β-lactam/β-lactamase inhibitor combinations: from then to now
TRANSCRIPT

Annals of Pharmacotherapy 1 –13© The Author(s) 2014Reprints and permissions: sagepub.com/journalsPermissions.navDOI: 10.1177/1060028014556652aop.sagepub.com
Review Article
Backgroundβ-Lactam antibiotics have been the backbone of treatment for a variety of infections for more than 70 years.1 Unfortunately, increasing resistance to these antibiotics limits their utility. One of the primary mechanisms of bacte-rial resistance to β-lactams is through the production of β-lactamase enzymes.1 β-Lactam/β-lactamase inhibitor combinations (BLICs) are particularly useful for the treat-ment of infections caused by organisms that produce β-lactamases. However, bacterial evolution has progressed; bacteria that are resistant to most or even all β-lactams, such as carbapenem-resistant Enterobacteriaceae (CRE), are proliferating.2 The recent increase in these organisms and their associated effect on mortality worldwide presents an urgent need for both additional therapeutic options and increased antimicrobial stewardship.3,4 The objective of this article is for the reader to be able to recognize the clinical utility of the historical BLICs and to understand the poten-tial uses of the new BLICs in the pipeline. We review the spectrum of activity (microbiological and enzymatic) and
discuss controversy associated with BLIC use for some organisms. Clinical and microbiological data supporting the pipeline BLICs is described and discussed. For the sake of clarity, a brief review of β-lactamases is included; for more information, the reader is directed to several excellent reviews.5-7
Data SourcesA systematic electronic literature search using the MEDLINE database was performed using the search terms β-lactamase, β-lactamase inhibitor, clavulanate, sulbac-tam, tazobactam, avibactam, NXL104, relebactam, and RPX7009. English-language studies published from 1960 to
556652 AOPXXX10.1177/1060028014556652Annals of PharmacotherapyToussaint and Gallagherresearch-article2014
1Temple University School of Pharmacy, Philadelphia, PA, USA
Corresponding Author:Kimberly A. Toussaint, Pharmacy Practice Department, Temple University School of Pharmacy, 3307 N Broad St, Philadelphia, PA 19140, USA. Email: [email protected]
β-Lactam/β-Lactamase Inhibitor Combinations: From Then to Now
Kimberly A. Toussaint, PharmD1, and Jason C. Gallagher, PharmD1
AbstractObjective: To review the available evidence regarding the utility of the currently available β-lactam/β-lactamase inhibitor combinations (BLICs) as well as the emerging body of data for the novel agents in the pipeline. Data Sources: A MEDLINE literature search (1960-August 2014) was performed using the search terms β-lactamase, β-lactamase inhibitor, clavulanate, sulbactam, tazobactam, avibactam, NXL104, MK-7655, and RPX7009. Current studies focusing on new agents were obtained from clinicaltrials.gov. Additional references were identified from a review of literature citations and meeting abstracts. Study Selection and Data Extraction: All English-language studies pertaining to BLICs were evaluated. Data Synthesis: Historical clinical and in vitro data focusing on the characteristics of the conventional BLICs are reviewed. Avibactam, relebactam (formerly MK-7655), and RPX7009 are new β-lactamase inhibitors that are being studied in combination with β-lactams. Clinical and in vitro data that provide support for their use for multidrug-resistant organisms are reviewed. β-Lactam antibiotics are a mainstay for the treatment of many infections. The addition of β-lactamase inhibitors enhances their activity against organisms that produce β-lactamases; however, organisms that produce extended-spectrum β-lactamases, AmpC β-lactamases, and carbapenemases are proliferating. The BLICs (amoxicillin/clavulanate, ticarcillin/clavulanate, ampicillin/sulbactam, and piperacillin/tazobactam) lack activity against some of these enzymes, presenting a critical need for new antibiotics. Conclusions: The historical BLICs are useful for many infections; however, evolving resistance limits their use. The new BLICs (combinations with avibactam, relebactam, and RPX7009) may be valuable options for patients infected with multidrug-resistant organisms.
Keywordsbacterial resistance, β-lactamase, carbapenemase, β-lactamase inhibitor, clavulanate, tazobactam, sulbactam, avibactam, MK-7655, relebactam, RPX7009
at TEMPLE UNIV on November 3, 2014aop.sagepub.comDownloaded from

2 Annals of Pharmacotherapy
August 2014 were considered. Current trials focusing on new agents were obtained from clinicaltrials.gov. Additional references were identified from conference proceedings and citations in relevant review articles.
β-Lactamase EnzymesThough multiple mechanisms of resistance exist, the most common cause of bacterial resistance to β-lactam antibiot-ics is through the production of β-lactamase enzymes.5 These enzymes deactivate β-lactam antibiotics by binding covalently to their carbonyl moiety and hydrolyzing the β-lactam ring. The effect of these enzymes ranges from slight to complete inhibition of antibiotic activity and varies depending on the quantity of enzyme production.6 β-Lactamases are produced extracellularly by Gram-positive organisms and in the periplasmic space by Gram-negative organisms.7,8 Genes for β-lactamase enzymes can be transmitted on plasmids (plasmid mediated) or encoded within an organism’s chromosome (chromosomally medi-ated).9-11 Transferrable plasmid-mediated genes often encode for diverse resistance mechanisms, allowing them to express resistance to multiple and unrelated antibiotics.8 With some organisms, exposure to a β-lactam antibiotic can cause the induction of enzyme production, resulting in high concentrations of β-lactamase, which leads to clinical resis-tance.12 It should be noted that low levels of β-lactamase may increase the minimum inhibitory concentration (MIC) of an organism within the susceptible range and that some-times the expression of multiple mechanisms of resistance are required for non-susceptibility.13
ClassificationMore than 1400 β-lactamase enzymes have been identi-fied.14 This large group of enzymes is heterogeneous, and each β-lactamase exhibits its own spectrum of hydrolysis for specific antibiotics.15 Classification is done primarily by
1 of 2 schemes: the Ambler and Bush-Jacoby classifica-tions. The Bush-Jacoby classification consists of 4 groups based on molecular class and functional groups, whereas the Ambler classification is based on the genetic amino acid sequences and phenotypic properties of the enzymes.16,17 For the purposes of this article, we will focus on the Ambler classifications (Table 110,12,18-27). Ambler class A enzymes can be subdivided into class A narrow-spectrum β-lactamases, extended-spectrum β-lactamases (ESBLs), and serine carbapenemases. They are the most prevalent in the Enterobacteriaceae family.13 Class A narrow-spectrum β-lactamases and ESBLs are generally inhibited in vitro by sulbactam, clavulanate, and tazobactam, and they cannot destroy carbapenems. However, the expression of newly evolved class A carbapenemases by Enterobacteriaceae is a major health concern. These enzymes possess the same drug-hydrolyzing activity as ESBLs as well as the addi-tional ability to inactivate carbapenems.20 Class B enzymes are metallo-β-lactamases that are characterized by a zinc atom at the active site. These enzymes are generally not inhibited by the currently available β-lactamase inhibitors but are inhibited by metal ion chelators such as edetic acid.21,22 Class C enzymes are produced by Gram-negative organisms and are usually chromosomally mediated, though plasmid-mediated class C β-lactamases exist and can be exchanged by conjugation.10 These enzymes are often inducible and include AmpC enzymes.23 The overuse of third-generation cephalosporins has been associated with the selection and promotion of these β-lactamases.8,24 Hyperproduction of AmpC β-lactamases characteristically provides resistance to many extended-spectrum cephalo-sporins, and the genes for these enzymes are chromosom-ally encoded by the “SPACE” genera (Serratia, Pseudomonas, Acinetobacter, Citrobacter, and Enterobacter) and some others, such as Providencia species and Morganella morganii. High levels of AmpC production in combination with other mechanisms of resistance, such as porin channel changes, can lead to resistance to
Table 1. β-Lactamases (Ambler Classification).
TypeAmbler Molecular
Class Characteristics Examples of Enzymes
Narrow-spectrum β-lactamases12,18,19
A Hydrolyze penicillin; produced primarily by Enterobacteriaceae
Staphylococcal penicillinase, TEM-1, TEM-2, SHV-1
Extended-spectrum β-lactamases20
A Hydrolyze narrow and extended-spectrum β-lactam antibiotics
SHV-2, CTX-M-15, PER-1, VEB-1
Serine carbapenemases20 A Hydrolyze carbapenems KPC-1, IMI-1, SME-1Metallo-β-lactamases21,22 B Hydrolyze carbapenems VIM-1, IMP-1, NDM-1Cephalosporinases10,23,24 C Hydrolyze cephamycins and some oxyimino β-
lactams; inducible; chromosomally mediatedAmpC, P99, ACT-1, CMY-2,
FOX-1, MIR-1OXA-type enzymes25-27 D Hydrolyze oxacillin, oxyimino β-lactams, and
carbapenems; produced by Pseudomonas aeruginosa and Acinetobacter baumannii
OXA enzymes
at TEMPLE UNIV on November 3, 2014aop.sagepub.comDownloaded from

Toussaint and Gallagher 3
carbapenems as well.13 Finally, class D enzymes include OXA enzymes, most of which are ESBLs and carbapene-mases.25 In contrast to class A ESBLs and carbapenemases, which are generally produced by Enterobacteriaceae, OXA enzymes are primarily produced by Pseudomonas aerugi-nosa and Acinetobacter baumanni.26,27
β-Lactamase Inhibitors
PropertiesIn the mid-1960s, research on compounds that could inhibit β-lactamases was conducted in response to the increasing frequency of β-lactamase-producing organisms. The first β-lactamase inhibitor, clavulanate (or clavulanic acid), was identified from Streptomyces clavuligerus in 1972, fol-lowed by sulbactam in 1978 and tazobactam in 1984.28-30 These β-lactamase inhibitors are structurally similar to pen-icillin but have weak antibacterial activity alone. When administered in combination with β-lactam antibiotics, they irreversibly bind β-lactamases and protect the active antibi-otic from inactivation.29,30 This restores the activity of the parent drug against organisms that produce many types of β-lactamases.
