinal cord, and is currently a drug with a good titration profile in critically ill pa-
Table 1. Pharmacological options for acute pain management.
Main drugs/mechanisms of action Indications/advantages Adverse effects/considerations
Opioids29
G-protein-coupled opioid receptor ago-nists, promoting K-channel opening and inhibition of voltage-dependent calcium channels
Important role in severe acute pain Respiratory depression, pruritus, metabolic ileus, urinary retention
Use should be rationalized due to adverse effects and especially to dependence and OIH
Non-steroidal anti-inflammatory drugs40
Cyclooxygenase inhibitors
Good pain control, reducing inflammation
Low, time-limited doses (< 48 h) are well tolerated in most patients
Bleeding, renal dysfunction and acute coronary syndrome
Multiple regimens and doses used in studies, most data against use is controversial
Gabapentinoids40,56
Calcium channel agonist – voltage-depen-dent
Anticonvulsants with effect on neuropathic pain or progression to chronic pain
Sedation, visual disturbances and vertigoSpecial care in the elderly and renal patients
Multiple regimens in studies involving postopera-tive and acute pain, with controversial data
Lidocaine47
Multimodal mechanism; main effect in blocking sodium channels
Multimodal analgesic effect, with action on OIH, in low dose (± bolus) continuous infusion
Continuous infusion should be avoided for >24hAvoid in extremes of weight (< 40kg or > 120kg)Do not use intravenous dose concomitant with use or action time of other local anestheticsRisk of central nervous system and cardiovascular toxicity, especially in the presence of hepatic and renal dysfunction
Dexmedetomidine41
Central alpha-2-agonist
Good control of delirium/sedative effect, without respiratory depression
Analgesic effect in perioperative studies and aid in OIH
Hypotension and bradycardia, especially associa-ted with dose and frail patients
Ketamine43
Blockade of N-methyl-D-aspartate recep-tors
Analgesic effect and in control of OIHLow dose continuous infusion (± bolus) can be used as adjunct in perioperative, burn and mechanic ventilation patients
Dissociative symptoms, hallucinations
Cardiovascular effects and increased intracranial pressure
OIH = opioid-induced hyperalgesia

151
Acute pain in the critically ill patient: revisiting the literature BrJP. São Paulo, 2022 apr-jun;5(2):147-53
tients41. Especially in surgical patients, several publications point to pain control during adjuvancy, with good tolerability (atten-tion to hypotension and bradycardia, in particular, is required). In laparoscopic surgeries, the use of the drug reduces the intense PO pain, the need for analgesia and the time of use of rescue analgesia42. The literature also contains references of the adjuvant use of dexmedetomidine in the modality of patient-controlled analgesia (PCA) and as an adjunct drug in regional blockades, providing good pain control in ERAS41 (Enhanced Recovery af-ter Surgery) patients with opioid-free approach.Ketamine is a drug that induces sedation and analgesia mediated by inhibition of N-methyl-D-aspartate (NMDA) receptors and activation of µ-type opioid receptors. It can cause tachycardia and hypertension, with minimal central depressant effect, but attention is required to its dissociative effects described in the literature43. The latest pain management consensus (2018) re-commends the use of ketamine as an adjunct drug to the use of opioids for the management of PO pain in critically ill patients5. In addition, publications on the adjuvant use of sub-anesthetic doses (~0.1mg/kg/h) in the management of mechanical ventila-tion44 and its use in the control of opioid-induced hyperalgesia43 have been increasing. In a recent systematic review in the surgical setting, the use of ketamine was well tolerated and significantly reduced the consumption of opioids and other analgesics in ge-neral PO patients, including in orthopedic procedures45. Lidocaine is an antiarrhythmic drug with an anesthetic effect of multimodal mechanism, and is currently used in intrave-nous administration for PO pain control, in addition to its use in oncologic, OIH or neuropathic pain patients. In therapeutic concentrations, it promotes sodium channel blockade, suppres-sion of action potentials in injured neuronal fibers, and an an-ti-inflammatory effect; however, at higher doses, it can promote blockade in a wide range of receptors, which can lead to high cardiovascular risk and neurotoxicity. The correlation between adequate plasma levels and signs and symptoms of toxicity does not seem to be linear46. As described in a recent international consensus on efficacy and safety in the use of PO analgesia, one should use up to 1.5 mg/kg/h in continuous infusion for no more than 24 h, under mo-nitoring and reevaluation, not concomitant to the use of regional blockades47. The most recent systematic review, including several types of open and laparoscopic surgeries (4525 patients in 68 studies), concluded, due to the heterogeneity of the studies, that there was no significant effect on the use of lidocaine to reduce opioid consumption and pain scores in the use over 24 h48. In the last decades, there has been a great advance in interven-tional techniques for pain management. The current blockades, which are ultrasound-guided, seem safe, even in critically ill pa-tients with coagulopathy49. There are benefits in analgesia, re-duction of opioid consumption and chronic postoperative pain through adrenergic, inflammatory, and immune modulation, even in patients with higher morbidity and oncologic surgery patients, profiles that are very present in modern ICUs50,51. In orthopedic hip and knee surgeries, the role of neuroaxis anesthe-sia in relation to general anesthesia in reducing worse outcomes, including mortality, is well established52.
Especially in complex thoracic and abdominal surgery patients, the use of regional blocks combined with epidural anesthesia are emphasized in the literature for better PO pain control5,50. Fur-thermore, there is the emergence of fascial planes blockades, with good evidence in acute pain management and less adverse effects (urinary retention and hypotension), especially in thoraco-abdo-minal approaches53,54, favoring satisfaction, early rehabilitation, and shorter hospital stay. Despite current advances, there is still a large field of ongoing research on the topic, especially in tech-niques of application and management of infusions directly into more complex wounds, use of anesthetics with longer half-life (16 h x 72 h), and use of intravenous drugs and adjunct perineu-ral to increase analgesic effects55.The use of opioids in PCA systems seems to be effective for pain control and improvement of patient satisfaction57. Modern pumps allow the drug release by the patients themselves in doses program-med by the healthcare team and with administration limits per dose and time intervals, in order to avoid build-ups and toxicity. Besides the use of opioids, the current systems allow the infusion of other analgesics (such as NSAIDs, anesthetics, and dexmedeto-midine) in epidural, subcutaneous, and transdermal use58. Other methods of non-invasive and easy management pain con-trol have been published, such as sublingual tablets, patches, and transdermal systems (fentanyl, lidocaine and, more recently, dex-medetomidine), but evidence is still scarce regarding their use and effectiveness in acute pain55,58,59. There is also a recommendation to expand the use of non-phar-macological therapies and psychotherapeutic follow-up in pain management, especially in cancer patients, such as music therapy, acupuncture, and cryotherapy5. The entire multiprofessional team must be familiar with these therapies, and each therapeutic pro-posal must be individually adapted to each patient. It is essential that reassessments be done frequently and therapies readjusted at any time, aiming at a balance between comfort and adverse effects. It is also worth noting that the increasing use of specialized pain services within the critically ill care environment seems to impro-ve satisfaction and quality of care60, especially in patients of more difficult management, such as those with chronic acute pain, acute pain difficult to manage after extensive trauma, patients with to-lerance/dependence to opioids and in subpopulations of higher risk (elderly, sedated, severe). These (multidisciplinary) teams also assist in registries, protocol management, continued education on treatments, adverse effects encountered, and data auditing.
About the futureTranslational study for promising pain control therapies in the ICU may represent a future breakthrough61. Among the most promising drugs, nicotinic acetylcholine receptor agonists seem to reduce glial activation, modulating the inflammatory immune response and promoting a central effect on pain and hyperalgesia mechanisms62. There are still issues to be explored, for example: which factors associated with gender, age, ethnicity, and behaviors affect pain perception and the pharmacogenomics of the various drugs in this context, what is the best objective measure of pain in pa-tients who cannot communicate63, how serum biomarkers of

152
BrJP. São Paulo, 2022 apr-jun;5(2):147-53 Vieira Junior JM and Prinz LH
pain could assist in this process64, what are the best combinations and doses of analgesic drugs adjunct to opioids, and which other negative outcomes acute pain can cause in target organs. Furthermore, there is a lack of randomized clinical trials on this subject, largely due to ethical issues. New studies may help in the further understanding of pain intensity assessment, efficiency of sedatives and analgesics, adverse events and complications asso-ciated with analgesics, negative outcomes, and even the associa-tion between pain and inflammation through the serum dosage of circulating neuropeptides and biochemical markers.
CONCLUSION Because of its systemic effects and prevalence, acute pain is still a relevant problem in the ICU. New diagnostic methods are being marketed with the proposal to objectify this evaluation in complex patients. The approach to acute pain must prioritize multimodal techniques, which present more consistent clinical responses, in addition to reducing opioid consumption. The existence of mul-tidisciplinary teams specialized in pain control in the hospital envi-ronment is able to assist in difficult cases and help in quality audits.
AUTHORS’ CONTRIBUTION
Jose Mauro Vieira Junior Conceptualization, Writing - Review and EditingLaura Herranz Prinz Conceptualization, Writing - Preparation of the original, Wri-ting - Review and Editing
REFERENCES
1. Puntillo KA. Pain experiences of intensive care unit patients. Heart Lung. 1990;19(5 Pt 1):526-33.
2. Morone NE, Weiner. DK. Pain as the 5th vital sign: exposing the vital need for pain education. Clin Ther. 2013;35(11):1728-32.
3. Gan TJ. Poorly controlled postoperative pain: prevalence, consequences and preven-tion. J Pain Res. 2017;10:2287-98.
4. Cohen M, Quintner J, van Rysewyk S. Reconsidering the International Association for the Study of Pain definition of pain. Pain Rep. 2018;(2):e634.
5. Devlin JW, Skrobik Y, Vice-chair F, Gélinas C, Needham DM, Slooter AJC, et al. Clinical practice guidelines for the prevention and management of pain, agitation / sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018;46(9):e825-e873.
6. Basbaum AI, Bautista DM, Scherrer G, Julius D. Cellular and molecular mechanisms of pain. Cell. 2009;139(2):267-84.
7. Gregory J, McGowan L. An examination of the prevalence of acute pain for hospita-lised adult patients: a systematic review. J Clin Nurs. 2016;25(5-6):583-98.
8. Puntillo KA, Max A, Timsit J, Vignoud L, Chanques G, Robleda G, et al. Determi-nants of procedural pain intensity in the intensive care unit. Am J Respir Crit Care Med. 2014;189(1):39-47.
9. Puntillo KA, Max A, Timsit JF, Ruckly S, Chanques G, Robleda G, et al. Pain distress: the negative emotion associated with procedures in ICU patients. Intensive Care Med. 2018;44(9):1493-501.
10. Olsen BF, Rustøen T, Sandvik L, Jacobsen M, Valeberg BT. Results of implementing a pain management algorithm in intensive care unit patients: the impact on pain assessment, length of stay, and duration of ventilation. J Crit Care. 2016;(36):207-11.
11. Hoc AP. Pain Assessment is associated with decreased duration of mechanical ventila-tion in the intensive care unit. Crit Care Med. 2009;111(6):1308-16.
12. Sebbane M, Perrigault P, Mann C. Impact of systematic evaluation of pain and agita-tion in an intensive care unit. 2006;34(6):1691-9.
13. Vaurio LE, Sands LP, Wang Y, Mullen EA, Leung JM. Postoperative delirium: the importance of pain and pain management. Anesth Analg. 2006;102(4):1267-73.
14. Georgiou E, Hadjibalassi M, Lambrinou E, Andreou P, Papathanassoglou ED. The impact of pain assessment on critically ill patients outcomes: a systematic review. Bio-med Res Int. 2015:2015:503830.
15. Puntillo KA, Naidu R. Chronic pain disorders after critical illness and ICU-acquired opioid dependence. Curr Opin Crit Care. 2016;22(5):506-12.
16. Pöpping D. Impact of epidural analgesia on mortality and morbidity after surgery - systematic review and meta-analysis of randomized controlled trials. Ann Surg. 2014;259(6):1056-67.
17. Seers T, Derry S, Seers K, Moore RA. Professionals underestimate patients’ pain: a comprehensive review. Pain. 2018;195(5):811-8.
18. Burry LD, Williamson DR, Perreault MM, Rose L, Cook DJ, Ferguson ND, et al. Analgesic, sedative, antipsychotic, and neuromuscular blocker use in Canadian in-tensive care units: a prospective, multicentre, observational study. Can J Anesth. 2014;61(7):619-30.
19. Ahlers SJ, van Gulik L, van der Veen AM, van Dongen HP, Bruins P, Belitser SV, et al. Comparison of different pain scoring systems in critically ill patients in a general ICU. Crit Care. 2008;12(1):R15.
20. Arbour C, Gélinas C. Are vital signs valid indicators for the assessment of pain in pos-toperative cardiac surgery ICU adults? Intensive Crit Care Nurs. 2010;26(2):83-90.
21. Payen J, Bru O, Bosson J, Lagrasta A. Assessing pain in critically ill sedated patients by using a behavioral pain scale. Crit Care Med. 2001;29(12):2258-63.
22. Fillion L, Puntillo KA, Viens C, Fortier M, City Q. Validation of the critical-care pain observation tool in adult patients. Am J Crit Care. 2006;15(4):420-7.
23. Lukaszewicz A, Dereu D, Gayat E, Payen D. The relevance of pupillometry for evalua-tion of analgesia. Anesth Analg. 2015;120(6):1297-300.
24. Aubrun F, Beaussier M. Objective assessment of the immediate postoperative analge-sia using pupillary reflex measurement. a prospective and observational study. Anes-thesiology. 2012;116(5):1006-12.
25. Daccache G, Jeanne M, Fletcher D. The analgesia nociception index: tailoring opioid administration. Anesth Analg. 2017;125(1):15-7.
26. Upton HD, Hons B, Ludbrook GL, Wing A, Hons B, Hons B, et al. Intraoperati-ve “analgesia nociception index”– guided fentanyl administration during sevoflurane anesthesia in lumbar discectomy and laminectomy: a randomized clinical trial. Anesth Analg. 2017;125(1):81-90.
27. Edry R, Recea V, Dikust Y, Sessler D. Preliminary intraoperative validation of the nociception level index. Anesthesiology. 2016;125(1):193-203.
28. Bargshady G, Zhou X, Deo RC, Soar J, Whittaker F, Wang H. Enhanced deep lear-ning algorithm development to detect pain intensity from facial expression images. Expert Syst Appl. 2020;149.
29. Martyn JAJ, Mao J, Bittner EA. Opioid tolerance in critical illness. N Engl J Med. 2019;380(4):365-78.
30. Stevens JP, Wall MJ, Novack L, Marshall J, Hsu DJ, Howell MD. The critical care crisis of opioid overdoses in the United States. Ann Am Thorac Soc. 2017;14(12):1803-9.
31. Kosciuczuk U, Knapp P, Lotowska-Cwiklewska AM. Opioid-induced immunosu-ppression and carcinogenesis promotion theories create the newest trend in acute and chronic pain pharmacotherapy. Clinics. 2020;75:e1554.
32. Hutchinson MR, Shavit Y, Grace PM, Rice KC, Maier SF, Watkins LR. Exploring the neuroimmunopharmacology of opioids: an integrative review of mechanisms of central immune signaling and their implications for opioid analgesia. Pharmacol Rev. 2011;63(3):772-810.
33. Faust A, Rajan P, Sheperd LA. Impact of an analgesia-based sedation protocol on mechanically ventilated patients in a medical intensive care unit. Anesth Analg. 2016;123(4):903-9.
34. Vincent JL, Shehabi Y, Walsh TS, Pandharipande PP, Ball JA, Spronk P, et al. Comfort and patient-centred care without excessive sedation: the eCASH concept. Intensive Care Med. 2016;42(9):962-71.
35. Marra A, Ely E, Pandharipande P. The ABCDEF Bundle in Critical Care. Crit Care Clin. 2017;33(2):225-43.
36. Rustam JS, Kongsuwan W, Kitrungrote L. Comfort in patients receiving mechanical ventilation : a literature review. Crit Care Nurs J. 2018;11(2):1-7.
37. Hamrick KL, Beyer CA, Lee JA, Cocanour CS, Duby JJ. Multimodal analgesia and opioid use in critically ill trauma patients. J Am Coll Surg. 2019;228(5):769-775.e1.
38. Frauenknecht J, Kirkham KR, Albrecht E. Analgesic impact of intra-operative opioids vs opioid-free anaesthesia: a systematic review and meta-analysis. Anaesthesia. 2019;(74):651-62.
39. Wampole CR, Smith KE. Beyond opioids for pain management in adult critically ill patients. J Pharm Pract. 2019;32(3):256-70.
40. Harvin JA, Kao LS. Pain management in the surgical ICU patient. Curr Opin Crit Care. 2020;26(6):628-33.
41. Kaye AD, Chernobylsky DJ, Thakur P, Siddaiah H, Kaye RJ, Eng LK, et al. Dexmede-tomidine in enhanced recovery after surgery (ERAS) protocols for postoperative pain. Curr Pain Headache Rep. 2020;24(5):21.
42. Panchgar V, Shetti AN, Sunitha HB, Dhulkhed VK, Nadkarni AV. The effectiveness of intravenous dexmedetomidine on perioperative hemodynamics, analgesic requi-rement, and side effects profile in patients undergoing laparoscopic surgery under general anesthesia. Anesth Essays Res. 2017;11(1):72-7.
43. Brown K, Tucker C. Ketamine for acute pain management and sedation. Crit Care Nurse. 2020;40(5):26-33.
44. Lipscomb J. Subanesthetic ketamine for acute pain in critically ill patients. US Pharm. 2020;45(4):1-10.
45. Brinck EC, Tiippana E, Heesen M, Bell RF, Straube S, Moore RA, et al. Perioperative intravenous ketamine for acute postoperative pain in adults (Review). Cochrane Da-tabase Syst Rev. 2018;(12):CD012033.
153
Acute pain in the critically ill patient: revisiting the literature BrJP. São Paulo, 2022 apr-jun;5(2):147-53
46. Mo Y, Thomas MC, Antigua AD, Ebied AM, Karras GE Jr. Continuous lidocaine infusion as adjunctive analgesia in intensive care unit patients. J Clin Pharmacol. 2017;57(7):830-6.
47. Foo I, Macfarlane AJR, Srivastava D, Bhaskar A, Barker H, Knaggs R, et al. The use of intravenous lidocaine for postoperative pain and recovery: international consensus statement on efficacy and safety. Anaesthesia. 2021;76(2):238-50.
48. Weibel S, Jelting Y, Pace NL, Helf A, Eberhart LH, Hahnenkamp K, et al. Conti-nuous intravenous perioperative lidocaine infusion for postoperative pain and reco-very in adults. Cochrane Database Syst Rev. 2018;(6):CD009642.
49. Wiebalck A, Grau T. Ultrasound imaging techniques for regional blocks in intensive care patients. Crit Care Med. 2007;35(5 Suppl)S268-74.
50. Albrecht E, Chin KJ. Advances in regional anaesthesia and acute pain management: a narrative review. Anaesthesia. 2020;75:(Suppl 1):e101-e110.
51. Cata JP. Outcomes of regional anesthesia in cancer patients. Curr Opin Anaesthesiol. 2018;(31):593-600.
52. Perlas A, Chan VW, Beattie S. Anesthesia technique and mortality after total hip or knee arthroplasty: a retrospective. Propensity score-matched cohort study. Anesthesio-logy. 2016;125(4):724-31.
53. Shaker TM, Carroll JT, Chung MH, Koehler TJ, Lane BR, Wolf AM, et al. Efficacy and safety of transversus abdominis plane blocks versus thoracic epidural anesthesia in patients undergoing major abdominal oncologic resections: a prospective, randomized controlled trial. Am J Surg. 2018;215(3):498-501.
54. Sari S, Kumar J, Turan A. New peripheral nerve blocks and local anesthetics. Curr Opin Crit Care. 2021;27(6):732-42.
55. Mudumbai SC, Auyong DB, Memtsoudis SG, Mariano ER. A pragmatic approach
to evaluating new techniques in regional anesthesia and acute pain medicine. Pain Manag. 2018;8(6):475-85.
56. Savard X, Pinard A, Perioperative use of gabapentinoids for the management of pos-toperative acute pain. Anesthesiology. 2020;133(2):265-79.
57. McNicol ED, Ferguson MC, Hudcova J. Patient controlled opioid analgesia versus non-patient controlled opioid analgesia for postoperative pain. Cochrane Database Syst Rev. 2015;(6):CD003348.
58. Morlion B, Schäfer M, Betteridge N, Kalso E, Morlion B, Schäfer M, et al. Non-inva-sive patient-controlled analgesia in the management of acute postoperative pain in the hospital setting. Curr Med Res Opin. 2018;34(7):1179-86.
59. Bai Y, Miller T, Tan M, Law LS, Gan TJ. Lidocaine patch for acute pain management: a meta-analysis of prospective controlled trials. Curr Med Res Opin. 2015;(31):575-81.
60. Farooq F, Khan R, Ahmed A. Assessment of patient satisfaction with acute pain ma-nagement service: Monitoring quality of care in clinical setting. Indian J Anaesth. 2016;(30):248-52.
61. Knezevic NN, Yekkirala A, Yaksh TL. Basic/translational development of forthcoming opioid- and nonopioid-targeted pain therapeutics. Anesth Analg. 2017;125(5):1714-32.
62. Ren C, Tong YL, Li JC, Lu ZQ, Yao YM. The protective effect of alpha 7 nicotinic acetylcholine receptor activation on critical illness and its mechanism. Int J Biol Sci. 2017;13(1):46-56.
63. Gélinas C. Pain assessment in the critically ill adult : recent evidence and new trends. Intensive Crit Care Nurs. 2016;34:1-11.
64. Niculescu AB, Le-Niculescu H, Levey DF, Roseberry K, Soe KC, Rogers J, Jones FK, et al. Towards precision medicine for pain: diagnostic biomarkers and repurposed drugs. Mol Psychiatry. 2019;24(24):501-22.

154
BrJP. São Paulo, 2022 apr-jun;5(2):154-60
ABSTRACT
BACKGROUND AND OBJECTIVES: It is estimated that up to 40% of patients with migraine have at least one episode of major depression during their lifetime. On the other hand, pa-tients with depression are twice as likely to suffer from migraine when compared to the population without the mood disorder. The comorbidity of both conditions increases the frequency of pain crises and the individual’s disability. A therapy that could act on the disorders, when simultaneous, would offer advantages through a broader and more effective action, such as botulinum toxin (BTX). Due to the lack of a clear definition on the subject, the objective of this study was to review how the concomitant treatment with BTX of the two morbidities behaves.CONTENTS: A review of articles in English, Portuguese, and Spanish indexed in Pubmed/Medline, LILACS and Scielo data-bases was carried out. Of the eight articles selected, most indivi-duals were women aged 40 to 50 years. The sample size ranged from 30 to 715 subjects. The predominance was of prospective studies. All studies found a significant reduction in pain. Six stu-dies found a significant decrease in depression. The frequency of adverse effects ranged from 4.1% to 30%, with eyelid ptosis and headache being the most frequent.CONCLUSION: BTX seems to be useful for the treatment of chronic headache and depression. There was a tendency to rela-te the improvement in depression with the decrease in pain. The specific action of the toxin in the treatment of depression was in-conclusive. New studies, with high methodological rigor, as well as systematic reviews, should be carried out to reach a greater depth of comprehension of the subject and to determine the real efficacy of BTX in relieving concomitant headache and depression.Keywords: Depression, Botulinum toxins type A, Disorder hea-dache.
Comorbidity between chronic headache and depression treated with botulinum toxin: literature reviewA comorbidade entre cefaleia crônica e depressão tratada com toxina botulínica: revisão da literatura
Denis Eduardo Bertini Bo1, Eduardo de Melo Carvalho Rocha1
Denis Eduardo Bertini Bo – https://orcid.org/0000-0001-8821-748X;Eduardo de Melo Carvalho Rocha – https://orcid.org/0000-0003-2078-5450. 1. Federal University of São Carlos, Gerontology Department, São Carlos, SP, Brazil.
Submitted on September 27, 2021.Accepted for publication on May 09, 2022.Conflict of interests: none – Sponsoring sources: none.
Correspondence to: Denis Eduardo Bertini Bo E-mail: [email protected]
© Sociedade Brasileira para o Estudo da Dor
RESUMO
JUSTIFICATIVA E OBJETIVOS: Estima-se que até 40% dos pacientes com migrânea apresentam, pelo menos, um episódio de depressão maior ao longo da vida. Por outro lado, pacientes com depressão apresentam duas vezes mais chance de ter migrâ-nea quando comparados à população sem transtorno de humor. A comorbidade dos dois quadros aumenta a frequência das crises de dor e a incapacidade do indivíduo. Uma terapêutica que pu-desse agir nos transtornos, quando simultâneos, ofereceria van-tagens, por uma ação mais ampla e eficaz, a exemplo da toxina botulínica (TXB). Por faltar ainda uma clara definição sobre o tema, o objetivo deste estudo foi revisar como se comporta o tratamento concomitante das duas morbidades com a TXB.CONTEÚDO: Foi realizada revisão de artigos indexados nas bases de dados Pubmed/Medline, LILACS, Scielo nos idiomas inglês, português e espanhol. Dos oito artigos selecionados, a maioria dos indivíduos foram mulheres de 40 a 50 anos. O tama-nho das amostras variou de 30 a 715 pacientes. A predominância foi de estudos prospectivos. Todos os estudos encontraram redu-ção significativa da dor. Seis trabalhos encontraram diminuição significativa da depressão. A frequência dos efeitos adversos va-riou de 4,1% a 30%, sendo ptose palpebral e dor de cabeça os mais frequentes.CONCLUSÃO: A TXB parece ser útil para tratamento da ce-faleia crônica e depressão. Houve uma tendência a relacionar a melhora da depressão com a diminuição da dor. A ação específica da toxina no tratamento da depressão foi inconclusiva. Novos estudos, com alto rigor metodológico, assim como revisões sis-temáticas, devem ser realizados para alcançar maior aprofunda-mento do assunto, a fim de determinar a real eficácia da TXB no alívio da cefaleia e depressão concomitantes.Descritores: Depressão, Toxina botulínica tipo A, Transtornos de enxaqueca
INTRODUCTION
The term cephalalgia encompasses all existing headaches. It is es-timated that more than 90% of the population has some type of headache throughout their lives1. It can be manifested as chronic pain and substantially interfere with quality of life and ability to work2. According to the World Health Organization (WHO)3, headaches are among the 10 most disabling conditions for both genders, although they are among the five worst for women, be-cause they are the most frequently affected by the disorder1.
DOI 10.5935/2595-0118.20220028-en
REVIEW ARTICLE

155
Comorbidity between chronic headache and depression treated with botulinum toxin: literature review
BrJP. São Paulo, 2022 apr-jun;5(2):154-60
Primary headaches are understood as the disease itself, without a clear underlying cause, such as a tumor, infection, or trauma4. Among the primary headaches, the most prevalent are migraine and tension-type headache. In Brazil, the occurrence of migrai-ne is around 15.8%, while tension-type headaches may reach 22.9%. However, migraine causes a strong impact on the indivi-dual’s quality of life, which motivates him/her to seek treatment1.The association between chronic pain and mental disorders, especially depression, has been reported in the literature5,6. In some reviews, the concomitant occurrence between pain and depression ranges between 30% and 60%7,8. In an article analy-zing 1000 patients of a specific health plan, those with at least one pain condition had more depression and anxiety than indi-viduals without pain9. In hospitalized patients, this association becomes even more evident10. In the case of headaches, the strong relationship with depres-sion is also stated by other authors. The two conditions, when concomitant, cause an increase in the frequency of pain crises, as well as a greater patient disability. This connection seems to be bidirectional. It is estimated that up to 40% of patients with migraine have at least one episode of major depression in their lifetime. In addition, migraine patients have a three times higher risk of developing depression than the general population. On the other hand, patients with depression are twice as likely to develop migraine when compared to the population without the mood disorder1,11-15.The present study’s objective was to expose, in some level of de-tail, the pathophysiology of the association between migraine and major depression as an example and as an illustration of how the connection between headaches and psychiatric mood disorders is comprehended. The reasoning being that the mechanisms of the comorbidity between migraine and major depression are clearer.The condition called major depression (whose prevalence in the population may reach 17% throughout life)16 is constituted, ac-cording to the Diagnostic and Statistical Manual of Mental Di-sorders (DSM-5)17, by the following criteria, as shown in table 1.
Table 1. Diagnostic criteria for major depressive episode
At least 5 symptoms, present for at least 2 weeks, on most days:
One symptom must necessarily be:Depressed mood;Marked decrease in interest or pleasure in most or all activities.
Other symptoms:Weight loss unrelated to dieting, significant weight gain, or appe-tite changes;Hypersomnia or insomnia;Psychomotor agitation or depression;Fatigue or feeling of loss of energy;Feeling of worthlessness or excessive or inappropriate guilt;Indecisiveness or difficulty concentrating or reasoning;Recurrent thoughts of death or suicidal ideation (with or without planning).
Symptoms that cause significant impact in various spheres, such as social or work-related.
Symptoms that are not due to substance/drug use or other illness.
Symptoms not explained by schizoaffective or psychotic disorder, and no presence of hypomanic or manic episode.
Source: DSM-517.
Migraine is often accompanied by photophobia and/or vomi-ting; it is very intense, unilateral, and pulsatile. The crisis can last up to 72 hours if not treated properly18.Several elements are involved when it emerges, as well as in its chronification, which are genetic, hormonal, inflammatory, en-vironmental, dietary, related to sleep, psychological, and psychia-tric1,19,20. All these elements, in some way, have an intersection with the mechanisms that generate depression.From the genetic angle, research also reaffirm the strong link bet-ween major depression and migraine. A recent study showed a greater association (by analyzing the whole genome) of migraine with psychiatric disorders when compared to other neurologi-cal disorders21. Both migraine and depression have about 20% of their variability attributed to shared genes, as suggested by a study with twins22,23. In addition, a polymorphism in the seroto-nin transporter gene has been associated with migraine as well as depression24. Alterations through DNA methylation in the cor-ticotropin-releasing factor in the hypothalamic-pituitary-adrenal (HPA) axis points to a hypersensitivity to pain caused by stress25. Psychosocial stress, in turn, is pointed out as an important in-fluencing factor for both depression and migraine26,27.It is known that the reaction to stress, initially, is a healthy res-ponse of the body. Challenging and frightening situations requi-re mobilizing action from human beings. The reaction to stress can provide a more active, vigorous, and productive behavior. However, in excess and/or when it is prolonged, it can cause damage28,29. In moments of threat, the sympathetic autonomic nervous system and the HPA axis are activated, which generates catecholamine release (mainly adrenaline) and cortisol secretion by the adrenal gland. When the stressful situation ceases, these substances return to their initial stage. But if it persists, the stress hormones lead to an overload of the organism with cardiovascular consequences, bone density alteration, weight loss, amenorrhea, and alteration in the regulation of future responses to stress, anxiety, and de-pression30. The modification in the responsiveness of the HPA axis results in a mismatch in cortisol secretion, influencing in-flammatory reactions. Among other consequences, there is an in-crease in cytokines, facilitating the development of autoimmune and inflammatory diseases26 that can develop with pain.The increased activity of the HPA axis can also induce functional changes in neurons and consequent neuronal death, accompa-nied by structural changes in the cerebral cortex, such as atrophy or decrease in its volume. Such a situation can have consequences on behavior, including mood worsening. A significant portion of depressed patients present evident increased activity of the HPA axis: 20% to 40% of those seen in outpatient clinics and 40% to 60% of hospitalized patients16.In fact, from the neurofunctional viewpoint, brain structures are pointed out as acting in common in pain and depression. The anterior cingulate cortex, the thalamus, the amygdala, the peria-queductal gray matter, in addition to areas that initially would not be related to pain processing, such as the parahippocampal and fusiform gyrus, retrosplenal cortex, posterior cingulate cor-tex, and striatum, seem to be involved sometimes in the expe-rience of pain itself; sometimes in its emotional components,

