using lean six sigma and dawn ac to improve ... - 4s dawn
TRANSCRIPT

Using Lean Six
Sigma and Dawn
AC to Improve
ProductivityDaniel M. Witt, PharmD,
FCCP, BCPS, CACP
Pharmacy Department

2
Lean Management Principles
� Lean management principles have been used effectively in manufacturing companies for decades, particularly in Japan
� Lean thinking begins with driving out waste so that all work adds value and serves the customer's needs
� Identifying value-added and non-value-added steps in every process is the beginning of the journey toward lean operations

3
In July 2008, the Clinical Pharmacy Anticoagulation Service
(CPAS) Unit Based Team (UBT) initiated a project to assess
and evaluate the current practice of monitoring Complete
Blood Counts (CBC) in 100% of their patients.
� A study conducted at KPCO supported restricting CBC orders to certain high risk populations without compromising care for low risk populations
� High risk populations include:
1. Mechanical Heart Valve
2. Bleeding History
3. Lovenox Therapy
Introduction

4
Is Routine CBC Monitoring Necessary?
� 573 of 4033 (14.3%) had Hgb drop of 2 gm/dl or more
� Occult bleeding ‘confirmed’ in 121 (3% of all monitored patients)
� 13 of these patients had major bleeding (0.3% of all monitored patients)
� The annual detection rate of occult bleeding through routine CBC monitoring = 0.8%
� Most patients do not need routine CBCs (exceptions mechanical valves, thrombophilia)
Journal Thrombosis & Thrombolysis 2005;20:183-88

5
The existing practice of ordering CBC labs for all CPAS
patients is time intensive and has been shown to be
clinically unnecessary for low risk patients.
�There appears to be some overlap and duplication of work with the existing process
� Creating multiple CBC lab orders
� Lab staff does not always respond in a timely manner
� Non-compliant patients
�This practice occupies CPAS staff time that could be better spent on more value added or relevant patient care activities
Problem Statement
6
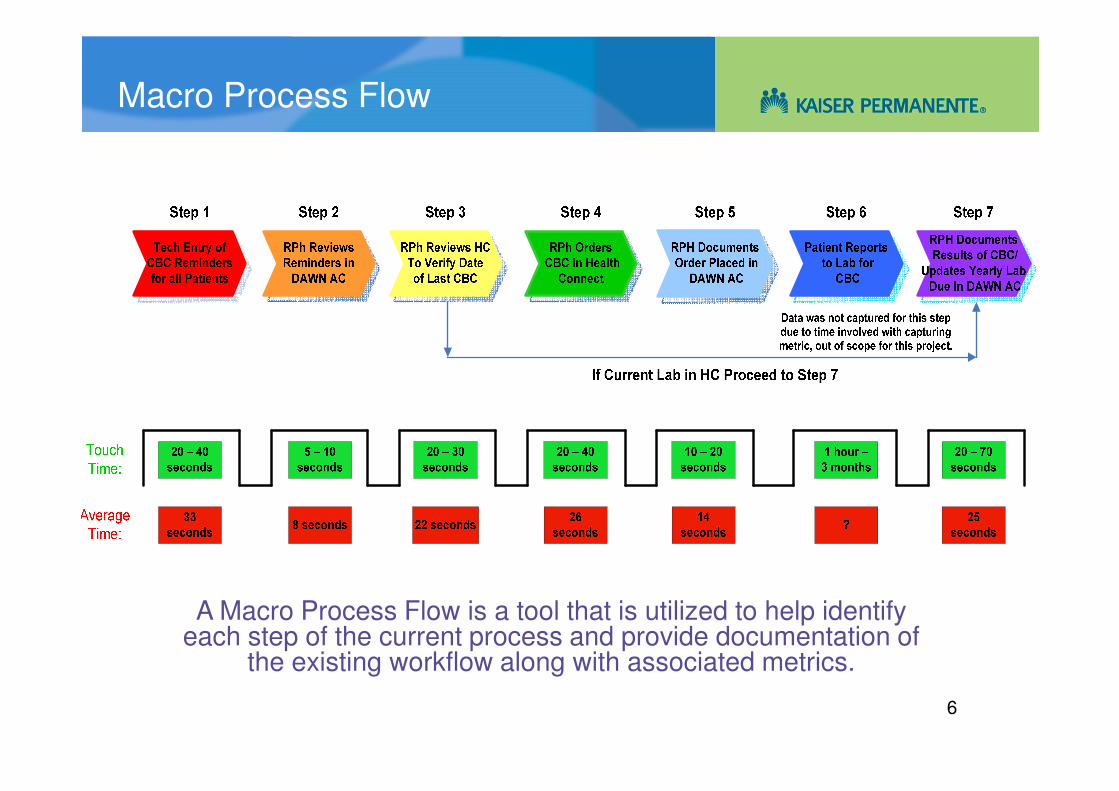
Macro Process Flow
A Macro Process Flow is a tool that is utilized to help identify each step of the current process and provide documentation of
the existing workflow along with associated metrics.