There are 4 BLICs that are widely used in the United States: amoxicillin/clavulanate, ticarcillin/clavulanate, ampicillin/sulbactam, and piperacillin/tazobactam. These combinations all undergo hepatic metabolism and urinary excretion and require dose adjustment in renal dysfunction.
These antibiotics have favorable tissue penetration, includ-ing the skin, lungs, gastrointestinal tract, and urine. All 4 BLICs exhibit time-dependent, bactericidal activity.7,31
The first BLIC was amoxicillin/clavulanate, available in Europe in 1981 and in the United States in 1984. Amoxicillin/clavulanate remains the only marketed oral BLIC today. Clavulanate was available in combination with ticarcillin starting in 1985, and this combination was the first paren-teral BLIC available.7 Sulbactam, a semisynthetic β-lactamase inhibitor, is available in the United States as ampicillin/sulbactam, which was approved in 1987.7 Like the other β-lactamase inhibitors, sulbactam has weak anti-bacterial activity alone but is active against Acinetobacter species and has been used clinically for this organism.32,33 Tazobactam has a similar structure to sulbactam and was originally developed with piperacillin.34
ComparisonThe 4 historical BLICs are generally active against class A β-lactamase enzymes, but their level of activity differs between the inhibitors (Table 2). Although the BLICs are active against organisms producing many types of β-lactamases, there is controversy surrounding their clinical use for some infections. These combinations do not have activity against carbapenemases and do not have clinically useful activity against class C enzymes such as AmpC.19 Additionally, they do not have activity against most class B or class D enzymes.35,36
Table 2. β-Lactamase Inhibitor Combinations.
Inhibitor Spectrum Combination Antibiotics
Clavulanic acid28-30 Class A narrow spectrum AmoxicillinClass A ESBLs Ticarcillin
Tazobactam6,39 Class A narrow spectrum PiperacillinClass A ESBLs CeftolozaneSome class C enzymes
Sulbactam19,35,37 Class A narrow spectrum AmpicillinClass A ESBLs Piperacillin Cefoperazone
Avibactam46-48 Class A narrow spectrum CeftarolineClass A ESBLs CeftazidimeClass A carbapenemases AztreonamSome class C and class D enzymes
MK-765575,76 Class A narrow spectrum ImipenemClass A ESBLs Class A carbapenemases Some class C enzymes
RPX700983,84,85 Class A narrow spectrum BiapenemClass A ESBLs Class A carbapenemases Some class C enzymes
Abbreviation: ESBL, extended-spectrum β-lactamase.
at TEMPLE UNIV on November 3, 2014aop.sagepub.comDownloaded from

4 Annals of Pharmacotherapy
In practical terms, all the BLICs are useful against infec-tions caused by organisms that produce many types of plas-mid-mediated β-lactamases, including class A narrow-spectrum β-lactamases and class A ESBLs. Although sulbactam is not as potent as tazobactam and cla-vulanate,37 its advantages include greater stability, less like-lihood of inducing chromosomal β-lactamases compared with clavulanate, and enhanced intrinsic antibacterial activ-ity against certain organisms. For infections caused by P aeruginosa, piperacillin/tazobactam and ticarcillin/clavula-nate are useful. This is because of the activity of the parent β-lactam because most resistance to Pseudomonas is the result of impermeability or an efflux pump rather than β-lactamase production.38 However, clavulanate can induce AmpC production in Pseudomonas, leading to antagonism of ticarcillin.10
Novel BLICs
Ceftolozane/TazobactamCeftolozane is a novel oxyimino-aminothiazolyl cephalos-porin that has activity against many Gram-negative bacilli and has potent activity against P aeruginosa. In vitro stud-ies suggest that ceftolozane has greater bactericidal activity against P aeruginosa than ceftazidime and is active against carbapenem-resistant strains.39 Ceftolozane is susceptible to destruction by ESBLs, and the addition of tazobactam to ceftolozane has been shown in vitro to substantially increase its activity against organisms producing ESBLs.39
Ceftolozane/tazobactam has been granted fast-track sta-tus by the Food and Drug Administration (FDA). Phase III study results in studies of complicated urinary tract infec-tions (cUTIs) and complicated intra-abdominal infections (cIAIs) have yet to be published but were presented in 2014 (Table 3).40,41 For cUTIs, ceftolozane/tazobactam was supe-rior to levofloxacin in the outcomes of composite cure and microbiological eradication. Ceftolozane/tazobactam was superior in the large subset of patients with infections caused by Enterobacteriaceae (281/316, 88.9% vs 255/327, 78.0%; P < 0.001). Notably, composite cure (microbiologi-cal and clinical combined) was also higher for ceftolozane/tazobactam among ESBL-producing organisms (62.3% vs 35.1%, P < 0.05). Microbiological eradication rates for ESBL-producing Escherichia coli were 27/36 (75%) for ceftolozane/tazobactam and 18/36 (50%) for levofloxacin (P = 0.051). Microbiological eradication rates for ESBL-producing Klebsiella pneumoniae were 7/10 (70%) for ceftolozane/tazobactam and 2/7 (28.6%) for levofloxacin (P = 0.15). The number of patients with P aeruginosa infec-tions was too small to determine differences between agents (ceftolozane/tazobactam 6/7 [85.7%] vs levofloxacin 7/12 [58.3%], P > 0.05). Microbiological eradication was lower for ceftolozane/tazobactam than levofloxacin for Enterobacter cloacae (2/6, 33.3%, vs 6/7, 85.7%, P < 0.05)
and for Gram-positive aerobes as well (8/21, 38.1%, vs 16/20, 80.0%, P < 0.05).40
Ceftolozane/tazobactam 1.5 g IV every 8 hours in com-bination with metronidazole 500 mg IV every 8 hours was noninferior to meropenem 1 g IV every 8 hours for clinical cure of cIAI. The most common pathogens were Escherichia coli (n = 426), K pneumoniae (n = 53), and P aeruginosa (n = 53). The ceftolozane/tazobactam group had high rates of eradication among Enterobacteriaceae, including all ESBL-producing isolates of Escherichia coli (14/14, 100%) and K pneumoniae (6/6, 100%). Success rates in the ceftolo-zane/tazobactam group were also high for P aeruginosa (25/25, 100%).41 These rates were not significantly higher than those with meropenem (see Table 3).
