us court of appeals for veterans claims
TRANSCRIPT
1
IN THE UNITED STATES COURT OF APPEALS FOR VETERANS CLAIMS
KENNETH J. CLAPP, ) Appellant, ) ) vs. ) Vet. App. No. 17-0776 ) DENIS MCDONOUGH, ) Secretary of Veterans Affairs, ) Appellee. )
APPELLANT’S SUPPLEMENTAL MEMORANDUM OF LAW
In response to the Court’s January 21, 2021 Order, Appellant submits this
supplemental memorandum of law discussing Long v. Wilkie, -- Vet.App. --, 2020 WL
7757076 (Vet.App. Dec. 30, 2020), and its application to this case. He asserts that the
Court’s decisions in Long, 2020 WL 7757076 and Morgan v. Wilkie, 31 Vet.App. 162
(2019) provide further support for remand here because Mr. Clapp’s abnormal acoustic
reflexes are not contemplated by the hearing loss rating criteria, and the Board failed to
provide this analysis in the first instance.
The Board erred when it failed to analyze the Veteran’s abnormal
ipsilateral and contralateral acoustic reflexes. See R-670. Acoustic reflexes do not
measure hearing thresholds; rather, they measure reflected energy, which is a function
of stapedius muscle contraction and allows an examiner to assess the middle ear.
Jackie L. Clark, Open Access Guide to Audiology and Hearing Aids for Otolaryngologists,
available at https://vula.uct.ac.za/access/content/group/27b5cb1b-1b65-4280-9437-
2
a9898ddd4c40/Acoustic%20_stapedius_%20reflexes.pdf (last accessed Feb. 22,
2021)1; see Appellant’s Br. at 6 n. 1, Appendix 1. Sensorineural hearing loss, such as
Mr. Clapp’s, R-670, obstructs transmissions of signals within the ear and causes
reduced or absent acoustic reflexes. See Clark, Open Access Guide to Audiology and
Hearing Aids for Otolaryngologists at 3.
Whether the Veteran’s abnormal acoustic reflexes meet the first step of the
extraschedular framework is a factual determination that the Board must make in the
first instance. See Hensley v. West, 212 F. 3d 1255, 1263 (Fed. Cir. 2000). But in
evaluating the Veteran’s disability picture, the Board did not discuss the Veteran’s
non-auditory symptoms of abnormal ipsilateral and contralateral acoustic reflexes. See
R-2-9; R-670. In Long, the Court reaffirmed its long-standing extraschedular
framework requiring the Board to assess “the veteran’s disability picture as a whole” to
determine whether he or she “presents an impairment that is so exceptional that the
rating schedule is not capable of assessing it in the first instance.” 2020 WL 7757076
at *3 (emphasis added). While the Board need not in engage in “a line-item
accounting of each symptoms and effect,” it must make a “reasoned assessment of
both the veteran’s full disability picture and the capacity of the rating schedule to
evaluate such.” Id. This holding is consistent with the Court’s previous decision in
Morgan, which held that VA’s duty to maximize benefits requires the Board to
1 For the Court’s convenience, a copy of this article is attached in the appendix.
3
examine “all possible rating methods in search of the highest possible level of
established compensation as a schedular matter before resorting to the extraschedular
referral process.” 31 Vet. App. at 168. When read together, Morgan and Long require
the Board to determine whether a veteran’s disability picture is fully contemplated by
the assigned rating. If it is not, the Board must first consider the available schedular
rating tools before resorting, in the truly exceptional case, to extraschedular referral.
In this case, the Board failed to conduct the analysis required by Morgan and
Long. This was prejudicial because the record raised the theory of entitlement to
either a schedular alternative or extraschedular consideration. See Long, 2020 WL
7757076 at *5. Mr. Clapp raised the theory that his non-compensable schedular rating
did not adequately compensate him for his full disability picture and requested a 50%
disability rating. R-61; see also R-387-88; R-423-24.
Although the Veteran pointed to difficulties communicating, his pleadings did
not relieve the Board of its duty to assess his full disability picture, which included his
abnormal acoustic reflexes. See Long, 2020 WL 7757076 at *3. The Federal Circuit
recently found that this Court’s holding in Clemons v. Shinseki, 23 Vet.App. 1 (2009)
“provides valuable guidance as to how the VA should interpret filings from a
veteran.” Murphy v. Wilkie, 983 F. 3d 1313, 1318 (Fed. Cir. 2020). Specifically,
interpreting a veteran’s filings “is best accomplished by looking to the veteran’s
reasonable expectations in filing the claim and the evidence developed in processing
that claim.” Id.

4
Here, the record makes clear the Mr. Clapp reasonably expected VA to provide
proper consideration to his claim and believed that a minimum rating of 50% was
appropriate. R-61. In the process of developing the Veteran’s claim, VA obtained
evidence of abnormal acoustic reflexes. R-670. These abnormalities were diagnosed
during the Veteran’s VA hearing loss examination and are therefore clearly related to
his service-connected hearing loss. See Long, 2020 WL 7757076 at *5. Thus, where
the Board only considered the Veteran’s hearing and communication impairment, it
failed to analyze his complete disability picture. Moreover, the Board’s incomplete
analysis of the first step resulted in its failure to assess the second step, despite
evidence that Mr. Clapp experienced interference with work. See Appellant’s Br. at 8-
10; R-314-15; R-672; see also Yancy v. McDonald, 27 Vet.App. 484, 495 n. 5 (2016).
In order to establish that remand is warranted under Morgan, a veteran must
simply show that he or she has symptoms or complications related to a service-
connected disability, but which are not compensated by his or her assigned schedular
rating. See Morgan, 31 Vet.App. at 168. It is the Board’s duty to maximize benefits
based on the availability of schedular rating tools when those “schedular alternatives
for rating a disability are either raised by the claimant or reasonably raised by the
record.” See id. This Court’s recent decision in Bailey v. Wilkie, --Vet.App. --, 2021
WL 45679 (Vet. App. Jan. 6, 2021), reaffirmed the Board’s duty to maximize benefits
by considering schedular alternatives to compensate complications of a service-
connected disability. Similar to its holding in Long, the Court held that there must be
5
some “causal or aggravative relationship” between the primary service-connected
disability and the disability for which a schedular alternative is sought. Bailey, 2021
WL 45679 at *9.
Such a relationship exists here. As discussed above, the Veteran’s acoustic
reflexes were noted during a VA hearing loss examination. R-670. And sensorineural
hearing loss causes reduced or absent acoustic reflexes. See Clark, Open Access Guide to
Audiology and Hearing Aids for Otolaryngologists, supra. Therefore, there exists a causal
relationship between the Veteran’s hearing loss and his abnormal acoustic reflexes.
See Bailey, at *9.