7
Project Scope
The scope includes 6 of the 7 steps involved in processing a CBC reminder (reviewing, ordering and documenting) outlined in the Macro Process Flow on the previous slide.
�Step 6 (Patient Reports to Lab for CBC) will be considered out of scope at this time due to the nature of Rapid Cycle Change
� Amount of time involved in tracking this metric
� Project completion date could be pushed out several months
�Streamlining step 6 of the process to ensure lab work is done timely is an integral piece of the process and could be considered as a future area of opportunity

8
On average CPAS staff spend approximately 2 minutes
(128 seconds) processing a CBC reminder (ordering,
reviewing and documenting) for one patient.
�CPAS Service monitors ~7200 patients annually
� 20% high risk
� 80% low risk
�Low risk patients (~5760) receive a CBC lab twice yearly
� Across the entire CPAS Service, the annual average total time
spent monitoring CBC labs for low risk patients is 410 hours or
51 days
� Each pharmacist spends an average of 27.3 hours or 3.5 days
monitoring CBC labs each year
CBC Monitoring Metrics

9
Implementation
� Based on the information from the Lean Six Sigma process a decision was made to stop routine CBC monitoring
• Patients with mechanical heart valves exempted
• CBC monitoring at discretion of managing pharmacist
� A process was developed in Dawn AC to automatically identify patients who no longer needed monitoring
� Reminders for these patients were converted to ‘complete’

10
In January 2009, the Clinical Pharmacy Anticoagulation Service (CPAS) Unit
Based Team (UBT) initiated a project to assess and evaluate the current
practice of double documentation in DAWN AC and Health Connect on
100% of their patients

11
Problem Statement
The existing practice of documenting information in
DAWN AC and Health Connect is time intensive
�There is duplication of work with the existing process
�Patient encounter information is copied from DAWN AC directly into Health Connect by CPAS staff
�This practice occupies CPAS staff time that could be better spent on more value added or relevant patient care activities

12
Macro Process Flow

13
Data Collection
�Average time for telephone communication is 86 seconds
�Average time to generate a patient letter is 18 seconds
Some pharmacists prefer to communicate with patients ‘Step 3’ with an ‘In Range’ INR lab value via patient letter
versus contacting the patient via phone
Average Time for Method of Communication
0
20
40
60
80
100
120
140
160
0 2 4 6 8 10 12 14
Individual Observations
Tim
e (
se
co
nd
s)
Phone Call Patient Letter

14
On average, pharmacists spend an additional 68 seconds
communicating with patients with an ‘In Range’ lab level
via phone versus sending a patient letter
�Each CPAS pharmacist processes ~50 patients per day
�~60% of patients have an ‘In Range’ INR lab value
�Pharmacists may spend an average of 34 minutes per day speaking with patients via phone vs. utilizing the patient letter functionality
�This translates to 2.8 hours per week or 0.07 FTE
Telephone vs. Patient Letter Metrics