Taken together, these studies show the utility of ceftolo-zane/tazobactam against clinically important pathogens in these commonly studied infections. Though one of the most important attributes of ceftolozane/tazobactam is its potency against P aeruginosa, the utility against ESBL-producing Enterobacteriaceae seen in the studies is reassuring and helps position the drug for empirical use in settings where these organisms are common. Although the numbers were small, the poor results against Enterobacter cloacae are concerning and will require further clinical data to eluci-date. An ongoing study of hospital-acquired pneumonia should help elicit the clinical utility of the drug for Pseudomonas infections.42
AvibactamAvibactam (formerly NXL104) is a β-lactamase inhibitor from the novel diazabicyclooctane class.43 Avibactam is a covalent, reversible, non-β-lactam β-lactamase inhibitor.44 Instead of the 4-membered β-lactam ring, avibactam has a 5-membered ring with an amide group that targets the active-site serine of β-lactamases.45 Like the other β-lactamase inhibitors, avibactam has very little antibiotic activity alone. However, in combination with a β-lactam, it can inhibit a broad range of β-lactamases, including class A, class C, and some class D enzymes.46-48 Avibactam is the most potent β-lactamase inhibitor to date because only 1 to 5 molecules are required to inhibit 1 molecule of β-lactamase, compared with >50 for tazobactam and clavu-lanate.49 Avibactam deacylates slowly instead of undergo-ing reactive transformation to an irreversible complex as is the case with historical β-lactamase inhibitors.43,50 Avibactam is currently in phase III studies with ceftazi-dime,51,52 phase II studies with ceftaroline,53 and a phase I study with aztreonam.54
Ceftazidime/AvibactamThe addition of avibactam restores the intrinsic activity of ceftazidime against many organisms, including multidrug resistant (MDR) Enterobacteriaceae that produce class A
at TEMPLE UNIV on November 3, 2014aop.sagepub.comDownloaded from
5
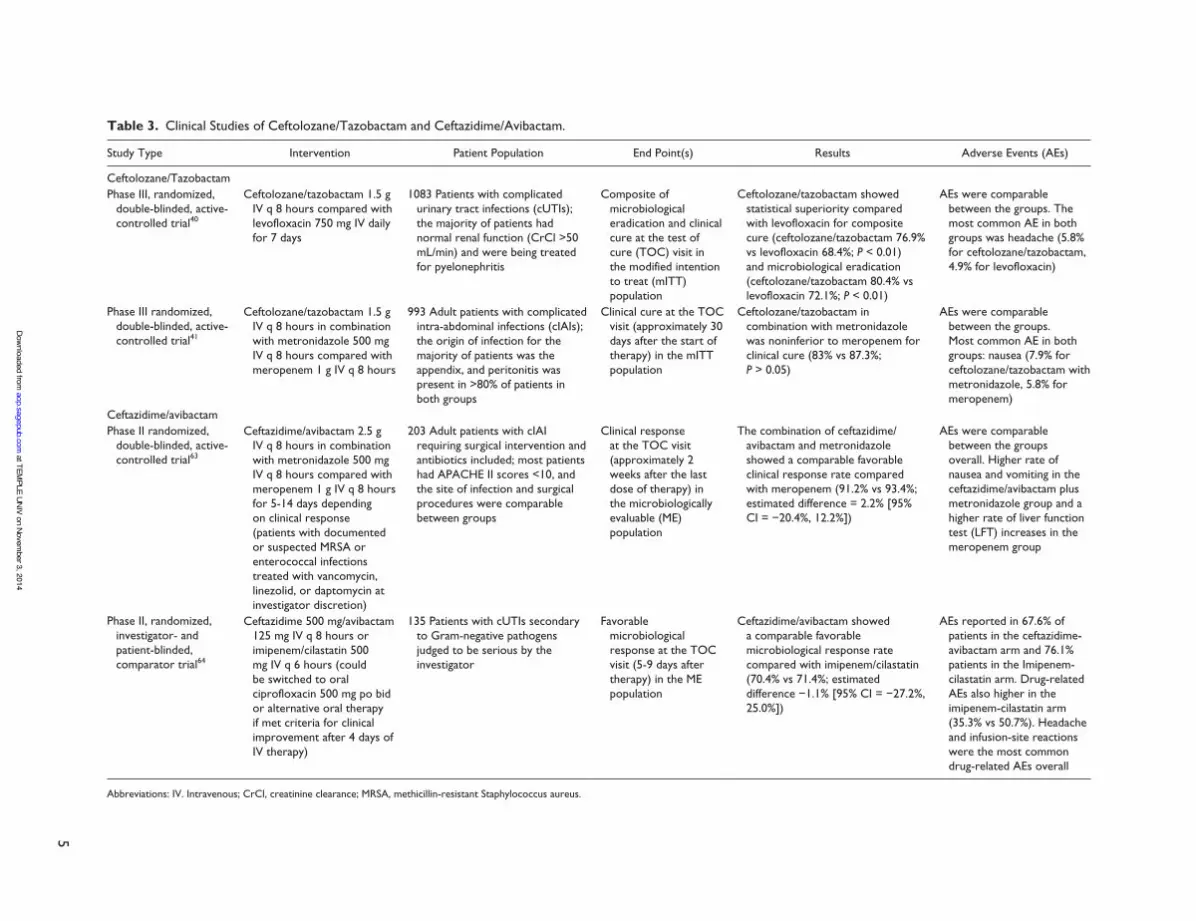
Table 3. Clinical Studies of Ceftolozane/Tazobactam and Ceftazidime/Avibactam.
Study Type Intervention Patient Population End Point(s) Results Adverse Events (AEs)
Ceftolozane/TazobactamPhase III, randomized,
double-blinded, active-controlled trial40
Ceftolozane/tazobactam 1.5 g IV q 8 hours compared with levofloxacin 750 mg IV daily for 7 days
1083 Patients with complicated urinary tract infections (cUTIs); the majority of patients had normal renal function (CrCl >50 mL/min) and were being treated for pyelonephritis
Composite of microbiological eradication and clinical cure at the test of cure (TOC) visit in the modified intention to treat (mITT) population
Ceftolozane/tazobactam showed statistical superiority compared with levofloxacin for composite cure (ceftolozane/tazobactam 76.9% vs levofloxacin 68.4%; P < 0.01) and microbiological eradication (ceftolozane/tazobactam 80.4% vs levofloxacin 72.1%; P < 0.01)
AEs were comparable between the groups. The most common AE in both groups was headache (5.8% for ceftolozane/tazobactam, 4.9% for levofloxacin)
Phase III randomized, double-blinded, active-controlled trial41
Ceftolozane/tazobactam 1.5 g IV q 8 hours in combination with metronidazole 500 mg IV q 8 hours compared with meropenem 1 g IV q 8 hours
993 Adult patients with complicated intra-abdominal infections (cIAIs); the origin of infection for the majority of patients was the appendix, and peritonitis was present in >80% of patients in both groups
Clinical cure at the TOC visit (approximately 30 days after the start of therapy) in the mITT population
Ceftolozane/tazobactam in combination with metronidazole was noninferior to meropenem for clinical cure (83% vs 87.3%; P > 0.05)
AEs were comparable between the groups. Most common AE in both groups: nausea (7.9% for ceftolozane/tazobactam with metronidazole, 5.8% for meropenem)
Ceftazidime/avibactamPhase II randomized,
double-blinded, active-controlled trial63
Ceftazidime/avibactam 2.5 g IV q 8 hours in combination with metronidazole 500 mg IV q 8 hours compared with meropenem 1 g IV q 8 hours for 5-14 days depending on clinical response (patients with documented or suspected MRSA or enterococcal infections treated with vancomycin, linezolid, or daptomycin at investigator discretion)
203 Adult patients with cIAI requiring surgical intervention and antibiotics included; most patients had APACHE II scores <10, and the site of infection and surgical procedures were comparable between groups
Clinical response at the TOC visit (approximately 2 weeks after the last dose of therapy) in the microbiologically evaluable (ME) population
The combination of ceftazidime/avibactam and metronidazole showed a comparable favorable clinical response rate compared with meropenem (91.2% vs 93.4%; estimated difference = 2.2% [95% CI = −20.4%, 12.2%])
AEs were comparable between the groups overall. Higher rate of nausea and vomiting in the ceftazidime/avibactam plus metronidazole group and a higher rate of liver function test (LFT) increases in the meropenem group
Phase II, randomized, investigator- and patient-blinded, comparator trial64
Ceftazidime 500 mg/avibactam 125 mg IV q 8 hours or imipenem/cilastatin 500 mg IV q 6 hours (could be switched to oral ciprofloxacin 500 mg po bid or alternative oral therapy if met criteria for clinical improvement after 4 days of IV therapy)
135 Patients with cUTIs secondary to Gram-negative pathogens judged to be serious by the investigator
Favorable microbiological response at the TOC visit (5-9 days after therapy) in the ME population
Ceftazidime/avibactam showed a comparable favorable microbiological response rate compared with imipenem/cilastatin (70.4% vs 71.4%; estimated difference −1.1% [95% CI = −27.2%, 25.0%])
AEs reported in 67.6% of patients in the ceftazidime-avibactam arm and 76.1% patients in the Imipenem-cilastatin arm. Drug-related AEs also higher in the imipenem-cilastatin arm (35.3% vs 50.7%). Headache and infusion-site reactions were the most common drug-related AEs overall
Abbreviations: IV. Intravenous; CrCl, creatinine clearance; MRSA, methicillin-resistant Staphylococcus aureus.
at TEMPLE U
NIV on N
ovember 3, 2014
aop.sagepub.comD
ownloaded from

6 Annals of Pharmacotherapy
(TEM-, SHV-, KPC- and CTX-M) and class C enzymes. Additionally, this combination has been shown to have sig-nificantly increased activity against Pseudomonas com-pared with ceftazidime alone, with studies showing up to a 4-fold reduction in MIC.55-58 The addition of avibactam combats mechanisms of Pseudomonas resistance to antip-seudomonal cephalosporins, including both hyperproduc-tion of chromosomal AmpC β-lactamases and the expression of acquired ESBLs.59 One study of 126 highly resistant P aeruginosa strains found that the addition of avibactam changed ceftazidime resistance from 35% with ceftazidime alone to 6% with the combination.55
Carbapenemases are a pressing resistance issue that sig-nificantly reduces β-lactam utility. Ceftazidime/avibactam has shown promising activity against CRE in multiple stud-ies. In addition to its activity against ESBL-producing organisms such as CTX-M type K pneumoniae and Escherichia coli, ceftazidime/avibactam is also active against those organisms expressing carbapenem resistance. Ceftazidime/avibactam was found to be highly active against nonfermenting Gram-negative bacilli producing OXA-48 carbapenemases.60,61 However, ceftazidime/avi-bactam has not been shown to be active against class B NDM-type carbapenemases.