Had the Board found that the Veteran’s hearing loss rating did not adequately
contemplate his acoustic reflexes, it might have determined that they warranted a
separate rating under an alternative diagnostic code, pursuant to its duty to maximize
benefits. The Veteran’s abnormal acoustic reflexes were noted in the
“(Tympanometry) Findings” section of his examination. R-670. Tympanometry
measures the pressure, presence of fluid, and mobility in the middle ear. Claude
Laurent, “Tympanometry,” Open Access Guide to Audiology and Hearing Aids for
Otolaryngologists, https://vula.uct.ac.za/access/content/group/27b5cb1b-1b65-4280-
9437-a9898ddd4c40/Tympanometry.pdf (last accessed Feb. 22, 2021)2. These
2 For the Court’s convenience, a copy of this article is attached in the appendix.
6
measurements can evaluate otitis media, which is a compensable disability under 38
C.F.R. § 4.87, Diagnostic Code 6200. See id.
This Court’s holdings in Long and Morgan demonstrate that remand is required
because the Board failed to analyze the Veteran’s complete disability picture when it
did not determine whether his hearing loss rating contemplated his abnormal acoustic
reflexes. The Board needs to assess the Veteran’s entitlement to maximized
benefits—either via a schedular alternative or via extraschedular consideration—in the
first instance. See Wagner v. United States, 365 F.3d 1358, 1365 (Fed. Cir. 2004)
(“Where the effect of an error on the outcome of a proceeding is unquantifiable,
however, we will not speculate as to what the outcome might have been had the error
not occurred.”).
Respectfully submitted,
/s/Alec Saxe ALEC SAXE CHISHOLM CHISHOLM & KILPATRICK 321 S Main St #200 Providence, RI 02903 (401) 331-6300 Telephone (401) 421-3185 Facsimile Attorneys for Appellant

APPENDIX
OPEN ACCESS GUIDE TO AUDIOLOGY AND HEARING
AIDS FOR OTOLARYNGOLOGISTS
ACOUSTIC (STAPEDIUS) REFLEXES Jackie L. Clark
The acoustic reflex, also known as the
stapedius reflex refers to an involuntary
muscle contraction of the stapedius muscle
in response to a high-intensity sound sti-
mulus. Due to ease of administration and
information yielded, the acoustic reflex is
considered one of the most powerful
differential diagnostic audiological proce-
dures.
The acoustic reflex and the tympanogram
(see tympanometry chapter) are commonly
used to assess middle ear function and are
considered best practice. Each test yields
invaluable information based on the
delivery of acoustic energy (sound) to the
ear canal. Thanks to microprocessors, the
instruments used are now capable of rapid
middle ear function assessment (typically
<1min/ear).
Acoustic reflexes do not measure hearing
threshold. Rather, they measure reflected
energy which is a function of stapedius
muscle contraction; it allows one to indi-
rectly assess the middle ear, cochlea and
neural innervation of the stapedius muscle.
As the acoustic reflex is involuntary and
bilateral, it is replicable and provides
valuable diagnostic information when
comparing the amount of reflected energy
according to signal intensity, as well as the
presence of ipsilateral and bilateral acous-
tic reflexes.
Premise behind instrumentation
An acoustic stimulus is presented to the
external auditory canal; energy is transfer-
red from the ear canal through the middle
ear, some of which is reflected and some
absorbed by the tympanic membrane and
external ear structures.
The premise behind the immittance
instrumentation used to measure the
acoustic reflex is the ability to accurately
measure changes in reflected energy
occurring from stiffening of the tympanic
membrane as a result of contraction of the
stapedius muscle (For the premise behind
tympanometry see tympanometry chapter).
The amount of reflected and absorbed
energy varies depending on the admit-
tance/impedance (flow/resistance) of ener-
gy within the system and the complex
interaction between the ear structures.
The presence of reflexes within normal
intensity limits is consistent with normal
middle ear and brainstem function and
suggests that auditory sensitivity is not
significantly impaired. An elevated or ab-
sent acoustic reflex threshold is consistent
with a middle ear disorder, hearing loss in
the stimulated ear, and/or interruption of
neural innervation of the stapedius muscle.
Anatomy & Physiology
Neural mechanisms mediate the acoustic
reflex that results in involuntary stapedius
muscle contraction stiffening the stapes
within the middle ear. It is presumed that
the physiologic reason for the reflex is that
it serves as an inhibitory response to re-
duce the sound intensities reaching the in-
ner ear by as much as 20 dB evoked when
individuals vocalise (Møller, 2000).
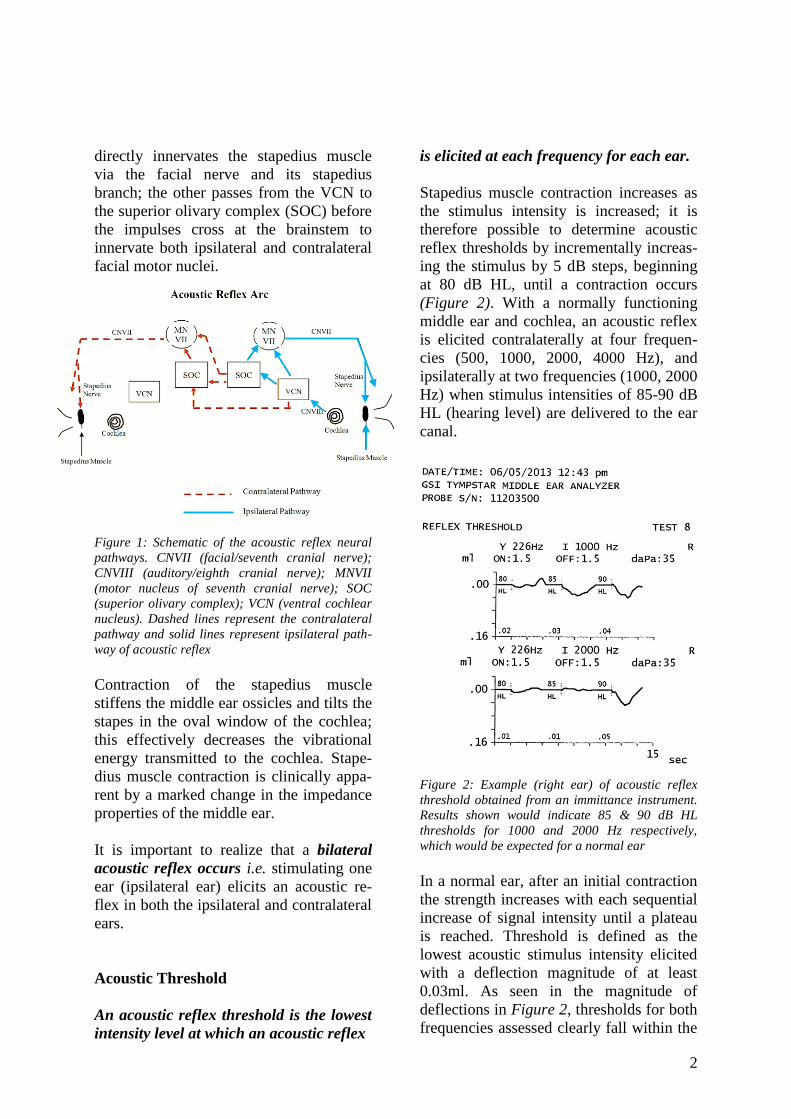
As is illustrated in Figure 1, once a high
intensity auditory stimulus is initiated and
reaches the cochleae, neural impulses from
the auditory nerves (CN VIII) ascend from
both cochleae to each ipsilateral ventral
cochlear nucleus (VCN). From VCN the
reflex has two main neural pathways: one
passes from the VCN directly to the ipsi-
lateral facial motor nucleus (CN VII) that
2
directly innervates the stapedius muscle
via the facial nerve and its stapedius
branch; the other passes from the VCN to
the superior olivary complex (SOC) before
the impulses cross at the brainstem to
innervate both ipsilateral and contralateral
facial motor nuclei.