15
Project Scope
The project scope includes 3 of the 8 steps outlined in
the Macro Process Flow on slide 4
�Step 5 ‘DAWN AC Progress Note’ and Step 6 ‘Copy Note in Health Connect’ represent the double documentation piece in this workflow
�Streamlining Step 7 ‘Check HC for INR Order and Order lab if Needed’ of the process to ensure a standing INR lab order is available in Health Connect may be an additional area of opportunity if DAWN AC can automatically generate this order into Health Connect

16
Data Collection
Time for Health Connect documentation ranged from 19 seconds to 52 seconds, with an average
documentation time of 30 seconds
Average Time for Health Connect Documentation
0
10
20
30
40
50
60
0 5 10 15 20 25 30 35 40
Individual Observations
Tim
e (
seco
nd
s)
This data was manually collected during observations of four CPAS pharmacist’s daily work to establish current state

17
On average, CPAS pharmacists spend ~23 seconds
performing duplicate documentation (Steps 5 & 6) into
Health Connect for one patient
�Each CPAS pharmacist processes ~50 patients per day
� Each pharmacist spends an average of 19 minutes per day
documenting information into Health Connect. This translates to
1.6 hours per week or 0.04 FTE per pharmacist
�Annually, each pharmacist spends ~81 hours, or 11
days, documenting duplicate information in Health
Connect
Health Connect Documentation Metrics

18
CPAS pharmacists spend an additional 7 seconds
verifying an INR Order (Step 7) in Health Connect.
This increases the average documentation time to
~30 seconds for each patient
Each CPAS pharmacist processes ~50 patients per day
� Each pharmacist spends an average of 25 minutes per day
documenting information into Health Connect. This translates to
2 hours per week or 0.05 FTE per pharmacist
�Annually, each pharmacist spends ~106 hours, or 14
days, documenting duplicate information in Health
Connect
Health Connect Documentation Metrics

19
Across the entire CPAS Service, the average total time spent documenting information in Health Connect (by all 15 pharmacists) is ~1,594 hours or 213 days per year
�This time could be better spent on more value added or relevant patient care activities
Health Connect Documentation Metrics
20
The time it takes to complete this entire workflow
(Steps 1 through 8) for one patient ranges from an
average of 2.9 minutes for patients with an ‘In Range’
INR lab value, up to 4.5 minutes for patients with an
‘Out of Range’ lab value
�The CPAS Service takes care of ~750 patients per day
�~ 60% of patients have INR labs ‘In Range’
�~ 40% of patients have INR labs ‘Out of Range’
Health Connect Documentation Metrics

21
Removing duplicate documentation in Health
Connect frees up ~31.25 hours per week
�This time could be used to serve an additional:
�646 patients with an INR lab value ‘In Range’
OR
�417 patients with an INR lab value ‘Out of
Range’
Health Connect Documentation Metrics

22
Initial Focus: Letters for In-range Results
Dose Letter Score Card 7/6 - 7/19
89
76
120
85
67
63 69
64 71
92
79
62 7
8 78 84
0
20
40
60
80
100
120
140
160
180
200
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
INR Recall >3 Weeks Dose Letters % Dose Letters

23
Dose Letters + Email Score Card 7/6 -7/199
0
76
20
4
99
68 8
0 87
78
72
10
2
83
66 8
9
83 86
0
50
100
150
200
250
300
350
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Pharmacist
INR Recall >3 Weeks Dose Letters + Emails % Dose Letters + Emails

24
Out of Range Dose Letters 7/6 - 7/19
5
11
56
42 3
8
36
18
10
5 6
14
0
10
20
30
40
50
60
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Pharmacist
Out of Range Dose Letters

25
Out of Range Emails 7/6 - 7/19
0 0
52
2 0
5 42 0 1 2 0 1 1 1
0
10
20
30
40
50
60
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Pharmacist
Out of Range Emails