Combinations of avibactam with cephalosporins have only moderate activity against anaerobes. Though many strains of clinically important anaerobes are susceptible to combinations of avibactam and cephalosporins, to increase activity against anaerobic bacteria, adjunctive metronida-zole is being administered in clinical trials where these organisms are clinically important.62 Adjunctive metronida-zole should be considered in suspected intra-abdominal infections being treated with ceftazidime/avibactam.62
Clinical Data: Ceftazidime/AvibactamCeftazidime/avibactam was evaluated in 2 phase II studies for the treatment of cIAIs and cUTIs (Table 3). Ceftazidime/avibactam with metronidazole had comparable clinical and microbiological responses compared with meropenem for the treatment of cIAI. The primary pathogen was Escherichia coli, and all of these were susceptible to both ceftazidime/avibactam and meropenem. In the ceftazidime/avibactam arm, the majority of patients with infections who were non-susceptible to ceftazidime alone at baseline (25/26, 96.2%) had a favorable microbiological response.63 These results support the results of the aforementioned in vitro studies and showed that ceftazidime/avibactam is effective against ceftazidime-nonsusceptible organisms.
The second trial evaluated the use of ceftazidime/avibac-tam compared with imipenem/cilastatin for the treatment of serious cUTIs. The majority of patients were women with pyelonephritis (44/68 [64.7%] in the ceftazidime/avibactam group and 41/67 [61.2%] in the imipenem/cilastatin group).
Concomitant bacteremia was seen in only 3/68 (4.4%) patients in the ceftazidime/avibactam group and 4/67 (6.0%) patients in the imipenem/cilastatin group. The pri-mary pathogen was Escherichia coli. All the 63 isolated pathogens were susceptible to imipenem based on CSLI cri-teria, whereas 20 of them were resistant to ceftazidime alone. Favorable microbiological response in the microbio-logical-evaluable population was found in 19/27 (70.4%) patients in the ceftazidime/avibactam group and 25/35 (71.4%) patients in the imipenem/cilastatin group (observed difference = −1.1% [95% CI = −27.2%, 25.0%]). Among pathogens resistant to ceftazidime alone, favorable response at the TOC visit was obtained in 6/7 (85.7%) patients in the ceftazidime/avibactam group and 9/11 (81.8%) patients in the imipenem/cilastatin group. The authors concluded that the efficacy and safety of ceftazidime/avibactam is compa-rable to that of imipenem/cilastatin.64
Several other phase II studies involving ceftazidime/avi-bactam have been completed but the data have not yet been reported.65 Phase III trials for ceftazidime/avibactam in cUTIs and cIAIs are under way.66 Until more experience in treating resistant pathogens is gained, the types of studies required by the drug approval process are unlikely to reveal much about the utility of ceftazidime/avibactam in highly resistant infections, leading clinicians to abstract the value of this agent in difficult situations such as carbapenem-resistant infections based on in vitro results and clinical studies with more susceptible pathogens. These pathogens have not been seen in the phase II studies of ceftazidime/avibactam described to date.
Ceftaroline/AvibactamCeftaroline was FDA approved in 2010 for community-acquired bacterial pneumonia (CABP) and acute bacterial skin and skin structure infections. This cephalosporin pos-sesses activity against Streptococcus pneumoniae and Staphylococcus aureus, including methicillin-resistant Staphylococcus aureus (MRSA).67,68 Although ceftaroline may have utility for a variety of infections because of its broad coverage of Gram-positive and Gram-negative organ-isms, it is hydrolyzed by the increasingly prevalent ESBL, AmpC, and carbapenemase enzymes that Gram-negative organisms can produce.69 Ceftaroline is not active against P aeruginosa or other nonfermenting Gram-negative organ-isms, and the addition of avibactam does not give ceftaro-line this activity.69
Similar to ceftazidime, the addition of avibactam expands the spectrum of ceftaroline to include many MDR Enterobacteriaceae. In a study of more than 20 000 con-temporary bacterial isolates from US medical centers, cef-taroline/avibactam was found to be highly active against Enterobacteriaceae (98.5% susceptibility using the FDA, CLSI [Clinical Laboratory Standards Institute], and
at TEMPLE UNIV on November 3, 2014aop.sagepub.comDownloaded from

Toussaint and Gallagher 7
EUCAST (the European Committee on Antimicrobial Susceptibility Testing) breakpoints for ceftaroline as ≤0.5 µg/mL), including Klebsiella species, Escherichia coli, and Enterobacter cloacae, with only 0.2% of isolates with MICs in the likely resistance range (MIC >2 µg/mL). Ceftaroline/avibactam was found to be active against 90.8% of K pneu-moniae and 98.7% of Escherichia coli strains that were clas-sified as ESBL phenotype. Additionally, 68% of carbapenem-resistant K pneumoniae strains were found to be susceptible to ceftaroline/avibactam. Another study evaluat-ing ceftaroline/avibactam against more than 400 Gram-positive and Gram-negative isolates from 15 clinical species showed high activity against isolates carrying plasmid-medi-ated AmpC enzymes, with all isolates found to be susceptible, including those that were ceftazidime resistant. Ceftaroline/avibactam showed activity against organisms that produced serine carbapenemases, inhibiting 84% of strains at an MIC ≤1 µg/mL. Additionally, ceftaroline/avibactam was shown to be active against 90% of strains of Enterobacteriaceae pro-ducing multiple β-lactamases.70 Although these data provide support that ceftaroline/avibactam shows promising activity against ESBL-, AmpC-, and serine carbapenemase-producing organisms, multiple studies have shown that ceftaroline/avi-bactam has little activity against isolates expressing metallo-β-lactamases such as bacteria producing NDM-1.69,70
Clinical Data: Ceftaroline/AvibactamCeftaroline/avibactam was studied in a phase II trial com-paring it to doripenem for complicated cUTI, but results are not yet available.53 Participants are currently being recruited for a pharmacokinetic study of ceftaroline/avibactam in adults with an augmented renal clearance. Additionally, a phase I, open-label, multiple-dose, single-center study is being planned to investigate the effect of ceftaroline/avi-bactam and ceftazidime/avibactam on the intestinal flora of healthy volunteers.71 Phase III studies of ceftaroline/avibac-tam are likely to be initiated.
Aztreonam/AvibactamAvibactam is currently being investigated in combination with aztreonam in a phase I, randomized, double-blind, 3-part study that investigates the safety and tolerability of the combination in healthy individuals.72 Because aztreo-nam is stable against many metallo-β-lactamases but sus-ceptible to other β-lactamases that organisms containing metallo-β-lactamases often coexpress, this combination could be useful in practice. Avibactam would protect aztre-onam from many β-lactamases, and aztreonam itself would be stable against metallo-β-lactamases. The combination may be useful against organisms producing NDM-type car-bapenemases; however, clinical trials need to be conducted to determine its clinical efficacy.20,72,73
RelebactamRelebactam (formerly MK-7655) is a β-lactamase inhibitor in clinical development that has a similar structure to avi-bactam, with the addition of a piperidine ring. Like avibac-tam, relebactam is active against class A and C enzymes in vitro.74 The combination of relebactam and imipenem has shown synergistic activity against various MDR organisms.