Figure 1: Schematic of the acoustic reflex neural
pathways. CNVII (facial/seventh cranial nerve);
CNVIII (auditory/eighth cranial nerve); MNVII
(motor nucleus of seventh cranial nerve); SOC
(superior olivary complex); VCN (ventral cochlear
nucleus). Dashed lines represent the contralateral
pathway and solid lines represent ipsilateral path-
way of acoustic reflex
Contraction of the stapedius muscle
stiffens the middle ear ossicles and tilts the
stapes in the oval window of the cochlea;
this effectively decreases the vibrational
energy transmitted to the cochlea. Stape-
dius muscle contraction is clinically appa-
rent by a marked change in the impedance
properties of the middle ear.
It is important to realize that a bilateral
acoustic reflex occurs i.e. stimulating one
ear (ipsilateral ear) elicits an acoustic re-
flex in both the ipsilateral and contralateral
ears.
Acoustic Threshold
An acoustic reflex threshold is the lowest
intensity level at which an acoustic reflex
is elicited at each frequency for each ear.
Stapedius muscle contraction increases as
the stimulus intensity is increased; it is
therefore possible to determine acoustic
reflex thresholds by incrementally increas-
ing the stimulus by 5 dB steps, beginning
at 80 dB HL, until a contraction occurs
(Figure 2). With a normally functioning
middle ear and cochlea, an acoustic reflex
is elicited contralaterally at four frequen-
cies (500, 1000, 2000, 4000 Hz), and
ipsilaterally at two frequencies (1000, 2000
Hz) when stimulus intensities of 85-90 dB
HL (hearing level) are delivered to the ear
canal.
Figure 2: Example (right ear) of acoustic reflex
threshold obtained from an immittance instrument.
Results shown would indicate 85 & 90 dB HL
thresholds for 1000 and 2000 Hz respectively,
which would be expected for a normal ear
In a normal ear, after an initial contraction
the strength increases with each sequential
increase of signal intensity until a plateau
is reached. Threshold is defined as the
lowest acoustic stimulus intensity elicited
with a deflection magnitude of at least
0.03ml. As seen in the magnitude of
deflections in Figure 2, thresholds for both
frequencies assessed clearly fall within the
3
criteria of at least 0.03ml deflection. To
identify a threshold it is advisable to
confirm the magnitude of the deflection
with a repeat presentation. Once a thres-
hold has been established at one frequency,
the intensity is recorded, and the other
frequencies are then assessed. During
quick screening it is not unusual to assess
an acoustic reflex threshold at only one
frequency and a single set intensity (~95 or
100 dB HL. An ipsilateral acoustic reflex
threshold tends to be attained at a slightly
lower intensity stimulus than an acoustic
reflex threshold elicited by a contralateral
stimulus.
Factors affecting acoustic reflexes
• Ipsilateral conductive hearing loss:
Anything that obstructs transmission of
a sound signal to the cochlea in the
stimulated ear results in reduced or
absent contraction of the stapedius
muscles. Middle ear disorders therefore
easily mask an acoustic reflex. Forty
percent of patients with conductive
hearing loss of >20 dB HL do not have
an acoustic reflex. Once conductive
hearing loss reaches 40 dB HL, about
80% of patients do not have a reflex
(Jerger, Anthony, Jerger and Mauldin,
1974)
• Ipsilateral sensorineural hearing loss:
This may obstruct transmission of a
signal beyond the cochlea of the stimu-
lated ear and usually causes reduced or
absent contraction of the stapedius
muscles. However, because of recruit-
ment of loudness in cochlear sensori-
neural hearing loss, acoustic reflexes
may occur even within the expected
normal or partially elevated intensity
range in the presence of mild or
moderate-to-severe sensorineural hear-
ing loss.
• Stapes fixation: The stapes footplate is
more-or-less fixed to the surrounding
bone with otosclerosis (and sometimes
with tympanosclerosis). This may in-
terfere with the acoustic reflex in two
ways: it causes a conductive hearing
loss; and reduced mobility of the stapes
prevents stiffening of the tympanic
membrane when the stapedius muscle
contracts
• Ossicular disarticulation: As with
otosclerosis, it causes a conductive
hearing loss, and if located lateral to
the stapes, prevents stiffening of the
ossicles and tympanic membrane when
the stapedius muscle contracts
• Middle ear effusion: This causes a
conductive hearing loss, and reduces
compliance of the tympanic membrane
and middle ear structures and may
mask the presence of an acoustic reflex
• Tympanic membrane perforation:
This causes a conductive hearing loss.
Furthermore, due to the perforation,
changes in compliance caused by con-
traction of the stapedius muscle cannot
be measured
• Negative/abnormal middle ear pres-
sure: To maximize the likelihood that a
reflex will be detected, the pressure on
either side of the tympanic membrane
has to be equal for the tympanic mem-
brane to be at or near the point of
maximum compliance (see tympano-
metry chapter for further explanation).
This necessitates one to match the peak
pressure of the tympanogram to the
actual middle ear pressure so that valid
acoustic reflex threshold values may be
obtained
• Facial nerve dysfunction: The stape-
dius muscle is innervated by the facial
nerve. Contraction of the stapedius
muscle has to occur for both ipsi- and
contralateral acoustic reflexes.
4
Interpretation of acoustic reflexes
Acoustic reflexes may be reported as:
• Ipsilateral: Reflex recorded in ear to
which auditory stimulus is presented
• Contralateral: Reflex recorded in ear
contralateral to which auditory stimu-
lus is presented
• Partially present: Reflex present at
some frequencies and absent at others
• Elevated threshold: Reflex thresholds
elicited >100 dB HL
• Absent reflex: No reflex elicited
Partial or elevated reflex thresholds may
indicate the presence of hearing loss at the
frequencies where they are specifically
absent.