156
BrJP. São Paulo, 2022 apr-jun;5(2):154-60 Bo DE and Rocha EM
contributing to its chronification; and sometimes in the very emergence of the depressive disorder31,32. Furthermore, it must be mentioned that some of these struc-tures, such as the periaqueductal gray matter, together with the hypothalamus, the raphe nuclei, and the locus coeruleus, com-pose a central pain modulation system, of which serotonin and norepinephrine are the main neurotransmitters. This system can inhibit or amplify nociceptive signals from the periphery. Dys-regulation of such neurotransmitters has been used to explain depression and may contribute to the onset of pain/migraine symptoms concomitant with the mental disorder33-35.On the other hand, it is important to remember inflammatory factors already described in the etiology of migraine and de-pression. Not only tissue injury and/or an infection can release pro-inflammatory cytokines. Chronic cortisol dysregulation, for example, can also induce them (as already seen). These cytokines can cross the hematoencephalic barrier and act in the brain36. Observations of the appearance of depressive symptoms in pa-tients treated with cytokines such as interferon have shown the connection between inflammation and depression. Pain is a form of tissue response that promotes defense behavioral reactions. However, when pain becomes chronic, unrelated to tissue injury itself, it becomes a problem. Likewise, when depressive symp-toms persist, despite the absence of a clear cause or grief, they are considered pathological25.A still very controversial aspect of the association between mi-graine and psychiatric/psychological symptoms is the possibility that there are specific personality characteristics of those who suffer from migraine. One of the earliest works in this line37 talks about the “migraine personality”, which would be composed of traits of rigidity, compulsiveness, perfectionism, ambition, com-petitiveness, chronic resentment, and centralization of tasks due to the impossibility of delegating them.Currently, studies suggest that patients with migraine would present traits of the DSM517 avoidant personality disorder. They would be excessively worried, fearful, insecure people, with high sensitivity to stress, and therefore prone to develop anxiety and depression. However, there are still doubts if such traits would be responsible for the association between migraine and depression1.The fact is that the comorbidity between the two conditions, headache (migraine in particular) and depression, is frequent. Therefore, a therapeutic strategy that could act on both disor-ders, when they occur simultaneously, could offer advantages through a broader and more effective action, such as the botuli-num toxin (BTX).BTX is an agent produced from the fermentation of Clostridium botulinum, a gram-positive anaerobic bacteria in spore form, common in soil and in marine environments38. Eight immu-nologically distinct serotypes are identified in its composition. Of these, seven are neurotoxins (A, B, C1, D, E, F, G)39. Their action consists of inhibiting the release of acetylcholine in the synaptic cleft, and BTX-A is the most studied and applied in clinical practice.To exert its effect, BTX, since it has a high affinity for choliner-gic synapses, penetrates the motor neuron that innervates the skeletal muscles. Inside the cytoplasm, it binds specifically to the
SNARE protein complex. Similar to enzymes, the toxin clea-ves the peptide bonds of the SNARE proteins39. As a result, the synaptic vesicle is not anchored to the inner surface of the cell membrane, blocking vesicle fusion, a necessary condition for the release of acetylcholine. Then, a flaccid paralysis in the affected muscle fibers occurs (chemical denervation)40.The action of BTX happens in two to five days on average and can last for up to six months (usually about four months). The restoration of physiology usually happens through two known mechanisms. The first occurs through the formation of new axo-nal sprouts with the formation of new smaller end plates, leading to temporary reinnervation. The second comes from the rege-neration of the SNARE complex proteins, allowing the return of the coupling of acetylcholine vesicles on the inner side of the neuronal membrane41.The contribution of BTX in the treatment of headaches results (although it is not definitively confirmed) from the relaxation of the muscles affected by the substance. A relation with decrease in pressure on the trigeminal nerve roots is also suggested42. And, more recently, there is evidence that the toxin acts on the release of substances and neurotransmitters involved in inflammation and nociception43.In the case of depression, BTX also contributes to the improve-ment of dysphoric symptoms44,45. This action is based on the so--called facial feedback effect. The hypothesis proposes a bidirectio-nal link between the emotion regulatory centers in the brain and the facial muscles46. It seems natural to conclude that our facial expressions are influenced by our emotional state, but the opposite is not so easy to accept. Nevertheless, researchers47-49 have detected that, regardless of the reason, expressing a more serious or smiling face affects our emotions. In the first case, frowning by contrac-ting the corrugator muscles in the glabellar region can lead to a more negativistic view. Otherwise, in the second case, contracting the zygomatic muscles to smile would provide more joy and opti-mism. Therefore, broadly speaking, evidence adds up in affirming a significant effect of facial muscles on mood. Study50 suggests a hypothesis of how this influence would take place, especially for depression. The same mechanism, according to the authors, would explain the antidepressant action of BTX. The activity of the muscles in the eyebrows area would act on the proprioception of the optic branch of the trigeminal nerve. From there, through the mesencephalic trigeminal nucleus, there would be activation of the ventromedial prefrontal cortex and the locus coeruleus, and from the latter to the amygdala (struc-tures important for emotional regulation)51. As BTX is injected into the forehead in the glabellar region, paralyzing the corruga-tor muscle, the proprioceptive signal sent by the optic branch of the trigeminal nerve to the brain would be altered. As a result, there would be a change in mood.The present study’s objective was to observe if the improvement of depressive symptoms would enable pain relief. On the other hand, due to the bidirectional relationship between headache and depression, to observe if the improvement of pain would in-fluence psychiatric symptoms. Some studies evaluate the treat-ment with BTX in patients with both conditions, but there is no clear definition on the subject.
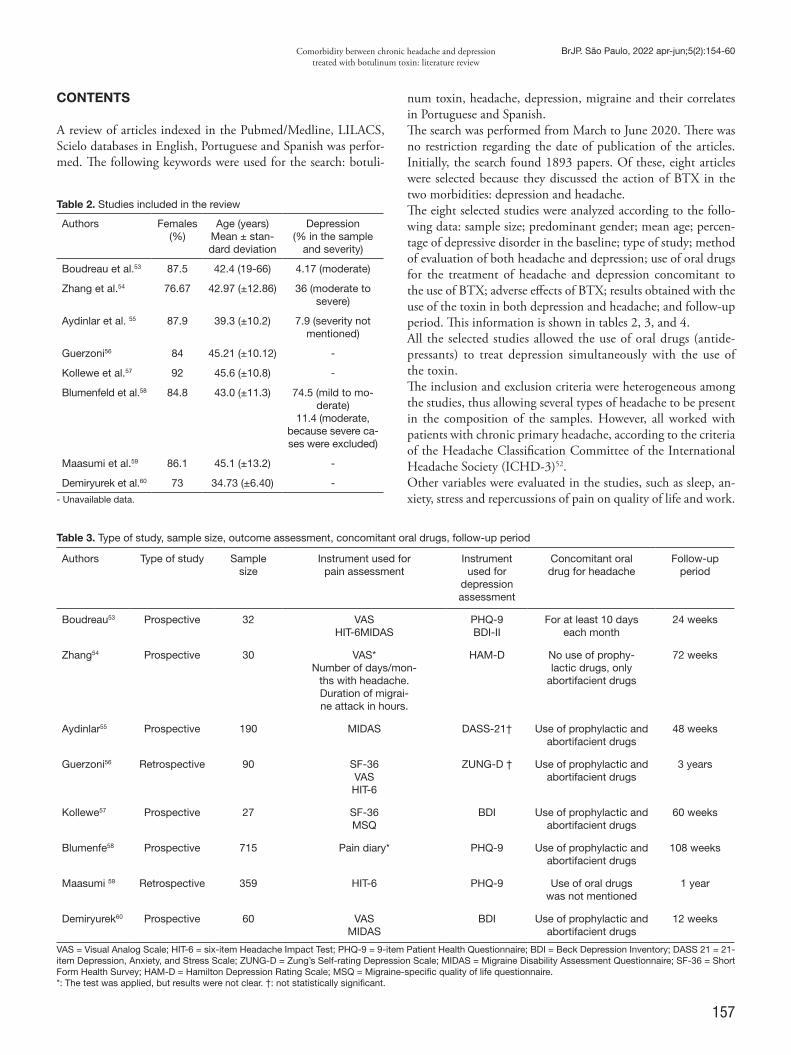
157
Comorbidity between chronic headache and depression treated with botulinum toxin: literature review
BrJP. São Paulo, 2022 apr-jun;5(2):154-60
CONTENTS
A review of articles indexed in the Pubmed/Medline, LILACS, Scielo databases in English, Portuguese and Spanish was perfor-med. The following keywords were used for the search: botuli-
num toxin, headache, depression, migraine and their correlates in Portuguese and Spanish.The search was performed from March to June 2020. There was no restriction regarding the date of publication of the articles. Initially, the search found 1893 papers. Of these, eight articles were selected because they discussed the action of BTX in the two morbidities: depression and headache.The eight selected studies were analyzed according to the follo-wing data: sample size; predominant gender; mean age; percen-tage of depressive disorder in the baseline; type of study; method of evaluation of both headache and depression; use of oral drugs for the treatment of headache and depression concomitant to the use of BTX; adverse effects of BTX; results obtained with the use of the toxin in both depression and headache; and follow-up period. This information is shown in tables 2, 3, and 4.All the selected studies allowed the use of oral drugs (antide-pressants) to treat depression simultaneously with the use of the toxin.The inclusion and exclusion criteria were heterogeneous among the studies, thus allowing several types of headache to be present in the composition of the samples. However, all worked with patients with chronic primary headache, according to the criteria of the Headache Classification Committee of the International Headache Society (ICHD-3)52.Other variables were evaluated in the studies, such as sleep, an-xiety, stress and repercussions of pain on quality of life and work.
Table 2. Studies included in the review
Authors Females (%)
Age (years)Mean ± stan-dard deviation
Depression(% in the sample
and severity)
Boudreau et al.53 87.5 42.4 (19-66) 4.17 (moderate)
Zhang et al.54 76.67 42.97 (±12.86) 36 (moderate to severe)
Aydinlar et al. 55 87.9 39.3 (±10.2) 7.9 (severity not mentioned)
Guerzoni56 84 45.21 (±10.12) -
Kollewe et al.57 92 45.6 (±10.8) -
Blumenfeld et al.58 84.8 43.0 (±11.3) 74.5 (mild to mo-derate)
11.4 (moderate, because severe ca-ses were excluded)
Maasumi et al.59 86.1 45.1 (±13.2) -
Demiryurek et al.60 73 34.73 (±6.40) -
- Unavailable data.
Table 3. Type of study, sample size, outcome assessment, concomitant oral drugs, follow-up period
Authors Type of study Sample size
Instrument used for pain assessment
Instrument used for
depression assessment
Concomitant oral drug for headache
Follow-up period
Boudreau53 Prospective 32 VASHIT-6MIDAS
PHQ-9BDI-II
For at least 10 days each month
24 weeks
Zhang54 Prospective 30 VAS*Number of days/mon-
ths with headache.Duration of migrai-ne attack in hours.
HAM-D No use of prophy-lactic drugs, only
abortifacient drugs
72 weeks
Aydinlar55 Prospective 190 MIDAS DASS-21† Use of prophylactic and abortifacient drugs
48 weeks
Guerzoni56 Retrospective 90 SF-36VASHIT-6
ZUNG-D † Use of prophylactic and abortifacient drugs
3 years
Kollewe57 Prospective 27 SF-36MSQ
BDI Use of prophylactic and abortifacient drugs
60 weeks
Blumenfe58 Prospective 715 Pain diary* PHQ-9 Use of prophylactic and abortifacient drugs
108 weeks
Maasumi 59 Retrospective 359 HIT-6 PHQ-9 Use of oral drugs was not mentioned
1 year
Demiryurek60 Prospective 60 VASMIDAS
BDI Use of prophylactic and abortifacient drugs
12 weeks
VAS = Visual Analog Scale; HIT-6 = six-item Headache Impact Test; PHQ-9 = 9-item Patient Health Questionnaire; BDI = Beck Depression Inventory; DASS 21 = 21-item Depression, Anxiety, and Stress Scale; ZUNG-D = Zung’s Self-rating Depression Scale; MIDAS = Migraine Disability Assessment Questionnaire; SF-36 = Short Form Health Survey; HAM-D = Hamilton Depression Rating Scale; MSQ = Migraine-specific quality of life questionnaire.*: The test was applied, but results were not clear. †: not statistically significant.
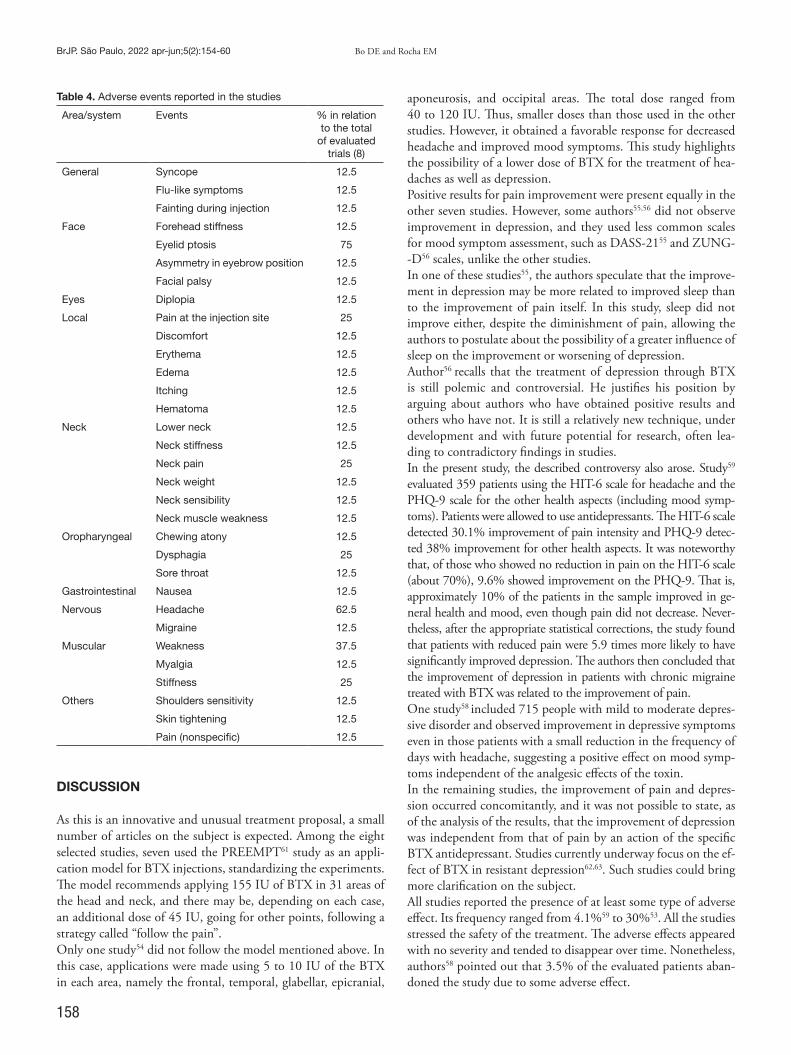
158
BrJP. São Paulo, 2022 apr-jun;5(2):154-60 Bo DE and Rocha EM
DISCUSSION
As this is an innovative and unusual treatment proposal, a small number of articles on the subject is expected. Among the eight selected studies, seven used the PREEMPT61 study as an appli-cation model for BTX injections, standardizing the experiments. The model recommends applying 155 IU of BTX in 31 areas of the head and neck, and there may be, depending on each case, an additional dose of 45 IU, going for other points, following a strategy called “follow the pain”.Only one study54 did not follow the model mentioned above. In this case, applications were made using 5 to 10 IU of the BTX in each area, namely the frontal, temporal, glabellar, epicranial,
aponeurosis, and occipital areas. The total dose ranged from 40 to 120 IU. Thus, smaller doses than those used in the other studies. However, it obtained a favorable response for decreased headache and improved mood symptoms. This study highlights the possibility of a lower dose of BTX for the treatment of hea-daches as well as depression.Positive results for pain improvement were present equally in the other seven studies. However, some authors55,56 did not observe improvement in depression, and they used less common scales for mood symptom assessment, such as DASS-2155 and ZUNG--D56 scales, unlike the other studies.In one of these studies55, the authors speculate that the improve-ment in depression may be more related to improved sleep than to the improvement of pain itself. In this study, sleep did not improve either, despite the diminishment of pain, allowing the authors to postulate about the possibility of a greater influence of sleep on the improvement or worsening of depression.Author56 recalls that the treatment of depression through BTX is still polemic and controversial. He justifies his position by arguing about authors who have obtained positive results and others who have not. It is still a relatively new technique, under development and with future potential for research, often lea-ding to contradictory findings in studies.In the present study, the described controversy also arose. Study59 evaluated 359 patients using the HIT-6 scale for headache and the PHQ-9 scale for the other health aspects (including mood symp-toms). Patients were allowed to use antidepressants. The HIT-6 scale detected 30.1% improvement of pain intensity and PHQ-9 detec-ted 38% improvement for other health aspects. It was noteworthy that, of those who showed no reduction in pain on the HIT-6 scale (about 70%), 9.6% showed improvement on the PHQ-9. That is, approximately 10% of the patients in the sample improved in ge-neral health and mood, even though pain did not decrease. Never-theless, after the appropriate statistical corrections, the study found that patients with reduced pain were 5.9 times more likely to have significantly improved depression. The authors then concluded that the improvement of depression in patients with chronic migraine treated with BTX was related to the improvement of pain.One study58 included 715 people with mild to moderate depres-sive disorder and observed improvement in depressive symptoms even in those patients with a small reduction in the frequency of days with headache, suggesting a positive effect on mood symp-toms independent of the analgesic effects of the toxin.In the remaining studies, the improvement of pain and depres-sion occurred concomitantly, and it was not possible to state, as of the analysis of the results, that the improvement of depression was independent from that of pain by an action of the specific BTX antidepressant. Studies currently underway focus on the ef-fect of BTX in resistant depression62,63. Such studies could bring more clarification on the subject.All studies reported the presence of at least some type of adverse effect. Its frequency ranged from 4.1%59 to 30%53. All the studies stressed the safety of the treatment. The adverse effects appeared with no severity and tended to disappear over time. Nonetheless, authors58 pointed out that 3.5% of the evaluated patients aban-doned the study due to some adverse effect.
Table 4. Adverse events reported in the studies
Area/system Events % in relation to the total
of evaluated trials (8)
General
Syncope 12.5
Flu-like symptoms 12.5
Fainting during injection 12.5
Face Forehead stiffness 12.5
Eyelid ptosis 75
Asymmetry in eyebrow position 12.5
Facial palsy 12.5
Eyes Diplopia 12.5
Local
Pain at the injection site 25
Discomfort 12.5
Erythema 12.5
Edema 12.5
Itching 12.5
Hematoma 12.5
Neck Lower neck 12.5
Neck stiffness 12.5
Neck pain 25
Neck weight 12.5
Neck sensibility 12.5
Neck muscle weakness 12.5
Oropharyngeal Chewing atony 12.5
Dysphagia 25
Sore throat 12.5
Gastrointestinal Nausea 12.5
Nervous Headache 62.5
Migraine 12.5
Muscular Weakness 37.5
Myalgia 12.5
Stiffness 25
Others Shoulders sensitivity 12.5
Skin tightening 12.5
Pain (nonspecific) 12.5

159
Comorbidity between chronic headache and depression treated with botulinum toxin: literature review
BrJP. São Paulo, 2022 apr-jun;5(2):154-60
The limitations were the restricted number of studies (only eight), which restricts the possibility of more robust conclusions with the intent of extending the treatment to clinical practice in general. The analyzed studies used samples with varied inclusion and exclusion criteria, grouping patients with different characte-ristics, making comparisons difficult. It’s important to specially highlight the difficulty of comparing the various types of heada-ches in the different samples, in addition to the varied severity of symptoms in relation to headache and depression. The use of a drug concomitant to the treatment with BTX should also be remembered because this practice can influence the result, since, initially, it adds its effects to those of the toxin evaluated. Only one study53 limited the use of analgesic drugs. No studies used control or placebo groups, thus exposing an extremely im-portant methodological bias. This bias prevents the elucidation of doubts about the phenomenon of spontaneous improvement and/or improvement caused by the action of some other element other than the specific drug (the toxin, in this case). However, for the present study, an integrative review, there was no concern to deepen the analysis of the quality of evidence.On the other hand, there was almost total consensus in the man-ner of using the toxin, i.e., as described above, seven studies used the PREEMPT protocol as a model for toxin application, con-tributing to the comparative analysis. Finally, there is a language limitation, as the search focused on articles in English, Portugue-se, and Spanish.
CONCLUSION
BTX seems to be useful for treating chronic headache and depres-sion. However, there was a tendency to relate the improvement of depression with the decrease in pain. The specific action of the toxin in the treatment of depression was inconclusive. Due to the apparent positive potential, new clinical trial-type studies with high methodological rigor and systematic reviews should be carried out to determine the real efficacy of the treatment of BTX in the comor-bidity between headache and depression. This study hopes, within its limitations, to have contributed to the elucidation of the subject.
AUTHORS’ CONTRIBUTIONS
Denis Eduardo Bertini Bo Data Collection, Writing - Preparation of the original Eduardo de Melo Carvalho RochaWriting - Review and Editing, Supervision
REFERENCES
1. Teixeira AL, Gomez RS. Cefaleias na prática clínica. Belo Horizonte: Folium; 2017.2. Zukerman E. Cefaleia e qualidade de vida. Einstein. 2004;2(Suppl 1):S73-5.3. Organização Mundial da Saúde (OMS). Relatório sobre a saúde no mundo. Saúde men-
tal: nova concepção, nova esperança. Genebra: World Health Organization, 2001.4. Krymchantowski, AV. Condutas em cefaleias. São Paulo: Wolters Kluwer Health;
2008.5. Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison
of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther. 1995;33(3):335-43.
6. Krishnan RRK. France RD, Pelton S, McCann UD, Davidson J, Urban BJ. Chronic pain and depression. II. Symptoms of anxiety in chronic low back pain patients and
their relationship to subtypes of depression. Pain. 1985;22(3):289-94.7. Bair MJ, Robinson RL, Katon W, Kroenke K. Depression and pain comorbidity: a
literature review. Arch Intern Med. 2003;163(20):2433-45.8. Gallagher RM, Verma S. Managing pain and comorbid depression: a public health
challenge. Semin Clin Neuropsychiatry. 1999;4(3):203-20.9. Fields HL. Pain modulation: expectation, opioid analgesia and virtual pain. Prog
Brain Res. 2000;122:245-53.10. Levenson JL, Hamer R, Silverman JJ, Rossiter LF. Psychopathology in medical inpa-
tients and its relationship to length of hospital stay: a pilot study. Int J Psychiatry Med. 1986-1987:16(3):231-6.
11. Merikangas KR, Stevens DE, Angst J. Psychopathology and headache syndromes in the community. Headache. 1994;34(8):S17-S22.
12. Mercante JP, Peres MF, Guendler V, Zukerman E, Bernik MA. Depression in chronic migraine: severity and clinical features. Arq Neuropsiquiatr. 2005;63(2A):217-20.
13. McLean G, Mercer SW. Chronic migraine, comorbidity, and socioeconomic depriva-tion: cross-sectional analysis of a large nationally representative primary care database. J Comorb. 2017;7(1):89-95.
14. Moschiano F, D’Amico D, Canavero I, Pan I, Micieli G, Bussone G. Migraine and de-pression: common pathogenetic and therapeutic ground? Neurol Sci. 2011;32(Suppl 1):S85-8.
15. Breslau N, Davis GC, Schultz LR, Peterson EL. Joint 1994 Wolff Award Presentation. Migraine and major depression: a longitudinal study. Headache. 1994;34(7):387-93.
16. Sadock B, Sadock VA, Ruiz P. Compêndio de psiquiatria: ciência do comportamento e psiquiatria clínica. 11ª ed. Porto Alegre: Artmed; 2017.
17. DSM-5/American Psychiatric Association. Manual diagnóstico e estatístico de trans-tornos mentais. 5ª ed. Porto Alegre: Artmed; 2014.
18. Martins NM, Oliveira OWB, Dutra LQ, Rezende AQM, Dantas EF, Pereira ABC. Migrânea com aura, qualidade de vida e tratamento: um relato de caso. Rev Saúde. 2010;1(1):15-24.
19. Natoli JL, Manack A, Dean B, Butler Q, Turkel CC, Stovner L, Lipton RB. Global prevalence of chronic migraine: a systematic review. Cephalalgia. 2010;30(5):599-609.
20. Buse DC, Silberstein SD, Manack AN, Papapetropoulos S, Lipton RB. Psychiatric comorbidities of episodic and chronic migraine. J Neurol. 2013;260(8):1960-9.
21. Antilla V, Bulik-Sullivan B, Finucane HK, Walters RK, Bras J, Duncan L, Escott-Price V, et al. Analysis of shared heritability in common disorders of the brain. Science. 2018;360(6395):eaapp8757.
22. Ligthart L, Nyholt DR, Penninx BW, Boomsma DI. The shared genetics of migraine and anxious depression. Headache. 2010;50(10):1549-60.
23. Schur EA, Noonan C, Buchwald D, Goldberg J, Afari N. A twin study of de-pression and migraine: evidence for a shared genetic vulnerability. Headache. 2009;49(10):1493-502.
24. Marino E, Fanny B, Lorenzi C, Pirovano A, Franchini L, Colombo C, et al. Genetic bases of comorbidity between mood disorders and migraine: possible role of serotonin transporter gene. Neurol Sci. 2010;31(3):387-91.
25. Duailibi K. Depressão e seus impactos. São Paulo: Editora Omnifarma; 2018.26. Tsuji SR, Carvalho SD. Aspectos psíquicos das cefaleias primárias. Rev Neuroci.
2002;10(3):129-36.27. Haque B, Rahman KM, Hoque A, Hasan AT, Chowdhury RN, Khan SU, et al. Preci-
pitating and relieving factors of migraine versus tension type headache. BMC Neurol. 2012;12:82.
28. Lipp M, Malagris L. O stress emocional e seu tratamento. Terapias cogntivo-compor-tamentais: um diálogo com a psiquiatra. São Paulo: Artmed; 2001. 475-89p.
29. Ebrecht M, Hextall J, Kirtley LG, Taylor A, Dyson M, Weinman J. Perceived stress and cortisol levels predict speed of wound healing in healthy male adults. Psychoneu-roendocrinology. 2004;29(6):798-809.
30. McEwen BS. Protective and damaging effects of stress mediators. N Engl J Med. 1998;338(3):171-9.
31. Doan L, Manders T, Wang J. Neuroplasticity underlying the comorbidity of pain and depression. Neural Plast. 2015;2015:504691.
32. Maizels M, Aurora S, Heinricher M. Beyond neurovascular: migraine as a dysfunctio-nal neurolimbic pain network. Headache. 2012;52(10):1553-65.
33. Lynch ME. Antidepressants as analgesics: a review of randomized controlled trials. J Psychiatry Neurosci. 2001;26(1):30-6.
34. Von Korff M, Dworkin SF, Le Resche L, Kruger A. An epidemiologic comparison of pain complaints. Pain. 1988;32(2):173-83.
35. Wise TN, Fishbain DA, Holder-Perkins V. Sintomas físicos dolorosos na depressão: um desafio clínico. Pain Med. 2007;8(S2):S75-S76.
36. Walter AK, Kavelaars A, Heijnen CJ, Dantzer R. Neuroinflammation and comorbi-dity of pain and depression. Pharmacol Rev. 2013;66(1):80-101.
37. Wolff HG. Personality features and reactions of subjects with migraine. Arch Neurol Psychiatry. 1937;37(4):895-921.
38. Wenzel RG. Pharmacology of botulinum neurotoxin serotype A. Am J Health Syst Pharm. 2004;61(22 Suppl 6):S5-S10.
39. Setler PE. Therapeutic use of botulinum toxins: background and history. Clin J Pain. 2002;18(6):S119-24.
40. Dressler D, Saberi FA. Botulinum toxin: mechanisms of action. Eur Neurol. 2005;53(1):3-9.
41. Cardoso F. Toxina botulínica tipo B no manejo de distonia não-responsiva a toxina botulínica tipo A. Arq Neuropsiquiatr. 2003;61(3A):607-10.
42. Smuts JA, Schultz DB, Barnard A. Mechanism of action of botulinum toxin type A in
160
BrJP. São Paulo, 2022 apr-jun;5(2):154-60 Bo DE and Rocha EM
migraine prevention: a pilot study. Headache. 2004;44(8):801-5.43. de Mello Sposito MM. Toxina botulínica do tipo A: mecanismo de ação. Acta Fisiátri-
ca. 2009;16(1):25-37.44. Finzi E, Wasserman E. Treatment of depression with botulinum toxin A: a case series.
Dermatol Surg. 2006;32(5):645-50.45. Wollmer MA, de Boer C, Kalak N, Beck J, Götz T, Schmidt T, et al. Facing depression
with botulinum toxin: a randomized controlled trial. J Psychiatr Res. 2012;46(5):574-81.46. Niedenthal P M. Embodying emotion. Science. 2007;316(5827):1002-5.47. Larsen RJ, Kasimatis M, Frey K. Facilitating the furrowed brow: an unobtrusi-
ve test of the facial feedback hypothesis applied to unpleasant affect. Cogn Emot. 1992;6(5):321-38.
48. Ekman P, Levenson RW, Friesen WV. Autonomic nervous system activity distingui-shes among emotions. Science. 1983;221(4616):1208-10.
49. Strack F, Martin LL, Stepper S. Inhibiting and facilitating conditions of the hu-man smile: a nonobtrusive test of the facial feedback hypothesis. J Pers Soc Psychol. 1988;54(5):768-77.
50. Finzi E, Rosenthal NE. Emotional proprioception: treatment of depression with affe-rent facial feedback. J Psychiatr Res. 2016;80:93-6.
51. Matsuo K. Ban R, Hama Y, Yuziriha S. Eyelid opening with trigeminal proprioceptive activation regulates a brainstem arousal mechanism. PLoS One, 2015;10(8):e0134659.
52. Headache Classification Committee of the International Headache Society – IHS. Classificação internacional de cefaleias. 3rd ed. (ICHD). Sinapse. 2018;18(2):1-170.
53. Boudreau GP, Grosberg BM, McAllister PJ, Lipton RB, Buse DC. Prophylactic on a botulinumtoxin A in patients with chronic migraine and comorbid depression: an open-label, multicenter, pilot study of efficacy, safety and effect on headache-related disability, depression, and anxiety. Int J Gen Med. 2015;8:79-86.
54. Zhang H, Zhang H, Wei Y, Lian Y, Chen Y, Zheng Y. Treatment of chronic daily hea-dache with comorbid anxiety and depression using botulinum toxin A: a prospective pilot study. Int J Neurosci. 2017;127(4):285-90.
55. Aydinlar EI. Dikmen PY, Kosak S, Kocaman AS. On a botulinumtoxin A effectiveness on chronic migraine, negative emotional states and sleep quality: a single-center pros-
pective cohort study. J Headache Pain. 2017;18(1):1-10.56. Guerzoni S, Pellesi L, Baraldi C, Cainazzo MM, Negro A, Martelletti P, et al. Long-
-term treatment benefits and prolonged efficacy of on a botulinum toxin A in patients affected by chronic migraine and medication overuse headache over 3 years of therapy. Front Neurol. 2017;8:586.
57. Kollewe K, Escher CM, Wulff DU, Fathi D, Paracka L, Mohammadi B, et al. Long--term treatment of chronic migraine with on a botulinum toxin A: efficacy, quality of life and tolerability in a real-life setting. J Neural Transm. 2016;123(5):533-40.
58. Blumenfeld AM, Tepper SJ, Robbins LD, Manack Adams A, Buse DC, Orejudos A, et al. Effects of on a botulinum toxin A treatment for chronic migraine on com-mon comorbidities including depression and anxiety. J Neurol Neurosurg Psychiatry. 2019;90(3):353-60.
59. Maasumi K, Thompson NR, Kriegler JS, Tepper SJ. Effect of on a botulinum toxin A injection on depression in chronic migraine. Headache. 2015;59(9):1218-24.
60. Demiryurek BE, Erten DH, Tekin A, Ceylan M, Aras YG, Gungen BD. Effects of onabotulinumtoxinA treatment on efficacy, depression, anxiety, and disability in Tur-kish patients with chronic migraine. Neurol Sci. 2016;37(11):1779-84.
61. Dodick DW, Turkel CC, DeGryse RE, Aurora SK, Silverstein SD, Lipton RB, et al. OnabotulinumtoxinA for treatment of chronic migraine: pooled results from the dou-ble‐blind, randomized, placebo‐controlled phases of the PREEMPT clinical program. Headache. 2010;50(6);921-36.
62. Charles E. Infiltrations of on a botulinum toxin in resistant depression: comparison of two facial injection sites. Clinicaltrials.gov: NCT03484754. Última atualização pos-tada: 5 de out de 2021. Diponível em: <https://www.clinicaltrials.gov/ct2/resultis?-cond=Depression&term=BOTULINUMTOXIN&cntry=&state=&city=&dist=>. Acesso em 10 de jan 2021.
63. Helse Stavanger HF. Glabellar botulinum toxin injections for the treatment of ge-riatric depression. Clinicaltrials.gov:NCT03833063. Última atualização postada: 11 de ago de 2021. Disponível em:<https://clinicaltrials-gov.translate.goog/ct2/show/NCT03833063?term=botulinum+toxin&cond=Depression&draw=2&rank=2&_x_tr_sl=auto&_x_tr_tl=pt&_x_tr_hl=pt>. Acesso em 10 de jan 2021.