Imipenem/RelebactamThe addition of relebactam to imipenem has shown sig-nificant reductions in MICs and synergistic killing for resistant strains of P aeruginosa and K pneumoniae in several in vitro studies.74-76 The greatest effect of the combination of imipenem/relebactam seems to be on K pneumoniae isolates that express KPCs and ESBLs as well as on P aeruginosa isolates that overexpress AmpC and lack the OrpD porin, a combination associated with decreased antibiotic uptake and imipenem resistance. In a study that evaluated this combination against Enterobacteriaceae, Pseudomonas, and other nonfermen-ters with various resistance mechanisms, it was observed that in those isolates dependent on resistance based on combinations of β-lactamase activity and impermeability, the MICs of imipenem were decreased from 2 to 16 µg/mL, to <1 µg/mL.76 In a study that evaluated >200 P aerugi-nosa clinical isolates, most of which were not susceptible to imipenem, the addition of relebactam restored suscepti-bility of the majority of the organisms.77 The addition of relebactam reduced MICs of the organisms to imipenem significantly, lowering the MICs to <4 µg/mL (the 2009 CLSI breakpoint for resistance)78 of 69% of organisms with MICs to imipenem of 32 µg/mL, 95% of those with MICs of 16 µg/mL, and 100% of those with MICs of 8 µg/mL. However, it is unknown how many MICs were reduced to the current breakpoint MIC of 1 µg/mL.79 These data provide support for future studies examining the effect of this combination on AmpC- and KPC-producing Gram-negative organisms. For organisms that express certain class B and D carbapenemases (OXA-48, IMP, NDM, and VIM), MICs remained in the resistant range even after the addition of relebactam.77
Clinical Data: RelebactamRelebactam is not as far along in clinical development as avibactam combinations or ceftolozane/tazobactam, so not much clinical data are available. Two phase 2 studies are currently under way to evaluate imipenem/cilastatin in combination with relebactam and imipenem/cilastatin alone for both cUTIs and cIAIs.80,81 Phase III studies are planned for 2015.82
at TEMPLE UNIV on November 3, 2014aop.sagepub.comDownloaded from

8 Annals of Pharmacotherapy
RPX7009RPX7009 is a novel boronic acid β-lactamase inhibitor. Boronic acids, similar to bridged bicyclic ureas such as avi-bactam and relebactam, have been shown to have activity against class A and C β-lactamases. Like the other β-lactamase inhibitors, RPX7009 has little antimicrobial activity alone. It is being studied in combination with biape-nem, a carbapenem.83 Biapenem was approved in Japan in 2001 and has significant advantages compared with other carbapenems.83,84 Its spectrum of activity is similar to that of meropenem and imipenem, but it is more stable against efflux by P aeruginosa than meropenem.84 Additionally, biapenem has been reported to be more stable to hydrolysis by metallo-β-lactamases and OXA-48 β-lactamases com-pared with others in its class.85 It also possesses better activ-ity against anaerobes than meropenem.86
Biapenem/RPX7009The potential of RPX7009 in combination with biapenem was evaluated in several in vitro studies.85,86 When 145 iso-lates of KPC-producing organisms were tested against bia-penem alone and in combination with RPX7009, it was found that 89.7% of these isolates were inhibited by <1 µg/mL of biapenem with 2 µg/mL of RPX7009. When the RPX7009 concentration was increased to 8 µg/mL, 94.4% were inhibited, demonstrating dose-dependent potentiation. The combination of biapenem and RPX7009 was not sig-nificant against isolates with metallo-β-lactamases or OXA-48 β-lactamases, but MICs were generally lower for biapenem/RPX7009 than for other carbapenems.85
Clinical Data: RPX7009Phase 1 studies of biapenem/RPX7009 have been com-pleted, but no phase 2 data are yet available. Biapenem was approved in Japan in 2001 based on its efficacy for intra-abdominal infections.87 In the US, RPX7009 is currently being evaluated with meropenem in a Phase III study for serious infections caused by CREs. 88
Clinical ControversyCarbapenem antibiotics have become generally accepted as the drugs of choice for the treatment of ESBLs because of concerns regarding clinical failure with the use of other agents.89,90 They are favorable options because of the fact that they are relatively stable against destruction by a wide variety of ESBLs and they are not subject to an inoculum effect, where higher bacterial densities decrease the effec-tiveness of antibiotics.91 Whereas in vitro and in vivo data show activity of BLICs against ESBLs,92,93 concerns with their use include the treatment of isolates with concomitant expression of multiple resistance mechanisms, the use of
traditional dosing that may not achieve the appropriate pharmacodynamic targets, and the decreased activity of BLICs in cases of high bacterial innoculum.94 Several in vitro and in vivo studies explored the importance of MIC and bacterial inoculum on the efficacy of BLICs in these instances.95,96 Piperacillin/tazobactam activity was found to be decreased in cases of high bacterial inoculum because of increased susceptibility to hydrolysis.96 However, several animal studies did not find the same inoculum effect with amoxicillin/clavulanate.97,98
Increased use of carbapenems has been shown to increase resistance to them in some organisms.99,100 Therefore, reas-sessing the use of carbapenem alternatives for ESBL-producing infections is prudent antibiotic stewardship.101 Despite earlier data that cautioned against the use of BLICs for infections caused by ESBLs, for the reasons mentioned above, recent studies have shown favorable outcomes with their use, particularly in UTIs caused by ESBL-producing organisms, community-onset acute pyelonephritis caused by ESBL-producing Escherichia coli,102 and bacteremia caused by ESBL-producing Escherichia coli and K pneu-moniae.103,104 A study of infections caused by ESBL-producing organisms included 23 patients who were treated with piperacillin/tazobactam. Treatment was successful in 10/11 (91%) patients with nonurinary infections, with MICs less than the breakpoint of ≤16/4 µg/mL but only 1/5 (20%) with MICs >16/4 µg/mL. For UTIs specifically, piperacil-lin/tazobactam treatment was successful in 6/6 (100%), regardless of MIC.105 Finally, the aforementioned recent phase III trials of ceftolozane/tazobactam showed high suc-cess rates in treating cUTIs and cIAIs caused by ESBL-producing bacteria.40,41 The numbers of patients in these subgroups were not high but are comparable to that in many retrospective studies of BLIC use for ESBL-producing infection and are not subject to the biases associated with retrospective study designs.
Based on a summary of the findings available, BLICs are viable options for certain cases of infection caused by ESBL-producing organisms, though there are concerns with their use. Some data have suggested that BLIC therapy may be most appropriate in cases of low to moderate bacte-rial burden because of the concern of an inoculum effect with piperacillin/tazobactam. The inoculum effect is most worrisome in cases of infection with high bacterial burdens, including abscesses, meningitis, endocarditis, and pneumo-nia.96 However, this effect may be a mostly in vitro phe-nomenon.96 Recent data support the fact that the in vitro MIC is most predictive of in vivo efficacy, regardless of the influence of an inoculum effect or ESBL expression.106-110 Because ceftolozane alone is efficiently destroyed by ESBLs,69 the positive results with ceftolozane/tazobactam for ESBL-producing cIAIs and cUTIs suggest that some BLICs can be reasonable options for these types of infec-tions. If studies are completed in patients with pneumonia, they may help determine if in vitro inoculum effects with
at TEMPLE UNIV on November 3, 2014aop.sagepub.comDownloaded from

Toussaint and Gallagher 9
BLICs are important clinically. In practical terms, it is logi-cal to treat patients with severe sepsis with a high risk of infection from ESBL-producing organisms empirically with carbapenems. However, the common practice of changing from a BLIC such as piperacillin/tazobactam to a carbapenem in a patient with a confirmed ESBL-producing pathogen who is improving should be reconsidered.
ConclusionsBLICs have been a mainstay of treatment since the avail-ability of clavulanate in the 1980s. They expand the spec-trum of β-lactams to include organisms that produce a variety of β-lactamases and are useful for a variety of infec-tions. The spectrum and activity of the individual BLICs vary depending on the parent β-lactam and the types of β-lactamase produced. Unfortunately, the historical BLICs lack utility against certain β-lactamase-producing organ-isms, most notably the emerging strains that produce carbapenemases.
New BLICs are currently being evaluated and may pro-vide an answer for patients with infections caused by these difficult-to-treat organisms. The combinations of ceftazi-dime and ceftaroline with avibactam restore the utility of these β-lactams against organisms that produce some car-bapenemases and give clinicians an option for CRE beyond therapy with polymyxins or tigecycline. The addition of avi-bactam to aztreonam would create a unique antimicrobial because aztreonam itself is stable against NDM-variant car-bapenemases currently spreading among Enterobacteriaceae worldwide. Relebactam was shown to enhance the activity of imipenem against Pseudomonas as well as MDR Enterobacteriaceae, including those producing AmpC, ESBLs, and KPCs.75,77 RPX7009 is a boronic acid β-lactamase inhibitor that is currently being studied with biapenem, a carbapenem with the advantage of being more stable to efflux by Pseudomonas than meropenem.85,86 Ceftolozane/tazobactam is furthest along in development and may be a useful option against MDR P aeruginosa infections, though clinical studies that include these organ-isms are likely to be limited.40-42
The role of the new agents in therapy is not defined. Limitations in trial design and the need to achieve regula-tory benchmarks may preclude their study in high-risk patient populations as well as in infections caused by highly resistant organisms. If clinical experience reflects both in vitro effects and the safety profile of β-lactams, it is likely that they will become useful therapeutic options for Gram-negative infections with highly resistant organisms that pro-duce β-lactamases. Their safety, local resistance patterns, pricing, and other considerations will determine how clini-cians utilize them in practice. Even now, there are organ-isms that produce β-lactamases that confer resistance to these not-yet-approved agents, such as NDM-producing
Enterobacteriaceae. Strains of these extremely resistant organisms are endemic in India and will inevitably spread throughout the world.111,112 It is inevitable that further resis-tance to these agents will be seen, and it will be vital for antimicrobial stewardship programs to take a lead role in their appropriate use.
Declaration of Conflicting InterestsThe author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JCG was speaker for Cubist, Astellas, and Forest; consul-tant for Forest, Theravance, Pfizer, Cubist, and Astellas; and had research support from Merck. KAT has no conflicts of interest to disclose.
FundingThe author(s) received no financial support for the research, authorship, and/or publication of this article.
References 1. Wilke M, Lovering A, Strynadka N. Beta-lactam antibi-
otic resistance: a current structural perspective. Curr Opin Microbiol. 2005;8:525-533.
2. Gupta N, Limbag B, Patel J, Kallen A. Carbapenem-resistant Enterobacteriaceae: epidemiology and prevention. Clin Infect Dis. 2011;53:60-67.
3. Schwaber MJ, Klarfeld-Lidji S, Navon-Venezia S, Schwartz D, Leavitt A, Carmeli Y. Predictors of carbapenem-resistant Klebsiella pneumonia acquisition among hospitalized adults and effect of acquisition on mortality. Antimicrob Agents Chemother. 2008;52:1028-1033.
4. Tumbarello M, Viale P, Viscoli C, et al. Predictors of mortal-ity in bloodstream infections caused by Klebsiella pneumo-nia carbapenemase-producing K. pneumoniae: importance of combination therapy. Clin Infect Dis. 2012;55:943-950.