Absent reflexes have also been observed in
individuals with normal or near-normal
hearing, which may then indicate middle
ear disease or neurological involvement of
the 8th cranial nerve, such as in pontine
angle tumours and auditory neuropathy
(see below), or neurological involvement
of the 7th cranial nerve. With facial nerve
paralysis, the absence of acoustic reflexes
in the presence of normal middle ear
function suggests a lesion in the neural
pathway proximal to the stapedius nerve,
whereas the presence of an acoustic reflex
in patients with facial nerve paralysis sug-
gests that the lesion is distal to the origin
of the nerve. A very small percentage of
people will have normal auditory sensiti-
vity and absent acoustic reflexes across all
frequencies without other identifiable pa-
thology.
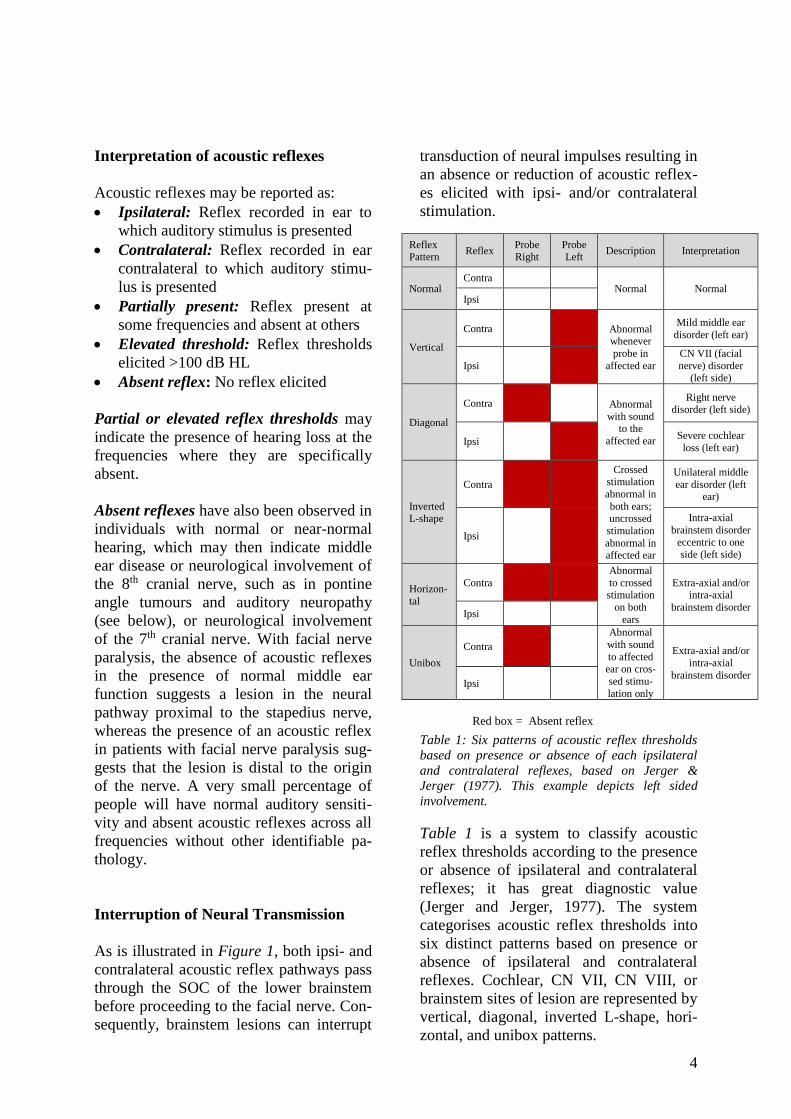
Interruption of Neural Transmission
As is illustrated in Figure 1, both ipsi- and
contralateral acoustic reflex pathways pass
through the SOC of the lower brainstem
before proceeding to the facial nerve. Con-
sequently, brainstem lesions can interrupt
transduction of neural impulses resulting in
an absence or reduction of acoustic reflex-
es elicited with ipsi- and/or contralateral
stimulation.
Table 1: Six patterns of acoustic reflex thresholds
based on presence or absence of each ipsilateral
and contralateral reflexes, based on Jerger &
Jerger (1977). This example depicts left sided
involvement.
Table 1 is a system to classify acoustic
reflex thresholds according to the presence
or absence of ipsilateral and contralateral
reflexes; it has great diagnostic value
(Jerger and Jerger, 1977). The system
categorises acoustic reflex thresholds into
six distinct patterns based on presence or
absence of ipsilateral and contralateral
reflexes. Cochlear, CN VII, CN VIII, or
brainstem sites of lesion are represented by
vertical, diagonal, inverted L-shape, hori-
zontal, and unibox patterns.
Reflex Pattern
Reflex Probe Right
Probe Left
Description Interpretation
Normal Contra
Normal Normal Ipsi
Vertical
Contra Abnormal whenever
probe in
affected ear
Mild middle ear
disorder (left ear)
Ipsi
CN VII (facial
nerve) disorder (left side)
Diagonal
Contra Abnormal
with sound to the
affected ear
Right nerve disorder (left side)
Ipsi Severe cochlear
loss (left ear)
Inverted L-shape
Contra
Crossed stimulation
abnormal in
both ears; uncrossed
stimulation
abnormal in affected ear
Unilateral middle
ear disorder (left ear)
Ipsi
Intra-axial
brainstem disorder
eccentric to one side (left side)
Horizon-
tal
Contra
Abnormal
to crossed stimulation
on both
ears
Extra-axial and/or intra-axial
brainstem disorder Ipsi
Unibox
Contra
Abnormal
with sound
to affected ear on cros-
sed stimu-
lation only
Extra-axial and/or
intra-axial
brainstem disorder Ipsi
Red box = Absent reflex
5
Wideband reflectance technique
This is a newer measuring technique (Fee-
ney, Douglas and Sanford, 2004) to assess
acoustic stapedius reflex thresholds by
using complex wideband (125 - 10,000 Hz
range) reflectance with a stimulus
resembling “chirplike” sounds instead of a
single probe tone frequency. The wideband
reflectance technique reportedly yields
more reliable results than the single probe
tone technique, and appears to hold
promise as a clinical procedure for
measuring acoustic reflexes for normal-
hearing subjects who fail to demonstrate
reflexes with the standard clinical proce-
dure.