161
ABSTRACT
BACKGROUND AND OBJECTIVES: Neuromuscular elec-trical stimulation (NMES) is one of the resources that can be used in the treatment of patients with chronic low back pain. It is possible that issues related to the stimulation parameters may affect the results obtained with the use of these currents. Therefo-re, the aim of this review was to investigate the effects of NMES on aspects of lumbopelvic muscle function in individuals with chronic low back pain. CONTENTS: The study is a systematic review that used 10 da-tabases for the search through a comprehensive combination of descriptors that met the research question. The selection crite-ria based on the PICOT strategy were population - individuals with chronic low back pain (specific and/or non-specific); inter-vention - NMES; outcomes - paravertebral and/or abdominal muscle changes (muscle power and endurance). The articles were selected by two independent reviewers, who developed the tools for data extraction. Four articles were included in this review. In three of them, there was a significant increase in muscle stren-gth and endurance, as well as muscle cross-sectional area in the group that received NMES compared to the control group. CONCLUSION: NMES showed positive effects in optimizing aspects of muscle function in individuals with chronic low back pain. However, the methods employed are very heterogeneous, which made it impossible to perform a quantitative analysis.Keywords: Electric stimulation therapy, Low back pain, Skeletal muscle.
Effect of neuromuscular electrical stimulation on muscle function in chronic low back pain patients: systematic reviewEfeito da estimulação elétrica neuromuscular na função muscular em pacientes com dor lombar crônica: revisão sistemática
Alessandra Linzmeyer1, Camila Amaral Coracini1, Gladson Ricardo Flor Bertolini1, Alberito Rodrigo Carvalho1
Alessandra Linzmeyer – https://orcid.org/0000-0002-4730-9473;Camila Amaral Coracini – https://orcid.org/0000-0003-2036-156X;Gladson Ricardo Flor Bertolini – https://orcid.org/0000-0003-0565-2019;Alberito Rodrigo Carvalho – https://orcid.org/0000-0002-5520-441X.
1. State University of East Paraná, Biosciences and Health Program, Cascavel, PR, Brazil.
Submitted on December 09, 2021.Accepted for publication on April 12, 2022. Conflict of interests: none – Sponsoring sources: none.
Correspondence to: Gladson Ricardo Flor BertoliniE-mail: [email protected] [email protected]
© Sociedade Brasileira para o Estudo da Dor
RESUMO
JUSTIFICATIVA E OBJETIVOS: A estimulação elétrica neu-romuscular (EENM) é um dos recursos que podem ser utilizados no tratamento de pacientes com dor lombar crônica. É possível que questões relacionadas aos parâmetros de estimulação possam afetar os resultados obtidos com o uso dessas correntes. Portanto, o objetivo deste estudo foi investigar os efeitos da EENM em aspectos da função muscular da região lombopélvica em indiví-duos com dor lombar crônica. CONTEÚDO: Trata-se de uma revisão sistemática que utilizou 10 bases de dados para a busca por meio da combinação abran-gente de descritores que atendessem a pergunta da investigação. Os critérios de seleção com base na estratégia PICOT foram: população - indivíduos com dor lombar crônica (específica e/ou não específica); intervenção - EENM; desfechos – alterações musculares de paravertebrais e/ou abdominais (potência e resis-tência muscular). A seleção dos artigos foi feita por dois reviso-res independentes que elaboraram as ferramentas para extração dos dados. Ao todo, quatro artigos foram incluídos nesta revisão. Em três deles, houve aumento significativo de força e resistência muscular, assim como da área de secção transversa muscular no grupo que recebeu EENM, em relação ao controle. CONCLUSÃO: A EENM apresentou efeitos positivos na otimi-zação dos aspectos da função muscular em indivíduos com dor lombar crônica. Porém, os métodos empregados são muito hete-rogêneos, o que impossibilitou a realização da análise quantitativa.Descritores: Dor lombar, Musculoesquelético, Terapia por esti-mulação elétrica.
INTRODUCTION
Chronic low back pain (CLBP) is characterized by functional loss, pain or discomfort located in the area below the last rib and above the iliac crest in the lumbosacral region lasting for three months or longer1,2. In the urban area of São Paulo, a prevalence of individuals with low back pain (LBP) of 48.1%3 was observed and the prevalence of chronic pain in Brazil was indicated at 45.59%, ranging from 23.02 to 76.17%4. CLBP is considered one of the greatest causes of limitations and absence from work activities, making it not only a disease of great clinical relevance, but also economic5. Since it is a multifactorial condition, more than 85% of cases have no specific cause1,6. Its treatment is of-ten multidisciplinary, involving a combination of therapies such as pharmacotherapy and physical therapy, as well as physical
BrJP. São Paulo, 2022 apr-jun;5(2):161-7
DOI 10.5935/2595-0118.20220025-en
REVIEW ARTICLE

162
BrJP. São Paulo, 2022 apr-jun;5(2):161-7 Linzmeyer A, Coracini CA, Bertolini GR and Carvalho AR
exercises to increase power and endurance of the trunk muscles, aerobic and aquatic exercises to increase mobility and control movements, among others7,8. Currently, there is evidence of the occurrence of fat infiltration and uni or bilateral atrophy of the multifidus in individuals with CLBP, the mechanism that would lead to this may be related to a scenario of arthrogenic muscle inhibition and its occurrence seems to be proportional to the duration of symptoms, but diffi-cult to reverse9. A decrease in the activation of the multifidus and transversus abdominis has also been observed in CLBP, a disor-der that determines loss of lumbar spine support, increased stress and load on joints and ligaments located in the lumbar region10. Systematic reviews suggest that interventions that promote co--contraction of the transverse abdominis and multifidus muscles are effective in both improving function and relieving symptoms related to CLBP, which may be a local mechanical phenomenon or through central analgesia pathways11,12. Studies support the use of endurance training and muscle stabilization for reducing the pain levels of these patients7,13.One form of muscle training that promotes strength increase is neuromuscular electrical stimulation (NMES), which consists of an external application of an electrical current that excites the nerve and causes involuntary muscle contraction2. NMES is often used in cases of osteomuscular system injuries or post--surgery, and it can also be an important tool in the treatment of patients with CLBP. However, because the current can be un-comfortable, it is often adjusted according to the patient’s tole-rance, which does not necessarily reflect the intensity required to produce contraction and, consequently, muscle gains14.In traditional exercise training, the external load (defined as the overload imposed by the ratio between the intensity and volu-me of the stimulus) is a determining parameter for the genera-tion of muscle adaptation15. Taking into account the functional and histomorphological characteristics of lumbopelvic stabilizer muscles related to strength endurance, the dosimetric parameters should respect the principle of training specificity in order to induce muscle benefits. Despite not presenting an advantage in strength gain when compared to voluntary exercise16, NMES is useful in early rehabilitation phases or in individuals with seve-re motor disabilities17,18. Thus, it is important to analyze in the literature the effects of NMES use in patients with CLBP and its standardization in order to ensure its effects on muscle stren-gth. Therefore, the present study’s objective was to investigate the NMES parameters in the optimization of muscle function aspects of the lumbopelvic region in patients with CLBP.
CONTENTS
A systematic review based on the PRISMA statute, which used the following databases: Pubmed, CINAHL, Cochrane, Embase, Scopus, Web of Science, Livivo, LILACS, PsycINFO, and Goo-gle Scholar. The electronic search occurred between June and July 2021 and made use of the following descriptors: “Chronic low back pain”, “Neuromuscular electrical stimulation”, “Core stabili-zation” and “Muscle strength” plus the Boolean operators (“AND” and “OR”); the same terms were also used in Portuguese and Spa-
nish. The terms were searched in the titles and abstracts of the ar-ticles. Studies published in English, Portuguese, and Spanish were considered without restriction as to year of publication. In order to formulate the selection criteria, the PICO strategy was used. Therefore, to be included in this review, the studies should have: used as samples individuals with CLBP (for at least 3 months, regardless of being specific or not) of any age or gen-der; used NMES as intervention; evaluated muscle outcomes of paravertebral and/or abdominal function, both power and en-durance; and presented comparison with some kind of control group (no therapy or placebo) or alternative therapy. The follo-wing were excluded: studies that evaluated acute LBP, experi-mental studies, cross-sectional studies, studies without a control group, observational studies, book chapters, randomized clinical trial records, and studies that did not evaluate muscle outcomes or that provided incomplete data.A reference management software (EndNote Web®, Thomson Reuters), which allowed the initial exclusion of duplicate refe-rences, was used for the selection of studies and collection of results. Next, they were imported into Rayyan QCRI® (Qatar Computing Research Institute), which was used to double--check references and perform the study analysis process. Two independent reviewers performed an exploratory reading of all titles and abstracts to see if they met the research criteria. In the next step, the selected articles were read in full and ranked again. Divergences between reviewers were resolved by a third reviewer. Finally, the included studies had the information extracted in tables prepared by the researchers themselves in order to sort and summarize the information. The data collected were: country; characteristics and sample quantitative; interventions; compara-tive group(s); variables related to strength (endurance or power); dosimetry relative to the current; number of sessions, sets, and contractions; analyzed muscle outcomes; and results. In order to calculate the external load through the NMES, the load control calculations used in weight training were adapted. For this, the terminology already proposed was used15,19, in whi-ch the load volume (LV) is the product of the intensity multi-plied by the number of repetitions (the NMES intensity here would replace the endurance mass); the total of repetitions (TR) is the product of the number of sets multiplied by the number of repetitions (repetitions = number of contractions); and the stimulation intensity (SI) would be calculated by the result of the load volume divided by the number of repetitions. The sti-mulation density (SD) was obtained by the result of the volume divided by the stimulation duration.LV = intensity * number of repetitionsTR = number of sets * number of repetitionsSI = LV / number of repetitionsDE = LV / stimulation durationThe ROB2® instrument was used to analyze the risk of bias, in which five dimensions were analyzed (randomization process, deviations from planned interventions, missing outcome data, outcome measures, and selection of reported outcomes), and the scoring in the system is generated as: low risk, some concerns, and high risk, thus automatically presented for the dimensions and as an overall result.
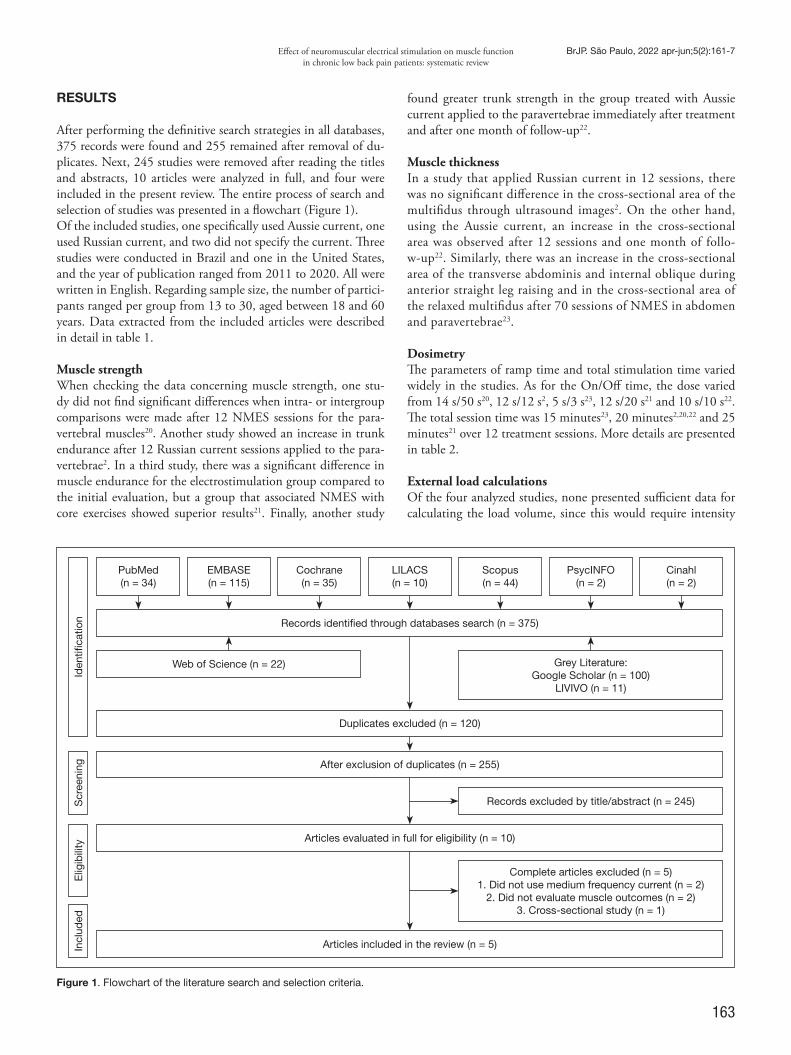
163
Effect of neuromuscular electrical stimulation on muscle function in chronic low back pain patients: systematic review
BrJP. São Paulo, 2022 apr-jun;5(2):161-7
Figure 1. Flowchart of the literature search and selection criteria.
RESULTS
After performing the definitive search strategies in all databases, 375 records were found and 255 remained after removal of du-plicates. Next, 245 studies were removed after reading the titles and abstracts, 10 articles were analyzed in full, and four were included in the present review. The entire process of search and selection of studies was presented in a flowchart (Figure 1). Of the included studies, one specifically used Aussie current, one used Russian current, and two did not specify the current. Three studies were conducted in Brazil and one in the United States, and the year of publication ranged from 2011 to 2020. All were written in English. Regarding sample size, the number of partici-pants ranged per group from 13 to 30, aged between 18 and 60 years. Data extracted from the included articles were described in detail in table 1.
Muscle strengthWhen checking the data concerning muscle strength, one stu-dy did not find significant differences when intra- or intergroup comparisons were made after 12 NMES sessions for the para-vertebral muscles20. Another study showed an increase in trunk endurance after 12 Russian current sessions applied to the para-vertebrae2. In a third study, there was a significant difference in muscle endurance for the electrostimulation group compared to the initial evaluation, but a group that associated NMES with core exercises showed superior results21. Finally, another study
found greater trunk strength in the group treated with Aussie current applied to the paravertebrae immediately after treatment and after one month of follow-up22.
Muscle thickness In a study that applied Russian current in 12 sessions, there was no significant difference in the cross-sectional area of the multifidus through ultrasound images2. On the other hand, using the Aussie current, an increase in the cross-sectional area was observed after 12 sessions and one month of follo-w-up22. Similarly, there was an increase in the cross-sectional area of the transverse abdominis and internal oblique during anterior straight leg raising and in the cross-sectional area of the relaxed multifidus after 70 sessions of NMES in abdomen and paravertebrae23.
Dosimetry The parameters of ramp time and total stimulation time varied widely in the studies. As for the On/Off time, the dose varied from 14 s/50 s20, 12 s/12 s2, 5 s/3 s23, 12 s/20 s21 and 10 s/10 s22. The total session time was 15 minutes23, 20 minutes2,20,22 and 25 minutes21 over 12 treatment sessions. More details are presented in table 2.
External load calculationsOf the four analyzed studies, none presented sufficient data for calculating the load volume, since this would require intensity
Incl
uded
Elig
ibili
tyS
cree
ning
Iden
tifica
tion
PubMed (n = 34)
Web of Science (n = 22)
Records identified through databases search (n = 375)
Duplicates excluded (n = 120)
After exclusion of duplicates (n = 255)
Articles evaluated in full for eligibility (n = 10)
Articles included in the review (n = 5)
EMBASE (n = 115)
Cochrane (n = 35)
LILACS (n = 10)
Scopus (n = 44)
PsycINFO (n = 2)
Cinahl (n = 2)
Grey Literature:Google Scholar (n = 100)
LIVIVO (n = 11)
Records excluded by title/abstract (n = 245)
Complete articles excluded (n = 5)1. Did not use medium frequency current (n = 2)
2. Did not evaluate muscle outcomes (n = 2)3. Cross-sectional study (n = 1)
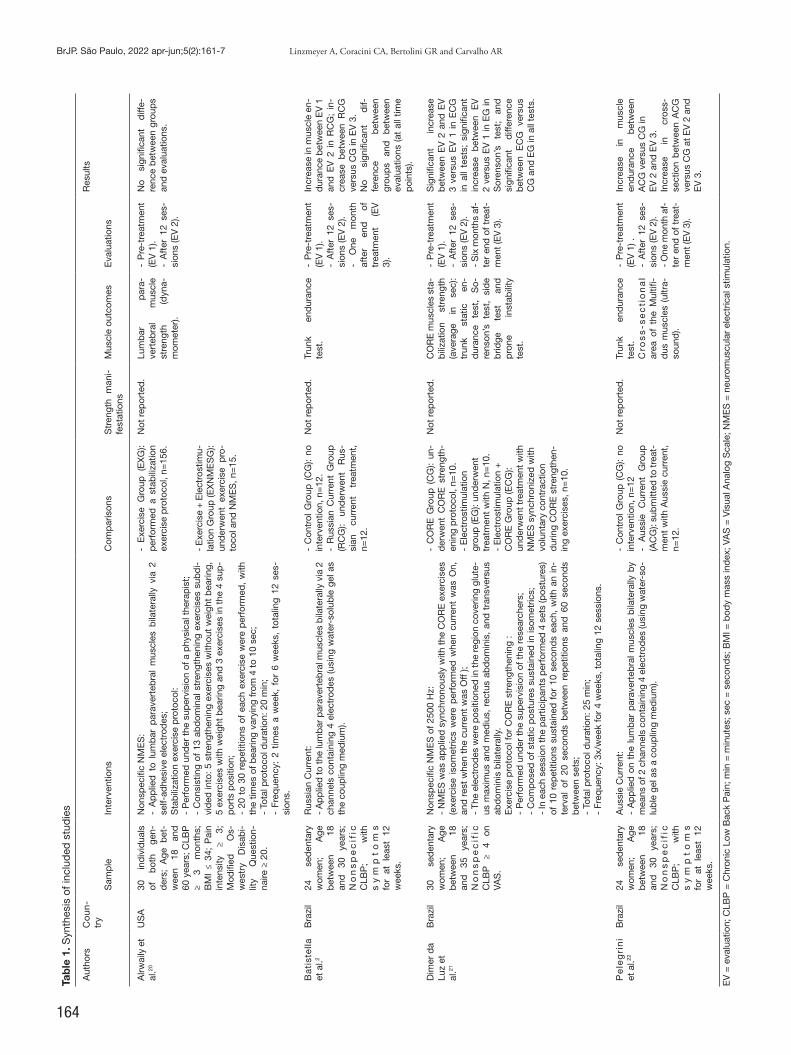
164
BrJP. São Paulo, 2022 apr-jun;5(2):161-7 Linzmeyer A, Coracini CA, Bertolini GR and Carvalho ARTa
ble
1. S
ynth
esis
of i
nclu
ded
stu
die
s
Aut
hors
C
oun
-tr
yR
esul
ts
Sam
ple
Inte
rven
tions
Com
par
ison
sS
tren
gth
man
i-fe
stat
ions
Mus
cle
outc
omes
Eva
luat
ions
Alrw
aily
et
al.20
US
A30
in
div
idua
ls
of
bot
h ge
n-d
ers;
Age
bet
-w
een
18
and
60
yea
rs; C
LBP
≥
3 m
onth
s;
BM
I ≤
34;
Pai
n in
tens
ity
≥ 3;
M
odifi
ed
Os-
wes
try
Dis
abi-
lity
Que
stio
n-na
ire ≥
20.
Non
spec
ific
NM
ES
:-
Ap
plie
d t
o lu
mb
ar p
arav
erte
bra
l m
uscl
es b
ilate
rally
via
2
self-
adhe
sive
ele
ctro
des
;S
tab
iliza
tion
exer
cise
pro
toco
l:-
Per
form
ed u
nder
the
sup
ervi
sion
of a
phy
sica
l the
rap
ist;
- C
onsi
stin
g of
13
abd
omin
al s
tren
gthe
ning
exe
rcis
es s
ubd
i-vi
ded
into
: 5 s
tren
gthe
ning
exe
rcis
es w
ithou
t w
eigh
t b
earin
g,
5 ex
erci
ses
with
wei
ght
bea
ring
and
3 e
xerc
ises
in t
he 4
sup
-p
orts
pos
ition
;-
20 t
o 30
rep
etiti
ons
of e
ach
exer
cise
wer
e p
erfo
rmed
, w
ith
the
times
of b
earin
g va
ryin
g fr
om 4
to
10 s
ec;
- To
tal p
roto
col d
urat
ion:
20
min
;-
Freq
uenc
y: 2
tim
es a
wee
k, f
or 6
wee
ks,
tota
ling
12 s
es-
sion
s.
- E
xerc
ise
Gro
up (
EX
G):
per
form
ed a
sta
bili
zatio
n ex
erci
se p
roto
col,
n=15
6.
- E
xerc
ise
+ E
lect
rost
imu-
latio
n G
roup
(EX
NM
ES
G):
und
erw
ent
exer
cise
pro
-to
col a
nd N
ME
S, n
=15
.
Not
rep
orte
d.
Lum
bar
p
ara-
vert
ebra
l m
uscl
e st
reng
th
(dyn
a-m
omet
er).
- P
re-t
reat
men
t (E
V 1
).-
Aft
er 1
2 se
s-si
ons
(EV
2).
No
sign
ifica
nt
diff
e-re
nce
bet
wee
n gr
oup
s an
d e
valu
atio
ns.
Ba
tist
ella
et
al.2
Bra
zil
24
sed
enta
ry
wom
en;
Age
b
etw
een
18
and
30
ye
ars;
N
on
sp
ec
ific
C
LBP
; w
ith
sy
mp
to
ms
for
at l
east
12
wee
ks.
Rus
sian
Cur
rent
:-
Ap
plie
d to
the
lum
bar
par
aver
teb
ral m
uscl
es b
ilate
rally
via
2
chan
nels
con
tain
ing
4 el
ectr
odes
(usi
ng w
ater
-sol
uble
gel
as
the
coup
ling
med
ium
).
- C
ontr
ol G
roup
(C
G):
no
inte
rven
tion,
n=
12.
- R
ussi
an C
urre
nt G
roup
(R
CG
): un
der
wen
t R
us-
sian
cu
rren
t tr
eatm
ent,
n=
12.
Not
rep
orte
d.
Trun
k en
dur
ance
te
st.
- P
re-t
reat
men
t (E
V 1
).-
Aft
er 1
2 se
s-si
ons
(EV
2).
- O
ne
mon
th
afte
r en
d
of
trea
tmen
t (E
V
3).
Incr
ease
in m
uscl
e en
-d
uran
ce b
etw
een
EV
1
and
EV
2 i
n R
CG
; in
-cr
ease
bet
wee
n R
CG
ve
rsus
CG
in E
V 3
.N
o si
gnifi
cant
d
if-fe
renc
e b
etw
een
grou
ps
and
b
etw
een
eval
uatio
ns (a
t al
l tim
e p
oint
s).
Dim
er d
a Lu
z et
al
.21
Bra
zil
30
sed
enta
ry
wom
en;
Age
b
etw
een
18
and
35
ye
ars;
N
on
sp
ec
ific
C
LBP
≥
4 on
VA
S.
Non
spec
ific
NM
ES
of 2
500
Hz:
- N
ME
S w
as a
pp
lied
syn
chro
nous
ly w
ith t
he C
OR
E e
xerc
ises
(e
xerc
ise
isom
etric
s w
ere
per
form
ed w
hen
curr
ent
was
On,
an
d r
est
whe
n th
e cu
rren
t w
as O
ff );
- Th
e el
ectr
odes
wer
e p
ositi
oned
in th
e re
gion
cov
erin
g gl
ute-
us m
axim
us a
nd m
ediu
s, r
ectu
s ab
dom
inis
, an
d t
rans
vers
us
abd
omin
is b
ilate
rally
.E
xerc
ise
pro
toco
l for
CO
RE
str
engt
heni
ng :
- P
erfo
rmed
und
er t
he s
uper
visi
on o
f the
res
earc
hers
;-
Com
pos
ed o
f sta
tic p
ostu
res
sust
aine
d in
isom
etric
s;-
In e
ach
sess
ion
the
par
ticip
ants
per
form
ed 4
set
s (p
ostu
res)
of
10
rep
etiti
ons
sust
aine
d f
or 1
0 se
cond
s ea
ch,
with
an
in-
terv
al o
f 20
sec
ond
s b
etw
een
rep
etiti
ons
and
60
seco
nds
bet
wee
n se
ts;
- To
tal p
roto
col d
urat
ion:
25
min
;-
Freq
uenc
y: 3
x/w
eek
for
4 w
eeks
, tot
alin
g 12
ses
sion
s.
- C
OR
E G
roup
(C
G):
un-
der
wen
t C
OR
E s
tren
gth-
enin
g p
roto
col,
n=10
.-
Ele
ctro
stim
ulat
ion
grou
p (E
G):
und
erw
ent
trea
tmen
t w
ith N
, n=
10.
- E
lect
rost
imul
atio
n +
C
OR
E G
roup
(EC
G):
und
erw
ent
trea
tmen
t w
ith
NM
ES
syn
chro
nize
d w
ith
volu
ntar
y co
ntra
ctio
n d
urin
g C
OR
E s
tren
gthe
n-in
g ex
erci
ses,
n=
10.
Not
rep
orte
d.
CO
RE
mus
cles
sta
-b
iliza
tion
stre
ngth
(a
vera
ge
in
sec)
: tr
unk
stat
ic
en-
dur
ance
te
st,
So-
rens
on’s
te
st,
sid
e b
ridge
te
st
and
p
rone
in
stab
ility
te
st.
- P
re-t
reat
men
t (E
V 1
).-
Aft
er 1
2 se
s-si
ons
(EV
2).
- S
ix m
onth
s af
-te
r en
d of
tre
at-
men
t (E
V 3
).
Sig
nific
ant
incr
ease
b
etw
een
EV
2 a
nd E
V
3 ve
rsus
EV
1 i
n E
CG
in
all
test
s; s
igni
fican
t in
crea
se
bet
wee
n E
V
2 ve
rsus
EV
1 in
EG
in
Sor
enso
n’s
test
; an
d
sign
ifica
nt
diff
eren
ce
bet
wee
n E
CG
ve
rsus
C
G a
nd E
G in
all
test
s.
Pe
leg
rin
i et
al.22
Bra
zil
24
sed
enta
ry
wom
en;
Age
b
etw
een
18
and
30
ye
ars;
N
on
sp
ec
ific
C
LBP
; w
ith
sy
mp
to
ms
for
at l
east
12
wee
ks.
Aus
sie
Cur
rent
:-
Ap
plie
d o
n th
e lu
mb
ar p
arav
erte
bra
l mus
cles
bila
tera
lly b
y m
eans
of 2
cha
nnel
s co
ntai
ning
4 e
lect
rod
es (u
sing
wat
er-s
o-lu
ble
gel
as
a co
uplin
g m
ediu
m).
- C
ontr
ol G
roup
(C
G):
no
inte
rven
tion,
n=
12-
Aus
sie
Cur
rent
G
roup
(A
CG
): su
bm
itted
to tr
eat-
men
t w
ith A
ussi
e cu
rren
t,
n=12
.
Not
rep
orte
d.
Trun
k en
dur
ance
te
st.
Cro
ss
-se
cti
on
al
area
of
the
Mul
tifi-
dus
mus
cles
(ul
tra-
soun
d).
- P
re-t
reat
men
t (E
V 1
) .-
Aft
er 1
2 se
s-si
ons
(EV
2).
- O
ne m
onth
af-
ter
end
of t
reat
-m
ent (
EV
3).
Incr
ease
in
m
uscl
e en
dur
ance
b
etw
een
AC
G v
ersu
s C
G in
E
V 2
and
EV
3.
Incr
ease
in
cr
oss-
sect
ion
bet
wee
n A
CG
ve
rsus
CG
at E
V 2
and
E
V 3
.
EV
= e
valu
atio
n; C
LBP
= C
hron
ic L
ow B
ack
Pai
n; m
in =
min
utes
; sec
= s
econ
ds;
BM
I = b
ody
mas
s in
dex
; VA
S =
Vis
ual A
nalo
g S
cale
; NM
ES
= n
euro
mus
cula
r el
ectr
ical
stim
ulat
ion.
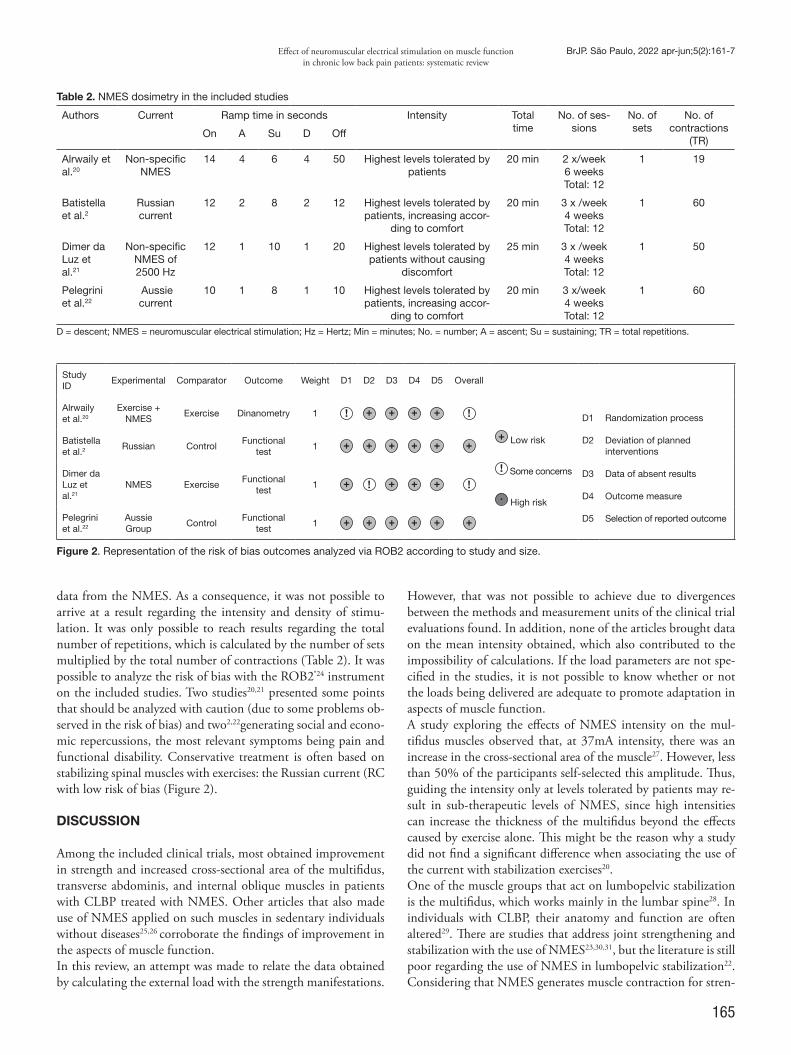
165
Effect of neuromuscular electrical stimulation on muscle function in chronic low back pain patients: systematic review
BrJP. São Paulo, 2022 apr-jun;5(2):161-7
data from the NMES. As a consequence, it was not possible to arrive at a result regarding the intensity and density of stimu-lation. It was only possible to reach results regarding the total number of repetitions, which is calculated by the number of sets multiplied by the total number of contractions (Table 2). It was possible to analyze the risk of bias with the ROB2®24 instrument on the included studies. Two studies20,21 presented some points that should be analyzed with caution (due to some problems ob-served in the risk of bias) and two2,22generating social and econo-mic repercussions, the most relevant symptoms being pain and functional disability. Conservative treatment is often based on stabilizing spinal muscles with exercises: the Russian current (RC with low risk of bias (Figure 2).
DISCUSSION
Among the included clinical trials, most obtained improvement in strength and increased cross-sectional area of the multifidus, transverse abdominis, and internal oblique muscles in patients with CLBP treated with NMES. Other articles that also made use of NMES applied on such muscles in sedentary individuals without diseases25,26 corroborate the findings of improvement in the aspects of muscle function.In this review, an attempt was made to relate the data obtained by calculating the external load with the strength manifestations.
However, that was not possible to achieve due to divergences between the methods and measurement units of the clinical trial evaluations found. In addition, none of the articles brought data on the mean intensity obtained, which also contributed to the impossibility of calculations. If the load parameters are not spe-cified in the studies, it is not possible to know whether or not the loads being delivered are adequate to promote adaptation in aspects of muscle function.A study exploring the effects of NMES intensity on the mul-tifidus muscles observed that, at 37mA intensity, there was an increase in the cross-sectional area of the muscle27. However, less than 50% of the participants self-selected this amplitude. Thus, guiding the intensity only at levels tolerated by patients may re-sult in sub-therapeutic levels of NMES, since high intensities can increase the thickness of the multifidus beyond the effects caused by exercise alone. This might be the reason why a study did not find a significant difference when associating the use of the current with stabilization exercises20.One of the muscle groups that act on lumbopelvic stabilization is the multifidus, which works mainly in the lumbar spine28. In individuals with CLBP, their anatomy and function are often altered29. There are studies that address joint strengthening and stabilization with the use of NMES23,30,31, but the literature is still poor regarding the use of NMES in lumbopelvic stabilization22. Considering that NMES generates muscle contraction for stren-
Table 2. NMES dosimetry in the included studies
Authors Current Ramp time in seconds Intensity Total time
No. of ses-sions
No. of sets
No. of contractions
(TR)On A Su D Off
Alrwaily et al.20
Non-specific NMES
14 4 6 4 50 Highest levels tolerated by patients
20 min 2 x/week6 weeksTotal: 12
1 19
Batistella et al.2
Russian current
12 2 8 2 12 Highest levels tolerated by patients, increasing accor-
ding to comfort
20 min 3 x /week4 weeksTotal: 12
1 60
Dimer da Luz et al.21
Non-specific NMES of 2500 Hz
12 1 10 1 20 Highest levels tolerated by patients without causing
discomfort
25 min 3 x /week4 weeksTotal: 12
1 50
Pelegrini et al.22
Aussiecurrent
10 1 8 1 10 Highest levels tolerated by patients, increasing accor-
ding to comfort
20 min 3 x/week4 weeksTotal: 12
1 60
D = descent; NMES = neuromuscular electrical stimulation; Hz = Hertz; Min = minutes; No. = number; A = ascent; Su = sustaining; TR = total repetitions.
Study ID
Experimental Comparator Outcome Weight D1 D2 D3 D4 D5 Overall
Alrwaily et al.20
Exercise + NMES
Exercise Dinanometry 1
Low risk
Some concerns
High risk
D1
D2
D3
D4
D5
Randomization process
Deviation of planned interventions
Data of absent results
Outcome measure
Selection of reported outcome
Batistella et al.2 Russian Control
Functionaltest
1
Dimer da Luz et al.21
NMES ExerciseFunctional
test1
Pelegrini et al.22
Aussie Group
ControlFunctional
test1
Figure 2. Representation of the risk of bias outcomes analyzed via ROB2 according to study and size.