5. Livermore DM. Beta-lactamases in laboratory and clinical resistance. Clin Microbiol Rev. 1995;8:557-584.
6. Livermore DM. Determinants of the activity of beta-lac-tamase inhibitor combinations. J Antimicrob Chemother. 1993;31:9-21
7. Bush K. Beta-lactamase inhibitors from laboratory to clinic. Clin Microbiol Rev. 1988;1:109-123.
8. Medeiros A. Evolution and dissemination of beta-lactamases accelerated by generations of beta-lactam antibiotics. Clin Infect Dis. 1997;24:S19-S45.
9. Sirot D. Extended-spectrum plasmid-mediated beta lacta-mases. J Antimicrob Chemother. 1995;36:19-34.
10. Jacoby G, Munoz-Price LS. The new beta-lactamases. N Engl J Med. 2005;352:380-391.
11. Lister P. Beta-lactamase inhibitor combinations with extended-spectrum penicillins: factors influencing antibac-terial activity against Enterobacteriaceae and Pseudomonas aeruginosa. Pharmacotherapy. 2000;20:213S-218S.
12. Livermore DM. Clinical significance of beta-lactamase induction and stable depression in Gram-negative rods. Eur J Clin Microbiol. 1987;6:439-445.
at TEMPLE UNIV on November 3, 2014aop.sagepub.comDownloaded from

10 Annals of Pharmacotherapy
13. Paterson D. Resistance in Gram negative bacteria: Enterobacteriaceae. Am J Med. 2006;119:S20-S28.
14. Leonard D, Bonomo K, Powers R. Class D beta-lactamases: a reappraisal after five decades. Acc Chem Res. 2013;46: 2407-2415.
15. Bush K, Jacoby GA, Medeiros A. A functional classification scheme for beta-lactamases and its correlation with molec-ular structure. Antimicrob Agents Chemother. 1995;39: 1211-1233.
16. Bush K, Jacoby GA. Updated functional classifica-tion of beta-lactamases. Antimicrob Agents Chemother. 2010;54:969-976.
17. Bush K. New beta-lactamases in Gram-negative bacteria: diversity and impact on the selection of antimicrobial ther-apy. Clin Infect Dis. 2001;32:1085-1089.
18. Lacey R, Kruczenk S. Epidemiology of antibiotic resis-tance in Staphylococcus aureus. J Antimicrob Chemother. 1986;18:207-214.
19. Livermore D. Beta-lactamase mediated resistance and oppor-tunities for its control. J Antimicrob Chemother. 1998;41: 25-41.
20. Queenan AM, Bush K. Carbapenemases: the versatile beta-lactamases. Clin Microbiol Rev. 2007;20:440-458.
21. Tamilselvi A, Mugesh G. Zn and antibiotic resistance: metallo beta-lactamases and their synthetic analogues. J Biol Inorg Chem. 2008;13:1039-1053.
22. Aoki N, Ishii Y, Tateda K, et al. Efficacy of calcium-EDTA as an inhibitor for metallo beta-lactamases in a mouse model of Pseudomonas aeruginosa pneumonia. Antimicrob Agents Chemother. 2010;54:4582-4588.
23. Jacoby G. AmpC beta-lactamases. Clin Microbiol Rev. 2009;22:161.
24. Jones R. Important and emerging beta-lactamase-mediated resistances in hospital-based pathogens: the AmpC enzymes. Diagn Microbiol Infect Dis. 1998;31:461-466.
25. Ledent P, Raquet K, Joris B, et al. A comparative study of class D beta-lactamases. Biochem J. 1993;292:555-562.
26. Poirel L, Naas T, Nordmann P. Diversity, epidemiology, and genetics of class D beta-lactamases. Antimicrob Agents Chemother. 2010;54:24-38.
27. Naas T, Sougakoff W, Casetta A, et al. Molecular character-ization of OXA-20, a novel, Class D beta-lactamase, and its integrin from Pseudomonas aeruginosa. Antimicrob Agents Chemother. 1998;42:2074-2083.
28. Brown AG, Butterworth D, Cole M, et al. Naturally occur-ring beta-lactamase inhibitors with antibacterial activity. J Antibiot (Tokyo). 1976;29:668-669.
29. Bebrone C, Lassaux P, Vercheval L, et al. Current challenges in antimicrobial chemotherapy: a focus on beta-lactamase inhibition. Drugs. 2010;70:651-679.
30. Drawz S, Bonomo R. Three decades of beta-lactamase inhib-itors, Clin Microbiol Rev. 2010;23:160-201.
31. Lodise T, Lomaestro B, Rodvold K, Danzinger L, Drusano G. Pharmacodynamic profiling of piperacillin in the pres-ence of tazobactam in patients through the use of popula-tion pharmacokinetic models and Monte Carlo simulation. Antimicrob Agents Chemother. 2004;48:4718-4724.
32. Urban C, Go E, Mariano N, Rahal JJ. Interaction of sulbactam, clavulanic acid, and tazobactam with pen-
icillin-binding proteins of imipenem-resistant and imipe-nem-susceptible Acinetobacter baumannii. FEMS Microbiol Lett. 1995;125:193-197.
33. Poulikakos P, Tansarli G, Falagas M. Combination antibiotic treatment versus monotherapy for multidrug-resistant, exten-sively-drug resistant, and pandrug-resistant Acinetobacter infections: a systematic review. Euro J Clin Microbiol Infect Dis. 2014;33:1675-1685.
34. Kuck N, Jacobus N, Petersen P, Weiss W, Testa R. Comparative in vitro and in vivo activities of piperacillin combined with the beta-lactamase inhibitors tazobactam, cla-vulanic acid, and sulbactam. Antimicrob Agents Chemother. 1989;33:1964-1969.
35. Totir MA, Cha J, Ishiwata A, et al. Why clinically used tazo-bactam and sulbactam are poor inhibitors of OXA-10 beta lactamases: Raman crystallographic evidence. Biochemistry. 2008;47:4094-4101.
36. Payne D, Cramp R, Winstanley D, Knowles D. Comparative activities of clavulanic acid, sulbactam, and tazobactam against clinically important beta-lactamases. Antimicrob Agents Chemother. 1994;38:767-772.
37. Sood S. Comparative evaluation of the in-vitro activity of six beta-lactam/beta-lactamase inhibitor combinations against Gram negative bacilli. J Clin Diagn Res. 2013;7:224-228.
38. Bonfiglio G, Laksai Y, Franchino L, Amicosante G, Nicoletti G. Mechanisms of beta-lactam resistance amongst Pseudomonas aeruginosa isolated in an Italian survey. J Antimicrob Chemother. 1998;l42:697-702.
39. Craig WA, Andes DR. In vivo activities of Ceftolozane, a new cephalosporin, with and without tazobactam against Pseudomonas aeruginosa and Enterobacteriaceae, includ-ing strains with extended-spectrum-lactamases, in the thighs of neutropenic mice. Antimicrob Agents Chemother. 2013;57:1577-1582.
40. Wagenlehner F, Umeh O, Huntington J, et al. Efficacy and safety of ceftolozane/tazobactam versus levofloxacin in the treatment of complicated urinary tract infections (cUTI)/pyelonephritis in hospitalized adults: results from the phase 3 ASPECT-cUTI trial (abstract eP449). Paper presented at: European Congress of Clinical Microbiology and Infectious Diseases (ECCMID); May 10-13, 2014; Barcelona, Spain.
41. Eckmann C, Hershberger E, Miller B, et al. Efficacy and safety of ceftolozane/tazobactam versus meropenem in the treatment of complicated intra-abdominal infections (cIAI) in hospitalized adults: results from the phase 3 ASPECT-cIAI trial (abstract P0266-a). Paper presented at: European Congress of Clinical Microbiology and Infectious Diseases (ECCMID); May 10-13, 2014; Barcelona, Spain.
42. Cubist Pharmaceuticals. Safety and efficacy study of ceftolozane/tazobactam to treat ventilated nosocomial pneu-monia (ASPECT-NP). http://clinicaltrials.gov/ct2/show/NCT02070757. NLM Identifier: NCT02070757. Accessed August 11, 2014.
43. Coleman K. Diazabicyclooctanes (DBOs): a potent new class of non-beta-lactam beta-lactamase inhibitors. Curr Opin Microbiol. 2011;14:550-555.
44. Shales D. New beta-lactam/beta-lactamase inhibitor com-binations in clinical development. Ann N Y Acad Sci. 2013;1277:105-114.
at TEMPLE UNIV on November 3, 2014aop.sagepub.comDownloaded from

Toussaint and Gallagher 11
45. Lahiri SD, Mangani S, Durand-Reville T, et al. Structural insight into potent broad-spectrum inhibition with reversible recyclization mechanism: avibactam in complex with CTX-M-15 and Pseudomonas aeruginosa AmpC beta-lactamases. Antimicrob Agents Chemother. 2013;57:2496-2505.