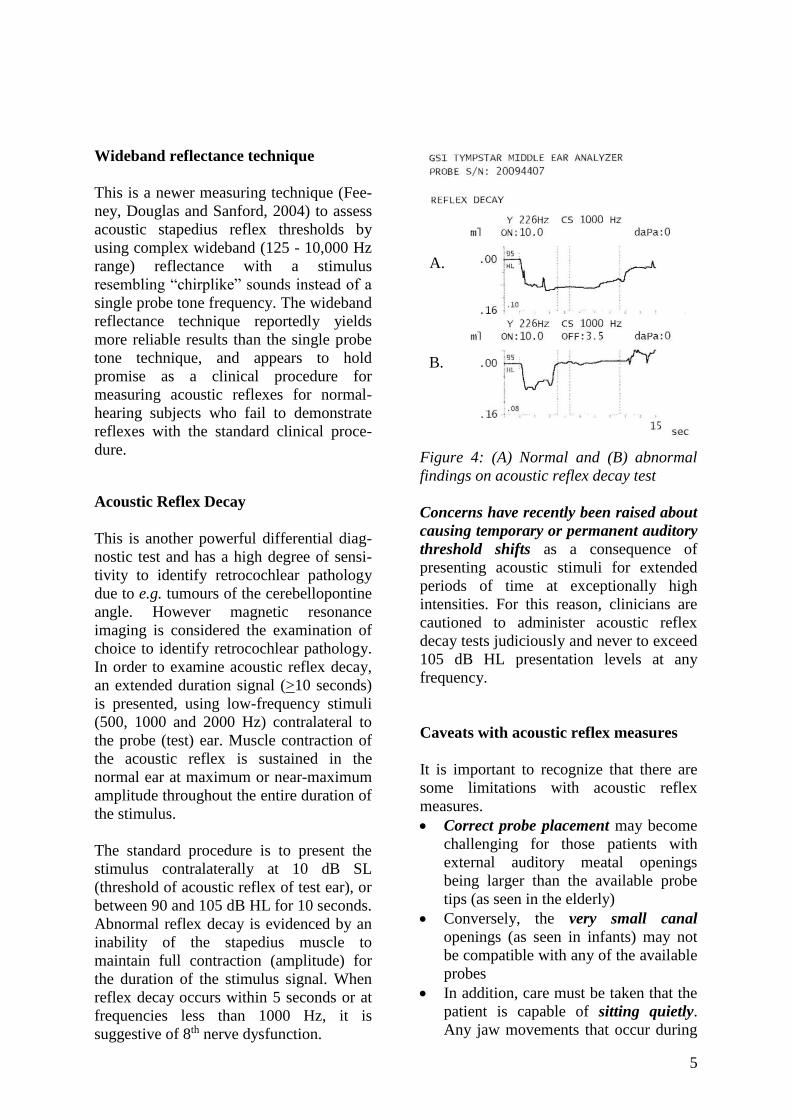
Acoustic Reflex Decay
This is another powerful differential diag-
nostic test and has a high degree of sensi-
tivity to identify retrocochlear pathology
due to e.g. tumours of the cerebellopontine
angle. However magnetic resonance
imaging is considered the examination of
choice to identify retrocochlear pathology.
In order to examine acoustic reflex decay,
an extended duration signal (>10 seconds)
is presented, using low-frequency stimuli
(500, 1000 and 2000 Hz) contralateral to
the probe (test) ear. Muscle contraction of
the acoustic reflex is sustained in the
normal ear at maximum or near-maximum
amplitude throughout the entire duration of
the stimulus.
The standard procedure is to present the
stimulus contralaterally at 10 dB SL
(threshold of acoustic reflex of test ear), or
between 90 and 105 dB HL for 10 seconds.
Abnormal reflex decay is evidenced by an
inability of the stapedius muscle to
maintain full contraction (amplitude) for
the duration of the stimulus signal. When
reflex decay occurs within 5 seconds or at
frequencies less than 1000 Hz, it is
suggestive of 8th nerve dysfunction.
Figure 4: (A) Normal and (B) abnormal
findings on acoustic reflex decay test
Concerns have recently been raised about
causing temporary or permanent auditory
threshold shifts as a consequence of
presenting acoustic stimuli for extended
periods of time at exceptionally high
intensities. For this reason, clinicians are
cautioned to administer acoustic reflex
decay tests judiciously and never to exceed
105 dB HL presentation levels at any
frequency.
Caveats with acoustic reflex measures
It is important to recognize that there are
some limitations with acoustic reflex
measures.
• Correct probe placement may become
challenging for those patients with
external auditory meatal openings
being larger than the available probe
tips (as seen in the elderly)
• Conversely, the very small canal
openings (as seen in infants) may not
be compatible with any of the available
probes
• In addition, care must be taken that the
patient is capable of sitting quietly.
Any jaw movements that occur during
A.
B.

6
coughing, crying, talking, swallowing,
or jaw clenching will result in artifact
and provide fallacious results.
• Reportedly, collapsed canals due to
placement of supra-aural headphones
on the pinna of the contralateral ear
may also result in fallacious findings
Concluding remarks
Despite the few limitations with acoustic
reflex threshold testing, the advantages far
overshadow those limitations. Although
few new discoveries have been made with
acoustic reflex threshold testing, it is still
considered one of the most powerful
differential diagnostic tools that should be
within the standard battery of tests
attempted with all patients. Within a very
brief time period it allows one to identify
middle ear pathology; cochlear or retro-
cochlear pathology; evaluate neural trans-
mission efficiency; while providing a
general indicator of magnitude of hearing
loss.
References
• Feeney MP, Douglas HK, & Sanford
CA (2004). Wideband reflectance
measures of the ipsilateral acoustic
stapedium reflex threshold. Ear
Hearing, 25: 421-30
• Jerger S & Jerger J (1977). Diagnostic
value of cross vs. uncrossed acoustic
reflexes: Eighth nerve and brain stem
disorders. Arch Otolaryngol, 103: 445-
53
• Jerger J, Anthony L, Jerger S, and
Mauldin L. (1974). Studies in impe-
dance audiometry. III. Middle ear dis-
orders. Arch Otolaryngol, 99: 165-71
• Møller A. (2000). Hearing: Its physio-
logy and pathophysiology. Academic
Press.181-90
Author
Jackie L. Clark, PhD/CCC-A; F-AAA
Clinical Associate Professor
School of Behavioral & Brain Sciences,
UT Dallas/Callier Center
Research Scholar; Univ Witwatersrand,
Johannesburg, South Africa
Managing Editor International Journal of
Audiology
http://www.utdallas.edu/~jclark
Editors
Claude Laurent, MD, PhD
Professor in ENT
ENT Unit, Department of Clinical Science
University of Umeå
Umeå, Sweden
De Wet Swanepoel PhD
Associate Professor
Department of Communication Pathology
University of Pretoria
Pretoria, South Africa
Johan Fagan MBChB, FCS(ORL), MMed
Professor and Chairman
Division of Otolaryngology
University of Cape Town
Cape Town, South Africa
OPEN ACCESS GUIDE TO
AUDIOLOGY & HEARING AIDS
FOR OTOLARYNGOLOGISTS
http://www.entdev.uct.ac.za
Open Access Guide to Audiology & Hearing Aids for
Otolaryngologists by Johan Fagan (Editor)
[email protected] is licensed under a Creative
Commons Attribution - Non-Commercial 3.0 Unported
License
OPEN ACCESS GUIDE TO AUDIOLOGY AND HEARING
AIDS FOR OTOLARYNGOLOGISTS
TYMPANOMETRY Claude Laurent
Tympanometry is not a test of a patient’s
hearing. It objectively provides an indi-
cation of the status of the middle ear and
the mobility of the ear drum. It does this
by measuring the degree to which sound
transmission through the eardrum and
middle ear is modified when there is a
change in air pressure applied to the
eardrum. Tympanometry provides useful
information about:
• Pressure in the middle ear space
• Presence of fluid in the middle ear
space
• Mobility of the middle ear system
• Volume of the ear canal
Indications for tympanometry
Not all patients with ear pathology require
tympanometry.