166
BrJP. São Paulo, 2022 apr-jun;5(2):161-7 Linzmeyer A, Coracini CA, Bertolini GR and Carvalho AR
gth gain, using it according to strength training principles tends to generate better results. Of the included studies, only two2,22 specified which current was used – Russian and Aussie, respectively. Authors32 con-ducted a study comparing the effects of the Russian current (medium frequency) with low frequency currents, and conclu-ded that there was no significant difference regarding muscle torque, however, the discomfort with the Russian current was lower and the level of tolerated current amplitude increased. As for the Aussie current, which features a medium frequency base current but is modulated at low frequency, is considered the most comfortable and effective among the different forms of NMES. Nevertheless, even though this current is a good option for CLBP treatment, its use for this purpose is still scarce in the literature33.Based on this, it is a challenge to develop NMES protocols for patients with CLBP based on available literature, since there is no consistency in the parameters to be used. There is great di-vergence in the choice of physical parameters applied in the tests related to the choice of frequency, ramp time, current intensity and methodology of NMES use, directly influencing the results obtained. The limited number of studies included in the present review and the heterogeneity of methods and parameters employed are pointed out as limitations of this study, besides a possible bias of the publication language, since only studies in Portuguese, English and Spanish were considered. New randomized clinical trials conducted in a standardized manner must be encouraged, aiming to aid in the better unders-tanding of the parameters and efficacy of NMES, since a conclu-sion as to the ideal parameters to achieve muscle benefits has not yet been reached. However, it should be emphasized that, due to the low risks of bias observed, it is possible to identify that me-thodologically the studies can be considered viable for clinicians to make use of this resource in individuals with CLBP.
CONCLUSION
Based on the analyzed studies, NMES has positive effects in op-timizing aspects of muscle function in individuals with CLBP. However, new clinical trials are still needed in order to clarify the methods and parameters used, since important information is still scarce in the literature.
AUTHORS’ CONTRIBUTIONS
Alessandra Linzmeyer Data Collection, Conceptualization, Resource Management, Research, Methodology, Writing - Preparation of the original, Visualização Camila Amaral Coracini Data Collection, Conceptualization, Research, Methodology, Writing - Preparation of the original, Visualizing Gladson Ricardo Flor Bertolini Data Collection, Conceptualization, Project Management, Me-thodology, Writing - Review and Editing, Supervision
Alberito Rodrigo Carvalho Conceptualization, Resource Management, Project Manage-ment, Methodology, Writing - Review and Editing, Supervision
REFERENCES
1. Bahns C, Happe L, Thiel C, Kopkow C. Physical therapy for patients with low back pain in Germany: a survey of current practice. BMC Musculoskelet Disord. 2021;22(1):563.
2. Batistella CE, Bidin F, Giacomelli I, Nunez MA, Gasoto E, Albuquerque CE, et al. Ef-fects of the Russian current in the treatment of low back pain in women: a randomized clinical trial. J Bodyw Mov Ther. 2020;24(2):118-22.
3. Gonzalez GZ, Silva T, Avanzi MA, Macedo GT, Alves SS, Indini LS, et al. Low back pain prevalence in Sao Paulo, Brazil: a cross-sectional study. Braz J Phys Ther. 2011;26:837-45.
4. Aguiar DP, Souza CP, Barbosa WJ, Santos-Júnior FF, Oliveira AS. Prevalence of chro-nic pain in Brazil: systematic review. BrJP. 2021;4(3):257-67.
5. Liu M, Shaparin N, Nair S, Kim RS, Hascalovici JR. Chronic low back pain: the therapeutic benefits of diagnostic medial branch nerve blocks. Pain Physician. 2021;24(4):E521-E528. doi:10.36076/ppj.2021.24.E521.
6. Frizziero A, Pellizzon G, Vittadini F, Bigliardi D, Costantino C. Efficacy of core stabi-lity in non-specific chronic low back pain. J Funct Morphol Kinesiol. 2021;6(2):37.
7. George SZ, Fritz JM, Silfies SP, Schneider MJ, Beneciuk JM, Lentz TA, et al. Inter-ventions for the management of acute and chronic low back pain: Revision 2021. J Orthop Sports Phys Ther. 2021;51(11):CPG1-CPG60.
8. Bardin LD, King P, Maher CG. Diagnostic triage for low back pain: a practical approach for primary care. Med J Aust. 2017;206(6):268-73.
9. Russo M, Deckers K, Eldabe S, Kiesel K, Gilligan C, Vieceli J, et al. Muscle control and non-specific chronic low back pain. Neuromodulation. 2018;21(1):1-9.
10. Songjaroen S, Sungnak P, Piriyaprasarth P, Wang HK, Laskin JJ, Wattananon P. Com-bined neuromuscular electrical stimulation with motor control exercise can improve lumbar multifidus activation in individuals with recurrent low back pain. Sci Rep. 2021;11(1):14815.
11. Ferreira PH, Ferreira ML, Maher CG, Herbert RD, Refshauge K. Specific stabi-lisation exercise for spinal and pelvic pain: a systematic review. Aust J Physiother. 2006;52(2):79-88.
12. van Tulder M, Malmivaara A, Esmail R, Koes B. Exercise therapy for low-back pain. In: Cochrane Database of Systematic Reviews. John Wiley & Sons, Ltd; 2000. doi:10.1002/14651858.CD000335
13. Ibrahim T, Tleyjeh IM, Gabbar O. Surgical versus non-surgical treatment of chronic low back pain: a meta-analysis of randomised trials. Int Orthop. 2008;32(1):107-13.
14. Almeida GJ, Khoja SS, Piva SR. Dose-response relationship between neuromuscular electrical stimulation and muscle function in people with rheumatoid arthritis. Phys Ther. 2019;99(9):1167-76.
15. Impellizzeri FM, Marcora SM, Coutts AJ. Internal and external training load: 15 years on. Int J Sports Physiol Perform. 2018;14(2):270-3.
16. Dehail P, Duclos C, Barat M. Electrical stimulation and muscle strengthening. Ann Readapt Med Phys. 2008;51(6):441-51.
17. Bosques G, Martin R, McGee L, Sadowsky C. Does therapeutic electrical stimulation improve function in children with disabilities? A comprehensive literature review. J Pediatr Rehabil Med. 2016;9(2):83-99.
18. Chughtai M, Elmallah RD, Mistry JB, Bhave A, Cherian JJ, McGinn TL, et al. Non-pharmacologic pain management and muscle strengthening following total knee ar-throplasty. J Knee Surg. 2016;29(3):194-200.
19. Marston KJ, Peiffer JJ, Newton MJ, Scott BR. A comparison of traditional and novel metrics to quantify resistance training. Sci Rep. 2017;7(1):5606.
20. Alrwaily M, Schneider M, Sowa G, Timko M, Whitney SL, Delitto A. Stabilization exercises combined with neuromuscular electrical stimulation for patients with chronic low back pain: a randomized controlled trial. Braz J Phys Ther. 2019;23(6):506-15.
21. Dimer da Luz R, Santos MS, Evaldt AS, Matos LS, Daitx RB, Döhnert MB. Neu-romuscular electrical stimulation associated with core stability exercises in nonspeci-fic postural low back pain: a randomized clinical trial. Muscle Ligaments Tendons J. 2019;9(03):446-56.
22. Pelegrini ACA, Gasoto E, Bussolaro JM, Segatti G, Albuquerque CE, Bertolini GRF. The analgesic action of Aussie current in women with non-specific chronic lumbar pain. Int J Ther Rehabil. 2019;26(7):1-10.
23. Coghlan S, Crowe L, McCarthyPersson U, Minogue C, Caulfield B. Neuromuscular electrical stimulation training results in enhanced activation of spinal stabilizing mus-cles during spinal loading and improvements in pain ratings. Annu Int Conf IEEE Eng Med Biol Soc. 2011;2011:7622-5.
24. Sterne JAC, Savović J, Page MJ, Elberts RG, Blencowe NS, Boutron I, et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898.
25. Lopes AB, Amboni DE, Schmidel MM, Maciel MJ, de Carvalho AR, Bertolini GRF. Evaluation of the dose-response for electrostimulation with Aussie current in the core strength. Eur J Clin Exp Med. 2020;18(2):81-7.
26. Camilo IR, Silva P, Mata TB, Peres CPA, Bertolini GRF. Estimulação elétrica neu-romuscular na diástase, flacidez e trofismo da musculatura abdominal: uma revisão

167
Effect of neuromuscular electrical stimulation on muscle function in chronic low back pain patients: systematic review
BrJP. São Paulo, 2022 apr-jun;5(2):161-7
sistemática. Saúde.Com. 2021;16(3):1894-900. 27. Sions JM, Crippen DC, Hicks GE, Alroumi AM, Manal TJ, Pohlig RT. Exploring
neuromuscular electrical stimulation intensity effects on multifidus muscle activity in adults with chronic low back pain: an ultrasound imaging–informed investigation. Clin Med Insights Arthritis Musculoskelet Disord. 2019;20:12:11795441119849570.
28. Kim SH, Park KN, Kwon OY. Pain intensity and abdominal muscle activation during walking in patients with low back pain. Medicine (Baltimore). 2017;96(42):e8250.
29. Goubert D, Oosterwijck J Van, Meeus M, Danneels L. Structural changes of lumbar muscles in non-specific low back pain. Pain Physician. 2016;19(7):E985-E999.
30. Mukaino M, Ono T, Shindo K, et al. Efficacy of brain-computer interface-driven neuromuscular electrical stimulation for chronic paresis after stroke. J Rehabil Med.
2014;46(4):378-82. 31. Mettler JA, Bennett SM, Doucet BM, Magee DM. Neuromuscular electrical sti-
mulation and anabolic signaling in patients with stroke. J Stroke Cerebrovasc Dis. 2017;26(12):2954-63.
32. Fukuda TY, Marcondes FB, Anjos Rabelo N, Vasconcelos RA, Cazarini Junior C. Com-parison of peak torque, intensity and discomfort generated by neuromuscular electrical stimulation of low and medium frequency. Isokinets Exerc Sci. 2013;21(2):167-73.
33. Dantas LO, Vieira A, Siqueira AL, Salvini TF, Durigan JLQ. Comparison between the effects of four different electrical stimulation current waveforms on isometric knee extension torque and perceived discomfort in healthy women. Muscle Nerve. 2015;51(1):76-82.

168
BrJP. São Paulo, 2022 apr-jun;5(2):168-71
ABSTRACT
BACKGROUND AND OBJECTIVES: Erector spinae plane block is an interfascial plane block used as a tool for manage-ment of pain resulting from thoracic and abdominal surgical procedures described in the literature since 2016 and widely used in clinical practice. In the context of the pandemic caused by Sars-CoV-2, multiple pulmonary complications arising from severe viral pneumonia and respiratory failure that required sur-gical approaches for their investigation and/or treatment were observed. The present study’s objective was to present a series of three cases of patients affected by COVID-19 who had pulmo-nary complications due to infection or exacerbation of previous pulmonary diseases caused by the new coronavirus, in which the continuous fascial plane block was successfully used for postope-rative pain management.CASE REPORTS: Three cases of patients with COVID-19 viral pneumonia requiring diagnostic or therapeutic thoracic surgery who underwent erector spinae plane block for perioperative pain management were presented.CONCLUSION: The use of a catheter with continuous infu-sion of local anesthetic was useful for reducing analgesic rescue and maintaining good postoperative analgesia with no evidence of adverse effects in the presented patients, also allowing acce-leration of postoperative recovery and a better outcome for the patients.
Erector spinae plane block on pain management after thoracic surgical approaches due to COVID-19 complications. Case reportsBloqueio do plano dos músculos eretores da espinha no manejo de dor pós-abordagens cirúrgicas torácicas por complicações da COVID-19. Relato de casos
Leonardo de Freitas Nascimento1, Felipe Chiodini Machado1, Adriana Madeleine Dominguez Gaibor1, Lucas Snioka Zuretti1, Hazem Adel Ashmawi1
Leonardo de Freitas Nascimento – https://orcid.org/0000-0003-1187-1584;Felipe Chiodini Machado – https://orcid.org/0000-0003-1615-2597;Adriana Madeleine Dominguez Gaibor – https://orcid.org/0000-0001-5075-7464;Lucas Snioka Zuretti – https://orcid.org/0000-0002-5713-1760;Hazem Adel Ashmawi – https://orcid.org/0000-0003-0957-971X.
1. University of São Paulo, Medicine School, Teaching Hospital, Central Institute, Anesthe-siology, São Paulo, SP, Brazil.
Submitted on March 02, 2021.Accepted for publication on May 03, 2022.Conflict of interests: none – Sponsoring sources: none.
Correspondence to: Leonardo de Freitas Nascimento E-mail: [email protected]
© Sociedade Brasileira para o Estudo da Dor
Keywords: Acute pain, Case reports, Conduction anesthesia, Coronavirus Infections, Video-assisted thoracic surgery.
RESUMO
JUSTIFICATIVA E OBJETIVOS: O bloqueio do plano dos músculos eretores da espinha é um bloqueio do plano interfa-cial usado como ferramenta para manejo de dor consequente a procedimentos cirúrgicos torácicos e abdominais descrito na literatura desde 2016 e amplamente utilizado na prática clíni-ca. No contexto da pandemia causada pelo Sars-CoV-2, foram observadas múltiplas complicações pulmonares decorrentes de pneumonia viral grave e insuficiência respiratória que demanda-ram abordagens cirúrgicas para sua investigação e/ou tratamento. O objetivo deste estudo foi apresentar uma série de três casos de pacientes acometidos pela COVID-19 que tiveram complicações pulmonares pela infecção ou exacerbação de doença pulmonar prévia causada pelo novo coronavírus, nos quais o recurso do bloqueio do plano fascial contínuo foi utilizado para manejo de dor pós-operatória com sucesso.RELATO DOS CASOS: Foram apresentados três casos de pa-cientes acometidos pelo COVID-19 em sua forma de pneumo-nia viral, para os quais houve necessidade de cirurgia torácica diagnóstica ou terapêutica, e que foram submetidos ao bloqueio do plano dos músculos eretores da espinha para manejo da dor perioperatória.CONCLUSÃO: O uso de cateter com infusão contínua de anes-tésico local foi útil para a diminuição dos resgates analgésicos e manutenção de boa analgesia pós-operatória sem evidência de efeitos adversos nos pacientes apresentados, possibilitando ainda a aceleração da recuperação pós-operatória e um melhor desfe-cho para os pacientes. Descritores: Anestesia por condução, Cirurgia torácica vídeoas-sistida, Dor aguda, Infecções por coronavírus, Relato de caso.
INTRODUCTION
Analgesia for patients undergoing thoracic surgery is often the subject of discussion given the high incidence of pain in this po-pulation. Currently, the main analgesia guidelines for the posto-perative period of thoracic surgery involve the use of multimodal analgesia and regional or neuroaxis blocks1.
DOI 10.5935/2595-0118.20220026-en
CASE REPORT

169
Erector spinae plane block on pain management after thoracic surgical approaches due to COVID-19 complications. Case reports
BrJP. São Paulo, 2022 apr-jun;5(2):168-71
Erector spinae muscles plane block (ESPb) is cited as a regio-nal analgesia option for postoperative pain control in different thoracic surgery techniques2-4. Described in 2016, it is an in-filtration of local anesthetic into the spinal erector musculature in paravertebral topography with the objective of blocking the innervation of the thoracic and upper abdominal area, with pos-sible somatic and autonomic components5.In the context of the pandemic caused by Sars-CoV-2, many patients developed pulmonary complications from viral pneu-monia, requiring surgical intervention in the thoracic region for diagnostic or therapeutic procedures. In some cases, such pa-tients underwent surgeries with high potential of pain, adding to the physiological complications related to COVID-19.The study’s objective was to present a case series of three patients who developed COVID-19 in its viral pneumonia form, for whom there was a need for diagnostic or therapeutic thoracic surgery and who underwent ESPb for perioperative pain management. CASE REPORTS
The CAse REport (CARE) Checklist was used for preparation of this manuscript in order to increase accuracy, transparency, and usefulness of case reports6,7.
Case 1A 73-year-old male patient, previously hypertensive, firstly pre-sented flu-like symptoms and later developed dyspnea and was admitted to a tertiary hospital due to acute respiratory failure requiring orotracheal intubation. During hospitalization, the patient presented a bilateral pulmo-nary embolism complication due to deep venous thrombosis of the right popliteal vein, associated with extensive pulmonary in-farction to the right. Next, the patient developed a bronchopleural fistula and pneumothorax to the right, with placement of a pigtail drain in the anterior wall, which only resolved satisfactorily after continuous aspiration, without the need for lung expansion. He was submitted to emptying of the pleural space by right vi-deo-assisted thoracic surgery (VATS) and anterior pleural drai-nage with 28 French (Fr) drain and posterior pleural drainage with 38 Fr drain. The Pain Control Team was asked to evaluate the case. On the first day after surgery, the patient presented in-tense pain in the right hemithorax, was ventilatory-dependent, burning with irradiation throughout the hemithorax from the axillary region, worsening when deep breathing and coughing. The prescription included intravenous (IV) morphine 4mg if ne-cessary, oral methadone 10mg once a day, oral paracetamol 2 g a day, and oral dipyrone 8 g a day. Oral pregabalin 75mg per day was introduced and the right ESPb was performed with passage of a local catheter. A patient-controlled analgesia (PCA) pump was started with 0.2% ropivacaine, with a continuous infusion of 7mL per hour (h), bolus of 5 mL, at minimum interval of 30 minutes, and a limit of 17 mL in 4 hours. The patient condition developed with a report of significant pain improvement, with pain of zero/10 on the numerical rating scale (NRS) at rest, and pain 2/10 when immobilized in bed (sitting and walking), with no other complaints. In the following days, there was
a reduction in opioid consumption, and the catheter was disconti-nued on the 5th day after its implementation. The patient had no more pain complaints until hospital discharge, 20 days after surgery.
Case 2A 70-year-old male patient, hypertensive, diagnosed with dia-betes mellitus and type 2 chronic kidney disease, former smo-ker, admitted to a tertiary hospital with a confirmed diagnosis of COVID-19 on the 30th day of symptoms. The patient presented dyspnea during moderate/severe exertion associated with cough and developed tachydyspnea, abolished ve-sicular murmurs to the right, and use of a 3L/min nasal catheter.A relief thoracentesis was performed, with an output of 2 liters of serous hematic fluid, improving the symptoms. A pigtail drain was passed without effective drainage and decortication, pleural debridement and VATS thoracentesis were indicated. In the immediate postoperative period, the patient presented 10/10 pain on the NRS, and the right side ESPb was indicated with passage of a local catheter and infusion of 0.2% ropivacaine solution in PCA with an infusion of 4mL/h; bolus of 5 mL, at 30-minute intervals, with a 4-hour limit of 60mL. The patient was also prescribed gabapentin 900mg/day, dipyrone 4g/day in-travenously, and tramadol 100 mg 6/6 hours intravenously if ne-cessary. The condition developed with mild pain (NR: 2/10) in the right hemithorax during deep breathing, with no pain when immobilized and no need for opioids. Cyclobenzaprine 5mg once a day was later introduced due to complaint of myofascial pain, by decubitus. On the 8th posto-perative day, the catheter was discontinued (the catheter broke when the bacteriostatic filter was attached) and weaning of ga-bapentin was initiated, with no pain complaints. The patient was discharged from the hospital three weeks after surgery, with only occasional use of dipyrone.
Case 3A 53-year-old male patient, hypertensive, obese, with a diagnosis of COVID-19, requiring orotracheal intubation on the 12th day of symptoms in addition to the use of neuromuscular block in continuous infusion, prone positioning, and nitric oxide (NO). The patient remained on mechanical ventilation for a prolonged period and underwent tracheotomy. Necrotizing pneumonia developed, and thoracic surgery was needed. Right apical segmentectomy by VATS and thoracotomy were indicated. Afterwards, a closed drainage was performed with a 38 Fr chest drain. During the intraoperative period, a catheter was placed in the right spinal erector muscles plane. The patient was brought to the intensive care unit with conti-nuous infusion of 0.2% ropivacaine solution at a rate of 6 mL/h, with prescription for manual bolus by the medical team of 6mL, if needed. On the first day after surgery, the nursing team re-ported that the catheter had been lost. During a new visit by the pain team, after a test dose of 10mL of lidocaine 1% and 50% pain relief, the catheter viability, and its effective fixation at 13cm on the skin mark were confirmed. After weaning from mechanical ventilation, the patient was conscious and focused, with no complaints of pain during rest