46. Stachyra T, Péchereau MC, Bruneau JM, et al. Mechanistic studies of the inactivation of TEM-1 and P99 by NXL104, a novel non-beta-lactam beta-lactamase inhibitor. Antimicrob Agents Chemother. 2010;54:5132-5138.
47. Boucher H, Talbot G, Benjamin D, et al. 10x’20 Progress: development of new drugs active against Gram-negative bacilli: an update from the Infectious Diseases Society of America. Clin Infect Dis. 2013;56:1685-1694.
48. Ehmann D, Jahic H, Ross P, et al. Kinetics of avibactam inhibition against class A, C and D beta-lactamases. J Biol Chem. 2013;288:27960-27971.
49. Stachyra T, Levasseur P, Péchereau MC, et al. In vitro activ-ity of the beta-lactamase inhibitor NXL104 against KPC-2 carbapenemase and Enterobacteriaceae expressing KPC carbapenemases. Antimicrob Agents Chemother. 2009;64: 326-329.
50. Ehmann D, Jahic H, Ross PL, et al. Avibactam is a covalent, reversible, non-beta-lactam beta-lactamase inhibitor. Proc Natl Acad Sci U S A. 2012;109:11663-11668.
51. AztraZeneca. Ceftazidime-avibactam for the treatment of infections due to ceftazidime resistant pathogens. http://clinicaltrials.gov/ct2/show/NCT01644643?term=avibactam&rank=6. Accessed January 2, 2014.
52. AztraZeneca. A study comparing ceftazidime-avibactam versus meropenem in hospitalized adults with nosocomial pneumonia. http://clinicaltrials.gov/ct2/show/NCT01808092?term=avibactam&rank=11. Accessed January 27, 2014.
53. Cerexa, Inc. Comparative study of coadministered cef-taroline foxamil and NXL 104 vs. intravenous doripenem in adult subjects with complicated urinary tract infections. http://clinicaltrials.gov/ct2/show/NCT01281462?term=avibactam&rank=5. Accessed January 2, 2014.
54. AstraZeneca. To investigate the safety and tolerability of aztreonam-avibactam (ATM-AVI). http://clinicaltrials.gov/ct2/show/NCT01689207?term=aztreonam+avibactam&rank=1. Accessed August 11, 2014.
55. Levasseur P, Girard AM, Claudon M, et al. In vitro antibac-terial activity of the ceftazidime-avibactam (NXL104) com-bination against Pseudomonas aeruginosa clinical isolates. Antimicrob Agents Chemother. 2012;56:1606-1608.
56. Crandon J, Shuck V, Banevicius M, et al. Comparative in vitro and in vivo efficacies of human simulated doses of ceftazidime and ceftazidime-avibactam against Pseudomonas aeruginosa. Antimicrob Agents Chemother. 2012;56:6137-6146.
57. Walkty A, DeCorby M, Lagace-Wiens PRS, Karlowsky J, Hoban D, Zhanel G. In vitro activity of ceftazidime com-bined with nxl104 versus Pseudomonas aeruginosa isolates obtained from patients in Canadian hospitals. Antimicrob Agents Chemother. 2011;55:2992-2994.
58. Mushtaq S, Warner M, Livermore D. In vitro activity of ceftazidime1NXL104 against Pseudomonas aerugi-nosa and other non-fermenters. J Antimicrob Chemother. 2010;65:2376-2381.
59. Lister P, Wolter D, Hanson N. Antibacterial-resistant Pseudomonas aeruginosa: clinical impact and complex reg-ulation of chromosomally encoded resistance mechanisms. Clin Microbiol Rev. 2009;22:582-610.
60. Atkas Z, Kayacan C, Oncul O. In vitro activity of avibac-tam (NXL104) in combination with beta-lactams against Gram-negative bacteria, including OXA-48 beta-lactamase-producing Klebsiella pneumoniae. Int J Antimicrob Agents. 2012;39:86-89.
61. Endimiani A, Hujer K, Hujer A, Pulse M, Weiss W, Bonomo R. Evaluation of ceftazidime and NXL 104 in two murine models of infection due to KPC-producing Klebsiella pneu-moniae. Antimicrob Agents Chemother. 2011;55:82-85.
62. Dubreuil LJ, Mahieux S, Neut C, Miossec C, Pace J. Anti-anaerobic activity of a new beta-lactamase inhibitor NXL104 in combination with beta-lactams and metronidazole. Int J Antimicrob Agents. 2012;39:500-504.
63. Lucasti C, Popescu I, Ramesh M, Lipka J, Sable C. Comparative study of the efficacy and safety of ceftazi-dime/avibactam plus metronidazole in the treatment of intra-abdominal infections in hospitalized adults: results of a randomized, double-blind, phase II trial. J Antimicrob Chemother. 2013;68:1183-1192.
64. Vazquez JA, Gonzalez Patzan LD, Stricklin D, et al. Efficacy and safety of ceftazidime-avibactam versus imipenem-cilas-tatin in the treatment of complicated urinary tract infections, including acute pyelonephritis, in hospitalized adults: results of a prospective, investigator-blinded, randomized study. Curr Med Res Opin. 2012;28:1921-1931.
65. AstraZeneca. Comparative study of NXL104/ceftazidime versus comparator in adults with complicated urinary tract infections. http://clinicaltrials.gov/ct2/show/NCT00690378?term=avibactam&rank=15. Accessed August 18, 2011.
66. Ceftazidime/avibactam trials. http://clinicaltrials.gov/ct2/show/NCT01726023?term=ceftazidime%2Favibactam&rank=4. Accessed February 10, 2014.
67. Biek D, Critchley IA, Riccobene TA, Thye DA. Ceftaroline fosamil: a novel broad-spectrum cephalosporin with expanded anti-Gram-positive activity. J Antimicrob Chemother. 2010;65(suppl 4):iv9-iv16.
68. Karlowsky J, Adam H, Decorby M, Lagace-Wiens P, Hoban D, Zhanel GG. In vitro activity of ceftaroline against Gram-positive and Gram-negative pathogens isolated from patients in Canadian hospitals in 2009. Antimicrob Agents Chemother. 2011;55:2837-2846.
69. Sader H, Flamm R, Jones R. Antimicrobial activity of cef-taroline-avibactam tested against clinical isolates collected from US medical centers in 2010-2011. Antimicrob Agents Chemother. 2013;57:1982-1988.
70. Mushtaq S, Warner M, Williams G, Critchley I, Livermore D. Activity of chequerboard combinations of ceftaroline and NXL104 versus beta-lactamase-pro-ducing Enterobacteriaceae. J Antimicrob Chemother. 2010;65:1428-1432.
71. AztraZeneca. A study to investigate the effect of administra-tion of ceftazidime-avibactam (CAZ-AVI) and ceftaroline fosamil-avibactam (CXL) on the intestinal flora of healthy volunteers. http://clinicaltrials.gov/ct2/show/NCT01789528. Accessed December 5, 2013.
at TEMPLE UNIV on November 3, 2014aop.sagepub.comDownloaded from
12 Annals of Pharmacotherapy
72. AstraZeneca. To investigate the safety and tolerability of aztreonam-avibactam (ATM-AVI). http://clinicaltrials.gov/show/NCT01689207. Accessed January 2, 2014.
73. Livermore DM, Mushtaq S, Warner M, et al. Activities of NXL104 combinations with ceftazidime and aztreonam against carbapenemase-producing Enterobacteriaceae. Antimicrob Agents Chemother. 2011;55:390-394.
74. Young K, Raghoobar S, Hairston N, et al. In vitro activity of the class A and class C beta-lactamase inhibitor MK-7655 [abstract F1-2139]. Paper presented at: 50th Interscience Conference on Antimicrobial Agents and Chemotherapy Annual Meeting; September 12-15, 2010; Boston, MA.
75. Livermore D, Warner M, Mushtaq S. Activity of MK-7655 combined with imipenem against Enterobacteriaceae and Pseudomonas aeruginosa. J Antimicrob Chemother. 2013;68:2286-2290.
76. Hirsch E, Ledesma K, Chang KT, Schwartz M, Motyl M, Tam V. In vitro activity of MK-7655, a novel beta-lactamase inhibitor, in combination with imipenem against carbape-nem resistant Gram-negative bacteria. Antimicrob Agents Chemother. 2012;56:3753-3757.
77. Young K, Hackel M, Lascols C, et al. Response to imipenem plus MK-7655, a novel beta-lactamase inhibitor, in a sur-veillance study population of P. aeruginosa from SMART 2009. Paper presented at: 52nd Interscience Conference on Antimicrobial Agents and Chemotherapy Annual Meeting; September 9-12, 2012; San Francisco, CA.
78. Performance Standards for Antimicrobial Susceptibility Testing; 18th Informational Supplement. Wayne, PA: Clinical Laboratory Standards Institute; 2007. CLSI docu-ment M100-S19.
79. Performance Standards for Antimicrobial Susceptibility Testing; 24th Informational Supplement. Wayne, PA: Clinical Laboratory Standards Institute; 2014. CLSI docu-ment M100-S24.
80. Merck Sharp & Dohme Corp. Study of the safety, tolerabil-ity, and efficacy of MK-7655 + imipenem/cilastatin alone for the treatment of complicated urinary tract infection (cUTI). http://clinicaltrials.gov/ct2/show/NCT01505634?term=MK-7655&rank=2. Accessed January 22, 2014.