1. Suspected middle ear effusion (OME)
Tympanometry is recommended main-ly to
evaluate suspected OME/secre-tory otitis
media (SOM). It is done in conjunction
with information obtained from the history,
appearance and mobility of the eardrum.
Otoscopic and otomicroscopic evidence of
OME may include yellowness, redness,
hypervascularity, bulging or retraction of
the ear-drum, visible air-fluid levels, and
diminished mobility on pneumatic
otoscopy. Otomicroscopic and pneu-matic
otoscopy have been reported to have a high
accuracy for diagnosing OME in children1.
Yet it is uncertain what degree of training
and expertise is required to obtain high
accuracy 1. Tympanometry however requi-
res minimal training, is quick and simple to
perform, and provides objective
information.
2. Patency of tympanostomy/ventilation
tubes/grommets
3. Whether there is a perforation in the
eardrum
4. Mobility of the eardrum
5. Mobility of the ossicular chain
Principles of tympanometry
Tympanometry provides a measurement
of impedance of the middle ear system
including the eardrum. It allows one to
determine how much resistance the
middle ear system renders to passage of
sound to the inner ear.
Impedance of the middle ear is increased
if:
• The middle ear is filled with fluid,
especially with thick secretion
• There is increased stiffness of the
ossicular chain, for example when
there is a fixation of the malleus or
stapes (hammer or stirrup). In oto-
sclerosis the stapes becomes progress-
sively fixed in the oval window; due to
this the impedance increases in later
stages of the disease.
Impedance of the middle ear is reduced
if:
• The eardrum is overly mobile or flac-
cid
• There is a disruption of the ossicular
chain
How does tympanometry work?
A constant low-pitch sound (~220Hz) is
introduced into the ear through an opening
in the head (tip) of the tympanometer that
is tightly introduced into the external ear
canal using a plastic or foam rubber collar
(Figure 1). In the same tip there is another
opening that leads to a microphone that
continuously registers the sound reflected
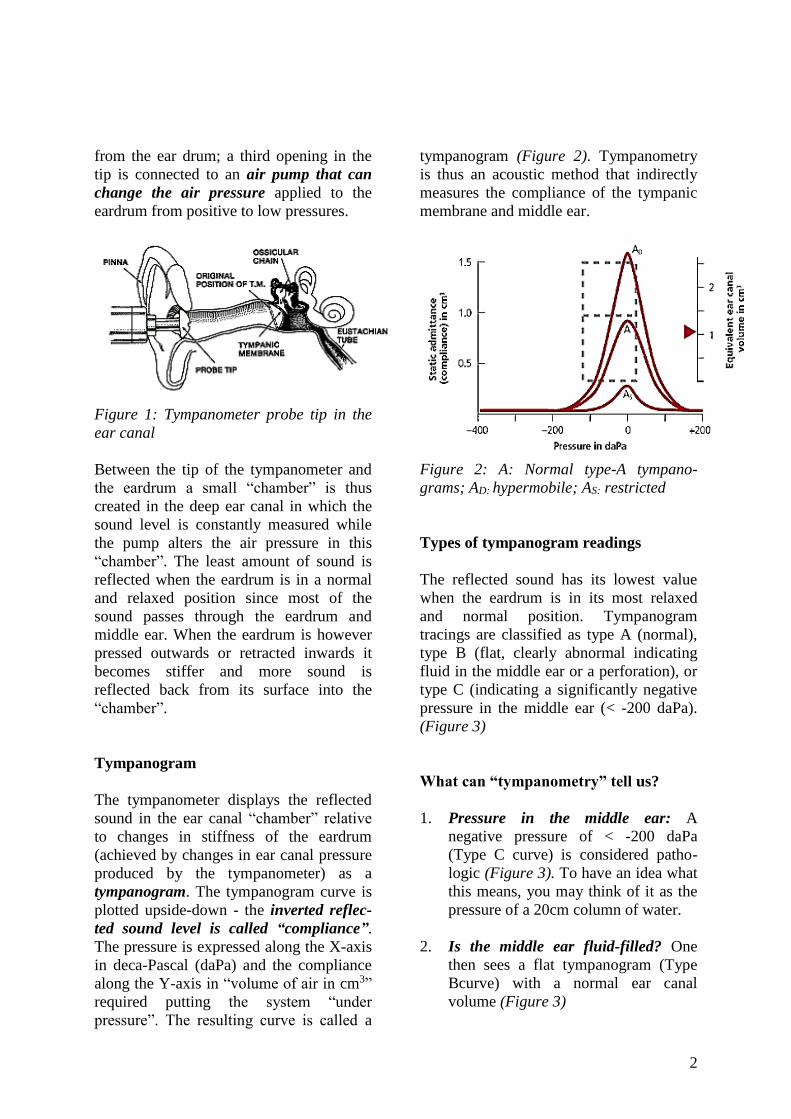
2
from the ear drum; a third opening in the
tip is connected to an air pump that can
change the air pressure applied to the
eardrum from positive to low pressures.
Figure 1: Tympanometer probe tip in the
ear canal
Between the tip of the tympanometer and
the eardrum a small “chamber” is thus
created in the deep ear canal in which the
sound level is constantly measured while
the pump alters the air pressure in this
“chamber”. The least amount of sound is
reflected when the eardrum is in a normal
and relaxed position since most of the
sound passes through the eardrum and
middle ear. When the eardrum is however
pressed outwards or retracted inwards it
becomes stiffer and more sound is
reflected back from its surface into the
“chamber”.
Tympanogram
The tympanometer displays the reflected
sound in the ear canal “chamber” relative
to changes in stiffness of the eardrum
(achieved by changes in ear canal pressure
produced by the tympanometer) as a
tympanogram. The tympanogram curve is
plotted upside-down - the inverted reflec-
ted sound level is called “compliance”.
The pressure is expressed along the X-axis
in deca-Pascal (daPa) and the compliance
along the Y-axis in “volume of air in cm3”
required putting the system “under
pressure”. The resulting curve is called a
tympanogram (Figure 2). Tympanometry
is thus an acoustic method that indirectly
measures the compliance of the tympanic
membrane and middle ear.