170
BrJP. São Paulo, 2022 apr-jun;5(2):168-71 Nascimento LF, Machado FC, Gaibor AM, Zuretti LS and Ashmawi HA
or immobilization and cooperative to respiratory rehabilitation. There was no need for the use of schedule or rescue opioids, maintaining only the use of intravenous dipyrone 8g/day and infusion of local anesthetic through the catheter. On the 5th pos-toperative day, the interfascial catheter presented a breakage. The catheter and chest drain were then removed on the same day, with no complaints of pain.After physical therapy treatment for motor and respiratory re-covery, the scenario developed with a successful tracheostomy occlusion and decannulation, and the patient was discharged from the hospital with an outpatient follow-up 51 days after the surgical procedure with no complaints of pain.
DISCUSSION
Initially described by Forero et al.2 for the treatment of neuropathic pattern chest pain, ESPb is a fascial plane block. The erector spinae muscles comprise a series of muscles that extend along the cervical, thoracic, and lumbar region. These muscles are in the lateral sulcus of the spine and include the iliocostalis, spinal, and dorsalis longus.In the version of this block used in the described patients, the patients are positioned in lateral dorsal decubitus or sitting posi-tion leaning forward, and the posterior chest wall is exposed. The procedure is performed under aseptic technique. A high-frequency linear ultrasound transducer is placed in longitudinal orientation over the midline of the spine at T4-T6, with the objective of iden-tifying the spinous process of the vertebra. Once identified, the transducer is laterally slid toward the side to be blocked until the transverse process of the vertebra is identified, the anatomical re-ference of the block. The blocking needle is inserted in the skin in plane with the ultrasound transducer beams toward the transverse spinal process in the cephalocaudal orientation, until contact with it is established. The needle is then retracted by a few fractions of a millimeter, only so it loses its contact with the bone surface, and the local anesthetic of choice is infused in the fascial plane. The formation of an interfascial pocket is observed between the verte-bral transverse process and the erector spinae muscles.Studies indicate that its probable site of action occurs in the dor-sal and ventral branches of the spinal nerves, besides covering the sympathetic chain in thoracic topography2,5. There is evidence that, during ESPb, the injected volume is distributed over several adjacent dermatomes in the anterior, lateral and posterior chest wall6. The hypothesis is that alterations in intrathoracic pressure in a live model would allow dispersion into the paravertebral space, an event not likely to be observed in cadavers5. Another potential mechanism described is the epidural dissemination of the local anesthetic7.Currently, the application of ESPb has been extended beyond thoracic surgery and several approaches have been described. There are reports that show its efficacy for analgesia in proce-dures such as breast reconstruction, hip surgery, coronary artery bypass graft surgery, and others3,4,8,9.Regional anesthesia is strongly recommended to reduce the use of opioids and the related adverse effects, including hypoventi-lation10, sedation, nausea, and vomiting11. ESPb is technically simple to perform, with low chances of complications, such as
traumatic nerve injury, pneumothorax, or formation of hema-toma. Anticoagulation may be a relative contraindication for ESPb, although there are no specific guidelines. The reported patients were on prophylactic anticoagulation, and this was not stopped for the procedure. The most recent 2018 American Society of Regional Anesthesia (ASRA) consensus does not specifically address paraspinal blocks and anticoagulation12. In addition, there are fewer contraindi-cations for fascial plane block compared to neuroaxial techni-ques, making ESPb a potential alternative to neuroaxial blocks13. Therefore, the ESPb technique can be an important locoregional analgesia tool for pain management in this context.The three patients presented in this report maintained satisfac-tory pain scores in the days following the surgical intervention, with good tolerance to the early introduction of routine respira-tory physical therapy, even when using a chest drain, sometimes in more than one location. These patients’ condition developed with low opioid consumption in the follow-up, showing the be-nefit of analgesia with continuous ESPb associated with adjuvants such as gabapentinoids and common analgesics. In this specific group of patients, which are those affected by COVID-19 with multiple comorbidities, the benefit of regional analgesia is even more important when considering their borderline status of res-piratory, neurological, and hemodynamic functions.However, there are still obstacles to using and maintaining the viability of the interfascial peripheral catheter during postopera-tive care. The refinement of catheter fixation techniques is neces-sary, as well as the training of the teams involved in patient care and manipulation. Continuous interfascial infusion is a relati-vely recent option of analgesia, and it is necessary to familiarize the entire multidisciplinary team with this tool to avoid catheter losses or infusions through unusual routes. The little experience of the assistance teams outside the operating room with the ca-theter care and the comprehension of the importance of maintai-ning its viability are still obstacles to be overcome.The continuous ESPb (interfascial catheter passage) becomes, therefore, an important ally in the management of surgical pain, especially in patients with significant respiratory issues undergoing thoracic surgical procedures, resulting in better outcome and early recovery. Dissemination of the technique should be encouraged, as well as stimulation of its reproduction and learning by anesthe-siologists in training or already in practice in order to expand the range of action and good practices in intraoperative and postope-rative management of patients. Future studies can help to prove the benefits and optimization of outcomes found in these reports, expanding the practice of continuous ESPb to other types of pro-cedures, as well as showing its applicability in other locations, such as thoracolumbar or lumbar region transition. CONCLUSION
ESPb is a technique that substantially impacts pain management in patients undergoing thoracic surgery, including in the presen-ted scenario of patients undergoing such surgical procedures for complications arising from COVID-19. The use of a catheter with continuous infusion of local anesthetic was useful in reducing

171
Erector spinae plane block on pain management after thoracic surgical approaches due to COVID-19 complications. Case reports
BrJP. São Paulo, 2022 apr-jun;5(2):168-71
analgesic rescue and maintaining good postoperative analgesia wi-thout evidence of adverse effects in the presented patients. The little experience of the assistance teams outside the operating room with the catheter care and the comprehension of the importance of maintaining its viability are still obstacles to be overcome.
AUTHORS’ CONTRIBUTIONS
Leonardo de Freitas Nascimento Data Collection, Writing - Preparation of the original, Writing - Review and Editing, Supervision Felipe Chiodini Machado Project Management, Writing - Preparation of the original, Wri-ting - Review and Editing, Supervision Adriana Madeleine Dominguez Gaibor Data Collection, Writing - Preparation of the original, Writing - Review and EditingLucas Snioka Zuretti Data Collection, Writing - Preparation of the originalHazem Adel Ashmawi Project management, Writing - Review and Editing, Supervision
REFERENCES
1. Batchelor TJP, Rasburn NJ, Abdelnour-Berchtold E, Brunelli A, Cerfolio RJ, Gonza-lez M, et al. Guidelines for enhanced recovery after lung surgery: recommendations of the Enhanced Recovery After Surgery (ERAS®) Society and the European Society of Thoracic Surgeons (ESTS). Eur J Cardiothorac Surg. 2019;55(1):91-115.
2. Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ. The erector spinae plane block:
a novel analgesic technique in thoracic neuropathic pain. Reg Anesth Pain Med. 2016;41(5):621-7.
3. Balaban O, Aydin T, Yaman M. Is ultrasound guided erector spinae plane block sufficient for surgical anesthesia in minor surgery at thoracal region? J Clin Anesth. 2018;47(1):7-8.
4. Chanowski EJP, Horn JL, Boyd JH, Tsui BCH, Brodt JL. Opioid-free ultra-fast-track on-pump coronary artery bypass grafting using erector spinae plane catheters. J Car-diothorac Vasc Anesth. 2019;33(7):1988-90.
5. Chin KJ, Malhas L, Perlas A. The erector spinae plane block provides visceral abdominal analgesia in bariatric surgery: a report of 3 cases. Reg Anesth Pain Med. 2017;42(3):372-6.
6. Riley DS, Barber MS, Kienle GS, Aronson JK, von Schoen-Angerer T, Tugwell P, et al. CARE guidelines for case reports: explanation and elaboration document. J Clin Epidemiol. 2017;89:218-35.
7. Gagnier JJ, Kienle G, Altman DG, Moher D, Sox H, Riley DS, CARE Group. The CARE Guidelines: Consensus-based Clinical Case Reporting Guideline Develop-ment. Glob Adv Health Med. 2013;2(5):38-43.
8. Ueshima H, Hiroshi O. Spread of local anesthetic solution in the erector spinae plane block. J Clin Anesth. 2018;45:23.
9. Yang HM, Choi YJ, Kwon HJ, O J, Cho TH, Kim SH. Comparison of injectate spread and nerve involvement between retrolaminar and erector spinae plane blocks in the thoracic region: a cadaveric study. Anaesthesia. 2018;73(10):1244-50.
10. Bonvicini D, Tagliapietra L, Giacomazzi A, Pizzirani E. Bilateral ultrasound-guided erector spinae plane blocks in breast cancer and reconstruction surgery. J Clin Anesth. 2018;44(1):3-4.
11. Tulgar S, Senturk O. Ultrasound guided Erector Spinae Plane block at L-4 transverse process level provides effective postoperative analgesia for total hip arthroplasty. J Clin Anesth. 2018;44:68.
12. Bos EME, Haumann J, de Quelerij M, Vandertop WP, Kalkman CJ, Hollmann MW, et al. Haematoma and abscess after neuraxial anaesthesia: a review of 647 cases. Br J Anaesth. 2018;120(4):693-704.
13. Richardson J, Sabanathan S, Shah R. Post-thoracotomy spirometric lung function: the effect of analgesia. A review. J Cardiovasc Surg (Torino). 1999;40(3):445-56.
14. Horlocker TT, Vandermeuelen E, Kopp SL, Gogarten W, Leffert LR, Benzon HT. Regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy: American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guideli-nes (Fourth Edition). Reg Anesth Pain Med. 2018;43(3):263-309.
15. Yeung JH, Gates S, Naidu BV, Wilson MJ, Gao Smith F. Paravertebral block versus thoracic epidural for patients undergoing thoracotomy. Cochrane Database Syst Rev. 2016;(2):CD009121.

172
BrJP. São Paulo, 2022 apr-jun;5(2):172-7
ABSTRACT
BACKGROUND AND OBJECTIVES: Psychological inter-vention can contribute to repairing the quality of life and alte-ring behavior while dealing with chronic orofacial pain, espe-cially those that can become refractory to treatments. Thus, the objective of this study was to present the narratives of three pa-tients with refractory chronic neuropathic pain during the pro-cess of psychotherapeutic intervention and the follow-up results. CASE REPORTS: Pain behavior, pain perception and depres-sive and anxious symptoms were assessed. Patients were under treatment at the Orofacial Pain Clinic and the instruments used in the beginning and end of psychotherapy were the visual ana-log scale, Beck Inventories (anxiety and depression), Wisconsin Pain Inventory, McGill Pain Questionnaire and Pain Catastro-phizing Scale. They attended weekly 50-minute sessions. Each narrative was qualitatively analyzed and the comparison between the evaluations made before and after psychotherapy was inclu-ded in the context of a phenomenological approach. CONCLUSION: Emotional familiar conflicts and fear of pain crises were the most important aspects described by these pa-tients. Case 1 presented the less cooperative profile and secon-dary gains. Despite of that, all cases presented improvement and psychotherapy helped to cope with their problems and pain. There was a remarkable impact on the life of patients as well as on their cooperation with pain treatments while helping the patients to build a proactive attitude and to understand their role in their condition. Keywords: Chronic pain, Neuropathic orofacial pain. Pain behavior, Psychotherapy, Trigeminal neuralgia.
Psychotherapy in the treatment of chronic refractory orofacial pain. Case reportsPsicoterapia no tratamento da dor orofacial crônica refratária. Relato de casos
Marianna Barbosa Yamaguchi1, Maria de Fatima Vidotto Oliveira1, Silvia Regina DT de Siqueira1
Marianna Barbosa Yamaguchi – https://orcid.org/0000-0002-8501-4748;Maria de Fatima Vidotto Oliveira – https://orcid.org/0000-0002-5967-7708;Silvia Regina DT de Siqueira – https://orcid.org/0000-0003-0207-0072.
1. University of São Paulo, School of Medicine, Interdisciplinary Pain and Orofacial Pain Groups, Neurology Department, São Paulo, SP, Brazil.
Submitted on April 16, 2021.Accepted for publication on April 19, 2022.Conflict of interests: none – Sponsoring sources: none.
Correspondence to:Silvia R D T de Siqueira E-mail: [email protected]
© Sociedade Brasileira para o Estudo da Dor
RESUMO
JUSTIFICATIVA E OBJETIVOS: A intervenção psicoterapêu-tica é uma ferramenta importante para melhorar a qualidade de vida de pacientes com dor orofacial crônica, especialmente aque-les que se tornam refratários aos tratamentos. Assim, o objetivo deste estudo foi apresentar, na forma de narrativa, três casos de pacientes com dor facial refratária ao longo do processo de inter-venção psicoterapêutica e os resultados obtidos. RELATO DOS CASOS: Observou-se o comportamento, a per-cepção da dor e sintomas ansiosos e depressivos. Os pacientes estavam sob tratamento na Equipe de Dor Orofacial e os ins-trumentos utilizados no início e no final da intervenção foram a Escala Visual Analógica, os Inventários de Beck para Ansiedade e Depressão, o Inventário de Dor de Wisconsin, o Questionário de Dor McGill e a Escala de Catastrofização de Dor. Os pacientes foram atendidos semanalmente em sessões de 50 minutos. Cada narrativa foi analisada qualitativamente e a comparação entre as avaliações (antes e depois do tratamento) foi incluída em um contexto de abordagem fenomenológica. CONCLUSÃO: Conflitos familiares emocionais e medo das cri-ses de dor foram os aspectos mais importantes descritos pelos pacientes. O caso 1 apresentou um perfil menos cooperador, em-bora todos tenham apresentado melhora em algum âmbito ava-liado. A proposta psicoterapêutica os auxiliou no enfrentamento do sofrimento por conta de seus problemas e da dor. Houve um impacto notável na vida dos pacientes como em sua cooperação com os tratamentos, uma vez que aprender a lidar com seu sofri-mento os conduziu a uma postura mais proativa através do en-tendimento de seus papéis no tratamento da condição dolorosa. Descritores: Comportamento da dor, Dor crônica, Dor orofa-cial neuropática, Neuralgia do trigêmeo.
INTRODUCTION
According to the International Association for the Study of Pain, pain is characterized by ‘’an unpleasant sensory and emo-tional experience associated with, or resembling that associated with, actual or potential tissue damage’’. As a complex biop-sychosocial phenomenon, it becomes chronic when its duration surpasses three to six months. Sensory and emotional experien-ce results in suffering and triggers pain behaviors, which can also become chronic1. These behaviors depend on personality, anxiety and depression traits or diagnoses and patients´ strate-gies for coping. Pain is subjective and individualized, and its duration and natural history can interfere with clinical features.
DOI 10.5935/2595-0118.20220017
CASE REPORT

173
Psychotherapy in the treatment of chronic refractory orofacial pain. Case reports
BrJP. São Paulo, 2022 apr-jun;5(2):172-7
Chronic pain is prevalent, and 30% to 40% of individuals with pain go five times more to the emergency room than other patients2-4. It is a highlighted reason for absenteeism, and it has a severe impact on life. Orofacial pain affects 10% to 30% of the population and its psychological impact is re-markable due to the psychological and social importance of the face, and vital functions of this body area such as eating, breathing and talking5,6. Most patients present perceptual dis-tortions of the face7. Moreover, a subgroup of orofacial pain that is neuropathic is responsible for 4-18% of cases, and their treatment often results in partial alleviation of symptoms8. Neuropathic pain is associated with dysfunction or lesion of the nervous system9.The most common types of neuropathic orofacial pain are tri-geminal neuralgia, burning mouth syndrome and post-trau-matic neuropathic pain; other chronic facial pain syndromes that have complex assessment are persistent idiopathic facial pain and atypical odontalgia8. Trigeminal neuralgia is consi-dered one of the worst pain conditions and the intense suf-fering can even lead to suicide. In general, it is idiopathic, however around 5% of the patients present a primary cause (eg. meningioma, schwannoma, multiple sclerosis)10,11. Burning mouth syndrome is characterized by continuous burning pain at the oral cavity with no primary cause. These patients often present emotional comorbidities and severe im-pairment in daily activities12. Persistent idiopathic facial pain and atypical odontalgia consist in constant, dull, aching pain with unclear pathophysiology8. Neuropathic pain patients often suffer from sequelae of sur-gical procedures including complications from invasive pro-cedures to treat pain. There are several psychiatric comorbi-dities in these patients, including depression, dystimia, social phobia, generalized anxiety, and worrying about the pain is a main associated factor in patients with orofacial pain13. This complex clinical condition requires special medical and psychological assessment. Chronic pain can be associated with subjective bad self-description, reinforced by words the patients heard previously in their lives14,15.Psycho-educative tools are part of the strategy for pain co-ping, and philosophical precepts are the base of intervention techniques to alleviate or eliminate suffering. Treatment mo-dalities include psychoanalysis, cognitive behavior therapy, biofeedback and hypnosis. Graduated exposure to pain and systematized desensitization helps the patient release from the fear of pain and return to normal life, both constituting po-sitive coping mechanisms. Negative coping in chronic pain is associated with secondary gains and/or avoidance of several activities that were part of the normal daily life of the pa-tient16. Positive and negative reinforcements or punishments need to be identified and addressed. There is evidence in the literature that chronic pain patients can benefit from psychotherapy17; however, there is a lack of studies on orofacial or neuropathic pain. Thus, the objective of this research was to present the narratives of three patients with refractory chronic neuropathic pain during the process of psychotherapeutic intervention and the follow-up results.
CASE REPORTS
All patients were informed about the purposes of this study and signed the informed consent. The local ethics committee from University of São Paulo (1.172.960) approved this study. This manuscript was written based on CAse REport Guidelines (CARE)18.
Patient InformationPrimary concerns and patient symptoms.The narratives of three patients at the Orofacial Pain Clinic of a general hospital are here recorded. They were a woman with burning mouth syndrome, a man with idiopathic trigeminal neuralgia and a woman with secondary trigeminal neuralgia and multiple sclerosis. All of them were literate and had had orofacial pain for more than 6 months. There were no complaints of generalized pain or pain in other parts of the body. They were under pain treatment, which was not changed during the period of psychotherapy and evaluation of this study. It consisted of antidepressants and physical treat-ments (heat packs and exercises).
Timeline Patients were individually evaluated and the weekly individual sessions lasted 50 minutes by a trained psychologist, with su-pervision of a psychologist with robust experience with orofacial pain. Duration of the treatment was individually determined, and the cases were discussed among the researchers after the ses-sions to establish the assessment. It included psychoanalysis, fa-miliar and systemic psychological approaches.
Diagnostic assessmentIn the beginning and in the end of psychotherapy, the patients were evaluated with:1. Visual analog scale to determine the pain intensity. Consists of a scale from zero to 10: zero represents no pain and 10 represents the worst possible pain.2. Beck Depression Inventory19 validated to the Portuguese lan-guage to determine depressive symptoms. Consists of 21 ques-tions that can be scored from zero to 3. According to the final score, the patient can be classified as having absent or minimum (zero-13), mild (14-19), moderate (20-28) or severe (29-63) de-pression.3. Beck Anxiety Inventory19 validated to the Portuguese language to determine anxious symptoms. Consists of 21 questions that can be scored from zero to 3. According to the final score, the patient can be classified as having absent or minimum (zero-13), mild (14-19), moderate (20-28) or severe (29-63) anxiety.4. Wisconsin Pain Inventory20 validated to the Portuguese lan-guage to determine pain limitations. 5. McGill Pain Questionnaire (short form)21 validated to the Portuguese language to determine pain descriptors. Consists of 15 items divided into 3 domains (sensitive, evaluative, and af-fective).6. Pain Catastrophizing Scale22 validated to the Portuguese lan-guage to determine thoughts, perceptions or feelings associated

174
BrJP. São Paulo, 2022 apr-jun;5(2):172-7 Yamaguchi MB, Oliveira MF and Siqueira SR
with the pain. Consists of 13 items with numeric scores from zero to 4 for each of them.
Clinical findings, therapeutic intervention, follow-up and outcomesClinical findings are presented individually for each case, including relevant past symptoms, as well as interventions and their outcomes. Similarly, types and administration of therapeutic intervention besi-des changes in therapeutic interventions with explanations.Additionally, clinician- and patient-assessed outcomes, impor-tant follow-up diagnostic and other test results are presented in this section.
Data analysisEach narrative was qualitatively analyzed and the comparison bet-ween the evaluations made before and after psychotherapy was included in the context of a phenomenological approach. Each patient showed specific demands that are presented in this study. Parts of the exact narrative of the patients were transcribed.
Case 1Woman, 55 years old, having had pain for more than 20 years, was diagnosed with burning mouth syndrome at the Orofacial Pain Clinic. Pain started after a surgery for dental implant. Burning was moderate during the day and got worse at night. Burning mouth syndrome is a neuropathic orofacial pain, more common in wo-men after menopause, and causes intense suffering and emotional impairment22. Although not having reported her beliefs about the origin of her pain, she has described fear of the invisible as some-thing with high impact in her perception of life. At the pain onset, she already had depression and an episode of hospitalization because of a suicide attempt by ingesting an ex-cessive quantity of drug (90 tablets of clonazepam). “I swallowed 90 clonazepam pills with no use, I do not think any more about killing myself because I am no worthy”. She attempted suicide to free herself from work because she could not stand the people there. It happened after 11 years of health leaves that kept her away from work sporadically, until finally she had to come back; then she retired on disability. Recently she has been diagnosed with bipolar disorder.She studied social sciences and worked for a little time in a hos-pital. “I stopped doing my job because I did not believe in what I was doing”. After that, she worked in the public sector in a position of trust. She had also been a secretary and police officer. She is single and lives with her parents. Her daily routine is to wake at 3h in the morning, keep lying down in bed until 6h am, walk the dog, go shopping at the market and the drugstore and come back. She has lunch at 11h am and often takes her parents to doctor appointments in the afternoon. She lays down to sleep at 6 pm. She has limited interests which include going out to eat at the bakery. She does not like physical activities because the pain gets worse.
Love relationshipsThe patient avoided talking about her affective relations, espe-cially love relationships. “I do not cry anymore, I have cried a lot
in my life, I have cried a lot for men”. Among the relationships, there was a disappointment with a boyfriend at college and an alcoholic man she lived with: “I wanted to be there because I did not want to come back to my home (parents’ house)”. After that, she was in love with a doctor she had worked with as a secretary but got disappointed. Currently, she is not in any love relationship because “after this burning I do not want to kiss, it makes me sick”.From the last boyfriend she got herpes papilloma virus. Since diagnosed, she has not treated it. She thinks she should treat it now to avoid cancer.
Family and friendsThis patient reported a terrible relationship with her father. “He is a religious fanatic, always saying that I am not a God’s person and that I am possessed”. She does not respond to these provoca-tions because she fears she will be injured. She considers her mo-ther a good person although the mother is too submissive to her father. “All he says, she accepts. She is on his side”. Her mother has cardiac disease, which worries her. She is afraid of her mother dying because she will miss her and will not be able to deal with that. She is worried about having to take care of her parents. “I will be the one who will have to take care, change diapers, take to the doctor, I don´t know if I can do that”. “I will do that because I will have to, if there was somebody else, I would like that”.She is the oldest daughter, and she cannot count on her sister or brother. “My sister lives in another state and my brother does not care”. They do not help her financially with the parents either. Other relatives are distant. There are no friends.She has a restricted social life. “I tried to go out and talk to people, I am always crying, it is useful. I like to stay in my room”. Although the psychologist has told her that activities help to manage pain, she does not want to do any. “I come here to treat my pain”. “I do not want to talk to others because my mouth burns, and I do not want to hear others complaining. I want to end this pain, only” She got a dog to help her lose her fear of being alone. “I am afraid of spirits”.
Self-descriptionShe describes herself as a woman who hardly smiles or laughs. She talks loudly and has bad temper, feels bad about being overweight, but does not do anything to change it. She does not take care of herself due to laziness. She prefers to lie in bed. Her hair is white, and she does not want to spend money with that. She prefers to spend the money with medicine. Before being retired, she liked to go shopping and was compulsive with that. “I’ve bought many things, I loved to buy clothes”. She takes laxatives every day. “I need to go to the toilet every day, otherwise I get sick”. She does not like to take a shower every day. She feels that the best would be to live in the hospital. “You have to enjoy when you are young, I do not see the world through rose-colored glasses”.
Behavior repertoire The behavior repertoire is limited with few reinforcements. The only positive ones are to go to the bakery and to come to therapy. Howe-ver, to go to the bakery is not always possible because it is expensive