81. Merck Sharp & Dohme Corp. Study of the safety, tolerabil-ity, and efficacy of MK-7655 + imipenem/cilastatin versus imipenem/cilastatin alone to treat complicated intra-abdom-inal infection [cIAI]. http://clinicaltrials.gov/ct2/show/NCT01506271?term=MK-7655&rank=3. Accessed January 15, 2014.
82. Merck Sharp & Dohme Corp. Merck’s investigational beta-lactamase inhibitor relebactam (MK-7655) granted qualified infectious disease product (QIDP) and fast track designations by FDA. http://www.mercknewsroom.com/news-release/cor-porate-news/mercks-investigational-beta-lactamase-inhibitor-relebactam-mk-7655-grant. Accessed October 9, 2014.
83. Rempex Pharmaceuticals. Rempex Pharmaceuticals to pres-ent data at ICAAC on Carbavance, a new agent designed to treat multi-drug resistant (MDR) Gram-negative bacteria, September 2012. http://www.rempexpharma.com/news/9-7-12. Accessed January 18, 2014.
84. Chen HY, Livermore DM. In-vitro activity of biapenem, com-pared with imipenem and meropenem, against Pseudomonas
aeruginosa strains and mutants with known resistance mech-anisms. J Antimicrob Chemother. 1994;33:949-958.
85. Livermore D, Mushtaq S. Activity of biapenem (RPX2003) combined with the boronate beta-lactamase inhibitor RPX7009 against carbapenem-resistant Enterobacteriaceae. J Antimicrob Chemother. 2013;68:1825-1831.
86. Goldstein E, Citron D, Tyrrell K, Merriam C. In vitro activity of biapenem plus RPX7009, a carbapenem combined with a serine beta-lactamase inhibitor, against anaerobic bacteria. Antimicrob Agents Chemother. 2013;57:2620-2630.
87. Brismar B, Akerlund JE, Sjostedt S, et al. Biapenem versus imipenem/cilastatin in the treatment of complicated intra-abdominal infections: report from a Swedish study group. Scand J Infect Dis. 1996;28:507-512.
88. Efficacy, safety, tolerability of carbavance compared to best available therapy in serious infections due to carbapenem resistant Enterobacteriaceae, in adults. http://clinicaltrials.gov/ct2/show/NCT02168946?term=RPX7009&rank=6. Accessed October 21, 2014.
89. Endimiani A, Luzzaro F, Perilli M. Bacteremia due to Klebsiella pneumonia isolates producing the TEM-52 Extended-spectrum beta-lactamase: Treatment outcome of patients receiving imipenem or ciprofloxacin. Clin Infect Dis. 2004;38:243-251.
90. Paterson D, Wen-Chien K, Gottberg A, et al. Antibiotic ther-apy for Klebsiella pneumonia bacteremia: implications of the production of extended-spectrum beta-lactamases. Clin Infect Dis. 2003;39:31-37.
91. Pitout JD, Laupland KB. Extended spectrum beta-lactamase producing Enterobacteriaceae: an emerging public-health concern. Lancet Infect Dis. 2008;8:159-166.
92. Mentec H, Vallois JM, Bure A, et al. Piperacillin, tazo-bactam, and gentamicin alone or combined in an endocar-ditis model of infection by a TEM-3-producing strain of Klebsiella pneumonia or its susceptible variant. Antimicrob Agents Chemother. 1992;36:1883-1889.
93. Rice LB, Carias LL, Shales DM. In vivo efficacies of beta-lactam beta-lactamase inhibitor combinations in Klebsiella pneumonia and in vivo response to beta-lactam therapy. J Infect Dis. 1996;173:151-158.
94. Perez F, Bonomo R. Can we really use beta-lactam/beta-lactam inhibitor combinations for the treatment of infections caused by extended-spectrum beta-lactamase-producing bacteria? Clin Infect Dis. 2012;54:175-177.
95. Thauvin-Eliopoulous C, Tripodi MF, Moellering JR, Eliopoulos GM. Efficacies of piperacillin-tazobactam and cefepime in rats with experimental intra-abdominal abscesses due to an extended-spectrum beta-lactamase-producing strain of Klebsiella pneumonia. Antimicrob Agents Chemother. 1994;41:1053-1057.
96. Thompson K, Smith Moland E. Cefepime, piperacillin-tazobactam, and the inoculum effect in tests with extended-spectrum beta-lactamase-producing Enterobacteriaceae. Antimicrob Agents Chemother. 2001;45:3548-3554.
97. Lopez-Cerero L, Picon E, Morillo C, et al. Comparative assessment of inoculum effects on the antimicrobial activity of amoxicillin/clavulanate and piperacillin/tazobactam with extended-spectrum beta-lactamase-producing and extended-spectrum beta-lactamase-nonproducing Escherichia coli iso-lates. Clin Microbiol Infect. 2010;16:132-136.
at TEMPLE UNIV on November 3, 2014aop.sagepub.comDownloaded from

Toussaint and Gallagher 13
98. Docobo-Perez F, Lopez-Cereo L, Lopez-Rojas R, et al. Inoculum effect on the efficacies of amoxicillin-clavulanate, piperacillin-tazobactam, and imipenem against extended-spectrum beta-lactamase (ESBL)-producing Escherichia coli in an experimental murine sepsis model. Antimicrob Agents Chemother. 2013;57:2109-2113.
99. Rahal JJ, Urban C, Horn D, et al. Class restriction of cepha-losporin use to control total cephalosporin resistance in nos-ocomial Klebsiella. JAMA. 1998;280:1233-1237.
100. McLaughlin M, Advincula MR, Malcynski M, et al. Correlations of antibiotic use and carbapenem resistance in Enterobacteriaceae. Antimicrob Agents Chemother. 2013;57:5131-5133.
101. Siedner M, Galar A, Guzman-Suarez BB, et al. Cefepime vs other antibacterial agents for the treatment of Enterobacter species bacteremia. Clin Infect Dis. 2014;58:1554-1563.
102. Park S, Choi S, Lee D. The efficacy of non-carbapenem antibi-otics for the treatment of community-onset pyelonephritis due to extended-spectrum beta-lactamase-producing Escherichia coli. J Antimicrob Chemother. 2014;69:2848-2856.
103. Vardakas K, Tansarli G, Rafailidis P, Falagas M. Carbapenems versus alternative antibiotics for the treatment of bactere-mia due to Enterobacteriaceae producing extended-spectrum beta-lactamases: a systematic review and meta-analysis. J Antimicrob Chemother. 2012;67:2793-2803.
104. Rodriguez-Bano J, Navarro M, Retamar P, et al. Beta lac-tam/beta lactam inhibitor combinations for the treatment of bacteremia due to Extended-spectrum Beta-lactamase pro-ducing Escherichia coli: a post hoc analysis of prospective cohorts. Clin Infect Dis. 2012;54:167-174.
105. Gavin P, Suseno M, Peterson L. Clinical correlation of CLSI susceptibility breakpoint for piperacillin-tazobactam against
extended-spectrum-beta-lactamase-producing Escherichia coli and Klebsiella species. Antimicrob Agents Chemother. 2006;50:2244-2247.
106. Bhavnani S, Ambrose P, Craig W. Outcomes evaluation of patients with ESBL and non-ESBL-producing Escherichia coli and Klebsiella species as defined by CLSI reference meth-ods: report from the SENTRY Antimicrobial Surveillance Program. Diagn Microbiol Infect Dis. 2006;54:231-236.
107. Craig W. The inoculum effect: fact or artifact? Diagn Microbiol Infect Dis. 2004;50:229-230.
108. Dudley M, Ambrose P, Bhavnani SM, et al. Background and rationale for revised clinical and laboratory standards institute interpretive criteria (breakpoints) for Entero-bacteriaceae and Pseudomonas aeruginosa: I. cephalospo-rins and aztreonam. Clin Infect Dis. 2013;56:1301-1309.
109. Retamar P, Lopez-Cerero L, Muniain M, et al. Impact of the MIC of piperacillin/tazobactam on the outcome of patients with bacteremia due to extended-spectrum beta-lactamase-producing Escherichia coli. Antimicrob Agents Chemother. 2013;57:3402-3404.
110. Peterson L. Antibiotic policy and prescribing strategies for therapy of extended-spectrum beta-lactamase-producing Enterobacteriaceae: the role of piperacillin/tazobactam. Clin Microbiol Infect. 2008;14(suppl 1):181-184.
111. Johnson A, Woodford N. Global spread of antibiotic resis-tance: the example of New Delhi metallo-beta-lactamase (NDM)-mediated carbapenem resistance. J Med Microbiol. 2013;62:599-613.
112. Ahammad Z, Sreekrishnan T, Hands C, Knapp C, Graham D. Increased waterborne bla
NDM-1 resistance gene abundances
associated with seasonal human pilgrimages to the upper Ganges river. Environ Sci Technol. 2013;48:3014-3020.
at TEMPLE UNIV on November 3, 2014aop.sagepub.comDownloaded from