Figure 2: A: Normal type-A tympano-
grams; AD: hypermobile; AS: restricted
Types of tympanogram readings
The reflected sound has its lowest value
when the eardrum is in its most relaxed
and normal position. Tympanogram
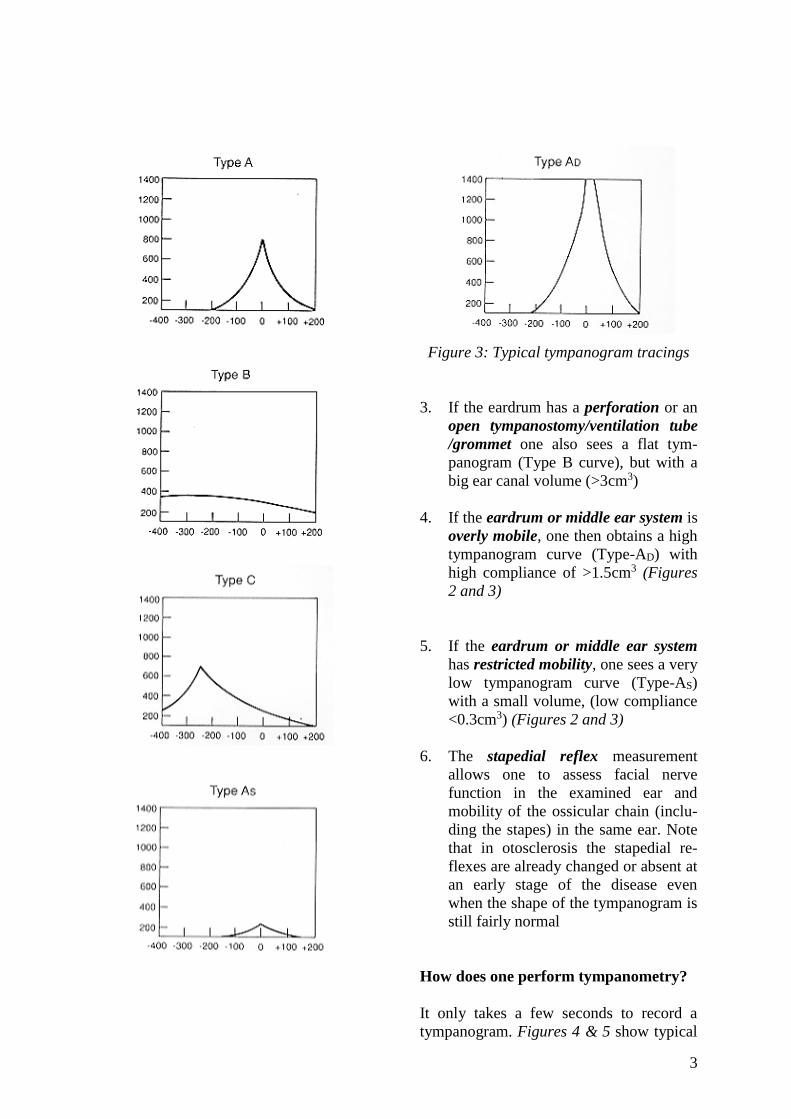
tracings are classified as type A (normal),
type B (flat, clearly abnormal indicating
fluid in the middle ear or a perforation), or
type C (indicating a significantly negative
pressure in the middle ear (< -200 daPa).
(Figure 3)
What can “tympanometry” tell us?
1. Pressure in the middle ear: A
negative pressure of < -200 daPa
(Type C curve) is considered patho-
logic (Figure 3). To have an idea what
this means, you may think of it as the
pressure of a 20cm column of water.
2. Is the middle ear fluid-filled? One
then sees a flat tympanogram (Type
Bcurve) with a normal ear canal
volume (Figure 3)
3
Figure 3: Typical tympanogram tracings
3. If the eardrum has a perforation or an
open tympanostomy/ventilation tube
/grommet one also sees a flat tym-
panogram (Type B curve), but with a
big ear canal volume (>3cm3)
4. If the eardrum or middle ear system is
overly mobile, one then obtains a high
tympanogram curve (Type-AD) with
high compliance of >1.5cm3 (Figures
2 and 3)
5. If the eardrum or middle ear system
has restricted mobility, one sees a very
low tympanogram curve (Type-AS)
with a small volume, (low compliance
<0.3cm3) (Figures 2 and 3)
6. The stapedial reflex measurement
allows one to assess facial nerve
function in the examined ear and
mobility of the ossicular chain (inclu-
ding the stapes) in the same ear. Note
that in otosclerosis the stapedial re-
flexes are already changed or absent at
an early stage of the disease even
when the shape of the tympanogram is
still fairly normal
How does one perform tympanometry?
It only takes a few seconds to record a
tympanogram. Figures 4 & 5 show typical
4
examples of tympanometers. Tympanome-
ters found in developing countries are
usually automatic screening tympano-
meters that automatically start to record
when the tip is tightly introduced into the
ear canal to create an airtight seal; the
pump that alters the pressure in the ear
canal is automatically activated when the
tip of the instrument is tightly fitted into
the ear. It is important that it is kept tightly
fitted during the whole recording process
to ensure the airtight seal is not interrupted
during testing. The tympanometer
produces a tympanometric curve that
represents the compliance of the middle
ear system, including the ear drum, as a
function of the pressure applied to the
eardrum (Figure 2). From the shape of the
curve or the figures, one can also read the
volume between the tip of the
tympanometer and the eardrum and
determine the compliance of the middle ear
system. Many screening tympanometers
also have a function to automatically
measure the ipsilateral (same side)
stapedial reflex at 1-3 supraliminal sound
stimuli (90-100 dB).
Advantages of tympanometry
It is an objective audiometric method
because it does not depend on information
that the patient gives us but rather
measures something without subjective
feedback from the patient. The patient then
becomes the object and does not have to
say whether he or she has heard or
experienced anything.
It also does not require clinical expertise
to diagnose middle ear effusions.
Pitfalls of tympanometry
• An undiagnosed, perforated eardrum or
an inadequate seal between the tip of
the tympanometer and the ear canal
will produce a Type B tympanogram
which may be misconstrued as a
middle ear effusion
• Diagnosis of a middle ear effusion per
se is not an indication for insertion of
ventilation tubes; it must be
accompanied by clinically significant
and persistent conductive hearing loss
• Although a conventional probe tone of
220 Hz is sufficient for tympanometry
in almost all populations it is not
effective for evaluating infants younger
than 7 months. For these young infants
a higher frequency probe tone of 1000
Hz is recommended.