175
Psychotherapy in the treatment of chronic refractory orofacial pain. Case reports
BrJP. São Paulo, 2022 apr-jun;5(2):172-7
for her. The main negative reinforcement is the father by whom she is afraid of being punished. The pain is the reason for why she does not go out, travel, or change the routine. She is very resistant to suggestions such as new activities, self-care, or social contact.
Psychotherapy results and pain alleviationAfter six weeks of psychotherapy and severe pain (pain intensity = 10), her pain intensity became 9. She started to make jokes, to use makeup and to smile. The initial and final scores can be ob-served in table 1. The depression scores did not change but there was a remarkable difference in the anxiety and catastrophizing scores. An increase in sensitive and evaluative McGill indexes is possibly associated with the attention given to pain issues during therapy, and it was associated with the increase in catastrophi-zing score. Wisconsin scores for humor, walking ability, work, personal relationships, sleep and enjoy life improved.
Case 2A 63-year-old man, retired, has had idiopathic trigeminal neu-ralgia for 23 years. He had treated it, and during the first 8 years, the pain was controlled, although there were several adverse effects. “You are and are not there, you get slow”. Trigeminal neuralgia is an excruciating paroxysmal shock-like pain, usually triggered by a light touch. He underwent four neurosurgeries. The last was 4 months ago and now the pain has been relieved. His routine is to wake up, do housekeeping, make woodcrafts and help the community he lives in.At the early stages of his pain, an intense crisis was associated with suicidal thoughts, of which he spoke about nervously. “I do not wish that pain to anyone; if I could I would have taken my life away”. He was in the bathroom and remained standing with his hands against the wall for hours. “I could not move; any movement caused pain”. He wanted to commit suicide but could not write a note to explain the reason.After the first surgery, he got depressed because his face became numb. “A person who has this type of pain loses 50% of their lives (…) I feel mutilated”.
Family, relationships, and self-descriptionChildhood was complicated and full of family problems, with the need to work since being a kid. He learned several jobs and now dedicates himself to his family and the community. He li-ves with his wife and has a good relationship with his sons. He described himself as being sensitive and full of hope. However, “people who live close to my house are negative”.
CopingHe has many plans and wants to start computer and chess cou-rses. He wants to meet new people in these courses. His feelings about the pain possibly reoccurring are contradicting: although he hopes the pain does not come back, at the same time he is afraid that happens.
Psychotherapy results and pain alleviationListening about the crisis was the assessment tool in this case. To avoid the expectation of new crises is the challenge for trigeminal
neuralgia patients. The scores for pain intensity, depression, an-xiety, Wisconsin, McGill, and catastrophizing decreased (Table 1). Accepting the condition and developing an action plan in case the pain returns were the contents developed.
Case 3A married woman aged 36 years old has had trigeminal neu-ralgia crises for 10 months. At the diagnosis, she also fulfilled the criteria for multiple sclerosis, which characterized secondary trigeminal neuralgia. Multiple sclerosis is a neurodegenerative autoimmune disease that can present demyelination at the entry zone of the trigeminal root, as it happens in this case23. Emo-tional stress and weather variations can trigger crises and this patient showed several familiar issues to be assessed. Her routine is to wake up early and work at a public service in the mornings, prepare lunch for three kids and her husband, and in the after-noon help her husband at work. He is a school bus driver. At night, she does some housekeeping.
Familiar relationshipsHer oldest son is 15 years old. He is from a previous marriage. Her daughter is 10 years old, and the younger son is 6 years old. She complained about difficulties in the relationship between her current husband and the older boy “although they know each other for a long time”. “I got separated from my first husband when he was 1 year old, they are always arguing”. She thinks her husband is too much demanding, especially with the older one. “I always feel my face burning when they fight. It happens always when they are both at home”. This son had problems with drugs at school at the same time as the biological father started to have a relationship with him. Af-ter that, his father disappeared. He changed schools and failed a year. The current husband speaks too loudly, which is one of the reasons for arguing. She thinks her marriage is great and there are rare arguments about the relationship. The arguments are about the son. “He (husband) misses my attention, but I do not like to demonstrate my love. I have this same difficulty with my older son too”. She wanted a closer relationship with both, especially the husband. The older son is lazy with home tasks, and she does them for him to avoid the arguments. Once, one argument tur-ned into a pain crisis. “I went to bed and cried; my husband does not believe in my symptoms”.
Self-descriptionAt 14 years old, her father died, and she became independent. She worked since a young age and had her first son with only 21 years old. Disagreements were the cause of separation and divorce. “I was sensitive and accepted what the others told me to do”. She cried when her husband yelled at her and was very insecure and shy. “After this diagnosis, I am not so submissive anymore”.
Psychotherapy results and pain alleviationListening to complaints and working on family communication were the strategies in this case. A pain diary was also created to find out the relation between the crises and other issues24. She
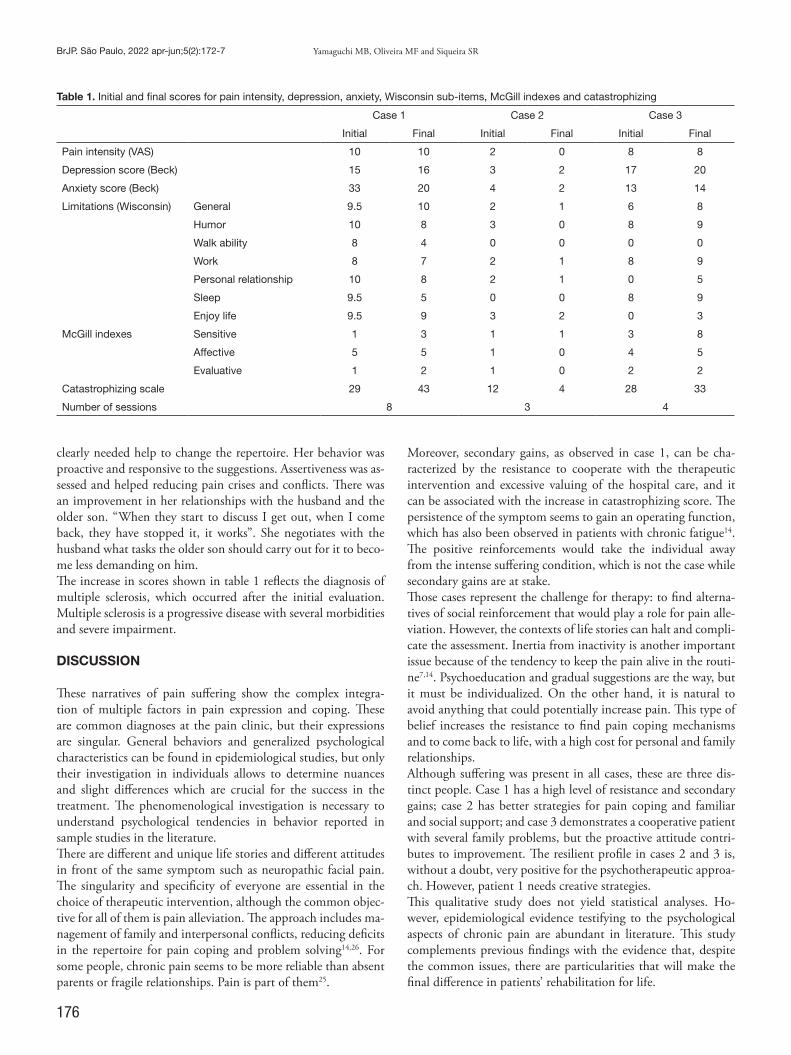
176
BrJP. São Paulo, 2022 apr-jun;5(2):172-7 Yamaguchi MB, Oliveira MF and Siqueira SR
clearly needed help to change the repertoire. Her behavior was proactive and responsive to the suggestions. Assertiveness was as-sessed and helped reducing pain crises and conflicts. There was an improvement in her relationships with the husband and the older son. “When they start to discuss I get out, when I come back, they have stopped it, it works”. She negotiates with the husband what tasks the older son should carry out for it to beco-me less demanding on him.The increase in scores shown in table 1 reflects the diagnosis of multiple sclerosis, which occurred after the initial evaluation. Multiple sclerosis is a progressive disease with several morbidities and severe impairment.
DISCUSSION
These narratives of pain suffering show the complex integra-tion of multiple factors in pain expression and coping. These are common diagnoses at the pain clinic, but their expressions are singular. General behaviors and generalized psychological characteristics can be found in epidemiological studies, but only their investigation in individuals allows to determine nuances and slight differences which are crucial for the success in the treatment. The phenomenological investigation is necessary to understand psychological tendencies in behavior reported in sample studies in the literature. There are different and unique life stories and different attitudes in front of the same symptom such as neuropathic facial pain. The singularity and specificity of everyone are essential in the choice of therapeutic intervention, although the common objec-tive for all of them is pain alleviation. The approach includes ma-nagement of family and interpersonal conflicts, reducing deficits in the repertoire for pain coping and problem solving14,26. For some people, chronic pain seems to be more reliable than absent parents or fragile relationships. Pain is part of them25.
Moreover, secondary gains, as observed in case 1, can be cha-racterized by the resistance to cooperate with the therapeutic intervention and excessive valuing of the hospital care, and it can be associated with the increase in catastrophizing score. The persistence of the symptom seems to gain an operating function, which has also been observed in patients with chronic fatigue14. The positive reinforcements would take the individual away from the intense suffering condition, which is not the case while secondary gains are at stake.Those cases represent the challenge for therapy: to find alterna-tives of social reinforcement that would play a role for pain alle-viation. However, the contexts of life stories can halt and compli-cate the assessment. Inertia from inactivity is another important issue because of the tendency to keep the pain alive in the routi-ne7,14. Psychoeducation and gradual suggestions are the way, but it must be individualized. On the other hand, it is natural to avoid anything that could potentially increase pain. This type of belief increases the resistance to find pain coping mechanisms and to come back to life, with a high cost for personal and family relationships. Although suffering was present in all cases, these are three dis-tinct people. Case 1 has a high level of resistance and secondary gains; case 2 has better strategies for pain coping and familiar and social support; and case 3 demonstrates a cooperative patient with several family problems, but the proactive attitude contri-butes to improvement. The resilient profile in cases 2 and 3 is, without a doubt, very positive for the psychotherapeutic approa-ch. However, patient 1 needs creative strategies.This qualitative study does not yield statistical analyses. Ho-wever, epidemiological evidence testifying to the psychological aspects of chronic pain are abundant in literature. This study complements previous findings with the evidence that, despite the common issues, there are particularities that will make the final difference in patients’ rehabilitation for life.
Table 1. Initial and final scores for pain intensity, depression, anxiety, Wisconsin sub-items, McGill indexes and catastrophizing
Case 1 Case 2 Case 3
Initial Final Initial Final Initial Final
Pain intensity (VAS) 10 10 2 0 8 8
Depression score (Beck) 15 16 3 2 17 20
Anxiety score (Beck) 33 20 4 2 13 14
Limitations (Wisconsin) General 9.5 10 2 1 6 8
Humor 10 8 3 0 8 9
Walk ability 8 4 0 0 0 0
Work 8 7 2 1 8 9
Personal relationship 10 8 2 1 0 5
Sleep 9.5 5 0 0 8 9
Enjoy life 9.5 9 3 2 0 3
McGill indexes Sensitive 1 3 1 1 3 8
Affective 5 5 1 0 4 5
Evaluative 1 2 1 0 2 2
Catastrophizing scale 29 43 12 4 28 33
Number of sessions 8 3 4

177
Psychotherapy in the treatment of chronic refractory orofacial pain. Case reports
BrJP. São Paulo, 2022 apr-jun;5(2):172-7
CONCLUSION
This study showed that psychotherapy had a remarkable impact in the life of patients as well as in the cooperation with pain treatments, even in a less resilient patient. While assessing in-dividual profiles and particularities of each case, it is possible to help patients have a proactive attitude and to understand their role in their condition.
AUTHORS’ CONTRIBUTIONS
Marianna Barbosa Yamaguchi Data Collection, Research Maria de Fatima Vidotto Oliveira Supervision Silvia Regina DT de Siqueira Project Management, Methodology, Writing - Preparation of the original, Writing - Review and Editing, Supervision
REFERENCES
1. Bernacchio RMG, Contin I, Mori M. Modifying factors of pain perception. Rev Dor 2005;3:621-33.
2. Von Korff M, Dworkin SF, Le Resche L, Kruger A. An epidemiologic comparison of pain complaints. Pain. 1988;32(2):173-83.
3. Nickel R, Raspe HH. Chronic pain: epidemiology and health care utilization. Nerve-narzt. 2001;72(12):897-906.
4. Watkins EA, Wollan PC, Melton LJ 3rd, Yawn BP. A population in pain: report from the Olmsted Country health study. Pain Med. 2008;9(2):166-74.
5. Oliveira SB, de Siqueira SR, Sanvovski AR, do Amaral LM, de Siqueira JT. Tempo-romandibular disorder in Brazilian patients: a preliminary study. J Clin Psychol Med Settings. 2008;15(4):338-43.
6. Castro AR, Siqueira SR, Perissinotti DM, Teixeira MJ, Siqueira JT. Emotional aspects of chronic orofacial pain and surgical treatment. Int J Surg. 2009;7(3):196-9.
7. Dagsdóttir LK, Skyt I, Vase L, Baad-Hansen L, Castrillon E, Svensson P. Reports of perceptual distortion of the face are common in patients with different types of chro-nic orofacial pain. J Oral Rehabil. 2016;43(6):409-16.
8. de Siqueira SR, Teixeira MJ, de Siqueira JT. Somatosensory investigation of pa-tients with orofacial pain compared with controls. J Neuropsychiatry Clin Neurosci. 2014;26(4):376-81.
9. Schestatsky P, Ehlers JA, Ehlers BC. Neuropathic pain. In: Chaves MLF, Finkelsztejn A, Stefani MA. Eds. Routines in neurology and neurosurgery. Porto Alegre: Artmed. 2009. 757-67p.
10. Zakrzewska JM. Multi-dimensionality of chronic pain of the oral cavity and face. J Headache Pain. 2013;14(1):37.
11. Reddy GD, Viswanathan A. Trigeminal and glossopharyngeal neuralgia. Neurol Clin. 2014;32(2):539-52.
12. Nasri C, Teixeira MJ, Okada M, Formigoni G, Heir G, Siqueira JT. Burning mouth complaints: clinical characteristics of a Brazilian sample. Clinics. 2007;62(5):561-6.
13. Bonathan CJ, Zakrzewska JM, Love J, Williams AC. Beliefs and distress about oro-facial pain: patient journey through a specialist pain consultation. Oral Facial Pain Headache. 2014;28(3):223-32.
14. Wielenska RC, Banaco RA. Chronic fatigue syndrome: antibehavior perspective of a case. Themes Psychol. 2010;18:415-24.
15. Schönenberg M, Mares L, Smolka R, Jusyte A, Zipfel S, Hautzinger M. Facial affect perception and mentalizing abilities in female patients with persistent somatoform pain disorder. Eur J Pain. 2014;18(7):949-56.
16. Vanderberghe L. Pain behavior. In: Portnoi AG. Ed. Pain psychology. São Paulo: Gua-nabara Koogan. 2014; 15-31p.
17. Goldthorpe J, Peters S, Lovell K, McGowan L, Aggarwal V. ‘I just wanted someone to tell me it wasn’t all in my mind and do something for me’: Qualitative exploration of acceptability of a CBT based intervention to manage chronic orofacial pain. Br Dent J. 2016;220(9):459-63.
18. Gagnier JJ, Kienle G, Altman DG, Moher D, Sox H, Riley DS, CARE Group. The CARE Guidelines: Consensus-based Clinical Case Reporting Guideline Develop-ment.
19. Gorenstein C, Andrade L. Validation of a Portuguese version of the Beck Depression Inventory and the state-trait anxiety inventory in Brazilian subjects. Braz J Med Biol Res. 1996;29(4):453-57.
20. Teixeira MJ, Yeng LT. Pain evaluation. In: Teixeira MJ. Pain: clinical manual. São Paulo: Ateneu; 2006. 25-38p.
21. Menezes Costa Lda C, Maher CG, McAuley JH, Hancock MJ, de Melo Oliveira W, Azevedo DC, et al. The Brazilian-Portuguese versions of the McGill Pain Question-naire were reproducible, valid, and responsive in patients with musculoskeletal pain. J Clin Epidemiol. 2011;64(8):903-12.
22. Azevedo F, Pereira A, Dias C, Agualusa L, Lemos L, Romão J, et al. Translation, cultu-ral adaptation and multicentric study for validation of instruments for the evaluation of chronic pain. Rev Dor. 2007;15(1):6-56.
23. Nery S, Lauria RA, Sarmento VA, Oliveira MGA. Evaluation of anxiety and depres-sion in patients at the third age and the association with burning mouth syndrome. Rev Cir Med Biol. 2004;3(1):20-9.
24. Finkelsztejn A. Multiple sclerosis. In Chaves, MLF, Finkelsztejn A, Stefani MA. Eds. Routines in neurology and neurosurgery. Porto Alegre: Artmed; 2009. 351-62p.
25. Oliveira MFV. Psychotherapy in the treatment of facial chronic pain: clinical dis-cussion. In: Siqueira JT, Teixeira MJ. Eds. Orofacial pain: diagnosis, treatment and quality of life. Curitiba: Editora Maio, 2001; 149-55p.
26. Mundle R. A narrative analysis of spiritual distress in geriatric physical rehabilitation. J Health Psychol. 2015;20(3):273-85.

178
BrJP. São Paulo, 2022 apr-jun;5(2):178-82
ABSTRACT
BACKGROUND AND OBJECTIVES: The design of research with monozygotic twins discordant for the disease has emerged as a powerful tool for the detection of phenotypic risk factors. The aim of this study is to report a clinical case of monozygo-tic twins discordant for pain-related temporomandibular joint disorder (TMD) from a cognitive-behavioral-emotional phe-notypic analysis, from the comparison of clinical variables of pain, history of exposure to painful procedures in early chil-dhood, and coping with pain.CASE REPORT: TMD-Twin presented a diagnosis of painful (myofascial pain with referral) and joint (disk displacement with reduction) TMD according to the criteria of the DC/TMD. Control-Twin did not show TMD, however she presented other chronic pains. TMD-Twin showed reduced pressure pain thre-shold, hyperalgesia in trigeminal and extra-trigeminal regions compared to the Control-Twin. TMD-Twin was more exposed to painful procedures and emotional events due to congenital heart problems. Both had central sensitization based on the Central Sensitization Inventory, although TMD-Twin had more catastrophic thoughts about pain. TMD-Twin presented an in-ternal locus of control.CONCLUSION: Both monozygotic twins presented a chronic pain phenotype, although they were discordant with the TM-
Phenotypic analysis of discordant monozygotic twins for pain-related temporomandibular joint disorder. Case reportAnálise fenotípica de gêmeas monozigóticas discordantes para disfunção temporomandibular dolorosa. Relato de caso
Lais Valencise Magri1,2,3, Melissa de Oliveira Melchior1,4, Graziela Valle da-Silva4, Edilaine Cristina Silva Gherardi-Donato4, Christie Ramos Andrade Leite-Panissi3
Lais Valencise Magri – https://orcid.org/0000-0001-8050-4396;Melissa de Oliveira Melchior – https://orcid.org/0000-0003-4943-1242;Graziela Valle da-Silva – https://orcid.org/0000-0003-7045-5655;Edilaine Cristina Silva Gherardi-Donato – https://orcid.org/0000-0001-7475-6650;Christie Ramos Andrade Leite-Panissi – https://orcid.org/0000-0003-1762-2730.
1. University of São Paulo, Dentistry School, Department of Restorative Dentistry, Ribeirão Preto, SP, Brazil.2. University of Ribeirão Preto, Dentistry Course, Ribeirão Preto, SP, Brazil.3. University of São Paulo, Faculty of Philosophy, Sciences and Letters, Ribeirão Preto, SP, Brazil.4. University of São Paulo, Nursing School, Psychiatric Nursing Department - - PAHO/WHO Collaborating Centre for Nursing Research Development, Ribeirão Preto, SP, Brazil.
Submitted on December 15, 2021.Accepted for publication on April 08, 2022.Conflict of interests: none – Sponsoring sources: none.
Correspondence to: Lais Valencise Magri E-mail: [email protected] [email protected]
© Sociedade Brasileira para o Estudo da Dor
D-related pain. The main differences were the lower pressu-re pain threshold and higher hyperalgesia locally presented by TMD-Twin. The internal locus of control indicates greater pain sensitivity, with better coping of the painful experience for the TMD-Twin. One possible explanation for this clinical condition can be that painful experiences in early childhood have shaped a phenotype of greater sensitivity with better coping and resilience to the painful condition.Keywords: Chronic pain, Facial pain, Monozygotic twin, Tem-poromandibular joint disorders, Central nervous system sensi-tization.
RESUMO
JUSTIFICATIVA E OBJETIVOS: O desenho da pesquisa com gêmeos monozigóticos discordantes para a doença surgiu como uma ferramenta poderosa para a detecção de fatores de risco fenotípicos. O objetivo deste estudo foi relatar um caso clíni-co de gêmeas monozigóticas discordantes para disfunção tem-poromandibular (DTM) dolorosa a partir de análise fenotípica cognitivo-comportamental-emocional entre elas, por meio de comparação de variáveis clínicas de dor, histórico de exposição a procedimentos dolorosos na primeira infância e enfrentamento de dor (autoeficácia e locus de controle). RELATO DOCASO: A gêmea-DTM apresentou diagnóstico de DTM dolorosa (dor miofascial com referência) e articular (des-locamento do disco com redução) segundo os critérios do DC/TMD. A gêmea-controle não apresentou DTM, contudo apre-sentou manifestação clínica de outras dores crônicas. A gêmea--DTM apresentou limiar de dor à pressão reduzido, hiperalgesia em regiões trigeminais/extra-trigeminais quando comparados à gêmea-controle, que na primeira infância foi mais exposta a procedimentos dolorosos devido a problemas cardíacos congê-nitos. Ambas apresentaram sensibilização central de acordo com o Inventário de Sensibilização Central, embora a gêmea-DTM apresentou mais pensamentos catastróficos sobre a dor. A gêmea--DTM apresentou locus de controle interno. CONCLUSÃO: Ambas as gêmeas apresentaram fenótipo de dor crônica, apesar do fato de serem discordantes para a DTM. Den-tre as avaliações, as que mais diferiram entre o par foram o baixo limiar de dor à pressão e hiperalgesia local presentes na gêmea com DTM. O Iocus de controle interno associado à maior sensi-bilidade indicou melhor enfrentamento da experiência dolorosa para a gêmea-DTM. Uma possível explicação para esta manifes-
DOI 10.5935/2595-0118.20220021
CASE REPORT

179
Phenotypic analysis of discordant monozygotic twins for pain-related temporomandibular joint disorder. Case report
BrJP. São Paulo, 2022 apr-jun;5(2):178-82
tação clínica está pautada na hipótese de que experiências dolo-rosas na primeira infância vivenciadas por ela tenham moldado um fenótipo de maior sensibilidade com melhor enfrentamento e resiliência frente à condição dolorosa.Descritores: Dor crônica, Dor facial, Gêmeos monozigóticos, Síndrome da disfunção da articulação temporomandibular, Sen-sibilização do sistema nervoso central.
INTRODUCTION
Temporomandibular disorder (TMD) can be understood as an orofacial musculoskeletal pain syndrome, which mainly affects women. It is characterized by orofacial signs and symptoms, usually easy to manage and/or self-resolving. However, a portion of the population develops an imbalance in the endogenous pain modulation system, resulting in challenging management. In these cases, the association of multisystem alterations, changes in behavior, emotional status, and social interactions are frequently observed1-3. Therefore, TMD symptoms must be understood as a complex and specific individual response, with individualized signs and symptoms, which can be amplified or attenuated, de-pending on the genetic composition and epigenetic factors4-7.Studies about twins have played an essential role in estimating the hereditary fraction of hundreds of phenotypic characteristics and pathological conditions. The design of research with mono-zygotic twins (MZ) discordant for the disease has emerged as a powerful tool for the detection of phenotypic risk factors, as it allows for the reduction of a range of unknown confounding fac-tors, typically found in population studies, especially concerning research with epigenetics8. MZ twins share a common genotype, whereas the most are not identical. Several types of phenotypic disagreement can be observed, such as differences in disease sus-ceptibility and a wide range of anthropomorphic characteristics. There are several possible explanations for these observations, but one of them is the existence of epigenetic differences9,10.Considering the complexity of factors involved in the manifes-tation of TMD, the aim of this article is to report a clinical case of MZ twins discordant for pain-related TMD from the cog-nitive-behavioral-emotional phenotypic analysis between them, the comparison of clinical pain variables, history of exposure to painful procedures in early childhood and coping with pain (sel-f-efficacy and locus control).
CASE REPORT
This case report is part of a research approved by the Ethics Re-search Committee of the Faculty of Philosophy, Sciences and Letters – Ribeirão Preto (São Paulo University) under CAAE protocol 98129918.6.0000.5407. CaRe (Case Report) guideli-ne was used to prepare this manuscript and guarantee accuracy, transparency, and usefulness of case reports11.
Patient informationTwins 1 and 2, 20 years old, monozygotic identical, university students, single, living in the same family from birth to the pre-sent time.
Primary concerns/symptoms and clinical findingsTwin 1 presented a diagnosis of painful (myofascial pain with re-ferral) and joint (disk displacement with reduction) TMD accor-ding to the Diagnostic Criteria for Temporomandibular Disor-ders (DC/TMD – Brazilian Portuguese version)12. In addition, she reported a history of recurrent otitis and difficulties in speech development, however she did not suffer any injury in the TMJ region during childbirth. Twin 2 did not present TMD according to the same clinical evaluation protocol, but reported a painful condition for appro-ximately 10 years, including the paranasal sinuses, temples close to the eyes, the frontal region of the head, and trapezius muscles. She also reported to having restless legs syndrome and polycystic ovary.
TimelineTwin 1 (TMD-twin) reported she had a congenital heart condi-tion, and due to this, during her early childhood, she underwent three cardiac surgeries. In addition, she had a low birth weight and was kept in the incubator for two months. Such health con-ditions exposed her to more painful procedures (surgeries, sutu-res, venous access, injections, among others) and salient emotio-nal events (incubator, hospitalization, among others) than Twin 2 (control-twin).
Diagnostic assessment and methodsThe twins were evaluated according to: • Oral Behavior Checklist - Brazilian Portuguese version1,13: scores sum for both was high, totaling 29 for the twin with pain-related TMD and 32 for the control-twin (Table 1). According to the total scores, both twins presented possible awake bruxism. • Pressure pain threshold (PPT) in trigeminal areas (anterior temporalis, masseter, and TMJ) and extra-trigeminal areas (tra-pezius, lateral epicondyle, and knee) were compared bilaterally (IDDK digital compression algometer™, Kratos, Cotia, São Paulo, Brazil): TMD-twin had lower PPT for all areas evaluated compared to the control-twin, that is, more sensitivity to pain in trigeminal and extra trigeminal areas (Figure 1).• Presence of hyperalgesia was also analyzed with the same algo-meter. A constant compression (5 seconds) of 1.5 kg/f in each trigeminal point and 2 kg/f in each extra-trigeminal point was applied. A score representing the perceived intensity of pain felt was requested (VAS - zero to 10). TMD-twin reported greater pain intensity during the exam, especially in the trigeminal areas and in the trapezius, region compared to the control-twin, indi-cating a higher level of hyperalgesia14 (Figure 2).• Brief Pain Inventory (BPI - Reduced Version, in Portuguese15): the scores are represented by the mean of the values assigned in each dimension of perception (Table 2).• Locus of Control Pain Scale - Form C (PLOC-C, Portuguese version16): it was observed that the TMD-twin had a higher internal locus of control and in other people (relatives, friends) than the control-twin, with the same locus of control being equal between them at random and other health professionals (Table 2).
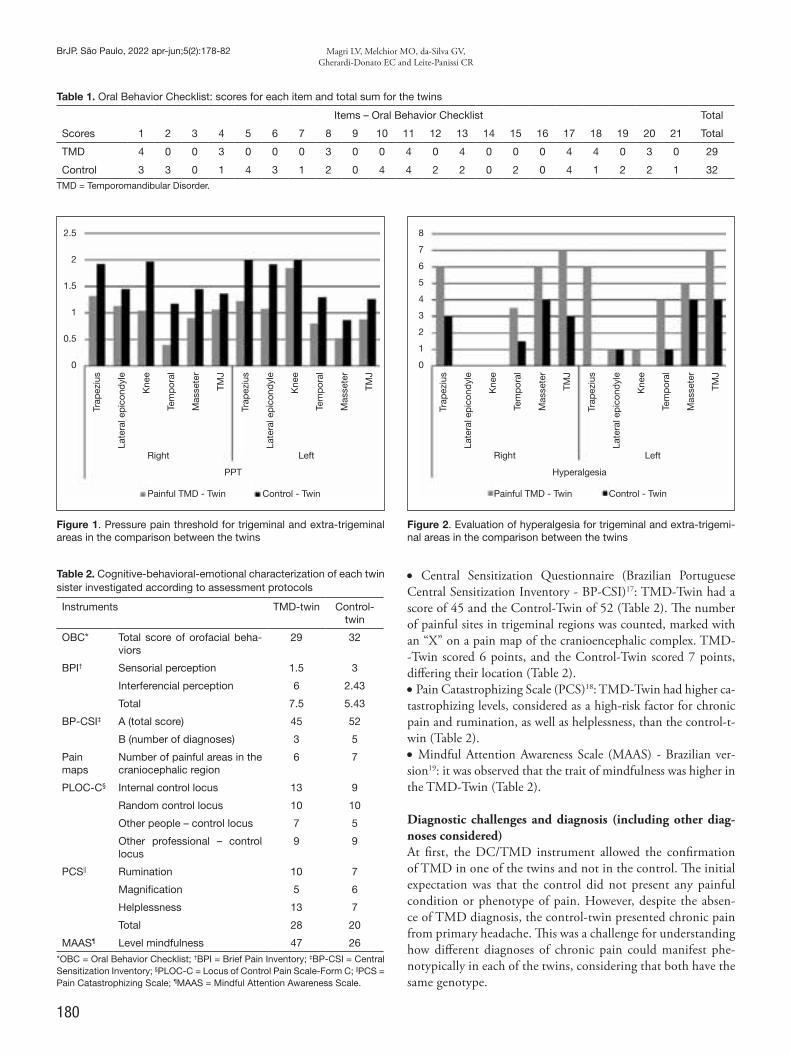
180
BrJP. São Paulo, 2022 apr-jun;5(2):178-82 Magri LV, Melchior MO, da-Silva GV, Gherardi-Donato EC and Leite-Panissi CR
Table 1. Oral Behavior Checklist: scores for each item and total sum for the twins
Items – Oral Behavior Checklist Total
Scores 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 Total
TMD 4 0 0 3 0 0 0 3 0 0 4 0 4 0 0 0 4 4 0 3 0 29
Control 3 3 0 1 4 3 1 2 0 4 4 2 2 0 2 0 4 1 2 2 1 32TMD = Temporomandibular Disorder.
Table 2. Cognitive-behavioral-emotional characterization of each twin sister investigated according to assessment protocols
Instruments TMD-twin Control-twin
OBC* Total score of orofacial beha-viors
29 32
BPI† Sensorial perception 1.5 3
Interferencial perception 6 2.43
Total 7.5 5.43
BP-CSI‡ A (total score) 45 52
B (number of diagnoses) 3 5
Pain maps
Number of painful areas in the craniocephalic region
6 7
PLOC-C§ Internal control locus 13 9
Random control locus 10 10
Other people – control locus 7 5
Other professional – control locus
9 9
PCS|| Rumination 10 7
Magnification 5 6
Helplessness 13 7
Total 28 20
MAAS¶ Level mindfulness 47 26
*OBC = Oral Behavior Checklist; †BPI = Brief Pain Inventory; ‡BP-CSI = Central Sensitization Inventory; §PLOC-C = Locus of Control Pain Scale-Form C; ||PCS = Pain Catastrophizing Scale; ¶MAAS = Mindful Attention Awareness Scale.
Figure 1. Pressure pain threshold for trigeminal and extra-trigeminal areas in the comparison between the twins
Figure 2. Evaluation of hyperalgesia for trigeminal and extra-trigemi-nal areas in the comparison between the twins
Trap
eziu
s
Late
ral e
pic
ond
yle
Kne
e
Tem
por
al
Mas
sete
r
TMJ
Trap
eziu
s
Late
ral e
pic
ond
yle
Kne
e
Tem
por
al
Mas
sete
r
TMJ
PPT
Right Left
Painful TMD - Twin Control - Twin
2.5
2
1.5
1
0.5
0
Trap
eziu
s
Late
ral e
pic
ond
yle
Kne
e
Tem
por
al
Mas
sete
r
TMJ
Trap
eziu
s
Late
ral e
pic
ond
yle
Kne
e
Tem
por
al
Mas
sete
r
TMJ
Hyperalgesia
Right Left
Painful TMD - Twin Control - Twin
8
7
6
5
4
3
2
1
0
• Central Sensitization Questionnaire (Brazilian Portuguese Central Sensitization Inventory - BP-CSI)17: TMD-Twin had a score of 45 and the Control-Twin of 52 (Table 2). The number of painful sites in trigeminal regions was counted, marked with an “X” on a pain map of the cranioencephalic complex. TMD--Twin scored 6 points, and the Control-Twin scored 7 points, differing their location (Table 2).• Pain Catastrophizing Scale (PCS)18: TMD-Twin had higher ca-tastrophizing levels, considered as a high-risk factor for chronic pain and rumination, as well as helplessness, than the control-t-win (Table 2). • Mindful Attention Awareness Scale (MAAS) - Brazilian ver-sion19: it was observed that the trait of mindfulness was higher in the TMD-Twin (Table 2).
Diagnostic challenges and diagnosis (including other diag-noses considered)At first, the DC/TMD instrument allowed the confirmation of TMD in one of the twins and not in the control. The initial expectation was that the control did not present any painful condition or phenotype of pain. However, despite the absen-ce of TMD diagnosis, the control-twin presented chronic pain from primary headache. This was a challenge for understanding how different diagnoses of chronic pain could manifest phe-notypically in each of the twins, considering that both have the same genotype.

181
Phenotypic analysis of discordant monozygotic twins for pain-related temporomandibular joint disorder. Case report
BrJP. São Paulo, 2022 apr-jun;5(2):178-82
DISCUSSION
Identical (monozygotic) twins have always intrigued resear-chers since they have the same genotype at birth, and they de-velop different phenotypes throughout their lives, becoming completely different individuals. In the last decade, several stu-dies with discordant monozygotic twins have been published, as with this methodology, it is possible to establish a case-con-trol study design in which a series of variables are controlled, as they are shared between the siblings: genetic material, social environment (if raised by the same family), age, gender, among many others20-22.TMD-twin had greater pain sensitivity (lower PPT) and hype-ralgesia in trigeminal and extra-trigeminal areas when com-pared to the control-twin, indicating a picture of generalized chronic pain3. These findings point to the fact that the noci-ceptive experience goes beyond inherited genetic components and is modulated by a series of biopsychosocial variables, such as attention, assessment with cognitive and emotional meaning attribution of perceived sensations, the role of the disease in re-lation to social norms and expectations and behavior, often ma-ladaptive2. Reduced PPT and hyperalgesia were also identified in regions not affected by painful TMD, indicating a lack of modulation and descending pain control. Added to this, scores for the CSI questionnaire for both suggest central sensitization of the pain system, which justifies the presence of pain referred to palpation found in the TMD-twin.Complementarily, the painful TMD-twin had a total BPI and interferential pain perception score with higher values than the control-twin, but with a lower level of pain sensory perception, representing a cognitive interpretation of the pain experience perhaps indicating greater resilience acquired by previous pain-ful experiences. Perhaps, in this case, the difference was the exposure to several painful procedures in early childhood to which the TMD-twin was submitted. In this case, it is inte-resting to note that sensory intensity of pain was inversed to the perception of interference in the twins’ lives. The one with greater sensory perception (control-twin) scored less percep-tion of interference, and the one with less sensory perception had a greater perception of pain interference in daily activities (TMD-twin), corroborating the concept of multidimensiona-lity of the painful experience.It was observed that the TMD-twin had more catastrophic thoughts related to rumination and helplessness, with scores that suggest a high risk for painful chronicity. The rumination factor seems to be related to the subject’s excessive attention to the painful event and the helplessness factor related to a self-as-sessment of inability to deal with this threat value. Magnifica-tion, on the other hand, with a high score for the control-twin according to the 75th percentile previously established, concer-ns the magnitude of importance attributed to the possible risks of worsening the condition, reiterating the idea that she is also a chronic pain patient, although it is not manifesting in the stomatognathic system23,24.Locus of pain control was similar between the twins, differing mainly in the locus of internal control dimension, higher for
the TMD-twin. This demonstrates internal accountability to deal with the pain greater than the control-twin. Perhaps the more pronounced mindfulness trait can contribute to a more autonomous and optimistic coping with managing one’s own body, while it can also lead to thoughts fixed on the painful state and its expectation of improvement or worsening, related to catastrophizing of pain. It is possible that the increase or de-crease in pain is also related to attention, depending on where the focus is directed. In this case, mindfulness-based interven-tion would contribute by providing training in non-judgment and equanimity of attention to different bodily sensations, for example25,26.Knowing the levels of the mindfulness trait in people with pain-ful TMD can elucidate, at least in part, the level of awareness about thoughts and behaviors and internal processes resulting from the presence of pain. Furthermore, it also brings a posi-tive perspective to the management of chronic painful TMD, contemplating the biopsychosocial model, with neurophysio-logical and epigenetic results18,19. A higher level of mindfulness trait was observed in the TMD-twin, where the rumination factor seems to be related to the subject’s excessive attention to the painful event and the helplessness factor related to a self-as-sessment of inability to deal with the threat value, both presen-ted by her as well18,27. With a broader view, this multisystem deregulation of the orga-nism leads to its internal imbalance, that is, to illness, in whi-ch the perception of pain, accompanied by the attribution of cognitive and emotional meaning, is the main motivation for seeking professional help27. On the other hand, this professio-nal help has its role well-performed when the gaze turns to pain control and to alleviating the suffering of those who seek it, to alleviate primary symptoms and prevent the consequences of unrelieved pain, since a delay in healing can depress the immu-ne system28,29.The strengths of this case are related to the possibility of applying specific instruments to analyze a cognitive-behavior--emotional model linked to chronic pain conditions. But there were limitations related to the absence of genetics and epigene-tics analyses, which could clarify specific characteristics in the DNA of each twin.
CONCLUSION
This case report shows that although the twins are discordant for painful TMD, the control-twin also has a chronic pain phe-notype, based on this cognitive-behavioral-emotional analysis. Among the assessments performed, the greater difference bet-ween the pair were the pressure pain threshold and hyperalge-sia of trigeminal and extra-trigeminal regions, and the locus of internal control, which indicates greater pain sensitivity, with better coping of the painful experience for the TMD-twin. The genetic and epigenetic analysis could highlight other specifici-ties of these manifestations. This study hypothesizes that ex-posure to painful experiences in early childhood has made the TMD-Twin more sensitized and molded her coping of the pain experience of TMD.

182
BrJP. São Paulo, 2022 apr-jun;5(2):178-82 Magri LV, Melchior MO, da-Silva GV, Gherardi-Donato EC and Leite-Panissi CR
AUTHORS’ CONTRIBUTIONS
Lais Valencise Magri Data Collection, Research, Methodology, Writing - Review and Editing Melissa de Oliveira Melchior Data Collection, Project Management, Research, Writing - Pre-paration of the original Graziela Valle da-Silva Data Collection, Writing - Preparation of the original Edilaine Cristina Silva Gherardi-Donato Conceptualization, Project Management, Writing - Review and Editing Christie Ramos Andrade Leite-Panissi Conceptualization, Project Management, Methodology, Writing - Review and Editing
REFERENCES
1. Ohrbach R, Dworkin SF. The Evolution of TMD Diagnosis: Past, Present, Future. J Dent Res 2016;95(10):1093-101.
2. Slade GD, Ohrbach R, Greenspan JD, Fillingim RB, Bair E, Sanders AE, et al. Painful Temporomandibular Disorder: Decade of Discovery from OPPERA Studies. J Dent Res. 2016;95(10):1084-92.
3. Sessle BJ. Chronic orofacial pain: models, mechanisms, and genetic and related envi-ronmental influences. Int J Mol Sci. 2021;22(13):7112.
4. Diatchenko L, Anderson AD, Slade GD, Fillingim RB, Shabalina SA, Higgins TJ, et al. Three major haplotypes of the beta2 adrenergic receptor define psychological profile, blood pressure, and the risk for development of a common musculoskeletal pain disorder. Am J Med Genet B Neuropsychiatr Genet. 2006;141B(5):449-62.
5. Meloto CB, Serrano PO, Ribeiro Dasilva MCR, Rizzatti-Barbosa C. Genomi-cs and the new perspectives for temporomandibular disorders. Arch Oral Biol. 2011;56(11)1181-9.
6. Smith SB, Maixner DW, Greenspan JD, Dubner R, Fillingim RB, Ohrbach, R et al. Potential genetic risk factors for chronic TMD: genetic associations from the OPPE-RA case control study. J Pain. 2011;12(11):T92-T101.
7. Nissenbaum J, Devor M, Seltzer Z, Gebauer M, Michaelis M, Tal M, et al. Suscep-tibility to chronicpain following nerve injury is genetically affected by CACNG2. Genome Res. 2010;20(9):1180-90.
8. Vitaro F, Brendgen M, Arseneault L. The discordant MZ twin method: one step closer to the holy grail of causality. Int J Behav Dev. 2009;33:376-82.
9. Kuratomi G, Iwamoto K, Bundo M, Kusumi I, Kato N, Iwata N, et al. Aberrant DNA methylation associated with bipolar disorder identified from discordant monozygotic twins. Mol Psychiatry. 2008;13(4):429-41.
10. Bell JT, Spector TD. A twin approach to unravelling epigenetics. Trends Genet. 2011;27(3):116-25.
11. Riley DS, Barber MS, Kienle GS, Aronson JK, von Schoen-Angerer T, Tugwell P, Kie-ne H, Helfand M, Altman DG, Sox H, Werthmann PG, Moher D, Rison RA, Sham-seer L, Koch CA, Sun GH, Hanaway P, Sudak NL, Kaszkin-Bettag M, Carpenter JE, Gagnier JJ. CARE guidelines for case reports: explanation and elaboration document. J Clin Epidemiol. 2017 May 18. pii: S0895-4356(17)30037-9.
12. Ohrbach R, editor. Diagnostic Criteria for Temporomandibular Disorders: Assess-ment Instruments. Version 15 May 2016. [Critérios de Diagnóstico para Desordens Temporomandibulares: Protocolo Clínico e Instrumentos de Avaliação: Brazilian Por-tuguese Version 25 May 2016] Pereira Jr. FJ, Gonçalves DAG, Trans. www.rdc-tmdin-ternational.org Accessed on 27 Oct 2021.
13. Barbosa C, Manso MC, Reis T, Soares T, Gavinha S, Ohrbach R. Cultural equivalen-ce, reliability, and utility of the Portuguese version of the Oral Behaviours Checklist. J Oral Rehabil. 2018;45(12):924-931.
14. Campi LB, Jordani PC, Tenan HL, Camparis CM, Gonçalves DA. Painful tempo-romandibular disorders and central sensitization: implications for management-a pilot study. Int J Oral Maxillofac Surg. 2017 Jan;46(1):104-110. doi: 10.1016/j.ijom.2016.07.005. Epub 2016 Aug 21. PMID: 27553896.
15. Ferreira KA, Teixeira MJ, Mendonza TR, Cleeland CS. Validation of brief pain inven-tory to Brazilian patients with pain. Support Care Cancer. 2011 Apr;19(4):505-11. doi: 10.1007/s00520-010-0844-7. Epub 2010 Mar 10. PMID: 20221641.
16. Araújo LG, Lima DMF; Sampaio RF; Pereira LSM. Pain Locus of control scale: adap-tation and reliability for elderly. Braz J Phys Ther. October 2010; 14(5):438-445. DOI: 10.1590/S1413-35552010000500014.
17. Caumo W, Antunes LC, Elkfury JL, Herbstrith EG, Busanello Sipmann R, Souza A, et al. The Central Sensitization Inventory validated and adapted for a Brazilian popu-lation: psychometric properties and its relationship with brain-derived neurotrophic factor. J Pain Res. 2017; 10:2109-122.
18. Sullivan MJL. The Pain Catastrophizing Scale: User Manual. 2009. 36 p.19. Barros VV, Kozasa, EH, Souza, IC, Ronzani, TM. Validity evidence of the Brazi-
lian version of the Five Facet Mindfulness Questionnaire (FFMQ). Psicol Teor Pesq. 2014;30(3):317-27.
20. Hellman A, Chess A. Extensive sequence-influenced DNA methylation polymorphis-min the human genome. Epigenetics Chromatin. 2010;3(1):11.
21. Zwijnenburg PJ, Meijers-Heijboer H, Boomsma DI. Identical but not the same: the value of discordant monozygotic twins in genetic research. Am J Med Genet B Neu-ropsychiatr Genet. 2010;153B(6):1134-49.
22. Tan Q, Christiansen L, von Bornemann Hjelmborg J, Christensen K. Twin methodo-logy in epigenetic studies. J Exp Biol. 2015;218(Pt 1):134-9.
23. Suvinen TI, Reade PC, Hanes KR, Könönen M, Kemppainen P. Temporomandibular disorder subtypes according to self-reported physical and psychosocial variables in fe-male patients: a re-evaluation. J Oral Rehabil. 2005;32(3):166-73.
24. Zhi D, Aslibekyan S, Irvin MR, Claas SA, Borecki IB, Ordovas JM, et al. SNPs located at CpG sites modulate genome-epigenome interaction. Epigenetics. 2013;8(8):802-6.
25. Baer RA, Smith GT, Lykins E, Button D, Krietemeyer J, Sauer S, et al. Construct validity of the five-facet mindfulness questionnaire in meditating and non-meditating samples. Assessment. 2008;15(3):329-42.
26. Chiesa A, Serretti A. A systematic review of neurobiological and clinical features of mindfulness meditations. Psychol Med. 2010;40(8):1239-52.
27. Sullivan MJ, Thorn B, Rodgers W, Ward C. A path model of psychological antecedents of pain experience: clinical and experimental findings. Clin J Pain. 2004;20(3):164-73.
28. Stålnacke C, Ganzer N, Liv P, Wänman A, Lövgren A. Prevalence of temporomandi-bular disorder in adult patients with chronic pain. Scand J Pain. 2020;21(1):41-7.
29. Chichorro JG, Porreca F, Sessle B. Mechanisms of craniofacial pain. Cephalalgia. 2017;37(7):613-26.

INSTRUÇÕES AOS AUTORES
SCOPE & JOURNAL INFORMATIONBRAZILIAN JOURNAL OF PAIN®, printed version: ISSN 2595-0118 and electronic version: ISSN 2595-3192, is the official publication of the Brazi-lian Society for the Study of Pain® (Sociedade Brasileira para o Estudo da Dor - SBED®). SBED® publishes original research on the nature, mechanisms, as-sessment and treatment of pain and provides a multidisciplinary forum for the dissemination of research in both basic and applied pain research.The BrJP is directed towards all health professionals, including biologists, biome-dical professionals, dentists, physical educators, nurses, pharmacists, pharmaco-logists, physiologists, physiotherapists, doctors, veterinary doctors, nutritionists, psychologists, occupational therapists, etc., and all professionals in any area of knowledge interested in the study and treatment of pain, members or not of the SBED. The authors are fully responsible for the articles. The periodicity is quarterly and since May 2020 the articles have also been published in the modality of advanced publication or Ahead of Print (AOP). All papers submitted are peer-reviewed and the journal complies with the Uniform Requirements of Manuscripts Submitted to Biomedical Journals (URM - The International Committee of Medical Jour-nal Editors - ICMJE). Articles received are sent to 3-5 reviewers, who are asked to inform whether or not they accept the review within 3 days. After accepting to review the article, the evaluation must be returned in up to 15 days. The articles that require ad-justments are returned to the authors. After the authors response, the articles are reevaluated by the same reviewers who did the first evaluation or by reviewers chosen by the Editor. BrJP accepts the submission of articles with a maximum of 3500 words (exclu-ding title page, abstract, references, tables, figures and legends). A total of six illustrations (tables and/or figures) are allowed.Articles with no response from the authors after six months will be rejected, but may be resubmitted. There will be as many reviews as necessary, being the final approval decision made by the Editor. The authors shall guarantee that none of the material infringes any existing copyright or a third party right. BrJP follows the Editorial Policy Statements of the Council of Science Editors (CSE). Additional information on ethical aspects and misconduct can be found on the website (http://www.dor.org.br) and the online submission system. The evaluation process is very rigorous and anonymity between authors and reviewers is protected. The journal does not charge authors for the articles submission. Manuscripts submitted to the BrJP are subject to evaluation through tools in order to detect plagiarism, duplication or fraud, and whenever these situations are identified, the Editor will contact the authors and their institutions. If such situations are detected, authors should be prepared for an immediate refusal of the manuscript. If the Editor is not aware of this situation prior to publication, the following issue will bring a disclaimer. The authors will have open access through the https://sbed.org.br/publicacoes-publicacoes-bjp portal.The BRAZILIAN JOURNAL OF PAIN web site can be found at https://brjp.org.br/.
Contact details for submissionAll manuscripts must be submitted online at https://www.gnpapers.com.br/brjp/default.asp.Questions may be directed to the Editorial Office at [email protected].
INTRODUCTION Conditions for submissionThe author: (1) assures that the manuscript is an original study that has not been previously published; (2) assures that the manuscript is not under consideration by any other publisher; (3) accepts full responsibility for the accuracy of all con-
tent, including findings, citations, quotations, and references contained within the manuscript; (4) releases and assigns all rights for the publication of the ma-nuscript to the SBED and the publisher; (5) discloses in the acknowledgement section and on the title page any conflicts of interest related to the research or the manuscript; (6) discloses on the title page any previous presentation of the research, manuscript, or abstract; (7) * assures that authorship has been gran-ted only to those individuals who have contributed substantially to the research or manuscript; (8) discloses in the methods section of the manuscript that any investigation involving human subjects or the use of patient data for research purposes was approved by the committee on research ethics at the institution in which the research was conducted in accordance with the Declaration of the World Medical Association (www.wma.net) and that any informed consent from human subjects was obtained as required; (9) discloses in the methods section of the manuscript that any investigation involving animals for research purposes was approved by the animal care committee on research ethics at the institution; (10) attaches documents showing all relevant permissions to publish quotations, text, tables, or illustrations from copyrighted sources; (11) discloses in the ma-nuscript references and/or table/figure footnotes the full citation and permission of the copyright owner as required. The journal will only consider publication of work that includes information that is sufficient to permit replication by other laboratories. Manuscripts reporting data from novel chemical probes will not be considered unless the structure and pharmacological characterization, including selectivity and relevant formulation, are reported or directly described in a prior peer-reviewed publication.*Authors’ role: BrJP abides by the Authorship Criteria as set by the International Committee of Medical Journal Editors (ICMJE). Please visit http://www.icmje.org/index.html to review the criteria and determine whether contributors should be listed as authors or listed in the acknowledgements. Attributing authorship to those who do not meet the requirements set forth by the ICMJE is not accepta-ble. Similarly, it is unacceptable to exclude individuals meeting the requirements for authorship. Each person listed as an author is expected to have participated in the preparation of the manuscript in a significant way. Although BrJP endorses the ICMJE authorship requirements, the Editorial Board is not in a position to adjudicate disputed authorship issues. These must be resolved by the authors or by the institution responsible for the research. Should further guidance be needed, authors should consult the Committee on Publication Ethics (COPE) guidelines for authorship disputes at https://bit.ly/3Ef2MJw.
SUBMISSION OF ARTICLESArticles should be submitted online through the platform https://www.gnpapers.com.br/brjp/default.asp, including the Copyright Assignment document, avai-lable in the publications folder of the portal https://sbed.org.br/publicacoes-pu-blicacoes-bjp, duly signed by the author(s). A Submission Letter should be sent along with the manuscript’s files, containing information regarding originality, conflict of interests, sponsoring sources, indication of thre potential reviewers, as well as confirmation that the article is not under evaluation by another journal and has not been previously published. This letter should also confirm that the article, if accepted, will be entitled to exclusive publication in the BrJP, and that it respects ethical aspects, in the case of studies involving animals or humans. The articles may be sent in Portuguese or English. The printed publication will be in Portuguese and the electronic publication in both Portuguese and English. Authors have the responsibility to declare conflict of interests in the manuscript itself, as well as to acknowledge financial support when appropriate. BrJP con-siders the duplicate or fragmented publication of the same research an ethical infraction and is careful in using mechanisms to find text similarities and detect plagiarism.
© Sociedade Brasileira para o Estudo da Dor

SUBMISSION CHECKLISTIn anticipation, you are invited to use this list to perform an initial verification and final review of your material before submitting it to the BrJP for considera-tion. Check the relevant section in these instructions for authors for more details.Ensure that the following items are present in you files before submitting your manuscript:
Title page• Title• Abbreviated title• Key-words• Complete name of authors, their affiliations (department, institution, city/sta-te/country, e-mail address) and ORCID numbers.• Corresponding author with contact details: complete name and e-mail address• Wordcount• Declaration of conflict of interest
Manuscript• Main text (according to guideline recommended in the section of ‘type of stu-dy’)• Ethical information (number of approval, name of Ethics Committee, more information as needed)• References (following standardized rules of BrJP)• Figures (with legends, in grey scale, and appropriately cited in the text)• Tables (with title, legends and/or footnotes, and appropriately cited in the text)• Source of support• Acknowledgment (people, institutions and/or funding agencies)• Suplemental files (when needed)
More verifications are recommended:• Manuscript has been ‘spell checked’ and ‘grammar checked’ • Report guideline as indicated for any type of study was considered and presen-ted at the end of the manuscript as a checklist• All references mentioned in the Reference List are cited in the text, and vice versa • Permission has been obtained for the use of copyrighted material from other sources (including the internet) or authors assume the responsability for elabora-ting all ilustrations contained in the manuscript• A competing interests statement is provided, even if the authors have no com-peting interests to declare • Journal policies detailed in this guide have been reviewed • Referee suggestions and contact details (e-mail address) provided, based on journal requirements
ETHICAL/LEGAL CONSIDERATIONSAuthor rights Authors keep the author rights and grant brjp magazine and SBED the right of first publication, and the work is simultaneously licensed under CC BY, which allows the sharing of work with recognition of the authorship of the work and initial publication in this journal. Upon acceptance of an article, the authors will be asked to complete a Journal Publishing Agreement to assign to the Brazilian Society for the Study of Pain (SBED) the copyright of the manuscript and any tables, illustrations or other materials submitted for publication as part of the manuscript in all forms and media (now known or later developed), worldwide, in all languages, for the full term of copyright, from when the article is accepted for publication. An email will be sent to the corresponding author confirming receipt of the manuscript along with a Publication Agreement form or a link to the online version of this agreement.
Authorship and changes to authroshipAll authors should have made substantial contributions to all of the following: 1. the conception and design of the study, or acquisition of data, or analysis and interpretation of data;2. drafting the article or revising it critically for important intellectual contente;3. final approval of the version to be submitted. To recognize individual author contributions, reducing authorship disputes and facilitating collaboration, authors are required to mention the contribution(s) of each author in the title page based on CRediT (Contributor Roles Taxonomy)
author statement. Main activities correspond to Conceptualization, Metho-dology; Software; Validation; Formal analysis; Investigation; Resources; Data Curation; Writing - Original Draft; Writing - Review & Editing; Visualization; Supervision; Project administration; Funding acquisition whose definition can be seen at https://www.elsevier.com/authors/policies-and-guidelines/credit-au-thor-statement. Authors are expected to consider carefully the list and order of authors before submitting their manuscript and provide the definitive list of authors at the time of the original submission. Any addition, deletion or rearrangement of author names in the authorship list should be made only before the manuscript has been published and only if approved by the journal Editor. To request such a change, the Editor must receive the following from the corresponding author: (a) the reason for the change in author list and (b) written confirmation (e-mail, letter) from all authors that they agree with the addition, removal or rearrangement. In the case of addition or removal of authors, this includes confirmation from the author being added or removed.Requests that are not sent by the corresponding author will be forwarded by the Journal Manager to the corresponding author, who must follow the procedure as described above. Note that: (1) Journal Managers will inform the Journal Editors of any such requests and (2) publication of the accepted manuscript in an online issue is suspended until authorship has been agreed. Changes will only be done before the accepted manuscript is published in an online issue.
Declaration of interest All authors must disclose any financial and personal relationships with other people or organizations that could inappropriately influence (bias) their work. Examples of potential competing interests include employment, consultancies, stock ownership, honoraria, paid expert testimony, patent applications/registra-tions, and grants or other funding. Authors must disclose any interests in two places: 1. A summary declaration of interest statement in the title page file (if double--blind) or the manuscript file (if single-blind). If there are no interests to declare, then please state this: ‘Declarations of interest: none’. This summary statement will be ultimately published if the article is accepted. 2. Detailed disclosures as part of a separate Declaration of Interest form, which forms part of the journal’s official records. It is important for potential interests to be declared in both places and that the information matches.
Verification of originality and validity of manuscriptSubmission of an article implies that the work described has not been published previously (except in the form of an abstract, a published lecture or academic thesis, see ‘Multiple, redundant or concurrent publication’ for more informa-tion), that it is not under consideration for publication elsewhere, that its pu-blication is approved by all authors and tacitly or explicitly by the responsible authorities where the work was carried out, and that, if accepted, it will not be published elsewhere in the same form, in English or in any other language, including electronically without the written consent of the copyright-holder. To verify originality, your article may be checked by the originality detection service Crossref Similarity Check at https://www.crossref.org/services/similarity-check/. Although the editors and referees make every effort to ensure the validity of pu-blished manuscripts, the final responsibility rests with the authors, not with BrJP, its editors, or the publisher.
Role of the funding source You are requested to identify who provided financial support for the conduct of the research and/or preparation of the article and to briefly describe the role of the sponsor(s), if any, in study design; in the collection, analysis and interpre-tation of data; in the writing of the report; and in the decision to submit the article for publication. If the funding source(s) had no such involvement then this should be stated.
CopyrightThe copyright transfer agreement and the ICMJE Conflict of Interest forms should be filled out and be uploaded by the corresponding author at original submission. Coauthors are required to complete both forms at the revision stage. All authors are required to submit both a Clinical Trial Application (CTA) and an ICMJE Conflict of Interest Form. Once we have received all forms from all

authors, your revision will be assigned to the editors. If you have questions about this process, please contact the editorial office at [email protected].
PermissionsAuthors must submit written permission from the copyright owner (usually the publisher) to use direct quotations, tables, or illustrations that have appeared in copyrighted form elsewhere, along with complete details about the source.
Informed consent and patient anonimityStudies on patients or volunteers require ethics committee approval and infor-med consent, which should be documented in the paper. Appropriate consents, permissions and releases must be obtained where an author wishes to include case details or other personal information or images of patients and any other indi-viduals. Written consents must be retained by the author but copies should not be provided to the journal. Only if specifically requested by the journal in excep-tional circumstances (for example if a legal issue arises), the author must provide copies of the consents or evidence that such consents have been obtained. Unless authors have written permission from the patient (or, where applicable, the next of kin), personal details of any patient included in any part of the article and in any supplementary materials (including all illustrations and videos) must be removed before submission. It is the author’s responsibility to ensure that a patient’s anonymity is carefully protected. For photographs, author(s) must obtain written and signed permis-sion from the patient if the patient would be recognizable. Author(s) must state in their manuscript that informed consent was sought and granted.It is also very important to make textual mention of the General Personal Data Protection Law (LGPD) (https://bit.ly/35r177b), in na attempt to legally extend the protection of the research subject.
Ethics with laboratory animalsAll animal studies must comply with arrive guidelines (see ‘type of studies’ section) and should be carried out in accordance with the UK Animal Act (Scientific Proce-dures) (1986), EU Directive 2010/63/EU for animal experiments, National Guide of the Institutes of Health for the Care and Use of Laboratory Animals (NIH Pu-blications No 8023), Federal Law No. 11,794/08 (Arouca Law), a Brazilian prac-tice guideline for the care and use of animals for scientific and teaching purposes (DBPA). The authors should clearly indicate in the article that such guidelines were considered and followed. The sex of the animals should be indicated and, when and if applicable, the possible interference of sex in the results of the study. Use of inclusive language Inclusive language acknowledges diversity, conveys respect to all people, is sensi-tive to differences, and promotes equal opportunities. Content should: 1. make no assumptions about the beliefs or commitments of any reader; 2. contain no-thing which might imply that one individual is superior to another on the grou-nds of age, gender, race, ethnicity, culture, sexual orientation, disability or health condition; and 3. use inclusive language throughout. Authors should ensure that writing is free from bias, stereotypes, slang, reference to dominant culture and/or cultural assumptions. We advise to seek gender neu-trality by using plural nouns (“clinicians, patients/clients”) as default/wherever possible to avoid using “he, she,” or “he/she.” We recommend avoiding the use of descriptors that refer to personal attributes such as age, gender, race, ethnicity, culture, sexual orientation, disability or health condition unless they are relevant and valid. These guidelines are meant as a point of reference to help identify appropriate language but are by no means exhaustive or definitive.
MANUSCRIPT PREPARATION BrJP accepts online submission of manuscripts through GNPapers. The site con-tains instructions and advice on how to use the system, guidance on the creation/scanning and saving of electronic art, and supporting documentation.All manuscripts must be submitted online via GNPapers, at https://www.gnpa-pers.com.br/brjp/default.asp.If you have previously submitted to BrJP, you already have an account in the system and can use your same log in credentials or click on “Send Username/Password” if you do not recall your credentials to have them emailed to you. If you have never submitted to BrJP, see instructions for first-time users below.
Editorial review. The BrJP Editor-in-Chief, Josimari M. DeSantana, and Sec-tion Editors do the initial review of all submissions.If you experience any problems with Editorial Manager or have any questions, please contact the Editorial Office by clicking on the ‘Contact Us’ link in the navigation bar or by emailing [email protected].
PREPARING THE SUBMISSIONDouble-blind review This journal uses double-blind review, which means the identities of the authors are concealed from the reviewers, and vice versa. To facilitate this, please include a title page separately from the blinded manus-cript.
Title page (with author details). In the title page, authors should included all author details, ORCID information (see https://orcid.org/register if you are not registered yet), correspongin author details, highlights. Please clearly indicate the given name(s) and family name(s) of each author and check that all names are accurately spelled. Present the authors’ affiliation addresses (where the actual work was done) below the names. Indicate all affiliations with a superscript arabic numerals immediately after the author’s name and in front of the appropriate address. Provide the full postal address of each affiliation, including the country name and, if available, the e-mail address of each author. Also, ORCID informa-tion should be informed for each author in a list.
Corresponding author. Clearly indicate who will handle correspondence at all stages of refereeing and publication, also post-publication. This responsibility includes answering any future queries about Methodology and Materials. Ensure that the e-mail address is given and that contact details are kept up to date by the corresponding author. Thus, authors need to provide information as follow: “Correspondence to ‘author´s name’ and ‘email address’.
Present/permanent address. If an author has moved since the work described in the article was done, or was visiting at the time, a ‘Present address’ (or ‘Permanent address’) may be indicated as a footnote to that author’s name. The address at which the author actually did the work must be retained as the main, affiliation address. Superscript lowered letters are used for such footnotes.
ORCID. ORCID (Open Researcher and Contributor ID) is a non-proprietary alphanumeric code for unique identification of scientists and their collaborators, providing persistent identity to humans, similar to what is created for content entities related to digital networks by digital object identifiers (DOIs). Your OR-CID number must be entered on the title page. If you do not already have your ORCID, registration can be made in https://orcid.org/register.
Highlights. Highlights are mandatory for this journal as they help to increase the discoverability of an article via search engines. They consist of a short collection of bullet points that capture the novel results of your research as well as new me-thods that were used during the study (if any). Highlights should be submitted in a separate page after the title page file. Please use ‘Highlights’ as a topic in the top of the page. Include 3 to 5 bullet points (maximum 85 characters, including spaces, per bullet point). MAIN STRUCTURE OF ORIGINAL ARTICLESBlinded manuscript (no author details): main body of the paper (including references, figures, tables and any acknowledgements) should not include any identifying information, such as authors’ names or affiliations.
Abstract. Abstracts should bring the main important information from the ma-nuscript. Like the paper itself, abstracts should include all of the IMRaC ele-ments: Introduction, Methods, Results, and Conclusion. Initially, on the intro-duction, authors should provide a broad overview of the entire study, write out the hypothesis or research question or problem it attempts to solve and why the reader should be interested. Two to three phrases may be enough to highlight the main idea, followed by the objective. Then, the methods section must inform the type of study, the procedure for collecting data, including descriptions of variables, instruments, software, or participants / groups of participants. Timeli-ne measurements and analytical methods should also be presented. Main results