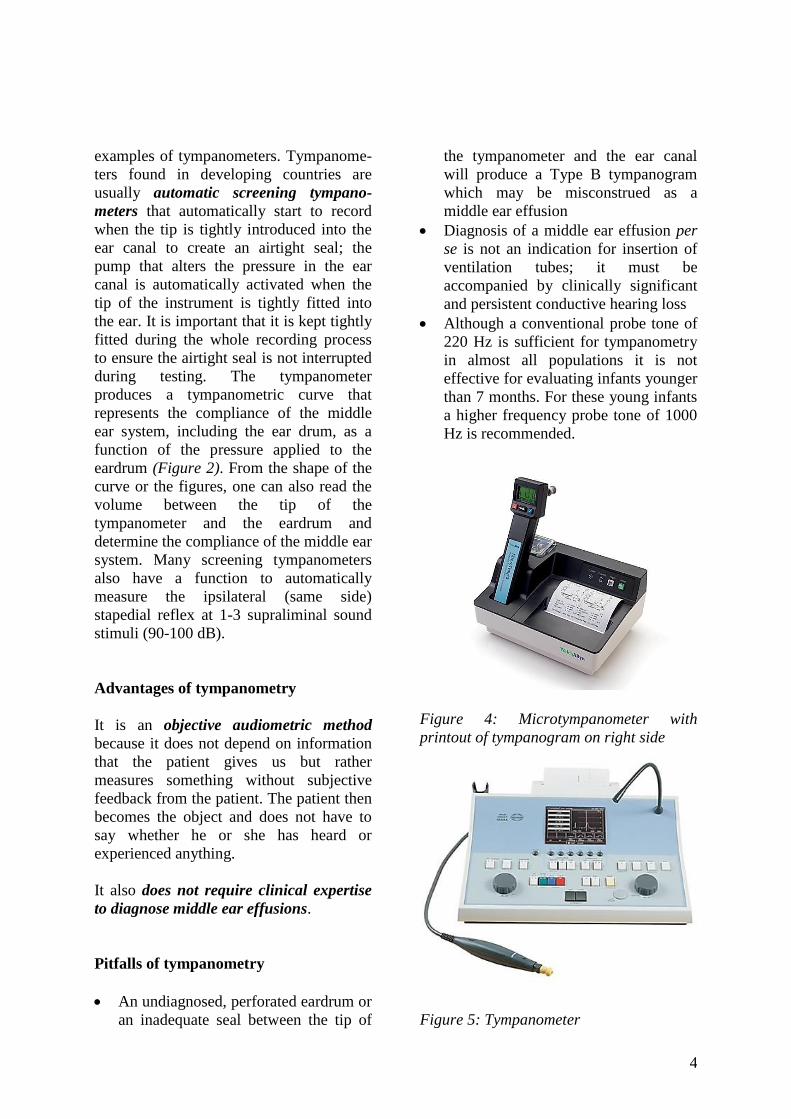
Figure 4: Microtympanometer with
printout of tympanogram on right side
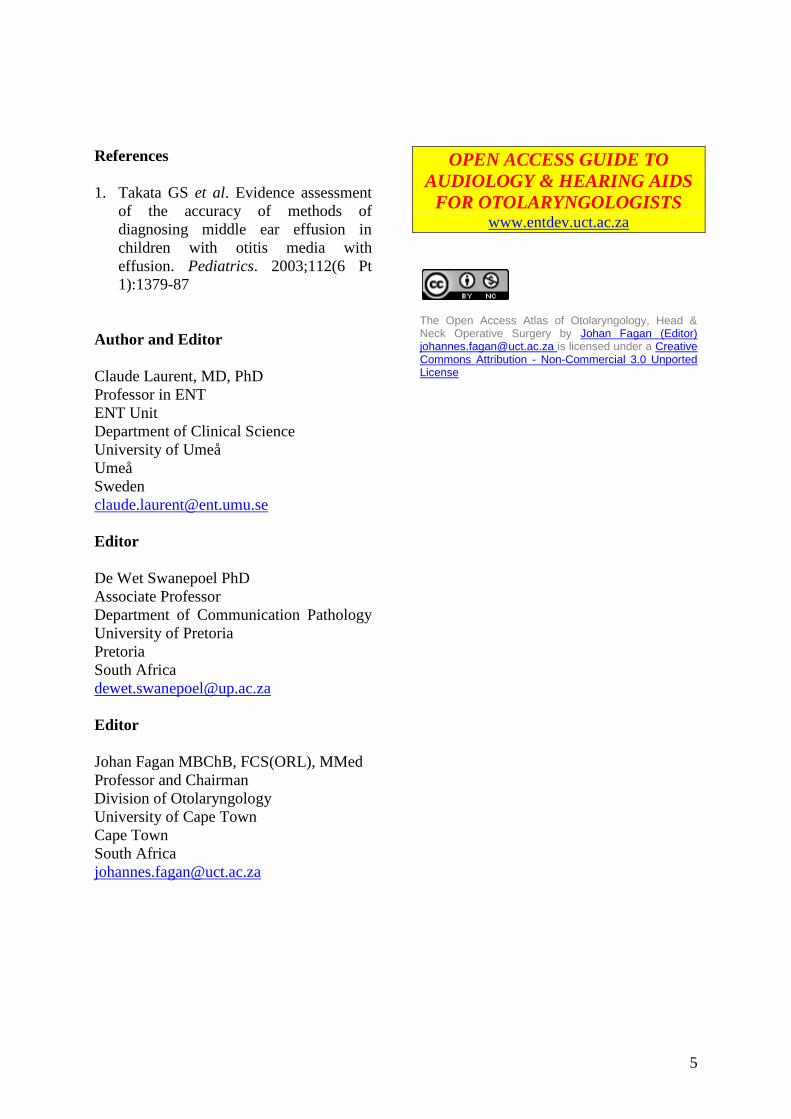
Figure 5: Tympanometer
5
References
1. Takata GS et al. Evidence assessment
of the accuracy of methods of
diagnosing middle ear effusion in
children with otitis media with
effusion. Pediatrics. 2003;112(6 Pt
1):1379-87
Author and Editor
Claude Laurent, MD, PhD
Professor in ENT
ENT Unit
Department of Clinical Science
University of Umeå
Umeå
Sweden
Editor
De Wet Swanepoel PhD
Associate Professor
Department of Communication Pathology
University of Pretoria
Pretoria
South Africa
Editor
Johan Fagan MBChB, FCS(ORL), MMed
Professor and Chairman
Division of Otolaryngology
University of Cape Town
Cape Town
South Africa
OPEN ACCESS GUIDE TO
AUDIOLOGY & HEARING AIDS
FOR OTOLARYNGOLOGISTS www.entdev.uct.ac.za
The Open Access Atlas of Otolaryngology, Head & Neck Operative Surgery by Johan Fagan (Editor) [email protected] is licensed under a Creative Commons Attribution - Non-Commercial 3.0 Unported License