should be presented, comparing groups when necesssary, and presenting values between parenthesis. The discussion section explains the ultimate conclusion and its ramifications. The discussion section often goes beyond the scope of the pro-ject itself, including the implications of the research or what it adds to its field as a whole.
Key-words. Immediately after the abstract, provide a maximum of 6 keywords, using American spelling and avoiding general and plural terms and multiple con-cepts (avoid, for example, ‘and’, ‘of ’). Be sparing with abbreviations: only abbre-viations firmly established in the field may be eligible. These keywords will be used for indexing purposes. Preferably, key-words must be selected from MeSH Database at https://www.ncbi.nlm.nih.gov/mesh.
Introduction. In this section, authors must sucintamente descrever o escopo e o conhecimento prévio baseado em evidência (state of the art) para o delineamen-to da pesquisa, tendo como base referências bibliográficas relacionadas ao tema, preferencialmente mais recentes conforme possível. Adicionalmente, a lacuna de conhecimento ou o problema em questão deve ser apresentado. Ao final, deve incluir o objetivo da pesquisa de forma clara e a relevância do assunto estudado. Methods. Specific information about methods can be seen in the section of “Types of Article once each type of manuscript requires disctinct items. We must reinforce that report guidelines must be used to any type of article.Results. devem ser descritos de forma objetiva, elucidados por figuras e tabelas quando necessário. Incluir análises realizadas e seus resultados.Discussion. In this section, authors must discuss their results and three different phases to each conjunct of findings should be considered: interpretation of re-sults, use of previous publication to confirm or refute findings and considerations of authors to each topic discussed. Previous information must be appropriately cited. Discussion can be optionally divided into subchapters. Limitations of the study, clinical implications (always when adequate), information about the importance / relevance, and perspectives for future researches are mandatoryly required.Conclusion. Conclusions must be concise and directly repond to the objectives of the study. No extra commentaries are needed.Acknowledgments. Collate acknowledgements in a separate section at the end of the article before the references and do not, therefore, include them on the title page, as a footnote to the title or otherwise. List here those individuals who pro-vided help during the research (e.g., providing language help, writing assistance or proof reading the article, etc.). Formatting of funding sources. List funding sources in this standard way to facilitate compliance to funder’s requirements: Funding: This work was supported by the xxxxxxxxxxx [grant numbers xxxx, yyyy]; yyyyyyyyyy [grant number yyyyyyyyy]. It is not necessary to include detailed descriptions on the program or type of grants and awards. When funding is from a block grant or other resources availa-ble to a university, college, or other research institution, submit the name of the institute or organization that provided the funding. If no funding has been provided for the research, please include the following sentence: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. References. References must follow Vancouver style (http://www.icmje.org).Figures and Tables. They must be sent in the same file of the main manuscript just after references inserting break page between them.
More information:Summary. When completing the submission process of their manuscript, au-thors must enter the text in Portuguese and English in a specific field on the platform, followed by the descriptors (from 3 to 6, which must be included in the Descriptors in Health (DeCs) or MeSH Database.Style. Pattern manuscript style after the American Medical Association Manual of Style (10th edition). Stedman’s Medical Dictionary (27th edition) and Merriam Webster’s Collegiate Dictionary (10th edition) should be used as standard references. Keep the layout of the text as simple as possible. Most formatting codes will be removed and replaced on processing the article. In particular, do not use the word processor’s options to justify text or to hyphenate words. However, do use bold face, italics, subscripts, superscripts etc.
Refer to drugs and therapeutic agents by their accepted generic or chemical na-mes, and do not abbreviate them. Use code numbers only when a generic name is not yet available. In that case, supply the chemical name and a figure giving the chemical structure of the drug.Capitalize the trade names of drugs and place them in parentheses after the ge-neric names. Also, capitalize all equipments and apparatus used in the methods section. To comply with trademark law, include the name and location (city and state and country) of the manufacturer of any equipment mentioned in the manuscript followed by the symbol. Use the metric system to express units of measure and degrees Celsius to express temperatures, and use SI units rather than conventional units.It is important that the file be saved in the native format of the word processor used. The text should be in single-column format. When preparing tables, if you are using a table grid, use only one grid for each individual table and not a grid for each row. If no grid is used, use tabs, not spa-ces, to align columns. The electronic text should be prepared in a way very similar to that of conventional manuscripts. Note that source files of figures, tables and text graphics will be required whether or not you embed your figures in the text. To avoid unnecessary errors you are strongly advised to use the ‘spell-check’ and ‘grammar-check’ functions of your word processor.
Math formulae. Please submit math equations as editable text and not as ima-ges. Present simple formulae in line with normal text where possible and use the solidus (/) instead of a horizontal line for small fractional terms, e.g., X/Y. In principle, variables are to be presented in italics. Powers of e are often more conveniently denoted by exp. Number consecutively any equations that have to be displayed separately from the text (if referred to explicitly in the text).
Footnotes. Footnotes should be used sparingly. Number them consecutively throughout the article. Many word processors can build footnotes into the text, and this feature may be used. Otherwise, please indicate the position of footnotes in the text and list the footnotes themselves separately at the end of the article. Do not include footnotes in the Reference list.
Reference style. Submissions should adhere to the BrJP® reference style, full de-tails of which can be found in the information provided for each article type under section “Article Types” above. Authors are highly recommended to manage theirs references by using softwares such as Endnote, Mendeley or Zotero.Cite literature references in the text should be presente as a superscript number as follows: “Pain pain pain pain pain pain pain pain4.” For multiple references in the text, please use the format “Pain pain pain pain pain pain pain pain4,5.” or “Pain pain pain pain pain pain pain pain4-7,10.” (with a comma and no spaces). ‐ All references cited in the text must be listed at the end of the paper. They should be numbered, double spaced, and arranged alphabetically by first author last name. ‐ All authors must be listed in the references; the use of et al. is not acceptable.‐ Journal titles should be abbreviated according to the National Library of Me-dicine’s Index Medicus. Please refer to the NLM website’s FAQ on how to find Index Medicus journals: www.nlm.nih.gov/services/aim.html. ‐ Unpublished data, personal communications, abstracts that cannot be retrieved by casual readers (e.g., meeting abstracts that require logging into a members‐only site), and other inaccessible materials should not be listed as references. Unpublished materials may be cited in parentheses within the text. Figures. BrJP has strict guidelines on image quality. You must ensure your figures follow these rules. Failure to supply files in the format specified below will result in the images being returned to you for re-formatting. This may lead to an asso-ciated delay in the review and publication of your manuscript.A) Creating Digital ArtworkLearn about the publication requirements for Digital Artwork: http://links.lww.com/ES/A42Create, Scan and Save your artwork and compare your final figure to the Digital Artwork Guideline Checklist (below).Upload each figure to Editorial Manager in conjunction with your manuscript text and tables.B) Digital Artwork Guideline ChecklistHere are the basics to have in place before submitting your digital art to BrJP:Artwork should be saved as TIFF, PDF, Word Doc, PPT, or EPS files.

Artwork is created as the actual size (or slightly larger) it will appear in the jour-nal. (To get an idea of the size images should be when they print, study a copy of the journal to which you wish to submit. Measure the artwork typically shown and scale your image to match.)Crop out any white or black space surrounding the image.Diagrams, drawings, graphs, and other line art must be vector or saved at a reso-lution of at least 1200 dpi. If the art is created in an MS Office program, convert to a hi-res PDF. If the PDF creation process is unifamiliar, then submit the MS Office doc.Photographs, radiographs and other halftone images must be saved at a resolu-tion of at least 300 dpi.Photographs and radiographs with text must be saved as postscript or at a reso-lution of at least 600 dpi.Each figure must be saved and submitted as a separate file by using sequential numbers. Figures should not be embedded in the manuscript text file.
General points: • Make sure you use uniform lettering and sizing of your original artwork. • Embed the used fonts if the application provides that option. • Aim to use the following fonts in your illustrations: Arial, Courier, Times New Roman, Symbol, or use fonts that look similar. • Number the illustrations according to their sequence in the text, consecutively in your manuscript.• Number figures in the figure legend in the order in which they are discussed.• Use a logical naming convention for your artwork files. • Provide captions to illustrations separately. • Size the illustrations close to the desired dimensions of the published version. • Submit each illustration after reference section in the manuscript file. • Ensure that color images are accessible to all, including those with impaired color vision.
Please do not: • Supply files that are optimized for screen use (e.g., GIF, BMP, PICT, WPG); these typically have a low number of pixels and limited set of colors. • Supply files that are too low in resolution.• Submit graphics that are disproportionately large for the content.
Color figures. All figures will appear in a grey scale in both online and printed versions, according submitted by authorors and approved by the editotrial board/reviewers.Figure legends. Legends must be submitted for all figures. Provide each illus-tration with a title and an explanatory legend. The title should be part of the legend; do not reproduce the title and legend on the figure itself. They should be brief and specific and appear on a separate manuscript page after the references in the same file. Each legend should begin with a brief statement that identifies the figure. Each legend should be numbered consecutively with Arabic numerals (i.e., Fig. 1, Fig. 2, etc.), and should begin with the number of the illustration to which they refer. Explain all symbols and abbreviations used in the figure. Use scale markers in the image for electron micrographs and indicate the type of stain used for tissue, if this is the case. Tables. Tables can be included within the manuscript document on a separate manuscript page after the references in the same file. Do not upload images of tables. All tabular matter must be editable (in Word). An image of a table, such as a scan, is not acceptable for publication. Tables, with their captions and legends, should be intelligible with minimal reference to the text. Tables of numerical data should each be typed (double spaced) on a separate page, numbered in sequence with Arabic numerals (i.e., Table 1, Table 2, etc.), provided with a title/heading, and referred to in the text as Table 1, Table 2, etc. Provide a detailed description of its contents and any footnotes below the body of the table.
Social media promotion of individual articles. At the revision stage, authors will be asked to enter a question at re-submission to be used for social media purposes. Please compose a question for which your paper’s subject, topic, or title is an answer. We will take your question, attach your paper’s web address, and use it for SBED´s social media promotion. Example of author composed question: What is the relationship between pain and fear in fibromyalgia patients? The
answer is the title of author´s paper, such as in this example “Fear is a predictor to increase pain in fibromyalgia patients,” which the BrJP® editorial office will trans-late to a bit.ly URL (a shortened web address) and attach it to the question. The final product, the question, and the shortened web address, is the message we will promote on social media, to boost awareness and drive traffic to the published content. What everyone will see on social media: What is the relationship bet-ween pain and fear in fibromyalgia patients? http://bit.ly/vvXvxV, for example.
ARTICLE TYPESThe journal will only consider publication of work that includes information that is sufficient to permit replication by other laboratories or groups. Manuscripts re-porting data from novel chemical probes will not be considered unless the struc-ture and pharmacological characterization, including selectivity and relevant for-mulation, are reported or directly described in a prior peer-reviewed publication.Brazilian Journal of Pain (BrJP) publishes original research articles, reviews, and brief communications on topics related to distinct areas of pain. Our Editorial Board is committed to disseminate high-quality research in the field of pain. BrJP follows principles of publication ethics included in the code of conduct of the Committee on Publication Ethics (COPE). BrJP accepts submission of manuscripts with up to 4,000 words (excluding title page, abstract, references, tables, figures and legends). Information contained in any appendices will be included in the total number of words allowed for pu-blication. A total of six (6) either tables and/or figures is allowed. The following types of study can be considered for publication, if directly rela-ted to the journals scope. Click on the article type to see details on manuscript formatting. The below article types are considered for publication in BrJP.a) Intervention studies (clinical trials): studies that investigate the effect(s) of one or more treatment interventions on outcomes directly related to pain. World Health Organization defines a clinical trial as any research study that prospec-tively allocates human participants to one or more health-related interventions to evaluate the effect(s) on health outcome(s). Clinical trials include single-case experimental studies, case series, nonrandomized controlled trials, and randomi-zed controlled trials. Randomized clinical trials (RCTs) must follow Consolidated Standards of Re-porting Trials (CONSORT) available at http://www.consort-statement.org/. In the manuscript, authors must provide the CONSORT Checklist and the CON-SORT Flow Diagram which illustrates the progress of patients through the trial, including all phases, at the endo f the manuscript in the same file. Registration of clinical trials Registration in a public trials registry is a condition for publication of clinical trials in this journal in accordance with International Committee of Medical Journal Editors recommendations. Trials must register at or before the onset of patient enrolment. Clinical trial registration number should be included at the end of the abstract of the article. A clinical trial is defined as any research study that prospectively assigns human participants or groups of humans to one or more health-related interventions to evaluate the effects of health outcomes.Moreover, CONSORT-Abstract must be used in an attempt that authors provide a minimum list of itens in the abstract section (see https://bit.ly/3OG1IUS). For the RCTs, title must consider information from the PICOT strategy (P: popula-tion; I: intervention: C: comparation; O: outcome; T: time).RCTs must provide registration that satisfies the requirements of the Interna-tional Committee of Medical Journal Editors (ICMJE), e.g. http://clinicaltrials.gov/ and / or http://www.anzctr.org.au. The complete list of all clinical trial re-gistries can be found at: http://www.who.int/ictrp/network/primary/en/index.html. We suggest that all authors register clinical trials prospectively via websites such as http://www.clinicaltrials.gov or https://ensaiosclinicos.gov.br/. Note: We accept single case studies and series of cases (i.e. clinical trials without a compari-son group) in a low proportion if they are really interesting in the area of interest. Template for Intervention Description and Replication (TIDieR) checklist and guide must also be used to promote a complete description of both pharma-cological and non-pharmacological interventions, in an attempt that clinicians and patients can reliably implement interventions that are shown to be useful, and other researchers can replicate or build on research findings. The TIDieR guide provides, for each item, an explanation, elaboration, and examples of good

reporting and can be found at https://www.equator-network.org/wp-content/uploads/2014/03/TIDieR-Checklist-PDF.pdf. TIDieR checklist must be sub-mitted at the end of the manuscript in the same file.The resultant 12 item TIDieR checklist is an extension of the CONSORT 2010 statement (item 5). For authors of reports of randomised trials, it is recommen-ded that TIDieR is used in conjunction with the CONSORT checklist: when authors complete item 5 of the CONSORT checklist, they should insert “refer to TIDieR checklist” and provide a separate completed TIDieR checklist.Sample size must be presente in all details in all manuscripts which are clinical trials. P value and confidence interval will be required as well.In line with the position of the International Committee of Medical Journal Editors, BrJP will not consider results posted in the same clinical trials registry in which primary registration resides to be prior publication if the results posted are presented in the form of a brief structured (less than 500 words) abstract or table. However, divulging results in other circumstances (e.g., investors’ meetings) is discouraged and may jeopardise consideration of the manuscript. b) Observational studies: studies that investigate the relationship(s) between variables of interest related to pain. Observational studies include transversal or longitudinal cross-sectional studies, cohort studies, and case-control studies. All observational studies must be reported following the recommendation from Strengthening the reporting of observational studies in epidemiology (STROBE) statement (http://strobe-statement.org/index.php?id=strobe-home). STROBE checklist must be submitted at the end of the manuscript in the same file. c) Qualitative studies: studies that focus on understanding needs, motivations, perceptions, opinions, experiences, and human behavior. The object of a qualita-tive study is guided by in-depth analysis of a topic, including opinions, attitudes, motivations, and behavioral patterns without quantification. All qualitative stu-dies must be reported following the recommendation from Standards for Repor-ting Qualitative Research (SRQR) statement (https://www.equator-network.org/reporting-guidelines/srqr/). SRQR checklist must be submitted at the end of the manuscript in the same file.d) Systematic reviews: studies that analyze and/or synthesize the literature on a topic related to the scope of pain. Systematic reviews that include meta-analysis will have priority over other systematic reviews. Those that have an insufficient number of articles or articles with low quality in the methods section and do not include an assertive and valid discussion/conclusion about the topic will be evaluated with caution. Authors must follow the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist to presente a systematic reviews. This checklist is available at http://prisma-statement.org/prismastatement/Checklist.aspx and must be filled in and submitted with the manuscript. PRISMA checklist must be submitted at the end of the manuscript in the same file.The risk of bias analysis should be performed, according to the authors’ choice, using the Risk Analysis tools of the Cochrane RoB2 Collaboration (https://bit.ly/31PpnOW) or PeDro Scale (https://bit .ly/3zR7FY0).GRADE is a systematic approach to classifying the certainty of evidence in sys-tematic reviews and other evidence syntheses and should be used in systematic reviews. The checklist covers the key determinants for each of the five factors (risk of bias, inconsistency, indirect evidence, imprecision, publication bias) that can lead to reduced quality in the system. Check information about GRADE at https://bit.ly/3qkwwjV.e) Studies on the translation and cross-cultural adaptation of questionnaires or assessment tools: studies that aim to translate and/or cross-culturally adapt questionnaires from other countries to a language other than that of the original version of existing assessment instruments. Authors must use the checklist (in Appendix) to format this type of paper and adhere to the other recommendations of the BrJP. Answers to the checklist must be submitted with the manuscript at the end of the manuscript in the same file. At the time of submission, authors must also include written permission from the authors of the original manuscript that whose instrument was translated and/or cross-culturally adapted. f ) Methodological studies: studies related to the development and/or evaluation of clinimetric properties and characteristics of assessment instruments. Authors are required to use the Guidelines for Reporting Reliability and Agreement Stu-dies (GRRAS) to format methodological papers, in addition to following BrJP instructions, which can be found at https://bit.ly/3KODxBE. g) Clinical trial protocols: BrJP welcomes the publication of pain-related clini-cal trial protocols. We only accept trial protocols that are substantially funded,
have ethics approval, have been prospectively registered and of very high quality. We expect that clinical trial protocols must be novel and with a large sample size. Finally, authors have to provide that the clinical trial is on its first stages of recruitment. Authors must use Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) statement while formatting the manuscript (http://www.spirit-statement.org). h) Animal pre-clinical studies: Animal experiments should be carried out in ac-cordance with the U.K. Animals (Scientific Procedures) Act, 1986 and associated guidelines, EU Directive 2010/63/EU for animal experiments, or the National Institutes of Health guide for the care and use of Laboratory animals (NIH Pu-blications No. 8023, revised 1978), Federal Law 11.794/08 (Lei Arouca), Brazi-lian practice guideline for the care and use of animals for scientific and teaching purposes (DBPA). Authors should clearly indicate in the manuscript that such guidelines have been followed. Authors must use Animal Research: Reporting of In Vivo Experiments (ARRIVE) statement while formatting the manuscript (https://www.equator-network.org/reporting-guidelines/improving-bioscience--research-reporting-the-arrive-guidelines-for-reporting-animal-research/).All experiments involving animals should be approved by a local Animal Care Committee and should be in accordance with the guidelines of the correspon-ding country. If guidelines are not available in the country where the research is being performed, we recommend following the guidelines described by the National Institutes of Health, USA. We propose that the following general gui-delines be followed to establish reliability and robustness of the data presented.Pharmacological studies. General pharmacological principles such as dose-res-ponse curves and testing an antagonist against its agonist, which indicate recep-tor-mediated interactions and specificity of the proposed drug, are recommen-ded. In a few cases, there are well-established doses of pharmacological drugs that can be used but these should be justified by appropriate literature. Vehicle control data are needed.Behavioral studies. To perform unbiased studies, it is essential that the following principles be used in behavioral studies: blinding of the behavioral tester (pre-ferably to the condition, but essentially to the drug/genotype/manipulation or vehicle, phenotype, etc.) and also randomization of animals to groups. It is also recommended that when possible behavioral studies should be performed by the same tester, or interrater reliability should be performed and reported between multiple testors. Details on the randomization procedures and blinding should be included in the methods.Genetic studies or usage of gene delivery tools. Studies on genetically-modified mice should employ control mice of the corresponding genetic background as con-trols. When viral tools are used for gene delivery, virions expressing a functionally--neutral gene, such as GFP, should be included as controls. In RNAi experiments, scrambled/sense/functionally-neutral constructs should be included as controls.
Animals. Age, sex, species, and source of animals should be reported. The num-ber of replicates and animals used per experiment and group should be clearly outlined in the methods. We recommend use of both male and female animals in experiments where appropriate and possible.Sham controls for surgical and other interventions are recommended.Drug formulation. All drugs used in the study should be listed with the vendor for which it was purchased, dosing, how the drug was dissolved, site (city, state and country, route of administration and symbol of trade mark.Studies involving molecular profiling data, i.e. ‘Omics’. Descriptive data from Omics approaches on animal models or clinical groups, such as transcriptomi-cs, genomics, proteomics, microRNA profiling etc., should be accompanied by secondary validation of data sets, such as by quantitative PCR. The analysis of functional implications of the genes, proteins or microRNAs identified via such approaches is recommended.Statistics. Care should be taken that the statistical measures adopted are appro-priate for the data sets being analyzed. For example, while comparing multiple groups or time points, application of a t-test is inappropriate. ANOVA and pos-t-hoc tests that enable multiple comparisons (e.g., Bonferroni) should be used. The choice of one-way or two-way ANOVA is dependent upon the number of independent variables being tested such as treatment, time, sex or other. If the authors are unsure about which statistical measures to implement, receiving help from a statistician is recommended.Secondary analyses of data. BrJP abides by the ICMJE guidelines regarding ma-nuscripts based on secondary analyses of data. Such manuscripts should address
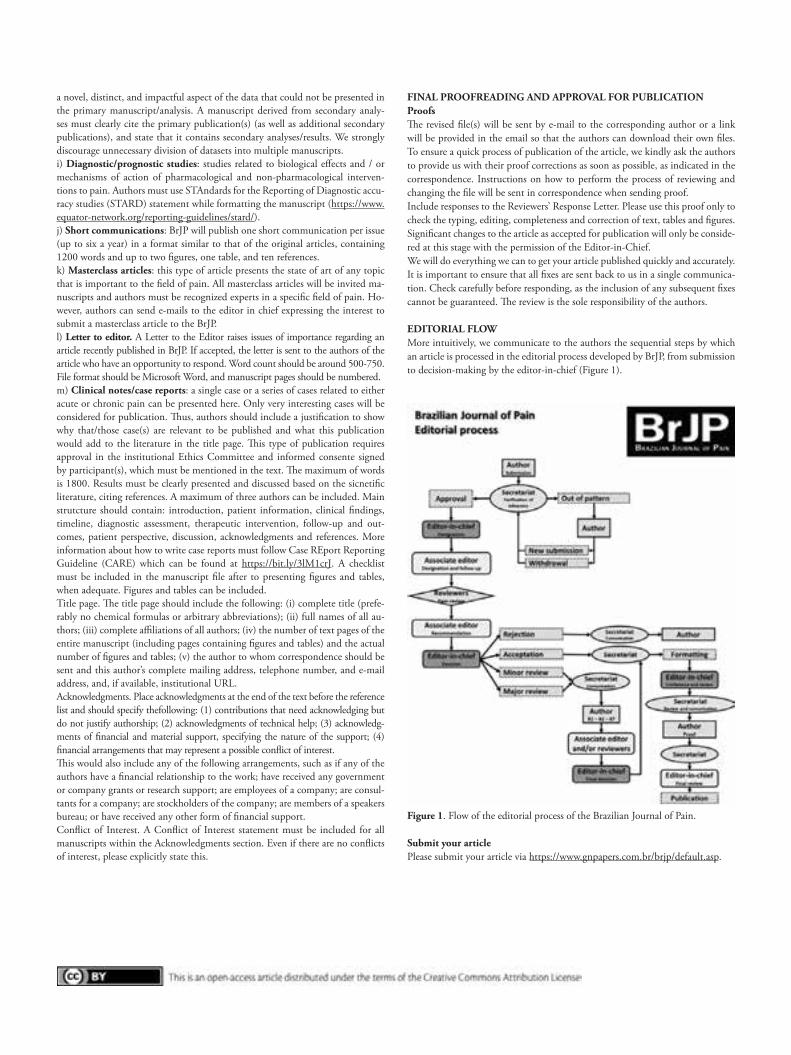
a novel, distinct, and impactful aspect of the data that could not be presented in the primary manuscript/analysis. A manuscript derived from secondary analy-ses must clearly cite the primary publication(s) (as well as additional secondary publications), and state that it contains secondary analyses/results. We strongly discourage unnecessary division of datasets into multiple manuscripts.i) Diagnostic/prognostic studies: studies related to biological effects and / or mechanisms of action of pharmacological and non-pharmacological interven-tions to pain. Authors must use STAndards for the Reporting of Diagnostic accu-racy studies (STARD) statement while formatting the manuscript (https://www.equator-network.org/reporting-guidelines/stard/).j) Short communications: BrJP will publish one short communication per issue (up to six a year) in a format similar to that of the original articles, containing 1200 words and up to two figures, one table, and ten references.k) Masterclass articles: this type of article presents the state of art of any topic that is important to the field of pain. All masterclass articles will be invited ma-nuscripts and authors must be recognized experts in a specific field of pain. Ho-wever, authors can send e-mails to the editor in chief expressing the interest to submit a masterclass article to the BrJP.l) Letter to editor. A Letter to the Editor raises issues of importance regarding an article recently published in BrJP. If accepted, the letter is sent to the authors of the article who have an opportunity to respond. Word count should be around 500‐750. File format should be Microsoft Word, and manuscript pages should be numbered.m) Clinical notes/case reports: a single case or a series of cases related to either acute or chronic pain can be presented here. Only very interesting cases will be considered for publication. Thus, authors should include a justification to show why that/those case(s) are relevant to be published and what this publication would add to the literature in the title page. This type of publication requires approval in the institutional Ethics Committee and informed consente signed by participant(s), which must be mentioned in the text. The maximum of words is 1800. Results must be clearly presented and discussed based on the sicnetific literature, citing references. A maximum of three authors can be included. Main strutcture should contain: introduction, patient information, clinical findings, timeline, diagnostic assessment, therapeutic intervention, follow-up and out-comes, patient perspective, discussion, acknowledgments and references. More information about how to write case reports must follow Case REport Reporting Guideline (CARE) which can be found at https://bit.ly/3lM1crJ. A checklist must be included in the manuscript file after to presenting figures and tables, when adequate. Figures and tables can be included. Title page. The title page should include the following: (i) complete title (prefe-rably no chemical formulas or arbitrary abbreviations); (ii) full names of all au-thors; (iii) complete affiliations of all authors; (iv) the number of text pages of the entire manuscript (including pages containing figures and tables) and the actual number of figures and tables; (v) the author to whom correspondence should be sent and this author’s complete mailing address, telephone number, and e‐mail address, and, if available, institutional URL. Acknowledgments. Place acknowledgments at the end of the text before the reference list and should specify thefollowing: (1) contributions that need acknowledging but do not justify authorship; (2) acknowledgments of technical help; (3) acknowledg-ments of financial and material support, specifying the nature of the support; (4) financial arrangements that may represent a possible conflict of interest. This would also include any of the following arrangements, such as if any of the authors have a financial relationship to the work; have received any government or company grants or research support; are employees of a company; are consul-tants for a company; are stockholders of the company; are members of a speakers bureau; or have received any other form of financial support.Conflict of Interest. A Conflict of Interest statement must be included for all manuscripts within the Acknowledgments section. Even if there are no conflicts of interest, please explicitly state this.
FINAL PROOFREADING AND APPROVAL FOR PUBLICATIONProofs The revised file(s) will be sent by e-mail to the corresponding author or a link will be provided in the email so that the authors can download their own files. To ensure a quick process of publication of the article, we kindly ask the authors to provide us with their proof corrections as soon as possible, as indicated in the correspondence. Instructions on how to perform the process of reviewing and changing the file will be sent in correspondence when sending proof. Include responses to the Reviewers’ Response Letter. Please use this proof only to check the typing, editing, completeness and correction of text, tables and figures. Significant changes to the article as accepted for publication will only be conside-red at this stage with the permission of the Editor-in-Chief. We will do everything we can to get your article published quickly and accurately. It is important to ensure that all fixes are sent back to us in a single communica-tion. Check carefully before responding, as the inclusion of any subsequent fixes cannot be guaranteed. The review is the sole responsibility of the authors.
EDITORIAL FLOWMore intuitively, we communicate to the authors the sequential steps by which an article is processed in the editorial process developed by BrJP, from submission to decision-making by the editor-in-chief (Figure 1).
Figure 1. Flow of the editorial process of the Brazilian Journal of Pain.
Submit your article Please submit your article via https://www.gnpapers.com.br/brjp/default.asp.